Embed Size (px)
Citation preview

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
GENERAL COMMENTS:
1 The numbers included in the table represent the per centage of
coinsurance responsible of the insured.
2 For official definitions of each code and payments policies
you must refer to the Dentist Participant Manual.
(In the table we only include notes for your refer ences).
NOTES GOVERNMENT HEALTH PLAN
NOTE DEFINITION
SERVICIOS
X Services covered at 100%.
ь It covers only bucal surface .
ç D0160 service code cover only to the Oral and Maxil lofacial Surgeons, (replaces the code D0150) .
D1206 service code cover only to generalists and Pe diatric dentists and is mutually exclusive with the code D1208 (it's one or the other), not both, unti l the age of 5 years.
Þ It covers a maximum of 6 periapical radiographs per policy year between the combination of D0220 and D 0230 codes .
ś D9220 and D9241 services code, are only covered on the Government Health Plan to Oral and Maxillofacia l Surgeons (019 ) with active Sedation certificate.
NOTE DEFINITION
100 No deductible.
110 Deductible per visit of $1.00; for preventive servi ces, (only adults 21+ ) and deductible per visit of $1.00 for restorative services, (applies to all in sured).
300 No deductible.
230 No deductible.
310 Deductible per visit of $1.00; for preventive servi ces, (only adults 21+ ) and deductible per visit of $1.00 for restorative services, (applies to all in sured).
(applies to all insured).
320 Deductible per visit of $2.00; for preventive servi ces, (only adults 21+ ) and deductible per visit of $5.00 for restorative services, (applies to all in sured).
(applies to all insured).
330 Deductible per visit of $3.00; for preventive servi ces, (only adults 21+ ) and deductible per visit of $6.00 for restorative services, (applies to all in sured).
(applies to all insured).
400 Deductible per visit of $3.00; for preventive servi ces, (only adults 21+ ) and deductible per visit of $10.00 for restorative services, (applies to all i nsured).
(applies to all insured).
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CC 100F 110F 300E 230F 310E 320E 330E 400ECODES DESCRIPTION
Maximum Benefit Cover ($)Note 100 110 300 230 310 320 330 400
Deductible N/A $1 / $1 N/A N/A $1 / $1 $2 / $5 $3 / $6 $3 / $10
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluation X X X X X X X XD0140 Limited oral evalation - problem focused X X X X X X X XD0150 Comprehensive oral evaluation X X X X X X X XD0160 Detailed and extensive oral evaluation Xç Xç Xç Xç Xç Xç Xç Xç
ImagingD0210 Intraoral - complete series of radiographic im ages X X X X X X X XD0220 Intraoral - periapical first X Þ X Þ X Þ X Þ X Þ X Þ X Þ X ÞD0230 Additional radiographic image X X X X X X X XD0270 Bitewing - single radiographic images X X X X X X X XD0272 Bitewing - two radiographic images X X X X X X X XD0330 Panoramic radiographic image X X X X X X X X
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adult X X X X X X X XD1120 Prophylaxis - child X X X X X X X X
Topical Fluoride TreatmentD1206 Topical application of fluoride varnish X X X X X X X X D1208 Topical application of fluoride - child X X X X X X X X
SealantD1351 Sealant - per tooth X X X X X X X X
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140 Amalgam - one surface primary or permanent X X X X X X X XD2150 Amalgam - two surface primary or permanent X X X X X X X XD2160 Amalgam - three surface primary or permanent X X X X X X X XD2161 Amalgam - four surface primary or permanent X X X X X X X XD2330 Resin - one surface - anterior (primary or per manent) X X X X X X X XD2331 Resin - two surface - anterior (primary or per manent) X X X X X X X XD2332 Resin - three surface - anterior (primary or p ermanent) X X X X X X X XD2335 Resin - four or more surface - anterior (prima ry or permanent) X X X X X X X XD2391 Resin - one surface posterior (bucal): primary or permanent Xь Xь Xь Xь Xь Xь Xь XьD2930 Prefabricated stainless steel crown – primary tooth X X X X X X X XD2940 Protective restoration X X X X X X X X
COVERS GOVERNMENT HEALTH PLAN
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CC 100F 110F 300E 230F 310E 320E 330E 400ECODES DESCRIPTION
Maximum Benefit Cover ($)Note 100 110 300 230 310 320 330 400
Deductible N/A $1 / $1 N/A N/A $1 / $1 $2 / $5 $3 / $6 $3 / $10
ENDODONTIC
NoteD3120 Pulp cap - indirect (excluding final restorati on) X X X X X X X XD3220 Therapeutic pulpotomy (excluding final restora tion) X X X X X X X XD3221 Pulpal debridement, primary and permanent teet h X X X X X X X XD3310 Endodontic therapy, anterior (excluding final restoration) X X X X X X X XD3320 Endodontic therapy, bicúspid (excluding final resto ration) X X X X X X X X
ORAL SURGERY
NoteExtractions
D7140 Extraction, erupted tooth or exposed root X X X X X X X XD7510 Incision and drainage of abscess- intraoral soft ti ssue X X X X X X X XD7210 Surgical removal of erupted tooth X X X X X X X XD7220 Removal of impacted tooth – soft tissue / part ially bony / completely bony X X X X X X X XD7230 Removal of impacted tooth – soft tissue / part ially bony / completely bony X X X X X X X XD7240 Removal of impacted tooth – soft tissue / part ially bony / completely bony X X X X X X X XD7250 Surgical removal of residual tooth roots X X X X X X X X
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedure X X X X X X X XD9223 Deep Sedation X ś X ś X ś X ś X ś X ś X ś X śD9243 Conscious Sedation X ś X ś X ś X ś X ś X ś X ś X śD9420 Hospital or ambulatory surgical center call X X X X X X X XD9930 Reatment of complications (post-surgical) - unusual circumstances, by report X X X X X X X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
GENERAL COMMENTS:
1 The numbers included in the table represent the per centage of
coinsurance responsible of the insured.
2 For official definitions of each code and payments policies
you must refer to the Dentist Participant Manual.
(In the table we only include notes for your refere nces).
NOTE DEFINITIONMAXIMUM COVERAGE
P Maximum per policy year.
₪ Maximum of $300 per year policy for each service ca tegory; periodontics and prosthodontics
LL Maximum of $450 per arch for general dentist and $ 500 per arch for prosthodontists every 5 years.
@ Maximum of $450 per arch for general dentist ($ 900 for the two arcs per year). Maximum of $ 500 per a rc for prosthodontist (1,000 for the two arch per year)
all prostheses are limited to 1 every 5 years (fix ed and removable).
m Maximum of $500.00 per policy year.
I Maximum of $500 per policy year for Triple-S rate.
™ Maximum of $500 per policy year for periodontics se rvices
Қ Maximum of $500 per policy year for all covered den tal services.
Maximum of $500 per policy year for prosthodontics services , adjustments and repairs.
Maximum of $500 per policy year for the following c ategories restorative, endodontics, oral surgery/su rgical and general adjuntive services.
¤ Maximum of $500 per policy year for the following c ategories; diagnostic, preventive, restorative, end odontics, oral surgery and
adjunctive general services
Maximum of $700 per policy year for all covered den tal services.
ij Maximum of $750 per policy year for all covered den tal services.
Maximum of $750 per policy year for all covered den tal services excluding orthodontics.
# Maximum of $800 between prosthodontics and periodon tics services.
Ϟ Maximum of $800 per policy year for all covered d ental services.
ש Maximum of $800 per policy year for prosthodontics services.
ת Maximum of $800 per policy year for periodontics se rvices .
ΰ Maximum of $800 for all comprehensive, periodontics and prosthodontics services.
Maximum of $800 per policy year, per covered person for all covered dental services except orthodontic s.
æ Maximum of $800 from D2140 to D2335 procedures, D23 91, D3310, D3320, D7140 to D7240, D7250, D7510 and D7286.
ⱴ Maximum of $800 per policy year, per covered person for all services, excluding periodontics and prost hodontics services.
ß Maximum of $850.00 for all services including perio dontics.
ê Maximum of $1,000 per policy year, per covered pers on.
Ψ Maximum of $1,000 for all services excluding prosth odontics
U Maximum of $1,000 for all services excluding orthod ontics.
¶ Maximum of $1,000 for all services excluding period ontics.
ŧ Maximum of $1,000 for all services, including perio dontics.
ΠMaximum of $1,000 per policy year for all prosthodo ntics services.
Ƿ Maximum of $1,000 per policy year for all periodont ics services.
M Maximum of $1,000 per policy year for all covered d ental services.
Maximum of $1,000 per dentures for general dentists or specialist.
Maximum of $1,000 per policy year, per covered pers on including periodontics.
π Maximum of $1,000 for all services excluding prosth odontics, periodontics and orthodontics.
Ø Maximum of $1,000 for all covered dental services f or a period of two years.
§ Maximum of $1,000 per policy year for preventive se rvices, restorative and periodontics.
⋈ Maximum of $1,000 per policy year for all dental se rvices excluding periodontics and prosthodontics.
Æ Maximum of $1,000 per policy year for all dental se rvices excluding periodontics and orthodontics.
ϰ Maximum of $1,000 per policy year for all dental se rvices, excluding prosthodontics,repairs and orthod ontics.
ť Maximum of $1,000 per policy year for all posterior resins and surgical services.
& Maximum of $1,000 per policy year for restorative, endodontics, prosthodontics, oral surgery and gener al adjunctive services.
Maximum of $1,000 per policy year excluding codes; D0120, D0140, D0150, D0220, D0230, D0270, D0272, D1110, D1120, D1206 and D1208.
Ŧ Maximum of $1,000 per policy year, per covered pers on for all services, excluding implant services tha t maintain a separate $ 1,000 cap.
B Maximum of $1,200 per policy year for all dental se rvices covered excluding periodontics and orthodont ics.
♠ Maximum of $1,250 for all services covered excludin g orthodontics.
C Maximum of $1,300 per policy year for all dental se rvices covered excluding periodontics and orthodon tics.
Ø Maximum of $1,300 per policy year for all covered d ental services, excluding orthodontics.
ά Maximum of $1,333 per policy year for all covered d ental services.
Ϡ Maximum of $1,333 per policy year for all prosthodo ntics services covered.
ď Maximum of $1,500, does not apply to diagnostic and preventive services.
Ñ Maximum of $1,500 per policy year for all covered d ental services except orthodontic.
Maximum of $1,500 per policy year for all covered d ental services, excluding periodontics and orthodon tics.
∻ Maximum of $1,500 per policy year for all prosthodo ntics servives covered, excluding all other service s except periodontics and orthodontic services that have their own maximum.
ἆ Maximum of $1,500 and an initial deductible of $ 50 .00 per insured, per policy year, does not apply to services: diagnostic, preventive, restorative, ora l surgery and
endodontics, required by federal law.
ε Maximum of $1,750 for all services excluding orthod ontics and periodontics.
Ü Maximum of $1,750 per policy year for all dental co vered services except orthodontics.
¥ The assignment rate may not exceed the maximum bene fit of $1,750 per policy year established for cover ed dental services except orthodontics.
Њ Maximum of $2,000 for all services excluding orthod ontics
Ψ Maximum of $2,500 per policy yearfor all coveed den tal services except orthodontics.
≈ Maximum benefit does not apply to children under ag e 19 insured for the following categories of servic es: diagnostic, preventive, restorative,
oral surgery and endodontics.
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
RADIOGRAPHS
: Covered service D0330 1 every 6 months
p Covers D0210 or D0330 service, not both, 1 every 2 years.
ϫ Covered D0272, two sets per policy year with iterv al of 6 month.
¢ Covers up to 4 periapical radiographs per policy ye ar between the combination of D0220 and D0230 codes .
ю It covers a maximum of 5 periapicals per policy yea r between the combination of D0220 and D0230 codes.
Þ It covers a maximum of 6 periapicals per policy yea r between the combination of D0220 and D0230 codes .
δ Covers up to 6 periapical radiographs per calendar year between the combination of D0220 and D0230 co des.
⋆ Covers up to 8 periapical radiographs per policy ye ar between the combination of D0220 and D0230 codes .
• It covers a maximum of 13 periapical radiographs ev ery 3 years between the combination of D0220 and D0 230 codes.
WAITING PERIOD OR LIMIT
L 24-month limit
Z One year contract
Has waiting period of one month.
^^ Covers 1 every 6 months for insured persons age 19 and older, with no exclusions.
SERVICES
--- Service not covered.
ᵾ Only covers D3450.
X Services covered at 100%.
« D2954 service is not covered.
» D2952 service is not covered.
Ξ D9950 service is not covered.
Б Only cover code D1510 .
ҩ Only cover code D7471.
ɂ Only cover code D9440.
ᵳ Only cover code D9940.
ª Only cover codes D5730, D5731.
ä Only cover codes D5820, D5821.
Ǿ D2394 service is maintained with 30% coinsurance.
Ш Covered only the group 1-20005 Platinum Select Serv ice.
♣ Only covers dependent children up to age 22.
ᴥ Only cover codes D2510, D2520, D2530, D2542, D2543, D2544.
K Services not covered: D2722, D4270, D4271, D5650, D 5810 and D5811.
T Periodontics and Prosthodontics services DO NOT re quire predetermination.
S Covered service if they are related to covered surg ical procedure.
V Covered service when the extraction of 7 or more pe rmanent teeth is required.
O Services covered if they are related to accident, t he bill requires to be accompanied by a report.
ъ Service code D0160 replaces the D0150 and applies o nly to the specialties of Endodontists (088) and Or al and Maxillofacial Surgeon (019).
Ŀ D3330 service code only covered for the following g roups: Lanco Manufacturing, Lanco / Enco Manufactur ing Corp. and Harris Paints Open Access and applies 25 % coinsurance.
D1206 service code covers only generalists and Pedi atric dentists and is mutually exclusive with code D1208 (it's one or the other), not both, until the age of 5 years.
This code covers the groups that qualify with Obama Federal Reform.
DEDUCTIBLE
º Deductible of $ 5.00 for this categories services ; restorative, endodontics, periodontics, prosthodon tics( adjustments/ repairs) and oral surgery.
ς Deductible of $ 1.00 for this categories services ; diagnostic, restorative, endodontics, periodontics and oral surgery.
≙ Deductible of $25.00 (individual) and $100.00 (fami ly) applies for all covered dental services.
Ď Deductible of $25.00 (individual) and $100.00 (fami ly) applies for all covered dental services, except ; diagnosis and preventive.
₫ Deductible is $ 5.00 per service applies to the fol lowing categories: diagnostic, preventive, restorat ive and endodontic. If the rate is less than the de ductible,
the insured will pay the lesser amount.
Ł Deductible is $ 10.00 per service applies to the fo llowing categories: diagnostic, preventive, restora tive and endodontic. If the rate is less than the d eductible
the insured will pay the lesser amount.
ѓ Deductible is $ 1.00 per service applies to the fol lowing categories: diagnostic, preventive, restorat ive, endodontics. If the rate is less than the dedu ctible,
the insured will pay the lesser amount.
џ Deductible is $ 5.00 per service, it applies to the following categories: diagnostic, preventive, rest orative, endodontics. If the rate is less than the deductible,
the insured will pay the lesser amount.
ά Initial deductible of $ 50.00 per insured, per poli cy year, does not apply to the following services: diagnostic, preventive, restorative, oral surgery and
endodontics, required by federal law.
COINSURANCE
// Coinsurance service will be applied to assested ser vice
± No coinsurance applies to diagnostic, preventive an d restorative services offered in the Integrated Ca re Centers More Health.
ORTHODONTIC
◊ Service covered without age limit.
µ Has waiting period of 12 months.
£ It has a waiting period of 24 months to receive ser vice.
Ə Orthodontic services shall be paid subject to the c harge.
ą Maximum of $ 250 per policy year for orthodontic se rvices.
ề Maximum of $ 1,000 per policy year, per person for orthodontic services.
F Orthodontic services are paid by the covered Major Expense.
Ð This code is part of the initial visit (D8660) of o rthodontic treatment.
Ə1 Orthodontic services will be paid at the cash submi tted by January 1, 2012.
® Breaks habit covered until 14 years of age.
ф Orthodontic Service covered only up to age 18.
∏ Covers orthodontic direct dependents up to age 18.
** Covers direct dependents up to age 19.
* Orthodontics service covered until their 19th birth day.
… Orthodontic Services are limited only to eligible c hildren until the day they turn 19.
ℓ Covers orthodontics only until age 21.
Ω Covers orthodontics until the insured reaches 25 ye ars.
© Only covers dependent children up to age 25.
W It covers the policyholder only orthodontics and de pendents up to age 25.
ő It covers orthodontic service until age 26.
Effective March 1, 2014 the top orthodontic servic e changes to $1,200.
ï Policyholder service covers orthodontics and spouse without age limit and direct dependents up to age 26.
Θ Orthodontic Services "covered only for orthodontic specialists (Orthodontists / 109)," as requested by the group.
OTHER
(P) For periodontists only.
e Apply 20% for specialists.
¤ Optional dependents are eligible.
f This dental coverage has termination date 12/31/201 3.
Y Insured with 65 or more continue to be elegible.
r Covers only through secured to Reimbursement Fee Su bmitted.
^ Please refer to the Participating Dentist Handbook policies relevant to this payment service.
ċ For participants who have agreed to participate in the plan of Government Employees ELA Integrated Car e.
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
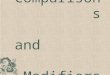
CODES DESCRIPTION D01 D02 D04 D05Maximum Benefit Cover ($) 1000
Note U ≈Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluation X X X XD0140 Limited oral evalation - problem focused X X X XD0150 Comprehensive oral evaluation X X X XD0160 Detailed and extensive oral evaluation --- --- --- ---
D0180 (P) Comprehensive periodontal evaluation --- X X XImaging
D0210 Intraoral - complete series of radiographic im ages X X X XD0220;D0230 Intraoral - periapical first or each add itional radiographic image X X X X
D0240 Intraoral - occlusal radiographic image X X X XD0250 Extra-oral - 2D projection radiographic image --- --- --- ---D0251 Extra-oral - posterior dental radiographic im age --- --- --- ---
D0270;D0272 Bitewing - single or two radiographic im ages X X X XD0273 Bitewings - three radiographic images --- --- --- ---D0274 Bitewings - four radiographic images --- --- --- ---D0277 Vertical bitewings - 7 to 8 radiographic image s --- --- --- ---D0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic image --- --- --- ---D0330 Panoramic radiographic image X X X XD0340 Cephalometric radiographic image --- --- --- ---
OthersD0350 Oral / facial photographic image --- --- --- ---D0415 Collection of microorganisms for culture and sensit ivity --- --- --- ---D0460 Pulp vitality tests X X X XD0470 Diagnostic casts --- --- --- ---D0473 Accession of tissue, gross and microscopic exa mination --- --- --- ---D0999 Unspecified diagnostic procedure, by report X X X X
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adult X X X XD1120 Prophylaxis - child X X X X
Topical Fluoride TreatmentD1206 Topical application of fluoride varnish --- --- --- ---D1208 Topical application of fluoride - child X X X XD1208 Topical application of fluoride - adult (by report) --- X^ X^ X^
SealantD1351 Sealant - per tooth --- X X X
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral --- 20 20 X
D1520 Space maintainer - removable- unilateral --- --- --- ---D1525 Space maintainer - removable bilateral --- --- --- ---D1550 Re - cementation of space maintainer --- --- --- ---D1999 Unspecified preventive procedure, by report X // // X
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanent X X X 25D2330-D2335 Resin - based composite - anterior (prim ary or permanent) X X X 25
D2391 Resin - based composite - posterior (primary o r permanent) 30 30 20 25D2392-D2394 Resin - based composite - posterior (pri mary or permanent) 30 30 20 25D2410-D2430 Gold foil --- --- --- ---D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic --- --- --- ---
D2630 Inlay- porcelain / ceramic - three or more sur faces --- --- --- ---D2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite --- --- --- ---
D2799 Provisional crown --- X X 25D2910 Recement inlay, onlay, or partial coverage restorat ion X X X 25D2915 Recement cast or prefabricated post and core --- X X 25D2920 Recement crown X X X 25D2930 Prefabricated stainless steel crown – primary tooth X X X 25D2931 Prefabricated stainless steel crown – permanen t tooth --- --- --- ---D2932 Prefabricated resin crown --- --- --- ---D2933 Prefabricated stainless steel crown with resin window --- --- --- ---D2940 Protective restoration X X X 25 D2950 Core buildup, including any pins when requir ed --- X X 25D2951 Pin retention - per tooth, in addition to rest oration X X X 25D2960 Labial veneer (resin laminate) – chairside --- --- --- ---
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora tory --- --- --- ---D2980 Crown repair necessitated by restaurative mate rial failure --- X X 25
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure --- --- --- --- D2999 Unspecified restorative procedure, by report X X X 25
January 01, 2016
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTION D01 D02 D04 D05Maximum Benefit Cover ($) 1000
Note U ≈Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration ) X X X 25D3120 Pulp cap - indirect (excluding final restorati on) X X X 25D3220 Therapeutic pulpotomy (excluding final restora tion) X X X 25D3221 Pulpal debridement, primary and permanent teet h X X X 25
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration) X X X 25D3330 Endodontic therapy, molar (excluding final res toration) --- X X 25
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspid X X X 25D3348 Retreatment of previous root canal therapy - m olar --- X X 25
D3351-D3353 Apexification / recalcification - inicia l / interim / final visit --- --- --- ---D3355-D3357 Pulpal regeneration - inicial / interim / final visit --- --- --- ---D3410;D3421 Apicoectomy - anterior / bicuspid (first root) X X X 25D3425;D3426 Apicoectomy - molar - first root / each additional root X X X 25
D3430 Retrograde filling – per root X X X 25D3450;D3920 Root amputation - per root / Hemisection --- --- --- ---
D3999 Unspecified endodontic procedure, by report X X X 25BASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosis --- X 20 XD4910 Periodontal maintenance --- X 20 X
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibular X X X XD5421;D5422 Adjust partial denture – maxillary / man dibular X X X X
D5510 Repair broken complete denture base X X X XD5520 Replace missing or broken teeth-complete dentu re (each tooth) X X X XD5610 Repair resin denture base X X X XD5620 Repair cast framework --- --- --- ---D5630 Repair or replace broken clasp X X X XD5640 Replace broken teeth – per tooth X X X X
D5650;D5660 Add tooth / clasp to existing partial de nture X X X XD5710-D5721 Rebase: complete / partial denture --- 50 50 50D5730-D5761 Reline:complete / partial denture --- 50 50 50D5850;D5851 Tissue conditioning, maxillary / mandibu lar --- --- --- ---
D6930 Recement fixed partial denture X X X XD6980 Fixed partial denture repair necessitated by restor ative material failure --- X X X
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous tooth --- --- --- ---D7140 Extraction, erupted tooth or exposed root X X X 25D7510 Incision and drainage of abscess- intraoral soft ti ssue X X X 25
CATEGORY III
MAYOR SERVICES PERIODONTICS
Note ULimit per policy year ($) --- 1000 --- 1000Periodontics deductible ($) --- --- --- ---
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teeth --- X 20 XD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth --- X 20 X
D4245 Apically positioned flap --- X 20 XD4249 Clinical crown lengthening - hard tissue --- X 20 X
D4260;D4261 Osseous surgery --- X 20 XD4263;D4264 Bone replacement graft -first / addition al site in quadrant --- X 20 XD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site --- X 20 XD4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth --- X 20 X
D4277 Free soft tissue graft procedure - first tooth or edentulous tooth --- X 20 XD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous tooth --- --- --- - --D4320 Provisional splinting - intracoronal --- --- --- --- D4321 Provisional splinting - extracoronal --- X 20 X
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrant --- X 20 XD4920 Unscheduled dressing change (by someone other than treating dentist or their staff) --- --- --- ---D4999 Unspecified periodontal procedure, by report --- X 20 X
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect) --- --- --- ---D2720 Crown - resin with high noble metal --- 57 50 50D2722 Crown - resin with noble metal --- 50 50 50D2740 Crown - porcelain / ceramic substrate --- 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTION D01 D02 D04 D05Maximum Benefit Cover ($) 1000
Note U ≈Deductible
D2750 Crown - porcelain fused to high noble metal --- 57 50 50D2751 Crown - porcelain fused to predominantly base metal --- 50 50 50D2752 Crown - porcelain fused to noble metal --- 50 50 50D2780 Crown - ¾ cast high noble metal --- 57 50 50
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramic --- 50 50 50D2790 Crown - full cast high noble metal --- 57 50 50D2791 Crown - full cast predominantly base metal --- 50 50 50D2792 Crown - full cast noble metal --- 50 50 50D2794 Crown - titanium --- 57 50 50
D2952;D2954 Post and core --- 50 50 50D2975 Coping --- --- --- ---
D5110;D5120 Complete denture - maxilary / mandibular --- 50 50 50D5130;D5140 Immediate denture - maxilary / mandibula r --- 50 50 50D5211;D5212 Partial denture - resin base - maxilary / mandibular --- 50 50 50D5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibular --- 50 50 50D5221;D5222 Immediate partial denture-resin base - m axilary / mandibular --- --- --- ---D5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r --- --- --- ---
D5281 Removable unilateral partial denture - one pie ce cast metal --- 50 50 50D5810-D5821 Interim complete and partial denture - m axilary / mandibular --- --- --- ---D5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar --- --- --- ---
D5862 Precision attachment, by report --- --- --- ---D5899 Unspecified removable prosthodontic procedure , by report X 50 50 50D6058 Abutment supported porcelain / ceramic crown --- 50 50 50D6059 Abutment supported porcelain fused to metal cr own (high noble metal) --- 57 50 50D6060 Abutment supported porcelain fused to metal cr own predominantly base metal --- --- --- ---D6061 Abutment supported porcelain fused to metal cr own (noble metal) --- 50 50 50D6062 Abutment supported cast metal crown (high nobl e metal) --- 57 50 50D6063 Abutment supprted cast metal crown (predominan tly base metal) --- --- --- ---D6064 Abutment supported cast metal crown (noble met al) --- 50 50 50D6065 Implant supported porcelain / ceramic crown --- 50 50 50D6066 Implant supported porcelain fused to metal cro wn --- 57 50 50D6067 Implant supported metal crown --- 57 50 50D6068 Abutment supported retainer for porcelain/cera mic FPD --- 50 50 50D6075 Implant supported retainer for ceramic FPD --- 50 50 50D6076 Implant supported retainer for porcelain fused to metal FPD --- 57 50 50D6077 Implant supported retainer for cast metal FPD --- 57 50 50D6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal) --- 57 50 50D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal) --- 50 50 50D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal) --- 50 50 50D6072 Abutment supported retainer for cast metal FPD (high noble metal) --- 57 50 50D6073 Abutment supported retainer for cast metal FPD (predominantly base metal) --- 50 50 50D6074 Abutment supported retainer for cast metal FPD (noble metal) --- 50 50 50D6210 Pontic - cast high noble metal --- 57 50 50D6211 Pontic - cast predominantly base metal --- 50 50 50D6212 Pontic - cast noble metal --- 50 50 50D6214 Pontic - titanium --- 57 50 50D6240 Pontic - porcelain fused to high noble metal --- 57 50 50D6241 Pontic - porcelain fused to predominantly base metal --- 50 50 50D6242 Pontic - porcelain fused to noble metal --- 50 50 50D6245 Pontic - porcelain / ceramic --- --- --- ---D6250 Pontic - resin with high noble metal --- 57 50 50
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metal --- --- --- ---D6253 Provisional pontic --- --- --- ---D6545 Retainer - cast metal for resin bonded fixed p rosthesis --- 50 50 50D6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis --- --- --- ---
D6600-D6605 Inlays: porcelain;metalic --- --- --- ---D6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfaces --- --- 50 50D6608-D6615 Onlays:porcelain;metalic --- --- --- ---D6624;D6634 Inlays / onlays - titanium --- --- --- ---
D6710 Crown - indirect resin based composite --- --- --- ---D6720 Crown - resin with high noble metal --- 57 50 50
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metal --- --- --- ---D6740 Crown - porcelain / ceramic --- --- --- ---D6750 Crown - porcelain fused to high noble metal --- 57 50 50D6751 Crown - porcelain fused to predominantly base metal --- 50 50 50D6752 Crown - porcelain fused to noble metal --- 50 50 50D6780 Crown - ¾ cast high noble metal --- --- --- ---
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metal --- 50 50 50D6783 Crown - ¾ porcelain / ceramic --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTION D01 D02 D04 D05Maximum Benefit Cover ($) 1000
Note U ≈Deductible
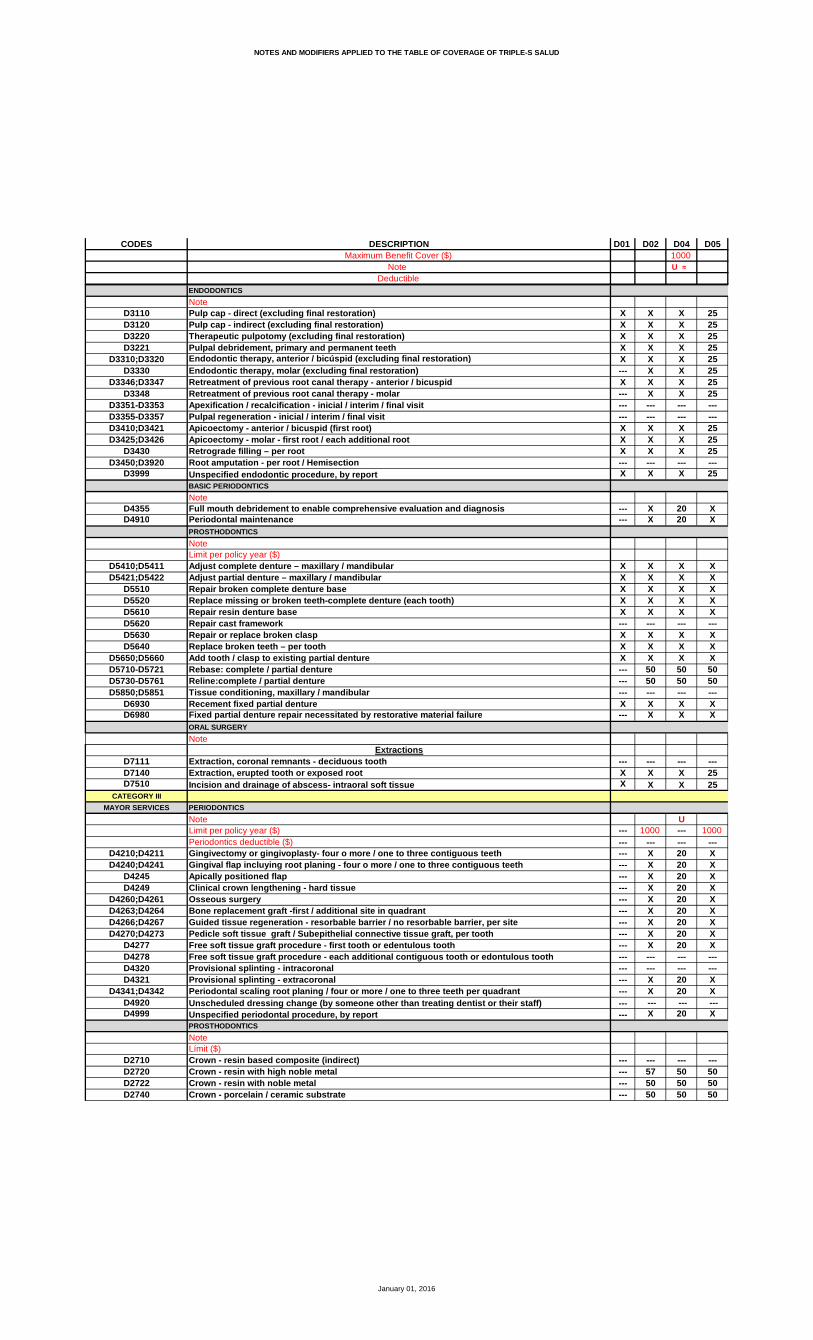
D6790 Crown - full cast high noble metal --- 57 50 50D6791;D6792 Crown - full cast predominantly base metal / noble metal --- 50 50 50
D6794 Crown - titanium --- 57 50 50D6920 Connector bar --- --- --- ---D6940 Stress breaker --- --- --- ---D6950 Precision attachment --- --- --- ---D6999 Unspecified, fixed prosthodontic procedure, by repo rt --- 50 50 50
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection --- --- --- ---D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis --- --- --- ---D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator --- --- --- ---
D5986 Fluoride gel carrier --- --- --- ---IMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgery --- --- --- ---ORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth X 30 20 25
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bony X 30 20 25D7241 Removal of impacted tooth – completely bony, w ith unusual surgical complication --- --- --- ---D7250 Surgical removal of residual tooth roots X 30 20 25D7260 Oroantral fistula closure --- --- --- ---D7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced tooth --- --- --- -- -D7272 Tooth transplantation --- --- --- --- D7280 Surgical access of an unerupted tooth --- 30 20 25 D7283 Placement of device to facilitate eruption of impac ted tooth --- 30 20 ---D7285 Biopsy of oral tissue - hard (bone, tooth) --- --- --- ---D7286 Biopsy of oral tissue - soft X 30 20 25D7290 Surgical repositioning of teeth --- --- --- ---D7291 Transseptal fiberotomy/supra crestal fiberotomy, by report --- --- --- ---
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractions --- 50 50 5 0D7340 Vestibuloplasty-ridge extension (secondary epi thelialization) --- --- --- ---D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….) --- --- --- ---
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularis --- --- --- ---D7520 Incision and drainage of abscess – extraoral s oft tissue --- --- --- ---D7550 Partial ostectomy /Sequestrectomy for removal of non-vital bone --- --- --- ---D7880 Occlusal orthotic device, by report --- --- --- ---D7881 Occlusal orthotic device adjustment --- --- --- ---D7910 Suture of recent small wounds up to 5 cm --- --- --- ---D7953 Bone replacement graft for ridge preservation – per site --- --- --- ---D7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedure --- --- --- ---D7970 Excision of hyperplastic tissue - per arch --- --- --- ---D7971 Excision of pericoronal gingiva X 30 20 25D7999 Unspecified oral surgery procedure, by report X 30 20 25
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedure --- --- --- ---D9230 Inhalation of nitrous oxide / analgesia, anxio lysis --- --- --- ---D9243 Intravenous moderate (conscious) sedation/anal gesia --- --- --- ---D9310 Consultation - diagnostic service provided by dentist or physician --- --- --- ---D9410 House / extended care facility call --- --- --- ---D9420 Hospital or ambulatory surgical center call --- X X X
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours) --- --- --- ---D9630 Other drugs and / or medicaments, by report X X X 25D9910 Application of desensitizing medicament X X X 25D9930 Reatment of complications (post-surgical) - un usual circumstances, by report X X X 25
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted case --- --- --- ---D9943 Occlusal guard adjustment --- --- --- ---
D9951;D9952 Occlusal adjustment - limited / complete --- X X XD9973;D9974 External / Internal bleaching – per tooth --- --- --- ---
D9999 Unspecified adjunctive procedure – by report X X X XORTHODONTIC
Note --- Ə1 ** Ə ---D8210-D8690 Orthodontic Services --- X 50 ---
D8691 Repair of orthodontic appliance --- --- --- ---Lifetime limit ($) --- 1000 1500 ---Límit per policy year ($) --- --- --- ---Deductible Orthodontics ($) --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
D06 D07 D08 D10 D12 D20
X X Z X X 20 XX --- X X 20 XX X X X 20 X--- --- --- --- --- ---X --- --- X 20 X
X --- --- X 20 XX --- X δ X 20 X ÞX --- --- X 20 ------ --- --- --- --- ------ --- --- --- --- ---X --- X X 20 X--- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ---X --- 30 X 20 X--- --- --- --- --- ---
------ --- --- --- --- ------ --- --- --- --- ---X --- --- X 20 X--- --- --- --- --- ------ --- --- --- --- ---X --- 30 X 20 X
X X X X 20 XX X X X 20 X
--- --- --- --- --- ---X --- X X 20 X--- --- 30^ --- 20^ X^
--- --- --- --- 20 20
X --- --- 50 20 20--- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ---X X // // 20 //
X --- 30 X 30 20X --- 30 X 30 2030 --- 30 30 30 3030 --- 30 30 30 30--- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ---X --- --- X 30 ---X --- --- X 30 ---X --- --- X 30 ---X --- --- X 30 ---X --- --- X 30 ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ---X --- 30 X 30 20X --- --- X 30 ---X --- 30 X 30 ------ --- --- --- --- ------ --- --- --- --- ---X --- --- X 30 ------ --- --- --- --- ---X --- 30 X 30 20
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
D06 D07 D08 D10 D12 D20
X --- 30 X 30 ---X --- 30 X 30 20X --- --- X 30 20X --- 30 X 30 20X --- --- X 30 20X --- --- X 30 20X --- --- X 30 20X --- --- X 30 ------ --- --- --- --- ------ --- --- --- --- ---X --- --- X 30 ---X --- --- X --- ---X --- --- X 30 ------ --- --- --- --- ---X --- --- X 30 20
X --- --- 50 30 ---X --- --- 50 30 20
X --- --- X X ---X --- --- X X 40X --- --- X X 40X --- --- X X ---X --- --- X X 40--- --- --- --- --- ---X --- --- X X ---X --- --- X X 40X --- --- X X ---X --- --- 50 50 40X --- --- 50 50 40--- --- --- --- --- ---X --- --- X X ---X --- --- X X ---
--- --- --- --- --- ---X X 30 X X 20X --- 30 X X 20
1000 --- --- 800 1000 ---50 --- --- 50 --- ---X --- --- 50 30 ---X --- --- 50 30 ---X --- --- 50 30 ---X --- --- 50 30 ---X --- --- 50 30 ---X --- --- 50 30 ---X --- --- 50 30 ---X --- --- 50 30 ---X --- --- 50 30 ------ --- --- --- --- ------ --- --- --- 30 ---X --- --- 50 30 ---X --- --- 50 30 20--- --- --- --- 30 ---X --- --- 50 30 ---
1000--- --- --- --- --- ---X --- --- --- 50 ---X --- --- 50 50 ---X --- --- 50 50 ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
D06 D07 D08 D10 D12 D20
X --- --- --- 50 ---X --- --- 50 50 ---X --- --- 50 50 ---X --- --- --- 50 ---X --- --- 50 50 ---X --- --- --- 50 ---X --- --- 50 50 ---X --- --- 50 50 ---X --- --- --- 50 ---X --- --- 50 50 ------ --- --- --- --- ---X --- --- 50 50 40X --- --- 50 50 ---X --- --- 50 50 ---X --- --- 50 50 40--- --- --- --- --- ------ --- --- --- --- ---X --- --- 50 50 ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ---X --- --- 50 50 40--- --- --- 50 50 ------ --- --- --- 50 ------ --- --- --- --- ------ --- --- 50 50 ------ --- --- --- 50 ------ --- --- --- --- ------ --- --- 50 50 ------ --- --- 50 50 ------ --- --- --- 50 ------ --- --- --- 50 ------ --- --- 50 50 ------ --- --- 50 50 ------ --- --- --- 50 ------ --- --- --- 50 ------ --- --- --- 50 ------ --- --- 50 50 ------ --- --- 50 50 ------ --- --- --- 50 ------ --- --- 50 50 ------ --- --- 50 50 ---X --- --- --- 50 ---X --- --- 50 50 ---X --- --- 50 50 ---X --- --- --- 50 ---X --- --- --- 50 ---X --- --- 50 50 ---X --- --- 50 50 ------ --- --- --- --- ---X --- --- --- 50 ------ --- --- --- --- ------ --- --- --- --- ---X --- --- 50 50 ------ --- --- --- --- ------ --- --- --- --- ---X --- --- 50 50 ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ---X --- --- --- 50 ------ --- --- --- --- ------ --- --- --- --- ---X --- --- --- 50 ---X --- --- 50 50 ---X --- --- 50 50 ------ --- --- --- --- ---X --- --- 50 50 ------ --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
D06 D07 D08 D10 D12 D20
X --- --- --- 50 ---X --- --- 50 50 ---X --- --- --- 50 ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ---X --- --- 50 50 ---
--- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ---
--- --- --- 50 --- ---
X --- 30 X 30 20X --- 30 X 30 20--- --- --- --- --- ---X --- 30 X 30 20--- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ---X --- --- X --- ---X --- --- X --- ------ --- --- --- --- ---X --- --- X 30 ------ --- --- --- --- ------ --- --- --- --- ---X --- --- 50 50 ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- X --- ------ --- --- --- --- ------ --- --- --- --- ---X --- --- X 30 ---X --- 30 X 30 20
--- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- 30 --- X 20--- --- --- --- --- ---X --- --- X X ---X --- 30 X X 20X --- 30 X X 20--- --- --- --- --- ------ --- --- --- --- ---X --- --- X --- ------ --- --- --- --- ---X --- 30 X X 20
Ə1 --- --- ◊ Ə --- ---X --- --- 50 --- ------ --- --- --- --- ---
1000 --- --- 3000 --- ------ --- --- --- --- ------ --- --- 50 --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
D21 D22 D24 D26 D27 D28 D291000 1500
M ≈ Ñ ≈
X X X X X X X ZX X X X X X ---X X X X X X X--- --- --- --- --- --- ---X X X X X X ---
X X X X X X ---X X X X X X ---X X X X X X ------ --- --- --- --- ------ --- --- --- --- --- ---X X X X X X ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X ------ --- --- --- --- --- ---
------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X ---
X X X X X X XX X X X X X X
--- --- --- X X --- ---X X X X X X ---
X^ X^ X^ X^ X^ X^ ---
X X X X X X ---
20 20 X X X 30 ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// // X X X // X
X X X 20 20 25 ---X X X 20 20 25 ---30 20 30 20 20 25 ---30 20 30 20 20 25 --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X --- 20 25 ---X X X 20 20 25 ---X X X --- 20 25 ---X X X 20 20 25 ---X X X 20 20 25 ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X 20 20 25 ---X X X --- 20 25 ---X X X 20 20 25 ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X --- 20 25 ------ --- --- --- --- --- ---X X X 20 20 25 ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
D21 D22 D24 D26 D27 D28 D291000 1500
M ≈ Ñ ≈
X 50 30 20 20 25 ---X 50 30 20 20 25 ---X 50 30 20 20 25 ---X 50 30 20 20 25 ---X 50 30 20 20 25 ---X 50 30 20 20 25 ---X 50 30 20 20 25 ---X 50 30 20 20 25 ------ --- --- --- --- --- ------ --- --- --- --- --- ---X 50 30 20 20 25 ---X 50 30 20 20 25 ---X 50 30 20 20 25 ------ --- --- --- --- --- ---X 50 30 20 20 25 ---
X 50 30 20 20 50 ---X 50 30 20 20 50 ---
X X X 30 X X ---X X X 30 X X ---X X X 30 X X ---X X X 30 X X ---X X X 30 X X ------ --- --- --- --- --- ---X X X 30 X X ---X X X 30 X X ---X X X 30 X X ---50 50 50 --- 50 50 ---50 50 50 --- 50 50 ------ --- --- --- --- --- ---X X X 30 X X ---X X X --- X X ---
--- --- --- --- --- --- ---X 50 X 20 20 X 15X 50 X 20 20 X ---
M Ñ1000 1000 1000 --- --- 800 ---
--- --- --- --- --- --- ---X 50 30 20 20 50 ---X 50 30 20 20 50 ---X 50 30 20 20 50 ---X 50 30 20 20 50 ---X 50 30 20 20 50 ---X 50 30 20 20 50 ---X 50 30 20 20 50 ---X 50 30 20 20 50 ---X 50 30 20 20 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ---X 50 30 20 20 50 ---X 50 30 20 20 50 ---
--- --- --- --- --- --- ---X 50 30 20 20 50 ---
800--- --- --- --- --- --- ---57 50 50 --- 50 50 ---50 50 50 --- 50 50 ---50 50 50 --- 50 50 ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
D21 D22 D24 D26 D27 D28 D291000 1500
M ≈ Ñ ≈
57 50 50 --- 50 50 ---50 50 50 --- 50 50 ---50 50 50 --- 50 50 ---57 50 50 --- 50 50 ---50 50 50 --- 50 50 ---57 50 50 --- 50 50 ---50 50 50 --- 50 50 ---50 50 50 --- 50 50 ---57 50 50 --- 50 50 ---50 50 50 --- 50 50 --- --- --- --- --- --- --- ---50 50 50 --- 50 50 ---50 50 50 --- 50 50 ---50 50 50 --- 50 50 ---50 50 50 --- 50 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 30 50 50 ---50 50 50 --- --- 50 ---57 50 50 --- --- 50 ------ --- --- --- --- --- ---50 50 50 --- --- 50 ---57 50 50 --- --- 50 ------ --- --- --- --- --- ---50 50 50 --- --- 50 ---50 50 50 --- --- 50 ---57 50 50 --- --- 50 ---57 50 50 --- --- 50 ---50 50 50 --- --- 50 ---50 50 50 --- --- 50 ---57 50 50 --- --- 50 ---57 50 50 --- --- 50 ---57 50 50 --- --- 50 ---50 50 50 --- --- 50 ---50 50 50 --- --- 50 ---57 50 50 --- --- 50 ---50 50 50 --- --- 50 ---50 50 50 --- --- 50 ---57 50 50 --- 50 50 ---50 50 50 --- 50 50 ---50 50 50 --- 50 50 ---57 50 50 --- 50 50 ---57 50 50 --- 50 50 ---50 50 50 --- 50 50 ---50 50 50 --- 50 50 ------ --- --- --- --- --- ---57 50 50 --- 50 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- 50 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- 50 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---57 50 50 --- 50 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ---57 50 50 --- 50 50 ---50 50 50 --- 50 50 ---50 50 50 --- 50 50 ------ --- --- --- --- --- ---50 50 50 --- 50 50 ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
D21 D22 D24 D26 D27 D28 D291000 1500
M ≈ Ñ ≈
57 50 50 --- 50 50 ---50 50 50 --- 50 50 ---57 50 50 --- 50 50 ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- 50 50 ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
X 50 30 20 20 30 ---X 50 30 20 20 30 ------ --- --- 20 20 --- ---X 50 30 20 20 30 ------ --- --- 20 20 --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 50 30 20 20 30 ---30 50 30 --- 20 30 ------ --- --- --- --- --- ---30 50 30 20 20 30 ------ --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 50 --- 50 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- 20 20 --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- 20 20 --- ------ --- --- --- --- --- ---30 50 30 20 20 30 ---30 50 30 20 20 30 ---
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X ---
--- --- --- --- --- --- ---X X X X X X ---X X X X X X ---X X X X X X ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X --- X X ------ --- --- --- --- --- ---X X X X X X ---
Ə1 ф Ə1 Ə1 --- Ə Ə1 ---X X 50 --- 50 50 ------ --- --- --- --- --- ---
1250 1500 1000 --- 1500 --- ------ --- --- --- --- 1500 ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
D30 D31 D331000
Ø
X X XX X XX X X--- --- ---X X X
X X XX X X ÞX --- X--- --- ------ --- ---X X X--- --- ------ --- ------ --- --- --- --- ---X X X--- --- ---
--- --- --- --- --- ---X --- X--- --- --- --- --- ---X X X
X X XX --- X
--- --- ---X X X
X^ --- X^
X X X
20 X X--- --- ------ --- ------ --- ---// X X
20 X X20 X X20 30 X20 30 X --- --- --- --- --- ------ --- --- --- --- ---20 --- X20 --- X20 --- ---20 --- X20 --- X--- --- ------ --- ------ --- ---20 X X20 --- ---20 X X--- --- --- --- --- ---20 --- ------ --- ---20 // X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
D30 D31 D331000
Ø
X X XX X XX --- XX X XX X XX --- XX --- XX --- ------ --- ------ --- ---X --- XX --- ---X --- X--- --- ---X X X
X X ---X X X
X --- XX --- XX --- X êX --- X êX --- X ê--- --- ---X --- XX --- XX --- X ê50 --- X50 --- X--- --- ---X --- X êX --- X ê
--- --- ---X X XX X X
1500 --- 800--- --- ---X X ---X X ---X --- ---X --- ---X X XX --- ---X --- ---X --- ---X --- ------ --- ------ --- ---X --- ---X X X
--- --- ---X X ---
@
--- --- ---50 --- ---50 --- ---50 --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
D30 D31 D331000
Ø
50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- --- --- --- ---50 --- X50 --- ---50 --- X50 --- X--- --- ------ --- ---50 --- --- --- --- --- --- --- ------ --- ---50 --- X50 --- ---50 --- ------ --- ---50 --- ---50 --- ------ --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 --- ------ --- ---50 --- ------ --- ------ --- ---50 --- ------ --- ------ --- ---50 --- ------ --- ------ --- ------ --- ---50 --- ------ --- ------ --- ---50 --- ---50 --- ---50 --- ------ --- ---50 --- ------ --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
D30 D31 D331000
Ø
50 --- ---50 --- ---50 --- ------ --- --- --- --- ------ --- ---50 --- ---
--- --- --- --- --- --- --- --- --- --- --- ---
--- --- ---
30 30 X30 30 X--- --- ---30 --- X--- --- ------ --- --- --- --- ---30 --- X30 --- ------ --- ---30 30 X--- --- --- --- --- ---50 --- ------ --- ------ --- ------ --- ------ --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- ------ --- ---30 30 X30 30 X
--- --- ------ --- ------ --- ------ --- --- --- --- ---X --- X
--- --- ---X --- XX X XX --- X--- --- ------ --- ---X --- ------ --- ---X X X
Ə1 --- ---X --- ------ --- ---
1500 --- ------ --- ------ --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
D34 D36 D37 D38 D40 D41 D42 1000
Æ ≈ ♣
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- X ъ ------ X X X X X X
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- X ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- X ------ --- --- --- --- X ------ --- --- --- --- X --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- X Ð ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X --- X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
--- X --- --- --- --- ---X X X X X X X
X^ --- X^ X^ X^ X^ ---
X X X X X X X
20 20 20 X 50 X 50--- --- --- --- --- X ------ --- --- --- --- X ------ --- --- --- --- --- ---// // // X // X //
X X X 30 X 30 XX 20 X 30 X 30 X30 20 30 30 30 30 3030 20 30 30 30 30 30 --- --- --- --- --- --- --- --- --- --- --- --- 60 ᴥ ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X 30 XX X X X X 30 XX X --- X X 30 XX X X X X 30 XX X X X X 30 X--- --- --- --- --- 30 ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X 30 XX X --- X X 30 XX X X X X 30 X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X --- X X 30 X--- --- --- --- --- 60 ---X X X X X 30 X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
D34 D36 D37 D38 D40 D41 D42 1000
Æ ≈ ♣
X X X 30 X 30 XX X X 30 X 30 XX X X 30 X 30 XX X X 30 X 30 XX X X 30 X 30 XX X --- 30 X 30 XX X X 30 X 30 XX X --- 30 X 30 X--- --- --- --- --- 30 ------ --- --- --- --- --- ---X X X 30 X 30 X--- X --- 30 X 30 XX X X 30 X 30 X--- --- --- --- --- 30 ᵾ ---X X X 30 X 30 X
--- X --- 30 X 60 50--- X 50 30 X 30 50
X 50 X X X 30 XX 50 X X X 30 XX 50 X X X 30 XX 50 X X X 30 XX 50 X X X 30 X--- --- --- --- --- 30 ---X 50 X X X 30 XX 50 X X X 30 XX 50 X X X 30 X50 50 --- 50 50 30 5050 50 --- 50 50 30 50--- --- --- --- --- 30 ---X 50 X X X 30 XX --- X X X 30 X
--- --- --- --- --- 30 ---X 20 X X X 30 XX 20 X X X 30 X
#--- 800 1000 1250 800 --- 800--- --- --- --- 50 --- 50--- X 50 30 X 60 50--- X 50 30 X 60 50--- X 50 30 X 60 50--- X 50 30 X 60 50--- X 50 30 X 60 50--- X 50 30 X 60 50--- X 50 30 X 60 50--- X 50 30 X 60 50--- X 50 30 X 60 50--- --- --- --- --- 60 ------ --- --- --- --- --- ------ X 50 30 X 60 50--- X 50 30 X 30 50 --- --- --- --- --- --- ------ X 50 30 X // 50
#800
--- --- --- --- --- --- ---57 50 --- 50 57 60 5750 50 --- 50 50 60 5050 50 --- 50 50 60 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
D34 D36 D37 D38 D40 D41 D42 1000
Æ ≈ ♣
57 50 --- 50 57 60 5750 50 --- 50 50 60 5050 50 --- 50 50 60 5057 50 --- 50 57 60 5750 50 --- 50 50 60 5057 50 --- 50 57 60 5750 50 --- 50 50 60 5050 50 --- 50 50 60 5057 50 --- 50 57 60 5750 50 --- 50 50 30 50 --- --- --- --- --- --- ---50 50 --- 50 50 60 5050 50 --- 50 50 60 5050 50 --- 50 50 60 5050 50 --- 50 50 60 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 60 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 X 50 50 60 5050 --- --- 50 50 60 ---57 --- --- 50 57 60 ------ --- --- --- --- 60 ---50 --- --- 50 50 60 ---57 --- --- 50 57 60 ------ --- --- --- --- 60 ---50 --- --- 50 50 60 ---50 --- --- 50 50 60 ---57 --- --- 50 57 60 ---57 --- --- 50 57 60 ---50 --- --- 50 50 60 ---50 --- --- 50 50 --- ---57 --- --- 50 57 --- ---57 --- --- 50 57 60 ---57 --- --- 50 57 60 ---50 --- --- 50 50 60 ---50 --- --- 50 50 60 ---57 --- --- 50 57 60 ---50 --- --- 50 50 60 ---50 --- --- 50 50 60 ---57 50 --- 50 57 60 5750 50 --- 50 50 --- 5050 50 --- 50 50 60 5057 50 --- 50 57 --- 5757 50 --- 50 57 60 5750 50 --- 50 50 60 5050 50 --- 50 50 60 50--- --- --- --- --- 60 ---57 50 --- 50 57 60 57--- --- --- --- --- 60 ------ --- --- --- --- 60 ---50 50 --- 50 50 60 50--- --- --- --- --- 60 ------ --- --- --- --- 60 ---50 50 --- 50 50 60 50--- --- --- --- --- 60 ------ --- --- --- --- 60 ------ --- --- --- --- 60 ---57 50 --- 50 57 60 57--- --- --- --- --- 60 ------ --- --- --- --- 60 ---57 50 --- 50 57 60 5750 50 --- 50 50 60 5050 50 --- 50 50 60 50--- --- --- --- --- 60 ---50 50 --- 50 50 60 50--- --- --- --- --- 60 ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
D34 D36 D37 D38 D40 D41 D42 1000
Æ ≈ ♣
57 50 --- 50 57 60 5750 50 --- 50 50 60 5057 50 --- 50 57 60 57--- --- --- --- --- 60 --- --- --- --- --- --- 60 ------ --- --- --- --- 60 ---50 50 --- 50 50 60 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- 60 ---
30 20 30 30 30 30 X30 20 30 30 30 30 X--- --- --- --- --- 30 ---30 20 30 30 30 30 X--- --- --- --- --- --- ------ --- --- --- --- 30 --- --- --- --- --- --- --- ------ 20 30 30 --- 30 X--- 20 --- 30 --- 30 X--- --- --- --- --- --- ---30 20 30 30 30 30 X--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 --- --- 50 50 30 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- 30 ҩ ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 30 --- --- --- --- --- --- 30 ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 20 30 30 30 30 X30 20 30 30 30 30 X
--- --- --- --- --- X ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- X --- --- --- --- --- --- --- ---X --- --- X --- 30 ---
--- --- --- --- --- 60 ɂ ---X X X X X --- XX X X X X 30 XX X X X X 30 X--- X --- --- --- 60 ᵳ ------ --- --- --- --- --- ------ X --- X X --- X --- --- --- --- --- --- ---X X X X X // X
--- * Ə1 --- --- --- µ Ə ő Ə1--- X --- --- --- 50 50 --- --- --- --- --- --- ------ 1000 --- --- --- 2000 1050--- --- --- --- --- --- ------ --- --- --- --- --- 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
D43 D45 D47 D48 D49 D50 D511750
ε ≈ f
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
X --- --- --- --- --- ---X X X X X X X
X^ X^ --- X^ --- X^ X^
X X X X X X X
20 X 50 20 50 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// X // --- // // //
30 20 X X X X 20X 20 X X X X 2030 20 30 30 30 30 2030 20 30 30 30 30 20 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X 20 X X X X 20X 20 X X X X 20X 20 X X X X 20X 20 X X X X 20X 20 X X X X 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X 20 X X X X 20X 20 X X X X 20X 20 X X X X 20--- --- --- --- --- --- --- --- --- --- --- --- --- ---X 20 X X X X 20--- --- --- --- --- --- ---X 20 X X X X 20
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
D43 D45 D47 D48 D49 D50 D511750
ε ≈ f
40 20 X X X X 2040 20 X X X X 2040 20 X X X X 2040 20 X X X X 2040 20 X X X X 2040 20 X 20 X X ---40 20 X X X X 2040 20 X X X X ------ --- --- --- --- --- ------ --- --- --- --- --- ---40 20 X X X X 2040 20 X X X X ---40 20 X X X X 20--- --- --- --- --- --- ---40 20 X X X X 20
50 50 X X X 30 2050 50 X X X 30 20
X X X X X X XX X X X X X XX X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X50 50 50 X 50 50 5050 50 50 X 50 50 50--- --- --- --- --- --- ---X X X X X X XX X X X X X X
--- --- --- --- --- --- ---30 20 X 20 X X 2030 20 X 20 X X 20
1750 1000 800 1000 800 1000 1000--- --- --- --- 50 --- ---50 50 X X X 30 2050 50 X X X 30 2050 50 X X X 30 2050 50 X X X 30 2050 50 X X X 30 2050 50 X X X 30 2050 50 X X X 30 2050 50 X X X 30 2050 50 X X X 30 20--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 X X X 30 2050 50 X X X 30 20 --- --- --- --- --- --- ---50 50 X X X 30 20
--- --- --- --- --- --- ---57 50 57 57 50 57 5050 50 50 50 50 50 5050 50 50 50 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
D43 D45 D47 D48 D49 D50 D511750
ε ≈ f
57 50 57 57 50 57 5050 50 50 50 50 50 5050 50 50 50 50 50 5057 50 57 57 50 57 5050 50 50 50 50 50 5057 50 57 57 50 57 5050 50 50 50 50 50 5050 50 50 50 50 50 5057 50 57 57 50 57 5050 50 50 50 50 50 50 --- --- --- --- --- --- ---50 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 5050 50 --- 50 --- 50 5057 50 --- 57 --- 57 50--- --- --- --- --- --- ---50 50 --- 50 --- 50 5057 50 --- 57 --- 57 50--- --- --- --- --- --- ---50 50 --- 50 --- 50 5050 50 --- 50 --- 50 5057 50 --- 57 --- 57 5057 50 --- 57 --- 57 5050 50 --- 50 --- 50 5050 50 --- 50 --- 50 5057 50 --- 57 --- 57 5057 50 --- 57 --- 57 5057 50 --- 57 --- 57 5050 50 --- 50 --- 50 5050 50 --- 50 --- 50 5057 50 --- 57 --- 57 5050 50 --- 50 --- 50 5050 50 --- 50 --- 50 5057 50 50 57 50 57 5050 50 50 50 50 50 5050 50 50 50 50 50 5057 50 50 57 50 57 5057 50 50 57 50 57 5050 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- --- ---57 50 50 57 50 57 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---57 50 50 57 50 57 50--- --- --- --- --- --- ------ --- --- --- --- --- ---57 50 50 57 50 57 5050 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
D43 D45 D47 D48 D49 D50 D511750
ε ≈ f
57 50 50 57 50 57 5050 50 50 50 50 50 5057 50 50 57 50 57 50--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 20 30 20 30 30 2030 20 30 20 30 30 20--- --- --- --- --- --- ---30 20 30 20 30 30 20--- --- --- --- --- --- ------ --- --- 20 --- --- --- --- --- --- --- --- --- ---30 20 30 30 30 30 ---30 20 30 30 30 30 ------ --- --- --- --- --- ---30 20 30 30 30 30 20--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 20 30 30 30 30 2030 20 30 30 30 30 20
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X 20 --- 20 --- X X
--- --- --- --- --- --- ---X 20 X X X X XX 20 X X X X XX 20 X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X 20 X X X X ------ --- --- --- --- --- ---X 20 X X X X X
Ə1 Ə * Ə Ə1 Ə1 Ə1 ---50 50 50 X X 50 ------ --- --- --- --- --- ---
1750 650 1000 1000 1000 1000 ------ --- --- --- --- --- ------ --- --- --- 50 --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
D53 D54
X XX XX X--- ---X X
X XX XX X--- X--- ---X X--- ------ X--- --- --- ---X X--- X Ð
--- X --- ---X X--- X --- ---X X
X XX X
--- ---X X
X^ X^^
X X
X 50--- ------ 50--- 50X //
X XX X30 3030 30 --- --- --- ------ X --- ---X XX XX XX XX X--- X--- X--- ---X XX XX X--- X --- ---X X--- ---X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
D53 D54
30 X30 X30 X30 X30 X30 X30 X30 X--- X--- ---30 X30 X30 X--- ---30 X
X XX X
X XX XX XX XX X--- XX XX XX X50 5050 50--- 50X XX X
--- ---X XX X
1000 1000 --- ---X XX XX XX XX XX XX XX XX X--- ------ XX XX X
--- ---X X
--- 5050 5050 5050 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
D53 D54
50 5050 5050 5050 5050 5050 5050 5050 5050 5050 50 --- ---50 5050 5050 5050 50--- ------ ---50 50 --- --- --- ------ 5050 5050 5050 50--- 5050 5050 50--- 5050 5050 5050 5050 5050 5050 5050 5050 5050 5050 5050 5050 5050 5050 5050 5050 5050 5050 5050 5050 5050 50--- ---50 50--- ------ ---50 50--- ------ ---50 50--- ------ ------ ---50 50--- ------ ---50 5050 5050 50--- 5050 50--- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
D53 D54
50 5050 5050 50--- --- --- ------ 5050 50
--- --- --- --- --- --- --- ---
ê
--- 50
30 3030 30--- ---30 30--- 30--- --- --- ---30 3030 30--- 3030 30--- --- --- ---50 50--- 30--- ------ 30--- 30--- 30 --- --- --- --- --- --- --- 30--- 30--- 3030 3030 30
--- ------ ------ ------ X --- ---X ---
--- ---X XX XX X--- X--- ---X X--- XX X
Ə ƏX 50--- ---
1200 2000--- ------ 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
D57 D58 D59 D60 D61 D63 D64
X X X 30 X X XX X X 30 X X XX X X 30 X X X--- --- --- --- --- --- ---X X X --- X --- ---
X X X 30 X X XX X X 30 X X XX X X 30 X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X 30 X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X 30 X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X 30 X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X 30 X X X
X X X 30 X X XX X X 30 X X X
--- --- --- --- --- --- ---X X X 30 X X X
X^ --- --- 30^ X^ X^ X^
X X --- --- X X X
50 40 X 30 20 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// // X // // // //
X 20 X 30 X X XX 20 X 30 X X X30 20 30 30 30 30 3030 20 30 30 30 30 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X 20 X 30 X X XX 20 X 30 X X XX 20 X --- X --- XX 20 X 30 X X XX 20 X 30 X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X 20 X 30 X X XX 20 X --- X --- XX 20 X 30 X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X 20 X --- X --- X--- --- --- --- --- --- ---X 20 X 30 X X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
D57 D58 D59 D60 D61 D63 D64
X 20 X 30 X X XX 20 X 30 X X XX 20 X 30 X X XX 20 X 30 X X XX 20 X 30 X X XX 20 X --- X --- ---X 20 X 30 X X XX 20 X --- X --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X 20 X 30 X X XX 20 X --- X --- ---X 20 X 30 X X X--- --- --- --- --- --- ---X 20 X 30 X X X
X 20 X --- X --- ---X 20 X --- X --- ---
X X X 30 X X XX X X 30 X X XX 20 X 30 X X XX 20 X 30 X X XX 20 X 30 X X X--- --- --- --- --- --- ---X 20 X 30 X X XX 20 X 30 X X XX 20 X 30 X X X50 40 X --- 50 --- 5050 40 X --- 50 --- 50--- --- --- --- --- --- ---X X X 30 X X XX X X --- X X X
--- --- --- --- --- --- ---X X X 30 X X XX X X 30 X X X
1000 1000 1000 --- 1000 --- --- --- --- 50 --- --- --- ---X 20 X --- X --- ---X 20 X --- X --- ---X 20 X --- X --- ---X 20 X --- X --- ---X 20 X --- X --- ---X 20 X --- X --- ---X 20 X --- X --- ---X 20 X --- X --- ---X 20 X --- X --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X 20 X --- X --- ---X 20 X --- X --- ---
--- --- --- --- --- --- ---X 20 X --- X --- ---
--- --- --- --- --- --- ---57 40 X --- 57 --- 5750 40 X --- 50 --- 5050 40 X --- 50 --- 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
D57 D58 D59 D60 D61 D63 D64
57 40 X --- 57 --- 5750 40 X --- 50 --- 5050 40 X --- 50 --- 5057 40 X --- 57 --- 5750 40 X --- 50 --- 5057 40 X --- 57 --- 5750 40 X --- 50 --- 5050 40 X --- 50 --- 5057 40 X --- 57 --- 5750 40 X --- 50 --- 50 --- --- --- --- --- --- ---50 40 X --- 50 --- 5050 40 X --- 50 --- 5050 40 X --- 50 --- 5050 40 X --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 40 X --- 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 40 X 30 50 X 5050 --- --- --- 50 --- 5057 --- --- --- 57 --- 57--- --- --- --- --- --- ---50 --- --- --- 50 --- 5057 --- --- --- 57 --- 57--- --- --- --- --- --- ---50 --- --- --- 50 --- 5050 --- --- --- 50 --- 5057 --- --- --- 57 --- 5757 --- --- --- 57 --- 5750 --- --- --- 50 --- 5050 --- --- --- 50 --- 5057 --- --- --- 57 --- 5757 --- --- --- 57 --- 5757 --- --- --- 57 --- 5750 --- --- --- 50 --- 5050 --- --- --- 50 --- 5057 --- --- --- 57 --- 5750 --- --- --- 50 --- 5050 --- --- --- 50 --- 5057 40 X --- 57 --- 5750 40 X --- 50 --- 5050 40 X --- 50 --- 5057 40 X --- 57 --- 5757 40 X --- 57 --- 5750 40 X --- 50 --- 5050 40 X --- 50 --- 50--- --- --- --- --- --- ---57 40 X --- 57 --- 57--- --- --- --- --- --- ------ --- --- --- --- --- ---50 40 X --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 40 X --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---57 40 X --- 57 --- 57--- --- --- --- --- --- ------ --- --- --- --- --- ---57 40 X --- 57 --- 5750 40 X --- 50 --- 5050 40 X --- 50 --- 50--- --- --- --- --- --- ---50 40 X --- 50 --- 50--- --- --- --- --- --- ---
January 01, 2016
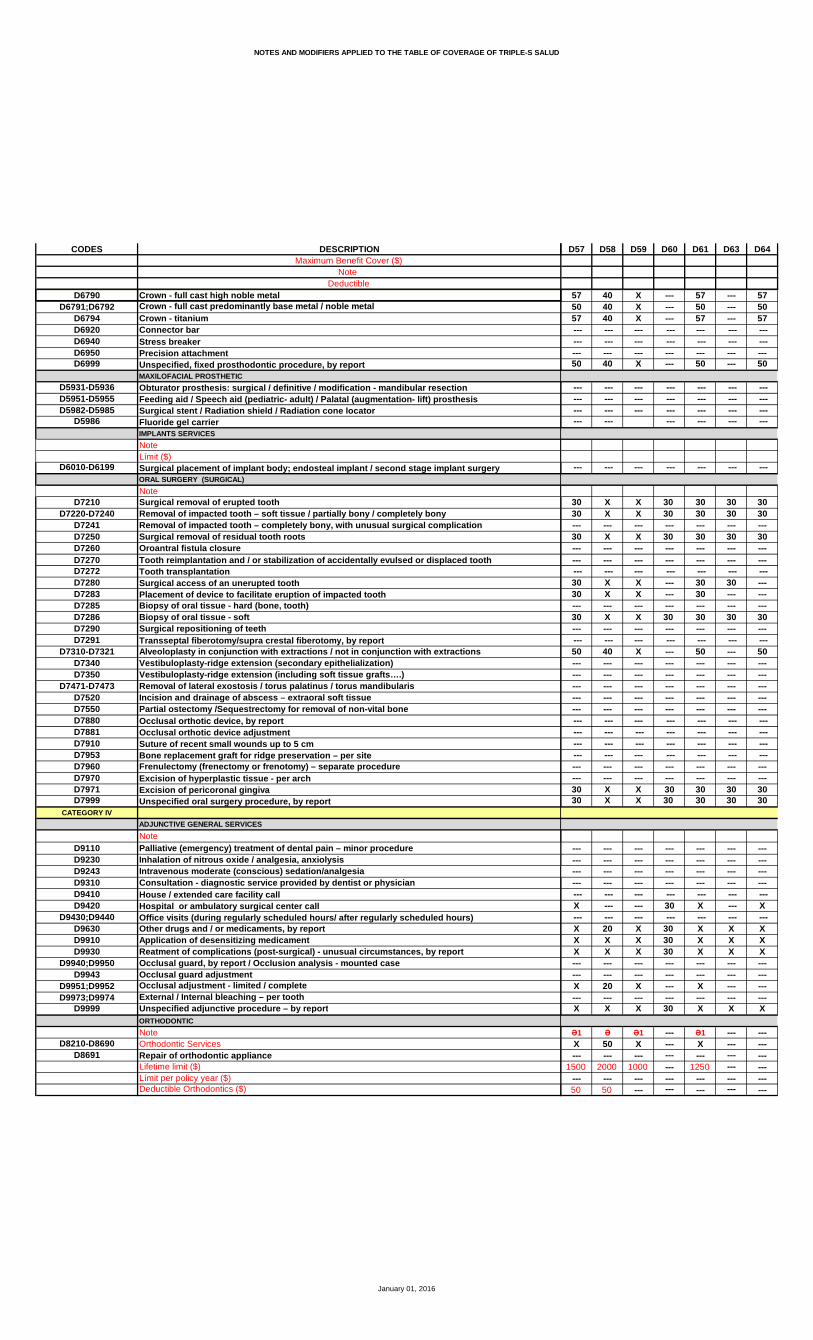
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
D57 D58 D59 D60 D61 D63 D64
57 40 X --- 57 --- 5750 40 X --- 50 --- 5057 40 X --- 57 --- 57 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 40 X --- 50 --- 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 X X 30 30 30 3030 X X 30 30 30 30--- --- --- --- --- --- ---30 X X 30 30 30 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 X X --- 30 30 ---30 X X --- 30 --- ------ --- --- --- --- --- ---30 X X 30 30 30 30--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 40 X --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 X X 30 30 30 3030 X X 30 30 30 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X --- --- 30 X --- X
--- --- --- --- --- --- ---X 20 X 30 X X XX X X 30 X X XX X X 30 X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X 20 X --- X --- ------ --- --- --- --- --- ---X X X 30 X X X
Ə1 Ə Ə1 --- Ə1 --- ---X 50 X --- X --- ------ --- --- --- --- --- ---
1500 2000 1000 --- 1250 --- ------ --- --- --- --- --- ---50 50 --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
D66 D67 D68 D69 D70 D75 D761750 1000
Ü ≈ ≈
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- X ------ --- --- --- --- --- --- --- --- --- --- --- X ---X X X X X X X--- --- --- --- --- X Ð ---
--- --- --- --- --- X --- --- --- --- --- --- X ---X X X X X X X--- --- --- --- --- X --- --- --- --- --- --- X ---X X X X X X X
X X X X X X XX X X X X X X
--- --- --- --- --- X XX X X X X X X--- --- --- X^ X^ --- X^
X X X X X X X
30 X 20 X 20 X X--- --- --- --- --- X ------ --- --- --- --- X ------ --- --- X --- X ---// X // X // X X
X X X X X X 25X X X X X 20 2530 X 30 X 30 20 2530 X 30 X 30 20 25 --- --- --- --- --- 40 --- --- --- --- --- --- 40 ------ --- --- --- --- 40 --- --- --- --- --- --- 40 ---X X X X X 20 25X X X X X 20 25X X X X X 20 25X X X X X 20 25X X X X X 20 25--- --- --- --- --- 20 ------ --- --- --- --- 20 ------ --- --- --- --- 20 ---X X X X X 20 25X X X X X 20 25X X X X X 20 25--- --- --- --- --- 20 --- --- --- --- --- --- 20 ---X X X X X 20 25--- --- --- --- --- --- ---X X X X X 20 25
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
D66 D67 D68 D69 D70 D75 D761750 1000
Ü ≈ ≈
X X X X X 20 25X X X X X 20 25X X X X X 20 25X X X X X 20 25X X X X X 20 25X X X X X 20 ---X X X X X 20 25X X X X X 20 ------ --- --- --- --- 20 ------ --- --- --- --- --- ---X X X X X 20 25X X X X X 20 ---X X X X X 20 25--- --- --- --- --- 20 ---X X X X X 20 25
X X X X X 20 25X X X X X 20 25
X X X X X 40 XX X X X X 40 XX X X X X 40 XX X X X X 40 XX X X X X 40 X--- --- --- --- --- 40 ---X X X X X 40 XX X X X X 40 XX X X X X 40 X50 X 50 X 50 40 5050 X 50 X 50 40 50--- --- --- --- --- 40 ---X X X X X X XX X X X X X X
--- --- --- --- --- --- ---X X X X X 20 30X X X X X 20 30
# Ü800 1000 1000 800 1000 --- ------ --- --- --- --- --- ---X X X --- X 20 25X X X X X 20 25X X X --- X 20 25X X X --- X 20 25X X X X X 20 25X X X --- X 20 25X X X --- X 20 25X X X --- X 20 25X X X --- X 20 25--- --- --- --- --- --- ------ --- --- --- --- 20 ---X X X --- X 20 25X X X X X 20 25
--- --- --- --- --- 20 ---X X X X X 20 25
# @800--- --- --- --- --- 40 ------ X 57 --- 57 40 4050 X 50 --- 50 40 4050 X 50 --- 50 40 40
January 01, 2016
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
D66 D67 D68 D69 D70 D75 D761750 1000
Ü ≈ ≈
--- X 57 --- 57 40 4050 X 50 --- 50 40 4050 X 50 --- 50 40 40--- X 57 --- 57 40 4050 X 50 --- 50 40 40--- X 57 --- 57 40 4050 X 50 --- 50 40 4050 X 50 --- 50 40 40--- X 57 --- 57 40 4050 X 50 --- 50 40 40 --- --- --- --- --- 40 ---50 X 50 X 50 40 4050 X 50 --- 50 40 4050 X 50 X 50 40 4050 X 50 X 50 40 40--- --- --- --- --- --- ------ --- --- --- --- --- ---50 X 50 X 50 40 40 --- --- --- --- --- 40 --- --- --- --- --- --- 40 ------ --- --- --- --- 40 ---50 X 50 X 50 40 40--- --- --- --- 50 40 40--- --- --- --- 57 40 40--- --- --- --- --- 40 ------ --- --- --- 50 40 40--- --- --- --- 57 40 40--- --- --- --- --- 40 ------ --- --- --- 50 40 40--- --- --- --- 50 40 40--- --- --- --- 57 40 40--- --- --- --- 57 40 40--- --- --- --- 50 40 40--- --- --- --- 50 40 40--- --- --- --- 57 40 40--- --- --- --- 57 40 40--- --- --- --- 57 40 40--- --- --- --- 50 40 40--- --- --- --- 50 40 40--- --- --- --- 57 40 40--- --- --- --- 50 40 40--- --- --- --- 50 40 40--- X 57 --- 57 40 4050 X 50 X 50 40 4050 X 50 X 50 40 40--- X 57 --- 57 40 40--- X 57 --- 57 40 4050 X 50 X 50 40 4050 X 50 X 50 40 40--- --- --- --- --- --- ------ X 57 --- 57 40 40--- --- --- --- --- --- ------ --- --- --- --- --- ---50 X 50 --- 50 40 40--- --- --- --- --- --- ------ --- --- --- --- --- ---50 X 50 --- 50 40 40--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ X 57 --- 57 40 40--- --- --- --- --- --- ------ --- --- --- --- --- ------ X 57 --- 57 40 4050 X 50 X 50 40 4050 X 50 X 50 40 40--- --- --- --- --- 40 ---50 X 50 --- 50 40 40--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
D66 D67 D68 D69 D70 D75 D761750 1000
Ü ≈ ≈
--- X 57 X 57 40 4050 X 50 --- 50 40 40--- X 57 --- 57 40 40 --- --- --- --- --- --- --- --- --- --- --- --- 40 ------ --- --- --- --- 40 ---50 X 50 --- 50 40 40
--- --- --- --- --- 40 --- --- --- --- --- --- 40 --- --- --- --- --- --- 40 --- --- --- --- --- --- 40 ---
--- --- --- --- --- 40 ¥ ---
30 X 30 X 30 20 4030 X 30 X 30 20 40--- --- --- --- --- --- ---30 X 30 X 30 20 40--- --- --- --- --- 20 ------ --- --- --- --- 20 --- --- --- --- --- --- 20 ------ X 30 --- 30 20 ------ X 30 X 30 20 ------ --- --- --- --- 20 ---30 X 30 X 30 20 40--- --- --- --- --- 20 --- --- --- --- --- --- 20 ---50 X 50 --- 50 20 40--- --- --- --- --- 20 ------ --- --- --- --- 20 ------ --- --- --- --- 20 ------ --- --- --- --- 20 ------ --- --- --- --- 20 --- --- --- --- --- --- 20 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 20 ------ --- --- --- --- 20 ------ --- --- --- --- 20 ---30 X 30 X 30 20 4030 X 30 X 30 20 40
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- X --- --- --- X --- X X X --- --- --- --- --- X ---X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X --- X 20 ------ --- --- --- --- --- ---X X X X X X X
** Ə1 Ə Ə1 --- * Ə1 Ə ---X X X --- X 50 ------ --- --- --- --- --- ---
1000 2000 1000 --- 1000 1750 ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
D77 D78 D80 D82 D83 D85 D86
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X --- X X
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
--- --- --- --- --- --- ---X X X X X X X--- X^ --- X^ X^ X^ X^
X X X X X X X
20 20 X X 20 20 X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// // X X // // X
X X X 20 X X XX X X 20 X X X30 30 X 20 30 30 2030 30 X 20 30 30 20 --- --- --- --- --- --- --- --- --- --- --- --- --- 20--- --- --- --- --- --- 20 --- --- --- --- --- --- 20X X X 20 X 30 XX X X 20 X 30 XX X X 20 --- 30 XX X X 20 X 30 XX X X 20 X 30 X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X 20 X X XX X X 20 --- 30 XX X X 20 X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X 20 --- 30 X--- --- --- --- --- --- ---X X X 20 X 30 X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
D77 D78 D80 D82 D83 D85 D86
X X X 20 X X XX X X 20 X X XX X X 20 X X XX X X 20 X X XX X X 20 X X XX X X 20 --- X XX X X 20 X X XX X X 20 --- X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X 20 X X XX X X 20 --- X XX X X 20 X X X--- --- --- --- --- --- ---X X X 20 X X X
X X X 20 --- X XX X X 20 --- X X
X X X 20 X 50 XX X X 20 X 50 XX X 20 20 X 50 XX X 20 20 X 50 XX X 20 20 X 50 X--- --- --- --- --- --- ---X X 20 20 X 50 XX X 20 20 X 50 XX X 20 20 X 50 X50 50 40 40 --- 50 5050 50 40 40 --- 50 50--- --- --- --- --- --- ---X X X 20 X 30 XX X X 20 X 30 X
--- --- --- --- --- --- ---X X X 20 X X 20X X X 20 X X 20
1000 1000 1250 1000 --- 1000 1000--- --- --- --- --- --- ---X X X 20 --- X XX X X 20 --- X XX X X 20 --- X XX X X 20 --- X XX X X 20 --- X XX X X 20 --- X XX X X 20 --- X XX X X 20 --- X XX X X 20 --- X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X 20 --- X XX X X 20 --- X X
--- --- --- --- --- --- ---X X X 20 --- X X
--- --- --- --- --- --- ---57 57 40 40 --- 50 5050 50 40 40 --- 50 5050 50 40 40 --- 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
D77 D78 D80 D82 D83 D85 D86
57 57 40 40 --- 50 5050 50 40 40 --- 50 5050 50 40 40 --- 50 5057 57 40 40 --- 50 5050 50 40 40 --- 50 5057 57 40 40 --- 50 5050 50 40 40 --- 50 5050 50 40 40 --- 50 5057 57 40 40 --- 50 5050 50 40 40 --- 50 50 --- --- --- --- --- --- ---50 50 40 40 --- 50 5050 50 40 40 --- 50 5050 50 40 40 --- 50 5050 50 40 40 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 40 40 --- 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 40 40 X 50 50--- 50 --- 40 --- 50 50--- 57 --- 40 --- 50 50--- --- --- --- --- --- ------ 50 --- 40 --- 50 50--- 57 --- 40 --- 50 50--- --- --- --- --- --- ------ 50 --- 40 --- 50 50--- 50 --- 40 --- 50 50--- 57 --- 40 --- 50 50--- 57 --- 40 --- 50 50--- 50 --- 40 --- 50 50--- 50 --- 40 --- 50 50--- 57 --- 40 --- 50 50--- 57 --- 40 --- 50 50--- 57 --- 40 --- 50 50--- 50 --- 40 --- 50 50--- 50 --- 40 --- 50 50--- 57 --- 40 --- 50 50--- 50 --- 40 --- 50 50--- 50 --- 40 --- 50 5057 57 40 40 --- 50 5050 50 40 40 --- 50 5050 50 40 40 --- 50 5057 57 40 40 --- 50 5057 57 40 40 --- 50 5050 50 40 40 --- 50 5050 50 40 40 --- 50 50--- --- --- --- --- --- ---57 57 40 40 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 40 40 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 40 40 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---57 57 40 40 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---57 57 40 40 --- 50 5050 50 40 40 --- 50 5050 50 40 40 --- 50 50--- --- --- --- --- --- ---50 50 40 40 --- 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
D77 D78 D80 D82 D83 D85 D86
57 57 40 40 --- 50 5050 50 40 40 --- 50 5057 57 40 40 --- 50 50--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 40 40 --- 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 30 X 20 30 X 2030 30 X 20 30 X 20--- --- --- --- --- --- ---30 30 X 20 30 X 20--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 30 X 20 30 --- 2030 30 X 20 --- --- 20--- --- --- --- --- --- ---30 30 X 20 30 X 20--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 40 40 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 30 X 20 30 X 2030 30 X 20 30 X 20
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- X X 20 --- X X --- --- --- --- --- --- ---X X X 20 X X XX X X 20 X X XX X X 20 X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X 20 --- X X--- --- --- --- --- --- ---X X X 20 X X X
Ə1 Ə1 Ə1 Ə1 --- --- Ə1X 50 X X --- --- X--- --- --- --- --- --- ---
1250 1000 1250 1000 --- --- 1000--- --- --- --- --- --- ---50 --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
D88 D90 D91 D92 D93 D94 D99800 500
≈ ¤
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X --- X X X X X
X X X X X X XX X X X X • X XX X X X --- X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
--- --- --- --- --- --- ---X X X X X X X
X^ --- X^ X^ X X^ X^
X X X X X X X
20 20 20 X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- X ---// // // X X X X
20 X X X X X X20 X X X X X X20 30 30 X X X X20 30 30 X X X X --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X XX X X X X X XX --- X X --- X XX X X X X X XX X X X --- X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X XX --- X X --- X XX X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X --- X X --- X X--- --- --- --- --- --- ---X X X X X X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
D88 D90 D91 D92 D93 D94 D99800 500
≈ ¤
X X X X X X XX X X X X X XX X X X --- X XX X X X --- X X20 X X X X X X20 --- X X --- X XX X X X X X XX --- X X --- X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X --- X XX --- X X --- X XX X X X --- X X--- --- --- --- --- --- ---X X X X X X X
X --- X 25 --- X XX --- X 25 --- X X
500
20 X X X X X X20 X X X X X XX X X X X X XX X X X X X XX X X X X X X--- --- --- --- X --- ---X X X X X X XX X X X X X XX X X X X X X40 --- 50 X X X X40 --- 50 X --- X X--- --- --- --- --- --- ---20 X X X --- X XX X X X X X X
--- --- --- --- --- --- ---20 X X X X X X20 X X X X X X
™1000 --- 1000 --- 500 800 1000
--- --- --- --- --- --- ---X --- X 25 X --- XX --- X 25 X X XX --- X 25 X --- XX --- X 25 X --- XX --- X 25 X X XX --- X 25 X --- XX --- X 25 X --- XX --- X 25 X --- XX --- X 25 X --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---X --- X 25 --- --- X20 --- X 25 --- X X --- --- --- --- --- --- ---X --- X 25 X X X
@500
--- --- --- --- --- --- ---40 --- 57 25 --- --- X40 --- 50 25 --- --- X40 --- 50 25 --- --- X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
D88 D90 D91 D92 D93 D94 D99800 500
≈ ¤
40 --- 57 25 --- 25 X40 --- 50 25 --- 25 X40 --- 50 25 --- 25 X40 --- 57 25 --- --- X40 --- 50 25 --- --- X40 --- 57 25 --- --- X40 --- 50 25 --- --- X40 --- 50 25 --- --- X40 --- 57 25 --- --- X40 --- 50 25 --- --- X --- --- --- --- --- --- ---40 --- 50 25 X 25 X40 --- 50 25 --- --- X40 --- 50 25 --- 25 X40 --- 50 25 X 25 X--- --- --- --- --- --- ------ --- --- --- --- --- ---40 --- 50 25 --- 25 X --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---40 X 50 25 X 25 X40 --- 50 25 --- --- X40 --- 57 25 --- --- X--- --- --- --- --- --- ---40 --- 50 25 --- --- X40 --- 57 25 --- --- X--- --- --- --- --- --- ---40 --- 50 25 --- --- X40 --- 50 25 --- --- X40 --- 57 25 --- --- X40 --- 57 25 --- --- X40 --- 50 25 --- --- X40 --- 50 25 --- --- X40 --- 57 25 --- --- X40 --- 57 25 --- --- X40 --- 57 25 --- --- X40 --- 50 25 --- --- X40 --- 50 25 --- --- X40 --- 57 25 --- --- X40 --- 50 25 --- --- X40 --- 50 25 --- --- X40 --- 57 25 --- --- X40 --- 50 25 --- 25 X40 --- 50 25 --- 25 X40 --- 57 25 --- --- X40 --- 57 25 --- --- X40 --- 50 25 --- 25 X40 --- 50 25 --- 25 X--- --- --- --- --- --- ---40 --- 57 25 --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---40 --- 50 25 --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---40 --- 50 25 --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---40 --- 57 25 --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---40 --- 57 25 --- --- X40 --- 50 25 --- 25 X40 --- 50 25 --- 25 X--- --- --- --- --- --- ---40 --- 50 25 --- --- X--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
D88 D90 D91 D92 D93 D94 D99800 500
≈ ¤
40 --- 57 25 --- 25 X40 --- 50 25 --- --- X40 --- 57 25 --- --- X--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---40 --- 50 25 --- --- X
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
20 30 30 25 X X X20 30 30 25 X X X--- --- --- --- --- --- ---20 30 30 25 X X X--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 --- 30 25 X --- X20 --- 30 25 --- X X--- --- --- --- --- --- ---20 30 30 25 X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---40 --- 50 25 --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 30 30 25 --- X X20 30 30 25 X X X
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X --- X X --- --- X
--- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X --- X X --- --- X--- --- --- --- --- --- ---X X X X X X X
Ə1 --- Ə1 Ə --- --- Ə1X --- X 50 --- --- X--- --- --- --- --- --- ---
1500 --- 1000 1000 --- --- 1000--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DA02 DA05 DA07 DA08 DA09 DA11 DA12500 1000 500¤ ≈ ¤
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X • X X X X • XX --- X X X --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
--- --- --- --- X --- ---X X X X X X X--- X X^ X^ X^ X ---
X X X X X X X
20 X X X 30 X 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- X --- --- ---// X X X // X //
20 X 25 X 30 X 20X X 25 X X X 2020 X 25 X 30 X 2020 X 25 X 30 X 20 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X 25 X X X 20X X 25 X X X 20X --- 25 X X --- 20X X 25 X X X 20X --- 25 X X --- 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X 25 X X X 20X --- 25 X X --- 20X X 25 X X X 20--- --- --- --- --- --- --- --- --- --- --- --- --- ---X --- 25 X X --- 20--- --- --- --- --- --- ---X X 25 X X X 20
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DA02 DA05 DA07 DA08 DA09 DA11 DA12500 1000 500¤ ≈ ¤
20 X X X 30 X 5020 X X X 30 X 5020 X X X 30 X 5020 --- X X 30 --- 5020 X X X 30 X 5020 --- X X --- --- 5020 X X X 30 X 5020 --- X X --- --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---20 --- X X 30 --- 5020 --- X X --- --- 5020 --- X X 30 --- 50--- --- --- --- --- --- ---20 X X X 30 X 50
20 --- X X 30 --- 5020 --- X X 30 --- 50
500
X --- X X 50 X XX --- X X 50 X XX --- X X 50 X XX --- X X 50 X XX --- X X 50 X X--- --- --- --- --- X ---X --- X X 50 X XX --- X X 50 X XX --- X X 50 X X50 --- 50 X 50 X 5050 --- 50 X 50 --- 50--- --- --- --- --- --- ---X --- X X 50 --- XX --- X X 50 X X
--- --- --- --- --- --- ---X X X X 30 X 50X X X X 30 X 50
™ ™1000 500 1000 800 --- 500 1000
--- --- --- --- --- --- ---20 X X --- 30 X 5020 X X X 30 X 5020 X X --- 30 X 5020 X X --- 30 X 5020 X X X 30 X 5020 X X --- 30 X 5020 X X --- 30 X 5020 X X --- 30 X 5020 X X --- 30 X 50--- --- --- --- --- --- ------ --- --- --- 30 --- ---20 --- X --- 30 --- 5020 --- X X 30 --- 50 --- --- --- --- 30 --- ---20 X X X 30 X 50
@ --- 500
--- --- --- --- --- --- ---50 --- 57 --- 50 --- 5750 --- 50 --- 50 --- 5050 --- 50 --- 50 --- 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DA02 DA05 DA07 DA08 DA09 DA11 DA12500 1000 500¤ ≈ ¤
50 --- 57 25 50 --- 5750 --- 50 25 50 --- 5050 --- 50 25 50 --- 5050 --- 57 --- 50 --- 5750 --- 50 --- 50 --- 5050 --- 57 --- 50 --- 5750 --- 50 --- 50 --- 5050 --- 50 --- 50 --- 5050 --- 57 --- 50 --- 5750 --- 50 --- 50 --- 50 --- --- --- --- --- --- ---50 --- 50 25 50 X 5050 --- 50 --- 50 --- 5050 --- 50 25 50 --- 5050 --- 50 25 50 X 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 25 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 25 50 X 50 --- --- 50 --- 50 --- --- --- --- 57 --- 50 --- ------ --- --- --- --- --- ------ --- 50 --- 50 --- --- --- --- 57 --- 50 --- ------ --- --- --- --- --- ------ --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- 57 --- 50 --- --- --- --- 57 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- 57 --- 50 --- --- --- --- 57 --- 50 --- ------ --- 57 --- 50 --- ------ --- 50 --- 50 --- ------ --- 50 --- 50 --- ------ --- 57 --- 50 --- ------ --- 50 --- 50 --- ------ --- 50 --- 50 --- ---50 --- 57 --- 50 --- 5750 --- 50 25 50 --- 5050 --- 50 25 50 --- 5050 --- 57 --- 50 --- 5750 --- 57 --- 50 --- 5750 --- 50 25 50 --- 5050 --- 50 25 50 --- 50--- --- --- --- --- --- ---50 --- 57 --- 50 --- 57--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 57 --- 50 --- 57--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 57 --- 50 --- 5750 --- 50 25 50 --- 5050 --- 50 25 50 --- 50--- --- --- --- --- --- ---50 --- 50 --- 50 --- 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DA02 DA05 DA07 DA08 DA09 DA11 DA12500 1000 500¤ ≈ ¤
50 --- 57 25 50 --- 5750 --- 50 --- 50 --- 5050 --- 57 --- 50 --- 57--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 --- 50 --- 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
20 X 25 X 30 X 5020 X 25 X 30 X 50--- --- --- --- --- --- ---20 X 25 X 30 X 50--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 X 25 --- --- X 5020 --- 25 X --- --- ------ --- --- --- --- --- ---20 X 25 X 30 X ------ --- --- --- --- --- --- --- --- --- --- --- --- ---50 --- 50 --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---20 --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 --- 25 X 30 --- ---20 X 25 X 30 X 50
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- X --- X --- --- --- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X --- X --- --- --- X--- --- --- --- --- --- ---X X X X X X X
Ə --- Ə1 --- --- --- ---50 --- 50 --- --- --- ------ --- --- --- --- --- ---
1500 --- 1000 --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DA13 DA14 DA16 DA18 DA20 DA22 DA24
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ X X X X X X
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
--- --- --- --- --- --- ---X X X X X X X--- X^ X^ X^ X^ X^ X^
X X X X X X X
X 20 50 20 20 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X // // // // // //
X X 25 X X X XX X 25 X X X XX 30 25 30 30 30 30X 30 25 30 30 30 30
--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X 25 X X X XX X 25 X X X X--- X 25 --- X X XX X 25 X X X XX X 25 X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X 25 X X X X--- X 25 --- X X XX X 25 X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ------ X 25 --- X X X--- --- --- --- --- --- ---X X 25 X X X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DA13 DA14 DA16 DA18 DA20 DA22 DA24
X X X X X X XX X X X X X XX X X X X X XX X X X X X XX X X X X X X--- X X --- X X XX X X X X X X--- X X --- X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- X X --- X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X X
--- 20 50 50 X 20 X--- 20 50 50 X 20 X
X X X X X X XX X X X X X XX X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X--- 50 50 --- 50 50 50 --- 50 50 --- 50 50 50--- --- --- --- --- --- ---X X X X X X XX X X --- X X X
--- --- --- --- --- --- ---X X X X X X XX X X X X X X
--- 1000 500 1000 1000 1000 1000--- --- --- --- --- --- ------ 20 50 50 X 20 X--- 20 50 50 X 20 X--- 20 50 50 X 20 X--- 20 50 50 X 20 X--- 20 50 50 X 20 X--- 20 50 50 X 20 X--- 20 50 50 X 20 X--- 20 50 50 X 20 X--- 20 50 50 X 20 X--- --- --- --- --- --- ------ --- --- --- --- --- ------ 20 50 50 X 20 X--- 20 50 50 X 20 X --- --- --- --- --- --- ------ 20 50 50 X 20 X
500--- --- --- --- --- --- ------ 57 50 --- 57 57 57--- 50 50 --- 50 50 50--- 50 50 --- 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DA13 DA14 DA16 DA18 DA20 DA22 DA24
--- 57 50 --- 57 57 57--- 50 50 --- 50 50 50--- 50 50 --- 50 50 50--- 57 50 --- 57 57 57--- 50 50 --- 50 50 50--- 57 50 --- 57 57 57--- 50 50 --- 50 50 50--- 50 50 --- 50 50 50--- 57 50 --- 57 57 57--- 50 50 --- 50 50 50 --- --- --- --- --- --- ------ 50 50 --- 50 50 50--- 50 50 --- 50 50 50--- 50 50 --- 50 50 50--- 50 50 --- 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 --- 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---X 50 50 X 50 50 50--- 50 50 --- 50 50 50--- 57 50 --- 57 57 57--- --- --- --- --- --- ------ 50 50 --- 50 50 50--- 57 50 --- 57 57 57--- --- --- --- --- --- ------ 50 50 --- 50 50 50--- 50 50 --- 50 50 50--- 57 50 --- 57 57 57--- 57 50 --- 57 57 57--- 50 50 --- 50 50 50--- 50 50 --- 50 50 50--- 57 50 --- 57 57 57--- 57 50 --- 57 57 57--- 57 50 --- 57 57 57--- 50 50 --- 50 50 50--- 50 50 --- 50 50 50--- 57 50 --- 57 57 57--- 50 50 --- 50 50 50--- 50 50 --- 50 50 50--- 57 50 --- 57 57 57--- 50 50 --- 50 50 50--- 50 50 --- 50 50 50--- 57 50 --- 57 57 57--- 57 50 --- 57 57 57--- 50 50 --- 50 50 50--- 50 50 --- 50 50 50--- --- --- --- --- --- ------ 57 50 --- 57 57 57--- --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 --- 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 --- 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ 57 50 --- 57 57 57--- --- --- --- --- --- ------ --- --- --- --- --- ------ 57 50 --- 57 57 57--- 50 50 --- 50 50 50--- 50 50 --- 50 50 50--- --- --- --- --- --- ------ 50 50 --- 50 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DA13 DA14 DA16 DA18 DA20 DA22 DA24
--- 57 50 --- 57 57 57--- 50 50 --- 50 50 50--- 57 50 --- 57 57 57--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 --- 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
X 20 30 30 30 20 30X 20 30 30 30 20 30--- --- --- --- --- --- ---X 20 30 30 30 20 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ 20 30 --- 30 20 30--- 20 30 --- 30 20 30--- --- --- --- --- --- ---X 20 30 30 30 20 30--- --- --- --- --- --- --- --- --- --- --- --- --- ------ 50 50 --- 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X 20 30 30 30 20 30X 20 30 30 30 20 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- X X X X X X --- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ 20 X --- X 20 X--- --- --- --- --- --- ---X X X X X X X
--- ő Θ Ə1 Ə1 --- Ə1 Θ Ə1 Ə1--- 50 50 --- X 50 50--- --- --- --- --- --- ------ 1500 3000 --- 1000 1500 1000--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DA25 DA26 DA28 DA33 DA38 DA401750
Ü ≈
X X X X X XX X X X X XX X X X X X--- --- --- --- --- ---X --- X --- X X
X X X --- X XX X X X Þ X XX X X --- X X--- --- --- --- --- ------ --- --- --- --- ---X X X X X X--- --- --- --- --- ------ --- --- --- --- X--- --- --- --- --- --- --- --- --- --- --- XX X X --- X X--- --- --- --- --- X Ð
--- --- --- --- --- X --- --- --- --- --- XX X X --- X X--- --- --- --- --- X --- --- --- --- --- XX X X 30 X X
X X X X X XX X X X X X
--- --- --- --- --- XX X X X X X--- X^ --- X^ X^ ---
X X X --- X X
20 20 20 --- 20 X--- --- --- --- --- X--- --- --- --- --- X--- --- --- --- --- X// // // X // X
20 X X 30 X X20 X 30 30 X 2020 30 50 30 30 2020 30 50 30 30 20 --- --- --- --- --- 40 --- --- --- --- --- 40--- --- --- --- --- 40 --- --- --- --- --- 4020 X X --- X 2020 X X --- X 2020 X X --- X 2020 X X --- X 2020 X X --- X 20--- --- --- --- --- 20--- --- --- --- --- 20--- --- --- --- --- 2020 X X 30 X 2020 X X --- X 2020 X X 30 X 20--- --- --- --- --- 20 --- --- --- --- --- 2020 X X --- X 20--- --- --- --- --- ---20 X X 30 X 20
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DA25 DA26 DA28 DA33 DA38 DA401750
Ü ≈
20 X X 30 X 2020 X X 30 X 2020 X X --- X 2020 X X --- X 2020 X X --- X 2020 X X --- X 2020 X X --- X 2020 X X --- X 20--- --- --- --- --- 20--- --- --- --- --- ---20 X X --- X 2020 --- X --- X 2020 X X --- X 20--- --- --- --- --- 2020 X X --- X 20
20 --- X --- X 2020 --- X --- X 20
X X X --- X 40X X X --- X 40X X X --- X 40X X X --- X 40X X X --- X 40--- --- --- --- --- 40X X X --- X 40X X X --- X 40X X X --- X 4050 50 50 --- 50 4050 50 50 --- 50 40--- --- --- --- --- 40X X X --- X XX X X --- X X
--- --- --- --- --- ---50 X 20 30 X 2050 X 20 30 X 20
Ü1000 --- 1000 --- 1000 ---
--- --- --- --- --- ---20 --- X --- X 2020 --- X --- X 2020 --- X --- X 2020 --- X --- X 2020 --- X --- X 2020 --- X --- X 2020 --- X --- X 2020 --- X --- X 2020 --- X --- X 20--- --- --- --- --- ------ --- --- --- --- 2020 --- X --- X 2020 --- X --- X 20 --- --- --- --- --- 2020 --- X --- X 20
--- --- --- --- --- 4050 57 57 --- 57 4050 50 50 --- 50 4050 50 50 --- 50 40
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DA25 DA26 DA28 DA33 DA38 DA401750
Ü ≈
50 57 57 --- 57 4050 50 50 --- 50 4050 50 50 --- 50 4050 57 57 --- 57 4050 50 50 --- 50 4050 57 57 --- 57 4050 50 50 --- 50 4050 50 50 --- 50 4050 57 57 --- 57 4050 50 50 --- 50 40 --- --- --- --- --- 4050 50 50 --- 50 4050 50 50 --- 50 4050 50 50 --- 50 4050 50 50 --- 50 40--- --- --- --- --- ------ --- --- --- --- ---50 50 50 --- 50 40 --- --- --- --- --- 40 --- --- --- --- --- 40--- --- --- --- --- 4050 50 50 --- 50 40 --- 50 50 --- 50 40 --- 57 57 --- 57 40--- --- --- --- --- 40--- 50 50 --- 50 40 --- 57 57 --- 57 40--- --- --- --- --- 40--- 50 50 --- 50 40 --- 50 50 --- 50 40 --- 57 57 --- 57 40 --- 57 57 --- 57 40 --- 50 50 --- 50 40 --- 50 50 --- 50 40 --- 57 57 --- 57 40 --- 57 57 --- 57 40--- 57 57 --- 57 40--- 50 50 --- 50 40--- 50 50 --- 50 40--- 57 57 --- 57 40--- 50 50 --- 50 40--- 50 50 --- 50 4050 57 57 --- 57 4050 50 50 --- 50 4050 50 50 --- 50 4050 57 57 --- 57 4050 57 57 --- 57 4050 50 50 --- 50 4050 50 50 --- 50 40--- --- --- --- --- ---50 57 57 --- 57 40--- --- --- --- --- ------ --- --- --- --- ---50 50 50 --- 50 40--- --- --- --- --- ------ --- --- --- --- ---50 50 50 --- 50 40--- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ---50 57 57 --- 57 40--- --- --- --- --- ------ --- --- --- --- ---50 57 57 --- 57 4050 50 50 --- 50 4050 50 50 --- 50 40--- --- --- --- --- 4050 50 50 --- 50 40--- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DA25 DA26 DA28 DA33 DA38 DA401750
Ü ≈
50 57 57 --- 57 4050 50 50 --- 50 4050 57 57 --- 57 40--- --- --- --- --- --- --- --- --- --- --- 40--- --- --- --- --- 4050 50 50 --- 50 40
--- --- --- --- --- 40 --- --- --- --- --- 40 --- --- --- --- --- 40 --- --- --- --- --- 40
--- --- --- --- --- 40 ¥
50 30 20 30 30 2050 30 20 30 30 20--- --- --- --- --- ---50 30 20 30 30 20--- --- --- --- --- 20--- --- --- --- --- 20 --- --- --- --- --- 2050 --- 20 --- 30 2050 --- 20 --- 30 20--- --- --- --- --- 2050 30 20 --- 30 20--- --- --- --- --- 20 --- --- --- --- --- 2050 50 50 --- 50 20--- --- --- --- --- 20--- --- --- --- --- 20--- --- --- --- --- 20--- --- --- --- --- 20--- --- --- --- --- 20 --- --- --- --- --- 20 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 20--- --- --- --- --- 20--- --- --- --- --- 2050 30 20 --- 30 2050 30 20 30 30 20
--- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- X --- X --- 30 X X --- --- --- --- --- XX X X --- X XX X X 30 X XX X X 30 X XX --- --- --- --- ------ --- --- --- --- ---X --- X --- X 20--- --- --- --- --- ---X X X 30 X X
Ə1 --- Ə1 --- Ə1 Ə50 --- 50 --- X 50--- --- --- --- --- ---
1000 --- 2000 --- 1250 1750--- --- --- --- --- ------ --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DA43 DA45 DA46 DA49 DA51 DA52 DA531500
ἆ ≈
X X 30 X X X XX X 30 X X X XX X 30 X X X X--- --- --- --- --- --- ------ X 30 X X X X
X X 30 X X X XX X 30 X X X XX X 30 X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X 30 X X X X--- --- --- --- --- --- ------ --- 30 --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X 30 X X X X--- --- 30 Ð --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X 30 X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X 30 X X X X
X X 30 X X X XX X 30 X X X X
--- --- --- --- --- X ---X X 30 X X X X
X^ X^ 30^ X^ X^ X^ X^
X X 30 X X X X
20 X 30 20 20 20 20--- --- 30 --- --- --- ------ --- 30 --- --- --- ------ --- 30 --- --- --- ---// X 30 // // // //
X X 30 X X X XX X 30 X X X X30 30 30 30 30 30 3030 30 30 30 30 30 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X 30 X X X XX X 30 X X X X--- X 30 X X X XX X 30 X X X XX X 30 X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X 30 X X X X--- X 30 X X X XX X 30 X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ------ X 30 X X X X--- --- --- --- --- --- ---X X 30 X X X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DA43 DA45 DA46 DA49 DA51 DA52 DA531500
ἆ ≈
X X 40 X X X XX X 40 X X X XX X 40 X X X XX X 40 X X X XX X 40 X X X X--- --- 40 X X X XX X 40 X X X X--- --- 40 X X X X--- --- 40 --- --- --- ------ --- --- --- --- --- ---X X 40 X X X X--- --- --- X X --- XX X 40 X X X X--- --- --- --- --- --- ---X X 40 X X X X
--- 25 50 X X 30 X--- 25 50 X X 30 X
X X 50 X X 30 XX X 50 X X 30 XX X 50 X X 30 XX X 50 X X 30 XX X 50 X X 30 X--- --- 50 --- --- --- ---X X 50 X X 30 XX X 50 X X 30 XX X 50 X X 30 X--- 50 50 50 50 30 50 --- 50 50 50 50 30 50--- --- 50 --- --- --- ---X X 50 X X 30 XX X 50 X X 30 X
--- --- --- --- --- --- ---X X 30 X X X XX X 30 X X X X
--- 1000 1000 1000 1000 1000 1000--- --- --- --- --- --- ------ 25 50 X X 30 X--- 25 50 X X 30 X--- 25 50 X X 30 X--- 25 50 X X 30 X--- 25 50 X X 30 X--- 25 50 X X 30 X--- 25 50 X X 30 X--- 25 --- X X 30 X--- 25 --- X X 30 X--- --- --- --- --- --- ------ --- --- --- --- --- ------ 25 50 X X 30 X--- 25 50 X X 30 X --- --- --- --- --- --- ------ 25 50 X X 30 X
--- --- --- --- --- --- ------ 57 50 57 57 50 57--- 50 50 50 50 30 50--- 50 50 50 50 30 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DA43 DA45 DA46 DA49 DA51 DA52 DA531500
ἆ ≈
--- 57 50 57 57 50 57--- 50 50 50 50 30 50--- 50 50 50 50 30 50--- 57 50 57 57 50 57--- 50 50 50 50 30 50--- 57 50 57 57 50 57--- 50 50 50 50 30 50--- 50 50 50 50 30 50--- 57 50 57 57 50 57--- 50 50 50 50 30 50 --- --- --- --- --- --- ------ 50 50 50 50 30 50--- 50 50 50 50 30 50--- 50 50 50 50 30 50--- 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 50 30 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---X 50 50 50 50 30 50--- 50 50 50 50 30 50--- 57 50 57 57 50 57--- --- 50 --- --- --- ------ 50 50 50 50 30 50--- 57 50 57 57 50 57--- --- 50 --- --- --- ------ 50 50 50 50 30 50--- 50 50 50 50 30 50--- 57 50 57 57 50 57--- 57 50 57 57 50 57--- 50 50 50 50 30 50--- 50 50 50 50 30 50--- 57 50 57 57 50 57--- 57 50 57 57 50 57--- 57 50 57 57 50 57--- 50 50 50 50 30 50--- 50 50 50 50 30 50--- 57 50 57 57 50 57--- 50 50 50 50 30 50--- 50 50 50 50 30 50--- 57 50 57 57 50 57--- 50 50 50 50 30 50--- 50 50 50 50 30 50--- 57 50 57 57 30 57--- 57 50 57 57 50 57--- 50 50 50 50 30 50--- 50 50 50 50 30 50--- --- --- --- --- --- ------ 57 50 57 57 50 57--- --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 50 30 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 50 30 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ 57 50 57 57 50 57--- --- --- --- --- --- ------ --- --- --- --- --- ------ 57 50 57 57 50 57--- 50 50 50 50 30 50--- 50 50 50 50 30 50--- --- --- --- --- --- ------ 50 50 50 50 30 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DA43 DA45 DA46 DA49 DA51 DA52 DA531500
ἆ ≈
--- 57 50 57 57 50 57--- 50 50 50 50 30 50--- 57 50 57 57 50 57--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 50 30 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 25 50 30 30 30 3030 25 50 30 30 30 30--- --- --- --- --- --- ---30 25 50 30 30 30 30--- --- 30 --- --- --- ------ --- 30 --- --- --- --- --- --- --- --- --- --- ------ --- 30 30 30 --- 30--- --- 30 30 30 --- 30--- --- 30 --- --- --- ---30 25 30 30 30 30 30--- --- 30 --- --- --- --- --- --- --- --- --- --- ------ 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- 30 --- --- --- ------ --- 30 --- --- --- ---30 25 30 30 30 30 3030 25 30 30 30 30 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- 30 --- --- --- --- --- --- --- --- --- --- --- --- X 30 X X X X --- --- --- --- --- --- ---X X 30 X X X XX X 30 X X X XX X 30 X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- 30 X X --- X--- --- --- --- --- --- ---X X 30 X X X X
--- --- Ə1 Ə1 Ə1 W Ə1 Ə1--- --- X X X 50 X --- --- --- --- --- --- ------ --- 1000 1500 1000 2000 1500--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DA54 DA55 DA56 DA61 DA63 DA65 DA66
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X --- X X
X X X X X X XX X X X X X X X X X X X --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- X ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- X Ð ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X --- X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
--- --- --- --- --- --- ---X X X X X X X
X^ --- X^ --- X^ X^ ---
X --- X X X X ---
20 50 20 X 20 X 30--- --- --- --- --- X ------ --- --- --- --- X ------ --- --- --- --- X ---// // // X // X //
X X X X X X XX X X X X X X30 30 30 X 30 X 3030 30 30 X 30 X 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X --- XX X X X X X XX X X X --- X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X XX X X X --- X XX X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X --- X X--- --- --- --- --- --- ---X X X X X X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DA54 DA55 DA56 DA61 DA63 DA65 DA66
X X X X X X XX X X X X X XX X X X X X XX X X X X X XX X X X X X XX X X X X X XX X X X X --- XX X X X X --- X--- --- --- --- --- X ------ --- --- --- --- --- ---X X X X X X XX X X X --- --- XX X X X X X X--- --- --- --- --- --- ---X X X X X X X
X 50 X X --- --- 30X 50 X X --- 50 30
X X X X X 50 XX X X X X 50 XX X X 20 X 50 XX X X 20 X 50 XX X X 20 X 50 X--- --- --- --- --- 50 ---X X X 20 X 50 XX X X 20 X 50 XX X X 20 X 50 X50 50 50 40 --- 50 5050 50 50 40 --- 50 50--- --- --- --- --- 50 ---X X X X X 50 XX X X X X 50 X
--- --- --- --- --- --- ---X X X X X 30 XX X X X X 30 X
1000 800 1000 1250 --- 1000 1000--- 50 --- --- --- --- ---X 50 X X --- 50 30X 50 X X --- 50 30X 50 X X --- --- 30X 50 X X --- --- 30X 50 X X --- 50 30X 50 X X --- --- 30X 50 X X --- 50 30X 50 X X --- 50 30X 50 X X --- 50 30--- --- --- --- --- --- ------ --- --- --- --- --- ---X 50 X X --- --- 30X 50 X X --- 50 30
--- --- --- --- --- --- ---X 50 X X --- 50 30
800--- --- --- --- --- --- ---57 --- 57 40 --- --- 5050 50 50 40 --- --- 5050 50 50 40 --- 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DA54 DA55 DA56 DA61 DA63 DA65 DA66
57 --- 57 40 --- --- 5050 50 50 40 --- 50 5050 50 50 40 --- 50 5057 --- 57 40 --- --- 5050 50 50 40 --- 50 5057 --- 57 40 --- --- 5050 50 50 40 --- 50 5050 50 50 40 --- 50 5057 --- 57 40 --- --- 5050 50 50 40 --- 50 50 --- --- --- --- --- --- ---50 50 50 40 --- 50 5050 50 50 40 --- 50 5050 50 50 40 --- 50 5050 50 50 40 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 40 --- 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 40 X 50 5050 50 50 --- --- 50 ---57 --- 57 --- --- 50 ------ --- --- --- --- 50 ---50 50 50 --- --- 50 ---57 --- 57 --- --- 50 ------ --- --- --- --- 50 ---50 50 50 --- --- 50 ---50 50 50 --- --- 50 ---57 --- 57 --- --- 50 ---57 --- 57 --- --- 50 ---50 50 50 --- --- 50 ---50 50 50 --- --- 50 ---57 --- 57 --- --- 50 ---57 --- 57 --- --- 50 ---57 --- 57 --- --- 50 ---50 50 50 --- --- 50 ---50 50 50 --- --- 50 ---57 --- 57 --- --- 50 ---50 50 50 --- --- 50 ---50 50 50 --- --- 50 ---57 --- 57 40 --- 50 5050 50 50 40 --- 50 5050 50 50 40 --- 50 5057 --- 57 40 --- 50 5057 --- 57 40 --- 50 5050 50 50 40 --- 50 5050 50 50 40 --- 50 50--- --- --- --- --- --- ---57 --- 57 40 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 40 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 40 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---57 --- 57 40 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---57 --- 57 40 --- 50 5050 50 50 40 --- 50 5050 50 50 40 --- 50 50--- --- --- --- --- --- ---50 50 50 40 --- 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DA54 DA55 DA56 DA61 DA63 DA65 DA66
57 --- 57 40 --- 50 5050 50 50 40 --- 50 5057 --- 57 40 --- 50 50--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 40 --- 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- 50 --- --- --- --- ---
30 X 30 X 30 50 X30 X 30 X 30 50 X--- --- --- --- --- --- ---30 X 30 X 30 50 X--- --- --- --- --- 30 ------ --- --- --- --- 30 --- --- --- --- --- --- --- ---30 X 30 X --- 30 3030 X 30 X --- 30 30--- --- --- --- --- 30 ---30 X 30 X 30 30 30--- --- --- --- --- 30 --- --- --- --- --- --- --- ---50 50 50 40 --- 50 X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- X --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- X --- --- --- --- ------ --- --- --- --- 30 ------ --- --- --- --- 30 ---30 X 30 X 30 30 3030 X 30 X 30 30 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- X --- --- --- --- --- --- --- ---X --- X X --- X ---
--- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X --- X X --- --- --- --- --- --- ---X X X X X X X
Ə1 Ω Ə Ə1 Ə1 --- Ə1 Ə1X 50 X X --- X X--- --- --- --- --- --- ---
1500 3000 1000 1000 --- 1000 1000--- --- --- --- --- --- ------ --- --- --- --- --- 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DA68 DA71 DA72 DA73 DA78 DA80 DA811200
B ≈
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X --- X X
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
X --- --- --- --- --- ---X X X X X X X
X^ X^ X^ X^ X^ X^ X^
X X X X X X X
20 20 20 20 20 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// // // // // // //
20 X 30 X X 20 2020 X 30 X X 20 2020 30 30 30 30 20 2020 30 30 30 30 20 20 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 X 30 X X 20 2020 X 30 X X 20 2020 X 30 X X 20 2020 X 30 X X 20 2020 X 30 X X 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 X 30 X X 20 2020 X 30 X X 20 2020 X 30 X X 20 20--- --- --- --- --- --- --- --- --- --- --- --- --- ---20 X 30 X X 20 20--- --- --- --- --- --- ---20 X 30 X X 20 20
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DA68 DA71 DA72 DA73 DA78 DA80 DA811200
B ≈
X X 30 X X X XX X 30 X X X XX X 30 X X X XX X 30 X X X XX X 30 X X X XX X 30 X --- X ---X X 30 X X X XX X 30 X --- X ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X 30 X X X XX X 30 X --- X ---X X 30 X X X X--- --- --- --- --- --- ---X X 30 X X X X
X X 30 X --- X XX X 30 X --- X X
X X 30 X X X XX X 30 X X X XX X 30 X X X XX X 30 X X X XX X 30 X X X X--- --- --- --- --- --- ---X X 30 X X X XX X 30 X X X XX X 30 X X X X50 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- --- ---X X 30 X X X XX X 30 X X X X
--- --- --- --- --- --- ---20 X 30 X X 20 2020 X 30 X X 20 20
1000 1000 1000 1000 --- 1000 1000--- --- --- --- --- --- ---X X 30 X --- X XX X 30 X --- X XX X 30 X --- X XX X 30 X --- X XX X 30 X --- X XX X 30 X --- X XX X 30 X --- X XX X 30 X --- X XX X 30 X --- X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X 30 X --- X XX X 30 X --- X X
--- --- --- --- --- --- ---X X 30 X --- X X
--- --- --- --- --- --- ---50 57 57 57 57 57 5750 50 50 50 50 50 5050 50 50 50 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DA68 DA71 DA72 DA73 DA78 DA80 DA811200
B ≈
50 57 57 57 57 57 5750 50 50 50 50 50 5050 50 50 50 50 50 5050 57 57 57 57 57 5750 50 50 50 50 50 5050 57 57 57 57 57 5750 50 50 50 50 50 5050 50 50 50 50 50 5050 57 57 57 57 57 5750 50 50 50 50 50 50 --- --- --- --- --- --- ---50 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 5050 50 50 50 50 50 5050 57 57 57 57 57 57--- --- --- --- --- --- ---50 50 50 50 50 50 5050 57 57 57 57 57 57--- --- --- --- --- --- ---50 50 50 50 50 50 5050 50 50 50 50 50 5050 57 57 57 57 57 5750 57 57 57 57 57 5750 50 50 50 50 50 5050 50 50 50 50 50 5050 57 57 57 57 57 5750 57 57 57 57 57 5750 57 57 57 57 57 5750 50 50 50 50 50 5050 50 50 50 50 50 5050 57 57 57 57 57 5750 50 50 50 50 50 5050 50 50 50 50 50 5050 57 57 57 57 57 5750 50 50 50 50 50 5050 50 50 50 50 50 5050 57 57 57 57 57 5750 57 57 57 57 57 5750 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- --- ---50 57 57 57 57 57 57--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 57 57 57 57 57 57--- --- --- --- --- --- ------ --- --- --- --- --- ---50 57 57 57 57 57 5750 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DA68 DA71 DA72 DA73 DA78 DA80 DA811200
B ≈
50 57 57 57 57 57 5750 50 50 50 50 50 5050 57 57 57 57 57 57--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
20 30 30 30 30 20 2020 30 30 30 30 20 20--- --- --- --- --- --- ---20 30 30 30 30 20 20--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 30 30 30 --- 20 ---20 30 30 30 --- 20 ------ --- --- --- --- --- ---20 30 30 30 30 20 20--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 30 30 30 30 20 2020 30 30 30 30 20 20
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
--- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X --- X ------ --- --- --- --- --- ---X X X X X X X
* Ə1 Ə1 Ə1 Ə --- Ə1 ---50 X 50 50 --- X ------ --- --- --- --- --- ---
1000 1500 1000 1500 --- 1500 ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DA82 DA84 DA86 DA87 DA88 DA89 DA901500 1500
Ñ ≈ Ñ ≈
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X --- X X
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- X --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- X Ð --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
--- --- --- --- --- X XX X X X X X X
X^ X^ X^ X^ X^ X^ X^
X X X X --- X X
X 20 20 X X 20 20--- --- --- X --- --- ------ --- --- X --- --- ------ --- --- X --- --- ---X // // X X // //
X X X X X 30 30X X X X X 30 30X 30 30 X X 30 30X 30 30 X X 30 30
--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X --- 30 30X X X X X 30 30X X X X --- 30 30X X X X X 30 30X X X X X 30 30--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X 30 30X X X X --- 30 30X X X X X 30 30--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X --- 30 30--- --- --- --- --- --- ---X X X X X 30 30
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DA82 DA84 DA86 DA87 DA88 DA89 DA901500 1500
Ñ ≈ Ñ ≈
X X X 40 30 30 30X X X 40 30 30 30X X X 40 30 30 30X X X 40 30 30 30X X X 40 30 30 30X X X 40 --- 30 30X X X 40 30 30 30X X X --- --- 30 30--- --- --- 40 --- --- ------ --- --- --- --- --- ---X X X 40 30 30 30X X X 40 --- 30 30X X X 40 30 30 30--- --- --- --- --- --- ---X X X 40 30 30 30
X X X 50 --- 30 30X X X 50 --- 30 30
X X X 50 30 50 50X X X 50 30 50 50X X X 50 30 50 50X X X 50 30 50 50X X X 50 30 50 50--- --- --- 50 --- --- ---X X X 50 30 50 50X X X 50 30 50 50X X X 50 30 50 50X 50 50 50 --- 50 50X 50 50 50 --- 50 50--- --- --- 50 --- --- ---X X X 50 30 50 50X X X 50 --- 50 50
--- --- --- --- --- --- ---X X X 30 30 30 30X X X 30 30 30 30
1000 1000 1000 1000 --- --- ------ --- --- --- --- --- ---X X X 50 --- 30 30X X X 50 --- 30 30X X X 50 --- 30 30X X X 50 --- 30 30X X X 50 --- 30 30X X X 50 --- 30 30X X X 50 --- 30 30X X X 50 --- 30 30X X X 50 --- 30 30--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X 50 --- 30 30X X X 50 --- 30 30
--- --- --- --- --- --- ---X X X 50 --- 30 30
--- --- --- --- --- --- ---X 50 57 50 --- 50 50X 50 50 50 --- 50 50X 50 50 50 --- 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DA82 DA84 DA86 DA87 DA88 DA89 DA901500 1500
Ñ ≈ Ñ ≈
X 50 57 50 --- 50 50X 50 50 50 --- 50 50X 50 50 50 --- 50 50X 50 57 50 --- 50 50X 50 50 50 --- 50 50X 50 57 50 --- 50 50X 50 50 50 --- 50 50X 50 50 50 --- 50 50X 50 57 50 --- 50 50X 50 50 50 --- 50 50
--- --- --- --- --- --- ---X 50 50 50 --- 50 50X 50 50 50 --- 50 50X 50 50 50 --- 50 50X 50 50 50 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---X 50 50 50 --- 50 50
--- --- --- 50 --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---X 50 50 50 30 50 50X 50 50 50 --- 50 50X 50 57 50 --- 50 50--- --- --- 50 --- --- ---X 50 50 50 --- 50 50X 50 57 50 --- 50 50--- --- --- 50 --- --- ---X 50 50 50 --- 50 50X 50 50 50 --- 50 50X 50 57 50 --- 50 50X 50 57 50 --- 50 50X 50 50 50 --- 50 50X 50 50 50 --- 50 50X 50 57 50 --- 50 50X 50 57 50 --- 50 50X 50 57 50 --- 50 50X 50 50 50 --- 50 50X 50 50 50 --- 50 50X 50 57 50 --- 50 50X 50 50 50 --- 50 50X 50 50 50 --- 50 50X 50 57 50 --- 50 50X 50 50 50 --- 50 50X 50 50 50 --- 50 50X 50 57 50 --- 50 50X 50 57 50 --- 50 50X 50 50 50 --- 50 50X 50 50 50 --- 50 50--- --- --- --- --- --- ---X 50 57 50 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---X 50 50 50 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---X 50 50 50 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X 50 57 50 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---X 50 57 50 --- 50 50X 50 50 50 --- 50 50X 50 50 50 --- 50 50--- --- --- --- --- --- ---X 50 50 50 --- 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DA82 DA84 DA86 DA87 DA88 DA89 DA901500 1500
Ñ ≈ Ñ ≈
X 50 57 50 --- 50 50X 50 50 50 --- 50 50X 50 57 50 --- 50 50--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---X 50 50 50 --- 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
I500
--- 50 --- --- --- 50 50
X 30 30 50 30 30 30X 30 30 50 30 30 30--- --- --- --- --- --- ---X 30 30 50 30 30 30--- --- --- 30 --- --- ------ --- --- 30 --- --- --- --- --- --- --- --- --- ---X 30 30 30 --- 30 30X 30 --- 30 --- 30 30--- --- --- 30 --- --- ---X 30 30 30 30 30 30--- --- --- 30 --- --- --- --- --- --- --- --- --- ---X 50 50 50 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 30 --- --- --- 30 30--- --- --- 30 --- --- ------ --- --- 30 --- --- ---X 30 30 30 30 30 30X 30 30 30 30 30 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- 30 --- --- --- --- --- --- --- --- --- ---X X X 30 30 X X
--- --- --- --- --- --- ---X X X 30 30 X XX X X 30 30 X XX X X 30 30 X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X 30 --- X X--- --- --- --- --- --- ---X X X 30 30 X X
Ə1 Ə1 --- Ə1 --- Ə1 Ə1X X --- X --- 50 50--- --- --- --- --- --- ---
1000 1250 --- 1000 --- 1500 1500--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DA91 DA92 DA93 DA94 DA95 DA96 DA97
æ
20 20 X 30 X X X20 20 X 30 X X X20 20 X 30 X X X--- --- --- --- --- --- ---20 --- X --- X X X
20 20 X 30 X X X20 20 X 30 X X Þ X20 20 X 30 X --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---20 20 X 30 X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 X 30 X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 X 30 X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 X 30 X X X
20 20 X 30 X X X20 20 X 30 X X X
--- --- --- --- --- --- ---20 20 X 30 X X X
20^ 20^ X^ 30^ X^ X^ X^
20 20 X --- X X X
20 20 X 30 X --- X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 20 X 30 X X X
X X 30 30 X X XX X 30 30 X X X30 30 30 30 X X X30 30 30 30 X X X --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X 30 --- X --- XX X 30 30 X --- XX X 30 --- X --- XX X 30 30 X --- XX X 30 30 X --- X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X 30 30 X X XX X 30 --- X --- XX X 30 30 X --- X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X 30 --- X --- X--- --- --- --- --- --- ---X X 30 30 X X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DA91 DA92 DA93 DA94 DA95 DA96 DA97
æ
X X 30 30 X --- XX X 30 30 X --- XX X 30 30 X --- XX X 30 30 X X XX X 30 30 X X XX --- 30 30 X --- XX X 30 30 X X XX --- 30 30 X --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X 30 30 X --- XX --- 30 --- X --- XX X 30 30 X --- X--- --- --- --- --- --- ---X X 30 30 X X X
X --- 50 --- X X XX --- 50 --- X X X
800X X X 30 X X XX X X 30 X X XX X X 30 X X XX X X 30 X X XX X X 30 X X X--- --- --- --- --- --- ---X X X 30 X X XX X X 30 X X XX X X 30 X X X50 50 50 --- X X X50 50 50 --- X --- X--- --- --- --- --- --- ---X X X 30 X X XX X X --- X X X
--- --- --- --- --- --- ---X X 30 30 X X XX X 30 30 X X X
1000 --- 1000 --- 800 800 1000--- --- --- --- --- --- ---X --- 50 --- --- --- XX --- 50 --- X --- XX --- 50 --- --- --- XX --- 50 --- --- --- XX --- 50 --- X X XX --- 50 --- --- --- XX --- 50 --- --- --- XX --- 50 --- --- --- XX --- 50 --- --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---X --- 50 --- --- --- XX --- 50 --- X X X
--- --- --- --- --- --- ---X --- 50 --- X X X
@800
--- --- --- --- --- --- ---57 57 50 --- --- --- X50 50 50 --- --- --- X50 50 50 --- --- --- X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DA91 DA92 DA93 DA94 DA95 DA96 DA97
æ
57 57 50 --- --- --- X50 50 50 --- --- --- X50 50 50 --- --- --- X57 57 50 --- --- --- X50 50 50 --- --- --- X57 57 50 --- --- --- X50 50 50 --- --- --- X50 50 50 --- --- --- X57 57 50 --- --- --- X50 50 50 --- --- --- X --- --- --- --- --- --- ---50 50 50 --- X X X50 50 50 --- --- X X50 50 50 --- X X X50 50 50 --- X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- X X X --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 30 X X X50 50 50 --- --- --- X57 57 50 --- --- --- X--- --- --- --- --- --- ---50 50 50 --- --- --- X57 57 50 --- --- --- X--- --- --- --- --- --- ---50 50 50 --- --- --- X50 50 50 --- --- --- X57 57 50 --- --- --- X57 57 50 --- --- --- X50 50 50 --- --- --- X50 50 50 --- --- --- X57 57 50 --- --- --- X57 57 50 --- --- --- X57 57 50 --- --- --- X50 50 50 --- --- --- X50 50 50 --- --- --- X57 57 50 --- --- --- X50 50 50 --- --- --- X50 50 50 --- --- --- X57 57 50 --- --- --- X50 50 50 --- X --- X50 50 50 --- X --- X57 57 50 --- --- --- X57 57 50 --- --- --- X50 50 50 --- X --- X50 50 50 --- X --- X--- --- --- --- --- --- ---57 57 50 --- --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---57 57 50 --- --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---57 57 50 --- --- --- X50 50 50 --- X --- X50 50 50 --- X --- X--- --- --- --- --- --- ---50 50 50 --- --- --- X--- --- --- --- --- --- ---
January 01, 2016
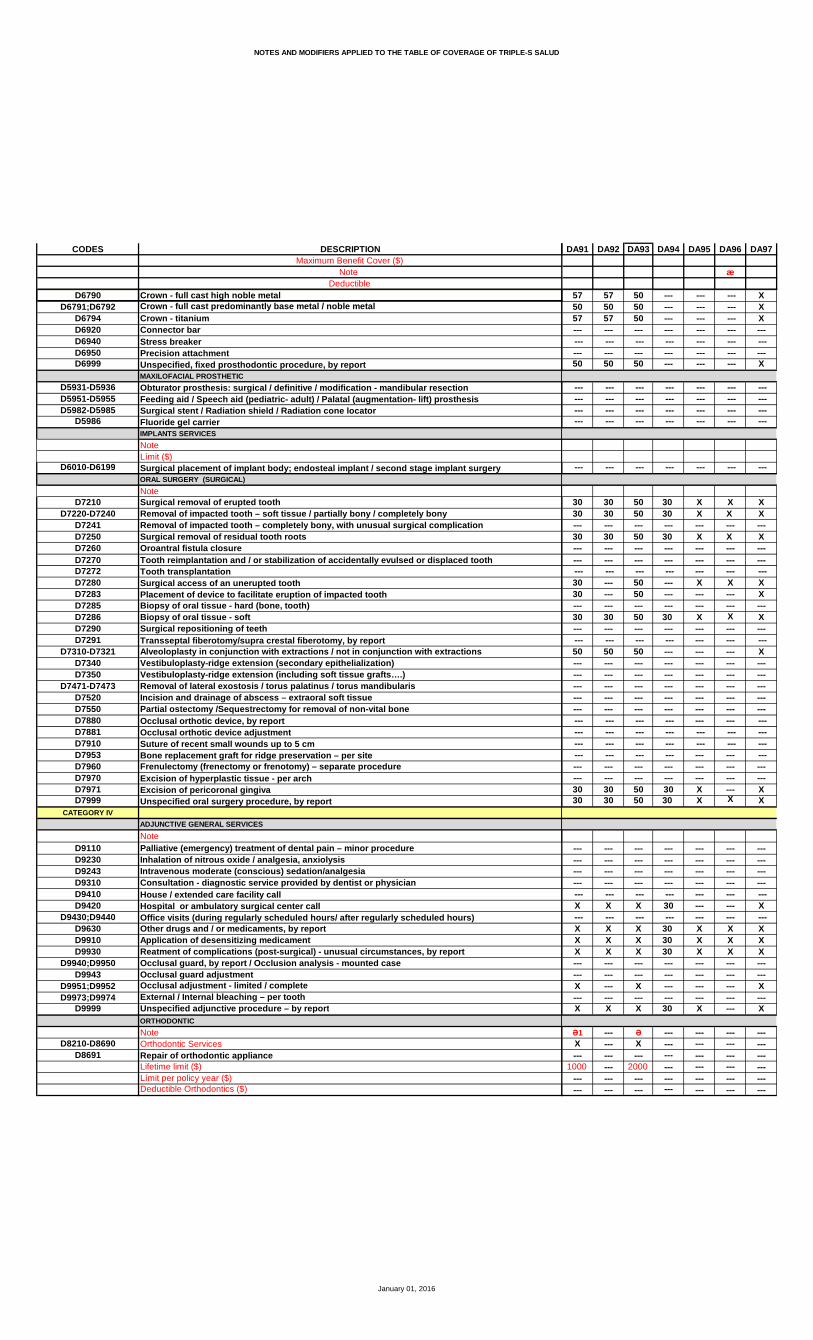
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DA91 DA92 DA93 DA94 DA95 DA96 DA97
æ
57 57 50 --- --- --- X50 50 50 --- --- --- X57 57 50 --- --- --- X--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- --- --- X
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 30 50 30 X X X30 30 50 30 X X X--- --- --- --- --- --- ---30 30 50 30 X X X--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 --- 50 --- X X X30 --- 50 --- --- --- X--- --- --- --- --- --- ---30 30 50 30 X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 50 --- --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 30 50 30 X --- X30 30 50 30 X X X
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X 30 --- --- X
--- --- --- --- --- --- ---X X X 30 X X XX X X 30 X X XX X X 30 X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X --- X --- --- --- X--- --- --- --- --- --- ---X X X 30 X --- X
Ə1 --- Ə --- --- --- ---X --- X --- --- --- ------ --- --- --- --- --- ---
1000 --- 2000 --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DA98 DA99 DB01 DB02 DB03 DB04 DB061000
U ≈
X X X X X X XX X X X 30 X XX X X X 30 X X--- --- --- --- --- --- ------ --- X X --- X X
X X X X 30 X XX X X X 30 Þ X XX X X --- 30 X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X 30 X X--- --- --- --- --- --- ------ --- --- X --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 30 L X X--- --- --- X Ð --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X --- 30 X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 30 X X
X X X X 30 X XX X X X 30 X X
--- --- --- --- --- X ---X X X X 30 X X
X^ X^ X^ X ^ 30^ X^ ---
X --- X X --- X X
20 X 20 X 30 20 20--- --- --- X --- --- ------ --- --- X --- --- ------ --- --- X --- --- ---// X // X 30 // //
X 30 X 30 25 X 20X 30 X 30 25 X 2030 30 30 30 25 30 2030 30 30 30 25 30 20 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X --- X --- --- X 20X 30 X 30 25 X 20--- --- X 30 --- X 20X 30 X 30 25 X 20X 30 X 30 25 X 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X 30 X 30 25 X 20--- --- X 30 --- X 20X 30 X 30 25 X 20--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- X 30 --- X 20--- --- --- --- --- --- ---X 30 X 30 25 X 20
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DA98 DA99 DB01 DB02 DB03 DB04 DB061000
U ≈
X 30 20 40 25 30 50X 30 20 40 25 30 50X 30 20 40 25 30 50X 30 20 40 25 30 50X 30 20 40 25 30 50--- --- 20 40 --- 30 50X 30 20 --- 25 30 50--- --- 20 --- --- 30 50--- --- --- 40 --- --- ------ --- --- --- --- --- ---X 30 20 40 25 30 50--- --- 20 --- --- 30 50X 30 20 40 25 30 50--- --- --- --- --- --- ---X 30 20 40 25 30 50
--- --- 20 --- --- X 50--- --- 20 50 --- X 50
X 30 X 50 30 X XX 30 X 50 30 X XX 30 X 50 30 X XX 30 X 50 30 X XX 30 X 50 30 X X--- --- --- 50 --- --- ---X 30 X 50 30 X XX 30 X 50 30 X XX 30 X 50 K 30 X X--- --- 50 --- --- 50 50 --- --- 50 50 --- 50 50--- --- --- 50 --- --- ---X 30 X 50 30 X XX --- X --- --- X X
--- --- --- --- --- --- ---X 30 20 30 25 X 50X 30 20 30 25 X 50
--- --- 1000 1000 --- --- 1000--- --- --- --- --- --- ------ --- 20 50 --- X 50--- --- 20 50 --- X 50--- --- 20 --- --- X 50--- --- 20 --- --- X 50--- --- 20 50 --- X 50--- --- 20 --- --- X 50--- --- 20 --- --- X 50--- --- 20 50K --- X 50--- --- 20 --- --- X 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- 20 --- --- X 50--- --- 20 50 --- X 50 --- --- --- --- --- --- ------ --- 20 50 --- X 50
--- --- --- --- --- --- ------ --- 50 --- --- 50 57--- --- 50 --- --- 50 50--- --- 50 50 --- 50 50
January 01, 2016
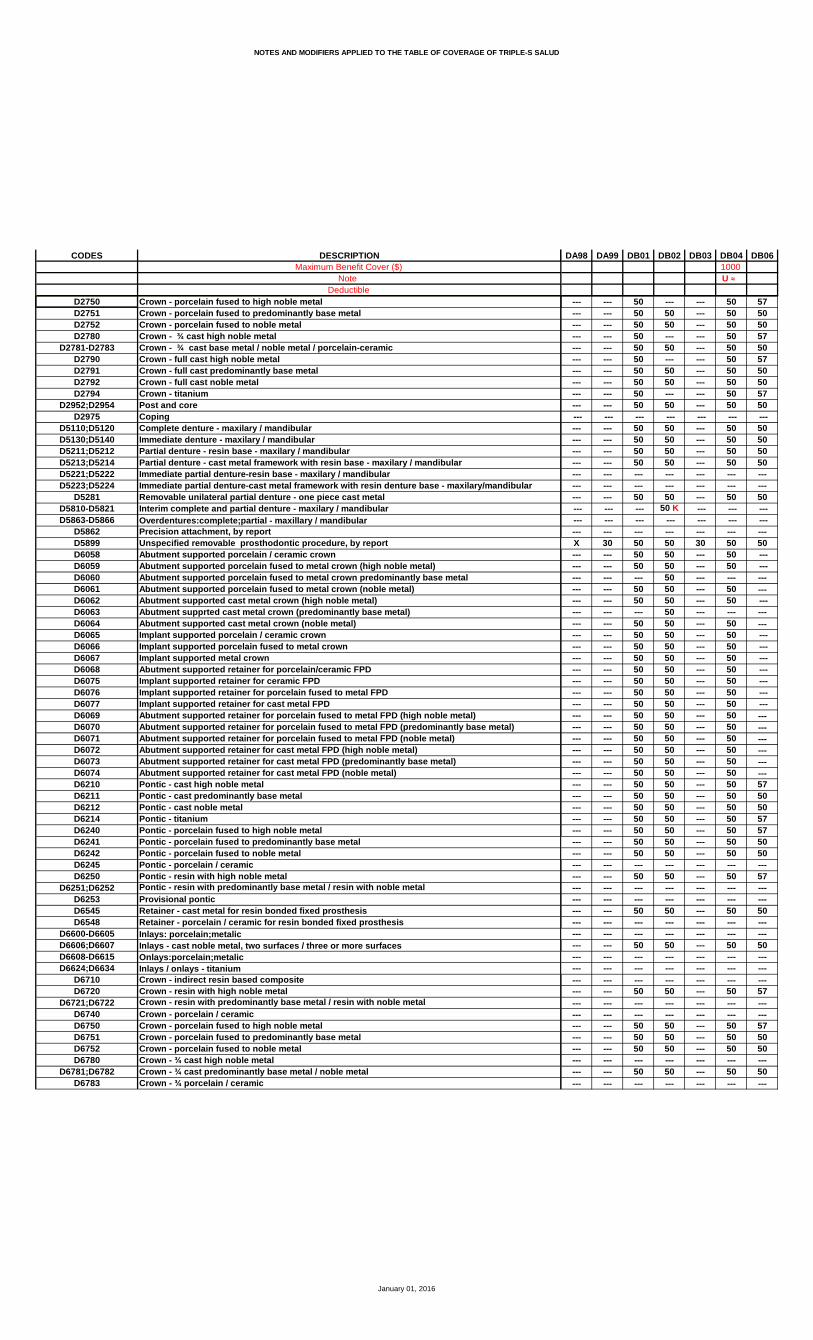
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DA98 DA99 DB01 DB02 DB03 DB04 DB061000
U ≈
--- --- 50 --- --- 50 57--- --- 50 50 --- 50 50--- --- 50 50 --- 50 50--- --- 50 --- --- 50 57--- --- 50 50 --- 50 50--- --- 50 --- --- 50 57--- --- 50 50 --- 50 50--- --- 50 50 --- 50 50--- --- 50 --- --- 50 57--- --- 50 50 --- 50 50 --- --- --- --- --- --- ------ --- 50 50 --- 50 50--- --- 50 50 --- 50 50--- --- 50 50 --- 50 50--- --- 50 50 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- 50 50 --- 50 50 --- --- --- 50 K --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---X 30 50 50 30 50 50--- --- 50 50 --- 50 ------ --- 50 50 --- 50 ------ --- --- 50 --- --- ------ --- 50 50 --- 50 ------ --- 50 50 --- 50 ------ --- --- 50 --- --- ------ --- 50 50 --- 50 ------ --- 50 50 --- 50 ------ --- 50 50 --- 50 ------ --- 50 50 --- 50 ------ --- 50 50 --- 50 ------ --- 50 50 --- 50 ------ --- 50 50 --- 50 ------ --- 50 50 --- 50 ------ --- 50 50 --- 50 ------ --- 50 50 --- 50 ------ --- 50 50 --- 50 ------ --- 50 50 --- 50 ------ --- 50 50 --- 50 ------ --- 50 50 --- 50 ------ --- 50 50 --- 50 57--- --- 50 50 --- 50 50--- --- 50 50 --- 50 50--- --- 50 50 --- 50 57--- --- 50 50 --- 50 57--- --- 50 50 --- 50 50--- --- 50 50 --- 50 50--- --- --- --- --- --- ------ --- 50 50 --- 50 57--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- 50 50 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- 50 50 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- 50 50 --- 50 57--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- 50 50 --- 50 57--- --- 50 50 --- 50 50--- --- 50 50 --- 50 50--- --- --- --- --- --- ------ --- 50 50 --- 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DA98 DA99 DB01 DB02 DB03 DB04 DB061000
U ≈
--- --- 50 50 --- 50 57--- --- 50 50 --- 50 50--- --- 50 50 --- 50 57--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- 50 50 --- 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 30 20 50 25 30 5030 30 20 50 25 30 50--- --- --- --- --- --- ---30 30 20 50 25 30 50--- --- --- 30 --- --- ------ --- --- 30 --- --- --- --- --- --- --- --- --- ---30 --- 20 30 --- 30 50--- --- 20 30 --- 30 ------ --- --- 30 --- --- ---30 30 20 30 25 30 ------ --- --- 30 --- --- --- --- --- --- --- --- --- ------ --- 50 50 --- 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- 30 --- --- ------ --- --- 30 --- --- ---30 30 20 30 25 30 ---30 30 20 30 25 30 50
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- X --- --- --- --- --- --- --- --- --- --- --- 30 X X 30 X --- --- --- --- --- --- --- ---X 30 X X 30 X XX 30 X X 25 X XX 30 X X 25 X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- X X --- X 50--- --- --- --- --- --- ---X 30 X X 30 X X
--- --- Ə1 Ə1 --- ** Ə1 ------ --- X X --- 50 ------ --- --- --- --- --- ------ --- 1500 1000 --- 1000 ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DB10 DB13 DB14 DB151500 1000 1000
Ñ ≈ Ø Ø
X X X XX X X XX X X X--- --- --- ---X X --- ---
X X X XX X X XX X --- ------ --- --- ------ --- --- ---X X X X--- --- --- ------ --- --- ------ --- --- --- --- --- --- ---X X X X--- --- --- ---
--- --- --- --- --- --- --- ---X X --- ------ --- --- --- --- --- --- ---X X X X
X X X XX X --- ---
X --- --- ---X X X X
X^ X^ --- ---
X X X X
20 20 --- ------ --- --- ------ --- --- ------ --- --- ---// // X X
X X X 20X X X 2030 30 --- 3030 30 --- 30 --- --- --- --- --- --- --- ------ --- --- --- --- --- --- ---X X --- ---X X --- ---X X --- ---X X --- ---X X --- ------ --- --- ------ --- --- ------ --- --- ---X X X 20X X --- ---X X --- ------ --- --- --- --- --- --- ---X X --- ------ --- --- ---X X X //
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DB10 DB13 DB14 DB151500 1000 1000
Ñ ≈ Ø Ø
X 20 --- 20X 20 --- 20X 20 --- ---X 20 X ---X 20 X 20X 20 --- 50X 20 --- 20X 20 --- 50--- --- --- ------ --- --- ---X 20 --- ---X 20 --- ---X 20 --- ------ --- --- ---X 20 X //
X X --- ---X X --- X
X X --- 20X X --- 20X X --- 30X X --- 30X X --- 30--- --- --- ---X X --- 30X X --- 30X X --- 3050 50 --- 5050 50 --- 50--- --- --- 20X X --- ---X X --- ---
--- --- --- ---X X X 20X X X ---
--- 1000 --- ------ --- --- ---X X --- ---X X --- ---X X --- ---X X --- ---X X --- ---X X --- ---X X --- ---X X --- ---X X --- ------ --- --- ------ --- --- ---X X --- ---X X --- ---
--- --- --- ---X X --- ---
--- --- --- ---57 50 --- ---50 50 --- ---50 50 --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DB10 DB13 DB14 DB151500 1000 1000
Ñ ≈ Ø Ø
57 50 --- ---50 50 --- ---50 50 --- ---57 50 --- ---50 50 --- ---57 50 --- ---50 50 --- ---50 50 --- ---57 50 --- ---50 50 --- --- --- --- --- ---50 50 --- 5050 50 --- 5050 50 --- 5050 50 --- 50--- --- --- ------ --- --- ---50 50 --- --- --- --- --- --- --- --- --- ------ --- --- ---50 50 --- //50 50 --- ---57 50 --- ------ --- --- ---50 50 --- ---57 50 --- ------ --- --- ---50 50 --- ---50 50 --- ---57 50 --- ---57 50 --- ---50 50 --- ---50 50 --- ---57 50 --- ---57 50 --- ---57 50 --- ---50 50 --- ---50 50 --- ---57 50 --- ---50 50 --- ---50 50 --- ---57 50 --- ---50 50 --- ---50 50 --- ---57 50 --- ---57 50 --- ---50 50 --- ---50 50 --- ------ --- --- ---57 50 --- ------ --- --- ------ --- --- ---50 50 --- ------ --- --- ------ --- --- ---50 50 --- ------ --- --- ------ --- --- ------ --- --- ---57 50 --- ------ --- --- ------ --- --- ---57 50 --- ---50 50 --- ---50 50 --- ------ --- --- ---50 50 --- ------ --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DB10 DB13 DB14 DB151500 1000 1000
Ñ ≈ Ø Ø
57 50 --- ---50 50 --- ---57 50 --- ------ --- --- --- --- --- --- ------ --- --- ---50 50 --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- ---
30 20 --- 3030 20 --- 30--- --- --- ---30 20 --- 30--- --- --- ------ --- --- --- --- --- --- ---30 20 --- ---30 20 --- ------ --- --- ---30 20 --- ------ --- --- --- --- --- --- ---50 50 --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- ------ --- --- ---30 20 --- ---30 20 --- 30
--- --- --- ------ --- --- ------ --- --- ------ --- --- --- --- --- --- ---X X --- ---
--- --- --- ---X X --- ---X X X ---X X X ------ --- --- ------ --- --- ---X X --- ------ --- --- ---X X X X
Ə1 Ə1 --- ---X X --- ------ --- --- ---
1000 1500 --- ------ --- --- ------ --- --- ---
January 01, 2016
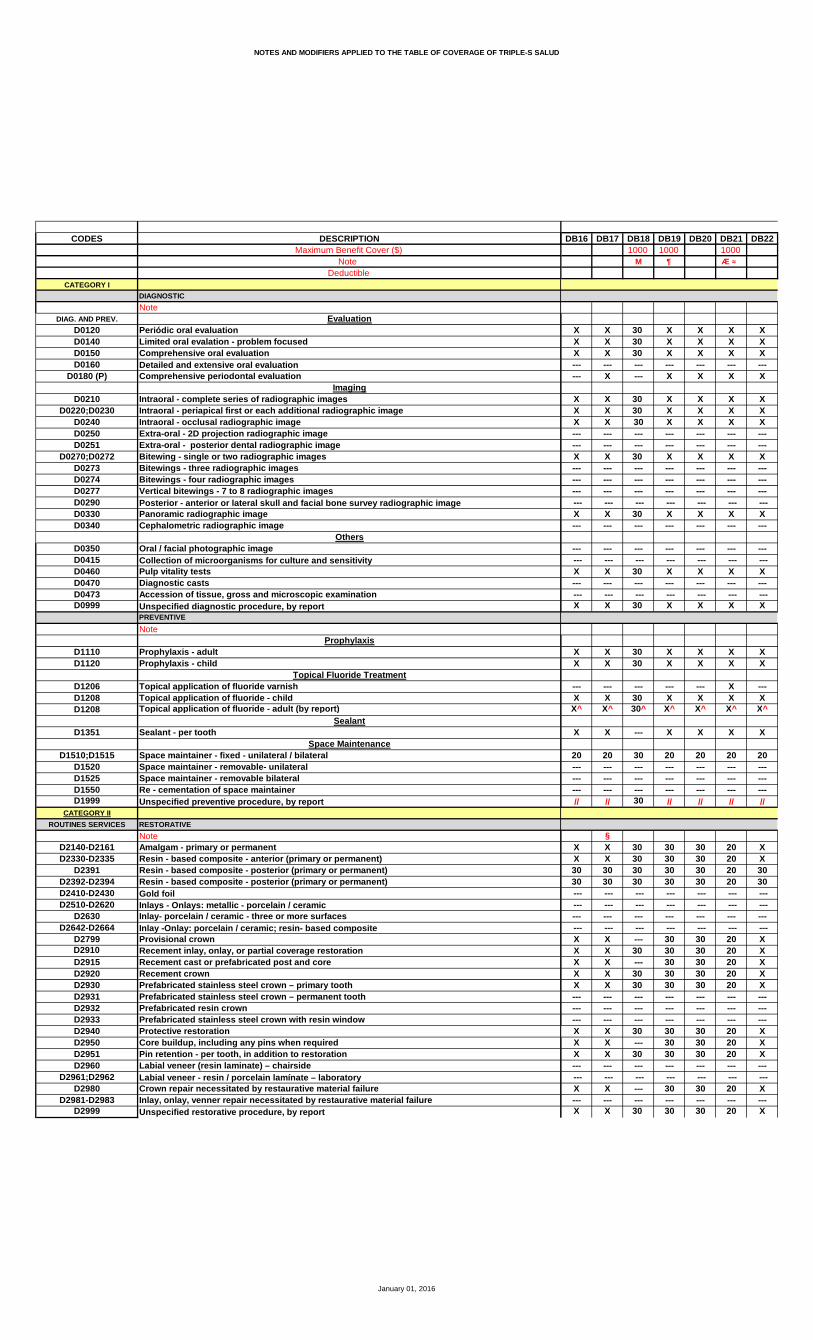
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DB16 DB17 DB18 DB19 DB20 DB21 DB221000 1000 1000
M ¶ Æ ≈
X X 30 X X X XX X 30 X X X XX X 30 X X X X--- --- --- --- --- --- ------ X --- X X X X
X X 30 X X X XX X 30 X X X XX X 30 X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X 30 X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X 30 X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X 30 X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X 30 X X X X
X X 30 X X X XX X 30 X X X X
--- --- --- --- --- X ---X X 30 X X X X
X^ X^ 30^ X^ X^ X^ X^
X X --- X X X X
20 20 30 20 20 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// // 30 // // // //
§X X 30 30 30 20 XX X 30 30 30 20 X30 30 30 30 30 20 3030 30 30 30 30 20 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X --- 30 30 20 XX X 30 30 30 20 XX X --- 30 30 20 XX X 30 30 30 20 XX X 30 30 30 20 X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X 30 30 30 20 XX X --- 30 30 20 XX X 30 30 30 20 X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X --- 30 30 20 X--- --- --- --- --- --- ---X X 30 30 30 20 X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DB16 DB17 DB18 DB19 DB20 DB21 DB221000 1000 1000
M ¶ Æ ≈
X X 30 30 30 X XX X 30 30 30 X XX X 30 30 30 X XX X 30 30 30 X XX X 30 30 30 X X--- X --- 30 30 X XX X 30 30 30 X X--- X --- 30 30 X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X 30 30 30 X X--- X --- 30 30 X XX X 30 30 30 X X--- --- --- --- --- --- ---X X 30 30 30 X X
--- X --- X X X X--- X --- X X X X
X X 30 X X X XX X 30 X X X XX X 30 X X X XX X 30 X X X XX X 30 X X X X--- --- --- --- --- --- ---X X 30 X X X XX X 30 X X X XX X 30 X X X X50 50 --- 50 50 50 5050 50 --- 50 50 50 50--- --- --- --- --- --- ---X X 30 X X X XX X --- X X X X
--- --- --- --- --- --- ---X X 30 X X 20 XX X 30 X X 20 X
§--- --- --- 1000 1000 1000 1333--- --- --- --- --- --- ------ X --- X X X X--- X --- X X X X--- X --- X X X X--- X --- X X X X--- X --- X X X X--- X --- X X X X--- X --- X X X X--- X --- X X X X--- X --- X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ X --- X X X X--- X --- X X X X --- --- --- --- --- --- ------ X --- X X X X
--- --- --- --- --- --- ---57 50 --- 50 50 50 5750 50 --- 50 50 50 5050 50 --- 50 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DB16 DB17 DB18 DB19 DB20 DB21 DB221000 1000 1000
M ¶ Æ ≈
57 50 --- 50 50 50 5750 50 --- 50 50 50 5050 50 --- 50 50 50 5057 50 --- 50 50 50 5750 50 --- 50 50 50 5057 50 --- 50 50 50 5750 50 --- 50 50 50 5050 50 --- 50 50 50 5057 50 --- 50 50 50 5750 50 --- 50 50 50 50 --- --- --- --- --- --- ---50 50 --- 50 50 50 5050 50 --- 50 50 50 5050 50 --- 50 50 50 5050 50 --- 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 30 50 50 50 5050 50 --- 50 50 50 5057 50 --- 50 50 50 57--- --- --- --- --- --- ---50 50 --- 50 50 50 5057 50 --- 50 50 50 57--- --- --- --- --- --- ---50 50 --- 50 50 50 5050 50 --- 50 50 50 5057 50 --- 50 50 50 5757 50 --- 50 50 50 5750 50 --- 50 50 50 5050 50 --- 50 50 50 5057 50 --- 50 50 50 5757 50 --- 50 50 50 5757 50 --- 50 50 50 5750 50 --- 50 50 50 5050 50 --- 50 50 50 5057 50 --- 50 50 50 5750 50 --- 50 50 50 5050 50 --- 50 50 50 5057 50 --- 50 50 50 5750 50 --- 50 50 50 5050 50 --- 50 50 50 5057 50 --- 50 50 50 5757 50 --- 50 50 50 5750 50 --- 50 50 50 5050 50 --- 50 50 50 50--- --- --- --- --- --- ---57 50 --- 50 50 50 57--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---57 50 --- 50 50 50 57--- --- --- --- --- --- ------ --- --- --- --- --- ---57 50 --- 50 50 50 5750 50 --- 50 50 50 5050 50 --- 50 50 50 50--- --- --- --- --- --- ---50 50 --- 50 50 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DB16 DB17 DB18 DB19 DB20 DB21 DB221000 1000 1000
M ¶ Æ ≈
57 50 --- 50 50 50 5750 50 --- 50 50 50 5057 50 --- 50 50 50 57 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 30 30 30 30 20 3030 30 30 30 30 20 30--- --- --- --- --- --- ---30 30 30 30 30 20 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ 30 --- 30 30 20 30--- 30 --- 30 30 20 30--- --- --- --- --- --- ---30 30 30 30 30 20 30--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 --- 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 30 30 30 30 20 3030 30 30 30 30 20 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X 30 X X X X
--- --- --- --- --- --- ---X X 30 X X X XX X 30 X X X XX X 30 X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ X --- X X X X--- --- --- --- --- --- ---X X 30 X X X X
Ə1 Ə1 --- --- Ə1 Ə1 Ə1X X --- --- X X X--- --- --- --- --- --- ---
1000 1000 --- --- 1000 1000 1250--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DB23 DB24 DB25 DB26 DB27 DB28 DB291000 1000 1000 1200
Æ ≈ Æ ¶ ≈ B ≈
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
--- X --- --- X X ---X X X X X X X
X^ X^ X^ X^ X^ X^ X^
X X X X X X X
20 20 20 X 20 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// // // X // // //
25 X 20 20 25 20 X25 X 20 20 25 20 X25 30 20 20 25 20 3025 30 20 20 25 20 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---25 X 20 X 25 20 X25 X 20 X 25 20 X25 X 20 X 25 20 X25 X 20 X 25 20 X25 X 20 20 25 20 X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---25 X 20 X 25 20 X25 X 20 X 25 20 X25 X 20 X 25 20 X--- --- --- --- --- --- --- --- --- --- --- --- --- ---25 X 20 X 25 20 X--- --- --- --- --- --- ---25 X 20 X 25 20 X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DB23 DB24 DB25 DB26 DB27 DB28 DB291000 1000 1000 1200
Æ ≈ Æ ¶ ≈ B ≈
X X X 20 25 20 XX X X 20 25 20 XX X X 20 25 20 XX X X 20 25 20 XX X X 20 25 20 XX X X 20 25 20 XX X X 20 25 20 XX X X 20 25 20 X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X 20 25 20 XX X X 20 25 20 XX X X 20 25 20 X--- --- --- --- --- --- ---X X X 20 25 20 X
X X X 20 X X XX X X 20 X X X
X X X X X X XX X X X X X XX X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X50 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- --- ---X X X X X X XX X X X X X X
--- --- --- --- --- --- ---X X X 20 25 20 XX X X 20 25 20 X
1000 1000 1000 1000 1000 1000 1000--- --- --- --- --- --- ---X X X 20 X X XX X X 20 X X XX X X 20 X X XX X X 20 X X XX X X 20 X X XX X X 20 X X XX X X 20 X X XX X X 20 X X XX X X 20 X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X 20 X X XX X X 20 X X X
--- --- --- --- --- --- ---X X X 20 X X X
--- --- --- --- --- --- ---50 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DB23 DB24 DB25 DB26 DB27 DB28 DB291000 1000 1000 1200
Æ ≈ Æ ¶ ≈ B ≈
50 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 50 --- --- --- --- --- --- ---50 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- --- ---50 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- --- ---50 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DB23 DB24 DB25 DB26 DB27 DB28 DB291000 1000 1000 1200
Æ ≈ Æ ¶ ≈ B ≈
50 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- 50 ---
30 30 30 20 25 20 3030 30 30 20 25 20 30--- --- --- --- --- --- ---30 30 30 20 25 20 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 30 30 20 25 20 3030 30 30 20 25 20 30--- --- --- --- --- --- ---30 30 30 20 25 20 30--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- 20 --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- 20 --- --- ------ --- --- --- --- --- ---30 30 30 20 25 20 3030 30 30 20 25 20 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
--- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---X X X X X X X
Ə1 Ə1 Ə1 Ə1 Ə1 Ə1X X X 50 --- 50 X--- --- --- --- --- --- ---
1000 1000 1000 1000 --- 1000 1000--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DB30 DB31 DB32 DB33 DB34 DB35 DB361000 1000
& Æ ≈
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X --- X X --- --- X
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
--- --- --- X --- --- ---X X X X X X X
X^ X^ X^ X^ X^ X^ X^
X X X X X --- X
X X 20 X 20 X X--- X --- --- --- --- ------ X --- --- --- --- ------ X --- --- --- --- ---X X // X // X X
20 25 30 20 X X X20 25 X 20 X X X20 25 30 20 30 X 3020 25 30 20 30 X 30 --- --- --- --- --- --- ---50 --- --- --- --- --- ---50 --- --- --- --- --- ---50 --- --- --- --- --- ---20 X X 20 X --- X20 X X 20 X X X20 --- X 20 --- --- X20 X X 20 X X X20 25 X 20 X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X 25 X 20 X X X20 --- X 20 --- --- X20 X X 20 X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---20 --- X 20 --- --- X--- --- --- --- --- --- ---20 X X 20 X X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DB30 DB31 DB32 DB33 DB34 DB35 DB361000 1000
& Æ ≈
20 X 50 20 X X X20 X 50 20 X X X20 X 50 20 X X X20 25 50 20 X X X20 25 50 20 X X X20 25 50 20 --- --- X20 25 50 20 X X X20 25 50 20 --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---20 X 50 20 X X X20 --- 50 20 --- --- ---20 X 50 20 X X X--- --- --- --- --- --- ---20 X 50 20 X X X
20 --- 50 20 --- --- 2520 --- 50 20 --- --- 25
X X X X X X XX X X X X X XX X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X50 --- 50 50 --- --- 5050 --- 50 50 --- --- 50--- --- --- --- --- --- ---X X X X X X XX X X X X --- X
--- --- --- --- --- --- ---20 25 X 20 X X X20 25 X 20 X X X
1000 --- 1000 1000 --- --- 1000--- --- --- --- --- --- ---20 --- 50 20 --- --- 2520 --- 50 20 --- --- 2520 --- 50 20 --- --- 2520 --- 50 20 --- --- 2520 --- 50 20 --- --- 2520 --- 50 20 --- --- 2520 --- 50 20 --- --- 2520 --- 50 20 --- --- 2520 --- 50 20 --- --- 25--- --- --- --- --- --- ------ --- --- --- --- --- ---20 --- 50 20 --- --- 2520 --- 50 20 --- --- 25 --- --- --- --- --- --- ---20 --- 50 20 --- --- 25
--- --- --- --- --- --- ---50 --- 50 50 --- --- 5750 --- 50 50 --- --- 5050 --- 50 50 --- --- 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DB30 DB31 DB32 DB33 DB34 DB35 DB361000 1000
& Æ ≈
50 --- 50 50 --- --- 5750 --- 50 50 --- --- 5050 --- 50 50 --- --- 5050 --- 50 50 --- --- 5750 --- 50 50 --- --- 5050 --- 50 50 --- --- 5750 --- 50 50 --- --- 5050 --- 50 50 --- --- 5050 --- 50 50 --- --- 5750 --- 50 50 --- --- 50 --- --- --- --- --- --- ---50 --- 50 50 --- --- 5050 --- 50 50 --- --- 5050 --- 50 50 --- --- 5050 --- 50 50 --- --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 50 --- --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 X 50 50 X X 5050 --- 50 50 --- --- 5050 --- 50 50 --- --- 57--- --- --- --- --- --- ---50 --- 50 50 --- --- 5050 --- 50 50 --- --- 57--- --- --- --- --- --- ---50 --- 50 50 --- --- 5050 --- 50 50 --- --- 5050 --- 50 50 --- --- 5750 --- 50 50 --- --- 5750 --- 50 50 --- --- 5050 --- 50 50 --- --- 5050 --- 50 50 --- --- 5750 --- 50 50 --- --- 5750 --- 50 50 --- --- 5750 --- 50 50 --- --- 5050 --- 50 50 --- --- 5050 --- 50 50 --- --- 5750 --- 50 50 --- --- 5050 --- 50 50 --- --- 5050 --- 50 50 --- --- 5750 --- 50 50 --- --- 5050 --- 50 50 --- --- 5050 --- 50 50 --- --- 5750 --- 50 50 --- --- 5750 --- 50 50 --- --- 5050 --- 50 50 --- --- 50--- --- --- --- --- --- ---50 --- 50 50 --- --- 57--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 50 --- --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 50 --- --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 50 --- --- 57--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 50 --- --- 5750 --- 50 50 --- --- 5050 --- 50 50 --- --- 50--- --- --- --- --- --- ---50 --- 50 50 --- --- 50--- --- --- --- --- --- ---
January 01, 2016
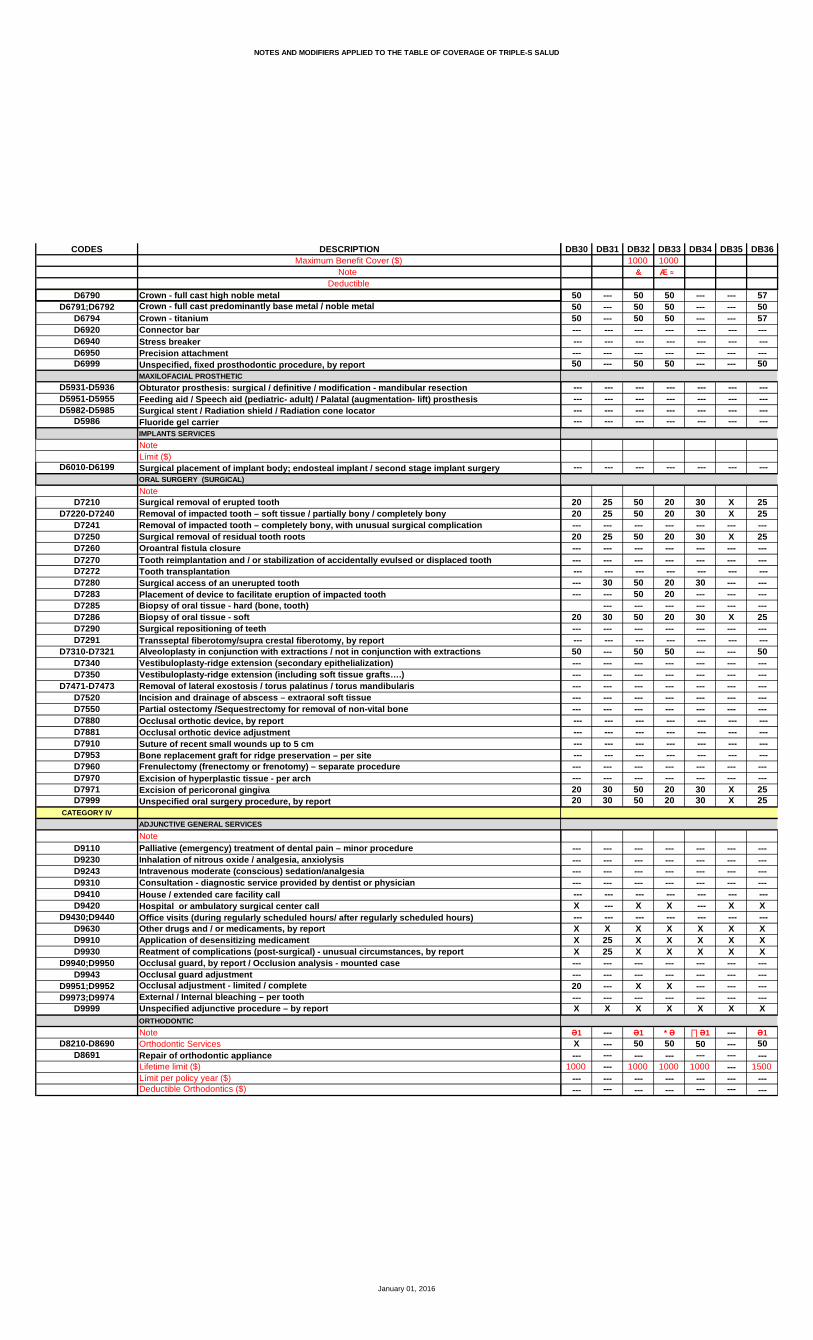
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DB30 DB31 DB32 DB33 DB34 DB35 DB361000 1000
& Æ ≈
50 --- 50 50 --- --- 5750 --- 50 50 --- --- 5050 --- 50 50 --- --- 57--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 50 --- --- 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
20 25 50 20 30 X 2520 25 50 20 30 X 25--- --- --- --- --- --- ---20 25 50 20 30 X 25--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ 30 50 20 30 --- ------ --- 50 20 --- --- ---
--- --- --- --- --- ---20 30 50 20 30 X 25--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 --- 50 50 --- --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 30 50 20 30 X 2520 30 50 20 30 X 25
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X --- X X --- X X
--- --- --- --- --- --- ---X X X X X X XX 25 X X X X XX 25 X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---20 --- X X --- --- ------ --- --- --- --- --- ---X X X X X X X
Ə1 --- Ə1 * Ə ∏ Ə1 --- Ə1X --- 50 50 50 --- 50--- --- --- --- --- --- ---
1000 --- 1000 1000 1000 --- 1500--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DB37 DB38 DB39 DB40 DB41 DB42 DB441000 1000 1000 2000
¶ Æ U ≈ Њ ≈
X X X X X 20 XX X X X X 20 XX X X X X 20 X--- --- --- --- --- --- ---X X X X X --- X
X X X X X 20 XX X X X X Þ 20 XX X X X --- 20 X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X 20 X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X 20 X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X 20 X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X 20 X
X X X X X 20 XX X X X X 20 X
--- --- X --- --- --- XX X X X X 20 X
X^ X^ X^ X^ X^ 20^ X^
X X X X 20 20 X
20 30 20 20 20 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// // // // // 20 //
20 X 20 X 20 20 2020 X 20 X 20 20 2020 30 20 30 30 30 2020 30 20 30 30 30 20 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 X 20 X --- 20 2020 X 20 X --- 20 2020 X 20 X --- --- 2020 X 20 X --- 20 2020 X 20 X --- 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 X 20 X 20 20 2020 X 20 X --- --- 2020 X 20 X --- 20 20--- --- --- --- --- --- --- --- --- --- --- --- --- ---20 X 20 X --- --- 20--- --- --- --- --- --- ---20 X 20 X 20 20 20
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DB37 DB38 DB39 DB40 DB41 DB42 DB441000 1000 1000 2000
¶ Æ U ≈ Њ ≈
20 X 20 X --- 20 2020 X 20 X 20 20 2020 X 20 X 20 20 2020 X 20 X 20 20 2020 X 20 X 20 20 2020 X 20 X 20 --- 2020 X 20 X 20 20 2020 X 20 X --- --- 20--- --- --- --- --- --- ------ --- --- --- --- --- ---20 X 20 X --- 20 2020 X 20 X --- --- 2020 X 20 X --- 20 20--- --- --- --- --- --- ---20 X 20 X 20 20 20
X 50 20 X --- --- 40X 50 20 X 20 --- 40
X X 20 X --- X 20X X 20 X 40 X 20X X 20 X 40 X 20X X 20 X --- X 20X X 20 X 40 X 20--- --- --- --- --- --- ---X X 20 X 40 X 20X X 20 X 40 X 20X X 20 X --- X 2050 50 50 50 40 --- 4050 50 50 50 40 --- 40--- --- --- --- --- --- ---X X 20 X --- X 20X X 20 X --- X 20
--- --- --- --- --- --- ---X X 20 X 20 20 XX X 20 X 20 20 X
1000 1000 --- 1000 --- --- ------ --- --- --- --- --- ---X 50 20 X --- --- 40X 50 20 X --- --- 40X 50 20 X --- --- 40X 50 20 X --- --- 40X 50 20 X --- --- 40X 50 20 X --- --- 40X 50 20 X --- --- 40X 50 20 X --- --- 40X 50 20 X --- --- 40--- --- --- --- --- --- ------ --- --- --- --- --- ---X 50 20 X --- --- 40X 50 20 X 20 --- 40
--- --- --- --- --- --- ---X 50 20 X --- --- 40
1000--- --- --- --- --- --- ---50 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 20 --- 40
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DB37 DB38 DB39 DB40 DB41 DB42 DB441000 1000 1000 2000
¶ Æ U ≈ Њ ≈
50 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 40 --- --- --- --- --- --- ---50 50 50 50 40 --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 40 --- 40--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 --- --- 40 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 40 X 4050 50 50 50 --- --- 4050 50 50 50 --- --- 40--- --- --- --- --- --- ---50 50 50 50 --- --- 4050 50 50 50 --- --- 40--- --- --- --- --- --- ---50 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 40--- --- --- --- --- --- ---50 50 50 50 --- --- 40--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 --- --- 40--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 --- --- 40--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 --- --- 40--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 40--- --- --- --- --- --- ---50 50 50 50 --- --- 40--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DB37 DB38 DB39 DB40 DB41 DB42 DB441000 1000 1000 2000
¶ Æ U ≈ Њ ≈
50 50 50 50 --- --- 4050 50 50 50 --- --- 4050 50 50 50 --- --- 40--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 --- --- 40
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
20 30 20 30 20 20 2020 30 50 30 20 20 20--- --- --- --- --- --- ---20 30 20 30 20 20 20--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 30 50 30 --- 20 20--- 30 50 30 --- --- 20--- --- --- --- --- --- ---20 30 50 30 --- 20 20--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 50 50 --- --- 40--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 30 50 30 --- 20 2020 30 50 30 20 20 20
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 20 --- X
--- --- --- --- --- --- ---X X X X --- X XX X X X 20 X XX X X X 20 X X--- --- X --- --- --- X--- --- --- --- --- --- ---X X X X --- --- X--- --- --- --- --- --- ---X X X X 20 X X
--- Ə1 Ə1 Ə1 --- --- Ə--- 50 50 50 --- --- X--- --- --- --- --- --- ------ 1000 1000 1000 --- --- 1000--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DB45 DB46 DB47 DB48 DB49 DB50 DB511000 1000
ΰ ê ê
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X Þ X X X XX X --- X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
--- --- --- --- --- --- ---X X X X X X X
X^ X^ X X^ X^ X^ X^
X X X X X X X
20 X --- 20 20 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// X X // // // //
20 X X X X 30 3020 X X X X 30 3030 X X 30 20 30 3030 X X 30 20 30 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 X X X X 30 3020 X X X X 30 3020 X --- X X 30 3020 X X X X 30 3020 X --- X X 30 30--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 X X X X 30 3020 X --- X X 30 3020 X --- X X 30 30--- --- --- --- --- --- --- --- --- --- --- --- --- ---20 X --- X X 30 30--- --- --- --- --- --- ---// X X X X 30 30
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DB45 DB46 DB47 DB48 DB49 DB50 DB511000 1000
ΰ ê ê
50 X --- X X 30 3050 X --- X X 30 3050 X --- X X 30 3050 X --- X X 30 3050 X X X X 30 3050 X XШ X X 30 3050 X X X X 30 3050 X --- X X 30 30--- --- --- --- --- --- ------ --- --- --- --- --- ---50 X --- X X 30 3050 X --- X X 30 3050 X --- X X 30 30--- --- --- --- --- --- ---50 X X X X 30 30
50 X --- X X 30 3050 X --- X X 30 30
X X X X X 30 30X X X X X 30 30X X X X X 30 30X X X X X 30 30X X X X X 30 30--- --- --- --- --- --- ---X X --- X X 30 30X X --- X X 30 30X X --- X X 30 3050 X X 50 50 50 5050 X --- 50 50 50 50--- --- --- --- --- --- ---X X --- X X 30 30X X X X X 30 30
--- --- --- --- --- --- ---30 X X X X 30 3030 X X X X 30 30
1000 800 --- 1000 1000 --- ------ --- --- --- --- --- ---50 --- --- X X 30 3050 --- --- X X 30 3050 --- --- X X 30 3050 --- --- X X 30 3050 X X X X 30 3050 --- --- X X 30 3050 --- --- X X 30 3050 --- --- X X 30 3050 --- --- X X 30 30--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- X X 30 3050 X --- X X 30 30 --- --- --- --- --- --- ---50 X --- X X 30 30
@
--- --- --- --- --- --- ---50 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DB45 DB46 DB47 DB48 DB49 DB50 DB511000 1000
ΰ ê ê
50 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- X 50 50 50 50 --- --- --- --- --- --- ---50 X X 50 50 50 5050 --- --- 50 50 50 5050 X X 50 50 50 5050 X X 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 X --- 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 X X 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 50--- --- --- --- --- --- ---50 --- --- 50 50 50 5050 --- --- 50 50 50 50--- --- --- --- --- --- ---50 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 X --- 50 50 50 5050 X --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 5050 X --- 50 50 50 5050 X --- 50 50 50 50--- --- --- --- --- --- ---50 --- --- 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- 50 50 50 5050 X --- 50 50 50 5050 X --- 50 50 50 50--- --- --- --- --- --- ---50 --- --- 50 50 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DB45 DB46 DB47 DB48 DB49 DB50 DB511000 1000
ΰ ê ê
50 --- --- 50 50 50 5050 --- --- 50 50 50 5050 --- --- 50 50 50 50--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- 50 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
50 X X 30 20 30 3050 X X 30 20 30 30--- --- --- --- --- --- ---50 X X 30 20 30 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---50 X X 30 20 30 30--- --- --- 30 20 --- ------ --- --- --- --- --- ---50 X X 30 20 30 30--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 --- --- 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- 30 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- 30 30--- --- --- --- --- --- ---50 X --- 30 20 30 3050 X X 30 20 30 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X --- --- X X X X
--- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X --- --- X X X X--- --- --- --- --- --- ---X X --- X X X X
--- --- --- Ə1 Ə1 --- ------ --- --- 50 X --- ------ --- --- --- --- --- ------ --- --- 1000 1000 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DB52 DB53 DB54 DB55 DB56 DB57 DB581000 1000 1000 750 1500 1000
Ŧ ≈ ê ê ≈ ij ≈ Ñ ≈ ê ≈
X 30 X X X X XX 30 X X X X XX 30 X X X X X--- --- --- --- --- --- ---X 30 --- --- --- X X
X 30 X X X X XX 30 X X X X XX 30 X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X 30 X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X 30 X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X 30 X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X 30 X X X X X
X 30 X X X X XX 30 X X X X X
X --- --- X X X XX 30 X X X X X
X^ 30^ X^ X^ X^ X^ X^
X 30 X X X X X
20 30 20 30 20 X 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// 30 // // // X //
30 30 X X X 30 3030 30 X X X 30 3030 30 30 30 30 30 3030 30 30 30 30 30 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 30 X X --- 30 3030 30 X X X 30 3030 30 X X --- 30 3030 30 X X X 30 3030 30 X X X 30 30--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 30 X X X 30 3030 30 X X --- 30 3030 30 X X X 30 30--- --- --- --- --- --- --- --- --- --- --- --- --- ---30 30 X X --- 30 30--- --- --- --- --- --- ---30 30 X X X 30 30
January 01, 2016
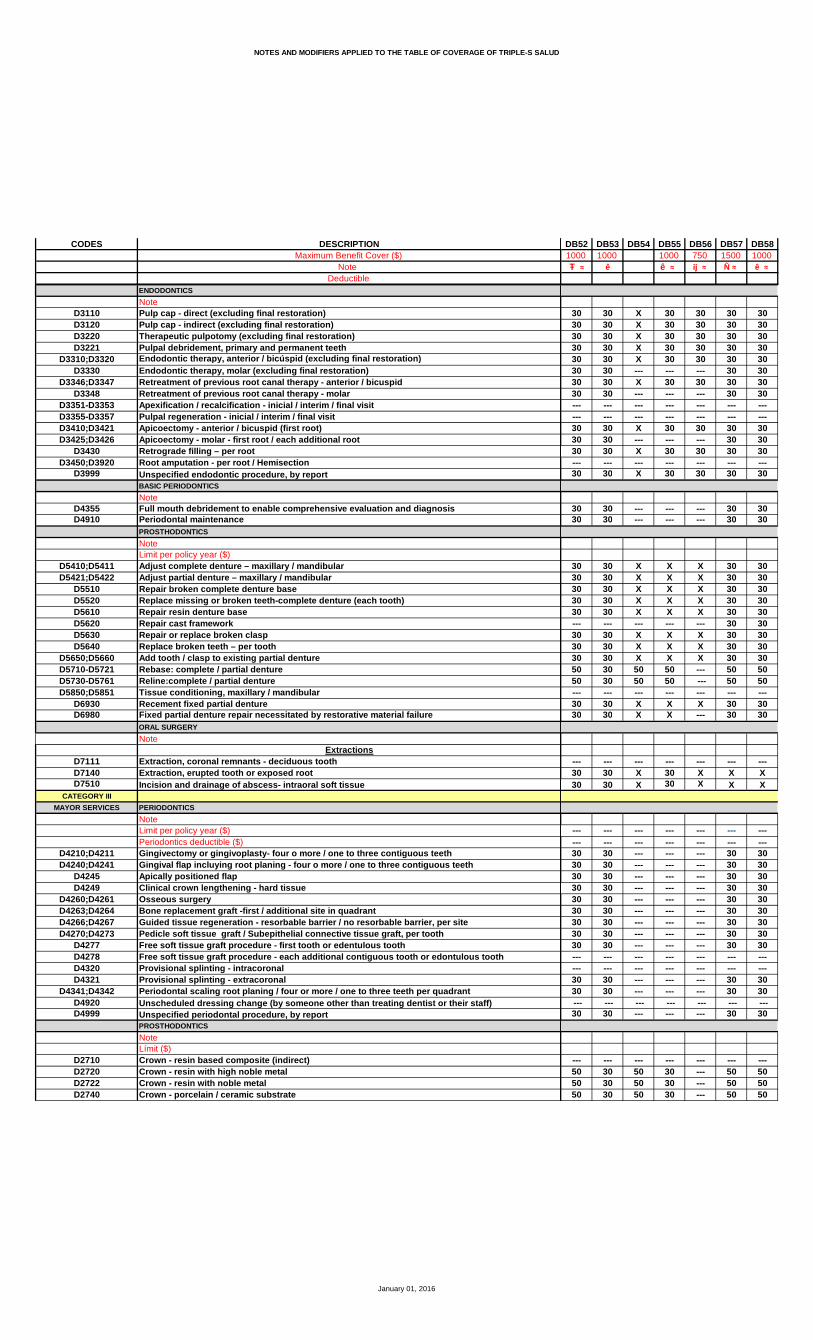
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DB52 DB53 DB54 DB55 DB56 DB57 DB581000 1000 1000 750 1500 1000
Ŧ ≈ ê ê ≈ ij ≈ Ñ ≈ ê ≈
30 30 X 30 30 30 3030 30 X 30 30 30 3030 30 X 30 30 30 3030 30 X 30 30 30 3030 30 X 30 30 30 3030 30 --- --- --- 30 3030 30 X 30 30 30 3030 30 --- --- --- 30 30--- --- --- --- --- --- ------ --- --- --- --- --- ---30 30 X 30 30 30 3030 30 --- --- --- 30 3030 30 X 30 30 30 30--- --- --- --- --- --- ---30 30 X 30 30 30 30
30 30 --- --- --- 30 3030 30 --- --- --- 30 30
30 30 X X X 30 3030 30 X X X 30 3030 30 X X X 30 3030 30 X X X 30 3030 30 X X X 30 30--- --- --- --- --- 30 3030 30 X X X 30 3030 30 X X X 30 3030 30 X X X 30 3050 30 50 50 --- 50 5050 30 50 50 --- 50 50--- --- --- --- --- --- ---30 30 X X X 30 3030 30 X X --- 30 30
--- --- --- --- --- --- ---30 30 X 30 X X X30 30 X 30 X X X
--- --- --- --- --- --- ------ --- --- --- --- --- ---30 30 --- --- --- 30 3030 30 --- --- --- 30 3030 30 --- --- --- 30 3030 30 --- --- --- 30 3030 30 --- --- --- 30 3030 30 --- --- --- 30 3030 30 --- --- --- 30 3030 30 --- --- --- 30 3030 30 --- --- --- 30 30--- --- --- --- --- --- ------ --- --- --- --- --- ---30 30 --- --- --- 30 3030 30 --- --- --- 30 30 --- --- --- --- --- --- ---30 30 --- --- --- 30 30
--- --- --- --- --- --- ---50 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DB52 DB53 DB54 DB55 DB56 DB57 DB581000 1000 1000 750 1500 1000
Ŧ ≈ ê ê ≈ ij ≈ Ñ ≈ ê ≈
50 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 50 --- --- --- --- --- --- ---50 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 30 50 30 --- 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 30 50 30 X 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 50--- --- --- --- --- --- ---50 30 50 30 --- 50 5050 30 50 30 --- 50 50--- --- --- --- --- --- ---50 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 50--- --- --- --- --- --- ---50 30 50 30 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 30 50 30 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 30 50 30 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 30 50 30 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 50--- --- --- --- --- --- ---50 30 50 30 --- 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DB52 DB53 DB54 DB55 DB56 DB57 DB581000 1000 1000 750 1500 1000
Ŧ ≈ ê ê ≈ ij ≈ Ñ ≈ ê ≈
50 30 50 30 --- 50 5050 30 50 30 --- 50 5050 30 50 30 --- 50 50--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 30 50 30 --- 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
100050 --- --- --- --- --- ---
30 30 30 30 X 30 3030 30 30 30 X 30 30--- --- --- --- --- --- ---30 30 30 30 X 30 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 30 --- --- --- 30 30--- --- --- --- --- 30 30--- --- --- --- --- --- ---30 30 30 30 X 30 30--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 30 50 30 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---30 30 --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---30 30 --- --- --- --- ------ --- --- --- --- --- ---30 30 30 30 X 30 3030 30 30 30 X 30 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
--- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X --- --- --- X X--- --- --- --- --- --- ---X X X X X X X
--- --- --- --- --- Ə1 ------ --- --- --- --- 50 ------ --- --- --- --- --- ------ --- --- --- --- 2000 ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DB59 DB60 DB61 DB62 DB63 DB64 DB651000 1000 1000
M ≈ M M ≈
X X X 30 25 X XX X X 30 25 X XX X X 30 25 X X--- --- --- --- --- --- ---X X X 30 25 X X
X X X 30 25 X XX X X 30 25 X X X X X 30 25 X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X 30 25 X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X 30 25 X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X 30 25 X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X 30 25 X X
X X X 30 25 X XX X X 30 25 X X
--- --- --- X --- X ---X X X 30 25 X X--- X^ X^ 30^ 25^ X^ X^
X X X 30 25 X X
30 X X 30 25 X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// X X 30 25 X X
X X X 50 25 30 X30 X X 50 25 30 X30 X X 50 25 30 X30 X X 50 25 30 X --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X 50 25 30 XX X X 50 25 30 XX X X 50 25 30 XX X X 50 25 30 XX X X 50 25 30 X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X 50 25 30 XX X X 50 25 30 XX X X 50 25 30 X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X 50 25 30 X--- --- --- --- --- --- ---X X X 50 25 30 X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DB59 DB60 DB61 DB62 DB63 DB64 DB651000 1000 1000
M ≈ M M ≈
X X X 50 25 30 XX X X 50 25 30 XX X X 50 25 30 XX X X 50 25 30 XX X X 50 25 30 XX X X 50 25 30 XX X X 50 25 30 XX X X 50 25 30 X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X 50 25 30 XX X X 50 25 30 XX X X 50 25 30 X--- --- --- --- --- --- ---X X X 50 25 30 X
30 X X 50 25 30 X30 X X 50 25 30 X
X X X 50 50 50 XX X X 50 50 50 XX X X 50 50 50 XX X X 50 50 50 XX X X 50 50 50 X--- --- --- --- --- --- ---X X X 50 50 50 XX X X 50 50 50 XX X X 50 50 50 X50 X X 50 50 50 X50 X X 50 50 50 X--- --- --- --- --- --- ---X X X 50 50 50 XX X X 50 50 50 X
--- --- --- --- --- --- ---30 X X 50 25 30 X30 X X 50 25 30 X
M M M1000 800 800 --- --- --- 800
--- --- --- --- --- --- ---30 --- --- 50 25 30 ---30 X X 50 25 30 X30 --- --- 50 25 30 ---30 --- --- 50 25 30 ---30 X X 50 25 30 X30 --- --- 50 25 30 ---30 --- --- 50 25 30 ---30 --- --- 50 25 30 ---30 --- --- 50 25 30 ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 --- --- 50 25 30 ---30 X X 50 25 30 X --- --- --- --- --- --- ---30 X X 50 25 30 X
@ @ @
--- --- --- --- --- --- ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DB59 DB60 DB61 DB62 DB63 DB64 DB651000 1000 1000
M ≈ M M ≈
50 --- --- 50 50 50 X50 --- --- 50 50 50 X50 --- --- 50 50 50 X50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 --- --- --- --- --- --- --- ---50 X X 50 50 50 X 50 --- --- 50 50 50 ---50 X X 50 50 50 X 50 X X 50 50 50 X --- --- --- --- --- --- ------ --- --- --- --- --- ---50 X X 50 50 50 X --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 X X 50 50 50 X 50 --- --- 50 50 50 ---50 --- --- 50 50 50 ------ --- --- --- --- --- ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ------ --- --- --- --- --- ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 X X 50 50 50 X 50 X X 50 50 50 X 50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 X X 50 50 50 X 50 X X 50 50 50 X--- --- --- --- --- --- ---50 --- --- 50 50 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- 50 50 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- 50 50 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- 50 50 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- 50 50 50 ---50 X X 50 50 50 X 50 X X 50 50 50 X --- --- --- --- --- --- ---50 --- --- 50 50 50 ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DB59 DB60 DB61 DB62 DB63 DB64 DB651000 1000 1000
M ≈ M M ≈
50 --- --- 50 50 50 ---50 --- --- 50 50 50 ---50 --- --- 50 50 50 ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- 50 50 50 ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 X X 50 25 30 X30 X X 50 25 30 X--- --- --- --- --- --- ---30 X X 50 25 30 X--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 X X 50 25 30 X30 --- --- --- --- 30 ------ --- --- --- --- --- ---30 X X 50 25 30 X--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 --- --- 50 50 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 X X 50 25 30 X30 X X 50 25 30 X
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- X X X --- --- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X --- --- X X X ------ --- --- --- --- --- ---X X X X X X X
--- --- --- --- --- Ə1 ------ --- --- --- --- 50 ------ --- --- --- --- --- ------ --- --- --- --- 1000 ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DB66
XXX---X
XXX------X--------- ---X---
--- ---X--- ---X
XX
---X
X^
X
X---------X
XX3030 --- ------ ---XXXXX---------XXX--- ---X---X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DB66
XXXXXXXX------XXX---X
5050
XXXXX---XXX5050---XX
---XX
1000---505050505050505050------5050 ---50
---505050
January 01, 2016
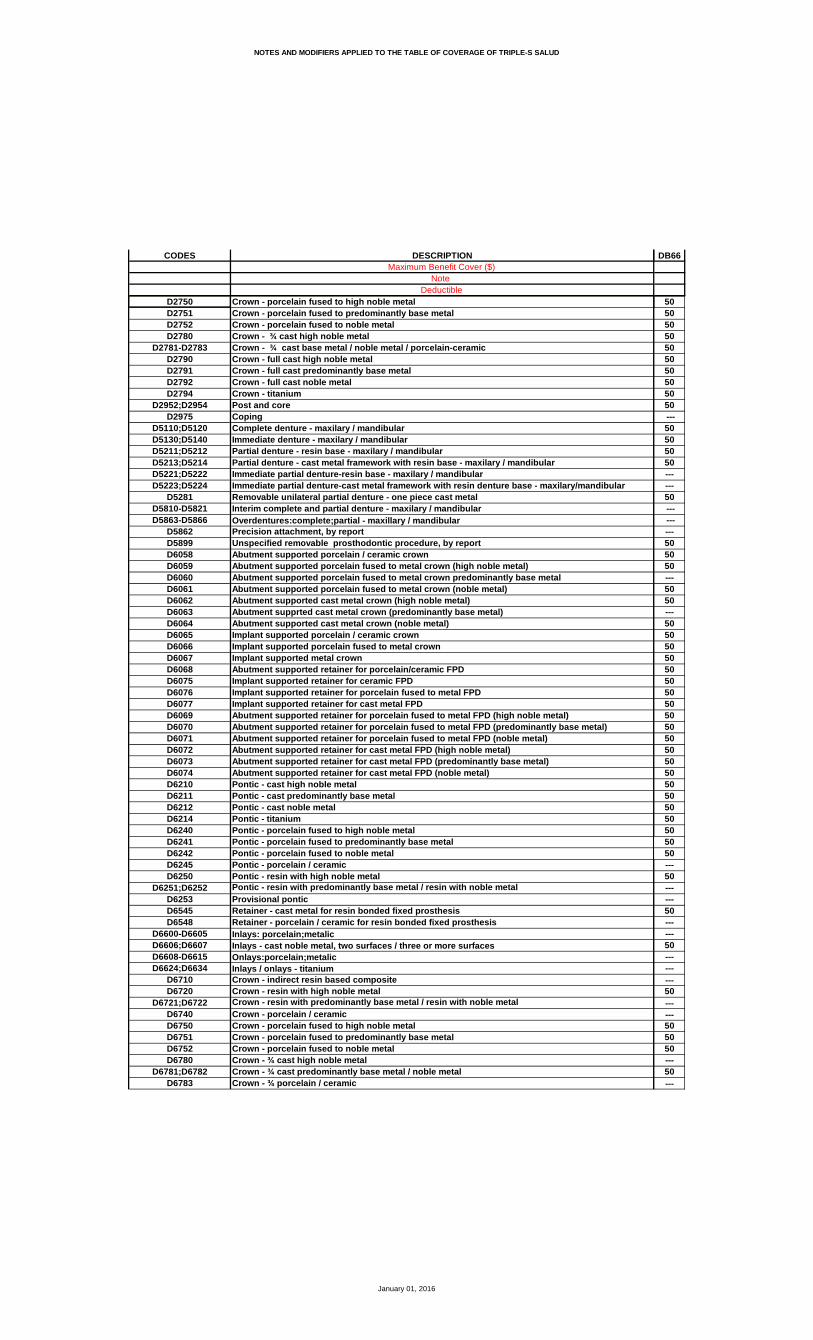
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DB66
50505050505050505050 ---50505050------50 --- ------505050---5050---505050505050505050505050505050505050505050---50------50------50---------50------505050---50---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DB66
505050--- ------50
--- --- --- ---
---
3030---30------ ---3030---30--- ---50--------------- --- --- --- ---------3030
------------ ---X
---XXX------X---X
Ə150---
1000------
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DB67 DB68 DB69 DB70 DB71 DB72 DB731500 1000 750 750 1000 1000Ñ ≈ Ψ ij ≈ Æ ê
20 X X X 20 X X20 X X X 20 X X20 X X X 20 X X--- --- --- --- --- --- ---20 X X X 20 X ---
20 X X X 20 X X20 X X Þ X Þ 20 X X20 X --- --- 20 X X--- --- --- --- --- --- ------ --- --- --- --- --- ---20 X X X 20 X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 X X X 20 X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---20 X X X 20 X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---20 X X X 20 X X
20 X X X 20 X X20 X X X 20 X X
X --- --- --- X --- ---20 X X X 20 X X
20^ X^ X^ X^ 20^ X^ X^
20 X 20 X 20 X X
20 20 20 X 20 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 // // X 20 // //
20 X 20 --- 30 X X20 X 20 --- 30 X X20 30 30 --- 30 30 3020 30 20 Ǿ --- 30 30 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 X 50 --- 30 X X20 X 50 --- 30 X X20 X 50 --- 30 X X20 X 50 --- 30 X X20 X 50 --- 30 X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 X 20 --- 30 X X20 X --- --- 30 X X20 X --- --- 30 X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---20 X --- --- 30 X X--- --- --- --- --- --- ---20 X 20 --- 30 X X
January 01, 2016
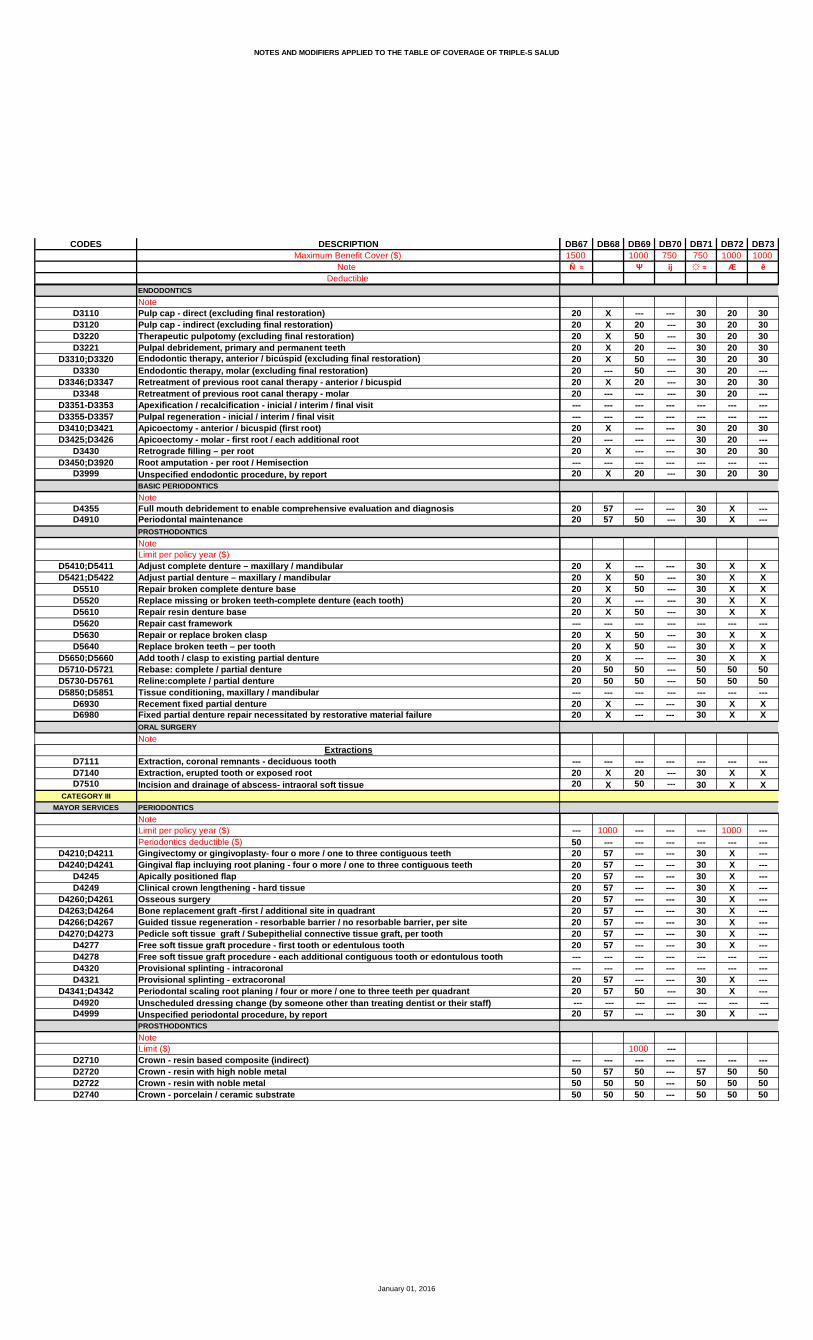
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DB67 DB68 DB69 DB70 DB71 DB72 DB731500 1000 750 750 1000 1000Ñ ≈ Ψ ij ≈ Æ ê
20 X --- --- 30 20 3020 X 20 --- 30 20 3020 X 50 --- 30 20 3020 X 20 --- 30 20 3020 X 50 --- 30 20 3020 --- 50 --- 30 20 ---20 X 20 --- 30 20 3020 --- --- --- 30 20 ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 X --- --- 30 20 3020 --- --- --- 30 20 ---20 X --- --- 30 20 30--- --- --- --- --- --- ---20 X 20 --- 30 20 30
20 57 --- --- 30 X ---20 57 50 --- 30 X ---
20 X --- --- 30 X X20 X 50 --- 30 X X20 X 50 --- 30 X X20 X --- --- 30 X X20 X 50 --- 30 X X--- --- --- --- --- --- ---20 X 50 --- 30 X X20 X 50 --- 30 X X20 X --- --- 30 X X20 50 50 --- 50 50 5020 50 50 --- 50 50 50--- --- --- --- --- --- ---20 X --- --- 30 X X20 X --- --- 30 X X
--- --- --- --- --- --- ---20 X 20 --- 30 X X20 X 50 --- 30 X X
--- 1000 --- --- --- 1000 ---50 --- --- --- --- --- ---20 57 --- --- 30 X ---20 57 --- --- 30 X ---20 57 --- --- 30 X ---20 57 --- --- 30 X ---20 57 --- --- 30 X ---20 57 --- --- 30 X ---20 57 --- --- 30 X ---20 57 --- --- 30 X ---20 57 --- --- 30 X ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 57 --- --- 30 X ---20 57 50 --- 30 X --- --- --- --- --- --- --- ---20 57 --- --- 30 X ---
1000 ------ --- --- --- --- --- ---50 57 50 --- 57 50 5050 50 50 --- 50 50 5050 50 50 --- 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DB67 DB68 DB69 DB70 DB71 DB72 DB731500 1000 750 750 1000 1000Ñ ≈ Ψ ij ≈ Æ ê
50 57 50 --- 57 50 5050 50 50 --- 50 50 5050 50 50 --- 50 50 5050 57 50 --- 57 50 5050 50 50 --- 50 50 5050 57 50 --- 57 50 5050 50 50 --- 50 50 5050 50 50 --- 50 50 5050 57 50 --- 57 50 5050 50 50 --- 50 50 50 --- --- 50 --- --- --- ---50 50 50 --- 50 50 5050 50 --- --- 50 50 5050 50 --- --- 50 50 5050 50 50 --- 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- --- 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- 50 50 5050 50 --- --- 50 50 5050 57 --- --- 57 50 50--- --- --- --- --- --- ---50 50 --- --- 50 50 5050 57 --- --- 57 50 50--- --- --- --- --- --- ---50 50 50 --- 50 50 5050 50 50 --- 50 50 5050 57 50 --- 57 50 5050 57 50 --- 57 50 5050 50 50 --- 50 50 5050 50 50 --- 50 50 5050 57 50 --- 57 50 5050 57 50 --- 57 50 5050 57 50 --- 57 50 5050 50 50 --- 50 50 5050 50 50 --- 50 50 5050 57 50 --- 57 50 5050 50 50 --- 50 50 5050 50 50 --- 50 50 5050 57 50 --- 57 50 5050 50 50 --- 50 50 5050 50 50 --- 50 50 5050 57 50 --- 57 50 5050 57 50 --- 57 50 5050 50 50 --- 50 50 5050 50 50 --- 50 50 50--- --- --- --- --- --- ---50 57 50 --- 57 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 57 50 --- 57 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 57 50 --- 57 50 5050 50 50 --- 50 50 5050 50 50 --- 50 50 50--- --- --- --- --- --- ---50 50 50 --- 50 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DB67 DB68 DB69 DB70 DB71 DB72 DB731500 1000 750 750 1000 1000Ñ ≈ Ψ ij ≈ Æ ê
50 57 50 --- 57 50 5050 50 50 --- 50 50 5050 57 --- --- 57 50 50--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- --- 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
20 30 50 --- 30 20 3020 30 50 --- 30 20 30--- --- --- --- --- --- ---20 30 50 --- 30 20 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 --- --- --- 30 20 ---20 --- --- --- 30 20 ------ --- --- --- --- --- ---20 30 --- --- 30 20 30--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 --- --- 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 30 --- --- 30 20 3020 30 20 --- 30 20 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X 20 --- X X X
--- --- --- --- --- --- ---X X --- --- X X XX X 20 --- X X XX X 20 --- X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X --- --- --- X X ------ --- --- --- --- --- ---X X 20 --- X X X
Ə1 --- --- --- Ə1 Ə1 ---X --- --- --- X 50 ------ --- --- --- --- --- ---
1500 --- --- --- 1500 1000 ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DB74 DB76 DB77 DB78 DB87 DB88 DB89500 1300 1000
Қ C Æ
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ X X --- X X X
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
--- --- --- --- --- --- ---X X X X X X X
X^ X^ X^ X^ X^ X^ X^
X X X X X X X
20 20 20 20 X 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// // // // X // //
X X X X X X XX X X X X X X30 30 30 30 X 30 3030 30 30 30 X 30 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X XX X X X X X X--- X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- X X X X X XX X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ------ X X X X X X--- --- --- --- --- --- ---X X X X X X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DB74 DB76 DB77 DB78 DB87 DB88 DB89500 1300 1000
Қ C Æ
30 X X X X X X30 X X X X X X30 X X X X X X30 X X X X X X30 X X X X X X--- X --- --- X X X30 X X X X X X--- X --- --- X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---30 X X X X X X--- X --- --- X X X30 X X X X X X--- --- --- --- --- --- ---30 X X X X X X
--- X X --- X X X--- X X --- X X X
X X X X X X XX X X X X X XX X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X--- 50 50 50 X 50 50 --- 50 50 50 X 50 50--- --- --- --- --- --- ---X X X X X X XX X X X X X X
--- --- --- --- --- --- ---X X X X X X XX X X X X X X
--- 1000 1000 --- 800 1000 1000--- --- --- --- --- --- ------ X X --- --- X X--- X X --- X X X--- X X --- --- X X--- X X --- --- X X--- X X --- X X X--- X X --- --- X X--- X X --- --- X X--- X X --- --- X X--- X X --- --- X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ X X --- --- X X--- X X --- X X X --- --- --- --- --- --- ------ X X --- X X X
@
--- --- --- --- --- --- ------ 50 50 57 --- 57 57--- 50 50 50 --- 50 50--- 50 50 50 --- 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DB74 DB76 DB77 DB78 DB87 DB88 DB89500 1300 1000
Қ C Æ
--- 50 50 57 --- 57 57--- 50 50 50 --- 50 50--- 50 50 50 --- 50 50--- 50 50 57 --- 57 57--- 50 50 50 --- 50 50--- 50 50 57 --- 57 57--- 50 50 50 --- 50 50--- 50 50 50 --- 50 50--- 50 50 57 --- 57 57--- 50 50 50 --- 50 50 --- --- --- --- --- --- ------ 50 50 50 X 50 50--- 50 50 50 --- 50 50--- 50 50 50 X 50 50--- 50 50 50 X 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 X 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---X 50 50 50 X 50 50--- 50 50 50 --- 50 50--- 50 50 57 --- 57 57--- --- --- --- --- --- ------ 50 50 50 --- 50 50--- 50 50 57 --- 57 57--- --- --- --- --- --- ------ 50 50 50 --- 50 50--- 50 50 50 --- 50 50--- 50 50 57 --- 57 57--- 50 50 57 --- 57 57--- 50 50 50 --- 50 50--- 50 50 50 --- 50 50--- 50 50 57 --- 57 57--- 50 50 57 --- 57 57--- 50 50 57 --- 57 57--- 50 50 50 --- 50 50--- 50 50 50 --- 50 50--- 50 50 57 --- 57 57--- 50 50 50 --- 50 50--- 50 50 50 --- 50 50--- 50 50 57 --- 57 57--- 50 50 50 X 50 50--- 50 50 50 X 50 50--- 50 50 57 --- 57 57--- 50 50 57 --- 57 57--- 50 50 50 X 50 50--- 50 50 50 X 50 50--- --- --- --- --- --- ------ 50 50 57 --- 57 57--- --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 57 --- 57 57--- --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 57 --- 57 57--- 50 50 50 X 50 50--- 50 50 50 X 50 50--- --- --- --- --- --- ------ 50 50 50 --- 50 50--- --- --- --- --- --- ---
January 01, 2016
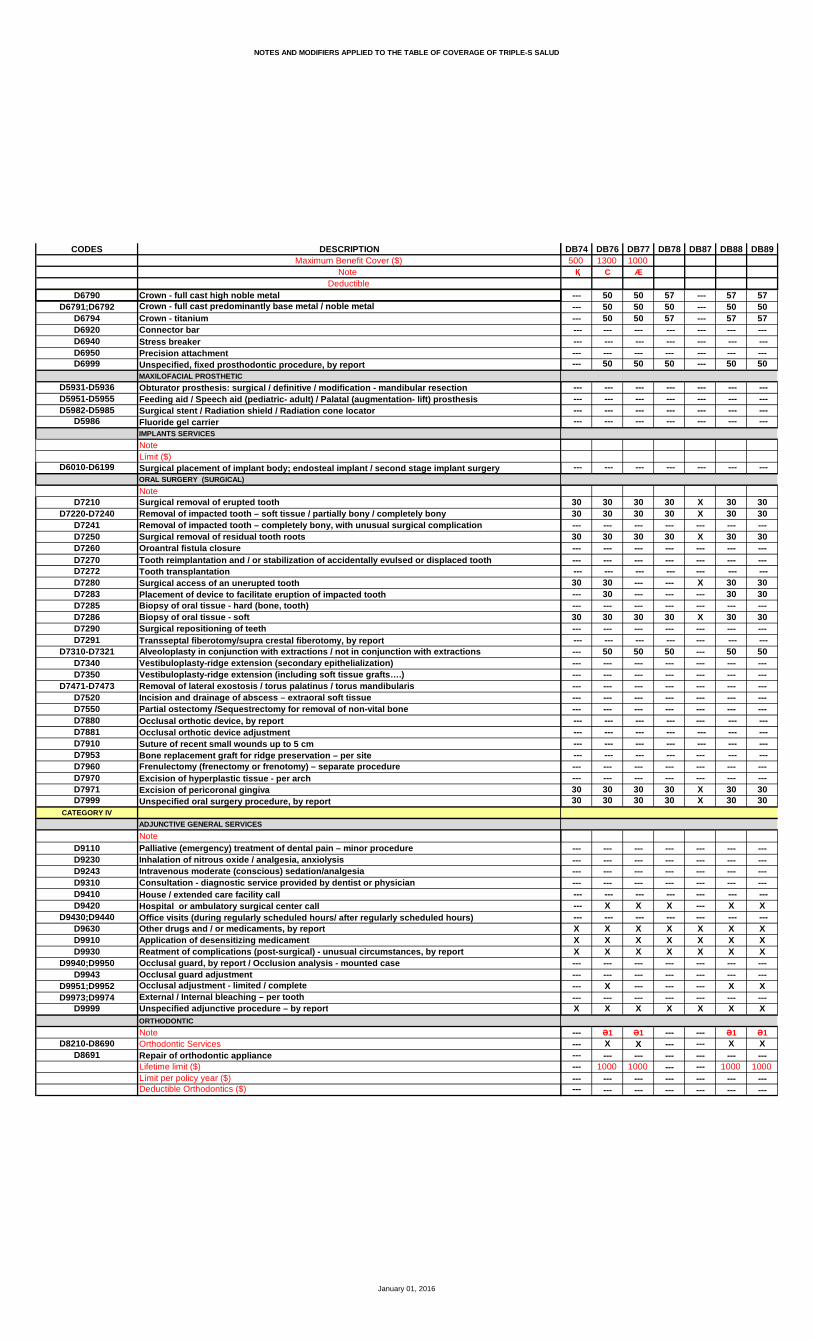
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DB74 DB76 DB77 DB78 DB87 DB88 DB89500 1300 1000
Қ C Æ
--- 50 50 57 --- 57 57--- 50 50 50 --- 50 50--- 50 50 57 --- 57 57 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 --- 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 30 30 30 X 30 3030 30 30 30 X 30 30--- --- --- --- --- --- ---30 30 30 30 X 30 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 30 --- --- X 30 30--- 30 --- --- --- 30 30--- --- --- --- --- --- ---30 30 30 30 X 30 30--- --- --- --- --- --- --- --- --- --- --- --- --- ------ 50 50 50 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 30 30 30 X 30 3030 30 30 30 X 30 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- X X X --- X X --- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ X --- --- --- X X--- --- --- --- --- --- ---X X X X X X X
--- Ə1 Ə1 --- --- Ə1 Ə1--- X X --- --- X X--- --- --- --- --- --- ------ 1000 1000 --- --- 1000 1000--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016
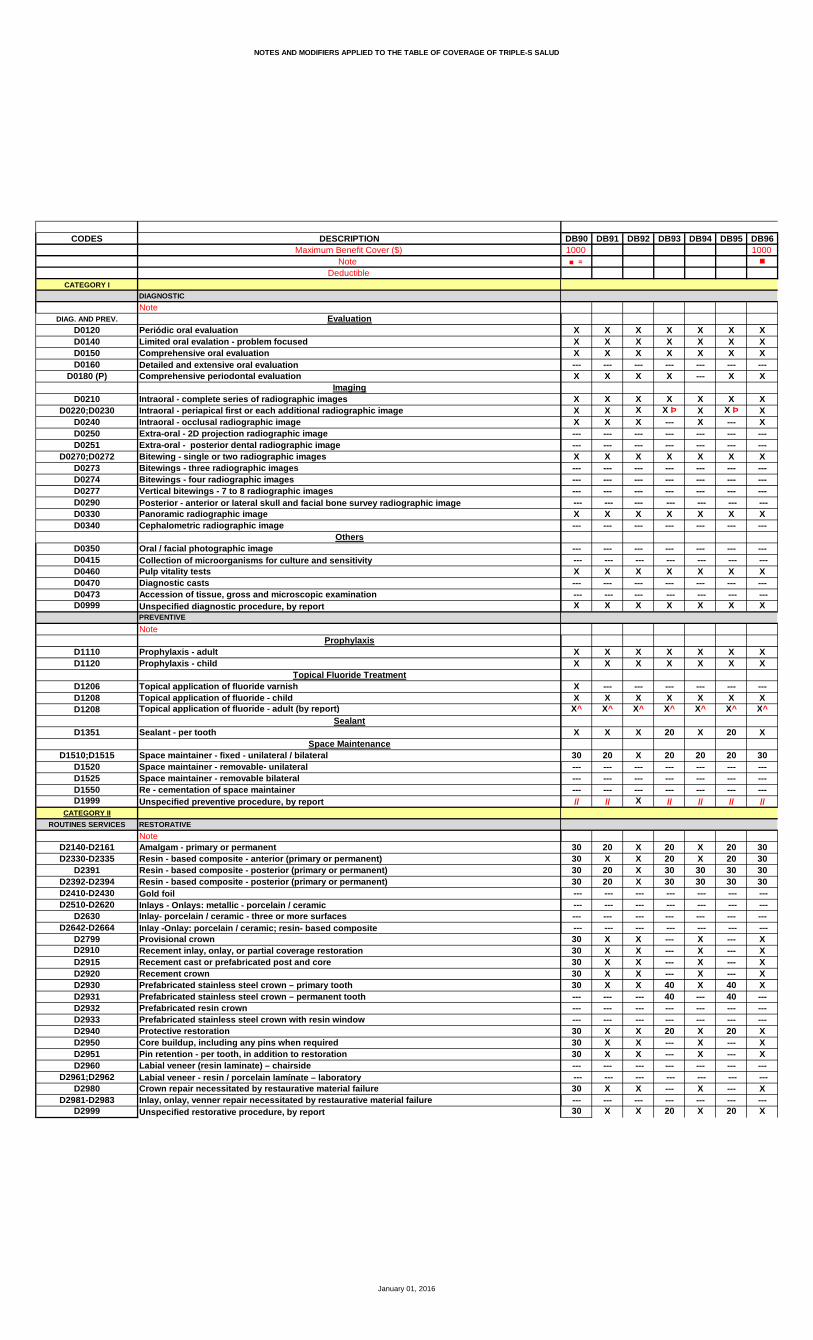
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DB90 DB91 DB92 DB93 DB94 DB95 DB961000 1000
≈
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X --- X X
X X X X X X XX X X X Þ X X Þ XX X X --- X --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
X --- --- --- --- --- ---X X X X X X X
X^ X^ X^ X^ X^ X^ X^
X X X 20 X 20 X
30 20 X 20 20 20 30--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// // X // // // //
30 20 X 20 X 20 3030 X X 20 X 20 3030 20 X 30 30 30 3030 20 X 30 30 30 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 X X --- X --- X30 X X --- X --- X30 X X --- X --- X30 X X --- X --- X30 X X 40 X 40 X--- --- --- 40 --- 40 ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 X X 20 X 20 X30 X X --- X --- X30 X X --- X --- X--- --- --- --- --- --- --- --- --- --- --- --- --- ---30 X X --- X --- X--- --- --- --- --- --- ---30 X X 20 X 20 X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DB90 DB91 DB92 DB93 DB94 DB95 DB961000 1000
≈
30 X X --- X --- 3030 X X 20 X 20 3030 X X 20 X 20 3030 X X 20 X 20 3030 X X 20 X 20 3030 X X 20 --- 20 3030 X X 20 X 20 3030 X X --- --- --- 30--- --- --- --- --- --- ------ --- --- --- --- --- ---30 X X --- X --- 3030 X X --- --- --- 3030 X X --- X --- 30--- --- --- --- --- --- ---30 X X 20 X 20 30
50 X X --- --- --- 5050 X X 20 --- 20 50
X X X --- X --- 50X X X 40 X 40 50X X X 40 X 40 50X X X --- X --- 50X X X 40 X 40 50--- --- --- --- --- --- ---X X X 40 X --- 50X X X 40 X 40 50X X X --- X --- 5050 50 X 40 50 40 5050 50 X 40 50 40 50--- --- --- --- --- --- ---X X X --- X --- XX X X --- X --- X
--- --- --- --- --- --- ---30 X X 20 X 20 X30 X X 20 X 20 X
--- 1000 800 --- --- ------ --- --- --- --- --- ---50 X --- --- --- --- 5050 X X --- --- --- 5050 X --- --- --- --- 5050 X --- --- --- --- 5050 X X --- --- --- 5050 X --- --- --- --- 5050 X --- --- --- --- 5050 X --- --- --- --- 5050 X --- --- --- --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 X --- --- --- --- 5050 X X 20 --- 20 50 --- --- --- --- --- --- ---50 X X --- --- --- 50
@1000 1000
--- --- --- --- --- --- ---50 50 --- --- 57 --- 5050 50 --- 40 50 40 5050 50 --- 40 50 40 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DB90 DB91 DB92 DB93 DB94 DB95 DB961000 1000
≈
50 50 --- --- 57 --- 5050 50 --- --- 50 --- 5050 50 --- 40 50 40 5050 50 --- --- 57 --- 5050 50 --- --- 50 --- 5050 50 --- --- 57 --- 5050 50 --- --- 50 --- 5050 50 --- --- 50 --- 5050 50 --- --- 57 --- 5050 50 --- --- 50 40« 50 --- --- --- --- --- --- ---50 50 X 40 50 40 5050 50 --- --- 50 --- 5050 50 X --- 50 --- 5050 50 X 40 50 40 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 X --- 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 X 40 50 40 5050 50 --- --- 50 --- 5050 50 --- --- 57 --- 50--- --- --- --- --- --- ---50 50 --- --- 50 --- 5050 50 --- --- 57 --- 50--- --- --- --- --- --- ---50 50 --- --- 50 --- 5050 50 --- --- 50 --- 5050 50 --- --- 57 --- 5050 50 --- --- 57 --- 5050 50 --- --- 50 --- 5050 50 --- --- 50 --- 5050 50 --- --- 57 --- 5050 50 --- --- 57 --- 5050 50 --- --- 57 --- 5050 50 --- --- 50 --- 5050 50 --- --- 50 --- 5050 50 --- --- 57 --- 5050 50 --- --- 50 --- 5050 50 --- --- 50 --- 5050 50 --- --- 57 --- 5050 50 X --- 50 --- 5050 50 X --- 50 --- 5050 50 --- --- 57 --- 5050 50 --- --- 57 --- 5050 50 X --- 50 40 5050 50 X --- 50 40 50--- --- --- --- --- --- ---50 50 --- --- 57 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- --- 57 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- --- 57 --- 5050 50 X --- 50 --- 5050 50 X --- 50 40 50--- --- --- --- --- --- ---50 50 --- --- 50 --- 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DB90 DB91 DB92 DB93 DB94 DB95 DB961000 1000
≈
50 50 --- --- 57 --- 5050 50 --- --- 50 --- 5050 50 --- --- 57 --- 50--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- --- 50 --- 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 30 X 20 30 20 3030 30 X 20 30 20 30--- --- --- --- --- --- ---30 30 X 20 30 20 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 30 X --- --- --- 3030 30 --- --- --- --- 30--- --- --- --- --- --- ---30 30 X --- 30 --- 30--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 --- --- 50 --- 30--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 30 X --- 30 --- 3030 30 X 20 30 20 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 X --- --- X 20 X --- --- --- --- --- --- ---30 X X --- X --- X30 X X 20 X 20 X30 X X 20 X 20 X--- --- --- --- --- --- ------ --- --- --- --- --- ---30 X --- --- --- --- X--- --- --- --- --- --- ---30 X X 20 X 20 X
Ə Ə1 --- --- --- --- Ə150 X --- --- --- --- 50--- --- --- --- --- --- ---
1250 1250 --- --- --- --- 1000--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DB97 DB98 DB99 DD02 DE01 DE02 DE031250 750 1500 1000 1000♠ ≈ ≈ Ñ U M
OSX X 10 X X X XX X 10 X X X XX X 10 X X X X--- --- --- --- --- --- ---X --- 10 X X X X
OSX X 10 X X X XX X 10 X X X ю XX X 10 X --- X X--- --- --- X --- X X--- --- --- --- --- --- ---X X 10 X X X ю X--- --- --- --- --- --- ------ --- --- --- X --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X 10 X X X X--- --- --- X Ð --- X X
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X 10 --- --- X X--- --- 10 --- --- X X --- --- --- --- --- --- ---X X 10 --- X X X
X X 10 --- X X XX X 10 --- X X X
X X --- --- --- --- ---X X 10 --- X X X
X^ X^ --- --- --- X^ ---
X X 10 --- X X X
20 20 10 --- 30 X X--- --- --- --- 30 X X--- --- --- --- 30 X X--- --- --- --- 30 X X// // 10 --- // X X
O40 30 25 X X X X40 30 25 X X X X40 30 25 X --- X X40 30 25 X --- X X --- --- --- --- --- --- --- --- --- 50 --- 50 --- ------ --- --- --- --- --- --- --- --- --- --- 50 --- ---40 30 25 X --- 50 5040 30 25 X 30 50 5040 --- 25 X --- --- ---40 30 25 X 30 50 5040 30 25 X X 50 50--- --- --- --- --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---40 30 25 X X 50 5040 --- 25 X 50 50 5040 30 25 X --- 50 50--- --- --- --- --- --- --- --- --- --- --- --- --- ---40 --- 25 X 30 50 50--- --- --- --- --- --- ---40 30 25 X 30 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DB97 DB98 DB99 DD02 DE01 DE02 DE031250 750 1500 1000 1000♠ ≈ ≈ Ñ U M
O40 30 25 X 30 50 5040 30 25 X --- 50 5040 30 25 X 30 50 5040 30 25 --- 30 50 5040 30 25 X 30 50 5040 --- 25 X 30 50 5040 30 25 X 30 50 5040 --- 25 X 30 50 50--- --- --- --- 30 50 50--- --- --- --- --- --- ---40 30 25 X 30 50 5040 --- 25 X --- 50 5040 30 25 X 30 50 50--- --- --- --- 30 50 5040 30 25 X 30 50 50
40 --- 25 --- --- --- ---40 --- 25 X 50 X X
40 30 25 X --- 50 5040 30 25 X --- 50 5040 30 25 X --- 50 5040 30 25 X --- 50 5040 30 25 X 30 50 50--- --- --- --- 30 50 5040 30 25 X 30 50 5040 30 25 X 30 50 5040 30 25 X --- 50 5040 --- 25 X --- --- ---40 --- 25 X --- 50 50--- --- 25 --- --- 50 5040 30 25 X 30 50 5040 30 25 X --- --- ---
OV--- --- --- --- --- X ---40 X 25 X X X X40 X 25 X X X X
--- --- --- 800 ------ --- --- --- --- --- ---X --- 25 X 50 --- ---X --- 25 --- 50 --- ---X --- 25 --- --- --- ---X --- 25 X --- --- ---X --- 25 X 50 --- ---X --- 25 X 50 --- ---X --- 25 X 50 --- ---X --- 25 --- --- --- ---X --- 25 --- --- --- ------ --- --- --- --- --- ------ --- --- X --- --- ---X --- 25 X --- --- ---X --- 25 --- 50 --- ---
--- --- --- --- --- --- ---X --- 25 X 50 --- ---
--- --- --- --- --- --- ---50 --- 50 X --- --- ---50 --- 50 X 50 50 5050 --- 50 X 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DB97 DB98 DB99 DD02 DE01 DE02 DE031250 750 1500 1000 1000♠ ≈ ≈ Ñ U M
50 --- 50 X 50 50 5050 --- 50 X --- 50 5050 --- 50 X 50 50 5050 --- 50 X 50 --- ---50 --- 50 X 50 50 5050 --- 50 X 50 --- ---50 --- 50 X --- 50 5050 --- 50 X 50 50 5050 --- 50 X --- --- ---50 --- 50 X 50 50 50 --- --- --- --- --- --- ---50 --- 50 X 50 X X50 --- 50 X 50 --- ---50 --- 50 X 50 --- ---50 --- 50 X 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 X --- 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 30 50 X 50 50 5050 --- 50 --- --- --- ---50 --- 50 --- --- --- ------ --- --- --- --- --- ---50 --- 50 --- --- --- ---50 --- 50 --- --- --- ------ --- --- --- --- --- ---50 --- 50 --- --- --- ---50 --- 50 --- --- --- ---50 --- 50 --- --- --- ---50 --- 50 --- --- --- ---50 --- 50 --- --- --- ---50 --- 50 --- --- --- ---50 --- 50 --- --- --- ---50 --- 50 --- --- --- ---50 --- 50 --- --- --- ---50 --- 50 --- --- --- ---50 --- 50 --- --- --- ---50 --- 50 --- --- --- ---50 --- 50 --- --- --- ---50 --- 50 --- --- --- ---50 --- 50 X 30 50 5050 --- 50 X 30 50 5050 --- 50 X --- 50 5050 --- 50 X --- --- ---50 --- 50 X 30 50 5050 --- 50 X 30 50 5050 --- 50 X 30 50 50--- --- --- --- --- --- ---50 --- 50 X --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 X --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 X --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 X --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 X 30 50 5050 --- 50 X 30 50 5050 --- 50 X 30 50 50--- --- --- --- 30 50 5050 --- 50 X --- --- ------ --- --- --- 30 --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DB97 DB98 DB99 DD02 DE01 DE02 DE031250 750 1500 1000 1000♠ ≈ ≈ Ñ U M
50 --- 50 X 30 50 5050 --- 50 X --- 50 5050 --- 50 X --- --- ------ --- --- --- --- --- --- --- --- --- --- --- 50 50--- --- --- --- --- --- ---50 --- 50 X 30 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- 50 --- --- --- ---
40 30 25 X O X X X40 30 25 X X X X--- --- --- --- --- X ---40 30 25 X O --- X X--- --- --- --- X --- ------ --- --- O --- --- --- --- --- --- --- --- --- ---40 30 25 --- --- X X40 --- 25 --- --- --- ------ --- --- --- --- --- ---40 30 25 --- X X X--- --- --- --- X --- --- --- --- --- --- --- --- ---50 --- 50 X X X X--- --- --- --- X --- ------ --- --- --- X --- ------ --- --- --- X X X--- --- --- X --- X X--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- X --- ------ --- --- --- X --- ---40 30 25 X X --- ---40 30 25 X X X X
--- --- --- --- --- X ------ --- --- --- --- X ------ --- --- --- --- X ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X --- X --- X --- ---
--- --- --- --- --- --- ---X X X O X --- ---X X X --- X X XX X X O X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X --- X X X --- ------ --- --- --- --- --- ---X X X --- X --- ---
Ə1 --- ф Ə1 --- Ə1 … Ə ---50 --- 50 --- F X ------ --- --- --- --- --- ---
1250 --- 1000 --- --- 800 ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DE04 DE05
X XX XX X--- ------ ---
X XX XX X--- ------ ---X X--- ------ ------ --- --- ------ ------ ---
--- --- --- ------ ------ --- --- ---X X
X X X X
--- ------ ------ ---
--- ---
--- ------ ------ ------ ---X X
X XX X
--- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ ------ ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- ---
January 01, 2016
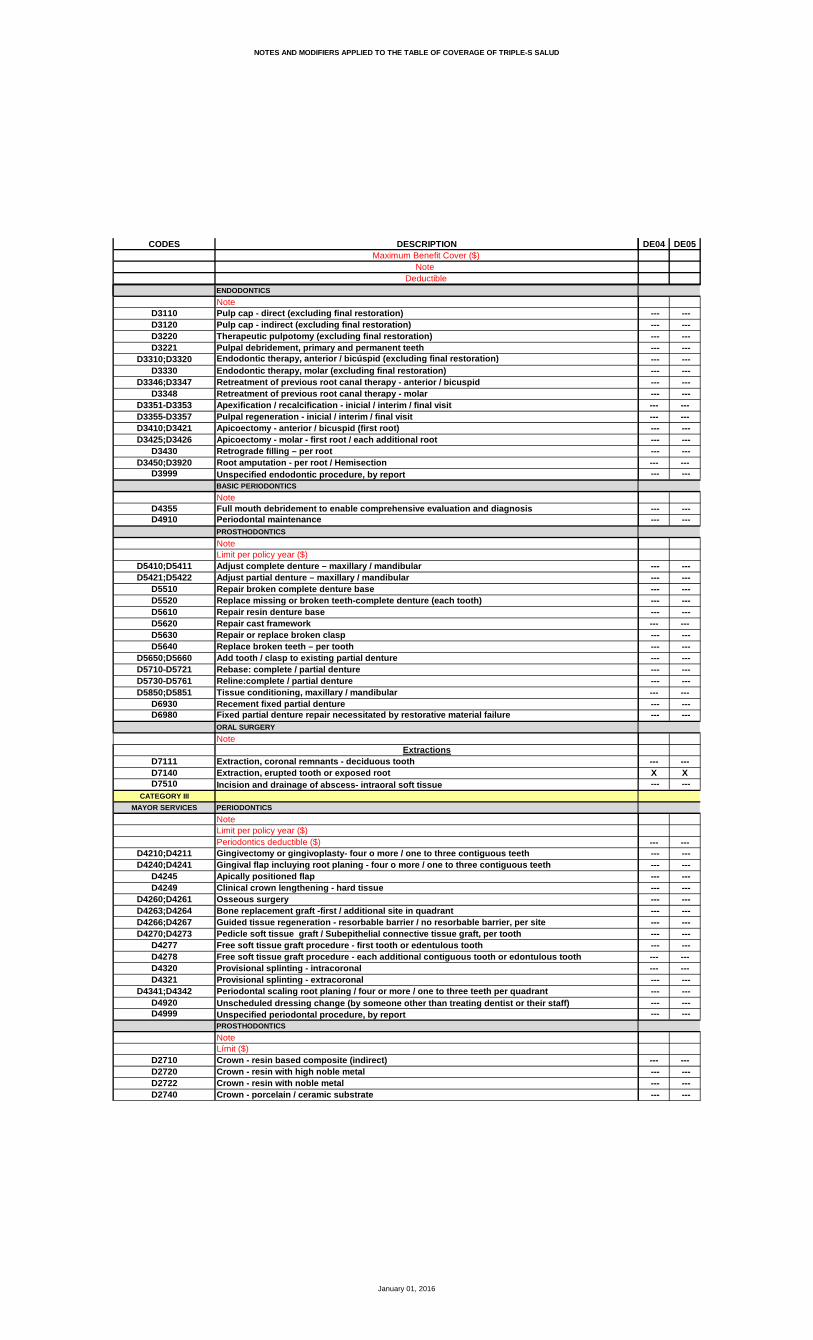
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DE04 DE05
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ ------ --- --- --- --- --- --- ------ --- --- ---
--- --- --- ---
--- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- ---
--- ---X X
--- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ ------ --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DE04 DE05
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ ------ --- --- ------ ------ --- --- ------ ------ --- --- ------ ------ ------ --- --- ------ ------ --- --- --- --- --- --- ------ --- --- ------ ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DE04 DE05
--- --- --- --- --- ------ --- --- ------ --- --- ---
--- --- --- --- --- --- --- ---
--- ---
--- --- --- ------ --- --- ------ ------ --- --- --- --- --- --- ------ --- --- ------ --- --- --- --- ------ ------ ------ ------ ------ --- --- --- --- --- --- --- --- ------ ------ --- --- --- --- ---
--- ------ ------ ------ --- --- --- --- --- --- --- --- --- --- ---X X--- ------ --- --- ------ ---X X
--- --- --- ------ --- --- ------ ------ ---
January 01, 2016
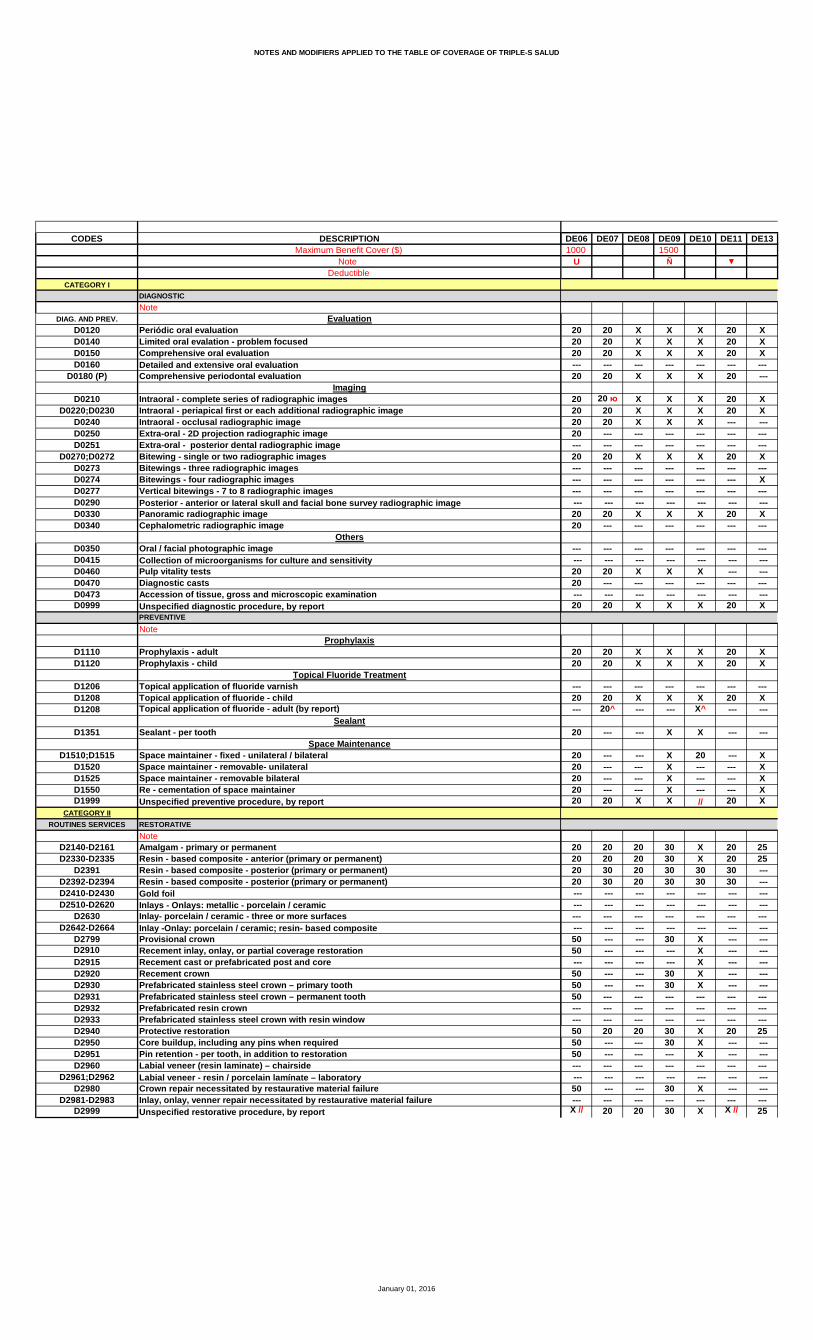
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DE06 DE07 DE08 DE09 DE10 DE11 DE131000 1500
U Ñ
20 20 X X X 20 X20 20 X X X 20 X20 20 X X X 20 X--- --- --- --- --- --- ---20 20 X X X 20 ---
20 20 ю X X X 20 X20 20 X X X 20 X20 20 X X X --- ---20 --- --- --- --- --- ------ --- --- --- --- --- ---20 20 X X X 20 X--- --- --- --- --- --- ------ --- --- --- --- --- X--- --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 X X X 20 X20 --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 X X X --- ---20 --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 X X X 20 X
20 20 X X X 20 X20 20 X X X 20 X
--- --- --- --- --- --- ---20 20 X X X 20 X--- 20^ --- --- X^ --- ---
20 --- --- X X --- ---
20 --- --- X 20 --- X20 --- --- X --- --- X20 --- --- X --- --- X20 --- --- X --- --- X20 20 X X // 20 X
20 20 20 30 X 20 2520 20 20 30 X 20 2520 30 20 30 30 30 ---20 30 20 30 30 30 --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---50 --- --- 30 X --- ---50 --- --- --- X --- --- --- --- --- --- X --- ---50 --- --- 30 X --- ---50 --- --- 30 X --- ---50 --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 20 20 30 X 20 2550 --- --- 30 X --- ---50 --- --- --- X --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---50 --- --- 30 X --- ------ --- --- --- --- --- ---X // 20 20 30 X X // 25
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DE06 DE07 DE08 DE09 DE10 DE11 DE131000 1500
U Ñ
50 --- 20 30 X --- 2550 --- 20 30 X --- ---50 --- 20 30 X --- 2550 20 20 30 X --- 2550 20 20 30 X 20 2550 --- 20 30 X --- 2550 --- 20 30 X 20 ---50 --- 20 30 X --- ---50 --- 20 --- --- --- ------ --- --- --- --- --- ---50 --- 20 --- X --- ---50 --- 20 --- X --- ---50 --- 20 --- X --- ---50 --- 20 --- --- --- ---50 20 20 30 X 20 25
--- 20 20 --- X --- ---20 20 20 X X 20 ---
50 20 --- --- X --- ---50 20 --- --- X --- ---50 --- --- --- X --- ---50 --- --- --- X --- ---50 20 20 30 X 20 ---50 --- 20 30 --- 20 ---50 20 20 30 X 20 ---50 --- 20 30 X 20 ---50 20 20 30 X 20 --- --- --- --- --- 50 --- ---50 --- --- --- 50 --- ---50 --- --- --- --- --- ---50 --- --- 30 X --- --- --- --- --- --- X --- ---
--- --- --- --- --- --- ---20 20 20 30 X 20 2520 --- 20 30 X --- ---
--- --- 1000 ------ --- --- --- --- --- --- --- --- 20 30 X --- --- --- --- 20 30 X --- --- --- --- --- --- X --- --- --- --- 20 30 X --- --- --- --- 20 30 X --- --- --- --- 20 30 X --- --- --- --- 20 --- X --- --- --- --- 20 --- X --- --- --- --- 20 --- X --- ------ --- --- --- --- --- ------ --- 20 --- --- --- --- --- --- 20 --- X --- --- --- --- 20 30 X --- --- --- --- 20 --- --- --- --- --- --- 20 30 X --- ---
--- --- --- --- --- --- --- --- --- --- --- 50 --- ---50 --- --- 30 50 --- ---50 --- --- 30 50 --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DE06 DE07 DE08 DE09 DE10 DE11 DE131000 1500
U Ñ
50 --- --- 30 50 --- ---50 --- --- 30 50 --- ---50 --- --- 30 50 --- --- --- --- --- --- 50 --- --- --- --- --- --- 50 --- --- --- --- --- --- 50 --- ---50 --- --- 30 50 --- ---50 --- --- 30 50 --- --- --- --- --- --- 50 --- ---50 --- --- 30 50 --- --- --- --- --- --- --- --- ---X --- --- 30 50 --- ---
--- --- --- --- 50 --- --- --- --- --- --- 50 --- ---50 --- --- 30 50 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- 30 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 20 20 30 50 20 --- --- --- --- --- 50 --- --- --- --- --- --- 50 --- ------ --- --- --- --- --- --- --- --- --- --- 50 --- --- --- --- --- --- 50 --- ------ --- --- --- --- --- --- --- --- --- --- 50 --- --- --- --- --- --- 50 --- --- --- --- --- --- 50 --- --- --- --- --- --- 50 --- --- --- --- --- --- 50 --- --- --- --- --- --- 50 --- --- --- --- --- --- 50 --- --- --- --- --- --- 50 --- --- --- --- --- --- 50 --- --- --- --- --- --- 50 --- --- --- --- --- --- 50 --- --- --- --- --- --- 50 --- --- --- --- --- --- 50 --- --- --- --- --- --- 50 --- ---50 --- --- 30 50 --- ---50 --- --- 30 50 --- ---50 --- --- 30 50 --- --- --- --- --- 30 50 --- ---50 --- --- 30 50 --- ---50 --- --- 30 50 --- ---50 --- --- 30 50 --- ------ --- --- --- --- --- --- --- --- --- --- 50 --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- 50 --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- 50 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- 50 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- 30 50 --- ---50 --- --- 30 50 --- ---50 --- --- 30 50 --- ---50 --- --- 30 --- --- --- --- --- --- --- 50 --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DE06 DE07 DE08 DE09 DE10 DE11 DE131000 1500
U Ñ
50 --- --- 30 50 --- ---50 --- --- 30 50 --- --- --- --- --- --- 50 --- ------ --- --- --- --- --- ---50 --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- 30 50 --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
20 --- 20 30 30 --- 2520 --- 20 30 30 --- 25--- --- --- --- --- --- ---20 --- 20 30 30 --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 --- --- --- 30 --- --- --- --- --- --- 30 --- ------ --- --- --- --- --- ---20 --- --- --- 30 --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 --- --- --- 50 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 --- --- 30 --- --- ---20 --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- 30 --- ---20 --- 20 30 30 20 25
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 20 --- X --- --- --- --- --- --- --- --- --- --- --- --- --- X X ---X --- 20 X X X 25X --- 20 X X X 25--- --- 20 --- X --- ------ --- --- --- --- --- --- --- --- 20 --- X X ------ --- --- --- --- --- --- --- --- 20 X X X 25
* Ə1 --- --- --- Ə1 --- ℓ ƏX --- --- --- X --- 30--- --- --- --- --- --- ---
800 --- --- --- 1500 --- ------ --- --- --- --- --- 800--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DE14 DE17 DE181000 1000
U ê
X X XX X XX X X--- --- ---X --- X
X X XX X XX X X--- --- ------ --- ---X X X--- --- ------ --- ------ --- --- --- --- ---X X XX --- ---
--- --- --- --- --- --- --- X ------ --- --- --- --- ---X X X
X X XX X X
--- --- ---X X X
--- --- ---
--- X ---
--- 20 30--- --- 30--- --- 30--- 20 30X // //
X 20 30X 20 30X 20 30X 20 30
--- --- ---50 --- 30--- --- --- --- --- --- --- --- --- --- 50 --- --- --- ---50 50 30 --- 50 ------ --- ------ 50 ------ --- ---X 20 3050 50 30 --- 50 ------ --- --- --- --- --- --- --- ------ --- ---X X // 30
January 01, 2016
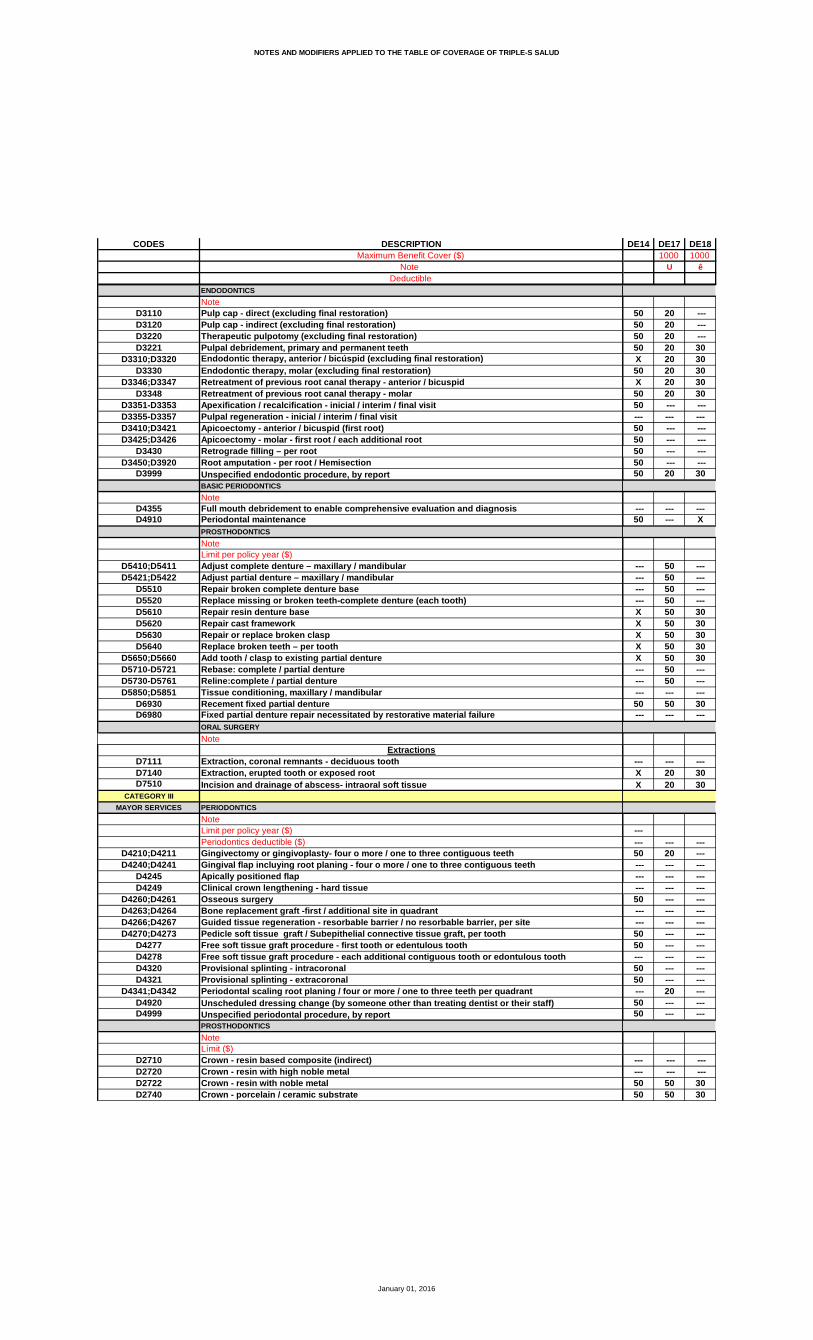
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DE14 DE17 DE181000 1000
U ê
50 20 ---50 20 ---50 20 ---50 20 30X 20 3050 20 30X 20 3050 20 3050 --- ------ --- ---50 --- ---50 --- ---50 --- ---50 --- ---50 20 30
--- --- ---50 --- X
--- 50 --- --- 50 --- --- 50 --- --- 50 ---X 50 30X 50 30X 50 30X 50 30X 50 30
--- 50 --- --- 50 --- --- --- ---50 50 30 --- --- ---
--- --- ---X 20 30X 20 30
------ --- ---50 20 --- --- --- --- --- --- --- --- --- ---50 --- --- --- --- --- --- --- ---50 --- ---50 --- ------ --- ---50 --- ---50 --- --- --- 20 ---50 --- ---50 --- ---
--- --- ------ --- ---50 50 3050 50 30
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DE14 DE17 DE181000 1000
U ê
50 50 30--- --- ------ 50 3050 50 3050 --- 3050 50 30--- --- ------ 50 30--- --- ---50 50 30 --- --- ---50 50 3050 50 ---50 50 ---50 50 30--- --- ------ --- ---50 50 --- --- --- --- --- --- ------ --- ---50 50 30--- --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- 30--- --- 30--- 50 ------ --- ---50 --- 3050 50 3050 50 30--- --- ------ --- ------ --- ------ --- ------ 50 ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ------ --- ---50 --- 3050 --- 3050 50 3050 --- 30--- --- ---50 --- 30
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DE14 DE17 DE181000 1000
U ê
50 --- 3050 50 ------ --- ------ --- --- --- --- ------ --- ---50 50 30
--- --- --- --- --- --- --- --- ---X 20 ---
--- --- ---
X 20 30X 20 30--- --- ---50 20 30--- --- ---50 20 ---50 --- ---50 20 --- --- --- ---50 20 ---50 20 ---50 --- --- --- --- ---50 --- ------ --- ------ --- ------ --- ------ --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- ---50 20 --- --- 20 ---50 20 30
--- --- ------ --- ------ --- ------ --- --- --- --- --- --- --- --- --- --- ---X --- ---X 20 30X 20 30
50 Ξ --- ------ --- ---50 --- ------ --- ---X 20 30
* Ə1 Ə1 ---50 50 ------ --- ---
3000 1000 ------ --- ------ --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DE19 DE20 DE21 DE22 DE23 DE26 DE271000 1000 1000 1000 1000
U Æ ≈ ê U ≈
X X X X 20 X 20X X X X 20 X 20X X X X 20 X 20--- --- --- --- --- --- ---X X X X 20 X 20
X X X X 20 X 20X X X X 20 X 20X --- --- X 20 --- ------ --- --- X --- --- ------ --- --- --- --- --- ---X X X X 20 X 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 20 X 20--- X --- --- 20 X ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- X --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 20 X 20
X X X X 20 X 20X X X X 20 X 20
--- --- X --- --- X ---X X X X 20 X 20 --- --- --- --- --- --- ---
X --- X --- --- --- ---
X --- 30 25 --- --- ------ --- --- 25 --- --- ------ --- --- 25 --- --- ------ --- --- 25 --- --- ---X X // // 20 X 20
30 20 30 25 20 X 2030 20 30 25 20 X 20 --- 30 50 25 30 X 30 --- 30 50 25 30 X 30 --- --- --- --- --- --- --- --- 50 --- --- 50 X ------ --- --- --- --- --- --- --- 50 --- --- 50 --- --- --- --- --- --- --- --- --- --- --- 50 --- --- --- --- --- --- --- --- --- --- --- --- 50 50 50 50 X --- --- --- 50 --- --- --- ------ --- 50 --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 20 30 20 20 X 20 --- 50 50 50 50 X --- --- --- 50 --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---X // X // X // X // X // X //
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DE19 DE20 DE21 DE22 DE23 DE26 DE271000 1000 1000 1000 1000
U Æ ≈ ê U ≈
--- 50 50 --- 50 X --- --- 50 50 --- 50 X ---30 50 50 --- 50 X ---20 50 50 25 50 X ---30 50 50 25 50 X 2030 50 50 25 50 X --- --- 50 50 25 50 X 20 --- 50 50 25 50 X ------ 50 50 --- 50 X ------ --- --- --- --- --- --- --- 50 50 --- 50 X --- --- 50 50 --- 50 X --- --- 50 50 --- 50 X ------ 50 50 --- 50 X ---30 50 50 25 50 X 20
30 50 50 --- 50 X ---30 50 50 X 50 X 20
--- --- 30 --- --- --- ---50 --- 30 --- --- --- ---50 --- 30 --- --- --- ------ --- 30 --- --- --- ------ 20 30 50 20 X 20--- 20 30 50 20 X 2050 20 30 50 20 X 2050 20 30 50 20 X 20--- 20 30 50 20 X 20--- --- 30 --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 50 X ------ --- --- --- --- --- ---
--- --- --- --- --- --- ---30 20 30 25 20 X 2030 20 30 25 20 X ---
U
800 1000 --- ------ --- --- --- --- --- ---30 50 50 --- 50 X ---30 50 50 --- 50 X ---30 50 --- --- 50 X ---30 50 50 --- 50 X ---30 50 50 --- 50 X ---30 50 50 --- 50 X ---30 50 --- --- 50 X ---30 50 50 --- 50 X ---30 50 50 --- 50 X ------ --- --- --- --- --- ------ 50 --- --- 50 X ---30 50 --- --- 50 X ---30 50 50 --- 50 X --- --- 50 --- --- 50 X ---30 50 50 --- 50 X ---
------ --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 50 X ------ 50 50 50 50 X ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DE19 DE20 DE21 DE22 DE23 DE26 DE271000 1000 1000 1000 1000
U Æ ≈ ê U ≈
--- 50 50 50 50 X ------ --- --- --- --- --- ------ 50 50 50 50 X ------ 50 --- --- 50 X ------ 50 --- --- 50 X ------ 50 50 50 50 X ------ --- --- --- --- --- ------ 50 50 50 50 X ------ --- --- --- --- --- ------ 50 50 50 50 X ------ --- --- --- --- --- ------ 50 50 50 50 X ------ 50 50 50 50 X ------ 50 50 50 50 X ------ 50 50 50 50 X ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- 50 --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 50 X 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 50 X ------ 50 --- 50 50 X ------ --- 50 --- --- --- ------ --- --- --- --- --- ------ 50 50 50 50 X ------ 50 50 50 50 X ------ 50 50 50 50 X ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- 50 --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 50 X ------ 50 --- 50 50 X ------ 50 50 50 50 X ------ 50 50 --- 50 X ------ --- --- --- --- --- ------ 50 --- --- 50 X ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DE19 DE20 DE21 DE22 DE23 DE26 DE271000 1000 1000 1000 1000
U Æ ≈ ê U ≈
--- 50 50 50 50 X ------ --- 50 --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 50 X ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 20 X ---
--- --- --- --- --- --- ---
30 50 50 25 50 X ---30 50 50 25 50 X ------ --- --- --- --- --- ---30 50 50 25 50 X ------ --- 50 --- --- --- ------ 50 50 --- 50 X --- --- 50 --- --- 50 X --- --- 50 50 --- 50 X --- --- --- --- --- --- --- --- --- 50 50 --- 50 X --- --- 50 50 --- 50 X --- --- 50 50 --- 50 X --- --- --- --- --- --- --- --- --- 50 50 --- 50 X ------ --- 50 --- --- --- ------ --- 50 --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- 50 --- --- --- ------ 50 50 --- 50 X --- --- --- 50 --- --- --- ---30 50 50 25 50 X 20
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 30 --- --- X X20 20 30 20 20 X X20 20 30 20 20 X X--- 20 Ξ --- --- 20 Ξ 20 Ξ ------ --- --- --- --- --- --- --- 20 30 --- 20 X X --- --- --- --- --- --- --- --- 20 30 20 20 X X
--- Ə1 Ə1 --- Ə1 * Ə1 ------ 50 X --- 50 X ------ --- --- --- --- --- ------ 1000 1000 --- 1000 1000 ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DE28 DE291000
M ≈
20 2020 2020 20--- ---20 20
20 2020 20--- ------ ------ ---20 20--- ------ ------ --- --- ---20 2020 20
--- --- --- --- --- ------ --- --- ---20 20
20 2020 20
X ---20 20 --- ---
--- ---
--- ------ ------ ------ ---20 20
20 2020 2030 3030 30 --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ ------ ------ ---20 20 --- --- --- ------ --- --- --- --- ------ --- // //
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICS
NoteD4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metalD2740 Crown - porcelain / ceramic substrate
DE28 DE291000
M ≈
50 ---50 ---50 ---50 ---50 2050 ---50 2050 ---50 ------ ---50 ---50 ---50 ---50 ---50 20
50 ---50 20
--- ------ ------ ------ ---20 ---20 ---20 ---20 ---20 ------ ------ ------ ------ ------ ---
--- ---20 2020 20
--- ------ ---50 ---50 ------ ---50 ---50 ---50 ---50 ---50 ---50 ------ ---50 ---50 ---50 ---50 ---50 ---
--- ------ ------ ------ ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DE28 DE291000
M ≈
--- ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ---20 ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ------ ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesia D9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DE28 DE291000
M ≈
--- ------ ------ ------ ------ ------ ------ ---
--- ------ ------ ------ ---
--- ---
50 ---50 20--- ---50 ------ ---50 ---50 ---50 ------ ---50 ---50 ---50 --- --- ---50 ------ ------ ------ ------ ------ --- --- --- --- --- --- --- --- ------ ---50 ------ ---50 20
--- ------ ------ ------ --- --- --- --- ------ ---20 X20 X20 X20 ------ ---20 X--- ---20 X
--- ------ ------ ------ ------ ------ ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTION DE30 DE31 DE32 DE33 DE34 DE35 DE46Maximum Benefit Cover ($) 1000 1000 1000 1000 1000
Note U U ≈ ê M U
DeductibleCATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluation 20 X X X X X XD0140 Limited oral evalation - problem focused 20 X X X X X XD0150 Comprehensive oral evaluation 20 X X X X X XD0160 Detailed and extensive oral evaluation --- --- --- --- --- --- ---
D0180 (P) Comprehensive periodontal evaluation 20 --- X X X --- XImaging
D0210 Intraoral - complete series of radiographic im ages 20 --- X X X X XD0220;D0230 Intraoral - periapical first or each add itional radiographic image 20 X X X X X X
D0240 Intraoral - occlusal radiographic image --- --- --- --- X --- ---D0250 Extra-oral - 2D projection radiographic image --- --- --- --- --- --- ---D0251 Extra-oral - posterior dental radiographic im age --- --- --- --- --- --- ---
D0270;D0272 Bitewing - single or two radiographic im ages 20 --- X X X X XD0273 Bitewings - three radiographic images --- --- --- --- --- --- ---D0274 Bitewings - four radiographic images --- --- --- --- --- X XD0277 Vertical bitewings - 7 to 8 radiographic image s --- --- --- --- --- --- ---D0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic image --- --- --- --- --- --- ---D0330 Panoramic radiographic image 20 --- X X X X XD0340 Cephalometric radiographic image 20 --- --- X Ð --- --- ---
OthersD0350 Oral / facial photographic image --- --- --- --- --- --- ---D0415 Collection of microorganisms for culture and sensit ivity --- --- --- --- --- --- ---D0460 Pulp vitality tests --- --- --- --- --- --- ---D0470 Diagnostic casts --- --- --- --- --- --- ---D0473 Accession of tissue, gross and microscopic exa mination --- --- --- --- --- --- ---D0999 Unspecified diagnostic procedure, by report 20 X X X X X X
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adult 20 X X X X 20 XD1120 Prophylaxis - child 20 X X X X 20 X
Topical Fluoride TreatmentD1206 Topical application of fluoride varnish --- --- --- X --- --- ---D1208 Topical application of fluoride - child 20 X X X X 20 XD1208 Topical application of fluoride - adult (by report) --- --- --- --- --- --- ---
SealantD1351 Sealant - per tooth --- --- --- --- --- --- ---
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral --- --- --- --- --- X X
D1520 Space maintainer - removable- unilateral --- --- --- --- --- X XD1525 Space maintainer - removable bilateral --- --- --- --- --- X XD1550 Re - cementation of space maintainer --- --- --- --- --- X XD1999 Unspecified preventive procedure, by report 20 X X X X // X
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanent 20 --- X X 25 X XD2330-D2335 Resin - based composite - anterior (prim ary or permanent) 20 --- X X 25 X X
D2391 Resin - based composite - posterior (primary o r permanent) 30 --- X X 25 --- ---D2392-D2394 Resin - based composite - posterior (pri mary or permanent) 30 --- X X 25 --- ---D2410-D2430 Gold foil --- --- --- --- --- --- ---D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic 50 --- --- X --- --- 50
D2630 Inlay- porcelain / ceramic - three or more sur faces --- --- --- --- --- --- ---D2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite 50 --- --- X --- --- 50
D2799 Provisional crown --- --- --- --- --- --- ---D2910 Recement inlay, onlay, or partial coverage restorat ion --- --- --- --- --- --- ---D2915 Recement cast or prefabricated post and core --- --- --- --- --- --- ---D2920 Recement crown 50 --- --- X --- --- 50D2930 Prefabricated stainless steel crown – primary tooth --- --- --- --- --- --- ---D2931 Prefabricated stainless steel crown – permanen t tooth --- --- --- --- --- --- ---D2932 Prefabricated resin crown --- --- --- --- --- --- ---D2933 Prefabricated stainless steel crown with resin window --- --- --- --- --- --- ---D2940 Protective restoration 20 --- X X 20 20 25 D2950 Core buildup, including any pins when requir ed 50 --- --- X --- --- 50D2951 Pin retention - per tooth, in addition to rest oration --- --- --- --- --- --- ---D2960 Labial veneer (resin laminate) – chairside --- --- --- --- --- --- ---
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora tory --- --- --- --- --- --- ---D2980 Crown repair necessitated by restaurative mate rial failure --- --- --- --- --- --- ---
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure --- --- --- --- --- --- --- D2999 Unspecified restorative procedure, by report X // --- X X 25 X X //
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTION DE30 DE31 DE32 DE33 DE34 DE35 DE46Maximum Benefit Cover ($) 1000 1000 1000 1000 1000
Note U U ≈ ê M U
DeductibleENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration ) 50 --- --- X --- 25 25D3120 Pulp cap - indirect (excluding final restorati on) 50 --- --- X --- --- 25D3220 Therapeutic pulpotomy (excluding final restora tion) 50 --- --- X --- 25 25D3221 Pulpal debridement, primary and permanent teet h 50 --- X X 25 25 25
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration) 50 --- X X 25 25 25D3330 Endodontic therapy, molar (excluding final res toration) 50 --- --- X 25 25 25
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspid 50 --- --- X 25 25 25D3348 Retreatment of previous root canal therapy - m olar 50 --- --- X 25 25 25
D3351-D3353 Apexification / recalcification - inicia l / interim / final visit 50 --- --- X --- --- ---D3355-D3357 Pulpal regeneration - inicial / interim / final visit --- --- --- --- --- --- ---D3410;D3421 Apicoectomy - anterior / bicuspid (first root) 50 --- --- X --- --- ---D3425;D3426 Apicoectomy - molar - first root / each additional root 50 --- --- X --- --- ---
D3430 Retrograde filling – per root 50 --- --- X --- --- ---D3450;D3920 Root amputation - per root / Hemisection 50 --- --- X --- --- ---
D3999 Unspecified endodontic procedure, by report 50 --- X X 25 25 25BASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosis 50 --- --- X 25 --- 50D4910 Periodontal maintenance 50 --- X X 25 --- 50
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibular --- --- --- --- --- --- ---D5421;D5422 Adjust partial denture – maxillary / man dibular --- --- --- --- --- --- ---
D5510 Repair broken complete denture base --- --- --- --- --- --- ---D5520 Replace missing or broken teeth-complete dentu re (each tooth) --- --- --- --- --- --- ---D5610 Repair resin denture base 20 --- --- X --- --- 50D5620 Repair cast framework 20 --- --- X --- --- 50D5630 Repair or replace broken clasp 20 --- --- X --- --- 50D5640 Replace broken teeth – per tooth 20 --- --- X --- --- 50
D5650;D5660 Add tooth / clasp to existing partial de nture 20 --- --- X --- --- 50D5710-D5721 Rebase: complete / partial denture --- --- --- --- --- --- ---D5730-D5761 Reline:complete / partial denture --- --- --- --- --- --- ---D5850;D5851 Tissue conditioning, maxillary / mandibu lar --- --- --- --- --- --- ---
D6930 Recement fixed partial denture 50 --- --- X --- --- 50D6980 Fixed partial denture repair necessitated by restor ative material failure --- --- --- --- --- --- ---
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous tooth --- --- --- --- --- --- ---D7140 Extraction, erupted tooth or exposed root 20 --- X X 25 25 25D7510 Incision and drainage of abscess- intraoral soft ti ssue 20 --- X X 25 25 25
CATEGORY III
MAYOR SERVICES PERIODONTICS
Note U
Limit per policy year ($) --- --- --- --- --- --- 500Periodontics deductible ($) --- --- --- --- --- --- ---
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teeth 50 --- --- X 25 --- 50D4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth 50 --- --- X 25 --- 50
D4245 Apically positioned flap 50 --- --- X --- --- 50D4249 Clinical crown lengthening - hard tissue 50 --- --- X 25 --- 50
D4260;D4261 Osseous surgery 50 --- --- X 25 --- 50D4263;D4264 Bone replacement graft -first / addition al site in quadrant 50 --- --- X 25 --- 50D4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site 50 --- --- X 25 --- 50D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth 50 --- --- X 25 --- 50
D4277 Free soft tissue graft procedure - first tooth or edentulous tooth 50 --- --- X 25 --- 50D4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous tooth --- --- --- - -- --- --- ---D4320 Provisional splinting - intracoronal 50 --- --- X 25 --- 50 D4321 Provisional splinting - extracoronal 50 --- --- X 25 --- 50
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrant 50 --- --- X 2 5 --- 50D4920 Unscheduled dressing change (by someone other than treating dentist or their staff) 50 --- --- X 25 --- 50D4999 Unspecified periodontal procedure, by report 50 --- --- X 25 --- 50
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect) --- --- --- --- --- --- ---D2720 Crown - resin with high noble metal --- --- --- --- --- --- ---D2722 Crown - resin with noble metal --- --- --- X --- --- 50
January 01, 2016
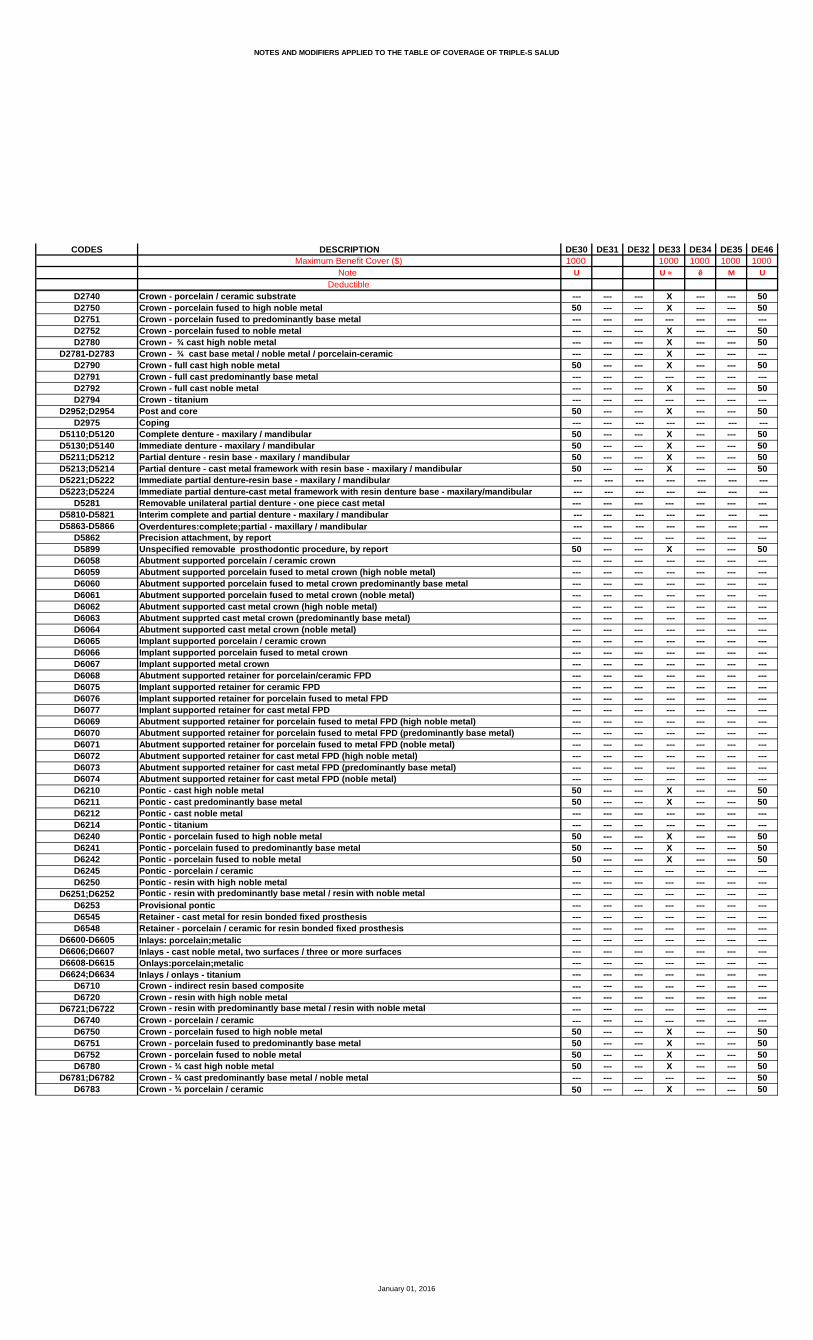
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTION DE30 DE31 DE32 DE33 DE34 DE35 DE46Maximum Benefit Cover ($) 1000 1000 1000 1000 1000
Note U U ≈ ê M U
DeductibleD2740 Crown - porcelain / ceramic substrate --- --- --- X --- --- 50D2750 Crown - porcelain fused to high noble metal 50 --- --- X --- --- 50D2751 Crown - porcelain fused to predominantly base metal --- --- --- --- --- --- ---D2752 Crown - porcelain fused to noble metal --- --- --- X --- --- 50D2780 Crown - ¾ cast high noble metal --- --- --- X --- --- 50
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramic --- --- --- X --- --- ---D2790 Crown - full cast high noble metal 50 --- --- X --- --- 50D2791 Crown - full cast predominantly base metal --- --- --- --- --- --- ---D2792 Crown - full cast noble metal --- --- --- X --- --- 50D2794 Crown - titanium --- --- --- --- --- --- ---
D2952;D2954 Post and core 50 --- --- X --- --- 50D2975 Coping --- --- --- --- --- --- ---
D5110;D5120 Complete denture - maxilary / mandibular 50 --- --- X --- --- 50D5130;D5140 Immediate denture - maxilary / mandibula r 50 --- --- X --- --- 50D5211;D5212 Partial denture - resin base - maxilary / mandibular 50 --- --- X --- --- 50D5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibular 50 --- --- X --- - -- 50D5221;D5222 Immediate partial denture-resin base - m axilary / mandibular --- --- --- --- --- --- ---D5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r --- --- --- --- --- --- ---
D5281 Removable unilateral partial denture - one pie ce cast metal --- --- --- --- --- --- ---D5810-D5821 Interim complete and partial denture - m axilary / mandibular --- --- --- --- --- --- ---D5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar --- --- --- --- --- --- ---
D5862 Precision attachment, by report --- --- --- --- --- --- ---D5899 Unspecified removable prosthodontic procedure , by report 50 --- --- X --- --- 50D6058 Abutment supported porcelain / ceramic crown --- --- --- --- --- --- ---D6059 Abutment supported porcelain fused to metal cr own (high noble metal) --- --- --- --- --- --- ---D6060 Abutment supported porcelain fused to metal cr own predominantly base metal --- --- --- --- --- --- ---D6061 Abutment supported porcelain fused to metal cr own (noble metal) --- --- --- --- --- --- ---D6062 Abutment supported cast metal crown (high nobl e metal) --- --- --- --- --- --- ---D6063 Abutment supprted cast metal crown (predominan tly base metal) --- --- --- --- --- --- ---D6064 Abutment supported cast metal crown (noble met al) --- --- --- --- --- --- ---D6065 Implant supported porcelain / ceramic crown --- --- --- --- --- --- ---D6066 Implant supported porcelain fused to metal cro wn --- --- --- --- --- --- ---D6067 Implant supported metal crown --- --- --- --- --- --- ---D6068 Abutment supported retainer for porcelain/cera mic FPD --- --- --- --- --- --- ---D6075 Implant supported retainer for ceramic FPD --- --- --- --- --- --- ---D6076 Implant supported retainer for porcelain fused to metal FPD --- --- --- --- --- --- ---D6077 Implant supported retainer for cast metal FPD --- --- --- --- --- --- ---D6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal) --- --- --- --- --- -- - ---D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal) --- --- --- --- --- --- ---D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal) --- --- --- --- --- --- ---D6072 Abutment supported retainer for cast metal FPD (high noble metal) --- --- --- --- --- --- ---D6073 Abutment supported retainer for cast metal FPD (predominantly base metal) --- --- --- --- --- --- ---D6074 Abutment supported retainer for cast metal FPD (noble metal) --- --- --- --- --- --- ---D6210 Pontic - cast high noble metal 50 --- --- X --- --- 50D6211 Pontic - cast predominantly base metal 50 --- --- X --- --- 50D6212 Pontic - cast noble metal --- --- --- --- --- --- ---D6214 Pontic - titanium --- --- --- --- --- --- ---D6240 Pontic - porcelain fused to high noble metal 50 --- --- X --- --- 50D6241 Pontic - porcelain fused to predominantly base metal 50 --- --- X --- --- 50D6242 Pontic - porcelain fused to noble metal 50 --- --- X --- --- 50D6245 Pontic - porcelain / ceramic --- --- --- --- --- --- ---D6250 Pontic - resin with high noble metal --- --- --- --- --- --- ---
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metal --- --- --- --- --- --- ---D6253 Provisional pontic --- --- --- --- --- --- ---D6545 Retainer - cast metal for resin bonded fixed p rosthesis --- --- --- --- --- --- ---D6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis --- --- --- --- --- --- ---
D6600-D6605 Inlays: porcelain;metalic --- --- --- --- --- --- ---D6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfaces --- --- --- --- --- --- ---D6608-D6615 Onlays:porcelain;metalic --- --- --- --- --- --- ---D6624;D6634 Inlays / onlays - titanium --- --- --- --- --- --- ---
D6710 Crown - indirect resin based composite --- --- --- --- --- --- ---D6720 Crown - resin with high noble metal --- --- --- --- --- --- ---
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metal --- --- --- --- --- --- ---D6740 Crown - porcelain / ceramic --- --- --- --- --- --- ---D6750 Crown - porcelain fused to high noble metal 50 --- --- X --- --- 50D6751 Crown - porcelain fused to predominantly base metal 50 --- --- X --- --- 50D6752 Crown - porcelain fused to noble metal 50 --- --- X --- --- 50D6780 Crown - ¾ cast high noble metal 50 --- --- X --- --- 50
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metal --- --- --- --- --- --- 50D6783 Crown - ¾ porcelain / ceramic 50 --- --- X --- --- 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTION DE30 DE31 DE32 DE33 DE34 DE35 DE46Maximum Benefit Cover ($) 1000 1000 1000 1000 1000
Note U U ≈ ê M U
DeductibleD6790 Crown - full cast high noble metal 50 --- --- X --- --- 50
D6791;D6792 Crown - full cast predominantly base metal / noble metal --- --- --- --- --- --- ---D6794 Crown - titanium --- --- --- --- --- --- ---D6920 Connector bar --- --- --- --- --- --- ---D6940 Stress breaker --- --- --- --- --- --- ---D6950 Precision attachment --- --- --- --- --- --- ---D6999 Unspecified, fixed prosthodontic procedure, by repo rt 50 --- --- X --- --- 50
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection --- --- --- --- --- --- ---D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis --- --- --- --- --- --- ---D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator --- --- --- --- --- --- ---
D5986 Fluoride gel carrier --- --- --- --- --- --- ---IMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgery --- --- --- --- --- --- ---ORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth 50 --- --- X 25 25 25
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bony 50 --- X X 25 25 25D7241 Removal of impacted tooth – completely bony, w ith unusual surgical complication --- --- --- --- --- --- ---D7250 Surgical removal of residual tooth roots 50 --- --- X 25 --- ---D7260 Oroantral fistula closure --- --- --- --- --- --- ---D7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced tooth 50 --- --- X --- --- ---D7272 Tooth transplantation 50 --- --- X --- --- --- D7280 Surgical access of an unerupted tooth 50 --- --- X --- --- --- D7283 Placement of device to facilitate eruption of impac ted tooth --- --- --- --- --- --- ---D7285 Biopsy of oral tissue - hard (bone, tooth) 50 --- --- X --- --- ---D7286 Biopsy of oral tissue - soft 50 --- --- X --- --- ---D7290 Surgical repositioning of teeth 50 --- --- X --- --- ---D7291 Transseptal fiberotomy/supra crestal fiberotomy, by report --- --- --- --- --- --- ---
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractions 50 --- -- - X --- --- ---D7340 Vestibuloplasty-ridge extension (secondary epi thelialization) --- --- --- --- --- --- ---D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….) --- --- --- --- --- --- ---
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularis --- --- --- --- --- --- ---D7520 Incision and drainage of abscess – extraoral s oft tissue --- --- --- --- --- --- ---D7550 Partial ostectomy /Sequestrectomy for removal of non-vital bone --- --- --- --- --- --- ---D7880 Occlusal orthotic device, by report --- --- --- --- --- --- ---D7881 Occlusal orthotic device adjustment --- --- --- --- --- --- ---D7910 Suture of recent small wounds up to 5 cm --- --- --- --- --- --- ---D7953 Bone replacement graft for ridge preservation – per site --- --- --- --- --- --- ---D7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedure --- --- --- --- --- --- ---D7970 Excision of hyperplastic tissue - per arch 50 --- --- X --- --- ---D7971 Excision of pericoronal gingiva --- --- --- --- --- --- ---D7999 Unspecified oral surgery procedure, by report 50 --- X X 25 25 25
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedure --- --- --- --- --- --- ---D9230 Inhalation of nitrous oxide / analgesia, anxio lysis --- --- --- --- --- --- ---D9243 Intravenous moderate (conscious) sedation/anal gesia --- --- --- --- --- --- ---D9310 Consultation - diagnostic service provided by dentist or physician --- --- --- --- --- --- ---D9410 House / extended care facility call --- --- --- --- --- --- ---D9420 Hospital or ambulatory surgical center call --- --- --- --- --- --- ---
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours) --- --- --- --- --- --- ---D9630 Other drugs and / or medicaments, by report 20 --- X --- --- --- ---D9910 Application of desensitizing medicament 20 --- X X 20 20 25D9930 Reatment of complications (post-surgical) - un usual circumstances, by report 20 --- X X --- 20 25
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted case 20 --- --- X --- --- ---D9943 Occlusal guard adjustment --- --- --- --- --- --- ---
D9951;D9952 Occlusal adjustment - limited / complete 20 --- --- X --- --- ---D9973;D9974 External / Internal bleaching – per tooth --- --- --- --- --- --- ---
D9999 Unspecified adjunctive procedure – by report 20 --- X X --- 20 25ORTHODONTIC
Note * Ə1 --- --- * Ə1 --- --- Ə1D8210-D8690 Orthodontic Services 50 --- --- X --- --- 50
D8691 Repair of orthodontic appliance --- --- --- --- --- --- ---Lifetime limit ($) 1000 --- --- 1000 --- --- 1000Límit per policy year ($) --- --- --- --- --- --- ---Deductible Orthodontics ($) --- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DE47 DE50 DE52 DE541000 1000
U ≈
X X X XX X X XX X X X--- --- --- ------ X X X
X X X XX X X XX --- --- ------ --- --- ------ --- --- ---X X X X--- --- --- ------ --- --- X--- --- --- --- --- --- --- ---X X X X--- --- --- ---
--- --- --- --- --- --- --- ---X --- --- ------ --- --- --- --- --- --- ---X X X X
X X X XX X X X
X --- --- ---X X X X--- --- --- ---
X --- X X
20 --- 20 X--- --- --- ------ --- --- ---20 --- --- ---// X // X
20 30 20 2020 30 20 2020 30 --- 2020 30 --- 20 --- --- --- --- --- 50 --- ------ --- --- --- --- --- --- --- --- --- --- ---50 --- --- --- --- --- --- ---50 --- --- ---50 --- --- ------ --- --- ---50 --- --- ------ --- --- ---20 X 20 2050 50 --- ---50 --- --- ------ --- --- --- --- --- --- --- --- --- --- ------ --- --- ---X // X // 20 20
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DE47 DE50 DE52 DE541000 1000
U ≈
20 30 --- ---20 30 --- ---20 30 20 ---20 30 20 2020 30 20 2020 30 20 2020 30 --- 2020 30 --- 20--- --- --- ------ --- --- ------ 30 --- ------ 30 --- ------ 30 --- ------ 30 --- ---20 30 20 20
Œ--- --- --- ------ X 20 X
Œ1000
50 --- --- 2050 --- 40 ---50 --- --- ---50 --- --- ---50 50 --- ---50 50 --- ---50 50 40 ---50 50 40 ---50 50 --- ---50 --- --- ---50 --- --- ------ --- --- ---50 50 --- 20--- --- --- X
--- --- --- ---20 30 20 2020 30 20 20
U
--- --- --- ------ --- --- ---20 30 --- ------ 30 --- ------ 30 --- ------ 30 --- ------ 30 --- 20--- 30 --- ------ --- --- ------ 30 --- ------ 30 --- ------ --- --- ------ 30 --- ------ 30 --- ---20 30 --- 20--- 30 --- ---20 30 --- 20
Œ1000
--- --- --- ------ --- --- ---50 50 --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DE47 DE50 DE52 DE541000 1000
U ≈
50 50 --- ---50 50 --- 50--- --- --- ---50 --- --- ---50 50 --- 50--- --- --- ---50 50 --- ------ --- --- ---50 --- --- 50--- --- --- ---50 50 --- --- --- --- --- ---50 50 40 5050 50 --- ---50 50 --- ---50 50 40 50 --- --- --- --- --- --- --- ---50 --- --- --- --- --- --- --- --- --- --- ------ --- --- ---50 50 40 50--- --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- 50--- --- --- ---50 --- --- ------ --- --- ------ 50 --- 5050 50 --- ---50 50 --- ------ --- --- ------ --- --- 50--- --- --- ------ --- --- ---50 --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- 50--- --- --- ------ --- --- ------ 50 --- 50--- 50 --- ---50 --- --- ------ 50 --- ------ --- --- ------ --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DE47 DE50 DE52 DE541000 1000
U ≈
--- 50 --- 5050 --- --- ------ --- --- ------ --- --- --- --- --- --- ------ --- --- ---50 50 --- 50
--- --- --- --- --- --- --- --- --- --- --- ---20 --- --- ---
--- --- --- ---
20 30 20 2020 30 20 20--- --- --- ---20 30 20 ------ --- --- ---20 30 --- --- --- 30 --- ---20 30 --- ------ --- --- ------ 30 --- ---20 30 --- ------ 30 --- --- --- --- --- --- --- 30 --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- ------ --- --- ---20 30 --- ---20 --- --- ---20 30 20 20
--- --- --- ------ --- --- ------ --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---20 X 20 2020 X 20 ------ X --- ------ --- --- --- --- X --- ------ --- --- ---20 X 20 20
* Ə1 Ə1 --- * Ə150 50 --- 50--- --- --- ---
1000 1000 --- 1000--- --- --- ------ --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DE55 DE56 DE57 DE58 DE59 DE60 DE611000 1000 1000 1500
ê d ê ≈ Ñ
X X X X 20 X XX X X X 20 X XX X X X 20 X X--- --- --- --- --- --- ---X X --- X --- --- X
X X X X 20 --- XX X X X 20 X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X X 20 --- X--- --- --- --- --- --- ------ --- X --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 20 --- X--- --- --- X --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 20 X X
X X X X 20 X XX X X X 20 X X
--- --- --- --- X --- ---X X X X 20 X X--- --- --- --- --- --- ---
--- --- --- --- --- --- ---
--- --- X --- --- --- ------ --- X --- --- --- ------ --- X --- --- --- ------ --- X --- --- --- ---X X X X 20 X X
X 20 X X 20 30 50X 20 X X 20 30 50X 20 --- X 20 30 50X 20 --- X 20 30 50
--- --- --- --- --- --- --- --- 50 50 --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 --- 20 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---X 20 25 X 20 --- X
--- 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---X 20 X // X 20 --- 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DE55 DE56 DE57 DE58 DE59 DE60 DE611000 1000 1000 1500
ê d ê ≈ Ñ
--- 50 25 X --- --- 50 --- 50 25 X --- --- 50 --- 50 25 X 20 --- 50X 50 25 X 20 --- 50X 50 25 X 20 --- 50
--- 50 25 X 20 --- 50X 50 25 X 20 --- ---
--- 50 25 X 20 --- ------ 50 --- X --- --- 50--- --- --- --- --- --- --- --- 50 --- X --- --- 50 --- 50 --- X --- --- 50 --- 50 --- X --- --- 50--- 50 --- X --- --- 50X 50 25 X 20 --- 50
--- 50 --- X --- --- ---X 50 --- X --- --- 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---X 20 50 X 20 --- 50X 20 50 X 20 --- 50X 20 50 X 20 --- 50X 20 50 X 20 --- 50X 20 50 X 20 --- 50
--- --- --- --- --- --- --- --- --- --- --- 20 --- 50 --- --- --- --- --- --- --- --- 50 50 --- --- --- 50 --- --- --- --- --- ---
--- --- --- --- --- --- ---X 50 25 X 20 --- 50X 50 25 X 20 --- 50
--- 1000 --- --- --- --- ------ --- --- --- --- --- ------ 50 --- X --- --- 50--- 50 --- X --- --- ------ --- --- --- --- --- ------ 50 --- X --- --- ------ 50 --- X --- --- 50--- 50 --- X --- --- ------ 50 --- X --- --- ------ 50 --- X --- --- 50--- 50 --- X --- --- 50--- --- --- --- --- --- ------ 50 --- X --- --- 50--- 50 --- X --- --- 50--- 50 --- X --- --- 50--- 50 --- X --- --- 50--- 50 --- X --- --- 50
--- --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DE55 DE56 DE57 DE58 DE59 DE60 DE611000 1000 1000 1500
ê d ê ≈ Ñ
--- 50 50 --- --- --- ------ 50 50 --- --- --- ------ --- --- --- --- --- ------ 50 50 --- --- --- ------ 50 50 --- --- --- ------ 50 50 --- --- --- ------ 50 50 --- --- --- ------ --- --- --- --- --- ------ 50 50 --- --- --- ------ --- --- --- --- --- ------ 50 50 --- --- --- ------ --- --- --- --- --- ------ 50 50 --- --- --- 50--- 50 50 --- --- --- 50--- 50 50 --- --- --- 50--- 50 50 --- --- --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X 50 50 X 20 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 --- --- --- ------ 50 50 --- --- --- ------ 50 --- --- --- --- ------ --- --- --- --- --- ------ 50 50 --- --- --- 50--- 50 50 --- --- --- 50--- 50 50 --- --- --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 --- --- --- 50--- 50 50 --- --- --- 50--- 50 50 --- --- --- 50--- 50 50 --- --- --- 50--- --- --- --- --- --- ------ 50 50 --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DE55 DE56 DE57 DE58 DE59 DE60 DE611000 1000 1000 1500
ê d ê ≈ Ñ
--- 50 50 --- --- --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ 50 --- --- --- --- 50
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X --- --- X --- --- 50
--- --- --- --- --- --- ---
--- 50 25 X --- --- 50--- 50 25 X --- --- 50--- --- --- --- --- --- --- --- 50 --- X --- --- 50--- --- --- --- --- --- ------ 50 --- X --- --- 50--- 50 --- X --- --- 50--- 50 --- X --- --- 50--- --- --- --- --- --- ------ --- --- X --- --- 50--- 50 --- X --- --- 50--- 50 --- X --- --- 50--- --- --- --- --- --- ------ 50 --- X --- --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ 50 --- X --- --- 50--- --- --- --- --- --- ------ 50 25 X --- --- 50
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X 20 25 X 20 --- X--- --- --- --- --- --- X--- --- --- X --- --- X Ξ--- --- --- --- --- --- ------ --- --- X --- --- X--- --- --- --- --- --- ------ 20 --- --- --- --- X
--- * Ə1 --- --- ą Ə1 --- *Ə1--- X --- --- 20 --- X--- --- --- --- --- --- ------ 1000 --- --- --- --- 1000--- --- --- --- 250 --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DE62 DE63 DE64 DE65 DE66 DE67 DE681000 1000 1000π ê U
30 X X X X X 3030 X X X X X 3030 X X X X X 30--- --- --- --- --- --- ---30 X --- X X X 30
30 X X X X X 3030 X X X X X 3030 --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 X X X X X 30--- --- --- --- --- --- ------ --- X --- X X ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 X X X X X 30--- --- --- --- X XÐ 30
--- --- --- --- --- --- --- --- --- --- --- --- --- ---30 --- --- X X --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 X X X X X 30
30 X X X X X 3030 X X X X X 30
--- --- --- --- --- --- ---30 X X X X X 30
30 ^ --- --- X^ --- --- ---
30 X X 20 X X ---
30 20 X 20 X X ------ --- X --- X X ------ --- X --- X X ------ --- X --- X X ---30 // X // X X 30
30 50 X 20 30 30 3030 50 X 20 30 30 3030 50 --- 20 --- --- 3030 50 --- 20 --- --- 30 --- --- --- --- --- --- --- --- --- 50 --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 20 --- --- ---30 20 --- 20 --- 50 --- --- --- --- --- --- 50 ---30 20 50 20 --- --- ---30 --- --- 20 --- 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 X 25 20 X X 30--- --- 50 20 --- 50 ---30 --- --- 20 --- 50 ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 20 --- 50 ------ --- --- --- --- --- ---30 X // X // 20 X // X // 30
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DE62 DE63 DE64 DE65 DE66 DE67 DE681000 1000 1000π ê U
30 --- 25 50 30 30 ---30 --- 25 X --- --- ---30 --- 25 50 30 30 ---30 X 25 20 30 30 ---30 20 25 50 30 30 50--- --- 25 50 30 30 ---30 20 25 50 30 30 50--- --- 25 50 30 30 ------ --- --- --- 30 30 ------ --- --- --- --- --- ---30 20 --- 50 30 30 ------ --- --- 50 --- --- ------ --- --- --- 30 30 ------ --- --- 50 30 30 ---30 20 25 50 30 30 50
30 --- --- 50 --- --- ------ 20 --- 50 30 30 30
30 --- --- X 30 30 ---30 --- --- X 30 30 ---30 --- --- X 30 30 ---30 --- --- X 30 30 ---30 20 50 X 30 30 ------ 20 50 --- 30 30 ---30 20 50 X 30 30 X30 20 50 X 30 30 X30 20 50 X 30 30 X--- --- --- 50 --- --- ------ --- --- 50 30 30 ------ --- --- --- 30 30 ---30 20 X X 50 50 ------ --- --- X --- --- ---
--- --- --- --- --- --- ---30 30 25 X 30 30 2030 30 25 X 30 30 20
--- --- --- 1000 --- --- ------ --- --- --- --- --- ------ --- --- 50 30 30 ------ --- --- 50 30 30 ------ --- --- 50 --- --- ------ --- --- 50 --- --- ------ --- --- 50 30 30 ------ --- --- 50 --- --- ------ --- --- 50 --- --- ------ --- --- 50 --- --- ------ --- --- 50 --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- 50 --- --- ------ --- --- 50 30 30 --- --- --- --- --- --- --- ------ --- --- 50 30 30 ---
500--- --- --- --- --- --- ------ --- --- 50 --- --- ------ --- 50 50 --- 50 ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DE62 DE63 DE64 DE65 DE66 DE67 DE681000 1000 1000π ê U
--- --- 50 50 --- 50 ------ --- 50 50 --- --- ------ --- --- --- --- 50 ------ --- 50 50 --- 50 ------ --- 50 50 --- --- ------ --- 50 50 --- --- ------ --- 50 50 --- --- ------ --- --- --- --- 50 ------ --- 50 50 --- 50 ------ --- --- --- --- --- ------ --- 50 50 --- 50 ------ --- --- --- --- --- ------ --- 50 50 --- 50 ------ --- 50 50 --- 50 ------ --- 50 --- --- 50 ------ --- 50 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- 50 --- 50 ------ --- --- --- 30 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 20 50 50 30 50 X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- 50 50 --- --- ------ --- 50 --- --- 50 ------ --- --- 50 --- 50 ------ --- --- --- --- --- ------ --- 50 50 --- --- ------ --- 50 50 --- 50 ------ --- 50 50 --- 50 ------ --- --- --- --- --- ------ --- --- 50 --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- 50 ------ --- --- --- --- --- ------ --- --- --- --- 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- 50 --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- 50 50 --- --- ------ --- 50 --- --- 50 ------ --- 50 50 --- 50 ------ --- 50 --- --- --- ------ --- --- --- --- --- ------ --- 50 --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DE62 DE63 DE64 DE65 DE66 DE67 DE681000 1000 1000π ê U
--- --- 50 50 --- --- ------ --- --- 50 --- 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- 50 50 --- 50 ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 30 30 ---
--- --- --- --- --- --- ---
30 --- 25 50 30 30 ---30 30 25 50 30 30 ------ --- --- --- --- --- ---30 --- --- 50 30 30 ------ --- --- --- 30 30 ------ --- --- 50 30 30 --- --- --- --- --- --- --- ---30 --- --- 50 30 30 ------ --- --- --- --- --- ------ --- --- --- 30 30 ---30 --- --- 50 30 30 ------ --- --- --- 30 30 --- --- --- --- --- --- --- --- --- --- --- 50 30 30 ------ --- --- --- 30 30 ------ --- --- --- 30 30 ------ --- --- --- 30 30 ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- 30 --- ------ --- --- 50 30 30 --- --- --- --- --- 30 30 ---30 30 25 50 30 30 20
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- 30 30 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---30 --- --- X --- --- ---30 X 25 20 X 30 3030 X --- 20 30 30 30--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- X --- --- ------ --- --- --- --- --- ---30 --- 25 X 30 30 30
--- --- --- Ə1 --- Ə1 ------ --- --- 50 --- 50 ------ --- --- --- --- --- ------ --- --- 1000 --- 1500 ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DE69 DE70 DE73 DE74 DF02 DF03 DF041000
ê
X X X X 20 X XX X X X 20 X XX X X X 20 X X--- --- --- --- --- --- ------ X X X --- --- X
X X X X 20 X XX X X X 20 X X Þ--- --- --- --- 20 X ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X X 20 X X--- --- --- --- --- --- ------ --- X X --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 20 X XX --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 20 X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 20 X X
X X X X 20 X XX X X X 20 X X
--- --- --- --- --- --- ---X X X X 20 X X
--- --- --- --- 20^ X^ X
--- X X X 20 X X
--- 20 30 30 --- --- XБ--- --- 30 30 --- --- ------ --- 30 30 --- --- ------ --- 30 30 --- --- ---X // // // 20 X X
25 20 X X 20 X X 25 20 X X 20 X X 25 20 --- --- 30 30 X 25 20 --- --- 30 30 X --- --- --- --- --- --- --- --- --- 50 50 --- --- ------ --- --- --- --- --- --- --- --- 50 50 --- --- --- --- --- --- --- 20 X X --- 20 30 30 20 X X --- --- --- --- --- --- ---50 20 30 30 20 X X --- --- X X 20 X ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 X X X 20 X X50 --- 50 50 --- --- --- --- --- --- --- 20 X ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 30 30 --- --- ------ --- --- --- --- --- ---X // 20 30 30 20 X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DE69 DE70 DE73 DE74 DF02 DF03 DF041000
ê
--- --- 30 30 X X --- --- --- --- --- X X --- --- --- 30 30 X X X --- X 30 30 X X ---25 20 30 30 X X X25 --- 30 30 --- --- X25 20 30 30 X X X 25 --- 30 30 --- --- --- --- --- 30 30 --- --- ------ --- --- --- --- --- --- --- 20 30 30 X X --- --- --- --- --- --- --- --- --- --- 30 30 X X --- --- --- 30 30 --- --- ---25 20 30 30 X X X
--- --- --- --- --- --- ------ 20 50 50 --- --- ---
--- --- --- --- X X X--- --- --- --- X X X--- --- --- --- X X X--- --- --- --- X X X--- 20 30 30 X X X--- 20 30 30 --- --- ---X 20 30 30 X X ---X 20 30 30 X X ---X 20 --- --- X X ------ --- --- --- --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---50 20 30 30 X X ------ --- --- --- X X X
--- --- --- --- --- --- ---25 30 X X X X X 25 30 X X --- --- X
#--- --- --- --- --- --- 800--- --- --- --- --- --- ------ --- 50 50 --- --- ------ --- 50 50 --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- 50 50 --- --- X--- --- 50 50 --- --- ------ --- 50 50 --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- 50 50 --- --- --- --- --- --- --- --- --- ------ --- 50 50 --- --- ---
#800
--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 50 --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DE69 DE70 DE73 DE74 DF02 DF03 DF041000
ê
50 --- 50 50 --- --- ---50 --- 50 50 --- --- ------ --- --- --- --- --- ---50 --- 50 50 --- --- ------ --- 50 50 --- --- ------ --- 50 50 --- --- ---50 --- 50 50 --- --- ------ --- --- --- --- --- ---50 --- 50 50 --- --- ------ --- --- --- --- --- ---50 --- 50 50 --- --- ------ --- --- --- --- --- ---50 --- 50 50 --- --- X50 --- 50 50 --- --- ---50 --- 50 50 --- --- X50 --- 50 50 --- --- X --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 20 50 50 X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 30 30 --- --- ---50 --- 30 30 --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 30 30 --- --- ---50 --- 30 30 --- --- ---50 --- 30 30 --- --- ------ --- --- --- --- --- ---50 --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 30 30 --- --- ---50 --- 30 30 --- --- ---50 --- 30 30 --- --- ------ --- 30 30 --- --- ------ --- --- --- --- --- ------ --- 30 30 --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DE69 DE70 DE73 DE74 DF02 DF03 DF041000
ê
50 --- 30 30 --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 30 30 --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
25 --- X X --- --- X25 30 X X --- --- X --- --- --- --- --- --- ---25 --- --- --- --- --- X --- --- X X --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- X --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- X X --- --- X --- --- X X --- --- ------ --- --- --- --- --- ------ --- X X --- --- ------ --- X X --- --- ------ --- X X --- --- ------ --- X X --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- X X --- --- ------ --- X X --- --- ------ --- X X --- --- ---25 30 X X --- --- X
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- X X --- --- --- --- --- --- --- --- --- --- --- --- X X X X X 20 X X X X X X 20 X X X X X X --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- X X --- --- ------ --- --- --- --- --- ---20 --- X X X X ---
--- --- Ə1 Ə1 --- --- ------ --- F F --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DF05 DF06 DF07 DF08
X X X 30X X X 30X X X 30--- --- --- ---X X X ---
X Xp Xp 30X Þ X X 30--- X X 30--- --- --- ------ --- --- ---X X X 30--- --- --- ------ --- --- ------ --- --- --- --- --- --- ---X : Xp Xp 30--- --- --- ---
--- --- --- --- --- --- --- ---X X X 30--- --- --- --- --- --- --- ---X X X 30
X X X 30X X X 30
--- --- --- ---X X X 30
X^ X^ X^ 30^
20 X X 30
20 X X 30--- --- --- ------ --- --- ------ --- --- ---// X X 30
20 20 20 X20 20 20 X30 20 20 3030 20 20 30 --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- 20 20 X --- 20 20 X --- 20 20 X --- 20 20 X --- 20 20 X --- --- --- --- --- --- --- --- --- --- --- ---20 20 20 X --- 20 20 X --- 20 20 X--- --- --- --- --- --- --- --- --- 20 20 X--- --- --- ---20 20 20 X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DF05 DF06 DF07 DF08
--- 20 20 X20 20 20 X20 20 20 X20 20 20 X20 20 20 X20 20 20 X20 20 20 X --- 20 20 X --- --- --- ------ --- --- --- --- 20 20 X --- 20 20 --- --- 20 20 X --- --- --- ---20 20 20 X
--- 20 20 ---20 20 20 ---
1000 --- 20 20 X40 20 20 X40 20 20 X --- 20 20 X40 20 20 X --- --- --- ---40 20 20 X40 20 20 X --- 20 20 X40 20 20 5040 20 20 50 --- --- --- --- --- 20 20 X --- 20 20 X
--- --- --- ---20 X X X20 X X X
--- --- --- ------ --- --- ------ 20 20 ------ 20 20 ------ 20 20 ------ 20 20 ------ 20 20 ------ 20 20 ------ 20 20 ------ 20 20 ------ 20 20 ------ --- --- ------ --- --- ------ 20 20 ---20 20 20 ------ --- --- ------ 20 20 ---
1000 --- --- --- --- --- 20 20 5720 20 20 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DF05 DF06 DF07 DF08
20 20 20 50 --- 20 20 57 --- 20 20 5020 20 20 50 --- 20 20 57 --- 20 20 50 --- 20 20 57 --- 20 20 50 --- 20 20 50 --- 20 20 57 --- 20 20 50 --- --- --- ---40 20 20 50 --- 20 20 50 --- 20 20 5040 20 20 50 --- --- --- --- --- --- --- --- --- 20 20 50 --- --- --- --- --- --- --- ------ --- --- ---40 20 20 50 --- 20 20 50 --- 20 20 57 --- --- --- --- --- 20 20 50 --- 20 20 57 --- --- --- --- --- 20 20 50 --- 20 20 50 --- 20 20 57 --- 20 20 57 --- 20 20 50 --- 20 20 50 --- 20 20 57 --- 20 20 57 --- 20 20 57 --- 20 20 50 --- 20 20 50 --- 20 20 57 --- 20 20 50 --- 20 20 50 --- 20 20 57 --- 20 20 50 --- 20 20 50 --- 20 20 57 --- 20 20 57 --- 20 20 50 --- 20 20 50 --- --- --- --- --- 20 20 57 --- --- --- --- --- --- --- --- --- 20 20 50 --- --- --- --- --- --- --- --- --- 20 20 50 --- --- --- --- --- --- --- --- --- --- --- --- --- 20 20 57 --- --- --- --- --- --- --- --- --- 20 20 57 --- 20 20 50 --- 20 20 50 --- --- --- --- --- 20 20 50 --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DF05 DF06 DF07 DF08
--- 20 20 57 --- 20 20 50 --- 20 20 57 --- --- --- --- --- --- --- --- --- --- --- --- --- 20 20 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- ---
20 20 20 3020 20 20 30--- --- --- ---20 20 20 30--- --- --- ------ --- --- --- --- --- --- --- --- 20 20 --- --- 20 20 --- --- --- --- --- --- 20 20 30 --- --- --- --- --- --- --- --- --- 20 20 50--- --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- ---20 --- --- ------ --- --- --- --- 20 20 3020 20 20 30
--- --- --- ------ --- --- ------ --- --- --- --- --- --- --- --- --- --- ---20 X X X --- --- --- --- --- X X X20 X X X20 X X X --- --- --- ------ --- --- --- --- X X --- --- --- --- ---20 X X X
--- Ə --- --- --- 50 --- ------ --- --- ------ 1500 --- ------ --- --- ------ --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DF09 DF10 DF11 DF12 DF13 DF14 DF151000 1000
ċ ŧ ≈ U ≈
20 X X X X X 2020 X X X X X 2020 X X X X X 20--- --- --- --- --- --- ---20 X X X X X 20
20 X X X X X 2020 X X X Þ X Þ X 2020 X X X X X 20--- --- --- --- --- --- ------ --- --- --- --- --- ---20 X X X X X 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 X X X : X : X 20--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---20 X X X X X 20--- --- --- --- --- --- --- --- --- --- --- --- --- ---20 X X X X X 20
20 X X X X X 2020 X X X X X 20
--- --- --- --- --- X 2020 X X X X X 20
20^ X^ X^ X^ X^ X^ 20^
20 X X 20 20 X 20
20 X 20 20 20 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 X // // // // 20
30 20 X 20 20 50 5030 20 X 20 20 50 5030 20 20 30 30 50 5030 20 20 30 30 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 20 X --- --- X X30 20 X --- --- X X30 20 --- --- --- X X30 20 X --- --- X X30 20 X --- --- X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 20 X 20 20 X X30 20 --- --- --- X X30 20 X --- --- X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---30 20 --- --- --- X X--- --- --- --- --- --- ---30 20 X 20 20 X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DF09 DF10 DF11 DF12 DF13 DF14 DF151000 1000
ċ ŧ ≈ U ≈
30 20 X --- --- X X30 20 X 50 20 X X30 20 X 50 20 X X30 20 X 50 20 X X30 20 X 50 20 X X30 20 --- 50 20 --- X30 20 X 50 20 X X30 20 --- --- --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---30 20 X --- --- X X30 20 --- --- --- --- X30 20 X --- --- X X--- --- --- --- --- --- ---30 20 X 50 20 X X
X 20 --- --- --- 50 50X 20 50 20 20 50 50
1000 1000X 20 X --- --- 50 50X 20 X --- 40 50 50X 20 X --- 40 50 50X 20 X --- --- 50 50X 20 X 40 40 50 50--- --- --- --- --- --- ---X 20 X --- 40 50 50X 20 X --- 40 50 50X 20 X --- --- 50 5050 20 --- 40 40 50 5050 20 --- 40 40 50 50--- --- --- --- --- --- ---X 20 X --- --- 50 50X 20 X --- --- 50 50
--- --- --- --- --- --- ---30 X 20 30 20 50 5030 X 20 30 20 50 50
1000 --- 1000 --- --- --- 1000--- --- --- --- --- --- ---X --- 50 --- --- 50 50X 20 50 --- --- 50 50X --- 50 --- --- 50 50X --- 50 --- --- 50 50X 20 50 --- --- 50 50X --- 50 --- --- 50 50X --- 50 --- --- 50 50X --- 50 --- --- 50 50X --- 50 --- --- 50 50--- --- --- --- --- --- ------ --- --- --- --- 50 ---X --- 50 --- --- 50 50X 20 50 20 20 50 50
--- --- --- --- --- 50 ---X 20 50 --- --- 50 50
1000 1000 1000--- --- --- --- --- --- ---57 --- --- --- --- 50 5050 --- --- 20 20 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DF09 DF10 DF11 DF12 DF13 DF14 DF151000 1000
ċ ŧ ≈ U ≈
50 --- --- 20 20 50 5057 --- --- --- --- 50 5050 --- --- --- --- 50 5050 --- --- 20 20 50 5057 --- --- --- --- 50 5050 --- --- --- --- 50 5057 --- --- --- --- 50 5050 --- --- --- --- 50 5050 --- --- --- --- 50 5057 --- --- --- --- 50 5050 --- --- --- --- 50 50 --- --- --- --- --- --- ---50 20 --- --- 40 50 5050 --- --- --- --- 50 5050 20 --- --- --- 50 5050 20 --- --- 40 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ---50 20 --- --- --- 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 20 X 40 40 50 5050 --- --- --- --- 50 5057 --- --- --- --- 50 50--- --- --- --- --- --- ---50 --- --- --- --- 50 5057 --- --- --- --- 50 50--- --- --- --- --- --- ---50 --- --- --- --- 50 5050 --- --- --- --- 50 5057 --- --- --- --- 50 5057 --- --- --- --- 50 5050 --- --- --- --- 50 5050 --- --- --- --- 50 5057 --- --- --- --- 50 5057 --- --- --- --- 50 5057 --- --- --- --- 50 5050 --- --- --- --- 50 5050 --- --- --- --- 50 5057 --- --- --- --- 50 5050 --- --- --- --- 50 5050 --- --- --- --- 50 5057 --- --- --- --- 50 5050 20 --- --- --- 50 5050 20 --- --- --- 50 5057 --- --- --- --- 50 5057 --- --- --- --- 50 5050 20 --- --- --- 50 5050 20 --- --- --- 50 50--- --- --- --- --- --- ---57 --- --- --- --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- --- --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- --- --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---57 --- --- --- --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---57 --- --- --- --- 50 5050 20 --- --- --- 50 5050 20 --- --- --- 50 50--- --- --- --- --- --- ---50 --- --- --- --- 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DF09 DF10 DF11 DF12 DF13 DF14 DF151000 1000
ċ ŧ ≈ U ≈
57 --- --- --- --- 50 5050 --- --- --- --- 50 5057 --- --- --- --- 50 50--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- --- --- 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 20 20 30 20 50 5030 20 20 30 20 50 50--- --- --- --- --- --- ---30 20 20 30 20 50 50--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 20 20 --- --- --- 5030 --- --- --- --- --- 50--- --- --- --- --- --- ---30 20 20 --- --- 50 50--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 --- --- --- --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- 30 20 --- ------ --- --- --- --- --- ---30 20 20 --- --- 50 5030 20 20 30 20 50 50
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X --- --- 20 20 X X
--- --- --- --- --- --- ---X X X --- --- X XX X X 20 20 X XX X X 20 20 X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X --- --- --- --- --- X--- --- --- --- --- --- ---X X X 20 20 X X
Ə1 Ə *µ Ə1 --- --- --- Ə1X 50 X --- --- --- 50--- --- --- --- --- --- ---
1000 1500 1000 --- --- --- 1000--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DF16 DF17 DF18 DF19 DF20 DF21 DF221000 1000 1000 1000
¶ ≈ Æ ≈ ê ê ≈
X X X X X 30 XX X X X X 30 XX X X X X 30 X--- --- --- --- --- --- ---X X --- --- X --- X
X X X X X 30 XX X X X X 30 XX X X X X --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X 30 X--- --- --- --- --- --- ------ --- --- --- --- 30 X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X 30 X--- --- --- --- --- 30 X
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X 30 X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X 30 X
X X X X X 30 XX X X X X 30 X
X --- --- --- X --- XX X X X X 30 X--- X^ X^ X^ X^ 30^ ---
X X X X X 30 X
30 20 20 20 20 --- 30--- --- --- --- --- --- 30--- --- --- --- --- --- 30--- --- --- --- --- --- 30// // // // // 30 //
30 X X X X --- 3030 X X X X --- 3030 30 30 30 30 --- 3030 30 30 30 30 --- 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 30 X X X --- ---30 30 X X X --- ---30 30 --- X X --- ---30 30 X X X --- ---30 30 X X X --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 X X X X --- 3030 30 --- X X --- ---30 30 X X X --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 30 --- X X --- ------ --- --- --- --- --- ---30 30 X X X --- 30
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DF16 DF17 DF18 DF19 DF20 DF21 DF221000 1000 1000 1000
¶ ≈ Æ ≈ ê ê ≈
30 X X X X --- ---30 X X X X --- ---30 X X X X --- ---30 X X X X --- ---30 X X X X --- ---30 X --- --- X --- ---30 X X X X --- ---30 X --- --- X --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 X X X X --- ---30 X --- --- X --- ---30 X X X X --- ------ --- --- --- --- --- ---30 X X X X --- ---
50 X --- --- X --- ---50 X --- --- X --- ---
30 50 X X X --- ---30 50 X X X --- ---30 50 X X X --- ---30 50 X X X --- ---30 50 X X X --- ------ --- --- --- --- --- ---30 50 X X X --- ---30 50 X X X --- ---30 50 X X X --- ---30 50 --- 50 50 --- ---30 50 --- 50 50 --- ------ --- --- --- --- --- ---30 30 X X X --- ---30 30 X X X --- ---
--- --- --- --- --- --- ---30 X X X X --- ---30 X X X X --- ---
1000 800 --- --- 1000 --- ------ --- --- --- --- --- ---50 X --- --- X --- ---50 X --- --- X --- ---50 X --- --- X --- ---50 X --- --- X --- ---50 X --- --- X --- ---50 X --- --- X --- ---50 X --- --- X --- ---50 X --- --- X --- ---50 X --- --- X --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 X --- --- X --- ---50 X --- --- X --- --- --- --- --- --- --- --- ---50 X --- --- X --- ---
--- --- --- --- --- --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DF16 DF17 DF18 DF19 DF20 DF21 DF221000 1000 1000 1000
¶ ≈ Æ ≈ ê ê ≈
50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- --- --- --- --- --- --- --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 --- 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 X 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ------ --- --- --- --- --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ------ --- --- --- --- --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ------ --- --- --- --- --- ---50 50 --- 50 50 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ------ --- --- --- --- --- ---50 50 --- 50 50 --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DF16 DF17 DF18 DF19 DF20 DF21 DF221000 1000 1000 1000
¶ ≈ Æ ≈ ê ê ≈
50 50 --- 50 50 --- ---50 50 --- 50 50 --- ---50 50 --- 50 50 --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 30 30 30 30 --- ---30 30 30 30 30 --- 30--- --- --- --- --- --- ---30 30 30 30 30 --- ------ --- --- --- --- --- 30--- --- --- --- --- --- 30 --- --- --- --- --- --- ---30 --- 30 --- 30 --- 3030 --- --- --- 30 --- ------ --- --- --- --- --- 3030 30 30 30 30 --- 30--- --- --- --- --- --- 30 --- --- --- --- --- --- ---50 50 --- 50 50 --- 30--- --- --- --- --- --- 30--- --- --- --- --- --- 30--- --- --- --- --- --- 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- 30--- --- --- --- --- --- 3030 30 30 30 30 --- 3030 30 30 30 30 --- 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- 30 --- --- --- --- --- --- --- --- X --- X X --- --- --- --- --- --- --- --- ---X X X X X --- ---X X X X X --- XX X X X X --- 30--- --- --- --- --- --- ------ --- --- --- --- --- ---X X --- --- X --- ------ --- --- --- --- --- ---X X X X X --- 30
--- --- --- --- Ə1 --- ------ --- --- --- 50 --- ------ --- --- --- --- --- ------ --- --- --- 1000 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DF23 DF24 DF25 DF26 DF27 DF28 DF301000 1000 1000 500 700 1333
U M ≈ M ≈ Қ ≈ ≈ ά ≈
X X X 30 20 X XX X X 30 20 X XX X X 30 20 X X--- --- --- --- --- --- ---X --- --- --- --- X X
X X X 30 20 X XX X X 30 20 X ⋆ X--- X X 30 20 --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X 30 20 X ϫ X--- --- --- --- --- --- ---X --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X 30 20 X X
XÐ --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- X X 30 20 X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X 30 20 X X
X X X 30 20 X XX X X 30 20 X X
--- X X X X X ---X X X 30 20 X X
--- X^ X^ 30^ 20^ X^ X^
X X X --- 20 20 X
30 X X 30 20 20 2030 --- --- --- --- --- ---30 --- --- --- --- --- ---30 --- --- --- --- --- ---// X X 30 20 // //
30 25 30 30 X 20 3030 25 30 30 X 20 30 --- 25 30 30 30 30 30 --- 25 30 30 30 30 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- 25 30 30 X --- 3030 25 30 30 X --- 3030 25 30 --- X --- 30 --- 25 30 30 X --- 3030 25 30 30 X --- 30--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 25 30 30 X 20 3030 25 30 --- X --- 3030 25 30 30 X --- 30--- --- --- --- --- --- ------ --- --- --- --- --- ---30 25 30 --- X --- 30--- --- --- --- --- --- ---30 25 30 30 X 20 30
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DF23 DF24 DF25 DF26 DF27 DF28 DF301000 1000 1000 500 700 1333
U M ≈ M ≈ Қ ≈ ≈ ά ≈
50 25 30 30 X --- X--- 25 30 30 X 20 X50 25 30 30 X 20 X50 25 30 30 X 20 X50 25 30 30 X 20 X50 --- --- --- --- 20 X50 25 30 30 X 20 X50 --- --- --- --- --- X50 --- --- --- --- --- ------ --- --- --- --- --- ---50 25 30 30 X --- X--- --- --- --- --- --- X50 25 30 30 X --- X50 --- --- --- --- --- ---50 25 30 30 X 20 X
--- --- --- --- --- --- X50 --- --- --- --- 20 X
50 25 30 30 X --- X50 25 30 30 X 40 X50 25 30 30 X 40 X50 25 30 30 X --- X50 25 30 30 X 40 X50 --- --- --- --- --- ---50 25 30 30 X 40 X50 25 30 30 X 40 X50 25 30 30 X --- X--- 25 30 --- 50 40 5050 25 30 --- 50 40 5050 --- --- --- --- --- ---50 25 30 30 X --- X--- 25 30 --- X --- X
--- --- --- --- --- --- ---30 25 30 30 X 20 X30 25 30 30 X 20 X
--- --- --- --- --- --- 1000--- --- --- --- --- --- ---50 --- --- --- --- --- X50 --- --- --- --- --- X--- --- --- --- --- --- X--- --- --- --- --- --- X50 --- --- --- --- --- X--- --- --- --- --- --- X--- --- --- --- --- --- X--- --- --- --- --- --- X--- --- --- --- --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- X50 --- --- --- --- 20 X --- --- --- --- --- --- ---50 --- --- --- --- --- X
--- --- --- --- --- --- ------ 25 50 30 50 --- 5050 25 50 30 50 --- 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DF23 DF24 DF25 DF26 DF27 DF28 DF301000 1000 1000 500 700 1333
U M ≈ M ≈ Қ ≈ ≈ ά ≈
50 25 50 30 50 20 50--- 25 50 30 50 20 5050 25 50 30 50 --- 5050 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- 25 50 30 50 --- 5050 25 50 30 50 --- 5050 25 50 30 50 --- 50--- 25 50 30 50 --- 5050 25 50 30 50 20 » 50--- --- --- --- --- --- ---50 25 50 30 50 40 5050 25 50 30 50 --- 5050 25 50 30 50 --- 5050 25 50 30 50 40 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ---50 25 50 30 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 25 50 30 50 40 50--- 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- --- --- --- --- --- ------ 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- --- --- --- --- --- ------ 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- 25 50 30 50 --- 5050 25 50 30 50 --- 5050 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- 25 50 30 50 --- 5050 25 50 30 50 --- 5050 25 50 30 50 --- 50--- --- --- --- --- --- ------ 25 50 30 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 25 50 30 50 --- 50--- --- --- --- --- --- ---50 --- --- --- --- --- ------ 25 50 30 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ 25 50 30 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ 25 50 30 50 --- 5050 25 50 30 50 --- 5050 25 50 30 50 --- 50--- --- --- --- --- --- ------ 25 50 30 50 --- 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DF23 DF24 DF25 DF26 DF27 DF28 DF301000 1000 1000 500 700 1333
U M ≈ M ≈ Қ ≈ ≈ ά ≈
--- 25 50 30 50 --- 5050 25 50 30 50 --- 50--- 25 50 30 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 25 50 30 50 --- 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---50 --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 25 30 30 30 20 3030 25 30 30 30 20 30--- --- --- --- --- --- ---30 25 30 30 30 20 3030 --- --- --- --- --- ---30 --- --- --- --- --- --- --- --- --- --- --- --- ---30 --- --- --- --- --- 30--- --- --- --- --- --- 3030 --- --- --- --- --- ---30 25 30 30 30 --- 3030 --- --- --- --- --- --- --- --- --- --- --- --- ---30 25 30 30 50 --- 5030 --- --- --- --- --- ---30 --- --- --- --- --- ---30 --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---30 --- --- --- --- --- ---30 25 30 30 30 --- 3030 25 30 30 30 20 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 --- --- --- --- --- --- --- --- --- --- --- --- --- --- X X 30 X 20 X --- --- --- --- --- --- --- --- X X 30 X --- X30 X X 30 X 20 X30 X X 30 X 20 X --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- X --- --- --- --- --- --- ---30 X X 30 X 20 X
Ə1 --- --- --- --- Ə150 --- --- --- --- --- 50--- --- --- --- --- --- ---
1500 --- --- --- --- --- 1000--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DF31 DF33 DF34 DF36 DF37 DF38 DF39750 1000 1750 1000 1500 1000 U r ε ≈ Ñ ≈ ≈
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X XX X X X X X X--- --- X --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- X --- --- --- ------ --- X --- --- --- ------ --- X --- --- --- ---X X X X X X X--- --- X --- --- --- ---
--- --- X --- --- --- --- --- --- X --- --- --- ---X X X X X X X--- --- X --- --- --- ------ --- X --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
--- --- --- X --- --- XX X X X X X X
X^ X^ X X^ X^ X^ X^
X X X X X X X
X 20 X 20 30 X X--- --- X --- --- --- ------ --- X --- --- --- ------ --- X --- --- --- ---X // X // // X X
rX X X 20 30 20 XX X X X X 20 XX 30 X X 30 20 30X 30 X X 30 20 30
--- --- X --- --- --- --- --- --- X --- --- --- --- --- --- X --- --- --- --- --- --- X --- --- --- ---X X X X X 20 XX X X X X 20 XX X X X X 20 XX X X X X 20 XX X X X X 20 X
--- --- X --- --- --- --- --- --- X --- --- --- --- --- --- X --- --- --- ---X X X X X 20 XX X X X X 20 XX X X X X 20 X
--- --- X --- --- --- --- --- --- X --- --- --- ---X X X X X 20 X--- --- --- --- --- --- ---X X X X X 20 X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DF31 DF33 DF34 DF36 DF37 DF38 DF39750 1000 1750 1000 1500 1000 U r ε ≈ Ñ ≈ ≈
X 30 X 40 30 20 30X 30 X 40 30 20 30X 30 X 40 30 20 30X 30 X 40 30 20 30X 30 X 40 30 20 30X 30 X 40 --- 20 30X 30 X 40 30 20 30X 30 X 40 --- 20 30
--- --- X --- --- --- ------ --- --- --- --- --- ---X 30 X 40 30 20 30X 30 X 40 --- 20 30X 30 X 40 30 20 30
--- --- X --- --- --- ---X 30 X 40 30 20 30
rX X X 50 30 20 30X X X 50 30 20 30
r
X X X X 50 X XX X X X 50 X XX X X X 50 X XX X X X 50 X XX X X X 50 X X
--- --- X --- --- --- ---X X X X 50 X XX X X X 50 X XX X X X 50 X XX 50 X 50 50 50 50X 50 X 50 50 50 50
--- --- X --- --- --- ---X X X X 50 X XX X X X 50 X X
--- --- --- --- --- --- ---X X X X 30 20 XX X X X 30 20 X
r Ñ800 --- --- 1750 --- ------ --- --- --- --- --- ------ X X 50 30 20 30X X X 50 30 20 30--- X X 50 30 20 30--- X X 50 30 20 30X X X 50 30 20 30--- X X 50 30 20 30--- X X 50 30 20 30--- X X 50 30 20 30--- X X 50 30 20 30--- --- --- --- --- --- ------ --- X --- 30 --- ------ X X 50 30 20 30X X X 50 30 20 30--- --- X --- 30 --- ---X X X 50 30 20 30
@ r
--- --- X --- --- --- ------ 50 X 40 50 50 50--- 50 X 40 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DF31 DF33 DF34 DF36 DF37 DF38 DF39750 1000 1750 1000 1500 1000 U r ε ≈ Ñ ≈ ≈
--- 50 X 40 50 50 50--- 50 X 40 50 50 50--- 50 X 40 50 50 50--- 50 X 40 50 50 50--- 50 X 40 50 50 50--- 50 X 40 50 50 50--- 50 X 40 50 50 50--- 50 X 40 50 50 50--- 50 X 40 50 50 50--- 50 X 40 50 50 50--- 50 X 40 50 50 50 --- --- X --- --- --- ---X 50 X 40 50 50 50--- 50 X 40 50 50 50X 50 X 40 50 50 50X 50 X 40 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ---X 50 X 40 50 50 50--- --- X --- --- --- --- --- --- X --- --- --- --- --- --- X --- --- --- ---X 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- --- X --- --- 50 --- --- 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- --- X --- --- 50 --- --- 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- 50 X 40 50 50 50X 50 X 40 50 50 50X 50 X 40 50 50 50--- 50 X 40 50 50 50--- 50 X 40 50 50 50X 50 X 40 50 50 50X 50 X 40 50 50 50--- --- X --- --- --- --- --- 50 X 40 50 50 50--- --- X --- --- --- ------ --- X --- --- --- --- --- 50 X 40 50 50 50--- --- X --- --- --- ------ --- X --- --- --- ------ 50 X 40 50 50 50--- --- X --- --- --- ------ --- X --- --- --- ------ --- X --- --- --- --- --- 50 X 40 50 50 50--- --- X --- --- --- ------ --- X --- --- --- --- --- 50 X 40 50 50 50X 50 X 40 50 50 50X 50 X 40 50 50 50 --- --- X --- --- --- --- --- 50 X 40 50 50 50--- --- X --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DF31 DF33 DF34 DF36 DF37 DF38 DF39750 1000 1750 1000 1500 1000 U r ε ≈ Ñ ≈ ≈
--- 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- 50 X 40 50 50 50 --- --- X --- --- --- --- --- --- X --- --- --- --- --- --- X --- --- --- --- --- 50 X 40 50 50 50
--- --- X --- --- --- --- --- --- X --- --- --- --- --- --- X --- --- --- --- --- --- X --- --- --- ---
--- --- X --- --- --- ---
X 30 X 20 30 20 30X 30 X 20 30 20 30--- --- --- --- --- --- ---X 30 X 20 30 20 30--- --- X --- --- --- ------ --- X --- --- --- ------ --- X --- --- --- ---X 30 X 20 --- 20 30--- 30 X 20 --- 20 30--- --- X --- --- --- ---X 30 X 20 30 20 30--- --- X --- --- --- ------ --- X --- --- --- ------ 50 X 40 50 50 50--- --- X --- --- --- ------ --- X --- --- --- ------ --- X --- --- 20 ------ --- X --- --- --- ------ --- X --- --- --- ------ --- X --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- X --- --- --- ------ --- X --- --- 20 ------ --- X --- --- --- ---X 30 X 20 30 20 30X 30 X 20 30 20 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- X --- --- --- ------ --- X --- --- --- ------ X X X X X X--- --- X --- --- --- ---X X X X X X XX X X X X X XX X X X X X X--- --- X --- --- --- ------ --- --- --- --- --- ------ X X X --- X X--- --- X --- --- --- ---X X X X X X X
--- Ə1 ф r Ə Ə1 --- Ə Ə
--- X X 50 --- 50 50--- --- --- --- --- --- ------ 1000 2000 1750 --- 1500 1000--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DF40 DF41 DF42 DF43 DF44 DF45 DF461500 1500 500 Ñ ≈ Ñ ≈ Қ ≈
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X • X • X X X ÞX X --- --- X X ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
--- --- --- --- X --- ---X X X X X X X
X^ X^ X X X^ X^ X^
X X X X X X X
X X X X X 20 X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X --- --- --- --- ---X X X X X // X
X X X X 20 20 30X X X X 20 20 30X X X X 20 20 30X X X X 20 20 30
--- --- --- --- --- --- --- --- --- --- --- 20 --- --- --- --- --- --- 20 --- --- --- --- --- --- 20 --- ---X X X X 20 20 ---X X X X 20 20 ---X X --- --- 20 20 ---X X X X 20 20 ---X X --- --- 20 20 ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 20 20 30X X --- --- 20 20 ---X X --- --- 20 20 ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X --- --- 20 20 ------ --- --- --- --- --- ---X X X X 20 20 30
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DF40 DF41 DF42 DF43 DF44 DF45 DF461500 1500 500 Ñ ≈ Ñ ≈ Қ ≈
X X X X 20 20 ---X X X X 20 20 30X X X --- 20 20 30X X --- --- 20 20 30X X X X 20 20 30X X X --- 20 20 30X X X X 20 20 30X X --- --- 20 20 ---
--- --- --- --- --- --- ------ --- --- --- --- --- ---X X --- --- 20 20 ---X X --- --- 20 20 ---X X --- --- 20 20 ---
--- --- --- --- --- --- ---X X X X 20 20 30
X X --- --- 20 20 ---X X --- --- 20 20 30
---
X X X X 50 20 ---X X X X 50 20 ---X X X X 50 20 ---X X X X 50 20 ---X X X X 50 20 ---
--- --- --- --- --- --- ---X X --- --- 50 20 ---X X --- --- 50 20 ---X X --- --- 50 20 ---X X X X 50 20 ---X X --- --- 50 20 ---
--- --- --- --- --- --- ---X X --- --- 50 20 ---X X X X 50 20 ---
--- --- --- --- --- --- ---X X X X 20 20 30X X X X 20 20 30
™ ™ Ñ800 800 500 500 --- --- ------ --- --- --- --- 50 ------ --- --- --- 20 20 ---X X --- --- 20 20 ------ --- --- --- 20 20 ------ --- --- --- 20 20 ---X X X X 20 20 ------ --- --- --- 20 20 ------ --- --- --- 20 20 ------ --- --- --- 20 20 ------ --- --- --- 20 20 ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- 20 20 ---X X --- --- 20 20 30--- --- --- --- --- --- ---X X --- --- 20 20 ---
@ @ 500 500 ---
--- --- --- --- --- --- ------ --- --- --- 50 50 ------ --- --- --- 50 50 ---
January 01, 2016
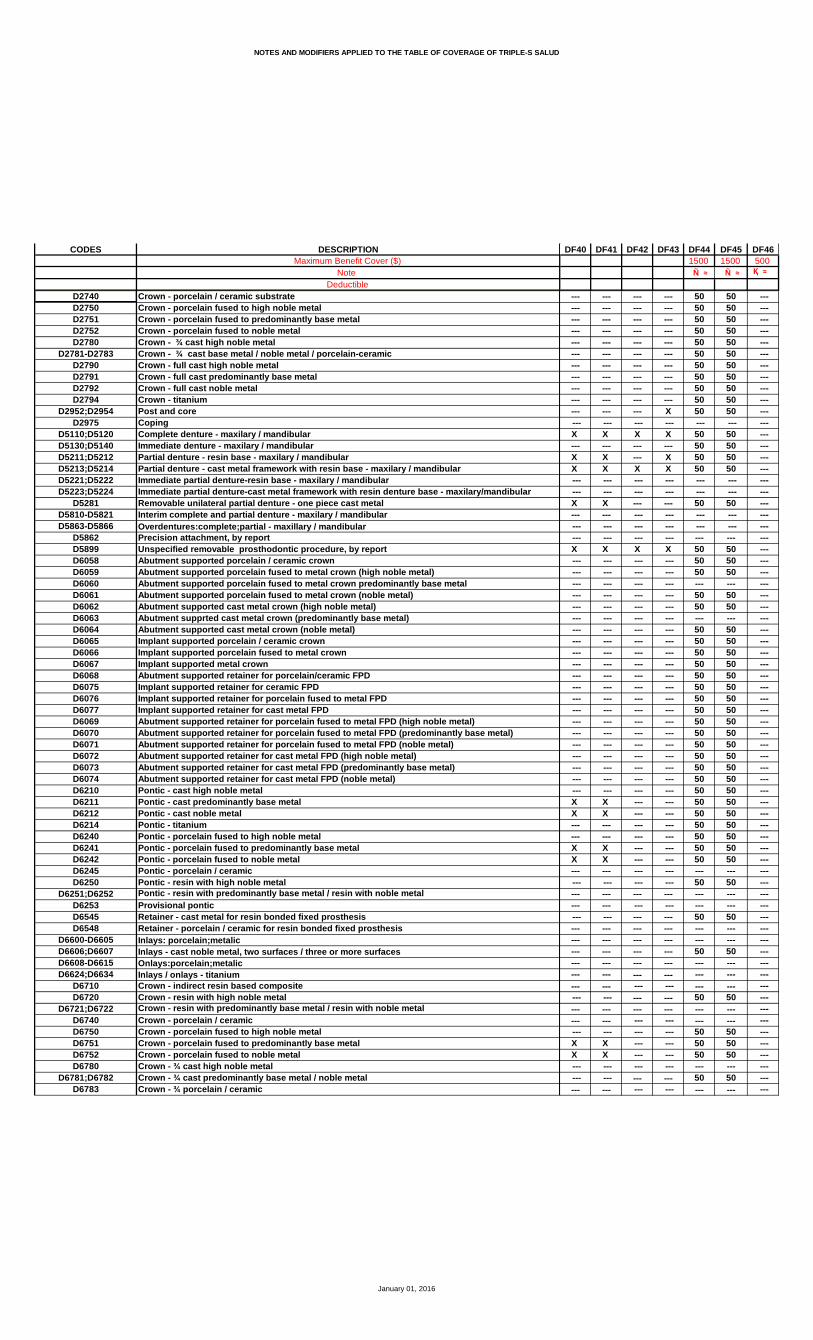
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DF40 DF41 DF42 DF43 DF44 DF45 DF461500 1500 500 Ñ ≈ Ñ ≈ Қ ≈
--- --- --- --- 50 50 ------ --- --- --- 50 50 ------ --- --- --- 50 50 ------ --- --- --- 50 50 ------ --- --- --- 50 50 ------ --- --- --- 50 50 ------ --- --- --- 50 50 ------ --- --- --- 50 50 ------ --- --- --- 50 50 ------ --- --- --- 50 50 ------ --- --- X 50 50 --- --- --- --- --- --- --- ---X X X X 50 50 ------ --- --- --- 50 50 ---X X --- X 50 50 ---X X X X 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---X X --- --- 50 50 ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- --- --- --- --- --- --- --- 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- --- --- --- --- --- --- --- 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- 50 50 ---X X --- --- 50 50 ---X X --- --- 50 50 ------ --- --- --- 50 50 ------ --- --- --- 50 50 ---X X --- --- 50 50 ---X X --- --- 50 50 ------ --- --- --- --- --- --- --- --- --- --- 50 50 ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- 50 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- 50 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- 50 50 ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- 50 50 ---X X --- --- 50 50 ---X X --- --- 50 50 --- --- --- --- --- --- --- --- --- --- --- --- 50 50 ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DF40 DF41 DF42 DF43 DF44 DF45 DF461500 1500 500 Ñ ≈ Ñ ≈ Қ ≈
--- --- --- --- 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
X X X X 20 20 30X X X X 20 20 30--- --- --- --- --- --- ---X X X X 20 20 30--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- X X 20 20 ------ --- --- --- 20 20 ------ --- --- --- --- --- ---X X X X 20 20 ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- 50 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- 30--- --- --- --- --- --- ---X X --- --- 20 20 ---X X X X 20 20 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- X X 30--- --- --- --- --- --- ---X X X X X X ---X X X X X X 30X X X X X X 30--- --- --- --- 20 --- ------ --- --- --- --- --- ------ --- --- --- X X ------ --- --- --- --- --- ---X X --- --- X X 30
--- --- --- --- Ə1 * Ə1 ------ --- --- --- 50 20 ------ --- --- --- --- --- ------ --- --- --- 1500 1500 ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DF47 DF48 DF49 DF50 DF51 DF52 DF54500 1000 1000
ċ Қ ≈ U ≈ Æ ≈
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X --- X X X X
X X X X X X XX Þ X Þ X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
--- --- X --- --- X XX X X X X X X
X^ X^ X^ X^ X^ X^ X^
20 20 X X X X X
20 20 30 X 30 X 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// // // X // X //
20 20 X 20 25 30 X20 20 X 20 25 30 X30 30 30 20 25 30 3030 30 30 20 25 30 30 --- --- --- --- --- --- --- --- --- --- 20 --- --- ------ --- --- 20 --- --- --- --- --- --- 20 --- --- --- --- --- X 20 25 X X --- --- X 20 25 X X --- --- X 20 25 X X --- --- X 20 25 X X --- --- X 20 25 X X --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 X 20 25 X X --- --- X 20 25 X X --- --- X 20 25 X X--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- X 20 25 X X--- --- --- --- --- --- ---20 20 X 20 25 X X
January 01, 2016
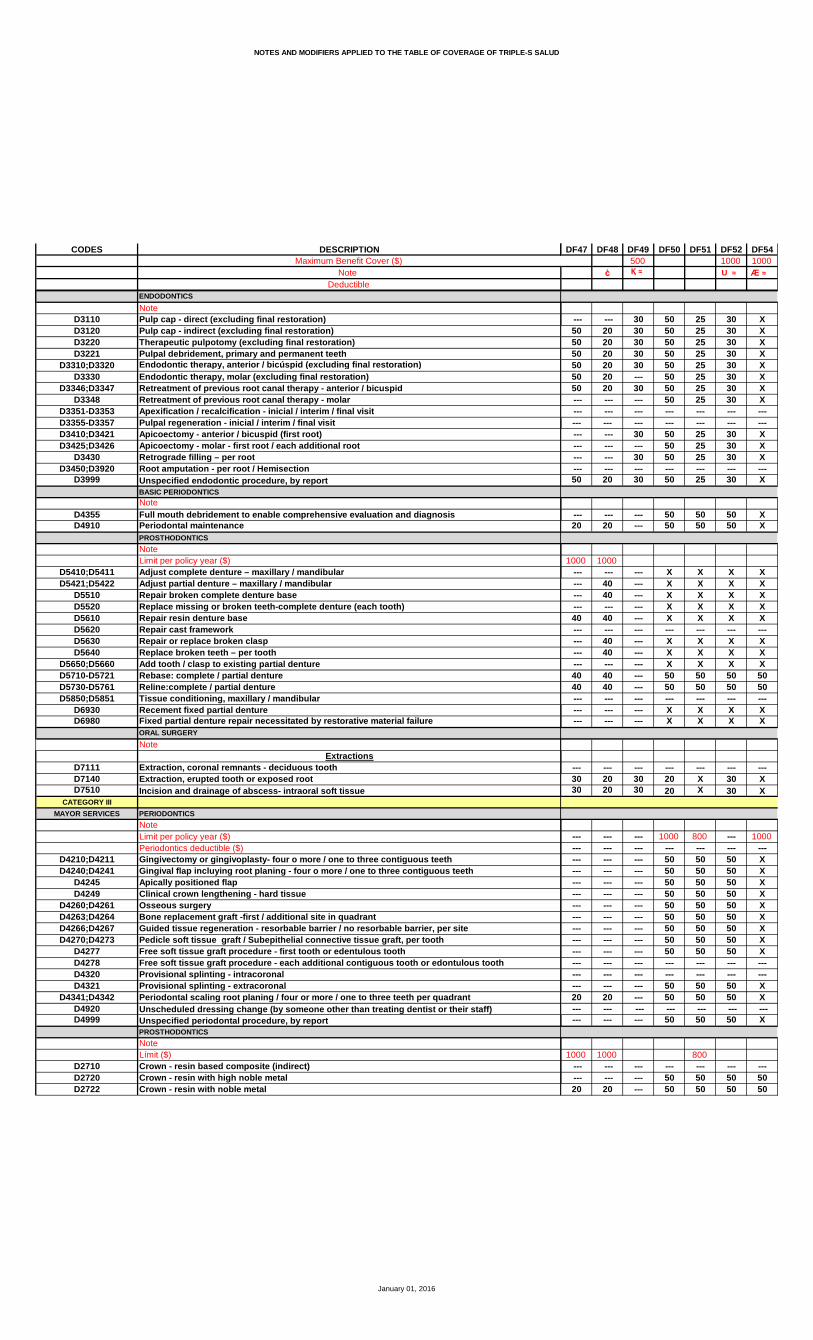
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DF47 DF48 DF49 DF50 DF51 DF52 DF54500 1000 1000
ċ Қ ≈ U ≈ Æ ≈
--- --- 30 50 25 30 X50 20 30 50 25 30 X50 20 30 50 25 30 X50 20 30 50 25 30 X50 20 30 50 25 30 X50 20 --- 50 25 30 X50 20 30 50 25 30 X --- --- --- 50 25 30 X --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- 30 50 25 30 X --- --- --- 50 25 30 X --- --- 30 50 25 30 X --- --- --- --- --- --- ---50 20 30 50 25 30 X
--- --- --- 50 50 50 X20 20 --- 50 50 50 X
1000 1000 --- --- --- X X X X --- 40 --- X X X X --- 40 --- X X X X --- --- --- X X X X40 40 --- X X X X --- --- --- --- --- --- --- --- 40 --- X X X X --- 40 --- X X X X --- --- --- X X X X40 40 --- 50 50 50 5040 40 --- 50 50 50 50 --- --- --- --- --- --- --- --- --- --- X X X X --- --- --- X X X X
--- --- --- --- --- --- ---30 20 30 20 X 30 X30 20 30 20 X 30 X
--- --- --- 1000 800 --- 1000--- --- --- --- --- --- ------ --- --- 50 50 50 X--- --- --- 50 50 50 X--- --- --- 50 50 50 X--- --- --- 50 50 50 X--- --- --- 50 50 50 X--- --- --- 50 50 50 X--- --- --- 50 50 50 X--- --- --- 50 50 50 X--- --- --- 50 50 50 X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- 50 50 50 X20 20 --- 50 50 50 X--- --- --- --- --- --- ------ --- --- 50 50 50 X
1000 1000 800 --- --- --- --- --- --- --- --- --- --- 50 50 50 5020 20 --- 50 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DF47 DF48 DF49 DF50 DF51 DF52 DF54500 1000 1000
ċ Қ ≈ U ≈ Æ ≈
20 20 --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 5020 20 --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- --- --- --- --- --- 40 --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- 40 --- 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---40 40 --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- --- --- --- --- --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- --- --- --- --- --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- --- --- --- --- --- --- --- 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- --- --- --- --- --- --- --- 50 50 50 50 --- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DF47 DF48 DF49 DF50 DF51 DF52 DF54500 1000 1000
ċ Қ ≈ U ≈ Æ ≈
--- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 20 30 20 30 30 3030 20 30 20 30 30 30--- --- --- --- --- --- ---30 20 30 20 30 30 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 20 30 30 30 --- --- --- 20 30 30 30 --- --- --- --- --- --- --- --- --- 30 20 30 30 30 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---30 20 --- --- --- --- ------ --- --- --- --- --- --- --- --- --- 20 30 30 3030 20 30 20 30 30 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 X X X X X --- --- --- --- --- --- --- --- --- X X X X X20 20 X X X X X20 20 X X X X X --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- X X X X --- --- --- --- --- --- ---20 20 X X X X X
--- --- --- * Ə1 Ə1 Ə1 Ə1 --- --- --- X 50 X X--- --- --- --- --- --- ------ --- --- 1000 --- 1000 1000--- --- --- --- 1500 --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DF55 DF56 DF57 DF58 DF59 DF60500 850 1000
Қ ≈ ß ≈ U ≈ ċ
20 10 X X X X20 10 X X X X20 10 X X X X--- --- --- --- --- ---20 10 X X X X
20 10 X X X X20 10 X X Þ X Þ X Þ--- --- --- --- X X--- --- --- --- --- ------ --- --- --- --- ---20 10 X X X X--- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- ---20 10 X X X X--- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- ---20 10 X X X X--- --- --- --- --- --- --- --- --- --- --- ---20 10 X X X X
20 10 X X X X20 10 X X X X
X X X --- --- ---20 10 X X X X20 10 X^ X^ X^ X^
20 10 X 30 X 20
20 10 X 30 X 20--- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ---20 10 X // X //
40 30 20 20 X 2040 30 20 20 X 2040 30 20 30 X 3040 30 20 30 X 30 --- --- --- --- --- --- --- 70 50 --- --- ------ 70 50 --- --- --- --- 70 50 --- --- --- --- --- --- --- X --- --- 30 20 --- X --- --- --- --- --- --- --- --- 30 20 --- X --- --- --- --- --- X --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---40 30 20 20 X 20 --- 30 20 --- --- --- --- 30 20 --- X ------ --- --- --- --- --- --- --- --- --- --- --- --- 30 20 --- --- ------ --- --- --- --- ---40 // // 20 X 20
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DF55 DF56 DF57 DF58 DF59 DF60500 850 1000
Қ ≈ ß ≈ U ≈ ċ
--- --- --- --- X ---40 70 50 50 X 2040 70 50 50 X 2040 70 50 50 X 2040 70 50 50 X 2040 70 50 50 X 2040 70 50 50 X 20 --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- X --- --- --- --- --- --- --- --- --- --- --- X --- --- --- --- --- --- ---40 70 50 50 X 20
--- --- --- --- --- --- --- 70 50 20 X 20
1000 1000 --- --- --- --- X --- --- 70 50 40 X 40 --- 70 50 40 X ê 40 --- --- --- --- X ê --- --- 70 50 40 X ê 40 --- --- --- --- --- --- --- 70 50 40 X 40 --- 70 50 40 X 40 --- --- --- --- X ê --- --- 70 50 40 X 40 --- 70 50 40 X 40 --- --- --- --- --- --- --- --- --- --- X ê --- --- --- --- --- X ê ---
--- --- --- --- --- ---40 30 20 20 X 2040 30 20 20 X 20
--- --- --- --- 800 ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- X ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- --- --- 70 50 20 X 20--- --- --- --- --- ------ --- --- --- --- ---
1000 --- --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- 20
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DF55 DF56 DF57 DF58 DF59 DF60500 850 1000
Қ ≈ ß ≈ U ≈ ċ
--- 70 50 --- --- 20 --- --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- 20 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- X 40 --- --- --- --- --- --- --- --- --- --- X --- --- 70 50 --- X 40 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- 70 50 --- X 40 --- 70 50 --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- 70 50 --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- 70 50 --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- 70 50 --- --- --- --- 70 50 --- --- --- --- 70 50 --- --- --- --- 70 50 --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DF55 DF56 DF57 DF58 DF59 DF60500 850 1000
Қ ≈ ß ≈ U ≈ ċ
--- --- --- --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- 70 50 --- --- ---
40 30 20 20 X 2040 30 20 20 X 20--- --- --- --- --- ---40 30 20 20 X 20--- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- X --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- X --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---40 30 20 --- --- 20--- --- --- --- --- --- --- --- --- --- X ---40 30 20 20 X 20
--- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---40 70 50 20 X 20 --- --- --- --- --- --- --- --- --- --- X ---40 30 20 20 X 2040 30 20 20 X 20 --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---40 // // 20 X 20
--- --- Ə1 --- --- --- --- --- X --- --- ------ --- --- --- --- ------ --- 1000 --- --- ------ --- --- --- --- ------ --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DF61 DF62 DF63 DF64 DF65 DF66 DF671000 1000
ċ U ≈ M ≈
X X X X X X 20X X X X X X 20X X X X X X 20--- --- --- --- --- --- ---X X X X X X 20
X X X X X X 20X Þ X Þ X Þ X X Þ X 20 Þ--- --- X X X --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X 20--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X 20--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X 20
X X X X X X 20X X X X X X 20
--- --- --- --- X --- XX X X X X X 20
X^ X^ X^ X^ X^ X^ 20
X X 20 X X 20 30
X X 20 20 20 20 30--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X // // // // ---
20 20 20 X 20 20 2020 20 20 X 20 20 2020 20 30 30 20 20 3020 20 30 30 20 20 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- X 20 --- ------ --- --- X 20 --- ------ --- --- X 20 --- ------ --- --- X 20 --- ---20 20 --- X 20 --- ---20 20 --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 20 20 X 20 20 20--- --- --- X 20 --- ------ --- --- X 20 --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- X 20 --- ------ --- --- --- --- --- ---20 20 20 X 20 20 20
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DF61 DF62 DF63 DF64 DF65 DF66 DF671000 1000
ċ U ≈ M ≈
--- --- --- X X --- ---20 20 20 X X 20 5020 20 20 X X 20 5020 20 20 X X 20 5020 20 20 X X 20 5020 20 20 X X 20 5020 20 20 X X 20 50--- --- --- X X --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- X X --- ------ --- --- X X --- ------ --- --- X X --- ------ --- --- --- --- --- ---20 20 20 X X 20 50
X X --- X X --- ---X X 20 X X 20 20
1000 1000--- --- --- X X --- ---40 40 40 X X 40 4040 40 40 X X 40 40--- --- --- X X --- ---40 40 40 X X 40 40--- --- --- --- --- --- ---40 --- 40 X X 40 4040 40 40 X X 40 40--- --- --- X X --- ---40 40 40 50 50 40 4040 40 40 50 50 40 40--- --- --- --- --- --- ------ --- --- X X --- ------ --- --- X X --- ---
--- --- --- --- --- --- ---20 20 20 X X 20 2020 20 20 X X 20 20
1000 1000 --- 1000 --- --- ------ --- --- --- --- --- ---X X --- X X --- ---X X --- X X --- ---X X --- X X --- ---X X --- X X --- ---X X --- X X --- ---X X --- X X --- ---X X --- X X --- ---X X --- X X --- ---X X --- X X --- ------ --- --- --- --- --- ---X X --- --- --- --- ---X X --- X X --- ---X X 20 X X 20 20X X --- --- --- --- ---X X --- X X --- ---
Œ Œ1000 1000 1000 1000
X X --- --- --- --- ---X X --- 50 50 --- ---X X 20 50 50 50 ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DF61 DF62 DF63 DF64 DF65 DF66 DF671000 1000
ċ U ≈ M ≈
X X 20 50 50 50 ---X X --- 50 50 --- ---X X --- 50 50 --- ---X X 20 50 50 50 ---X X --- 50 50 --- ---X X --- 50 50 --- ---X X --- 50 50 --- ---X X --- 50 50 --- ---X X --- 50 50 --- ---X X --- 50 50 --- ---
X« X« --- 50 50 --- ---X X --- --- --- --- ---X X 40 50 50 50 ---X X --- 50 50 --- ---X X --- 50 50 --- ---X X 40 50 50 50 ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X --- 50 50 --- ---X X --- --- --- --- ---X X --- --- --- --- ---X X --- --- --- --- ---X X 40 50 50 50 ------ --- --- 50 50 --- ------ --- --- 50 50 --- ------ --- --- --- --- --- ------ --- --- 50 50 --- ------ --- --- 50 50 --- ------ --- --- --- --- --- ------ --- --- 50 50 --- ------ --- --- 50 50 --- ------ --- --- 50 50 --- ------ --- --- 50 50 --- ------ --- --- 50 50 --- ------ --- --- 50 50 --- ------ --- --- 50 50 --- ------ --- --- 50 50 --- ------ --- --- 50 50 --- ------ --- --- 50 50 --- ------ --- --- 50 50 --- ------ --- --- 50 50 --- ------ --- --- 50 50 --- ------ --- --- 50 50 --- ---X X --- 50 50 --- ---X X --- 50 50 --- ---X X --- 50 50 --- ---X X --- 50 50 --- ---X X --- 50 50 --- ---X X --- 50 50 --- ---X X --- 50 50 --- ---X X --- --- --- --- ---X X --- 50 50 --- ---X X --- --- --- --- ---X X --- --- --- --- ---X X --- 50 50 --- ---X X --- --- --- --- ---X X --- --- --- --- ---X X --- 50 50 --- ---X X --- --- --- --- ---X X --- --- --- --- ---X X --- --- --- --- ---X X --- 50 50 --- ---X X --- --- --- --- ---X X --- --- --- --- ---X X --- 50 50 --- ---X X --- 50 50 --- ---X X --- 50 50 --- ---X X --- --- --- --- ---X X --- 50 50 --- ---X X --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DF61 DF62 DF63 DF64 DF65 DF66 DF671000 1000
ċ U ≈ M ≈
X X --- 50 50 --- ---X X --- 50 50 --- ---X X --- 50 50 --- ---X X --- --- --- --- ---X X --- --- --- --- ---X X --- --- --- --- ---X X --- 50 50 50 ---
X X --- --- --- --- ---X X --- --- --- --- ---X X --- --- --- --- ---X X --- --- --- --- ---
--- --- --- --- --- --- ---
20 20 20 30 30 20 2020 20 20 30 30 20 20--- --- --- --- --- --- ---20 20 20 30 30 20 20--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- 30 30 --- ------ --- --- 30 30 --- ------ --- --- --- --- --- ------ --- --- 30 30 --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- 50 50 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- 20 --- --- --- ------ --- --- --- --- --- ------ --- --- 30 30 --- ---20 20 20 30 30 20 20
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ 20 20 X X 20 20 --- --- --- --- --- --- ------ --- --- X X --- ---20 20 20 X X 20 2020 20 20 X X 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- X X --- ------ --- --- --- --- --- ---20 20 20 X X 20 20
Ə Ə --- Ə1 Ω Ə1 Ə1 ---X X --- 50 X X ------ --- --- --- --- --- ---
1000 1000 --- 1500 1000 1000 ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DF68 DF69 DF70 DF71 DF72 DF73 DF74500 500 850 1000
ċ m ċ ≈ Қ ≈ ß ≈ ŧ ≈
X X X 30 20 10 XX X X 30 20 10 XX X X 30 20 10 X--- --- --- --- --- --- ---X X X --- 20 10 X
X X X 30 20 10 XX Þ X Þ X Þ 30 20 10 XX --- --- 30 --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X 30 20 10 X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X 30 20 10 X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X 30 20 10 X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X 30 20 10 X
X X X 30 20 10 XX X X 30 20 10 X
--- --- --- X X X XX X X 30 20 10 X
X^ X^ X^ 30 20 10 X^
20 ± 20 20 --- 20 10 X
20 ± 20 20 30 20 10 X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// // // 30 20 10 X
20 ± 20 20 30 40 30 2020 ± 20 20 30 40 30 2030 ± 30 30 30 40 30 2030 ± 30 30 30 40 30 20 --- --- --- --- --- --- --- --- --- --- --- --- 70 50--- --- --- --- --- 70 50 --- --- --- --- --- 70 50 --- --- --- 30 --- --- --- --- --- --- 30 --- 30 20 --- --- --- --- --- --- --- --- --- --- 30 --- 30 20 --- --- --- 30 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
20 ± 20 20 30 40 30 20 --- --- --- --- --- 30 20 --- --- --- 30 --- 30 20--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 30 20--- --- --- --- --- --- ---
20 ± 20 20 30 40 // //
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DF68 DF69 DF70 DF71 DF72 DF73 DF74500 500 850 1000
ċ m ċ ≈ Қ ≈ ß ≈ ŧ ≈
--- --- --- 30 --- --- ---20 20 20 30 40 70 5020 20 20 30 40 70 5020 20 20 30 40 70 5020 20 20 30 40 70 5020 20 20 --- 40 70 5020 20 20 30 40 70 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- 30 --- --- --- --- --- --- --- --- --- --- --- --- --- 30 --- --- --- --- --- --- --- --- --- ---20 20 20 30 40 70 50
--- --- --- --- --- --- ---20 20 20 --- --- 70 50
Œ1000 1000 1000
--- --- --- 30 --- --- ---40 40 40 30 --- 70 5040 40 40 30 --- 70 50 --- --- --- 30 --- --- ---40 40 40 30 --- 70 50 --- --- --- --- --- --- ---40 40 40 30 --- 70 5040 40 40 30 --- 70 50 --- --- --- 30 --- --- ---40 40 40 --- --- 70 5040 40 40 --- --- 70 50 --- --- --- --- --- --- --- --- --- --- 30 --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---20 20 20 30 40 30 2020 20 20 30 40 30 20
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 20 20 --- --- 70 50--- --- --- --- --- --- ------ --- --- --- --- --- ---
Œ1000 1000 1000
--- --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 20 --- --- 70 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DF68 DF69 DF70 DF71 DF72 DF73 DF74500 500 850 1000
ċ m ċ ≈ Қ ≈ ß ≈ ŧ ≈
20 20 20 --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 20 --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---40 40 40 --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ---40 40 40 --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---40 40 40 30 --- 70 50 --- --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- --- 70 50 --- --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- --- 70 50 --- --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- --- 70 50 --- --- --- --- --- 70 50 --- --- --- --- --- 70 50 --- --- --- --- --- 70 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DF68 DF69 DF70 DF71 DF72 DF73 DF74500 500 850 1000
ċ m ċ ≈ Қ ≈ ß ≈ ŧ ≈
--- --- --- --- --- --- --- --- --- --- --- --- 70 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 70 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- 70 50
20 20 20 30 40 70 5020 20 20 30 40 70 50--- --- --- --- --- --- ---20 20 20 30 40 70 50--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 30 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 20 --- 40 70 50--- --- --- --- --- --- --- --- --- --- 30 --- --- ---20 20 20 30 40 70 50
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 20 30 40 70 50 --- --- --- --- --- --- --- --- --- --- 30 --- --- ---20 20 20 30 40 30 2020 20 20 30 40 30 20 --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 20 30 40 // //
--- --- --- --- --- --- Ə1 --- --- --- --- --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- 1000--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016
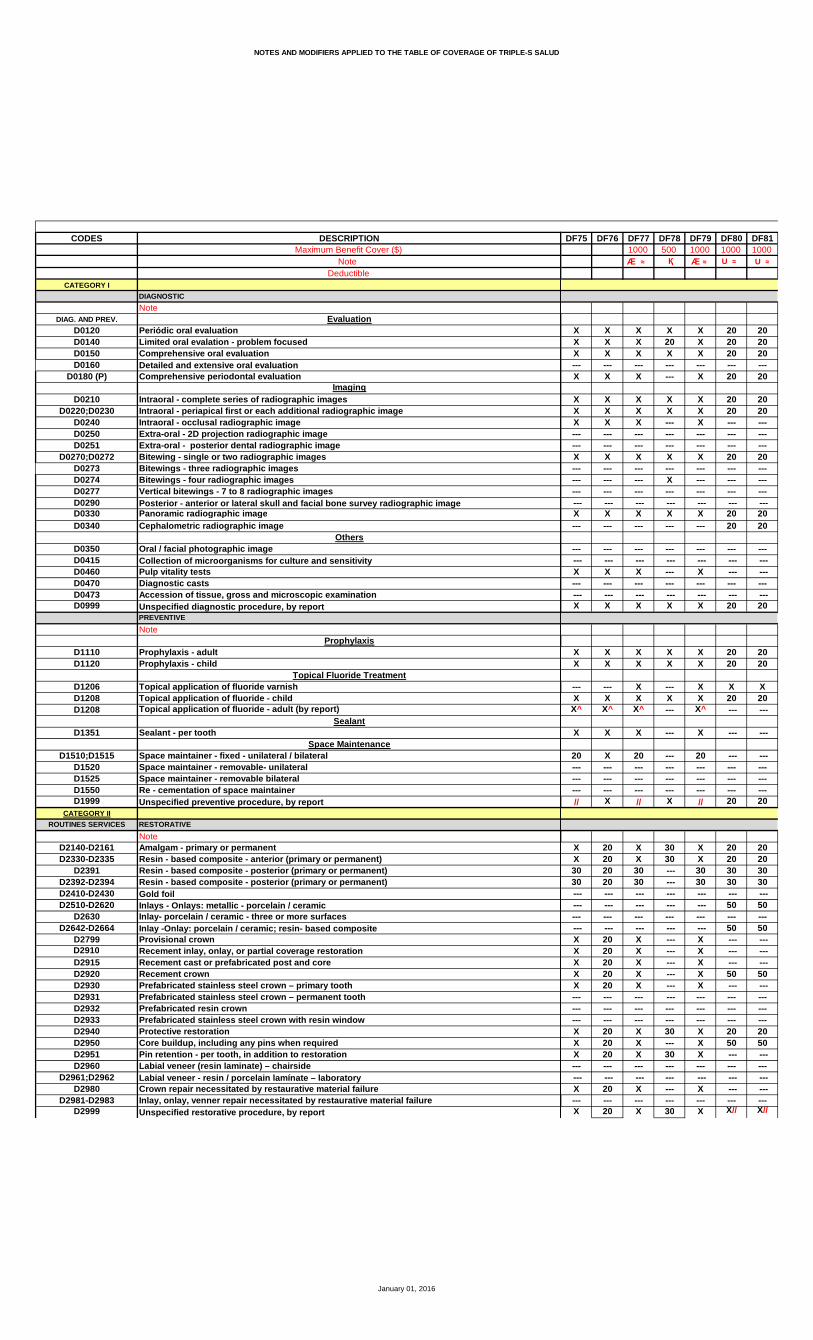
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DF75 DF76 DF77 DF78 DF79 DF80 DF811000 500 1000 1000 1000
Æ ≈ Қ Æ ≈ U ≈ U ≈
X X X X X 20 20X X X 20 X 20 20X X X X X 20 20--- --- --- --- --- --- ---X X X --- X 20 20
X X X X X 20 20X X X X X 20 20X X X --- X --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X 20 20--- --- --- --- --- --- ------ --- --- X --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X 20 20--- --- --- --- --- 20 20
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X --- X --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X 20 20
X X X X X 20 20X X X X X 20 20
--- --- X --- X X XX X X X X 20 20
X^ X^ X^ --- X^ --- ---
X X X --- X --- ---
20 X 20 --- 20 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// X // X // 20 20
X 20 X 30 X 20 20X 20 X 30 X 20 2030 20 30 --- 30 30 3030 20 30 --- 30 30 30 --- --- --- --- --- --- --- --- --- --- --- --- 50 50--- --- --- --- --- --- --- --- --- --- --- --- 50 50X 20 X --- X --- ---X 20 X --- X --- ---X 20 X --- X --- ---X 20 X --- X 50 50X 20 X --- X --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X 20 X 30 X 20 20X 20 X --- X 50 50X 20 X 30 X --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X 20 X --- X --- ------ --- --- --- --- --- ---X 20 X 30 X X// X//
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DF75 DF76 DF77 DF78 DF79 DF80 DF811000 500 1000 1000 1000
Æ ≈ Қ Æ ≈ U ≈ U ≈
X 20 X 30 X 50 50X 20 X 30 X 50 50X 20 X --- X 50 50X 20 X --- X 50 50X 20 X 30 X 50 50X 20 X --- X 50 50X 20 X --- X 50 50X 20 X --- X 50 50--- --- --- --- --- 50 50--- --- --- --- --- --- ---X 20 X --- X 50 50X 20 X --- X 50 50X 20 X --- X 50 50--- --- --- --- --- 50 50X 20 X 30 X 50 50
X 20 X --- X 50 50X 20 X --- X 50 50
X X X 50 X --- ---X X X 50 X --- ---X X X 50 X --- ---X X X 50 X --- ---X X X 50 X 20 20--- --- --- 50 --- 20 20X X X 50 X 20 20X X X 50 X 20 20X X X 50 X 20 2050 50 50 --- 50 --- ---50 50 50 50 ª 50 --- ------ --- --- 50 --- --- ---X X X --- X 50 50X X X --- X --- ---
--- --- --- --- --- --- ---X 20 X 30 X 20 20X 20 X 30 X 20 20
1000 800 1000 1000 --- ------ --- --- --- --- --- ---X 20 X --- X 50 50X 20 X --- X 50 50X 20 X --- X 50 50X 20 X --- X 50 50X 20 X --- X 50 50X 20 X --- X 50 50X 20 X --- X 50 50X 20 X --- X 50 50X 20 X --- X 50 50--- --- --- --- --- --- ------ --- --- --- --- 50 50X 20 X --- X 50 50X 20 X --- X 50 50
--- --- --- --- --- 50 50X 20 X --- X 50 50
800--- --- --- --- --- --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DF75 DF76 DF77 DF78 DF79 DF80 DF811000 500 1000 1000 1000
Æ ≈ Қ Æ ≈ U ≈ U ≈
50 50 50 --- 50 --- ---50 50 50 --- 50 50 5050 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 50 5050 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 50 50 --- --- --- --- --- --- ---50 50 50 50 50 50 5050 50 50 --- 50 50 5050 50 50 --- 50 50 5050 50 50 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 50 --- 50 --- --- --- --- --- 50 ä --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- 50 50 5050 50 50 --- 50 --- ---50 50 50 --- 50 --- ------ --- --- --- --- --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ------ --- --- --- --- --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 50 5050 50 50 --- 50 50 5050 50 50 --- 50 --- ---50 50 50 --- 50 --- ---50 50 50 --- 50 50 5050 50 50 --- 50 50 5050 50 50 --- 50 50 50--- --- --- --- --- --- ---50 50 50 --- 50 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- 50 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- 50 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- 50 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- 50 50 5050 50 50 --- 50 50 5050 50 50 --- 50 50 50--- --- --- --- --- 50 5050 50 50 --- 50 --- ------ --- --- --- --- 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DF75 DF76 DF77 DF78 DF79 DF80 DF811000 500 1000 1000 1000
Æ ≈ Қ Æ ≈ U ≈ U ≈
50 50 50 --- 50 50 5050 50 50 --- 50 --- ---50 50 50 --- 50 --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 20 30 30 30 50 5030 20 30 --- 30 50 50--- --- --- --- --- --- ---30 20 30 --- 30 50 50--- --- --- --- --- --- ------ --- --- --- --- 50 50 --- --- --- --- --- 50 5030 20 30 --- 30 50 5030 20 30 --- 30 --- ------ --- --- --- --- 50 5030 20 30 --- 30 50 50--- --- --- --- --- 50 50 --- --- --- --- --- --- ---50 50 50 --- 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- 50 5030 20 30 --- 30 --- ---30 20 30 30 30 50 50
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X --- X --- ---
--- --- --- --- --- --- ---X X X --- X 20 20X X X 30 X 20 20X X X --- X 20 20--- --- --- --- --- 20 20--- --- --- --- --- --- ---X X X --- X 20 20--- --- --- --- --- --- ---X X X 30 X 20 20
Ə1 Ə Ə1 --- Ə1 * Ə1 * Ə1X 50 X --- X 50 50--- --- --- --- --- --- ---
1000 1000 1000 --- 1000 1000 1000--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DF82 DF83 DF84 DF85 DF86 DF87 DF881000 1000 1000 1000 1000
ŧ ≈ ¶ ≈ Æ ≈ U ≈ U ≈
X X X X X 20 XX X X X X 20 XX X X X X 20 X--- --- --- --- --- --- ---X X X X X 20 X
X X X X X 20 XX X X X X 20 XX X X X X --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X 20 X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X 20 X--- --- --- --- --- 20 ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X --- X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X 20 X
X X X X X 20 XX X X X X 20 X
X --- X --- X X XX X X X X 20 X
X^ X^ X^ X^ X^ --- X^
X X X X X --- ---
50 X 20 20 30 --- 30--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// X // // // 20 //
50 X X X 30 20 30X X X X 30 20 X30 30 30 30 30 30 3030 30 30 30 30 30 30 --- --- --- --- --- --- --- --- --- --- --- --- 50 ------ --- --- --- --- --- --- --- --- --- --- --- 50 ---X X X X 30 --- XX X X X 30 --- XX X X X 30 --- XX X X X 30 50 XX X X X 30 --- X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X X 30 20 XX X X X 30 50 XX X X X 30 --- X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 30 --- X--- --- --- --- --- --- ---X X X X 30 X// X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DF82 DF83 DF84 DF85 DF86 DF87 DF881000 1000 1000 1000 1000
ŧ ≈ ¶ ≈ Æ ≈ U ≈ U ≈
X 30 X X 30 50 XX 30 X X 30 50 XX 30 X X 30 50 XX 30 X X 30 50 XX 30 X X 30 50 X--- 30 X X 30 50 ---X 30 X X 30 50 X--- 30 X X 30 50 ------ --- --- --- --- 50 ------ --- --- --- --- --- ---X 30 X X 30 50 30--- 30 X X 30 50 ---X 30 X X 30 50 X--- --- --- --- --- 50 ---X 30 X X 30 50 X
50 30 X X 30 50 5050 30 X X 30 50 50
50 X X X 30 --- X50 X X X 30 --- X50 X X X 30 --- X50 X X X 30 --- X50 X X X 30 20 X--- --- --- --- --- 20 ---50 X X X 30 20 X50 X X X 30 20 X50 X X X 30 20 X50 50 50 50 30 --- ---50 50 50 50 30 --- ------ --- --- --- --- --- ---50 X X X 30 50 X50 X X X 30 --- X
--- --- --- --- --- --- ---50 X X X 30 20 3050 X X X 30 20 30
--- 1000 1000 1000 1000 --- ------ --- --- --- --- --- ---50 30 X X 30 50 5050 30 X X 30 50 5050 30 X X 30 50 5050 30 X X 30 50 5050 30 X X 30 50 5050 30 X X 30 50 5050 30 X X 30 50 5050 30 X X 30 50 5050 30 X X 30 50 50--- --- --- --- --- --- ---50 --- --- --- --- 50 ---50 30 X X 30 50 5050 30 X X 30 50 5050 --- --- --- --- 50 ---50 30 X X 30 50 50
--- --- --- --- --- --- ---50 50 --- 50 50 --- 5050 50 --- 50 50 --- 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DF82 DF83 DF84 DF85 DF86 DF87 DF881000 1000 1000 1000 1000
ŧ ≈ ¶ ≈ Æ ≈ U ≈ U ≈
50 50 --- 50 50 --- 5050 50 --- 50 50 50 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 50 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 50 50 --- --- --- --- --- --- ---50 50 --- 50 50 50 5050 50 --- 50 50 50 5050 50 --- 50 50 50 5050 50 --- 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 --- 50 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 50 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 50--- --- --- --- --- --- ---50 50 --- 50 50 --- 5050 50 --- 50 50 --- 50--- --- --- --- --- --- ---50 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 50 5050 50 --- 50 50 50 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 5050 50 --- 50 50 50 5050 50 --- 50 50 50 5050 50 --- 50 50 50 50--- --- --- --- --- --- ---50 50 --- 50 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 50 5050 50 --- 50 50 50 5050 50 --- 50 50 50 50--- --- --- --- --- 50 ---50 50 --- 50 50 --- 50--- --- --- --- --- 50 ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DF82 DF83 DF84 DF85 DF86 DF87 DF881000 1000 1000 1000 1000
ŧ ≈ ¶ ≈ Æ ≈ U ≈ U ≈
50 50 --- 50 50 50 5050 50 --- 50 50 --- 5050 50 --- 50 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
50 30 30 30 50 50 3050 30 30 30 50 50 30--- --- --- --- --- --- ---50 30 30 30 50 50 30--- --- --- --- --- --- ------ --- --- --- --- 50 --- --- --- --- --- --- 50 ------ 30 30 30 50 50 30--- 30 30 30 50 --- 30--- --- --- --- --- 50 ---50 30 30 30 50 50 30--- --- --- --- --- 50 --- --- --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- 50 ---50 30 30 30 50 --- 3050 30 30 30 50 50 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 30 --- X
--- --- --- --- --- --- ---X X X X 30 20 XX X X X 30 20 XX X X X 30 20 X--- --- X X --- 20 ------ --- --- --- --- --- ------ X X X 30 20 X--- --- --- --- --- --- ---X X X X 30 20 X
--- Ə1 --- --- Ə1 * Ə1 Ə1
--- 50 --- --- 50 50 X--- --- --- --- --- --- ------ 1000 --- --- 1000 1000 1500--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DF89 DF90 DF91 DF92 DF93 DF94 DF951000 1000 1000 1000 1000 1500
U ≈ π ≈ M ≈ U ≈ ê ≈ Ñ ≈
20 35 X X X X 1020 35 X X X X 1020 35 X X X X 10--- --- --- --- --- --- ---20 --- X X X X 10
20 35 X X X X 1020 35 X X X X 10--- 35 X X X X 10--- --- --- --- --- --- 10--- --- --- --- --- --- ---20 35 X X X X 10--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 35 X X X X 1020 --- --- --- --- --- 10
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 35 X X X X 10--- --- --- --- --- --- 10 --- --- --- --- --- --- ---20 35 X X X X 10
20 35 X X X X 1020 35 X X X X 10
X --- X X X X X20 35 X X X X 10 --- 35^ X^ X^ X^ X^ ---
--- --- X --- --- X 10
--- 35 X 30 30 20 10--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 35 X // // // 10
20 35 25 30 30 X 2520 35 25 X X X 2530 35 25 30 30 30 2530 35 25 30 30 30 25 --- --- --- --- --- --- ---50 --- --- --- --- --- 50--- --- --- --- --- --- ---50 --- --- --- --- --- --- --- 35 25 X X X 25 --- 35 25 X X X 25 --- --- 25 X X X 2550 35 25 X X X 25 --- 35 25 X X X 25--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 35 25 X X X 2550 --- 25 X X X 25 --- 35 25 X X X 25--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 25 X X X 25--- --- --- --- --- --- ---X// 35 25 X X X 25
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DF89 DF90 DF91 DF92 DF93 DF94 DF951000 1000 1000 1000 1000 1500
U ≈ π ≈ M ≈ U ≈ ê ≈ Ñ ≈
50 35 X X X 30 2550 35 X X X 30 2550 35 X X X 30 2550 35 X X X 30 2550 35 X X X 30 2550 --- X --- --- --- 2550 35 X X X 30 2550 --- X --- --- --- 2550 --- --- --- --- --- ------ --- --- --- --- --- ---50 35 X 30 30 30 2550 --- X --- --- --- 2550 35 X X X 30 2550 --- --- --- --- --- ---50 35 X X X 30 25
50 --- 50 50 50 30 2550 --- 50 50 50 30 25
--- 35 X X X X 25--- 35 X X X X 25--- 35 X X X X 25--- 35 X X X X 2520 35 X X X X 2520 --- --- --- --- --- ---20 35 X X X X 2520 35 X X X X 2520 35 X X X X 25--- --- 50 --- --- 50 25--- --- 50 --- --- 50 25--- --- --- --- --- --- 2550 35 X X X X 25--- --- X X X X 25
--- --- --- --- --- --- ---20 35 X 30 30 X 2520 35 X 30 30 X 25
--- --- 800 --- --- --- ------ --- --- --- --- --- ---50 --- 50 50 50 30 2550 --- 50 50 50 30 2550 --- 50 50 50 30 2550 --- 50 50 50 30 2550 --- 50 50 50 30 2550 --- 50 50 50 30 2550 --- 50 50 50 30 2550 --- 50 50 50 30 2550 --- 50 50 50 30 25--- --- --- --- --- --- ---50 --- --- --- --- 30 2550 --- 50 50 50 30 2550 --- 50 50 50 30 2550 --- --- --- --- 30 ---50 --- 50 50 50 30 25
800--- --- --- --- --- --- ------ --- 50 50 50 50 50--- --- 50 50 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DF89 DF90 DF91 DF92 DF93 DF94 DF951000 1000 1000 1000 1000 1500
U ≈ π ≈ M ≈ U ≈ ê ≈ Ñ ≈
--- --- 50 50 50 50 5050 --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 5050 --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 5050 --- 50 50 50 50 50--- --- --- --- --- --- ---50 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- 50 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 35 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- --- --- --- --- ------ --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- --- --- --- --- ------ --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 50--- --- --- --- --- --- ------ --- 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- --- --- --- --- ------ --- 50 50 50 50 5050 --- --- --- --- --- ---
January 01, 2016
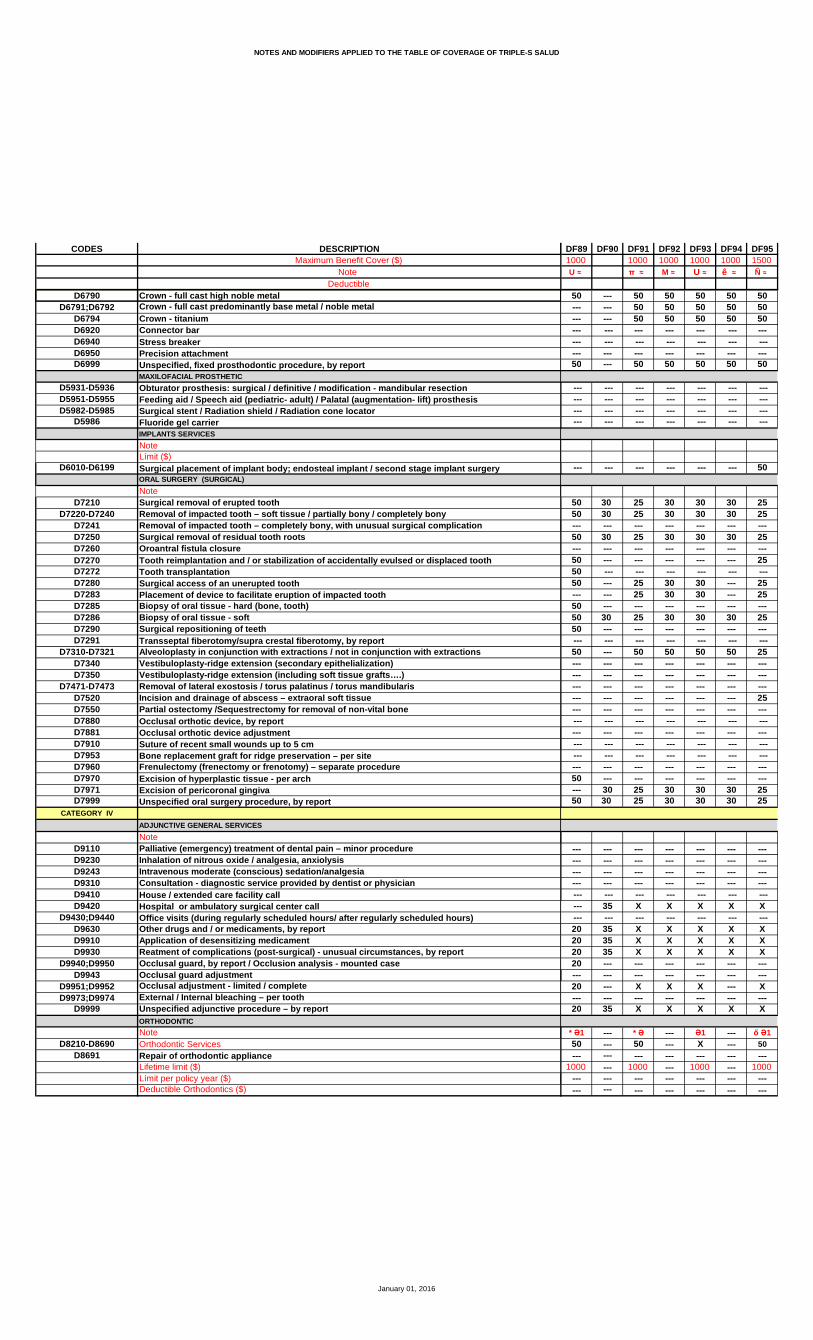
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DF89 DF90 DF91 DF92 DF93 DF94 DF951000 1000 1000 1000 1000 1500
U ≈ π ≈ M ≈ U ≈ ê ≈ Ñ ≈
50 --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 50 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- 50
50 30 25 30 30 30 2550 30 25 30 30 30 25--- --- --- --- --- --- ---50 30 25 30 30 30 25--- --- --- --- --- --- ---50 --- --- --- --- --- 2550 --- --- --- --- --- ---50 --- 25 30 30 --- 25--- --- 25 30 30 --- 2550 --- --- --- --- --- ---50 30 25 30 30 30 2550 --- --- --- --- --- --- --- --- --- --- --- --- ---50 --- 50 50 50 50 25--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- 25--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- --- --- --- --- ------ 30 25 30 30 30 2550 30 25 30 30 30 25
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- 35 X X X X X --- --- --- --- --- --- ---20 35 X X X X X20 35 X X X X X20 35 X X X X X20 --- --- --- --- --- ------ --- --- --- --- --- ---20 --- X X X --- X--- --- --- --- --- --- ---20 35 X X X X X
* Ə1 --- * Ə --- Ə1 --- ő Ə150 --- 50 --- X --- 50
--- --- --- --- --- --- ---1000 --- 1000 --- 1000 --- 1000
--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DF96 DF97 DF98 DF99 DG01 DG02 DG031000 1000 1300 1300 1000 1000 1000
Æ ≈ Æ ≈ C ≈ C ≈ ê ≈ ê ≈ U ≈
X X X X 30 X XX X X X 30 X XX X X X 30 X X--- --- --- --- --- --- ---X X X X 30 X X
X X X X 30 X XX X X X 30 X XX X X X 30 X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X 30 X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 30 X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 30 X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 30 X X
X X X X 30 X XX X X X 30 X X
X X X X X X XX X X X 30 X X
X^ X^ X^ X^ 30^ X^ X^
X X X X 30 X X
30 20 20 20 30 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// // // // 30 // //
X X X X 30 30 XX X X X 30 30 X30 30 30 30 30 30 2030 30 30 30 30 30 20 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 30 30 XX X X X 30 30 XX X X X 30 30 XX X X X 30 30 XX X X X 30 30 X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X X 30 30 XX X X X 30 30 XX X X X 30 30 X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 30 30 X--- --- --- --- --- --- ---X X X X 30 30 X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DF96 DF97 DF98 DF99 DG01 DG02 DG031000 1000 1300 1300 1000 1000 1000
Æ ≈ Æ ≈ C ≈ C ≈ ê ≈ ê ≈ U ≈
X 30 X X 30 30 XX 30 X X 30 30 XX 30 X X 30 30 XX 30 X X 30 30 XX 30 X X 30 30 XX 30 X X 30 30 XX 30 X X 30 30 XX 30 X X 30 30 X--- --- --- --- --- --- ------ --- --- --- --- --- ---X 30 X X 30 30 XX 30 X X 30 30 XX 30 X X 30 30 X--- --- --- --- --- --- ---X 30 X X 30 30 X
50 30 X X 30 30 2050 30 X X 30 30 20
X X X X 30 30 XX X X X 30 30 XX X X X 30 30 XX X X X 30 30 XX X X X 30 30 X--- --- --- --- --- --- ---X X X X 30 30 XX X X X 30 30 XX X X X 30 30 X50 50 50 50 30 50 5050 50 50 50 30 50 50--- --- --- --- --- --- ---X X X X 30 30 XX X X X 30 30 X
--- --- --- --- --- --- ---X X X X 30 30 XX X X X 30 30 X
U1000 1000 1000 1000 --- --- ---
--- --- --- --- --- --- ---50 30 X X 30 30 2050 30 X X 30 30 2050 30 X X 30 30 2050 30 X X 30 30 2050 30 X X 30 30 2050 30 X X 30 30 2050 30 X X 30 30 2050 30 X X 30 30 2050 30 X X 30 30 20--- --- --- --- --- --- ------ 30 --- --- --- --- ---50 30 X X 30 30 2050 30 X X 30 30 20 --- 30 --- --- --- --- ---50 30 X X 30 30 20
--- --- --- --- --- --- ---50 50 50 50 30 50 5050 50 50 50 30 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DF96 DF97 DF98 DF99 DG01 DG02 DG031000 1000 1300 1300 1000 1000 1000
Æ ≈ Æ ≈ C ≈ C ≈ ê ≈ ê ≈ U ≈
50 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 50 --- --- --- --- --- --- ---50 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 50 50 30 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 50--- --- --- --- --- --- ---50 50 50 50 30 50 5050 50 50 50 30 50 50--- --- --- --- --- --- ---50 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 50--- --- --- --- --- --- ---50 50 50 50 30 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 30 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 30 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 30 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 50--- --- --- --- --- --- ---50 50 50 50 30 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DF96 DF97 DF98 DF99 DG01 DG02 DG031000 1000 1300 1300 1000 1000 1000
Æ ≈ Æ ≈ C ≈ C ≈ ê ≈ ê ≈ U ≈
50 50 50 50 30 50 5050 50 50 50 30 50 5050 50 50 50 30 50 50--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 30 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 30 30 30 30 30 2030 30 30 30 30 30 20--- --- --- --- --- --- ---30 30 30 30 30 30 20--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 30 30 30 30 30 3030 30 30 30 --- --- 30--- --- --- --- --- --- ---30 30 30 30 30 30 30--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 50 50 30 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- 30 30 ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- 30 30 ------ --- --- --- --- --- ---30 30 30 30 30 30 3030 30 30 30 30 30 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
--- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---X X X X X X X
Ə1 Ə1 Ə1 Ə1 --- --- ** Ə50 X X X --- --- 50
--- --- --- --- --- --- ---1000 1000 --- --- --- --- 1500
--- --- 1000 1000 --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DG04 DG05 DG06 DG091000 1000 1000
Æ ≈ U ≈ U ≈
X X X XX X X XX X X X--- --- --- ---X X X X
X X X XX X X Þ XX X --- X--- --- --- ------ --- --- ---X X X X--- --- --- ------ --- --- ------ --- --- --- --- --- --- ---X X X X--- --- --- ---
--- --- --- --- --- --- --- ---X X X X--- --- --- --- --- --- --- ---X X X X
X X X XX X X X
X X --- XX X X X
X^ X^ X^ X^
X X 20 X
20 X 20 X--- --- --- ------ --- --- ------ --- --- ---// X // X
X X 20 XX X 20 X30 20 30 X30 20 30 X --- --- --- --- --- --- --- ------ --- --- --- --- --- --- ---X X --- XX X --- XX X --- XX X --- XX X --- X--- --- --- ------ --- --- ------ --- --- ---X X 20 XX X --- XX X --- X--- --- --- --- --- --- --- ---X X --- X--- --- --- ---X X 20 X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DG04 DG05 DG06 DG091000 1000 1000
Æ ≈ U ≈ U ≈
X 20 --- XX 20 20 XX 20 20 XX 20 20 XX 20 20 XX 20 20 XX 20 20 XX 20 --- X--- --- --- ------ --- --- ---X 20 --- XX 20 --- XX 20 --- X--- --- --- ---X 20 20 X
X 20 --- XX 20 20 X
1000X X --- XX X 40 XX X 40 XX X --- XX X 40 X--- --- --- ---X X 40 XX X 40 XX X --- X50 50 40 X50 50 40 X--- --- --- ---X X --- XX X --- X
--- --- --- ---X 20 20 XX 20 20 X
T1000 --- --- ---
--- --- --- ---X 20 --- XX 20 --- XX 20 --- XX 20 --- XX 20 --- XX 20 --- XX 20 --- XX 20 --- XX 20 --- X--- --- --- ------ --- --- ---X 20 --- XX 20 20 X
--- --- --- ---X 20 --- X
T1000
--- --- --- ---50 50 --- X50 50 20 X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DG04 DG05 DG06 DG091000 1000 1000
Æ ≈ U ≈ U ≈
50 50 20 X50 50 --- X50 50 --- X50 50 20 X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X --- --- --- ---50 50 40 X50 50 --- X50 50 --- X50 50 40 X --- --- --- --- --- --- --- ---50 50 --- X --- --- --- --- --- --- --- ------ --- --- ---50 50 40 X50 50 --- X50 50 --- X--- --- --- ---50 50 --- X50 50 --- X--- --- --- ---50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X50 50 --- X--- --- --- ---50 50 --- X--- --- --- ------ --- --- ---50 50 --- X--- --- --- ------ --- --- ---50 50 --- X--- --- --- ------ --- --- ------ --- --- ---50 50 --- X--- --- --- ------ --- --- ---50 50 --- X50 50 --- X50 50 --- X--- --- --- ---50 50 --- X--- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DG04 DG05 DG06 DG091000 1000 1000
Æ ≈ U ≈ U ≈
50 50 --- X50 50 --- X50 50 --- X--- --- --- --- --- --- --- ------ --- --- ---50 50 --- X
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- ---
30 20 20 X30 20 20 X--- --- --- ---30 20 20 X--- --- --- ------ --- --- --- --- --- --- ---30 20 --- X30 20 --- X--- --- --- ---30 20 --- X--- --- --- --- --- --- --- ---50 50 --- X--- --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- ------ --- 20 ------ --- --- ---30 20 --- X30 20 20 X
--- --- --- ------ --- --- ------ --- --- ------ --- --- --- --- --- --- ---X X 20 X
--- --- --- ---X X --- XX X 20 XX X 20 X--- --- --- ------ --- --- ---X X --- X--- --- --- ---X X 20 X
Ə1 Ə --- Ə
X 50 --- X
--- --- --- ---1000 1000 --- 1000
--- --- --- ------ --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DG10 DG11 DG12 DG13 DG14 DG15 DG161500 1000 1250 1000 1300 1000
Ñ ≈ U ≈ ♠ ≈ M ≈ Ø ≈ U ≈
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X Þ X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
X --- X X X X XX X X X X X X
X^ X^ X^ X^ X^ X^ X^
X X X X X X X
X X 20 20 20 X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X // // // X X
º20 X 20 20 30 20 3020 X 20 20 30 20 3020 X 20 20 30 20 3020 X 20 20 30 20 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 X 20 20 30 20 3020 X 20 20 30 20 3020 --- 20 20 30 20 3020 X 20 20 30 20 3020 X 20 20 30 20 30--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 X 20 20 30 20 3020 --- 20 20 30 20 3020 X 20 20 30 20 30--- --- --- --- --- --- --- --- --- --- --- --- --- ---20 --- 20 20 30 20 30--- --- --- --- --- --- ---20 X 20 20 30 20 30
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DG10 DG11 DG12 DG13 DG14 DG15 DG161500 1000 1250 1000 1300 1000
Ñ ≈ U ≈ ♠ ≈ M ≈ Ø ≈ U ≈
º20 X 50 50 50 20 3020 X 50 50 50 20 3020 X 50 50 50 20 3020 X 50 50 50 20 3020 X 50 50 50 20 3020 X 50 50 50 20 3020 X 50 50 50 20 3020 --- 50 50 50 20 30--- --- --- --- --- --- ------ --- --- --- --- --- ---20 X 50 50 50 20 3020 --- 50 50 50 20 3020 X 50 50 50 20 30--- --- --- --- --- --- ---20 X 50 50 50 20 30
º20 --- 50 50 50 20 3020 X 50 50 50 20 30
º
20 X X X X 20 5020 X X X X 20 5020 X ê X X X 20 5020 X ê X X X 20 5020 X ê X X X 20 50--- --- --- --- --- --- ---20 X X X X 20 5020 X X X X 20 5020 X ê X X X 20 5020 X 50 50 50 50 5020 X 50 50 50 50 50--- --- --- --- --- --- ---20 X ê X X X 20 5020 X ê X X X 20 50
º
--- --- --- --- --- --- ---20 X 20 20 30 20 3020 X 20 20 30 20 30
º--- 800 --- --- --- --- ------ --- --- --- --- --- ---20 --- 50 50 50 20 3020 --- 50 50 50 20 3020 --- 50 50 50 20 3020 --- 50 50 50 20 3020 X 50 50 50 20 3020 --- 50 50 50 20 3020 --- 50 50 50 20 3020 --- 50 50 50 20 3020 --- 50 50 50 20 30--- --- --- --- --- --- ------ --- --- --- --- --- ---20 --- 50 50 50 20 3020 X 50 50 50 20 30 --- --- --- --- --- --- ---20 --- 50 50 50 20 30
@ º
--- --- --- --- --- --- ---50 --- 50 50 50 50 5050 --- 50 50 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DG10 DG11 DG12 DG13 DG14 DG15 DG161500 1000 1250 1000 1300 1000
Ñ ≈ U ≈ ♠ ≈ M ≈ Ø ≈ U ≈
50 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 50 --- --- --- --- --- --- ---50 X 50 50 50 50 5050 --- 50 50 50 50 5050 X 50 50 50 50 5050 X 50 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ---50 --- 50 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 X 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 50--- --- --- --- --- --- ---50 --- 50 50 50 50 5050 --- 50 50 50 50 50--- --- --- --- --- --- ---50 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 50--- --- --- --- --- --- ---50 --- 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 50--- --- --- --- --- --- ---50 --- 50 50 50 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DG10 DG11 DG12 DG13 DG14 DG15 DG161500 1000 1250 1000 1300 1000
Ñ ≈ U ≈ ♠ ≈ M ≈ Ø ≈ U ≈
50 --- 50 50 50 50 5050 --- 50 50 50 50 5050 --- 50 50 50 50 50--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 --- 50 50 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
º20 X 20 20 30 20 3020 X 20 20 30 20 30--- --- --- --- --- --- ---20 X 20 20 30 20 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 X 20 20 30 20 3020 --- 20 20 30 20 30--- --- --- --- --- --- ---20 X 20 20 30 20 30--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 --- 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 X 20 20 30 20 3020 X 20 20 30 20 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
--- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X --- X X X X X--- --- --- --- --- --- ---X X X X X X X
Ə1 --- Ə1 Ə1 --- ® Ə1 Ə150 --- X 50 --- 50 50
--- --- --- --- --- --- ---1500 --- 1000 1500 --- 1400 1000
--- --- --- --- --- --- ---50 --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DG17 DG18 DG19 DG20 DG21 DG22 DG231000 1000 1000 1000 1000 1000
M ≈ M ≈ ≈ ≈ ≈ Æ ≈
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
X X X X X X ---X X X X X X X
X^ X^ X^ X^ X^ --- X^
X X X X X X X
X 20 X X X 50 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X // X X X // //
30 30 20 30 25 X X30 30 20 30 25 X X30 30 20 30 25 30 3030 30 20 30 25 30 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 30 20 30 25 X X30 30 20 30 25 X X30 30 20 30 25 X X30 30 20 30 25 X X30 30 20 30 25 X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 30 20 30 25 X X30 30 20 30 25 X X30 30 20 30 25 X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---30 30 20 30 25 X X--- --- --- --- --- --- ---30 30 20 30 25 X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DG17 DG18 DG19 DG20 DG21 DG22 DG231000 1000 1000 1000 1000 1000
M ≈ M ≈ ≈ ≈ ≈ Æ ≈
30 50 20 30 30 X X30 50 20 30 30 X X30 50 20 30 30 X X30 50 20 30 30 X X30 50 20 30 30 X X30 50 20 30 30 X X30 50 20 30 30 X X30 50 20 30 30 X X--- --- --- --- --- --- ------ --- --- --- --- --- ---30 50 20 30 30 X X30 50 --- 30 30 X X30 50 20 30 30 X X--- --- --- --- --- --- ---30 50 20 30 30 X X
30 50 50 30 25 X X30 50 50 30 25 X X
--- X X X 25 X X--- X X X 25 X X--- X X X 25 X X--- X X X 25 X X--- X X X 25 X X--- --- --- --- --- --- ------ X X X 25 X X--- X X X 25 X X--- X X X 25 X X--- 50 50 50 25 50 50--- 50 50 50 25 50 50--- --- --- --- --- --- ------ X X X 25 X X--- X X X 25 X X
--- --- --- --- --- --- ---30 30 20 30 30 X X30 30 20 30 30 X X
--- --- --- --- --- 800 1000--- --- --- --- --- 50 ---30 50 50 30 25 X X30 50 50 30 25 X X30 50 50 30 25 X X30 50 50 30 25 X X30 50 50 30 25 X X30 50 50 30 25 X X30 50 50 30 25 X X30 50 50 30 25 X X30 50 50 30 25 X X--- --- --- --- --- --- ------ --- --- --- --- --- ---30 50 50 30 25 X X30 50 50 30 25 X X --- --- --- --- --- --- ---30 50 50 30 25 X X
--- --- --- --- --- --- ------ 50 50 50 50 50 57--- 50 50 50 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DG17 DG18 DG19 DG20 DG21 DG22 DG231000 1000 1000 1000 1000 1000
M ≈ M ≈ ≈ ≈ ≈ Æ ≈
--- 50 50 50 50 50 50--- 50 50 50 50 50 57--- 50 50 50 50 50 50--- 50 50 50 50 50 50--- 50 50 50 50 50 57--- 50 50 50 50 50 50--- 50 50 50 50 50 57--- 50 50 50 50 50 50--- 50 50 50 50 50 50--- 50 50 50 50 50 57--- 50 50 50 50 50 50--- --- --- --- --- --- ------ 50 50 50 50 50 50--- 50 50 50 50 50 50--- 50 50 50 50 50 50--- 50 50 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 50 50 50--- 50 50 50 50 --- 50--- 50 50 50 50 --- 57--- --- --- --- --- --- ------ 50 50 50 50 --- 50--- 50 50 50 50 --- 57--- --- --- --- --- --- ------ 50 50 50 50 --- 50--- 50 50 50 50 --- 50--- 50 50 50 50 --- 57--- 50 50 50 50 --- 57--- 50 50 50 50 --- 50--- 50 50 50 50 --- 50--- 50 50 50 50 --- 57--- 50 50 50 50 --- 57--- 50 50 50 50 --- 57--- 50 50 50 50 --- 50--- 50 50 50 50 --- 50--- 50 50 50 50 --- 57--- 50 50 50 50 --- 50--- 50 50 50 50 --- 50--- 50 50 50 50 50 57--- 50 50 50 50 50 50--- 50 50 50 50 50 50--- 50 50 50 50 50 57--- 50 50 50 50 50 57--- 50 50 50 50 50 50--- 50 50 50 50 50 50--- --- --- --- --- --- ------ 50 50 50 50 50 57--- --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 50 50 57--- --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 50 50 57--- 50 50 50 50 50 50--- 50 50 50 50 50 50--- --- --- --- --- --- ------ 50 50 50 50 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DG17 DG18 DG19 DG20 DG21 DG22 DG231000 1000 1000 1000 1000 1000
M ≈ M ≈ ≈ ≈ ≈ Æ ≈
--- 50 50 50 50 50 57--- 50 50 50 50 50 50--- 50 50 50 50 50 57--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ 50 50 50 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 30 20 30 30 30 3030 30 20 30 30 30 30--- --- --- --- --- --- ---30 30 20 30 30 30 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 30 --- 30 30 30 3030 30 --- 30 30 30 30--- --- --- --- --- --- ---30 30 20 30 30 30 30--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 30 20 30 30 30 3030 30 20 30 30 30 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 25 --- X
--- --- --- --- --- --- ---X X X X 25 X XX X X X 25 X XX X X X 25 X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X --- X 25 X X--- --- --- --- --- --- ---X X X X 25 X X
--- --- --- Ə Ə Ə Π Ə --- --- --- 50 X 50 X --- --- --- --- --- --- ------ --- --- 2000 1000 1000 1000--- --- --- --- --- ------ --- --- --- --- 50 ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DG24 DG25 DG26 DG27 DG28 DG29 DG301000 1000 1000 ≈ ⋈ ≈ ⋈ ≈
X X 30 30 X X XX X 30 30 X X XX X 30 30 X X X--- --- --- --- --- --- ---X X 30 30 --- X X
X X 30 30 X X XX X 30 30 X X Þ X ÞX X 30 30 X --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X 30 30 X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X 30 30 X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X 30 30 X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X 30 30 X X X
X X 30 30 X X XX X 30 30 X X X
X --- X X --- --- ---X X 30 30 X X X
X^ X^ 30^ 30^ X^ X^ X^
X X --- --- X 20 20
X X 30 30 X 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X 30 30 X // //
X 25 30 30 25 20 20X 25 30 30 X 20 2030 25 30 30 25 30 3030 25 30 30 25 30 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X 25 --- --- X --- ---X 25 30 30 X --- ---X 25 --- --- --- --- ---X 25 30 30 X --- ---X 25 30 30 X --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X 25 30 30 X 20 20X 25 --- --- --- --- ---X 25 30 30 X --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X 25 --- --- --- --- ------ --- --- --- --- --- ---X 25 30 30 X 20 20
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DG24 DG25 DG26 DG27 DG28 DG29 DG301000 1000 1000 ≈ ⋈ ≈ ⋈ ≈
25 25 30 30 25 --- ---25 25 30 30 25 20 5025 25 30 30 25 20 5025 25 30 30 25 20 5025 25 30 30 25 20 5025 Ŀ --- --- --- 20 5025 25 30 30 25 20 5025 Ŀ --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---25 25 30 30 25 --- ---25 --- --- --- --- --- ---25 25 30 30 25 --- ------ --- --- --- --- --- ---25 25 30 30 25 20 50
25 20 X X --- --- ---25 20 X X --- 20 20
1000 1000X X 30 30 X --- ---X X 30 30 X 40 ---X X 30 30 X 40 ---X X 30 30 X --- ---X X 30 30 X 40 40--- --- --- --- --- --- ---X X 30 30 X 40 ---X X 30 30 X 40 ---X X 30 30 X --- ---50 50 --- --- --- 40 4050 50 --- --- --- 40 40--- --- --- --- --- --- ---X X 30 30 X --- ---X X --- --- X --- ---
--- --- --- --- --- --- ---25 X 30 30 25 20 3025 X 30 30 25 20 30
₪ ₪1000 300 300 --- --- ---
--- --- --- --- --- --- ---25 20 X X --- --- ---25 20 X X --- --- ---25 20 X X --- --- ---25 20 X X --- --- ---25 20 X X --- --- ---25 20 X X --- --- ---25 20 X X --- --- ---25 20 X X --- --- ---25 20 X X --- --- ------ --- --- --- --- --- ------ --- X X --- --- ---25 20 X X --- --- ---25 20 X X --- 20 20 --- --- X X --- --- ---25 20 X X --- --- ---
m ₪ ₪500 800 300 300 1000 1000--- --- X X --- --- ---50 50 X X --- --- ---50 50 X X --- 20 20
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DG24 DG25 DG26 DG27 DG28 DG29 DG301000 1000 1000 ≈ ⋈ ≈ ⋈ ≈
50 50 X X --- 20 2050 50 X X --- --- ---50 50 X X --- --- ---50 50 X X --- 20 2050 50 X X --- --- ---50 50 X X --- --- ---50 50 X X --- --- ---50 50 X X --- --- ---50 50 X X --- --- ---50 50 X X --- --- ---50 50 X X --- --- --- --- --- X X --- --- ---50 50 X X --- 40 ---50 50 X X --- --- ---50 50 X X --- --- ---50 50 X X --- 40 --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 X X --- --- --- --- --- X X --- --- --- --- --- X X --- --- ------ --- X X --- --- ---50 50 X X X 40 4050 50 --- --- --- --- ---50 50 --- --- --- --- ------ --- --- --- --- --- ---50 50 --- --- --- --- ---50 50 --- --- --- --- ------ --- --- --- --- --- ---50 50 --- --- --- --- ---50 50 --- --- --- --- ---50 50 --- --- --- --- ---50 50 --- --- --- --- ---50 50 --- --- --- --- ---50 50 --- --- --- --- ---50 50 --- --- --- --- ---50 50 --- --- --- --- ---50 50 --- --- --- --- ---50 50 --- --- --- --- ---50 50 --- --- --- --- ---50 50 --- --- --- --- ---50 50 --- --- --- --- ---50 50 --- --- --- --- ---50 50 X X --- --- ---50 50 X X --- --- ---50 50 X X --- --- ---50 50 X X --- --- ---50 50 X X --- --- ---50 50 X X --- --- ---50 50 X X --- --- ------ --- X X --- --- ---50 50 X X --- --- ------ --- X X --- --- ------ --- X X --- --- ---50 50 X X --- --- ------ --- X X --- --- ------ --- X X --- --- ---50 50 X X --- --- ------ --- X X --- --- ------ --- X X --- --- ------ --- X X --- --- ---50 50 X X --- --- ------ --- X X --- --- ------ --- X X --- --- ---50 50 X X --- --- ---50 50 X X --- --- ---50 50 X X --- --- ------ --- X X --- --- ---50 50 X X --- --- ------ --- X X --- --- ---
January 01, 2016
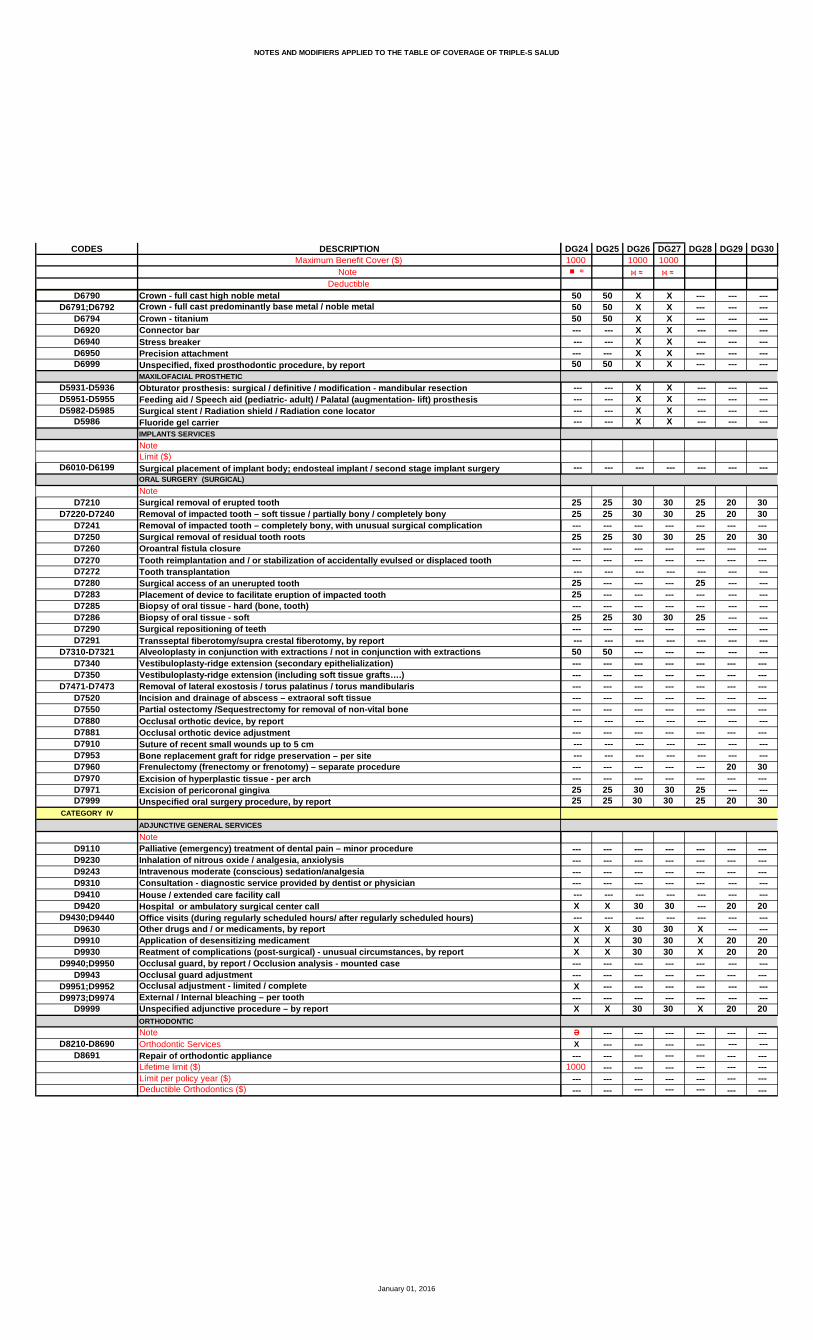
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DG24 DG25 DG26 DG27 DG28 DG29 DG301000 1000 1000 ≈ ⋈ ≈ ⋈ ≈
50 50 X X --- --- ---50 50 X X --- --- ---50 50 X X --- --- ------ --- X X --- --- --- --- --- X X --- --- ------ --- X X --- --- ---50 50 X X --- --- ---
--- --- X X --- --- --- --- --- X X --- --- --- --- --- X X --- --- --- --- --- X X --- --- ---
--- --- --- --- --- --- ---
25 25 30 30 25 20 3025 25 30 30 25 20 30--- --- --- --- --- --- ---25 25 30 30 25 20 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---25 --- --- --- 25 --- ---25 --- --- --- --- --- ------ --- --- --- --- --- ---25 25 30 30 25 --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- 20 30--- --- --- --- --- --- ---25 25 30 30 25 --- ---25 25 30 30 25 20 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X 30 30 --- 20 20
--- --- --- --- --- --- ---X X 30 30 X --- ---X X 30 30 X 20 20X X 30 30 X 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ---X --- --- --- --- --- ------ --- --- --- --- --- ---X X 30 30 X 20 20
Ə --- --- --- --- --- ---X --- --- --- --- --- ------ --- --- --- --- --- ---
1000 --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DG31 DG34 DG41 DG42 DG43 DG44 DG45500 1000¤ Æ ≈
ς
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X --- X X X X
X X X X X X XX Þ X Þ X X X Þ X • X--- --- X X X --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
--- --- --- --- --- --- XX X X X X X X
X^ X^ X^ X^ X^ X X^
20 20 X X X X X
20 20 X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// // X X X X X
º ς20 20 X X X X 3020 20 X X X X 3030 30 30 30 X X 3030 30 30 30 X X 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- X X X X 30 --- --- X X X X 30 --- --- X X --- --- 30 --- --- X X X X 30 --- --- X X X --- 30 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 X X X X 30 --- --- X X --- --- 30 --- --- X X X X 30--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- X X --- --- 30--- --- --- --- --- --- ---20 20 X X X X 30
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DG31 DG34 DG41 DG42 DG43 DG44 DG45500 1000¤ Æ ≈
º ς --- --- 30 30 X X 3020 20 30 30 X X 3020 20 30 30 X X 3020 20 30 30 X --- 3020 20 30 30 X X 3020 20 30 30 X --- 3020 20 30 30 X X 30 --- --- 30 30 --- --- 30 --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- 30 30 X --- 30 --- --- 30 30 --- --- 30 --- --- 30 30 X --- 30 --- --- --- --- --- --- ---20 20 30 30 X X 30
º --- --- --- X --- --- 3020 20 --- X X --- 30
º1000 1000
--- --- X X X --- X40 40 X X X --- X40 40 X X X ê --- X --- --- X X X ê --- X40 40 X X X ê --- X --- --- --- --- --- --- ---40 40 X X X --- X40 40 X X X --- X --- --- X X X ê --- X40 40 50 50 X --- 5040 40 50 50 X --- 50 --- --- --- --- --- --- --- --- --- X X X ê --- X --- --- X X X ê --- X
º
--- --- --- --- --- --- ---20 20 X X X X 3020 20 X X X X 30
º ™ ς--- --- --- 1000 800 500 1000--- --- --- --- --- --- ------ --- --- X --- X 30--- --- --- X --- X 30--- --- --- X --- X 30--- --- --- X --- X 30--- --- --- X X X 30--- --- --- X --- X 30--- --- --- X --- X 30--- --- --- X --- X 30--- --- --- X --- X 30--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- X --- --- 3020 20 --- X X --- 30--- --- --- --- --- --- ------ --- --- X --- X 30
@ º1000 1000 ---
--- --- --- --- --- --- --- --- --- 50 50 --- --- 5020 20 50 50 --- --- 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DG31 DG34 DG41 DG42 DG43 DG44 DG45500 1000¤ Æ ≈
20 20 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 5020 20 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- --- --- --- --- ---40 40 50 50 X --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 X --- 5040 40 50 50 X --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 --- --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---40 40 50 50 X --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- --- --- --- --- --- --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- --- --- --- --- --- --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- --- --- --- --- --- --- --- 50 50 --- --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 --- --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 --- --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 --- --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- --- --- --- --- --- --- --- 50 50 --- --- 50 --- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DG31 DG34 DG41 DG42 DG43 DG44 DG45500 1000¤ Æ ≈
--- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- 50 50 --- --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 --- --- 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
º ς
20 20 30 30 X X 3020 20 30 30 X X 30--- --- --- --- --- --- ---20 20 30 30 X X 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 30 30 X X 30 --- --- 30 30 --- --- 30 --- --- --- --- --- --- --- --- --- 30 30 X X 30 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 --- --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 --- --- --- --- ------ --- --- --- --- --- --- --- --- 30 30 X --- 3020 20 30 30 X X 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 X X X --- X --- --- --- --- --- --- --- --- --- X X X X X20 20 X X X X X20 20 X X X X X --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- X X --- --- X --- --- --- --- --- --- ---20 20 X X X X X
Ə --- --- --- --- --- Ə
50 --- --- --- --- --- 50--- --- --- --- --- --- ---
2000 --- --- --- --- --- 1000--- --- --- --- --- ---
--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DG46 DG47 DG48 DG49 DG50 DG51 DG521000 1000 1000 1000 1500 1500 1000
U ≈ ≈ ≈ U ≈ Ñ ≈ Ñ ≈ ď U ≈
Ď
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- X ------ --- --- --- --- X --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
X X X X X X XX X X X X X X
X^ X^ X^ X^ X^ X^ X^
X X X X X X X
X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X
X 20 20 20 20 20 30X 20 20 20 20 20 30X 20 20 20 20 20 30X 20 20 20 20 20 30
--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X 20 20 20 20 20 30X 20 20 20 20 20 30X 20 20 20 20 20 30X 20 20 20 20 20 30X 20 20 20 20 20 30--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X 20 20 20 20 20 30X 20 20 20 20 20 30X 20 20 20 20 20 30--- --- --- --- --- --- --- --- --- --- --- --- --- ---X 20 20 20 20 20 30--- --- --- --- --- --- ---X 20 20 20 20 20 30
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DG46 DG47 DG48 DG49 DG50 DG51 DG521000 1000 1000 1000 1500 1500 1000
U ≈ ≈ ≈ U ≈ Ñ ≈ Ñ ≈ ď U ≈
Ď
X 20 20 20 20 20 30X 20 20 20 20 20 30X 20 20 20 20 20 30X 20 20 20 20 20 30X 20 20 20 20 20 30X --- 20 20 20 20 30X 20 20 20 20 20 30X --- 20 20 20 20 30--- --- --- --- --- --- ------ --- --- --- --- --- ---X 20 20 20 20 20 30X --- --- 20 20 20 30X 20 20 20 20 20 30--- --- --- --- --- --- ---X 20 20 20 20 20 30
50 20 20 20 20 20 X50 20 20 20 20 20 X
X X X X X 20 XX X X X X 20 XX X X X X 20 XX X X X X 20 XX X X X X 20 X--- --- --- --- --- --- ---X X X X X 20 XX X X X X 20 XX X X X X 20 X50 50 50 50 50 20 5050 50 50 50 50 20 50--- --- --- --- --- --- ---X X X X X 20 XX X X X X 20 X
--- --- --- --- --- --- ---X 20 20 20 20 20 30X 20 20 20 20 20 30
Ñ--- --- --- --- --- ------ --- --- --- --- --- ---50 20 20 20 20 20 X50 20 20 20 20 20 X50 20 20 20 20 20 X50 20 20 20 20 20 X50 20 20 20 20 20 X50 20 20 20 20 20 X50 20 20 20 20 20 X50 20 20 20 20 20 X50 20 20 20 20 20 X--- --- --- --- --- --- ------ --- --- --- --- --- ---50 20 20 20 20 20 X50 20 20 20 20 20 X --- --- --- --- --- --- ---50 20 20 20 20 20 X
--- --- --- --- --- --- ---50 50 50 50 50 50 5050 50 50 50 50 50 50
January 01, 2016
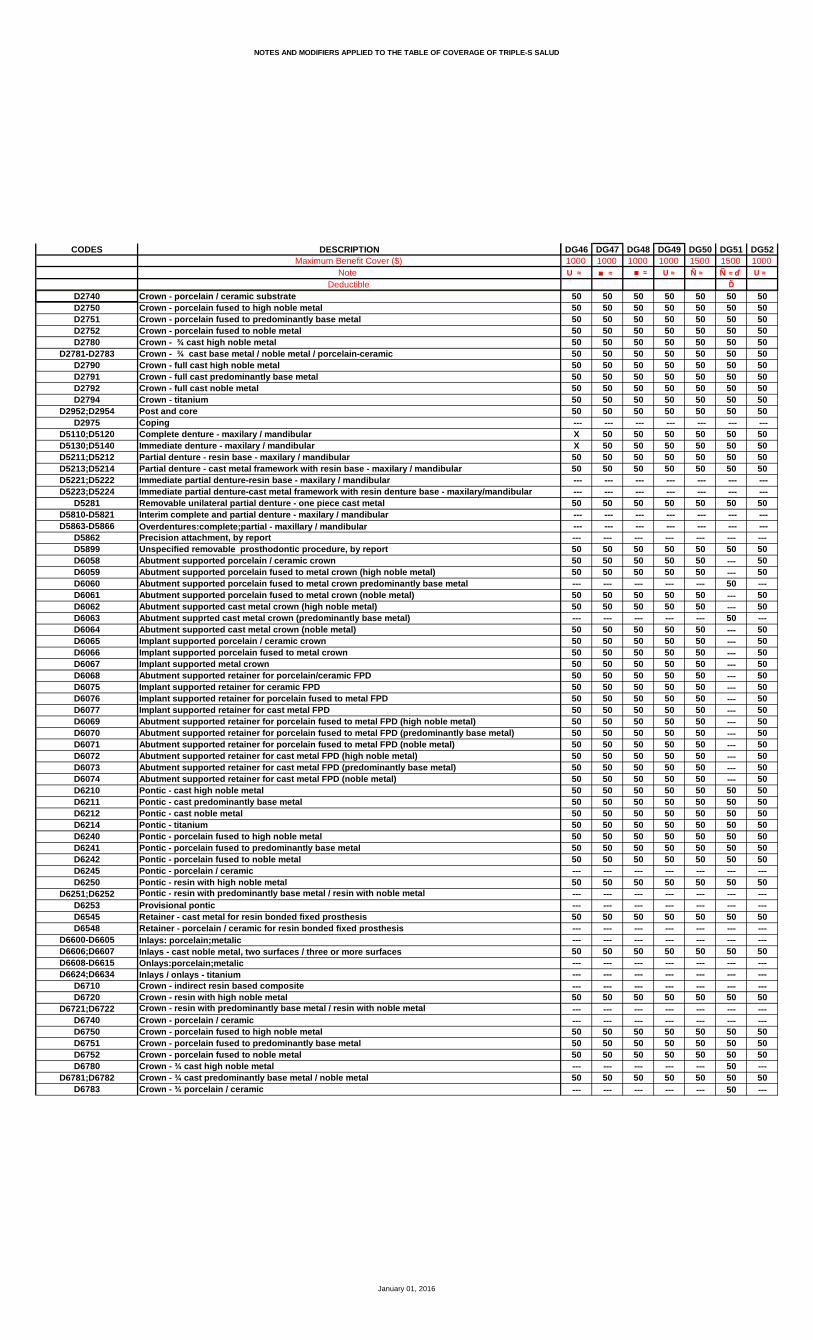
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DG46 DG47 DG48 DG49 DG50 DG51 DG521000 1000 1000 1000 1500 1500 1000
U ≈ ≈ ≈ U ≈ Ñ ≈ Ñ ≈ ď U ≈
Ď
50 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 50 --- --- --- --- --- --- ---X 50 50 50 50 50 50X 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 50 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 5050 50 50 50 50 --- 5050 50 50 50 50 --- 50--- --- --- --- --- 50 ---50 50 50 50 50 --- 5050 50 50 50 50 --- 50--- --- --- --- --- 50 ---50 50 50 50 50 --- 5050 50 50 50 50 --- 5050 50 50 50 50 --- 5050 50 50 50 50 --- 5050 50 50 50 50 --- 5050 50 50 50 50 --- 5050 50 50 50 50 --- 5050 50 50 50 50 --- 5050 50 50 50 50 --- 5050 50 50 50 50 --- 5050 50 50 50 50 --- 5050 50 50 50 50 --- 5050 50 50 50 50 --- 5050 50 50 50 50 --- 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- 50 ---50 50 50 50 50 50 50--- --- --- --- --- 50 ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DG46 DG47 DG48 DG49 DG50 DG51 DG521000 1000 1000 1000 1500 1500 1000
U ≈ ≈ ≈ U ≈ Ñ ≈ Ñ ≈ ď U ≈
Ď
50 50 50 50 50 50 5050 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
X 20 20 20 20 20 30X 20 20 20 20 20 30--- --- --- --- --- 20 ---X 20 20 20 20 20 30--- --- --- --- --- 20 ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X --- --- 20 20 20 30X --- --- 20 20 20 30--- --- --- --- --- --- ---X 20 20 20 20 20 30--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- 20 ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- 20 ------ --- --- --- --- --- ---X 20 20 20 20 20 30X 20 20 20 20 20 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
--- --- --- --- --- --- ---X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X --- --- X X X X--- --- --- --- --- --- ---X X X X X X X
Ə Ə --- Ə Ə --- Ə
X 50 --- 50 40 --- 50--- --- --- --- --- --- ---
1000 1500 --- 1000 1800 --- 1000--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016
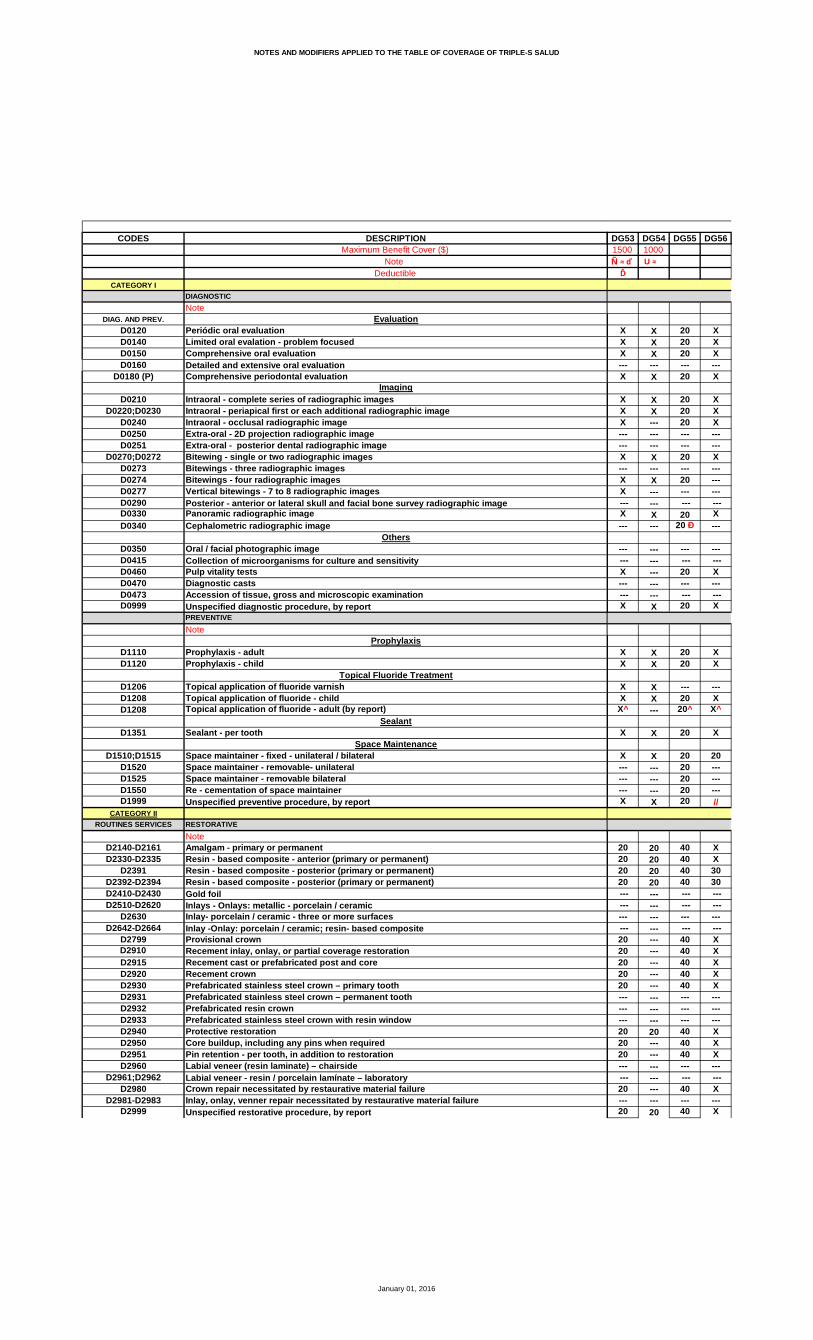
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DG53 DG54 DG55 DG561500 1000
Ñ ≈ ď U ≈Ď
X X 20 XX X 20 XX X 20 X--- --- --- ---X X 20 X
X X 20 XX X 20 XX --- 20 X--- --- --- ------ --- --- ---X X 20 X--- --- --- ---X X 20 ---X --- --- ---
--- --- --- ---X X 20 X--- --- 20 Ð ---
--- --- --- --- --- --- --- ---X --- 20 X--- --- --- --- --- --- --- ---X X 20 X
X X 20 XX X 20 X
X X --- ---X X 20 X
X^ --- 20^ X^
X X 20 X
X X 20 20--- --- 20 ------ --- 20 ------ --- 20 ---X X 20 //
20 20 40 X20 20 40 X20 20 40 3020 20 40 30 --- --- --- --- --- --- --- ------ --- --- --- --- --- --- ---20 --- 40 X20 --- 40 X20 --- 40 X20 --- 40 X20 --- 40 X--- --- --- ------ --- --- ------ --- --- ---20 20 40 X20 --- 40 X20 --- 40 X--- --- --- --- --- --- --- ---20 --- 40 X--- --- --- ---20 20 40 X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DG53 DG54 DG55 DG561500 1000
Ñ ≈ ď U ≈Ď
20 --- 40 X20 --- 40 X20 --- 40 X20 20 40 X20 20 40 X20 20 40 X20 20 40 X20 20 40 X--- --- 40 ------ --- --- ---20 --- 40 X20 --- --- X20 --- 40 X--- --- --- ---20 20 40 X
20 --- 40 X20 X 40 X
20 20 50 X20 --- 50 X20 --- 50 X20 --- 50 X20 --- 50 X--- --- 50 ---20 --- 50 X20 --- 50 X20 --- 50 X20 --- 50 5020 --- 50 50--- --- 50 ---20 20 50 X20 X 50 X
--- --- --- ---20 20 40 X20 20 40 X
Ñ--- --- 1000 1000--- --- --- ---20 --- 40 X20 --- 40 X20 --- 40 X20 --- 40 X20 20 40 X20 --- 40 X20 --- 40 X20 --- --- X20 --- --- X--- --- --- ------ --- --- ---20 --- 40 X20 20 40 X --- --- --- ---20 20 40 X
--- --- --- ---50 --- 50 5750 --- 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DG53 DG54 DG55 DG561500 1000
Ñ ≈ ď U ≈Ď
50 --- 50 5050 50 50 5750 --- 50 5050 --- 50 5050 50 50 5750 --- 50 5050 --- 50 5750 --- 50 5050 50 50 5050 --- 50 5750 --- 50 50 --- --- --- ---50 50 50 5050 --- 50 5050 --- 50 5050 50 50 50 --- --- --- --- --- --- --- ---50 --- 50 50 --- --- --- --- --- --- --- ------ --- --- ---50 50 50 50--- --- 50 50--- --- 50 5750 --- 50 ------ --- 50 50--- --- 50 5750 --- 50 ------ --- 50 50--- --- 50 50--- --- 50 57--- --- 50 57--- --- 50 50--- --- 50 50--- --- 50 57--- --- 50 57--- --- 50 57--- --- 50 50--- --- 50 50--- --- 50 57--- --- 50 50--- --- 50 5050 50 50 5750 --- 50 5050 --- 50 5050 --- 50 5750 50 50 5750 --- 50 5050 --- 50 50--- --- --- ---50 50 50 57--- --- --- ------ --- --- ---50 --- 50 50--- --- --- ------ --- --- ---50 --- 50 50--- --- --- ------ --- --- ------ --- --- ---50 50 50 57--- --- --- ------ --- --- ---50 50 50 5750 --- 50 5050 --- 50 5050 --- --- ---50 --- 50 5050 --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DG53 DG54 DG55 DG561500 1000
Ñ ≈ ď U ≈Ď
50 50 50 5750 --- 50 5050 --- 50 57--- --- --- --- --- --- --- ------ --- --- ---50 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- ---
20 20 40 3020 20 40 3020 --- --- ---20 --- 40 3020 --- 40 ------ --- 40 --- --- --- --- ---20 --- 40 3020 --- 40 30--- --- 40 ---20 --- 40 30--- --- 40 --- --- --- --- ---50 --- 50 50--- --- --- ------ --- --- ---20 --- --- ------ --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- ---20 --- 40 ------ --- 40 ---20 --- 40 3020 20 40 30
--- --- --- ------ --- --- ------ --- --- ------ --- 30 --- --- --- --- ---X --- 30 X
--- --- --- ---X --- 30 XX 20 30 XX --- 30 X--- --- --- ------ --- --- ---X --- 30 X--- --- --- ---X 20 30 X
--- * Ə Ə Ə
--- X X X--- --- --- ------ 1000 1000 1000--- --- --- ------ --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DG57 DG58 DG59 DG60 DG61 DG62 DG68500 1000 1000 500¤ M ≈ ê ≈ ¤
₫ Ł џ ѓ
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X • X Þ X X • XX X --- --- X --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X
₫ Ł џ ѓ
X X X X X X XX X X X X X X
--- --- --- X X --- ---X X X X X X X
X^ X^ X X^ X^ X X^
X X X 20 X X X
X X X 20 20 X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X --- --- --- --- ---X X X // // --- X
₫ Ł џ ѓX X X 20 X X 25X X X 20 X X 25X X X 30 30 X 25X X X 30 30 X 25
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X --- X X 25X X X --- X X 25X X --- --- X --- 25X X X --- X X 25X X --- --- X --- 25
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X 20 X X 25X X --- --- X --- 25X X X --- X X 25
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X --- --- X --- 25--- --- --- --- --- --- ---X X X 20 X X 25
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DG57 DG58 DG59 DG60 DG61 DG62 DG68500 1000 1000 500¤ M ≈ ê ≈ ¤
₫ Ł џ ѓX X X --- X X 25X X X 20 X X 25X X --- 20 X X 25X X --- 20 X --- 25X X X 20 X X 25X X --- 20 X --- 25X X X 20 X X 25X X --- --- X --- 25
--- --- --- --- --- --- ------ --- --- --- --- --- ---X X --- --- X --- 25X X --- --- X --- 25X X --- --- X --- 25
--- --- --- --- --- --- ---X X X 20 X X 25
X X --- --- X --- 50X X --- 20 X --- 50
500 500
X X X --- X X XX X X 40 X X XX X X 40 X X XX X X --- X X XX X X 40 X X X
--- --- X --- --- X ---X X X 40 X X XX X X 40 X X XX X X --- X X XX X X 40 50 X 50X X --- 40 50 --- 50
--- --- --- --- --- --- ---X X --- --- X --- XX X X --- X X X
--- --- --- --- --- --- ---X X X 20 X X 25X X X 20 X X 25
™ ת ™800 500 500 --- 1000 500 800--- --- --- --- --- --- ------ --- X --- X X 50X X X --- X X 50--- --- X --- X X 50--- --- X --- X X 50X X X --- X X 50--- --- X --- X X 50--- --- X --- X X 50--- --- X --- X X 50--- --- X --- X --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- X --- 50X X --- 20 X --- 50--- --- --- --- --- --- ---X X X --- X X 50
@ @ ש500 500 800
--- --- --- --- --- --- ------ --- --- --- 50 --- 50--- --- --- --- 50 --- 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DG57 DG58 DG59 DG60 DG61 DG62 DG68500 1000 1000 500¤ M ≈ ê ≈ ¤
--- --- --- 20 50 --- 5025 25 --- 20 50 --- 5025 25 --- --- 50 --- 5025 25 --- --- 50 --- 50--- --- --- --- 50 --- 50--- --- --- --- 50 --- 50--- --- --- --- 50 --- 50--- --- --- --- 50 --- 50--- --- --- --- 50 --- 50--- --- --- --- 50 --- 50--- --- --- 20 » 50 --- 50 --- --- --- --- --- --- ---25 25 X 40 50 X 50--- --- --- --- 50 --- 5025 25 --- --- 50 --- 5025 25 X 40 50 X 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ---25 25 --- --- 50 --- 50--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---25 25 X 40 50 X 50 --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 5025 25 --- --- 50 --- 5025 25 --- --- 50 --- 50--- --- --- --- 50 --- 50--- --- --- --- 50 --- 5025 25 --- --- 50 --- 5025 25 --- --- 50 --- 50--- --- --- --- --- --- --- --- --- --- --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- 50 --- 5025 25 --- --- 50 --- 5025 25 --- --- 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- 50 --- 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DG57 DG58 DG59 DG60 DG61 DG62 DG68500 1000 1000 500¤ M ≈ ê ≈ ¤
25 25 --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 --- 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
X X X 20 30 X 25X X X 20 30 X 25--- --- --- --- --- --- ---X X X 20 30 X 25--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- X --- 30 X 25X X --- --- 30 --- 25--- --- --- --- --- --- ---X X X --- 30 X 25--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X --- --- 30 --- 25X X X 20 30 X 25
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- 20 X --- X--- --- --- --- --- X ---X X X --- X X XX X X 20 X X XX X X 20 X --- X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- X --- X--- --- --- --- --- --- ---X X X 20 X X X
--- --- --- Ə --- Ə
--- --- --- --- X --- 50--- --- --- --- --- --- ------ --- --- --- 1000 --- ------ --- --- --- --- --- 1000--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DG69 DG70 DG71 DG72 DG731500
ἆ ≈
X X X X XX X X X XX X X X X--- --- --- --- ---X --- X X ---
X X X X XX X X X XX X X X X--- --- --- --- ------ --- --- --- ---X X X X X--- --- --- --- ------ --- --- --- ------ --- --- --- --- --- --- --- --- ---X X X X X--- --- --- --- ---
--- --- --- --- --- --- --- --- --- ---X X X X X--- --- --- --- --- --- --- --- --- ---X X X X X
X X X X XX X X X X
--- X --- --- ---X X X X X
X^ X^ X^ X^ X^
X X X X X
20 20 20 20 30--- --- --- --- ------ --- --- --- ------ --- --- --- ---// // // // //
X X 20 X 20X X 20 X 2030 30 30 30 2030 30 30 30 20 --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- ---X X 20 X 20X X 20 X 20X X 20 X ---X X 20 X 20X X 20 X 20--- --- --- --- ------ --- --- --- ------ --- --- --- ---X X 20 X 20X X 20 X ---X X 20 X 20--- --- --- --- --- --- --- --- --- ---X X 20 X ------ --- --- --- ---X X // X 20
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DG69 DG70 DG71 DG72 DG731500
ἆ ≈
X X 30 X 20X X 30 X 20X X 30 X 20X X 30 X 20X X 30 X 20--- --- 30 X ---X X 30 X 20--- --- 30 X ------ --- --- --- ------ --- --- --- ---X X 30 X 20--- --- 30 X ---X X 30 X 20--- --- --- --- ---X X 30 X 20
50 --- X X ---50 --- X X ---
X X X X 40X X X X 40X X X X 40X X X X 40X X X X 40--- --- --- --- ---X X X X 40X X X X 40X X X X 4050 50 50 50 ---50 50 50 50 ------ --- --- --- ---X X X X 40X X X X 40
--- --- --- --- ---X X 20 X 20X X 20 X 20
1000 --- 1000 1000 ------ --- --- --- ---50 --- X X ---50 --- X X ---50 --- X X ---50 --- X X ---50 --- X X ---50 --- X X ---50 --- X X ---50 --- X X ---50 --- X X ------ --- --- --- ------ --- --- --- ---50 --- X X ---50 --- X X --- --- --- --- --- ---50 --- X X ---
--- --- --- --- ---57 57 57 57 ---50 50 50 50 ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DG69 DG70 DG71 DG72 DG731500
ἆ ≈
50 50 50 50 ---57 57 57 57 ---50 50 50 50 ---50 50 50 50 ---57 57 57 57 ---50 50 50 50 ---57 57 57 57 ---50 50 50 50 ---50 50 50 50 ---57 57 57 57 ---50 50 50 50 --- --- --- --- --- ---50 50 50 50 ---50 50 50 50 ---50 50 50 50 ---50 50 50 50 --- --- --- --- --- --- --- --- --- --- ---50 50 50 50 --- --- --- --- --- --- --- --- --- --- ------ --- --- --- ---50 50 50 50 4050 50 50 50 ---57 57 57 57 ------ --- --- --- ---50 50 50 50 ---57 57 57 57 ------ --- --- --- ---50 50 50 50 ---50 50 50 50 ---57 57 57 57 ---57 57 57 57 ---50 50 50 50 ---50 50 50 50 ---57 57 57 57 ---57 57 57 57 ---57 57 57 57 ---50 50 50 50 ---50 50 50 50 ---57 57 57 57 ---50 50 50 50 ---50 50 50 50 ---57 57 57 57 ---50 50 50 50 ---50 50 50 50 ---57 57 57 57 ---57 57 57 57 ---50 50 50 50 ---50 50 50 50 ------ --- --- --- ---57 57 57 57 ------ --- --- --- ------ --- --- --- ---50 50 50 50 ------ --- --- --- ------ --- --- --- ---50 50 50 50 ------ --- --- --- ------ --- --- --- ------ --- --- --- ---57 57 57 57 ------ --- --- --- ------ --- --- --- ---57 57 57 57 ---50 50 50 50 ---50 50 50 50 ------ --- --- --- ---50 50 50 50 ------ --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DG69 DG70 DG71 DG72 DG731500
ἆ ≈
57 57 57 57 ---50 50 50 50 ---57 57 57 57 --- --- --- --- --- --- --- --- --- --- ------ --- --- --- ---50 50 50 50 ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- ---
30 30 30 30 2030 30 30 30 20--- --- --- --- ---30 30 30 30 20--- --- --- --- ------ --- --- --- --- --- --- --- --- ------ --- 30 30 30--- --- 30 30 ------ --- --- --- ---30 30 30 30 30--- --- --- --- --- --- --- --- --- ---50 50 50 50 ------ --- --- --- ------ --- --- --- ------ --- --- --- ------ --- --- --- ------ --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- ------ --- --- --- ---30 30 30 30 3030 30 30 30 //
--- --- --- --- ------ --- --- --- ------ --- --- --- ------ --- --- --- --- --- --- --- --- ---X X 20 X ---
--- --- --- --- ---X X 20 X XX X 20 X XX X 20 X X--- --- --- --- ------ --- --- --- ------ --- 20 X ------ --- --- --- ---X X 20 X X
--- --- Ə --- ------ --- X --- ------ --- --- --- ------ --- 800 --- ------ --- --- --- ------ --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DG77 DG78 DG79 DG80 DG81 DG84 DG851000 1000 ≈ ŧ ≈
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X --- X
X X X X X X XX Þ X Þ X X X X X--- --- X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
--- --- X --- --- --- XX X X X X X X
X^ X^ X^ X^ X^ X^ X^
X X X X X X X
X X X X X 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X // //
20 20 30 25 X X 3020 20 30 25 X X 3020 20 30 25 30 30 3020 20 30 25 30 30 30X --- --- --- --- --- ---
--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- 30 25 X X 30--- --- 30 25 X X 30--- --- 30 25 X X 30--- --- 30 25 X X 3020 20 30 25 X X 3020 20 --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 20 30 25 X X 30--- --- 30 25 X X 30--- --- 30 25 X X 30--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- 30 25 X X 30--- --- --- --- --- --- ---20 20 30 25 X X 30
January 01, 2016
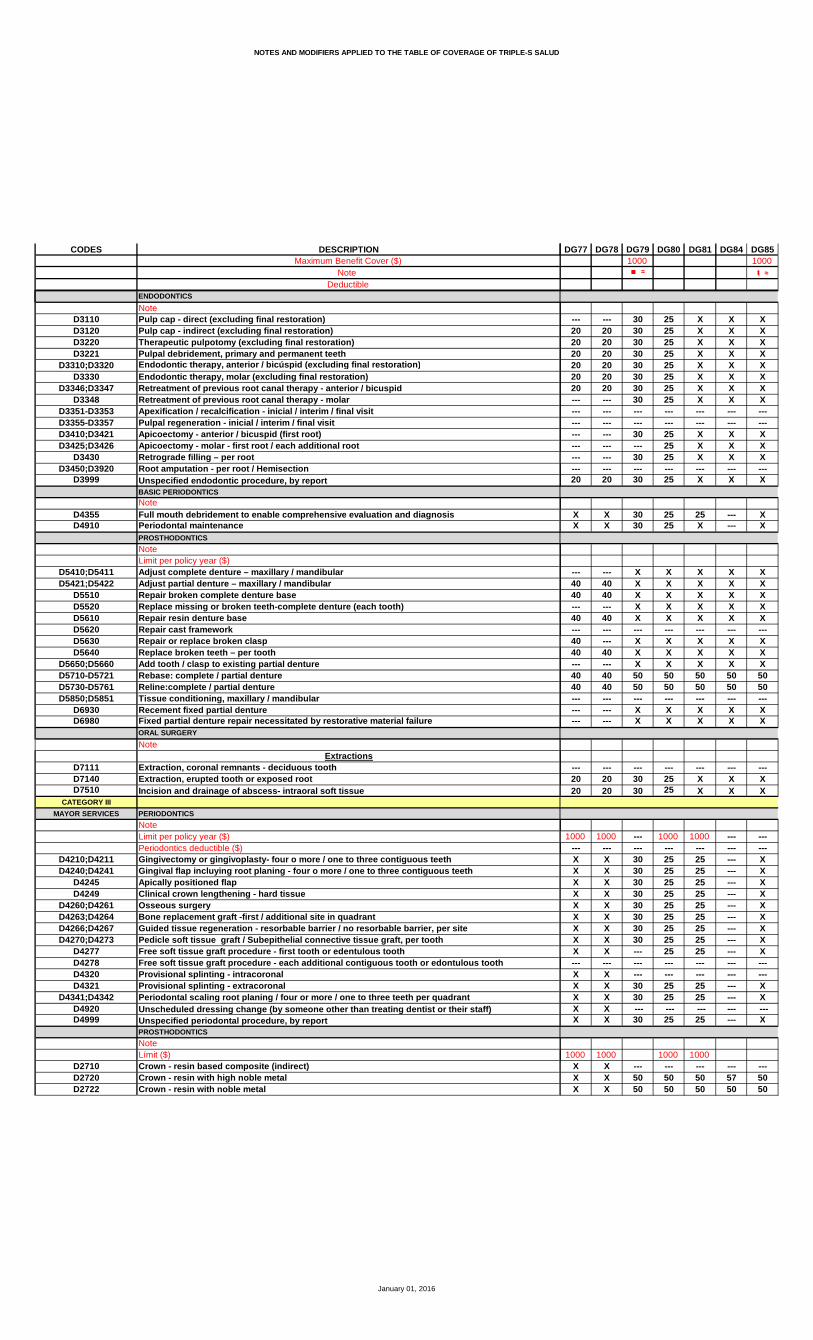
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DG77 DG78 DG79 DG80 DG81 DG84 DG851000 1000 ≈ ŧ ≈
--- --- 30 25 X X X20 20 30 25 X X X20 20 30 25 X X X20 20 30 25 X X X20 20 30 25 X X X20 20 30 25 X X X20 20 30 25 X X X--- --- 30 25 X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- 30 25 X X X--- --- --- 25 X X X--- --- 30 25 X X X--- --- --- --- --- --- ---20 20 30 25 X X X
X X 30 25 25 --- XX X 30 25 X --- X
--- --- X X X X X40 40 X X X X X40 40 X X X X X--- --- X X X X X40 40 X X X X X--- --- --- --- --- --- ---40 --- X X X X X40 40 X X X X X--- --- X X X X X40 40 50 50 50 50 5040 40 50 50 50 50 50--- --- --- --- --- --- ------ --- X X X X X--- --- X X X X X
--- --- --- --- --- --- ---20 20 30 25 X X X20 20 30 25 X X X
1000 1000 --- 1000 1000 --- ------ --- --- --- --- --- ---X X 30 25 25 --- XX X 30 25 25 --- XX X 30 25 25 --- XX X 30 25 25 --- XX X 30 25 25 --- XX X 30 25 25 --- XX X 30 25 25 --- XX X 30 25 25 --- XX X --- 25 25 --- X--- --- --- --- --- --- ---X X --- --- --- --- ---X X 30 25 25 --- XX X 30 25 25 --- XX X --- --- --- --- ---X X 30 25 25 --- X
1000 1000 1000 1000X X --- --- --- --- ---X X 50 50 50 57 50X X 50 50 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DG77 DG78 DG79 DG80 DG81 DG84 DG851000 1000 ≈ ŧ ≈
X X 50 50 50 50 50X X 50 50 50 57 50X X 50 50 50 50 50X X 50 50 50 50 50X X 50 50 50 57 50X X 50 50 50 50 50X X 50 50 50 57 50X X 50 50 50 50 50X X 50 50 50 50 50X X 50 50 50 57 50
X« X« 50 50 50 50 50X X --- --- --- --- ---X X 50 50 50 50 50X X 50 50 50 50 50X X 50 50 50 50 50X X 50 50 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X 50 50 50 50 50X X --- --- --- --- ---X X --- --- --- --- ---X X --- --- --- --- ---X X 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 57 50--- --- --- --- --- --- ------ --- 50 50 50 50 50--- --- 50 50 50 57 50--- --- --- --- --- --- ------ --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 57 50--- --- 50 50 50 57 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 57 50--- --- 50 50 50 57 50--- --- 50 50 50 57 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50--- --- 50 50 50 57 50--- --- 50 50 50 50 50--- --- 50 50 50 50 50X X 50 50 50 57 50X X 50 50 50 50 50X X 50 50 50 50 50X X 50 50 50 57 50X X 50 50 50 57 50X X 50 50 50 50 50X X 50 50 50 50 50X X --- --- --- --- ---X X 50 50 50 57 50X X --- --- --- --- ---X X --- --- --- --- ---X X 50 50 50 50 50X X --- --- --- --- ---X X --- --- --- --- ---X X 50 50 50 50 50X X --- --- --- --- ---X X --- --- --- --- ---X X --- --- --- --- ---X X 50 50 50 57 50X X --- --- --- --- ---X X --- --- --- --- ---X X 50 50 50 57 50X X 50 50 50 50 50X X 50 50 50 50 50X X --- --- --- --- ---X X 50 50 50 50 50X X --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DG77 DG78 DG79 DG80 DG81 DG84 DG851000 1000 ≈ ŧ ≈
X X 50 50 50 57 50X X 50 50 50 50 50X X 50 50 50 57 50X X --- --- --- --- ---X X --- --- --- --- ---X X --- --- --- --- ---X X 50 50 50 50 50
X X --- --- --- --- ---X X --- --- --- --- ---X X --- --- --- --- ---X X --- --- --- --- ---
--- --- --- --- --- --- ---
20 20 30 25 25 30 3020 20 30 25 25 30 30--- --- --- --- --- --- ---20 20 30 25 25 30 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- 25 25 30 30--- --- --- 25 25 30 30--- --- --- --- --- --- ------ --- 30 25 25 30 30--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- 50 50 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- 30 25 25 30 3020 20 30 25 25 30 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ 20 X X X X X --- --- --- --- --- --- ------ --- X X X X X20 20 X X X X X20 20 X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- X X X X--- --- --- --- --- --- ---20 20 X X X X X
Ə Ə --- Ə --- Ə
X X --- --- X --- 50--- --- --- --- --- --- ---
750 750 --- --- --- --- 1000--- --- --- --- 1500 --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DG87 DG88 DG89 DG90 DG91 DG92 DG931000 1000 800 1500 1000 1000 1000
Æ ≈ ≈ Ϟ ≈ Ñ ≈ ≈ ≈ ≈
X X X X 20 X XX X X X 20 X XX X X X 20 X X--- --- --- --- --- --- ---X X X X 20 X X
X X X X 20 X XX X X X 20 X XX X X X 20 X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X 20 X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 20 X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 20 X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X 20 X X
X X X X 20 X XX X X X 20 X X
X X X X X X XX X X X 20 X X
X^ X^ X^ X^ 20^ X^ X^
X X X X 20 X X
30 X 20 X 20 X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// X // X 20 X X
X 30 25 20 40 30 20X 30 25 20 40 30 2030 30 25 20 40 30 2030 30 25 20 40 30 20 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X 30 25 20 40 30 20X 30 25 20 40 30 20X 30 25 20 --- 30 20X 30 25 20 40 30 20X 30 25 20 40 30 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X 30 25 20 40 30 20X 30 25 20 --- 30 20X 30 25 20 40 30 20--- --- --- --- --- --- --- --- --- --- --- --- --- ---X 30 25 20 --- 30 20--- --- --- --- --- --- ---X 30 25 20 40 30 20
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DG87 DG88 DG89 DG90 DG91 DG92 DG931000 1000 800 1500 1000 1000 1000
Æ ≈ ≈ Ϟ ≈ Ñ ≈ ≈ ≈ ≈
X 30 25 20 40 30 20X 30 25 20 40 30 20X 30 25 20 40 30 20X 30 25 20 40 30 20X 30 25 20 40 30 20X 30 25 20 40 30 20X 30 25 20 40 30 20X 30 25 20 40 30 20--- --- --- --- --- --- ------ --- --- --- --- --- ---X 30 25 20 40 30 20X 30 25 20 40 30 20X 30 25 20 40 30 20--- --- --- --- --- --- ---X 30 25 20 40 30 20
X 30 30 20 40 30 20X 30 30 20 40 30 20
X X 30 X X X XX X 30 X X X XX X 30 X X X XX X 30 X X X XX X 30 X X X X--- --- --- --- --- --- ---X X 30 X X X XX X 30 X X X XX X 30 X X X X50 50 50 50 --- 50 5050 50 50 50 --- 50 50--- --- --- --- --- --- ---X X 30 X X X XX X 30 X X X X
--- --- --- --- --- --- ---30 30 25 20 X X X30 30 25 20 X X X
1000 --- --- --- --- --- ------ --- --- --- --- --- ---X 30 30 20 40 30 20X 30 30 20 40 30 20X 30 30 20 40 30 20X 30 30 20 40 30 20X 30 30 20 40 30 20X 30 30 20 40 30 20X 30 30 20 40 30 20X 30 30 20 40 30 20X 30 30 20 40 30 20--- --- --- --- --- ------ --- --- --- --- --- ---X 30 30 20 40 30 20X 30 30 20 40 30 20
--- --- --- --- --- --- ---X 30 30 20 40 30 20
--- --- --- --- --- --- ---50 50 50 50 --- 50 5050 50 50 50 --- 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DG87 DG88 DG89 DG90 DG91 DG92 DG931000 1000 800 1500 1000 1000 1000
Æ ≈ ≈ Ϟ ≈ Ñ ≈ ≈ ≈ ≈
50 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 50 --- --- --- --- --- --- ---50 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 50 50 --- 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 X 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 50--- --- --- --- --- --- ---50 50 50 50 --- 50 5050 50 50 50 --- 50 50--- --- --- --- --- --- ---50 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 50--- --- --- --- --- --- ---50 50 50 50 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 50--- --- --- --- --- --- ---50 50 50 50 --- 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DG87 DG88 DG89 DG90 DG91 DG92 DG931000 1000 800 1500 1000 1000 1000
Æ ≈ ≈ Ϟ ≈ Ñ ≈ ≈ ≈ ≈
50 50 50 50 --- 50 5050 50 50 50 --- 50 5050 50 50 50 --- 50 50--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 --- 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
30 30 30 20 40 30 2030 30 30 20 40 30 20--- --- --- --- --- --- ---30 30 30 20 40 30 20--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---30 30 30 20 40 30 2030 30 --- 20 --- 30 20--- --- --- --- --- --- ---30 30 30 20 40 30 20--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 50 50 --- 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- 30 --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- 30 --- --- --- ------ --- --- --- --- --- ---30 30 30 20 40 30 2030 30 30 20 40 30 20
--- --- --- 20 --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X 20 --- X X
--- --- --- --- --- --- ---X X X 20 X X XX X X 20 X X XX X X 20 X X X--- --- --- 20 --- --- ------ --- --- --- --- --- ---X X X 20 --- X X--- --- --- --- --- --- ---X X X 20 X X X
Ə Ə --- Ə --- Ə Ə
50 X --- 50 --- X X--- --- --- --- --- --- ---
1000 1000 --- 1500 --- 1000 1000--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DG94 DG95 DG981000 1000
≈ ≈
X X XX X XX X X--- --- ---X X X
X X XX X XX X X--- --- ------ --- ---X X X--- --- ------ --- ------ --- --- --- --- ---X X X--- --- ---
--- --- --- --- --- ---X X X--- --- --- --- --- ---X X X
X X XX X X
X --- XX X X
X^ X^ X^
X X X
X 20 X--- --- ------ --- ---X --- ---X // ---
X 30 30X 30 3030 30 3030 30 30 --- --- --- --- --- ------ --- --- --- --- ---X 30 30X 30 30X 30 30X 30 30X 30 30--- --- ------ --- ------ --- ---X 30 30X 30 30X 30 30--- --- --- --- --- ---X 30 30--- --- ---X 30 30
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DG94 DG95 DG981000 1000
≈ ≈
30 30 3030 30 3030 30 3030 30 3030 30 3030 30 3030 30 3030 30 30--- --- ------ --- ---30 30 30--- 30 3030 30 30--- --- ---30 30 30
30 X 3030 X 30
X X XX X XX X ---X X ---X X ------ --- ---X X ---X X ---X X ---50 50 ---50 50 ---50 --- ---X X XX X X
--- --- ---X 30 30X 30 30
--- 1000 ------ --- ---30 X 3030 X 3030 X 3030 X 3030 X ---30 X 3030 X 3030 X 3030 X 30--- --- ------ --- ---30 X 3030 X --- --- --- ---30 X 30
--- --- ---57 57 ---50 50 ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DG94 DG95 DG981000 1000
≈ ≈
50 50 ---57 57 ---50 50 ---50 50 ---57 57 ---50 50 ---57 57 ---50 50 ---50 50 ---57 57 ---50 50 --- --- --- ---50 50 ---50 50 ---50 50 ---50 50 --- --- --- --- --- --- ---50 50 --- --- --- --- --- --- ------ --- ---50 50 ---50 50 ---57 57 ------ --- ---50 50 ---57 57 ------ --- ---50 50 ---50 50 ---57 57 ---57 57 ---50 50 ---50 50 ---57 57 ---57 57 ---57 57 ---50 50 ---50 50 ---57 57 ---50 50 ---50 50 ---57 57 ---50 50 ---50 50 ---57 57 ---57 57 ---50 50 ---50 50 ------ --- ---57 57 ------ --- ------ --- ---50 50 ------ --- ------ --- ---50 50 ------ --- ------ --- ------ --- ---57 57 ------ --- ------ --- ---57 57 ---50 50 ---50 50 ------ --- ---50 50 ------ --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DG94 DG95 DG981000 1000
≈ ≈
57 57 ---50 50 ---57 57 --- --- --- --- --- --- ------ --- ---50 50 ---
--- --- --- --- --- --- --- --- --- --- --- ---
--- --- ---
30 30 ---30 30 ------ --- ---30 30 ------ --- ------ --- --- --- --- ------ 30 ------ 30 ------ --- ---30 30 ------ --- --- --- --- ---50 50 ---30 --- ---30 --- ---30 --- ------ --- ------ --- --- --- --- ------ --- --- --- --- --- --- --- ---30 --- ------ --- ---30 30 ---30 30 ---
--- --- ------ --- ------ --- ------ --- --- --- --- ---X X X
--- --- ---X X XX X XX X X--- --- ------ --- ------ X X--- --- ---X X X
--- Ə Ə
--- 50 50--- --- ------ 1500 1000--- --- ------ --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DG99 DH01 DH02 DH03 DH04 DH05 DH061250 1250
♠ ≈ ♠ ≈
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X --- X 30 --- X
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- 30 --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- 30 Ð --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
X X --- --- --- --- ---X X X X X X X
X^ X^ X^ X^ X^ X^ X^
X X X X X X X
X X 20 20 X X X--- --- --- --- 30 --- ------ --- --- --- 30 --- ------ --- --- --- 30 --- ------ --- // // // X X
30 20 X X X X X30 20 X X X X X30 20 30 X X X X30 20 30 X X X X --- --- --- --- --- --- ---50 50 --- --- --- --- ---50 50 --- --- --- --- ---50 50 --- --- --- --- ---30 20 X X X X X30 20 X X 30 X X30 20 X X X X X30 20 X X 30 X X30 20 X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 20 X X X X X30 20 X X 30 X X30 20 X X 30 X X--- --- --- --- --- --- ------ --- --- --- --- --- ---30 20 X X X X X--- --- --- --- --- --- ---30 20 X X X X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DG99 DH01 DH02 DH03 DH04 DH05 DH061250 1250
♠ ≈ ♠ ≈
30 20 X 20 40 X X30 20 X 20 X X X30 20 X 20 X X X30 20 X 20 X X X30 20 X 20 X X X30 20 --- 20 X X X30 20 X 20 40 X X30 20 --- 20 40 --- X--- --- --- --- 40 --- ------ --- --- --- --- --- ---30 20 X 20 40 X X30 20 --- 20 --- --- X30 20 X 20 40 X X--- --- --- --- --- --- ---30 20 X 20 X X X
30 20 --- 20 50 --- X30 20 --- 20 50 --- X
X X X 30 50 X XX X X 30 50 X X50 50 X 30 50 X X50 50 X 30 50 X X50 50 X 30 50 X X--- --- --- --- 50 --- ---50 50 X 30 50 X X50 50 X 30 50 X X50 50 X 30 50 X X50 50 50 30 50 50 5050 50 50 30 50 50 50--- --- --- --- 50 --- ---X X X 30 50 X XX X X 30 50 X X
--- --- --- --- --- --- ---30 20 X 20 X X X30 20 X 20 X X X
--- --- --- --- 1000 --- 1000--- --- --- --- --- --- ---30 20 --- 20 50 --- X30 20 --- 20 50 --- X30 20 --- 20 50 --- X30 20 --- 20 50 --- X50 50 --- 20 50 --- X30 20 --- 20 50 --- X30 20 --- 20 50 --- X30 20 --- 20 --- --- X30 20 --- 20 --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---30 20 --- 20 50 --- X50 50 --- 20 50 --- X --- --- --- --- --- --- ---// // --- 20 50 --- X
--- --- --- --- --- --- ---50 50 57 30 50 57 5750 50 50 30 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DG99 DH01 DH02 DH03 DH04 DH05 DH061250 1250
♠ ≈ ♠ ≈
50 50 50 30 50 50 5050 50 57 30 50 57 5750 50 50 30 50 50 5050 50 50 30 50 50 5050 50 57 30 50 57 5750 50 50 30 50 50 5050 50 57 30 50 57 5750 50 50 30 50 50 5050 50 50 30 50 50 5050 50 57 30 50 57 5750 50 50 30 50 50 50 --- --- --- --- --- --- ---50 50 50 30 50 50 5050 50 50 30 50 50 5050 50 50 30 50 50 5050 50 50 30 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 50 30 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 30 50 50 5050 50 50 30 50 50 5050 50 57 30 50 57 57--- --- --- --- 50 --- ---50 50 50 30 50 50 5050 50 57 30 50 57 57--- --- --- --- 50 --- ---50 50 50 30 50 50 5050 50 50 30 50 50 5050 50 57 30 50 57 5750 50 57 30 50 57 5750 50 50 30 50 50 5050 50 50 30 50 50 5050 50 57 30 50 57 5750 50 57 30 50 57 5750 50 57 30 50 57 5750 50 50 30 50 50 5050 50 50 30 50 50 5050 50 57 30 50 57 5750 50 50 30 50 50 5050 50 50 30 50 50 5050 50 57 30 50 57 5750 50 50 30 50 50 5050 50 50 30 50 50 5050 50 57 30 50 57 5750 50 57 30 50 57 5750 50 50 30 50 50 5050 50 50 30 50 50 50--- --- --- --- --- --- ---50 50 57 30 50 57 57--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 30 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 30 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 57 30 50 57 57--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 57 30 50 57 5750 50 50 30 50 50 5050 50 50 30 50 50 50--- --- --- --- --- --- ---50 50 50 30 50 50 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DG99 DH01 DH02 DH03 DH04 DH05 DH061250 1250
♠ ≈ ♠ ≈
50 50 57 30 50 57 5750 50 50 30 50 50 5050 50 57 30 50 57 57--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 30 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
250050 50 --- X --- --- ---
50 50 30 30 X X X50 50 30 30 X X X--- --- --- --- --- --- ---50 50 30 30 X X X--- --- --- --- 30 --- ------ --- --- --- 30 --- --- --- --- --- --- --- --- ---50 50 --- 30 30 --- 3050 50 --- --- 30 --- 30--- --- --- --- 30 --- ---50 50 30 30 30 30 30--- --- --- --- 30 --- --- --- --- --- --- --- --- ---50 50 50 30 50 50 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- 30 --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- 30 30 --- ------ --- --- --- 30 --- ---50 50 30 30 30 30 3050 50 30 30 X X X
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- 30 --- --- --- --- --- --- --- --- ---X X X X X X X
--- --- --- --- --- --- ---X X X X 30 X XX X X X X X XX X X X X X X50 50 --- --- --- --- ------ --- --- --- --- --- ---X X --- X 30 --- X--- --- --- --- --- --- ---// // X X X X X
Ə Ə Ə Ə Ə --- Ə
50 50 50 X X --- X--- --- --- --- --- --- ---
1000 1000 1000 2500 1000 --- 1000--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DH07 DH08 DH09 DH11750
ij ≈
X X X 30X X X 30X X X 30--- --- --- ---X X --- 30
X X X 30X X X 30 ÞX X --- ------ --- --- ------ --- --- ---X X X 30--- --- --- ------ --- --- ------ --- --- --- --- --- --- ---X X X 30--- --- --- ---
--- --- --- --- --- --- --- ---X X --- 30--- --- --- --- --- --- --- ---X X --- 30
X X X 30X X X 30
--- --- XX X X 30
X^ X^ X^ 30^
X X X 30
X X --- 30--- --- --- ------ --- --- ------ --- --- ---X X --- 30
X X --- 30X X --- 3030 30 --- 3030 30 --- 30 --- --- --- --- --- --- --- ------ --- --- --- --- --- --- ---X X --- ---X X --- ---X X --- ---X X --- ---X X --- ------ --- --- ------ --- --- ------ --- --- ---X X --- 30X X --- ---X X --- ------ --- --- --- --- --- --- ---X X --- ---
--- --- --- ---X X --- 30
January 01, 2016
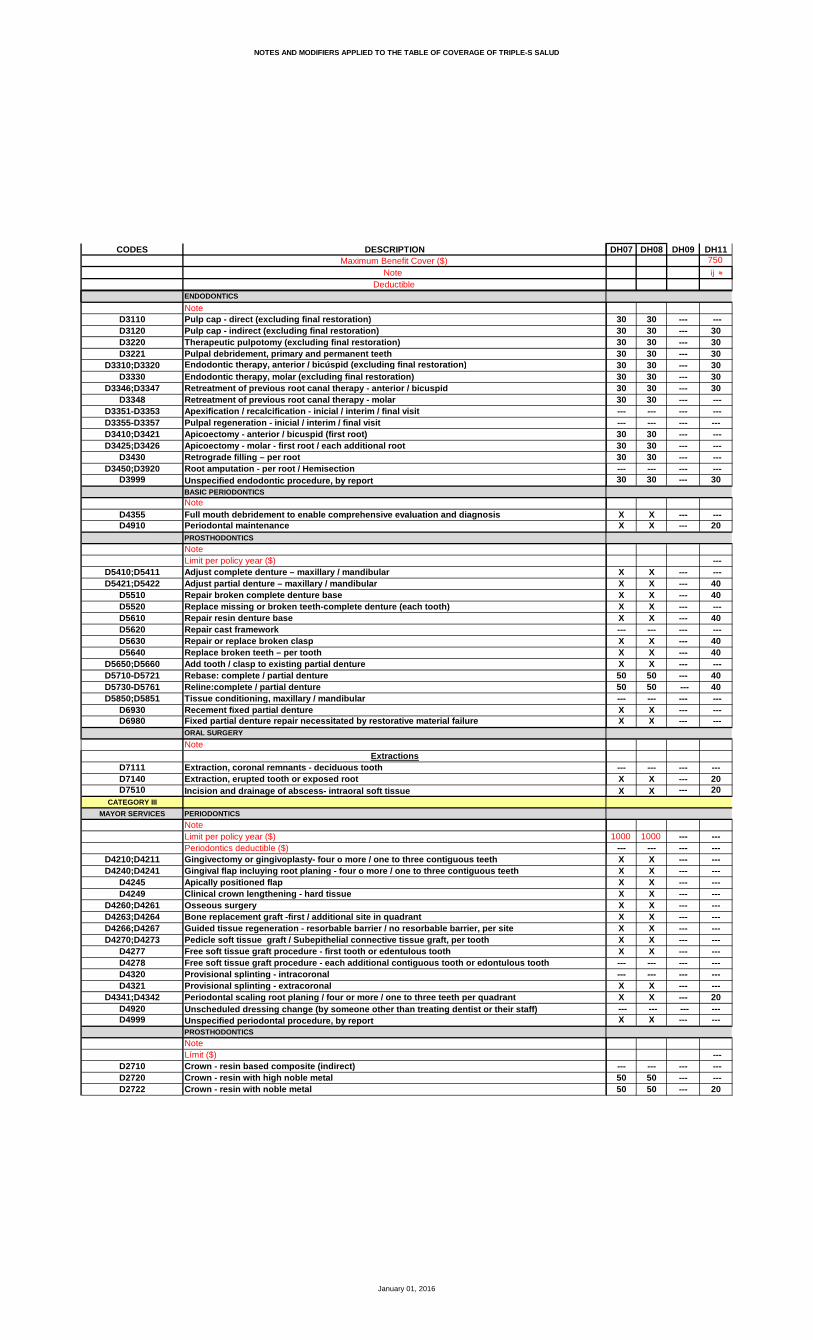
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DH07 DH08 DH09 DH11750
ij ≈
30 30 --- ---30 30 --- 3030 30 --- 3030 30 --- 3030 30 --- 3030 30 --- 3030 30 --- 3030 30 --- ------ --- --- ------ --- --- ---30 30 --- ---30 30 --- ---30 30 --- ------ --- --- ---30 30 --- 30
X X --- ---X X --- 20
---X X --- ---X X --- 40X X --- 40X X --- ---X X --- 40--- --- --- ---X X --- 40X X --- 40X X --- ---50 50 --- 4050 50 --- 40--- --- --- ---X X --- ---X X --- ---
--- --- --- ---X X --- 20X X --- 20
1000 1000 --- ------ --- --- ---X X --- ---X X --- ---X X --- ---X X --- ---X X --- ---X X --- ---X X --- ---X X --- ---X X --- ------ --- --- ------ --- --- ---X X --- ---X X --- 20
--- --- --- ---X X --- ---
------ --- --- ---50 50 --- ---50 50 --- 20
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DH07 DH08 DH09 DH11750
ij ≈
50 50 --- 2050 50 --- ---50 50 --- ---50 50 --- 2050 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- --- --- --- --- ---50 50 --- 4050 50 --- ---50 50 --- ---50 50 --- 40 --- --- --- --- --- --- --- ---50 50 --- --- --- --- --- --- --- --- --- ------ --- --- ---50 50 --- 4050 50 --- ---50 50 --- ------ --- --- ---50 50 --- ---50 50 --- ------ --- --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- ------ --- --- ---50 50 --- ------ --- --- ------ --- --- ---50 50 --- ------ --- --- ------ --- --- ---50 50 --- ------ --- --- ------ --- --- ------ --- --- ---50 50 --- ------ --- --- ------ --- --- ---50 50 --- ---50 50 --- ---50 50 --- ------ --- --- ---50 50 --- ------ --- --- ---
January 01, 2016
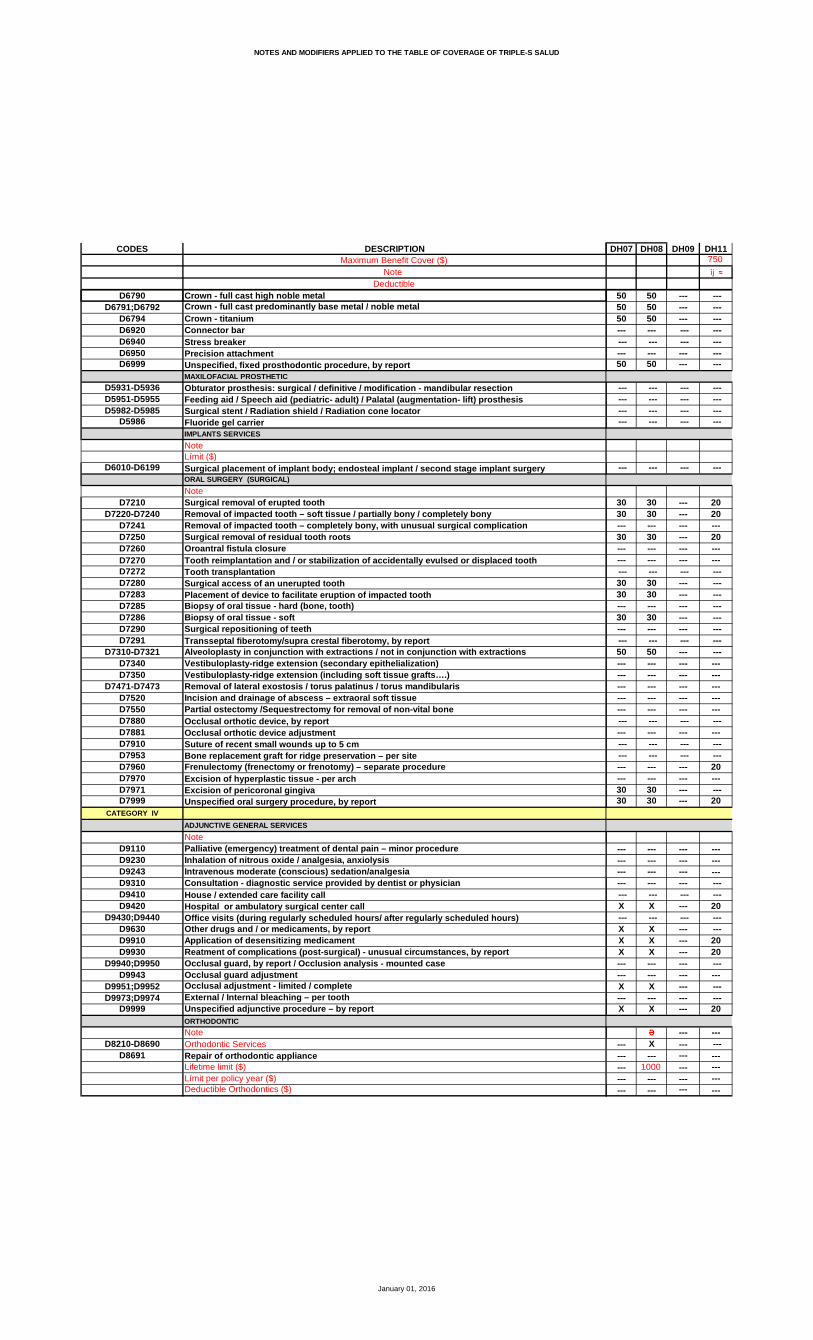
NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DH07 DH08 DH09 DH11750
ij ≈
50 50 --- ---50 50 --- ---50 50 --- ------ --- --- --- --- --- --- ------ --- --- ---50 50 --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- ---
30 30 --- 2030 30 --- 20--- --- --- ---30 30 --- 20--- --- --- ------ --- --- --- --- --- --- ---30 30 --- ---30 30 --- ------ --- --- ---30 30 --- ------ --- --- --- --- --- --- ---50 50 --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- ------ --- --- 20--- --- --- ---30 30 --- ---30 30 --- 20
--- --- --- ------ --- --- ------ --- --- ------ --- --- --- --- --- --- ---X X --- 20
--- --- --- ---X X --- ---X X --- 20X X --- 20--- --- --- ------ --- --- ---X X --- ------ --- --- ---X X --- 20
Ə --- ------ X --- ------ --- --- ------ 1000 --- ------ --- --- ------ --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DH12 DH13 DH14 DH17 DH18 DH19 DH201000 1000 1000 1000
ϰ ≈ U ≈ U ≈ ê ≈
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X X X X X ---
X X X X X X XX Þ X Þ X X X Þ X X--- --- X X --- X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
X --- X X --- --- XX X X X X X X
X^ X^ X^ X^ X^ X^ X^
20 20 X --- 20 X X
20 20 20 30 20 20 X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---// // // // // // X
20 20 X 30 20 X X20 20 X X 20 X X30 20 30 30 30 X 3030 20 30 30 30 X 30 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- X X --- X X --- --- X X --- X X --- --- X X --- X --- --- --- X X --- X X --- --- X X --- X X --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 X X 20 X X --- --- X X --- X --- --- --- X X --- X X--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- X X --- X ------ --- --- --- --- --- ---20 20 X X 20 X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DH12 DH13 DH14 DH17 DH18 DH19 DH201000 1000 1000 1000
ϰ ≈ U ≈ U ≈ ê ≈
--- --- X X --- X X20 20 X X 20 X X20 20 X X 20 X X20 20 X X 20 X X20 20 X X 20 X X20 20 X 50 20 X ---20 20 X X 20 X X --- --- X 50 --- X --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- X 30 --- X X --- --- X --- --- X --- --- --- X X --- X X --- --- --- --- --- --- ---20 20 X X 20 X X
--- --- 30 50 --- X ---20 20 30 50 20 X ---
1000 --- 1000 --- --- X X --- X X40 30 X X 40 X X40 30 X X 40 X X --- --- X X --- X X40 30 X X 40 X X --- --- --- --- --- --- ---40 30 X X 40 X X40 30 X X 40 X X --- --- X X --- X X40 30 50 --- 40 50 ---40 30 50 --- 40 50 --- --- --- --- --- --- --- --- --- --- X X --- X X --- --- X X --- X X
--- --- --- --- --- --- ---20 20 X 30 20 X X20 20 X 30 20 X X
--- --- --- --- 1000 ------ --- --- --- --- --- ------ --- 30 50 --- X ------ --- 30 50 --- X ------ --- 30 50 --- X ------ --- 30 50 --- X ------ --- 30 50 --- X ------ --- 30 50 --- X ------ --- 30 50 --- X ------ --- 30 50 --- X ------ --- 30 50 --- X ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- 30 50 --- X ---20 20 30 50 20 X ------ --- --- --- --- --- ------ --- 30 50 --- X ---
1000 --- 1000 --- --- --- --- --- --- --- --- 50 50 50 --- 50 ---20 50 50 50 20 50 ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DH12 DH13 DH14 DH17 DH18 DH19 DH201000 1000 1000 1000
ϰ ≈ U ≈ U ≈ ê ≈
20 50 50 50 20 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 ---20 50 50 50 20 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- --- --- --- --- --- ---40 30 50 50 40 50 --- --- 30 50 50 --- 50 --- --- 30 50 50 --- 50 ---40 30 50 50 40 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 30 50 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---40 50 50 50 40 50 X --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- --- --- --- --- --- --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- --- --- --- --- --- --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- --- --- --- --- --- --- --- 50 50 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- --- --- --- --- --- --- --- 50 50 50 --- 50 --- --- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DH12 DH13 DH14 DH17 DH18 DH19 DH201000 1000 1000 1000
ϰ ≈ U ≈ U ≈ ê ≈
--- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- 50 50 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 50 --- 50 ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
20 20 30 30 20 X 3020 20 30 30 20 X 30--- --- --- --- --- --- ---20 20 30 30 20 X 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 30 30 --- X 30 --- --- 30 30 --- X --- --- --- --- --- --- --- --- --- --- 30 30 --- X 30 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- 50 50 --- 50 ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 --- --- 20 --- ------ --- --- --- --- --- --- --- --- 30 30 --- X 3020 20 30 30 20 X 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---20 20 X X 20 X --- --- --- --- --- --- --- --- --- --- X X --- X X20 20 X X 20 X X20 20 X X 20 X X --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- X X --- X --- --- --- --- --- --- --- ---20 20 X X 20 X X
Ə Ə Ə Ə --- Ə ---50 X X X --- X ------ --- --- --- --- --- ---
1000 2000 1500 1500 --- 800 ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DH21 DH22 DH23
X X XX X XX X X--- --- ---X X X
X X XX X XX X X--- --- ------ --- ---X X X--- --- ------ --- ------ --- --- --- --- ---X X X--- --- ---
--- --- --- --- --- ---X X X--- --- --- --- --- ---X X X
X X XX X X
--- --- ---X X X
X^ X^ X^
X X X
X 20 20--- --- ------ --- ------ --- ---X // //
25 X 3025 X 3025 30 3025 30 30 --- --- --- --- --- ------ --- --- --- --- ---25 X 3025 X 3025 X 3025 X 3025 X 30--- --- ------ --- ------ --- ---25 X 3025 X 3025 X 30--- --- --- --- --- ---25 X 30--- --- ---25 X 30
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DH21 DH22 DH23
25 X 3025 X 3025 X 3025 X 3025 X 3025 X 3025 X 3025 X 30--- --- ------ --- ---25 X 3025 X 3025 X 30--- --- ---25 X 30
50 X X50 X X
X X XX X XX X XX X XX X X--- --- ---X X XX X XX X X50 50 5050 50 50--- --- ---X X XX X X
--- --- ---25 X 3025 X 30
ת800 1000 1000--- --- ---50 X X50 X X50 X X50 X X50 X X50 X X50 X X50 X X50 X X--- --- ------ --- ---50 X X50 X X --- --- ---50 X X
ש800--- --- ---50 57 ---50 50 ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DH21 DH22 DH23
50 50 ---50 57 ---50 50 ---50 50 ---50 57 ---50 50 ---50 57 ---50 50 ---50 50 ---50 57 ---50 50 --- --- --- ---50 50 ---50 50 ---50 50 ---50 50 --- --- --- --- --- --- ---50 50 --- --- --- --- --- --- ------ --- ---50 50 ---50 50 ---50 57 ------ --- ---50 50 ---50 57 ------ --- ---50 50 ---50 50 ---50 57 ---50 57 ---50 50 ---50 50 ---50 57 ---50 57 ---50 57 ---50 50 ---50 50 ---50 57 ---50 50 ---50 50 ---50 57 ---50 50 ---50 50 ---50 57 ---50 57 ---50 50 ---50 50 ------ --- ---50 57 ------ --- ------ --- ---50 50 ------ --- ------ --- ---50 50 ------ --- ------ --- ------ --- ---50 57 ------ --- ------ --- ---50 57 ---50 50 ---50 50 ------ --- ---50 50 ------ --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DH21 DH22 DH23
50 57 ---50 50 ---50 57 ------ --- --- --- --- ------ --- ---50 50 ---
--- --- --- --- --- --- --- --- --- --- --- ---
--- --- ---
25 30 3025 30 30--- --- ---25 30 30--- --- ------ --- --- --- --- ---25 30 3025 30 30--- --- ---25 30 30--- --- --- --- --- ---50 50 ------ --- ------ --- ------ --- ------ --- ------ --- --- --- --- ------ --- --- --- --- --- --- --- ------ --- ------ --- ---25 30 3025 30 30
--- --- ------ --- ------ --- ------ --- --- --- --- ---X X X
--- --- ---X X XX X XX X X--- --- ------ --- ---X X X--- --- ---X X X
Ə ---50 --- ------ --- ---
1000 --- ------ --- ------ --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DH24 DH25 DH26 DH27 DH28 DH29 DH30750 1000 1500 1000 1300
ij ≈ U ≈ Ñ ≈ M ≈ C ≈
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X X --- --- X --- X
X X --- X X X XX X X δ X X X XX X --- X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X 30 X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- ------ --- --- --- --- --- ---X X --- X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X 30 X X X X
X X X X X X XX X X X X X X
--- X --- X X --- XX X X X X X X--- X^ 30^ X^ X^ X^ X^
--- X --- X X X X
X 20 --- 20 X 20 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X // // // X // //
X X 30 X 20 X XX X 30 X 20 X X30 30 30 30 20 30 3030 30 30 30 20 30 30--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X --- X 20 X XX X --- X 20 X XX X --- --- 20 --- XX X --- X 20 X XX X --- X 20 X X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X 30 X 20 X XX X --- --- 20 --- XX X 30 X 20 X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X --- --- 20 --- X--- --- --- --- --- --- ---X X 30 X 20 X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DH24 DH25 DH26 DH27 DH28 DH29 DH30750 1000 1500 1000 1300
ij ≈ U ≈ Ñ ≈ M ≈ C ≈
X X 30 X 20 X XX X 30 X 20 X XX X --- X 20 X XX X 30 X 20 X XX X --- X 20 X XX --- --- --- 20 --- XX X --- X 20 X XX --- --- --- 20 --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X --- X 20 X XX --- --- --- 20 --- XX X --- X 20 X X--- --- --- --- --- --- ---X X --- X 20 X X
X 20 --- --- 20 --- XX 20 --- --- 20 --- X
X X --- X X X XX X --- X X X XX X --- X X X XX X --- X X X XX X --- X X X X--- --- --- --- --- --- ---X X --- X X X XX X --- X X X XX X --- X X X XX 50 --- --- 50 --- 50X 50 --- --- 50 --- 50--- --- --- --- --- --- ---X X --- X X X XX X --- X X X X
--- --- --- --- --- --- ---X X 30 X 20 X XX X 30 X 20 X X
1000 --- --- --- --- --- 100050 --- --- --- --- --- ---X 20 --- --- 20 --- XX 20 --- --- 20 --- XX 20 --- --- 20 --- XX 20 --- --- 20 --- XX 20 --- --- 20 --- XX 20 --- --- 20 --- XX 20 --- --- 20 --- XX 20 --- --- 20 --- XX 20 --- --- 20 --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---X 20 --- --- 20 --- XX 20 --- --- 20 --- X--- --- --- --- --- --- ---X 20 --- --- 20 --- X
--- --- --- --- --- --- ---30 50 --- --- 50 --- 5030 50 --- --- 50 --- 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DH24 DH25 DH26 DH27 DH28 DH29 DH30750 1000 1500 1000 1300
ij ≈ U ≈ Ñ ≈ M ≈ C ≈
30 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 50--- --- --- --- --- --- ---30 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ---30 50 --- --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 50 --- X 50 X 50--- 50 --- --- 50 --- 50--- 50 --- --- 50 --- 50--- --- --- --- --- --- ------ 50 --- --- 50 --- 50--- 50 --- --- 50 --- 50--- --- --- --- --- --- ------ 50 --- --- 50 --- 50--- 50 --- --- 50 --- 50--- 50 --- --- 50 --- 50--- 50 --- --- 50 --- 50--- 50 --- --- 50 --- 50--- 50 --- --- 50 --- 50--- 50 --- --- 50 --- 50--- 50 --- --- 50 --- 50--- 50 --- --- 50 --- 50--- 50 --- --- 50 --- 50--- 50 --- --- 50 --- 50--- 50 --- --- 50 --- 50--- 50 --- --- 50 --- 50--- 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 50--- --- --- --- --- --- ---30 50 --- --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---30 50 --- --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---30 50 --- --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 50 --- --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---30 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 50--- --- --- --- --- --- ---30 50 --- --- 50 --- 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DH24 DH25 DH26 DH27 DH28 DH29 DH30750 1000 1500 1000 1300
ij ≈ U ≈ Ñ ≈ M ≈ C ≈
30 50 --- --- 50 --- 5030 50 --- --- 50 --- 5030 50 --- --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---30 50 --- --- 50 --- 50
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---
--- --- --- --- --- --- ---
X 30 30 30 20 30 30X 30 30 30 20 30 30--- --- --- --- --- --- ---X 30 30 30 20 30 30--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X --- --- 30 20 30 30X --- --- --- 20 --- 30--- --- --- --- --- --- ---X 30 --- 30 20 30 30--- --- --- --- --- --- ------ --- --- --- --- --- ---30 50 --- --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X 30 --- 30 20 30 30X 30 30 30 20 30 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ X 30 --- X --- X--- --- --- --- --- --- ---X X --- X X X XX X 30 X X X XX X 30 X X X X--- --- --- --- --- --- ------ --- --- --- --- --- ---X --- --- --- X --- X--- --- --- --- --- --- ---X X 30 X X X X
--- --- --- Ə Ə --- Ə
--- --- --- X X --- X--- --- --- --- --- --- ------ --- --- 1000 1000 --- 1000--- --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DH31 DH32 DH33 DH34 DH35 DH361300 800 1000 1500
C ≈ ⱴ ≈ M ≈ ∻
≙
X X X 20 X XX X X 20 X XX X X 20 X X--- --- --- --- --- ---X X X 20 X X
X X X 20 X XX X X 20 X Þ XX X X 20 --- X--- --- --- --- --- ------ --- --- --- --- ---X X X 20 X X--- --- --- --- --- ------ --- --- --- --- X--- --- --- --- --- X --- --- --- --- --- ---X X X 20 X X--- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- ---X X X 20 X X--- --- --- --- --- --- --- --- --- --- --- ---X X X 20 X X
X X X 20 X XX X X 20 X X
X --- --- --- --- XX X X 20 X X
X^ X^ X^ 20^ X^ X^
X X X 20 X X
20 X X 20 X X--- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ---// X X 20 X X
X 25 25 25 30 20X 25 25 25 30 2030 25 25 30 30 2030 25 25 30 30 20 --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- ---X 25 25 25 --- 20X 25 25 25 --- 20X 25 25 25 --- 20X 25 25 25 --- 20X 25 25 25 --- 20--- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ---X 25 25 25 30 20X 25 25 25 --- 20X 25 25 25 --- 20--- --- --- --- --- --- --- --- --- --- --- ---X 25 25 25 --- 20--- --- --- --- --- ---X 25 25 25 30 20
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DH31 DH32 DH33 DH34 DH35 DH361300 800 1000 1500
C ≈ ⱴ ≈ M ≈ ∻
≙
X 25 25 25 --- 20X 25 25 25 30 20X 25 25 25 30 20X 25 25 25 30 20X 25 25 25 30 20X 25 25 25 30 20X 25 25 25 30 20X 25 25 25 --- 20--- --- --- --- --- ------ --- --- --- --- ---X 25 25 25 --- 20X 25 25 25 --- 20X 25 25 25 --- 20--- --- --- --- --- ---X 25 25 25 30 20
X 25 25 25 --- 20X 25 25 25 30 20
---X X X X --- 20X X X X 50 20X X X X 50 20X X X X --- 20X X X X 50 20--- --- --- --- --- ---X X X X 50 20X X X X 50 20X X X X --- 2050 50 50 50 50 2050 50 50 50 50 20--- --- --- --- --- ---X X X X --- 20X X X X --- 20
--- --- --- --- --- ---X 25 25 30 30 20X 25 25 30 30 20
ת Ƿ
1000 800 1000 800 --- 1500--- --- --- --- --- ---X 25 25 25 --- 20X 25 25 25 --- 20X 25 25 25 --- 20X 25 25 25 --- 20X 25 25 25 --- 20X 25 25 25 --- 20X 25 25 25 --- 20X 25 25 25 --- 20X 25 25 25 --- 20--- --- --- --- --- ------ --- --- --- --- ---X 25 25 25 --- 20X 25 25 25 30 20
--- --- --- --- --- ---X 25 25 25 --- 20
ש Œ800 1000 800 ---
--- --- --- --- --- ---50 50 50 50 --- 5050 50 50 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DH31 DH32 DH33 DH34 DH35 DH361300 800 1000 1500
C ≈ ⱴ ≈ M ≈ ∻
≙
50 50 50 50 50 5050 50 50 50 --- 5050 50 50 50 50 5050 50 50 50 50 5050 50 50 50 --- 5050 50 50 50 --- 5050 50 50 50 --- 5050 50 50 50 --- 5050 50 50 50 --- 5050 50 50 50 --- 5050 50 50 50 --- 50 --- --- --- --- --- ---50 50 50 50 50 5050 50 50 50 --- 5050 50 50 50 50 5050 50 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- ---50 50 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- ---50 50 50 50 50 5050 50 50 50 --- ---50 50 50 50 --- ------ --- --- --- --- 5050 50 50 50 --- ---50 50 50 50 --- ------ --- --- --- --- 5050 50 50 50 --- ---50 50 50 50 --- ---50 50 50 50 --- ---50 50 50 50 --- ---50 50 50 50 --- ---50 50 50 50 --- ---50 50 50 50 --- ---50 50 50 50 --- ---50 50 50 50 --- ---50 50 50 50 --- ---50 50 50 50 --- ---50 50 50 50 --- ---50 50 50 50 --- ---50 50 50 50 --- ---50 50 50 50 --- 5050 50 50 50 50 5050 50 50 50 50 5050 50 50 50 --- 5050 50 50 50 --- 5050 50 50 50 50 5050 50 50 50 50 50--- --- --- --- --- ---50 50 50 50 --- 50--- --- --- --- --- ------ --- --- --- --- ---50 50 50 50 --- 50--- --- --- --- --- ------ --- --- --- --- ---50 50 50 50 --- 50--- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ---50 50 50 50 --- 50--- --- --- --- --- ------ --- --- --- --- ---50 50 50 50 --- 5050 50 50 50 50 5050 50 50 50 50 50--- --- --- --- --- 5050 50 50 50 --- 50--- --- --- --- --- 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DH31 DH32 DH33 DH34 DH35 DH361300 800 1000 1500
C ≈ ⱴ ≈ M ≈ ∻
≙
50 50 50 50 50 5050 50 50 50 --- 5050 50 50 50 --- 50--- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- ---50 50 50 50 --- 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- ---
30 25 25 30 30 2030 25 25 30 30 20--- --- --- --- --- 2030 25 25 30 30 20--- --- --- --- --- 20--- --- --- --- --- --- --- --- --- --- --- ---30 25 25 30 --- 2030 25 25 30 --- 20--- --- --- --- --- ---30 25 25 30 --- 20--- --- --- --- --- --- --- --- --- --- --- ---50 50 50 50 --- 50--- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- 20--- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- 30 20--- --- --- --- --- ---30 25 25 30 --- 2030 25 25 30 30 20
--- --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- ---X X X X 30 X
--- --- --- --- --- ---X X X X --- XX X X X 30 XX X X X 30 X--- --- --- --- --- ------ --- --- --- --- ---X X X X --- X--- --- --- --- --- ---X X X X 30 X
Ə --- Ə --- --- Ə
X --- 50 --- --- X--- --- --- --- --- ---
1000 --- --- --- --- 1000--- --- 1000 --- --- ------ --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DH37 DH38 DH39 DH40 DH41 DH42 DH441500 1000 2500 1000 1000∻ U ≈ ∝ ≈ U ≈ M ≈
≙
X X X X X X XX X X X X X XX X X X X X X--- --- --- --- --- --- ---X --- X X X X X
X X X X X X XX X X X X Þ X Þ XX X --- X --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---X --- --- --- --- --- ---X --- --- --- --- --- ---
--- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X X X
X X X X X X XX X X X X X X
X --- X --- --- --- ---X X X X X X X
X^ X^ X^ X^ X^ X^ X^
X X X X X X X
X 20 X X X X 20--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X // X X X X //
20 X 20 20 20 30 X20 X 20 20 20 30 X20 30 20 20 20 30 50 ť20 30 20 20 20 30 50 ť --- --- --- --- --- --- --- --- --- 50 --- --- --- ------ --- 50 --- --- --- --- --- --- 50 --- --- --- ---20 X --- 20 --- --- X20 X 20 20 --- --- X20 --- --- 20 --- --- X20 X 20 20 --- --- X20 X --- 20 --- --- X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 X 20 20 20 30 X20 --- 20 20 --- --- X20 X 20 20 --- --- X--- --- --- --- --- --- --- --- --- --- --- --- --- ---20 --- 20 20 --- --- X--- --- --- --- --- --- ---20 X // 20 20 30 X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DH37 DH38 DH39 DH40 DH41 DH42 DH441500 1000 2500 1000 1000∻ U ≈ ∝ ≈ U ≈ M ≈
≙
20 X --- 20 --- --- X20 X 50 20 20 30 X20 X 50 20 20 30 X20 X 50 20 20 30 X20 X 50 20 20 30 X20 --- 50 20 20 30 ---20 X 50 20 20 30 X20 --- --- 20 --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 X --- 20 --- --- X20 --- --- 20 --- --- ---20 X --- 20 --- --- X--- --- --- --- --- --- ---20 X 50 20 20 30 X
20 --- 50 20 20 30 2520 --- 50 20 20 30 25
--- ---20 X --- X X X X20 X 50 X X X X20 X 50 X X X X20 X --- X X X X20 X 50 X X X X--- --- --- --- --- --- ---20 X 50 X X X X20 X 50 X X X X20 X --- X X X X20 --- 50 50 50 50 5020 --- 50 50 50 50 50--- --- --- --- --- --- ---20 X --- X X X X20 X --- X X X X
ť
--- --- --- --- --- --- ---20 X 20 20 20 30 X20 X 20 20 20 30 X
1500 --- --- --- --- 1000--- --- --- --- --- --- ---20 --- 50 20 20 30 2520 --- 50 20 20 30 2520 --- 50 20 20 30 2520 --- 50 20 20 30 2520 --- 50 20 20 30 2520 --- 50 20 20 30 2520 --- 50 20 20 30 2520 --- 50 20 20 30 2520 --- 50 20 20 30 25--- --- --- --- --- --- ------ --- --- --- --- --- ---20 --- 50 20 20 30 2520 --- 50 20 20 30 25 --- --- --- --- --- --- ---20 --- 50 20 20 30 25
--- ------ --- --- --- --- --- ---50 50 --- 50 50 50 5750 50 50 50 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DH37 DH38 DH39 DH40 DH41 DH42 DH441500 1000 2500 1000 1000∻ U ≈ ∝ ≈ U ≈ M ≈
≙
50 50 50 50 50 50 5050 50 --- 50 50 50 5750 50 --- 50 50 50 5050 50 50 50 50 50 5050 50 --- 50 50 50 5750 50 --- 50 50 50 5050 50 --- 50 50 50 5750 50 --- 50 50 50 5050 50 --- 50 50 50 5050 50 --- 50 50 50 5750 50 --- 50 50 50 50 --- --- --- --- --- --- ---50 50 50 50 50 50 5050 50 --- 50 50 50 5050 50 --- 50 50 50 5050 50 50 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 --- 50 50 50 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50--- 50 50 50 50 50 50--- 50 --- 50 50 50 5750 --- 50 --- --- --- ------ 50 50 50 50 50 50--- 50 --- 50 50 50 5750 --- 50 --- --- --- ------ 50 50 50 50 50 50--- 50 50 50 50 50 50--- 50 --- 50 50 50 57--- 50 --- 50 50 50 57--- 50 50 50 50 50 50--- 50 50 50 50 50 50--- 50 --- 50 50 50 57--- 50 --- 50 50 50 57--- 50 --- 50 50 50 57--- 50 50 50 50 50 50--- 50 50 50 50 50 50--- 50 --- 50 50 50 57--- 50 50 50 50 50 50--- 50 50 50 50 50 5050 50 --- 50 50 50 5750 50 50 50 50 50 5050 50 50 50 50 50 5050 50 --- 50 50 50 5750 50 --- 50 50 50 5750 50 50 50 50 50 5050 50 50 50 50 50 50--- --- --- --- --- --- ---50 50 --- 50 50 50 57--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 50 50--- --- --- --- --- --- ------ --- 50 --- --- --- ---50 50 50 50 50 50 50--- --- 50 --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 --- 50 50 50 57--- --- --- --- --- --- ------ --- 50 --- --- --- ---50 50 --- 50 50 50 5750 50 50 50 50 50 5050 50 50 50 50 50 5050 --- 50 --- --- --- ---50 50 50 50 50 50 5050 --- 50 --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DH37 DH38 DH39 DH40 DH41 DH42 DH441500 1000 2500 1000 1000∻ U ≈ ∝ ≈ U ≈ M ≈
≙
50 50 --- 50 50 50 5750 50 50 50 50 50 5050 50 --- 50 50 50 57--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 50 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- 50 50 --- --- ---
ť
20 30 20 20 20 30 5020 30 20 20 20 30 5020 --- --- --- --- --- ---20 30 20 20 20 30 5020 --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 30 --- 20 --- --- ---20 --- --- 20 --- --- ------ --- --- --- --- --- ---20 30 --- 20 --- --- 50--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 --- --- 50 --- --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---20 --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---20 --- 20 --- 20 30 ------ --- --- --- --- --- ---20 30 --- 20 --- --- 5020 30 20 20 20 30 50
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X --- 50 X 20 30 X
--- --- --- --- --- --- ---X X --- X --- --- XX X 20 X 20 30 XX X 20 X 20 30 X--- --- --- --- --- --- ------ --- --- --- --- --- ---X --- --- X --- --- ------ --- --- --- --- --- ---X X // X 20 30 X
Ə --- Ə Ə Ə --- ---X --- 50 50 50 --- ------ --- --- --- --- --- ---
1000 --- 1000 2500 1000 --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DH45 DH46 DH47 DH48 DH49 DH50 DH511300 1000 1000Ø ≈ M ≈
X X X X X X Z XX X X X X --- XX X X X X X X--- --- --- --- --- --- ---X X X --- X --- X
X X X X X --- XX X X X X --- XX X X X X --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X X X --- X--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X --- X--- --- --- --- --- --- ---
------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X --- X--- --- --- --- --- --- --- --- --- --- --- --- --- ---X X X X X --- X
X X X X X X XX X X X X X X
X --- X --- --- --- ---X X X X X --- X
X^ X^ X^ X^ X^ --- X^
X X X X X --- X
X X 20 20 30 --- 30--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---X X // // // X //
20 30 X X 25 --- 2520 30 X X 25 --- 2520 30 30 30 25 --- 2520 30 30 30 25 --- 25 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 30 X X 25 --- 2520 30 X X 25 --- 2520 30 X --- 25 --- 2520 30 X X 25 --- 2520 30 X X 25 --- 25--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 30 X X 25 --- 2520 30 X --- 25 --- 2520 30 X X 25 --- 25--- --- --- --- --- --- --- --- --- --- --- --- --- ---20 30 X --- 25 --- 25--- --- --- --- --- --- ---20 30 X X 25 --- 25
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DH45 DH46 DH47 DH48 DH49 DH50 DH511300 1000 1000Ø ≈ M ≈
20 25 30 X 25 --- 2520 25 30 X 25 --- 2520 25 30 X 25 --- 2520 25 30 X 25 --- 2520 25 30 X 25 --- 2520 25 30 --- 25 --- 2520 25 30 X 25 --- 2520 25 30 --- 25 --- 25--- --- --- --- --- --- ------ --- --- --- --- --- ---20 25 30 X 25 --- 2520 25 30 --- 25 --- 2520 25 30 X 25 --- 25--- --- --- --- --- --- ---20 25 30 X 25 --- 25
20 50 30 --- 50 --- 5020 50 30 --- 50 --- 50
20 X 50 X X --- X20 X 50 X X --- X20 X 50 X X --- X20 X 50 X X --- X20 X 50 X X --- X--- --- 50 --- --- --- ---20 X 50 X X --- X20 X 50 X X --- X20 X 50 X X --- X50 50 50 --- 50 --- 5050 50 50 --- 50 --- 50--- --- --- --- --- --- ---20 X 50 X X --- X20 X 50 X X --- X
--- --- --- --- --- --- ---20 25 30 X X 15 X20 25 30 X X --- X
ת--- 800 --- 800 --- 800--- --- --- --- --- --- ---20 50 30 --- 50 --- 5020 50 30 --- 50 --- 5020 50 30 --- 50 --- 5020 50 30 --- 50 --- 5020 50 30 --- 50 --- 5020 50 30 --- 50 --- 5020 50 30 --- 50 --- 5020 50 30 --- 50 --- 5020 50 30 --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---20 50 30 --- 50 --- 5020 50 30 --- 50 --- 50 --- --- --- --- --- --- ---20 50 30 --- 50 --- 50
ש800 800 800
--- --- --- --- --- --- ---50 50 57 --- 50 --- 5050 50 50 --- 50 --- 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DH45 DH46 DH47 DH48 DH49 DH50 DH511300 1000 1000Ø ≈ M ≈
50 50 50 --- 50 --- 5050 50 57 --- 50 --- 5050 50 50 --- 50 --- 5050 50 50 --- 50 --- 5050 50 57 --- 50 --- 5050 50 50 --- 50 --- 5050 50 57 --- 50 --- 5050 50 50 --- 50 --- 5050 50 50 --- 50 --- 5050 50 57 --- 50 --- 5050 50 50 --- 50 --- 50 --- --- --- --- --- --- ---50 50 50 --- 50 --- 5050 50 50 --- 50 --- 5050 50 50 --- 50 --- 5050 50 50 --- 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 50 --- 50 --- 50 --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 X 50 --- 5050 50 50 --- 50 --- 5050 50 57 --- 50 --- 50--- --- 50 --- --- --- ---50 50 50 --- 50 --- 5050 50 57 --- 50 --- 50--- --- --- --- --- --- ---50 50 50 --- 50 --- 5050 50 50 --- 50 --- 5050 50 57 --- 50 --- 5050 50 57 --- 50 --- 5050 50 50 --- 50 --- 5050 50 50 --- 50 --- 5050 50 57 --- 50 --- 5050 50 57 --- 50 --- 5050 50 57 --- 50 --- 5050 50 50 --- 50 --- 5050 50 50 --- 50 --- 5050 50 57 --- 50 --- 5050 50 50 --- 50 --- 5050 50 50 --- 50 --- 5050 50 57 --- 50 --- 5050 50 50 --- 50 --- 5050 50 50 --- 50 --- 5050 50 57 --- 50 --- 5050 50 57 --- 50 --- 5050 50 50 --- 50 --- 5050 50 50 --- 50 --- 50--- --- 50 --- --- --- ---50 50 57 --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 50 --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---50 50 57 --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 57 --- 50 --- 5050 50 50 --- 50 --- 5050 50 50 --- 50 --- 50--- --- --- --- --- --- ---50 50 50 --- 50 --- 50--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DH45 DH46 DH47 DH48 DH49 DH50 DH511300 1000 1000Ø ≈ M ≈
50 50 57 --- 50 --- 5050 50 50 --- 50 --- 5050 50 57 --- 50 --- 50--- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ---50 50 // --- 50 --- 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- ---
20 25 30 30 30 --- 3020 25 30 30 30 --- 30--- --- --- --- --- --- ---20 25 30 30 30 --- 30--- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---20 25 --- 30 30 --- 3020 25 --- --- 30 --- 30--- --- --- --- --- --- ---20 25 30 30 30 --- 30--- --- --- --- --- --- --- --- --- --- --- --- --- ---50 50 30 --- 50 --- 50--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ---20 25 30 30 30 --- 3020 25 30 30 30 --- 30
--- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- ---X X X --- X --- X
--- --- --- --- --- --- ---X X X X X --- XX X X X X --- XX X X X X --- X--- --- --- --- --- --- ------ --- --- --- --- --- ---X X X --- X --- X--- --- --- --- --- --- ---X X X X X --- X
® Ə Ə --- Ə1 --- Ə150 X --- 50 --- 50--- --- --- --- --- --- ---
1400 2000 --- --- --- --- ------ --- --- --- 1500 --- 1500--- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DH52 DH53 DH54 DH55 DH56 DH57 DH58 DH591500 1000
Ñ ≈ ש U ≈
X X X X X X X XX X X X X X X XX X X X X X X X--- --- --- --- --- --- --- ------ --- X X --- --- --- X
--- --- X X X X X XX X X X X X X X--- --- X X X X X X--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ---X X X X X X X X--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- X X X X X X--- --- --- --- --- --- --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- X X X X X X--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- X X X X X X
X X X X X X X XX X X X X X X X
X X X --- --- --- --- XX X X X X X X X
X^ X^ X^ X^ X^ X^ X^ X^
--- --- X X X X X X
--- --- X X 20 25 X 50--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- X X // // X //
--- --- 20 X X X X 50--- --- 20 X X X X 50--- --- 20 X 30 30 X 50--- --- 20 X 30 30 X 50--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- 20 X X X X X--- --- 20 X X X X X--- --- 20 X X X X X--- --- 20 X X X X X--- --- 20 X X X X X--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- 20 X X X X X--- --- 20 X X X X X--- --- 20 X X X X X--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- 20 X X X X X--- --- --- --- --- --- --- ------ --- 20 X X X X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DH52 DH53 DH54 DH55 DH56 DH57 DH58 DH591500 1000
Ñ ≈ ש U ≈
--- --- 20 X X X X X--- --- 20 X X X X X--- --- 20 X X X X X--- --- 20 X X X X X--- --- 20 X X X X X--- --- 20 X X --- X X--- --- 20 X X X X X--- --- 20 X X --- --- X--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- 20 X X X X X--- --- 20 X --- --- --- X--- --- 20 X X X X X--- --- --- --- --- --- --- ------ --- 20 X X X X X
--- --- 20 X --- --- --- 50--- --- 20 X --- --- --- 50
--- --- X X X X X 50--- --- X X X X X 50--- --- X X X X X 50--- --- X X X X X 50--- --- X X X X X 50--- --- --- --- --- --- --- ------ --- X X X X X 50--- --- X X X X X 50--- --- X X X X X 50--- --- 50 50 50 50 50 50--- --- 50 50 50 50 50 50--- --- --- --- --- --- --- ------ --- X X X X X 50--- --- X X X X X 50
--- --- --- --- --- --- --- ------ --- 20 X X X X 50--- --- 20 X X X X 50
--- 1000 1000 --- --- 1000--- --- --- --- --- --- --- ------ --- 20 X 50 --- --- 50--- --- 20 X 50 --- --- 50--- --- 20 X 50 --- --- 50--- --- 20 X 50 --- --- 50--- --- 20 X 50 --- --- 50--- --- 20 X 50 --- --- 50--- --- 20 X 50 --- --- 50--- --- 20 X 50 --- --- 50--- --- 20 X 50 --- --- 50--- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- 20 X 50 --- --- 50--- --- 20 X 50 --- --- 50--- --- --- --- --- --- --- ------ --- 20 X 50 --- --- 50
800--- --- --- --- --- --- --- ------ --- 50 57 57 50 57 50--- --- 50 50 50 50 50 50
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DH52 DH53 DH54 DH55 DH56 DH57 DH58 DH591500 1000
Ñ ≈ ש U ≈
--- --- 50 50 50 50 50 50--- --- 50 57 57 50 57 50--- --- 50 50 50 50 50 50--- --- 50 50 50 50 50 50--- --- 50 57 57 50 57 50--- --- 50 50 50 50 50 50--- --- 50 57 57 50 57 50--- --- 50 50 50 50 50 50--- --- 50 50 50 50 50 50--- --- 50 57 57 50 57 50--- --- 50 50 50 50 50 50--- --- --- --- --- --- --- ------ --- 50 50 50 50 50 50--- --- 50 50 50 50 50 50--- --- 50 50 50 50 50 50--- --- 50 50 50 50 50 50--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- 50 50 50 50 50 50--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- 50 50 50 50 50 50--- --- 50 50 50 50 50 50--- --- 50 57 57 50 57 50--- --- --- --- --- --- --- ------ --- 50 50 50 50 50 50--- --- 50 57 57 50 57 50--- --- --- --- --- --- --- ------ --- 50 50 50 50 50 50--- --- 50 50 50 50 50 50--- --- 50 57 57 50 57 50--- --- 50 57 57 50 57 50--- --- 50 50 50 50 50 50--- --- 50 50 50 50 50 50--- --- 50 57 57 50 57 50--- --- 50 57 57 50 57 50--- --- 50 57 57 50 57 50--- --- 50 50 50 50 50 50--- --- 50 50 50 50 50 50--- --- 50 57 57 50 57 50--- --- 50 50 50 50 50 50--- --- 50 50 50 50 50 50--- --- 50 57 57 50 57 50--- --- 50 50 50 50 50 50--- --- 50 50 50 50 50 50--- --- 50 57 57 50 57 50--- --- 50 57 57 50 57 50--- --- 50 50 50 50 50 50--- --- 50 50 50 50 50 50--- --- --- --- --- --- --- ------ --- 50 57 57 50 57 50--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- 50 50 50 50 50 50--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- 50 50 50 50 50 50--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- 50 57 57 50 57 50--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- 50 57 57 50 57 50--- --- 50 50 50 50 50 50--- --- 50 50 50 50 50 50--- --- --- --- --- --- --- ------ --- 50 50 50 50 50 50--- --- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DH52 DH53 DH54 DH55 DH56 DH57 DH58 DH591500 1000
Ñ ≈ ש U ≈
--- --- 50 57 57 50 57 50--- --- 50 50 50 50 50 50--- --- 50 57 57 50 57 50--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- 50 50 50 50 50 50
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- --- --- --- --- ---
--- --- 20 X 30 30 X 50--- --- 20 X 30 30 X 50--- --- --- --- --- --- --- ------ --- 20 X 30 30 X 50--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- 20 30 --- --- --- 50--- --- 20 30 --- --- --- 50--- --- --- --- --- --- --- ------ --- 20 30 30 30 30 50--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- 50 50 50 50 50 50--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- 20 30 30 30 30 50--- --- 20 X 30 30 X 50
--- --- 20 --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- --- --- --- --- --- --- ------ --- 20 X X X X X--- --- --- --- --- --- --- ------ --- 20 X X X X X--- --- 20 X X X X X--- --- 20 X X X X X--- --- 20 --- --- --- --- ------ --- --- --- --- --- --- ------ --- 20 X --- --- --- X--- --- --- --- --- --- --- ------ --- 20 X X X X X
Ə Ə Ə * --- --- Ə1
--- --- 50 X X --- --- 50--- --- --- --- --- --- --- ------ --- 1500 1000 1000 --- --- 1000--- --- --- --- --- --- --- ------ --- --- --- --- --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
CATEGORY I
DIAGNOSTIC
NoteDIAG. AND PREV. Evaluation
D0120 Periódic oral evaluationD0140 Limited oral evalation - problem focusedD0150 Comprehensive oral evaluationD0160 Detailed and extensive oral evaluation
D0180 (P) Comprehensive periodontal evaluationImaging
D0210 Intraoral - complete series of radiographic im agesD0220;D0230 Intraoral - periapical first or each add itional radiographic image
D0240 Intraoral - occlusal radiographic imageD0250 Extra-oral - 2D projection radiographic imageD0251 Extra-oral - posterior dental radiographic im age
D0270;D0272 Bitewing - single or two radiographic im agesD0273 Bitewings - three radiographic imagesD0274 Bitewings - four radiographic imagesD0277 Vertical bitewings - 7 to 8 radiographic image sD0290 Posterior - anterior or lateral skull and facial bo ne survey radiographic imageD0330 Panoramic radiographic imageD0340 Cephalometric radiographic image
OthersD0350 Oral / facial photographic imageD0415 Collection of microorganisms for culture and sensit ivityD0460 Pulp vitality testsD0470 Diagnostic castsD0473 Accession of tissue, gross and microscopic exa minationD0999 Unspecified diagnostic procedure, by report
PREVENTIVE
NoteProphylaxis
D1110 Prophylaxis - adultD1120 Prophylaxis - child
Topical Fluoride TreatmentD1206 Topical application of fluoride varnishD1208 Topical application of fluoride - childD1208 Topical application of fluoride - adult (by report)
SealantD1351 Sealant - per tooth
Space MaintenanceD1510;D1515 Space maintainer - fixed - unilateral / bilateral
D1520 Space maintainer - removable- unilateral D1525 Space maintainer - removable bilateralD1550 Re - cementation of space maintainerD1999 Unspecified preventive procedure, by report
CATEGORY II
ROUTINES SERVICES RESTORATIVE
NoteD2140-D2161 Amalgam - primary or permanentD2330-D2335 Resin - based composite - anterior (prim ary or permanent)
D2391 Resin - based composite - posterior (primary o r permanent) D2392-D2394 Resin - based composite - posterior (pri mary or permanent)D2410-D2430 Gold foil D2510-D2620 Inlays - Onlays: metallic - porcelain / ceramic
D2630 Inlay- porcelain / ceramic - three or more sur facesD2642-D2664 Inlay -Onlay: porcelain / ceramic; resin- based com posite
D2799 Provisional crown D2910 Recement inlay, onlay, or partial coverage restorat ionD2915 Recement cast or prefabricated post and coreD2920 Recement crownD2930 Prefabricated stainless steel crown – primary toothD2931 Prefabricated stainless steel crown – permanen t toothD2932 Prefabricated resin crownD2933 Prefabricated stainless steel crown with resin windowD2940 Protective restoration D2950 Core buildup, including any pins when requir edD2951 Pin retention - per tooth, in addition to rest orationD2960 Labial veneer (resin laminate) – chairside
D2961;D2962 Labial veneer - resin / porcelain lamínate – labora toryD2980 Crown repair necessitated by restaurative mate rial failure
D2981-D2983 Inlay, onlay, venner repair necessitated by restaurative material failure D2999 Unspecified restorative procedure, by report
DH60 DH61 DH98 DH99
X X X XX X X XX X X X--- --- --- ---30 X --- ---
X X X XX X X XX X X X--- --- --- ------ --- --- ---X X X X--- --- --- ---30 --- --- ------ --- --- --- --- --- --- ---X X X X
30 Ð --- --- ---
--- --- --- --- --- --- --- ---X X X X--- --- --- --- --- --- --- ---X X X X
X X X XX X X X
--- --- --- ---X X X X
X^ X^ X^ X^
X X X X
X 20 X X30 --- --- ---30 --- --- ---30 --- --- ---// // X X
X X X XX X X XX 30 X XX 30 X X
--- --- --- --- --- --- ------ --- --- --- --- --- --- ---X X X X30 X --- ---X X X X30 X --- ---X X X X--- --- --- ------ --- --- ------ --- --- ---X X X X30 X --- ---30 X --- ------ --- --- ------ --- --- ---X X X X--- --- --- ---X X X X
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
ENDODONTICS
NoteD3110 Pulp cap - direct (excluding final restoration )D3120 Pulp cap - indirect (excluding final restorati on)D3220 Therapeutic pulpotomy (excluding final restora tion)D3221 Pulpal debridement, primary and permanent teet h
D3310;D3320 Endodontic therapy, anterior / bicúspid (excluding final restoration)D3330 Endodontic therapy, molar (excluding final res toration)
D3346;D3347 Retreatment of previous root canal thera py - anterior / bicuspidD3348 Retreatment of previous root canal therapy - m olar
D3351-D3353 Apexification / recalcification - inicia l / interim / final visitD3355-D3357 Pulpal regeneration - inicial / interim / final visitD3410;D3421 Apicoectomy - anterior / bicuspid (first root) D3425;D3426 Apicoectomy - molar - first root / each additional root
D3430 Retrograde filling – per rootD3450;D3920 Root amputation - per root / Hemisection
D3999 Unspecified endodontic procedure, by reportBASIC PERIODONTICSNote
D4355 Full mouth debridement to enable comprehensive evaluation and diagnosisD4910 Periodontal maintenance
PROSTHODONTICS
NoteLimit per policy year ($)
D5410;D5411 Adjust complete denture – maxillary / ma ndibularD5421;D5422 Adjust partial denture – maxillary / man dibular
D5510 Repair broken complete denture baseD5520 Replace missing or broken teeth-complete dentu re (each tooth)D5610 Repair resin denture baseD5620 Repair cast frameworkD5630 Repair or replace broken claspD5640 Replace broken teeth – per tooth
D5650;D5660 Add tooth / clasp to existing partial de nture D5710-D5721 Rebase: complete / partial dentureD5730-D5761 Reline:complete / partial dentureD5850;D5851 Tissue conditioning, maxillary / mandibu lar
D6930 Recement fixed partial dentureD6980 Fixed partial denture repair necessitated by restor ative material failure
ORAL SURGERY
NoteExtractions
D7111 Extraction, coronal remnants - deciduous toothD7140 Extraction, erupted tooth or exposed rootD7510 Incision and drainage of abscess- intraoral soft ti ssue
CATEGORY III
MAYOR SERVICES PERIODONTICS
NoteLimit per policy year ($)Periodontics deductible ($)
D4210;D4211 Gingivectomy or gingivoplasty- four o mo re / one to three contiguous teethD4240;D4241 Gingival flap incluying root planing - f our o more / one to three contiguous teeth
D4245 Apically positioned flapD4249 Clinical crown lengthening - hard tissue
D4260;D4261 Osseous surgery D4263;D4264 Bone replacement graft -first / addition al site in quadrantD4266;D4267 Guided tissue regeneration - resorbable barrier / no resorbable barrier, per site D4270;D4273 Pedicle soft tissue graft / Subepitheli al connective tissue graft, per tooth
D4277 Free soft tissue graft procedure - first tooth or edentulous toothD4278 Free soft tissue graft procedure - each additi onal contiguous tooth or edontulous toothD4320 Provisional splinting - intracoronal D4321 Provisional splinting - extracoronal
D4341;D4342 Periodontal scaling root planing / four or more / one to three teeth per quadrantD4920 Unscheduled dressing change (by someone other than treating dentist or their staff)D4999 Unspecified periodontal procedure, by report
PROSTHODONTICS
NoteLímit ($)
D2710 Crown - resin based composite (indirect)D2720 Crown - resin with high noble metalD2722 Crown - resin with noble metal
DH60 DH61 DH98 DH99
40 X --- ---X X X XX X X XX X X XX X X XX X X X40 X --- ---40 X --- ---40 --- --- ------ --- --- ---40 X --- ------ X --- ---40 X --- ------ --- --- ---X X X X
50 X --- ---50 X --- ---
50 X --- ---50 X --- ---50 X --- ---50 X --- ---50 X --- ---50 --- --- ---50 X --- ---50 X --- ---50 X --- ---50 50 --- ---50 50 --- ---50 --- --- ---50 X --- ---50 X --- ---
--- --- --- ---X X X XX X X X
1000 1000 --- ------ --- --- ---50 X --- ---50 X --- ---50 X --- ---50 X --- ---50 X --- ---50 X --- ---50 X --- ------ X --- ------ X --- ------ --- --- ------ --- --- ---50 X --- ---50 X --- --- --- --- --- ---50 X --- ---
--- --- --- ---50 57 --- ---50 50 --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D2740 Crown - porcelain / ceramic substrateD2750 Crown - porcelain fused to high noble metalD2751 Crown - porcelain fused to predominantly base metalD2752 Crown - porcelain fused to noble metalD2780 Crown - ¾ cast high noble metal
D2781-D2783 Crown - ¾ cast base metal / noble meta l / porcelain-ceramicD2790 Crown - full cast high noble metalD2791 Crown - full cast predominantly base metalD2792 Crown - full cast noble metalD2794 Crown - titanium
D2952;D2954 Post and core D2975 Coping
D5110;D5120 Complete denture - maxilary / mandibularD5130;D5140 Immediate denture - maxilary / mandibula rD5211;D5212 Partial denture - resin base - maxilary / mandibularD5213;D5214 Partial denture - cast metal framework w ith resin base - maxilary / mandibularD5221;D5222 Immediate partial denture-resin base - m axilary / mandibularD5223;D5224 Immediate partial denture-cast metal fra mework with resin denture base - maxilary/mandibula r
D5281 Removable unilateral partial denture - one pie ce cast metalD5810-D5821 Interim complete and partial denture - m axilary / mandibularD5863-D5866 Overdentures:complete;partial - maxillary / mandibu lar
D5862 Precision attachment, by reportD5899 Unspecified removable prosthodontic procedure , by report D6058 Abutment supported porcelain / ceramic crownD6059 Abutment supported porcelain fused to metal cr own (high noble metal)D6060 Abutment supported porcelain fused to metal cr own predominantly base metalD6061 Abutment supported porcelain fused to metal cr own (noble metal)D6062 Abutment supported cast metal crown (high nobl e metal)D6063 Abutment supprted cast metal crown (predominan tly base metal)D6064 Abutment supported cast metal crown (noble met al)D6065 Implant supported porcelain / ceramic crownD6066 Implant supported porcelain fused to metal cro wnD6067 Implant supported metal crown D6068 Abutment supported retainer for porcelain/cera mic FPDD6075 Implant supported retainer for ceramic FPDD6076 Implant supported retainer for porcelain fused to metal FPDD6077 Implant supported retainer for cast metal FPDD6069 Abutment supported retainer for porcelain fuse d to metal FPD (high noble metal)D6070 Abutment supported retainer for porcelain fuse d to metal FPD (predominantly base metal)D6071 Abutment supported retainer for porcelain fuse d to metal FPD (noble metal)D6072 Abutment supported retainer for cast metal FPD (high noble metal)D6073 Abutment supported retainer for cast metal FPD (predominantly base metal)D6074 Abutment supported retainer for cast metal FPD (noble metal)D6210 Pontic - cast high noble metalD6211 Pontic - cast predominantly base metalD6212 Pontic - cast noble metalD6214 Pontic - titaniumD6240 Pontic - porcelain fused to high noble metalD6241 Pontic - porcelain fused to predominantly base metalD6242 Pontic - porcelain fused to noble metalD6245 Pontic - porcelain / ceramic D6250 Pontic - resin with high noble metal
D6251;D6252 Pontic - resin with predominantly base metal / resin with noble metalD6253 Provisional pontic D6545 Retainer - cast metal for resin bonded fixed p rosthesisD6548 Retainer - porcelain / ceramic for resin bonde d fixed prosthesis
D6600-D6605 Inlays: porcelain;metalicD6606;D6607 Inlays - cast noble metal, two surfaces / three or more surfacesD6608-D6615 Onlays:porcelain;metalicD6624;D6634 Inlays / onlays - titanium
D6710 Crown - indirect resin based composite D6720 Crown - resin with high noble metal
D6721;D6722 Crown - resin with predominantly base metal / resin with noble metalD6740 Crown - porcelain / ceramicD6750 Crown - porcelain fused to high noble metalD6751 Crown - porcelain fused to predominantly base metalD6752 Crown - porcelain fused to noble metalD6780 Crown - ¾ cast high noble metal
D6781;D6782 Crown - ¾ cast predominantly base metal / noble metalD6783 Crown - ¾ porcelain / ceramic
DH60 DH61 DH98 DH99
50 50 --- ---50 57 --- ---50 50 --- ---50 50 --- ---50 57 --- ---50 50 --- ---50 57 --- ---50 50 --- ---50 50 --- ---50 57 --- ---50 50 --- --- --- --- --- ---50 50 --- ---50 50 --- ---50 50 --- ---50 50 --- --- --- --- --- --- --- --- --- ---50 50 --- ------ --- --- --- --- --- --- ------ --- --- ---50 50 --- ---50 50 --- ---50 57 --- ---50 --- --- ---50 50 --- ---50 57 --- ---50 --- --- ---50 50 --- ---50 50 --- ---50 57 --- ---50 57 --- ---50 50 --- ---50 50 --- ---50 57 --- ---50 57 --- ---50 57 --- ---50 50 --- ---50 50 --- ---50 57 --- ---50 50 --- ---50 50 --- ---50 57 --- ---50 50 --- ---50 50 --- ---50 57 --- ---50 57 --- ---50 50 --- ---50 50 --- ------ --- --- ---50 57 --- ------ --- --- ------ --- --- ---50 50 --- ------ --- --- ------ --- --- ---50 50 --- ------ --- --- ------ --- --- ------ --- --- ---50 57 --- ------ --- --- ------ --- --- ---50 57 --- ---50 50 --- ---50 50 --- ------ --- --- ---50 50 --- ------ --- --- ---
January 01, 2016

NOTES AND MODIFIERS APPLIED TO THE TABLE OF COVERAG E OF TRIPLE-S SALUD
CODES DESCRIPTIONMaximum Benefit Cover ($)
Note Deductible
D6790 Crown - full cast high noble metalD6791;D6792 Crown - full cast predominantly base metal / noble metal
D6794 Crown - titaniumD6920 Connector barD6940 Stress breakerD6950 Precision attachmentD6999 Unspecified, fixed prosthodontic procedure, by repo rt
MAXILOFACIAL PROSTHETIC
D5931-D5936 Obturator prosthesis: surgical / definitive / modif ication - mandibular resection D5951-D5955 Feeding aid / Speech aid (pediatric- adult) / Palat al (augmentation- lift) prosthesis D5982-D5985 Surgical stent / Radiation shield / Radiation cone locator
D5986 Fluoride gel carrierIMPLANTS SERVICES
NoteLímit ($)
D6010-D6199 Surgical placement of implant body; endosteal impla nt / second stage implant surgeryORAL SURGERY (SURGICAL)
NoteD7210 Surgical removal of erupted tooth
D7220-D7240 Removal of impacted tooth – soft tissue / partially bony / completely bonyD7241 Removal of impacted tooth – completely bony, w ith unusual surgical complicationD7250 Surgical removal of residual tooth rootsD7260 Oroantral fistula closureD7270 Tooth reimplantation and / or stabilization of accidentally evulsed or displaced toothD7272 Tooth transplantation D7280 Surgical access of an unerupted tooth D7283 Placement of device to facilitate eruption of impac ted toothD7285 Biopsy of oral tissue - hard (bone, tooth)D7286 Biopsy of oral tissue - softD7290 Surgical repositioning of teethD7291 Transseptal fiberotomy/supra crestal fiberotomy, by report
D7310-D7321 Alveoloplasty in conjunction with extrac tions / not in conjunction with extractionsD7340 Vestibuloplasty-ridge extension (secondary epi thelialization)D7350 Vestibuloplasty-ridge extension (including sof t tissue grafts….)
D7471-D7473 Removal of lateral exostosis / torus pal atinus / torus mandibularisD7520 Incision and drainage of abscess – extraoral s oft tissueD7550 Partial ostectomy /Sequestrectomy for removal of non-vital boneD7880 Occlusal orthotic device, by reportD7881 Occlusal orthotic device adjustmentD7910 Suture of recent small wounds up to 5 cmD7953 Bone replacement graft for ridge preservation – per siteD7960 Frenulectomy (frenectomy or frenotomy) – separ ate procedureD7970 Excision of hyperplastic tissue - per archD7971 Excision of pericoronal gingivaD7999 Unspecified oral surgery procedure, by report
CATEGORY IV
ADJUNCTIVE GENERAL SERVICES
NoteD9110 Palliative (emergency) treatment of dental pai n – minor procedureD9230 Inhalation of nitrous oxide / analgesia, anxio lysisD9243 Intravenous moderate (conscious) sedation/anal gesiaD9310 Consultation - diagnostic service provided by dentist or physicianD9410 House / extended care facility callD9420 Hospital or ambulatory surgical center call
D9430;D9440 Office visits (during regularly scheduled hours/ af ter regularly scheduled hours)D9630 Other drugs and / or medicaments, by reportD9910 Application of desensitizing medicamentD9930 Reatment of complications (post-surgical) - un usual circumstances, by report
D9940;D9950 Occlusal guard, by report / Occlusion an alysis - mounted caseD9943 Occlusal guard adjustment
D9951;D9952 Occlusal adjustment - limited / completeD9973;D9974 External / Internal bleaching – per tooth
D9999 Unspecified adjunctive procedure – by reportORTHODONTIC
NoteD8210-D8690 Orthodontic Services
D8691 Repair of orthodontic appliance Lifetime limit ($)Límit per policy year ($)Deductible Orthodontics ($)
DH60 DH61 DH98 DH99
50 57 --- ---50 50 --- ---50 57 --- ------ --- --- --- --- --- --- ------ --- --- ---50 50 --- ---
--- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
--- --- --- ---
X 30 X XX 30 X X--- --- --- ---X 30 X X30 --- --- ---30 --- --- --- --- --- --- ---30 30 --- ---30 30 --- ---30 --- --- ---30 30 --- ---30 --- --- --- --- --- --- ---50 50 --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- ------ --- --- --- --- --- --- ------ --- --- --- --- --- --- --- --- ---30 --- --- ---30 --- --- ---30 30 --- ---X 30 X X
--- --- --- ------ --- --- ------ --- --- ---30 --- --- --- --- --- --- ---X X X X
--- --- --- ---30 --- --- ---X X X XX X X X--- X --- ------ --- --- ---30 X --- ------ --- --- ---X X X X
Ə Ə --- ---X X --- ------ --- --- ---
1000 2000 --- ------ --- --- ------ --- --- ---
January 01, 2016