Embed Size (px)
Citation preview
Not A Drop: Pulse Oximetry and the Noninvasive Measurement of Total Hemoglobin
John Salyer RRT-NPS, MBA, FAARCDirector Respiratory Care
Seattle Children’s Hospital, Research Institute, Foundation
Ottawa
Seattle
Children’s
What Motivates You?
Cures Everything Except Stupidity
• There is not the slightest indication that [nuclear energy] will ever be obtainable. It would mean that the atom would have to be shattered at will.
• Albert Einstein, 1932.
• Where a calculator on the ENIAC is equipped with 19,000 vacuum tubes and weighs 30 tons, computers in the future may have only 1,000 vacuum tubes and perhaps only weigh 1.5 tons.
• Popular Mechanics, March 1949.
Famous Technology Predictions
• I think there is a world market for maybe five computers.
• Thomas Watson, chairman of IBM, 1943.
• Heavier-than-air flying machines are impossible.
• Lord Kelvin, ca. 1895, British mathematician and physicist
• There is no need for any individual to have a computer in their home.
• Ken Olson, 1977, President, Digital Equipment Corp.
Famous Technology Predictions
May You Live in Interesting Times
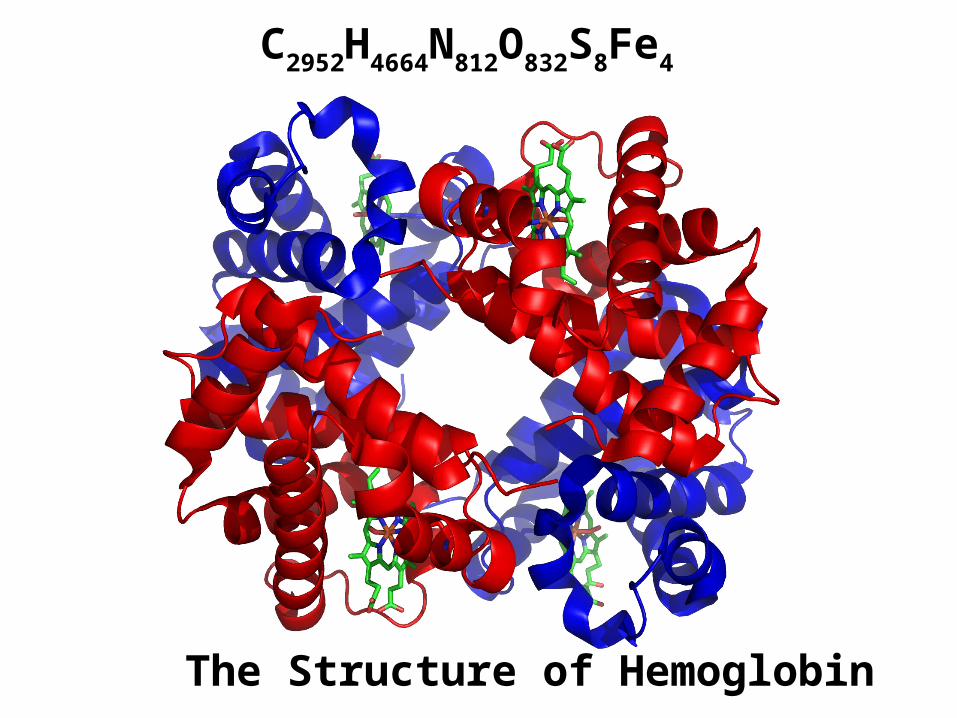
The Structure of Hemoglobin
C2952H4664N812O832S8Fe4
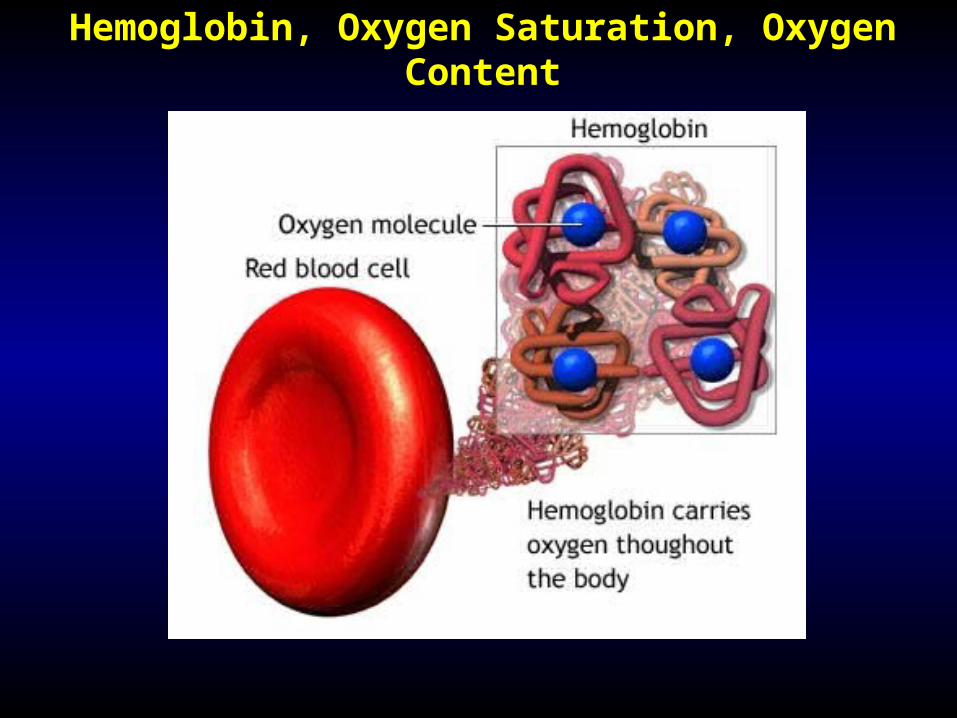
Hemoglobin, Oxygen Saturation, Oxygen Content
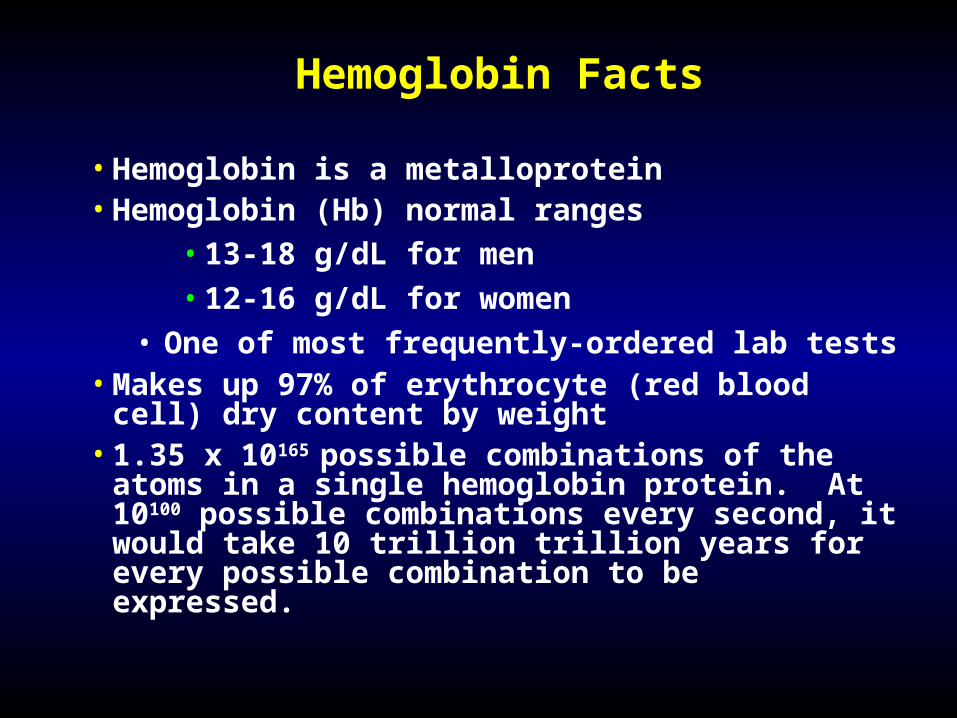
Hemoglobin Facts
• Hemoglobin is a metalloprotein• Hemoglobin (Hb) normal ranges
• 13-18 g/dL for men
• 12-16 g/dL for women
• One of most frequently-ordered lab tests• Makes up 97% of erythrocyte (red blood cell) dry
content by weight• 1.35 x 10165 possible combinations of the atoms in a
single hemoglobin protein. At 10100 possible combinations every second, it would take 10 trillion trillion years for every possible combination to be expressed.
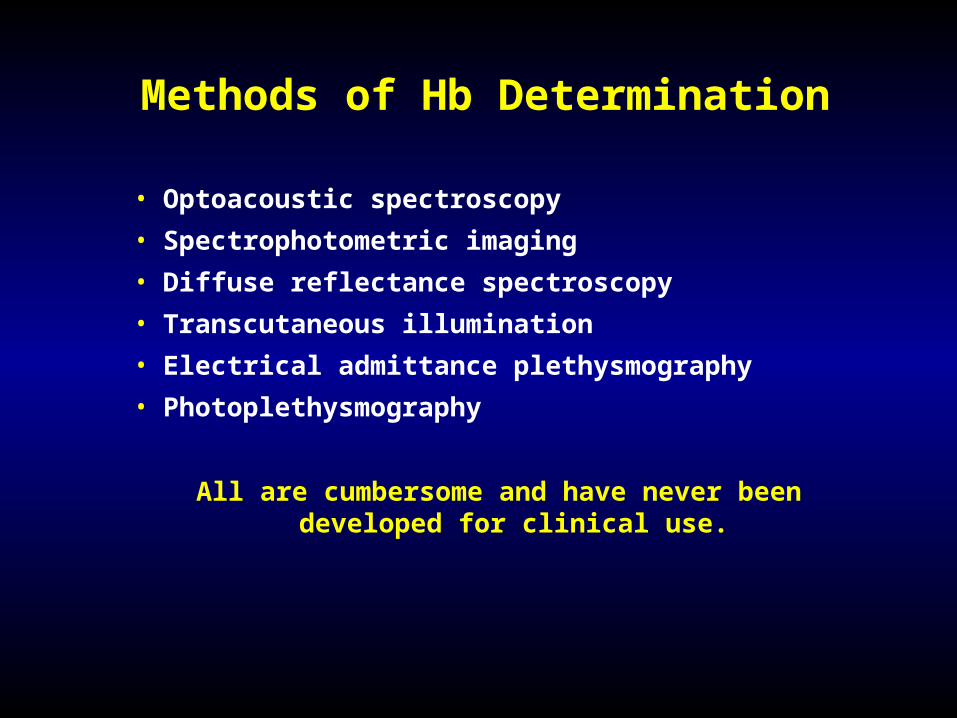
Methods of Hb Determination
• Optoacoustic spectroscopy
• Spectrophotometric imaging
• Diffuse reflectance spectroscopy
• Transcutaneous illumination
• Electrical admittance plethysmography
• Photoplethysmography
All are cumbersome and have never been developed for clinical use.
The Great Pulse Oximetry Debate
• Most brands of oximeters work equally well on 80 % of pts
• Masimo Signal Extraction Technology has the best performance during periods of motion artifact and low perfusion
• The lawsuit
• Claims and counter claims
• Sensors versus signal processing
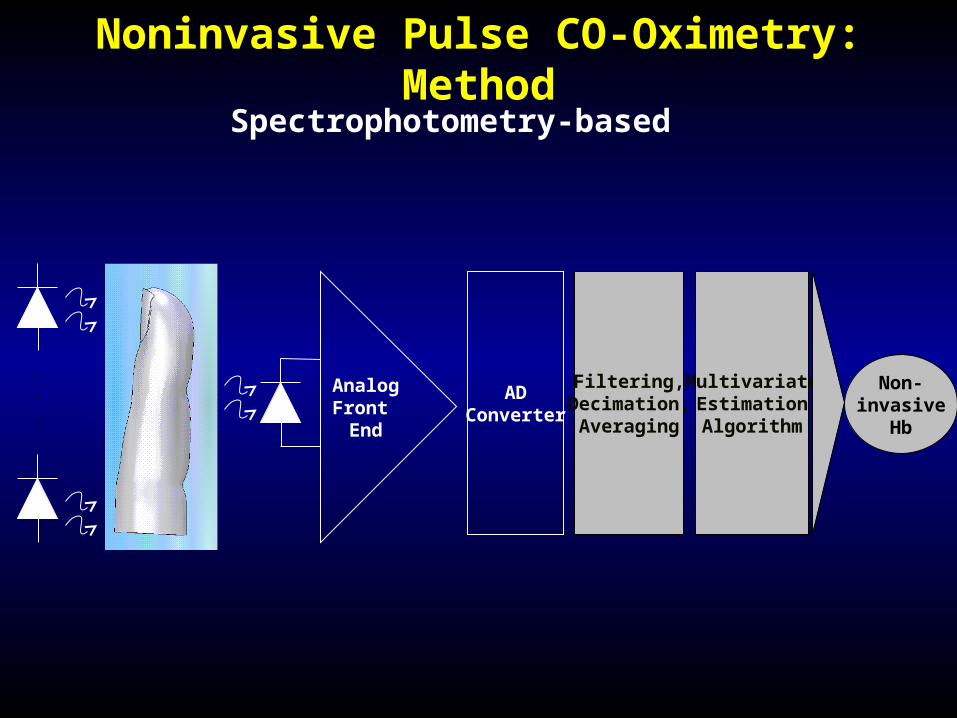
Noninvasive Pulse CO-Oximetry: Method
.
.
.
AnalogFront End
ADConverter
Filtering,Decimation,Averaging
MultivariateEstimationAlgorithm
Non-invasive
Hb
Spectrophotometry-based
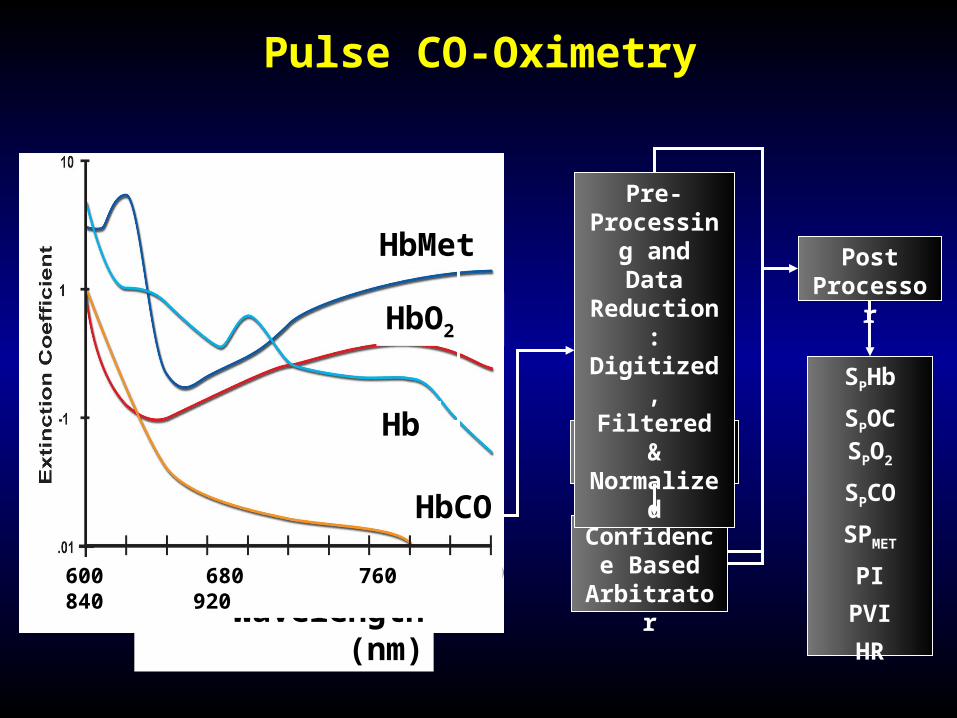
Pulse CO-Oximetry
Proprietary Algorithms
Confidence Based
Arbitrator
Pre-Processing
and Data Reduction: Digitized, Filtered &
Normalized
Post Processor
SPHb
SPOC SPO2
SPCO
SPMET
PI
PVI
HR
HbMet
HbO2
Hb
HbCO
Wavelength (nm)600 680 760 840 920
The Last 50 breathing treatments didn’t
work....but this one just might be the one.
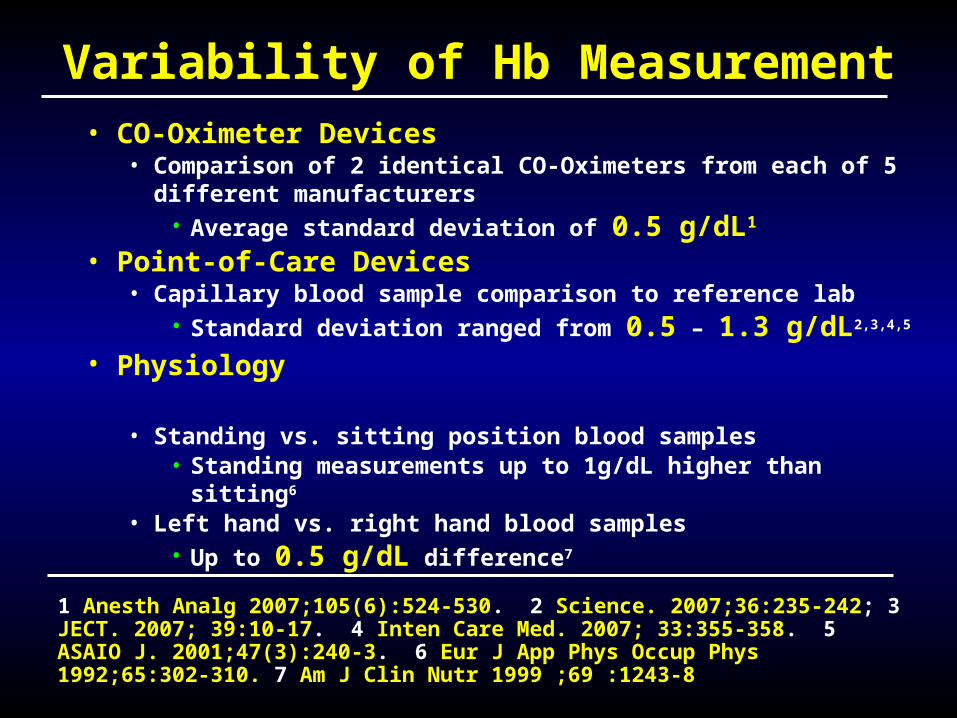
Variability of Hb Measurement• CO-Oximeter Devices
• Comparison of 2 identical CO-Oximeters from each of 5 different manufacturers
• Average standard deviation of 0.5 g/dL1
• Point-of-Care Devices• Capillary blood sample comparison to reference lab
• Standard deviation ranged from 0.5 – 1.3 g/dL2,3,4,5
• Physiology • Standing vs. sitting position blood samples
• Standing measurements up to 1g/dL higher than sitting6
• Left hand vs. right hand blood samples• Up to 0.5 g/dL difference7
1 Anesth Analg 2007;105(6):524-530. 2 Science. 2007;36:235-242; 3 JECT. 2007; 39:10-17. 4 Inten Care Med. 2007; 33:355-358. 5 ASAIO J. 2001;47(3):240-3. 6 Eur J App Phys Occup Phys 1992;65:302-310. 7 Am J Clin Nutr 1999 ;69 :1243-8
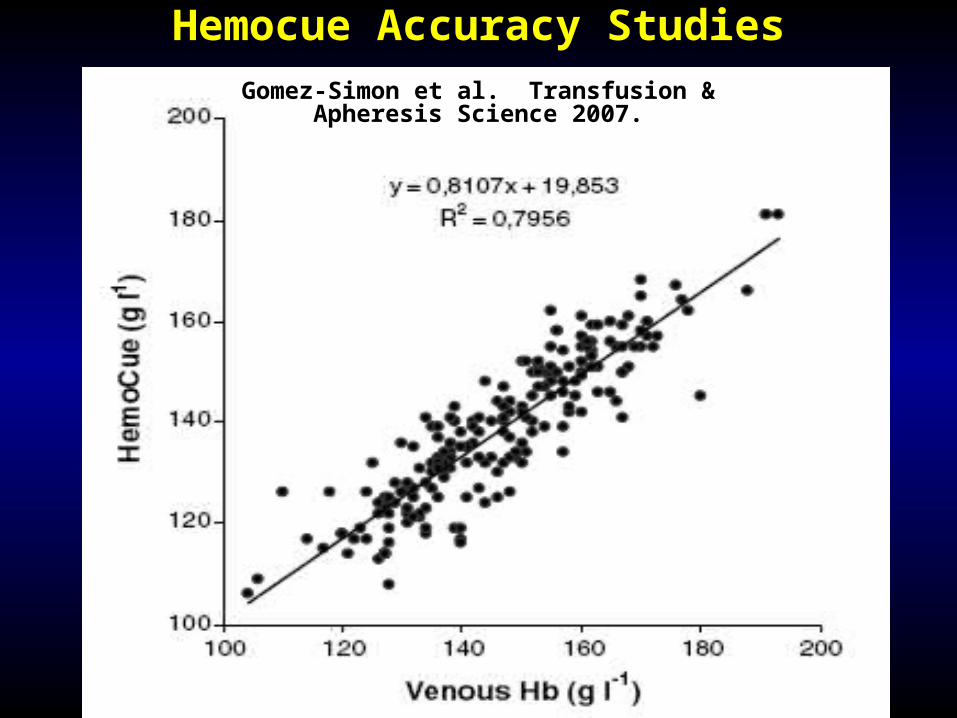
Hemocue Accuracy StudiesGomez-Simon et al. Transfusion &
Apheresis Science 2007.
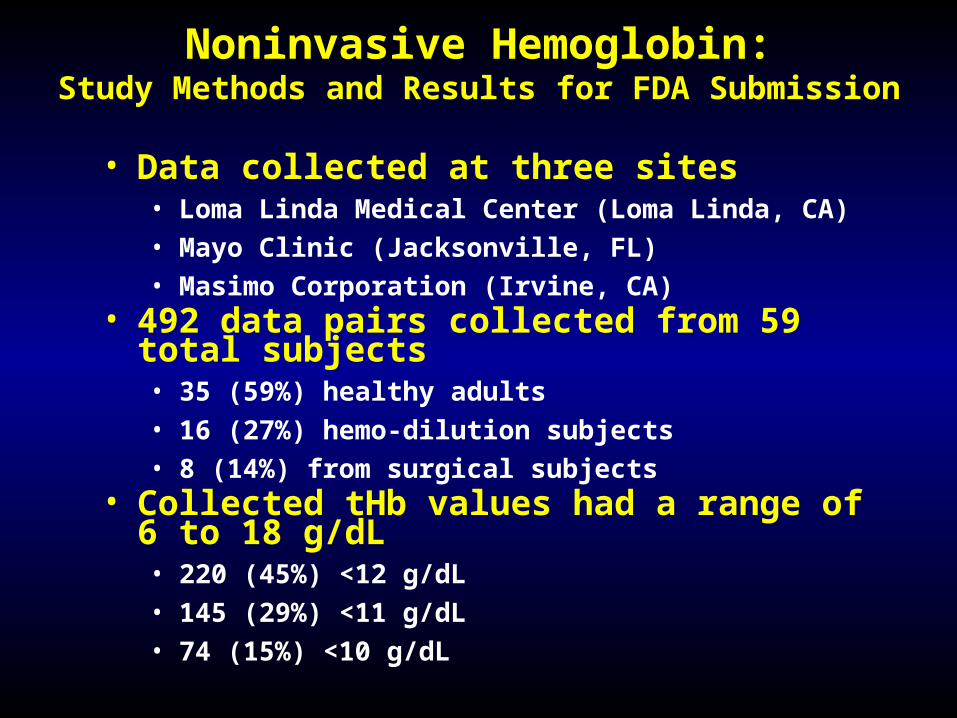
• Data collected at three sites• Loma Linda Medical Center (Loma Linda, CA)• Mayo Clinic (Jacksonville, FL)• Masimo Corporation (Irvine, CA)
• 492 data pairs collected from 59 total subjects• 35 (59%) healthy adults• 16 (27%) hemo-dilution subjects• 8 (14%) from surgical subjects
• Collected tHb values had a range of 6 to 18 g/dL• 220 (45%) <12 g/dL• 145 (29%) <11 g/dL• 74 (15%) <10 g/dL
Noninvasive Hemoglobin:Study Methods and Results for FDA Submission
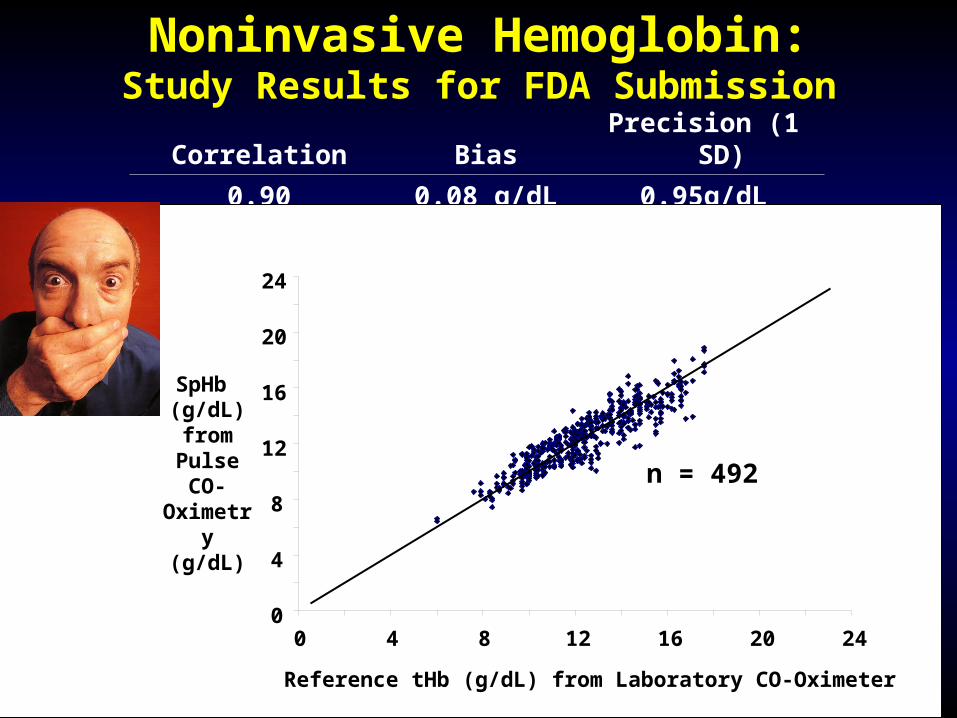
Noninvasive Hemoglobin:Study Results for FDA Submission
Correlation Bias Precision (1 SD)
0.90 0.08 g/dL 0.95g/dL
0
4
8
12
16
20
24
0 4 8 12 16 20 24
Reference tHb (g/dL) from Laboratory CO-Oximeter
SpHb (g/dL) from
Pulse CO-Oximetry
(g/dL)
n = 492
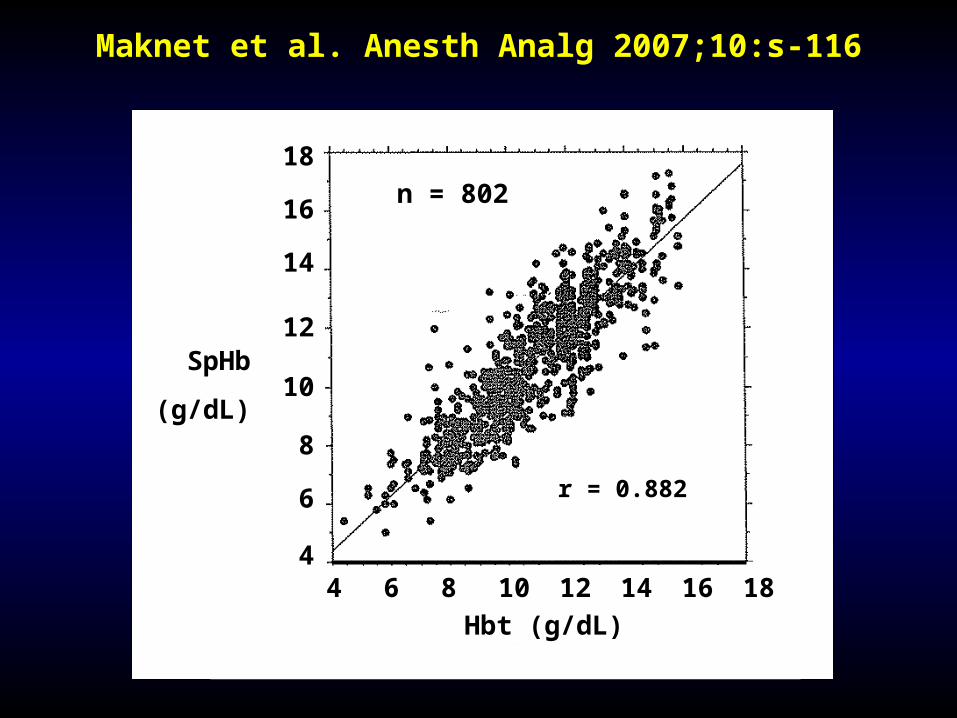
Maknet et al. Anesth Analg 2007;10:s-116
4 4 4 44 6 8 10 12 14 16 18
Hbt (g/dL)
18
16
14
12
10
8
6
4
SpHb
(g/dL)
r = 0.882
n = 802
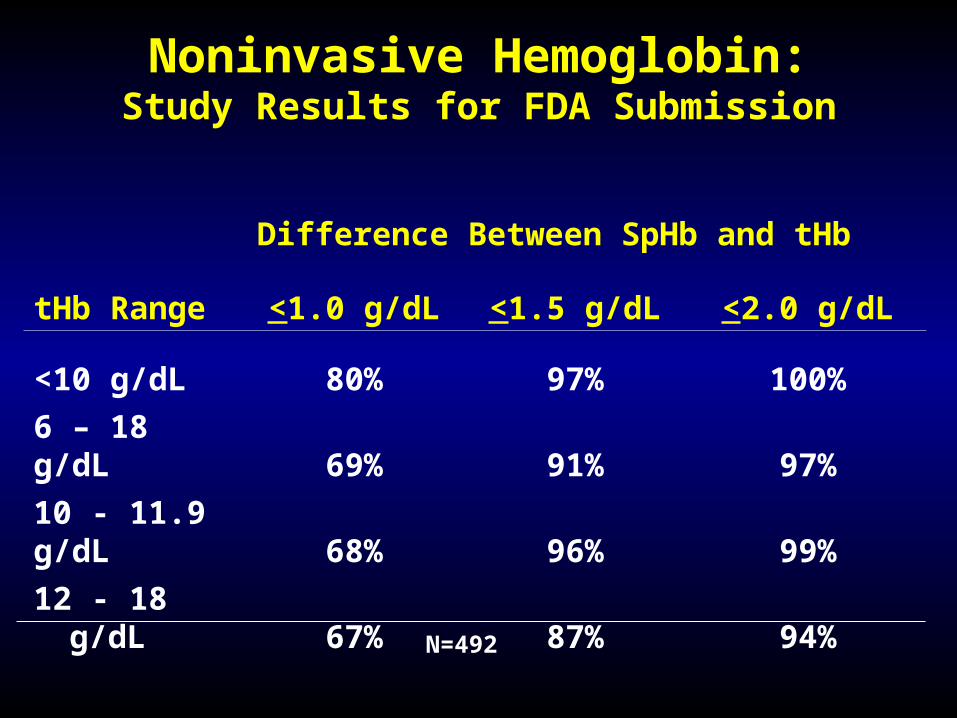
Noninvasive Hemoglobin:Study Results for FDA Submission
tHb Range
Difference Between SpHb and tHb
<1.0 g/dL <1.5 g/dL <2.0 g/dL
<10 g/dL 80% 97% 100%
6 – 18 g/dL 69% 91% 97%
10 - 11.9 g/dL 68% 96% 99%
12 - 18 g/dL 67% 87% 94%
N=492
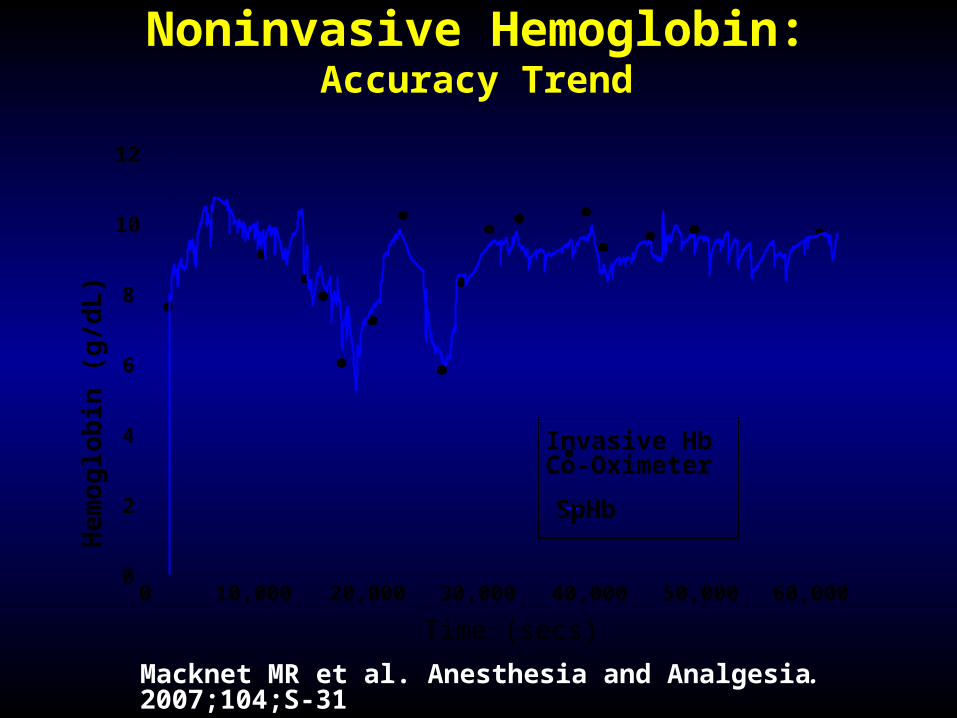
Noninvasive Hemoglobin:Accuracy Trend
Macknet MR et al. Anesthesia and Analgesia. 2007;104;S-31
0
2
4
6
8
10
12
0 10,000 20,000 30,000 40,000 50,000 60,000
Time (secs)
Hem
oglo
bin
(g/d
L)
SpHb
Invasive HbCo-Oximeter
Red
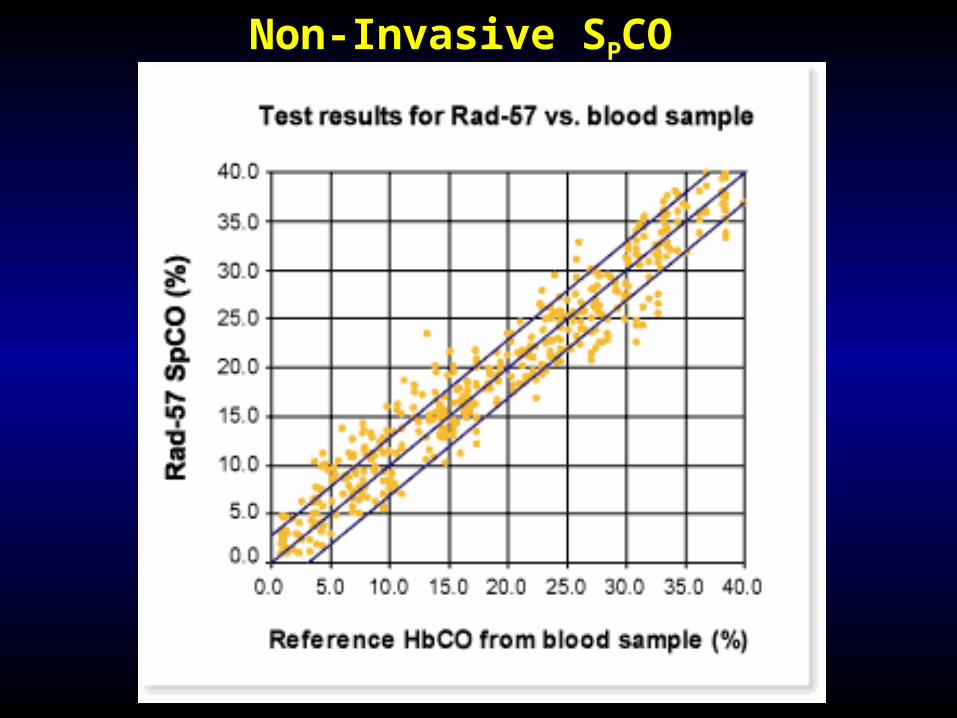
Non-Invasive SPCO
Potential Benefits of SPCO and SPMET
• SPCO
• Screening for carbon monoxide poisioning
• SPMET
• Screening for elevated levels of methemoglobinemia
• Inhaled nitric oxide therapy
• Certain poisons
Actual MD Notes in Charts
"Discharge status: Alive, but without my permission"
"The patient has been depressed since she began seeing me in 1993"
"The patient refused autopsy"
"The patient has no previous history of suicides"
Actual MD Notes in Charts
"Between you and me, we ought to be able to get this lady pregnant"
"She is numb from her toes down”
"Rectal examination revealed a normal sized thyroid"
"She stated that she had been constipated all of her life, until she got a divorce”
Actual MD Notes in Charts
And My All-time Favorite:
"The patient has two teen-aged children, but no other abnormalities"
Potential Uses-Benefits of SPHb
• Assessing Oxygenation Status• Assessing Anemia
• Operating Room• Emergency Room• Intensive Care
• Cost Savings
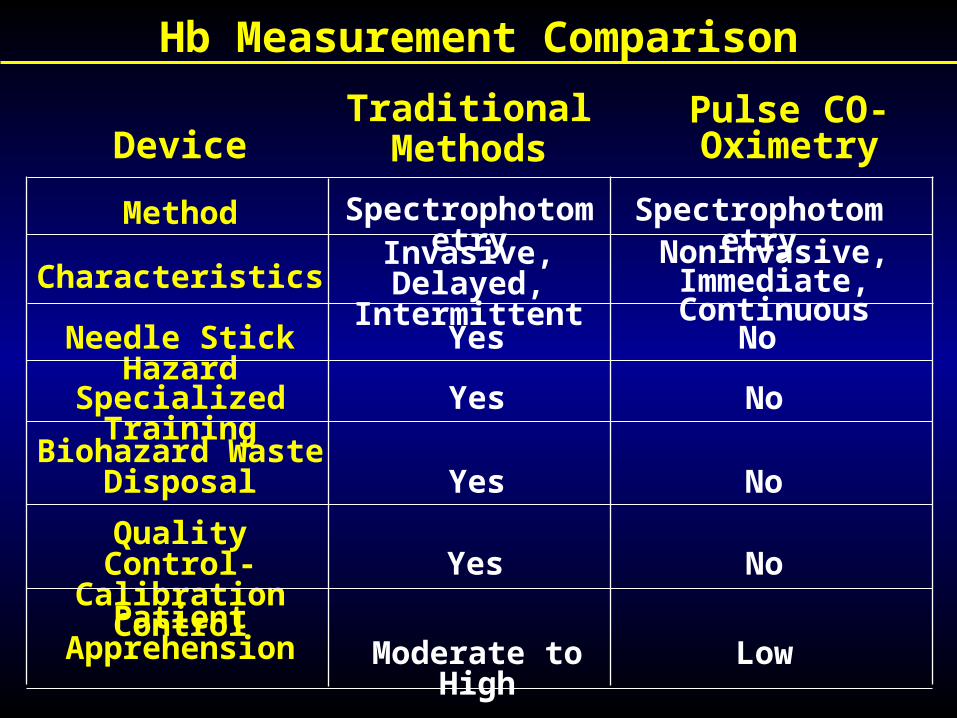
Hb Measurement Comparison
Device
Method
Characteristics
Needle Stick Hazard
Biohazard Waste Disposal
Quality Control-Calibration Control
Patient Apprehension
Traditional Methods
Pulse CO-Oximetry
Spectrophotometry SpectrophotometryInvasive, Delayed,
IntermittentNoninvasive, Immediate,
Continuous
Yes No
Yes No
Yes No
Yes No
Moderate to High Low
Specialized Training
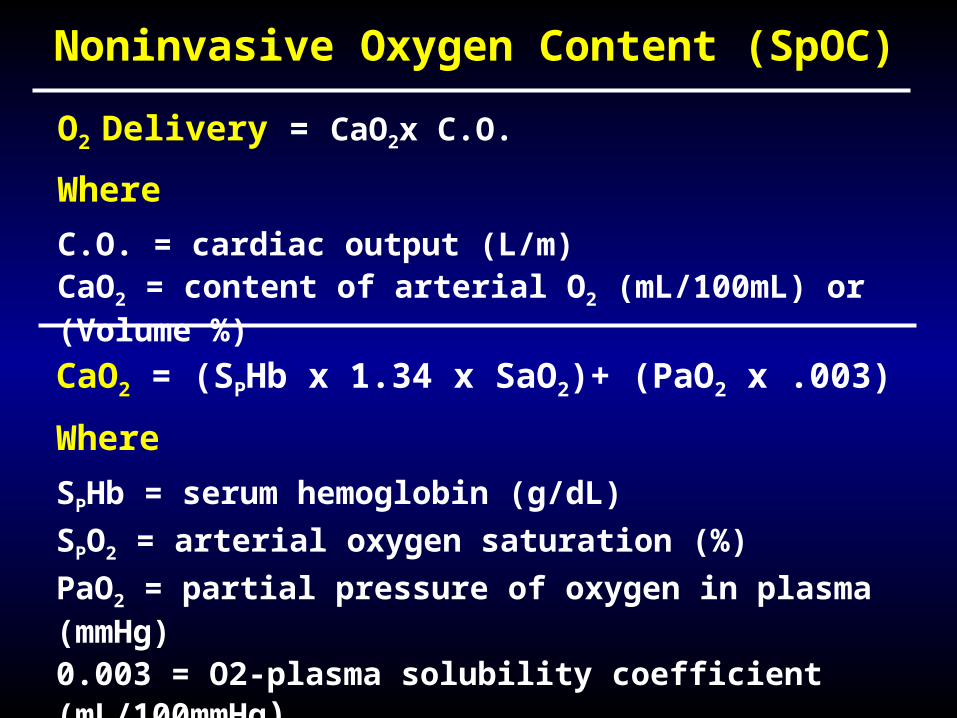
CaO2 = (SPHb x 1.34 x SaO2)+ (PaO2 x .003)
Where
SPHb = serum hemoglobin (g/dL)
SPO2 = arterial oxygen saturation (%)
PaO2 = partial pressure of oxygen in plasma (mmHg)
0.003 = O2-plasma solubility coefficient (mL/100mmHg)Normal = 20 mL/100mL or 20 volumes %
O2 Delivery = CaO2x C.O.
Where
C.O. = cardiac output (L/m)CaO2 = content of arterial O2 (mL/100mL) or (Volume %)
Noninvasive Oxygen Content (SpOC)
Blood Transfusions: Adverse Clinical & Financial Impact
• Adverse Clinical• Linked to higher morbidity and mortality• Linked to higher incidence of nosocomial infections and
multi-organ failure
• Financial• 9-44% of total transfusion costs are related to
inappropriate transfusions • Associated with increased hospital and ICU length of stay
• LOS 2-2.5 times longer vs. patients w/out transfusions
• Cost of blood has at least quadrupled over the last 20 years
• Many hidden costs associated with transfusion
Clinical Anesth. 2007:21(2);271-289.
Surgery 2007;142:S20-S25.
Noninvasive Hemoglobin
Potential Applications
• Initiate more timely blood transfusions• Avoid unnecessary transfusions• Decrease costs by more effectively titrating
blood and blood-replacement products
Benefits of Reducing Blood Transfusions
• TRICC randomized controlled trial in adult critical care• Compared liberal vs. restrictive transfusion strategies
• Restrictive group• Received 54% fewer red cell units• Overall - at least as effective as the liberal strategy• Associated with decreased mortality
• Implications - red cell transfusion• No longer “may help, can not hurt”• Approach as “first, do no harm”
Hebert PC et al. NEJM; 1999; 340; 409-417.
Cost of Blood Transfusions
• Steps in “cost of blood” equation• Donor costs
• Production of blood and transfusion logistics
• Actual transfusion
• Treatment of adverse transfusion outcomes
• Treatment of transfusion-transmitted disease
• Litigation
• Lost productivity
• True cost of blood often underestimated• Cost/unit ranged from $269 - $781
• Specialty-processed blood units• 40% - 230% higher than standard red cell units
Shander A et al. In Best Practice and Research Clinical Anes. 2007: Vol. 21(2); pp. 271-289.
From 1954 Popular Mechanics
Scientists from the RAND Corporation predict what the home computer will look like in the 2004
Because If They’re Not Breathing, They’re Not Doing Anything Else Either.
What Motivates You?
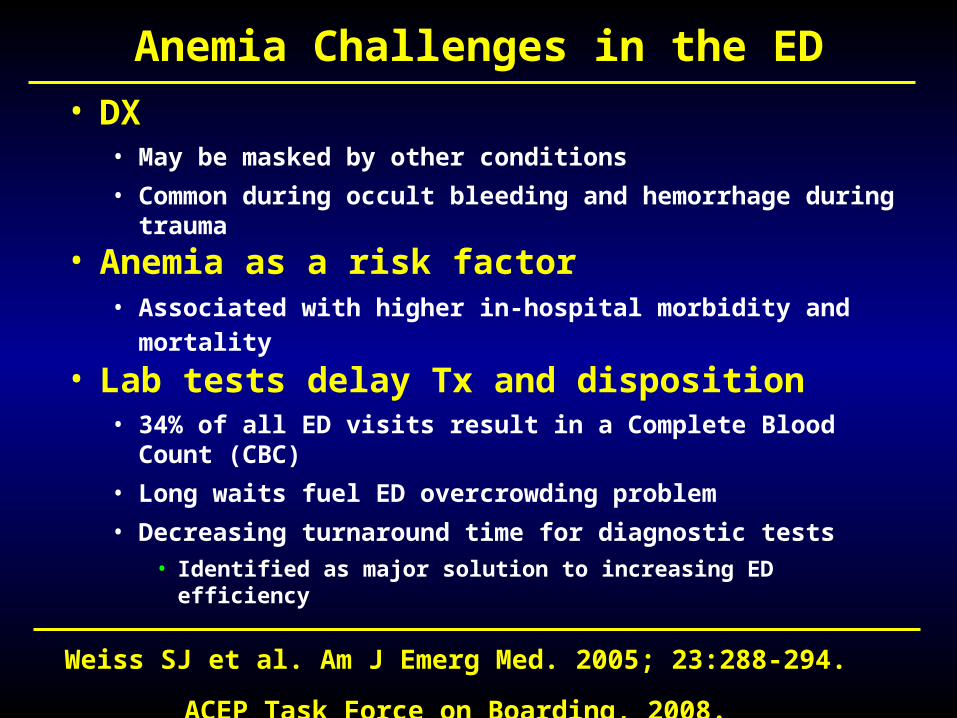
Anemia Challenges in the ED
• DX• May be masked by other conditions
• Common during occult bleeding and hemorrhage during trauma
• Anemia as a risk factor• Associated with higher in-hospital morbidity and mortality
• Lab tests delay Tx and disposition• 34% of all ED visits result in a Complete Blood Count (CBC)
• Long waits fuel ED overcrowding problem
• Decreasing turnaround time for diagnostic tests
• Identified as major solution to increasing ED efficiency
Weiss SJ et al. Am J Emerg Med. 2005; 23:288-294. ACEP Task Force on Boarding, 2008.
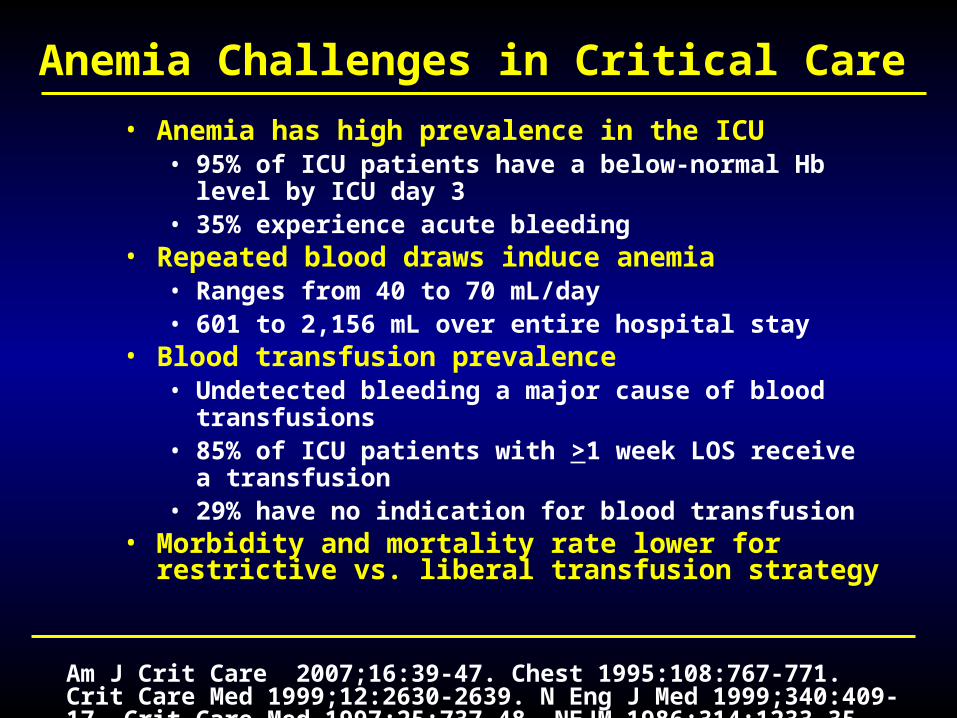
Anemia Challenges in Critical Care
• Anemia has high prevalence in the ICU• 95% of ICU patients have a below-normal Hb level by
ICU day 3• 35% experience acute bleeding
• Repeated blood draws induce anemia• Ranges from 40 to 70 mL/day• 601 to 2,156 mL over entire hospital stay
• Blood transfusion prevalence• Undetected bleeding a major cause of blood
transfusions • 85% of ICU patients with >1 week LOS receive a
transfusion• 29% have no indication for blood transfusion
• Morbidity and mortality rate lower for restrictive vs. liberal transfusion strategy
Am J Crit Care 2007;16:39-47. Chest 1995:108:767-771. Crit Care Med 1999;12:2630-2639. N Eng J Med 1999;340:409-17. Crit Care Med 1997;25:737-48. NEJM 1986;314:1233-35.
Noninvasive Hb: Summary
• Improved assessment of oxygenation
• Identify bleeding earlier• Allowing earlier interventions• Avoiding morbidity and
associated costs• Avoid induced anemia through
reduced blood draws• Avoid unnecessary transfusions
And You Thought You Had a Crummy Job