Embed Size (px)
Citation preview

The Second Annual ARS SummerSinus Symposium is taking place July19-20, 2013 in Chicago, IL at theWestin Michigan Avenue. Once again,this Symposium promises to be anexciting, highly educational programthat brings together interestedotolaryngologists in one forum todiscuss the latest aspects of rhinology,facial plastic surgery, reflux diseaseand obstructive sleep apnea.
On the first day, Dr. David Kennedywill kick off the event with a keynoteaddress, and this will be followed bypanels and discussions, which featurethe most seasoned experts discussingcommon situations and how tomanage even the most challenging
patients. Demonstration dissectionsperformed by Dr. Donald Lanza andDr. Michael Sillers will help surgeonsrefine their techniques in bothconventional sinus surgery as well asballoon dilation procedures. Audienceinteraction will be maximized tofacilitate discussion with the panelists.After an education-packed first day,join us on the 95th floor of the JohnHancock Tower to dine at theSignature Room and enjoy a fabulousskyline nighttime view of Chicago.
The second day will include a mixtureof combined and breakout sessionswhere attendees can select from avariety of subspecialty topics such asthe practice of allergy, rhinoplasty,
pediatric rhinology, practicemanagement and several excellentpanels featuring video and advicefrom the experts on “how they do it.”
Please come enjoy the fellowship ofyour Otolaryngology colleagues in oneof America’s great cities. Chicago hasmany engaging tourist attractions, aswell as opportunities for shopping,dining, theater, and professionalsports.
Participating physicians will have theopportunity to earn up to 16.75 AMAPRA Category 1 creditsTM. For details,please visit www.american-rhinologic.org/ars_courses.
www.american-rhinologic.org
join the ARS1
american rhinologic society
nose newsISSUE #2 May 2013
The American Rhinologic Society would like to thankAcclarent, Entellus, Olympus/Gyrus, SinuScience and Xoran
for partnering with the ARS Newsletter for 2013.
www.xorantech.com
Kevin C. Welch, MD, Rakesh Chandra, MD, James N. Palmer, MD
Summer Sinus Symposium 2013 - Just Around the Corner!
SinuScience
David Kennedy, MD (Keynote Speaker), Don Lanza, MDMichael Sillers, MD, Peter Hwang, MD, Tim Smith, MDJames Stankiewicz, MD, and many, many more...
2join the ARS
ARS OfficersTodd Kingdom, MDPresidentTimothy Smith, MDPresident-Elect James Palmer, MDSecretary Joseph Jacobs, MDTreasurerMichael Setzen, MDImmediate Past President Roy Casiano, MDFirst Vice President Peter Hwang, MDSecond Vice President
Board of DirectorsPete Batra, MDJohn DelGaudio, MDMarc Dubin, MDJoseph Han, MDRobert Kern, MD Rodney Schlosser, MD
Consultants to the BoardParul Goyal, MDRalph Metson, MDMichael Stewart, MDSarah Wise, MD
NoseNews EditorSarah K. Wise, MD
AdministratorWendi PerezPO Box 495, Warwick, NY 10990Tel:845.988.1631 Fax: [email protected]
SUMMER SINUS SYMPOSIUMJuly 19-20, 2013 Westin Michigan Avenue,Chicago, IL
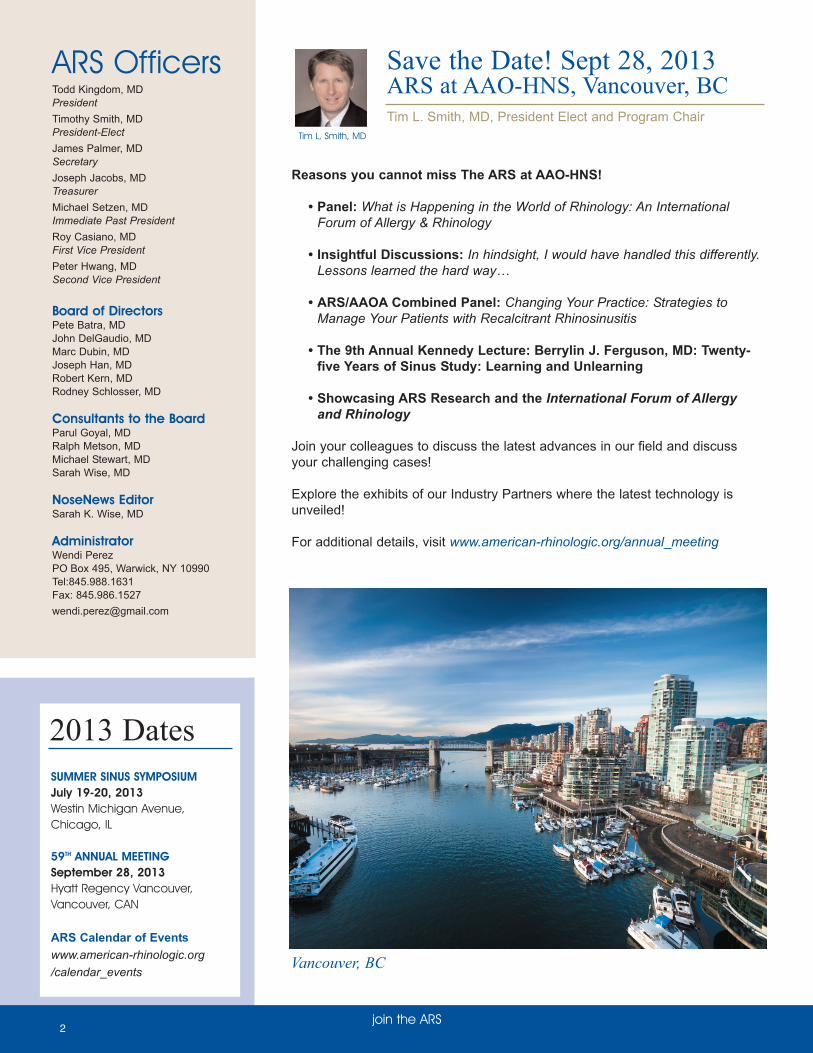
59TH ANNUAL MEETINGSeptember 28, 2013 Hyatt Regency Vancouver,Vancouver, CAN
ARS Calendar of Eventswww.american-rhinologic.org/calendar_events
2013 Dates
Reasons you cannot miss The ARS at AAO-HNS!
• Panel: What is Happening in the World of Rhinology: An International Forum of Allergy & Rhinology
• Insightful Discussions: In hindsight, I would have handled this differently. Lessons learned the hard way…
• ARS/AAOA Combined Panel: Changing Your Practice: Strategies to Manage Your Patients with Recalcitrant Rhinosinusitis
• The 9th Annual Kennedy Lecture: Berrylin J. Ferguson, MD: Twenty-five Years of Sinus Study: Learning and Unlearning
• Showcasing ARS Research and the International Forum of Allergy and Rhinology
Join your colleagues to discuss the latest advances in our field and discussyour challenging cases!
Explore the exhibits of our Industry Partners where the latest technology isunveiled!
For additional details, visit www.american-rhinologic.org/annual_meeting
Save the Date! Sept 28, 2013ARS at AAO-HNS, Vancouver, BCTim L. Smith, MD, President Elect and Program Chair
Tim L, Smith, MD
Vancouver, BC

33www.american-rhinologic.org
join the ARS
www.american-rhinologic.org
join the ARS
Summer is upon us, andI sincerely hope you are
able to enjoy this time with friends,family, and loved ones. Our meetingat COSM in Orlando was anenormous success on all fronts. Iwant to thank Program Chairman TimSmith and his committee for onceagain pulling together a wonderfulprogram that included broad andrelevant content. The next majorevent for the ARS on the calendar isthe Summer Sinus Symposium inChicago on July 19-20. Phenomenalefforts have come from our coursedirectors Rick Chandra and KevinWelch to make this a success.Additional information about this greatsummer program is contained in thisnewsletter. Then, moving on to thefall, we have our Annual Meeting inVancouver on September 28.Program Chairman Tim Smith willagain work his magic to deliver ascientific program that will provide atremendous breadth of clinical,research, and translational content forour members.
I would like to share a few commentsfrom our Board of Directors meetingheld in Orlando during COSM. Theenergy from our committee chairs andBoard leadership continues to beremarkable. The appetite to take onnew initiatives and explore differentopportunities has never been greater.With this comes challenges that wemust meet head on. Much of theconversation centered around ourgrowing educational and trainingprograms, the need to restructure anddefine our strategic initiatives inmarketing and communications, andour desire to expand our commitmentto research funding.
Sustainable funding for our researchefforts is a priority for the Board andme. The “Friends in Research”campaign for donations directed toresearch was launched in 2010 withearly initial success. I feel we can,and must, do better as a group. Ihave asked Board member Rob Kernto help me re-focus this importanteffort. I have challenged the Board ofDirectors and our committee chairs
with 100% participation over thecourse of the next 12-18 months. Ihope the all ARS members willparticipate at some level and helpsolidify our ability to remain thepremier organization fundingrhinologic research. Plans areunderway to revamp the on-linedonation process, but you may visithttp://www.american-rhinologic.org/donate to give today.Additional information andcommunications will be forthcomingas we roll out this important initiative.
I will close with thanking ourcorporate partners that continue toprovide tremendous support to ourmissions of research, training andeducation, and advocacy. Their initialresponse to our efforts to strengthenthis partnership has beenoverwhelmingly positive and a sourceof validation for what the Board istrying to achieve. I send out mysincere gratitude to the numerouscorporate partners that have steppedforth to work with us as we moveforward.
President’s ReportTodd Kingdom, MD
Todd Kingdom, MD
Once again,Rhinologic research
demonstrated substantial interest, asreflected in the number of grant sub-mission reviewed at the 2013 COREStudy Section review. The ARSreceived 16 proposals, one of thestrongest showings for a sister socie-ty and slightly more than we receivedlast year. This year we had one pro-posal in the New Investigator mecha-nism and two proposals in theResident Grant mechanism that wereworthy of funding and I would like tocongratulate this years ARS grantrecipients:
ARS Young Investigator Nithin Adappa, MD(University of Pennsylvania)“T2R38 Polymorphisms as a DiseaseModifier of CF ChronicRhinosinusitis”
ARS Resident Research AwardAdam Kimple, MD, PhD(University of North Carolina)“Regulator of G-Protein Signaling-22:a Putative Regulator of Motile Cilia”
Sarah Novis, MD(University of Michigan)“Variations in Antibiotic Usage for theTreatment of Acute Sinusitis”
Research Committee UpdateNoam Cohen, MD, PhD
Noam Cohen, MDThese awards will be officially acknowl-edged at the AAO-HNS Annual meetingin Vancouver on October 1st at 10:30 -hope to see you all there supportingour young Rhinologic researchers.
I would also like to extend my thanksand acknowledge the ARS memberswho spent substantial time and effort inreviewing the grants and serving on theCORE Study Section (Andrew Lane,Brad Woodworth, Eric Holbrook, SarahWise, Bruce Tan, Rod Schlosser, BenBleier, Murray Ramanathan, VijayRamakrishnan, Adam Zanation, ZachSoler, Eric Wang, Jay Pinto). We hopeto maintain this strong interest inRhinologic research and see evenmore applications next year.

join the ARS4
Patient Advocacy Committee (PAC)Corner: Proper Coding of Frontal SinusSurgery in 2013
Seth M. Brown, MD, MBA, FACS, PAC ChairSeth M. Brown, MD
For upcoming course information, visit:
www.american-rhinologic.org/ars_courses
One question I am often asked is how to properly code frontalsinus surgery. This has become more complex through the yearsas there are times where more than one approach is used for afrontal sinus (i.e. endoscopic assisted surgery), or for a moreextensive opening (i.e. frontal sinus drillout).
Furthermore, in 2012 we saw the emergence of new codes for bal-loon sinuplasty. The following sums up what should be done.
1. Every endoscopic code is a unilateral code (you may add a 50 modifier to these codes).
2.You may only use 1 code per sinus (i.e. you cannot bill an open code and an endoscopic code on the same sinus).
3.Understand that open codes fit into a 90 day global period and thus postoperative care, serial endoscopies and debridements are included in the code.
The most common frontal sinus codes and situations areexplained as follows:
1.31296 - when a balloon is used to open a frontal sinus and no additional dissection or tissue removal is done.
2.31276 - standard endoscopic frontal sinus code - for cannulation of the ostium and tissue removal.
3.Frontal sinus drill-out. No code exists. Options are to use 31276-50, 22 (plus image-guidance if used) or utilize the unlisted code 31299 and chose a comparison code when applying to the payor (I use an anterior skull base approach code). I prefer the unlisted code as I do not feel 31276 adequately describes the time, effort, risk and equipment required to per form this procedure.
4.Endoscopic assisted frontal sinusotomy (i.e. trephine and endoscopic) I use the endoscopic code 31276 and add the 22modifier (more complex than). This allows me a zero day global period and more appropriately describes that the main procedure was from below but the trephine was used for access (often used for a lateral cell).
Please feel free to contact the ARS for individual coding questionsor concerns.
The ARS, under the active leadershipof Todd Kingdom and the Board, hasundertaken a major revamping of our
fundraising process. Since our 50th AnniversaryMeeting, we have provided space for exhibitors, andour society has continued to knock on the door of ourcorporate partners to help support our educational,advocacy, and scientific programs. The ARS cannotexpand and serve our membership without thesecorporate relationships. Over time, as ourprogrammatic aspirations have increased, werecognized that a more secure and directedfundraising effort is required. Our administrator WendiPerez has always handled this responsibility inaddition to her other numerous roles and jobs.
In order to solidify and extend this process we haveestablished a Development Committee composed ofsenior members of the society. In addition, we haveenlisted the support of an additional staff member,Susan Arias, whose only responsibility will be toestablish and nurture corporate relationships. Our goalis to raise increasing amounts of funding to provideour membership with the underlying support that theydeserve. This is a time consuming as well as agrinding process, but we have been highly successfulin the initial 6 months and expect to raise over$500,000 to fund active society programs. I know thatwe will see the benefits of our program shortly.
Secondly, under the sound management of MellonBank our reserves are secure and are growing due tothe positive movement of the financial markets in thelast few years. However, due to our increasingexpenses we still depend on fundraising to avoid aloss of the corpus. So far, we are capable of doing so.In addition, in order to avoid a significant deficit I havebeen working with Shu Das, Chairman of the AuditCommittee, to secure this process. His report follows.
The Audit Committee of the ARS serves to assist theBoard of Directors in maintaining the overall integrity,financial credibility, and long-term viability of our non-profit organization. In this role, we serve as anindependent committee that reviews the governanceof our organization to mitigate risk and ensurecompliance with increasing federal, state, and locallaws and regulations facing the ARS and itsmembership; we assess business risk and providerecommendations to mitigate this risk, monitor ourfinancials, ensure internal and external audits of ourfinancials are performed on a timely and independentbasis, review our tax filings, and along with our Ethicscommittee, review our organization's conflict-of-interest, code-of-ethics, and whistleblower policies.Currently, the ARS is transitioning to a new financialaccountant; however, the audit committee hasmaintained an unqualified opinion without significantreservation in respect of matters contained within theARS financial statements for several years.
Treasurer’s ReportJoe Jacobs, MD
Joe Jacobs, MD
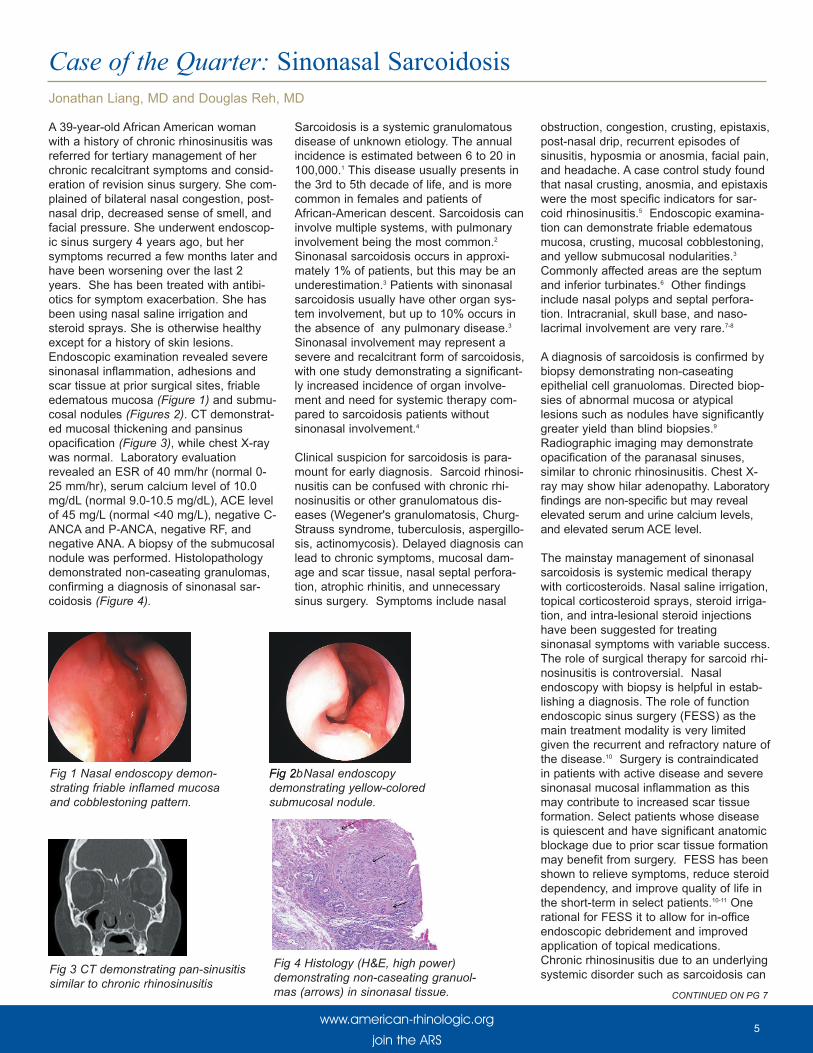
A 39-year-old African American womanwith a history of chronic rhinosinusitis wasreferred for tertiary management of herchronic recalcitrant symptoms and consid-eration of revision sinus surgery. She com-plained of bilateral nasal congestion, post-nasal drip, decreased sense of smell, andfacial pressure. She underwent endoscop-ic sinus surgery 4 years ago, but hersymptoms recurred a few months later andhave been worsening over the last 2years. She has been treated with antibi-otics for symptom exacerbation. She hasbeen using nasal saline irrigation andsteroid sprays. She is otherwise healthyexcept for a history of skin lesions. Endoscopic examination revealed severesinonasal inflammation, adhesions andscar tissue at prior surgical sites, friableedematous mucosa (Figure 1) and submu-cosal nodules (Figures 2). CT demonstrat-ed mucosal thickening and pansinusopacification (Figure 3), while chest X-raywas normal. Laboratory evaluationrevealed an ESR of 40 mm/hr (normal 0-25 mm/hr), serum calcium level of 10.0mg/dL (normal 9.0-10.5 mg/dL), ACE levelof 45 mg/L (normal <40 mg/L), negative C-ANCA and P-ANCA, negative RF, andnegative ANA. A biopsy of the submucosalnodule was performed. Histolopathologydemonstrated non-caseating granulomas,confirming a diagnosis of sinonasal sar-coidosis (Figure 4).
Sarcoidosis is a systemic granulomatousdisease of unknown etiology. The annualincidence is estimated between 6 to 20 in100,000.1 This disease usually presents inthe 3rd to 5th decade of life, and is morecommon in females and patients ofAfrican-American descent. Sarcoidosis caninvolve multiple systems, with pulmonaryinvolvement being the most common.2
Sinonasal sarcoidosis occurs in approxi-mately 1% of patients, but this may be anunderestimation.3 Patients with sinonasalsarcoidosis usually have other organ sys-tem involvement, but up to 10% occurs inthe absence of any pulmonary disease.3
Sinonasal involvement may represent asevere and recalcitrant form of sarcoidosis,with one study demonstrating a significant-ly increased incidence of organ involve-ment and need for systemic therapy com-pared to sarcoidosis patients withoutsinonasal involvement.4
Clinical suspicion for sarcoidosis is para-mount for early diagnosis. Sarcoid rhinosi-nusitis can be confused with chronic rhi-nosinusitis or other granulomatous dis-eases (Wegener's granulomatosis, Churg-Strauss syndrome, tuberculosis, aspergillo-sis, actinomycosis). Delayed diagnosis canlead to chronic symptoms, mucosal dam-age and scar tissue, nasal septal perfora-tion, atrophic rhinitis, and unnecessarysinus surgery. Symptoms include nasal
obstruction, congestion, crusting, epistaxis,post-nasal drip, recurrent episodes ofsinusitis, hyposmia or anosmia, facial pain,and headache. A case control study foundthat nasal crusting, anosmia, and epistaxiswere the most specific indicators for sar-coid rhinosinusitis.5 Endoscopic examina-tion can demonstrate friable edematousmucosa, crusting, mucosal cobblestoning,and yellow submucosal nodularities.3
Commonly affected areas are the septumand inferior turbinates.6 Other findingsinclude nasal polyps and septal perfora-tion. Intracranial, skull base, and naso-lacrimal involvement are very rare.7-8
A diagnosis of sarcoidosis is confirmed bybiopsy demonstrating non-caseatingepithelial cell granuolomas. Directed biop-sies of abnormal mucosa or atypicallesions such as nodules have significantlygreater yield than blind biopsies.9
Radiographic imaging may demonstrateopacification of the paranasal sinuses,similar to chronic rhinosinusitis. Chest X-ray may show hilar adenopathy. Laboratoryfindings are non-specific but may revealelevated serum and urine calcium levels,and elevated serum ACE level.
The mainstay management of sinonasalsarcoidosis is systemic medical therapywith corticosteroids. Nasal saline irrigation,topical corticosteroid sprays, steroid irriga-tion, and intra-lesional steroid injectionshave been suggested for treatingsinonasal symptoms with variable success.The role of surgical therapy for sarcoid rhi-nosinusitis is controversial. Nasalendoscopy with biopsy is helpful in estab-lishing a diagnosis. The role of functionendoscopic sinus surgery (FESS) as themain treatment modality is very limitedgiven the recurrent and refractory nature ofthe disease.10 Surgery is contraindicatedin patients with active disease and severesinonasal mucosal inflammation as thismay contribute to increased scar tissueformation. Select patients whose diseaseis quiescent and have significant anatomicblockage due to prior scar tissue formationmay benefit from surgery. FESS has beenshown to relieve symptoms, reduce steroiddependency, and improve quality of life inthe short-term in select patients.10-11 Onerational for FESS it to allow for in-officeendoscopic debridement and improvedapplication of topical medications.Chronic rhinosinusitis due to an underlyingsystemic disorder such as sarcoidosis can
5
Case of the Quarter: Sinonasal SarcoidosisJonathan Liang, MD and Douglas Reh, MD
www.american-rhinologic.org
join the ARS
Fig 3 CT demonstrating pan-sinusitissimilar to chronic rhinosinusitis
Fig 1 Nasal endoscopy demon-strating friable inflamed mucosaand cobblestoning pattern.
Fig 2b Fig 2 Nasal endoscopydemonstrating yellow-coloredsubmucosal nodule.
Fig 4 Histology (H&E, high power)demonstrating non-caseating granuol-mas (arrows) in sinonasal tissue. CONTINUED ON PG 7

6
Topical therapies have emerged as anintegral component in the comprehensivemanagement of chronic rhinosinusitis(CRS). Such targeted application affordsthe theoretical advantage of deliveringhigh concentrations of therapeutic agentsdirectly to diseased sinonasal mucosawhile reducing the risk of systemicabsorption and associated adverseeffects. Because irrigant penetration intounoperated sinuses is minimal (<2%),endoscopic sinus surgery (ESS) is pivotalin providing effective sinonasal distribu-tion of topical solutions. Currently, oto-laryngologists are confronted with a myri-ad of topical preparations available forCRS. We will briefly summarize thesevarious treatment strategies and theaccompanying evidence for each regi-men.
TOPICAL SALINE: The benefits of topi-cal saline irrigations in the treatment ofCRS have been well documented. In aCochrane review of 8 randomized controltrials (RCTs), Harvey, et al. determinedthat saline irrigations improved both CRSsymptoms and quality-of-life (QOL) whenused as the sole treatment modality andas adjunctive therapy (Harvey 2007).However, whether isotonic or hypertonicsaline (HS) is more effective still remainscontroversial. Hypertonic solutions havebeen shown to reduce symptoms inpatients with cystic fibrosis (CF) and asth-ma, but have also been associated withimpaired ciliary activity as well as localadverse effects (i.e. nasal irrigation, burn-ing, pain). No significant differences wereidentified between isotonic versus (vs.)HS in terms of symptom, nasal endoscop-ic (NE), or radiographic scores in theCochrane review. Thus, although salineirrigations are currently indicated in themanagement of CRS; definitive recom-mendations regarding optimal concentra-tion, frequency, and mode of delivery can-not be made at this time.
TOPICAL STEROIDS: The clinical effica-cy of intranasal steroids (INS) in the treat-ment of CRS is well-established; and theiruse as first-line therapy has been recom-mended by multiple evidence-based stud-ies. (Fokkens 2012, Rudmik 2012).Administration of off-label topical steroidpreparations (i.e. budesonide 0.5mg/2mlin 240ml saline) has also becomeincreasingly more common as a promis-
ing alternative to systemic steroids in thepost-operative management of CRS. In arecent prospective uncontrolled study,post-ESS steroid irrigations (budesonide1mg or betamethasone 1mg, 240mlsaline) led to significantly improved symp-tom, QOL, and NE scores in 111 CRSpatients (Snidvongs 2013). Such steroidsolutions have been shown to be well tol-erated in the short-term, with no evidenceof hypothalamic-pituitary-adrenal axissuppression as measured by changes inserum or 24-hour urinary cortisol.However, no RCTs have demonstratedtheir superiority over INS or saline rinses.In a double-blinded (DB) RCT of 60Samter's CRS patients randomized tosaline lavages (240ml), budesonide spray(64ug per nostril twice daily), or budes-onide saline irrigations; no significant dif-ferences in symptom, NE, or imagingscores were observed 6 months and 1year after treatment (Rotenberg 2011).Consequently, steroid delivery via irriga-tion modalities still warrants further inves-tigation to determine clinical efficacy aswell as the safety of long-term use.
TOPICAL ANTIFUNGALS: Since funguswas first postulated to contribute to thepathogenesis of CRS, extensive researchhas been conducted assessing the effec-tiveness of topical antifungal therapies.In the initial pilot study, intranasal ampho-tericin lavages appeared to successfullyreduce mucosal inflammation in CRS onboth imaging and NE after 6 months(Ponikau 2005). However, these resultshave not been replicated in subsequenttrials. Four DB-RCTs involving muchlarger patient cohorts failed to demon-strate any significant differences in sub-jective (symptom, QOL) or objective (NE,imaging) outcomes between CRSpatients treated with topical amphotericinvs. placebo (Ebbens 2006, Weschta2006, Liang 2008, Gerlinger 2009). Inaddition, 2 recent meta-analyses inde-pendently concluded that topical antifun-gals were not beneficial in the manage-ment of CRS based on a review of theaggregate evidence (Isaacs 2011, Sacks2011). Consequently, topical antifungaltherapy is not currently recommended inthe treatment of routine CRS.
TOPICAL ANTIBIOTICS: Thus far, theuse of topical antibiotics in CRS has onlybeen supported by low-level studies.
Optimal outcomes are achieved in post-surgical patients given culture-directed asopposed to empiric therapy (Lim 2008).Administration of topical antibiotics vianebulizer or spray techniques have failedto demonstrate significant clinical benefitsand their use has not been recommended(Rudmik 2012). However, topical antibi-otics delivered via irrigation methodshave shown promise in the treatment ofrefractory CRS. Tobramycin lavages havebeen reported to decrease nasal polypo-sis and the need for revision surgery inCF patients with Pseudonomas aerugi-nosa (PA) positive recalcitrant CRS (Moss1995). Likewise, mupirocin irrigationshave been found to significantly improvesymptoms, NE scores, and culture ratesin Staphylococcus aureus (SA) positiverefractory CRS (Solares 2006, Uren2008, Jervis-Bardy 2012). However, a73.7% re-culture positivity rate has alsobeen observed following therapy, so it isunclear if such benefits are sustainablelong-term. Additional research is stillrequired to elucidate the clinical implica-tions of microbiological relapse, risk ofsystemic toxicity, and development ofantibiotic resistance associated with pro-longed use. Therefore, topical antibioticsare not recommended as first-line therapyfor routine CRS, but can be consideredas a potential option for patients withrecalcitrant CRS who have failed tradi-tional medical and surgical intervention.
TOPICAL ADDITIVES: A vast array ofalternative agents with antimicrobial, anti-inflammatory, and immunomodulatoryproperties have been introduced aspotential additives to irrigation solutions.Manuka honey (MH) exhibits microbicidalactivity against SA/PA biofilms in vitro,and symptomatic improvement in CRSpatients has been reported with topicalapplication of MH mixtures (Thamboo2011). Likewise, dead sea salt rinses,which contain unique minerals with anti-inflammatory effects, have been shown toimprove symptoms and QOL in CRSpatients (Friedman 2012). Xylitol, anorganic sugar alcohol which enhancesthe potency of endogenous antimicrobialfactors, was also observed to significantlydecrease symptom scores in post-ESSCRS patients compared to saline (Brown2004). Finally, surfactants have potentiallydual benefits in the treatment of CRS,acting as both a mucolytic agent as well
join the ARS
Rhinology Perspectives: Topical Therapies in the Treatment of ChronicRhinosinusitisJivianne Lee, MD and Alex Chiu, MD

7
The International Forumof Allergy and Rhinology
(IFAR) began monthly publication inJanuary 2013, becoming the only sub-specialty journal within the field ofRhinology with 12 editions each year.This allows the Journal to decrease thetime for authors from article submissionto print publication. The Journal has alsopreviously been accepted for Medlineand ISI Impact Factor rating. Both ofthese extend back to the first edition ofthe Journal. Although the initial ImpactFactor is anticipated to be low, this willrapidly change. The Impact Factor isbased upon the average number of cita-tions and new journals do not have a sig-nificant track record of cited articles.Additionally, the calculations are basedupon an annual rolling average.However, the Editorial Board, the soci-eties (ARS, AAOA, IRS and ISIAN) andthe publishers (Wiley) are all committedto ensuring that this becomes a leadingjournal within the broader specialty.Accordingly, the Impact Factor will rapid-ly grow, and as the Impact Factor of theJournal continues to grow, additionalprestige will be added for authors whosubmit or who have already published inIFAR. The goal of the involved societies
is to ensure that IFAR is the premierejournal in the field internationally, as wellas developing online Journal educationalcontent for the societies. In each printedition, we try to keep a balancebetween basic research and clinicalpapers, and thus, the time to print publi-cation for more basic research tends tobe shorter than for clinically relatedpapers.
Even prior to print publication, articlesare published online and the online pub-lications are indexed in PubMed prior toprint publication. In 2012 there were35,681 IFAR articles downloaded fromthe Journal website. Wiley, as is cus-tomary when new journals havematured, started charging institutions foronline access in January 2013. I wouldbe very grateful if you would verifywhether your library has access tothe Journal at this point in time, andif not, please ask your librarian to obtainaccess to the Journal for residents,medical students and other otolaryngol-ogists who may not have a subscriptionthrough the societies. In addition to pro-viding an important educational opportu-nity within the field of rhinology, thewider such access occurs, the more
rapidly a major impact factor will evolvefor the Journal. Advertising, an impor-tant component for the long-term finan-cial success of the Journal, has contin-ued to grow nicely despite an overalltight economic environment.
With each edition, I have elected toeither write myself, or have one of theAssociate Editors write, an editorialhighlighting some of the articles in theJournal and providing some additionalperspective. I hope that you, as thereadership, enjoy the editorial and Iwould welcome your feedback andother comments regarding IFAR.
International Forum of Allergy and Rhinology (IFAR) UpdateDavid W. Kennedy, MD, IFAR Editor
www.american-rhinologic.org
join the ARS
be under-recognized even amongst oto-laryngologists. The aforementioned endo-scopic findings and laboratory evaluationshould raise clinical suspicion of sarcoido-sis which should prompt directed biopsiesto establish a histopathologic diagnosis.Corticosteroid therapy is the mainstay ofmanagement, and the role of FESS is limit-ed and controversial.
References1. Braun JJ, Gentine A, Pauli G. Sinonasal sarcoidosis:review and report of fifteen cases. Laryngoscope. Nov2004;114(11):1960-1963.2. Baughman RP, Lower EE, du Bois RM. Sarcoidosis.Lancet. Mar 29 2003;361(9363):1111-1118.3. McCaffrey TV, McDonald TJ. Sarcoidosis of the noseand paranasal sinuses. Laryngoscope. Oct1983;93(10):1281-1284.4. Aubart FC, Ouayoun M, Brauner M, et al. Sinonasalinvolvement in sarcoidosis: a case-control study of 20patients. Medicine (Baltimore). Nov 2006;85(6):365-371.5. Reed J, deShazo RD, Houle TT, Stringer S, WrightL, Moak JS, 3rd. Clinical features of sarcoid rhinosi-nusitis. Am J Med. Sep 2010;123(9):856-862.6. Tay HL, Vaughan-Jones R, Qureshi SS. Ethmoidalsarcoidosis. J Laryngol Otol. Aug 1994;108(8):682-684.7. Dessouky OY. Isolated sinonasal sarcoidosis withintracranial extension: case report. ActaOtorhinolaryngol Ital. Dec 2008;28(6):306-308.8. Fergie N, Jones NS, Downes RN, Bingham BJ.Dacryocystorhinostomy in nasolacrimal duct obstructionsecondary to sarcoidosis. Orbit. Sep 1999;18(3):217-222.9. Wilson NJ, King CM. Cutaneous sarcoidosis.Postgrad Med J. Nov 1998;74(877):649-652.10. Kay DJ, Har-El G. The role of endoscopic sinus sur-gery in chronic sinonasal sarcoidosis. Am J Rhinol. Jul-Aug 2001;15(4):249-254.11. Long CM, Smith TL, Loehrl TA, Komorowski RA,Toohill RJ. Sinonasal disease in patients with sarcoido-sis. Am J Rhinol. May-Jun 2001;15(3):211-215.
David Kennedy, MD
as a biocide with antibiofilm capabilities. In a prospective uncontrolled study, 1%baby shampoo irrigations improved overall symptoms, mucus thickness, and post-nasal discharge in refractory CRS patients (Chiu 2008). However, a subsequentRCT did not demonstrate any significant differences in symptoms, QOL, or olfactionthresholds between CRS patients given 1% baby shampoo irrigations vs. HS follow-ing routine ESS (Farag 2012). Issues with patient tolerability (nasal burning,headache), ciliotoxicity, and smell disturbances have also been reported dependingon the type of surfactant used. Thus, although topical additives may have a promis-ing role as adjunctive treatment for recalcitrant CRS, more studies are needed toinvestigate their clinical efficacy in comparison to other agents and establish respec-tive safety profiles.
CONCLUSION: The use of topical therapies for the treatment of CRS has expandedin scope and popularity over the past decade. The evidence is strongest for the useof saline irrigations but efficacy studies have been mixed over the use of topical anti-infectives, anti-inflammatories and other additives such as surfactant solutions.Despite this, these topical therapies retain promise in the treatment of post-ESSpatients who remain symptomatic despite adequate technical surgery and the use oftopical steroid sprays and saline irrigations. Further research is needed to betterelucidate the patient populations who will most benefit from each individual irrigationas well as to limit local side effects.
Rhinology Perspectives, continued from previous page
Case of the Qtr, continued from pg 5
8join the ARS
If you would like have your upcoming rhinology meeting noted here, simply provide the editor with pertinent information: [email protected] American Rhinologic Society does not endorse these meetings but simply provides the list as a service to its members.
The content of Nose News represents the opinions of the authors and does not necessarily reflect the opinions of the American Rhinologic Society.The American Rhinologic Society Newsletter Editorial Office
c/o Sarah K. Wise, MD, Emory Department of Otolaryngology, 550 Peachtree St., MOT 9th Floor, Atlanta, GA 30308Editor: Sarah K. Wise, MD l [email protected]
NON-PROFIT ORG.US POSTAGE PAID
WINONA, MNPERMIT NO. 193
American Rhinologic SocietyWendi PerezAdministratorPO Box 495Warwick, NY 10990
Note from the President:Note from the President:If you are a general otolaryngologist working in a community setting, the American
Rhinologic Society wants you! We want you to be a member, and we want you to participate in the committee structure and leadership of the society. The ARS is the only society within otolaryngology dedicated to promoting education, research, and advocacy issues related to rhinology, sinus, and skull base surgery. Our journal, International Forum of Allergy and Rhinology, is thelargest circulation rhinology journal presenting cutting edge and relevant rhinology information in an age of Maintenance of Certification--and it's a benefit of your membership. In short, the American Rhinologic Society deals with the issues you deal with and is concernedwith the issues you are concerned with. Numbers matter - please consider joining, and getting involved, in our society.
Please return to: American Rhinologic Society, PO Box 495, Warwick, NY 10990 Fax: 845-986-1527, Email: [email protected]
Please Print Clearly:
First Name: _________________________ Last Name: _________________________ Degree: ___________________________
Business Address: ____________________________________________________________________________________________
City:___________________________ State:_____________ ZipCode:_____________________
Tel:_____________________________ Ext.______ Fax: _______________________________
Email: ______________________________________ Web Address:______________________
The ARS wants to serve our members. Please help us get to know you.Please list issues that you feel are important to the field of Otolaryngology:
1) _________________________________________________________________________________________________________
2) _________________________________________________________________________________________________________
Please list committees that you may be interested in participating in: For a complete list of ARS committees, please go to www.american-rhinologic.org
1) ____________________________________________ 2) ____________________________________________
3) ____________________________________________ 4) ____________________________________________
Are you in Private Practice? __Yes __ No
Current Hospital affiliation: ____________________________________________ Academic Title: ___________________________
Have you ever attended an ARS meeting? __Yes __ No If yes, when? ___________________________________
The American RhinologicSociety wants YOU!