Embed Size (px)
Citation preview
Northern Local Commissioning Group Locality
Population Plan
2
Foreword The Northern Local Commissioning Group and the Northern Health and Social Care Trust have collaborated to produce this Population Plan in response to Transforming Your Care. This is a time of change and of challenge for the Northern Local Commissioning Group Locality and we want to ensure that the health and social care services we commission and provide are safe, sustainable and resilient. At the same time it is incumbent on us to address and facilitate the transformational change agenda in Transforming Your Care and our plan reflects the actions we will take to make that change a reality.
Key to the change will be the ‘shift left’ of activity and resources into primary and community care settings. With increasing demand on services and budgets comes the need to reshape care pathways that deliver seamless care to patients and clients and make best use of resources. The development of Integrated Care Partnerships will be our flagship project to help us deliver on this vision. Involving primary, community and secondary care partners and the voluntary and community sector, we believe that we can better organise care and services around the individual with better communication and networking across the system. Technology will be a key enabler of the delivery of this model of care, in particular in supporting care closer to home and allowing staff to work in effective, integrated teams.
Our Plan is for the next three years but it signals the direction of travel for health and social care beyond that. This is a journey to which we are committed and together we will work to ensure effective stakeholder engagement to ensure that the needs of our population are at the heart of this process.
Dr Brian Hunter Mr Sean Donaghy
Chair NLCG Chief Executive, NHSCT
3
Purpose of Document
Each Local Commissioning Group (LCG) and Health & Social Care (HSC) Trust within Northern Ireland, along with broader engagement with colleagues in Primary Care Partnerships, has been tasked to develop an area based Population Plan by June 2012 in response to Transforming Your Care, the regional independent Review of Health and Social Care Services. This population plan for the Northern Local Commissioning Group Locality explains how the growing needs and expectations within the locality will be addressed within a strictly constrained financial context, while ensuring that quality is improved and optimum outcomes achieved, through transforming the way care is delivered, both in terms of health care and social care. The plan sets out to ensure and demonstrate that optimum use is being made of existing resources across the locality, both within HSC organisations, and within partnership arrangements with independent sector providers. It outlines the approach and key milestones for the delivery of the transformational change agenda outlined in Transforming Your Care, whilst also taking account of local needs, expectations for the future and existing resources. It describes the development of new integrated arrangements for the planning and delivery of services to achieve optimum outcomes for service users and the broader community, transcending existing organisational structures and boundaries that impede effective person centered care. The success of the Population Plan will be measured in the achievement of the core principles underpinning the transformation plan, including a focus on preventing avoidable ill-health, personalisation of care, improved access to care and support for those who most need it at the time, supporting individuals to live independent and fulfilling lives.
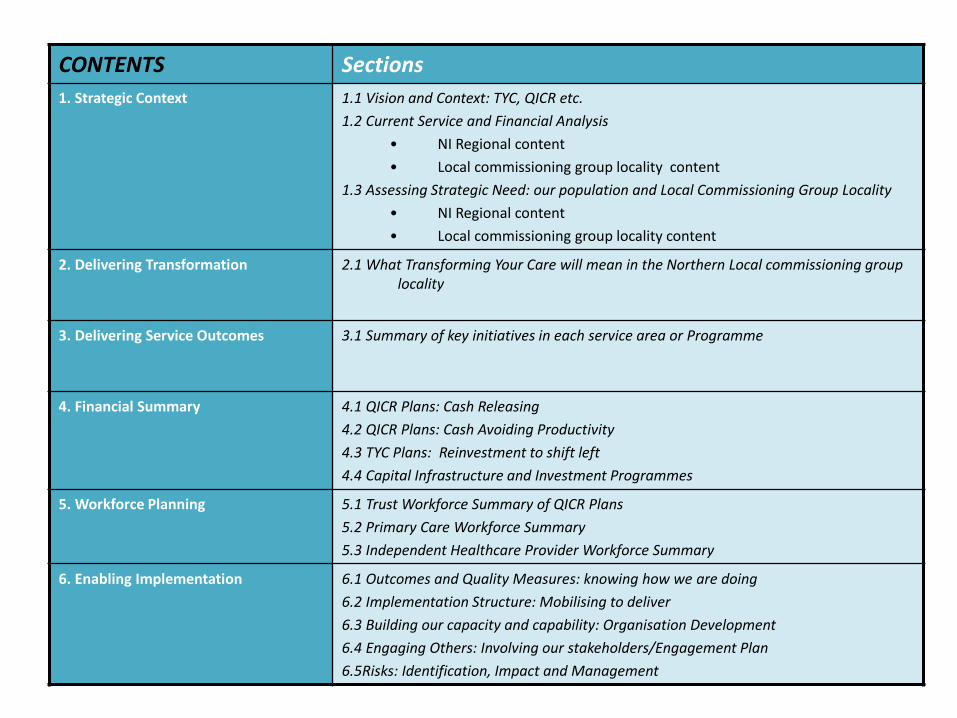
CONTENTS Sections
1. Strategic Context
1.1 Vision and Context: TYC, QICR etc.
1.2 Current Service and Financial Analysis
• NI Regional content
• Local commissioning group locality content
1.3 Assessing Strategic Need: our population and Local Commissioning Group Locality
• NI Regional content
• Local commissioning group locality content
2. Delivering Transformation 2.1 What Transforming Your Care will mean in the Northern Local commissioning group locality
3. Delivering Service Outcomes 3.1 Summary of key initiatives in each service area or Programme
4. Financial Summary 4.1 QICR Plans: Cash Releasing
4.2 QICR Plans: Cash Avoiding Productivity
4.3 TYC Plans: Reinvestment to shift left
4.4 Capital Infrastructure and Investment Programmes
5. Workforce Planning 5.1 Trust Workforce Summary of QICR Plans
5.2 Primary Care Workforce Summary
5.3 Independent Healthcare Provider Workforce Summary
6. Enabling Implementation 6.1 Outcomes and Quality Measures: knowing how we are doing
6.2 Implementation Structure: Mobilising to deliver
6.3 Building our capacity and capability: Organisation Development
6.4 Engaging Others: Involving our stakeholders/Engagement Plan
6.5Risks: Identification, Impact and Management
5
Section 1
Vision and Context
6
Section 1.1: Vision and Context
Northern Ireland Regional Context
This section sets out the key environmental factors influencing policy formulation and on the major policy imperatives which define the future direction of travel for service development and redesign.
Transforming Your Care In June 2011, the Minister for Health, Social Services and Public Safety, announced the need for a review of HSC services. The key objectives of the Review were to:
• Undertake a strategic assessment across all aspects of health and social care services;
• Undertake appropriate consultation and engagement on the way ahead;
• Make recommendations to the Minister on the future configuration and delivery of services; and
• Set out a specific implementation plan for the changes that need to be made in health and social care.
The Minister’s vision for the HSC Review was to drive up the quality of care for clients and patients, improving outcomes and enhancing the patient and client experience. In addition there is a need to improve productivity and make sure that every penny is spent effectively. The Minister emphasised the importance of promoting greater involvement of frontline professionals in decision making and service development and the crucial role which more powerful local commissioning and charity and voluntary sector providing services could play in driving change and innovation.
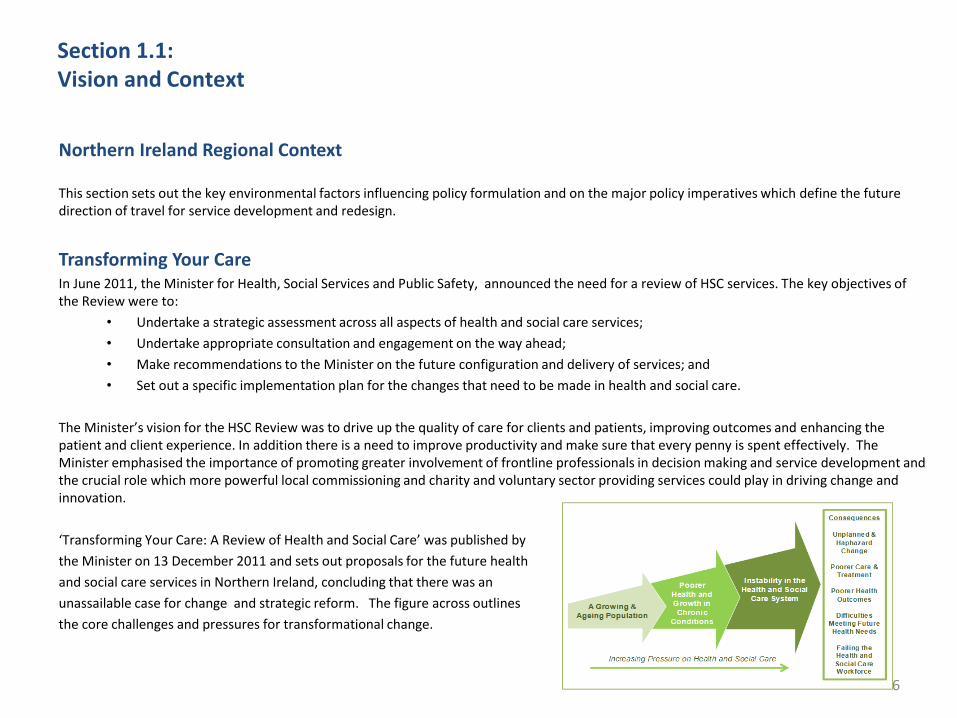
‘Transforming Your Care: A Review of Health and Social Care’ was published by
the Minister on 13 December 2011 and sets out proposals for the future health
and social care services in Northern Ireland, concluding that there was an
unassailable case for change and strategic reform. The figure across outlines
the core challenges and pressures for transformational change.
7
Section 1.1: Vision and Context
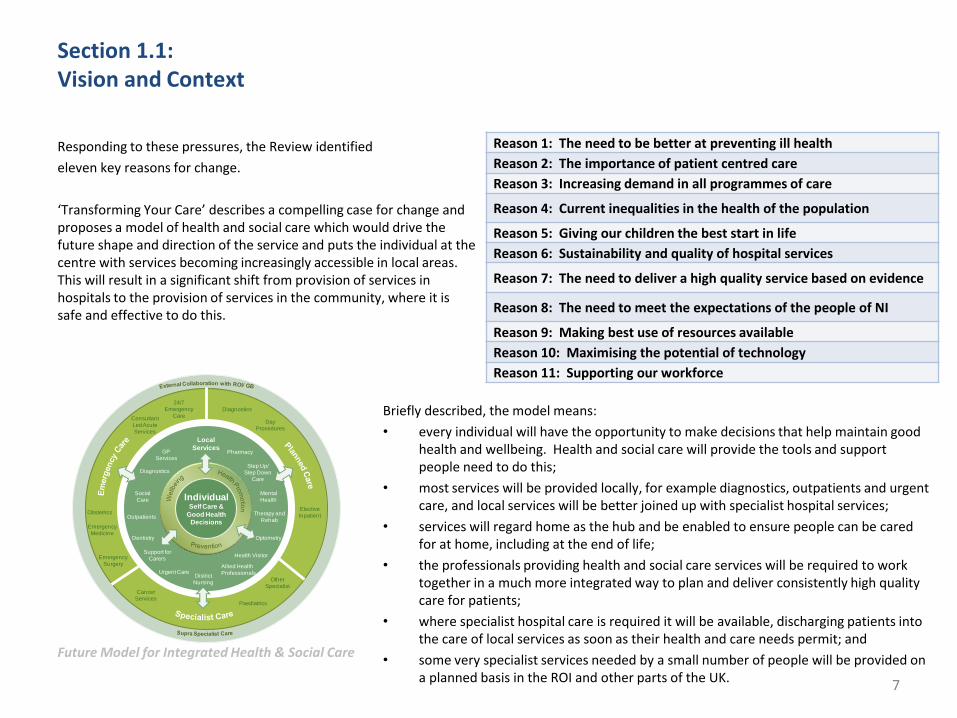
Responding to these pressures, the Review identified
eleven key reasons for change.
‘Transforming Your Care’ describes a compelling case for change and proposes a model of health and social care which would drive the future shape and direction of the service and puts the individual at the centre with services becoming increasingly accessible in local areas. This will result in a significant shift from provision of services in hospitals to the provision of services in the community, where it is safe and effective to do this.
Future Model for Integrated Health & Social Care
Reason 1: The need to be better at preventing ill health
Reason 2: The importance of patient centred care
Reason 3: Increasing demand in all programmes of care
Reason 4: Current inequalities in the health of the population
Reason 5: Giving our children the best start in life
Reason 6: Sustainability and quality of hospital services
Reason 7: The need to deliver a high quality service based on evidence
Reason 8: The need to meet the expectations of the people of NI
Reason 9: Making best use of resources available
Reason 10: Maximising the potential of technology
Reason 11: Supporting our workforce
u
24/7
Emergency
Care
GP
Services
Social
Care
Local
Services
Diagnostics
Urgent CareDistrict
Nursing
Health Visitor
Allied Health
Professionals
Pharmacy
Step Up/
Step Down
Care
Emergency
Surgery
Emergency
Medicine
Therapy and
Rehab
Consultant
Led Acute
Services
Cancer
ServicesPaediatrics
Day
Procedures
Elective
InpatientOutpatients
Other
Specialist
Dentistry Optometry
Support for
Carers
IndividualSelf Care &
Good Health Decisions
Mental
Health
Obstetrics
Diagnostics Briefly described, the model means:
• every individual will have the opportunity to make decisions that help maintain good health and wellbeing. Health and social care will provide the tools and support people need to do this;
• most services will be provided locally, for example diagnostics, outpatients and urgent care, and local services will be better joined up with specialist hospital services;
• services will regard home as the hub and be enabled to ensure people can be cared for at home, including at the end of life;
• the professionals providing health and social care services will be required to work together in a much more integrated way to plan and deliver consistently high quality care for patients;
• where specialist hospital care is required it will be available, discharging patients into the care of local services as soon as their health and care needs permit; and
• some very specialist services needed by a small number of people will be provided on a planned basis in the ROI and other parts of the UK.
8
Section 1.1: Vision and Context
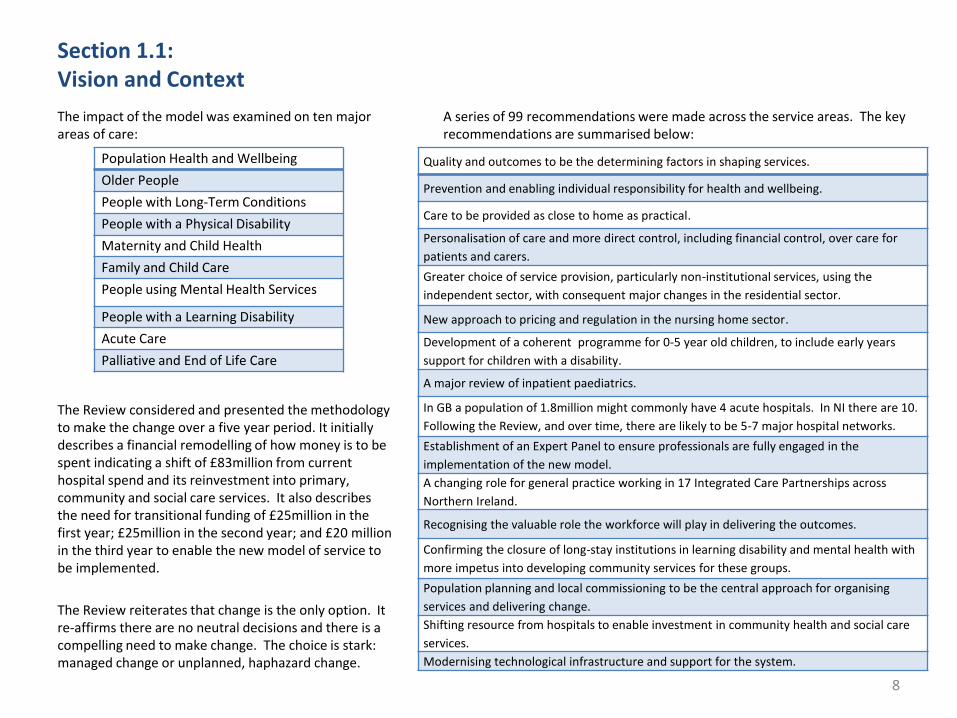
The impact of the model was examined on ten major areas of care:
The Review considered and presented the methodology to make the change over a five year period. It initially describes a financial remodelling of how money is to be spent indicating a shift of £83million from current hospital spend and its reinvestment into primary, community and social care services. It also describes the need for transitional funding of £25million in the first year; £25million in the second year; and £20 million in the third year to enable the new model of service to be implemented.
The Review reiterates that change is the only option. It re-affirms there are no neutral decisions and there is a compelling need to make change. The choice is stark: managed change or unplanned, haphazard change.
A series of 99 recommendations were made across the service areas. The key recommendations are summarised below:
Quality and outcomes to be the determining factors in shaping services.
Prevention and enabling individual responsibility for health and wellbeing.
Care to be provided as close to home as practical.
Personalisation of care and more direct control, including financial control, over care for
patients and carers.
Greater choice of service provision, particularly non-institutional services, using the
independent sector, with consequent major changes in the residential sector.
New approach to pricing and regulation in the nursing home sector.
Development of a coherent programme for 0-5 year old children, to include early years
support for children with a disability.
A major review of inpatient paediatrics.
In GB a population of 1.8million might commonly have 4 acute hospitals. In NI there are 10.
Following the Review, and over time, there are likely to be 5-7 major hospital networks.
Establishment of an Expert Panel to ensure professionals are fully engaged in the
implementation of the new model.
A changing role for general practice working in 17 Integrated Care Partnerships across
Northern Ireland.
Recognising the valuable role the workforce will play in delivering the outcomes.
Confirming the closure of long-stay institutions in learning disability and mental health with
more impetus into developing community services for these groups.
Population planning and local commissioning to be the central approach for organising
services and delivering change.
Shifting resource from hospitals to enable investment in community health and social care
services.
Modernising technological infrastructure and support for the system.
Population Health and Wellbeing
Older People
People with Long-Term Conditions
People with a Physical Disability
Maternity and Child Health
Family and Child Care
People using Mental Health Services
People with a Learning Disability
Acute Care
Palliative and End of Life Care
9
Section 1.1: Vision and Context
Quality Improvement and Cost Reduction Programme (QICR)
Health and Social Care in NI faces a considerable financial challenge over the next three years. The NI Budget settlement for the four year period 2011 to 2015 provides health and social care with a two per cent annual growth in resources to £4.65bn by 2014/15. It is anticipated that the funding requirement with no change to services would be £5.2bn by 2014/15, creating a funding gap of £600m.
To address this challenge, a number of opportunities have been identified to reduce cost whilst improving quality. Critical to this is the planning and delivery of the necessary reforms in an integrated fashion, and it is intended these will be brought together through the Quality Improvement and Cost Reduction Programme (QICR) with regional and local projects working in an effective, consistent manner.

10
Section 1.1: Vision and Context
Why we need to change in the Northern Local Commissioning Group Locality In Transforming Your Care , there are five main reasons outlined as to why change is required in Northern Ireland, the Northern Local Commissioning Group Locality is no exception. Therefore we have built our models of care and population plan to alleviate the pressure that these compounding factors have on our health system:
1. A growing and ageing population;
• In the Northern Local Commissioning Group Locality, it is projected that there will be an overall population growth rate of 8.8% between 2009 and 2023.
• This is mainly being driven by the increase in the number of older people, which is expected to rise by 42% in the same period.
• The overall population within the Northern area is projected to increase from 466,431 in 2012 to 474,604 in 2015.
2. Increased prevalence of Long Term Conditions
• Within the Northern area, hypertension and asthma are the most prevalent LTCs.
• The Northern area has a higher prevalence rate (per 1,000 patients) in the areas of hypertension, asthma, CHD, hyperthyroid, atrial fibrillation, diabetes mellitus and chronic kidney disease compared to NI averages.
3. Increased demand and over reliance on hospital beds • Based on DHSSPS 2010/11 figures, Northern HSCT had the highest
occupancy rate with 84.3% of beds occupied compared to other Trusts.
• Overall there was a 0.6% increase in the total number of admissions from 2006/07 to 2010/11.
4. Clinical workforce supply difficulties which have put pressure on service resilience • Workforce is key to providing high quality services to the population of the Northern Local Commissioning Group Locality. • To meet current clinical recommendations on staffing, further recruitment of consultants would be required. • Currently in the Northern Local Commissioning Group Locality, our key shortages are within Emergency Medicine, which requires 3 Consultants, 2 Middle Grade staff and 8 Trainee Grade clinicians , and in Medicine which requires 6 Consultants, 11 Middle Grade staff and 2 Trainee Grade staff. All but two of the above identified vacancies are currently being filled by locum staff.
5. The need for greater productivity and value for money • The Northern HSCT’s allocation from HSCB for 2012/13 is £528.6m. • Over the next 3 years the locality is expected to produce £52.0m in
savings, which is equivalent to 9.8% of the region’s budget. • The savings figure is made up of cash productivity savings of £36.0m
and productivity savings of £16.0m.
Data from QOF Prevalence on LTC for NHSCT (2011) Most Prevalent LTCs: 1. Hypertension – 133 per 1,000 population 2. Asthma- 60 per 1,000 population
Hospital Admissions Growth - Northern
Day Cases
Inpatients
06/07 07/08 08/09 09/10 10/11
88,523 91,999 92,845 90,562 89,092
11
Section 1.1: Vision and Context
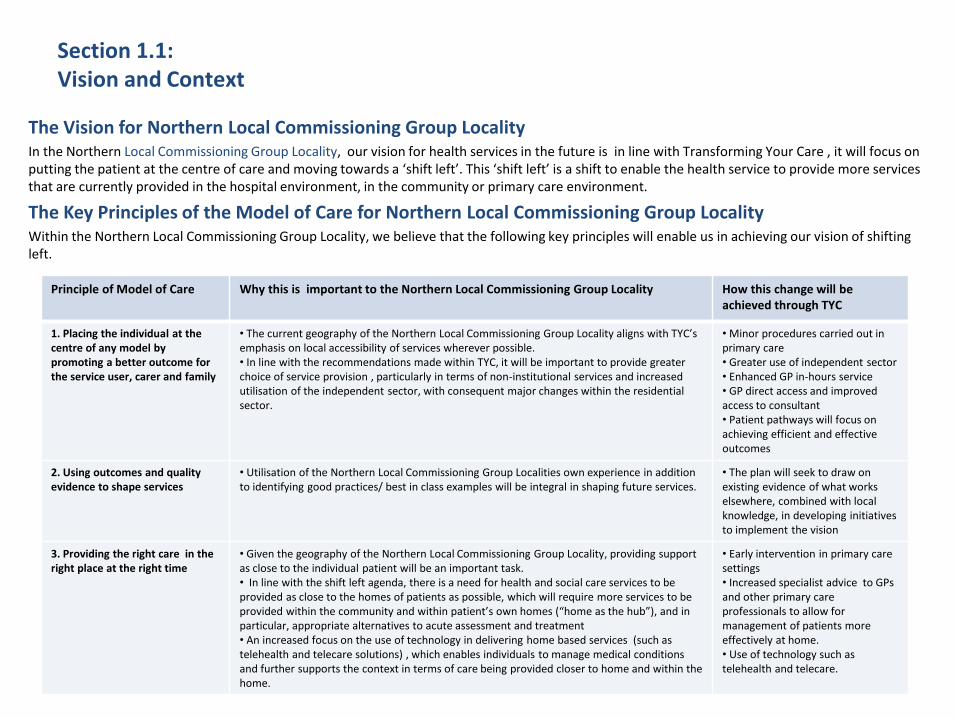
The Vision for Northern Local Commissioning Group Locality In the Northern Local Commissioning Group Locality, our vision for health services in the future is in line with Transforming Your Care , it will focus on putting the patient at the centre of care and moving towards a ‘shift left’. This ‘shift left’ is a shift to enable the health service to provide more services that are currently provided in the hospital environment, in the community or primary care environment.
The Key Principles of the Model of Care for Northern Local Commissioning Group Locality Within the Northern Local Commissioning Group Locality, we believe that the following key principles will enable us in achieving our vision of shifting left.
Principle of Model of Care
Why this is important to the Northern Local Commissioning Group Locality How this change will be achieved through TYC
1. Placing the individual at the centre of any model by promoting a better outcome for the service user, carer and family
• The current geography of the Northern Local Commissioning Group Locality aligns with TYC’s emphasis on local accessibility of services wherever possible. • In line with the recommendations made within TYC, it will be important to provide greater choice of service provision , particularly in terms of non-institutional services and increased utilisation of the independent sector, with consequent major changes within the residential sector.
• Minor procedures carried out in primary care • Greater use of independent sector • Enhanced GP in-hours service • GP direct access and improved access to consultant • Patient pathways will focus on achieving efficient and effective outcomes
2. Using outcomes and quality evidence to shape services
• Utilisation of the Northern Local Commissioning Group Localities own experience in addition to identifying good practices/ best in class examples will be integral in shaping future services.
• The plan will seek to draw on existing evidence of what works elsewhere, combined with local knowledge, in developing initiatives to implement the vision
3. Providing the right care in the right place at the right time
• Given the geography of the Northern Local Commissioning Group Locality, providing support as close to the individual patient will be an important task. • In line with the shift left agenda, there is a need for health and social care services to be provided as close to the homes of patients as possible, which will require more services to be provided within the community and within patient’s own homes (“home as the hub”), and in particular, appropriate alternatives to acute assessment and treatment • An increased focus on the use of technology in delivering home based services (such as telehealth and telecare solutions) , which enables individuals to manage medical conditions and further supports the context in terms of care being provided closer to home and within the home.
• Early intervention in primary care settings • Increased specialist advice to GPs and other primary care professionals to allow for management of patients more effectively at home. • Use of technology such as telehealth and telecare.
12
Section 1.1: Vision and Context
Principle of Model of Care
Why this is important to the Northern Local Commissioning Group Locality How this change will be achieved through TYC
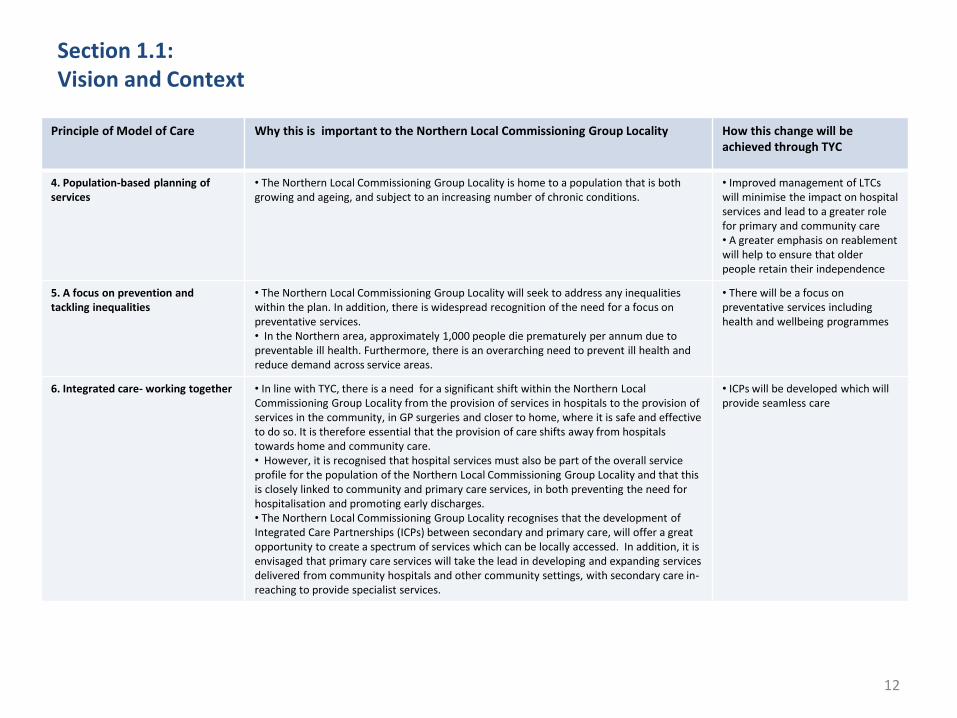
4. Population-based planning of services
• The Northern Local Commissioning Group Locality is home to a population that is both growing and ageing, and subject to an increasing number of chronic conditions.
• Improved management of LTCs will minimise the impact on hospital services and lead to a greater role for primary and community care • A greater emphasis on reablement will help to ensure that older people retain their independence
5. A focus on prevention and tackling inequalities
• The Northern Local Commissioning Group Locality will seek to address any inequalities within the plan. In addition, there is widespread recognition of the need for a focus on preventative services. • In the Northern area, approximately 1,000 people die prematurely per annum due to preventable ill health. Furthermore, there is an overarching need to prevent ill health and reduce demand across service areas.
• There will be a focus on preventative services including health and wellbeing programmes
6. Integrated care- working together • In line with TYC, there is a need for a significant shift within the Northern Local Commissioning Group Locality from the provision of services in hospitals to the provision of services in the community, in GP surgeries and closer to home, where it is safe and effective to do so. It is therefore essential that the provision of care shifts away from hospitals towards home and community care. • However, it is recognised that hospital services must also be part of the overall service profile for the population of the Northern Local Commissioning Group Locality and that this is closely linked to community and primary care services, in both preventing the need for hospitalisation and promoting early discharges. • The Northern Local Commissioning Group Locality recognises that the development of Integrated Care Partnerships (ICPs) between secondary and primary care, will offer a great opportunity to create a spectrum of services which can be locally accessed. In addition, it is envisaged that primary care services will take the lead in developing and expanding services delivered from community hospitals and other community settings, with secondary care in-reaching to provide specialist services.
• ICPs will be developed which will provide seamless care
13
Section 1.1: Vision and Context
Principle of Model of Care
Why this is important to the Northern Local Commissioning Group Locality How this change will be achieved through TYC
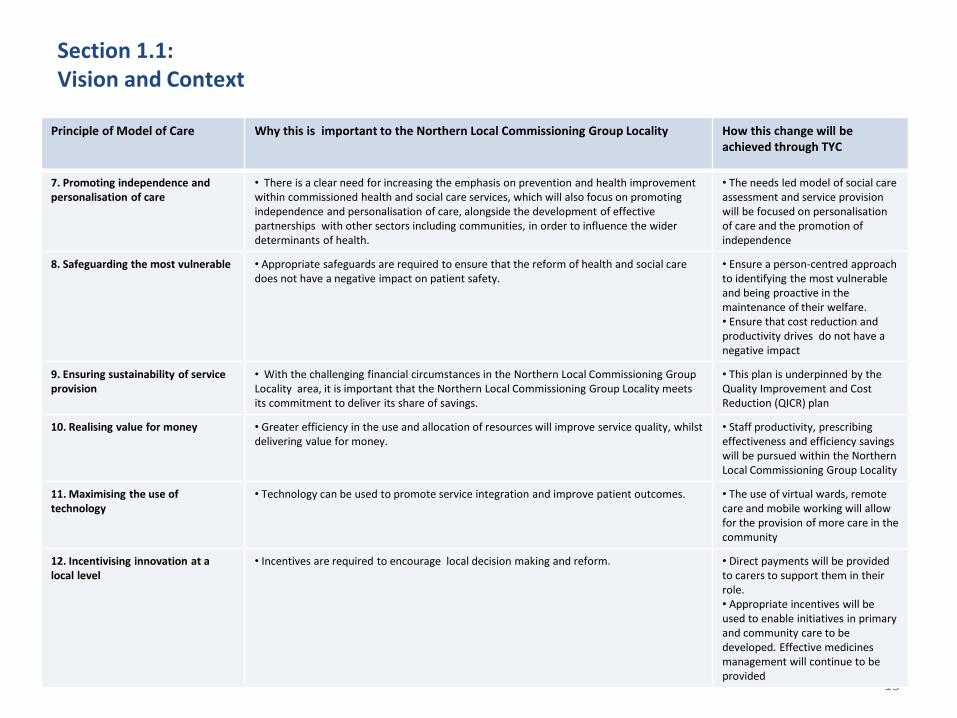
7. Promoting independence and personalisation of care
• There is a clear need for increasing the emphasis on prevention and health improvement within commissioned health and social care services, which will also focus on promoting independence and personalisation of care, alongside the development of effective partnerships with other sectors including communities, in order to influence the wider determinants of health.
• The needs led model of social care assessment and service provision will be focused on personalisation of care and the promotion of independence
8. Safeguarding the most vulnerable • Appropriate safeguards are required to ensure that the reform of health and social care does not have a negative impact on patient safety.
• Ensure a person-centred approach to identifying the most vulnerable and being proactive in the maintenance of their welfare. • Ensure that cost reduction and productivity drives do not have a negative impact
9. Ensuring sustainability of service provision
• With the challenging financial circumstances in the Northern Local Commissioning Group Locality area, it is important that the Northern Local Commissioning Group Locality meets its commitment to deliver its share of savings.
• This plan is underpinned by the Quality Improvement and Cost Reduction (QICR) plan
10. Realising value for money • Greater efficiency in the use and allocation of resources will improve service quality, whilst delivering value for money.
• Staff productivity, prescribing effectiveness and efficiency savings will be pursued within the Northern Local Commissioning Group Locality
11. Maximising the use of technology
• Technology can be used to promote service integration and improve patient outcomes. • The use of virtual wards, remote care and mobile working will allow for the provision of more care in the community
12. Incentivising innovation at a local level
• Incentives are required to encourage local decision making and reform. • Direct payments will be provided to carers to support them in their role. • Appropriate incentives will be used to enable initiatives in primary and community care to be developed. Effective medicines management will continue to be provided

14
Section 1.1: Vision and Context
The benefits of change for Northern Local Commissioning Group Locality Through our vision for the Northern Local Commissioning Group Locality, we aim to achieve progress in the six main areas of benefit for our population, staff and patients. These will be the benefits that will measure our success in transforming care within the Northern Local Commissioning Group Locality
Better patient outcomes
Better provision and consistency of health and social
care
Better staff skills, resourcing & development
Better models of care
Better quality estate
Better value for money
Targeted health and wellbeing improvement programmes
Collaborative working arrangements between statutory, community and voluntary groups
Appropriate clinical decisions made sooner through an increased consultant presence
Reduced waiting times
Reinvestment of estates value into other areas of the local commissioning group locality
Increased productivity of expensive resources
Reduction of unnecessary variations in patient care
Integrated planning and delivery of consistently high quality patient care
Sustainable level of staffing with appropriate mix of skills and experience
Reduced emergency hospital admissions
Looking beyond buildings will enable the provision of more flexible care options
Increased economies of scale due to improved use of resources
Centralisation of more complex day surgery at acute sites
Promotion of appropriate use of emergency and urgent care services
Optimisation of skilled staff resources
Reduced cancellations rate
Continuation of work to improve access to statutory buildings, services and amenities
Reduction of lengths of stay
Delivery of more care at home and closer to home
Introduction of palliative care as part of corporate induction and the development of e-learning packages
Alternative models of accommodation and support instead of residential homes
Decrease in incidents of hospital acquired infections
Increased patient involvement in the delivery of their own care
GP skills utilised more effectively
Alignment with best practice models of care
Decrease in the number of hospital serious incidents
Implementation of consistent evidence-based patient pathways
15
Section 1.2: Current Service and Financial Analysis
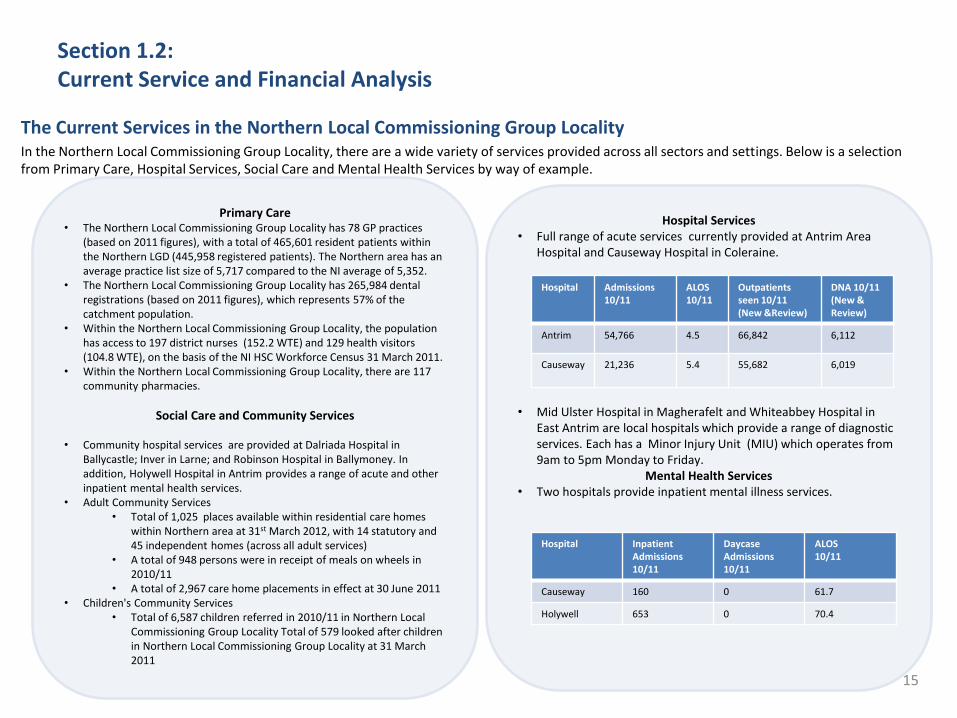
Hospital Services • Full range of acute services currently provided at Antrim Area
Hospital and Causeway Hospital in Coleraine.
• Mid Ulster Hospital in Magherafelt and Whiteabbey Hospital in
East Antrim are local hospitals which provide a range of diagnostic services. Each has a Minor Injury Unit (MIU) which operates from 9am to 5pm Monday to Friday.
Mental Health Services • Two hospitals provide inpatient mental illness services.
Primary Care • The Northern Local Commissioning Group Locality has 78 GP practices
(based on 2011 figures), with a total of 465,601 resident patients within the Northern LGD (445,958 registered patients). The Northern area has an average practice list size of 5,717 compared to the NI average of 5,352.
• The Northern Local Commissioning Group Locality has 265,984 dental registrations (based on 2011 figures), which represents 57% of the catchment population.
• Within the Northern Local Commissioning Group Locality, the population has access to 197 district nurses (152.2 WTE) and 129 health visitors (104.8 WTE), on the basis of the NI HSC Workforce Census 31 March 2011.
• Within the Northern Local Commissioning Group Locality, there are 117 community pharmacies.
Social Care and Community Services
• Community hospital services are provided at Dalriada Hospital in Ballycastle; Inver in Larne; and Robinson Hospital in Ballymoney. In addition, Holywell Hospital in Antrim provides a range of acute and other inpatient mental health services.
• Adult Community Services • Total of 1,025 places available within residential care homes
within Northern area at 31st March 2012, with 14 statutory and 45 independent homes (across all adult services)
• A total of 948 persons were in receipt of meals on wheels in 2010/11
• A total of 2,967 care home placements in effect at 30 June 2011 • Children's Community Services
• Total of 6,587 children referred in 2010/11 in Northern Local Commissioning Group Locality Total of 579 looked after children in Northern Local Commissioning Group Locality at 31 March 2011
The Current Services in the Northern Local Commissioning Group Locality In the Northern Local Commissioning Group Locality, there are a wide variety of services provided across all sectors and settings. Below is a selection from Primary Care, Hospital Services, Social Care and Mental Health Services by way of example.
Hospital Admissions 10/11
ALOS 10/11
Outpatients seen 10/11 (New &Review)
DNA 10/11 (New & Review)
Antrim 54,766 4.5 66,842 6,112
Causeway 21,236 5.4 55,682 6,019
Hospital Inpatient Admissions 10/11
Daycase Admissions 10/11
ALOS 10/11
Causeway 160 0 61.7
Holywell 653 0 70.4
16
Section 1.3: Assessing Strategic Need; our Population & the Local Commissioning Group Locality
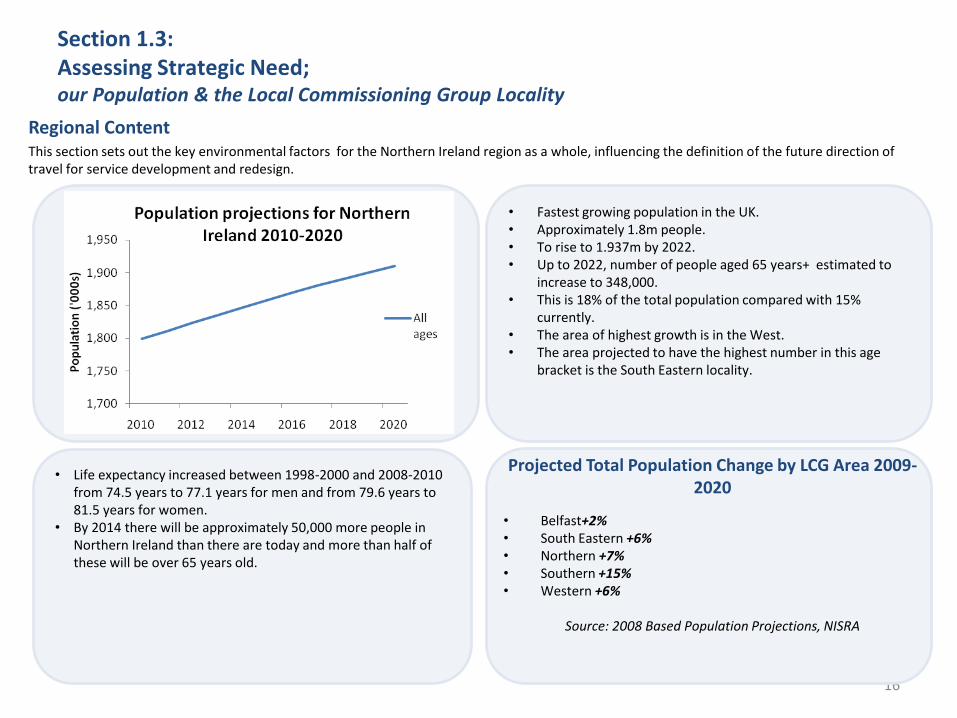
• Fastest growing population in the UK. • Approximately 1.8m people. • To rise to 1.937m by 2022. • Up to 2022, number of people aged 65 years+ estimated to
increase to 348,000. • This is 18% of the total population compared with 15%
currently. • The area of highest growth is in the West. • The area projected to have the highest number in this age
bracket is the South Eastern locality.
• Life expectancy increased between 1998-2000 and 2008-2010 from 74.5 years to 77.1 years for men and from 79.6 years to 81.5 years for women.
• By 2014 there will be approximately 50,000 more people in Northern Ireland than there are today and more than half of these will be over 65 years old.
Regional Content This section sets out the key environmental factors for the Northern Ireland region as a whole, influencing the definition of the future direction of travel for service development and redesign.
Projected Total Population Change by LCG Area 2009-2020
• Belfast+2% • South Eastern +6% • Northern +7% • Southern +15% • Western +6%
Source: 2008 Based Population Projections, NISRA

17
Section 1.3: Assessing Strategic Need; our Population & Local Commissioning Group Locality
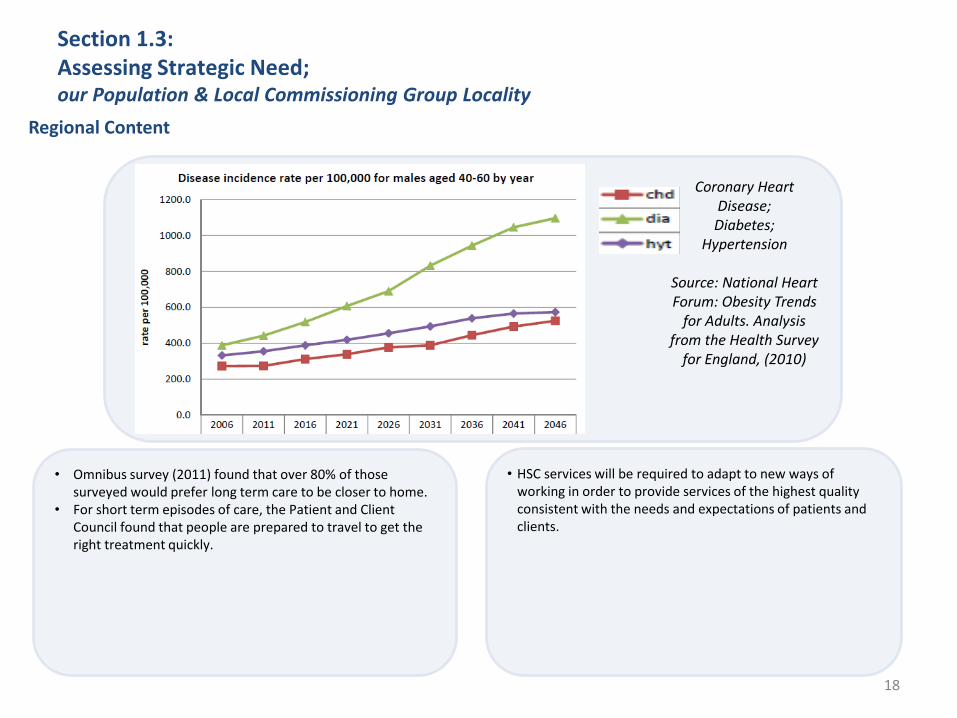
• An ever increasing older population. • Growing incidence rate of chronic conditions such as
hypertension, diabetes, asthma and obesity. • Incidence rate (new cases) is influenced in part by lifestyle
choices. • Government intervention and personal action is required to
make healthy choices easier.
• The total number of cases (prevalence rate) is influenced by survival rates.
• Early diagnosis and modern treatments reduce mortality, and increase the need for services to manage chronic conditions in the long term.
Regional Content
Projected Growth of 85+
Source: 2008 Based Population
Projections, NISRA
Source:
2010 Based
Population
Projections,
NISRA
18
Section 1.3: Assessing Strategic Need; our Population & Local Commissioning Group Locality
• Omnibus survey (2011) found that over 80% of those surveyed would prefer long term care to be closer to home.
• For short term episodes of care, the Patient and Client Council found that people are prepared to travel to get the right treatment quickly.
• HSC services will be required to adapt to new ways of working in order to provide services of the highest quality consistent with the needs and expectations of patients and clients.
Regional Content
Coronary Heart Disease; Diabetes;
Hypertension
Source: National Heart Forum: Obesity Trends
for Adults. Analysis from the Health Survey
for England, (2010)
19
Section 1.3: Assessing Strategic Need; our Population & Local Commissioning Group Locality
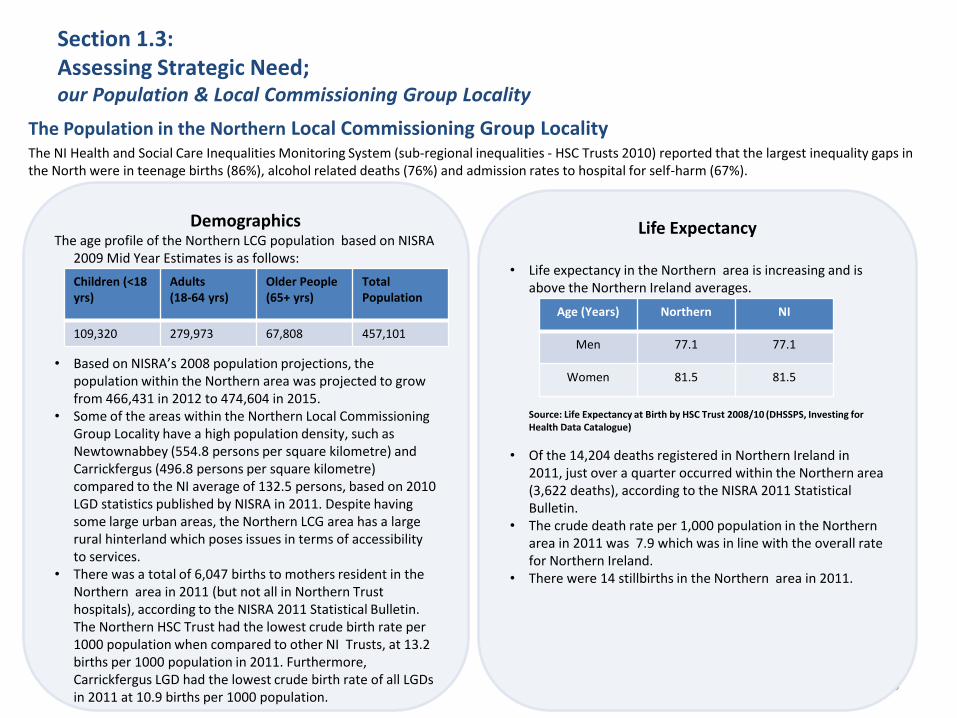
The Population in the Northern Local Commissioning Group Locality The NI Health and Social Care Inequalities Monitoring System (sub-regional inequalities - HSC Trusts 2010) reported that the largest inequality gaps in the North were in teenage births (86%), alcohol related deaths (76%) and admission rates to hospital for self-harm (67%).
Demographics The age profile of the Northern LCG population based on NISRA
2009 Mid Year Estimates is as follows: • Based on NISRA’s 2008 population projections, the
population within the Northern area was projected to grow from 466,431 in 2012 to 474,604 in 2015.
• Some of the areas within the Northern Local Commissioning Group Locality have a high population density, such as Newtownabbey (554.8 persons per square kilometre) and Carrickfergus (496.8 persons per square kilometre) compared to the NI average of 132.5 persons, based on 2010 LGD statistics published by NISRA in 2011. Despite having some large urban areas, the Northern LCG area has a large rural hinterland which poses issues in terms of accessibility to services.
• There was a total of 6,047 births to mothers resident in the Northern area in 2011 (but not all in Northern Trust hospitals), according to the NISRA 2011 Statistical Bulletin. The Northern HSC Trust had the lowest crude birth rate per 1000 population when compared to other NI Trusts, at 13.2 births per 1000 population in 2011. Furthermore, Carrickfergus LGD had the lowest crude birth rate of all LGDs in 2011 at 10.9 births per 1000 population.
Life Expectancy
• Life expectancy in the Northern area is increasing and is above the Northern Ireland averages.
Source: Life Expectancy at Birth by HSC Trust 2008/10 (DHSSPS, Investing for
Health Data Catalogue)
• Of the 14,204 deaths registered in Northern Ireland in 2011, just over a quarter occurred within the Northern area (3,622 deaths), according to the NISRA 2011 Statistical Bulletin.
• The crude death rate per 1,000 population in the Northern area in 2011 was 7.9 which was in line with the overall rate for Northern Ireland.
• There were 14 stillbirths in the Northern area in 2011.
Children (<18 yrs)
Adults (18-64 yrs)
Older People (65+ yrs)
Total Population
109,320 279,973 67,808 457,101
Age (Years) Northern NI
Men 77.1 77.1
Women 81.5 81.5
20
Section 1.3: Assessing Strategic Need; our Population & the Local Commissioning Group Locality
The Population and Local Commissioning Group Locality in the Northern Area
Deprivation • Three of the LGD areas within the Northern area were
ranked within the top ten most deprived areas (on extent) in Northern Ireland, on basis of NISRA Multiple Deprivation 2010 LGD Summary Measures- with Newtownabbey ranked eighth, Moyle ranked ninth and Coleraine ranked tenth.
• Three of the LGD areas within the Northern area were also ranked within the top ten most deprived areas in terms of employment rate- with Cookstown ranked fifth, Moyle ranked sixth and Ballymoney ranked tenth.
Health and Wellbeing
• Based on the Northern Ireland Continuous Household Survey 2009/10, 24% of persons aged 16 years and over within the Northern area smoke, which was in line with the overall rate for Northern Ireland.
• There were 53 alcohol related deaths in the Northern area in 2010, which accounted for 18.7% of the overall alcohol related deaths (284) in Northern Ireland .
• The Northern area had the highest proportion of obesity related deaths (12) when compared to other NI HSC Trusts areas from 2006 to 2010 (39 deaths in total).
• The Northern area had the lowest proportion of problem drug users present to an agency in 2010/11 (4% of overall NI figure of 2,593 users) when compared to other HSC Trusts in NI.
• Based on DHSSPS adult community statistics 2010/11, the Northern HSC Trust had contact with 2,393 learning disabled persons of the overall total for Northern Ireland of 9,173 persons.
• Based on DHSSPS adult community statistics 2010/11, the Northern HSCT had contact with 1,518 physically disabled persons under 65 years of the overall total for Northern Ireland of 6,381 persons.
21
The Shift Left
The Pressures
Financial envelope
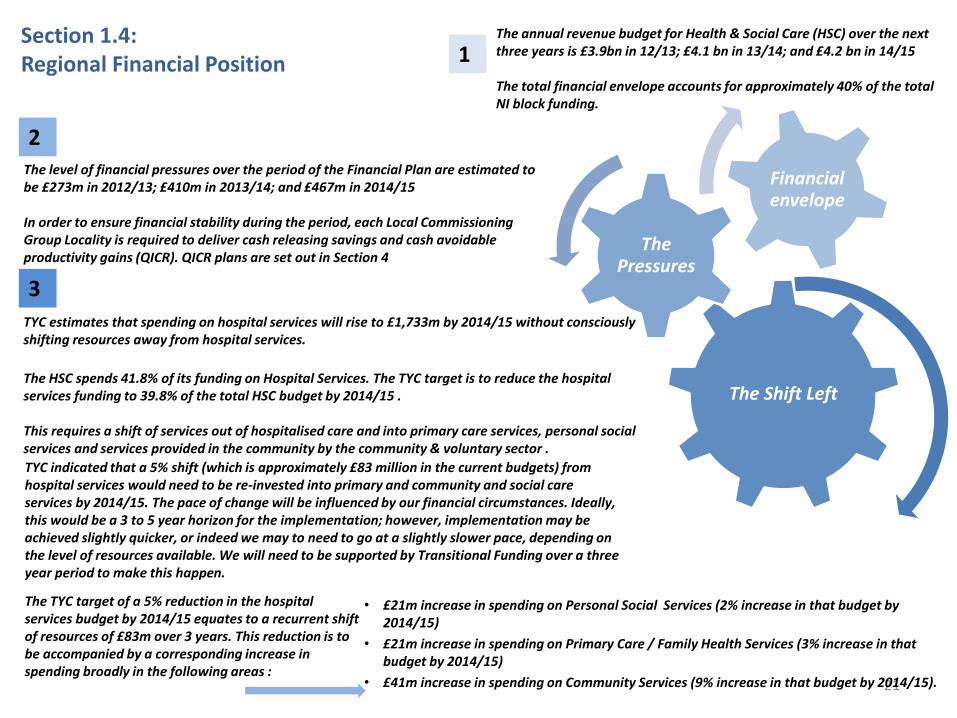
The annual revenue budget for Health & Social Care (HSC) over the next three years is £3.9bn in 12/13; £4.1 bn in 13/14; and £4.2 bn in 14/15 The total financial envelope accounts for approximately 40% of the total NI block funding.
The level of financial pressures over the period of the Financial Plan are estimated to be £273m in 2012/13; £410m in 2013/14; and £467m in 2014/15 In order to ensure financial stability during the period, each Local Commissioning Group Locality is required to deliver cash releasing savings and cash avoidable productivity gains (QICR). QICR plans are set out in Section 4
TYC estimates that spending on hospital services will rise to £1,733m by 2014/15 without consciously shifting resources away from hospital services.
The HSC spends 41.8% of its funding on Hospital Services. The TYC target is to reduce the hospital services funding to 39.8% of the total HSC budget by 2014/15 . This requires a shift of services out of hospitalised care and into primary care services, personal social services and services provided in the community by the community & voluntary sector .
Section 1.4: Regional Financial Position 1
2
3
• £21m increase in spending on Personal Social Services (2% increase in that budget by 2014/15)
• £21m increase in spending on Primary Care / Family Health Services (3% increase in that budget by 2014/15)
• £41m increase in spending on Community Services (9% increase in that budget by 2014/15).
The TYC target of a 5% reduction in the hospital services budget by 2014/15 equates to a recurrent shift of resources of £83m over 3 years. This reduction is to be accompanied by a corresponding increase in spending broadly in the following areas :
TYC indicated that a 5% shift (which is approximately £83 million in the current budgets) from hospital services would need to be re-invested into primary and community and social care services by 2014/15. The pace of change will be influenced by our financial circumstances. Ideally, this would be a 3 to 5 year horizon for the implementation; however, implementation may be achieved slightly quicker, or indeed we may to need to go at a slightly slower pace, depending on the level of resources available. We will need to be supported by Transitional Funding over a three year period to make this happen.
22
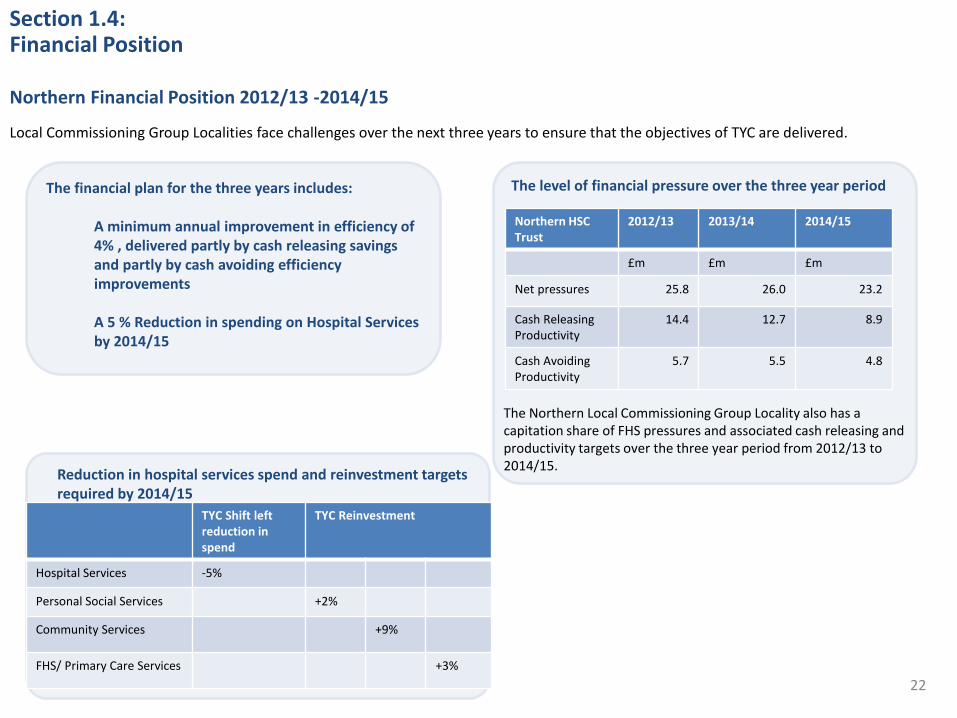
Local Commissioning Group Localities face challenges over the next three years to ensure that the objectives of TYC are delivered.
The level of financial pressure over the three year period
Section 1.4: Financial Position
0
50
100
150
200
250
Northern Financial Position 2012/13 -2014/15
The financial plan for the three years includes: A minimum annual improvement in efficiency of 4% , delivered partly by cash releasing savings and partly by cash avoiding efficiency improvements A 5 % Reduction in spending on Hospital Services by 2014/15
Reduction in hospital services spend and reinvestment targets required by 2014/15
The Northern Local Commissioning Group Locality also has a capitation share of FHS pressures and associated cash releasing and productivity targets over the three year period from 2012/13 to 2014/15.
Northern HSC Trust
2012/13 2013/14 2014/15
£m £m £m
Net pressures 25.8 26.0 23.2
Cash Releasing Productivity
14.4 12.7 8.9
Cash Avoiding Productivity
5.7 5.5 4.8
TYC Shift left reduction in spend
TYC Reinvestment
Hospital Services -5%
Personal Social Services +2%
Community Services +9%
FHS/ Primary Care Services +3%
23
Section 2
Delivering Transformation
24
Section 2 :Delivering Transformation
What Transforming Your Care will mean in the Northern Local commissioning group locality
Introduction
The Northern Local Commissioning Group Locality recognises the challenges presented in TYC, together with the need to deliver services which meet the needs of the local population and adhere to the Commissioning Specifications.
In light of the growing pressures presented by the changing demography and the need to demonstrate enhanced productivity and outcomes for our local population, there is without doubt an overwhelming case for radical change in how we commission and deliver services. There is also the need to take account of the opportunities presented by new and innovative service models, evidence based practice and emerging technology.
The following sections outline how the Northern Local Commissioning Group Locality will deliver the transformational change which is the vision presented in TYC and how the local population can expect to benefit from the proposed changes and initiatives.
Section 2 outlines the key transformational changes, whilst Section 3 provides greater detail in terms of the initiatives which will be taken forward, together with the expected outcomes for patients and clients in terms of enhanced quality and productivity.
25
Section 2.1: Delivering Transformation
What Transforming Your Care will mean in the Northern Local Commissioning Group Locality 1. Developing Integrated Care Partnerships and Managing Long Term Conditions
• TYC presents compelling evidence that if we are to meet the healthcare needs of our population , which is increasingly older, more frail and with increasing numbers of chronic conditions, we need to move away from a reactive model of service provision in hospitals to proactive provision of services in the community, in GP surgeries and closer to home (where it is safe and effective to do so).
• The development and implementation of Integrated Care Partnerships (ICPs) is recognised as key to improving integration across the whole of the health and social care system and to enable this refocusing of service delivery outside of hospital settings. The remit of the ICPs will be the provision of integrated, accessible healthcare services, by clinicians who are accountable for addressing the large majority of personal healthcare needs, through the development of a sustained partnership with patients, and practice in the context of family and community.
• ICPs will be commissioned provider organisations which will be clinically led, patient user centred and will focus on the redesign of services. GPs will have a critical leadership role in the ICPs. ICPs will be located within geographical boundaries and will use existing GP registered populations as their foundation.
•There are four existing Primary Care Partnerships (PCPs) in the Northern area, specifically in Antrim/ Ballymena, Causeway, East Antrim and Mid Ulster. It is envisaged that the existing PCPs will take forward the ICP agenda on a geographical basis.
• The experience gained in developing the existing PCPs in the Northern area will be used to develop ICPs, building on closer working relationships between primary and secondary care, and will include a more significant role for community providers.
• ICPs in the Northern area will join up local services including GPs, community pharmacists, community health and social care providers, hospital specialists and representatives from the independent and voluntary sector, as well as facilitating joined up working to deliver services locally. It is envisaged that this will mean new roles for professionals, both in secondary and primary care, as well as an expanding role for the voluntary and community sector in local service delivery.
•The alignment of ICPs with the proactive management of long term conditions (such as diabetes or hypertension) has been identified as a key goal in the Northern area, to improve patient experience and reduce unplanned hospital admissions. Ultimately it is envisaged that the implementation of ICPs will lead to a framework through which an effective chronic disease management model can be implemented within the Northern area. Much of the effort will focus on supporting people within a self-care and personalised care approach, which is about creating an environment where people feel supported to self-care and access services as appropriate to their specific needs.
26
Section 2.1: Delivering Transformation
What Transforming Your Care will mean in the Northern Local Commissioning Group Locality 1. Developing Integrated Care Partnerships and Managing Long Term Conditions (continued)
• This will be achieved by developing organisational structures and networks that enable services to be less fragmented and more accessible to individual needs, by providing appropriate information, access to interventions and technology that affords people the opportunity to improve their quality of life and manage their condition more effectively.
• There will also be an emphasis on:
– Risk stratification to ensure services are appropriately targeted;
– Strengthening public health initiatives to reduce unhealthy lifestyles and support healthy choices;
– Enhancing more timely diagnosis through direct access to diagnostics;
– Developing information solutions to help predict risk, direct interventions to those at greatest risk and more use of telehealth/telecare; and
– Personalised care plans that address functional, social, and psychological needs of patients that anticipate changing needs.
• It is important to acknowledge that the scale of change required, and the development of Integrated Care Partnerships (as one of the chief means of achieving change), is very challenging .
• The timeframe for the nature of the reform needed is fast paced, and within this there must be time given to developing the skills that the Primary Care workforce, in particular, in taking on many of these new ways of working within community settings.
• It will be important that workforce planning for Primary Care is an integral part of the development and ‘shift left’ planning processes, with skills training for GPs being an important part of that, as well as capacity planning.
• The design and nature of how Integrated Care Partnership operate will focus very much on the outcomes we seek to achieve, so dialogue with service users and other stakeholders will be important in shaping how the organisational arrangements are developed.
• We anticipate that, subject to the successful development of appropriate community based services for managing many long term conditions outside of hospital , there could be a significant number of hospital beds freed up in the Northern area, with appropriate resources moving into community settings and greater ability to cope with increasing demography.
27
Section 2.1: Delivering Transformation
What Transforming Your Care will mean in the Northern Local Commissioning Group Locality 2. Reform of Services for Older People
Across the Northern Area, a programme of reform is underway to refocus services for older people towards promoting independence, with support, and a positive approach to healthy aging. The programme is focused on developing and redefining services that will ensure older people are assisted to remain within their own home for as long as possible, given the appropriate level of care and support to do so safely, and to ensure that services are provided in the most effective way to support that aim. The following services for older people have been identified as key areas that need to continue to change and develop to achieve these aims:
– Home Care: This will include a greater emphasis on reablement which is short term, intensive care and support service delivered to people in their own home, generally accessed following a hospital admission or in the event of a health or social care crisis at home;
– Residential Care: The results of a needs assessment exercise indicated that the majority of people being admitted into residential care could have been maintained in their own home if appropriate support had been available. Plans will be developed to provide alternatives to statutory residential care homes, of which there are 11 at present, with 220 permanent residents in total. Already significant progress has been made in a number of localities to provide alternative home based services and develop new supported living facilities, in particular in Ballycastle and in Greenisland. A process of consultation will be planned across the other localities to help identify the requirements for future services in each locality, working closely with older people, their families and carers . We expect that over the next 3 years we will have made significant progress putting in place the alternative services that will enable us to move away from the current model of statutory residential care. The emphasis will be on providing care at home, with extended use of community/voluntary sector services particularly in the area of practical support and avoiding social isolation. This process is about planning appropriate services for the future and great sensitivity will be deployed in reassuring existing residents about our commitment to their continued care.
– Community and Voluntary Sector Services: The vision for enabling and supporting our growing elderly population sees more reliance on community/voluntary sector initiatives. Work will be taken forward to sustain and enhance the range of services provided by community and voluntary sector organisations which promote opportunities for increased individual support, either within the individual’s own home or through activities within local communities.
– Day Care Services – A programme of modernisation of day care services, addressing Reablement goal of promoting independence, has transformed these services. In order to ensure effective use of resources a review of the number of sites and the management arrangements will be undertaken.
28
Section 2.1: Delivering Transformation
What Transforming Your Care will mean in the Northern Local Commissioning Group Locality 2. Reform of Services for Older People (continued)
Intermediate Care Services:
– There will be a focus on the utilisation of a smaller number of strategically placed intermediate care bed based facilities which will focus on rehabilitation and recovery moving from approximately 18 locations (the number of facilities in use at a given time may vary depending on demand) to 6 as a first phase. There will be a mix of independent sector and Trust facilities.
– The first phase in reform will see the number of beds going from 143 to approximately 111.
– Benchmark information from across the UK would indicate that our current provision of 31 beds per 100,000 population is higher than the GB average of 17 intermediate care beds per 100,000 (though these range from 15 to 27 per 100,000 depending on area). Moving to 111 beds would bring our local figure to approximately 24 beds per 100,000 population.
– Throughout the first phase of change, as we move towards a reduced number of beds and facilities, there will be a move away from using beds in statutory residential homes for intermediate care, as those facilities are not designed for this purpose but rather for long stay care.
– With dedicated input from medical, nursing and other allied health professionals, and with a focus on enabling people who no longer require acute medical input, the intermediate care facilities will provide for a short period of accommodation based Reablement, assisting the individual to regain confidence and mobility. This type of service will have a positive impact on patient outcomes as well as reducing the existing pressures on acute hospital beds, avoiding delaying the patient in an acute hospital when their need is for a short period of rehabilitation and recovery. Intermediate care beds will also be used for step-up to provide short term support to prevent an admission to an acute hospital.
- Providing more Reablement based care in the person’s own home will allow alternatives to bed-based intermediate care to be developed and therefore future phases will also aim to reduce the number of facilities and the number of beds further and will look at a greater number of the facilities being provided by the independent sector.
- A new ward at Antrim Area Hospital will open in Spring 2013 and will provide a centre for acute rehabilitation for older people. Causeway hospital already has acute rehabilitation beds. The rehabilitation beds currently available in Mid Ulster and Whiteabbey will no longer be used for this purpose and this will present opportunities to further develop those sites as local community hubs. Already significant capital investment has been secured to develop the Mid Ulster site as a centre for a range of local services . This is the model we wish to replicate in other localities, making best use of the existing estate and levering in private finance, where appropriate, to develop a network of health and care centres delivering a range of primary and community services. The developing Integrated Care Partnerships will be key to this collaboration bringing together GPs, Pharmacists, Trust staff and the voluntary and community sector in a common enterprise.

29
The diagram below illustrates how service delivery changes will be supported by redesigning and streamlining the internal management of services including the use of Information Technology , improved access to equipment, and changes to the internal administration of services including
establishing a central point of contact for access to services.
What Transforming Your Care will mean in the Northern Local Commissioning Group Locality 2. Reform of Services for Older People (continued)
Section 2.1: Delivering Transformation
30
Section 2.1:Delivering Transformation
What Transforming Your Care will mean in the Northern Local Commissioning Group Locality 3.Hospital Services Reconfiguration – Introduction • Acute hospital services are a vital part of the overall profile of health and social care delivered in the Northern Area. Currently acute hospital services are delivered from two hospital sites: Antrim Area Hospital and Causeway Hospital, Coleraine. Northern area residents also access acute hospital services in Belfast and, to a lesser extent, Craigavon and Altnagelvin. The challenge is to provide a model of acute services that is accessible, safe and sustainable so that the population of the Northern area can be assured of access to services that can deliver the quality outcomes and patient experience that must be achieved across the whole of the NI acute hospitals network.
• The LCG and Trust have jointly established a process to give consideration to the range of issues relating to acute care and in so doing have sought to widely engage with front line clinical staff involved in the direct delivery of services, both in hospital settings and within community and primary care.
•The process has explored the interdependencies within the hospital setting, with a particular focus on the safety and sustainability of services, as well as effective outcomes and ensuring positive patient experience.
•While patients access services on an individual basis, it is very often the links between services that are key to ensuring effective , safe delivery and outcomes. For example, emergency surgery has a clear dependence on anaesthetics and critical care, and there are interdependencies between maternity services, anaesthetics and paediatrics.
•It is important too that the local acute hospital service model is also seen within a regional context, on the basis that a regional approach will be required for some specialist services to secure the professional staff who can deliver the quality and optimum outcomes for patients. These include Trauma, Orthopaedics and Cancer services for example.
•Throughout the process of reviewing the existing arrangements it is recognised that a number of challenges and specialty interdependencies between services must be addressed. While there is no immediate threat to maintaining the current model, staffing issues on the Causeway Hospital site in particular have been identified as a potential risk, and this needs to be factored into our planning to ensure the continuation of safe services .
•TYC also makes it clear that that new ways of working will be fundamental to transforming the way we deliver services. Much closer working between hospitals and primary care for example will be essential to achieving the vision set out. Most significantly, delivering services outside of hospital settings (where that is appropriate) will ensure acute hospitals services are focused on those patients with acute needs.
•While we look to the future, we must still continue to progress and thus the planned expansion at Antrim Area Hospital must continue, as this both protects existing services and will provide additional infrastructure that will enable new ways of working and support improved patient experience.
•We will continue to engage closely with NIAS to ensure that access to services is timely and responsive and we will work with colleagues regionally on the Review of the Patient Care Service.
•The new Emergency Department and 24 bedded ward will be complete at Antrim Hospital in 2013 and work will then progress on using vacated space to expand day surgery, endoscopy and outpatients. We would also expect that work will commence in the near future on improving the inpatient paediatric ward and on developing facilities for midwifery led maternity services. These are essential, both to meet required standards and to improve choice and patient experience. In addition, improved road infrastructure and investment in NI Ambulance transport services are developments we would wish to see progressed.
31
Section 2.1: Delivering Transformation 3.1 Acute Hospital Services – Current Model and Challenges
Acute hospitals provide a wide range of specialties, with much of the care and interventions provided to acutely ill or injured patients arriving at an Emergency
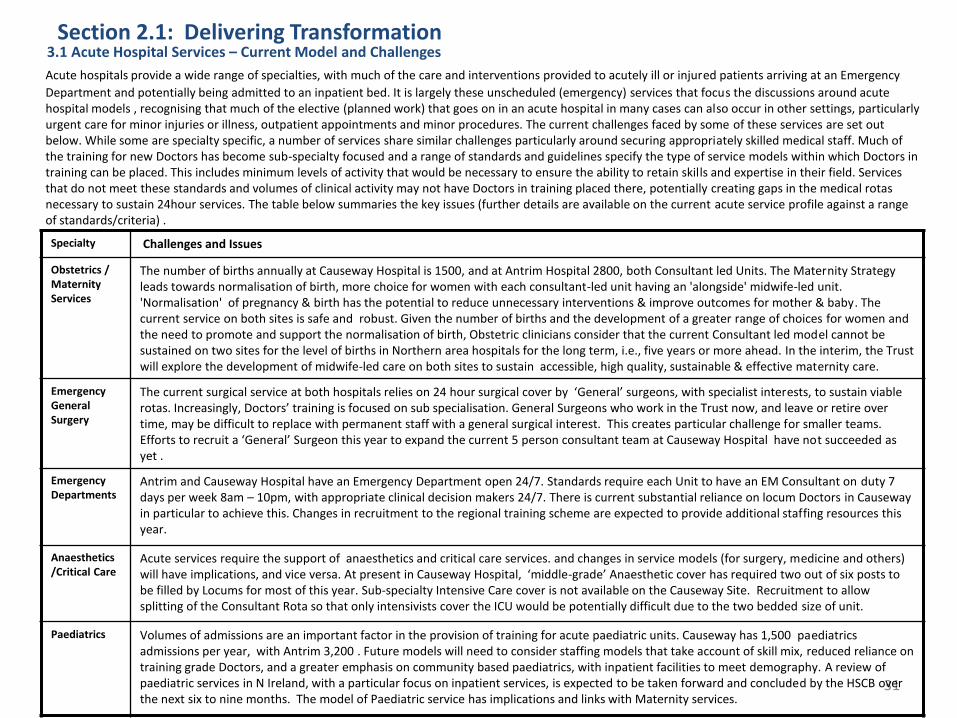
Department and potentially being admitted to an inpatient bed. It is largely these unscheduled (emergency) services that focus the discussions around acute hospital models , recognising that much of the elective (planned work) that goes on in an acute hospital in many cases can also occur in other settings, particularly urgent care for minor injuries or illness, outpatient appointments and minor procedures. The current challenges faced by some of these services are set out below. While some are specialty specific, a number of services share similar challenges particularly around securing appropriately skilled medical staff. Much of the training for new Doctors has become sub-specialty focused and a range of standards and guidelines specify the type of service models within which Doctors in training can be placed. This includes minimum levels of activity that would be necessary to ensure the ability to retain skills and expertise in their field. Services that do not meet these standards and volumes of clinical activity may not have Doctors in training placed there, potentially creating gaps in the medical rotas necessary to sustain 24hour services. The table below summaries the key issues (further details are available on the current acute service profile against a range of standards/criteria) .
Specialty Challenges and Issues
Obstetrics / Maternity Services
The number of births annually at Causeway Hospital is 1500, and at Antrim Hospital 2800, both Consultant led Units. The Maternity Strategy leads towards normalisation of birth, more choice for women with each consultant-led unit having an 'alongside' midwife-led unit. 'Normalisation' of pregnancy & birth has the potential to reduce unnecessary interventions & improve outcomes for mother & baby. The current service on both sites is safe and robust. Given the number of births and the development of a greater range of choices for women and the need to promote and support the normalisation of birth, Obstetric clinicians consider that the current Consultant led model cannot be sustained on two sites for the level of births in Northern area hospitals for the long term, i.e., five years or more ahead. In the interim, the Trust will explore the development of midwife-led care on both sites to sustain accessible, high quality, sustainable & effective maternity care.
Emergency General Surgery
The current surgical service at both hospitals relies on 24 hour surgical cover by ‘General’ surgeons, with specialist interests, to sustain viable rotas. Increasingly, Doctors’ training is focused on sub specialisation. General Surgeons who work in the Trust now, and leave or retire over time, may be difficult to replace with permanent staff with a general surgical interest. This creates particular challenge for smaller teams. Efforts to recruit a ‘General’ Surgeon this year to expand the current 5 person consultant team at Causeway Hospital have not succeeded as yet .
Emergency Departments
Antrim and Causeway Hospital have an Emergency Department open 24/7. Standards require each Unit to have an EM Consultant on duty 7 days per week 8am – 10pm, with appropriate clinical decision makers 24/7. There is current substantial reliance on locum Doctors in Causeway in particular to achieve this. Changes in recruitment to the regional training scheme are expected to provide additional staffing resources this year.
Anaesthetics /Critical Care
Acute services require the support of anaesthetics and critical care services. and changes in service models (for surgery, medicine and others) will have implications, and vice versa. At present in Causeway Hospital, ‘middle-grade’ Anaesthetic cover has required two out of six posts to be filled by Locums for most of this year. Sub-specialty Intensive Care cover is not available on the Causeway Site. Recruitment to allow splitting of the Consultant Rota so that only intensivists cover the ICU would be potentially difficult due to the two bedded size of unit.
Paediatrics Volumes of admissions are an important factor in the provision of training for acute paediatric units. Causeway has 1,500 paediatrics admissions per year, with Antrim 3,200 . Future models will need to consider staffing models that take account of skill mix, reduced reliance on training grade Doctors, and a greater emphasis on community based paediatrics, with inpatient facilities to meet demography. A review of paediatric services in N Ireland, with a particular focus on inpatient services, is expected to be taken forward and concluded by the HSCB over the next six to nine months. The model of Paediatric service has implications and links with Maternity services.
32
3.2 Acute Hospital Services – Phased Development In responding to these challenges the Local Commissioning Group Locality has explored a range of actions and models that seek to secure
safe, sustainable services in the Northern area. While there is no immediate/short term risk to the current service model, within the coming 18 months there is a need to have planned for risks that will be faced. Each of the following sub-sections sets out a range of actions and developments that will play a part in the journey of evolving services that will ensure safety is maintained throughout the process.
1. Actions to safely maintain the current two acute hospitals configuration All involved in considering the current model recognise that the challenges currently faced present risks to being able to continue to deliver
services and that the challenges set out, particularly relating to the medical staffing issues, would increasingly present as difficulties . To date efforts to recruit have not seen satisfactory or sustainable solutions. In order to direct further efforts to securing services the following actions are being taken:
A full review of current medical staffing profile in each specialty at Causeway Hospital leading to the development of a medical staffing recruitment plan which will include the following:
Additional efforts to recruit medical staff internationally;
Consider converting some training grade posts to non training grades;
Increased network working between Antrim and Causeway hospital sites; and
Further development of the Hospital at Night model and of the use of non-medical staff in service delivery rotas and models. 2. Developing Networks and Integrated Working with Primary Care To protect services and develop a model that is safe and sustainable, it is essential that we consider our acute service as a whole and
maximise its strengths across the existing two sites. It is our aim to ensure that across both sites there is access 24/7 to urgent/emergency care. We need to enable specialties to deploy their skills and expertise across the sites, including cross site working and where the patients acuity or condition requires it, direct that patient to the most appropriate service within the two site network to meet their needs and achieve the best possible outcome. We need to network too with other areas as we collectively provide the acute services to meet our population needs.
The traditional organisational divisions between secondary and primary care have inhibited the potential for joint working to deliver safe,
local services. In parallel with taking the above actions, work will be progressed to build service models that are safe, sustainable, local and outcome focussed . Initially this work will focus particularly on emergency department services and urgent care, joint working between the Trust with local GPs to consider models that optimise joint local strengths and expertise, including potential to develop new roles with special interests. We will look to other models that have successfully used a joint secondary /primary care approach to maximise local services and/or develop new models to meet our particular needs and take account of our demography.
Section 2.1: Delivering Transformation
33
3.2 Acute Hospital Services – Phased Development 3. Giving consideration to a ‘new build’ single acute hospital for the Northern population The current distribution of our acute hospital resources across the two hospital sites in Antrim and Coleraine, is a
legacy that the Local Commissioning Group Locality must take into account. Throughout the process of developing this population plan there has been open discussion about the location of the buildings that play such a large part in the delivery of local services and there has been broad support from a number of quarters for a new hospital to be more centrally located in the area, it being seen as the best means to ensure the population of the Northern area has equitable access to the full range of acute hospital services. It is acknowledged that such an endeavour would carry a timeframe for realisation estimated at 10 years, and would be subject to the provision of several hundred millions in capital funding. In addition this approach would have a material impact on other Trusts, impacting on patient flows and volumes.
4. Efficiency and Quality: All of these actions and developments are underpinned by the need for increased efficiency
in the use of our acute hospital services. The focus of improved efficiency is on improving throughputs so that the capacity is there to meet the demand for service. However, overwhelming emphasis on improved quality: clinical decisions being made promptly and effectively , reduced delays and overall improved clinical outcomes and better patient experience. This is not unique to the Northern area but is a regional programme of improvement and we set out in this plan actions that we will take to reduce delays, improve access to clinical decision makers, reduce non attendance and cancellation of services, all targeted towards an effective, efficient service that adopts best practice.
5. Conclusion: The Trust will pursue the maintenance and development of acute hospital services across the existing
hospital sites. The following diagram illustrates the actions and the journey that will underpin this approach:
Section 2.1: Delivering Transformation
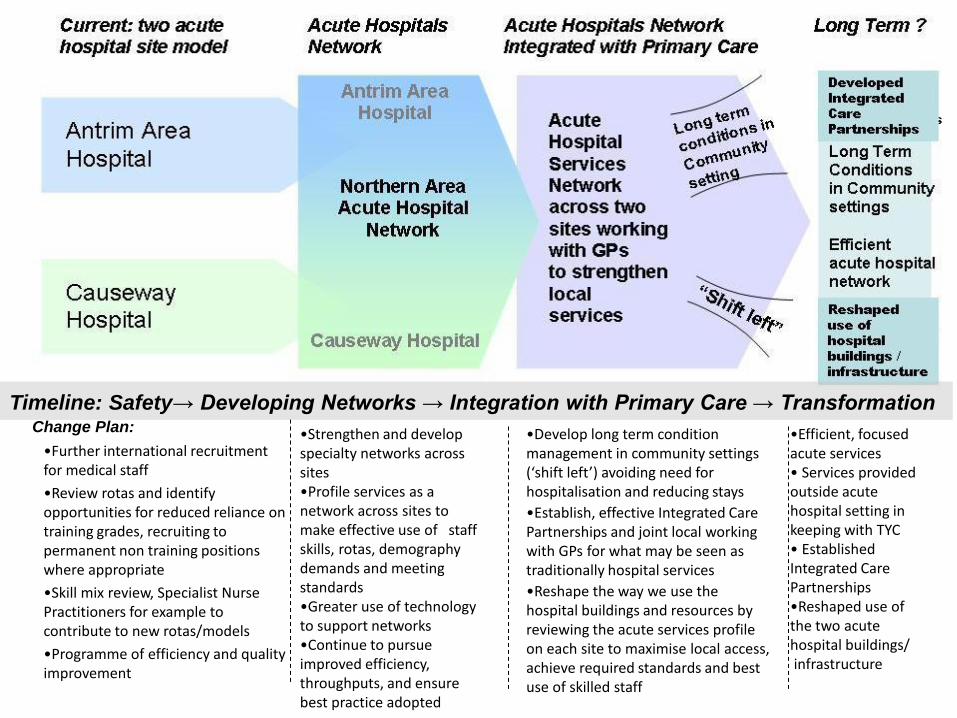
Change Plan:
•Further international recruitment for medical staff
•Review rotas and identify opportunities for reduced reliance on training grades, recruiting to permanent non training positions where appropriate
•Skill mix review, Specialist Nurse Practitioners for example to contribute to new rotas/models
•Programme of efficiency and quality improvement
•Strengthen and develop specialty networks across sites •Profile services as a network across sites to make effective use of staff skills, rotas, demography demands and meeting standards •Greater use of technology to support networks •Continue to pursue improved efficiency, throughputs, and ensure best practice adopted
•Develop long term condition management in community settings (‘shift left’) avoiding need for hospitalisation and reducing stays
•Establish, effective Integrated Care Partnerships and joint local working with GPs for what may be seen as traditionally hospital services
•Reshape the way we use the hospital buildings and resources by reviewing the acute services profile on each site to maximise local access, achieve required standards and best use of skilled staff
•Efficient, focused acute services • Services provided outside acute hospital setting in keeping with TYC • Established Integrated Care Partnerships •Reshaped use of the two acute hospital buildings/ infrastructure
Timeline: Safety→ Developing Networks → Integration with Primary Care → Transformation
35
Section 2.1: Delivering Transformation
3.3 Providing Local Services
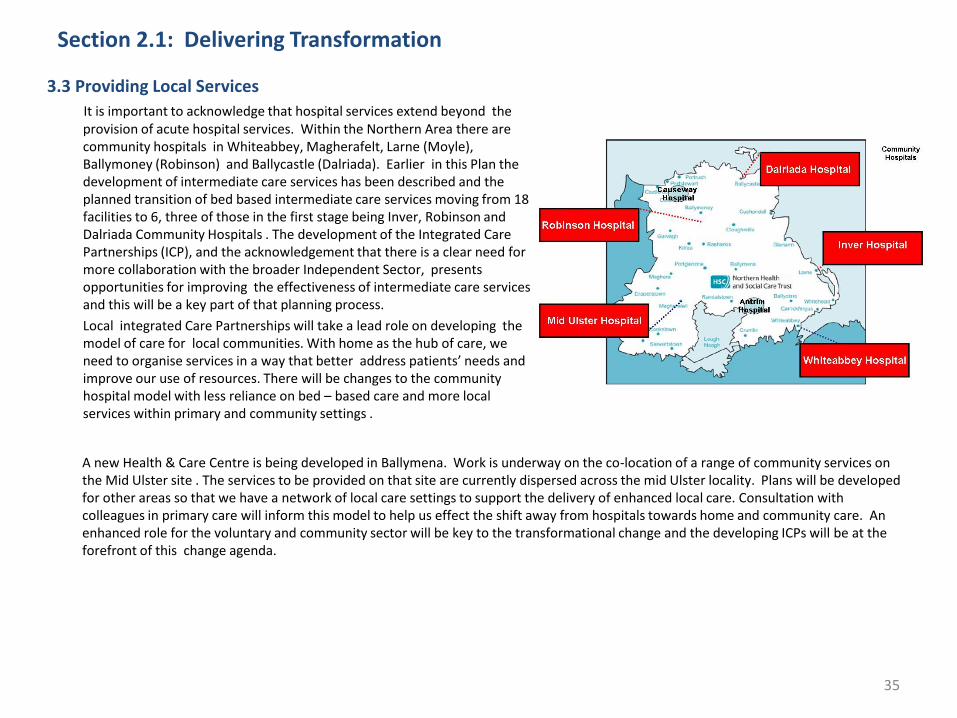
It is important to acknowledge that hospital services extend beyond the provision of acute hospital services. Within the Northern Area there are community hospitals in Whiteabbey, Magherafelt, Larne (Moyle), Ballymoney (Robinson) and Ballycastle (Dalriada). Earlier in this Plan the development of intermediate care services has been described and the planned transition of bed based intermediate care services moving from 18 facilities to 6, three of those in the first stage being Inver, Robinson and Dalriada Community Hospitals . The development of the Integrated Care Partnerships (ICP), and the acknowledgement that there is a clear need for more collaboration with the broader Independent Sector, presents opportunities for improving the effectiveness of intermediate care services and this will be a key part of that planning process.
Local integrated Care Partnerships will take a lead role on developing the model of care for local communities. With home as the hub of care, we need to organise services in a way that better address patients’ needs and improve our use of resources. There will be changes to the community hospital model with less reliance on bed – based care and more local services within primary and community settings .
A new Health & Care Centre is being developed in Ballymena. Work is underway on the co-location of a range of community services on the Mid Ulster site . The services to be provided on that site are currently dispersed across the mid Ulster locality. Plans will be developed for other areas so that we have a network of local care settings to support the delivery of enhanced local care. Consultation with colleagues in primary care will inform this model to help us effect the shift away from hospitals towards home and community care. An enhanced role for the voluntary and community sector will be key to the transformational change and the developing ICPs will be at the forefront of this change agenda.
36
Section 2.1: Delivering Transformation What Transforming Your Care will mean in the Northern Local Commissioning Group Locality
4. Improved Palliative Care and End of Life Services • A person-centred, integrated and holistic approach to service planning and delivery in relation to palliative care and end of life services will be taken
forward in the Northern area. The key focus will ensure that all patients receive high quality reliable care and retain control, choice and dignity to the end of their life.
• Service improvement work will continue to be taken forward, guided by the Northern Ireland Palliative Care Strategy.
• Significant progress has already been made in year one against all of the areas outlined within the Strategy which has included raising public awareness, education for staff involved, and the development of systems and processes to support clients in receipt of palliative care services .
• The focus of work will seek to ensure that patients, from diagnosis to the advanced non- curative stage of disease for all long terms conditions and cancer diagnosis in any setting, lives well and dies well in the way they have planned and in the place of their choosing.
• Our philosophy includes:
– Person led, integrated and holistic approach to service planning and delivery;
– Clinical programmes focused on chronic diseases and health system priorities (not only selected disease focus);
– Workforce and organisational redesign to support the development of new integrated service models across all settings where a person may choose to die, be that at home, care home, hospital, hospice;
– The development of integrated palliative care information systems that can be shared by staff/others involved in providing care and support and create a shared palliative care record, palliative care register;
– A more integrated approach across service providers will support new integrated patient led management approaches with one anticipatory care planning process which will result in less fragmentation of care;
– The implementation of the Liverpool Care Pathway across all settings will ensure consistency, improve patient experience and improve communication;
– Looking to workforce redesign, training and mentoring across all settings including joint work with community/voluntary and statutory care providers will add to the patient centred approach and attention to the needs of caregivers.
5. Improved Learning Disability Services The Northern Local Commissioning Group Locality will design and deliver services aimed at supporting and empowering people with a learning disability
based on the Bamford Equal Lives Principles aimed at improving social inclusion and community integration. A number of service changes will be taken forward across the following areas:
– Day Care Services: Day opportunities and centre based services will be further developed and refined. In addition, work will be undertaken with service users and carers to ensure staff skills reflect the changing needs of service users; We will review the number of buildings we use for day care, commensurate with the levels of activity, demand and locations.
– Respite Services: The range of available respite options will be extended to reduce reliance on bed based placements, through the increased use of carers in the community where appropriate. Bed based services will increasingly be focused on patients with high personal care or complex health needs or challenging behaviour. An overall shift towards a family based model of respite care provision for patients with less dependency requirements will lead to enhanced accessibility and flexibility in the provision of respite care
37
Section 2.1:Delivering Transformation
What Transforming Your Care will mean in the Northern Local Commissioning Group Locality
5. Improved Learning Disability Services (Continued) – Community Living Options:. There will be an increased focus on the use of adult placements which will include moving clients who do not have specific
assessed needs for institutional care into long term family placements as appropriate.
– Resettlement of People Living in Hospital: A number of patients have been identified who are currently living in Muckamore Abbey Hospital, who could benefit from resettlement. Suitable placements will be commissioned and sourced within the Northern area, based on the principle that everyone should live in their own home in the community, with the exception of individuals assessed as specifically requiring nursing or residential care.
6. Improved Physical Health and Disability Services There will be integrated planning across the statutory sector in the Northern area that ensures recognition of disability, promotes social inclusion in all aspects of life
and ensures joined up planning across sectors to enable people with disability to participate more fully within society. A number of service changes will be taken forward across the following areas:
– Further development of partnerships with statutory bodies such as the Northern Ireland Housing Executive to maximise housing support options such as floating services and peripatetic services;
– Further development of support services such as befriending and support networks, in conjunction with community and voluntary sector organisations;
– Increased focus on person centred service delivery so that people with physical disability needs who also have other medical conditions or social needs, will be able to access integrated care and support pathways which will take account of their changing individual needs;
– Utilisation of home based services to assist individuals in managing medical conditions which will include increased use of telehealth and telecare solutions;
– Early commencement of planning to prepare young persons for transition to adulthood which will include the use of early warning alerts at key stages from age 14 years onwards;
– Increased availability and usage of the direct payment approach which will enable individuals to create and buy their own service packages, enabling choice and independence; and
– Continued work to improve access to statutory buildings, services and amenities and appropriate parking at service delivery facilities, as well as collaborative working with other agencies to ensure the recognition of disability and the promotion of social inclusion, to enable people with a disability to participate fully within society.
38
Section 2.1: Delivering Transformation
What Transforming Your Care will mean in the Northern Local Commissioning Group Locality 7. Improved Family and Child Care Services • The Family and Child Care Services Plan within the Northern Local Commissioning Group Locality will shift the focus of care interventions from crisis management to
preventative services. This will necessitate a change in the skill mix of the social care workforce, on the basis that social care staff will increasingly undertake preventative work with families and children.
• As preventative interventions increase, there will be a reduced need for residential care homes for children and young people in the Northern area.
• There will be a continued drive to engage more foster carers and in supporting foster carers to develop a broader range of foster caring skills, in order to provide supportive family environments for children and young people within their own local communities.
• A strategic review will be undertaken within the Child and Adolescent Mental Health Service to review the current service model and compare it with models of best practice with the intention of improving Child and Adolescent Mental Health services locally and across the region by ensuring the implementation of the recommendations outlined in the RQIA CAMHS Review (2012) and the forthcoming DHSSPS Policy Guidance for CAMHS and our own local Review. These reports will provide a basis for reshaping service provision and will require a;
– focus on prevention and early intervention through the establishment of a Primary Mental Health Team and Crisis Resolution
– development of more modern and comprehensive population service through the establishment of Crisis Response and Intensive Home Treatment Services as part of Tier 3 CAMHs provision
– take local steps aimed at further streamlining and integrating CAMHS, Child Development and Behavioural Services with mainstream children's health and social services into a more coherent system of care.
8. Improved Mental Health Services • The vision for mental health services in the Northern Local Commissioning Group Locality is to provide person centred services which offer appropriate treatment and support
to people experiencing mental health difficulties to help them on their individual pathway to recovery. • The continued development of a stepped care approach, in partnership with primary care, with an emphasis on early interventions, and a shift on the reliance of medications
towards a range of alternative therapeutic interventions. • The focus on early intervention will include Early Intervention in Psychosis Service targeted at those aged 16 to 35. • Where hospital treatment is required, then inpatient care will be of a high quality and provided within a therapeutic environment. In this respect, an outline business case will
be completed to secure capital funding for replacement acute inpatient mental health facilities for the Northern area. The number of inpatient beds will be tailored to avoid hospital admissions through community based support and over the next five years we expect to review the current number of inpatient beds in line with that direction of travel.
• Community mental health services will work with the voluntary and community sectors, to strengthen recovery pathways and to support service user involvement in their own recovery.
• To support the shift towards home and community care based provision of care, community mental health teams will be further developed for adult and older people (to include people with dementia who have complex needs), so that assessment, treatment and support can be effectively provided within community settings, both in terms of longer term support and in response to crisis situations.
• The reprovision of statutory bed based EMI services to more appropriate accommodation such as supported living or working with other providers will be explored, in conjunction with service users and their families as appropriate. In addition, increased support will be provided within nursing, residential and intermediate care settings to those providing care to people with dementia within community settings.
• Increased use of supported working and closer working with voluntary sector providers, with a view to resettling people who are currently living in a hospital setting. This will include collaborative working with other providers to develop specialist community services for people including for those with Acquired Brain Injury and Korsokoffs syndrome
• The development of a Psychiatric Liaison Service for older people admitted to general hospital care to ensure improved inpatient care and patient experience and more timely discharge.
39
Section 3
Delivering Service Outcomes
Summary of key initiatives and outcomes
by Programme of Care
40
Section 3: Delivering Service Outcomes
Introduction and Commissioning Perspective
This Population Plan has set out the need for transformational change based on demographic changes together with increased prevalence of long term conditions and the associated demand on hospital beds. There are also the issues of clinical workforce supply difficulties and the need for greater productivity and value for money which must be addressed. In light of these challenges and taking account of the recommendations in TYC, the Northern Local Commissioning Group Locality has identified significant change initiatives that will realise major changes to service models and ways of working to achieve improved outcomes in both quality and productivity. The range of initiatives span all programmes of care but the most fundamental changes are based on the effective management of long term conditions outside of hospital, with the development of Integrated Care Partnerships , the reform of acute hospital services, the reform of services for older people and the continued integration into the community of people with a learning disability.
• Key to the transformation of long term condition management will be the risk stratification of patients with chronic co-morbidities including diabetes, COPD, heart failure, asthma and dementia. Integrated Care Partnerships are being developed to proactively manage long term conditions in primary and community care settings. This will mean new roles for professionals involved in the delivery of care and more integrated working with the voluntary and community sector.
• The reform of acute hospital services will maximise the planned development of outpatient and diagnostic activity within primary and community care settings; secure additional productivity from outpatient, inpatient, day case and diagnostic services from existing hospital infrastructure; support the development of Integrated Care Pathways which proactively manage long term conditions within primary and community care settings and develop pathways across the existing acute settings to promote improved access to services, and facilitate timely and supported discharge for both planned and unplanned attendances. It is also recognised that there is a requirement to continue to maintain safe, resilient and sustainable services across the existing acute sites within the Northern Area, taking account of the need to centralise services where necessary and provide more services within community and primary care where possible. A programme of work will underpin the reform of acute services in keeping with these intentions.
• The reform of services for older people focuses on promoting independence with a greater emphasis on reablement and providing care at home with the extended use of community and voluntary sector services, and reduced reliance on residential care.
• For people with learning disability who have lived for long periods in institutional settings, appropriate accommodation and support will be provided within local communities working closely with individuals, families and professionals to create bespoke arrangements to meet individual needs.
The summary of each of those plans now follow by programme of care, setting out the plan for the delivery of these commissioning intentions. These plans reflect the Commissioner Specifications which highlight the priorities to be addressed in the provision of local services across the programmes of care.
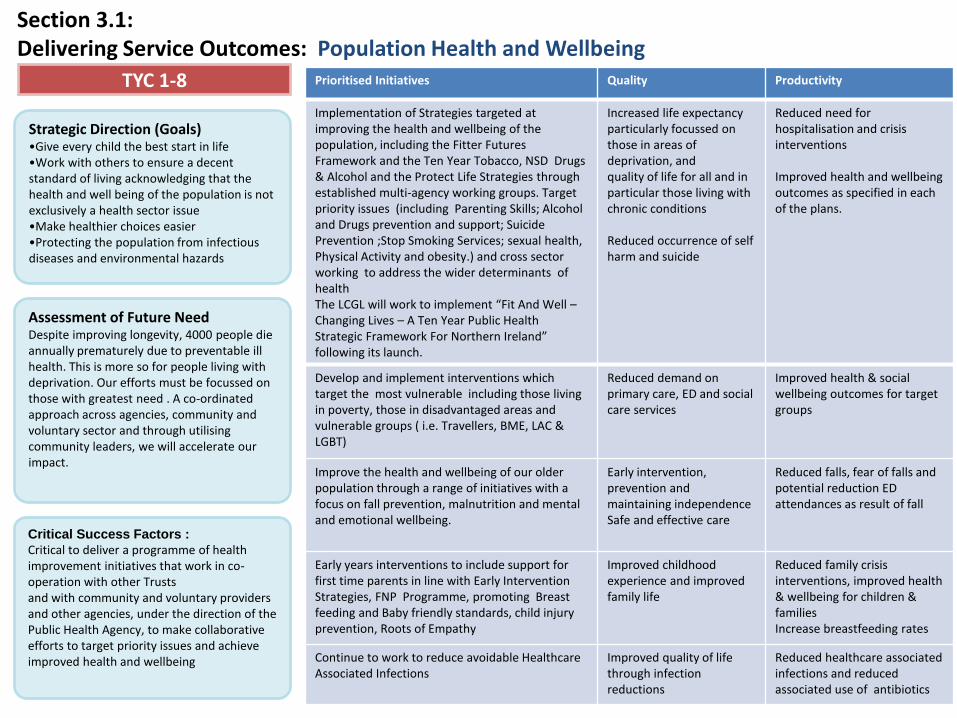
Critical Success Factors : Critical to deliver a programme of health improvement initiatives that work in co-operation with other Trusts and with community and voluntary providers and other agencies, under the direction of the Public Health Agency, to make collaborative efforts to target priority issues and achieve improved health and wellbeing
Section 3.1: Delivering Service Outcomes: Population Health and Wellbeing
Strategic Direction (Goals) •Give every child the best start in life •Work with others to ensure a decent standard of living acknowledging that the health and well being of the population is not exclusively a health sector issue •Make healthier choices easier •Protecting the population from infectious diseases and environmental hazards
Assessment of Future Need Despite improving longevity, 4000 people die annually prematurely due to preventable ill health. This is more so for people living with deprivation. Our efforts must be focussed on those with greatest need . A co-ordinated approach across agencies, community and voluntary sector and through utilising community leaders, we will accelerate our impact.
TYC 1-8 Prioritised Initiatives Quality Productivity
Implementation of Strategies targeted at improving the health and wellbeing of the population, including the Fitter Futures Framework and the Ten Year Tobacco, NSD Drugs & Alcohol and the Protect Life Strategies through established multi-agency working groups. Target priority issues (including Parenting Skills; Alcohol and Drugs prevention and support; Suicide Prevention ;Stop Smoking Services; sexual health, Physical Activity and obesity.) and cross sector working to address the wider determinants of health The LCGL will work to implement “Fit And Well – Changing Lives – A Ten Year Public Health Strategic Framework For Northern Ireland” following its launch.
Increased life expectancy particularly focussed on those in areas of deprivation, and quality of life for all and in particular those living with chronic conditions Reduced occurrence of self harm and suicide
Reduced need for hospitalisation and crisis interventions Improved health and wellbeing outcomes as specified in each of the plans.
Develop and implement interventions which target the most vulnerable including those living in poverty, those in disadvantaged areas and vulnerable groups ( i.e. Travellers, BME, LAC & LGBT)
Reduced demand on primary care, ED and social care services
Improved health & social wellbeing outcomes for target groups
Improve the health and wellbeing of our older population through a range of initiatives with a focus on fall prevention, malnutrition and mental and emotional wellbeing.
Early intervention, prevention and maintaining independence Safe and effective care
Reduced falls, fear of falls and potential reduction ED attendances as result of fall
Early years interventions to include support for first time parents in line with Early Intervention Strategies, FNP Programme, promoting Breast feeding and Baby friendly standards, child injury prevention, Roots of Empathy
Improved childhood experience and improved family life
Reduced family crisis interventions, improved health & wellbeing for children & families Increase breastfeeding rates
Continue to work to reduce avoidable Healthcare Associated Infections
Improved quality of life through infection reductions
Reduced healthcare associated infections and reduced associated use of antibiotics
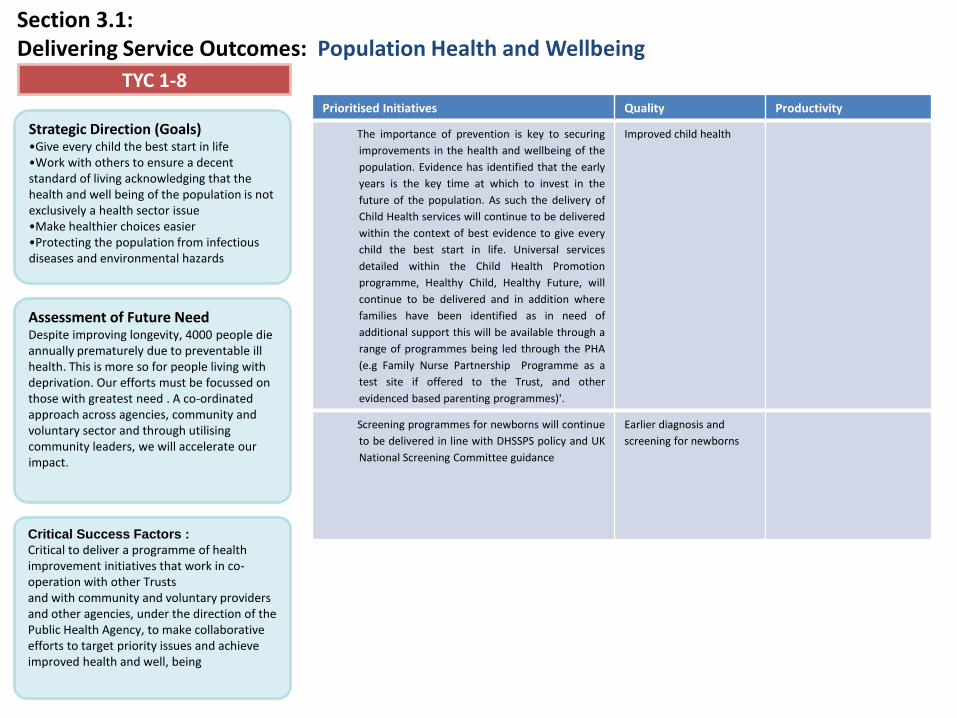
Critical Success Factors : Critical to deliver a programme of health improvement initiatives that work in co-operation with other Trusts and with community and voluntary providers and other agencies, under the direction of the Public Health Agency, to make collaborative efforts to target priority issues and achieve improved health and well, being
Section 3.1: Delivering Service Outcomes: Population Health and Wellbeing
Strategic Direction (Goals) •Give every child the best start in life •Work with others to ensure a decent standard of living acknowledging that the health and well being of the population is not exclusively a health sector issue •Make healthier choices easier •Protecting the population from infectious diseases and environmental hazards
Assessment of Future Need Despite improving longevity, 4000 people die annually prematurely due to preventable ill health. This is more so for people living with deprivation. Our efforts must be focussed on those with greatest need . A co-ordinated approach across agencies, community and voluntary sector and through utilising community leaders, we will accelerate our impact.
TYC 1-8 Prioritised Initiatives Quality Productivity
The importance of prevention is key to securing
improvements in the health and wellbeing of the
population. Evidence has identified that the early
years is the key time at which to invest in the
future of the population. As such the delivery of
Child Health services will continue to be delivered
within the context of best evidence to give every
child the best start in life. Universal services
detailed within the Child Health Promotion
programme, Healthy Child, Healthy Future, will
continue to be delivered and in addition where
families have been identified as in need of
additional support this will be available through a
range of programmes being led through the PHA
(e.g Family Nurse Partnership Programme as a
test site if offered to the Trust, and other
evidenced based parenting programmes)'.
Improved child health
Screening programmes for newborns will continue
to be delivered in line with DHSSPS policy and UK
National Screening Committee guidance
Earlier diagnosis and
screening for newborns
Section 3.2: Delivering Service Outcomes: Integrated Care Partnerships Overview • Key to the delivery of the new model of care proposed in Transforming Your Care is a more integrated approach to
service planning and delivery. The TYC report recommends the establishment of 17 Integrated Care Partnerships (4 in Belfast LCG locality, 4 in South Eastern LCG locality, 3 in Southern LCG locality, 4 in Northern LCG locality and 2 in Western LCG locality) which would join together the full range of health and social care services in each area, including GPs, health and social care providers, hospital specialists and representatives from the independent, voluntary and community sector.
• ICPs would be developed as collaborative networks of service providers. Their aim would be to focus on the ‘Shift
Left’, ensuring that services are delivered as close to patients’/users’ homes as possible, are personalised and seamless; empower patients and promote health and prevent illness where possible.
• Improving how providers work together to the benefit of patients and service users will mean challenging existing
systems and processes that impede effective health and social care in order to ensure: A multi-disciplinary approach to the planning and provision of treatment and care, co-ordinating how care is
planned and delivered; The individual is placed at the centre of care and promoting partnership working, both with individual
service users and within and across the statutory, independent, voluntary and community sectors; Better communication, including detailed, accurate and timely information flow; Safe, high quality treatment and care through taking a holistic approach to improving services; Improved speed of operational decision making; and The effective deployment of resources
43
Section 3.2: Delivering Service Outcomes: Integrated Care Partnerships Overview continued
The development of ICPs would be based on a number of key principles, including;
1. ICPs would be a collaborative alliance with membership that would include statutory, independent and voluntary and community practitioners and organisations. A key consideration would be the inclusion of the voluntary and community sector in the work of ICPs;
2. ICPs would not be established as separate legal entities but would be a networked group of service providers within the existing HSC structures;
3. The aim of ICPs would be to focus on identifying how the blockages and barriers to the integration of services might be overcome through re-designing care pathways and improving how services are planned and delivered to the benefit of patients and clients;
4. ICPs would not have a commissioning role. Responsibility for commissioning and funding services would continue to lie with the HSCB and its LCGs
5. ICPs would be established around natural communities (approximately 100,000 people) and would evolve from and replace the 17 Primary Care Partnerships;
6. ICPs should be clinically led and be based on multi-disciplinary working. Although it is envisaged that General Practitioners would have a key leadership role to play, clinical leadership should not be seen as exclusive to General Practitioners so that opportunities for leadership development should be available to other health and social care professionals
7. ICPs should be operated and regulated in a way that ensures equity of service across all regions.
It is anticipated that initially much of the focus of ICPs would be on the frail elderly and aspects of long term conditions, namely diabetes, stroke care and respiratory conditions. However, it is envisaged that over time ICPs would have the scope to address local priorities for service delivery improvement in line with identified local need and the direction of the Local Commissioning Group Locality.
• ICPs will operate in line with guidelines developed by the Health and Social Care Board and agreed by the Department of Health, Social Services and Public Safety.
• ICPs would play a key role in supporting people to manage their Long Term Conditions, for example in medicine management and community pharmacy. ICPs would also expand the role for community pharmacy in terms of health promotion and medicines management. Effective clinical pharmaceutical practice will significantly improve quality and safety leading to improved health outcomes as well as generating efficiencies.
44
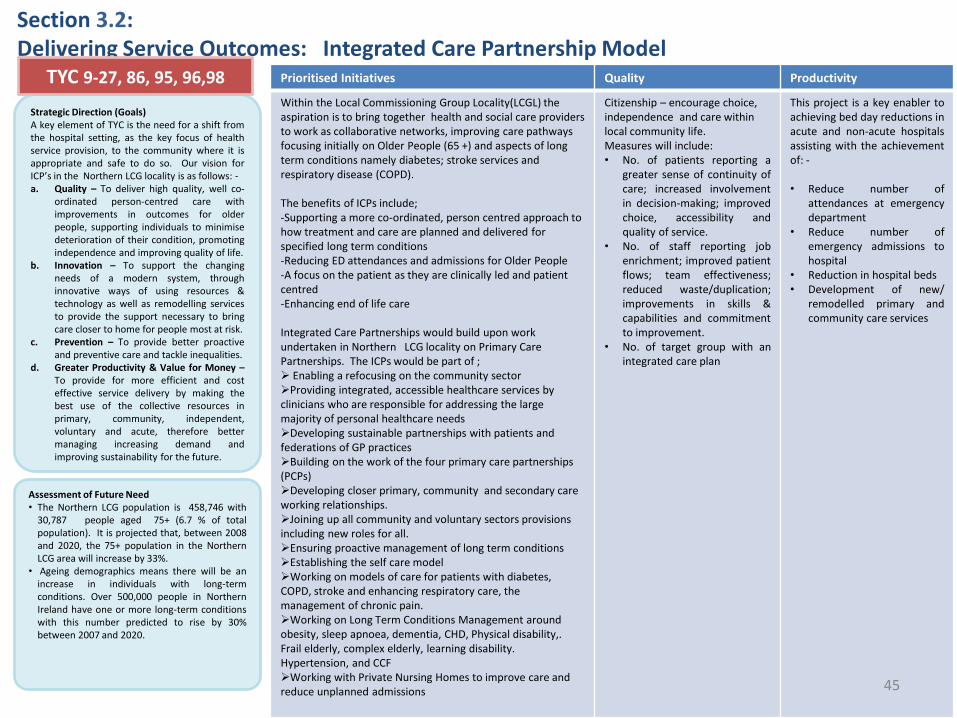
Section 3.2: Delivering Service Outcomes: Integrated Care Partnership Model
Strategic Direction (Goals) A key element of TYC is the need for a shift from the hospital setting, as the key focus of health service provision, to the community where it is appropriate and safe to do so. Our vision for ICP’s in the Northern LCG locality is as follows: - a. Quality – To deliver high quality, well co-
ordinated person-centred care with improvements in outcomes for older people, supporting individuals to minimise deterioration of their condition, promoting independence and improving quality of life.
b. Innovation – To support the changing needs of a modern system, through innovative ways of using resources & technology as well as remodelling services to provide the support necessary to bring care closer to home for people most at risk.
c. Prevention – To provide better proactive and preventive care and tackle inequalities.
d. Greater Productivity & Value for Money – To provide for more efficient and cost effective service delivery by making the best use of the collective resources in primary, community, independent, voluntary and acute, therefore better managing increasing demand and improving sustainability for the future.
Assessment of Future Need • The Northern LCG population is 458,746 with
30,787 people aged 75+ (6.7 % of total population). It is projected that, between 2008 and 2020, the 75+ population in the Northern LCG area will increase by 33%.
• Ageing demographics means there will be an increase in individuals with long-term conditions. Over 500,000 people in Northern Ireland have one or more long-term conditions with this number predicted to rise by 30% between 2007 and 2020.
Prioritised Initiatives Quality Productivity
Within the Local Commissioning Group Locality(LCGL) the aspiration is to bring together health and social care providers to work as collaborative networks, improving care pathways focusing initially on Older People (65 +) and aspects of long term conditions namely diabetes; stroke services and respiratory disease (COPD). The benefits of ICPs include; -Supporting a more co-ordinated, person centred approach to how treatment and care are planned and delivered for specified long term conditions -Reducing ED attendances and admissions for Older People -A focus on the patient as they are clinically led and patient centred -Enhancing end of life care Integrated Care Partnerships would build upon work undertaken in Northern LCG locality on Primary Care Partnerships. The ICPs would be part of ; Enabling a refocusing on the community sector Providing integrated, accessible healthcare services by clinicians who are responsible for addressing the large majority of personal healthcare needs Developing sustainable partnerships with patients and federations of GP practices Building on the work of the four primary care partnerships (PCPs) Developing closer primary, community and secondary care working relationships. Joining up all community and voluntary sectors provisions including new roles for all. Ensuring proactive management of long term conditions Establishing the self care model Working on models of care for patients with diabetes, COPD, stroke and enhancing respiratory care, the management of chronic pain. Working on Long Term Conditions Management around obesity, sleep apnoea, dementia, CHD, Physical disability,. Frail elderly, complex elderly, learning disability. Hypertension, and CCF Working with Private Nursing Homes to improve care and reduce unplanned admissions
Citizenship – encourage choice, independence and care within local community life. Measures will include: • No. of patients reporting a
greater sense of continuity of care; increased involvement in decision-making; improved choice, accessibility and quality of service.
• No. of staff reporting job enrichment; improved patient flows; team effectiveness; reduced waste/duplication; improvements in skills & capabilities and commitment to improvement.
• No. of target group with an integrated care plan
This project is a key enabler to achieving bed day reductions in acute and non-acute hospitals assisting with the achievement of: - • Reduce number of
attendances at emergency department
• Reduce number of emergency admissions to hospital
• Reduction in hospital beds • Development of new/
remodelled primary and community care services
TYC 9-27, 86, 95, 96,98
45
46
Critical Success Factors
• Availability of funding associated with the planning/design stage of the ICP pilot (incl. backfill for clinicians and project management); the testing of the model with a small number of identified GP Practices; and full implementation across the 4 ICPs to be developed in the Northern LCGL This will require the development of a business case and subsequent approval by HSCB.
• GP and Consultant ‘buy-in’ and commitment to the development of the ICP model – this will require agreement between the practices through a Memorandum of Understanding (MoU) working within the current governance & accountability framework, the sharing of practice information and time commitment to the design/planning of the ICP and implementation of the model (e.g. gaining patient consent, risk stratification, attendance at multi-disciplinary case conferences and performance review meetings and undertaking care planning processes). This will require agreement with the Commissioner on a realistic budget for the ICP and alignment of incentives.
• Agreement on an appropriate risk stratification tool/method to identify those patients aged 75+ most at risk of hospital admission and early availability of a common IT platform (likely to be ECR) which can facilitate the sharing of patient information between primary, community and secondary care teams.
• Shift of resources(both funding and staff) from hospital services to support the development of new/remodelled services within primary and community care, e.g. new community-based rapid access service.
• Involvement and engagement of patients/service users and carers and representative groups to inform the development of all elements of the ICP model and performance review/evaluation processes.
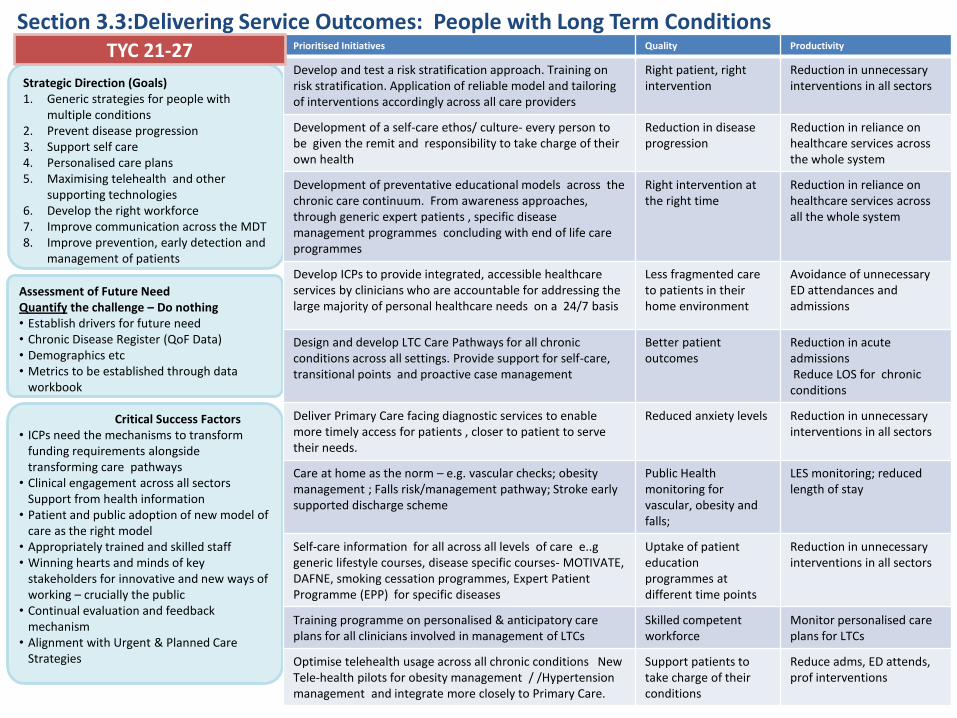
47
Section 3.3:Delivering Service Outcomes: People with Long Term Conditions
Strategic Direction (Goals) 1. Generic strategies for people with
multiple conditions 2. Prevent disease progression 3. Support self care 4. Personalised care plans 5. Maximising telehealth and other
supporting technologies 6. Develop the right workforce 7. Improve communication across the MDT 8. Improve prevention, early detection and
management of patients
Assessment of Future Need Quantify the challenge – Do nothing • Establish drivers for future need • Chronic Disease Register (QoF Data) • Demographics etc • Metrics to be established through data
workbook
Critical Success Factors • ICPs need the mechanisms to transform
funding requirements alongside transforming care pathways
• Clinical engagement across all sectors Support from health information
• Patient and public adoption of new model of care as the right model
• Appropriately trained and skilled staff • Winning hearts and minds of key
stakeholders for innovative and new ways of working – crucially the public
• Continual evaluation and feedback mechanism
• Alignment with Urgent & Planned Care Strategies
Prioritised Initiatives Quality Productivity
Develop and test a risk stratification approach. Training on risk stratification. Application of reliable model and tailoring of interventions accordingly across all care providers
Right patient, right intervention
Reduction in unnecessary interventions in all sectors
Development of a self-care ethos/ culture- every person to be given the remit and responsibility to take charge of their own health
Reduction in disease progression
Reduction in reliance on healthcare services across the whole system
Development of preventative educational models across the chronic care continuum. From awareness approaches, through generic expert patients , specific disease management programmes concluding with end of life care programmes
Right intervention at the right time
Reduction in reliance on healthcare services across all the whole system
Develop ICPs to provide integrated, accessible healthcare services by clinicians who are accountable for addressing the large majority of personal healthcare needs on a 24/7 basis
Less fragmented care to patients in their home environment
Avoidance of unnecessary ED attendances and admissions
Design and develop LTC Care Pathways for all chronic conditions across all settings. Provide support for self-care, transitional points and proactive case management
Better patient outcomes
Reduction in acute admissions Reduce LOS for chronic conditions
Deliver Primary Care facing diagnostic services to enable more timely access for patients , closer to patient to serve their needs.
Reduced anxiety levels Reduction in unnecessary interventions in all sectors
Care at home as the norm – e.g. vascular checks; obesity management ; Falls risk/management pathway; Stroke early supported discharge scheme
Public Health monitoring for vascular, obesity and falls;
LES monitoring; reduced length of stay
Self-care information for all across all levels of care e..g generic lifestyle courses, disease specific courses- MOTIVATE, DAFNE, smoking cessation programmes, Expert Patient Programme (EPP) for specific diseases
Uptake of patient education programmes at different time points
Reduction in unnecessary interventions in all sectors
Training programme on personalised & anticipatory care plans for all clinicians involved in management of LTCs
Skilled competent workforce
Monitor personalised care plans for LTCs
Optimise telehealth usage across all chronic conditions New Tele-health pilots for obesity management / /Hypertension management and integrate more closely to Primary Care.
Support patients to take charge of their conditions
Reduce adms, ED attends, prof interventions
TYC 21-27
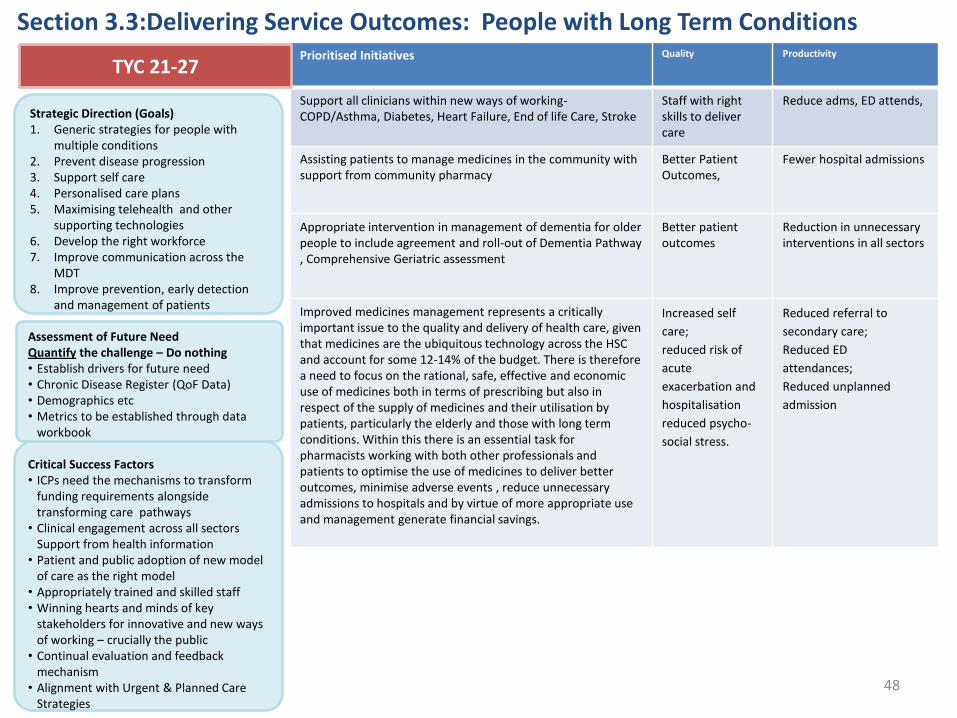
48
Section 3.3:Delivering Service Outcomes: People with Long Term Conditions
Strategic Direction (Goals) 1. Generic strategies for people with
multiple conditions 2. Prevent disease progression 3. Support self care 4. Personalised care plans 5. Maximising telehealth and other
supporting technologies 6. Develop the right workforce 7. Improve communication across the
MDT 8. Improve prevention, early detection
and management of patients
Assessment of Future Need Quantify the challenge – Do nothing • Establish drivers for future need • Chronic Disease Register (QoF Data) • Demographics etc • Metrics to be established through data
workbook Critical Success Factors • ICPs need the mechanisms to transform
funding requirements alongside transforming care pathways
• Clinical engagement across all sectors Support from health information
• Patient and public adoption of new model of care as the right model
• Appropriately trained and skilled staff • Winning hearts and minds of key
stakeholders for innovative and new ways of working – crucially the public
• Continual evaluation and feedback mechanism
• Alignment with Urgent & Planned Care Strategies
Prioritised Initiatives Quality Productivity
Support all clinicians within new ways of working- COPD/Asthma, Diabetes, Heart Failure, End of life Care, Stroke
Staff with right skills to deliver care
Reduce adms, ED attends,
Assisting patients to manage medicines in the community with support from community pharmacy
Better Patient Outcomes,
Fewer hospital admissions
Appropriate intervention in management of dementia for older people to include agreement and roll-out of Dementia Pathway , Comprehensive Geriatric assessment
Better patient outcomes
Reduction in unnecessary interventions in all sectors
Improved medicines management represents a critically important issue to the quality and delivery of health care, given that medicines are the ubiquitous technology across the HSC and account for some 12-14% of the budget. There is therefore a need to focus on the rational, safe, effective and economic use of medicines both in terms of prescribing but also in respect of the supply of medicines and their utilisation by patients, particularly the elderly and those with long term conditions. Within this there is an essential task for pharmacists working with both other professionals and patients to optimise the use of medicines to deliver better outcomes, minimise adverse events , reduce unnecessary admissions to hospitals and by virtue of more appropriate use and management generate financial savings.
Increased self
care;
reduced risk of
acute
exacerbation and
hospitalisation
reduced psycho-
social stress.
Reduced referral to
secondary care;
Reduced ED
attendances;
Reduced unplanned
admission
TYC 21-27
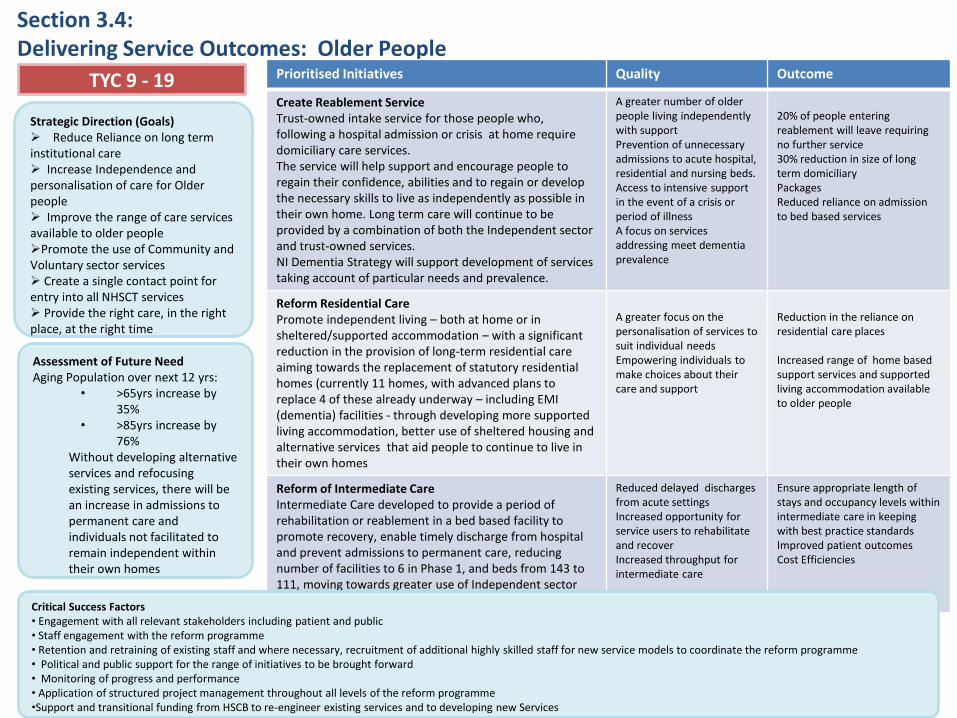
49
Section 3.4: Delivering Service Outcomes: Older People
Strategic Direction (Goals) Reduce Reliance on long term institutional care Increase Independence and personalisation of care for Older people Improve the range of care services available to older people Promote the use of Community and Voluntary sector services Create a single contact point for entry into all NHSCT services Provide the right care, in the right place, at the right time
Assessment of Future Need Aging Population over next 12 yrs:
• >65yrs increase by 35%
• >85yrs increase by 76%
Without developing alternative services and refocusing existing services, there will be an increase in admissions to permanent care and individuals not facilitated to remain independent within their own homes
Prioritised Initiatives Quality Outcome
Create Reablement Service Trust-owned intake service for those people who, following a hospital admission or crisis at home require domiciliary care services. The service will help support and encourage people to regain their confidence, abilities and to regain or develop the necessary skills to live as independently as possible in their own home. Long term care will continue to be provided by a combination of both the Independent sector and trust-owned services. NI Dementia Strategy will support development of services taking account of particular needs and prevalence.
A greater number of older people living independently with support Prevention of unnecessary admissions to acute hospital, residential and nursing beds. Access to intensive support in the event of a crisis or period of illness A focus on services addressing meet dementia prevalence
20% of people entering reablement will leave requiring no further service 30% reduction in size of long term domiciliary Packages Reduced reliance on admission to bed based services
Reform Residential Care Promote independent living – both at home or in sheltered/supported accommodation – with a significant reduction in the provision of long-term residential care aiming towards the replacement of statutory residential homes (currently 11 homes, with advanced plans to replace 4 of these already underway – including EMI (dementia) facilities - through developing more supported living accommodation, better use of sheltered housing and alternative services that aid people to continue to live in their own homes
A greater focus on the personalisation of services to suit individual needs Empowering individuals to make choices about their care and support
Reduction in the reliance on residential care places Increased range of home based support services and supported living accommodation available to older people
Reform of Intermediate Care Intermediate Care developed to provide a period of rehabilitation or reablement in a bed based facility to promote recovery, enable timely discharge from hospital and prevent admissions to permanent care, reducing number of facilities to 6 in Phase 1, and beds from 143 to 111, moving towards greater use of Independent sector
Reduced delayed discharges from acute settings Increased opportunity for service users to rehabilitate and recover Increased throughput for intermediate care
Ensure appropriate length of stays and occupancy levels within intermediate care in keeping with best practice standards Improved patient outcomes Cost Efficiencies
TYC 9 - 19
Critical Success Factors • Engagement with all relevant stakeholders including patient and public • Staff engagement with the reform programme • Retention and retraining of existing staff and where necessary, recruitment of additional highly skilled staff for new service models to coordinate the reform programme • Political and public support for the range of initiatives to be brought forward • Monitoring of progress and performance • Application of structured project management throughout all levels of the reform programme •Support and transitional funding from HSCB to re-engineer existing services and to developing new Services
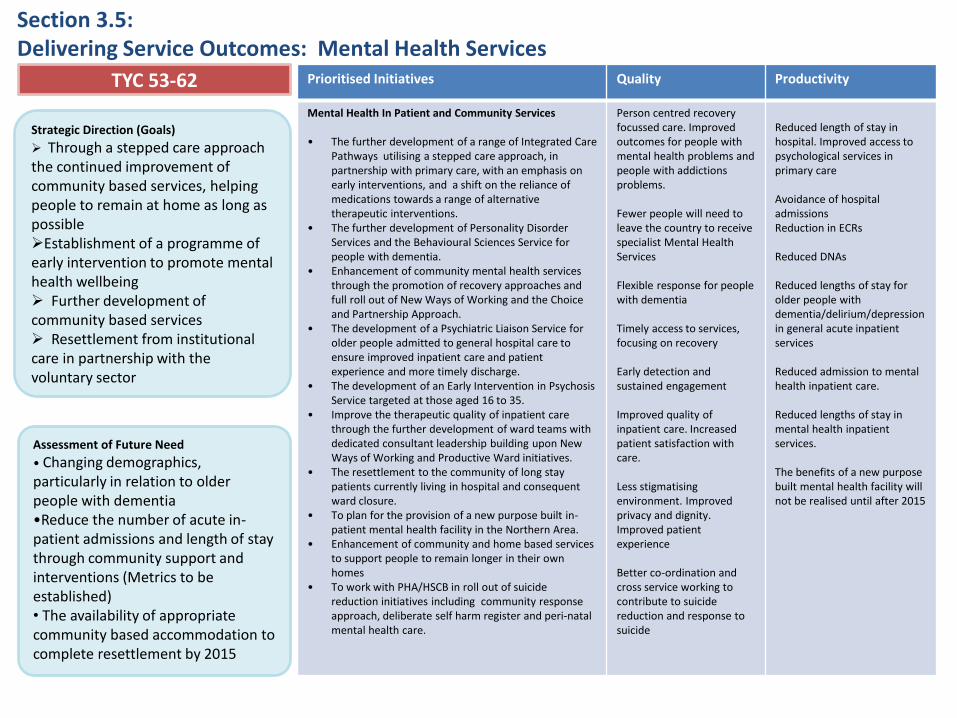
Section 3.5: Delivering Service Outcomes: Mental Health Services
Strategic Direction (Goals)
Through a stepped care approach the continued improvement of community based services, helping people to remain at home as long as possible Establishment of a programme of early intervention to promote mental health wellbeing Further development of community based services Resettlement from institutional care in partnership with the voluntary sector
Assessment of Future Need
• Changing demographics, particularly in relation to older people with dementia •Reduce the number of acute in-patient admissions and length of stay through community support and interventions (Metrics to be established) • The availability of appropriate community based accommodation to complete resettlement by 2015
Prioritised Initiatives Quality Productivity
Mental Health In Patient and Community Services • The further development of a range of Integrated Care
Pathways utilising a stepped care approach, in partnership with primary care, with an emphasis on early interventions, and a shift on the reliance of medications towards a range of alternative therapeutic interventions.
• The further development of Personality Disorder Services and the Behavioural Sciences Service for people with dementia.
• Enhancement of community mental health services through the promotion of recovery approaches and full roll out of New Ways of Working and the Choice and Partnership Approach.
• The development of a Psychiatric Liaison Service for older people admitted to general hospital care to ensure improved inpatient care and patient experience and more timely discharge.
• The development of an Early Intervention in Psychosis Service targeted at those aged 16 to 35.
• Improve the therapeutic quality of inpatient care through the further development of ward teams with dedicated consultant leadership building upon New Ways of Working and Productive Ward initiatives.
• The resettlement to the community of long stay patients currently living in hospital and consequent ward closure.
• To plan for the provision of a new purpose built in-patient mental health facility in the Northern Area.
• Enhancement of community and home based services to support people to remain longer in their own homes
• To work with PHA/HSCB in roll out of suicide reduction initiatives including community response approach, deliberate self harm register and peri-natal mental health care.
Person centred recovery focussed care. Improved outcomes for people with mental health problems and people with addictions problems. Fewer people will need to leave the country to receive specialist Mental Health Services Flexible response for people with dementia Timely access to services, focusing on recovery Early detection and sustained engagement Improved quality of inpatient care. Increased patient satisfaction with care. Less stigmatising environment. Improved privacy and dignity. Improved patient experience Better co-ordination and cross service working to contribute to suicide reduction and response to suicide
Reduced length of stay in hospital. Improved access to psychological services in primary care Avoidance of hospital admissions Reduction in ECRs Reduced DNAs Reduced lengths of stay for older people with dementia/delirium/depression in general acute inpatient services Reduced admission to mental health inpatient care. Reduced lengths of stay in mental health inpatient services. The benefits of a new purpose built mental health facility will not be realised until after 2015
TYC 53-62
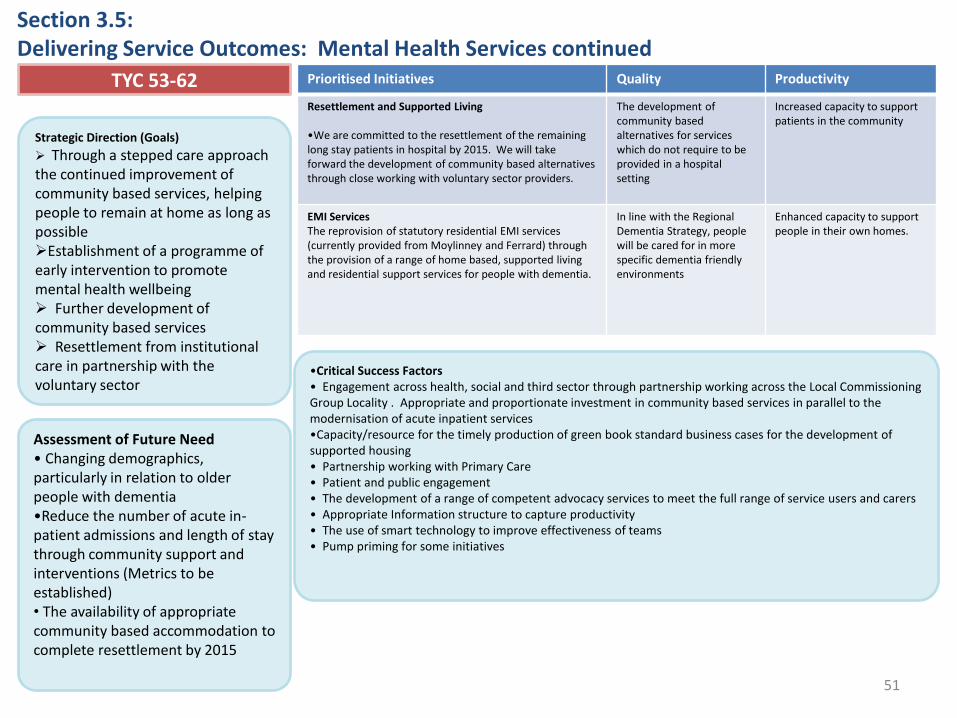
51
Section 3.5: Delivering Service Outcomes: Mental Health Services continued
Prioritised Initiatives Quality Productivity TYC 53-62
•Critical Success Factors • Engagement across health, social and third sector through partnership working across the Local Commissioning Group Locality . Appropriate and proportionate investment in community based services in parallel to the modernisation of acute inpatient services •Capacity/resource for the timely production of green book standard business cases for the development of supported housing • Partnership working with Primary Care • Patient and public engagement • The development of a range of competent advocacy services to meet the full range of service users and carers • Appropriate Information structure to capture productivity • The use of smart technology to improve effectiveness of teams • Pump priming for some initiatives
Prioritised Initiatives Quality Productivity
Resettlement and Supported Living •We are committed to the resettlement of the remaining long stay patients in hospital by 2015. We will take forward the development of community based alternatives through close working with voluntary sector providers.
The development of community based alternatives for services which do not require to be provided in a hospital setting
Increased capacity to support patients in the community
EMI Services The reprovision of statutory residential EMI services (currently provided from Moylinney and Ferrard) through the provision of a range of home based, supported living and residential support services for people with dementia.
In line with the Regional Dementia Strategy, people will be cared for in more specific dementia friendly environments
Enhanced capacity to support people in their own homes.
Strategic Direction (Goals)
Through a stepped care approach the continued improvement of community based services, helping people to remain at home as long as possible Establishment of a programme of early intervention to promote mental health wellbeing Further development of community based services Resettlement from institutional care in partnership with the voluntary sector
Assessment of Future Need • Changing demographics, particularly in relation to older people with dementia •Reduce the number of acute in-patient admissions and length of stay through community support and interventions (Metrics to be established) • The availability of appropriate community based accommodation to complete resettlement by 2015
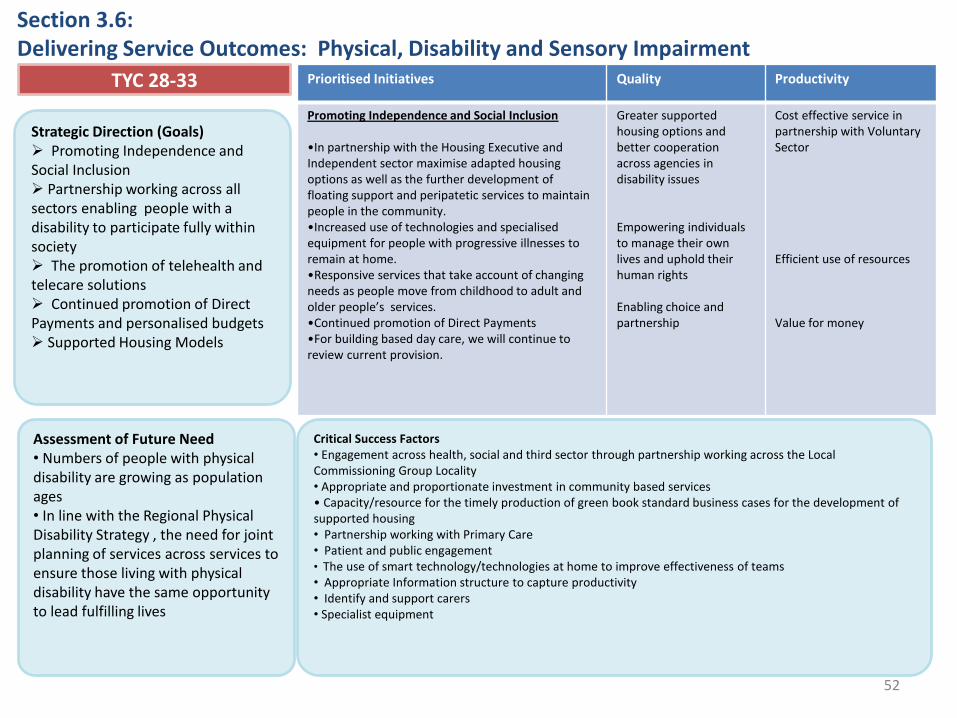
52
Section 3.6: Delivering Service Outcomes: Physical, Disability and Sensory Impairment
Strategic Direction (Goals) Promoting Independence and Social Inclusion Partnership working across all sectors enabling people with a disability to participate fully within society The promotion of telehealth and telecare solutions Continued promotion of Direct Payments and personalised budgets Supported Housing Models
Assessment of Future Need • Numbers of people with physical disability are growing as population ages • In line with the Regional Physical Disability Strategy , the need for joint planning of services across services to ensure those living with physical disability have the same opportunity to lead fulfilling lives
Prioritised Initiatives Quality Productivity
Promoting Independence and Social Inclusion •In partnership with the Housing Executive and Independent sector maximise adapted housing options as well as the further development of floating support and peripatetic services to maintain people in the community. •Increased use of technologies and specialised equipment for people with progressive illnesses to remain at home. •Responsive services that take account of changing needs as people move from childhood to adult and older people’s services. •Continued promotion of Direct Payments •For building based day care, we will continue to review current provision.
Greater supported housing options and better cooperation across agencies in disability issues Empowering individuals to manage their own lives and uphold their human rights Enabling choice and partnership
Cost effective service in partnership with Voluntary Sector Efficient use of resources Value for money
TYC 28-33
Critical Success Factors • Engagement across health, social and third sector through partnership working across the Local Commissioning Group Locality • Appropriate and proportionate investment in community based services • Capacity/resource for the timely production of green book standard business cases for the development of supported housing • Partnership working with Primary Care • Patient and public engagement • The use of smart technology/technologies at home to improve effectiveness of teams • Appropriate Information structure to capture productivity • Identify and support carers • Specialist equipment
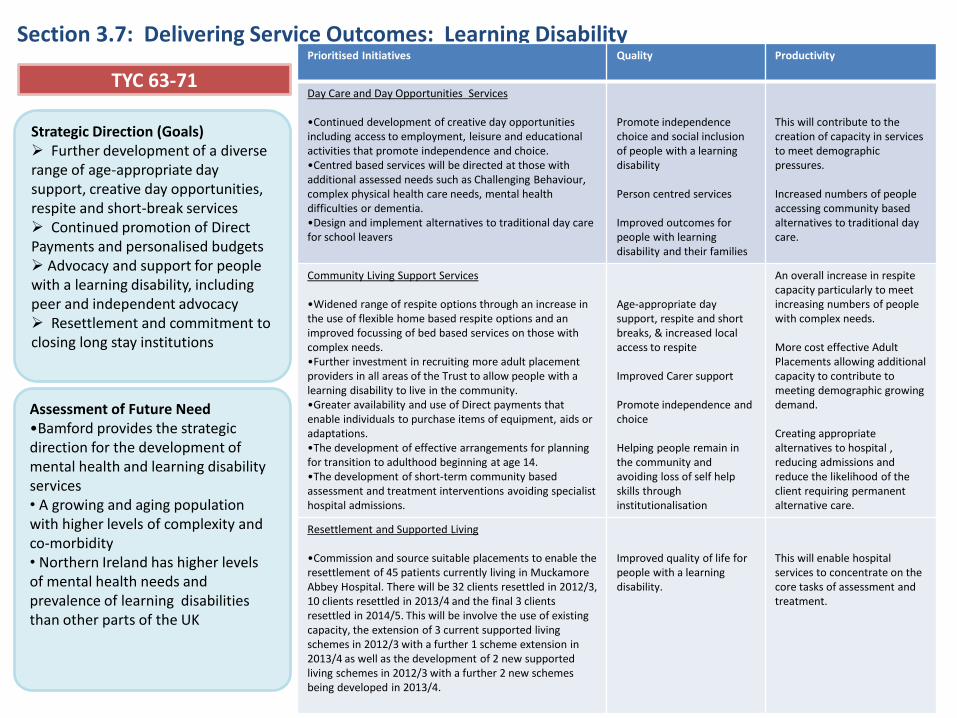
53
Section 3.7: Delivering Service Outcomes: Learning Disability
Strategic Direction (Goals) Further development of a diverse range of age-appropriate day support, creative day opportunities, respite and short-break services Continued promotion of Direct Payments and personalised budgets Advocacy and support for people with a learning disability, including peer and independent advocacy Resettlement and commitment to closing long stay institutions
Assessment of Future Need •Bamford provides the strategic direction for the development of mental health and learning disability services • A growing and aging population with higher levels of complexity and co-morbidity • Northern Ireland has higher levels of mental health needs and prevalence of learning disabilities than other parts of the UK
Prioritised Initiatives Quality Productivity
Day Care and Day Opportunities Services •Continued development of creative day opportunities including access to employment, leisure and educational activities that promote independence and choice. •Centred based services will be directed at those with additional assessed needs such as Challenging Behaviour, complex physical health care needs, mental health difficulties or dementia. •Design and implement alternatives to traditional day care for school leavers
Promote independence choice and social inclusion of people with a learning disability Person centred services Improved outcomes for people with learning disability and their families
This will contribute to the creation of capacity in services to meet demographic pressures. Increased numbers of people accessing community based alternatives to traditional day care.
Community Living Support Services •Widened range of respite options through an increase in the use of flexible home based respite options and an improved focussing of bed based services on those with complex needs. •Further investment in recruiting more adult placement providers in all areas of the Trust to allow people with a learning disability to live in the community. •Greater availability and use of Direct payments that enable individuals to purchase items of equipment, aids or adaptations. •The development of effective arrangements for planning for transition to adulthood beginning at age 14. •The development of short-term community based assessment and treatment interventions avoiding specialist hospital admissions.
Age-appropriate day support, respite and short breaks, & increased local access to respite Improved Carer support Promote independence and choice Helping people remain in the community and avoiding loss of self help skills through institutionalisation
An overall increase in respite capacity particularly to meet increasing numbers of people with complex needs. More cost effective Adult Placements allowing additional capacity to contribute to meeting demographic growing demand. Creating appropriate alternatives to hospital , reducing admissions and reduce the likelihood of the client requiring permanent alternative care.
Resettlement and Supported Living •Commission and source suitable placements to enable the resettlement of 45 patients currently living in Muckamore Abbey Hospital. There will be 32 clients resettled in 2012/3, 10 clients resettled in 2013/4 and the final 3 clients resettled in 2014/5. This will be involve the use of existing capacity, the extension of 3 current supported living schemes in 2012/3 with a further 1 scheme extension in 2013/4 as well as the development of 2 new supported living schemes in 2012/3 with a further 2 new schemes being developed in 2013/4.
Improved quality of life for people with a learning disability.
This will enable hospital services to concentrate on the core tasks of assessment and treatment.
TYC 63-71

54
Section 3.7: Delivering Service Outcomes: Learning Disability continued
Strategic Direction (Goals) Further development of a diverse range of age-appropriate day support, creative day opportunities, respite and short-break services Continued promotion of Direct Payments and personalised budgets Advocacy and support for people with a learning disability, including peer and independent advocacy Resettlement and commitment to closing long stay institutions
Assessment of Future Need •Bamford provides the strategic direction for the development of mental health and learning disability services • A growing and aging population with higher levels of complexity and co-morbidity • Northern Ireland has higher levels of mental health needs and prevalence of learning disabilities than other parts of the UK
Prioritised Initiatives Quality Productivity TYC 63-71
Critical Success Factors • Engagement across health, social and third sector through partnership working across the Local Commissioning Group Locality • Appropriate and proportionate investment in community based services in parallel to the modernisation of resettlement and commitment to closing long stay institutions • Capacity/resource for the timely production of green book standard business cases for the development of supported housing • Partnership working with Primary Care • Patient and public engagement, carer support particularly in relation to resettlement • The development of a range of competent advocacy services to meet the full range of service users and carers •Partnership working with housing providers •Investment in capacity to undertake project work • Appropriate Information structure to capture productivity •Investment to meet resettlement targets. •Regional review of specialist treatment models
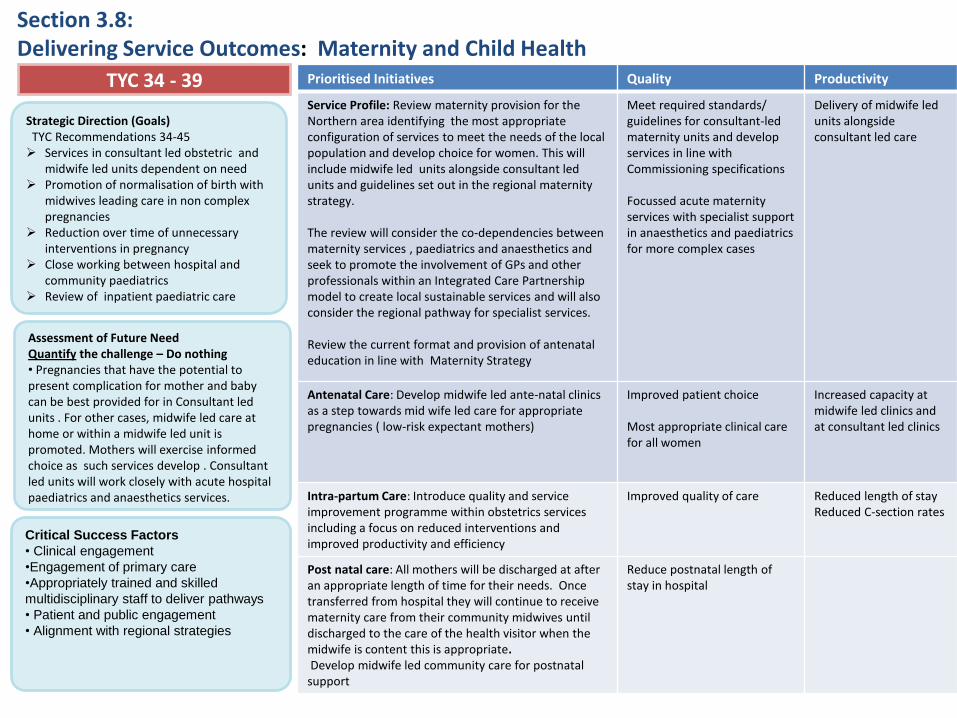
55
Section 3.8: Delivering Service Outcomes: Maternity and Child Health
Strategic Direction (Goals) TYC Recommendations 34-45 Services in consultant led obstetric and
midwife led units dependent on need Promotion of normalisation of birth with
midwives leading care in non complex pregnancies
Reduction over time of unnecessary interventions in pregnancy
Close working between hospital and community paediatrics
Review of inpatient paediatric care
Assessment of Future Need Quantify the challenge – Do nothing • Pregnancies that have the potential to present complication for mother and baby can be best provided for in Consultant led units . For other cases, midwife led care at home or within a midwife led unit is promoted. Mothers will exercise informed choice as such services develop . Consultant led units will work closely with acute hospital paediatrics and anaesthetics services.
Prioritised Initiatives Quality Productivity
Service Profile: Review maternity provision for the Northern area identifying the most appropriate configuration of services to meet the needs of the local population and develop choice for women. This will include midwife led units alongside consultant led units and guidelines set out in the regional maternity strategy. The review will consider the co-dependencies between maternity services , paediatrics and anaesthetics and seek to promote the involvement of GPs and other professionals within an Integrated Care Partnership model to create local sustainable services and will also consider the regional pathway for specialist services. Review the current format and provision of antenatal education in line with Maternity Strategy
Meet required standards/ guidelines for consultant-led maternity units and develop services in line with Commissioning specifications Focussed acute maternity services with specialist support in anaesthetics and paediatrics for more complex cases
Delivery of midwife led units alongside consultant led care
Antenatal Care: Develop midwife led ante-natal clinics as a step towards mid wife led care for appropriate pregnancies ( low-risk expectant mothers)
Improved patient choice Most appropriate clinical care for all women
Increased capacity at midwife led clinics and at consultant led clinics
Intra-partum Care: Introduce quality and service improvement programme within obstetrics services including a focus on reduced interventions and improved productivity and efficiency
Improved quality of care Reduced length of stay Reduced C-section rates
Post natal care: All mothers will be discharged at after an appropriate length of time for their needs. Once transferred from hospital they will continue to receive maternity care from their community midwives until discharged to the care of the health visitor when the midwife is content this is appropriate. Develop midwife led community care for postnatal support
Reduce postnatal length of stay in hospital
TYC 34 - 39
Critical Success Factors
• Clinical engagement
•Engagement of primary care
•Appropriately trained and skilled
multidisciplinary staff to deliver pathways
• Patient and public engagement
• Alignment with regional strategies
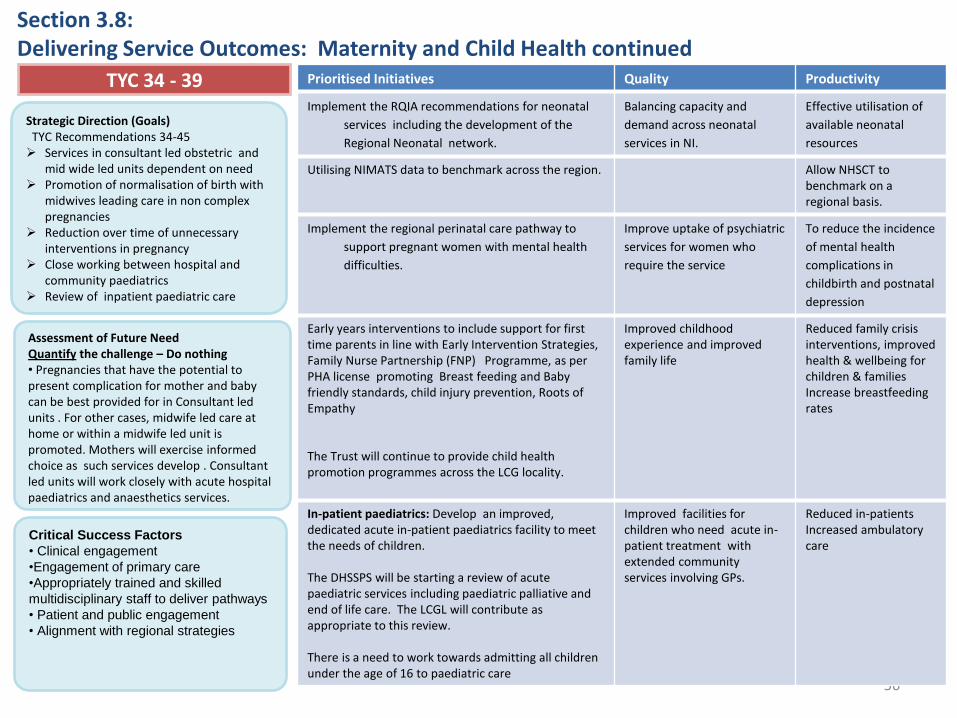
56
Section 3.8: Delivering Service Outcomes: Maternity and Child Health continued
Strategic Direction (Goals) TYC Recommendations 34-45 Services in consultant led obstetric and
mid wide led units dependent on need Promotion of normalisation of birth with
midwives leading care in non complex pregnancies
Reduction over time of unnecessary interventions in pregnancy
Close working between hospital and community paediatrics
Review of inpatient paediatric care
Assessment of Future Need Quantify the challenge – Do nothing • Pregnancies that have the potential to present complication for mother and baby can be best provided for in Consultant led units . For other cases, midwife led care at home or within a midwife led unit is promoted. Mothers will exercise informed choice as such services develop . Consultant led units will work closely with acute hospital paediatrics and anaesthetics services.
Prioritised Initiatives Quality Productivity
Implement the RQIA recommendations for neonatal
services including the development of the
Regional Neonatal network.
Balancing capacity and
demand across neonatal
services in NI.
Effective utilisation of
available neonatal
resources
Utilising NIMATS data to benchmark across the region.
Allow NHSCT to benchmark on a regional basis.
Implement the regional perinatal care pathway to
support pregnant women with mental health
difficulties.
Improve uptake of psychiatric
services for women who
require the service
To reduce the incidence
of mental health
complications in
childbirth and postnatal
depression
Early years interventions to include support for first time parents in line with Early Intervention Strategies, Family Nurse Partnership (FNP) Programme, as per PHA license promoting Breast feeding and Baby friendly standards, child injury prevention, Roots of Empathy The Trust will continue to provide child health promotion programmes across the LCG locality.
Improved childhood experience and improved family life
Reduced family crisis interventions, improved health & wellbeing for children & families Increase breastfeeding rates
In-patient paediatrics: Develop an improved, dedicated acute in-patient paediatrics facility to meet the needs of children. The DHSSPS will be starting a review of acute paediatric services including paediatric palliative and end of life care. The LCGL will contribute as appropriate to this review. There is a need to work towards admitting all children under the age of 16 to paediatric care
Improved facilities for children who need acute in-patient treatment with extended community services involving GPs.
Reduced in-patients Increased ambulatory care
TYC 34 - 39
Critical Success Factors
• Clinical engagement
•Engagement of primary care
•Appropriately trained and skilled
multidisciplinary staff to deliver pathways
• Patient and public engagement
• Alignment with regional strategies
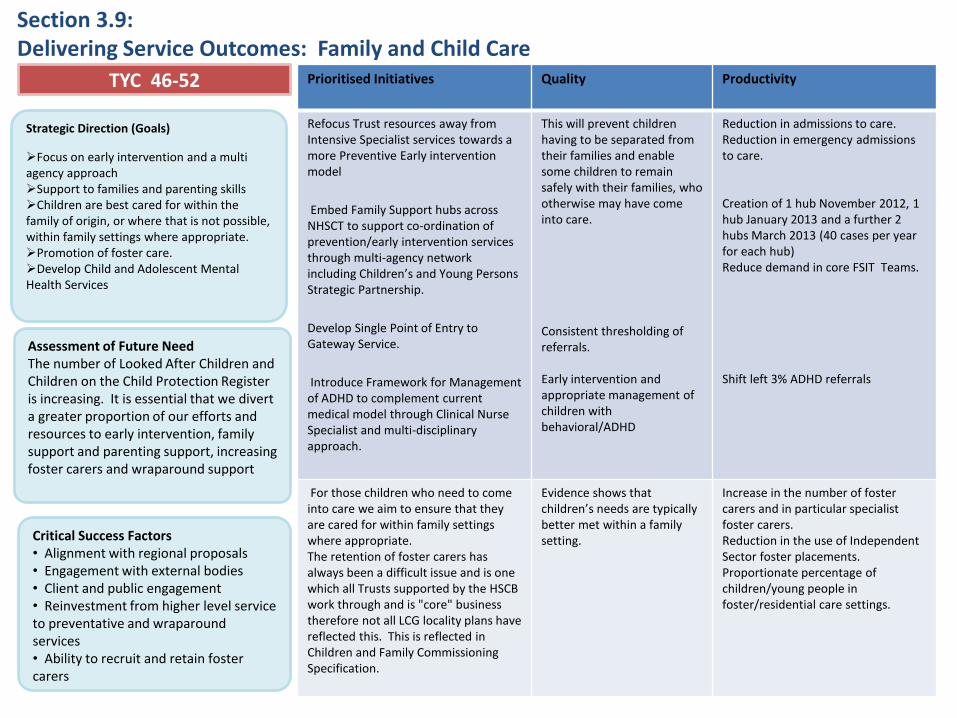
57
Section 3.9: Delivering Service Outcomes: Family and Child Care
Strategic Direction (Goals)
Focus on early intervention and a multi agency approach Support to families and parenting skills Children are best cared for within the family of origin, or where that is not possible, within family settings where appropriate. Promotion of foster care. Develop Child and Adolescent Mental Health Services
Assessment of Future Need The number of Looked After Children and Children on the Child Protection Register is increasing. It is essential that we divert a greater proportion of our efforts and resources to early intervention, family support and parenting support, increasing foster carers and wraparound support
Prioritised Initiatives Quality Productivity
Refocus Trust resources away from Intensive Specialist services towards a more Preventive Early intervention model
Embed Family Support hubs across NHSCT to support co-ordination of prevention/early intervention services through multi-agency network including Children’s and Young Persons Strategic Partnership.
Develop Single Point of Entry to Gateway Service.
Introduce Framework for Management of ADHD to complement current medical model through Clinical Nurse Specialist and multi-disciplinary approach.
This will prevent children having to be separated from their families and enable some children to remain safely with their families, who otherwise may have come into care. Consistent thresholding of referrals. Early intervention and appropriate management of children with behavioral/ADHD
Reduction in admissions to care. Reduction in emergency admissions to care. Creation of 1 hub November 2012, 1 hub January 2013 and a further 2 hubs March 2013 (40 cases per year for each hub) Reduce demand in core FSIT Teams. Shift left 3% ADHD referrals
For those children who need to come into care we aim to ensure that they are cared for within family settings where appropriate. The retention of foster carers has always been a difficult issue and is one which all Trusts supported by the HSCB work through and is "core" business therefore not all LCG locality plans have reflected this. This is reflected in Children and Family Commissioning Specification.
Evidence shows that children’s needs are typically better met within a family setting.
Increase in the number of foster carers and in particular specialist foster carers. Reduction in the use of Independent Sector foster placements. Proportionate percentage of children/young people in foster/residential care settings.
TYC 46-52
Critical Success Factors • Alignment with regional proposals • Engagement with external bodies • Client and public engagement • Reinvestment from higher level service to preventative and wraparound services • Ability to recruit and retain foster carers

58
Section 3.9: Delivering Service Outcomes: Family and Child Care… continued
Strategic Direction (Goals)
Focus on early intervention and a multi agency approach Support to families and parenting skills Children are best cared for within the family of origin, or where that is not possible, within family settings where appropriate. Promotion of foster care. Develop Child and Adolescent Mental Health Services
Assessment of Future Need The number of Looked After Children and Children on the Child Protection Register is increasing. It is essential that we divert a greater proportion of our efforts and resources to early intervention, family support and parenting support, increasing foster carers and wraparound support
Prioritised Initiatives Quality Productivity
In terms of provision of mainstream Children’s Homes the trust’s current model of 6 (provided/commissioned) will be reviewed with the intention of expanding family placements as a possible alternative to one of these homes. This review will take account of the regional review of residential care for children.
Evidence shows that children’s needs are typically better met within a family setting.
No. of residential places (statutory/Independent Sector)
In terms of provision of highly specialist Children’s Homes for children with highly complex needs the trust will develop its own in-house specialist facility to meet children’s needs. This will include consideration of the respite and longer term needs of children with complex physical health care needs.
There will be less reliance on Independent Sector provision. Efficiencies gained present the opportunity for developing the broader range of services described.
Number of children in Independent Sector Specialist placements.
There will be improved utilisation of existing bed based Respite Services and expanded capacity in family based Respite Services for children with complex and disability needs.
As a result there will be a reduction in bed based Respite accommodation from 15 to 12 places and a reinvestment in additional Respite capacity and support overall.
The proportion of bed based respite –v- family based respite volume.
TYC 46-52
Critical Success Factors • Alignment with regional proposals • Engagement with external bodies • Client and public engagement • Reinvestment from higher level service to preventative and wraparound services • Ability to recruit and retain foster carers
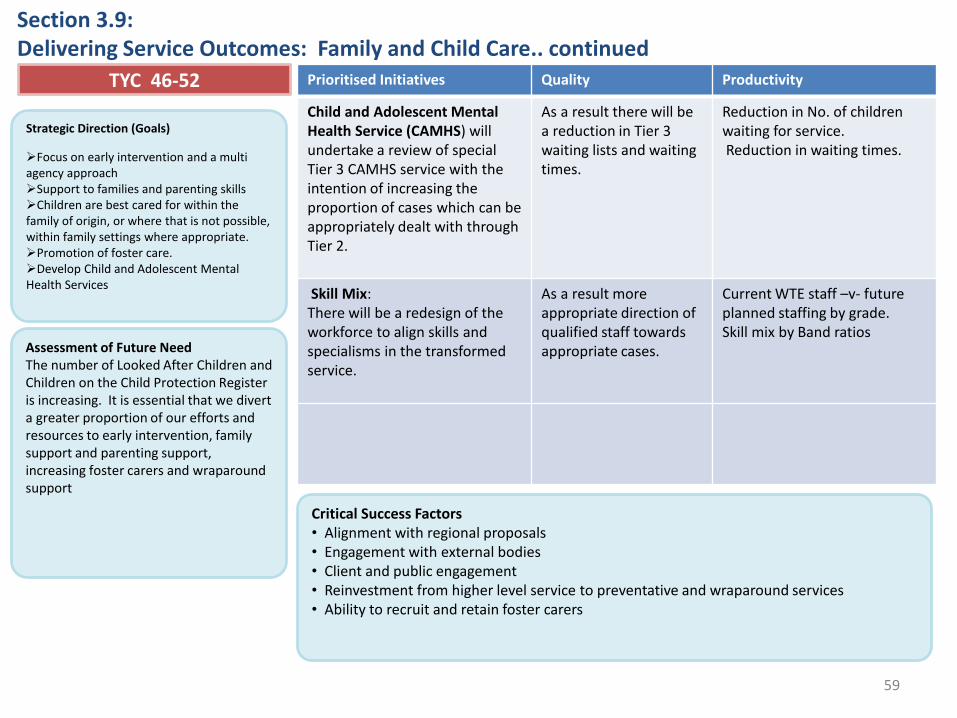
59
Section 3.9: Delivering Service Outcomes: Family and Child Care.. continued
Prioritised Initiatives Quality Productivity
Child and Adolescent Mental Health Service (CAMHS) will undertake a review of special Tier 3 CAMHS service with the intention of increasing the proportion of cases which can be appropriately dealt with through Tier 2.
As a result there will be a reduction in Tier 3 waiting lists and waiting times.
Reduction in No. of children waiting for service. Reduction in waiting times.
Skill Mix: There will be a redesign of the workforce to align skills and specialisms in the transformed service.
As a result more appropriate direction of qualified staff towards appropriate cases.
Current WTE staff –v- future planned staffing by grade. Skill mix by Band ratios
TYC 46-52
Strategic Direction (Goals)
Focus on early intervention and a multi agency approach Support to families and parenting skills Children are best cared for within the family of origin, or where that is not possible, within family settings where appropriate. Promotion of foster care. Develop Child and Adolescent Mental Health Services
Assessment of Future Need The number of Looked After Children and Children on the Child Protection Register is increasing. It is essential that we divert a greater proportion of our efforts and resources to early intervention, family support and parenting support, increasing foster carers and wraparound support
Critical Success Factors • Alignment with regional proposals • Engagement with external bodies • Client and public engagement • Reinvestment from higher level service to preventative and wraparound services • Ability to recruit and retain foster carers

60
Section 3.10 Delivering Service Outcomes: Acute Care: Elective Care
Strategic Direction (Goals) TYC Recommendations 72-79 Develop pathways that allow
direct access to diagnostic tests, one stop clinics, and initiatives that reduce the number of non-attendances.
Day case planned surgery where possible, and in the best location that secures quality and safety. Length of stays for in-patients comparable to best of peer groups.
A focus on productivity and prescribing efficiency.
Assessment of Future Need Without further reform and attention to productivity and best practice efficiency measures, capacity is being lost which leads to extended waiting times and pressures on hospital beds (Examples) •Admission on day of surgery: 66% •Non attendance of patients for out-patient appointments: • 6% new / 10% review
Prioritised Initiatives Quality Productivity
Maximise the number of procedures undertaken on a day case basis, where this is clinically safe
Eliminate unnecessary overnight stays in hospital
Increased day case rates
Further develop day of surgery admission Eliminate unnecessary overnight stays in hospital
Reduced length of stay
Centralise more complex day surgery where necessary at acute sites to ensure safety, best possible outcomes for patients and optimise the resources of skilled staff
Ensure the most appropriate clinical setting for all patients
Increased day case rates
Introduce enhanced recovery pathways to reduce length of stay for patients undergoing major bowel surgery
Faster recovery and improved outcomes for surgical patients
Reduced length of stay
Reduce the number of appointments lost through patients failing to attend using improved partial booking arrangements and the use of technology such as text messaging reminders
Reduction in patients failing to attend outpatient appointments
Develop e-mail screening for GP referrals
Ensure only appropriate patients referred to outpatient clinic
Reduced demand for outpatient appointments
TYC 76 - 77
Critical Success Factors • Clinical engagement throughout all specialties • Engagement of primary care to ensure appropriate referral to outpatients • Provision of additional daycase theatre capacity in Antrim Hospital • Appropriately trained and skilled multidisciplinary staff to deliver enhanced recovery pathways • Patient and public engagement • Alignment with unscheduled care and diagnostic strategies •Effective investment in and use of technology
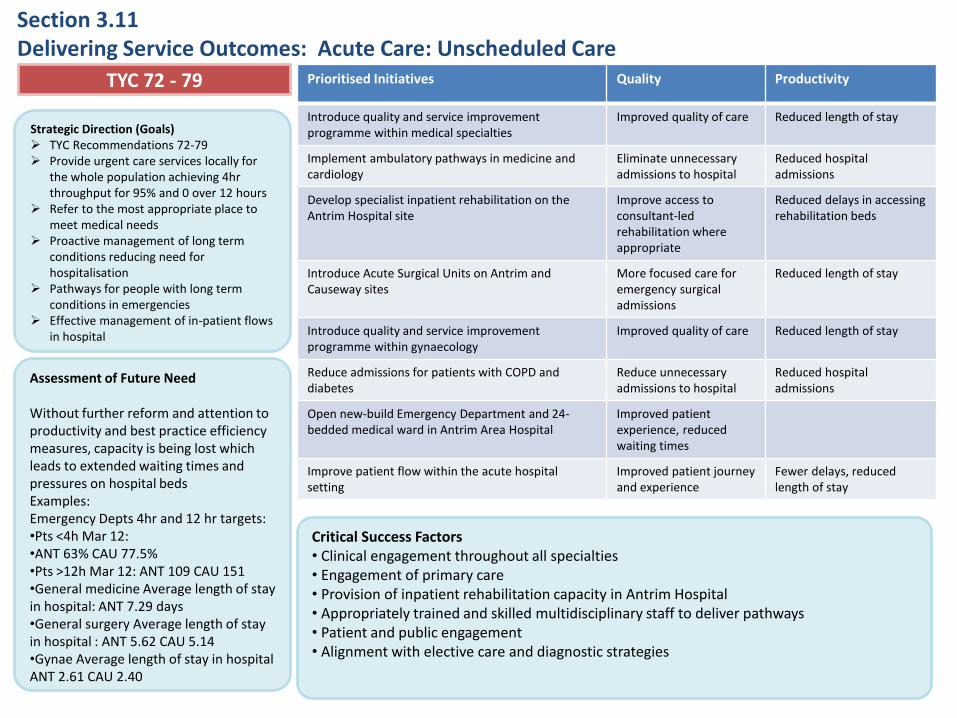
61
Section 3.11 Delivering Service Outcomes: Acute Care: Unscheduled Care
Strategic Direction (Goals) TYC Recommendations 72-79 Provide urgent care services locally for
the whole population achieving 4hr throughput for 95% and 0 over 12 hours
Refer to the most appropriate place to meet medical needs
Proactive management of long term conditions reducing need for hospitalisation
Pathways for people with long term conditions in emergencies
Effective management of in-patient flows in hospital
Assessment of Future Need Without further reform and attention to productivity and best practice efficiency measures, capacity is being lost which leads to extended waiting times and pressures on hospital beds Examples: Emergency Depts 4hr and 12 hr targets: •Pts <4h Mar 12: •ANT 63% CAU 77.5% •Pts >12h Mar 12: ANT 109 CAU 151 •General medicine Average length of stay in hospital: ANT 7.29 days •General surgery Average length of stay in hospital : ANT 5.62 CAU 5.14 •Gynae Average length of stay in hospital ANT 2.61 CAU 2.40
TYC 72 - 79
Critical Success Factors • Clinical engagement throughout all specialties • Engagement of primary care • Provision of inpatient rehabilitation capacity in Antrim Hospital • Appropriately trained and skilled multidisciplinary staff to deliver pathways • Patient and public engagement • Alignment with elective care and diagnostic strategies
Prioritised Initiatives Quality Productivity
Introduce quality and service improvement programme within medical specialties
Improved quality of care Reduced length of stay
Implement ambulatory pathways in medicine and cardiology
Eliminate unnecessary admissions to hospital
Reduced hospital admissions
Develop specialist inpatient rehabilitation on the Antrim Hospital site
Improve access to consultant-led rehabilitation where appropriate
Reduced delays in accessing rehabilitation beds
Introduce Acute Surgical Units on Antrim and Causeway sites
More focused care for emergency surgical admissions
Reduced length of stay
Introduce quality and service improvement programme within gynaecology
Improved quality of care Reduced length of stay
Reduce admissions for patients with COPD and diabetes
Reduce unnecessary admissions to hospital
Reduced hospital admissions
Open new-build Emergency Department and 24-bedded medical ward in Antrim Area Hospital
Improved patient experience, reduced waiting times
Improve patient flow within the acute hospital setting
Improved patient journey and experience
Fewer delays, reduced length of stay
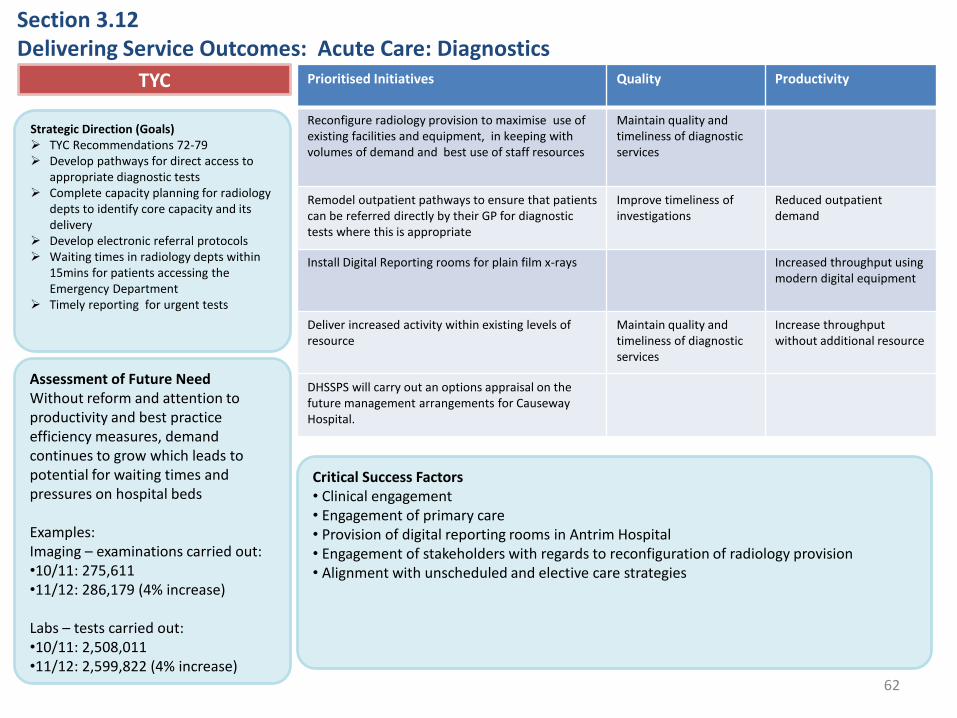
62
Section 3.12 Delivering Service Outcomes: Acute Care: Diagnostics
Strategic Direction (Goals) TYC Recommendations 72-79 Develop pathways for direct access to
appropriate diagnostic tests Complete capacity planning for radiology
depts to identify core capacity and its delivery
Develop electronic referral protocols Waiting times in radiology depts within
15mins for patients accessing the Emergency Department
Timely reporting for urgent tests
Assessment of Future Need Without reform and attention to productivity and best practice efficiency measures, demand continues to grow which leads to potential for waiting times and pressures on hospital beds Examples: Imaging – examinations carried out: •10/11: 275,611 •11/12: 286,179 (4% increase)
Labs – tests carried out: •10/11: 2,508,011 •11/12: 2,599,822 (4% increase)
Prioritised Initiatives Quality Productivity
Reconfigure radiology provision to maximise use of existing facilities and equipment, in keeping with volumes of demand and best use of staff resources
Maintain quality and timeliness of diagnostic services
Remodel outpatient pathways to ensure that patients can be referred directly by their GP for diagnostic tests where this is appropriate
Improve timeliness of investigations
Reduced outpatient demand
Install Digital Reporting rooms for plain film x-rays Increased throughput using modern digital equipment
Deliver increased activity within existing levels of resource
Maintain quality and timeliness of diagnostic services
Increase throughput without additional resource
DHSSPS will carry out an options appraisal on the future management arrangements for Causeway Hospital.
TYC
Critical Success Factors • Clinical engagement • Engagement of primary care • Provision of digital reporting rooms in Antrim Hospital • Engagement of stakeholders with regards to reconfiguration of radiology provision • Alignment with unscheduled and elective care strategies
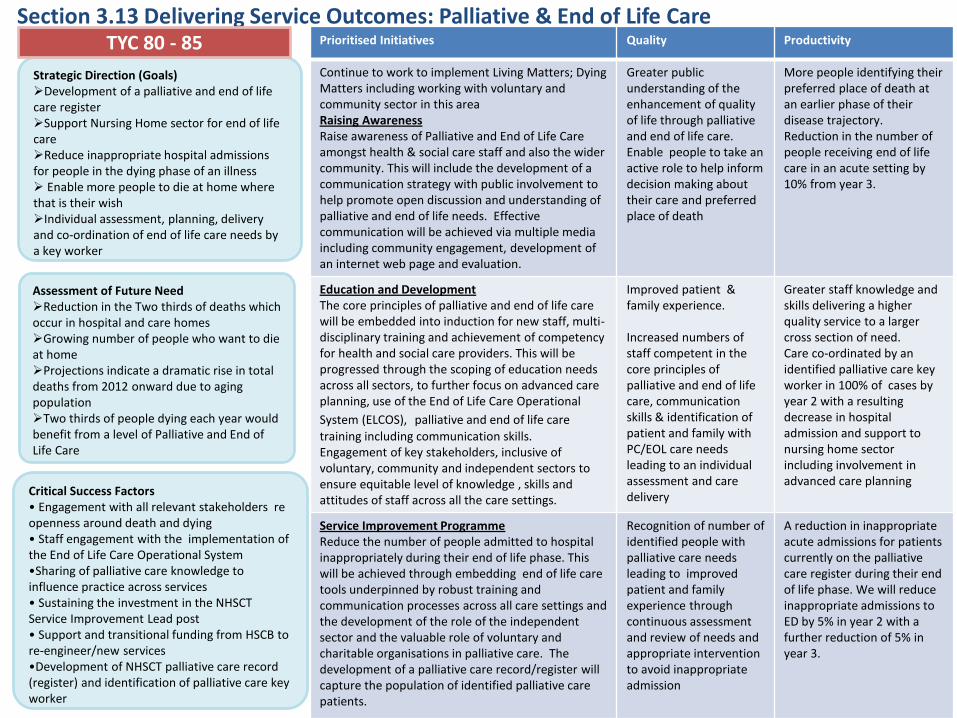
63
Critical Success Factors • Engagement with all relevant stakeholders re openness around death and dying • Staff engagement with the implementation of the End of Life Care Operational System •Sharing of palliative care knowledge to influence practice across services • Sustaining the investment in the NHSCT Service Improvement Lead post • Support and transitional funding from HSCB to re-engineer/new services •Development of NHSCT palliative care record (register) and identification of palliative care key worker
Section 3.13 Delivering Service Outcomes: Palliative & End of Life Care
Strategic Direction (Goals) Development of a palliative and end of life care register Support Nursing Home sector for end of life care Reduce inappropriate hospital admissions for people in the dying phase of an illness Enable more people to die at home where that is their wish Individual assessment, planning, delivery and co-ordination of end of life care needs by a key worker
Assessment of Future Need Reduction in the Two thirds of deaths which occur in hospital and care homes Growing number of people who want to die at home Projections indicate a dramatic rise in total deaths from 2012 onward due to aging population Two thirds of people dying each year would benefit from a level of Palliative and End of Life Care
Prioritised Initiatives Quality Productivity
Continue to work to implement Living Matters; Dying Matters including working with voluntary and community sector in this area Raising Awareness Raise awareness of Palliative and End of Life Care amongst health & social care staff and also the wider community. This will include the development of a communication strategy with public involvement to help promote open discussion and understanding of palliative and end of life needs. Effective communication will be achieved via multiple media including community engagement, development of an internet web page and evaluation.
Greater public understanding of the enhancement of quality of life through palliative and end of life care. Enable people to take an active role to help inform decision making about their care and preferred place of death
More people identifying their preferred place of death at an earlier phase of their disease trajectory. Reduction in the number of people receiving end of life care in an acute setting by 10% from year 3.
Education and Development The core principles of palliative and end of life care will be embedded into induction for new staff, multi-disciplinary training and achievement of competency for health and social care providers. This will be progressed through the scoping of education needs across all sectors, to further focus on advanced care planning, use of the End of Life Care Operational
System (ELCOS), palliative and end of life care
training including communication skills. Engagement of key stakeholders, inclusive of voluntary, community and independent sectors to ensure equitable level of knowledge , skills and attitudes of staff across all the care settings.
Improved patient & family experience. Increased numbers of staff competent in the core principles of palliative and end of life care, communication skills & identification of patient and family with PC/EOL care needs leading to an individual assessment and care delivery
Greater staff knowledge and skills delivering a higher quality service to a larger cross section of need. Care co-ordinated by an identified palliative care key worker in 100% of cases by year 2 with a resulting decrease in hospital admission and support to nursing home sector including involvement in advanced care planning
Service Improvement Programme Reduce the number of people admitted to hospital inappropriately during their end of life phase. This will be achieved through embedding end of life care tools underpinned by robust training and communication processes across all care settings and the development of the role of the independent sector and the valuable role of voluntary and charitable organisations in palliative care. The development of a palliative care record/register will capture the population of identified palliative care patients.
Recognition of number of identified people with palliative care needs leading to improved patient and family experience through continuous assessment and review of needs and appropriate intervention to avoid inappropriate admission
A reduction in inappropriate acute admissions for patients currently on the palliative care register during their end of life phase. We will reduce inappropriate admissions to ED by 5% in year 2 with a further reduction of 5% in year 3.
TYC 80 - 85
64
Section 4
Financial Summary &
Capital Investment

Section 4.1 / 4.2: Financial Summary 1
Northern Trust New Demand Pressures & New Service Initiatives
2012/13 £m
2013/14 £m
2014/15 £m
Specialist /Hospital Drugs (NICE) 4.4 4.1 1.6
Specialist Hospital Services (Renal)
Demographics (Older People etc) 7.3 6.8 6.6
LD/MH resettlements 1.3 1.6 1.4
Elective Care Reform
Revenue Consequences of Capital Exp
(RCCE)
1.2 1.1 0.5
Pay & Non Pay Inflation, incl Rates 11.0 11.4 10.5
Residual & Therapeutic Growth 0.8 0.9 0.9
Service Developments 0 0 1.8
Trust Total 25.8 26.0 23.2
FHS Pressures (including Prescribing) 10.7 9.8 10.1
LCGLTotal 36.7 35.8 33.3
QICR Plans 2012/13 to 2014/15 New demand and service initiatives
The Trust has achieved a breakeven position for the 2011/12 year which is a significant improvement on the previous two years when it had a
control total. The upcoming three years present a challenging environment given the scale of pressures and demands and the need to deliver
financing for these through productivity and cash releasing initiatives. The value of the demand pressures are set out in Table 1 and must be
seen in the context of:
I. the impact of the ageing population in the Northern Area which continues to grow at a faster pace than elsewhere in Northern
Ireland;
II. The continuing demands related to long-term conditions management and treatment associated with an ageing population;
III. The significant pressures and growing demand for Children’s Services;
IV. The need to maintain high quality acute services across a number of sites and the associated costs of risks.
Table 1 below outlines the ways in which the Local Commissioning Group Locality plans to make additional investments to meet increasing
demand and offer a range of new service developments over the period 2012/13 to 2014/15, for both the Northern HSC Trust, and the FHS
sector:
Table 1

Section 4.1 / 4.2 : Financial Summary 1 QICR Plans 2012/13 to 2014/15 Financing New Demand and Service Initiatives
The health and social care sector, like other public sector organisations in Northern Ireland, and across the UK, has been impacted by the financial
settlement under the 2010 Spending Review. The current settlement will not fully fund the new investment requirements set out in Tables 1 above. As a
consequence, both the Trust and the primary care sector are planning towards self-financing an element of these new developments by implementing a
range of efficiency and productivity initiatives. The Trust will be expected to fund 78% of the Trust related pressures in Year 1, 70% in Year 2 and 59% in
Year 3. There are also a large number of assumptions about future income streams and costs which underpin this approach and will need to be tested.
Table 2 below outlines how this self-financing approach will work over the period 2012/13 to 2014/15, for both the Northern HSC Trust, and the FHS
sector, however there are currently Gaps identified in the self financing model:
Northern HSC Trust 2012/13 £m
2013/14 £m
2014/15 £m
Total £m
New Demand pressures &
New Service initiatives
36.7 35.8 33.3 105.8
Funded as follows:
HSC funding & Other Measures 6.0 7.8 9.5 23.3
Trust-generated efficiencies (cash releasing) 10.4 11.8 7.3 29.5
Trust-generated productivity gains (cash avoiding) 5.7 4.6 3.5 13.8
Trust Cash Avoidance undelivered prior year - - (0.9) n/a
Projected Cash Avoidance carried forward - 0.9 2.2 2.2
Trust Cash target undelivered prior year - (3.9) (4.8) n/a
Trust non-recurring measures 0.4 1.0 - -
Gap Cumulative (Cash) 3.5 3.8 6.4 6.4
Trust Total 26.0 26.0 23.20 75.20
HSC funding & Other Measures 0.00 4.70 5.00 9.70
FHS-generated efficiencies (cash releasing) 0.80 0.00 0.00 0.80
FHS-generated productivity gains (cash avoiding) 9.90 5.10 5.10 20.10
FHS Totals 10.70 9.80 10.10 30.60
LCGL Total 36.70 35.80 33.30 105.80
Table 2
Section 4.1 / 4.2: Financial Summary 1 QICR Plans 2012/13 to 2014/15
Efficiency & Productivity approaches – Northern HSC Trust
The efficiency and productivity measures which the Trust will implement to self-finance part of the new investments have
been informed by the work and recommendations from the McKinsey, Appleby I & II, and PEDU reviews.
The Northern Health and Social Care Trust and the Local Commissioning Group recognise that the successful delivery of the
Quality Improvement and Cost Reduction Programme requires a new approach to working collaboratively across the HSC
economy and are committed to realising this.
The Trust’s QICR cash releasing plans for 2012/13 to 2014/15 is set out in Table 3 below, subdivided into the key
workstreams developed, and informed by, the McKinsey and Appleby reviews.
TYC indicated that a 5% shift (which is approximately £83 million in the current budgets) from hospital services would need
to be re-invested into primary and community and social care services by 2014/15. The pace of change will be influenced by
our financial circumstances. Ideally, this would be a 3 to 5 year horizon for the implementation; however, implementation
may be achieved slightly quicker, or indeed we may to need to go at a slightly slower pace, depending on the level of
resources available. We will need to be supported by Transitional Funding over a three year period to make this happen.
Efficiency & Productivity approaches – Northern LCG (FHS)
The Northern LCH (FHS) plans to meet its’ cash releasing and cash avoiding productivity targets over the three years,
mainly through demand management initiatives for prescribing and medicines management.

Section 4.1 /4.2: Financial Summary 1 QICR Plans 2012/13 to 2014/15 – Cash Releasing Proposals
Service area
2012/13
£m
2013/14
£m
2014/15
£m
Total
£m
Reduce GP Referrals 0.00 0.00 0.0 0.00
Application of SBA New to Review ratio 0.00 0.04 0.06 0.10
Reduce DNA New 0.00 0.00 0.00 0.00
Reduce DNA Review 0.00 0.00 0.00 0.00
Reduce Excess Bed days relating to Non-elective
Inpatients
0.00 3.38 0.77 4.15
Pre-Op LOS 0.00 0.00 0.00 0.00
Reduce Cancelled Operations 0.00 0.00 0.00 0.00
Basket of 24 daycase procedures from Inpatients 0.00 0.00 0.01 0.01
Reduce Readmission Rate 0.00 0.00 0.00 0.00
Establish Ambulatory Care patient management
rather than admission
0.00 0.00 0.00 0.00
Reduction of Admissions relating to Asthma, COPD,
Diabetes, Heart failure
0.00 0.15 0.15 0.30
Acute Reform Sub-Total 0.00 3.57 0.99 4.56
Table 3
The Trust has reviewed the IPOP analysis and identified those areas it believes will deliver cash releasing and
productivity gains. This work has been quality assured by E&Y consultants.
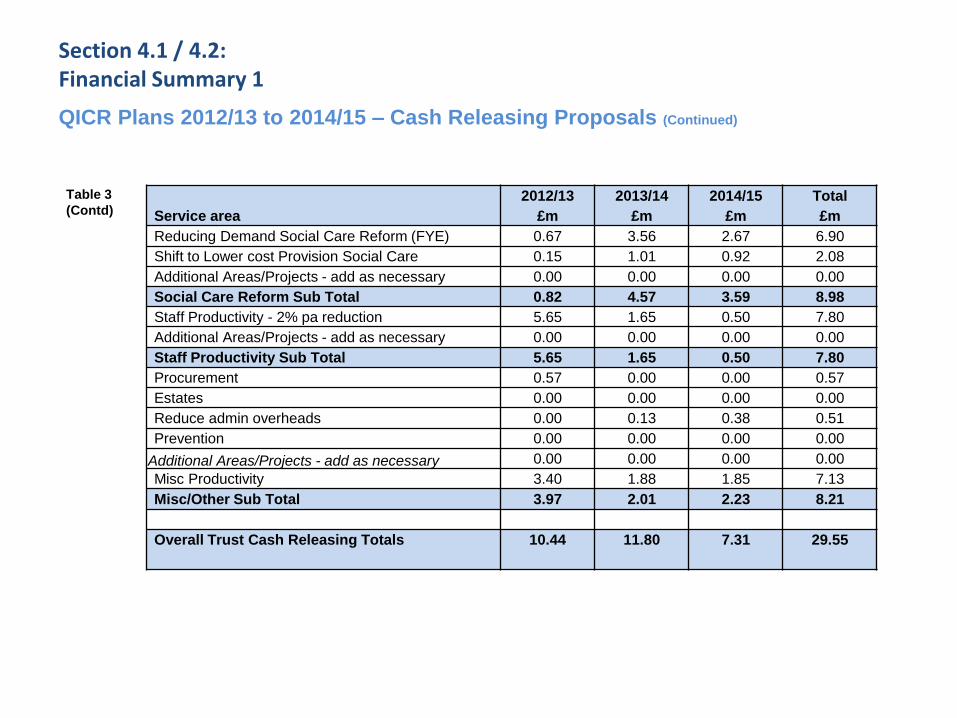
Section 4.1 / 4.2: Financial Summary 1 QICR Plans 2012/13 to 2014/15 – Cash Releasing Proposals (Continued)
Service area
2012/13
£m
2013/14
£m
2014/15
£m
Total
£m
Reducing Demand Social Care Reform (FYE) 0.67 3.56 2.67 6.90
Shift to Lower cost Provision Social Care 0.15 1.01 0.92 2.08
Additional Areas/Projects - add as necessary 0.00 0.00 0.00 0.00
Social Care Reform Sub Total 0.82 4.57 3.59 8.98
Staff Productivity - 2% pa reduction 5.65 1.65 0.50 7.80
Additional Areas/Projects - add as necessary 0.00 0.00 0.00 0.00
Staff Productivity Sub Total 5.65 1.65 0.50 7.80
Procurement 0.57 0.00 0.00 0.57
Estates 0.00 0.00 0.00 0.00
Reduce admin overheads 0.00 0.13 0.38 0.51
Prevention 0.00 0.00 0.00 0.00
Additional Areas/Projects - add as necessary 0.00 0.00 0.00 0.00
Misc Productivity 3.40 1.88 1.85 7.13
Misc/Other Sub Total 3.97 2.01 2.23 8.21
Overall Trust Cash Releasing Totals
10.44 11.80 7.31 29.55
Table 3
(Contd)
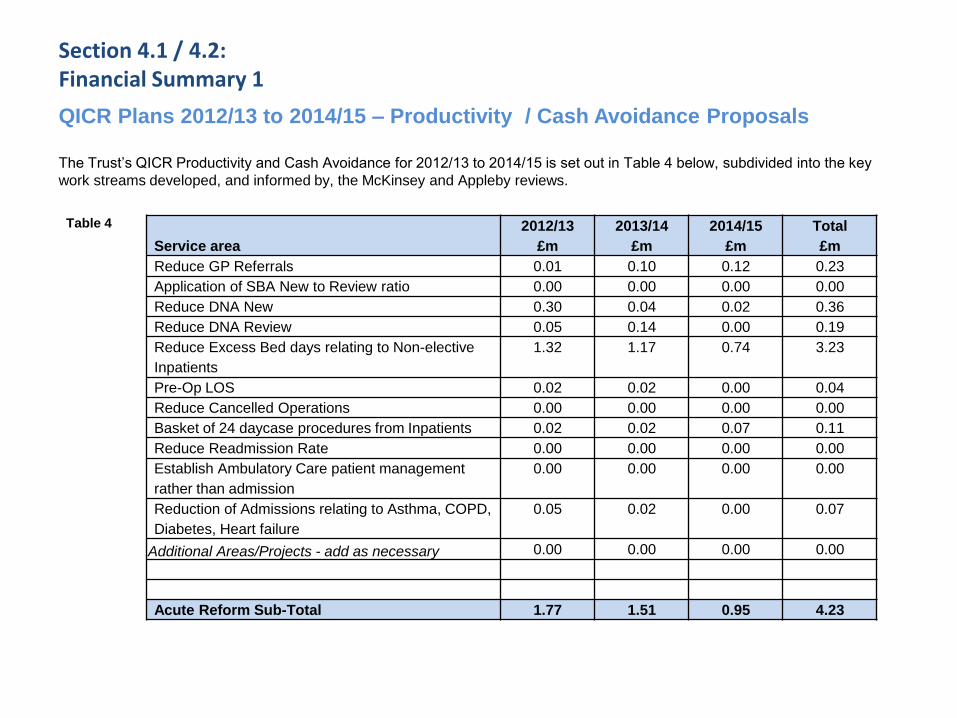
Section 4.1 / 4.2: Financial Summary 1 QICR Plans 2012/13 to 2014/15 – Productivity / Cash Avoidance Proposals
The Trust’s QICR Productivity and Cash Avoidance for 2012/13 to 2014/15 is set out in Table 4 below, subdivided into the key
work streams developed, and informed by, the McKinsey and Appleby reviews.
Service area
2012/13
£m
2013/14
£m
2014/15
£m
Total
£m
Reduce GP Referrals 0.01 0.10 0.12 0.23
Application of SBA New to Review ratio 0.00 0.00 0.00 0.00
Reduce DNA New 0.30 0.04 0.02 0.36
Reduce DNA Review 0.05 0.14 0.00 0.19
Reduce Excess Bed days relating to Non-elective
Inpatients
1.32 1.17 0.74 3.23
Pre-Op LOS 0.02 0.02 0.00 0.04
Reduce Cancelled Operations 0.00 0.00 0.00 0.00
Basket of 24 daycase procedures from Inpatients 0.02 0.02 0.07 0.11
Reduce Readmission Rate 0.00 0.00 0.00 0.00
Establish Ambulatory Care patient management
rather than admission
0.00 0.00 0.00 0.00
Reduction of Admissions relating to Asthma, COPD,
Diabetes, Heart failure
0.05 0.02 0.00 0.07
Additional Areas/Projects - add as necessary 0.00 0.00 0.00 0.00
Acute Reform Sub-Total 1.77 1.51 0.95 4.23
Table 4
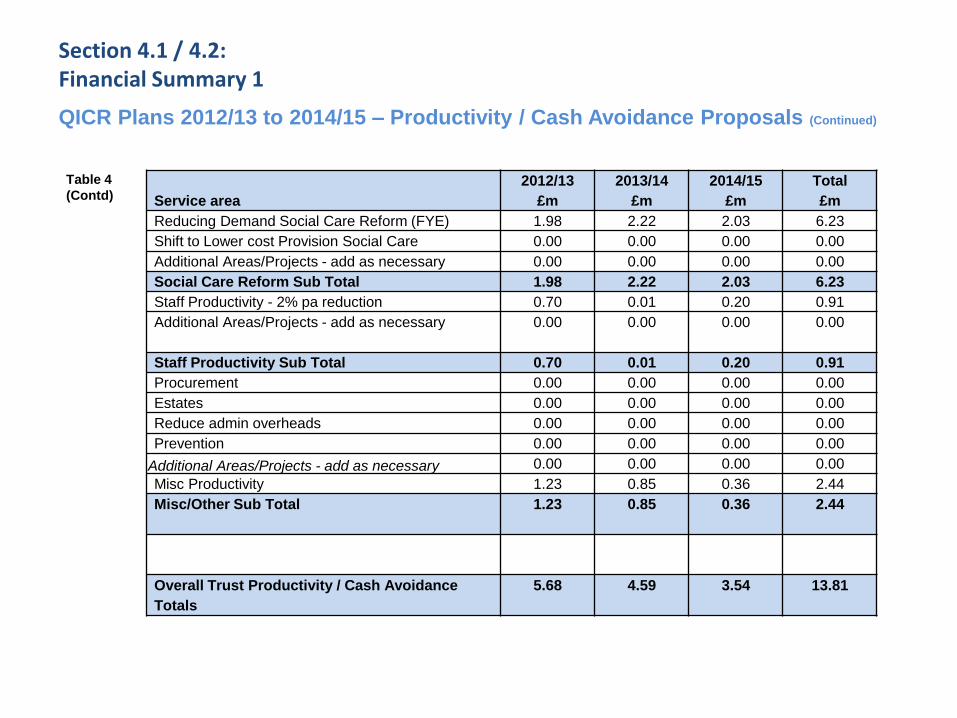
Section 4.1 / 4.2: Financial Summary 1 QICR Plans 2012/13 to 2014/15 – Productivity / Cash Avoidance Proposals (Continued)
Service area
2012/13
£m
2013/14
£m
2014/15
£m
Total
£m
Reducing Demand Social Care Reform (FYE) 1.98 2.22 2.03 6.23
Shift to Lower cost Provision Social Care 0.00 0.00 0.00 0.00
Additional Areas/Projects - add as necessary 0.00 0.00 0.00 0.00
Social Care Reform Sub Total 1.98 2.22 2.03 6.23
Staff Productivity - 2% pa reduction 0.70 0.01 0.20 0.91
Additional Areas/Projects - add as necessary 0.00 0.00 0.00 0.00
Staff Productivity Sub Total 0.70 0.01 0.20 0.91
Procurement 0.00 0.00 0.00 0.00
Estates 0.00 0.00 0.00 0.00
Reduce admin overheads 0.00 0.00 0.00 0.00
Prevention 0.00 0.00 0.00 0.00
Additional Areas/Projects - add as necessary 0.00 0.00 0.00 0.00
Misc Productivity 1.23 0.85 0.36 2.44
Misc/Other Sub Total 1.23
0.85 0.36 2.44
Overall Trust Productivity / Cash Avoidance
Totals
5.68 4.59 3.54 13.81
Table 4
(Contd)
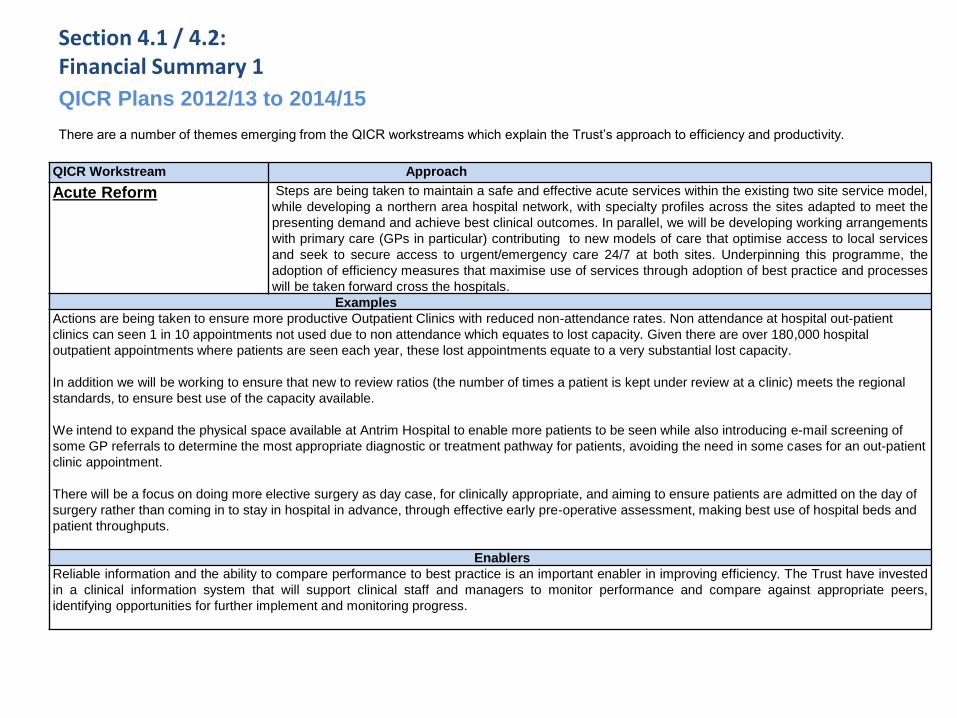
Section 4.1 / 4.2: Financial Summary 1 QICR Plans 2012/13 to 2014/15
There are a number of themes emerging from the QICR workstreams which explain the Trust’s approach to efficiency and productivity.
QICR Workstream Approach
Acute Reform Steps are being taken to maintain a safe and effective acute services within the existing two site service model,
while developing a northern area hospital network, with specialty profiles across the sites adapted to meet the
presenting demand and achieve best clinical outcomes. In parallel, we will be developing working arrangements
with primary care (GPs in particular) contributing to new models of care that optimise access to local services
and seek to secure access to urgent/emergency care 24/7 at both sites. Underpinning this programme, the
adoption of efficiency measures that maximise use of services through adoption of best practice and processes
will be taken forward cross the hospitals.
Examples
Actions are being taken to ensure more productive Outpatient Clinics with reduced non-attendance rates. Non attendance at hospital out-patient
clinics can seen 1 in 10 appointments not used due to non attendance which equates to lost capacity. Given there are over 180,000 hospital
outpatient appointments where patients are seen each year, these lost appointments equate to a very substantial lost capacity.
In addition we will be working to ensure that new to review ratios (the number of times a patient is kept under review at a clinic) meets the regional
standards, to ensure best use of the capacity available.
We intend to expand the physical space available at Antrim Hospital to enable more patients to be seen while also introducing e-mail screening of
some GP referrals to determine the most appropriate diagnostic or treatment pathway for patients, avoiding the need in some cases for an out-patient
clinic appointment.
There will be a focus on doing more elective surgery as day case, for clinically appropriate, and aiming to ensure patients are admitted on the day of
surgery rather than coming in to stay in hospital in advance, through effective early pre-operative assessment, making best use of hospital beds and
patient throughputs.
Enablers
Reliable information and the ability to compare performance to best practice is an important enabler in improving efficiency. The Trust have invested
in a clinical information system that will support clinical staff and managers to monitor performance and compare against appropriate peers,
identifying opportunities for further implement and monitoring progress.
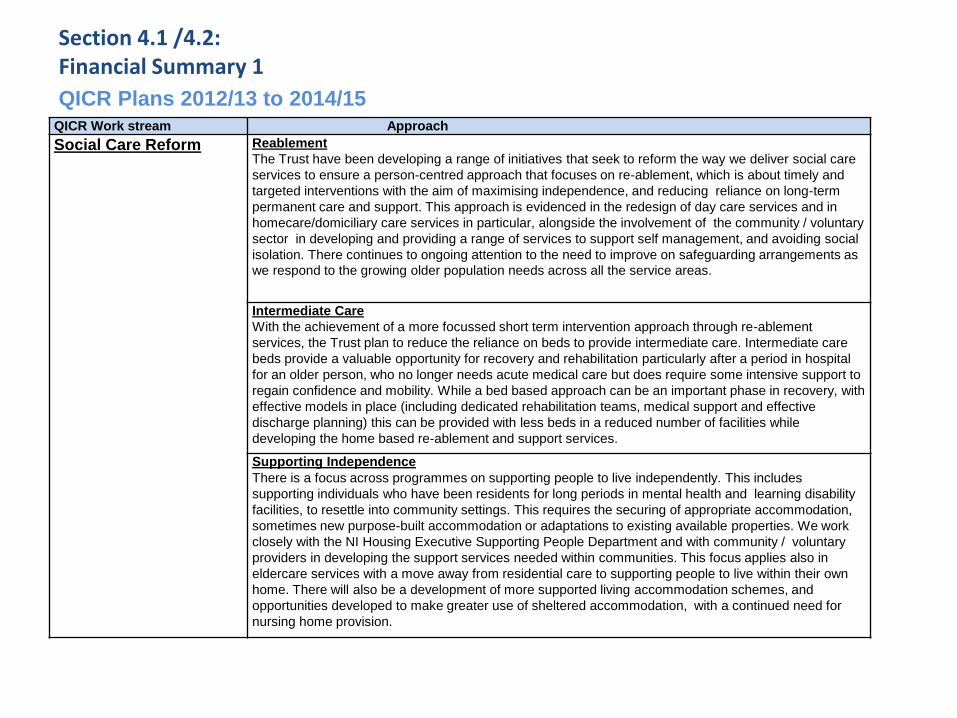
Section 4.1 /4.2: Financial Summary 1 QICR Plans 2012/13 to 2014/15
QICR Work stream Approach
Social Care Reform Reablement
The Trust have been developing a range of initiatives that seek to reform the way we deliver social care
services to ensure a person-centred approach that focuses on re-ablement, which is about timely and
targeted interventions with the aim of maximising independence, and reducing reliance on long-term
permanent care and support. This approach is evidenced in the redesign of day care services and in
homecare/domiciliary care services in particular, alongside the involvement of the community / voluntary
sector in developing and providing a range of services to support self management, and avoiding social
isolation. There continues to ongoing attention to the need to improve on safeguarding arrangements as
we respond to the growing older population needs across all the service areas.
Intermediate Care
With the achievement of a more focussed short term intervention approach through re-ablement
services, the Trust plan to reduce the reliance on beds to provide intermediate care. Intermediate care
beds provide a valuable opportunity for recovery and rehabilitation particularly after a period in hospital
for an older person, who no longer needs acute medical care but does require some intensive support to
regain confidence and mobility. While a bed based approach can be an important phase in recovery, with
effective models in place (including dedicated rehabilitation teams, medical support and effective
discharge planning) this can be provided with less beds in a reduced number of facilities while
developing the home based re-ablement and support services.
Supporting Independence There is a focus across programmes on supporting people to live independently. This includes
supporting individuals who have been residents for long periods in mental health and learning disability
facilities, to resettle into community settings. This requires the securing of appropriate accommodation,
sometimes new purpose-built accommodation or adaptations to existing available properties. We work
closely with the NI Housing Executive Supporting People Department and with community / voluntary
providers in developing the support services needed within communities. This focus applies also in
eldercare services with a move away from residential care to supporting people to live within their own
home. There will also be a development of more supported living accommodation schemes, and
opportunities developed to make greater use of sheltered accommodation, with a continued need for
nursing home provision.
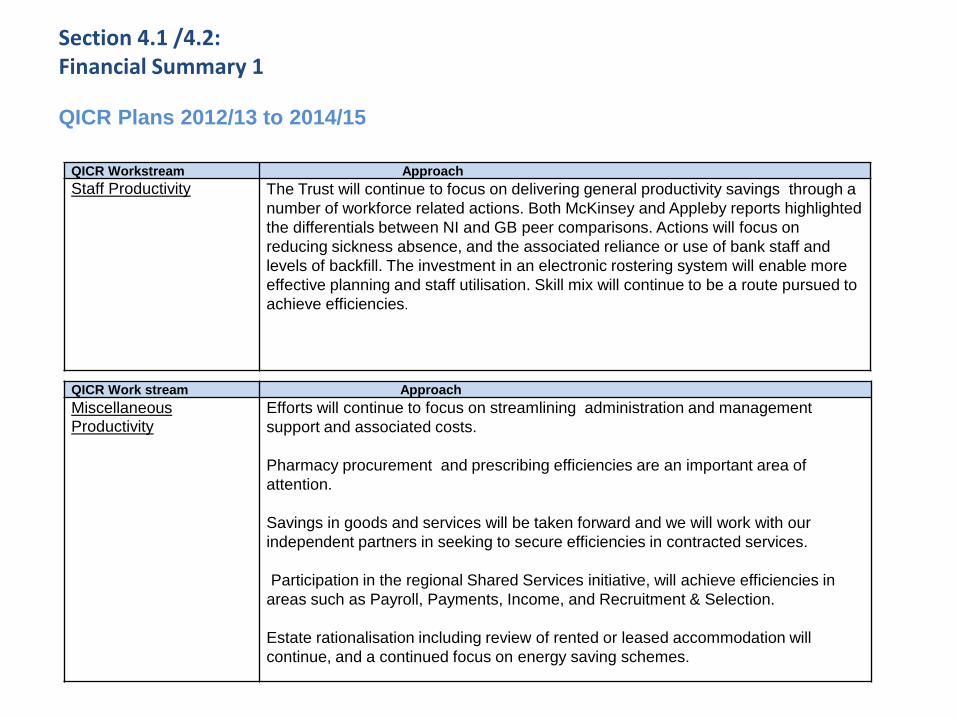
Section 4.1 /4.2: Financial Summary 1 QICR Plans 2012/13 to 2014/15
QICR Workstream Approach
Staff Productivity The Trust will continue to focus on delivering general productivity savings through a
number of workforce related actions. Both McKinsey and Appleby reports highlighted
the differentials between NI and GB peer comparisons. Actions will focus on
reducing sickness absence, and the associated reliance or use of bank staff and
levels of backfill. The investment in an electronic rostering system will enable more
effective planning and staff utilisation. Skill mix will continue to be a route pursued to
achieve efficiencies.
QICR Work stream Approach
Miscellaneous Productivity
Efforts will continue to focus on streamlining administration and management
support and associated costs.
Pharmacy procurement and prescribing efficiencies are an important area of
attention.
Savings in goods and services will be taken forward and we will work with our
independent partners in seeking to secure efficiencies in contracted services.
Participation in the regional Shared Services initiative, will achieve efficiencies in
areas such as Payroll, Payments, Income, and Recruitment & Selection.
Estate rationalisation including review of rented or leased accommodation will
continue, and a continued focus on energy saving schemes.
Section 4.2 Financial Assessment of Transforming Your Care
• In order to assess the degree to which Transforming Your Care will shift health and social care expenditure
away from hospital based care to community based care, a high level assessment process
was developed by the HSCB working closely with DHSSPS, PHA and the 5 Local Commissioning Group Localities.
• Key assumptions were used and new service re-provision models were considered at a preliminary and strategic level.
• The objective of the modelling and assessment process has been to determine the potential level of
additional health and social care expenditure which would be spent on providing community based
services closer to the patient’s home as a direct result of implementing Transforming Your Care proposals,
• This additional expenditure would be expected to shift primarily from hospital based services, as the need
for institutional care was avoided due to new community based integrated models of care .
• A number of key priority items were identified in the Population Plans put forward by the 5 Local Commissioning Group Localities
and the cost of providing these new models of care through Integrated Care Partnerships or other
service re-provision models in the community was estimated up to 2014/15.
• The potential for avoiding hospital based expenditure due to the above new models of care was estimated
along with the potential to redeploy existing hospital baseline resources. Any net additional funding
requirement was also assessed for affordability within the HSC 3 year Financial Plan to 2012/13-2014/15.
• The initial findings of the assessment process suggest that a significant proportion of the 5 % shift of
expenditure away from hospital based care to community based care, as envisaged by Transforming Your
Care is achievable by 2014/15. This assurance was informed by a number of assumptions and caveats.
Section 4.3: Capital Infrastructure & Investment Programmes
Looking ahead, the Investment Strategy for Northern Ireland provides for an indicative allocation of £1.7bn from 2015/16 – 2020/21 against an estimated need of £2.3bn, leaving a projected shortfall of over £800m some of which may be addressed by revenue financing solutions such as Public Private Partnership (PPP).
The current Health, Social Services and Public Safety capital programme contains the following elements:
• Major capital schemes agreed by DHSSPS Minister
• Ongoing annual capital requirement of each Trust such as IT, general ongoing maintenance, health and safety requirements and equipment needs.
In this context, it is increasingly likely that without additional sources of capital funding, the scope to take forward major modernisations projects will need to be phased to take account of budgetary availability.
The estimated need for backlog maintenance is well over £1bn. This is addition to the figures stated above although new developments when delivered will reduce the need for backlog maintenance.
76
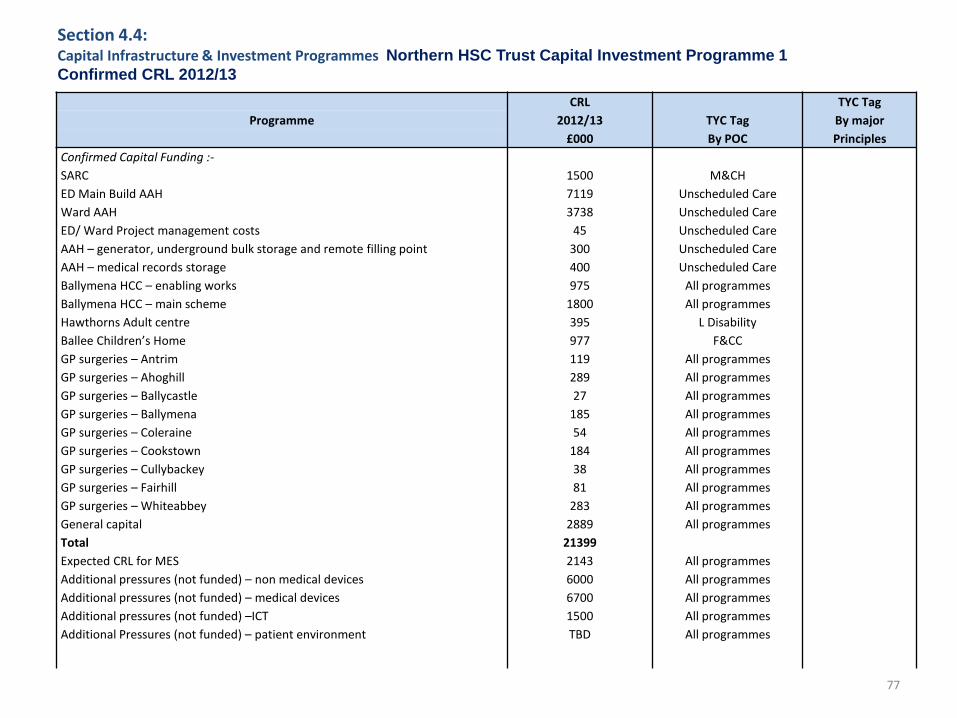
77
Section 4.4: Capital Infrastructure & Investment Programmes Northern HSC Trust Capital Investment Programme 1
Confirmed CRL 2012/13
CRL
2012/13
£000
TYC Tag
By POC
TYC Tag
By major
Principles
Programme
Confirmed Capital Funding :-
SARC
ED Main Build AAH
Ward AAH
ED/ Ward Project management costs
AAH – generator, underground bulk storage and remote filling point
AAH – medical records storage
Ballymena HCC – enabling works
Ballymena HCC – main scheme
Hawthorns Adult centre
Ballee Children’s Home
GP surgeries – Antrim
GP surgeries – Ahoghill
GP surgeries – Ballycastle
GP surgeries – Ballymena
GP surgeries – Coleraine
GP surgeries – Cookstown
GP surgeries – Cullybackey
GP surgeries – Fairhill
GP surgeries – Whiteabbey
General capital
Total
Expected CRL for MES
Additional pressures (not funded) – non medical devices
Additional pressures (not funded) – medical devices
Additional pressures (not funded) –ICT
Additional Pressures (not funded) – patient environment
1500
7119
3738
45
300
400
975
1800
395
977
119
289
27
185
54
184
38
81
283
2889
21399
2143
6000
6700
1500
TBD
M&CH
Unscheduled Care
Unscheduled Care
Unscheduled Care
Unscheduled Care
Unscheduled Care
All programmes
All programmes
L Disability
F&CC
All programmes
All programmes
All programmes
All programmes
All programmes
All programmes
All programmes
All programmes
All programmes
All programmes
All programmes
All programmes
All programmes
All programmes
All programmes
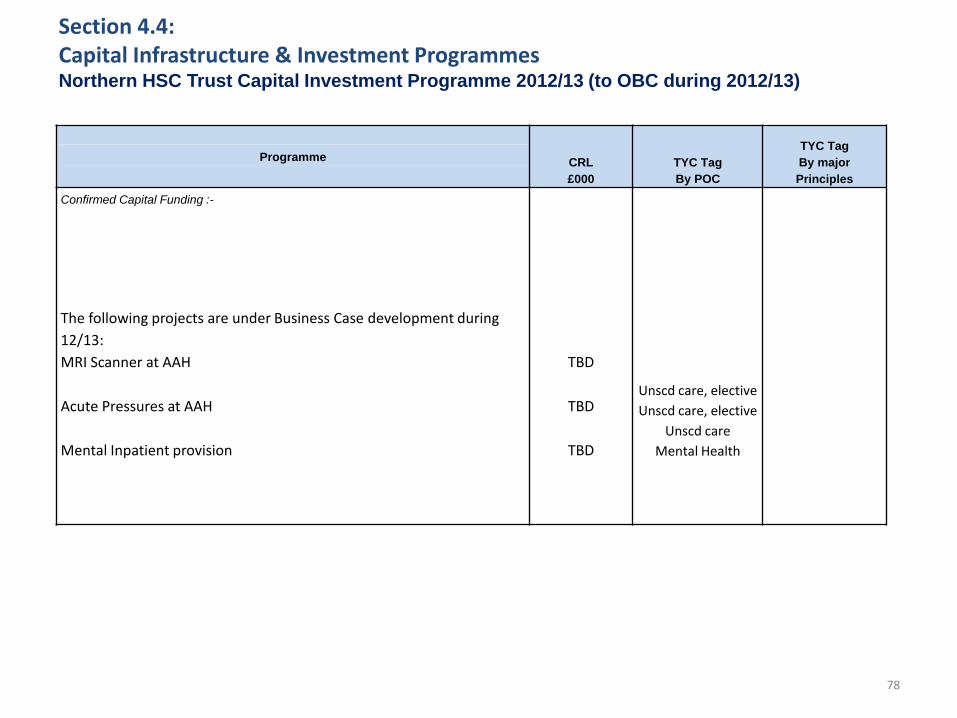
78
Section 4.4: Capital Infrastructure & Investment Programmes Northern HSC Trust Capital Investment Programme 2012/13 (to OBC during 2012/13)
CRL
£000
TYC Tag
By POC
TYC Tag
By major
Principles
Programme
Confirmed Capital Funding :-
The following projects are under Business Case development during
12/13:
MRI Scanner at AAH
Acute Pressures at AAH
Mental Inpatient provision
TBD
TBD
TBD
Unscd care, elective
Unscd care, elective
Unscd care
Mental Health
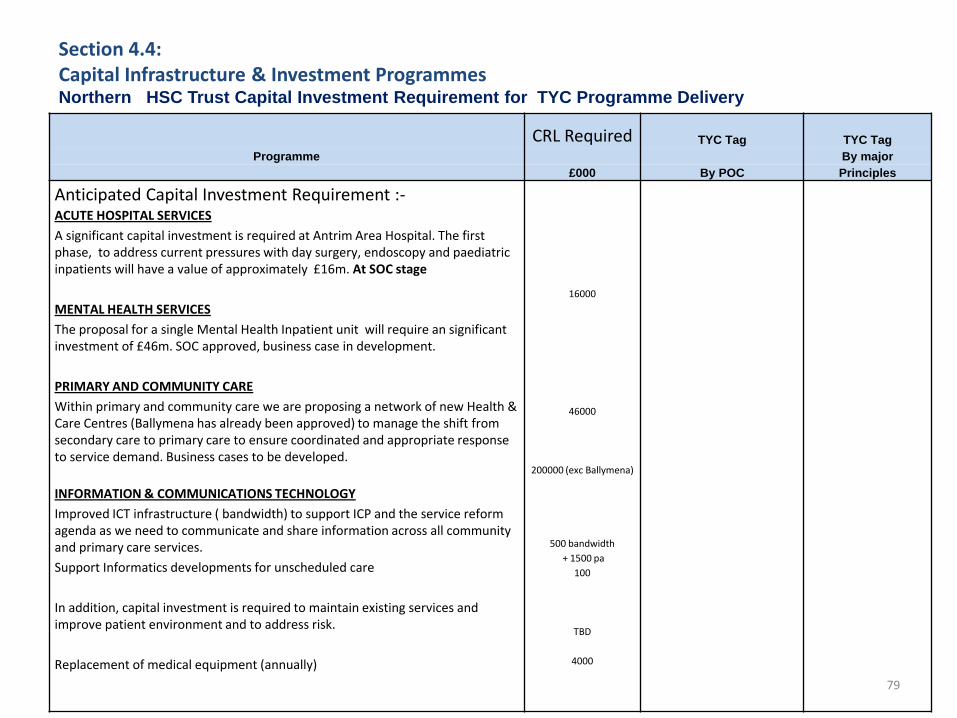
79
Section 4.4: Capital Infrastructure & Investment Programmes Northern HSC Trust Capital Investment Requirement for TYC Programme Delivery
CRL Required TYC Tag TYC Tag
Programme By major
£000 By POC Principles
Anticipated Capital Investment Requirement :-
ACUTE HOSPITAL SERVICES
A significant capital investment is required at Antrim Area Hospital. The first phase, to address current pressures with day surgery, endoscopy and paediatric inpatients will have a value of approximately £16m. At SOC stage
MENTAL HEALTH SERVICES
The proposal for a single Mental Health Inpatient unit will require an significant investment of £46m. SOC approved, business case in development.
PRIMARY AND COMMUNITY CARE
Within primary and community care we are proposing a network of new Health & Care Centres (Ballymena has already been approved) to manage the shift from secondary care to primary care to ensure coordinated and appropriate response to service demand. Business cases to be developed.
INFORMATION & COMMUNICATIONS TECHNOLOGY
Improved ICT infrastructure ( bandwidth) to support ICP and the service reform agenda as we need to communicate and share information across all community and primary care services.
Support Informatics developments for unscheduled care
In addition, capital investment is required to maintain existing services and improve patient environment and to address risk.
Replacement of medical equipment (annually)
16000
46000
200000 (exc Ballymena)
500 bandwidth
+ 1500 pa
100
TBD
4000
80
Our limited capital budget, which has also been impacted by the 2010 Spending Review settlement, has been prioritised to address a number of key estate risks, as well as facilitating elements of the transformational change which is planned within this plan. As we further develop the detail of the new service models, the need for additional capital and ICT resources will be better identified, particularly within community settings. In particular, the NHE recognises the need to further develop partnership working between the Trust, GPs and Integrated Care Partnerships to enhance community services, and improve the provision of primary care services. The precise nature of future capital and IT requirements will be determined and costed as the service models become clearer. In addition to DHSSPS capital funding for transformational change, DSD has committed £94m of additional capital funding, in partnership with NIHE, to support the health and social care sector to relocate patients and clients across mental health, learning & physical disability and older person services from institutional settings into community based accommodation across the region. This accommodation will be supported by integrated and responsive primary and community care services. This welcome investment will enable the Northern Local Commissioning Group Locality to achieve its vision for older people, people with mental health needs and those with learning and physical disabilities.
Section 4.4: Capital Infrastructure & Investment Programmes
81
Section 5
Workforce
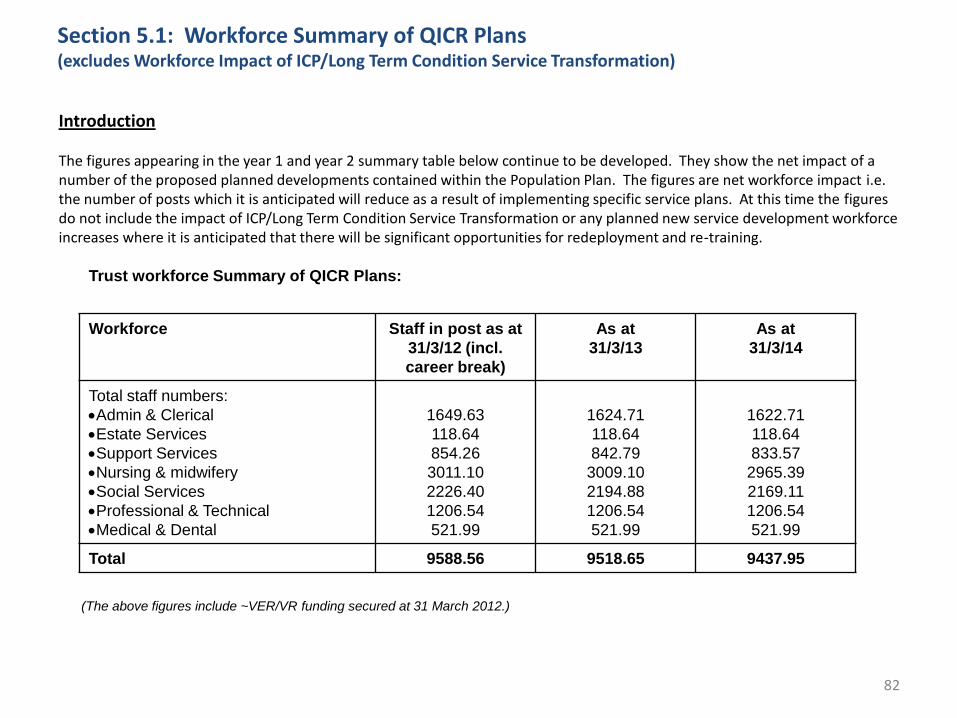
82
Section 5.1: Workforce Summary of QICR Plans (excludes Workforce Impact of ICP/Long Term Condition Service Transformation)
Introduction The figures appearing in the year 1 and year 2 summary table below continue to be developed. They show the net impact of a number of the proposed planned developments contained within the Population Plan. The figures are net workforce impact i.e. the number of posts which it is anticipated will reduce as a result of implementing specific service plans. At this time the figures do not include the impact of ICP/Long Term Condition Service Transformation or any planned new service development workforce increases where it is anticipated that there will be significant opportunities for redeployment and re-training.
Trust workforce Summary of QICR Plans:
Workforce Staff in post as at
31/3/12 (incl.
career break)
As at
31/3/13
As at
31/3/14
Total staff numbers:
Admin & Clerical
Estate Services
Support Services
Nursing & midwifery
Social Services
Professional & Technical
Medical & Dental
1649.63
118.64
854.26
3011.10
2226.40
1206.54
521.99
1624.71
118.64
842.79
3009.10
2194.88
1206.54
521.99
1622.71
118.64
833.57
2965.39
2169.11
1206.54
521.99
Total 9588.56 9518.65 9437.95
(The above figures include ~VER/VR funding secured at 31 March 2012.)
83
Section 5.1: Workforce Summary of QICR Plans (excludes Workforce Impact of ICP/Long Term Condition Service Transformation)
Workforce continued Organisation change impacting on staff will be managed utilising the Trust’s Management of Change - Human Resources Management Framework. This provides a framework to support strategic developments impacting on the workforce within the Northern Trust. It relates to all employees within the Trust affected by proposed changes. The framework ensures that the impact on staff is minimized and that service continuity is maintained and will assist in a smooth transition to new arrangements during periods of reorganisation. The fundamental aim of the framework is to help ensure a consistent approach to staff engagement and the management of change in employment patterns to maximise security of employment and minimize compulsory redundancies through the retraining and redeployment and so retention of staff. In addition to retraining and redeployment opportunities the Trust will avail of protected funding to allow a small number of organisational change affected staff to exit the Trust within the rules pertaining to Voluntary Redundancy and Voluntary Early Retirement.

84
Section 6
Enabling Implementation
85 85
Section 6: Enabling Transformation
In taking forward this Programme of Transformation, the joint LCG / Trust working arrangements have been formalised establishing a Programme Board and associated infrastructure to ensure effective delivery of the Programme and in particular:
•Implementation: Ensuring effective governance and programme management structures are in place to achieve sustainable delivery of the programme, including establishing new Integrated Care Partnerships
•Outcomes & Quality Measures: Measuring and demonstrating improvements as a result of change
•Building Capacity and Capability: ensuring individuals and then organisations as a whole have the skills and capacity to deliver a programme of change on a sustainable basis
•Engaging Others: Ensuring involvement of staff, service users and partner organisations in planning, delivering and monitoring achievements
•Programme Management •Given the joint delivery of this Programme through the LCG and Trust, the establishment of formal Programme Management arrangements is vital to create the joint working arrangements that will ensure the means to achieving the services changes set out, that there are clear targets and monitoring arrangements in place and that there is effective accountability for delivery and achievements. The following diagram illustrates how the workstreams and key projects will be taken forward by teams made up of Trust and LCG representatives, reporting through a jointly chaired Programme Board. A TYC Programme Database is established where each individual initiative is logged, along with expected timeframes and outputs. This forms the basis for regular project and Programme monitoring reports presented at the formal Programme Board meetings, and onward through the LCG and Trust Boards respectively, ensuring open and transparent reporting and accountability.
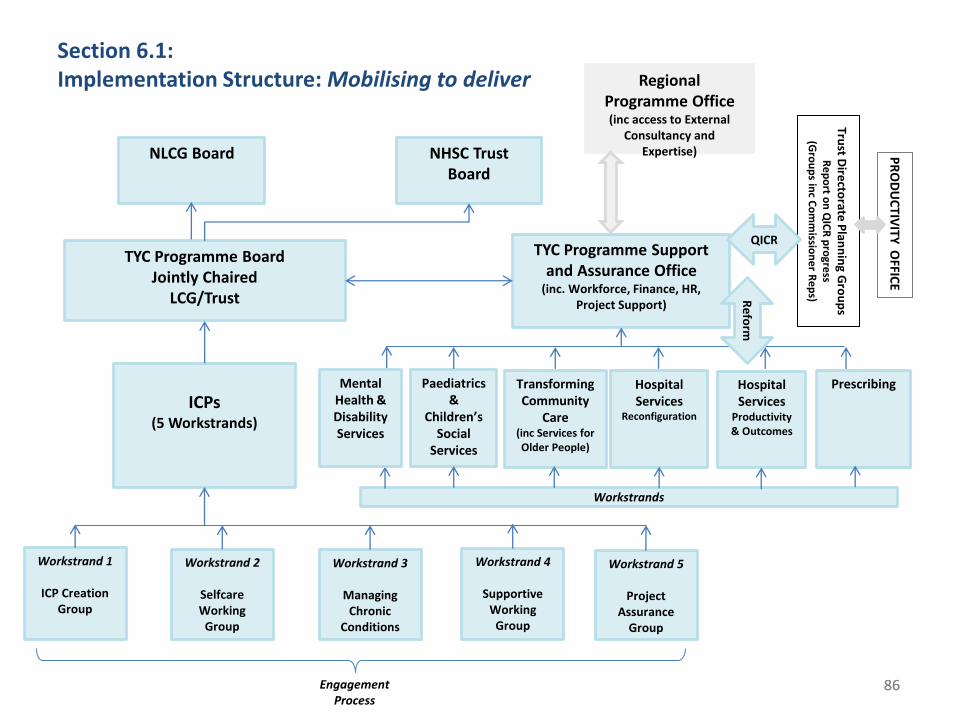
86 86
Section 6.1: Implementation Structure: Mobilising to deliver
TYC Programme Board Jointly Chaired
LCG/Trust
ICPs
(5 Workstrands)
TYC Programme Support and Assurance Office
(inc. Workforce, Finance, HR, Project Support)
Regional Programme Office (inc access to External
Consultancy and Expertise) NLCG Board NHSC Trust
Board
Transforming Community
Care (inc Services for Older People)
Paediatrics &
Children’s Social
Services
Hospital Services
Reconfiguration
Prescribing
Trust D
irecto
rate P
lann
ing G
rou
ps
Re
po
rt on
QIC
R p
rogre
ss (G
rou
ps in
c Co
mm
ission
er R
ep
s)
QICR
Re
form
PR
OD
UC
TIVITY
OFFIC
E
Workstrand 1
ICP Creation Group
Workstrand 2
Selfcare Working
Group
Workstrand 3
Managing Chronic
Conditions
Workstrand 4
Supportive Working
Group
Workstrand 5
Project Assurance
Group
Workstrands
Engagement Process
Hospital Services
Productivity & Outcomes
Mental Health & Disability Services
87
Section 6.2: Building our capacity & capability: Organisation Development Strategy
BUILDING CAPACITY TO DELIVER TRANSFORMATION
•The Northern Trust has developed an Organisation Development (OD) Strategy that provides the framework for the management and co-ordination of organisation and workforce development activities across the Trust ensuring that there is a direct link between the organisations corporate objectives and the skills and ability of the workforce to deliver those objectives within a challenging environment. This will be required to be extended to the joint working arrangements of the Trust and LCG.
•The key aim will be to ensure that all staff involved are equipped with the necessary clinical, social care, technical, managerial and personal skills to enable them to deliver safe and effective care and to contribute fully to the business of the organisations, including the pursuit of continuous improvement.
•An ongoing programme of development will seek to deliver a range of skills, training and techniques that include:
• Continuous Quality Improvement and Performance Management
• Communication and engagement
• Change Management
• Effective team working
• Leadership and management
•In addition to the ongoing commitment to enable staff through effective skills and knowledge training, the TYC Programme is committing additional Project Support staff for a two year period to ensure staff are supported in putting in place effective project management arrangements. Projects with clearly stated objectives, targets, timeframes, appropriate involvement, good communication arrangements and robust reporting are more likely to deliver positive outcomes.
•It is important to look to best practice and expertise outside the organisation and in this regard the TYC Programme will seek to have robust links with the Regional TYC Programme Office, for guidance and support, and onwards to expert panel members who can bring insight and challenge to the Northern Area Population Plans and implementation phase.
87

88
Section 6.3: Engaging Others: Communication and Engagement Strategy
COMMUNICATION AND ENGAGEMENT
• Consultation and engagement within the Trust is formally embedded within Trust structures and processes supported by the Communications and Engagement Strategy, Personal and Public Involvement Strategy and the Equality Scheme. These arrangements will continue to support the TYC Programme, under its joint LCG/Trust leadership, alongside LCG arrangements for involvement and engagement, particularly through its broad membership and ongoing communications and networks.
• The Trust Equality Scheme illustrates how formal consultation processes may be conducted and looks to regional and legislative arrangements for consultation particularly in cases of service change. This includes guidance around engagement through the planning stages as well as formal consultation and feedback arrangements. In agreement with the regional TYC Programme Office, formal consultation process will be taken forward under these arrangements.
• The LCG and TYC are committed to open and transparent involvement throughout the TYC programme. As well as each individual project or workstream detailing specific activities and timescales for engaging with relevant stakeholders, at a corporate level the TYC Programme Board will continue its efforts to engage with local District Councils, community / voluntary organisations, other independent partners as well as service users and communities.
• A series of 10 District Council based events have been undertaken as part of the Northern Area TYC Programme planning and development, meeting with local community/voluntary organisations around the issues, challenges and opportunities that lie ahead, these being shared with District Councils in a broad range discussion on the TYC programme of reform.
• The Trust has engaged with its already existing user panels on the key recommendations within TYC and will ensure their continued involvement during implementation
• A TYC Engagement Feedback Report detailing all the issues raised is available on the Trust’s website
• The TYC Programme Board will continue to focus on ensuring appropriate involvement and will table reports monthly on engagement and consultation activities.
88
89
Section 6.4: Risks - Identification, Impact and Management
MANAGING RISK
• The joint LCG/Trust Programme Board will manage the risks associated with the TYC Programme in accordance with the existing Trust based Risk Management Strategy and good practice relating to project management.
• Each individual Project or Workstream Lead will be responsible for engaging their team in identifying and managing the risks associated with their respective Workstream. Each will establish a project risk register identifying and rating risks, developing mitigating actions, setting timescales and expected outcomes , and will be responsible for reporting and escalating risks as necessary.
• Where there are common risks across all or many Workstreams, these will be identified and managed on a corporate basis utilising the TYC Programme Risk Register adopting the same approach to action taking and reporting.
• The TYC Risk Register will be presented to the Programme Board initially on a monthly basis, identifying the key risk, potential impact, and the actions being taken to mitigate the risk with outcomes.
• The Trust’s Corporate Risk Register for 2012/2013 will include a corporate risk associated with the risks to the successful implementation of the TYC programme
89
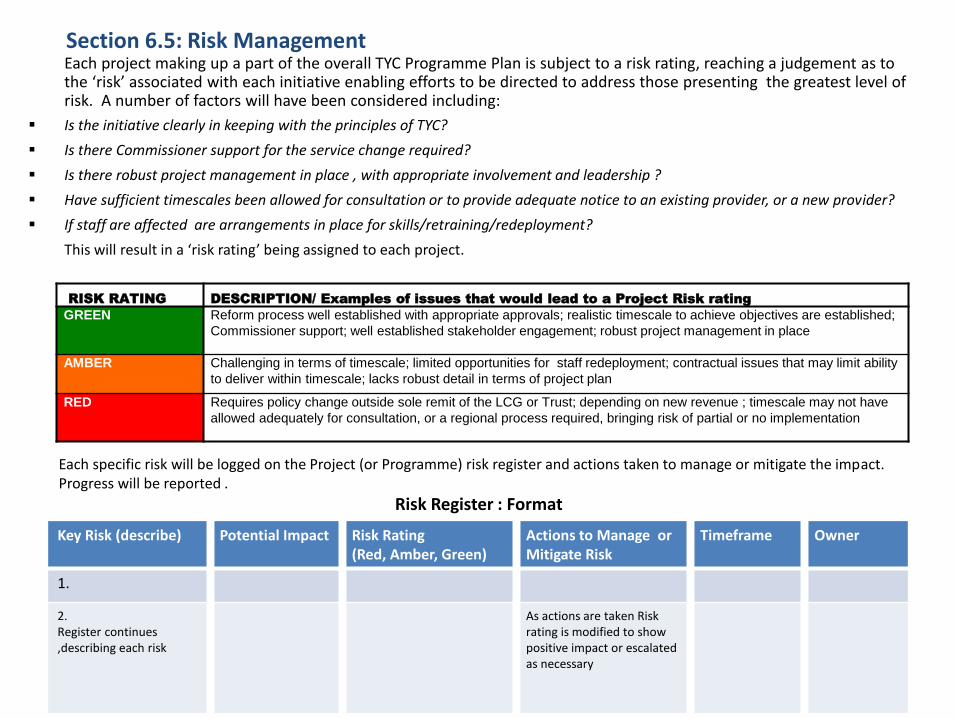
90
Section 6.5: Risk Management
90
Each project making up a part of the overall TYC Programme Plan is subject to a risk rating, reaching a judgement as to the ‘risk’ associated with each initiative enabling efforts to be directed to address those presenting the greatest level of risk. A number of factors will have been considered including:
Is the initiative clearly in keeping with the principles of TYC?
Is there Commissioner support for the service change required?
Is there robust project management in place , with appropriate involvement and leadership ?
Have sufficient timescales been allowed for consultation or to provide adequate notice to an existing provider, or a new provider?
If staff are affected are arrangements in place for skills/retraining/redeployment?
This will result in a ‘risk rating’ being assigned to each project.
RISK RATING DESCRIPTION/ Examples of issues that would lead to a Project Risk rating
GREEN Reform process well established with appropriate approvals; realistic timescale to achieve objectives are established;
Commissioner support; well established stakeholder engagement; robust project management in place
AMBER Challenging in terms of timescale; limited opportunities for staff redeployment; contractual issues that may limit ability
to deliver within timescale; lacks robust detail in terms of project plan
RED Requires policy change outside sole remit of the LCG or Trust; depending on new revenue ; timescale may not have
allowed adequately for consultation, or a regional process required, bringing risk of partial or no implementation
Key Risk (describe) Potential Impact Risk Rating (Red, Amber, Green)
Actions to Manage or Mitigate Risk
Timeframe Owner
1.
2. Register continues ,describing each risk
As actions are taken Risk rating is modified to show positive impact or escalated as necessary
Each specific risk will be logged on the Project (or Programme) risk register and actions taken to manage or mitigate the impact. Progress will be reported .
Risk Register : Format

Section 7 Glossary for the Population Plans
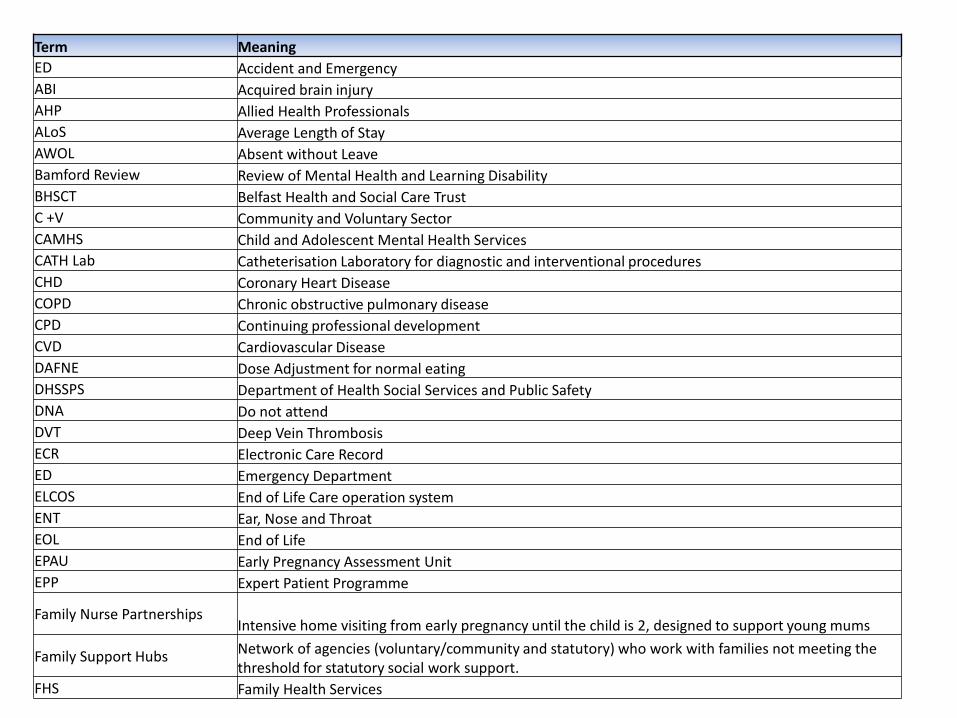
Term Meaning
ED Accident and Emergency
ABI Acquired brain injury
AHP Allied Health Professionals
ALoS Average Length of Stay
AWOL Absent without Leave
Bamford Review Review of Mental Health and Learning Disability
BHSCT Belfast Health and Social Care Trust
C +V Community and Voluntary Sector
CAMHS Child and Adolescent Mental Health Services
CATH Lab Catheterisation Laboratory for diagnostic and interventional procedures
CHD Coronary Heart Disease
COPD Chronic obstructive pulmonary disease
CPD Continuing professional development
CVD Cardiovascular Disease
DAFNE Dose Adjustment for normal eating
DHSSPS Department of Health Social Services and Public Safety
DNA Do not attend
DVT Deep Vein Thrombosis
ECR Electronic Care Record
ED Emergency Department
ELCOS End of Life Care operation system
ENT Ear, Nose and Throat
EOL End of Life
EPAU Early Pregnancy Assessment Unit
EPP Expert Patient Programme
Family Nurse Partnerships Intensive home visiting from early pregnancy until the child is 2, designed to support young mums
Family Support Hubs Network of agencies (voluntary/community and statutory) who work with families not meeting the threshold for statutory social work support.
FHS Family Health Services
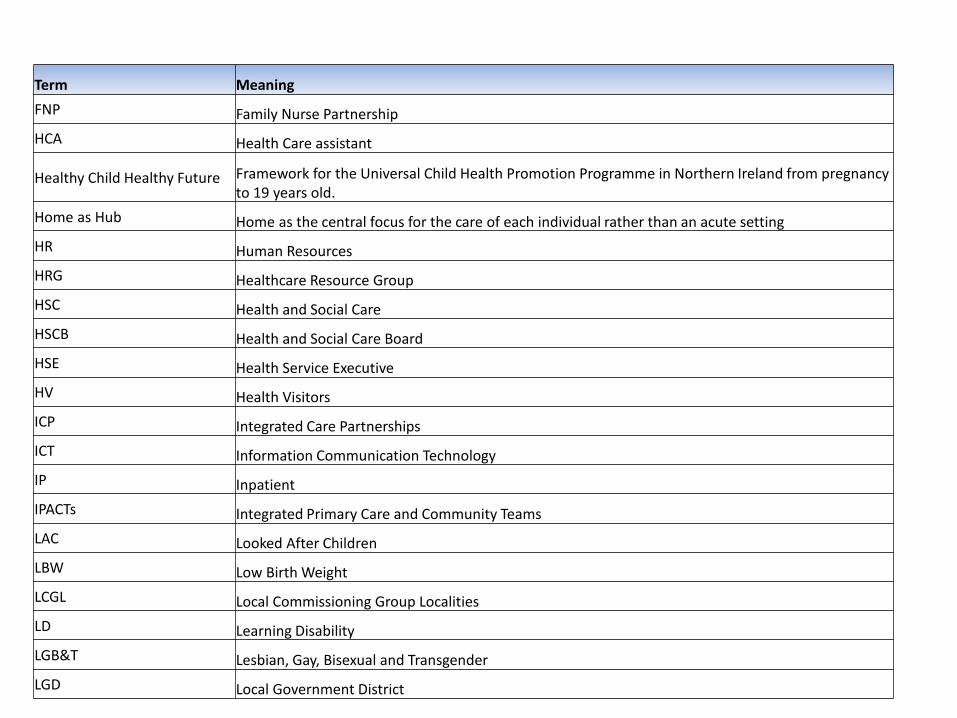
Term Meaning
FNP Family Nurse Partnership
HCA Health Care assistant
Healthy Child Healthy Future Framework for the Universal Child Health Promotion Programme in Northern Ireland from pregnancy to 19 years old.
Home as Hub Home as the central focus for the care of each individual rather than an acute setting
HR Human Resources
HRG Healthcare Resource Group
HSC Health and Social Care
HSCB Health and Social Care Board
HSE Health Service Executive
HV Health Visitors
ICP Integrated Care Partnerships
ICT Information Communication Technology
IP Inpatient
IPACTs Integrated Primary Care and Community Teams
LAC Looked After Children
LBW Low Birth Weight
LCGL Local Commissioning Group Localities
LD Learning Disability
LGB&T Lesbian, Gay, Bisexual and Transgender
LGD Local Government District
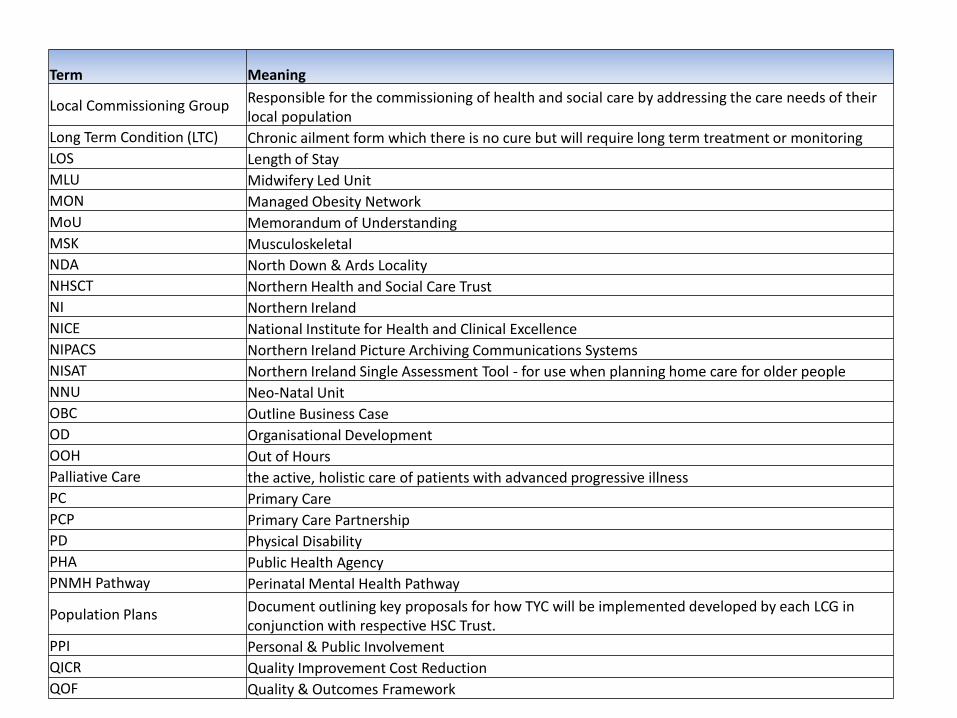
Term Meaning
Local Commissioning Group Responsible for the commissioning of health and social care by addressing the care needs of their local population
Long Term Condition (LTC) Chronic ailment form which there is no cure but will require long term treatment or monitoring
LOS Length of Stay
MLU Midwifery Led Unit
MON Managed Obesity Network
MoU Memorandum of Understanding
MSK Musculoskeletal
NDA North Down & Ards Locality
NHSCT Northern Health and Social Care Trust
NI Northern Ireland
NICE National Institute for Health and Clinical Excellence
NIPACS Northern Ireland Picture Archiving Communications Systems
NISAT Northern Ireland Single Assessment Tool - for use when planning home care for older people
NNU Neo-Natal Unit
OBC Outline Business Case
OD Organisational Development
OOH Out of Hours
Palliative Care the active, holistic care of patients with advanced progressive illness
PC Primary Care
PCP Primary Care Partnership
PD Physical Disability
PHA Public Health Agency
PNMH Pathway Perinatal Mental Health Pathway
Population Plans Document outlining key proposals for how TYC will be implemented developed by each LCG in conjunction with respective HSC Trust.
PPI Personal & Public Involvement
QICR Quality Improvement Cost Reduction
QOF Quality & Outcomes Framework
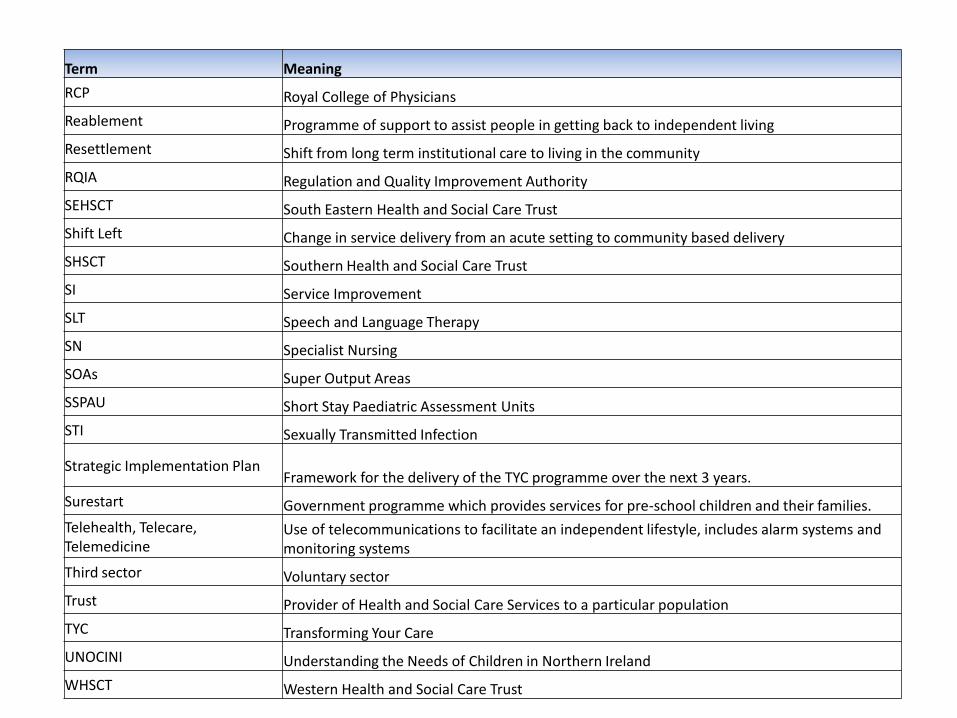
Term Meaning
RCP Royal College of Physicians
Reablement Programme of support to assist people in getting back to independent living
Resettlement Shift from long term institutional care to living in the community
RQIA Regulation and Quality Improvement Authority
SEHSCT South Eastern Health and Social Care Trust
Shift Left Change in service delivery from an acute setting to community based delivery
SHSCT Southern Health and Social Care Trust
SI Service Improvement
SLT Speech and Language Therapy
SN Specialist Nursing
SOAs Super Output Areas
SSPAU Short Stay Paediatric Assessment Units
STI Sexually Transmitted Infection
Strategic Implementation Plan Framework for the delivery of the TYC programme over the next 3 years.
Surestart Government programme which provides services for pre-school children and their families.
Telehealth, Telecare, Telemedicine
Use of telecommunications to facilitate an independent lifestyle, includes alarm systems and monitoring systems
Third sector Voluntary sector
Trust Provider of Health and Social Care Services to a particular population
TYC Transforming Your Care
UNOCINI Understanding the Needs of Children in Northern Ireland
WHSCT Western Health and Social Care Trust