Embed Size (px)
Citation preview

0
Trust Values
Infection Prevention and Control Annual Report 2012 - 2013

1
Trust Strategic Goals
Our strategic goals are: To deliver high quality person centered models of care, throughout the organisation. To be at the centre of an integrated network of partnerships to provide holistic approach to care. To engage with our communities to ensure we deliver the services they require. To be a dynamic organisation driven by innovation To be one of the most efficient providers

2
Contents
Introduction 4 Trust arrangements for Infection Prevention & Control 5 Compliance with the Health & Social Care Act 2008 7 Assurance framework 8 Annual Programme of Work 10 Legislative and Regulatory framework 10 Role of the IPCN 11 Surveillance and mandatory reporting 12 Meticillin resistant Staphylococcus aureus 13 Clostridium difficile infections (CDI) 14 Serious incidents 15 Escherichia coli 17 Antimicrobial prescribing 17 Hand Hygiene 18 Cleanliness 19 The Healthcare Environment 20 Seasonal Influenza Vaccine Campaign 21 Education and Training 23 Policy development and review 24 Quality Improvement 25 Mystery shopper programme 26 The Management of Medical Devices 27 Ambitions for 2013/14 28
3
Summary and Conclusions 29 References 30 Appendix I Infection Prevention and Control Annual Programmes of Work 32 Appendix II Role of the Director of Infection Prevention and Control (DIPC) 41

4
Introduction The Health and Social Care Act 2008 Code of Practice on the prevention and control of infections and related guidance (Department of Health 2010) requires the Trust to produce an annual report and release it publicly. This document produced on behalf of the Director of Infection Prevention and Control (DIPC) for North Staffordshire Combined Healthcare NHS Trust details the actions taken by the organisation to minimise the risk of infection for the period April 2012 to March 2013. This document serves to inform Trust Board members of the current position and to demonstrate that infection prevention and control is an integral part of the Trust’s assurance framework. The report outlines progress measured against the stated objectives detailed in the Trust’s Annual Programme of Work including responsibilities, timescales and priorities for action. The focus of this report is the work associated with prevention and the provision of a safe environment for patient care. Individual sections outline compliance with key documents such as the Health and Social Care Act 2008 Code of Practice, the Operating Framework for the NHS (Department of Health 2001) and the NHS Outcomes Framework (Department of Health 2011) including -
Surveillance
MRSA admission screening
Outbreak prevention and management
Quality improvement and audit
Cleanliness
Policy development and review
Specialist advice
Training and education The Directors of Infection Prevention and Control for the Staffordshire and Stoke-on-Trent Partnership Trust and the University Hospital of North Staffordshire produce annual reports for those organisations. Details can be found on their websites.

5
Trust Arrangements for Infection Prevention & Control
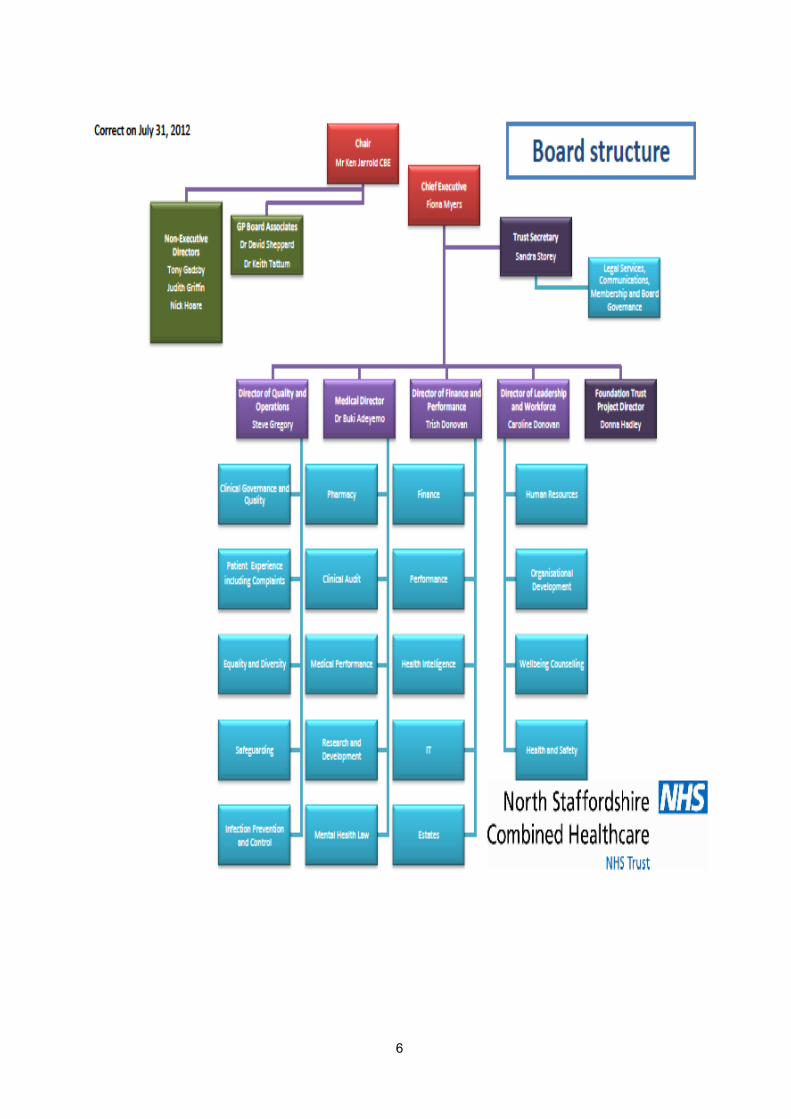
The Chief Executive (CE) has corporate responsibility for infection prevention and control and ensures that effective arrangements are in place throughout the Trust. The Chief Executive is Fiona Myers, who is also the Director of Infection Prevention and Control (DIPC).
Fiona Myers Chief Executive Steve Gregory Director of Quality and Operations The role of the Director of Infection Prevention & Control is to be directly accountable to members of the Trust Board and have the executive authority and responsibility for ensuring the implementation of strategies to prevent avoidable infection at all levels within the organisation. The role of DIPC transferred from Steve Gregory to Fiona Myers in December 2012. Infection Prevention and Control Specialist Nurse (IPCN) – The Trust employs one whole time Specialist Nurse who reports to the DIPC. The nominated Infection Prevention & Control Doctor (IPCD) is the University Hospital of North Staffordshire Consultant Microbiologist Dr Vasile Laza Stanca. Ward Managers and Service Leads work closely with the Trust IPCN to ensure that good infection prevention and control practice is applied by all. The Trust has a zero tolerance to avoidable infections and a collective responsibility which places a duty on all staff to minimise the risk of infection at all times. The Trust aims to care for patients in a safe environment protecting them from avoidable harm
6

7
Compliance with the Health and Social Care Act 2008 Code of Practice on the prevention and control of infections and related guidance
The Care Quality Commission (CQC) is the independent regulator established to ensure that providers of health and social care meet the required standards of quality and safety. The table below outlines the ten criteria against which a provider is assessed. The Trust is registered with the CQC and has declared full compliance with the criteria detailed below.
Criterion What the registered provider will need to demonstrate
1 Systems to manage and monitor the prevention and control of infection. These systems use risk assessments and consider how susceptible service users are and any risks that their environment and other users may pose to them.
2 Provide and maintain a clean and appropriate environment in managed premises that facilitates the prevention and control of infections.
3 Provide suitable accurate information on infections to service users and their visitors.
4 Provide suitable accurate information on infections to any person concerned with providing further support or nursing/ medical care in a timely fashion.
5 Ensure that people who have or develop an infection are identified promptly and receive the appropriate treatment and care to reduce the risk of passing on the infection to other people.
6 Ensure that all staff and those employed to provide care in all settings are fully involved in the process of preventing and controlling infection.
7 Provide or secure adequate isolation facilities.
8 Secure adequate access to laboratory support as appropriate.
9 Have and adhere to policies, designed for the individual’s care and provider organisations, that will help to prevent and control infections.
10 Ensure, so far as is reasonably practicable, that care workers are free of and are protected from exposure to infections that can be caught at work and that all staff are suitably educated in the prevention and control of infection associated with the provision of health and social care.

8
Assurance framework Infection Prevention and Control and the Management of Medical Devices Group The IPCMMDG meets four times a year and is chaired by the DIPC or deputy DIPC. Summary reports, briefing papers, policy and guidance documents, surveillance data, outbreaks, incidents and root cause analysis reports are presented to members of the Group for discussion, agreement and approval prior to submission to Quality and Governance Committee.
Membership of the Infection Prevention and Control and the Management of Medical Devices Group
Title Name
Director of Infection Prevention & Control (Chair) Steve Gregory & Fiona Myers
Deputy Director of Infection Prevention & Control
Kenny Laing
Infection Prevention & Control Specialist Nurse Sue Williams
Matron/s Jackie Wilshaw & Jackie Clowes
Support Services Advisor Anne Melville
Head of Estates Colin Plant
Senior Occupational Health Advisor Wendy Gould
Organisational safety representative Owen Myatt or Carol Sylvester
Senior Management Assistant, Harplands Joanne Orlando
Clinical Governance Lead Dianne Morris
Head of Pharmacy/Antimicrobial Pharmacist Louise Jackson/Rachel Tarbuck
Secretarial Support
Fay Smallman
Co-opted members as appropriate

9
Infection Prevention and Control and the Management of Medical Devices Summary of Attendance
Title Name 18.04.12 04.07.12 31.10.12 28.01.13
Director of Infection Prevention and Control (DIPC)
Steve Gregory or Fiona Myers
√ √ - -
Head of Nursing (Deputy DIPC appointed November 2012)
Kenny Laing
- - - √
IPCN Sue Williams
√ √ √ √
Head of Estates Colin Plant
√ - √ -
Matron Jackie Wilshaw/ Jackie Clowes
√ √ √ √
Support Services Advisor
Anne Melville √ √ √ √
Antimicrobial Pharmacist
Rachel Tarbuck √ √ √ √
Organisational safety representative
Owen Myatt/Carol Sylvester
√ √ √ √
Head of Service Transformation
Paul Devlin - √ - -
Lead Occupational Health Nurse
Wendy Gould/ Sarah Austin
- √ √ -
Senior Management Assistant
Joanne Orlando - √ - -
Mystery Shopper Programme Lead
Amanda Boyd √
IPC for Staffordshire Cluster Commissioning
Allison Heseltine √

10
Annual Programme The Health and Social Care Act 2008 Code of Practice requires the Trust to have an Infection Prevention and Control Annual Programme of Work which should:
Set clear objectives which meet the needs of the organisation and ensure the safety of service users
Identify priorities for action
Provide evidence that policies have been implemented to reduce infections
Report progress against the objectives in the DIPC’s annual report. The programme ensures that national objectives are met, assists operational performance and protects against variations in standards within and across the organisation. Members of the Infection Prevention and Control Group receive reports on progress of the Annual Programme, at each meeting, four times a year. The Annual Programme for the period of this report is detailed in Appendix 1.
Legislative and Regulatory Framework Department of Health 2010 The Health and Social Care Act 2008 Code of Practice on the prevention and control of infections and related guidance www.dh.gov.uk Department of Health 2010 The Operating Framework for the NHS in England 2012/2013 www.dh.gov.uk NHS Litigation Authority 2012 NHSLA Risk Management Standards for NHS Trusts providing Acute, Community or Mental Health and Learning Disability Services and Non- NHS Providers of NHS Care. www.nhsla.com/RiskManagement The Information Centre for health and social care 2011. Patient Environment Action Team Assessments 2012. www.ic.nhs.uk
11
The Role of the IPCN
Criterion 1.8 of the Health and Social Care Act 2008 Code of Practice requires the Trust to ensure that the Infection Prevention and Control infrastructure has an infection control nurse (IPCN). The Trust employs one whole time IPCN, based at the Harplands Hospital. The IPCN undertakes the core work associated with infection prevention and control including -
Surveillance
MRSA admission screening
Outbreak prevention and management
Quality improvement and audit
Cleanliness
Policy development and review
Training and education
Preparation of the annual programme
Preparation of the annual report
Support to the DIPC, senior managers, service leads and clinical teams
Seasonal influenza campaign lead
Operational work associated with the management of medical devices.
Specialist advice is provided to all staff within the Trust with a focus on clinical teams providing inpatient and community care. This may relate to -
The management of individual patients with an known or suspected infection
Infection risks to staff
Refurbishment, redevelopment and upgrade projects
Quality and performance reports
Relevance of safety alerts.
12
Surveillance and Mandatory Reporting
Criterion 4 and Criterion 8 of the Health and Social Care Act 2008 Code of Practice requires the Trust to provide suitable and accurate information on infection to any person concerned with providing further support or care in a timely fashion and to Secure adequate access to laboratory support as appropriate. Laboratory systems Clinical specimens generated by the Trust are managed by the University Hospital of North Staffordshire Pathology Laboratory. Reports are uploaded onto ICNet, a web based software system specific to the work of infection prevention and control teams. The purpose of surveillance Surveillance of laboratory reports allows the effective monitoring of specific and potentially pathogenic organisms. The subsequent review supports the analysis of trends and variances, the production of comparative data and the identification of emerging risks. The Consultant Microbiologists and the Trust Infection Prevention and Control Nurse undertake daily alert organism surveillance during periods of duty. Clinical teams are subsequently informed of the necessary actions required to minimise the risk of infection to the individual or other patients on the ward or unit.
Mandatory reporting The Department of Health requires the Trust to report Clostridium difficile infections (CDIs) Meticillin resistant Staphylococcus aureus (MRSA), Meticillin sensitive Staphylococcus aureus, and Escherichia coli blood stream infections (2011). National Objective For the period 2012/2013 the NHS in England was collectively asked to reduce the number of MRSA infections by a further twenty nine percent to reduce the number of bloodstream infections to 880 and the number of CDIs by seventeen percent from 19,754 to 16,100.

13
Meticillin resistant Staphylococcus aureus (MRSA) The Trust is pleased to announce that there have been no MRSA bacteraemias reported to the Trust IPCN since September 2007.
MRSA Admission screening
Department of Health guidance (2008) requires NHS provider Trusts to undertake MRSA screening of patients admitted to emergency and elective hospital inpatient beds. In mental health Trusts, swabs are taken from the nose, any wounds and indwelling devices if the individual meets the criteria detailed below -
Admitted following surgical procedures
Transferred from an Acute Trust
Intravenous drug user
Self harmer
Affected by chronic wounds such as leg ulcers and pressure sores
Living with long term indwelling devices such as enteral feeding tubes
Individuals with MRSA positive admission screening swabs, who are colonised with MRSA, are offered a five days decolonisation regime in accordance with national guidance and the Trust MRSA Policy. The Trust IPCN monitors implementation through weekly MRSA admission screening returns received from all hospital inpatient areas. The Performance Department receive monthly data summary reports, while members of the Trust Infection Prevention and Control Group receive updates at each meeting. MRSA admission screening and the subsequent decolonisation of individuals who are carriers of MRSA forms part of the Trust’s strategy to minimise the risk of infection.

14
Clostridium difficile infections (CDIs) The graph detailed below outlines the five year trend analysis for reported CDIs within the Trust.
During the period April 2012 to March 2013 one Clostridium difficile infection was reported at the Harplands Hospital. The case had been an inpatient for a few hours only when the symptoms of a CDI were noted and a stool sample obtained. In view of the time frame, this positive CDI reported for the organisation was clearly not acquired within the Trust and highlights the difficulties in attributing infections to organisations. The Trust is, therefore, pleased to announce that the organisation has sustained the same position for the equivalent period in the previous year.
0
2
4
6
8
10
12
14
2008-2009 2009-2010 2010-2011 2011-2012 2012-2013
13
6
2
1 1
Num
ber
of cases
Period
Clostridium difficile reports for the period April 2008- March 2013

15
Serious Incidents
The table below provides a summary of reported outbreaks of infection within inpatient units
Location Date Closed
Date Re-opened
Days Closed
Patients affected
Staff affected
Laboratory Reports
Florence House
Not closed - - 3 5 Norovirus
Ward 6 06.02.13 12.02.13 6 7 10 Norovirus
Ward 7 Harplands Hospital
11.02.13 20.02.13 9 10 7 Norovirus
Ward 5 Harplands Hospital
25.02.13 01.03.13 4 5 4 -
Total 19 25 26
Outbreaks of diarrhoea and vomiting affected three wards and one rehabilitation unit. The information and clinical picture reported by nursing teams resulted in all being managed as outbreaks of norovirus and subsequent laboratory reports supported this approach. All outbreaks of infection are managed in accordance with national guidance (HPA 2012), all are reported as serious incidents (SIs) and subject to a Root Cause Analysis (RCA) investigation. The aim is to determine the index case, the possible source of the outbreak and any contributory factors, while the subsequent action plan addresses the issues identified and lessons learned. Most patients are cared for in single rooms with hand washing facilities and this assists in implementing control measures during an outbreak of infection. The decision to isolate, however, is based on a balance of risk approach with consideration of any safety issues, particularly where the patient is confused, disorientated or in the acute phase of a mental illness. Patients with infections are therefore assessed individually and an appropriate plan implemented. The outbreak investigation for Wards, 5, 6 and 7 at the Harplands indicated that, against the advice from the IPCN, the movement of staff and equipment resulted in the spread of norovirus between the wards. Action plans have been developed to address this issue and will be revisited prior to the winter of 2013.
16
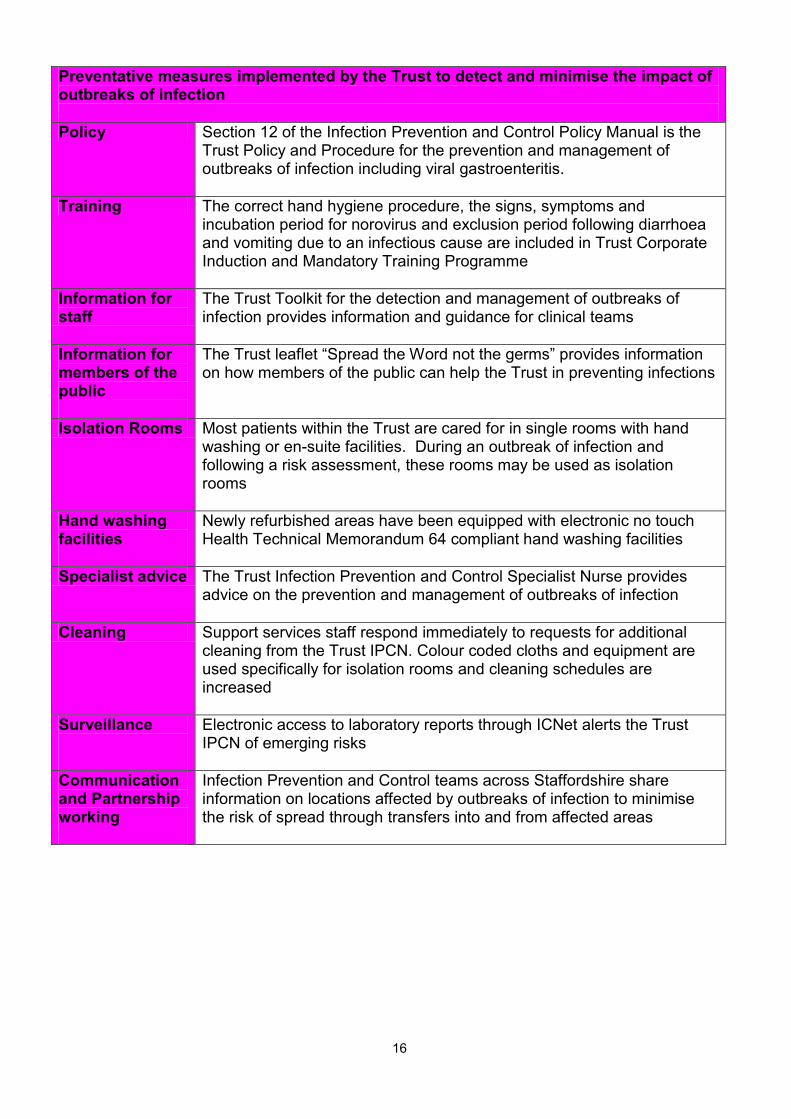
Preventative measures implemented by the Trust to detect and minimise the impact of outbreaks of infection
Policy Section 12 of the Infection Prevention and Control Policy Manual is the Trust Policy and Procedure for the prevention and management of outbreaks of infection including viral gastroenteritis.
Training The correct hand hygiene procedure, the signs, symptoms and incubation period for norovirus and exclusion period following diarrhoea and vomiting due to an infectious cause are included in Trust Corporate Induction and Mandatory Training Programme
Information for staff
The Trust Toolkit for the detection and management of outbreaks of infection provides information and guidance for clinical teams
Information for members of the public
The Trust leaflet “Spread the Word not the germs” provides information on how members of the public can help the Trust in preventing infections
Isolation Rooms Most patients within the Trust are cared for in single rooms with hand washing or en-suite facilities. During an outbreak of infection and following a risk assessment, these rooms may be used as isolation rooms
Hand washing facilities
Newly refurbished areas have been equipped with electronic no touch Health Technical Memorandum 64 compliant hand washing facilities
Specialist advice The Trust Infection Prevention and Control Specialist Nurse provides advice on the prevention and management of outbreaks of infection
Cleaning Support services staff respond immediately to requests for additional cleaning from the Trust IPCN. Colour coded cloths and equipment are used specifically for isolation rooms and cleaning schedules are increased
Surveillance
Electronic access to laboratory reports through ICNet alerts the Trust IPCN of emerging risks
Communication and Partnership working
Infection Prevention and Control teams across Staffordshire share information on locations affected by outbreaks of infection to minimise the risk of spread through transfers into and from affected areas
17
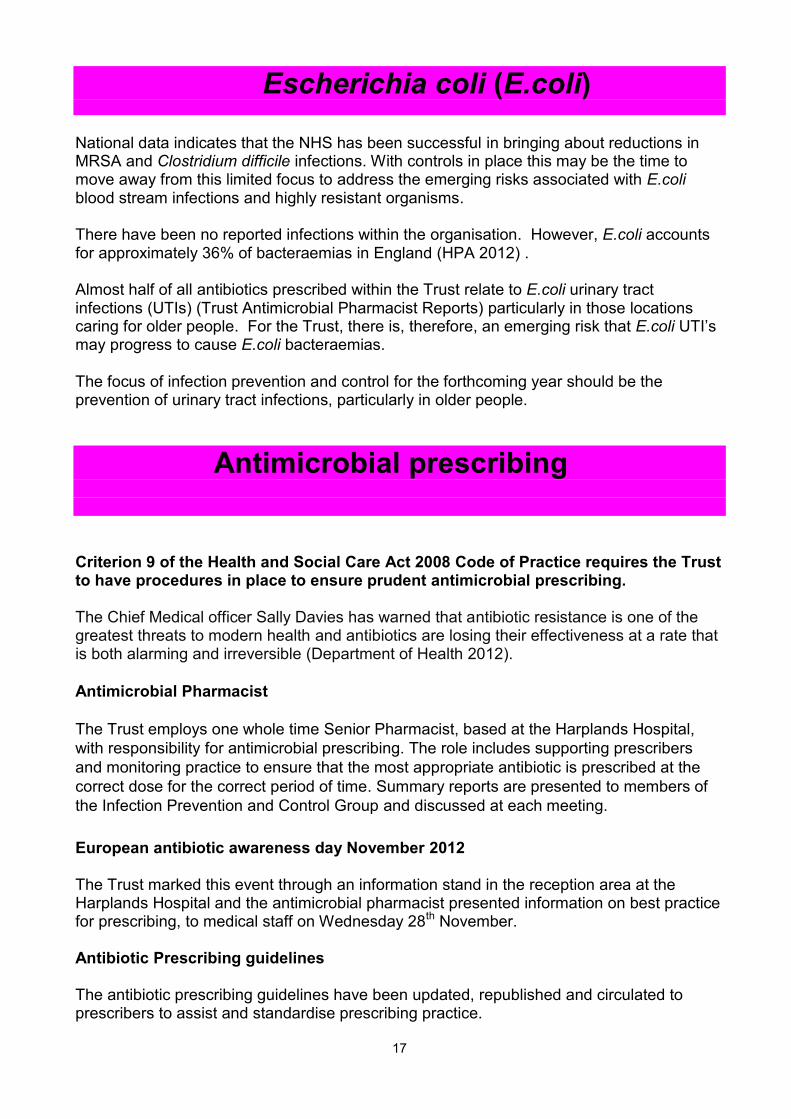
Escherichia coli (E.coli)
National data indicates that the NHS has been successful in bringing about reductions in MRSA and Clostridium difficile infections. With controls in place this may be the time to move away from this limited focus to address the emerging risks associated with E.coli blood stream infections and highly resistant organisms. There have been no reported infections within the organisation. However, E.coli accounts for approximately 36% of bacteraemias in England (HPA 2012) . Almost half of all antibiotics prescribed within the Trust relate to E.coli urinary tract infections (UTIs) (Trust Antimicrobial Pharmacist Reports) particularly in those locations caring for older people. For the Trust, there is, therefore, an emerging risk that E.coli UTI’s may progress to cause E.coli bacteraemias. The focus of infection prevention and control for the forthcoming year should be the prevention of urinary tract infections, particularly in older people.
Antimicrobial prescribing Criterion 9 of the Health and Social Care Act 2008 Code of Practice requires the Trust to have procedures in place to ensure prudent antimicrobial prescribing. The Chief Medical officer Sally Davies has warned that antibiotic resistance is one of the greatest threats to modern health and antibiotics are losing their effectiveness at a rate that is both alarming and irreversible (Department of Health 2012).
Antimicrobial Pharmacist
The Trust employs one whole time Senior Pharmacist, based at the Harplands Hospital,
with responsibility for antimicrobial prescribing. The role includes supporting prescribers
and monitoring practice to ensure that the most appropriate antibiotic is prescribed at the
correct dose for the correct period of time. Summary reports are presented to members of
the Infection Prevention and Control Group and discussed at each meeting.
European antibiotic awareness day November 2012 The Trust marked this event through an information stand in the reception area at the Harplands Hospital and the antimicrobial pharmacist presented information on best practice for prescribing, to medical staff on Wednesday 28th November. Antibiotic Prescribing guidelines The antibiotic prescribing guidelines have been updated, republished and circulated to prescribers to assist and standardise prescribing practice.

18
Hand Hygiene
Criterion 2 of the Health and Social Care Act 2008 Code of practice requires the Trust to ensure that there is adequate provision of suitable hand washing facilities and antimicrobial hand rubs.
Actions taken by the Trust to promote good hand hygiene practice
Hand Hygiene Training Hand hygiene training is included at Corporate Induction and all mandatory updates
Hand Hygiene equipment
In Trust premises, all staff have access to a hand wash basin, liquid soap and disposable paper towels in wall mounted dispensers
Refurbishment and upgrade projects
Clinical specification hand washing facilities are provided for staff in all refurbishment and upgrade projects
Alcohol hand rub
Clinical teams and staff supporting clinical teams all have personal dispensers of alcohol hand rub. This complements hand washing
Quality Improvement and audit
Compliance with national guidance and Trust policies are regularly audited
Cleanliness audits
The cleanliness of hand washing facilities is monitored during monthly cleanliness audits
Information
Posters and leaflets are available for staff and members of the public
Trust Policy The Trust has a Hand Hygiene Policy detailing the correct hand hygiene technique, the critical points for hand hygiene and the World Health Organisation Five Moments for Hand Hygiene
19
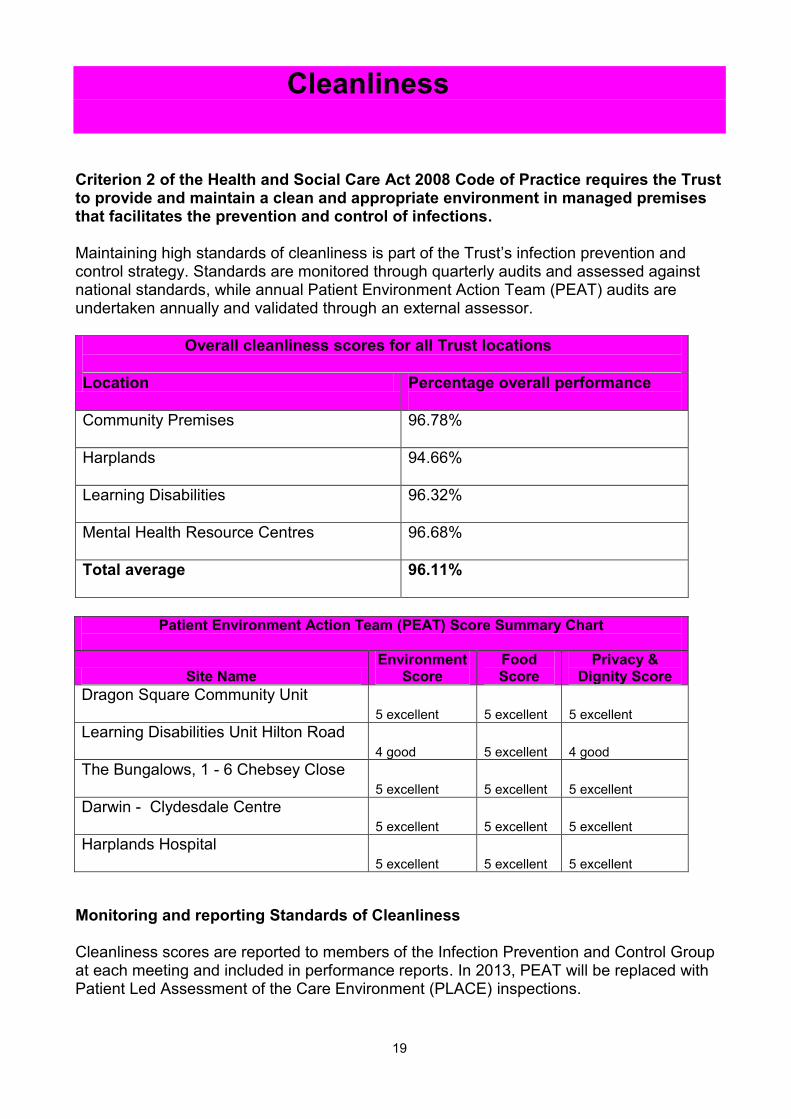
Cleanliness Criterion 2 of the Health and Social Care Act 2008 Code of Practice requires the Trust to provide and maintain a clean and appropriate environment in managed premises that facilitates the prevention and control of infections. Maintaining high standards of cleanliness is part of the Trust’s infection prevention and control strategy. Standards are monitored through quarterly audits and assessed against national standards, while annual Patient Environment Action Team (PEAT) audits are undertaken annually and validated through an external assessor.
Overall cleanliness scores for all Trust locations
Location Percentage overall performance
Community Premises
96.78%
Harplands
94.66%
Learning Disabilities
96.32%
Mental Health Resource Centres
96.68%
Total average 96.11%
Patient Environment Action Team (PEAT) Score Summary Chart
Site Name Environment
Score Food Score
Privacy & Dignity Score
Dragon Square Community Unit 5 excellent 5 excellent 5 excellent
Learning Disabilities Unit Hilton Road 4 good 5 excellent 4 good
The Bungalows, 1 - 6 Chebsey Close 5 excellent 5 excellent 5 excellent
Darwin - Clydesdale Centre 5 excellent 5 excellent 5 excellent
Harplands Hospital 5 excellent 5 excellent 5 excellent
Monitoring and reporting Standards of Cleanliness Cleanliness scores are reported to members of the Infection Prevention and Control Group at each meeting and included in performance reports. In 2013, PEAT will be replaced with Patient Led Assessment of the Care Environment (PLACE) inspections.
20
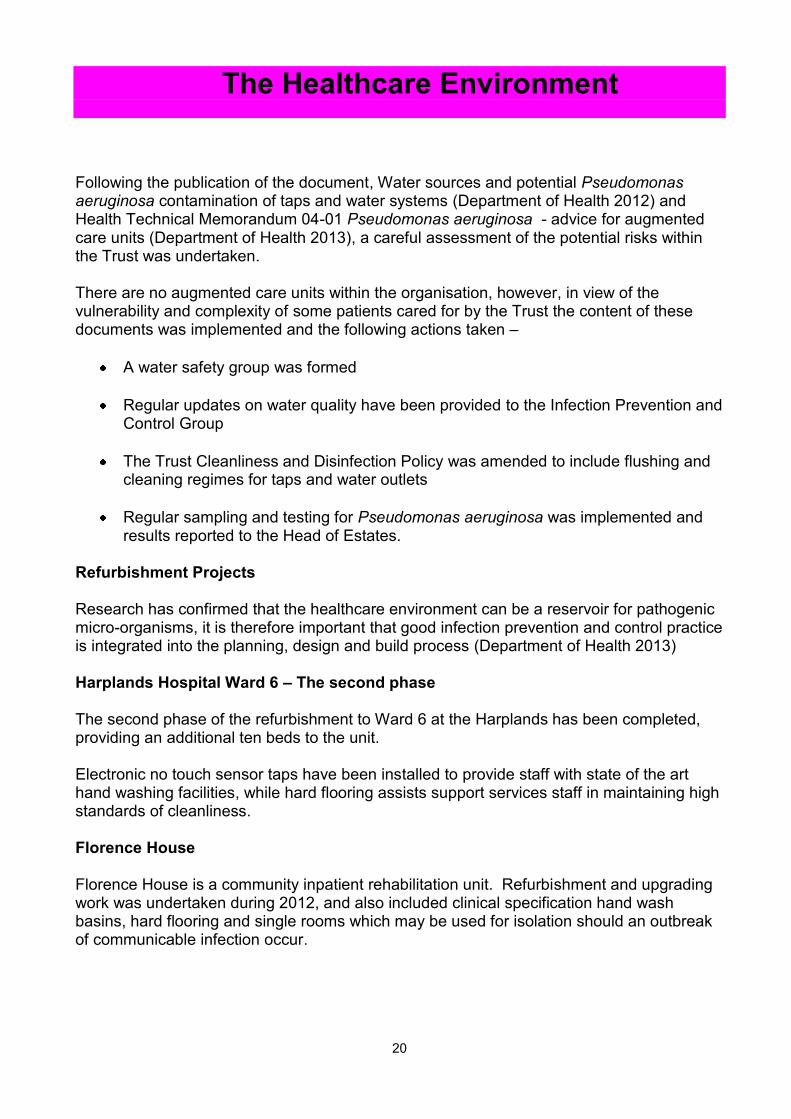
The Healthcare Environment Following the publication of the document, Water sources and potential Pseudomonas aeruginosa contamination of taps and water systems (Department of Health 2012) and Health Technical Memorandum 04-01 Pseudomonas aeruginosa - advice for augmented care units (Department of Health 2013), a careful assessment of the potential risks within the Trust was undertaken. There are no augmented care units within the organisation, however, in view of the vulnerability and complexity of some patients cared for by the Trust the content of these documents was implemented and the following actions taken –
A water safety group was formed
Regular updates on water quality have been provided to the Infection Prevention and Control Group
The Trust Cleanliness and Disinfection Policy was amended to include flushing and cleaning regimes for taps and water outlets
Regular sampling and testing for Pseudomonas aeruginosa was implemented and results reported to the Head of Estates.
Refurbishment Projects Research has confirmed that the healthcare environment can be a reservoir for pathogenic micro-organisms, it is therefore important that good infection prevention and control practice is integrated into the planning, design and build process (Department of Health 2013) Harplands Hospital Ward 6 – The second phase The second phase of the refurbishment to Ward 6 at the Harplands has been completed, providing an additional ten beds to the unit. Electronic no touch sensor taps have been installed to provide staff with state of the art hand washing facilities, while hard flooring assists support services staff in maintaining high standards of cleanliness. Florence House Florence House is a community inpatient rehabilitation unit. Refurbishment and upgrading work was undertaken during 2012, and also included clinical specification hand wash basins, hard flooring and single rooms which may be used for isolation should an outbreak of communicable infection occur.

21
Seasonal Influenza Vaccine Campaign Criterion 10 of the Health and Social Care Act 2008 Code of Practice requires the Trust to ensure that health and social care workers are free of and are protected from exposure to infections that can be caught at work.
During the 2012/13 winter period, influenza-like illnesses (ILI) remained low, however, the influenza virus is unstable and new strains are constantly emerging with the potential to have a devastating effect on individuals and service provision. Vaccination and immunisation is the most important way of protecting individuals from vaccine preventable infectious disease. Providing the seasonal influenza vaccine to healthcare workers benefits the individual and their families and helps to reduce the risk of transmitting the virus to vulnerable patients. Vaccinating staff is therefore part of the Trust’s strategy to prevent infections and is an integral part of winter planning and resilience. In January 2013 the Department of Health launched a “Catch it. Bin it. Kill it.” campaign (illustrated above) encouraging good practice to prevent the spread of the virus. In the Trust, this message was promoted in all mandatory training in addition to a poster, leaflet and electronic information campaign. Shropshire Community Health NHS Trust provide the Trust with Occupational Health Services from a centre in Fenton. In addition to the appointments system, a total of thirty one vaccination sessions were provided from a variety of locations across North Staffordshire, during the 2012/13 campaign.

22
Uptake of the seasonal influenza vaccine in the Trust The overall percentage uptake of the vaccine was 34%, this included
14 out of a total of 64 doctors
141 out of a total of 487 nursing staff
74 out of a total of 154 therapists. The Trust Human Resources Department report that there were 625 episodes of staff absences due to cold, cough, influenza, and respiratory illness, resulting in and equivalent of 451 full time equivalent days lost (email from HR Department) with a consequential impact upon service provision. Anecdotal evidence and verbal reports during mandatory training suggest that there are fears that the vaccine –
causes flu
is not sufficiently tested
is unnecessary if the individual has been vaccinated or had the illness in prior years Information provided by the communications team on the Staff Information Desk (SID), in Team Talk and News Round worked hard to dispel these myths. The Trust seasonal influenza vaccine campaign achieved some success, with uptake of the vaccine by frontline staff better than previous years.
0
5
10
15
20
25
30
35
2010-11 2011-12 2012-13
15
27
34
Perc
enta
ge U
pta
ke
Period
Uptake of the seasonal influenza vaccine by Trust staff
23
Education & Training Criterion 10 of the Health and Social Care Act 2008 Code of Practice requires the Trust to ensure that all staff are suitably educated in the prevention and control of infection. The principles and practice of the prevention and control of infection must be included in induction and training programmes for new staff and there must be appropriate on-going education for existing staff. The Trust includes infection prevention and control in Corporate induction and in the three- yearly mandatory update for all staff. A total of forty four “face to face” infection prevention and control training sessions were provided by the Trust IPCN. The interactive sessions which aim to foster a relationship with staff and promote best practice include –
An introduction to The Health and Social Care Act 2008 Code of Practice
Lines of accountability including the role of the Director of Infection Prevention and Control
Sharps awareness
Hand hygiene
Minimising the risks of outbreaks and exclusion periods for diarrhoea and vomiting
Topical issues such as seasonal influenza
Who to contact for advice and support. The Training Team report that the Trust overall percentage compliance with infection prevention and control mandatory training compares favourably with the equivalent period in previous years. 2012/2013 94% 2011/2012 89% 2010/2011 75% Feedback from face to face sessions is generally positive, however, releasing staff from clinical or service duties for training, remains an issue. In the forthcoming year staff will be offered the opportunity of infection prevention and control e-learning.
24
Policy Development and Review
Criterion 9 of the Health and Social Care Act 2008 Code of Practice requires the Trust to have and adhere to policies designed for the individual’s care and provider organisations that will help to prevent and control infections The following Trust policies reflect the requirements of the above Act:
No Policy Title
1 Sources of Advice
2 Infection Prevention & Control Operational Policy
3 Policy for minimising the risk of infection through standard precautions
4a Hand Hygiene Policy
4b Policy for the use of Personal Protective Equipment (PPE) for staff working within and supporting clinical teams
5 Isolation Policy
6 Notifiable Diseases
7 Policy for the prevention of occupational exposure to blood borne viruses and the management of inoculation or splash injuries
8 Cleaning and Disinfection Policy
9 Food Safety Policy
10 Management of Pulmonary Tuberculosis Policy
11 Meticillin resistant Staphylococcus aureus (MRSA) policy
12 Policy for The Prevention and Management of Outbreaks of Infection including viral gastroenteritis
13 Management of Linen and Laundry Policy
14 Specimen Management Policy
15 Policy for the prevention and management of Clostridium difficile infections (CDI)
All policies are available electronically on the Staff Information Desk (SID) in the Infection Prevention and Control folder. Each document is subject to a planned programme of

25
review every three years or prior to this date in response to changes in national guidance and published evidence based practice. All policies are up to date and the following polices have been revisited and updated during this period –
Cleaning and disinfection policy
Specimen Management Policy
Isolation Policy
Infection Prevention and Control Operational Policy. Guidance Documents The Trust Toolkit for the detection and Management of Outbreaks of Infection was updated and circulated to clinical teams in October 2012.
Quality Improvement
Criterion 2 of The Health and Social Care Act 2008 Code of Practice requires the Trust to ensure that a programme of audit is in place to ensure that key policies and practices are being implemented appropriately. Infection Prevention and Control standards are monitored through a structured programme of regular audit using nationally approved quality improvement tools endorsed by the Department of Health and the Infection Prevention Society (IPS 2012). Random unannounced visits and assessments are undertaken and a total of forty eight infection prevention and cleanliness audits were completed by the IPCN during the period of this report. A subsequent audit report details the standard required, the issue identified and the necessary action. The ward or unit manager is required to complete the report detailing the actions taken, the individual responsible and the timescale. Scores range from 77% - 100%. The lower scores are affected by compliance with the Trust Hand Hygiene Policy. Additional work is required to ensure that clinical staff do not wear nail polish, do not have long nails and do not wear jewellery while on duty.

26
Mystery shopper programme The Trust welcomed the opportunity of taking part in the Mystery Shopper pilot which included an infection prevention and control (IPC) component. The aim was to obtain feedback for the IPC Nurses on hand hygiene practice within North Staffordshire Combined Healthcare and the University Hospital of North Staffordshire. A cohort of nine mystery shoppers received basic infection prevention and control training during a formal session in December 2012. Eight nominees were included in the face to face meeting, while one completed a distance learning pack. The pilot commenced at the end of December 2012 and was completed on 31st March 2013 and a total of seven reports were generated. Outcomes from the feedback made reference to -
An infection prevention and control notice board in the Harplands Hospital reception
The importance of asking visitors to wash their hands
The need for signage directing members of the public of where to wash their hands.
The Mystery Shopper Programme has resulted in additional work being undertaken to make improvements at the Harplands. This unique opportunity has provided helpful feedback from service users.

27
The Management of Medical Devices The Health and Social Care Act 2008 Code of Practice requires the Trust to ensure that people who use services, work for, or visit the Trust should not be at risk or harmed from unsafe or unsuitable equipment. Outcome 11, Regulation 16 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 refers to the Safety, availability and suitability of equipment and requires providers to ensure that equipment is managed appropriately.
Trust systems to minimise risks associated with reusable medical devices
Policy Health and Safety Policy Folder 5.35 contains the Trust Policy and Guidance on the Management of Medical Devices
Equipment Managers All clinical teams have a nominated individual, called an Equipment Manager, who takes responsibility for the safe management of medical devices
Service Level Agreement with the University Hospital of North Staffordshire Clinical Technology Department
Ensures that all reusable mechanical and electrical items are serviced and tested to the appropriate safety standards. Where manufacturer’s instructions require, equipment is subject to a planned preventative maintenance programme
Head of Estates
Ensures that Trust engineers or external companies undertake maintenance and testing of clinical equipment such as hydraulic beds and hoists
Organisational Safety Department The Trust cascades safety bulletins and alerts to clinical teams to ensure the organisation responds to nationally reported issues
Infection Prevention and Control Specialist Nurse and the Senior Management Assistant
Unannounced and planned audits are undertaken to ensure that reusable medical devices have been tested and maintained as required.
Senior Management of Assistant (SMA) The Senior Management Assistant at the Harplands has a remit to centrally control and issue the stock of consumables for some key items of equipment

28
Ambitions for 2013/14 The year-end analysis and review provides an opportunity to celebrate positive outcomes and to agree the Trust’s ambitions for the forthcoming year. The Trust aims to focus on further success in the following areas:
Prevent urinary tract infections.
Promote prudent antibiotic prescribing
Increase compliance with mandatory training to 95%
Improve uptake of the seasonal influenza vaccine by frontline staff
Monitor and minimise the risk from emerging resistant micro-organisms.

29
Summary & Conclusion
People with a diagnosis of severe and enduring mental illness (SMI) such as schizophrenia and bipolar disorder are at increased risk of physical illness including infections (Department of Health 2006). The Trust, therefore, has a duty to protect vulnerable patients from avoidable infections through robust systems and procedures, particularly in inpatient locations. 2012/13 was a difficult and challenging year for everyone within the Trust with changes to structures, services and increasing cost pressures. Clinical teams, however, must be commended for their hard work in preventing infections and continuing to make some progress. The investigation into Mid Staffordshire NHS Foundation Trust considered the control of infection and viewed it as an important indicator of the quality of care. The Trust has noted the detail of the Francis inquiry and will carry forward the learning points into 2013/14. For the period of this report, the DIPC is pleased to announce that the organisation has sustained the position for the equivalent period in the previous year with one Clostridium difficile infection and no MRSA infections. Cleanliness scores are excellent or good, a reflection of the hard work and dedication of support services staff at the Harplands Hospital and community locations. The Trust’s commitment to learning is reflected in the number of training sessions provided at Corporate Induction and through the Mandatory Training programme, however, additional actions are required to achieve the target of 95% compliance. Standards are monitored through an on-going programme of audit and quality improvement undertaken by clinical teams and the Trust Infection Prevention and Control Nurse. Uptake of the seasonal influenza vaccine by Trust staff has increased to 34%, however, our ambition is to continue to make improvements in uptake by frontline staff. Outbreaks of infection affected three wards at the Harplands Hospital with evidence of spread between the wards. This is unacceptable and additional measures will be implemented prior to the winter of 2013. The Trust has noted the messages in the Chief Medical Officer’s Report (2012). There is a need for greater vigilance around the emerging risk from E.coli, highly resistant organisms and the necessity for prudent antimicrobial prescribing. The information provided in this report summarises the planned and responsive actions taken to minimise the risk of infection. This document serves to inform and provide assurance to members of the Board that the actions support the Trust’s aim to care for patients in a safe environment, protecting them from avoidable harm. .
30
References
Care Quality Commission 2012 The essential standards of quality and safety. www.cqc.org.uk Department of Health 2006 Choosing Health: Supporting the physical health needs of people with severe mental illness www.dh.gov.uk/publications Department of Health 2008 Dear colleague letter Gateway reference 10324 MRSA screening operational guidance www.dh.gov.uk Department of Health 2009 Clostridium difficile infection: How to deal with the problem. www.dh.gov.uk/publications Department of Health 2010 The Health and Social Care Act 2008 Code of Practice on the prevention and control of infections and related guidance. www.dh.gov.uk/publications
Department of Health 2011 The Operating Framework for the NHS in England 2012/13 www.dh.gov.uk Department of Health 2011 Dear Colleague letter. Gateway reference 15353. Extension to mandatory surveillance to Meticilllin Sensitive Staphylococcus aureus (MSSA) and update Healthcare Associated Infections clinical guidance ( “HCAI Compendium”) www.dh.gov.uk Department of Health 2011 The NHS Outcomes Framework 2012/2013 www.dh.gov.uk Department of Health 2011 Dear Colleague letter. Gateway reference 15980 Extension of mandatory surveillance to E.coli bloodstream infections – June 2011. www.dh.gov/uk Department of Health 2012 Web page update on Tuesday 8th May. www.dh.gov/uk Department of Health 2012 Water Sources and potential Pseudomonas aeruginosa contamination of taps and water systems. Advice for augmented care units. www.dh.gov/uk Department of Health 2013 Water Systems Health Technical Memorandum 04 – 01 Addendum. Pseudomonas aeruginosa – advice for augmented care units
Department of Health 2013 Health Building Note 00 - 09 : Infection Control in the Built Environment www.dh.gov/uk
Hawker J, Begg N, Blair I, Reintjes R, Weinburg J. 2005 Communicable Disease Control Handbook. Blackwell Publishing
Health Protection Agency 2012 English National Point Prevalence Survey on Healthcare Associated infection www.hpa,org.uk Infection Prevention Society 2012 Clinical Practice Rapid Improvement Tools and Care Setting Process Improvement Tools www.ips.uk.net/
31
National Patient Safety Agency 2007 The national specifications for cleanliness in the NHS: a framework for setting and measuring performance outcomes. npsa.nhs.uk National Patient Safety Agency 2009 The revised healthcare Cleaning Manual npsa.nhs.uk NHS Litigation Authority 2012 NHSLA Risk Management Standards for NHS Trusts providing Acute, Community or Mental Health and Learning Disability Services. www.nshla.com/RiskManagement Norovirus Working Party 2012 Guidelines for the management of norovirus outbreaks in acute and community health and social care settings. Health Protection Agency; British Infection Association; Healthcare Infection Society; Infection Prevention Society; National Concern for Healthcare Infections; NHS Confederation www.hpa.org.uk

Appendix I
Infection Prevention & Control and the Management of Medical Devices Annual Programme of Work for the period April 2012 – March 2013
The aim of this document is to set objectives and identify priorities for action through the Trust’s zero tolerance approach to avoidable infections and to minimise the risk of harm from medical devices. The stated actions aim to sustain and strengthen the Trust’s position in achieving compliance with The Health & Social Care Act 2008 Code of Practice on the prevention and control of infections and related guidance (Department of Health 2010) and other key national documents. The programme aims to capture the essential components of the infection prevention and control service including – surveillance, policy development and review, outbreak prevention and management, audit, education and training, specialist advice including promoting compliance with regulation, legislation, guidance and evidence based practice.
Objective Actions Person/s Responsible Time scale & Priority
DIPC – Director of Infection Prevention & Control IPCN – Infection Prevention and Control Specialist Nurse, Sue Williams
Criterion 1 Systems to manage and monitor the prevention and control of infection
Assurance framework Quality and Governance Committee and the Board will receive regular reports and presentations (quarterly as a minimum) from the Director of Infection Prevention and Control The DIPC will ensure the Board agree and approve the –
DIPC DIPC
Quarters 1-4 Quarter 1

Annual programme of work
Annual report
Policy, procedure and guidance documents
PEAT and cleanliness scores
The DIPC will ensure that the Board is made aware of –
Emerging issues with the potential to impact upon patient safety and the delivery of clinical services
Unforeseen issues impacting upon progress of the annual programme
Ensure that progress of the annual programme is monitored by the Infection Prevention & Control Group and any identified or emerging issues affecting the programme are reported to the committee Ensure that the Infection Prevention and Control and the Management of Medical Devices Group, chaired by the DIPC meet four times a year
Support Services DIPC IPCN DIPC
Quarter 2 Review date At each meeting
Make a suitable and sufficient assessment of the risks of infection and take action to minimise the risk.
Undertake alert organism surveillance. Using ICNet, review laboratory reports during periods of duty and provide specialist advice to clinical teams on the management of individual patients Inform the DIPC of all MRSA, MSSA, E.coli bacteraemias and C.difficile infection and initiate the root cause analysis investigation process.
IPCN IPCN
Daily during normal working hours On receipt of the lab. report
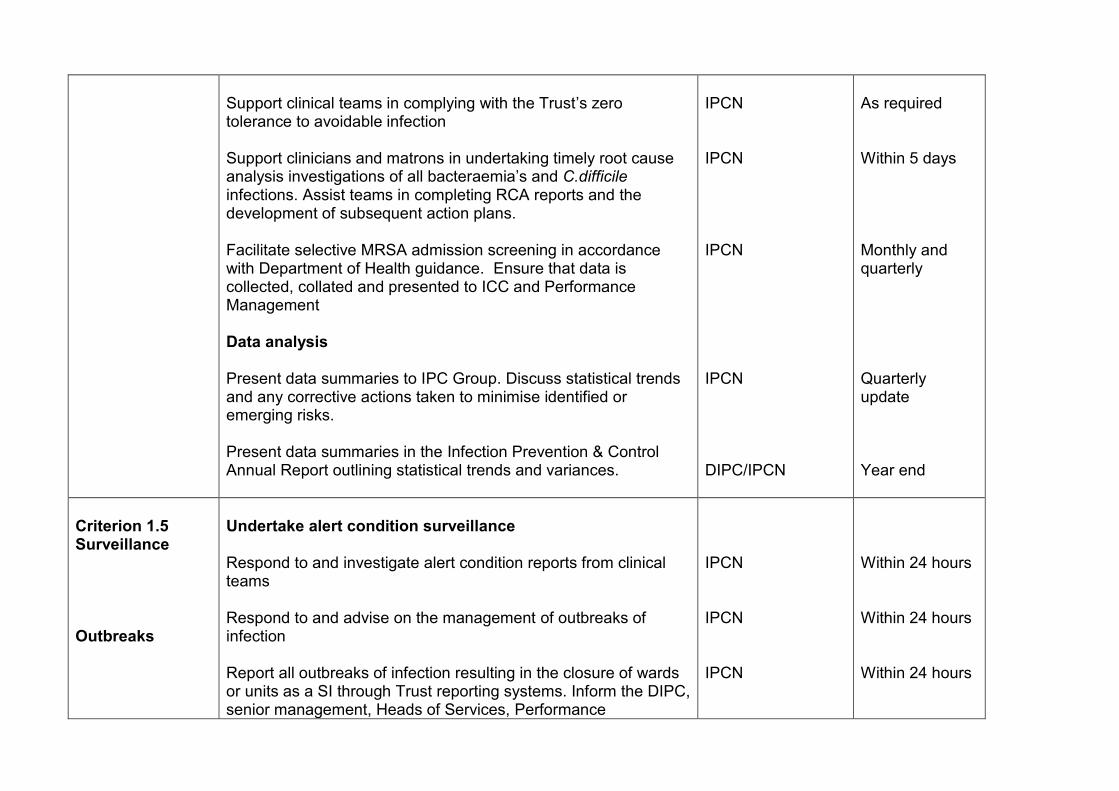
Support clinical teams in complying with the Trust’s zero tolerance to avoidable infection Support clinicians and matrons in undertaking timely root cause analysis investigations of all bacteraemia’s and C.difficile infections. Assist teams in completing RCA reports and the development of subsequent action plans. Facilitate selective MRSA admission screening in accordance with Department of Health guidance. Ensure that data is collected, collated and presented to ICC and Performance Management Data analysis Present data summaries to IPC Group. Discuss statistical trends and any corrective actions taken to minimise identified or emerging risks. Present data summaries in the Infection Prevention & Control Annual Report outlining statistical trends and variances.
IPCN IPCN IPCN IPCN DIPC/IPCN
As required Within 5 days Monthly and quarterly Quarterly update Year end
Criterion 1.5 Surveillance Outbreaks
Undertake alert condition surveillance Respond to and investigate alert condition reports from clinical teams Respond to and advise on the management of outbreaks of infection Report all outbreaks of infection resulting in the closure of wards or units as a SI through Trust reporting systems. Inform the DIPC, senior management, Heads of Services, Performance
IPCN IPCN IPCN
Within 24 hours Within 24 hours Within 24 hours
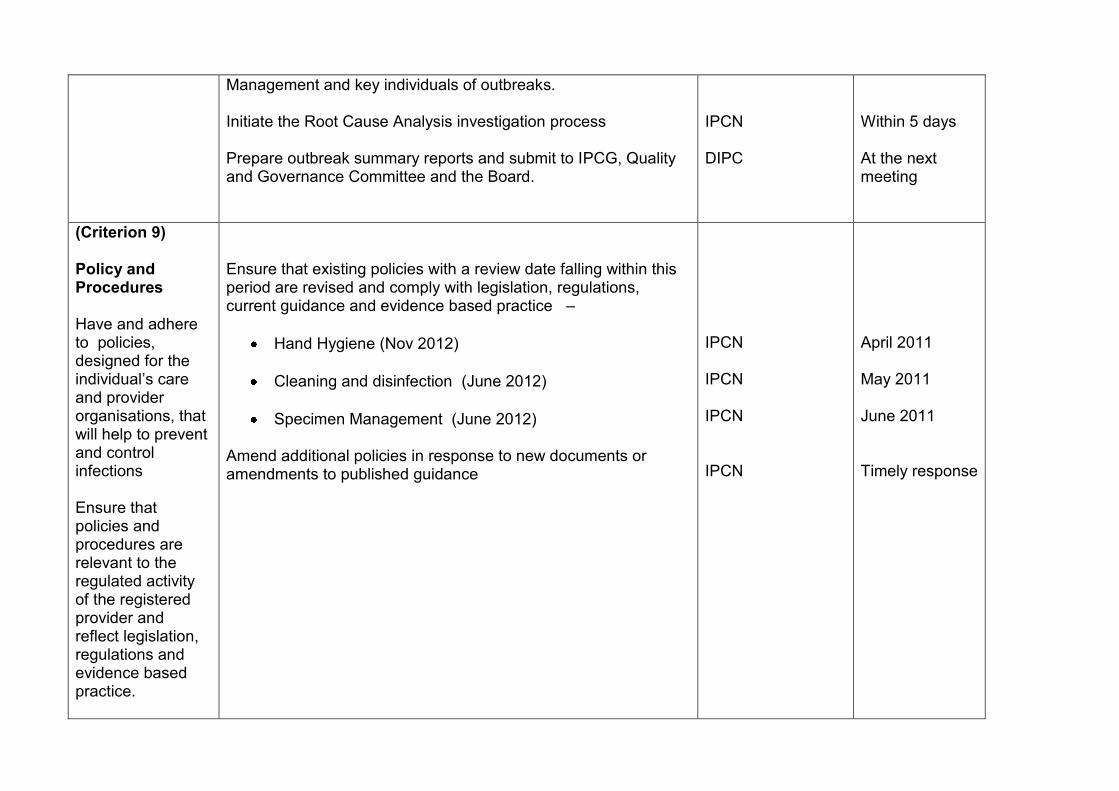
Management and key individuals of outbreaks. Initiate the Root Cause Analysis investigation process Prepare outbreak summary reports and submit to IPCG, Quality and Governance Committee and the Board.
IPCN DIPC
Within 5 days At the next meeting
(Criterion 9) Policy and Procedures Have and adhere to policies, designed for the individual’s care and provider organisations, that will help to prevent and control infections Ensure that policies and procedures are relevant to the regulated activity of the registered provider and reflect legislation, regulations and evidence based practice.
Ensure that existing policies with a review date falling within this period are revised and comply with legislation, regulations, current guidance and evidence based practice –
Hand Hygiene (Nov 2012)
Cleaning and disinfection (June 2012)
Specimen Management (June 2012)
Amend additional policies in response to new documents or amendments to published guidance
IPCN IPCN IPCN IPCN
April 2011 May 2011 June 2011 Timely response

Education and training: (Criterion 10) Ensure that all staff are suitably education in the prevention and control of infection
Liaise with the Learning Centre, Service Leads and matrons to ensure that all staff are suitably educated in the prevention and control of infection. Provide an IPC contribution to the following programmes -
Corporate induction
Mandatory training days
Scheduled programme of updates
Provide a bi-annual update for the Equipment Managers Review e-learning packages and liaise with the Training Manager to assess the feasibility of implementing infection prevention and control e-learning within the Trust
IPCN/Training team
Timescale in accordance with documented programmes
(Criterion 1) Audit Ensure that key policies and practices are being implemented through a programme of audit
The IPCN will support service leads, matrons and ward managers in delivering the annual programme of audit using nationally approved audit tools. The IPCN will undertake a programme of random audits in clinical areas The IPCG will receive regular progress reports on audits and subsequent action plans Incident reporting forms and the effectiveness of subsequent action plans will be reviewed
IPCN/matrons/ service leads Service leads /Matrons/IPCN Risk manager/IPCN IPCN
Quarterly Quarterly Quarterly Documented schedule

(Criterion 10) Healthcare workers Ensure, so far as is reasonably practicable that staff are free of and are protected from exposure to infection that can be caught at work
Liaise with and support the Occupational Health Department in protecting healthcare workers from infection through – The review and follow up of inoculation or splash injuries Work with partner organisations to ensure that the Trust has systems and procedures which minimise the risk from emerging and resistant organisms including influenza The planning and delivery of the seasonal influenza immunisation programme
IPCN/OH DIPC/IPCN IPCN /Lead Occupational Health Nurse
August – January As above
Performance management : To promote compliance with legislation, regulations and guidance.
Ensure that monthly data summaries, incidents and outbreaks are forwarded to the Performance Team Ensure that the Performance Team receive appropriate information to support on-going registration with the Care Quality Commission and NHSLA assessments
IPCN IPCN
Monthly As required
Specialist advice Duty to provide specialist advice and information: To provide information and specialist advice on the prevention and control of
Timely and responsive specialist advice will be provided to staff working within and on behalf of the Trust including -
DIPC/Deputy DIPC
Clinical teams
Service Leads, matrons and managers
Estates Agency
IPCN
As required

infection to staff and members of the public
Patients, relatives or members of the public
Representation at key committees
Representation will be provided at key committees detailed below-
Infection prevention and control and the management of medical devices group
Quality & Governance Committee
Risk Review Group
New Build and refurbishment project groups
Education and Learning Group (ELG)
Weekly health economy surveillance meeting
Flu preparedness group
Water Quality Group
IPCN/DIPC DIPC IPCN IPCN IPCN IPCN IPCN IPCN
In accordance with agreed dates/schedules
Provide and maintain a clean and appropriate environment (Criterion 2)
Actively contribute to the following programmes -
The management of re-usable medical devices
Updating Equipment Managers
Liaising with University Hospital of North Staffordshire Clinical Technology and Supplies Departments
IPCN IPCN
Bi - annual As required
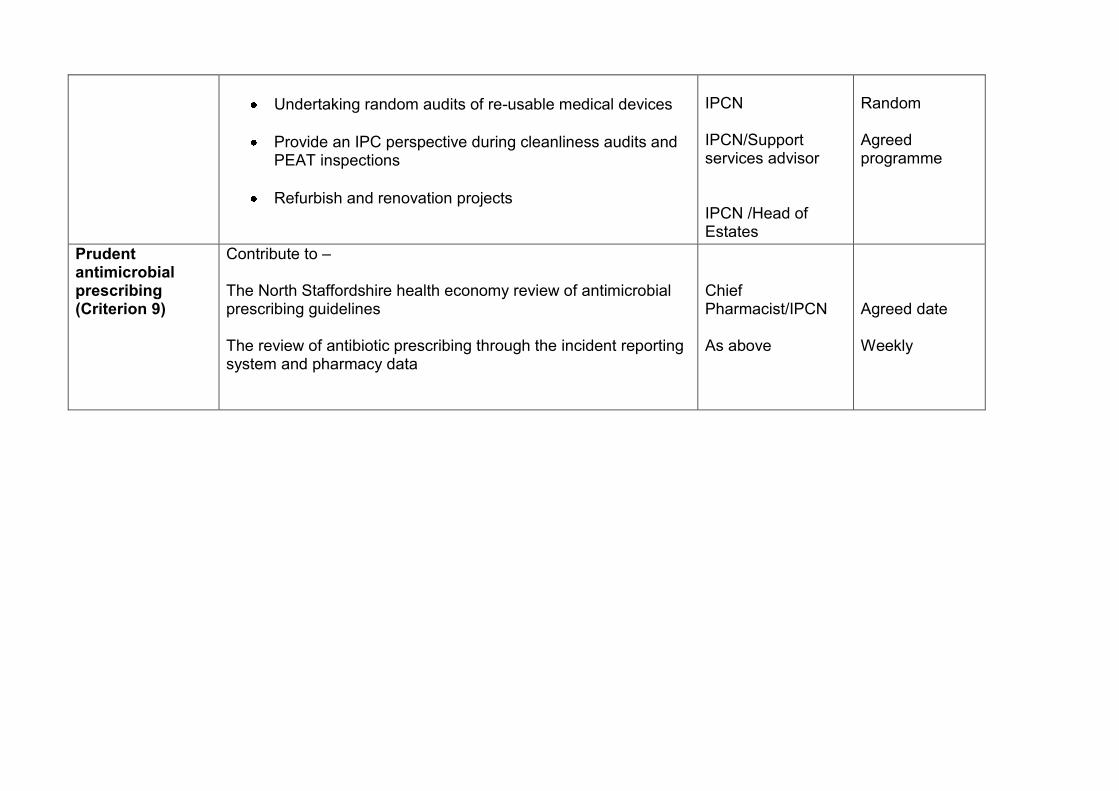
Undertaking random audits of re-usable medical devices
Provide an IPC perspective during cleanliness audits and PEAT inspections
Refurbish and renovation projects
IPCN IPCN/Support services advisor IPCN /Head of Estates
Random Agreed programme
Prudent antimicrobial prescribing (Criterion 9)
Contribute to – The North Staffordshire health economy review of antimicrobial prescribing guidelines The review of antibiotic prescribing through the incident reporting system and pharmacy data
Chief Pharmacist/IPCN As above
Agreed date Weekly

Appendix II Role of the Director of
Infection Prevention and Control
The role of the Director of Infection Prevention and Control is to:
Be accountable directly to the Chief Executive and to the Board (but not necessarily a member of the Board)
Be responsible for the organisation’s infection prevention and control team (IPT)
Oversee local prevention and control of infection policies and their implementation
Be a full member of the ICT and regularly attend its infection prevention and control meetings
Report directly to the NHS Board and, in non NHS care settings, the registered provider
Have the authority to challenge inappropriate practice and inappropriate antibiotic prescribing
Assess the impact of all existing and new policies on infections and make recommendations for change
Be an integral member of the organisation’s clinical governance and patient safety teams and structures
Produce an annual report and release it publicly as outlined in Winning Ways: working together to reduce healthcare associated infection in England.
Taken from the Health and Social Care Act 2008 Code of Practice on the prevention and control of infections and related guidance (Department of Health 2010)





























