Embed Size (px)
Citation preview

Medication Safety Quality Improvement: Collaboration to
Reduce Adverse Drug Events
Jayme Steig, PharmD, RPh Quality Improvement Specialist - Pharmacy Quality Health Associates of North Dakota

Disclosure
“I have had no financial relationship over the past 12 months with any commercial sponsor with a vested interest in this presentation.”
2

Objectives
Review the National Action Plan (NAP) for Adverse Drug Event (ADE) Prevention
Name the three drug classes targeted in NAP and explain the reasons for their inclusion
Compare ADE data at national, state and community level and identify strengths and areas for improvement in North Dakota
Review and discuss current collaborative approaches to prevent ADEs
Formulate opportunities to improve medication safety in your practice
3

Expectations
All teach, all learn
Active participation and discussion
Leave in action
Learn approaches to collaborate and improve medication safety in your practice
4

Background
5

The National Action Plan for Adverse Drug Event Prevention
6

Adverse Drug Event (ADE)
7
Source: National Action Plan for Adverse Drug Event Prevention
Definition

National Action Plan - The Need
8
Source: National Action Plan for Adverse Drug Event Prevention
Nationally

National Action Plan for ADE Prevention
Released in fall 2014 by US Department of Health and Human Services
Modeled after successful National Action Plan to Prevent Healthcare-Associated Infections
Federal interagency steering committee and workgroups
http://www.health.gov/hcq/ade.asp#overview
9

National Action Plan for ADE Prevention
Four-Pillared Approach
• Surveillance
• Prevention
• Incentives and Oversight
• Research
10

National Action Plan for ADE Prevention
High Impact Targets and Populations
• Common
• Clinically significant
• Preventable
• Measurable
11

National Action Plan for ADE Prevention
12
Source: National Action Plan for Adverse Drug Event Prevention
3 targeted drug classes

National Action Plan for ADE Prevention
13
Source: National Action Plan for Adverse Drug Event Prevention
The most vulnerable
• Elderly
• Low health literacy
• Limited access to health care service
• Low socioeconomic status
• Certain minority and ethnic groups

National Action Plan for ADE Prevention
14
Source: National Action Plan for Adverse Drug Event Prevention

National Action Plan – the Goal
Reduce preventable ADEs
The Triple Aim
15

Question to Run On
In what way(s) may the National Action Plan to Prevent ADEs impact your practice?
16

Medication Safety Data
17

18
240.00
250.00
260.00
270.00
280.00
290.00
300.00
310.00
320.00
330.00
340.001
2/1
/20
09
2/1
/20
10
4/1
/20
10
6/1
/20
10
8/1
/20
10
10
/1/2
01
0
12
/1/2
01
0
2/1
/20
11
4/1
/20
11
6/1
/20
11
8/1
/20
11
10
/1/2
01
1
12
/1/2
01
1
2/1
/20
12
4/1
/20
12
6/1
/20
12
8/1
/20
12
10
/1/2
01
2
12
/1/2
01
2
2/1
/20
13
4/1
/20
13
6/1
/20
13
8/1
/20
13
10
/1/2
01
3
12
/1/2
01
3
2/1
/20
14
4/1
/20
14
6/1
/20
14
8/1
/20
14
10
/1/2
01
4
12
/1/2
01
4
2/1
/20
15
Ad
mis
sio
ns
pe
r 1
00
0 M
ed
icar
e F
FS B
en
efi
ciar
ies
Year Ending
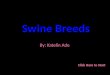
Hospital Admissions
Nation
ND

19
30.00
35.00
40.00
45.00
50.00
55.00
60.00
65.001
2/1
/20
09
2/1
/20
10
4/1
/20
10
6/1
/20
10
8/1
/20
10
10
/1/2
01
0
12
/1/2
01
0
2/1
/20
11
4/1
/20
11
6/1
/20
11
8/1
/20
11
10
/1/2
01
1
12
/1/2
01
1
2/1
/20
12
4/1
/20
12
6/1
/20
12
8/1
/20
12
10
/1/2
01
2
12
/1/2
01
2
2/1
/20
13
4/1
/20
13
6/1
/20
13
8/1
/20
13
10
/1/2
01
3
12
/1/2
01
3
2/1
/20
14
4/1
/20
14
6/1
/20
14
8/1
/20
14
10
/1/2
01
4
12
/1/2
01
4
2/1
/20
15
Re
adm
issi
on
s p
er
10
00
Me
dic
are
FFS
Be
ne
fici
arie
s
Year Ending
Hospital Readmissions
Nation
ND

ADE Surveillance
Types
• Active – Collects data from health records or previously collected information
Technology driven
• Passive – Voluntary reporting to surveillance system
Manual
Example – FDA Adverse Event Reporting System
20
Source: National Action Plan for Adverse Drug Event Prevention

ADE Surveillance
Barriers
• Active
Coding not designed for ADE
Cause and effect
• Passive
Manual
Sampling
Voluntary – Underreporting
21
Source: National Action Plan for Adverse Drug Event Prevention

ADE Surveillance
Additional considerations
• Reporting requirements
• Severity
• Settings
• Timeliness
22
Source: National Action Plan for Adverse Drug Event Prevention

ADE Data
National, Regional, State
23
State Total Beneficiaries
% at high risk for ADE
Anticoagulants Diabetic agents Opioids Total
Kansas 404,445 6.7% 13.7% 14.5% 25.1%
Nebraska 260,660 8.1% 12.2% 11.3% 22.9%
North Dakota 97,604 8.4% 14.9% 11.1% 25.6%
South Dakota 125,298 7.6% 12.6% 10.6% 22.7%
United States 37,079,097 5.8% 13.3% 13.2% 23.8%
Source: 2013 Medicare Part D claims analysis

24

25
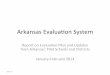
263.49
416.32
694.96 741.32
287.46
495.31
872.8
715.67
0
100
200
300
400
500
600
700
800
900
1000
FFS Beneficiaries HRM Benes -Diabetic Agents
HRM Benes -Anticoagulants
HRM Benes - Opioids
Admissions per 1,000 FFS Beneficiaries by Drug Class (CY 2013)
North Dakota Nation

26
41.21
80.18
128.83 147.93
51.86
106.18
192.39
158.29
0
50
100
150
200
250
FFS Beneficiaries HRM Benes -Diabetic Agents
HRM Benes -Anticoagulants
HRM Benes - Opioids
Readmissions per 1,000 FFS Beneficiaries by Drug Class (CY 2013)
North Dakota Nation

27

The Good News (and the Bad)
28
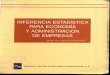
3
11
36
0
5
10
15
20
25
30
35
40
45
50
Diabetic agents Anticoagulants Opioids
Probably Adverse Drug Event Rates (CY 2013) ND’s National Rank (lower is better)

A Broader Picture
29
Sources: http://www.cdc.gov/drugoverdose/data/statedeaths.html http://blogs.cdc.gov/nchs-data-visualization/drug-poisoning-mortality/

Community Level Data
30
Minot Bismarck Grand Forks Fargo

Probable ADE Rates
31
Source: QHA analysis of Medicare Part D and Part A claims 8/1/14 thru 7/31/2015
0.00
20.00
40.00
60.00
80.00
100.00
120.00
140.00
State Bismarck Minot Fargo Grand Forks Outside
Pro
bab
le A
DE
per
10
00
HR
Ben
efic
iari
es
Combined Anticoagulants Diabetic Agents Opioids

Questions to Run On
What are your thoughts after seeing this data?
Have you noticed similar data/trends in your practice?
What is your greatest area of concern in relation to the three targeted high-risk drug classes?
32

ADE Prevention Approaches
33

ADE Determinants
34
Source: National Action Plan for Adverse Drug Event Prevention

ADE Determinants
Underlying drivers
• Communication failures
• Suboptimal management systems
• Inadequate access to medication information
• Low patient activation
What are drivers within your community?
35
Source: IPRO. Parade: Preventing and Reducing Adverse Drug Events in Care Coordination Communities (webinar). January 6, 2015.

Improving Medication Safety
Establish partnerships to improve communication among hospitals, skilled/LTC nursing facilities, home health agencies, pharmacists, physicians and other community stakeholders
Develop partnerships with patients and families to improve readiness for transitions of care, chronic disease self-management and to reduce medication harm
36

Example Interventions: Suboptimal Communication/Management
Nurse-to-nurse calls
SBAR
Follow-up MD appointments made before hospital discharge
Medication reconciliation by pharmacist
Readmission risk assessment
Post discharge telephone follow-up with high-risk patients
37

Example Interventions: Inadequate Access to Medication Information
Communication between senders and receivers
Medication reconciliation
Patient and family involvement during transitions
38

Example Interventions: Low Patient Activation
Teach-back
Patient and family education
Chronic disease self-management
Medication adherence programs
Personal health record
39

Example Interventions: Multiple Drivers
INTERACT Quality Improvement Program
Cross-setting workgroups
Project RED (Re-engineered Discharge)
Advance care planning
Medication Therapy Management (MTM)
40

Medication Safety Resources
http://greatplainsqin.org/initiatives/medication-safety/
http://greatplainsqin.org/initiatives/coordination-care/
41

Resources and Assistance
Great Plains QIN provides
• Learning and Action Network
• Facilitation
• Technical Assistance
• Tools and best practices
• Data analysis
• Promote and share resources
42

Area Examples
Medication reconciliation
• Hospital-SNF: Organizational
43
0.0
1.0
2.0
3.0
4.0
5.0
6.0
Pharmacist Inpatient Med Rec - Orders per SNF readmit requiring clarification
Orders per readmit requiring clarification - Readmit
Linear (Orders per readmit requiring clarification - Readmit )

Area Examples
Medication reconciliation
• Hospital-SNF: Collaborative
44
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15
SNF Cover Sheet - Orders per readmit requiring clarification
Orders per readmit requiring clarification - Readmit
Linear (Orders per readmit requiring clarification - Readmit)

Area Examples
More Hospital-SNF collaboration
45
15.7% 15.2%
15.9%
13.9% 14.1% 13.2%
11.0% 10.7% 10.1%
11.3%
14.5% 14.2% 13.8%
14.0% 14.2% 14.3%
15.7% 15.8%
14.3% 13.9%
6%
8%
10%
12%
14%
16%
18%
Rea
dm
issi
on
Rat
e
1 - Year Period Ending
Readmission Trends - Workgroup SNFs vs. Other SNFs
Workgroup SNFs All Other SNFs

Area Examples
ADE screening as part of medication adherence program - Pilot
Improving anticoagulation education
Increasing awareness of community resources
HEN – Inpatient and admission ADE tracking
SD – PMP utilization
46

Great Plains QIN ADE Environmental Scan
WHAT: A tool to collect information regarding current status of medication safety efforts to detect and prevent Adverse Drug Events (ADE) within the Great Plains Quality Innovation Network (QIN)
HOW: Link to environmental scan placed on the Great Plains QIN website during July and August 2015 and emails sent to providers and stakeholders
WHO: Distributed to providers and stakeholders within the Great Plains QIN (Kansas, Nebraska, North Dakota and South Dakota)
47

Overview – Great Plains
48

0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
Electronic Manual Other
Most track ADEs via electronic records
Overview – all settings
49

ND Responses
Use of data
• P&T/Medication safety committee review
• RCA on each event with aggregate reporting for trending
Barriers
• Time/resources
• Turnover
• Pharmacist availability (CAH, SNF)
50

ND Responses
Current initiatives
• Increase med rec reviews
• Bar coding
• Anticoagulant (INR w/antibiotic starts)
• Opioids (staff training, Narcan availability)
51

Question to Run On
What are some examples of your involvement in medication safety initiatives?
52

Reflection & Action
53

Learning Assessment
Which three drug classes are targeted in the NAP for ADE preventions?
Why were these 3 classes chosen?
Which drug class does ND have higher probable ADE rates than national average?
54

Questions to Run On
What action will you take to reduce ADEs in your practice?
What will you do in the next seven days to start this effort?
Name one community partner you will contact in the next two weeks regarding collaborative efforts to improve medication safety.
55

Action Plan Exercise
56

Action Plan Example
57

Leave in Action
Follow through on Action Plan
Sign up for the Learning and Action Network • http://greatplainsqin.org/lan-signup-page/
• Medication safety, care coordination, immunization, diabetes, and others
View website resources • Care Coordination
http://greatplainsqin.org/initiatives/coordination-care/
• Medication Safety
http://greatplainsqin.org/initiatives/medication-safety/
58

Contact Information
Jayme Steig, PharmD, RPh Quality Improvement Specialist-Pharmacy
P: 701-240-8135 [email protected]
59
Quality Health Associates of North Dakota 3520 North Broadway
Minot, ND 58703 P: 701.852.4231
www.greatplainsqin.org

Thank You!
This material was prepared by the Great Plains Quality Innovation Network, the Medicare Quality Improvement Organization for Kansas, Nebraska, North Dakota and South Dakota, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. 11S0W-GPQIN-ND-C3-43/0216