Embed Size (px)
Citation preview

.NORMALIZATION FOR INDIVIDUALS WITH MENTAL RETARDATION
Jane Strobino, D.S.W.Marywood College
School of social Work
Background
Currently, service delivery for individuals with mentalretardation is provided in accordance with the principleof normalization. Normalization means "making availableto the mentally retarded patterns and conditions ofeveryday life which are as close as possible to the normsand patterns of the mainstream of society" (Nirje, 1976,231) . This principle implies that individuals withmental retardation have the same individual rights as anyother citizen, and that there are services for them inthe community. Given these implications in light of thelong history of limited community based services topersons with mental retardation, one might· expect parentsto be particularly supportive of the normalizationprinciple.
Yet, practice experience yields the observation that someparents are not supportive of the principle ofnormalization. One example of this lack of support isindicated by parental request for institutional placementfor their son or daughter with mental retardation. Oftenthe social worker, in complying with the principal ofnormalization and the policy of deinstitutionalization,will take on the role of advocate for the individual withmental retardation. Such a situation leads todiscrepancies between the social worker and the familyover the identification of needs and services for theindividual with mental retardation. As a result, thesocial worker might be pitted against the parents inattempting to facilitate service delivery. Thus thequestion emerges as to what is the parental attitudeabout normalization. Furthermore, what factors influenceparents I decision about residential placement for theirson or daughter with mental retardation.
Because it offers an explanatory model for decisionmaking, symbolic interaction theory is appropriate to useas a gurde for focusing on the investigation of attitudesand decision making. This theory holds that experiencecoupled with knowledge"I'rom indirect experiences, combineto shape a person I s perceptions. perceptions in turninfluence behavior (Blumer, 1969). Applying thistheoretical premise to the situation of parental decision

284
mak~ng would result ~n the following argument. Parents'experience in caring for their son or daughter withmental retardation plus their understanding of theprinciple of normalization result in the parents'perception of the appropriateness of the normalizationprinciple vis a vis their child's activities or livingsituation. This perception in turn influences parents'decision about residential care and thus their action toselect a specific residential option.
Related Literature
Previous literature regarding parental decision makingabout residential placement has focused on three areas.These areas include characteristics of the individualwith mental retardation, family characteristics, andperception about residential service options.
Characteristics of the Individual with Mental RetardationAlthough some socio-demographic variables (gender, age)have been found to be associated with parental decisionabout residential placement (Eyman et al., 1972; Farberet al., 1960), there has been no consistent trenddocumented. However, IQ and physical problems have beendocumented consistently in that individuals with lower IQscores and individuals with physical disabilities aremore likely to be institutionalized (Eyman et al., 1972,Justice et al., 1971; Skelton, 1972). Additionally,social behavior or difficulty in managing the individualwith mental retardation has been associated withinstitutionalization (Eyman et al., 1972).
These findings related to characteristics of theindividuals with mental retardation, suggest thatparents' decision about out of home placement may be afunction of the assessment of the extraordinarycaregiving needs of their son or daughter in relation totheir own ability (directly or by accessing supportservices) to meet those needs.
Family CharacteristicsSeveral characteristics of the family system have beeninvestigated in terms of their relationship to parents'decision about out-of-home placement. Thesecharacteristics include: parents' age, religion, health,educational level, income, marital integration, stresslevel, and the presence of siblings in the home.
Younger parents are more likely to request institutionalplacement (Wolf & Whitehead, 1965) due to overwhelmingfeelings of lifetime care needs of their son or daughterwith mental retardation, recommendations of thephysician, and the limited interaction with reference

285
groups that support the notion of family home care(Darling, 1979). Those parents who are affiliated with areligion, because they may receive both tangible andspiritual/emotional support that reinforces the idea thatparents can provide the care in the home (ernie et al.,1983; Darling, 1979) are less likely to requestout-of-home placement. However, parents with poorhealth, especially the mother, may have a decreasedability to tend to the needs of the individual withmental retardation and thus a greater likelihood torequest out-of-home placement in order to assure thatthose needs are met (Murphy, 1982). More highly educatedparents are apt to request institutionalizationpresumably because their tolerance of deviance is limited(Holt, 1958). Likewise this rationale is used forparents in higher income levels who requestinstitutionalization. Some literature suggests thatrequest for institutionalization is a function of familyincome level or social class when parents attempt toassure that the needs of the individual with mentalretardation are met and that the family's financialstability is maintained (Darling, 1979; Dunlap &Hollinsworth, 1977; Farber et al., 1960; Murphy, 1982).The presence of a handicapped individual has been shownto impact variously on marital integration (Berggreen,1971; Dunlap & Hollinsworth, 1977; Fowle, 1968), stressand coping abilities of parents (Beckman, 1983;Birenbaum, 1971; Dunlap & Hollinsworth, 1977; Friedrich,1979; Holroyd, 1979; Holroyd et al., 1975) and onbehavior and roles of siblings (Berggreen, 1971; Dunlap &Hollinsworth, 1977; Farber et al., 1960).Parents' assessment of the impact of the handicappedfamily member on the family system in turn influencesparents' decision about out of home placement. Familycharacteristics, when viewed as contributors to theperception of caregiving capacity of parents, areexplanatory factors in parental decision making aboutout-of-home placement.
AttitudesAttitudes about mental retardation, residential serviceoptions, and normalization have been investigated invarying degrees, the findings of which generally supportthe institutional service model.
Darling (1979) found that families immersed in referencegroups who defined their handicapped child positivelyalso had positive attitudes about mental retardationwhereas parents immersed in reference groups who definedtheir handicapped child negatively had negativeattitudes. Thus, parents themselves possess aperception about the mental retardation and about thecapabilities and rights of persons with mentalretardation to be integrated into the community. It
286
seems logical to suppose that parents take in a myriad offactors when making a decision about residentialplacement for their son or daughter with mentalretardation including their own perception of mentalretardation and the community or the public response tomental retardation (Teeley, 1983; Woestendiek, 1983) 0
Additionally, parents' decision may be impacted by theirperception of residential alternatives 0 Meyer (1980)found that parents chose institutions over otheralternatives and their reasons included: the availabilityand quality of supervision, care and either resources 0
Payne (1976) found this same preference with the reasonsbeing the concentration of professionals to provideservices; the fact that the mentally retarded would bewith persons like themselves; the protection from thestress of everyday life; and the permanence of theinstitution. These findings also concur with those ofWoestendick (1983), Frohboese and Sales (1980), andSchodek et al. (1980) which indicate that the institutionis viewed as one that is likely to persist because of thestable funding source. Further, parents report morecontinuity in programing in the institution because staffturnover is not particularly high as compared with grouphomes.
Ferrara (1979) specifically addressed parents' attitudeabout normalization. Parents displayed more positiveattitudes about normalization when the referent wasgeneral and less postiive attitudes when the referent wastheir own son/daughter with mental retardation. Also,parents were in greater agreement with the valuesinherent in the normalization principle and in lesseragreement with the way the normalization principle was
'translated into community services. Ferrara concludedthat parental attitudes need to be assessed so that areasof parental concern and conflict with professionals orpublic policy can be resolved.
Parents' decision about out-of-home placement isinfluenced by a wealth of information that arises frominteraction with the individual with mental retardationas well as with others. Such information includes:parents' experiences related to caregiving; theirbeliefs about mental retardation and residential serviceoptions'; their assessment of the family's goals andneeds; and their understanding of the community'sresponse to persons with mental retardation.
Method
In an effort to understand._parental perceptlons about~Qrmedi~aLton and deci&iQn maklng related to ~es~dential-

287
care, an exploratory study was conducted. This was athree (3) group correlational study using a surveyresearch approach. The study was considered ex postfacto in nature since parents' preference for residentialplacement had been documented prior to theirparticipation in this study. Those parents who hadrequested institutional placement, those parents who hadrequested group home placement and those parents who hadnot requested out of home placement comprised the threegroups.
The study subjects included parents of individuals withmental retardation who resided in the state of Marylandand whose names appeared on the waiting list for aninstitution (Great Oaks Center), for a group home(Baltimore Association for Retarded citizens - BARC) , andwhose names appeared on an affiliation listing with BARCbut who had not requested out-of-home placement.
A systematic stratified random sampling plan was employedto select SUbjects from the BARC waiting list andaffiliation file. No sampling plan was used for theinstitutional waiting list since the N size of that groupwas so small. All persons on the institutional waitinglist were invited to participate.
A total of 65 individuals responded to the mailquestionnaire including 9 from the institutional waitinglist, 28 from the group home waiting list, and 23 whowere affilites of BARC (5 questionnaires were returnedand completed with group affiliationunidentifiable. This total number constitutes a 35.7%response rate and takes into consideration thosequestionnaires that were returned undeliverable orunanswered. Such a response rate is not atypical formail questionnaires (Babbie, 1973).
InstrumentsThe mail questionnaire contained three separateinstruments, a demographic questionnaire and two testinstruments. The demographic questionnaire consisted ofitems relating to characteristics of the parents, andcharacteristics of the individual with mental retardationincluding an estimate of the level of retardation andadaptive behavior. Test Instrument 1 was a 44 itemrevised version of Holroyd's Questionnaire on Resourcesand Stress (QRS). The QRS was used as a measure ofparents' experience in caring for their son/daughter withmental retardation. The Second Test Instrument was a 20item scale that measured attitude about normalization andwhich was developed by this writer based on the earlierwork of Ferrara (1979), Gottlieb & Siperstein (1976),Gottlieb & Corman (1975), and Gottwald (1970). Thisscale attempted to document the degree to which the

288
respondent agreed with the philosophical aspects ofnormalization (rights) and to the actualoperationalization of the normalization principle (waysof assuring those rights and integration in thecommunity) •
Both of the test instruments were reviewed by a panel forvalidity as well as clarity or readability and found tohave face validity/content validity. A reliabilityassessment was conducted on the test instrumentsutilizing the study data. Item analysis using theReliability program of the statistical package for theSocial Sciences (SPSS) (Hull et al., 1975) provided anitem total correlation and the Kuder-Richardson-20(KR-20) reliability coefficient of .87 for the QRS whichis the alpha for dichotomous variables (Friedrich et al.,1983) based on a total N size of 39 cases for which therewas no missing data. The attitude about normalizationscale also was exposed to a reliability test utilizingthe alpha coefficient for continuous variables, ascontained in the SPSS program. A Cronbach's Alpha of .76was obtained on a total of 49 cases for which there wasno missing data. Both reliability coefficients wereconsidered within the acceptable range in order toproceed with data analysis.
LimitationsA number of methodological factors pose limitations tothe results of this study. The data collectionmethodology being a mail questionnaire results in therespondents being a self-selected group and therefore notnecessarily representative of the total popUlation.Also, the N size of the sample was small thus furtherthreatening the ,generalizability of the results.Although the three group design is theoretically sound,the groups may not be as distinct as had been hoped. Aparent could have selected more than one kind ofresidential option and the decision about the residentialoption could have been influenced by a variety of otherfactors not accounted for in this study.
Despite these limitations however, the results do providea beginning documentation of what this group of parentshad experienced in caring for their son or daughter withmental retardation, and had thought about normalization.Indeed, if we are to provide a service delivery systemthat is efficacious, then we need to take into accountparents' concerns and allow for these concerns to beincluded in the planning process.
Findings
The RespondentsTable 1 displays the distribution of demographic
289
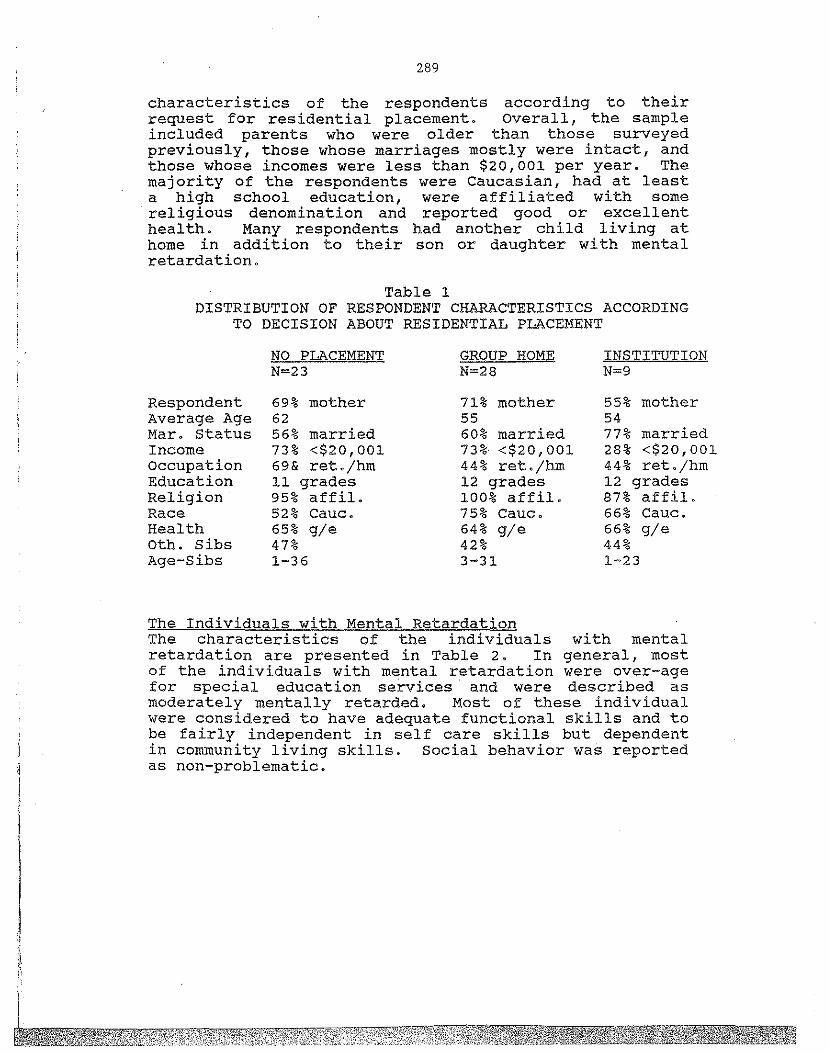
characteristics of the respondents according to theirrequest for residential placement. Overall, the sampleincluded parents who were older than those surveyedpreviously, those whose marriages mostly were intact, andthose whose incomes were less than $20,001 per year. Themajority of the respondents were Caucasian, had at leasta high school education, were affiliated with some
. religious denomination and reported good or excellenthealth. Many respondents had another child living athome in addition to their son or daughter with mentalretardation.
Table 1DISTRIBUTION OF RESPONDENT CHARACTERISTICS ACCORDING
TO DECISION ABOUT RESIDENTIAL PLACEMENT
RespondentAverage AgeMar. StatusIncomeoccupationEducationReligionRaceHealthoth. sibsAge-Sibs
NO PLACEMENTN=23
69% mother6256% married73% <$20,00169& ret./bm11 grades95% affil.52% Cauc.65% gle47%1-36
GROUP HOMEN=28
71% mother5560% married73% <$20,00144% ret./hm12 grades100% affil.75% Cauc.64% gle42%3-31
INSTITUTIONN=9
55% mother5477% married28% <$20,00144% ret./hm12 grades87% affil.66% Cauc.66% gle44%1-23
I·,i
II,
The Individuals with Mental RetardationThe characteristics of the individuals with mentalretardation are presented in Table 2. In general, mostof the individuals with mental retardation were over-agefor special education services and were described asmoderately mentally retarded. Most of these individualwere considered to have adequate functional skills and tobe fairly independent in self care skills but dependentin community living skills. Social behavior was reportedas non-problematic.

290
Table 2DISTRIBUTION OF CHARACTERISTICS OF THE INDIVIDUALS
WITH MENTAL RETARDATION BY PLACEMENT DECISION
Average AgeGenderDegree MRLevel Funct.
NO PLACEMENTN=23
3360% male82% mod.48.2
GROUP HOMEN-28
2753% male60% mod.49.8
INSTITUTIONN=9
2077% male55% mod.40.3
Parental Experience in CaregivingTest Instrument l, the Questionnaire on Resources andStress (QRS), consisted of eleven (11) subscales whichmeasured the parents' report of stress. Subscales thatclearly indicated stress for the majority of respondentswere those of lifetime care and terminal illness.Subscales that reflected minimal stress included: familyharmony, lack of personal reward, and physicallimitations of the individual with mental retardation.Table 3 indicates that parents awaiting institutionalplacement reported the greatest amount of stress overallas well as for each subscale.
Table 3AVERAGE SCORES OF THE QRS
ACCORDING TO DECISION ABOUT RESIDENTIAL PLACEMENT
NO PLACEMENT GROUP HOME INSTITUTION
Dep.jMan. 1.1 1.7 2.1Cog. Imp. 1.4 ;1.. 2 2.7Fam. Opp. 1.4 1.7 2.5Life Care 2.9 3.3 3.5Fam. Harm. 0.3 0.7 1.0Lack Reward 0.8 0.6 1.3Term. Ill. 2.0 1.9 2.7Phy. Limits 0.0 0.4 0.8Fin. Stab. 1.6 1.5 2.5Inst.Pref. 0.9 1.4 2.0Burd. Care 1.9 2.3 2.3
Total Score 15.0 17.1 28.1
Attitude About NormalizationRespondents were asked to indicate on this 20 item scale,the degree to which they agreed with each statement thatreferred to the normalization philosophy. An averagetotal score for each group was computed and found to be:75.4 no placement; 77.5 group home; 70.4 institution.Testing for differences in the mean score for each ofthese three groups revealed no significant differences.

291
Because this result was not expected, the distribution ofthe responses for each item of the scale wasre-examined. Those items for which a majority of thesample agreed included ones that addressed thephilosophical or conceptual aspects of normalization (seeTable 4).
Table 4ATTITUDE ABOUT NORMALIZATION
ITEMS OF AGREEMENT
The individual with mental- retardation:has the same basic needs as anyone elseneeds warmth and affection as anyone elsehas the same basic rights as anyone elseshould have an opportunity to pursue his/her desireshas a right to a pUblic educationshould dress like others his/her ageshould not be placed in an institutionshould expect to participate in community activitiesshould have habilitation programs available to him/her
The majority of the sample also disagreed with thoseitems that related to the manner in which thenormalization principle is operationalized.Specifically, items addressing the integration of theindividual with mental retardation into the community,the pUblic school system, and the integration of "specialservices" with other community services were ratedconsistently as disagree or strongly disagree.
HypothesesA number of hypotheses were tested and the followingresults obtained.
H (1): The higher the QRS score the more likely theparent is to request out-of-home
placement---supported.
H (2): The lower the attitude score, the more likely theparent is to request out-of-home placement---notsupported.
H (3): The higher the QRS score and the lower theattitude score the more likely the parent is to
request out-of-homeplacement---supported but probably due to the
strength of the first hypothesis.
Other AnalysesA variety of other analyses were completed of which thefollowing were found to be significant.The higher the level of functioning of the individual
individual with mental retardation, thethe parent is to request out-of-home
292
with mental retardation, the less stress reported by therespondent.The younger parent is more apt to report higher stress.
The older theless likelyplacement.
The higher the functional skills of the individual withmental retardation, the more positive the parents'attitude about normalization.
Discussion
One of the initial questions that this study explored waswhat factors influence parents' decision aboutout-of-home placement.Parents' decision about out-of-home placement for theirson or daughter with mental retardation was found to beassociated with the amount of stress that 'theyexperienced. The greater the amount of stressexperienced, the more likely the parent was to requestinstitutionalization. Parents indicated that in theirexperience of providing care for their sons or daughterswith mental retardation, their greatest stress orconcerns were the areas of lifetime care needs andterminal illness (ongoing health needs). Assurrance thatthe care and health needs of their children will be metmay reduce the stress experienced by the parents. Suchan assurrance can be given in the form of respiteservices being readily available and accessible toparents over the lifetime of the individual with mentalretardation. Additionally, daily program services for I
adults could serve to decrease the stress. Early on,parents need to be advised of the range of services thatare available. As time goes on, parents need thisknowledge reinforced so that in fact they can takeadvantage of the available services. If the necessaryservices are not available or accessible, then effortsmust be made to improve service delivery so that servicescan be utilized.
These concerns may also relate to the question of whowill be responsible for the care of the individual withmental retardation when the parent is no longer able toprovide the care. For some parents, the institutionprovides such an assurrance. Parents who did report thegreatest amount of stress may have perceived some urgencyin obtaining residential care for their son or daughterand therefore requested institutionalization in order tobypass the lengthy wait for community based residentialservices. Furthermore, parents may interpret theinstitution as being the most appropriate out-of-home'
293
placement for those young (adolescent andsignificantly impaired individualsretardation who present behavior management
younger) andwith mentalproblems.
The other issue that this study investigated was that ofparental attitude about normalization. Attitude was notfound to be associated with decision about out-of-homeplacement, possibly because of the negatively skewedtotal scores on the attitude scale. However, there-examination of the items on the attitude aboutnormalization scale supported earlier work (Ferrara,1979) in which parents agreed with the philosophicalaspects of normalization but not with the way in whichthe principle is operationalized. It appears thatparents prefer protection for their sons or daughterswith mental retardation. Perhaps parents viewintegration of the . individual with mental retardationinto the community as too great a risk which may resultin exploitation rather than growth toward independence.
The normalization principle assumes that that thecommunity is accepting of individuals with mentalretardation. Yet parents know through their ownexperience that the community is not as ready as theprinciple assumes (Woestendiek, 1983). Therefore, areview of the principle and its service options in lightof parents' attitude and community readiness is criticalif service delivery is to be efficacious.
Certainly, the attitude about normalization scale itselfcould be further developed so as to improve itsreliabiltiy. Also, the inclusion of items that referspecifically to the adult popUlation with mentalretardation could result in a clearer understanding ofparents' perceptions about the integration of their adultson or daughter into the community.
Because there is so little empirical information aboutparents I attitude about normalization, more widespreadresearch to document that attitude is needed.
Given additional information on parents' attitudes aboutnormalization, professionals, especially social workers,may be in a fine position to utilize this information toinfluence social policy. Involving the parents in theprocess of planning and designing of services that areconsistent with normalization has the potential to resultin services that will be utilized by the population forwhom they were intended. Furthermore, another potentialresult might be a changed attitude about normalization byboth the parents and the professionals involved.
The community too needs to be assessed for its readinessfor the integration of individuals with mental

294
retardation. Efforts to enhance that readiness hould bemade so that the physical integration also means socialand psychological integration into the community(Frohboese & Sales, 1980).
Finally, professionals need to acknowledge the breakdownin the normalization syllogism ("normalization is bestfor the growth and development of individuals with mentalretardation"; "parents want what is best for theirchildren with mental retardation"; therefore parentswant normalization") and to recognize the parents'perspective. Social workers in particular are trained tobe good listeners. They need to listen to what parentsare saying about their experiences and beliefs in caringfor their sons or daughters with mental retardation. Apartnership with parents needs to occur such that the"client" is redefined to include the parents as well asthe individual with mental retardation. Thus, the socialworker will not be pitted against the parent whileattempting to provide services.
Parents' goals for their children are tempered bynumerous factors including their experiences with theirchildren, the service delivery system that is available,and the responses from the larger population. Perhaps bycombining the pragmatism of the parents with the idealismof the professionals, effective advocacy can occur whichwill result in the physical, social, and psychologicalintegration of individuals with mental retardation intothe mainstream of society.
References
Babbie, E.R. (1973). survey research methods. Belmont,Ca.: Wadsworth.
Beckman, P.J. (1983). Influence of selected childcharacteristics on stress in families of handicappedchildren. American Journal of Mental Deficiency,88, 150-156.
Berggreen, S.M. (1971). A stUdy of the mental health ofthe near relatives of twenty multihandicappedchildren. Acta Pediatrica Scandanavica Supplement,215, 1-24.
Birenbaum, A. (1971). The mentallythe home and the family cycle.and Social Behavior, 12, 55-65.
retarded child inJournal of Health
Blumer, H. (1969).Cliffs, N.J.:
Symbolic interactionism.Prentice-Hall, Inc.
Englewood
295
Crnic, K., Friedrich, W., & Greenberg, M.T. (1983).Adaptation of families with mentally retardedchildren: A model of stress, coping, and familyecology. American Journal of Mental Deficiency, 88,125-136.
Darling, R.B. (1979).Beverly Hills, Ca.:
Families against society.Sage Publications.
Dunlap, W.R., & Hollinsworth, J.S. (1977). How does ahandicapped child affect the family? Implicationsfor practitioners. The Family Coordinator, 26,286-293.
Eyman, R.K., O'Connor, G., Tarjan, G., & Justice, R.S.(1972). Factors determining residential placement ofmentally retarded children. American Journal ofMental Deficiency, 76, 692-698.
Farber, G., Jenne, W.C., & Togio, R. (1960). Familycrisis and decision to institutionalize theretarded child. NEA Research Monograph Series(A-I) •
Ferrara, D.M.retardedAmerican
(1979). Attitudes of parents of mentallychildren toward normalization activities.
Journal of Mental Deficiency, 84, 145-151.
Friedrich, W.mothers ofConsulting
(1979). Predictors of coping behavior ofhandicapped children. Journal ofand Clinical Psychology, ±If 1140-1141.
Friedrich, W., Greenberg, M.T., & ernic, K. (1983). Ashort-form of the questionnaire on resources andstress. American Journal of Mental Deficiency, 88,41-48.
Frohboese, R., & Sales, B.D. (1980). Parentalopposition to deinstitutionalization: A challenge inneed of attention and resolution. Law and HumanBehavior,~, 1-87.
Gottlieb, J., & Siperstein, G.N. (1976). Attitudestoward mentally retarded persons: Effects ofatt i tude ref erent spec i f i city . ,-,Am""",e",r,""i"-,c",a",n"--"J,-,o",u""r=-n...,.a""l~,,,o",,,-f
Mental Deficiency, 80, 376-381.
Gottlieb, J., & Corman, L.toward mentally retardedof Mental Deficiency, 80,
(1975) .children.
72-80.
Public attitudesAmerican Journal
296
Gottwald, H. (1970) . Public awareness about mentalretardation. Council for Exceptional ChildrenResearch Monograph. Reston, Va.: Council forExceptional Children.
Holroyd, J. (1974). The questionnaire on resources andstress: An instrument to measure family response toa handicapped family member. Journal of colllrrtunityPsychology, £, 92-94.
Holroyd, J., Brown, N. wikler, L., & Simmons, J. (1975).stress in families of institutionalized andnoninstitutionalized autistic children. Journal ofCOlmnunity Psychology,~, 26-31.
Holt, K.S.children.
(1958). The home care of severely retardedPediatrics, 22, 744-755.
Hull, C.H., New, N.H., Jenkins, J.G., steinbrenner, K., &Bent, D.H. (1975) • Statistical package for thesocial sciences (2nd edition). New York:McGraw-Hill Book Company.
Justice, R.S., o'connor, G., & Warren, N. (1971).Problems reported by parents of mentally retardedchildren---who helps? American Journal of MentalDeficiency, 75, 685-691.
Meyer, R.J. (1980). Attitudes of parents ofinstitutionalized mentally retarded individualstoward deinstitutionalization. American Journal ofMental Deficiency, 85, 184-187.
Murphy, M.A. (1982). The family with a handicappedchild: A review of the literature. Developmental andBehavioral Pediatrics,~, 73-81.
Nihira, K. Foster, R., She1lhaas, M., & Leland, H.(1974). Adaptive behavior scales (rev. ed.),Washington, D.C.: American Association on MentalDeficiency.
Nirje, B. (1976). The normalization principle and itshuman management implications. !n R.B. Kugel & W.Wolfensberger (Eds.), Changing patterns in residentialservices for the mentally retarded (pp. 231-241).Washington, D.C.: President's Committee on MentalRetardation.
Payne, J. (1976). The deinstitutionalization backlash.Mental Retardation, 14, 43-45.
schodek, K., Chrostowski,P.M., & Yamaguchi, J.family involvement inCasework, 61, 67-73.
297
N.L., Adams, B.C., Minihan,(1980). The regulation ofdeinstitutionalization. Social
Skelton, M. (1972).retarded children.
Areas of parental concern aboutMental Retardation, 10, 38-41.
Teeley, S.E. (1983, September 10). Group homes forretarded draw community opposition. The Washingtonpost, pp. C1, C4.
Woestendiek, J. (1983, December 11). Community care isthe trend. The Philadelphia Inquirer, pp. 1B, 9B,lOB.
Wolf, L.C., & Whitehead, P.C. (1975).institutionalize retarded children:individually matched groups. Mental3-7.
The decision toComparison ofRetardation, 13,
Wolfensberger, W. (1975) .institutional models.Press.
The origin and nature of ourSyracuse, N.Y.: Human Policy
Wolfensberger, W. (1972). The principle ofnormalization in human services. Toronto: NationalInstitute on Mental Retardation.