Embed Size (px)
Citation preview

Normal and abnormal maturation patterns in myeloid cells, myeloid neoplasms
Wolfgang Kern
MLL Munich Leukemia Laboratorywww.mll.com

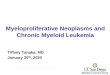
Antigen expression in myelopoiesis
Neutrophil Maturation
An
tig
en D
ensi
ty
CD16
CD11b
CD33
CD15
CD45
CD34
CD117
CD13
HLA-DR

CD34C
D11
7
CD34/CD117

CD36C
D34
CD34/CD36

HLA-DRC
D34
CD34/HLA-DR

CD34C
D13
CD34/CD13

CD34C
D33
CD34/CD33

CD117C
D38
CD38/CD117

CD36C
D38
CD38/CD36

CD14C
D33
CD33/CD14

CD34C
D14
CD14/CD34

CD11bC
D34
CD34/CD11b

HLA-DRC
D11
b
CD11b/HLA-DR

CD15C
D34
CD34/CD15

Multiparametric flow cytometry ofnormal human bone marrow:
analysis and display strategies
GEIL-GTLLF
2008
Part one : Leukocyte subsetsA colour code is applied trhoughout this atlas:Granulocytes in redMonocytes in greenLymphocytes in purpleAll other cells, in a region of maturation defined by the exclusion of mature cell types and thus dubbed « bermudes » in cyan
I.1

CD11b/CD16
I.6
CD45APCFSC-Height CD11bFITC
CD11bFITCCD11bFITC CD11bFITC
SS
C-H
eig
ht
SS
C-H
eig
ht
CD
16
PC
7
CD
16
PC
7
CD
16
PC
7
CD
16
PC
7
FLx
FL
y
FLx
FL
y
CD45
SS
C
FSC
SS
C
FLx
FL
y
FLx
FL
y

CD11b/CD117
I.9
CD45APCFSC-Height CD45APC
CD11bFITCCD11bFITC CD11bFITC
SS
C-H
eig
ht
SS
C-H
eig
ht
SS
C-H
eig
ht
CD
117
PE
CD
117
PE
CD
117
PE
FLx
FL
y
FLx
FL
y
CD45
SS
C
FSC
SS
C
FLx
FL
y
FLx
FL
y

ELN website: www.leukemia-net.org

Identification of cell compartments by CD45-SSC

CD11b/CD16 expression pattern in granulocytes

CD13/CD16 expression pattern in granulocytes

CD11b/CD13 expression pattern in granulocytes

CD56 expression in granulocytes

SSC signal in granulocytes

CD2 expression in monocytes

CD4/CD14 expression in monocytes

CD56 expression in monocytes

CD13/CD11b expression in monocytes

HLA-DR/CD11b expression in monocytes

Indications for immunophenotyping
Consensus: Davis et al. Cytometry Part B 2007;72B:S5-S13
Indicationen:
• Clinical signs• Cytopenias• Leukocytosis• Atypical cells / blasts, evaluation of body fluids• Plasmacytosis / monoclonal gammopathy• Organomegaly / tissue masses• Monitoring
No indication:
• Neutrophilia• Polyclonal hypergammaglobulinemia• Polycythemia• Thrombocytosis• Basophilia

Diagnosis in AML
Diagnosis and subclassification of AML is based on:
Cytomorphology and cytochemistryCytogenetics/FISHMolecular geneticsImmunophenotyping
Immunophenotyping for diagnosis of AML:
AML M7AML M0BAL
Immunophenotyping for subclassification of AML:
Hint to genetic abnormalitiest(15;17), t(8;21), inv(16)

Diagnosis in AML
Definition of AML M0:
positive for myeloid Antigensnegative for lymphatic Antigens

Diagnosis in AML
Definition of AML M7:
positive for CD41positive for CD61

Diagnosis in AML
CD7+CD33+ MPO+LF- TdT+cyCD3+
Biphenotypic acute leukemiaMixed phenotype acute leukemia

Typical findings in APL:
characteristic SSC/FSC-pattern
high auto-fluorescence
CD33+/HLA-DR-
AML M3
Normal BM AML M2
Subclassification in AML

Subclassification in AML
Typical findings in AML with t(8;21):
Coexpression of CD19 Coexpression of CD56

Subclassification in AML
Typical findings in AML with inv(16):
Coexpression of CD65 and CD34 Coexpression of CD2

Differential using CD45-SSC-Gate
Immunophenotyping11% blasts
Cytomorphology8% blasts

Differential using CD45-SSC-Gate
Immunophenotyping27% blasts
Cytomorphology27% blasts

Differential using CD45-SSC-Gate
Cytomorphology82% blasts
Immunophenotyping88% blasts

Differential using CD45-SSC-Gate
Immunophenotyping6% blasts
Cytomorphology18% blasts

Differential using CD45-SSC-Gate
Cytomorphology18% blasts
Immunophenotyping14% monocytic cells
Immunophenotyping6% blasts

Background
Prognostic factors in AML• Pre-therapeutic parameters:
Karyotype, molecular genetics, age, sAML• Heterogeneous prognosis within defined groups• Prognosis dependent on therapy
Therapy-dependent prognostic parameters

Monitoring of minimal residual disease (MRD)
CD34CD33
CD
56
DiagnosisDay 0
After 1st inductionDay 18
After 2nd inductionDay 68
After alloTxDay 100

Antibody panel
FITC PE PC5
CD34 CD2 CD33
CD7 CD33 CD34
CD34 CD56 CD33
CD11b CD117 CD34
CD64 CD4 CD45
CD34 CD13 CD19
CD65 CD87 CD34
CD15 CD34 CD33
HLA-DR CD33 CD34
CD4 CD13 CD14
CD34 CD135 CD117
CD34 CD116 CD33
FITC PE PC5
CD90 CD117 CD34
CD34 7.1 CD33
CD38 CD133 CD34
CD61 CD14 CD45
CD36 CD235a CD45
CD15 CD13 CD33
TdT CD33 CD45
MPO LF CD15
TdT CD22 CD3
TdT CD79a CD3

LAIP+ cells in normal bone marrow
Kern et al. Haematologica2003;88:646-653
nNormal BM, analyzed samples
total 26per LAIP (median, range) 24, 11-26
Analyses, total 2863
Median frequency of LAIP+ cells in normal BM median (range)
all LAIP (n=140) 0.07% (0.00%-1.20%)
only 1 LAIP per patient (n=68) 0.05% (0.00%-0.43%)

LAIP+ cells in normal and leukemic bone marrow
Kern et al. Haematologica2003;88:646-653 Frequency of LAIP+ cells in AML-BM median (range)
all LAIP (n=140) 25.10% (10.13%-76.14%)
only 1 LAIP per patient (n=68) 25.81% (10.13%-76.14%)
log-difference of LAIP+ cells (normal BM / AML)
median (range)
all LAIP (n=140) 2.47 (0.99-4.23)
only 1 LAIP per patient (n=68) 2.82 (1.58-4.23)

Serial dilution of AML cells in normal BM
Kern et al. Haematologica2003;88:646-653
0.0001
0.001
0.01
0.1
1
10
100
1E-050.00010.0010.010.1110100
% calculated
% m
easu
red
CD34+CD56+CD33+ cells

Day 16 blasts by cytomorphology
Kern et al.Blood2003;101:64-70

Day 16 MRD—Detection of cytoreduction
0.01
0.1
1
10
100
0.01
0.1
1
10
100
% bone marrow blasts
% LAIP+ cells in bone marrow
day 1 day 16
A
B
Cytomorphology
Multiparameterflow cytometry
Kern et al., Haematologica 2004;89(5):528-540

Day 16 MRD—Detection of cytoreduction
0.01
0.1
1
10
100
0.01
0.1
1
10
100
% bone marrow blasts
% LAIP+ cells in bone marrow
day 1 day 16
A
B
Cytomorphology
Multiparameterflow cytometry
Kern et al., Haematologica 2004;89(5):528-540

Day 16 MRD—Multivariate analysis
Kern et al., Haematologica 2004;89(5):528-540
Parameter CR EFS RFS OS
LD day 16 p 0.062 0.004 0.031 n.s.
RR 1.490 0.678 0.555
Favorable karyotype p n.s. 0.044 n.s. n.s.
RR 0.289
Unfavorable karyotype p 0.032 0.007 n.s. 0.021
RR 0.330 2.293

Day 16 MRD—Relapse-free survival
Kern et al., Haematologica 2004;89(5):528-540
10957303650
1.00
0.75
0.50
0.25
0.00
days

Prognostic impact of MRD after induction
10957303650
1.00
0.75
0.50
0.25
0.00
Separation according to 25-percentile Log-difference (=1.70)
LD >25%ile: median EFS 12.0 mos.LD <25%ile: median EFS 3.8 mos.p=0.0004
days
RFS
Kern et al., Blood 2004;104(10):3078-3085

Prognostic impact of MRD after consolidation
Separation according to 75-percentile Log-difference (=2.94)
RFS
10957303650
1.00
0.75
0.50
0.25
0.00
days
LD >75%ile: 2-year-EFS 83.3%LD <75%ile: 2-year-EFS 25.7%p=0.0034
Kern et al., Blood 2004;104(10):3078-3085

MRD after induction and after consolidation (multivariate)
Kern et al., Blood 2004;104(10):3078-3085
MRD MRD
(ind.) (cons.)
Parameter RFS OS RFS OS
LD p 0.006 n.s. 0.006 0.005
RR 0.348. 0.397 0.408
Unfavorable karyotype p 0.0001 n.s. 0.006 n.s.
RR 7.178 4.370

MRD assessment, extended cohort
Patients
Patients (n) 286 3y-OS 54%
MRD assessments (n) 550 EFS, median 14.5 M.
Standard therapy
LAIP+ BM cells at Dx 16.04% (2.54%-76.14%)
LAIP+ cells normal BM 0.02% (0.00%-1.01%)
Follow-up assessments
n Log-difference (median)
Up to day 28 85 2.02
Day 29 to day 60 122 2.29
Day 61 to day 120 158 2.39
Day 121 to day 365 137 2.53
After day 365 48 2.81
Kern et al., ASH 2005

Prognostic impact of MRD
EFS 3y-OS
Median p Months p
(Months)
Up to day 28 21.1 vs. 9.1 0.001 71% vs. 56% 0.035
Day 29 to day 60 21.5 vs. 9.3 <0.001 83% vs. 42% <0.001
Day 61 to day 120 39.3 vs. 13.5 <0.001 82% vs. 63% 0.011
Day 121 to day 365 57.1 vs. 13.7 <0.001 95% vs. 65% <0.001
After day 365 n.r. vs. 29.0 0.001 n.s.
Median Log-difference diagnosisMRD-assessment as separator
Kern et al., ASH 2005

Prognostic impact of MRD levels day 121 to day 365
Kern et al., ASH 2005
543210
Years
1,00
0,75
0,50
0,25
0,00
pCP4 EFS
543210
Years
1,00
0,75
0,50
0,25
0,00
p
CP4 OSRFS OS
median 57.1 vs. 13.7 95% vs. 65% at 3 yearsp<0.001 p<0.001

Prognostic impact of MRD (multivariable)
Kern et al., ASH 2005
EFS 3y-OS
RR p RR p
Up to day 28 0.831 0.085 n.s.
Day 29 to day 60 0.542 <0.001 0.538 0.001
Day 61 to day 120 0.754 0.035 n.s.
Day 121 to day 365 0.510 <0.001 0.422 <0.001
After day 365 0.413 <0.001 n.s.

Impact of MRD levels on RFS in cytogenetic subgroups
Kern et al., ASH 2005
0 365 730 1095 1460
days
0.00
0.25
0.50
0.75
1.00
p
LD <2.53: 37% at 2 years
LD >2.53: 80% at 2 years
p=0.0029
CG = 1
0 365 730 1095 1460
days
0.00
0.25
0.50
0.75
1.00
p
LD <2.53: 25% at 2 years
LD >2.53: 75% at 2 years
p=0.0221
CG = 2
0 365 730 1095 1460
days
0.00
0.25
0.50
0.75
1.00
p
LD <2.53: 0% at 2 y.
LD >2.53: 88% at 2 y.
p=0.0014
CG = 3favorable intermediate unfavorable

A
B
Improvement of MRD assessment by CD45-SSC-gating
Kern et al., Crit Rev Oncol Hematol 2005;56:283-309

Improvement of MRD assessment by CD45-SSC-gating
Kern et al., Hematol J 2004;5:410-418
AMLwithout CD45 gating
AMLwith CD45 gating
Normal BMwithout CD45 gating
Normal BMwith CD45 gating
0.002%
0.511%
69.714%
66.675%

Impact of CD45-gating on sensitivity/specificity
Kern et al., Hematol J 2004;5:410-418
without CD45 gating with CD45 gating
LAIP+ LAIP+ LD LAIP+ LAIP+ LD
AML normal BM AML normal BM
Median 20.86% 0.15% 2.26 20.16% 0.02% 3.07
Min 2.33% 0.02% 1.09 2.24% 0.01% 1.22
Max 82.52% 0.58% 3.34 81.94% 0.42% 4.01

Improvement of MRD assessment by 5-color-staining
Voskova et al., Leuk Lymphoma 2007;48(1):80-88
FITC PE ECD PC5 PC7
CD64 CD87 CD4 CD56 CD45
CD65 CD2 CD34 CD13 CD45
CD9 HLA-DR CD34 CD33 CD45
CD11b CD116 CD34 CD117 CD45
CD34 CD56 CD19 CD33 CD45
CD15 CD7 CD34 CD33 CD45
CD36 CD61 CD14 CD235a CD45
CD4 7.1 CD14 CD13 CD45
CD38 CD135 CD34 CD90 CD45
CD15 CD133 CD34 CD117 CD45
MPO LF CD34 CD33 CD45
TdT CD22 CD3 CD79a CD45

Improvement of MRD assessment by 5-color-staining
51.70%
0.004%
CD45-PC7 SSC
CD15-FITC CD34-ECD
SSC
FS
C
CD
7-P
E
CD
7-P
ES
SC
CD
33
-PC
5
CD45-PC7 SSC
CD15-FITC CD34-ECD
SSC
FS
C
CD
7-P
E
CD
7-P
ES
SC
CD
33
-PC
5
Voskova et al., Leuk Lymphoma 2007;48(1):80-88

Impact of 5-color analysis
Voskova et al., Leuk Lymphoma 2007;48(1):80-88
4-color 5-color
n=139 n=139
LAIP+ LAIP+ LD LAIP+ LAIP+ LD
AML normal BM AML normal BM
Median 19.09% 0.030% 2.86 13.65% 0.003% 3.66
Min 1.90% 0.001% 0.77 1.90% 0.001% 1.98
Max 84.83% 3.600% 4.91 77.57% 0.040% 4.89

Course of MRD using 5-color analysis
LAIP+ in %, CD15-CD7+CD34+CD33+CD45(+)
0,0001
0,001
0,01
0,1
1
10
100
Okt 06 Apr 07 Okt 07 Apr 08 Okt 08

Stability of LAIP between diagnosis and relapse
A
DC
B
Voskova et al., Clin Cytometry 2004;62B:25-38

MRD assessment by multiparameter flow cytometry in AML
1. Applicable to the vast majority of patients
2. Prognostic information in addition to cytogenetics
3. MRD useful as stratification parameter in clinical trials
4. Improvements of method by CD45-gating and 5-color-staining
5. Further assessment and standardization needed

AML with limited differentiation (AML-LD)
Kern et al., Leukemia 2009;23:1361-1364

AML with limited differentiation (AML-LD)
Kern et al., Leukemia 2009;23:1361-1364

AML with limited differentiation (AML-LD)
Kern et al., Leukemia 2009;23:1361-1364

Patient cohort of present GEP study
n
AML-LD 27
AML with NPM1 type A mutation and without cytogenetic abnormalities,
no AML-LD immunophenotype (NPM1-A) 24
AML with NPM1 mutation other than type A and without cytogenetic
abnormalities, no AML-LD immunophenotype (NPM1-other) 12
AML without NPM1 mutation and with normal karyotype,
no AML-LD immunophenotype (AML-NK) 30
Acute promyelocytic leukemia (APL) 15

Cluster analysis, four groups (excluding APL)
..
AML-LD

Cluster analysis, five groups (including APL)
AML-LD
APL

Diagnosis of BAL
Points B-cell lineage T-cell lineage myeloid lineage
2 CD79a cy/sCD3 Anti-MPO
2 cyIgM Anti-TCRαβ
2 cyCD22 Anti-TCRγδ
1 CD19 CD2 CD13
1 CD10 CD5 CD33
1 CD20 CD8 CD65
1 CD10 CD117
0,5 TdT TdT CD14
0,5 CD24 CD7 CD15
0,5 CD1a CD64
BAL: Score >2 for myeloid and B- or T-lymphatic

Diagnosis of MPAL

Immunophenotyping in acute leukemias
Determination of cell size and heterogeneity
Analysis of expression of multiple antigens on one cell
Characterization of cell populations by antigen
expression pattern
Quantification of cell populations

Definition of MDS
Group of myeloid neoplasms
Bone marrow failure with peripheral cytopenia
Morphologic dysplasia in one or more of the following hematopoieticcell lineages:(i) erythroid cells (also ringed sideroblasts >15% considered diagnostic)(ii) neutrophils and their precursors(iii) megakaryocytes

Prognosis in MDS
Points
0 0.5 1 1.5 2
% bone marrow blasts 5 5-10 11-20 21-30
Karyotype favorable intermediate unfavorable
Cytopenias 0/1 2/3
Karyotype favorable: normal, -Y, del(5q), del(20q)
Karyotype unfavorable: complex aberrant (≥3 aberrations), aberrations of chromosome 7
Points 0 0.5 to 1.0 1.5 to 2.0 ≥2.5
Risk group Low Int-1 Int-2 High

Minimal diagnostic criteria in MDS
(A) Prerequisite criteriaConstant cytopenia in one or more of the following cell lineages:
erythroid (hemoglobin <11 g/dl) orneutrophilic (ANC < 1,500/µl) ormegakaryocytic (platelets <100,000/µl)
Exclusion of all other hematopoietic or non-hematopoietic disorders asprimary reason for cytopenia/dysplasia
(B) MDS-related (decisive) criteriaDysplasia in ≥10% of all cells in one of the following lineages in bone marrow smear:
erythroid orneutrophilic ormegakaryocytic or>15% ringed sideroblasts (iron stain)
5–19% Blast cells in bone marrow smears
Typical chromosomal abnormality (by conventional karyotyping or FISH)
MDS: both (A) criteria and one (B) criterion
Valent et al., Leuk Res 2007;31:727-736

Minimal diagnostic criteria in MDS
(A) Prerequisite criteriaConstant cytopenia in one or more of the following cell lineages:
erythroid (hemoglobin <11 g/dl) orneutrophilic (ANC <1,500/µl) ormegakaryocytic (platelets <100,000/µl)
Exclusion of all other hematopoietic or non-hematopoietic disorders asprimary reason for cytopenia/dysplasia
(C) Co-criteriaAbnormal phenotype of bone marrow cells clearly indicative of a monoclonal population of erythroid or/and myeloid cells, determined by flow cytometry
Clear molecular signs of a monoclonal cell population in HUMARA assay, gene chip profiling, or point mutation analysis (e.g. RAS mutations)
Markedly and persistently reduced colony-formation (±cluster formation) of bone marrow or/and circulating progenitor cells (CFU-assay)
Highly suspective of MDS: both (A) criteria and one (C) criterion
Valent et al., Leuk Res 2007;31:727-736

Idiopathic cytopenia of uncertain significance (ICUS)
(A) DefinitionCytopenia in one or more of the following cell lineages (for ≥6months): erythroid (Hb <11 g/dl)
neutrophilic (<1,500/µl)platelet (<100,000/µl)
MDS excluded (see ‘B’ and ‘C’)All other causes of cytopenia also excluded (see ‘B’ and ‘C’)
(B) Initial investigations required to establish the diagnosis of ICUSDetailed case history (toxins, drugs, mutagenic events, etc.)Thorough clinical investigations including X-ray and sonography of spleenDifferential blood count (microscopic) and complete serum chemistryBone marrow histology and immunohistochemistryBone marrow smear including an iron stainFlow cytometry of bone marrow and peripheral blood cellsChromosome analysis including FISHMolecular analysis where appropriate (e.g. T cell receptor rearrangement—
neutropenia)Exclusion of viral infections (HCV, HIV, CMV, EBV, others)
(C) Recommended investigations in the follow-upBlood count and differential count as well as serum chemistry (1–6 months)Suspicion for MDS becomes evident: bone marrow examination
Valent et al., Leuk Res 2007;31:727-736

ELN working conference
Arjan A van de Loosdrecht, Canan Alhan, Marie Christine Béné, Matteo G
Della Porta, Angelika M Dräger, Jean Feuillard, Patricia Font, Ulrich Germing,
Detlef Haase, Christa H Homburg, Robin Ireland, Joop H Jansen, Wolfgang
Kern, Luca Malcovati, Jeroen G te Marvelde, Gulham J Mufti, Kiyoyuki Ogata,
Alberto Orfao, Gert J Ossenkoppele, Anna Porwit, Frank W Preijers, Steve
Richards, Gerrit Jan Schuurhuis, Dolores Subirá, Peter Valent, Vincent HJ van
den Velden, August H Westra, Theo M de Witte, Denise A Wells, Michael
Loken, Theresia M Westers
Amsterdam, March 27/28 2008Munich, October 29/30 2009London, November 5/6 2010Pavia, November 4/5 2011

Evaluation of MFC in MDS
Wells et al. Blood 2003
115 pts. with MDS, 104 pts. with various disorders, 25 healthy donors
Van de Loosdrecht et al. Blood 2008
50 pts. with MDS, 15 healthy volunteers, 3 pts. undergoing surgery
Kern et al. Cancer 2010
1013 pts. with suspected MDS

Parameters scored as aberrant in immature compartment
van de Loosdrecht et al., Haematologica 2009;94:1124-1134

Quantification of myeloblasts
Cytomorphology vs. MFC
Mean 4.67±4.18 vs. 3.78±2.97, r=0.362, p<0.001
Kern et al., Cancer 2010

Differential using CD45-SSC-Gate
Immunophenotyping6% blasts
Cytomorphology18% blasts
Kern et al., Cancer 2010

Differential using CD45-SSC-Gate
Cytomorphology18% blasts
Immunophenotyping14% monocytic cells
Immunophenotyping6% blasts
Kern et al., Cancer 2010

Parameters in maturing myeloid and monocytic compartment
van de Loosdrecht et al., Haematologica 2009;94:1124-1134

CD13/CD16 expression pattern in granulocytes
Normal BM MDS
Kern et al., Cancer 2010

CD11b/CD16 expression pattern in granulocytes
Normal BM MDS
Kern et al., Cancer 2010

Aberrant antigen expression in granulocytes
MFC findings Cytomorphologic findings p-value
No MDS(n=277)
MDS(n=511)
Suspected MDS(n=225)
Abnormal CD13/CD16
25 (9.0%) 219 (42.9%) 54 (24.0%) <0.001
Abnormal CD11b/CD16
9 (3.2%) 143 (28.0%) 25 (11.1%) <0.001
CD56+ 10 (3.6%) 90 (17.6%) 23 (10.2%) <0.001
CD33- 18 (6.5%) 53 (10.4%) 19 (8.4%) n.s.
CD64- 0 14 (2.7%) 8 (3.6%) 0.011
# of aberrant antigens
0.0±0.21,2 0.2±0.61 0.1±0.62 1<0.00120.003
Reduced SSC signal 14 (5.1%) 286 (56.0%) 42 (18.7%) <0.001
SSC-ratio G:L (mean±SD)
7.47±1.091,2 6.55±2.321 7.38±1.172 1<0.0012n.s.
Kern et al., Cancer 2010

Aberrant antigen expression in granulocytes
406 cases without dysgranulopoiesis by cytomorphology
aberrant CD13/CD16 expression pattern 104 (25.6%)
aberrant CD11b/CD16 expression pattern 62 (15.3%)
CD56 expression 38 (9.4%)
lack of CD33 expression 44 (10.8%)
lack of CD64 expression 2 (0.5%)
Aberrant expression ≥2 antigens
RA 16/31 (51.6%)
RARS 15/27 (55.6%)
Kern et al., Cancer 2010

Parameters scored as aberrant in erythroid compartment
van de Loosdrecht et al., Haematologica 2009;94:1124-1134

Proposed marker combinations
van de Loosdrecht et al., Haematologica 2009;94:1124-1134

Example of a screening panel for 4-color floy cytometry
van de Loosdrecht et al., Haematologica 2009;94:1124-1134

MDS 10 color panelBlast/Granulocyte
TubeMonocyte/Erythroid
TubeLymphatic/Granulocyte
Tube
FITC CD14 CD71 CD7
PE CD13 CD2 CD10
ECD CD38 CD64 CD8
PC5.5 CD123 CD56 CD5
PC7 CD117 CD117 CD4
APC CD11b CD36 CD3
APC-Alexa Fluor 700 CD34 CD34 CD34
APC-Alexa Fluor 750 CD33 CD33 CD19
Pacific Blue CD16 HLA-DR CD15
Krome Orange CD45 CD45 CD45

List of pathological controls to determine the specificity
van de Loosdrecht et al., Haematologica 2009;94:1124-1134

Recommended minimal requirements to assess MDS by MFC
Westers et al., Leukemia 2012
BONE MARROW SUBSET RECOMMENDED ANALYSES
Erythroid compartment* % of nucleated erythroid cellsrelation CD71 and CD235aexpression of CD71expression of CD36expression of CD117
Immature myeloid and monocytic progenitors % of cells in nucleated cell fraction**;expression of CD45;expression of CD34;expression of CD117;expression of HLA-DR;expression of CD13 and CD33; asynchronous expression of CD11b, CD15;expression of CD5, CD7, CD19, CD56***;
Maturing neutrophils % of cells as ratio to lymphocytesSSC as ratio vs. SSC of lymphocytesrelation of CD13 and CD11b relation of CD13 and CD16 relation CD15 and CD10
Monocytes % of cells as ratio to lymphocytesrelation of HLA-DR and CD11b relation of CD36 and CD14expression of CD13 and CD33;expression of CD56***
Progenitor B cells enumeration as fraction of total CD34+based on CD45/CD34/SSC in combination with CD10 or CD19

Diagnostic results in MFC and cytomorphology
1,013 patients with cytopenias and suspected MDS analyzed
Non-MDS malignancies excluded
MFC Cytomorphology
MDS no MDS suspected MDS
MDS 382 (74.8%) 13 (4.7%) 51 (22.7%)
no MDS 129 (25.2%) 264 (95.3%) 174 (77.3%)
Total 511 (100%) 277 (100%) 225 (100%)
Overall concordance 646/788 (82.0%)
Kern et al., Cancer 2010

Numbers of aberrantly expressed antigens
Kern et al., Cancer 2010
Cytomorphology: no MDS
Cytomorphology: suspected MDS
Cytomorphology: MDS

Diagnostic results in MFC and cytogenetics
MFC Cytogenetics
aberrant karyotype normal karyotype
MDS 189 (77.1%) 257 (33.5%)
no MDS 56 (22.9%) 511 (66.5%)
Total 245 (100%) 768 (100%)
Kern et al., Cancer 2010

Results in MFC, Cytomorphology, Cytogenetics
25 cases with aberrant karyotype and without clear-cut MDS
MFC Cytomorphology
no MDS suspected MDS
MDS 6 (50.0%) 11 (47.8%)
no MDS 6 (50.0%) 12 (52.2%)
Total 12 (100%) 23 (100%)
Kern et al., Cancer 2010

Correlation Immunophenotyping and Cytomorphology
Wells et al., Blood 2003;102:394-403

Correlation Immunophenotyping and Cytomorphology
van de Loosdrecht et al., Blood 2008;111:1067-1077

Correlation of MFC with cytogenetics and IPSS
van de Loosdrecht et al., Blood 2008;111:1067-1077

Correlation of MFC with IPSS
2
2,5
3
3,5
4
4,5
0 0,5 1 1,5 2 2,5 3
IPSS
Ab
erra
ntl
y ex
pre
ssed
an
tig
ens
(mea
n)
Kern et al., Cancer 2010

Correlation of MFC with outcome following allogeneic Tx
Wells et al., Blood 2003;102:394-403

Correlation of MFC with outcome
Survival after diagnosis
6-year-OS 68% vs. 100%p=0.008
Kern et al., Cancer 2010

IPSS low (n=309)
IPSS lnt-1 (n=435)
IPSS lnt-2 (n=112)
IPSS high (n=23)
IPSS low vs. IPSS Int-2: p=0.001
IPSS low vs. IPSS high: p=0.000
IPSS Int-1 vs. IPSS Int-2: p=0.001
IPSS Int-1 vs. IPSS high: p=0.000
OS according to IPSS
Kern et al., 11th Int. Symposium on MDS, Edinburgh, UK, 2011

OS according to number of aberrantly expressed antigens
OS according to flow score
Flow score=0 (n=463)
Flow score=1 (n=520)
Flow score 0 vs. 1: p=0.001
0-1 (n=492)
2-4 (n=395)
0-1 vs. 2-4: p=0.004
0-1 vs. >4: p<0.001
>4 (n=94)
OS according to MFC
Kern et al., 11th Int. Symposium on MDS, Edinburgh, UK, 2011

Cytomorphology MFC
MDS suspected (n=217)
MDS excluded (n=274)
MDS (n=493)
MDS vs. MDS suspected: p=0.095
MDS vs. MDS excluded: p=0.070
No MDS (n=554)
MDS (n=430)
MDS vs. No MDS: p<0.001
OS according to diagnostic result
Kern et al., 11th Int. Symposium on MDS, Edinburgh, UK, 2011

Cytomorphology: no MDS Cytomorphology: MDS
No MDS (n=124)
MDS (n=369)
MDS vs. No MDS: p=0.013
No MDS (n=261)
MDS (n=13)
MDS vs. No MDS: p=0.012
OS according to diagnostic result by MFC
Kern et al., 11th Int. Symposium on MDS, Edinburgh, UK, 2011

Flow score=0 (n=115)
Flow score=1 (n=378)
Flow score 0 vs. 1: p=0.008
0-1 (n=117)
2-4 (n=293)
0-1 vs. >4: p=0.009
>4 (n=82)
OS in cases with MDS by cytomorphology
OS according to number of aberrantly expressed antigens
OS according to flow score
Kern et al., 11th Int. Symposium on MDS, Edinburgh, UK, 2011

OS according to IPSS CG OS in IPSS CG=0.0
IPSS CG 0,0 (n=855)
IPSS CG 0,5 (n=95)
IPSS CG 1,0 (n=10)
IPSS CG 1,0 vs. IPSS CG 0,0: p=0.000
IPSS CG 1,0 vs. IPSS CG 0,5: p=0.000
No MDS (n=533)
MDS (n=322)
MDS vs. No MDS: p=0.003
OS according to diagnostic result by MFC
Kern et al., 11th Int. Symposium on MDS, Edinburgh, UK, 2011

OS in IPSS CG=0.5 OS in IPSS CG=1.0
MDS (n=77)
No MDS (n=18)
MDS vs. No MDS: n.s.
No MDS (n=3)
MDS (n=31)
MDS vs. No MDS: n.s.
OS according to diagnostic result by MFC
Kern et al., 11th Int. Symposium on MDS, Edinburgh, UK, 2011

in IPSS CG=0.0
OS according to number of aberrantly expressed antigens
in IPSS CG=0.5 in IPSS CG=1.0
>4 (n=19)
2-4 (n=62)
n.s.
0-1 (n=4)
2-4 (n=27)
>4 (n=3)
2-4 vs. >4: p=0.006
0-1 (n=474)
2-4 (n=306)
0-1 vs. >4: p=0.000
2-4 vs. >4: p=0.016
>4 (n=72)
OS in cytogenetic subgroups
Kern et al., 11th Int. Symposium on MDS, Edinburgh, UK, 2011

Flow score=0 (n=444)
Flow score=1 (n=410)
Flow score 0 vs. 1: p=0.004
Flow scor =0 (n=15)
Flow score=1 (n=80)
Flow score 0 vs. 1: n.s.ge25ssc63 =1 (n=30)
Flow score=0 (n=4)
Flow score 0 vs. 1: n.s.
OS according to flow score in IPSS CG=0.0
OS according to flow score in IPSS CG=0.5
OS accordingto flow score inIPSS CG=1.0
OS in cytogenetic subgroups
Kern et al., 11th Int. Symposium on MDS, Edinburgh, UK, 2011

Conclusions
MFC may significantly add to the present standard diagnostic
work-up of suspected MDS by CM and CG
The diagnostic result by MFC and the degree of aberrancies
detected by MFC may be used to estimate prognosis and
to stratify patients
Additional studies should be performed applying CM, CG and
MFC in parallel to further validate these findings















![Therapy-related Myeloid Neoplasms Following …Radiation therapy & t-MN • Have modern RT techniques [mega-voltage linear accelerators; intensity-modulated radiation therapy (IMRT)]](https://img.pdfslide.us/doc/110x75/5ed204196731c53a5734c2cd/therapy-related-myeloid-neoplasms-following-radiation-therapy-t-mn-a-have.jpg)