Embed Size (px)
Citation preview

INTRODUCTIONIn the mid-1990s, the issue of sludge in totally implanted vascular access ports was a topical issue. Investigation at that time, by the primary author of this poster, demonstrated that sludge existed yet the relationship of sludge to complications such as intravascular device-related bloodstream infection, occlusion, and patient outcomes were not studied.
Personal conversation, a review of pertinent literature and information on the internet about partial vascular access device occlusion motivated the primary author to investigate the issue of sludge once again. He shared his study design with his co-authors and the study was begun to answer:
Does sludge exist in todays vascular access ports?
METHODSA mailing was sent to the AVA membership describing the study and requesting that explanted ports be sent to Norfolk Medical for examination. All HIPAA guidelines were followed. An incentive was offered for each implanted port (illustrated in the pictures below).A prepaid return envelope along with appropriate packaging in keeping with regulations on handling and transportation of biohazardous waste was supplied on request to participants. In addition a kit with gloves, scalpel, biohazard bag, and cotton swabs were supplied.Participants were asked to complete a form identifying the port (if possible), the date of implantation, and the date of removal.Upon receipt of an explanted port(s), a photograph was taken. The port septum was then removed and photographs were taken of the septum and port chamber. Gross inspection of the port chamber was also performed and observations recorded.Explanted ports were received between March 2012 and September 2012. A report with photos of the removed septum and port chamber was sent to the participant for their records along with the appropriate incentive.
P74Does Sludge / Debris Exist in Today’s Vascular Access PortsMike Dalton, MSIA, Jim Lacy, BSN, RN, VA-BC, CRNI, Natan Pheil, BSBE7350 N. Ridgeway, Skokie, IL 60076
(847) 674-7075
Norfolk MedicalTM
Fig. 3 Implantation time: 2.5 years Ohio
Implanted 1 yearCanada
ABOUT THE AUTHORSMichael Dalton is the President and CEO of Norfolk Medical, Inc. As a R&D engineer, he developed several of the most popular implanted vascular access ports used over the past 20 years.
Jim Lacy is a Clinical Marketing Consultant and Principal of Clinmarked, LLC with many years experience in vascular access.
Natan Pheil is an engineer and employee of Norfolk Medical, Inc.The authors have no conflict of interest in performing this study. The study was completely funded by Norfolk Medical, Inc.
QUOTES FROM THE LITERATUREWhitman (1995)
“The most predictive culture specimen in a potentially infected port is the thrombotic material inside the reservoir.” 10
Douard (1999)“The infected deposits that accumulate under the VAP [Vascular
Access Port] septum are the source of VAP-BSI.” 5 Longuet (2001
“This pilot study found that the reservoir is the key piece of the catheter involved in VAP-related bacteremia.” 9
CONCLUSIONSSludge does occur in todays’ ports. The occurrence of sludge in implanted vascular ports may have a great impact on patient outcomes as well as patient satisfaction. A randomized prospective clinical study should be undertaken to determine: 1. The makeup of sludge 2. Risks associated with sludge formation related to intravascular device-related infection, thrombotic and non-thrombotic partial and complete occlusion 3. Best practices for flushing and locking implanted ports
The authors would encourage AVA, in partnership with implanted port manufacturers to take the lead in determining the significance of sludge and its effects on patient outcomes – clinically and from a cost standpoint.
1. O’Grady NP, Alexander M, Burns LA, et al. Guidelines for the prevention of intravascular catheter-related infections. American journal of infection control. May 2011;39(4 Suppl 1):S1-34.2. Athale UH, Siciliano S, Cheng J, Thabane L, Chan AK. Central venous line dysfunction is an independent predic tor of poor survival in children with cancer. Journal of pediatric hematology/oncology. Apr 2012;34(3):188-193.3. Bucki B, Tomaszewska R, Karpe J, Stoksik P, Sonta-Jakimczyk D, Szczepanski T. Central venous access ports in children treated for hematopoietic malignancies. Pediatric hematology and oncology. Dec 2008;25(8):751-755.4. Royle TJ, Davies RE, Gannon MX. Totally implantable venous access devices - 20 years’ experience of implantation in cystic fibrosis patients. Annals of the Royal College of Surgeons of England. Nov 2008;90(8):679-684.5. Douard MC, Arlet G, Longuet P, et al. Diagnosis of venous access port-related infections. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. Nov 1999;29(5):1197-1202.6. Moureau N, Poole S, Murdock MA, Gray SM, Semba CP. Central venous catheters in home infusion care: outcomes analysis in 50,470 patients. Journal of vascular and interventional radiology : JVIR. Oct 2002;13(10):1009-1016.7. deSwarte J. Experience with Residue in the Reservoirs of Implanted Ports. Journal of Vascular Access Networks. 1993;3(3):16-18.8. Herbst S. Accumulation of Blood Products and Drug Precipitates in VADs: A Set Up for Trouble. Journal of Vascular Access Networks. 1993;3(3):9-13.9. Longuet P, Douard MC, Arlet G, Molina JM, Benoit C, Leport C. Venous access port related bacteremia in patients with acquired immunodeficiency syndrome or cancer: the reservoir as a diagnostic and therapeutic tool. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. Jun 15 2001;32(12):1776-1783.10. Lorch H, Zwaan M, Kagel C, Weiss HD. Central venous access ports placed by interventional radiologists: experience with 125 consecutive patients. Cardiovascular and interventional radiology. May-Jun 2001;24(3):180-184.11. Nishinari K, Wolosker N, Bernardi CV, Yazbek G. Totally implantable ports connected to valved catheters for chemotherapy: experience from 350 Groshong devices. The journal of vascular access. Jan-Mar 2010;11(1):17-22.12. Suslu H, Arslan G, Tural K. [Venous port implantation in adult patients: retrospective evaluation]. Agri : Agri. 2012;24(1):32-36.13. Whitman ED, Boatman AM. Comparison of diagnostic specimens and methods to evaluate infected venous access ports. American journal of surgery. Dec 1995;170(6):665-669; discussion 669-670.14. Zhang Q, Jiao L, Zhou H. Comparison of implantable central venous ports with catheter insertion via external jugular cut down and subclavian puncture in children: single center experience. Pediatric surgery international. Jun 2009;25(6):499-501.15. Shannon RP, Patel B, Cummins D, Shannon AH, Ganguli G, Lu Y. Economics of central line associated bloodstream infections. American journal of medical quality : the official journal of the American College of Medical Quality. Nov-Dec 2006;21(6 Suppl):7S-16S.
References
For more information or a reprint of this poster contact:Mike Dalton: [email protected]
or Jim Lacy: jim.lacy@clinmarked
The study was undertaken as a limited uncontrolled study. There were no exclusion criteria. Explanted ports were received from several US states and Canada. The results of this study indicate: 1. Sludge does indeed exist – 18.6 % of explanted vascular access ports examined had sludge in the port chamber
2. Sludge was found in ports from all manufacturers submitted in the study
3. Sludge does not have a common appearance – Gross examination revealed that some sludge is dull and irregular, some bright and smooth with evidence of what appears to be crystals as well as irregularly colored and white “areas” within the sludge
RESULTS
LIMITATIONS
DISCUSSION
The study was undertaken by a private organization and more than 1,000 requests to participate were mailed to AVA members and others. Participation (explanted ports sent to us) represented 0.1% of the total mailing.
No data was gathered with the exception of 1) implantation time prior to removal and 2) Results were documented with photographs and report of findings on gross inspection.
Concern, prevalence and prevention of intravascular device-related infection has been at the forefront of clinical research for more a decade.1 A correlation between thrombotic complications and infection is accepted though not well studied.2-5 A review of the literature shows rates of partial occlusion of up to 33%, and total occlusion up to 28% in implanted vascular ports.2-14 Occlusion is the most frequent of all complications resulting in delays in treatment, rehospitalization and treatment with thrombolytics or device replacement.2-4,6,9-12,14 Sludge as risk factor for infection and occlusion has not been well studied and is mentioned in only 5 articles in our review.5,7-9,13 The cost of Intravascular Device-Related Infection is high, yet we were unable to find cost data related to port dysfunction and occlusion.1,15 The authors noted a paucity of implanted vascular port studies in the literature in the last 10 years, studies undertaken focus on implantation related complications rather than overall patient complications such as occlusion and infection.
sludge - noun \ˈsləj\A slushy mass, deposit, or sediment. In totally implanted vascular access ports - a build-up of
blood clot, fibrin, blood components, drug and mineral precipitate or residue and lipid.
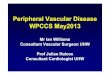
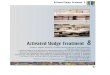
EXAMPLES OF EXPLANTED PORTS RECEIVED FOR STUDY
Ports with sludge
Ports without sludge
Fig. 4 Implantation time: 5+ years Louisiana
Fig. 5 Implantation time: 9 years Arkansas
Fig. 3 Implantation time: 1 year Canada
Fig. 7 Implantation time: 14 years Ohio
Fig. 8 Implantation time: 5 years Ohio
Fig. 9 Implantation time: unknown Ohio