Embed Size (px)
Citation preview
Non-‐Vitamin K Oral an/coagulants (NOACs)
in clinical prac/ce
Sco$ C. Woller, MD Co-‐Director, Thrombosis Program
Intermountain Medical Center Associate Professor of Medicine
University of Utah School of Medicine
Central Region Primary Care Clinical Program Learning Day Intermountain Medical Center 20 February 2015
Disclosures
• Poten/al Financial COI: – Inves/gator ini/ated grant recipient: Bristol-‐Myers-‐Squibb (paid to Intermountain Healthcare)
• Poten/al Intellectual COI: – Panelist American College of Chest Physicians (ACCP) Clinical Prac/ce Guideline: An/thrombo/c therapy for venous thromboembolic disease (AT10)
Objec/ves • Advances in warfarin management in iCentra – An#coagula#on Management Suite
• The Non-‐Vitamin K Oral an/coagulants (NOACs) – Atrial fibrilla/on – Venous thromboembolism – Choice of drug
• Peri-‐procedural interrup/on of the NOACs • Transi/on from: – NOAC → warfarin – Warfarin → NOAC
Transi/ons
HELP2 Cerner iCentra AnCcoagulaCon Management Suite
• Ini/a/on • Rou/ne warfarin dose adjustment • Peri-‐procedural management • Inpa/ent / outpa/ent transi/on of care • Feedback on performance • Iden/fica/on of candidates for alterna/ve therapy
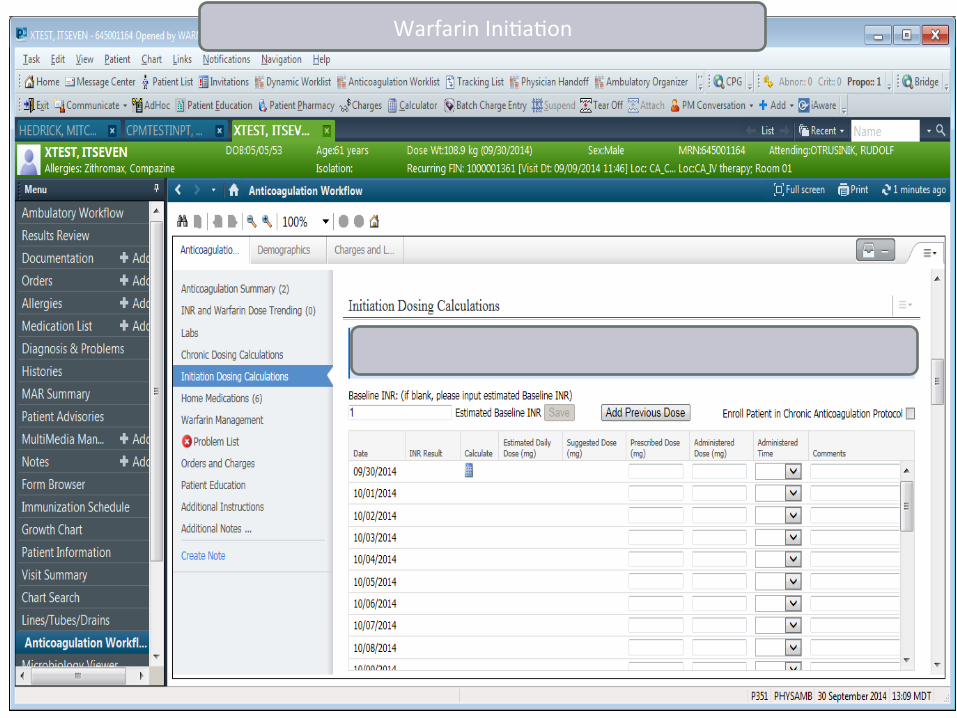
Warfarin Ini/a/on
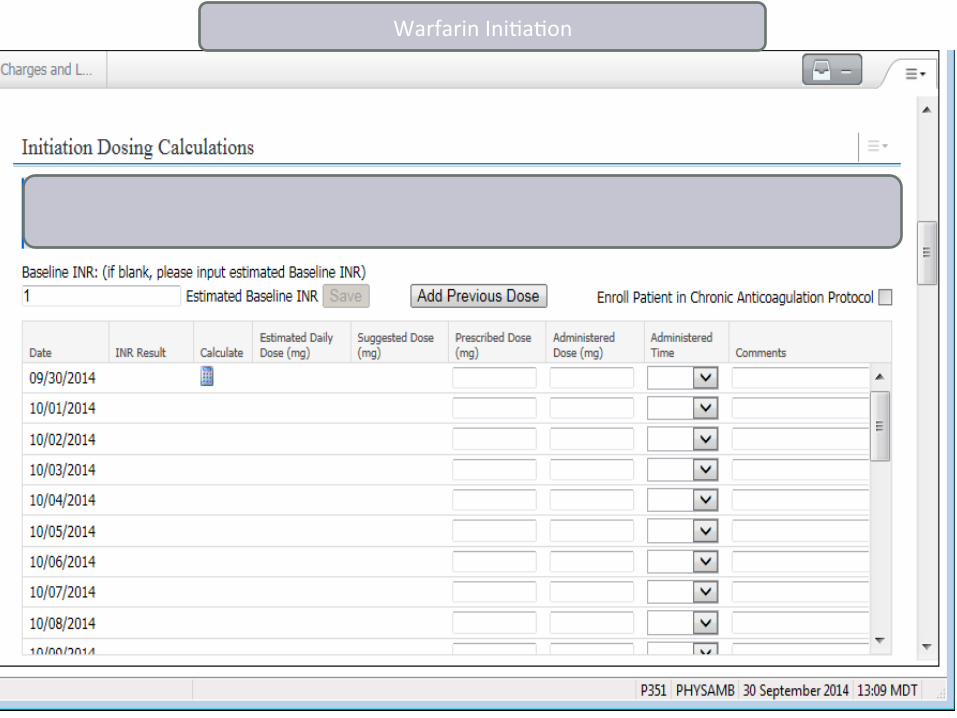
Warfarin Ini/a/on
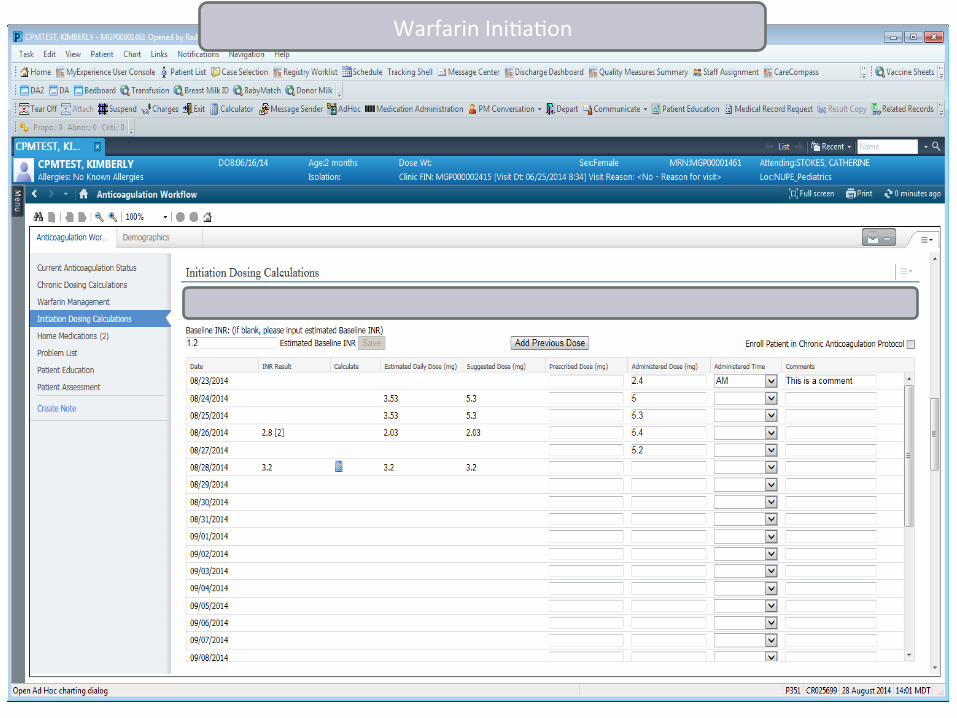
Warfarin Ini/a/on
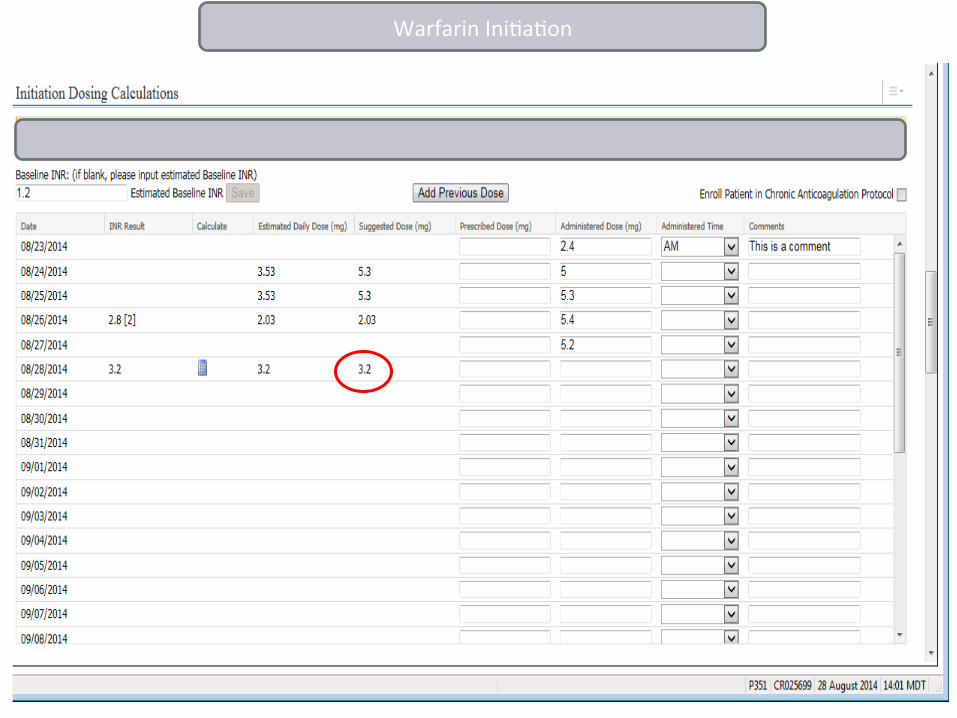
Warfarin Ini/a/on
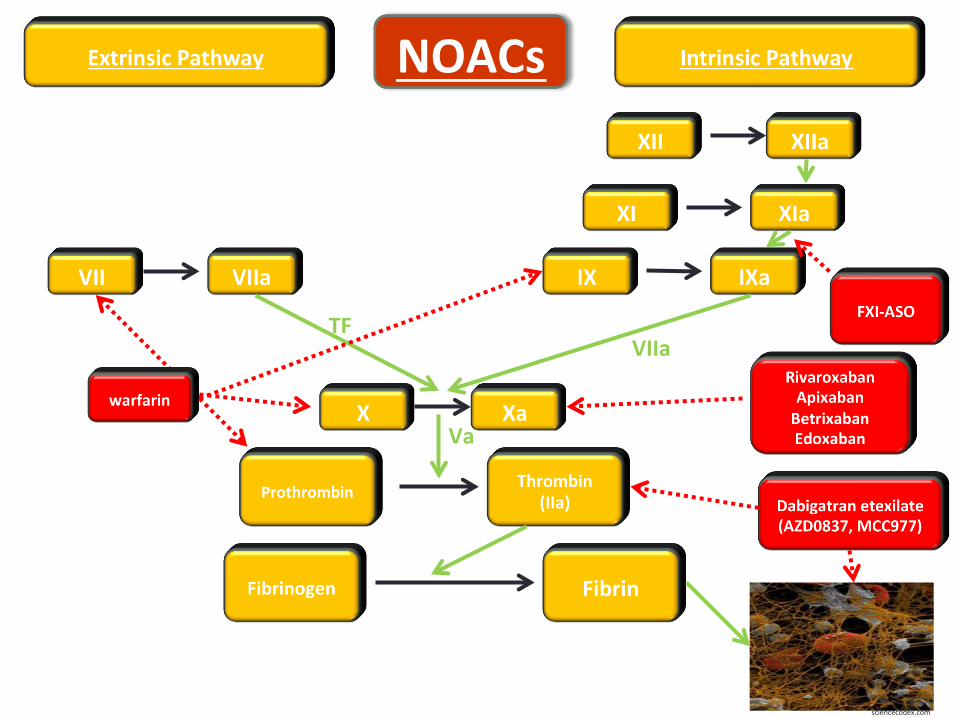
TF
Va
VIIa
sciencecodex.com
NOACs
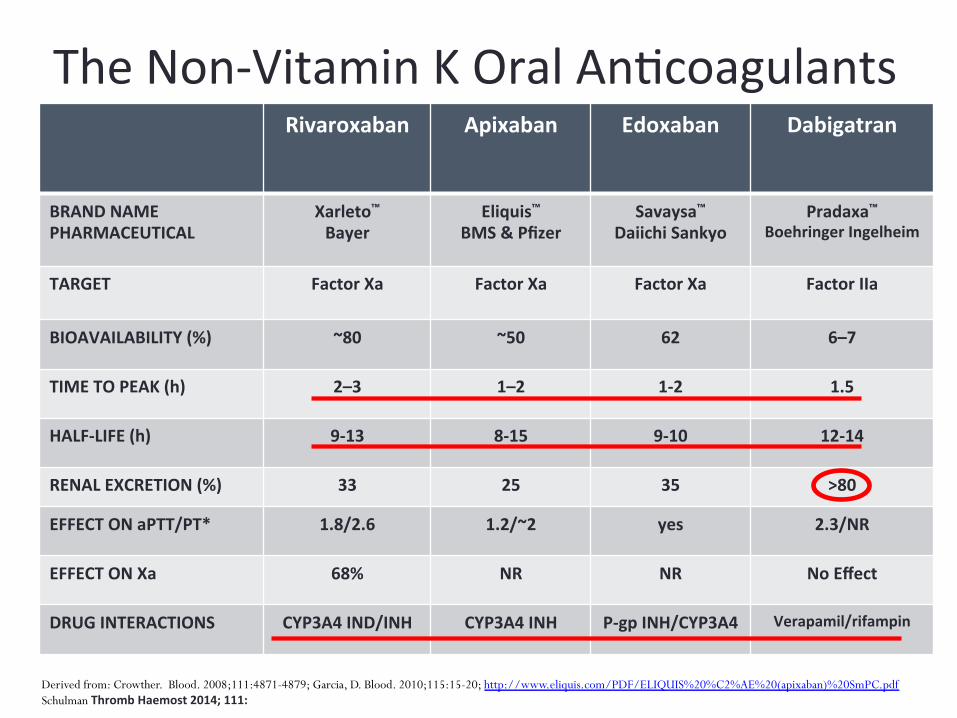
The Non-‐Vitamin K Oral An/coagulants Rivaroxaban Apixaban Edoxaban Dabigatran
BRAND NAME PHARMACEUTICAL
Xarleto™ Bayer
Eliquis™ BMS & Pfizer
Savaysa™ Daiichi Sankyo
Pradaxa™ Boehringer Ingelheim
TARGET Factor Xa Factor Xa Factor Xa Factor IIa
BIOAVAILABILITY (%) ~80 ~50 62 6–7
TIME TO PEAK (h) 2–3 1–2 1-‐2 1.5
HALF-‐LIFE (h) 9-‐13 8-‐15 9-‐10 12-‐14
RENAL EXCRETION (%) 33 25 35 >80
EFFECT ON aPTT/PT* 1.8/2.6 1.2/~2 yes 2.3/NR
EFFECT ON Xa 68% NR NR No Effect
DRUG INTERACTIONS CYP3A4 IND/INH CYP3A4 INH P-‐gp INH/CYP3A4 Verapamil/rifampin
Derived from: Crowther. Blood. 2008;111:4871-4879; Garcia, D. Blood. 2010;115:15-20; http://www.eliquis.com/PDF/ELIQUIS%20%C2%AE%20(apixaban)%20SmPC.pdf Schulman Thromb Haemost 2014; 111:
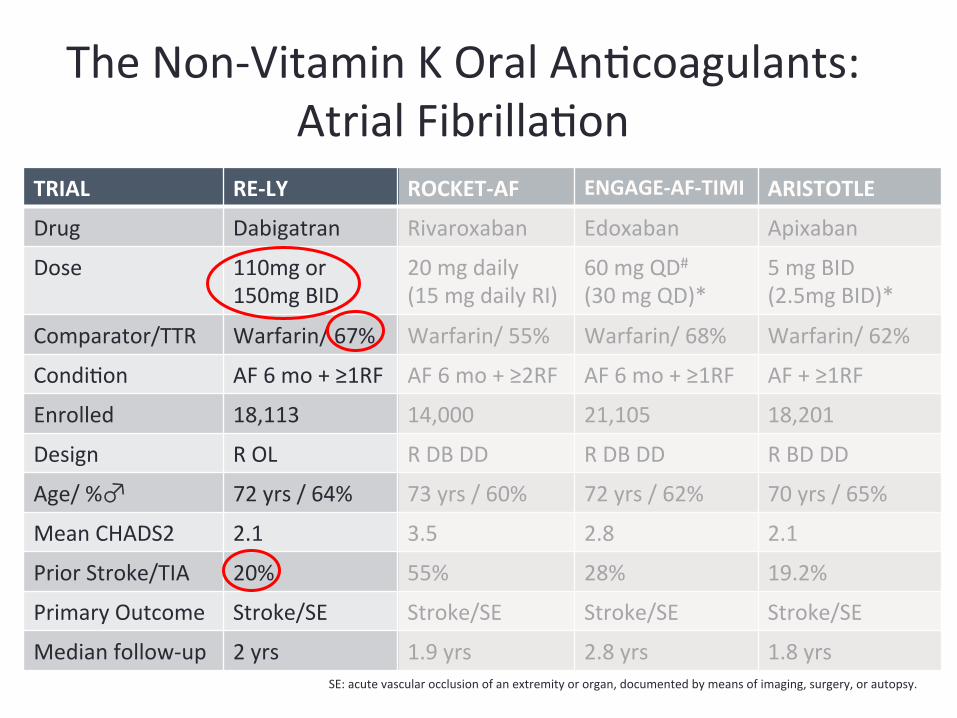
TRIAL RE-‐LY ROCKET-‐AF ENGAGE-‐AF-‐TIMI ARISTOTLE
Drug Dabigatran Rivaroxaban Edoxaban Apixaban
Dose 110mg or 150mg BID
20 mg daily (15 mg daily RI)
60 mg QD#
(30 mg QD)* 5 mg BID (2.5mg BID)*
Comparator/TTR Warfarin/ 67% Warfarin/ 55% Warfarin/ 68% Warfarin/ 62%
Condi/on AF 6 mo + ≥1RF AF 6 mo + ≥2RF AF 6 mo + ≥1RF AF + ≥1RF
Enrolled 18,113 14,000 21,105 18,201
Design R OL R DB DD R DB DD R BD DD
Age/ %♂ 72 yrs / 64% 73 yrs / 60% 72 yrs / 62% 70 yrs / 65%
Mean CHADS2 2.1 3.5 2.8 2.1
Prior Stroke/TIA 20% 55% 28% 19.2%
Primary Outcome Stroke/SE Stroke/SE Stroke/SE Stroke/SE
Median follow-‐up 2 yrs 1.9 yrs 2.8 yrs 1.8 yrs SE: acute vascular occlusion of an extremity or organ, documented by means of imaging, surgery, or autopsy.
The Non-‐Vitamin K Oral An/coagulants: Atrial Fibrilla/on
RE-‐LY: Summary Comparison of Dabigatran to Warfarin
• Dabigatran 150 mg BID was superior to warfarin – Systemic Embolism or Stroke: RR 0.66 – ICH: RR 0.4 – Major bleeding did not differ RR 0.93
• NNT to prevent one stroke: 357 • NNT to prevent one hemorrhagic stroke: 370 • Dabigatran 75mg BID CrCl 15-‐30 mL/min
Connolly NEJM 2009;361:1139-‐51
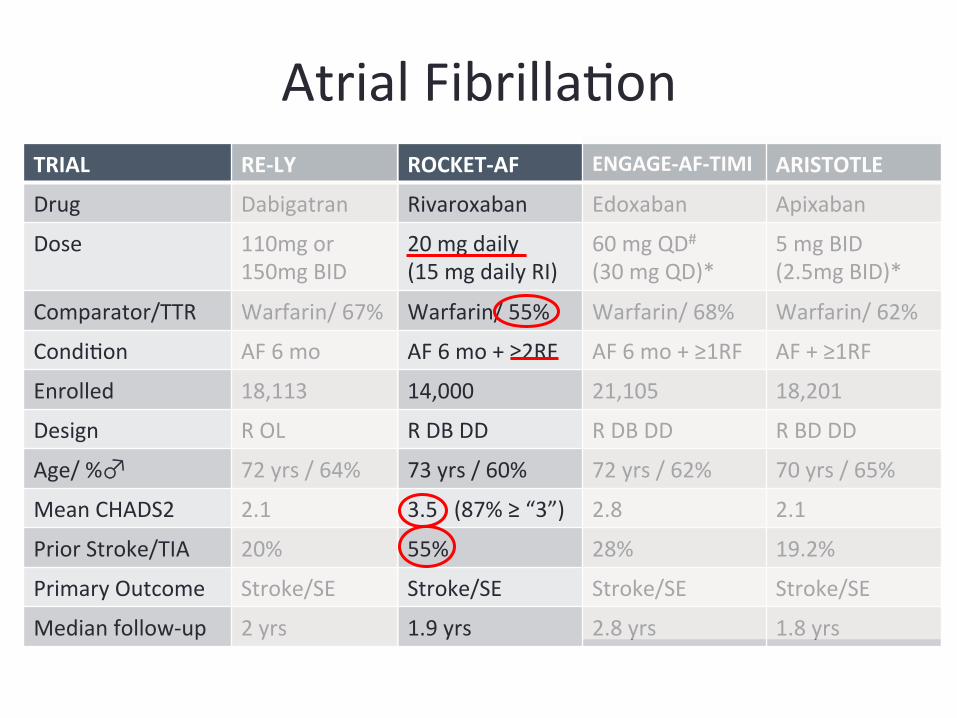
Atrial Fibrilla/on TRIAL RE-‐LY ROCKET-‐AF ENGAGE-‐AF-‐TIMI ARISTOTLE
Drug Dabigatran Rivaroxaban Edoxaban Apixaban
Dose 110mg or 150mg BID
20 mg daily (15 mg daily RI)
60 mg QD#
(30 mg QD)* 5 mg BID (2.5mg BID)*
Comparator/TTR Warfarin/ 67% Warfarin/ 55% Warfarin/ 68% Warfarin/ 62%
Condi/on AF 6 mo AF 6 mo + ≥2RF AF 6 mo + ≥1RF AF + ≥1RF
Enrolled 18,113 14,000 21,105 18,201
Design R OL R DB DD R DB DD R BD DD
Age/ %♂ 72 yrs / 64% 73 yrs / 60% 72 yrs / 62% 70 yrs / 65%
Mean CHADS2 2.1 3.5 (87% ≥ “3”) 2.8 2.1
Prior Stroke/TIA 20% 55% 28% 19.2%
Primary Outcome Stroke/SE Stroke/SE Stroke/SE Stroke/SE
Median follow-‐up 2 yrs 1.9 yrs 2.8 yrs 1.8 yrs
SE: acute vascular occlusion of an extremity or organ, documented by means of imaging, surgery, or autopsy.
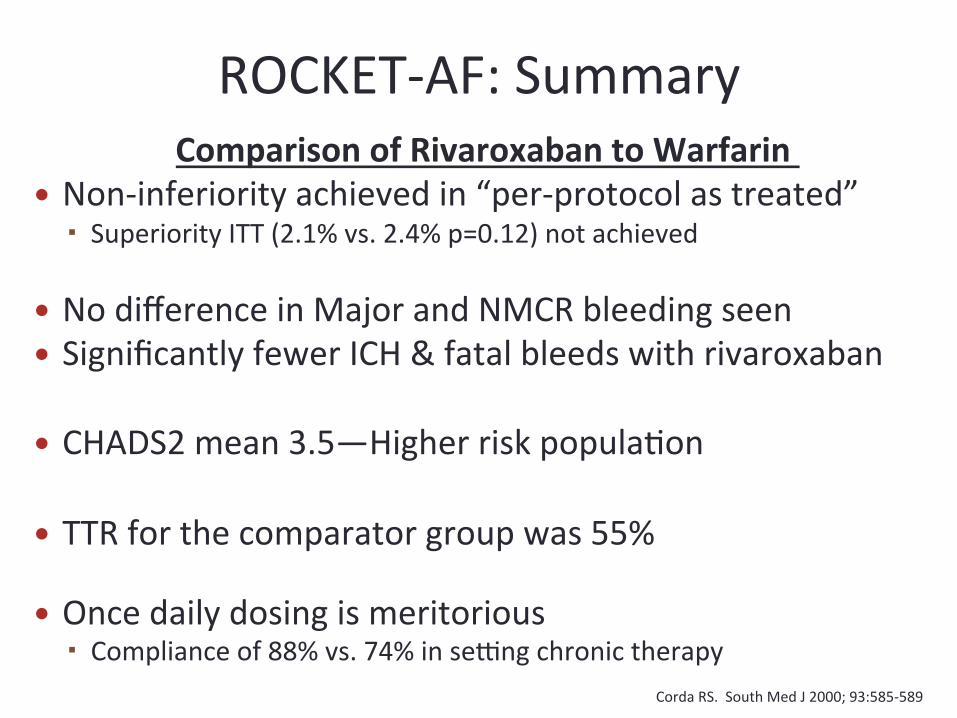
Comparison of Rivaroxaban to Warfarin � Non-‐inferiority achieved in “per-‐protocol as treated”
Superiority ITT (2.1% vs. 2.4% p=0.12) not achieved
� No difference in Major and NMCR bleeding seen � Significantly fewer ICH & fatal bleeds with rivaroxaban
� CHADS2 mean 3.5—Higher risk popula/on
� TTR for the comparator group was 55%
� Once daily dosing is meritorious Compliance of 88% vs. 74% in serng chronic therapy
Corda RS. South Med J 2000; 93:585-‐589 Patel NEJM Aug 10, 2011
ROCKET-‐AF: Summary
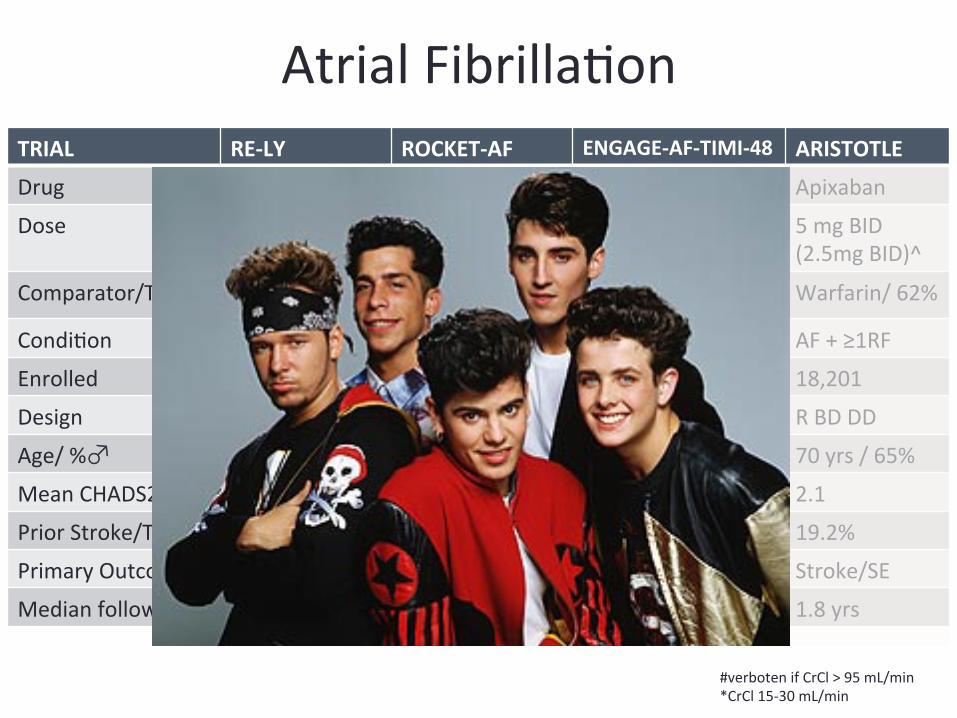
Atrial Fibrilla/on TRIAL RE-‐LY ROCKET-‐AF ENGAGE-‐AF-‐TIMI-‐48 ARISTOTLE
Drug Dabigatran Rivaroxaban Edoxaban Apixaban
Dose 110mg or 150mg BID
20 mg daily (15 mg daily RI)
60 mg QD#
(30 mg QD)* 5 mg BID (2.5mg BID)^
Comparator/TTR Warfarin/ 67% Warfarin/ 55% Warfarin/ 68% Warfarin/ 62%
Condi/on AF 6 mo AF 6 mo + ≥2RF AF 6 mo + ≥1RF AF + ≥1RF
Enrolled 18,113 14,000 21,105 18,201
Design R OL R DB DD R DB DD R BD DD
Age/ %♂ 72 yrs / 64% 73 yrs / 60% 72 yrs / 62% 70 yrs / 65%
Mean CHADS2 2.1 3.5 2.8 2.1
Prior Stroke/TIA 20% 55% 28% 19.2%
Primary Outcome Stroke/SE Stroke/SE Stroke/SE Stroke/SE
Median follow-‐up 2 yrs 1.9 yrs 2.8 yrs 1.8 yrs
#verboten if CrCl > 95 mL/min *CrCl 15-‐30 mL/min
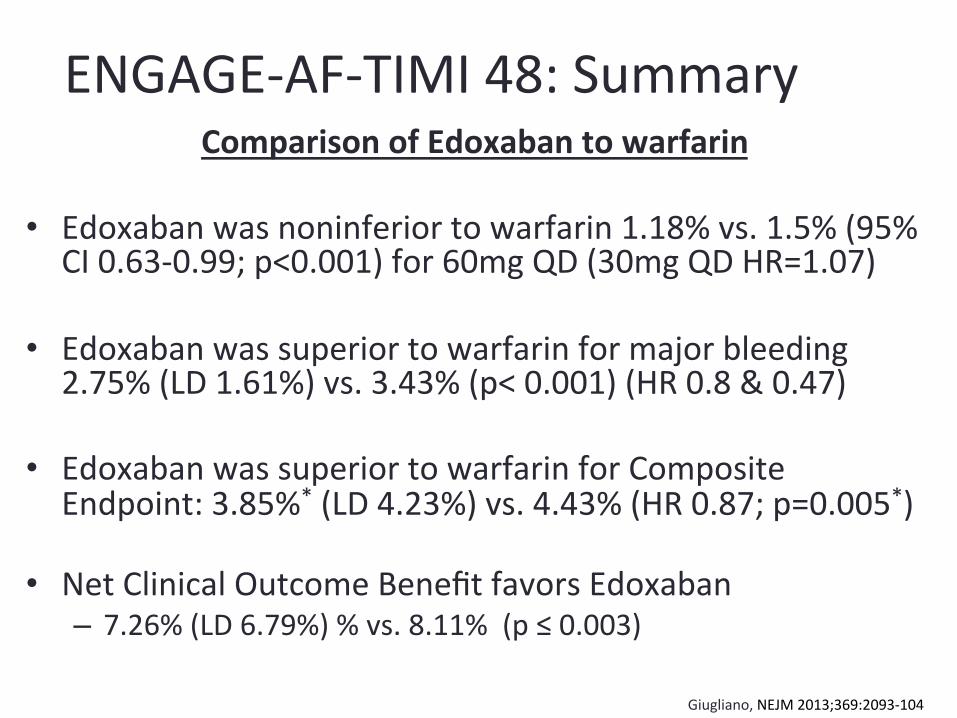
ENGAGE-‐AF-‐TIMI 48: Summary Comparison of Edoxaban to warfarin
• Edoxaban was noninferior to warfarin 1.18% vs. 1.5% (95% CI 0.63-‐0.99; p<0.001) for 60mg QD (30mg QD HR=1.07)
• Edoxaban was superior to warfarin for major bleeding 2.75% (LD 1.61%) vs. 3.43% (p< 0.001) (HR 0.8 & 0.47)
• Edoxaban was superior to warfarin for Composite Endpoint: 3.85%* (LD 4.23%) vs. 4.43% (HR 0.87; p=0.005*)
• Net Clinical Outcome Benefit favors Edoxaban – 7.26% (LD 6.79%) % vs. 8.11% (p ≤ 0.003)
Giugliano, NEJM 2013;369:2093-‐104
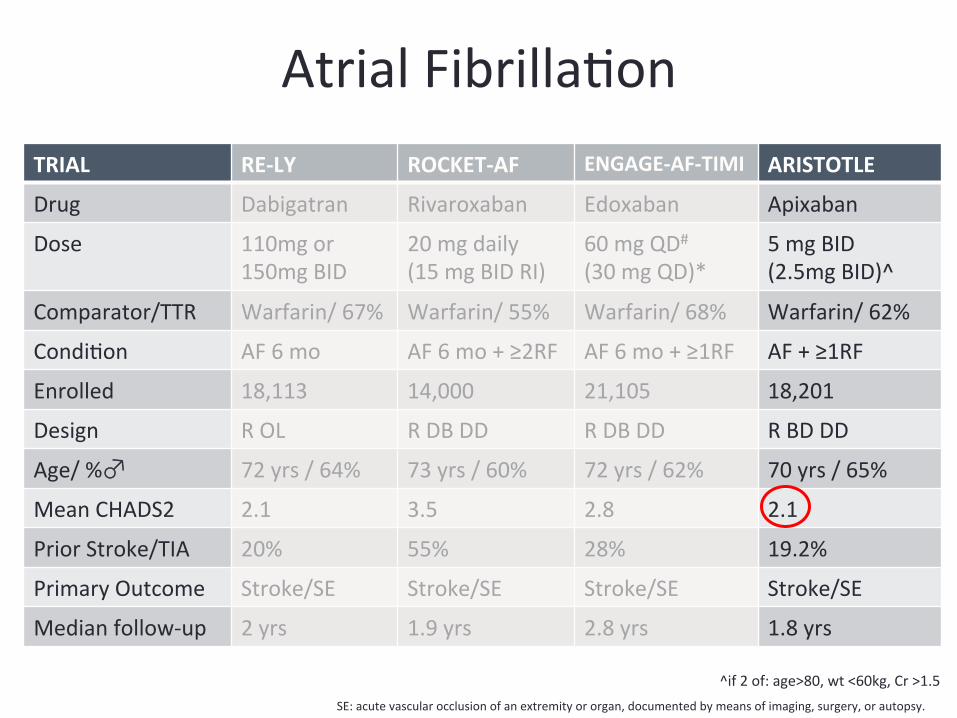
Atrial Fibrilla/on TRIAL RE-‐LY ROCKET-‐AF ENGAGE-‐AF-‐TIMI ARISTOTLE
Drug Dabigatran Rivaroxaban Edoxaban Apixaban
Dose 110mg or 150mg BID
20 mg daily (15 mg BID RI)
60 mg QD#
(30 mg QD)* 5 mg BID (2.5mg BID)^
Comparator/TTR Warfarin/ 67% Warfarin/ 55% Warfarin/ 68% Warfarin/ 62%
Condi/on AF 6 mo AF 6 mo + ≥2RF AF 6 mo + ≥1RF AF + ≥1RF
Enrolled 18,113 14,000 21,105 18,201
Design R OL R DB DD R DB DD R BD DD
Age/ %♂ 72 yrs / 64% 73 yrs / 60% 72 yrs / 62% 70 yrs / 65%
Mean CHADS2 2.1 3.5 2.8 2.1
Prior Stroke/TIA 20% 55% 28% 19.2%
Primary Outcome Stroke/SE Stroke/SE Stroke/SE Stroke/SE
Median follow-‐up 2 yrs 1.9 yrs 2.8 yrs 1.8 yrs
SE: acute vascular occlusion of an extremity or organ, documented by means of imaging, surgery, or autopsy.
^if 2 of: age>80, wt <60kg, Cr >1.5
ARISTOTLE: Summary Comparison of Apixaban to Warfarin
� Apixaban reduced the risk of stroke or systemic embolism by 21%, major bleeding by 31%, and death by 11%.
� For each 1000 pa/ents treated for 1.8 years, apixaban prevented 6 strokes 15 major bleedings and 8 deaths.
� Net Clinical Outcome Benefit favors apixaban � 6.13% vs. 7.2% p < 0.001
Granger NEJM 2011;365:981-‐92
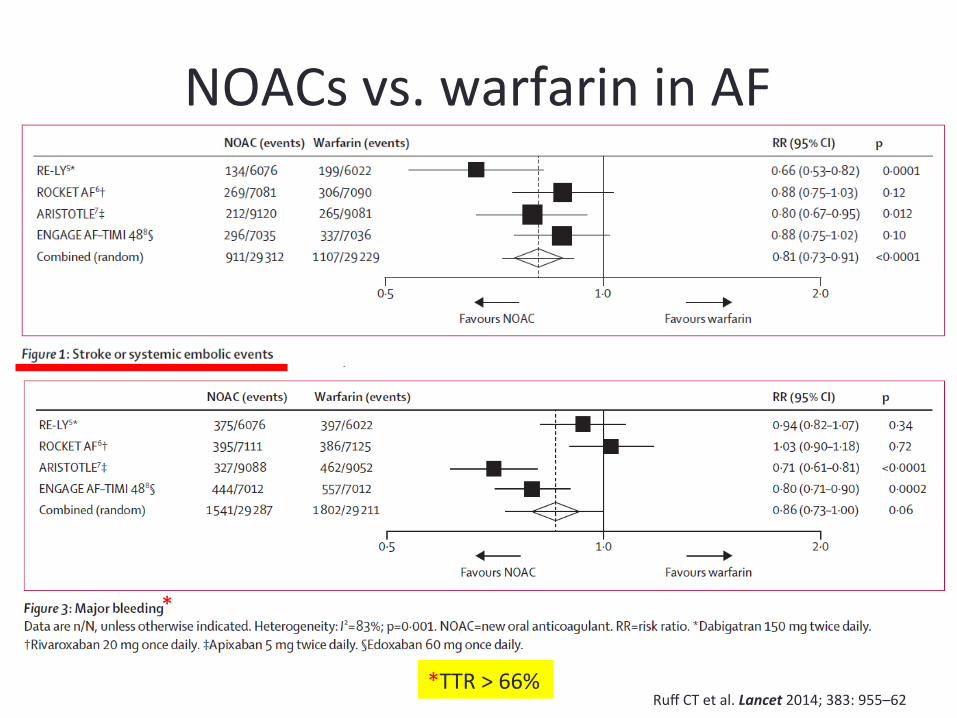
NOACs vs. warfarin in AF
Ruff CT et al. Lancet 2014; 383: 955–62 *TTR > 66%
*
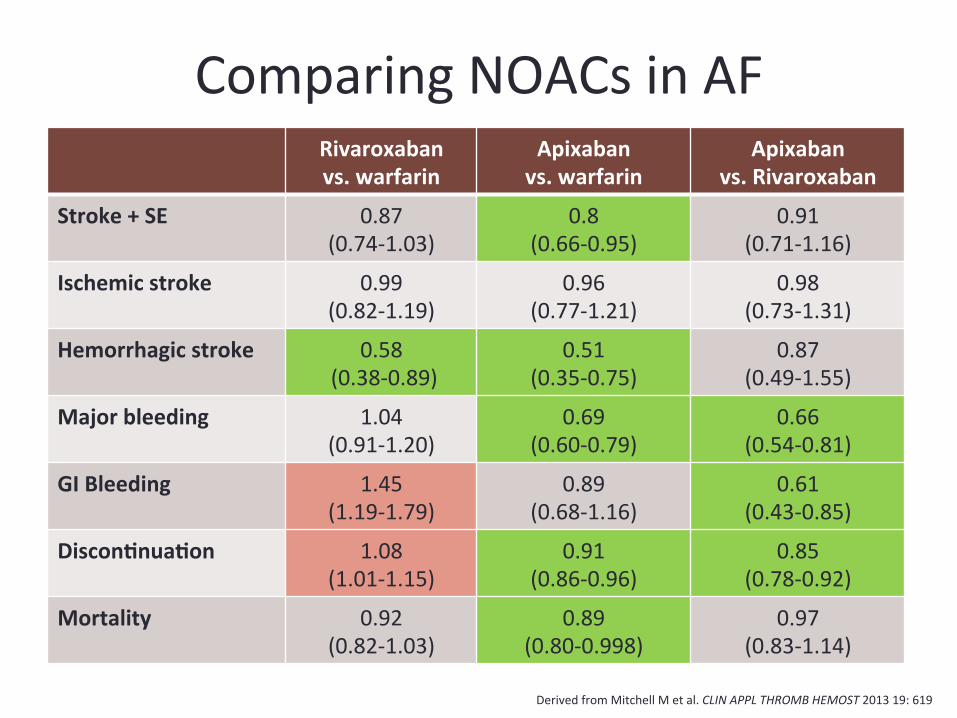
Comparing NOACs in AF Rivaroxaban vs. warfarin
Apixaban vs. warfarin
Apixaban vs. Rivaroxaban
Stroke + SE 0.87 (0.74-‐1.03)
0.8 (0.66-‐0.95)
0.91 (0.71-‐1.16)
Ischemic stroke 0.99 (0.82-‐1.19)
0.96 (0.77-‐1.21)
0.98 (0.73-‐1.31)
Hemorrhagic stroke 0.58 (0.38-‐0.89)
0.51 (0.35-‐0.75)
0.87 (0.49-‐1.55)
Major bleeding 1.04 (0.91-‐1.20)
0.69 (0.60-‐0.79)
0.66 (0.54-‐0.81)
GI Bleeding 1.45 (1.19-‐1.79)
0.89 (0.68-‐1.16)
0.61 (0.43-‐0.85)
DisconCnuaCon 1.08 (1.01-‐1.15)
0.91 (0.86-‐0.96)
0.85 (0.78-‐0.92)
Mortality 0.92 (0.82-‐1.03)
0.89 (0.80-‐0.998)
0.97 (0.83-‐1.14)
Derived from Mitchell M et al. CLIN APPL THROMB HEMOST 2013 19: 619
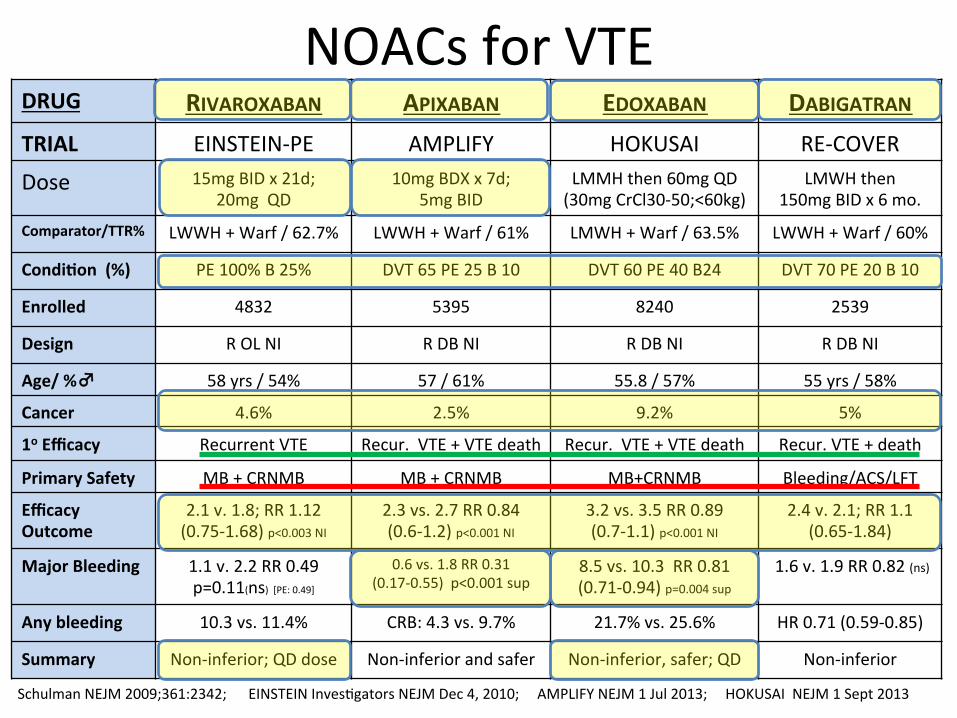
DRUG RIVAROXABAN APIXABAN EDOXABAN DABIGATRAN TRIAL EINSTEIN-‐PE AMPLIFY HOKUSAI RE-‐COVER
Dose 15mg BID x 21d; 20mg QD
10mg BDX x 7d; 5mg BID
LMMH then 60mg QD (30mg CrCl30-‐50;<60kg)
LMWH then 150mg BID x 6 mo.
Comparator/TTR% LWWH + Warf / 62.7% LWWH + Warf / 61% LMWH + Warf / 63.5% LWWH + Warf / 60%
CondiCon (%) PE 100% B 25% DVT 65 PE 25 B 10 DVT 60 PE 40 B24 DVT 70 PE 20 B 10
Enrolled 4832 5395 8240 2539
Design R OL NI R DB NI R DB NI R DB NI
Age/ %♂ 58 yrs / 54% 57 / 61% 55.8 / 57% 55 yrs / 58%
Cancer 4.6% 2.5% 9.2% 5%
1o Efficacy Recurrent VTE Recur. VTE + VTE death Recur. VTE + VTE death Recur. VTE + death
Primary Safety MB + CRNMB MB + CRNMB MB+CRNMB Bleeding/ACS/LFT
Efficacy Outcome
2.1 v. 1.8; RR 1.12 (0.75-‐1.68) p<0.003 NI
2.3 vs. 2.7 RR 0.84 (0.6-‐1.2) p<0.001 NI
3.2 vs. 3.5 RR 0.89 (0.7-‐1.1) p<0.001 NI
2.4 v. 2.1; RR 1.1 (0.65-‐1.84)
Major Bleeding 1.1 v. 2.2 RR 0.49 p=0.11(ns) [PE: 0.49]
0.6 vs. 1.8 RR 0.31 (0.17-‐0.55) p<0.001 sup
8.5 vs. 10.3 RR 0.81 (0.71-‐0.94) p=0.004 sup
1.6 v. 1.9 RR 0.82 (ns)
Any bleeding 10.3 vs. 11.4% CRB: 4.3 vs. 9.7% 21.7% vs. 25.6% HR 0.71 (0.59-‐0.85)
Summary Non-‐inferior; QD dose Non-‐inferior and safer Non-‐inferior, safer; QD Non-‐inferior
Schulman NEJM 2009;361:2342; EINSTEIN Inves/gators NEJM Dec 4, 2010; AMPLIFY NEJM 1 Jul 2013; HOKUSAI NEJM 1 Sept 2013
NOACs for VTE
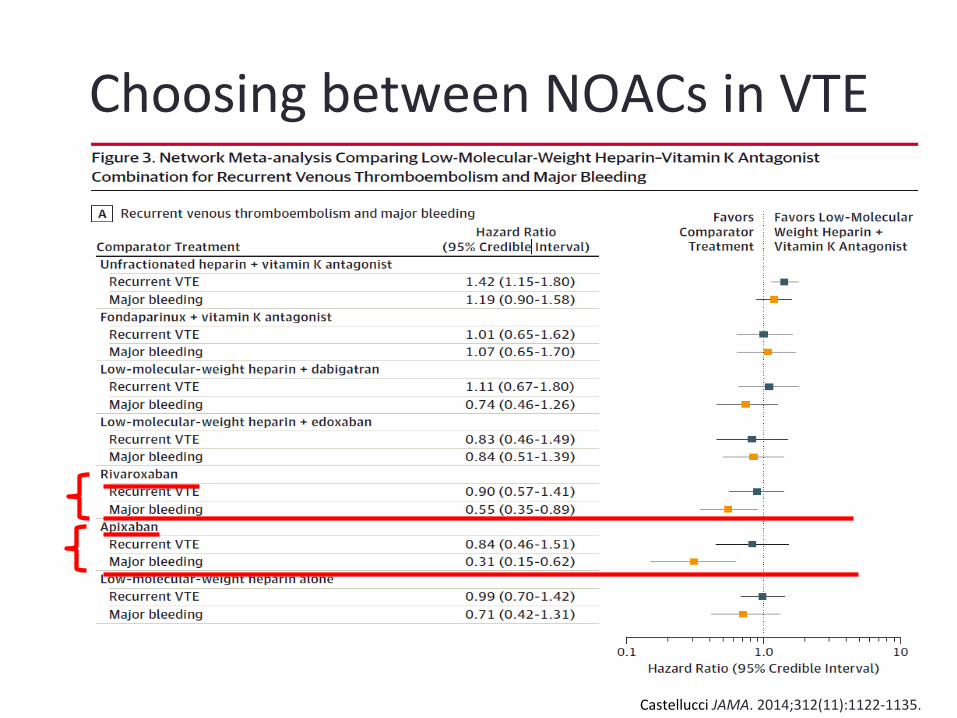
Choosing between NOACs in VTE
Castellucci JAMA. 2014;312(11):1122-‐1135.
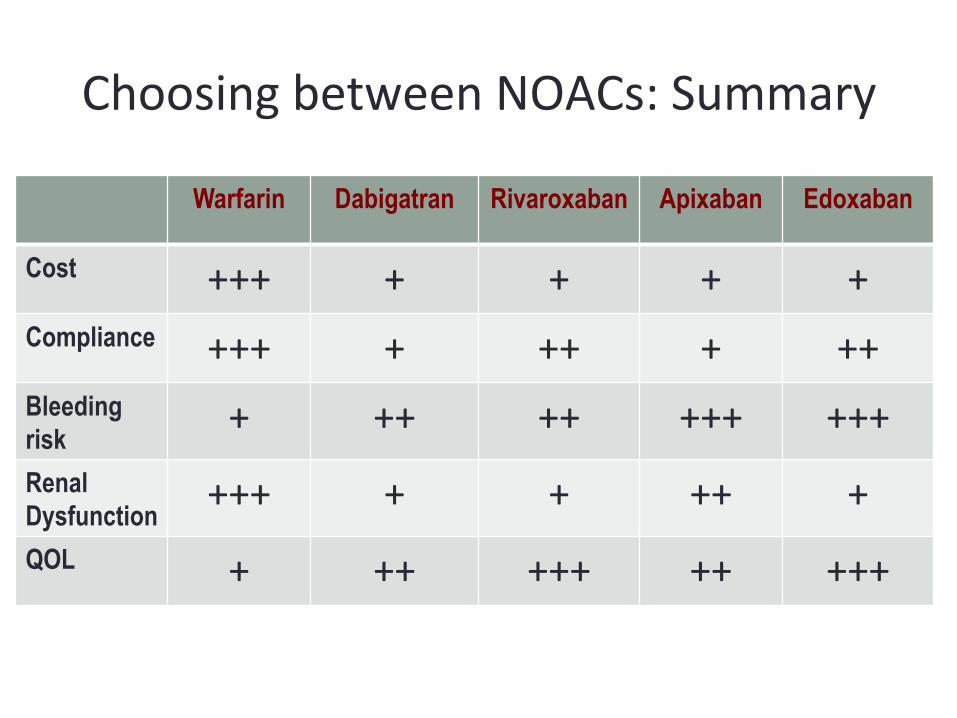
Choosing between NOACs: Summary
Warfarin Dabigatran Rivaroxaban Apixaban Edoxaban
Cost +++ + + + + Compliance +++ + ++ + ++ Bleeding risk + ++ ++ +++ +++ Renal Dysfunction +++ + + ++ + QOL + ++ +++ ++ +++
Anderson M Clev. Clin J Med, 2014, 8; 629;
� About 2.5M Americans require long-‐term an/coagula/on
� About 10% require interrup/on annually
� Generally, interrupt 4-‐5 half-‐lives before HBR procedure
� OK to interrupt 2-‐3 half-‐lives before LBR procedure
� Half-‐life increases as crea/nine clearance increases
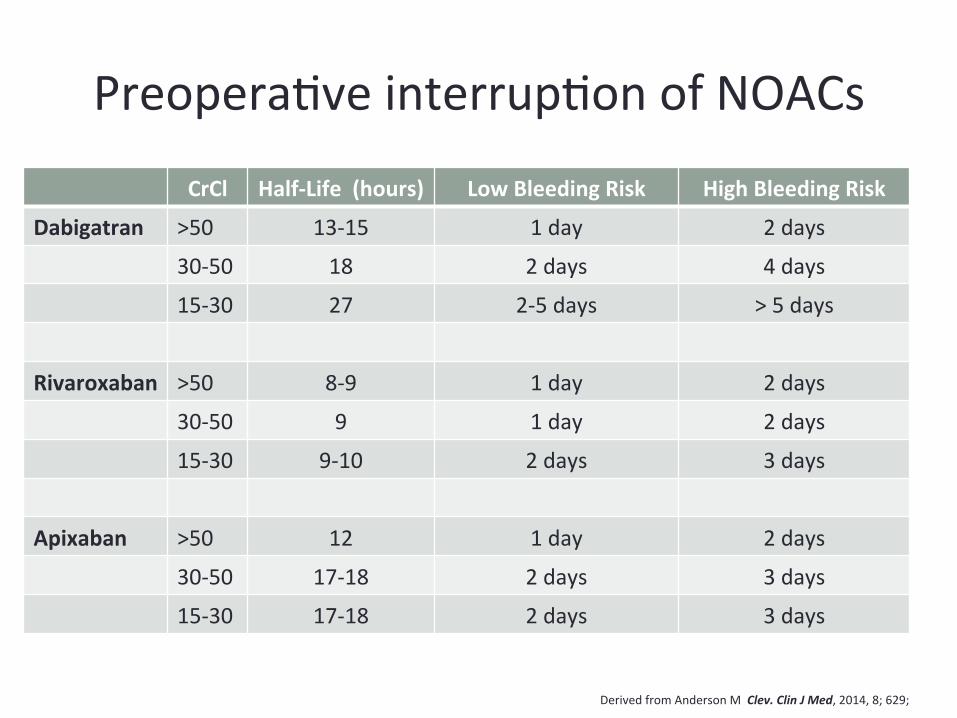
Preopera/ve interrup/on of NOACs
CrCl Half-‐Life (hours) Low Bleeding Risk High Bleeding Risk
Dabigatran >50 13-‐15 1 day 2 days
30-‐50 18 2 days 4 days
15-‐30 27 2-‐5 days > 5 days
Rivaroxaban >50 8-‐9 1 day 2 days
30-‐50 9 1 day 2 days
15-‐30 9-‐10 2 days 3 days
Apixaban >50 12 1 day 2 days
30-‐50 17-‐18 2 days 3 days
15-‐30 17-‐18 2 days 3 days
Derived from Anderson M Clev. Clin J Med, 2014, 8; 629;
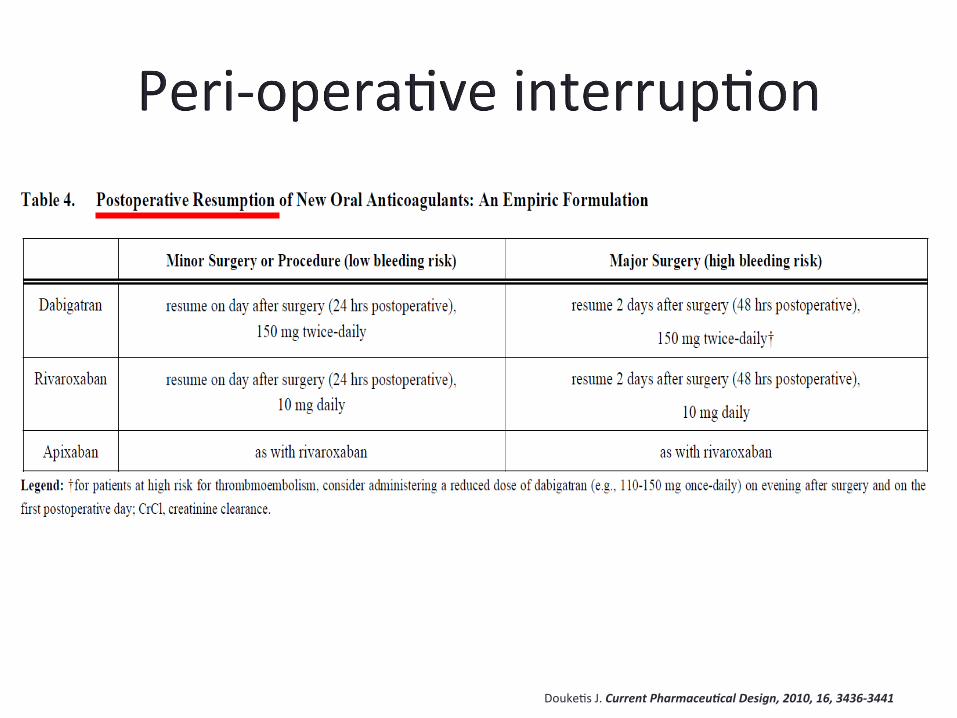
Douke/s J. Current Pharmaceu#cal Design, 2010, 16, 3436-‐3441
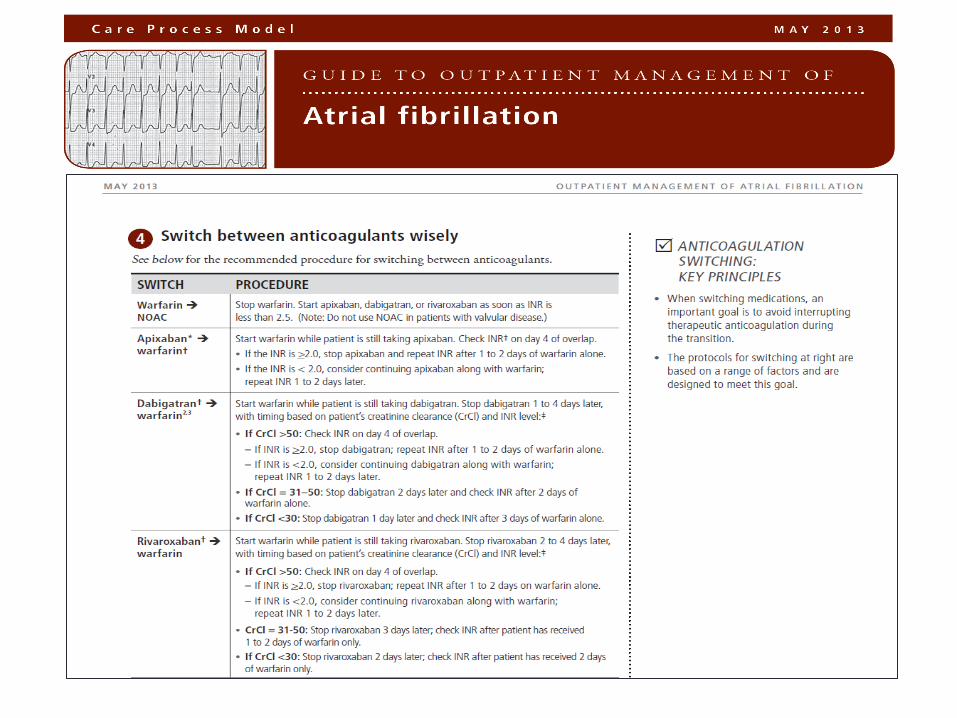
Transi/oning between an/coagulants
Warfarin → NOAC h|ps://kr.ihc.com/ext/Dcmnt?ncid=522592305
h|ps://kr.ihc.com/ext/Dcmnt?ncid=522592305
• Package inserts of the NOACs vary • Representa/ve of expert opinion
• Recommenda/on: Stop warfarin. Start apixaban, dabigatran, edoxaban, or rivaroxaban as soon as INR is less than 2.5.
Transi/oning between an/coagulants
NOAC → Warfarin
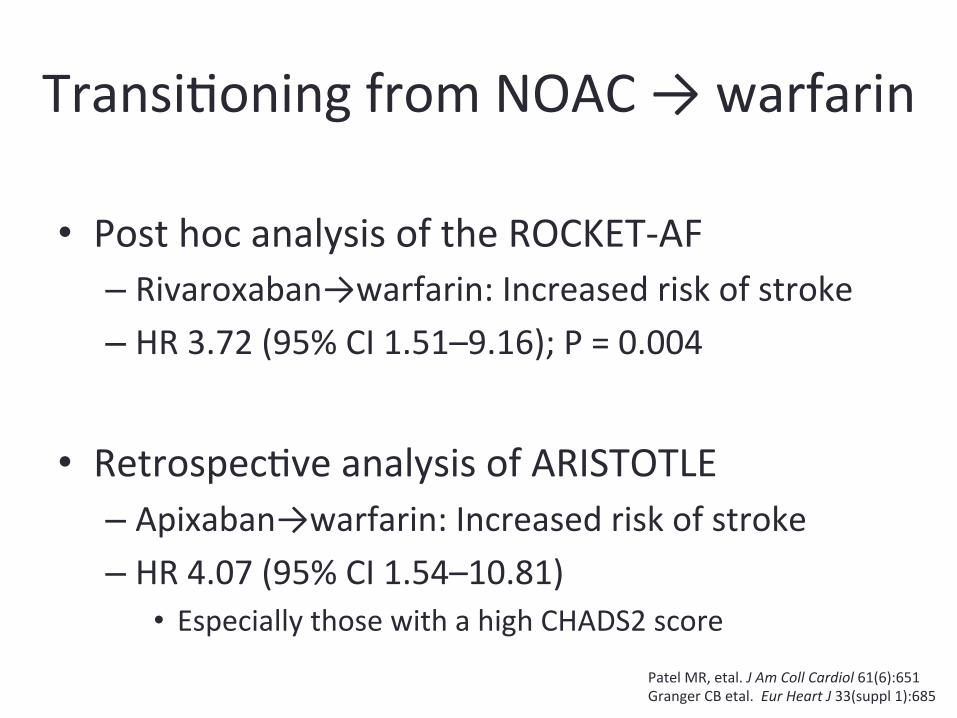
Transi/oning from NOAC → warfarin
• Post hoc analysis of the ROCKET-‐AF – Rivaroxaban→warfarin: Increased risk of stroke – HR 3.72 (95% CI 1.51–9.16); P = 0.004
• Retrospec/ve analysis of ARISTOTLE – Apixaban→warfarin: Increased risk of stroke – HR 4.07 (95% CI 1.54–10.81)
• Especially those with a high CHADS2 score Patel MR, etal. J Am Coll Cardiol 61(6):651 Granger CB etal. Eur Heart J 33(suppl 1):685
Summary • iCentra – An#coagula#on Management Suite
• The Non-‐Vitamin K Oral An/coagulants – Atrial fibrilla/on – Venous thromboembolism – Choice of drug
• Peri-‐procedural interrup/on of the NOACs – Drug, procedure, renal func/on
• Transi/on from: – NOAC → warfarin – Warfarin → NOAC
Thank you





![The 2018European Heart Rhythm Association Practical Guide ...€¦ · Europace 2015;17:1467–1507]. Non-vitamin K antagonist oral anticoagulants (NOACs) are an alter- native for](https://img.pdfslide.us/doc/110x75/5f0f33eb7e708231d442fee3/the-2018european-heart-rhythm-association-practical-guide-europace-2015171467a1507.jpg)




![Non-Vitamin K Antagonist Oral Anticoagulants: New Choices ... · 32]. NOACs have fewer drug–drug and drug–food inter-actions than warfarin. Although rivaroxaban should be administered](https://img.pdfslide.us/doc/110x75/5ed761642d26a13e8d6e99ec/non-vitamin-k-antagonist-oral-anticoagulants-new-choices-32-noacs-have-fewer.jpg)