Embed Size (px)
Citation preview

Nonvisualization of the ovaries on pelvicultrasound: does MRI add anything?
Christopher J. Lisanti, Jonathan R. Wood, Ryan B. Schwope
Department of Radiology, San Antonio Military Medical Center, 3851 Roger Brooke Dr., Ft. Sam Houston, TX 78234, USA
Abstract
Purpose: The purpose of our study is to assess the utilityof pelvic magnetic resonance imaging (MRI) in the eventthat either one or both ovaries are not visualized bypelvic ultrasound.Materials and methods: ThisHIPAA-compliant retrospec-tive study was approved by our local institutional reviewboard and informed consent waived. 1926 pelvic MRIexaminations between March 2007 and December 2011were reviewed and included if a combined transabdominaland endovaginal pelvic ultrasound had been performed inthe preceding 6 months with at least one ovary nonvisual-ized. Ovaries not visualized on pelvic ultrasound wereassumed to be normal and compared with the pelvic MRIfindings. MRI findings were categorized as concordant ordiscordant. Discordant findings were divided into malig-nant, non-malignant physiologic or non-malignant non-physiologic. The modified Wald, the ‘‘rule of thirds’’, andthe binomial distribution probability tests were performed.Results: 255 pelvic ultrasounds met inclusion criteria with364 ovaries not visualized. 0malignancieswere detectedonMRI. 6.9% (25/364) of nonvisualized ovaries had non-malignant discordant findings on MRI: 5.2% (19/364)physiologic, 1.6% (6/364) non-physiologic. Physiologicfindings included: 16 functional cysts and 3 hemorrhagiccysts. Non-physiologic findings included: 3 cysts in post-menopausalwomen, 1 hydrosalpinx, and 2broad ligamentfibroids. The theoretical risk of detecting an ovariancarcinoma on pelvic MRI when an ovary is not visualizedon ultrasound ranges from 0 to 1.3%.Conclusion: If an ovary is not visualized on pelvicultrasound, it can be assumed to be without carcinomaand MRI rarely adds additional information.
Key words: Pelvic ultrasound—Pelvic MRI—Nonvisualization—Ovaries
Pelvic ultrasound is the most commonly utilized imagingmodality for assessment of a wide variety of gynecologicsymptoms. It is non-invasive, inexpensive, widely avail-able, and lacks potentially harmful ionizing radiation.However, nonvisualization of the ovaries by ultrasoundoccurs commonly. Nonvisualization rates vary widely inthe literature dependent upon endpoints, sonographicmethod, and patient demographics with typical nonvi-sualization rates of 2–40% or more [1–5]. Nonvisualiza-tion of an ovary may be due to technical factors such assonographer experience, diligence, or properly function-ing equipment. Patient factors that can limit visualiza-tion include atrophic ovaries, obesity, overlying bowelgas, and patient discomfort during examination.
Pelvic pain is a common presenting symptom in bothpre- and post-menopausal women. There are many eti-ologies for pelvic pain including adhesions, endometri-osis, hemorrhagic cysts, and ovarian cancer. Althoughthe lifetime risk of developing ovarian cancer is only1.4%, it is the most concerning potential ovarianpathology that might be missed [6]. Nonvisualization ofan ovary on ultrasound can result in a diagnostic di-lemma, particularly if the patient’s symptoms are on thesame side as the nonvisualized ovary. In our experience,many clinicians and even some radiologists feel thatfurther investigation with a pelvic magnetic resonanceimaging (MRI) is warranted even though studies haveshown that the sensitivity for detection of ovarian cancerby pelvic MRI is no better than pelvic ultrasound [7].
The purpose of our study is to assess the utility ofpelvic MRI in the event that either one or both ovariesare not visualized by pelvic ultrasound.
Materials and methods
Our research protocol was HIPAA compliant and ap-proved by our institutional review board and informed
The opinions and assertions contained herein are those of the authorsand should not be construed as official or as representing the opinionsof the Department of the Army or the Department of Defense.
Correspondence to: Christopher J. Lisanti; email: [email protected]
ª Springer Science+Business Media New York (outside the USA) 2013
Published online: 24 November 2013AbdominalImaging
Abdom Imaging (2014) 39:162–167
DOI: 10.1007/s00261-013-0046-0

consent was waived. 1926 pelvic MRI examinationsperformed between March 2007 and December 2011were queried on our local Picture Archiving and Com-munication System databases. Inclusion criteria were asfollows: a preceding transabdominal and endovaginalpelvic ultrasound in the prior 6 months with nonvisual-ization of at least one ovary, and age greater than orequal to 18 years old. Exclusion criteria were knownovarian malignancy.
Ultrasound and MRI protocols
The pelvic ultrasound protocol included both transab-dominal ultrasound with a full bladder followed by atransvaginal ultrasound after voiding. The ultrasoundmachines utilized were Philips iU22 (Philips MedicalSolutions, Best, the Netherlands) and Siemens AcusonS2000 (Siemens Medical Solution, Malvern, PA, USA)with curved 8–4 MHz endovaginal and curved 5–1 MHztransabdominal ultrasound transducers.
Pelvic MRI was performed utilizing Siemens Espree,Avanto, and Verio (Siemens Medical Solution, Malvern,PA, USA) as well as General Electric Echospeed PlusMRI (GE Medical Systems, Milwaukee, WI, USA). Theprotocols varied although a typical protocol is seen inTable 1.
Evaluation of sonographically nonvisualizedovaries
Patient age, patient history, summary of the imagingreports, and any applicable pathology reports were re-corded. If either an ultrasound or MRI report did notmention the ovaries, the images were further reviewed todetermine if the ovaries were visible and to characterizetheir appearance. Results of the pelvic ultrasound andpelvic MRI were then compared. If MRI had a finding in
a nonvisualized ovary on pelvic ultrasound, then thatwas classified as a discordant finding. Later clinical notesand/or later imaging studies (CT, MR or ultrasound) forall subjects with discordant findings were reviewed todetermine whether the findings spontaneously resolvedor had any further intervention.
Statistical analysis was performed by using modifiedWald equation [8], the rule of thirds [9], and the binomialprobability distribution (BINOMDIST) (Microsoft Ex-cel, Redmond, Wash).
Results
255 women met inclusion criteria with an average age of49.9 years (range 21–85 years). There were 129 pre-menopausal women, 8 perimenopausal (within 5 years oflast menstrual cycle), and 82 post-menopausal as classi-fied per their clinical history. 36 women had an unknownmenstrual status, most of who were in their early fiftiesand were presumably perimenopausal. The average timefrom pelvic ultrasound to pelvic MRI was 43 days.
Clinical histories and ultrasound reportrecommendations
Of the 255 ultrasound reports, 81/255 (31.8%) includedrecommendations for a follow-up pelvic MRI for anonvisualized ovary by the interpreting radiologist. 23/81(28.4%) radiologist recommendations for follow-up MRIwere solely due to non-visualization of the ovaries (16 forfollow-up of prior adnexal abnormality on imaging; 3 forfamily history of ovarian cancer; 4 for adnexal finding onphysical examination). The other 58 recommendationswere made in conjunction with abnormalities seen onultrasound, clinical symptoms or findings, and/or limi-tations of the ultrasound in visualizing other pelvic or-gans (usually the endometrial stripe). Of the 255 clinicalhistories, 113/255 (44.3%) included a statement that anovary was not visualized on the previous pelvic ultra-sound. 19/113 (16.8%) of the clinical histories indicatedthat the examination was solely for the purpose of non-visualized ovaries. See Table 2 for other clinical histories.Five patients had a single absent ovary from prioroophorectomy for benign disease.
Table 1. Typical MRI protocol
Pulse Plane TR/TE(ms)
Slicethickness(mm)
HASTE/SSFSE Axial, Coronal,a
and Sagittal1100/100 6–8
T1 out-of-phase Axial 220/2.4 5–7T1 in-phase Axial 220/4.8 5–7T1 VIBE w/Fat Satb Axial 5.4/2.5 3–3.5T2 TSE/FSE w/Fat Satb Axial 6300/50 5–8
Sagittal 3200/53 5–8T1 VIBE w/Fat Satb
post gadoliniumcAxial 5.4/2.5 3–3.5Coronal or Sagittal 5.4/2.5 3–3.5
aTwo coronal acquisitions. One with large field of view to include thekidneys, and one of the pelvisbAll fat saturation techniques were chemical fat saturationc187 studies were performed with intravenous gadolinium with varyingdoses but usually weight-based at 0.1–0.2 mmol/kgHASTE half-Fourier acquisition single-shot turbo spin-echo, SSFSEsingle-shot fast spin echo, VIBE volumetric interpolated breath-holdexam, TSE turbo spin echo, FSE fast spin echo
Table 2. Other clinical histories
Pain or pressure 100
Abnormal vaginal bleeding 83Abnormal findings on a previous radiology examination 59Mass on examination 26Fibroids with consideration for uterine artery embolization 20Bloating or fullness 14Oligo-/amenorrhea 7Family history of ovarian cancer 3Limited physical examination 2Vaginal discharge 2Histories not provided 2
C. J. Lisanti et al.: Nonvisualization of the ovaries on pelvic ultrasound 163

Results of sonographically nonvisualized ovaries
364 ovaries were nonvisualized on ultrasound in 255women. See Table 3 for details. No MR findings weresuggestive of malignancy. The most concerning discor-dant findings were in the three post-menopausal women
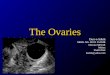
with cystic lesions. Their clinical scenarios were: (1) 72-year-old female with slowly decreasing cystic lesion sizeover 4 years previously measured 3.0 9 3.0 9 2.2 cmand measured 2.7 9 2.3 9 2.0 cm on study MRI pre-sumed to be benign, (2) 72-year-old female with threesmall cystic lesions the largest measuring 1.5 cm whichslowly enlarged over a period of 11 years with follow-uprecommended (Fig. 1), and (3) 66-year-old female ontamoxifen therapy with decreasing cystic lesion previ-ously measuring 5 cm and then measured 2.9 cm onstudy MRI presumed to be benign.
Results of sonographically visualized ovaries
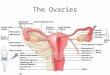
See Table 4 for results. Of the ultrasound findings con-firmed by MRI, only one solid mass found to be foreignbody giant cell reaction (Fig. 2) was pathologicallyconfirmed.
Statistical analysis regarding malignancy
Since there were no malignancies identified, we per-formed the modified Wald test [8], ‘‘rule of three’’ [9],
Fig. 1. 72-year-old post-menopausal female with threesmall cystic lesions the largest measuring 1.5 cm that slowlyenlarged over a period of 11 years when compared to priorCT scans. A Endovaginal ultrasound image shows no leftadnexal abnormality or ovary. Axial T2-weighted image (B)
demonstrates dominant cyst in the left ovary (arrow) with asmaller cyst anterior. Axial T1-weighted fat suppressed post-gadolinium VIBE image (C) demonstrates unenhancingdominant cyst in the left ovary (arrow) with a smaller cystanterior. Third cyst not shown.
Table 3. Results of sonographically nonvisualized ovaries
Nonvisualized ovaries 364Left ovary 72Right ovary 74Bilateral 109
Findings on MRNormal ovary 74.7% (272)Discordant findings 6.9% (25)Non-visualized ovary 18.4% (67)a
Discordant MR findingsPhysiologic 5.2% (19)b
Non-physiologic 1.6% (6)c
All percentages use 364 as the denominatoraNo adnexal abnormalities identified on MRb16 functional cysts and 3 hemorrhagic cystscThree cysts in post-menopausal women that showed persistence onfollow-up or prior imaging, one small hydrosalpinx in a pre-meno-pausal woman, and two small broad ligament fibroids in a postmeno-pausal woman
164 C. J. Lisanti et al.: Nonvisualization of the ovaries on pelvic ultrasound

and the binomial distribution probability test with a 95%
confidence interval. The chance of malignant ovarianpathology when the ovary was not visualized on ultra-sound when analyzed per ovary for the entire studygroup was as follows: modified Wald test 0–1.3%; ‘‘ruleof three’’ 0.8%; and the binominal distribution 0.1%.
When analyzing the 137 pre- or perimenopausal fe-males in our population, there were 237 nonvisualizedovaries yielding the following results: modified Wald test0.0–2.0%; ‘‘rule of three’’ 1.3%; and the binominal dis-tribution 0.8.
When analyzing the 82 postmenopausal females inour population, there were 127 nonvisualized ovariesyielding the following results: modified Wald test 0–3.6%; ‘‘rule of three’’ 2.4%; and the binominal distribu-tion 7.7%.
Discussion
From our population of 255 women with 364 nonvisu-alized ovaries, only 1.6% of the ovaries had true discor-dant findings with three benign-appearing cysts inpostmenopausal women, one hydrosalpinx and two
Fig. 2. 52-year-old post-menopausal female status posthysterectomy with chronic left lower quadrant pain. A Endo-vaginal ultrasound image demonstrates a hypoechoic mass inthe left adnexa (calipers). Right ovary was not visualized.Axial T1-weighted image (B) demonstrates isointense signalmass in the left adnexa (arrow). Axial T2-weighted fat-sup-
pressed image (C) demonstrates a mildly hyperintense signalmass in the left adnexa (arrow). Axial T1-weighted fat sup-pressed post-gadolinium VIBE subtraction image (D) dem-onstrates minimal enhancement (arrow). Surgical resectionrevealed a foreign body giant cell reaction.
Table 4. Results of sonographically visualized ovaries
Ovaries visualized on both US and MR 129
Normal on both US and MR 53.5% (69)Concordant findings on US and MR 33.3% (43)a
Findings only on US (normal on MR) 13.2% (17)b
All percentages use 129 as the denominatora19 simple cysts, 7 hemorrhagic cysts, 7 complex cysts, 8 hydrosal-pinges, 1 endometrioma, 1 foreign body giant cell reactionbPresumed to be hemorrhagic or functioning cysts
C. J. Lisanti et al.: Nonvisualization of the ovaries on pelvic ultrasound 165

small broad ligament fibroids. The other 358 ovaries(98.4%) were either normal or had transient physiologicfindings. None of the 364 ovaries that were sonographi-cally nonvisualized were found to have malignancy fea-tures such as solid components on follow-up MRI. Ourstudy demonstrates that the maximum risk of malignantpathology in a nonvisualized ovary on ultrasound is1.3%. Thus, pelvic ultrasound is a robust imagingmodality for excluding malignancy in a nonvisualizedovary.
The ovaries can have a variety of pathology that maycause symptoms or findings on physical examination thatwould prompt a request for a pelvic ultrasound. Thesepathologies include benign and malignant neoplasms,endometriomas, and hemorrhagic or functional cysts. Inour study, despite literature proving essentially equalsensitivity of ultrasound and MRI [7] for diagnosingovarian pathology, a nonvisualized ovary at ultrasoundappears to raise concern prompting follow-up MRIespecially when combined with other inconclusive find-ings. We compared the frequency of recommendationsby radiologists for MRI with that of the referring clini-cians, and were surprised to find that women were re-ferred to pelvic MRI almost as much by their radiologist(31.8%) as they were by their clinician (44.3%).
The value of performing a pelvic MRI to evaluateovaries that were sonographically nonvisualized dependson the accuracy of the test, and the amount of risk thepatient and her providers are willing to assume with therisk of malignancy being the most worrisome. Specifi-cally, since no test is perfect, what is an acceptable riskfor excluding malignancy? Is a risk of 1.3% low enough?The literature is relatively silent on presumed risk inmedical imaging although inferences can be made byanalyzing current management guidelines. For example,a recent consensus statement by the Society of Radiol-ogists in Ultrasound indicated that follow-up imagingwas no longer recommended for unilocular ovarian cystsless than 5 cm in pre-menopausal women. This recom-mendation was in part based upon data indicating lessthan a 1% risk of cancer in this population [10]. Simi-larly, the Fleischner Society recommendations for fol-low-up of solitary pulmonary nodules referenced a studyby Henschke et al. [11, 12] that demonstrated 0 lungcancers in 378 cases with noncalcified pulmonary nod-ules less than 5 mm with an estimated 0.6% risk ofmissing malignancy. We had nearly the same number ofovaries as pulmonary nodules for statistical analysis.Although our statistical methodology was different, ourmaximum risk (1.3%) of missing malignancy was similarto theirs.
Does pelvic symptomatology increase the risk ofovarian cancer? Pelvic pain is the most common pre-senting symptom in ovarian cancer in up to 57% ofwomen, and is the most common presenting symptom inwomen with stage 1 or 2 surgical disease [13, 14]. The
likelihood ratio of ovarian cancer for women presentingwith pelvic or abdominal pain, increased abdominal size,bloating, difficulty eating, or feeling full has been esti-mated to be 7.4 in one study [15]. When combined withan annual of incidence in the US population of 0.013%
[16], this would then increase the risk for this subset to0.10%. It should be noted that a later article using cri-teria to select out much higher symptom severity indi-cated increased odds ratios of up to 23.3 [17]. However,our population is more similar to the first study, and thuswas a better comparison. In summary, even a risk of0.10% may not justify the added cost of a follow-upMRI, the risk of potential false-positive findings, or thefalse reassurance of a false negative MRI.
Although ovarian cancer is the most concerningdiagnosis, benign pelvic pathologies are more commoncauses of pelvic complaints. One study found adhesionsand endometriosis as the most common etiologies inwomen with chronic pelvic pain [18]. Adhesions aregenerally not well seen by any imaging modality,including MRI, although their presence can sometimesbe indirectly inferred [19]. When comparing MRI andultrasound for the detection of endometriosis, severalstudies indicate mixed results in their overall accuracythat is influenced by patient selection, lesion size andlocation, and ultrasound technique [20–23]. To ourknowledge, there have been no studies evaluating theadded value of pelvic MRI following ultrasound in theassessment of pelvic pain in a more general patientpopulation, as in our study. We are not surprised thatneither adhesions were suggested nor endometriosisfound with either imaging modality in our study as apotential explanation for pelvic symptoms.
There are several limitations to our study. This is aretrospective study and therefore not every ovary notvisualized with ultrasound was followed up with pelvicMRI. A second limitation is that we used MRI as the‘‘gold standard’’ and not laparoscopy or pathology.However, the purpose of our study was to explicitlydetermine the added diagnostic value of MRI and not todetermine the absolute ability of either ultrasound orMRI to detect adnexal pathology. In addition, the threepost-menopausal women with cystic lesions were pre-sumed to be non-malignant given the clinical scenarios,however we did not have pathologic proof. Third, post-menopausal women are at increased risk for ovariancancer and our study included only 82 postmenopausalfemales with 127 nonvisualized ovaries. Due to the de-creased statistical power with this smaller group, thecalculated risk of significant ovarian pathology in thissubset was up to 7.7%, and this is an opportunity forfurther research. A fourth limitation is that we did notinvestigate each patient’s additional risk factors such asobesity, nulliparity, tubal ligation, or family history ofovarian cancer in a first degree relative [24], and thus ourpopulation’s risk cannot be precisely known. A final
166 C. J. Lisanti et al.: Nonvisualization of the ovaries on pelvic ultrasound

limitation of our study is that we had no cases of ovariancancer in our visualized ovary cohort. However, giventhe size of our study population, we would not expect tofind any ovarian cancer even with some increased riskdue to clinical symptoms given the very low incidence ofovarian cancer.
In conclusion, we demonstrate that when an ovary isnot visualized on pelvic ultrasound in a patient withoutknown ovarian disease that the risk of malignancy is atmost 1.3%. Furthermore, our study showed that lessthan 2% of patients had non-malignant findings on fol-low-up pelvic MRI none of which required intervention.Thus, pelvic MRI in a general cohort of patients willlikely be of little additional value. Reducing the volumeof pelvic MRI will allow better allocation of a valuable,limited resource as well as decrease the financial burdento our health care system. Considering the number ofwomen in the United States who present with pelvicsymptoms, there are potentially enormous financialsavings.
Acknowledgment. The authors thank Dr. John Ward for his assistancewith the statistical analysis.
References
1. Fleischer AC, McKee MS, Gordon AN, et al. (1990) Transvaginalsonography of postmenopausal ovaries with pathologic correlation.J Ultrasound Med 9:637–644
2. Fishman DA, Cohen L, Blank SV, et al. (2005) The role of ultra-sound evaluation in the detection of early-stage epithelial ovariancancer. Am J Obstet Gynecol 192(4):1214–1221
3. Van Nagell JR Jr, DePriest PD, Ueland FR, et al. (2007) Ovariancancer screening with annual transvaginal sonography: findings of25,000 women screened. Cancer 109(9):1887–1896
4. DiSantis DJ, Scatarige JC, Kemp G, et al. (1993) A prospectiveevaluation of transvaginal sonography for detection of ovariandisease. AJR 161:91–94
5. Hartge P, Hayes R, Reding D, et al. (2000) Complex ovarian cystsin postmenopausal women are not associated with ovarian cancerrisk factors. Preliminary data from the prostate, lung, colon, andovarian cancer screening trial. Am J Obstet Gynecol 183:1232–1237
6. Adusumilli S, Hussain HK, Caoili EM, et al. (2006) MRI of so-nographically indeterminate adnexal masses. AJR 187(3):732–740
7. Kinkel K, Lu Y, Mehdizade A, Pelte MF, Hricak H (2000) Inde-terminate ovarian mass at US: incremental value of second imaging
test for characterization—meta-analysis and Bayesian analysis.Radiology 236:85–94
8. Agresti A, Coull BA (1998) Approximate is better than ‘‘exact’’ forinterval estimation of binomial proportions. Am Stat 52:119–126
9. Hanley J, Lippman-Hand A (1983) If nothing goes wrong, iseverything alright? JAMA 249(13):1743–1745
10. Levine D, Brown DL, Andreotti RF, et al. (2010) Management ofasymptomatic ovarian and other adnexal cysts imaged at US:Society of Radiologists in Ultrasound Consensus ConferenceStatement. Radiology 256(3):943–954
11. Henschke CI, Yankelevitz DF, Naidich DP, et al. (2004) CTscreening for lung cancer: suspiciousness of nodules according tosize on baseline scans. Radiology 231(1):164–168
12. MacMahon H, Austin J, Gamsu G, et al. (2005) Guidelines formanagement of small pulmonary nodules detected on CT scans: astatement from the Fleischner society. Radiology 237:395–400
13. Khan A, Sultana K (2010) Presenting signs and symptoms ofovarian cancer at a tertiary care hospital. J Pak Med Assoc60(4):260–262
14. Eltabbakh GH, Yadav PR, Morgan A (1999) Clinical picture ofwomen with early stage ovarian cancer. Gynecol Oncol 75:476–479
15. Goff BA, Mandel LS, Melancon CH, Muntz HG (2004) Frequencyof symptoms of ovarian cancer in women presenting to primarycare clinics. JAMA 291(22):2705–2712
16. Age-Adjusted Invasive Cancer Incidence Rates 2004–2008 OvarianCancer (2012) Centers for disease control and prevention website.http://apps.nccd.cdc.gov/uscs/cancersrankedbystate.aspx. Accessed5 December 2012
17. Goff BA, Mandel LS, Drescher CW, et al. (2007) Development ofan ovarian cancer symptom index: possibilities for earlier detection.Cancer 109(2):221–227
18. Sharma D, Dahiya K, Duhan N, Bansal R (2011) Diagnostic lap-aroscopy in chronic pelvic pain. Arch Gynecol Obstet 283:295–297
19. Rodgers S, Kirby C, Smith R, Horrow MM (2012) Imaging aftercesarean delivery: acute and chronic complications. RadioGraphics32:1693–1712
20. Abrao MS, Goncalves M, Dias J, et al. (2007) Comparison betweenclinical examination, transvaginal sonography and magnetic reso-nance imaging for the diagnosis of deep endometriosis. Hum Re-prod 22:3092–3097
21. Bazot M, Bornier C, Dubernard G, et al. (2007) Accuracy ofmagnetic resonance imaging and rectal endoscopic sonography forthe prediction of location of deep pelvic endometriosis. Hum Re-prod 22:1457–1463
22. Grasso R, Di Giacomo V, Sedati P (2010) Diagnosis of deepinfiltrating endometriosis: accuracy of magnetic resonance imagingand transvaginal 3D ultrasonography. Abdom Imaging 35:716–725
23. Cicchiello L, Hamper U, Scoutt L (2011) Ultrasound evaluation ofgynecologic causes of pelvic pain. Obstet Gynecol Clin N Am38:85–114
24. Hunn J, Rodriguez GC (2012) Ovarian cancer: etiology, risk fac-tors, and epidemiology. Clin Obstet Gynecol 55(1):3–23
C. J. Lisanti et al.: Nonvisualization of the ovaries on pelvic ultrasound 167