Embed Size (px)
Citation preview

Nonsteroidal Anti-inflammatory Drug-RelatedGastrointestinal Toxicity:Definitions and Epidemiology
Denis McCarthy, MD, PhD, Albuquerque, New Mexico
Nonsteroidal anti-inflammatory drug (NSAID)-asso-ciated gastrointestinal (GI) toxicity is a broad topicencompassing symptoms as well as severe GI com-plications. GI bleeding and perforation are the 2 over-lapping components that account for the majority ofdeaths and disability associated with these drugs.Abnormal gastric endoscopic profiles as well assymptoms such as heartburn, pain, and dyspepsiaare common in NSAID users, but no correlation hasbeen found between these factors and the occur-rence of the more severe complications; therefore,neither symptoms nor endoscopic observations cannecessarily be considered reliable predictors of fu-ture outcomes. Confounding factors can increasethe risk of complications, and specific NSAIDs vary inthe magnitude and type of risk attending their use.Recent studies have focused on the contribution ofnonprescription NSAIDs to total complications, andcombined with evidence suggesting that the risk isgreatest during the first month of NSAID use, it isapparent that NSAID toxicity is an acute as well as achronic problem. Am J Med. 1998;105(5A):3S–9S.© 1998 by Excerpta Medica, Inc.
Nonsteroidal anti-inflammatory drugs (NSAIDs)are among the most widely prescribed and usedclasses of drugs, with consumption by .30 mil-
lion people in the United States alone.1 Worldwide salesof NSAIDs amount to more than $6 billion per year andaccount for a large portion of the global pharmaceuticalmarket. Nevertheless, some of the most important ques-tions concerning the development of new NSAIDs, theappropriate use of these drugs, and their adverse effectsremain unanswered.
Part of the dilemma in analyzing the risk of an adversegastrointestinal (GI) event is in defining the adverse out-come. NSAID-associated GI toxicity is a broad term in-clusive of manifestations that range from such symptomsas heartburn and dyspepsia that may dissipate after sev-eral weeks of treatment, to such severe complications asbleeding and perforation that lead to hospitalization ordeath. Although symptoms may be more prevalent andare probably the main cause of patient noncompliance,complications result in an estimated 10,000 –20,000deaths per year in the United States and in an even greaternumber of hospitalizations, placing a considerable eco-nomic burden on the healthcare system.2
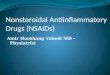
GI bleeding and perforation are 2 separate but overlap-ping components of NSAID-associated toxicity (Figure1). Both of these complications can result in death. Ahistory of peptic ulcer disease can increase the risk of theiroccurrence, although many episodes of GI bleeding andother GI complications do not arise from gastroduodenalulcers. Since there is considerable overlap among the dif-ferent groups circled in Figure 1, it is difficult to deter-mine the transition rates between subgroups, and the pre-cise dimensions of each identified problem are notknown.
This article presents a brief overview of the epidemiol-ogy of the GI complications associated with NSAIDs, in-cluding risk factors, the incidence of symptoms and ad-verse outcomes, and the timing of their occurrence dur-ing the course of treatment.
PREVALENCE AND RISK OF NSAID-ASSOCIATED TOXICITY
The irreversible acetylation of platelets by acetylsalicylicacid (aspirin) significantly affects the incidence of bleed-ing (Figure 1).3 Even regular low-dose and occasional use
From the Department of Veteran’s Affairs and the Division of Gastro-enterology, University of New Mexico School of Medicine, Albuquer-que, New Mexico.
Requests for reprints should be addressed to Denis McCarthy, MD,PhD, USAF/VA Medical Center–111F, 2100 Ridgecrest Drive SE, Build-ing 41, Room 5B-126, Albuquerque, New Mexico 87131–5271.
© 1998 by Excerpta Medica, Inc. 0002-9343/98/$19.00 3SAll rights reserved. PII S0002-9343(98)00274-5

of aspirin has been shown to increase significantly the riskof upper GI bleeding in doses of ,80 mg/day,4 but astatistically significant relation between aspirin use andulcer occurrence has not been observed at dosages ,3 3325 mg tablets daily.5 In contrast, nonaspirin NSAIDspose more of a risk for development of ulcers that maybleed than for causing bleeding from nonulcer sources.This is due in part to the fact that nonaspirin NSAIDsbind reversibly to cyclo-oxygenase. Therefore, throm-boxane (a cyclo-oxygenase– dependent prostaglandin re-quired for platelet aggregation) inhibition is dependenton other factors, such as the plasma levels and the half-lifeof the drug.6 The risk of bleeding is short-lived when us-ing drugs such as ibuprofen, but it is a more importantconsideration when using NSAIDs with long plasma half-lives,6 such as piroxicam, the use of which has been esti-mated to carry a relative risk of 18 (relative to ibuprofen)for upper GI bleeding.7 A long plasma half-life has alsobeen correlated with increased odds ratios for other GIcomplications8 and with increased risk of renal impair-ment.9
The other clinically important adverse GI event asso-ciated with NSAID use is GI perforation. Although theincidence of GI perforation is less than that of bleeding,GI perforation is strongly correlated with NSAID use; therelative risk of perforation is 6 –7, twice as great as that forbleeding, which is 3– 4.8,10 –12
In general, about two-thirds of long-term NSAID userswill have gastric lesions identified at endoscopy.13 Manyof the abnormalities seen are trivial: small mucosal hem-orrhages or erosions that may be scattered throughoutthe fundus and the body of the stomach. There is cur-rently little evidence that these lesions give rise to signif-icant complications.14 However, there is an overall prev-alence of peptic ulcer of about 25% in patients on long-
term NSAID therapy.15 The risk of gastric ulcer is slightlyhigher than that of duodenal ulcer,8,11,13,16 with gastriculcers observed in about 15% of patients and duodenalulcers in about 10%.15 Although no clear epidemiologiclink has been demonstrated between duodenal ulcer in-cidence and NSAID use, approximately half of the ulcercomplications associated with NSAIDs arise from duode-nal ulcers,15,17 indicating that NSAIDs cause complica-tions of peptic ulcers of any etiology, including Helicobac-ter pylori infection, which is present in most patients witha duodenal ulcer.
Many industry-sponsored studies define an ulcer as alesion .3 mm in diameter, without requiring any mea-surement of depth. However, most ulcers that bleed sig-nificantly are normally much larger (8 –30 mm), andbleeding ulcers caused by NSAIDs are usually solitary an-tral ulcers that develop after several months of NSAIDtherapy. From premarketing studies of 8 NSAIDs admin-istered to healthy volunteers screened before the start oftherapy, it has been observed that the cumulative inci-dence of GI bleeding or ulcer complications is constant atabout 2– 4% per year on drug and persists indefinite-ly.18 –20 The risk is also constant in large prescription-based databases.21 There is also a 1% incidence of seriouscomplications in the esophagus, intestine, and colon, anda 70% prevalence of subclinical small bowel enteropathyin patients receiving NSAIDs for $6 months.22–27
Heartburn, pain, and/or dyspepsia may occur in up to60% of patients taking NSAIDs,28 but there is no clearcorrelation between symptoms or endoscopic findingsand complications; several studies have determined thatsymptoms do not predict outcome. In one study, dyspep-sia was observed in ,10% of the patients on NSAIDs whohad abnormal endoscopic results,13 and in another study,55% of the patients with ulcers were asymptomatic.29 The
Figure 1. Overlapping areas of nonsteroidal anti-inflammatory drug (NSAID)–associated toxicity. BU 5 bleeding ulcer;PBU 5 perforated bleeding ulcer; PU 5 perforated ulcer; PUD 5 peptic ulcer disease; † 5 death. Thickness of the arrows indicatesrelative contribution.
A Symposium: NSAID-Associated GI Toxicity/McCarthy
4S November 2, 1998 THE AMERICAN JOURNAL OF MEDICINEt Volume 105 (5A)

Misoprostol Ulcer Complications Outcomes Safety As-sessment (MUCOSA) study30 reported that one-third ofthe patients who developed an adverse GI event, most ofwhich were not clinically significant complications, alsoreported symptoms. However, the more pertinent con-verse observation—the number of patients with symp-toms who had ulcers or complications—was not made.Two studies by Bijlsma28,31 suggested that although thepresence of symptoms was greatest at initiation of NSAIDtherapy, symptoms decreased significantly after 4 weeksof use. There is also some gastric mucosal adaptation tocontinued NSAID use.32 However, in a follow-up to theBijlsma study, patients who had persistent symptoms at 4weeks also had an increased risk of gastric ulceration.33
Thus, persistent symptoms may be more predictive ofserious complications than those at the start of therapy;the timing and persistence of symptoms was not stated inthe MUCOSA study. In another frequently cited article,12
the investigators determined that for 58.2% of patientstaking an NSAID, the first indication of an ulcer was alife-threatening complication. However, this value maybe overestimated by perhaps as much as 70%, since theinvestigators failed to distinguish between complicationsassociated with NSAID use and those attributable toNSAID use, about 30% of the total.
An analysis of several different studies determined therelative risk of specific outcomes associated with a varietyof factors in patients taking aspirin and nonaspirinNSAIDs (Table 1).34 What is apparent is that the risks ofthese outcomes are increased 3–5-fold in NSAID userswhen compared with those not taking such drugs. Thisanalysis, however, was not able to show a specific corre-lation between aspirin use and either perforation ordeath. Although there are few data linking aspirin withdeath, recent studies have suggested that a correlationdoes exist between aspirin use and GI perforation; insome cases aspirin use may be synergistic with other riskfactors, such as concomitant use of NSAIDs.10 In someepidemiologic studies, an increased risk of death has beenassociated with NSAID use.11,35 However, since manyother factors confound the association, not only is thefatality rate probably overestimated, but a direct causalrelation cannot be established. The clinical reality is thatthe attributable risk or etiologic fraction of deaths orcomplications attributable solely to NSAID use remainsunknown, but it is probably 20 –35%. Anecdotal evidencesuggests that the case fatality rate in patients with renalcomplications may be higher than in those with GI com-plications.
RISK FACTORSAll published studies have proposed additional con-founding factors that may increase the risk of NSAID-associated adverse GI events (Table 2).36 –39 However,contributions of these individual factors to the overall
risk, as well as their mechanisms of action, are subject toongoing debate.
AgeAge is a risk factor that appears in every study; there is anincreasing incidence of NSAID-associated GI complica-tions with age. Figure 2 shows relative risk by age ofbleeding or perforation.7 Other factors often associatedwith age, such as comorbidity, polypharmacy, or alteredpharmacokinetics, have also been implicated, but theirspecific contribution to overall risk has not been fullydetermined.40
Alcohol and SmokingHeavy drinking and smoking are 2 factors that may beimplicated in determining increased risk, but the extentof the risk has not been clearly ascertained, partly becauseof lack of data on the magnitude of alcohol and tobaccoconsumption. One study did suggest that alcohol con-sumption of .5 drinks at a time increased the risk signif-icantly above that seen in moderate drinkers and non-
Table 1. Relative Risk (Confidence Intervals) of Outcomesof Aspirin and Nonaspirin NSAID Therapy in Case ControlStudies
Outcome Aspirin Nonaspirin NSAIDs
GI hemorrhage 3.3 (2.39–4.54) 3.09 (2.26–4.24)Gastric ulcer 4.67 (3.06–7.14) 4.03 (2.80–5.78)Duodenal ulcer 1.17 (0.69–1.98) 3.16 (1.78–5.61)Ulcer perforation No data
(uncommon)5.93 (4.00–8.81)
Death No data 7.62 (6.17–9.41)
GI 5 gastrointestinal; NSAID 5 nonsteroidal anti-inflammatory drug.Data from BMJ.34
Table 2. Risk Factors for Developing NSAID-AssociatedGastrointestinal Toxicity
FactorRelative Risk/
Odds Ratio
History of previous peptic ulcer 9.5History of previous GI bleed 6.7History of prior use of H2-receptor
antagonist3.9
Concomitant use of corticosteroids 4.4Concomitant use of anticoagulants 12–16High NSAID dose (.120% average
daily dose)7.7
Concomitant use of $2 NSAIDs 23.3Regular use of NSAID 1 aspirin 3.6Presence of an alcohol-related diagnosis 5.0Irregularity of feeding 14.3
GI 5 gastrointestinal; NSAID 5 nonsteroidal anti-inflammatory drug.Data from Arch Intern Med,36 Am J Med,37 Ann Intern Med,38 and
Arch Intern Med.39
A Symposium: NSAID-Associated GI Toxicity/McCarthy
November 2, 1998 THE AMERICAN JOURNAL OF MEDICINEt Volume 105 (5A) 5S

drinkers.8 A further study suggested a strong associationbetween an alcohol-related diagnosis, such as cirrhosis orpancreatitis (i.e., long-term heavy drinking), and an in-creased risk of GI bleeding.41
The data implicating smoking or Helicobacter pylorigastritis in increasing the risks of NSAIDs, as distinctfrom being independent risk factors for ulcer disease, aremore equivocal, since most studies have not separatedthese risks. Smoking itself is a risk factor for the initiationand recurrence of gastric and duodenal ulcers and inhib-its ulcer healing; nicotine decreases gastric prostaglandinproduction and decreases the acid-buffering capacity ofthe duodenum.42– 44 Data from several studies suggestthat smoking increases the risk of NSAID-associated GItoxicity, but the studies are confounded by a failure toexamine the interactions of smoking and H. pylori infec-tion.8,10,45– 47
Helicobacter pylori InfectionThe question of whether or not H. pylori is a factor inNSAID-associated ulcer complications has not been re-solved. However, in any study of H. pylori, it is importantto consider the type of assay used to determine its pres-ence. Serology, which is generally used to determine H.pylori positivity, more accurately identifies patients whohave been infected but may not necessarily have active orsevere gastritis. This assay has no predictive value for ei-ther the presence of an ulcer or for development of anulcer; experience suggests that, at most, only 16% of se-rologically positive patients ever develop an ulcer, withthe actual risk varying with age of infection, geography,virulence, and host factors. The presence and severity ofgastritis are more predictive of ulcer development. Aslightly more sensitive indicator of ulcer risk is the gastri-tis seen on antral biopsy. In a study by Ekstrom et al,48
among patients not given prophylactic treatment withomeprazole, significantly more ulcers developed inNSAID users who were positive for H. pylori than in thosewho were H. pylori negative. H. pylori status was a better
predictor of ulcer risk in patients with no ulcer history;however, a previous history of ulcer disease was morepredictive of a patient on NSAID therapy developing anulcer than was H. pylori status. This is consistent withother studies that have shown that a prior history of pep-tic ulcer or GI bleeding is a strong predictor of develop-ment of a subsequent NSAID-associated GI complica-tion.7,11,30,37
A recently published study49 suggests that H. pylorigastritis may play some role in the risk of a patient devel-oping an NSAID ulcer. In this study, patients with arthri-tis who were being started on naproxen were randomizedinto groups to be either pretreated with H. pylori eradica-tion or not so treated; H. pylori gastritis was confirmed bybiopsy. The pretreated group developed significantlyfewer new ulcers during naproxen therapy. However,these data are based on an eradication regimen utilizingbismuth, a heavy metal that has been found to remain inGI mucosa for prolonged periods and that may poten-tially heal ulcers in ways unrelated to eradication of H.pylori.50 Thus, a gastroprotective effect of bismuth mayhave confounded interpretation of the study.
Variability Among NSAIDsIt has been shown in several studies that NSAIDs vary intheir likelihood of causing GI complications.51–53 Thereis a current tendency to attribute much of this variabilityto the differential inhibition by the NSAIDs of the 2isoenzymes involved in the synthesis of prostaglandins–cyclo-oxygenase-1 (COX-1) and cyclo-oxygenase-2(COX-2). Improved GI safety is observed with drugs thatspare COX-1,54,55 the isoenzyme responsible for gastro-protection. In contrast, the more toxic drugs demon-strate greater COX-1 inhibition. However, the complex-ity of the physiologic process suggests that these observa-tions may be only partly accurate.56 NSAIDs may haveother, nonprostaglandin-mediated effects that contrib-ute to their toxicity57,58; increasing evidence suggeststhat, in addition to high doses of NSAIDs, pharmacologicproperties, such as long plasma half-life and enterohe-patic recirculation, contribute significantly to GI compli-cations.6,8,59,60
Other FactorsPrior use of histamine-2 (H2)–receptor antagonists, re-gardless of diagnosis, is also an indicator of risk, as isconcomitant use of NSAIDs with corticosteroids, antico-agulants, or aspirin.37–39 Increased NSAID dosages abovethe average daily dose and use of multiple NSAIDs alsosignificantly increase the risk.7,16,52 These latter factorshave become problems in the United States, when pa-tients add NSAIDs purchased over the counter to thedrug prescribed by their physician and when physiciansincrease dosages to improve efficacy.
Figure 2. Relative risk by age for developing gastrointestinal(GI) bleeding or perforation in nonsteroidal anti-inflammatorydrug (NSAID) users. (Data from Lancet.7)
A Symposium: NSAID-Associated GI Toxicity/McCarthy
6S November 2, 1998 THE AMERICAN JOURNAL OF MEDICINEt Volume 105 (5A)

TIMING
One factor that consistently arises in the various studies isthe length of time that a person is on NSAIDs, i.e., acuteversus chronic use. Data from epidemiologic sources sug-gest that the risk of NSAID toxicity is greatest early in thecourse of treatment.8,11,16,61 A meta-analysis of 16 studiespublished by Gabriel et al11 showed that the greatest riskwas during the first month of therapy and subsequentlydecreased by the fourth month, remaining stable for aslong as the patient remained on the drug (Figure 3). Thistime frame has been consistent in most other studies, andit should be noted that in this respect the pattern of usebecomes an issue. By focusing the problem on chronicusers, the greatest part of the risk may be missed. How-ever, in prospective studies conducted before marketing,where high-risk patients with co-morbid conditions areexcluded from entry, the risk remains constant for years.This is also true of aspirin therapy.
A Dutch study62 of NSAID use determined that 74% ofthe users were taking NSAIDs for ,30 days and that al-though only 5% were long-term users, they accounted for17% of total drug use. It may be argued that acute NSAIDuse is more prevalent than chronic use, especially fortreatment of pain syndromes. In support of this notion, arecent US survey indicated that most cases of GI bleedingoccur in patients using nonprescription NSAIDs for briefperiods,63 confirming the results of previous studies.64,65
SUMMARY
The epidemiologic literature relating to NSAID-associ-ated toxicity is extensive, and conclusions drawn from itmay be contradictory and confusing because of differentstudy endpoints and considerable overlap among clinicaloutcomes. Nevertheless, large epidemiologic studies have
used the available data to estimate the incidence and riskof the 2 major GI side effects associated with NSAIDuse— bleeding and perforation. Some of these studieshave also identified additional patient factors that may beused as predictors for clinically relevant outcomes. Nocorrelation has been established between the presence ofsymptoms and clinical outcomes, although certain con-ditions or factors, such as age or a prior history of ulcer orbleeding, may be strongly predictive.
Results of epidemiologic studies in unscreened popu-lations strongly suggest that the greatest risk of seriousadverse events occurs early in the course of NSAID treat-ment. This observation, combined with recent reportsthat a significant proportion of patients having GI bleedsare users of over-the-counter aspirin or NSAIDs and withprevious data suggesting that many users take NSAIDsfor ,1 month, indicates that NSAID-associated toxicityis an acute as well as a chronic problem. Nevertheless,there is still much work that can be done to characterizeNSAID toxicity more clearly and to establish a viable ap-proach to assessing and decreasing risks in all patientsrequiring these drugs.
REFERENCES1. Gabriel SE, Fehring RA. Trends in the utilization of non-
steroidal anti-inflammatory drugs in the United States,1986–1990. J Clin Epidemiol. 1992;45:1041–1044.
2. Fries JF. NSAID gastropathy: the second most deadly rheu-matic disease? Epidemiology and risk appraisal. J Rheu-matol. 1991;18(suppl 28):6–10.
3. Lanas AI, Arroyo MT, Esteva F, et al. Aspirin related gas-trointestinal bleeders have an exaggerated bleeding timeresponse due to aspirin use. Gut. 1996;39:654–660.
4. Levy M, Miller DR, Kaufman DW, et al. Major upper gastro-intestinal tract bleeding: relation to the use of aspirin andother nonnarcotic analgesics. Arch Intern Med. 1988;148:281–285.
5. Graham DY, Smith JL. Aspirin and the stomach. Ann InternMed. 1986;104:390–398.
6. Schafer AI. Effects of nonsteroidal antiinflammatory drugson platelet function and systemic hemostasis. J Clin Phar-macol. 1995;35:209–219.
7. Garcıa Rodrıguez LA, Jick H. Risk of upper gastrointestinalbleeding and perforation associated with individual non-steroidal anti-inflammatory drugs. Lancet. 1994;343:769–772.
8. Henry D, Dobson A, Turner C. Variability in the risk of majorgastrointestinal complications from nonaspirin nonsteroidalanti-inflammatory drugs. Gastroenterology. 1993;105:1078–1088.
9. Henry D, Page J, Whyte I, et al. Consumption of non-steroidal anti-inflammatory drugs and the development offunctional renal impairment in elderly subjects: results of acase-control study. Br J Clin Pharmacol. 1997;44:85–90.
10. Lanas A, Serrano P, Bajador E, et al. Evidence of aspirinuse in both upper and lower gastrointestinal perforation.Gastroenterology. 1997;112:683–689.
11. Gabriel SE, Jaakkimainen L, Bombardier C. Risk for seriousgastrointestinal complications related to use of nonsteroi-dal anti-inflammatory drugs: a meta-analysis. Ann InternMed. 1991;115:787–796.
Figure 3. Risk of nonsteroidal anti-inflammatory drug(NSAID)–associated gastrointestinal (GI) toxicity and durationof therapy in retrospective case control studies with no exclu-sion for ulcer or GI disease. (Data from Ann Intern Med.11)
A Symposium: NSAID-Associated GI Toxicity/McCarthy
November 2, 1998 THE AMERICAN JOURNAL OF MEDICINEt Volume 105 (5A) 7S

12. Armstrong CP, Blower AL. Non-steroidal anti-inflammatorydrugs and life threatening complications of peptic ulcer-ation. Gut. 1987;28:527–532.
13. Larkai EN, Smith JL, Lidsky MD, Graham DY. Gastroduo-denal mucosa and dyspeptic symptoms in arthritic patientsduring chronic nonsteroidal anti-inflammatory drug use.Am J Gastroenterol. 1987;82:1153–1158.
14. Graham DY, Smith JL. Gastroduodenal complications ofchronic NSAID therapy. Am J Gastroenterol. 1988;83:1081–1084.
15. McCarthy DM. Nonsteroidal antiinflammatory drug-in-duced ulcers: management by traditional therapies. Gas-troenterology. 1989;96(suppl):662–674.
16. Griffin MR, Piper JM, Daugherty JR, et al. Nonsteroidalanti-inflammatory drug use and increased risk for pepticulcer disease in elderly persons. Ann Intern Med. 1991;114:257–263.
17. Soll AH, Weinstein WM, Kurata J, McCarthy D. Nonsteroi-dal anti-inflammatory drugs and peptic ulcer disease. AnnIntern Med. 1991;114:307–319.
18. Paulus HE. FDA Arthritis Committee Meeting: seriousgastrointestinal toxicity of nonsteroidal/anti-inflammatorydrugs; drug-containing renal and biliary stones; diclofenacand carprofen approved. Arthritis Rheum. 1988;31:1450–1451.
19. Temple R. Quoted in: FDA’s NSAID G-I warning. Scrip.December 15, 1986; No. 1163:11.
20. Labeling revisions for NSAIDs. FDA Drug Bulletin. February,1989;19:3–4.
21. MacDonald TM, Morant SV, Robinson GC, et al. Associa-tion of upper gastrointestinal toxicity of non-steroidal anti-inflammatory drugs with continued exposure: cohort study.BMJ. 1997;315:1333–1337.
22. Tympner F. Gastroscopic findings after therapy with non-steroid antirheumatic drugs. Z Rheumatol. 1981;40:179–181.
23. Kikendall JW, Friedman AC, Oyewole MA, et al. Pill-in-duced esophageal injury: case reports and review of themedical literature. Dig Dis Sci. 1983;28:174–182.
24. Heller SR, Fellows IW, Ogilvie AL, Atkinson M. Non-steroi-dal anti-inflammatory drugs and benign oesophageal stric-ture. BMJ. 1982;285:167–168.
25. Banerjee AK. Enteropathy induced by non-steroidal anti-inflammatory drugs. BMJ. 1989;298:1539–1540.
26. Lanas A, Sekar MC, Hirschowitz BI. Objective evidence ofaspirin use in both ulcer and nonulcer upper and lowergastrointestinal bleeding. Gastroenterology. 1992;103:862–869.
27. Langman MJS, Morgan L, Worrall A. Use of anti-inflamma-tory drugs by patients admitted with small or large bowelperforations and haemorrhage. Br Med J (Clin Res Ed).1985;290:347–349.
28. Bijlsma J. Treatment of endoscopy-negative NSAID-in-duced upper gastrointestinal symptoms with cimetidine.Aliment Pharmacol Ther. 1988;2(suppl 1):75–83.
29. Taha AS, Dahill S, Sturrock RD, et al. Predicting NSAIDrelated ulcers: assessment of clinical and pathological riskfactors and importance of differences in NSAID. Gut. 1994;35:891–895.
30. Simon LS, Hatoum HT, Bittman RM, et al. Risk factors forserious nonsteroidal-induced gastrointestinal complica-tions: regression analysis of the MUCOSA trial. Fam Med.1996;28:204–210.
31. Bijlsma JW. Treatment of NSAID-induced gastrointestinal
lesions with cimetidine: an international multicentre collab-orative study. Aliment Pharmacol Ther. 1988;2S:85–95.
32. Olivero JJ, Graham DY. Gastric adaptation to nonsteroidalanti-inflammatory drugs in man. Scand J Gastroenterol.1992;27(suppl 193):53–58.
33. Wallin BA, Grier CE, Fox MJ, et al. Prevention of NSAID-induced ulcers with cimetidine: results of a double-blind,placebo controlled trial. (Abstr.) Gastroenterology. 1990;98(suppl):A146..
34. Hawkey CJ. Non-steroidal anti-inflammatory drugs andpeptic ulcers: facts and figures multiply, but do they addup? BMJ. 1990;300:278–284.
35. Griffin MR, Ray WA, Schaffner W. Nonsteroidal anti-inflam-matory drug use and death from peptic ulcer in elderlypersons. Ann Intern Med. 1988;109:359–363.
36. Carson JL, Strom BL, Soper KA, et al. The association ofnonsteroidal anti-inflammatory drugs with upper gastroin-testinal tract bleeding. Arch Intern Med. 1987;147:85–88.
37. Fries JF, Williams CA, Bloch DA, Michel BA. Nonsteroidalanti-inflammatory drug-associated gastropathy: incidenceand risk factor models. Am J Med. 1991;91:213–222.
38. Piper JM, Ray WA, Daugherty JR, Griffin MR. Corticoste-roid use and peptic ulcer disease: role of nonsteroidalanti-inflammatory drugs. Ann Intern Med. 1991;114:735–740.
39. Shorr RI, Ray WA, Daugherty JR, Griffin MR. Concurrentuse of nonsteroidal anti-inflammatory drugs and oral anti-coagulants places elderly persons at high risk for hemor-rhagic peptic ulcer disease. Arch Intern Med. 1993;153:1665–1670.
40. Davies NM, Wallace JL. Selective inhibitors of cyclooxy-genase-2. Potential in elderly patients. Drugs Aging. 1996;9:406–417.
41. Hochain P, Berkelmans I, Czernichow P, et al. Which pa-tients taking non-aspirin non-steroidal anti-inflammatorydrugs bleed? A case-control study. Eur J GastroenterolHepatol. 1995;7:419–426.
42. Orlando RC. Peptic ulcer: factors influencing recurrence.J Clin Gastroenterol. 1987;9(suppl 1):2–7.
43. Lindell G, Farnebo LO, Chen D, et al. Acute effects ofsmoking during modified sham feeding in duodenal ulcerpatients: an analysis of nicotine, acid secretion, gastrin,catecholamines, epidermal growth factor, prostaglandinE2, and bile acids. Scand J Gastroenterol. 1993;28:487–494.
44. Baumeister B, Schmidt C, Schiermeyer-Dunkhase B, et al.Decreased gastric prostaglandin E2 synthesis in patientswith gastric ulcers and in smokers. Hepatogastroenterol-ogy. 1995;42:851–855.
45. Willoughby JM, Essigman WK, Weber JC, Pineura RF.Smoking and peptic ulcer in rheumatoid arthritis. Clin ExpRheumatol. 1986;4:31–35.
46. Yeomans ND, Elliott SL, Edwards J, et al. Gastroduodenaldamage during therapy with nonsteroidal antiinflammatorydrugs: prevalence in arthritis clinic patients and effect ofsmoking. (Abstr.) Gastroenterology. 1988;94:A510.
47. Farah D, Sturrock RD, Russell RI. Peptic ulcer in rheuma-toid arthritis. Ann Rheum Dis. 1988;47:478–480.
48. Ekstrom P, Carling L, Wetterhus S, et al. Prevention ofpeptic ulcer and dyspeptic symptoms with omeprazole inpatients receiving continuous non-steroidal anti-inflamma-tory drug therapy: a Nordic multicentre study. Scand JGastroenterol. 1996;31:753–758.
49. Chan FK, Sung JJ, Chung SC, et al. Randomised trial oferadication of Helicobacter pylori before non-steroidal anti-
A Symposium: NSAID-Associated GI Toxicity/McCarthy
8S November 2, 1998 THE AMERICAN JOURNAL OF MEDICINEt Volume 105 (5A)

inflammatory drug therapy to prevent peptic ulcers. Lancet.1997;350:975–979.
50. Wagstaff AJ, Benfield P, Monk JP. Colloidal bismuthsubcitrate: a review of its pharmacodynamic and pharma-cokinetic properties, and its therapeutic use in peptic ulcerdisease. Drugs. 1988;36:132–157.
51. Fries JF, Williams CA, Bloch DA. The relative toxicity ofnonsteroidal antiinflammatory drugs. Arthritis Rheum.1991;34:1353–1360.
52. Henry D, Lim LL-Y, Garcıa Rodrıguez LA, et al. Variability inrisk of gastrointestinal complications with individual non-steroidal anti-inflammatory drugs: results of a collaborativemeta-analysis. BMJ. 1996;312:1563–1566.
53. Singh G, Terry R, Ramey DR, et al. Comparative GI toxicityof NSAIDs. (Abstr.) Arthritis Rheum. 1997;40(suppl):S115.
54. Distel M, Mueller C, Bluhmki E, Fries J. Safety ofmeloxicam: a global analysis of clinical trials. Br J Rheuma-tol. 1996;35(suppl 1):68–77.
55. Lanza FL, Rack MF, Callison DA, et al. A pilot endoscopicstudy of the gastroduodenal effects of SC-58635, a novelCOX-2-selective inhibitor. (Abstr.) Gastroenterology. 1997;112(suppl):A194.
56. Blower PR. Non-steroidal anti-inflammatory drugs. Br JRheumatol. 1993;32(suppl 4):35–38.
57. Anthony A, Bahl AK, Oakley IG, et al. The b3-adrenoceptoragonist CL316243 prevents indomethacin-induced jejunalulceration in the rat by reversing early villous shortening.J Pathol. 1996;179:340–346.
58. Kuratani K, Kodama H, Yamaguchi I. Enhancement of gas-tric mucosal blood flow by b3 adrenergic agonists prevents
indomethacin-induced antral ulcer in the rat. J PharmacolExp Ther. 1994;270:559–565.
59. Reuter BK, Davies NM, Wallace JL. Nonsteroidal anti-in-flammatory drug enteropathy in rats: role of permeability,bacteria, and enterohepatic circulation. Gastroenterology.1997;112:109–117.
60. Brune K, Nurnberg B, Szelenyi I, Vergin H. The enterohe-patic circulation of some anti-inflammatory drugs maycause intestinal ulcerations. In: Rainsford KD, Velo GP, eds.Side-Effects of Anti-inflammatory Drugs. Part II: Studies inMajor Organ Systems. Lancaster: MTP Press, 1987:29–39.
61. Perez Gutthann S, Garcıa Rodrıguez LA, Raiford DS, et al.Non-steroidal anti-inflammatory drugs and the risk of hos-pitalization for acute renal failure. Arch Intern Med. 1996;156:2433–2439.
62. Leufkens HG, Ameling CB, Hekster YA, Bakker A. Utiliza-tion patterns of non-steroidal anti-inflammatory drugs in anopen Dutch population. Pharm Weekbl Sci. 1990;12:97–103.
63. Peura DA, Lanza FL, Gostout CJ, Foutch PG. The AmericanCollege of Gastroenterology Bleeding Registry: preliminaryfindings. Am J Gastroenterol. 1997;92:924–928.
64. Wilcox CM, Shalek KA, Cotsonis G. Striking prevalence ofover-the-counter nonsteroidal anti-inflammatory drug usein patients with upper gastrointestinal hemorrhage. ArchIntern Med. 1994;154:42–46.
65. Saleeby G, Holt L, Holt S. Pattern and prevalence of non-steroidal anti-inflammatory drug (NSAID) use in compli-cated peptic ulcer disease (CPUD). (Abstr.) Gastroenterol-ogy. 1991;100(suppl):A17.
A Symposium: NSAID-Associated GI Toxicity/McCarthy
November 2, 1998 THE AMERICAN JOURNAL OF MEDICINEt Volume 105 (5A) 9S








![Case Report - downloads.hindawi.comdownloads.hindawi.com/journals/cripe/2012/624168.pdf · 2 Case Reports in Pediatrics gastrointestinal toxicity, typically diarrhea [3]. Patients](https://img.pdfslide.us/doc/110x75/5e43da0eb5227f59f061c347/case-report-2-case-reports-in-pediatrics-gastrointestinal-toxicity-typically.jpg)