Embed Size (px)
Citation preview

Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Rx Topical CorticosteroidsHPA Axis Suppression HPA Axis Suppression
and and Cutaneous EffectsCutaneous Effects
Denise Cook, M.D.Medical Officer
Division of Dermatologyand Dental Drug Products

2Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
OUTLINEOUTLINE
• Background• Class Labeling for Topical Corticosteroids• HPA Axis Suppression – The FDA Experience
– Trial Data from Approved Drug Products– Resultant Labeling Changes– Postmarketing Summary
• Cutaneous Adverse Events from Topical Corticosteroid Use
• Background• Class Labeling for Topical Corticosteroids• HPA Axis Suppression – The FDA Experience
– Trial Data from Approved Drug Products– Resultant Labeling Changes– Postmarketing Summary
• Cutaneous Adverse Events from Topical Corticosteroid Use

3Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Topical Corticosteroid ClassificationTopical Corticosteroid Classification
• Seven Classes – Class I – Superpotent– Class II – High Potency– Classes III, IV, V, VI – Midpotency– Class VII – Low Potency
• Vasoconstrictor Assay
• Seven Classes – Class I – Superpotent– Class II – High Potency– Classes III, IV, V, VI – Midpotency– Class VII – Low Potency
• Vasoconstrictor Assay

4Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Cosyntropin Stimulation TestCosyntropin Stimulation Test
• Used to assess the function of the end organ - the adrenal gland - in the hypothalamic-pituitary- adrenal axis
• In the case of topical corticosteroids, assessing an exogenous unwanted treatment effect
• Cosyntropin 0.125 mg or 0.25 mg is administered IV at baseline and end of treatment
• Blood is drawn for serum cortisol values at 30 minutes and sometimes 60 minutes post stimulation
• Interpretation of the results determines a normal or abnormal response
• Used to assess the function of the end organ - the adrenal gland - in the hypothalamic-pituitary- adrenal axis
• In the case of topical corticosteroids, assessing an exogenous unwanted treatment effect
• Cosyntropin 0.125 mg or 0.25 mg is administered IV at baseline and end of treatment
• Blood is drawn for serum cortisol values at 30 minutes and sometimes 60 minutes post stimulation
• Interpretation of the results determines a normal or abnormal response

5Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Evolution of Interpretation of Normal Function of the HPA Axis
Evolution of Interpretation of Normal Function of the HPA Axis
• 1985– am serum cortisol– Urinary corticoid concentrations
• 1996 – Cosyntropin Stimulation Test– 30 minute post stimulation serum cortisol > 20 µg/dL– If prestimulation serum cortisol 20 µg/dL, then needed
a 6ug/dL increment
• 1999– 30 minute post stimulation cortisol > 18 µg/dL
• 1985– am serum cortisol– Urinary corticoid concentrations
• 1996 – Cosyntropin Stimulation Test– 30 minute post stimulation serum cortisol > 20 µg/dL– If prestimulation serum cortisol 20 µg/dL, then needed
a 6ug/dL increment
• 1999– 30 minute post stimulation cortisol > 18 µg/dL

6Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Evolution of Interpretation of Normal Function of the HPA Axis
Evolution of Interpretation of Normal Function of the HPA Axis
• 2001 - Cosyntropin Stimulation Test– Control plasma cortisol level should exceed 5 µg/100mL– 30 minute level should show an increment of at least 7 µg/100mL– 30 minute level should exceed 18 µg/100mL
• 2004– 30 minute level should exceed 18 µg/100mL
• 2001 - Cosyntropin Stimulation Test– Control plasma cortisol level should exceed 5 µg/100mL– 30 minute level should show an increment of at least 7 µg/100mL– 30 minute level should exceed 18 µg/100mL
• 2004– 30 minute level should exceed 18 µg/100mL

7Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Class Labeling for Rx Topical Corticosteroids - 1990
Class Labeling for Rx Topical Corticosteroids - 1990
• Effects on the HPA Axis• Effects on Glucose Metabolism• Development of Cushing’s Syndrome• Effects on Growth• Effects on Intracranial Pressure
• Effects on the HPA Axis• Effects on Glucose Metabolism• Development of Cushing’s Syndrome• Effects on Growth• Effects on Intracranial Pressure

8Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Two open-label trials withTemovateTM Ointment:
Two open-label trials withTemovateTM Ointment:
Trial 1:
• 6 adult patients with psoriasis applied 7 grams/day to 30% BSA for 7 days
• ACTH stimulation was performed at baseline and 2 post-treatment A.M. cortisols
• 3/6 or 50% of patients exhibited decreases in cortisol production
Trial 1:
• 6 adult patients with psoriasis applied 7 grams/day to 30% BSA for 7 days
• ACTH stimulation was performed at baseline and 2 post-treatment A.M. cortisols
• 3/6 or 50% of patients exhibited decreases in cortisol production

9Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Two open-label trials with TemovateTM Ointment (cont’d):
Two open-label trials with TemovateTM Ointment (cont’d):
Trial 2:
• Objective - determine the largest dose over a 7 day period that would not cause significant suppression of the adrenal gland
• 3 doses were used - 7 grams/day, 3.5 grams/day, 2.0 grams/day
• Suppression was determined by A.M. plasma cortisol levels and urinary corticoid concentrations
• None of the psoriatic patients suppressed at 7.0 grams/day or 3.5 grams/day but doses as low as 2.0 grams/day caused marked suppression of cortisol secretion in patients with atopic dermatitis.
Trial 2:
• Objective - determine the largest dose over a 7 day period that would not cause significant suppression of the adrenal gland
• 3 doses were used - 7 grams/day, 3.5 grams/day, 2.0 grams/day
• Suppression was determined by A.M. plasma cortisol levels and urinary corticoid concentrations
• None of the psoriatic patients suppressed at 7.0 grams/day or 3.5 grams/day but doses as low as 2.0 grams/day caused marked suppression of cortisol secretion in patients with atopic dermatitis.

10Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Temovate Label - 1985Temovate Label - 1985
• TEMOVATETM (clobetasol cream and ointment), 0.05%, a Class I steroid
• PRECAUTIONS: General: TEMOVATETM is a highly potent topical corticosteroid that has been shown to suppress the HPA axis at doses as low as 2 g per day.
• Pediatric Use: Use of TEMOVATETM Cream and Ointment in children under 12 years of age is not recommended.
• TEMOVATETM (clobetasol cream and ointment), 0.05%, a Class I steroid
• PRECAUTIONS: General: TEMOVATETM is a highly potent topical corticosteroid that has been shown to suppress the HPA axis at doses as low as 2 g per day.
• Pediatric Use: Use of TEMOVATETM Cream and Ointment in children under 12 years of age is not recommended.

11Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Class LabelPrecautions Section

12Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
General: Systemic absorption of topical corticosteroids can produce reversible hypothalamic-pituitary-adrenal (HPA) axis suppression with the potential for gluco- corticosteroid insufficiency after withdrawal from treatment. Manifestations of Cushing's syndrome, hyperglycemia, and glucosuria can also be produced in some patients by systemic absorption of topical corticosteroids while on treatment.
General: Systemic absorption of topical corticosteroids can produce reversible hypothalamic-pituitary-adrenal (HPA) axis suppression with the potential for gluco- corticosteroid insufficiency after withdrawal from treatment. Manifestations of Cushing's syndrome, hyperglycemia, and glucosuria can also be produced in some patients by systemic absorption of topical corticosteroids while on treatment.

13Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Patients applying a potent topical steroid to a large surface area or to areas under occlusion should be evaluated periodically for evidence of HPA axis suppression. This may be done by using the ACTH stimulation, A.M. plasma cortisol, and urinary free cortisol tests.
Patients applying a potent topical steroid to a large surface area or to areas under occlusion should be evaluated periodically for evidence of HPA axis suppression. This may be done by using the ACTH stimulation, A.M. plasma cortisol, and urinary free cortisol tests.

14Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
If HPA axis suppression is noted, an attempt should be made to withdraw the drug, to reduce the frequency of application, or to substitute a less potent steroid. Recovery of HPA axis function is generally prompt upon discontinuation of topical corticosteroids. Infrequently, signs and symptoms of glucocorticosteroid insufficiency may occur requiring supplemental systemic corticosteroids.
If HPA axis suppression is noted, an attempt should be made to withdraw the drug, to reduce the frequency of application, or to substitute a less potent steroid. Recovery of HPA axis function is generally prompt upon discontinuation of topical corticosteroids. Infrequently, signs and symptoms of glucocorticosteroid insufficiency may occur requiring supplemental systemic corticosteroids.

15Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Class LabelPediatric Use Section
Class LabelPediatric Use Section

16Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Safety and effectiveness in children and infants have not been established. Because of a higher ratio of skin surface area to body mass, children are at a greater risk than adults of HPA-axis-suppression when they are treated with topical corticosteroids. They are therefore also at greater risk of glucocorticosteroid insufficiency after withdrawal of treatment and of Cushing's syndrome while on treatment.
Safety and effectiveness in children and infants have not been established. Because of a higher ratio of skin surface area to body mass, children are at a greater risk than adults of HPA-axis-suppression when they are treated with topical corticosteroids. They are therefore also at greater risk of glucocorticosteroid insufficiency after withdrawal of treatment and of Cushing's syndrome while on treatment.

17Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
HPA axis suppression, Cushing's syndrome, linear growth retardation, delayed weight gain, and intracranial hypertension have been reported in pediatric patients receiving topical corticosteroids. Manifestations of adrenal suppression in pediatric patients include low plasma cortisol levels to an absence of response to ACTH stimulation. Manifestations of intracranial hypertension include bulging fontanelles, headaches, and bilateral papilledema.
HPA axis suppression, Cushing's syndrome, linear growth retardation, delayed weight gain, and intracranial hypertension have been reported in pediatric patients receiving topical corticosteroids. Manifestations of adrenal suppression in pediatric patients include low plasma cortisol levels to an absence of response to ACTH stimulation. Manifestations of intracranial hypertension include bulging fontanelles, headaches, and bilateral papilledema.

18Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Topical Corticosteroid DataHPA Axis Suppression
Topical Corticosteroid DataHPA Axis Suppression
• 10 drug products– 8 topical corticosteroid products– 2 topical combination drug products
• 11 studies• Ages 3 months – adult• Open-label trials• Cosyntropin stimulation test
• 10 drug products– 8 topical corticosteroid products– 2 topical combination drug products
• 11 studies• Ages 3 months – adult• Open-label trials• Cosyntropin stimulation test

19Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Topical Corticosteroid Drug ProductsTopical Corticosteroid Drug Products
• Dermatop – a mid potency steroid• Cutivate Cream – a mid potency steroid• Diprolene AF Cream – a high potency steroid• Diprosone Ointment – a high potency steroid• Diprosone Cream – a mid potency steroid• Diprosone Lotion – a mid potency steroid• Clobex Lotion – a super potent steroid• Temovate E Cream – a super potent steroid
• Dermatop – a mid potency steroid• Cutivate Cream – a mid potency steroid• Diprolene AF Cream – a high potency steroid• Diprosone Ointment – a high potency steroid• Diprosone Cream – a mid potency steroid• Diprosone Lotion – a mid potency steroid• Clobex Lotion – a super potent steroid• Temovate E Cream – a super potent steroid

20Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Dermatop (prednicarbate emollient cream), 0.1%a Class V steroid
Approved May 1996
Pediatric Atopic Dermatitis Trial
Dermatop (prednicarbate emollient cream), 0.1%a Class V steroid
Approved May 1996
Pediatric Atopic Dermatitis Trial

21Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
• 59 pediatric patients enrolled
• 2 targeted populations
- patients between 1 month and 2 years- patients between 2 and 12 years
• 10 patients were <2 years old
• 49 patients were ≥ 2 years old
• 59 pediatric patients enrolled
• 2 targeted populations
- patients between 1 month and 2 years- patients between 2 and 12 years
• 10 patients were <2 years old
• 49 patients were ≥ 2 years old

22Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Treatment CriteriaTreatment Criteria
• >20% body surface area (BSA) involvement Twice daily for 21 consecutive days
• ACTH Stimulation Test
• Cosyntropin administered at baseline and day 22 – Patients ≥ 15 kg received 0.25 mg IV– Patients < 15 kg received 0.125 mg IV
• >20% body surface area (BSA) involvement Twice daily for 21 consecutive days
• ACTH Stimulation Test
• Cosyntropin administered at baseline and day 22 – Patients ≥ 15 kg received 0.25 mg IV– Patients < 15 kg received 0.125 mg IV

23Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Criteria per protocol for a normal adrenal response to ACTH stimulation at 30 and 60 minutes:
Criteria per protocol for a normal adrenal response to ACTH stimulation at 30 and 60 minutes:
• Post stimulation serum cortisol >20 µg/dL
• If pre-stimulation serum cortisol levels > 20 µg/dL, an incremental increase >6 µg/dL in serum cortisol
• Post stimulation serum cortisol >20 µg/dL
• If pre-stimulation serum cortisol levels > 20 µg/dL, an incremental increase >6 µg/dL in serum cortisol

24Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Three patients according to the protocol criteria were suppressed:
2 patients, 1 an 18 month old, had a peak response of 5 µg/dL change from baseline. 1 patient had a post-stimulation cortisol value that decreased from baseline.
At that time, the Agency agreed with an outside endocrinologist that since these 3 patients had a post-stimulation response that was greater than 20 µg/dL, although they didn't have the required incremental rise, they would not be considered suppressed.
This led to the current label that reads that "none of the 59 patients showed evidence of HPA axis suppression."

25Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Cutivate (fluticasone) Cream, 0.05%a Class V steroid
Approved June 17, 1999
Pediatric Atopic Dermatitis andPsoriasis Trial

26Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
• 43 patients were evaluable ( all with moderate to severe atopic dermatitis)
• 29 patients – 3 months to 2 years old• 14 patients – 3 years to 5 years old
• 43 patients were evaluable ( all with moderate to severe atopic dermatitis)
• 29 patients – 3 months to 2 years old• 14 patients – 3 years to 5 years old

27Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Treatment CriteriaTreatment Criteria
• At least 35% BSA involvement
• Bid application for 3 - 4 weeks
• Patients up to 2 years limited to120 grams/week
• Patients 3-5 years of age limitedto 180 grams/week
• At least 35% BSA involvement
• Bid application for 3 - 4 weeks
• Patients up to 2 years limited to120 grams/week
• Patients 3-5 years of age limitedto 180 grams/week

28Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
BSA Improvement Over Time(N=46)
BSA Improvement Over Time(N=46)
• 23 (50%) had a decrease of 50% by 2 weeks
• 9 (20%) had a decrease of 50% by 3 weeks
• 4 (9%) had a 50% decrease by 4 weeks
• 23 (50%) had a decrease of 50% by 2 weeks
• 9 (20%) had a decrease of 50% by 3 weeks
• 4 (9%) had a 50% decrease by 4 weeks

29Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Cosyntropin Stimulation TestCosyntropin Stimulation Test
• Test administered at baseline andend of treatment
• Younger age group given 0.125 mg cosyntropin IV
• Older age group given 0.25 mg cosyntropin IV
• Test administered at baseline andend of treatment
• Younger age group given 0.125 mg cosyntropin IV
• Older age group given 0.25 mg cosyntropin IV

30Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Normal responseCosyntropin Stimulation Test
Normal responseCosyntropin Stimulation Test
A serum cortisol level >18 µg/dLat 30 minutes post-stimulation

31Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
2 out of 43 patients experienced adrenal suppression
2 out of 43 patients experienced adrenal suppression
Serum Cortisol (g/dL)
Baseline End-Tx Follow-up
Subject Age/Sex %BSA Severity Duration Amt. Used
Pre-stim
Post-stim
Pre-stim
Post-stim
Pre-stim
Post-stim
B201 5 yrs/M 95 (95) 22 (9) 4 weeks 561.0 grams
22.1 33.9 7.1 11.8 2.1 19.8
B202 2 yrs/M 35 (35) 17 (7) 5 weeks 176.5 grams
10.8 28.6 2.1 9.4 LTF LTF

32Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Label Change for Cutivate CreamLabel Change for Cutivate Cream
• Indication – Children as young as 3 months of age for up to 4 weeks of use
• Safety Update Information – Precautions: General and Pediatric Use Sections
• Indication – Children as young as 3 months of age for up to 4 weeks of use
• Safety Update Information – Precautions: General and Pediatric Use Sections

33Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Betamethasone Propionate - Approved in 2001Betamethasone Propionate - Approved in 2001
• Diprolene AF Cream, 0.05% - a Class II steroid
• Diprosone Ointment, 0.05% - a Class II steroid
• Diprosone Cream, 0.05% - a Class III steroid
• Diprosone Lotion, 0.05% - a Class V steroid
• Lotrisone Cream and Lotion (clotrimazole and betamethasone propionate)
• Diprolene AF Cream, 0.05% - a Class II steroid
• Diprosone Ointment, 0.05% - a Class II steroid
• Diprosone Cream, 0.05% - a Class III steroid
• Diprosone Lotion, 0.05% - a Class V steroid
• Lotrisone Cream and Lotion (clotrimazole and betamethasone propionate)

34Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Criteria for a Normal HPA Axis ResponseCriteria for a Normal HPA Axis Response
• Follow the Cortrosyn® label
• Failure of any one of 3 criteria would indicate suppression of the HPA axis
• Stimulation should occur at baseline and end of treatment
• Follow the Cortrosyn® label
• Failure of any one of 3 criteria would indicate suppression of the HPA axis
• Stimulation should occur at baseline and end of treatment

35Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Criteria - 30 minute post-stimulationCriteria - 30 minute post-stimulation
• The control plasma cortisol level should exceed 5 µg/100 mL
• The 30-minute level should show an increment of at least 7 µg/100mLabove the basal level
• The 30-minute level should exceed18 µg/100mL
• The control plasma cortisol level should exceed 5 µg/100 mL
• The 30-minute level should show an increment of at least 7 µg/100mLabove the basal level
• The 30-minute level should exceed18 µg/100mL

36Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Diprolene AF Cream, 0.05%Diprolene AF Cream, 0.05%
• 60 evaluable patients,ages 1-12 years with atopic dermatitis
• Mean BSA involvement - 58%(range: 35% - 95%)
• Used study drug bid for 2 - 3 weeks– Limited to 45 grams/week
• 60 evaluable patients,ages 1-12 years with atopic dermatitis
• Mean BSA involvement - 58%(range: 35% - 95%)
• Used study drug bid for 2 - 3 weeks– Limited to 45 grams/week

37Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Diprolene AF Cream, 0.05% (cont’d)Diprolene AF Cream, 0.05% (cont’d)
• 19/60 or 32% of these patients showed evidence of HPA axis suppression
• 11/19 (58%) had a post-stimulation plasma cortisol value < 18 µg/dL
• 6/19 (32%) failed to have an incremental change of at least 7 µg/dL
• 2/19 (11%) had a pre-stimulation cortisol< 5 µg/dL
• 19/60 or 32% of these patients showed evidence of HPA axis suppression
• 11/19 (58%) had a post-stimulation plasma cortisol value < 18 µg/dL
• 6/19 (32%) failed to have an incremental change of at least 7 µg/dL
• 2/19 (11%) had a pre-stimulation cortisol< 5 µg/dL

38Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Suppression by Age GroupSuppression by Age Group
• Recovery of normal HPA axis function
• 4 patients were retested 2 weeks post- treatment and 3 of the 4 recovered normal function of the HPA axis.
• Recovery of normal HPA axis function
• 4 patients were retested 2 weeks post- treatment and 3 of the 4 recovered normal function of the HPA axis.
Age Group 3mo-1 yrn=4
2yr-5yrn=16
6yr-8yrn=28
9yr-12yrn=12
# suppressed 2 6 9 2
% 50 38 32 17

39Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Statistical Analysis in the Development of HPA Axis Suppression
Statistical Analysis in the Development of HPA Axis Suppression
• No correlation between amount of drug used, body weight, age or sex and the incidence of adrenal gland suppression
• Statistical relationship did exist between BSA and risk of HPA axis suppression“for an increase of 1% BSA involved, risk of HPA axis suppression increased 4.4%”p ≤ 0.01
• No correlation between amount of drug used, body weight, age or sex and the incidence of adrenal gland suppression
• Statistical relationship did exist between BSA and risk of HPA axis suppression“for an increase of 1% BSA involved, risk of HPA axis suppression increased 4.4%”p ≤ 0.01

40Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Label Change for Diprolene AF Cream, 0.05%Label Change for Diprolene AF Cream, 0.05%
• Indication - added an age restriction to 13 years and older
• Clinical Safety Information - Updated in the Clinical Pharmacology, Precautions: General and Pediatric Use Sections
• Indication - added an age restriction to 13 years and older
• Clinical Safety Information - Updated in the Clinical Pharmacology, Precautions: General and Pediatric Use Sections

41Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Diprosone Ointment, 0.05%Diprosone Ointment, 0.05%
• 53 evaluable subjects with atopic dermatitis
• Age Range - 6 months to 12 years old
• Medication applied bid for 2 to 3 weeks
• Mean BSA Involvement - 58% (range:35% - 99%)
• 53 evaluable subjects with atopic dermatitis
• Age Range - 6 months to 12 years old
• Medication applied bid for 2 to 3 weeks
• Mean BSA Involvement - 58% (range:35% - 99%)

42Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Diprosone Ointment, 0.05% (cont’d)Diprosone Ointment, 0.05% (cont’d)
• 15/53 or 28% of patients showed evidence of HPA axis suppression
• 8/15 or 53% had a post-stimulation plasma cortisol value < 18 µg/dL
• 7/15 or 47% failed to have an incremental change of at least 7 µg/dL
• 15/53 or 28% of patients showed evidence of HPA axis suppression
• 8/15 or 53% had a post-stimulation plasma cortisol value < 18 µg/dL
• 7/15 or 47% failed to have an incremental change of at least 7 µg/dL

43Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Suppression by Age GroupSuppression by Age Group
Age Group 3mo-1 yrn=11
2yr-5yrn=21
6yr-8yrn=15
9yr-12yrn=6
# suppressed 4 6 4 1
% 36 29 27 17

44Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Statistical Analysis in the Development of HPA Axis Suppression
Statistical Analysis in the Development of HPA Axis Suppression
• No statistically significant effect for
– Drug usage– % BSA– Weight– Age
• Higher proportion of males than females (p=0.006) who developed HPA axis suppression
• No statistically significant effect for
– Drug usage– % BSA– Weight– Age
• Higher proportion of males than females (p=0.006) who developed HPA axis suppression

45Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Recovery of HPA Axis FunctionDiprosone Ointment
Recovery of HPA Axis FunctionDiprosone Ointment
• 2/15 patients were retested
• 100% recovery at 2 weeks
• 2/15 patients were retested
• 100% recovery at 2 weeks

46Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Label Change Diprosone Ointment, 0.05%Label Change Diprosone Ointment, 0.05%
• Indication - added an age restriction to 13 years and older
• Clinical Safety Information - Updated in the Clinical Pharmacology, Precautions, General and Pediatric Use Sections
• Indication - added an age restriction to 13 years and older
• Clinical Safety Information - Updated in the Clinical Pharmacology, Precautions, General and Pediatric Use Sections

47Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Diprosone Cream, 0.05%Diprosone Cream, 0.05%
• 43 evaluable patients with atopic dermatitis
• Age Range - 1 year to 12 years old
• Mean BSA Involvement - 40% (range:35% - 90%)
• Medication applied bid for 2-3 weeks
• 43 evaluable patients with atopic dermatitis
• Age Range - 1 year to 12 years old
• Mean BSA Involvement - 40% (range:35% - 90%)
• Medication applied bid for 2-3 weeks

48Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Diprosone Cream, 0.05% (cont’d)Diprosone Cream, 0.05% (cont’d)• 10/43 or 23% of patients showed evidence
of adrenal suppression
• 5/10 or 50% had a post-stimulation plasma cortisol value < 18 µg/dL
• 3/10 or 30% failed to have an incremental change of at least 7 µg/dL
• 2/10 or 20% had a pre-stimulation cortisol< 5 µg/dL
• 10/43 or 23% of patients showed evidence of adrenal suppression
• 5/10 or 50% had a post-stimulation plasma cortisol value < 18 µg/dL
• 3/10 or 30% failed to have an incremental change of at least 7 µg/dL
• 2/10 or 20% had a pre-stimulation cortisol< 5 µg/dL

49Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
HPA Axis Suppression by AgeHPA Axis Suppression by Age
Age Group
3mo-1yrn=3
2yr-5yrn=20
6yr-8yrn=13
9yr-12yrn=7
# suppressed
0 6 3 1
% 0 30 23 14

50Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Statistical Analysis in the Development of HPA Axis Suppression
Statistical Analysis in the Development of HPA Axis Suppression
• No statistically significant effect for
– Number of days treated– Weight– Age
• Statistical significance found for mean amount ofdrug used - 81 grams vs. 37 grams (p<0.001)
• There was a numerically higher %BSA involvement
• Numerically, more males developed suppression
• No statistically significant effect for
– Number of days treated– Weight– Age
• Statistical significance found for mean amount ofdrug used - 81 grams vs. 37 grams (p<0.001)
• There was a numerically higher %BSA involvement
• Numerically, more males developed suppression

51Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Recovery of HPA Axis FunctionDiprosone Cream
Recovery of HPA Axis FunctionDiprosone Cream
• 2/10 patients were retested
• 1/2 (50%) recovered HPA axis function at 2 weeks
• 2/10 patients were retested
• 1/2 (50%) recovered HPA axis function at 2 weeks

52Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Label Change Diprosone Cream, 0.05%Label Change Diprosone Cream, 0.05%
• Indication - added an age restriction to 13 years and older
• Clinical Safety Information - Updated in the Clinical Pharmacology, Precautions, General and Pediatric Use Sections
• Indication - added an age restriction to 13 years and older
• Clinical Safety Information - Updated in the Clinical Pharmacology, Precautions, General and Pediatric Use Sections

53Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Diprosone Lotion, 0.05%Diprosone Lotion, 0.05%
• 15 evaluable patients with atopic dermatitis
• Age Range - 6 to 12 years old
• Mean BSA Involvement - 45% (range:35% - 72%)
• Medication applied bid for 2-3 weeks
• 15 evaluable patients with atopic dermatitis
• Age Range - 6 to 12 years old
• Mean BSA Involvement - 45% (range:35% - 72%)
• Medication applied bid for 2-3 weeks

54Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Diprosone Lotion, 0.05% (cont’d)Diprosone Lotion, 0.05% (cont’d)
• 11/15 or 73% of patients showed evidence of HPA axis suppression
• 10/11 or 91% had a post-stimulation plasma cortisol value < 18 µg/dL
• 1/11 or 9% failed to have an incremental change of at least 7 µg/dL
• 11/15 or 73% of patients showed evidence of HPA axis suppression
• 10/11 or 91% had a post-stimulation plasma cortisol value < 18 µg/dL
• 1/11 or 9% failed to have an incremental change of at least 7 µg/dL

55Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Suppression by Age GroupSuppression by Age Group
Age Group 3mo-1 yrn=0
2yr-5yrn=0
6yr-8yrn=10
9yr-12yrn=5
# suppressed None enrolled
None enrolled
7 4
% - - 70 80

56Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Statistical Analysis in the Development of HPA Axis Suppression
Statistical Analysis in the Development of HPA Axis Suppression
• Numerical analysis
– Subjects exhibiting HPA axis suppression• Larger mean amount of drug used (92.8 g vs. 69.4 g)• Slightly higher %BSA involved (45.8% vs. 41.8%)• Lower mean weights at visit 1 (65 lbs. vs. 81 lbs.)• Lower mean weights at visit 4 (65 lbs. vs. 80 lbs.)• Differences with respect to age and days of treatment
were miniscule
• Numerical analysis
– Subjects exhibiting HPA axis suppression• Larger mean amount of drug used (92.8 g vs. 69.4 g)• Slightly higher %BSA involved (45.8% vs. 41.8%)• Lower mean weights at visit 1 (65 lbs. vs. 81 lbs.)• Lower mean weights at visit 4 (65 lbs. vs. 80 lbs.)• Differences with respect to age and days of treatment
were miniscule

57Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Recovery of HPA Axis FunctionDiprosone Lotion
Recovery of HPA Axis FunctionDiprosone Lotion
• 6/11 patients were retested• 4/6 (67%) recovered HPA axis function
at 2 weeks
• 6/11 patients were retested• 4/6 (67%) recovered HPA axis function
at 2 weeks

58Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Label Change Diprosone Lotion, 0.05%Label Change Diprosone Lotion, 0.05%
• Indication – added an age restriction to 13 years and older
• Clinical Safety Information – Updated in the Clinical Pharmacology, Precautions: General and Pediatric Use Sections
• Indication – added an age restriction to 13 years and older
• Clinical Safety Information – Updated in the Clinical Pharmacology, Precautions: General and Pediatric Use Sections

59Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Comparison of HPA Axis CriteriaBetamethasone Dipropionate
Comparison of HPA Axis CriteriaBetamethasone Dipropionate
HPA Axis Suppression Criteria - serum cortisol levels Drug Product 5 µg/dL ; >18 µg/dL; ≥7 µg/dL > 18 µg/dL
Diprolene AF Cream 19/60 (32%) 11/60 (18%)
Diprosone Ointment 15/53 (28%) 8/53 (15%)
Diprosone Cream 10/43 (23%) 5/43 (12%)
Diprosone Lotion 11/15 (73%) 10/15 (67%)

60Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Lotrisone CreamLotrisone Cream• Tinea Pedis Study• Tinea Cruris Study
• Both studies were in the adolescent population ages 12 – 16 years
• Medication was applied twice daily• Study duration
– 4 weeks for tinea pedis– 2 weeks for tinea cruris
• Tinea Pedis Study• Tinea Cruris Study
• Both studies were in the adolescent population ages 12 – 16 years
• Medication was applied twice daily• Study duration
– 4 weeks for tinea pedis– 2 weeks for tinea cruris

61Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Lotrisone Cream (cont’d)Lotrisone Cream (cont’d)
• 17/43 (39.5%) demonstrated adrenal suppression in the tinea pedis study
• 8/17 (47.1%) demonstrated adrenal suppression in the tinea cruris study
• 17/43 (39.5%) demonstrated adrenal suppression in the tinea pedis study
• 8/17 (47.1%) demonstrated adrenal suppression in the tinea cruris study

62Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Label ChangeLotrisone Cream and Lotion
Label ChangeLotrisone Cream and Lotion
• An Expanded Indications Section– Added an age restriction – patients 17 years and older– Recommended that effective treatment may be obtained
without the use of a corticosteroid for noninflammatory tinea infections
• Updated Safety Information – Precautions: General, Pediatric Use, Geriatric Use and Dosage and Administration Sections
• An Expanded Indications Section– Added an age restriction – patients 17 years and older– Recommended that effective treatment may be obtained
without the use of a corticosteroid for noninflammatory tinea infections
• Updated Safety Information – Precautions: General, Pediatric Use, Geriatric Use and Dosage and Administration Sections

63Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Clobex (clobetasol propionate), Lotion 0.05% a Class I steroid
Approved July 24, 2003
Atopic Dermatitis and Psoriasis Trials
Clobex (clobetasol propionate), Lotion 0.05% a Class I steroid
Approved July 24, 2003
Atopic Dermatitis and Psoriasis Trials

64Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Clobex LotionClobex Lotion
• 3 studies– 2 adult studies – one in psoriasis and one in atopic
dermatitis– 1 pediatric study (ages 12 – 17 years) in atopic
dermatitis
• Comparator drug – Temovate E Cream– Class I steroid– Same chemical moiety, clobetasol propionate– Different vehicle, an emollient cream
• 3 studies– 2 adult studies – one in psoriasis and one in atopic
dermatitis– 1 pediatric study (ages 12 – 17 years) in atopic
dermatitis
• Comparator drug – Temovate E Cream– Class I steroid– Same chemical moiety, clobetasol propionate– Different vehicle, an emollient cream

65Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Construct of HPA Axis EvaluationConstruct of HPA Axis Evaluation
• The control plasma cortisol level should exceed 5 micrograms/100 mL
• The 30 minute level should show an increment of at least 7 micrograms/100 mL above basal level
• The 30 minute level should exceed 18 micrograms/100 mL
• Exceptions: – plasma cortisol levels were drawn at 60 minutes post-stimulation. – In adult studies, subjects were stimulated with cosyntropin weekly.
• The control plasma cortisol level should exceed 5 micrograms/100 mL
• The 30 minute level should show an increment of at least 7 micrograms/100 mL above basal level
• The 30 minute level should exceed 18 micrograms/100 mL
• Exceptions: – plasma cortisol levels were drawn at 60 minutes post-stimulation. – In adult studies, subjects were stimulated with cosyntropin weekly.

66Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Adolescent studyAdolescent study
• 24 evaluable patients – 14 treated with Clobex Lotion and 10 treated with Temovate E Cream
• Moderate to severe atopic dermatitis• BSA treated – at least 20%• Medication applied BID for 2 weeks• 50 grams/week limit
• 24 evaluable patients – 14 treated with Clobex Lotion and 10 treated with Temovate E Cream
• Moderate to severe atopic dermatitis• BSA treated – at least 20%• Medication applied BID for 2 weeks• 50 grams/week limit

67Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
HPA axis suppressionHPA axis suppression
• 9/14 (64%) of subjects treated with Clobex Lotion suppressed
• 2/10 (20%) of subjects treated with Temovate E Cream suppressed
• 9/14 (64%) of subjects treated with Clobex Lotion suppressed
• 2/10 (20%) of subjects treated with Temovate E Cream suppressed

68Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Statistical AnalysisStatistical Analysis
• Mean %BSA treated was higher for patients with adrenal suppression
• 32.8% vs. 27.7% for Clobex Lotion• 35% vs. 25.3% for Temovate E Cream
• Mean %BSA treated was higher for patients with adrenal suppression
• 32.8% vs. 27.7% for Clobex Lotion• 35% vs. 25.3% for Temovate E Cream

69Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Recovery of HPA Axis FunctionRecovery of HPA Axis Function
• 1/4 of patients treated with Clobex Lotion remained suppressed after 2 weeks
• 1/1 patient retested after treatment with Temovate E Cream recovered
• 1/4 of patients treated with Clobex Lotion remained suppressed after 2 weeks
• 1/1 patient retested after treatment with Temovate E Cream recovered

70Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Adult StudyAdult Study
• 18 evaluable patients – 9 treated with Clobex Lotion and 9 treated with Temovate E Cream
• Moderate to Severe Atopic Dermatitis• Mean BSA treated – 19.3 % for Clobex Lotion
and 19.4% for Temovate E Cream• Medication applied BID for 2 weeks• 50 gram/week limit
• 18 evaluable patients – 9 treated with Clobex Lotion and 9 treated with Temovate E Cream
• Moderate to Severe Atopic Dermatitis• Mean BSA treated – 19.3 % for Clobex Lotion
and 19.4% for Temovate E Cream• Medication applied BID for 2 weeks• 50 gram/week limit

71Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
HPA Axis SuppressionHPA Axis Suppression
• 5 / 9 (56%) of subjects treated with Clobex Lotion suppressed
• 4 / 9 (44%) of subjects treated with Temovate E Cream suppressed
• 5 / 9 (56%) of subjects treated with Clobex Lotion suppressed
• 4 / 9 (44%) of subjects treated with Temovate E Cream suppressed

72Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Recovery of HPA Axis FunctionRecovery of HPA Axis Function
• 1 / 3 patients on Clobex Lotion failed to recover function 7 days post treatment
• 2 /2 patients on Temovate E Cream recovered function 7 days post treatment
• 1 / 3 patients on Clobex Lotion failed to recover function 7 days post treatment
• 2 /2 patients on Temovate E Cream recovered function 7 days post treatment

73Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Adult StudyAdult Study
• 20 evaluable patients – 10 treated with Clobex lotion and 10 treated with Temovate E Cream
• Moderate to Severe Plaque Psoriasis• Mean BSA treated – 16.2 % for Clobex Lotion
and 17.9 % for Temovate E Cream• Medication applied BID for 4 weeks• 50 gram/week limit
• 20 evaluable patients – 10 treated with Clobex lotion and 10 treated with Temovate E Cream
• Moderate to Severe Plaque Psoriasis• Mean BSA treated – 16.2 % for Clobex Lotion
and 17.9 % for Temovate E Cream• Medication applied BID for 4 weeks• 50 gram/week limit

74Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
HPA Axis FunctionHPA Axis Function
• 8 / 10 (80%) of subjects treated with Clobex Lotion suppressed
• 3 / 10 (30%) of subjects with Temovate E Cream suppressed
• 1 / 2 subjects with Clobex Lotion retested remained suppressed after 8 days
• 0 / 3 subjects on Temovate E Cream were retested
• 8 / 10 (80%) of subjects treated with Clobex Lotion suppressed
• 3 / 10 (30%) of subjects with Temovate E Cream suppressed
• 1 / 2 subjects with Clobex Lotion retested remained suppressed after 8 days
• 0 / 3 subjects on Temovate E Cream were retested

75Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Label for Clobex LotionLabel for Clobex Lotion
• Indication – restricted to patients 18 years or older
• 2 consecutive weeks not to exceed 50 grams (50 mL or 1.75 fl. Oz) per week
• Moderate or severe psoriasis, for localized lesions < 10% BSA can be treated an additional 2 weeks
• Updated Safety Information – Indications and Usage, Precautions: General and Pediatric Use, and Dosage and Administration Sections
• Indication – restricted to patients 18 years or older
• 2 consecutive weeks not to exceed 50 grams (50 mL or 1.75 fl. Oz) per week
• Moderate or severe psoriasis, for localized lesions < 10% BSA can be treated an additional 2 weeks
• Updated Safety Information – Indications and Usage, Precautions: General and Pediatric Use, and Dosage and Administration Sections

76Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Postmarketing SummaryHPA Axis Suppression
SourcesAERS Database
Medical Literature Case Reports
Postmarketing SummaryHPA Axis Suppression
SourcesAERS Database
Medical Literature Case Reports

77Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Adverse Event Reporting System(AERS)
Adverse Event Reporting System(AERS)
• Spontaneous, voluntary surveillance system– Voluntary reporting by health care professionals and consumers– Mandatory reporting by manufacturers
• Approximately 3 million reports in database• Database origin 1969 • Contains human drug and “therapeutic” biologic reports;
exception = vaccines (VAERS)• Quality of a report is variable and often incomplete• Subject to under-reporting (true numerator not known) • Duplicate reporting occurs
• Spontaneous, voluntary surveillance system– Voluntary reporting by health care professionals and consumers– Mandatory reporting by manufacturers
• Approximately 3 million reports in database• Database origin 1969 • Contains human drug and “therapeutic” biologic reports;
exception = vaccines (VAERS)• Quality of a report is variable and often incomplete• Subject to under-reporting (true numerator not known) • Duplicate reporting occurs

78Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Postmarketing SummaryHPA Axis Suppression
Postmarketing SummaryHPA Axis Suppression
• 94 cases spanning 3 decades– 65 adult cases– 29 pediatric cases
• Manifestations– Adrenal insufficiency– Cushing’s Syndrome– Growth Retardation
• 94 cases spanning 3 decades– 65 adult cases– 29 pediatric cases
• Manifestations– Adrenal insufficiency– Cushing’s Syndrome– Growth Retardation

79Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Postmarketing ReportsPediatric Cases
Postmarketing ReportsPediatric Cases
• 29 pediatric patients– 11 with adrenal insufficiency– 17 with Cushing’s Syndrome– 13 with Growth Retardation
• Characteristics– Age range 6 weeks – 15 years; mean age 5.0 years– duration of use 22 days – 7.5 years; mean use 20.8 months– 16 (55%) received medication for 3 months or longer– Varied indications but 34% used topical steroids for diaper rash– Betamethasone containing, clobetasol, and mometasone products
implicated most often, with 34% using high potency topical steroids
– Resulted in 14 hospitalizations and 2 deaths, the latter from Cushing’s Syndrome
• 29 pediatric patients– 11 with adrenal insufficiency– 17 with Cushing’s Syndrome– 13 with Growth Retardation
• Characteristics– Age range 6 weeks – 15 years; mean age 5.0 years– duration of use 22 days – 7.5 years; mean use 20.8 months– 16 (55%) received medication for 3 months or longer– Varied indications but 34% used topical steroids for diaper rash– Betamethasone containing, clobetasol, and mometasone products
implicated most often, with 34% using high potency topical steroids
– Resulted in 14 hospitalizations and 2 deaths, the latter from Cushing’s Syndrome

80Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Postmarketing ReportsAdult Cases
Postmarketing ReportsAdult Cases
• 65 adult cases– 46 with adrenal insufficiency/suppression– 32 with Cushing’s Syndrome
• Characteristics– Age range 19 years – 74 years; mean age 47.4 years– duration of use 7 days – 12.0 years; mean use 35.6 months– 30 (46%) received medication for 3 months or longer– Varied indications but 51% used topical steroids for psoriasis– Betamethasone containing and clobetasol products implicated
most often, with 61% using high potency topical corticosteroids– Resulted in 34 hospitalizations and 2 deaths– Deaths attributed in part to the adrenal event
• 65 adult cases– 46 with adrenal insufficiency/suppression– 32 with Cushing’s Syndrome
• Characteristics– Age range 19 years – 74 years; mean age 47.4 years– duration of use 7 days – 12.0 years; mean use 35.6 months– 30 (46%) received medication for 3 months or longer– Varied indications but 51% used topical steroids for psoriasis– Betamethasone containing and clobetasol products implicated
most often, with 61% using high potency topical corticosteroids– Resulted in 34 hospitalizations and 2 deaths– Deaths attributed in part to the adrenal event

81Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Postmarketing ReportsCommon Factors in Adverse Events
Postmarketing ReportsCommon Factors in Adverse Events
• Most AEs occurred in the setting of one or more of the following:– Prolonged use of topical corticosteroid – Use of a super potent topical corticosteroid– Use of multiple topical corticosteroid products or
concomitant use with other corticosteroid formulations– Use of an excessive amount or possible inappropriate
use of the topical corticosteroid product
• Most AEs occurred in the setting of one or more of the following:– Prolonged use of topical corticosteroid – Use of a super potent topical corticosteroid– Use of multiple topical corticosteroid products or
concomitant use with other corticosteroid formulations– Use of an excessive amount or possible inappropriate
use of the topical corticosteroid product

82Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Summary – HPA Axis SuppressionSummary – HPA Axis Suppression
• HPA axis suppression does occur with the use of topical corticosteroids
• The adrenal suppression is not limited to the super potent class of topical corticosteroids
• High BSA involvement and amount of drug used appear to be risk factors for HPA axis suppression
• HPA axis suppression does occur with the use of topical corticosteroids
• The adrenal suppression is not limited to the super potent class of topical corticosteroids
• High BSA involvement and amount of drug used appear to be risk factors for HPA axis suppression

83Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Summary – HPA Axis SuppressionSummary – HPA Axis Suppression
• The type of vehicle may contribute to the extent of absorption of the active chemical moiety
• The suppression appears, in most cases, to be reversible upon cessation of drug usage
• Long-term use of topical corticosteroids, particularly high potency ones, can lead to serious morbidity and even death
• The type of vehicle may contribute to the extent of absorption of the active chemical moiety
• The suppression appears, in most cases, to be reversible upon cessation of drug usage
• Long-term use of topical corticosteroids, particularly high potency ones, can lead to serious morbidity and even death

84Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Cutaneous SafetyCutaneous Safety
• Known cutaneous adverse events
• Question of cutaneous malignancy
• Known cutaneous adverse events
• Question of cutaneous malignancy

85Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Cutaneous SafetyCutaneous Safety
• Adverse Events associated with topical corticosteroid use– Atrophy of the skin– Telangiectasia– Striae– Erythema of the face– Steroid Rosacea– Hypopigmentation– Infection– Retarded Wound Healing
• Adverse Events associated with topical corticosteroid use– Atrophy of the skin– Telangiectasia– Striae– Erythema of the face– Steroid Rosacea– Hypopigmentation– Infection– Retarded Wound Healing

86Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Pictorial Presentationfrom
University of Erlangen Websiteand Bolognia Textbook of Dermatology
Pictorial Presentationfrom
University of Erlangen Websiteand Bolognia Textbook of Dermatology

87Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
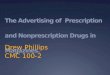
AtrophyAtrophy

88Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
TelangiectasiaTelangiectasia

89Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
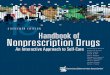
StriaeStriae

90Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
StriaeStriae

91Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Facial Erythema Facial Erythema

92Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Facial ErythemaFacial Erythema

93Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Steroid RosaceaSteroid Rosacea

94Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
HypopigmentationHypopigmentation

95Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Other Adverse EffectsOther Adverse Effects
• Topical corticosteroids placed on certain infections, e.g. tinea infections, may exacerbate them
• Topical corticosteroids placed on open or surgical wounds will retard healing
• Use of topical corticosteroids in the periorbital area may cause an increase in intraocular pressure
• Topical corticosteroids placed on certain infections, e.g. tinea infections, may exacerbate them
• Topical corticosteroids placed on open or surgical wounds will retard healing
• Use of topical corticosteroids in the periorbital area may cause an increase in intraocular pressure

96Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Cutaneous Malignancy Postmarketing ReportsCutaneous Malignancy Postmarketing Reports
• 2 reports in AERS database as of February 5, 2005; US Cases
– A 7 month old male with a history of mastocytoma was diagnosed with skin cancer several months after discontinuation of clobetasol
– A female of unknown age used betametasone cream for psoriasis and reported “what started as psoriasis became cancer”
• AERS data do not suggest a compelling safety signal for malignancy formation with the use of topical corticosteroids
• 2 reports in AERS database as of February 5, 2005; US Cases
– A 7 month old male with a history of mastocytoma was diagnosed with skin cancer several months after discontinuation of clobetasol
– A female of unknown age used betametasone cream for psoriasis and reported “what started as psoriasis became cancer”
• AERS data do not suggest a compelling safety signal for malignancy formation with the use of topical corticosteroids

97Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Cutaneous Adverse EventsCutaneous Adverse Events
• Corticosteroid induced AEs– Can be an early or late event– Depends on potency of drug and duration of use– Depends on site of application– Occlusion at the site may increase risk
• Corticosteroid induced AE – May resolve slowly– May not resolve
• Corticosteroid induced AEs– Can be an early or late event– Depends on potency of drug and duration of use– Depends on site of application– Occlusion at the site may increase risk
• Corticosteroid induced AE – May resolve slowly– May not resolve

98Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Conclusion HPA Axis Suppression
Conclusion HPA Axis Suppression
• Can occur with short term use of topical corticosteroids
• Can occur with even mid-potency topical steroids
• Can occur as early as two continuous weeks of therapy
• Can occur with short term use of topical corticosteroids
• Can occur with even mid-potency topical steroids
• Can occur as early as two continuous weeks of therapy

99Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
ConclusionHPA Axis Suppression
ConclusionHPA Axis Suppression
• Is usually reversible• The interrelationship between BSA, amount of
drug used, and potency of medication is complex
• Long term use and/or misuse of topical corticosteroids, particularly those of high potency, can lead to serious medical complications and death
• Is usually reversible• The interrelationship between BSA, amount of
drug used, and potency of medication is complex
• Long term use and/or misuse of topical corticosteroids, particularly those of high potency, can lead to serious medical complications and death

100Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
ConclusionCutaneous Adverse Events
ConclusionCutaneous Adverse Events
• Can be related to both duration of use and potency of topical corticosteroid
• Can occur with short-term or long-term use• Resolution is possible with some but not all of
these cutaneous events• There is no firm evidence to date to link
cutaneous malignancy with use of topical corticosteroids
• Can be related to both duration of use and potency of topical corticosteroid
• Can occur with short-term or long-term use• Resolution is possible with some but not all of
these cutaneous events• There is no firm evidence to date to link
cutaneous malignancy with use of topical corticosteroids

101Nonprescription Drugs Advisory Committee and the Dermatologic and Ophthalmic Drugs Advisory Committee March 24, 2005March 24, 2005
Rx Topical CorticosteroidsHPA Axis Suppression HPA Axis Suppression
and and Cutaneous EffectsCutaneous Effects