Embed Size (px)
Citation preview

Noninvasive Respiratory Support of Preterm Infants with RDS
Morgan Stanley Children’s Hospital
Columbia University
Richard A. Polin M.D.

Milestones in Neonatal Intensive Care
Epidemiology of bronchopulmonary dysplasia (BPD) and strategies
for prevention.
Rationale for use of CPAP as an initial mode of respiratory support
Randomized Clinical Trials of NIPPV or HFNC versus CPAP
Conclusions and Recommendations
Outline

✶ A 0.75 kg infant is born following a 27 week gestation. The infant exhibits
immediate signs of respiratory distress and is administered 30% O2 in the
delivery room. He is given ampicillin and gentamicin and transported to the
NICU. A chest x-ray demonstrates a ground glass appearance with air
bronchograms. What should be done now?
Case
A. Intubate, administer surfactant and rapidly extubate to NPCPAP (INSURE).
B. Withhold surfactant. Place the infant IMV-NPCPAP or HHHFN.
C. Withhold surfactant. Place on the infant on NPCPAP and observe.
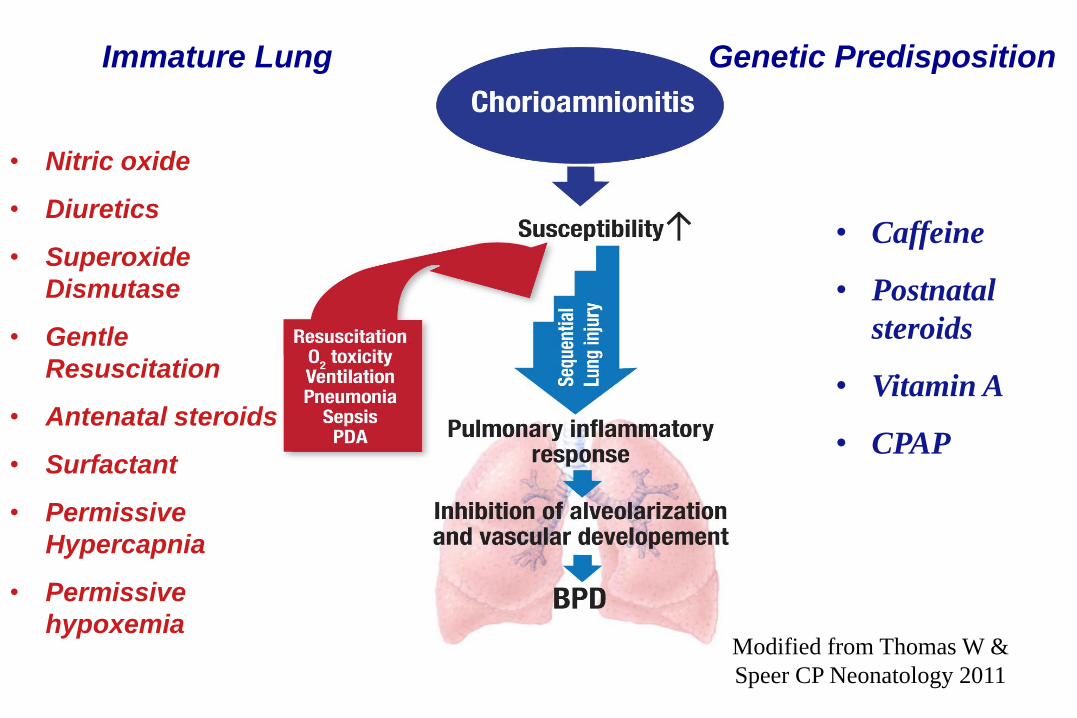
Modified from Thomas W &
Speer CP Neonatology 2011
Immature Lung Genetic Predisposition
• Nitric oxide
• Diuretics
• Superoxide
Dismutase
• Gentle
Resuscitation
• Antenatal steroids
• Surfactant
• Permissive
Hypercapnia
• Permissive
hypoxemia
• Caffeine
• Postnatal
steroids
• Vitamin A
• CPAP
Lung Injury in the Neonate: Fundamental Concept
S If you don’t ventilate an infant, it’s hard to cause BPD!
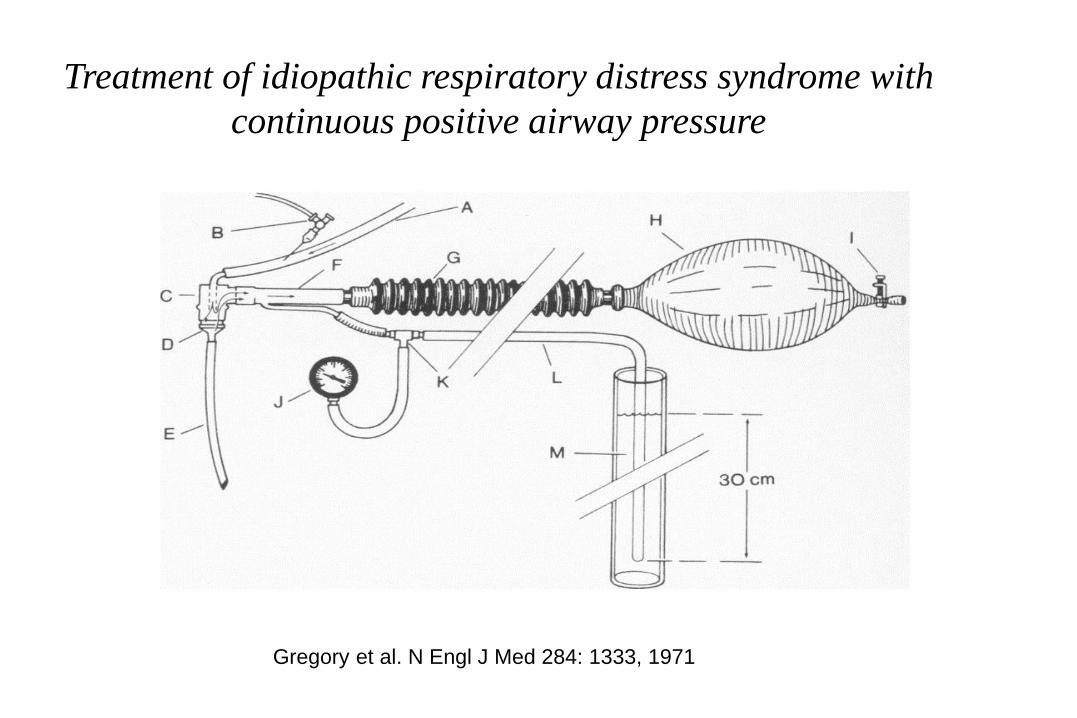
Gregory et al. N Engl J Med 284: 1333, 1971
Treatment of idiopathic respiratory distress syndrome with
continuous positive airway pressure
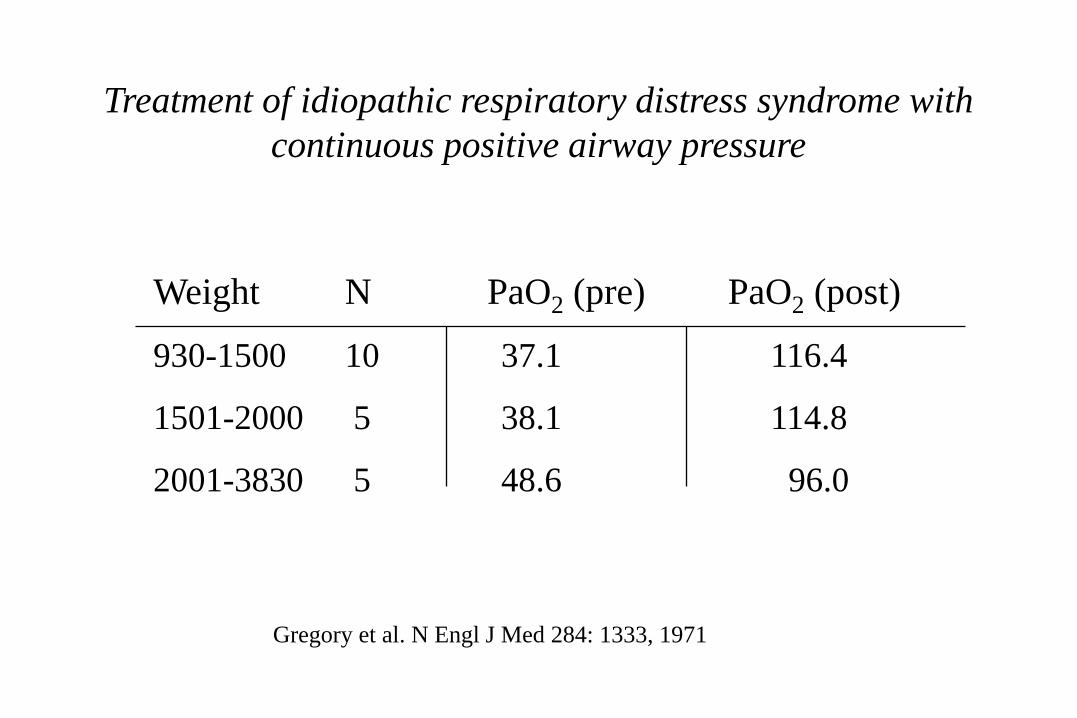
Weight N PaO2 (pre) PaO2 (post)
930-1500 10 37.1 116.4
1501-2000 5 38.1 114.8
2001-3830 5 48.6 96.0
Treatment of idiopathic respiratory distress syndrome with
continuous positive airway pressure
Gregory et al. N Engl J Med 284: 1333, 1971

CPAP is Controversial
Practical skepticism “ the position that new information may be
worthy of confidence, but that acceptance depends on the
strength of the supportive data.
Skepticism and CPAP
*Kamper et al Acta Paediatr. 1992
The fundamental concept of the Kamper* study that the “softly-
softly” approach will decrease morbidity is fundamentally flawed.
Putting seriously ill babies on CPAP alone gives the clinician much
less control of cardio-respiratory function at a time when the baby is
at major risk of sudden deterioration”
NRC Robertson Cambridge UK 1993
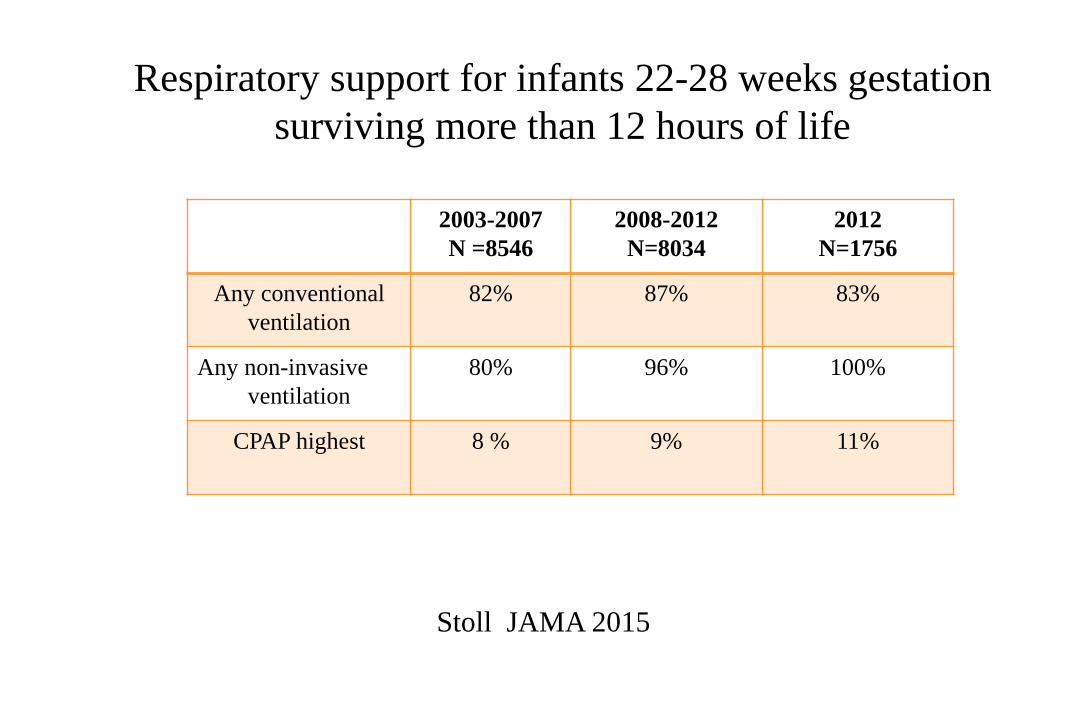
2003-2007
N =8546
2008-2012
N=8034
2012
N=1756
Any conventional
ventilation
82% 87% 83%
Any non-invasive
ventilation
80% 96% 100%
CPAP highest 8 % 9% 11%
Respiratory support for infants 22-28 weeks gestation
surviving more than 12 hours of life
Stoll JAMA 2015
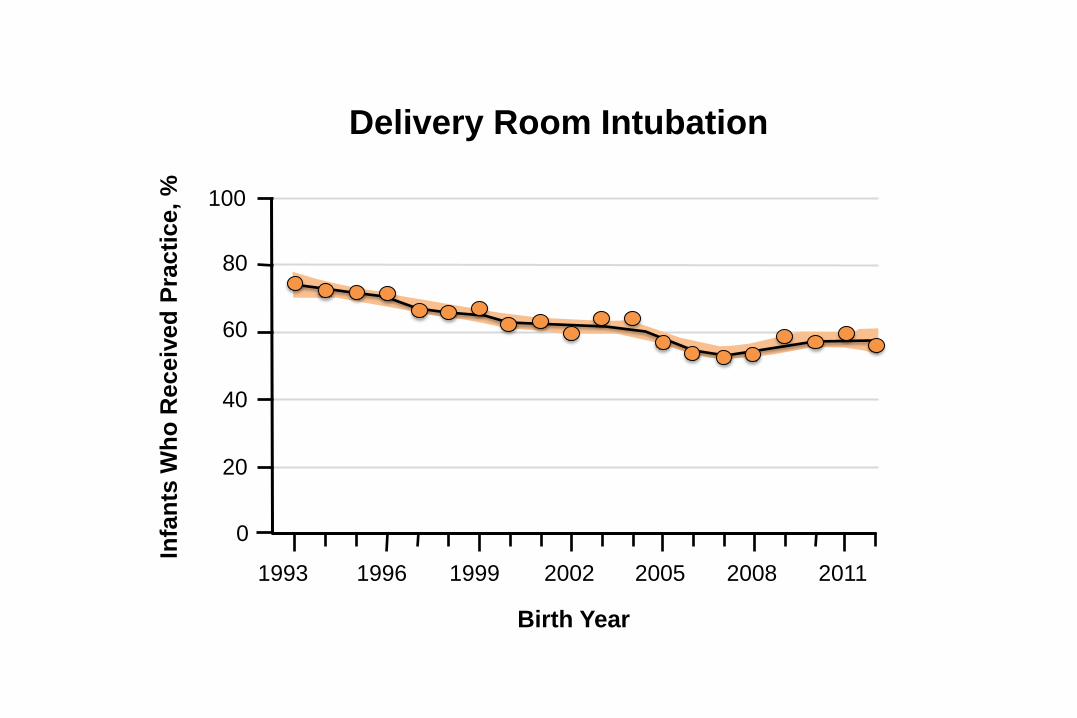
Delivery Room Intubation
Birth Year
Infa
nts
Wh
o R
eceiv
ed
Pra
cti
ce,
%
1993 1996 1999 2002 2005 2008 2011
100
80
60
40
20
0
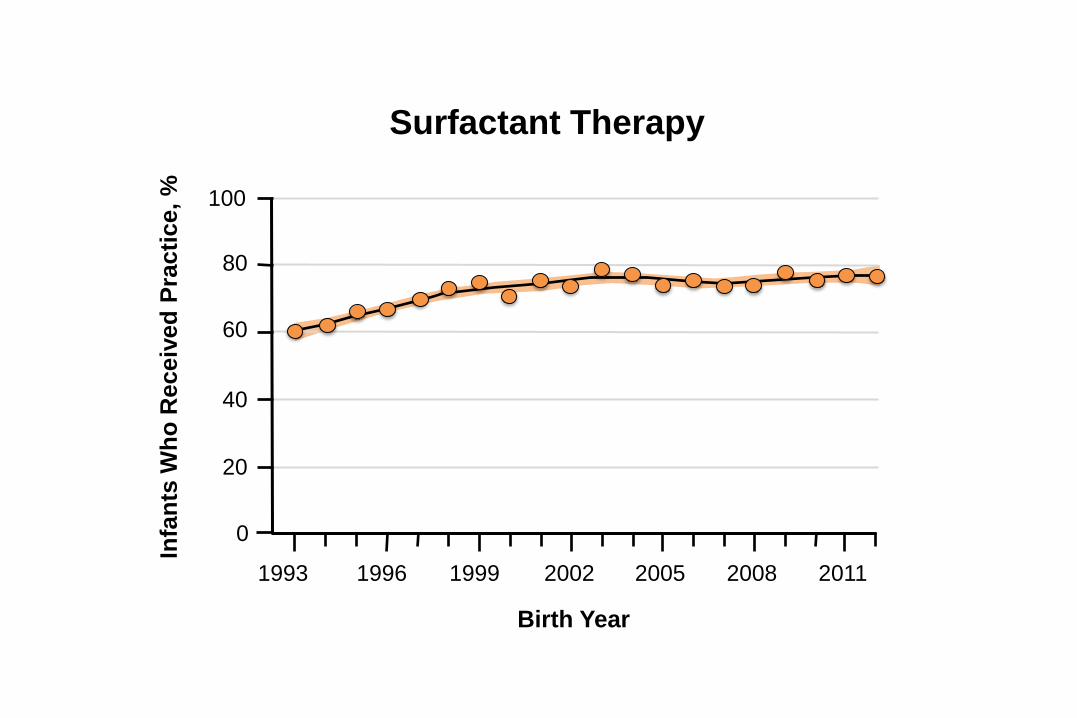
Surfactant Therapy
Birth Year
Infa
nts
Wh
o R
eceiv
ed
Pra
cti
ce,
%
1993 1996 1999 2002 2005 2008 2011
100
80
60
40
20
0
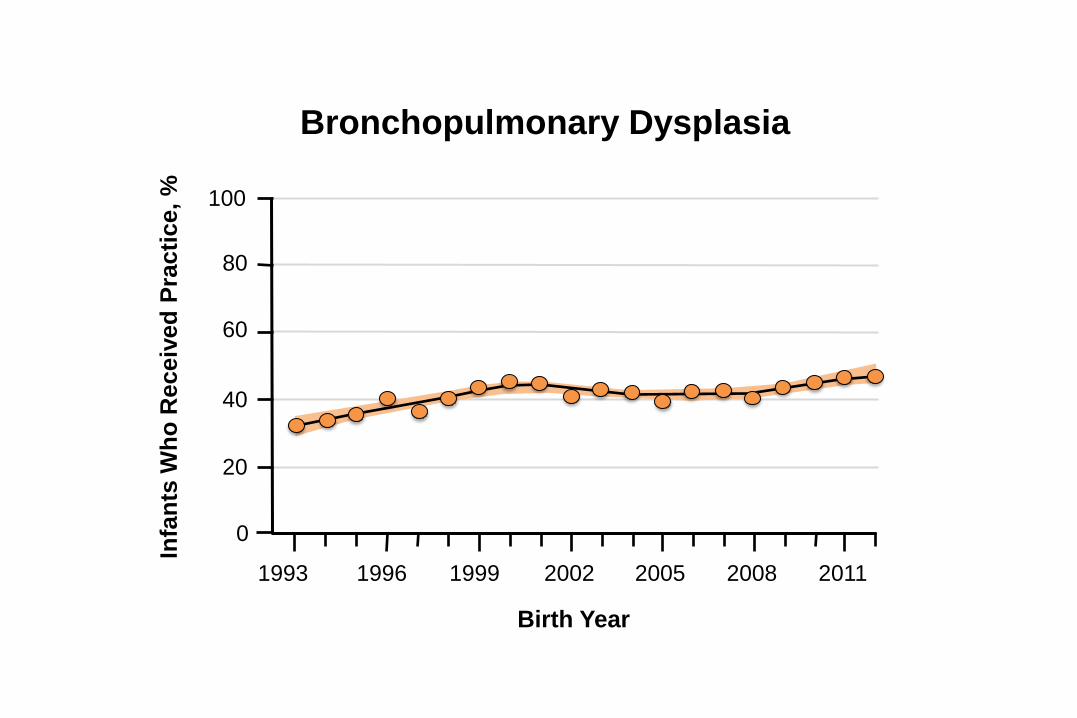
Bronchopulmonary Dysplasia
Birth Year
Infa
nts
Wh
o R
eceiv
ed
Pra
cti
ce,
%
1993 1996 1999 2002 2005 2008 2011
100
80
60
40
20
0
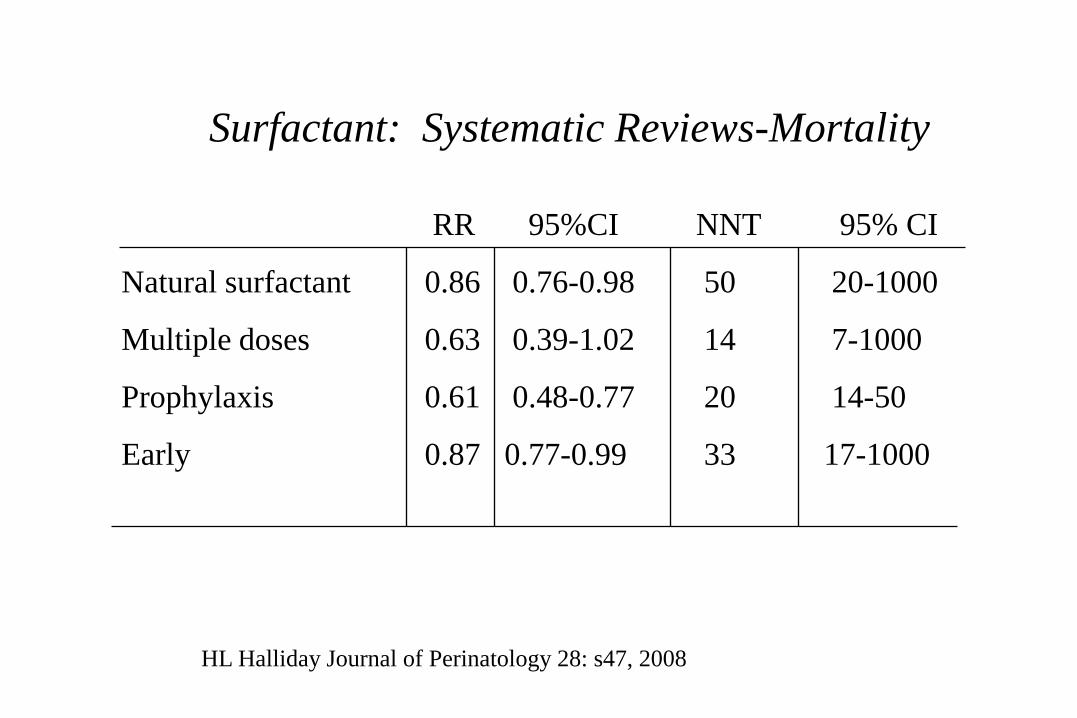
Surfactant: Systematic Reviews-Mortality
RR 95%CI NNT 95% CI
Natural surfactant 0.86 0.76-0.98 50 20-1000
Multiple doses 0.63 0.39-1.02 14 7-1000
Prophylaxis 0.61 0.48-0.77 20 14-50
Early 0.87 0.77-0.99 33 17-1000
HL Halliday Journal of Perinatology 28: s47, 2008
Critique of the Surfactant Trials
✶ Low rates of exposure to antenatal steroids
✶ Infants randomized to control arms of these trials were
routinely ventilated (without surfactant) rather than receiving
CPAP
“Simplicity is the Ultimate
sophistication”
KISS: Keep it simple stupid!
✶ Is the use of CPAP as an initial treatment for preterm infants
with RDS evidence-based?
Yes

Summary of CPAP Trials
Gestational age N Death or BPD Air-leaks
CPAP/control CPAP/control
✶ Support 240/7-276/7 1316 47.8%/51.1% 6.8%/7.4%
✶ COIN 250/7-286/7 610 33.9%/38.9% 9.1%/3.0%
✶ VON 266/7-296/7 648 29.6%/36.5% 4.8%/5.4%
✶ Neocosur 800-1500g 256 13.7%/19.2% 3.1%/5.6%
✶ CURPAP 250/7-286/7 208 21.0%/21.9% 4.9%/9.5%
Total 3038 29.2%/33.52% 5.7%/6.18%
If CPAP is going to be compared to any
other respiratory support modality
(intubation/surfactant or HFNC) it has be
used optimally
Why Has CPAP Been Only Marginally Better?
✶ Inexperience with CPAP in the centers participating in RCTs
(and greater skill with other forms of respiratory support)
✶ Thresholds for abandoning CPAP were too low.
✶ Limited duration of ventilation in the RCTs
✶ Some CPAP delivery stems, may be more effective than others.
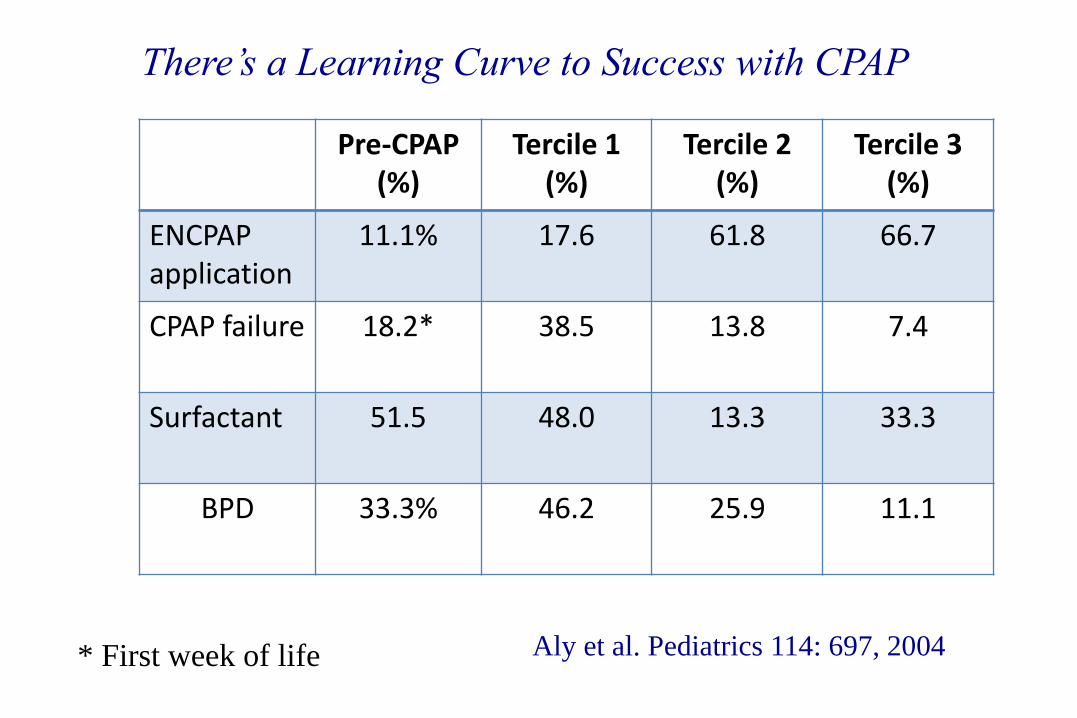
Pre-CPAP (%)
Tercile 1 (%)
Tercile 2 (%)
Tercile 3 (%)
ENCPAP application
11.1% 17.6 61.8 66.7
CPAP failure 18.2* 38.5 13.8 7.4
Surfactant 51.5 48.0 13.3 33.3
BPD 33.3% 46.2 25.9 11.1
Aly et al. Pediatrics 114: 697, 2004 * First week of life
There’s a Learning Curve to Success with CPAP
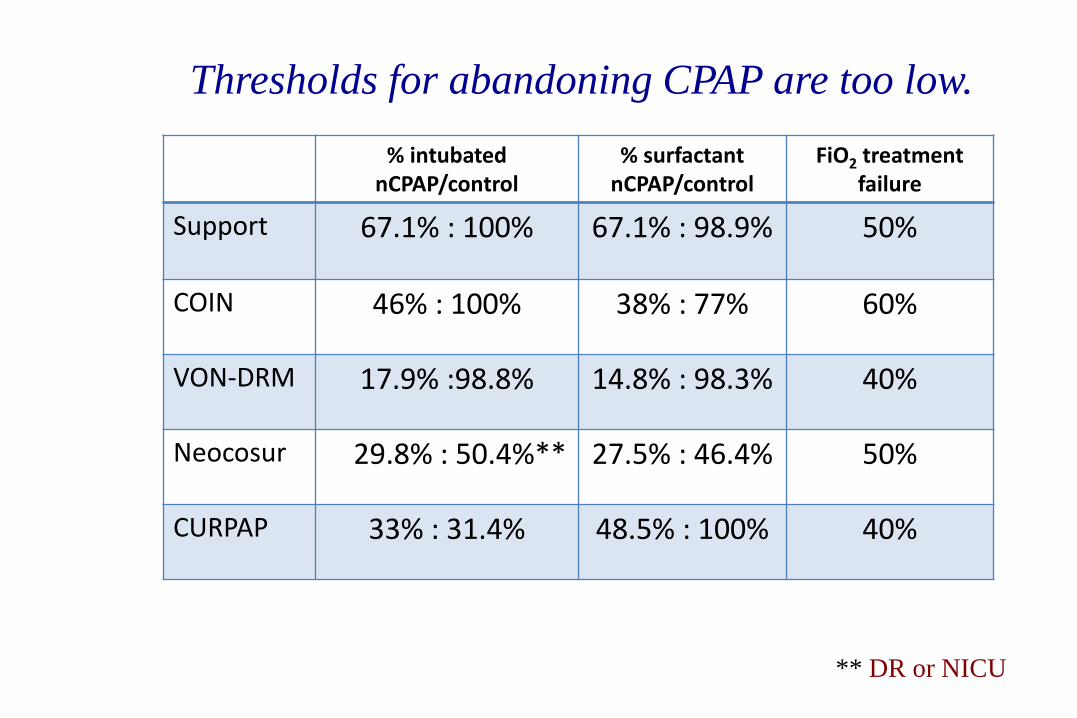
% intubated nCPAP/control
% surfactant nCPAP/control
FiO2 treatment failure
Support 67.1% : 100% 67.1% : 98.9%
50%
COIN 46% : 100% 38% : 77% 60%
VON-DRM 17.9% :98.8% 14.8% : 98.3% 40%
Neocosur 29.8% : 50.4%** 27.5% : 46.4% 50%
CURPAP 33% : 31.4% 48.5% : 100% 40%
Thresholds for abandoning CPAP are too low.
** DR or NICU

Duration ventilation
nCPAP/control
✶ Support 10 days / 13 days@
✶ COIN 3 days /4 days
✶ VON* 9.2 days / 12.5 days
✶ Neocosur 3.3 days / 4.3 days
✶ CURPAP 5.5 days / 5.4 days@
* CPAP vs. INSURE
Short Duration of Ventilation Limits the Utility of
BPD as an Endpoint.

All CPAP Devices are not Created Equal
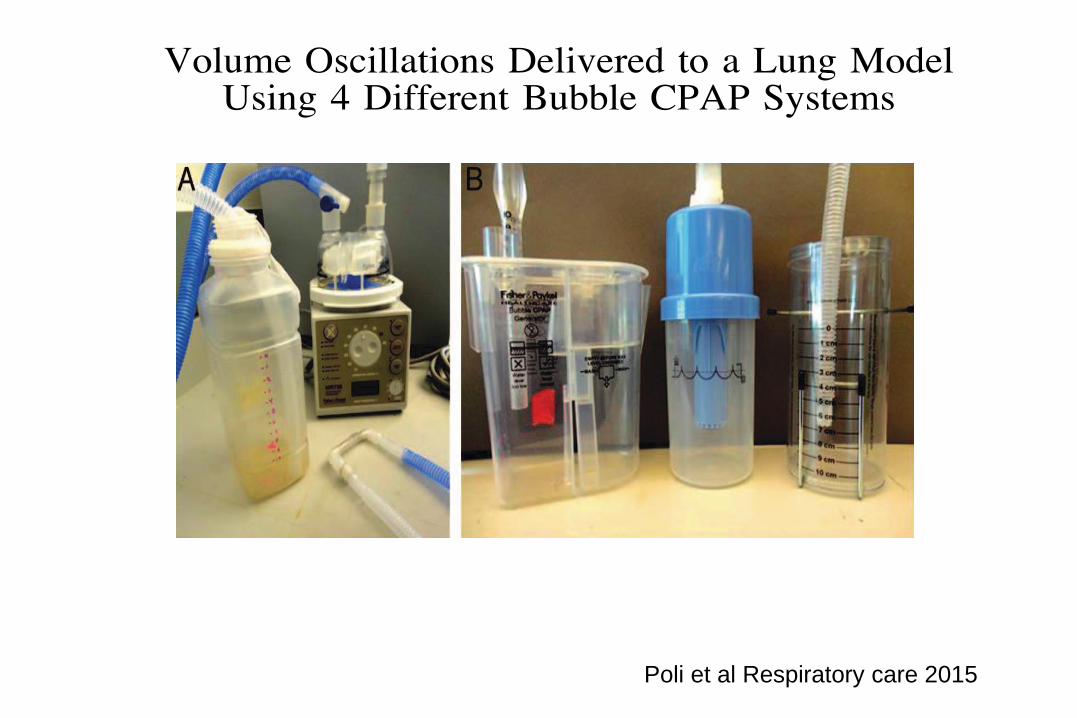
Poli et al Respiratory care 2015
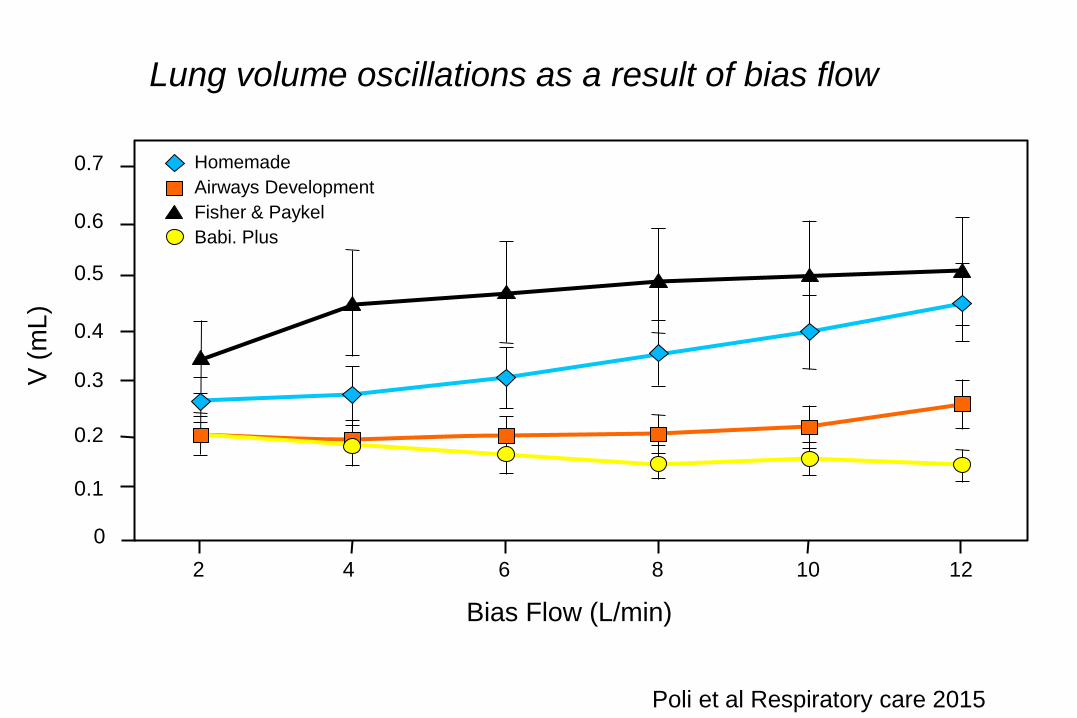
Bias Flow (L/min)
2 4 6 8 10 12
Homemade
Airways Development
Fisher & Paykel
Babi. Plus
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
V
(m
L)
Poli et al Respiratory care 2015
Lung volume oscillations as a result of bias flow
Time (s)
10
Paw (
cm
H2O
)
Homemade
Airways Development
Fisher & Paykel
Babi.Plus
5
0
10
Paw (
cm
H2O
) 5
0
10
Paw (
cm
H2O
)
5
0
10
Paw (
cm
H2O
)
5
0 2 1.5 1 0.5 0
Time (s) 2 1.5 1 0.5 0
Time (s) 2 1.5 1 0.5 0
Time (s) 2 1.5 1 0.5 0
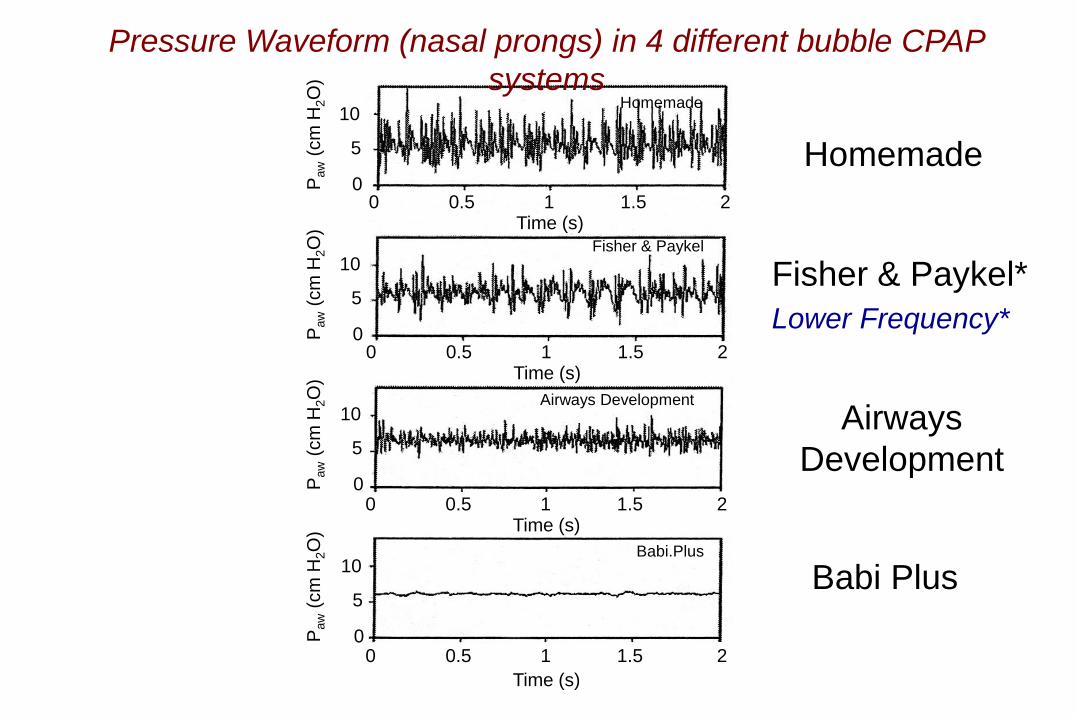
Pressure Waveform (nasal prongs) in 4 different bubble CPAP
systems
Homemade
Fisher & Paykel*
Airways
Development
Babi Plus
Lower Frequency*
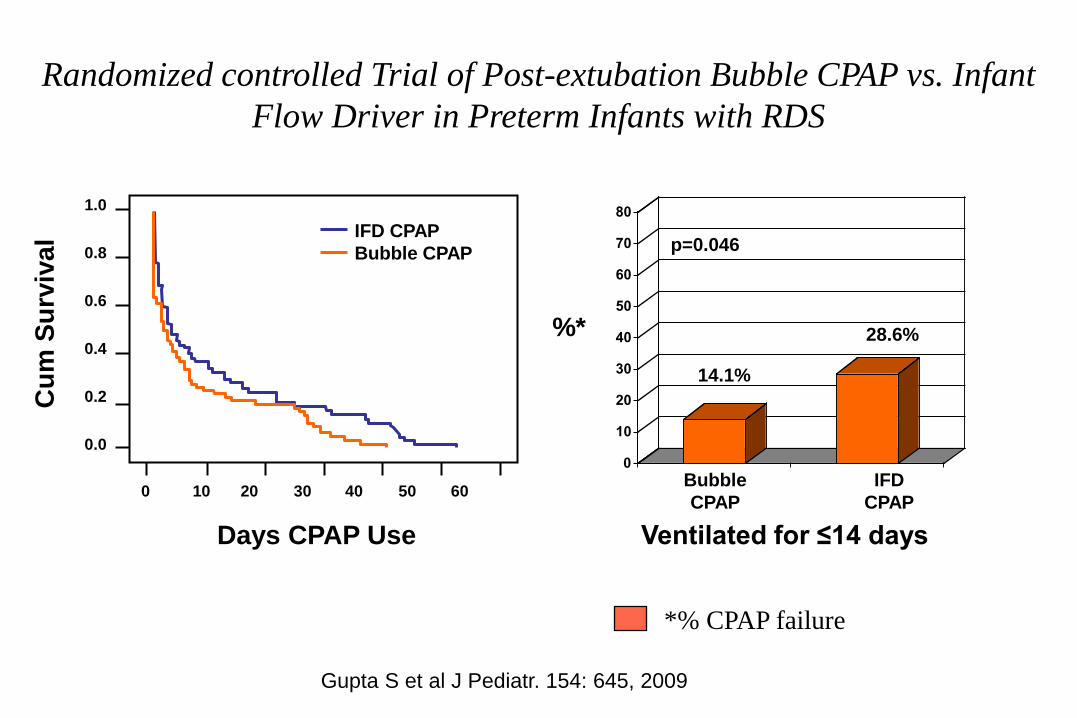
Gupta et al 2009 (n=140, mean GA ~ 27 weeks) BCPAP vs. Infant
Flow Driver IFD). No significant differences in the rate of post
extubation failure; however, in infants intubated < 14 days, infants on
BCPAP had a significantly lower extubation failure rate.
Randomized controlled Trial of Post-extubation Bubble CPAP vs.
Infant Flow Driver in Preterm Infants with RDS
0
10
20
30
40
50
60
70
80
14.1%
Ventilated for ≤14 days
28.6%
Bubble
CPAP
IFD
CPAP
p=0.046
%*
IFD CPAP
Bubble CPAP
1.0
0.8
0.6
0.4
0.2
0.0
Cu
m S
urv
iva
l
Days CPAP Use
0 10 20 30 40 50 60
*% CPAP failure
Randomized controlled Trial of Post-extubation Bubble CPAP vs. Infant
Flow Driver in Preterm Infants with RDS
Gupta S et al J Pediatr. 154: 645, 2009
Columbia Experience
• 4 year retrospective analysis (2008-11)
• 297 consecutive inborn infants BW ≤ 1000 gm
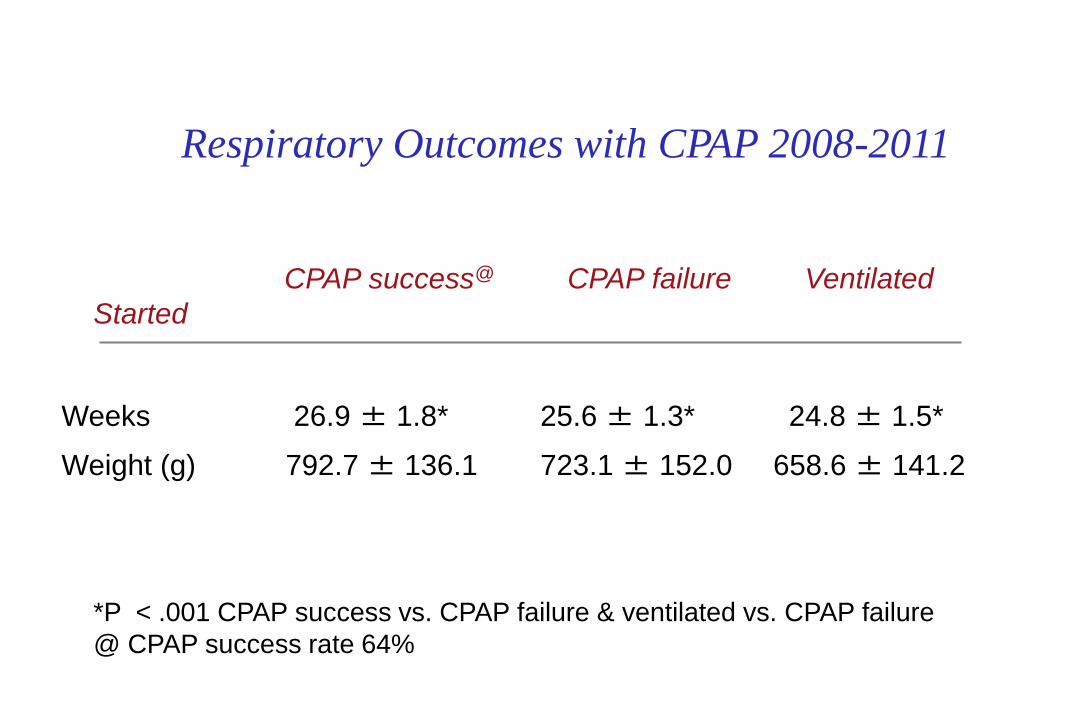
Respiratory Outcomes with CPAP 2008-2011
CPAP success@ CPAP failure Ventilated
Started
(n = 151) (n = 84) (n =62)
Weeks 26.9 ± 1.8* 25.6 ± 1.3* 24.8 ± 1.5*
Weight (g) 792.7 ± 136.1 723.1 ± 152.0 658.6 ± 141.2
*P < .001 CPAP success vs. CPAP failure & ventilated vs. CPAP failure
@ CPAP success rate 64%
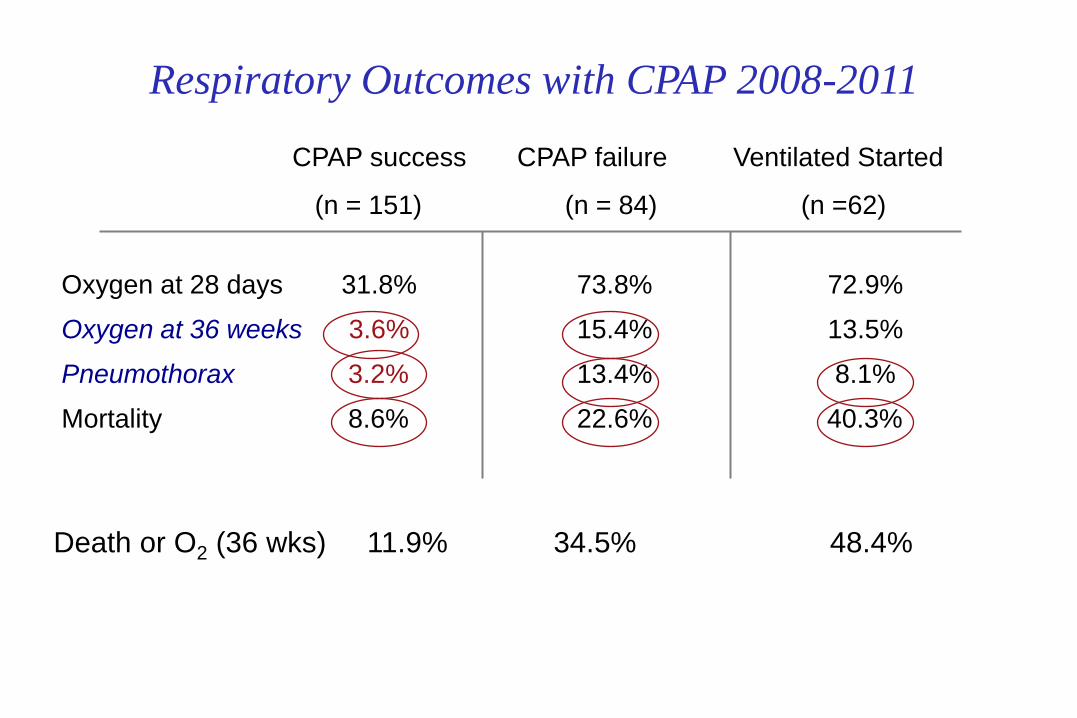
Respiratory Outcomes with CPAP 2008-2011
CPAP success CPAP failure Ventilated Started
(n = 151) (n = 84) (n =62)
Oxygen at 28 days 31.8% 73.8% 72.9%
Oxygen at 36 weeks 3.6% 15.4% 13.5%
Pneumothorax 3.2% 13.4% 8.1%
Mortality 8.6% 22.6% 40.3%
Death or O2 (36 wks) 11.9% 34.5% 48.4%
Why Do infants Fail CPAP?
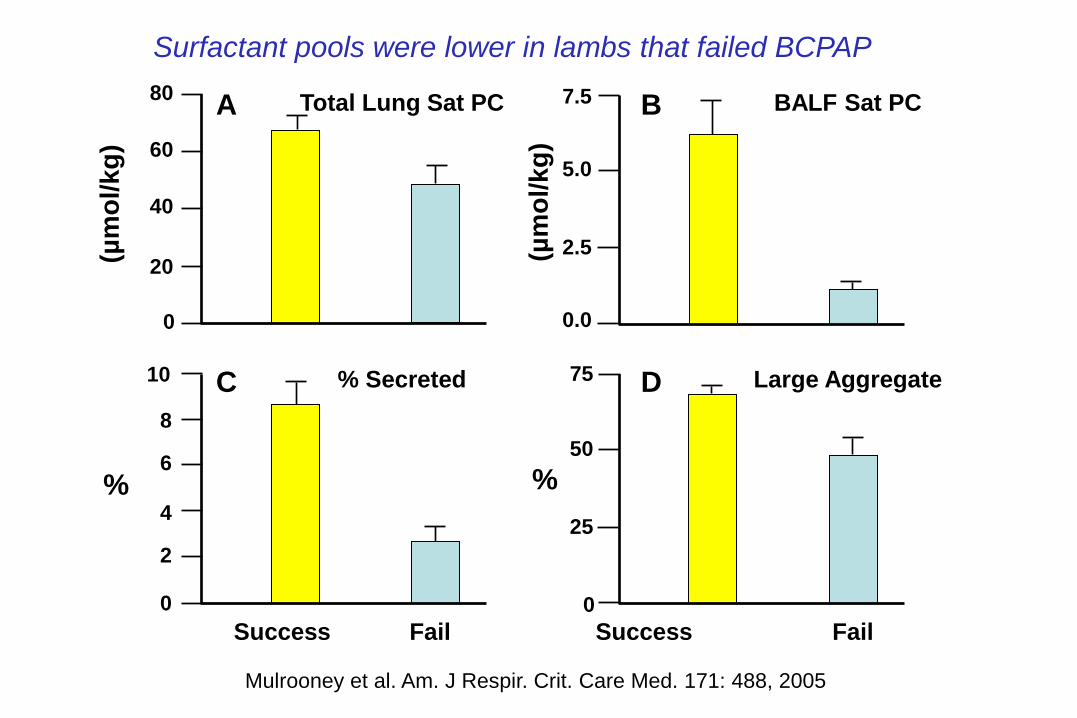
7.5 Total Lung Sat PC 80
Success Fail Success Fail
BALF Sat PC
Large Aggregate % Secreted
60
40
20
0
10
8
6
4
2
0
5.0
2.5
0.0
75
50
25
0
% %
(µm
ol/k
g)
(µm
ol/k
g)
A
C D
B
Surfactant pools were lower in lambs that failed BCPAP
Mulrooney et al. Am. J Respir. Crit. Care Med. 171: 488, 2005
Intubation >> Surfactant >> Extubation
INSURE
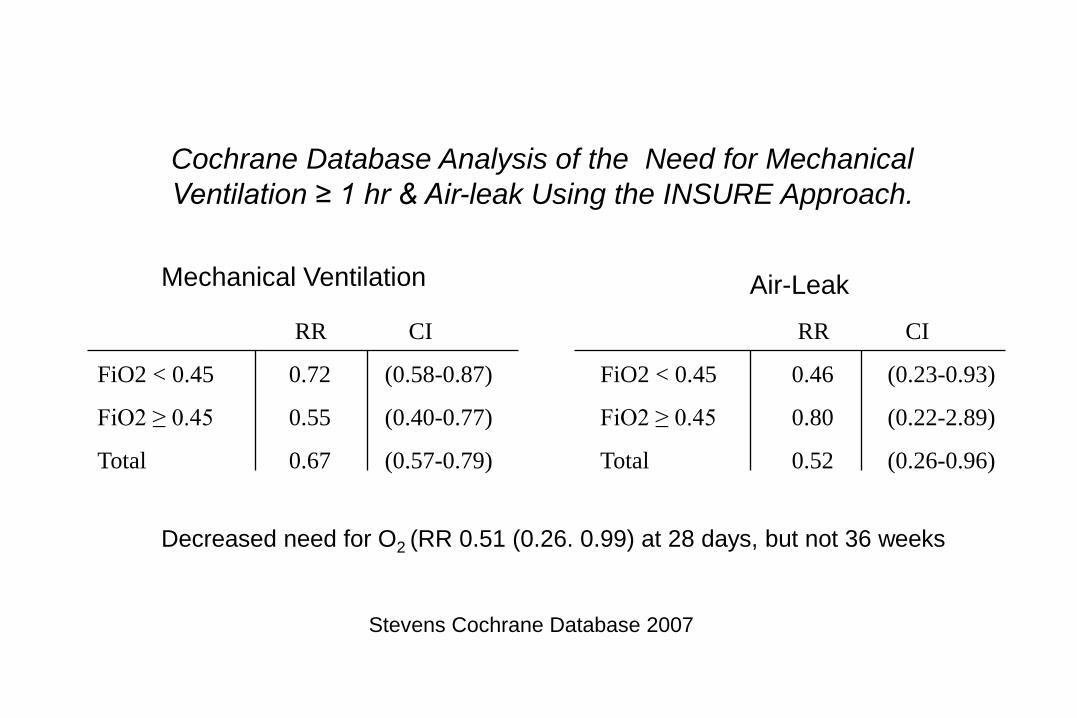
Cochrane Database Analysis of the Need for Mechanical
Ventilation ≥ 1 hr & Air-leak Using the INSURE Approach.
RR CI
FiO2 < 0.45 0.72 (0.58-0.87)
FiO2 ≥ 0.45 0.55 (0.40-0.77)
Total 0.67 (0.57-0.79)
Stevens Cochrane Database 2007
Mechanical Ventilation Air-Leak
RR CI
FiO2 < 0.45 0.46 (0.23-0.93)
FiO2 ≥ 0.45 0.80 (0.22-2.89)
Total 0.52 (0.26-0.96)
Decreased need for O2 (RR 0.51 (0.26. 0.99) at 28 days, but not 36 weeks
Noninvasive ventilation (CPAP) with or without early surfactant:
A systematic review and Meta-analysis
Isiyama et al JAMA Pediatrics 2015
✶ Nine studies were included in the meta-analysis (including 4 since
the last Cochrane review)
✶ There were no significant differences in any outcomes (CLD, death
and/or BPD, CLD, Mortality, IVH or air-leak.
✶ There was a 12% reduction in CLD or death** RR (CI 0.88-1.02), a
14% decrease in CLD** (CI 0.71-1.03) and a 50% reduction in
pneumothoraces* (CI 0.24-1.07)
✶ “CPAP and INSURE are at least equivalent”
* Low quality evidence
** Moderate quality evidence
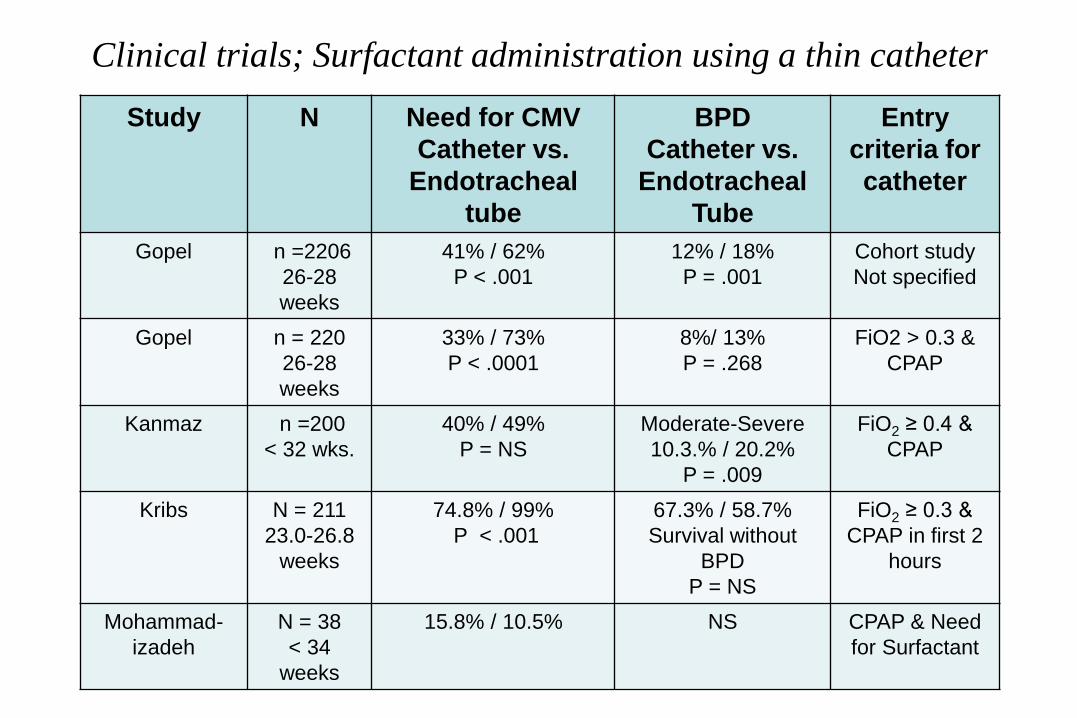
Clinical trials; Surfactant administration using a thin catheter
Study N Need for CMV
Catheter vs.
Endotracheal
tube
BPD
Catheter vs.
Endotracheal
Tube
Entry
criteria for
catheter
Gopel n =2206
26-28
weeks
41% / 62%
P < .001
12% / 18%
P = .001
Cohort study
Not specified
Gopel n = 220
26-28
weeks
33% / 73%
P < .0001
8%/ 13%
P = .268
FiO2 > 0.3 &
CPAP
Kanmaz n =200
< 32 wks.
40% / 49%
P = NS
Moderate-Severe
10.3.% / 20.2%
P = .009
FiO2 ≥ 0.4 &
CPAP
Kribs N = 211
23.0-26.8
weeks
74.8% / 99%
P < .001
67.3% / 58.7%
Survival without
BPD
P = NS
FiO2 ≥ 0.3 &
CPAP in first 2
hours
Mohammad-
izadeh
N = 38
< 34
weeks
15.8% / 10.5%
NS CPAP & Need
for Surfactant

VON Delivery Room Management (DRM) Groups
✶ Intubation, prophylactic surfactant administration with subsequent
stabilization on ventilator support (PS Group)
✶ Intubation, prophylactic surfactant administration and rapid
extubation to NCPAP (ISX Group)
✶ Early stabilization on NCPAP and selective intubation and surfactant
administration for clinical indications (NCPAP Group)
Gestational age 26+0 to 29+6 weeks
Study assignment was made prior to delivery

Von Delivery Room Management Trial
Death or CLD At 36 Weeks Post Menstrual Age
36.5% 28.5% 30.5%
36.5%
50
40
30
20
10
0
% C
ase
s
Death or CLD
RR 0.78
(95% CI 0.59, 1.03)
RR 0.83
(95% CI 0.64, 1.09)
PS ISX NCPAP
28.5% 30.5%
Rojas and Soll 2010 unpublished

VON-DRM
✶ In the nasal CPAP group 48% were managed without intubation and 54%
without surfactant.
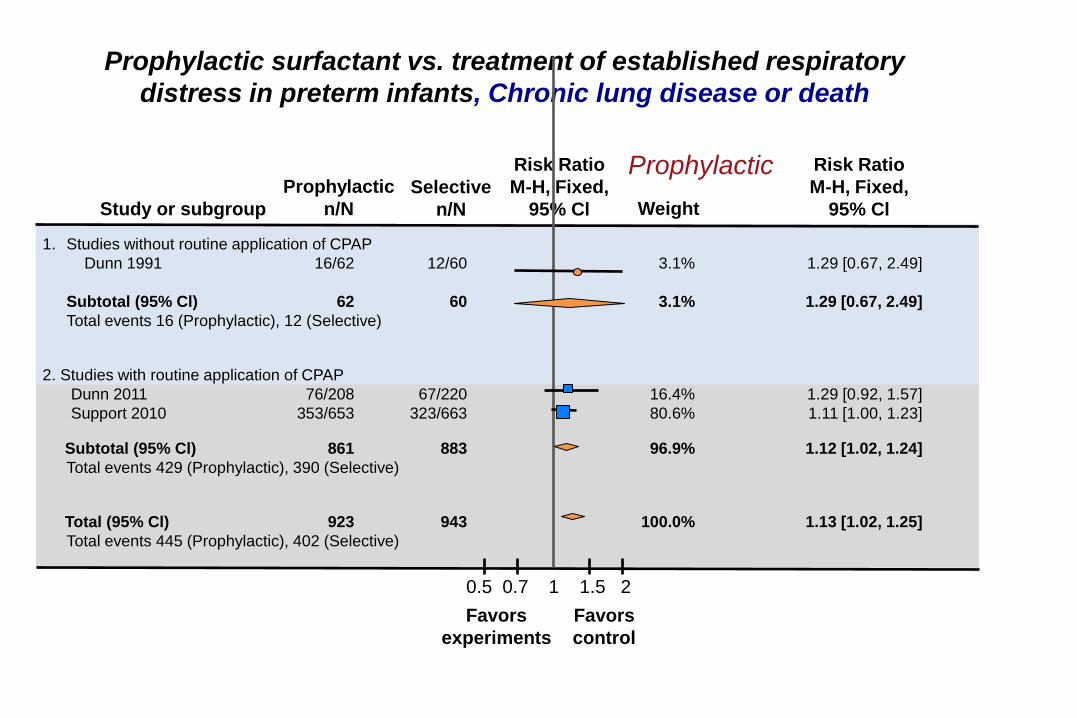
1. Studies without routine application of CPAP
Dunn 1991 16/62 12/60 3.1% 1.29 [0.67, 2.49]
Subtotal (95% Cl) 62 60 3.1% 1.29 [0.67, 2.49]
Total events 16 (Prophylactic), 12 (Selective)
2. Studies with routine application of CPAP
Dunn 2011 76/208 67/220 16.4% 1.29 [0.92, 1.57]
Support 2010 353/653 323/663 80.6% 1.11 [1.00, 1.23]
Subtotal (95% Cl) 861 883 96.9% 1.12 [1.02, 1.24]
Total events 429 (Prophylactic), 390 (Selective)
Total (95% Cl) 923 943 100.0% 1.13 [1.02, 1.25]
Total events 445 (Prophylactic), 402 (Selective)
0.5 0.7 1 1.5 2
Favors
experiments
Favors
control
Study or subgroup
Prophylactic
n/N Selective
n/N
Risk Ratio
M-H, Fixed,
95% Cl Weight
Risk Ratio
M-H, Fixed,
95% Cl
Prophylactic surfactant vs. treatment of established respiratory
distress in preterm infants, Chronic lung disease or death
Prophylactic
Nasal Intermittent Positive Pressure Ventilation
Nasal Intermittent Positive Pressure Ventilation
NIPPV commonly uses a ventilator to provide intermittent breaths
Theoretically, NIPPV provides better ventilation by delivering
breaths to the lower airway.
Randomized clinical trials in babies are very heterogeneous:
Wide range of set peak pressures (10-25 cm H2O pressure)
Different ventilator rates (10-60/minute)
Variable Inflation times (0.3-0.5 seconds)
Non-synchronized or Synchronized (Not available in the United
States)
30
25
20
15
10
5
0
14 18 22 26 30 34
Set PIP on Ventilator (cm H2O)
RAM - Vent
SBP - Vent
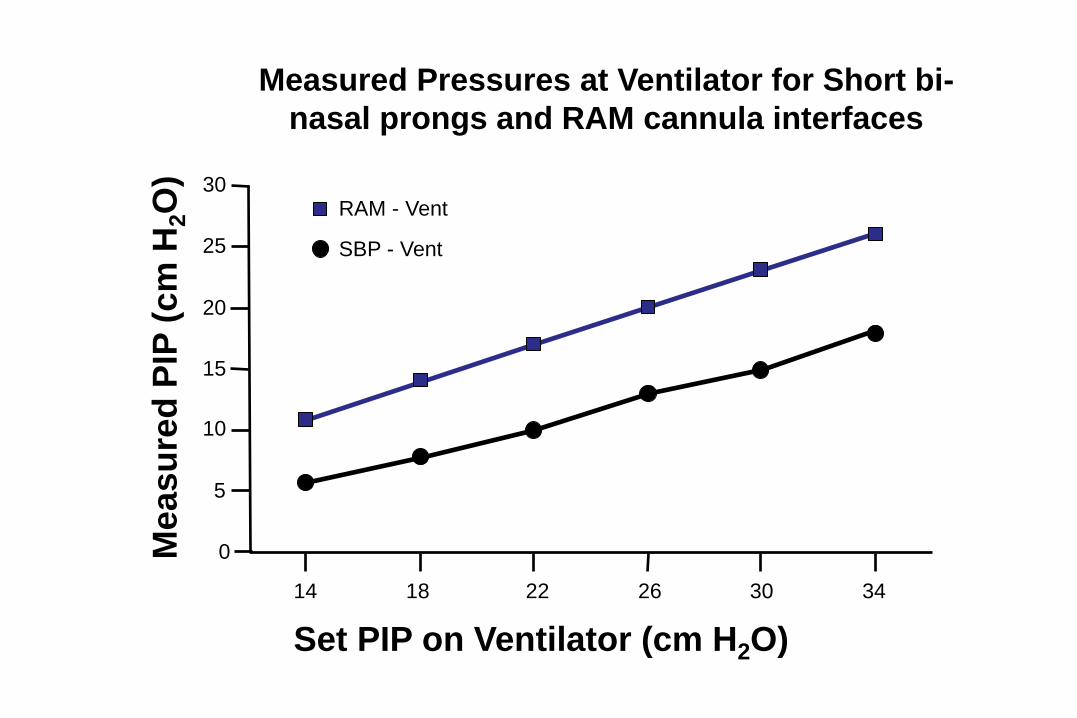
Measured Pressures at Ventilator for Short bi-
nasal prongs and RAM cannula interfaces
Me
as
ure
d P
IP (
cm
H2O
)
5.0 M
ea
su
red
PIP
(c
m H
2O
)
SBP RAM
Set PIP on Ventilator (cm H2O)
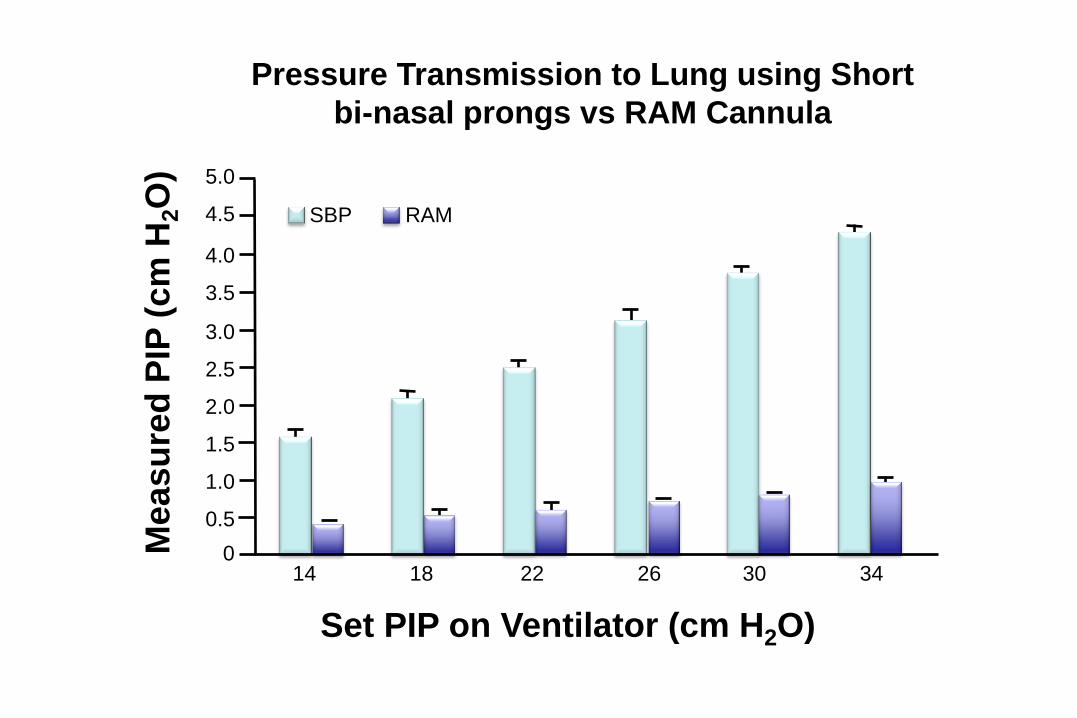
Pressure Transmission to Lung using Short
bi-nasal prongs vs RAM Cannula
14 18 22 26 30 34
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0
RAM
SBP
100 C
O2 r
em
ain
ing
in
th
e lu
ng
% Physiologic VT delivered to lungs
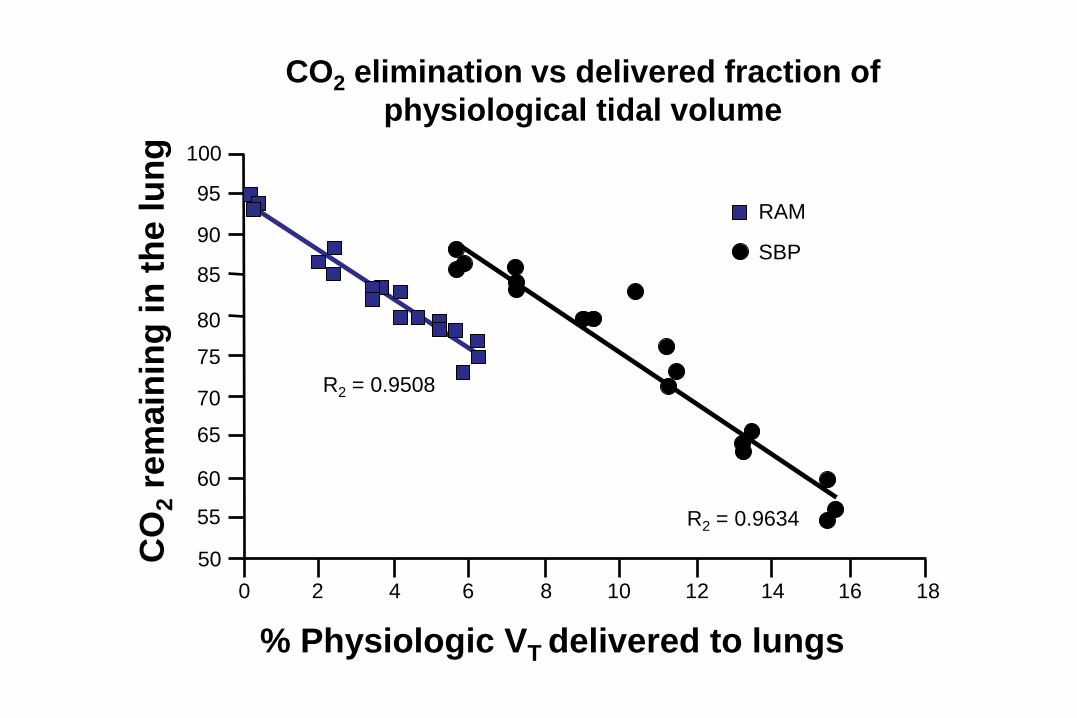
CO2 elimination vs delivered fraction of
physiological tidal volume
14 16 18 8 10 12 6 4 2 0
R2 = 0.9508
R2 = 0.9634
95
90
85
80
75
70
65
60
55
50
RAM
SBP
OFF CPAP
5
CPAP
10
NIPPV
14
NIPPV
18
NIPPV
22
NIPPV
26
NIPPV
30
NIPPV
34
100 C
O2O
re
ma
inin
g in
lun
gs
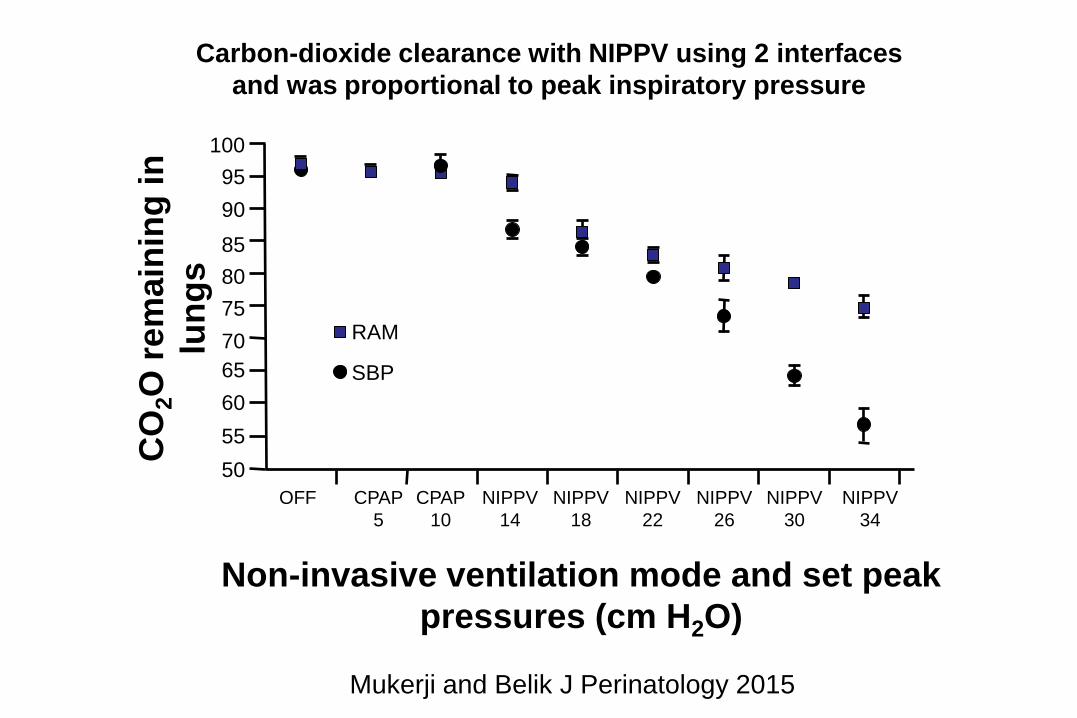
Carbon-dioxide clearance with NIPPV using 2 interfaces
and was proportional to peak inspiratory pressure
95
90
85
80
75
70
65
60
55
50
Non-invasive ventilation mode and set peak
pressures (cm H2O)
Mukerji and Belik J Perinatology 2015
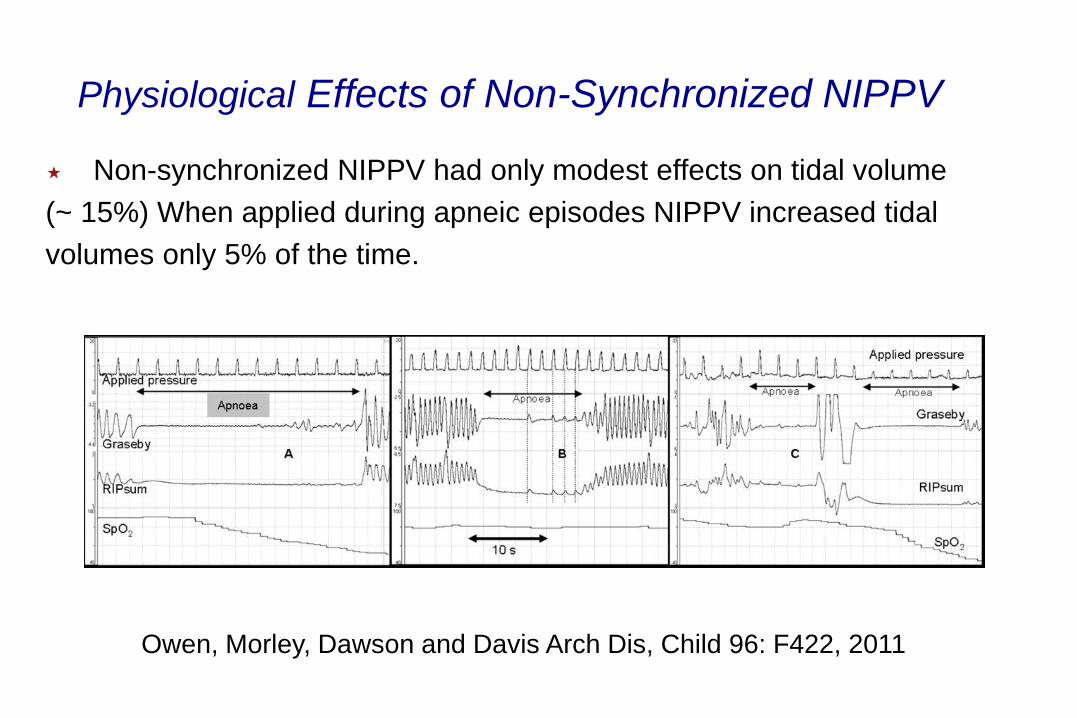
Non-synchronized NIPPV had only modest effects on tidal volume
(~ 15%) When applied during apneic episodes NIPPV increased tidal
volumes only 5% of the time.
Physiological Effects of Non-Synchronized NIPPV
Owen, Morley, Dawson and Davis Arch Dis, Child 96: F422, 2011
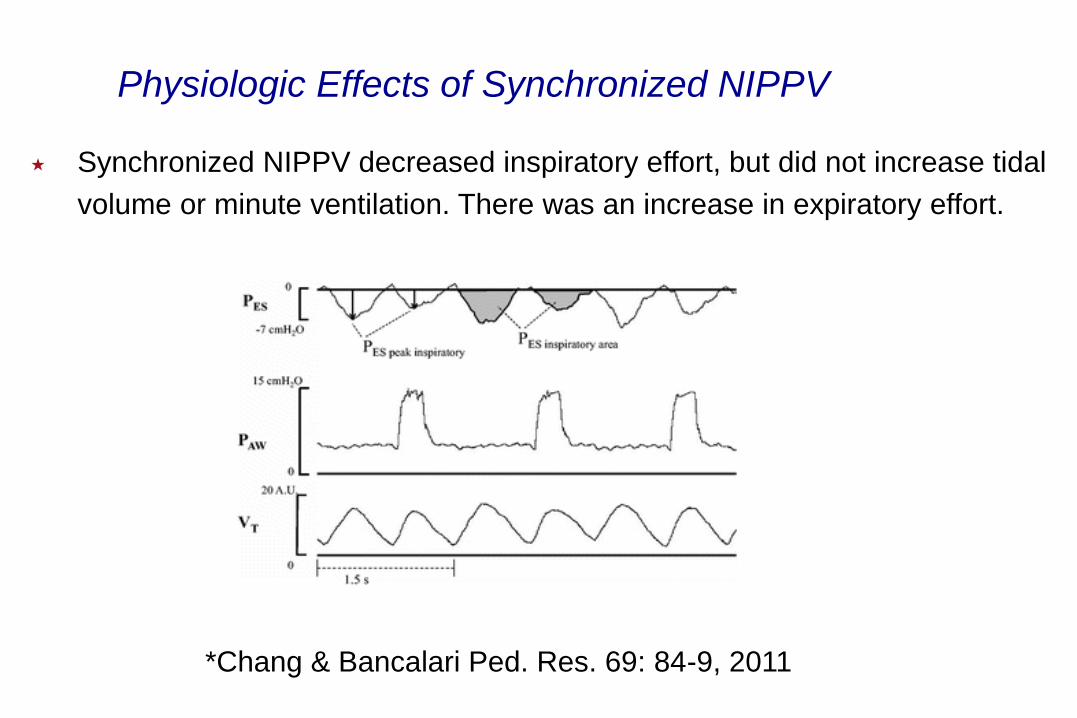
Synchronized NIPPV decreased inspiratory effort, but did not increase tidal
volume or minute ventilation. There was an increase in expiratory effort.
*Chang & Bancalari Ped. Res. 69: 84-9, 2011
Physiologic Effects of Synchronized NIPPV
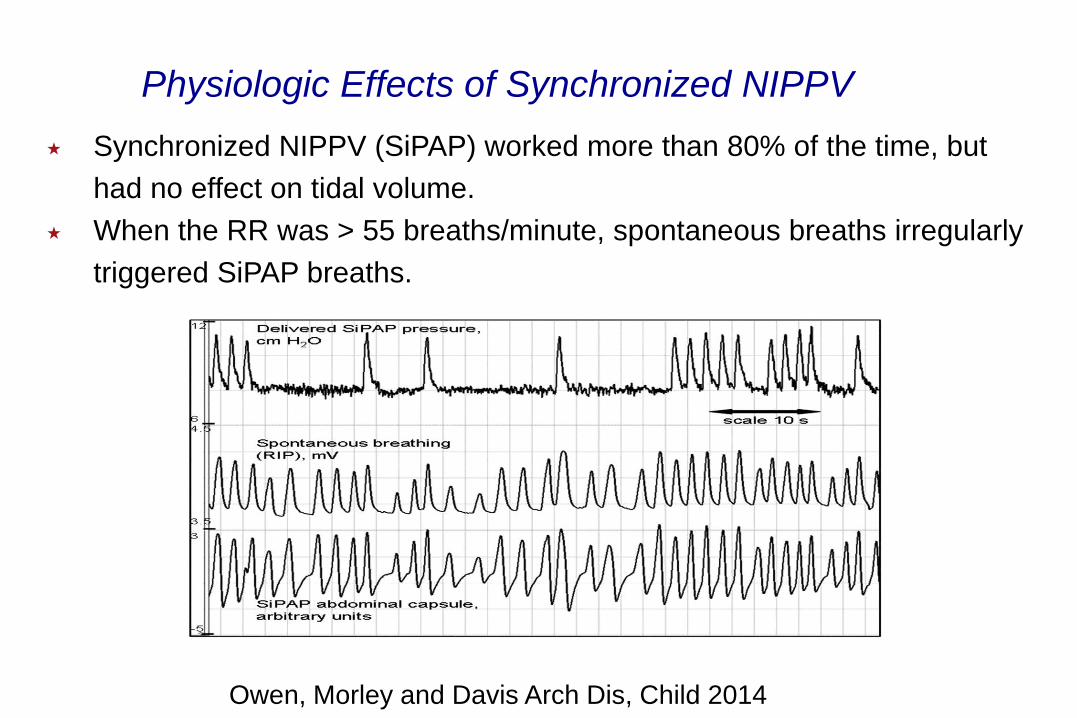
Synchronized NIPPV (SiPAP) worked more than 80% of the time, but
had no effect on tidal volume.
When the RR was > 55 breaths/minute, spontaneous breaths irregularly
triggered SiPAP breaths.
Physiologic Effects of Synchronized NIPPV
Owen, Morley and Davis Arch Dis, Child 2014
An in vitro study using short bi-nasal prongs (SBP) or a small caliber cannula
(RAM)
Using the lung model, a small amount of CO2 was infused and the amount
remaining after 100 seconds was determined.
Pressure transmission to the “lung” and tidal volume were also measured.
NIPPV: Efficacy and lung pressure transmission
Mukerji and Belik J Perinatology 2015
NIPPV: Physiologic Principles
In awake and sleeping adults, NIPPV produces vocal cord
adduction and glottal narrowing resulting in lower tidal volumes
and apneic episodes.
Data suggest that using higher peak pressures does not
consistently increase the likelihood of chest inflation.
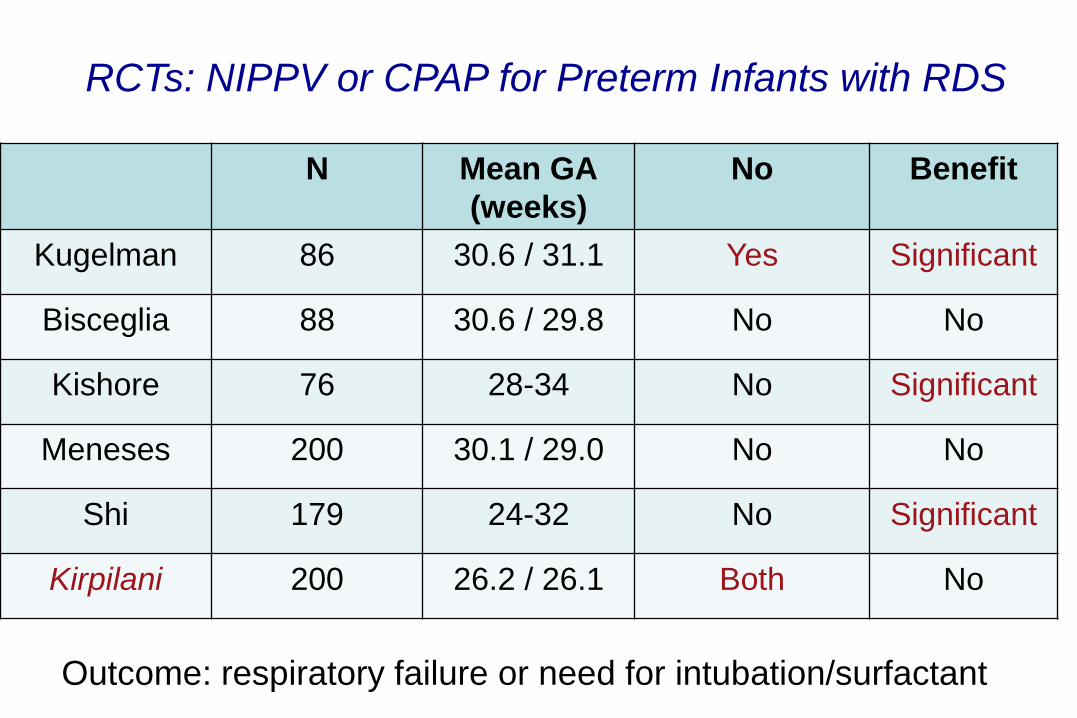
N Mean GA
(weeks)
No Benefit
Kugelman 86 30.6 / 31.1 Yes Significant
Bisceglia 88 30.6 / 29.8 No No
Kishore 76 28-34 No Significant
Meneses 200 30.1 / 29.0 No No
Shi 179 24-32 No Significant
Kirpilani 200 26.2 / 26.1 Both No
RCTs: NIPPV or CPAP for Preterm Infants with RDS
Outcome: respiratory failure or need for intubation/surfactant
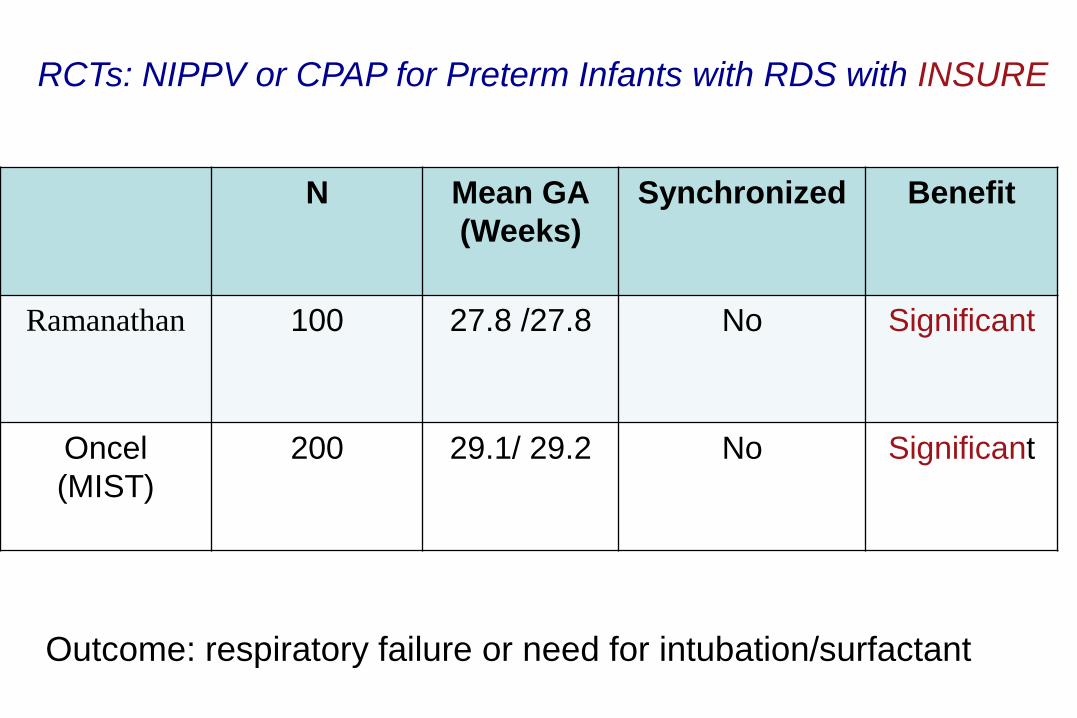
N Mean GA
(Weeks)
Synchronized Benefit
Ramanathan 100 27.8 /27.8 No Significant
Oncel
(MIST)
200 29.1/ 29.2 No Significant
RCTs: NIPPV or CPAP for Preterm Infants with RDS with INSURE
Outcome: respiratory failure or need for intubation/surfactant
1009 infants < 1,000 g randomized to NCPAP or NIPPV when they required
respiratory support in the first 28 days of life (either as the primary mode of
support (first 7 days of life) or following extubation (through day 28)
Median age of intubation: 3.4 days NIPPV group and 3.7 days nCPAP
group; ~ 50% of infants were never intubated;
Primary outcomes death before 36 weeks gestation or survival without BPD
Death or BPD: NIPPV 38.4%; CPAP 36.7% (aOR 1.09 (CI 0.83-1.43)
In a subgroup analysis synchronization made no difference
No differences in the rates of other morbidities, the duration of
respiratory support or time to reach full feeds.
Intubation was needed 59.1% of the CPAP group and 58.3% of the
NIPPV group.
NIPPV or CPAP for Preterm Infants
Kirpalani H et al NEJM 2013;369:611-20

N Synchronized Benefit
Khalaf 32 Yes Significant
Friedlich 41 Yes Significant
Barrington 54 Yes Significant
Khorana 48 No No
Moretti 63 Yes Significant
Kirpilani 845 Both Marginal
O’Brien
133 No No
RCTs: NIPPV or CPAP for Post-extubation Failure
Outcome: respiratory failure or need for intubation
NIPPV or nCPAP for Post Extubation Failure
The meta-analysis (8 trials 1316 infants) demonstrated a
statistically and clinically significant reduction in the risk of meeting
extubation failure criteria. RR 0.71 (CI 0.61-0.82) NNTB = 8.
No significant reduction in the rates of chronic lung disease
No significant differences in death or NEC
The benefits of synchronization need further study.
Davis PG, Lemyre B, De Paoli AG & Kirpalani H, Cochrane Library 2014
High Flow Nasal Cannula
Who is Using HFNC
2/3 of US academic units
Hochwald, J of Neonatal-Perinatal Medicine, 2010
2/3 of Australia and NZ NICUs
Hough, J Paediatr Child Health, 2012
>80% of UK NICUs
Nath, Pediatrics International, 2010
Why are HFNC So Popular
Easy to use
Safe
Decreased WOB
Nurses love it
Babies are calmer
Less CPAP belly
Less nasal trauma
No pneumothoraces
High Flow Nasal Cannula: Proposed Mechanisms
Reduction of inspiratory resistance
Washout of nasopharyngeal dead space
Provision of positive airway pressure
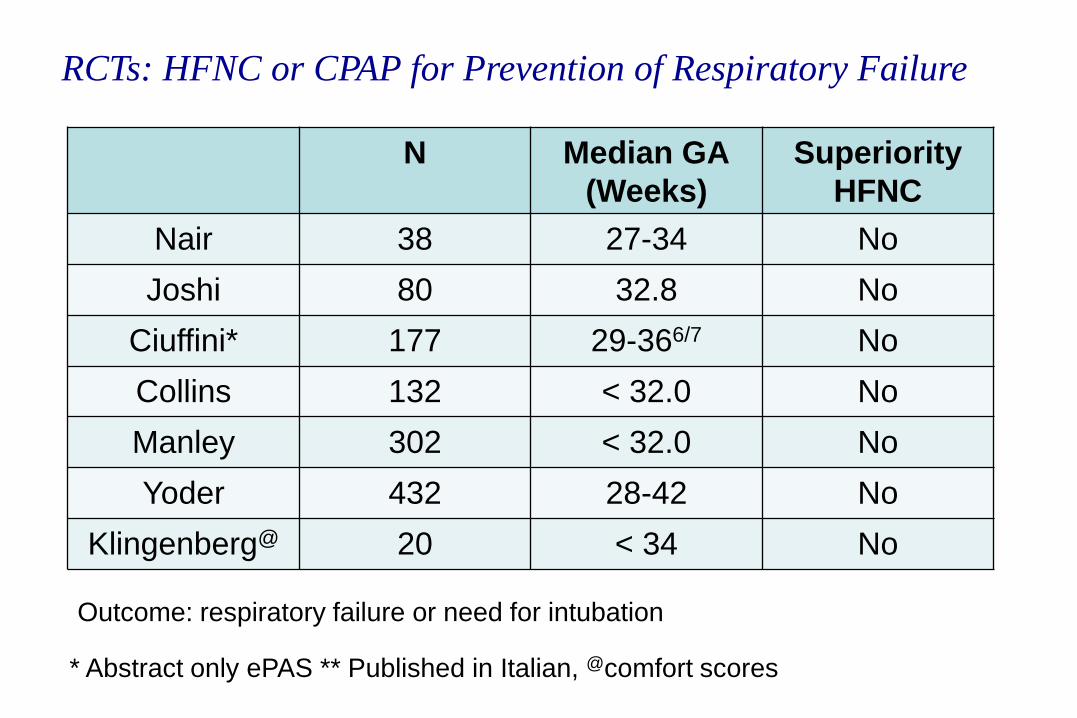
RCTs: HFNC or CPAP for Prevention of Respiratory Failure
Outcome: respiratory failure or need for intubation
* Abstract only ePAS ** Published in Italian, @comfort scores
N Median GA
(Weeks)
Superiority
HFNC
Nair 38 27-34 No
Joshi 80 32.8 No
Ciuffini* 177 29-366/7 No
Collins 132 < 32.0 No
Manley 302 < 32.0 No
Yoder 432 28-42 No
Klingenberg@ 20 < 34 No
A Randomized Controlled Trial to Compare Heated Humidified High-Flow
Nasal Cannulae with Nasal Continuous Positive Airway Pressure Post-
extubation in Premature Infants
Clare L. Collins, MBChB, FRACP1, James R. Holberton, MBBS, FRACP1,
Charles Barfield, MBBS, FRACP1, and Peter G. Davis, MD, FRACP2
J Pediatr. 2013: 162:949-54.
132 ventilated infants randomized to HHHFNC (n=67) or nCPAP (n=65)
after extubation to prevent post extubation failure within 7 days
Mean BW HFNC (1123 grams) nCPAP (1105 grams); 27-30% received
caffeine.
No difference in the rate of extubation failure (HFNC 22%; nCPAP 34%)
20% of infants assigned to nCPAP were changed to HFNC as a result of
nasal trauma (nasal trauma score).
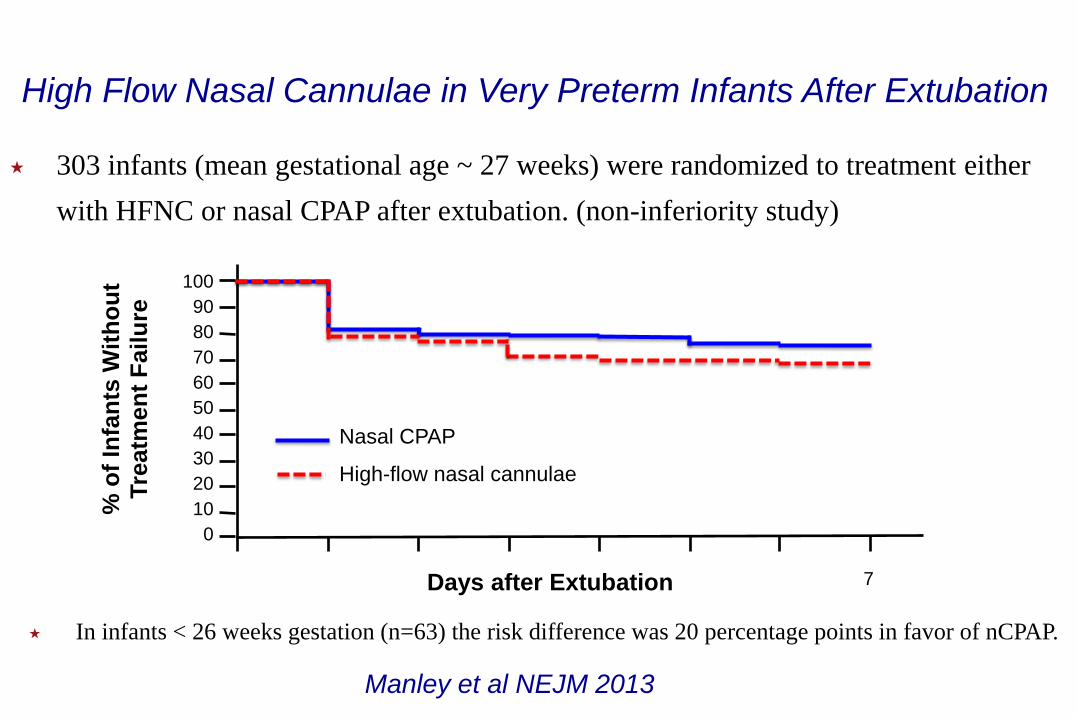
303 infants (mean gestational age ~ 27 weeks) were randomized to treatment either
with HFNC or nasal CPAP after extubation. (non-inferiority study)
Days after Extubation
100
90
80
70
60
50
40
30
20
10
0
Nasal CPAP
High-flow nasal cannulae
% o
f In
fan
ts W
ith
ou
t T
reatm
en
t F
ailu
re
7
In infants < 26 weeks gestation (n=63) the risk difference was 20 percentage points in favor of nCPAP.
High Flow Nasal Cannulae in Very Preterm Infants After Extubation
Manley et al NEJM 2013
DOI: 10.1542/peds.2012-2742; originally published online April 22, 2013; 2013;131;e1482PediatricsSoraya Abbasi
Bradley A. Yoder, Ronald A. Stoddard, Ma Li, Jerald King, Daniel R. Dirnberger andRespiratory Support in Neonates
Heated, Humidified High-Flow Nasal Cannula Versus Nasal CPAP for
http://pediatrics.aappublications.org/content/131/5/e1482.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Columbia University on August 26, 2014pediatrics.aappublications.orgDownloaded from at Columbia University on August 26, 2014pediatrics.aappublications.orgDownloaded from
432 infants 28-42 weeks gestation (≥ 1,000 grams) were randomized to
NCPAP or HFNC to prevent post-extubation failure within 72 hours.
66-69% of infants were ventilated and most received surfactant
There were no significant difference in the primary study outcome (nCPAP
8.2% failure; HFNC 10.8% failure).
Yoder et al Pediatrics 2013;131;e1482
Is the HFNC more “comfortable” than CPAP
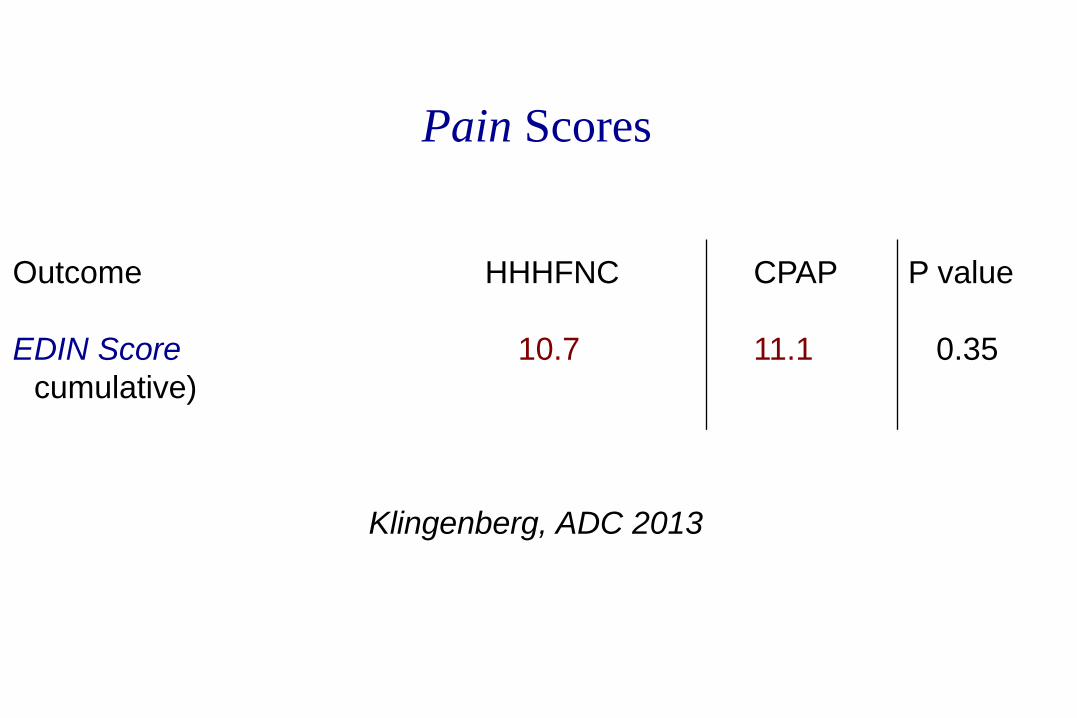
Pain Scores
Klingenberg, ADC 2013
Outcome HHHFNC CPAP P value
EDIN Score 10.7 11.1 0.35
((cumulative)
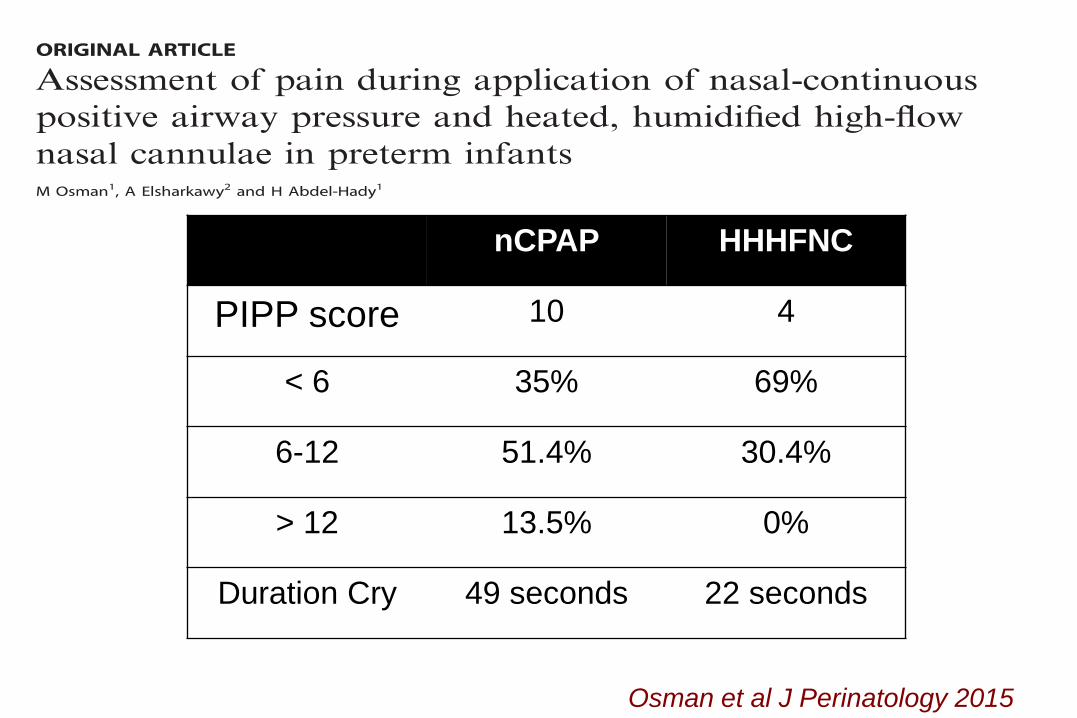
nCPAP HHHFNC
PIPP score 10 4
< 6 35% 69%
6-12 51.4% 30.4%
> 12 13.5% 0%
Duration Cry 49 seconds 22 seconds
Osman et al J Perinatology 2015
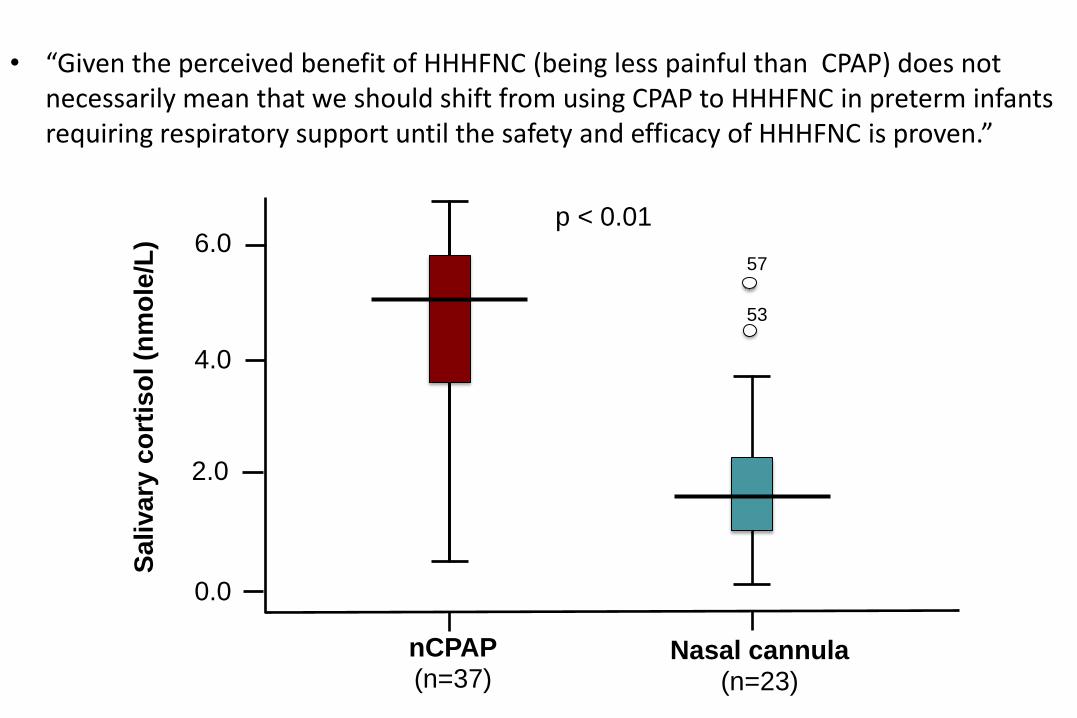
57
53
p < 0.01 6.0
4.0
2.0
0.0
Sa
liva
ry c
ort
iso
l (n
mo
le/L
)
nCPAP (n=37)
Nasal cannula (n=23)
• “Given the perceived benefit of HHHFNC (being less painful than CPAP) does not necessarily mean that we should shift from using CPAP to HHHFNC in preterm infants requiring respiratory support until the safety and efficacy of HHHFNC is proven.”
0 1.1
7.5
0 0 0 0 1.1
9.7
5.5
15.1
8.8
14.4
2.2
10.8
36.3
41.1
20
4.4
41.1
55.6
22.2
2.2 0 0
44
57 24-week, 500g
26-week, 750g
28-week, 1.2g
30-week, 1.5g
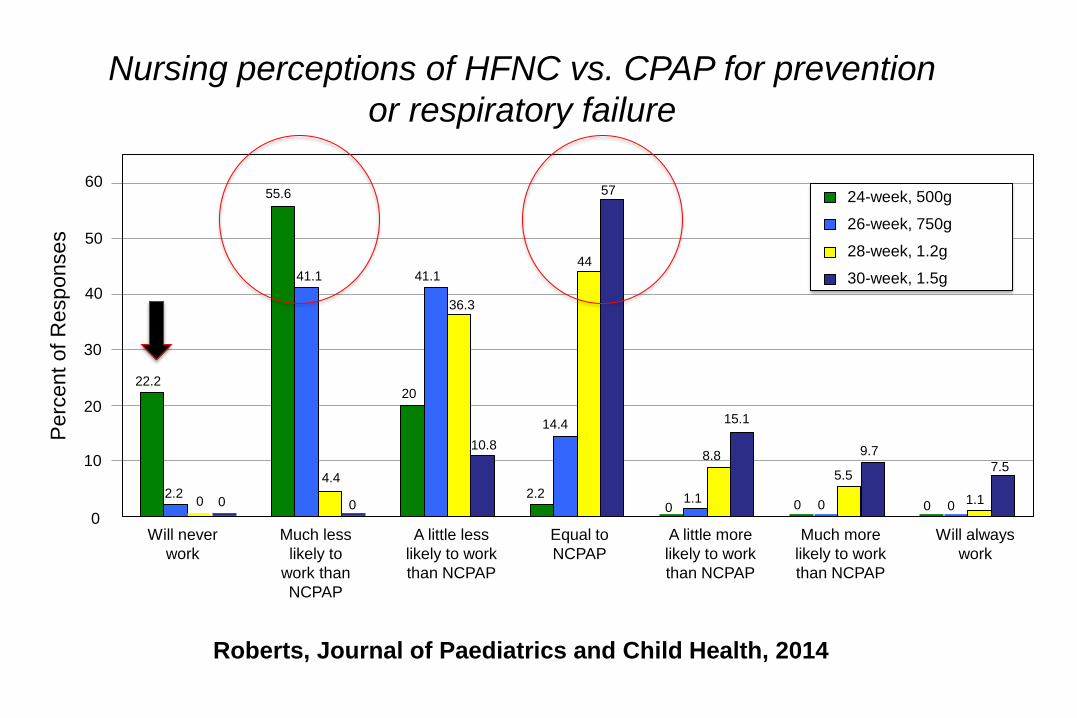
Nursing perceptions of HFNC vs. CPAP for prevention
or respiratory failure
60
50
40
30
20
10
0
Perc
ent
of
Responses
Will never
work
Much less
likely to
work than
NCPAP
A little less
likely to work
than NCPAP
Equal to
NCPAP
A little more
likely to work
than NCPAP
Much more
likely to work
than NCPAP
Will always
work
0
Roberts, Journal of Paediatrics and Child Health, 2014
CPAP: Conclusions
Early use of CPAP with subsequent selective surfactant administration
in extremely preterm infants results in lower rates of BPD/death when
compared to treatment with prophylactic or early surfactant therapy
(LOE 1).
If it is likely that respiratory support with a ventilator will be needed,
early administration of surfactant followed by rapid extubation, is
preferable to prolonged ventilation (LOE 1).
NIPPV: Conclusions
In comparison with nCPAP synchronized NIPPV decreases the frequency
of post-extubation failure
Studies using non-synchronized NIPPV are inconclusive
Data do not support the superiority of NIPPV (synchronized on non-
synchronized) over nasal CPAP for the management of infants with RDS
There is no benefit of NIPPV for apnea of prematurity; however, there
have been no published randomized trials using synchronized NIPPV.
HFNC may be an alternative to nCPAP to prevent post extubation
failure.
HFNC devices may be associated with less nasal trauma and may be
more comfortable (depends on the experience of nurses)
There may be a role for HFNC in infants have been on nCPAP for an
extended period of time.
HHHFNC vs. CPAP: Conclusions
Recommendation for Preterm Infants with RDS
✶ Preterm infants with RDS weighing < 1500 gms. should be allowed time
to demonstrate if they can achieve acceptable ventilation and oxygenation
on CPAP. During that time period, these infants must be monitored
closely. If ventilation is not improving or oxygenation is worsening, or
inadequate with an FiO2 of 60%, these infants should be intubated.
✶ Should infants < 26 weeks gestation receive prophylactic surfactant?
✶ Is there a role for aerosolized surfactant?