Embed Size (px)
Citation preview

Noninvasive Magnetic Resonance Thermography of Recurrent
Rectal Carcinoma in a 1.5 Tesla Hybrid System
Johanna Gellermann,1Waldemar Wlodarczyk,
1Bert Hildebrandt,
2Hildegard Ganter,
1
Anett Nicolau,2Beate Rau,
3Wolfgang Tilly,
1Horst Fahling,
1Jacek Nadobny,
1
Roland Felix,1and Peter Wust
1
1Clinic for Radiation Medicine, 2Clinic for Medicine, Hematology, and Medical Oncology, and 3Clinic for Surgery and Surgical Oncology,Charite Medical School, Berlin, Germany
Abstract
To implement noninvasive thermometry, we installed a hybridsystem consisting of a radiofrequency multiantenna applica-tor (SIGMA-Eye) for deep hyperthermia (BSD-2000/3D) inte-grated into the gantry of a 1.5 Tesla magnetic resonance (MR)tomograph Symphony. This system can record MR data duringradiofrequency heating and is suitable for application andevaluation of methods for MR thermography. In 15 patientswith preirradiated pelvic rectal recurrences, we acquiredphase data sets (25 slices) every 10 to 15 minutes over thetreatment time (60-90 minutes) using gradient echo sequences(echo time = 20 ms), transformed the phase differences to MRtemperatures, and fused the color-coded MR-temperaturedistributions with anatomic T1-weighted MR data sets. Wecould generate one complete series of MR data sets per patientwith satisfactory quality for further analysis. In fat, muscle,water bolus, prostate, bladder, and tumor, we delineatedregions of interest (ROI), used the fat ROI for drift correctionby transforming these regions to a phase shift zero, andevaluated the MR-temperature frequency distributions. MeanMR temperatures (TMR), maximum TMR, full width halfmaximum (FWHM), and other descriptors of tumors andnormal tissues were noninvasively derived and their depen-dencies outlined. In 8 of 15 patients, direct temperaturemeasurements in reference points were available. We corre-lated the tumor MR temperatures with direct measurements,clinical response, and tumor features (volume and location),and found reasonable trends and correlations. Therefore, themean TMR of the tumor might be useful as a variable toevaluate the quality and effectivity of heat treatments, andconsequently as optimization variable. Feasibility of noninva-sive MR thermography for regional hyperthermia has beenshown and should be further investigated. (Cancer Res 2005;65(13): 5872-80)
Introduction
Regional hyperthermia is applied to heat tumor–loadedanatomic regions such as the extremities or pelvis by radiative orcapacitative techniques. Of the different regional hyperthermiaapproaches, particularly radiofrequency regional hyperthermia hasbecome a well-established treatment option for patients withvarious (locally advanced) epithelial and mesenchymal malignan-cies. Together with the conduction of randomized trials that
showed the efficacy of regional hyperthermia in certain clinicalsituations, the proof of a clearcut dose-response relationship (withthermal variables) as well as standardization of the thermometryhas largely contributed to the acceptance of this approach (1–7).However, one unresolved problem of regional hyperthermia as anadjunct to radiotherapy and/or chemotherapy is that its efficacymay largely differ between individuals and tumor entities. We canroughly classify tumors as ‘‘easy-to-heat’’ and ‘‘difficult-to-heat’’.Consequently, a reliable method to recognize tumor diseases,where patients probably benefit from regional hyperthermia, wouldbe highly valuable. Therefore, one strategy to further improveregional hyperthermia is development of a monitoring technique,thus allowing a better navigation of regional hyperthermia systemsand a more precise judgement of the heating quality in anindividual patient (8, 9).Magnetic resonance (MR) imaging has been used for monitoring
of thermoablative interventions for more than a decade. MR signalsare influenced by a mixture of tissue effects (e.g., coagulation andperfusion) in addition to temperature changes (10, 11). Therefore,investigators attempted to separate temperature as an observablein laser-induced thermotherapy (12–15) and focused ultrasound(16, 17), and elucidate the reliability and limitations of MR-guidedthermography. Basically, three methods are available for MRthermography and are discussed in the literature. They are basedon the temperature dependency of the relaxation time T1 (18), thediffusion (apparent diffusion coefficient value; refs. 19, 20), or theproton resonance frequency shift (PFS; refs. 21–23). As T1-weightedsequences are particularly dependent on the type and status of thetissue (24, 25), they are mainly recommended in low-field systemsbecause of their higher contrast. On the contrary, diffusionmethods still suffer from technical and methodical limitations inclinical practice (26). Therefore, for magnetic fields z1 Tesla, PFS-based methods are preferred by most investigators today (27–32).Temperature accuracies of MR-based thermography applied
for ablation techniques are reported to be in the range F3jCto 4.5jC even under favorable in vitro conditions with liverspecimens (12–14, 33). Therefore, MR thermography duringregional hyperthermia seems to be even more challenging becausethe expected temperature differences during such a heat treatment(37-43jC) are near the uncertainties referenced for high temper-ature applications.In a small series, Carter et al. (34) employed a self-developed
cylindrical phased-array hyperthermia applicator (25 cm diameter)to treat sarcomas of the lower leg in a 1.5 Tesla MR scanner (SignaGeneral Electric, Milwaukee, WI). They acquired phase imagesduring regional hyperthermia and showed a satisfactory correla-tion with measured temperatures (SE F 1jC) at moderatepower levels of about 150 W. Peller et al. (35) described a hybridsystem consisting of a SIGMA-Eye applicator (BSD Medical Corp.,
Requests for reprints: Peter Wust, Clinic for Radiation Medicine, Charite MedicalSchool, Campus Virchow Klinikum, Augustenburger Platz 1, D-13353 Berlin, Germany.Phone: 49-450-557202; Fax: 49-450-557979; E-mail: [email protected].
I2005 American Association for Cancer Research.
Cancer Res 2005; 65: (13). July 1, 2005 5872 www.aacrjournals.org
Research Article
Cancer Research. on September 20, 2020. © 2005 American Association forcancerres.aacrjournals.org Downloaded from

Salt Lake City, UT) integrated in a low-field system (0.2 Tesla,Magnetom Open Viva, Siemens AG, Erlangen, Germany). With T1imaging they claimed to control heat treatments concerninghotspot detection and presented selected cases (lower extremity)with satisfactory correlation of T1 and directly measured temper-atures (36).Our group developed a hybrid system where a SIGMA-Eye
applicator (BSD Medical Corp.) was integrated into a mid-fieldsystem (1.5 Tesla, MR Symphony Quantum, Siemens) simulta-neously working with amplifier power levels as high as 1,800 W(37). In phantoms and patients in the SIGMA-Eye applicator,we compared the different thermographic methods as outlinedabove (T1, diffusion, and PFS), and found advantages of the PFSmethod (26).In experiments with an anthropomorphic phantom, we even
found an encouraging absolute agreement (better F0.5jC onaverage) between directly measured temperatures and MR temper-atures derived from phase measurements according to the PFSmethod when a drift correction is done employing MR signals inspecified regions of interest (ROI) of the water bolus (38).In this study, we investigated MR thermography (as developed
and already validated for phantoms in the hybrid system) for thefirst time in a homogenous group of patients with locally recurrentrectal cancer to estimate the potentials and limitations of in vivoMR thermography.
Patients and Methods
Deep pelvic hyperthermia as an adjunct to chemotherapy with
capecitabine (750 mg/m2 bd, d1-32) and five weekly applications ofoxaliplatin (50 mg/m2) was done in 15 preirradiated patients with locally
recurrent rectal cancer who were consecutively enrolled into a phase II
protocol, as described by Hildebrandt et al. (39). Regional hyperthermia in
an MR compatible SIGMA-Eye applicator (BSD Medical Corp.) was providedby the system BSD-2000/3D. The temporal evolution of the heating patterns
was monitored in an MR scanner Symphony (Siemens). Regional
hyperthermia up to a maximum power level (1,600 W amplifier power)and MR acquisitions were simultaneously operated as described by
Gellermann et al. (38). In short, in the hybrid approach, we succeeded to
decouple the two high-frequency systems [i.e., the high power path
(amplifier to applicator at 100 MHz) from the sensitive receiving line (bodycoil to MR receiver)] by suitable filters and other electronic modifications.
Regional hyperthermia was applied as described by Wust et al. (40),
adjusting balanced phases and amplitudes and positioning the tumor
region approximately in the central plane of the applicator.
We used the PFS method for MR thermometry. Before the power of the
heating system is switched on, an anatomic T1-weighted data set of 25slices (1 cm apart) is acquired using a gradient-echo-sequence with echo
time of 4 ms, 256 � 256 matrix, and total acquisition time of 155 seconds
(Fig. 1). Temperature-sensitive images are acquired during the entire heatsession (about every 10-15 minutes), and we employed uncorrected phase
distributions from a spoiled gradient-echo-sequence (echo time, 20 ms;
repetition time, 600 ms; 25 slices; 128 � 128 matrix; total acquisition time,
78 seconds). A reference phase data set is acquired before power-on. Fromthe phase differences, MR-temperature distributions are calculated and
superposed as color-coded distributions with the anatomic data. The MR
data sets are transferred to a planning workstation into the software
platform AMIRA-HyperPlan to calculate MR-temperature distributions asdescribed elsewhere (38).
For the PFS method, the drift correction (compensating for changes ofthe static magnetic field B0) is a critical issue. This is especially important
because the thermal load of patients to the surroundings during clinical
heat sessions is higher than in case of phantom experiments (patients
release in the steady state up to several hundred watts to the environment
in the MR gantry). In patients it proved successful to employ the fact thatthe resonance frequency of protons in fat has no temperature dependency:
After labeling suitable regions in the adipose tissue (Fig. 1, middle row),
a linear transformation of the MR phase data sets is done in a way that
the phase changes are reversed to zero in the selected fat regions. For thecalculation of this linear correction function, three MR temperature
gradients in lateral, vertical, and longitudinal direction are purported and
adapted in an iterative procedure until the fat is as homogeneous as
possible in green color (zero), as illustrated in Fig. 1 (right row). Thetransformation is interpolated/extrapolated to the entire data set
including the water bolus.
To quantify and further evaluate the MR-temperature distributions over
the full treatment course, we draw additional ROIs in selected tissues such
as muscle (M. glutaeus maximus, M. adductor), tumor, prostate, and
bladder (as also shown in Fig. 1). We delineated the tumor volume with lessextension than suspected from the anatomic MR sections (Fig. 1) to reduce
errors at boundaries, in particular caused by any kind of movement or shift.
Other tissues (in particular large and small intestine) are so afflicted with(susceptibility) artifacts that estimation of MR temperatures is not possible
(see the marked regions in Fig. 1).
We acquired four to eight phase data sets per heat treatment in 10- to
15-minute intervals in every patient/treatment corresponding to the
intervals for the thermal mapping under routine conditions. Whereas the
pure acquisition time is <5 minutes, the total time for data transfer andpostprocessing to generate and visualize the final MR-temperature
distributions amounts to 10 minutes.
Obviously, a visual control of the (corrected) MR temperature maps is not
precisely enough for treatment decisions. To perform a quantitative analysis
and to obtain objective criteria, we determined in every ROI mean MR
temperatures at every acquisition time and, in consequence, (mean) MRtemperature-time curves as shown in Fig. 2 (top).
In addition, we used utilities of AMIRA-HyperPlan to calculate MR-temperature frequency distributions for every ROI, which show the
variation of the MR temperature in the single voxels (Fig. 3). Based on
these frequency distributions, we derived various statistical descriptors,
not only mean values but also full width half maximums (FWHM), shownin Fig. 3, as well as index temperatures Tx . The index temperature Tx is
defined as the MR temperature exceeded by x% of the voxels of the ROI
under consideration. These index temperatures have been often used to
analyze thermal data and have been successfully correlated with clinicalend points (1, 3).
Univariate analysis of thermal variables with their attribution to responseand other tumor-related factors (e.g., location) is done by the distribution-
free Mann-Whitney test in the statistical program package SPSS. Correlation
analyses and graphical representations of the frequency distributions aredone in the Office program Excel.
This analysis of the MR data sets of a heat treatment is time-consuming
and not fully automated in the present software version. Presently, anexperienced assistant needs up to 2 days for the evaluation and
documentation of one heat treatment. Because in some patients only one
heat session was done in the hybrid system (by logistical reasons) and inother patients MR data sets were incomplete and/or disturbed (by various
technical reasons), we limited our analysis to one representative
hyperthermia session per patient with the best series of MR data sets
available. A few patients must be excluded from the study because we failedto record even one set of MR data useful for evaluation.
Results
Magnetic resonance–temperature distributions in tissues atsteady state. A total of 15 heat sessions of 15 patients (5 females,10 men) with satisfactory MR quality could be selected for theanalysis. In these patients with presacral recurrencies, the tumorvolumes have a large variation from 13 to 420 mL (mean, 77 mL).The longitudinal tumor position (along the patient axis) is variable,ranging from �2 cm below the symphysis to +7 cm above the
Regional Hyperthermia under MR Monitoring
www.aacrjournals.org 5873 Cancer Res 2005; 65: (13). July 1, 2005
Cancer Research. on September 20, 2020. © 2005 American Association forcancerres.aacrjournals.org Downloaded from

symphysis (mean, 2.5 cm). We assigned also the position of thecentral plane of the applicator with respect to the symphysis,ranging from �2 to +4 cm. We did the treatments applying a totalamplifier power of 1,000 to 1,600 W (mean, 1,300 W) with differentstandard adjustments of phases and amplitudes (38).The total treatment time (power-on) ranged from 62 to
92 minutes (mean, 80 minutes). At steady state time between 40and 88 minutes (mean, 66 minutes), a variety of statisticaldescriptors of the MR-temperature distribution in the ROI (seeDiscussion and Figs. 1–3) were derived for the tumors and thenormal tissues, which are summarized in Fig. 4.We find a higher range of temperatures (and fluctuations) in
tumors in comparison with the various ROI muscles. In one third ofthe tumors, an effective hyperthermia seems difficult with a meanvalue of <3.5 MR-deg (i.e., <41jC). In one third of the tumors(5 of 15), mean MR temperatures of >5 MR-deg (i.e., >42.5jC) areachieved corresponding to easy-to-heat tumors.The mean MR temperatures in the presacral tumors have
considerable variation extending from nearly 0 (0.6 MR-deg)
up to cytotoxic values of 8.9 MR-deg. The fluctuations of the MR-temperature distributions (FWHM) are also quite high in thetumors and of the same range (2.2-7.6 MR-deg). In the tumor ROIs,nearly always some spots with high MR temperatures were found.Therefore, we ascertained the mean temperature in the 5 mL of thetumor ROI with the highest MR temperatures (32 voxel of 0.16 mL;f5 mL). Only in 2 of 15 tumors the mean MR temperature in thishigh-temperature region was below 6 MR-deg (corresponding to<43.5jC); in 10 of 15 tumors we achieved considerable elevationsabove 8.5 MR-deg (corresponding to 45-46jC). For the estimationof the physical temperature (in degree Celsius), we neglectperfusion at this time (see Discussion).Evidently, areas (necroses?) exist in tumors, which are heated to
higher MR temperatures. Muscles are more homogeneous and theMR temperatures are below critical values. Only in a minority of themuscle ROI (<10%) we found elevations >8.0 MR-deg in appreciableportions of the volume (5 mL). In fact, 8.0 MR-deg wouldcorrespond to a potentially harmful temperature elevation of45jC to 46jC. However, a fraction of 1 to 4 MR-deg can be
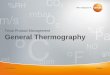
Figure 1. Part of a three-dimensional data set for a patient with extensive necrotic presacral recurrence. The color-coded MR temperatures are fused with theanatomic data set (left). Middle, without drift correction. Right, after drift correction according to fat labels. The ROIs of some muscles, tumor, and bolus (top left/right,bottom left/right ) are shown and assigned.
Cancer Research
Cancer Res 2005; 65: (13). July 1, 2005 5874 www.aacrjournals.org
Cancer Research. on September 20, 2020. © 2005 American Association forcancerres.aacrjournals.org Downloaded from

attributed to the increase of perfusion (41, 42) via increasedoxygenation (blood oxygen level–dependent effect) as furtherelucidated in Discussion.In muscle tissue, we identified lower mean MR temperatures
hTMRi with less fluctuations. Whereas the mean value in muscle isonly slightly below the mean tumor MR temperature (3.8 versus 4.2MR-deg), the fluctuations are considerably lower (FWHM, 3.8versus 4.8 MR-deg). Topmost is the difference of the high-temperature parts hTimax(5 mL) (i.e., 5.3 MR-deg in muscle versus8.5 MR-deg intratumorally). We found no single measurement (0 of60) in the muscle with a hTimax(5 mL) above 8.5 MR-deg.We also differentiated the muscle MR temperatures with
respect to anatomic regions (see Fig. 1). Whereas the MRtemperatures in the glutaeal muscles were found slightly below
the average value (right region, 3.5 F 1.0; left region, 3.8 F 1.2),the adductor muscles achieved slightly higher temperatures (rightregion, 4.2 F 1.6; left region, 4.0 F 1.8). No differences betweenright and left were found.In organs such as prostate and bladder, the variations were
considerably higher as in the muscle. Whereas the MR-temperaturedistributions of the prostate glands (determined in 10 men) arequite stable (Fig. 4) and seem to reflect true physiologic features,the distributions achieved for the bladders seemed unreliable andwere removed from the analysis (see Discussion). The contouredROIs of the fat tissue (Fig. 1) were used for the drift correction. TheFWHMs in fat are consequently low per construction, and the MRtemperatures in fat oscillate around 0 (0.0007 F 0.015 SD) and arethe main source of statistical error.
Figure 2. Time sequences of correctedMR-temperature distributions in a centralplane of the tumor. MR temperature-timecurves of some tissues (mean, valuesof the ROI according to Fig. 1). Note thedifferent behavior in the necrosis (increaseover the whole treatment time) and othertissues (transition into a plateau).
Regional Hyperthermia under MR Monitoring
www.aacrjournals.org 5875 Cancer Res 2005; 65: (13). July 1, 2005
Cancer Research. on September 20, 2020. © 2005 American Association forcancerres.aacrjournals.org Downloaded from

From the FWHM in fat, we estimate the statistical error for theMR temperatures, resulting from the drift or other spatialvariations, to be better than F1.4 MR-deg.Magnetic resonance–temperature-time curves and direct
temperature measurements. The time curves of mean MRtemperatures over f80 minutes are in accordance with typicaldirectly recorded temperature-time curves (see Fig. 2) well knownfrom invasive or minimal-invasive thermometry in regionalhyperthermia (3, 42). In the majority (11 of 15 heat sessions) wefound a transition of the mean MR-temperature of the tumor into aplateau with a thermal relaxation time of 15 to 20 minutes. Theplateau is typically achieved after a range of 25 to 50 minutes. In 2of 15 patients, we found a continuous increase of the mean MRtemperature over the whole treatment time (power-on), as shownin Fig. 2, for the central part in the tumor. In 2 of 15 patients, wecould not show any reasonable increase of the MR temperature andfound instead fluctuations in the range of 1 to 2 MR-deg or adecrease after a short increase of 1 to 2 MR-deg.We expected an increase of the width of the MR-temperature
distribution over time (caused by an accumulation of errors) andanalyzed the FWHM for different tissues by comparing the meanvalues at the start (around 16 minutes heating time) and end (afteraround 80 minutes heating time) of the heat treatments. In fact, thedistributions get broader in all tissues. However, the elevation isstrongest in the tumors (2 MR-deg) and not fully explained by the
increase of the width in fat (of only 1 MR-deg). The accuracy of theMR temperature by the PFS method (phase differences), assuggested by the fluctuations in the fat, is therefore F1 MR-deg(after 20 minutes treatment time) and increases during thetreatment up to a final value of less F1.5 MR-deg. The FWHMsin muscle exceed only a little the FWHMs in fat and are obviouslyalso due to statistical errors.Direct thermometry was done in the water bolus (upper bolus)
and in tumor-related endoluminal reference points (rectum, vagina,and bladder) in 8 of 15 patients. In 7 of 15 patients, a tumor-relatedthermometry was not possible by minimal-invasive methods(status after abdomino-perineal rectum resection) and/or wasrefused by the patient.Table 1 documents a good agreement on average of the
directly measured temperature increase in the upper bolus (by11.2jC) in comparison with the MR temperature increase in theROI in the upper bolus (by 10.9 MR-deg). In single cases wefound higher deviations between MR temperature and directlymeasured temperature by several degrees Celsius. This isexplained by the vertical thermal gradient from the lower tothe upper part of the bolus (Table 1, on average nearly 4 MR-deg)in conjunction with the uncertainty to find the position of thethermistor for direct thermometry in the upper bolus.The tumor-related minimal-invasive temperatures are correlat-
ed with the mean MR temperatures in the tumor volumes
Figure 3. Time sequences of the MR-temperature frequency distributions in some tissues of interest delineated in Fig. 1 and visualized in Fig. 2.
Cancer Research
Cancer Res 2005; 65: (13). July 1, 2005 5876 www.aacrjournals.org
Cancer Research. on September 20, 2020. © 2005 American Association forcancerres.aacrjournals.org Downloaded from

(R = 0.67). The correlation is not so good because in some tumors(but not in all) we found slightly higher MR temperatures incomparison with the reference temperatures (in degree Celsius).However, on the whole, the directly measured temperatures areuseful indicators for the hTMRi in the tumor. This is an ex postapology of the earlier concept to replace intratumoral (invasive)measurements by minimal-invasive endoluminal temperaturemeasurements for regional hyperthermia of the pelvic region(3, 43), which has been controversially discussed in the litera-ture (44).Dependencies of the magnetic resonance–temperature
distributions. We analyzed the dependencies of FWHM (tumor),which increase continuously during the treatment time and exceedthe FWHM of the normal tissues (Table 1).We found a trend that the FWHMs in the tumor depend on the
mean level of the MR temperature (P = 0.06, Mann-Whitney test),which we interpret as the width of the distribution increasing withthe temperature level. However, the FWHM (tumor) does not at alldepend on the FWHM ( fat). We conclude that the fluctuations ofthe MR-temperature distribution in the tumors are mainlyaddressed to the tumor biology and/or physiology, and might bea characteristic attribute of a tumor. We did not find anydependency of FWHM (tumor) on the tumor volume, amplifierpower, or, in particular, the response.Then we scrutinized the dependencies of the mean tumor MR
temperatures, which are summarized in Table 2. Most importantly,we found a significant correlation of clinical response with themean MR temperature in the tumor (P = 0.04) in correspondence
to the findings for tumor-related direct thermometry in numerousphase II studies (1, 45, 46).We found, in spite of the limited case number, additional
interesting interrelationships: The proximally (cranially) locatedtumors (>2 cm above the symphysis) are more difficult to heat(P = 0.05), which agrees with phantom measurements (38) andvarious modeling calculations (e.g., ref. 47). The correlationbetween the mean MR temperatures in the muscles and the meanMR temperatures in the tumors is also statistically evident(P = 0.02). From these data it seems that we can categorize thepatients into two groups (easy-to-heat and difficult-to-heat); in theeasy-to-heat group all tissues, including the muscles, are wellheated (with increase of MR temperature). No clear correlation (buta trend) was found for a correlation of hTMRi with the tumorvolume and the total power adjusted in the amplifier.
Discussion
The objective of this work is to develop a method to achievethree-dimensional data sets about heat treatments noninvasively byMR imaging (so-called MR temperatures), to analyze these data sets,and to discuss useful quality variables we can derive from them tocharacterize the heat treatment. Note that the identity of these MRvariables with temperatures in degree Celsius is not required as longas MR variables are usable to assess the quality and effectiveness ofthe heat treatment under monitoring (see below).We installed a hybrid system (37) to perform regional hyperther-
mia in a multiantenna applicator under simultaneous MR
Figure 4. MR temperatures (MR-deg) and width of the MR-temperature distributions (FWHM) and mean maximum MR temperatures in the warmest 5 mL of theROI for tumors and normal tissues at steady state. Mean F SD (over all patients) are given in brackets at the bottom. The mean MR temperature in fat is by definitionnear zero. The statistical descriptors are derived from frequency distributions as shown in Fig. 3.
Regional Hyperthermia under MR Monitoring
www.aacrjournals.org 5877 Cancer Res 2005; 65: (13). July 1, 2005
Cancer Research. on September 20, 2020. © 2005 American Association forcancerres.aacrjournals.org Downloaded from

monitoring and to acquire MR data sets during the entire treatmenttime of 90 minutes under routine conditions (37, 38). Achieving anundisturbed MR data set during radiofrequency heating is a difficulttask. Therefore, in the beginning not every heating session wassuccessful, and the number of evaluable MR data sets was limited.With increasing experience, the quality of the monitoring is moreand more improving.The data analysis to extract thermal MR variables is still time-
consuming and not online yet. However, a visual MR-temperaturedistribution is already available during the heat treatment (after5-10 minutes). Further development and/or refinement of softwaremodules is under way and will finally enable access to(quantitative) MR-thermal variables faster, ideally online.The drift correction is done by a fat correction procedure , which
is based on the postulate that the proton resonance frequency offat tissue has no frequency shift during the heat treatment (21). Fattissue (low-water content tissue) typically contains more than 70%fat and less than 10% water. During the segmentation process ofthe fat, we verify this low water content from the T1-weightedmagnitude images (high water content, e.g., caused by edema,would be recognized by an intensity loss, i.e. darkening, of the fattissue). The low water content might result in a slight systematicunderestimation of the final MR temperature in the range of 10%of the temperature increase of the fat tissue. However, thetemperature change in the s.c. adipose tissue is small becausethe power absorption is low (lower electrical conductivity) and theproximity to the water bolus provides a cooling reservoir to keepthe temperature constant during heating. Therefore, the error issmall (a few tenths of a degree).Larger deviations are observed in highly exposed regions such as
the ischiorectal fossa, probably because of the higher temperatures,which induce relevant phase changes even if the water content islow in conjunction with perfusion increase; however, these regionsare not segmented for the fat correction procedure (Fig. 1).A perfusion increase induces an MR temperature increase
(pseudo-temperature increase) via the blood oxygen level–
dependent contrast because the diamagnetic oxyhemoglobinreduces the local static magnetic field (changing the protonresonance frequency in the same direction as the temperatureincrease). In selected patients (data not shown here), we measuredtemperatures directly in degree Celsius as well as perfusionchanges (via contrast media dynamics) and MR temperature at thesame location, and found a perfusion increase of roughly 5 mL/100g/min, corresponding to 1 MR-deg (but this is just an estimationand thus needs further confirmation). Conversely, in case of ablood flow decrease, MR temperature might underestimate the realtemperature (in degree Celsius). If preferential perfusion directionsexist inside the image voxels, this can also influence the MRtemperature (48). This also could be a reason for the broadening ofthe FWHM of tumor tissue in comparison with normal tissues,which have a well-regulated blood supply.We should consider the interference of temperature and
perfusion when interpreting MR-temperature distributions. Inrecurrent tumors (and either the more if preirradiated), we do notexpect high perfusion and especially no or low reactive perfusionincreases under hyperthermia conditions (1). Therefore, MRtemperatures in the tumors should be near the real temperatures(Table 2; Fig. 4). A mean MR temperature >4 MR-deg indicates meantemperatures near 42jC, but higher temperatures are observed inparts of the tumor with Tmax (in 5 mL) approaching 45jC to 46jC.This is in agreement with our ideas of advanced tumors, which areheterogeneous and contain necrotic (i.e., low perfused) areas.In some tumors, decrease of perfusion during radiofrequency
hyperthermia is expected and, consequently, an underestimation oftemperatures in degree Celsius. In fact, we find a few tumors (onethird) in Fig. 4 with very low MR temperatures where we suspectdecline of perfusion.The mean MR temperatures in the specified muscle regions are
only slightly lower (<4 MR-deg), predicting temperatures between41jC and 42jC ( for perfusion change zero). However, we expectedlower temperatures of 39jC to 41jC (42) and, therefore, 1 to 2 MR-deg might be due to perfusion increase. Muscle is a reactive tissuewhere blood flow can be physiologically elevated 10- to 30-foldabove the basal value (of only a few milliliters per 100 g per minute)if an adequate stimulus is done (e.g., exercise).
Table 2. Dependence of the mean steady-state MRtemperature in the tumor on certain factors
hTMRitumor P
Response 0.04
Responder 7 of 15 5.5Nonresponder 8 of 15 3.1
Volume (mL) 0.16
<50 9 of 15 4.8
>50 6 of 15 3.3Location 0.05
V2 cm symphysis 7 of 15 5.4
>2 cm symphysis 8 of 15 3.1
Power (W) 0.20z1,300 9 of 15 5.0
<1,300 6 of 15 3.0
hTMRimuscle 0.02
>3.8 7 of 15 5.4V3.8 8 of 15 3.2
Table 1. Temporal evolution of the MR-temperaturedistributions in some tissues and regions in the bolus (incomparison with direct measurements in the upper bolus)
Start(16 F 3 min)
Difference End(80 F 9 min)
hFWHMitumor F SD 3.4 F 1.2 5.4 F 1.8hFWHMifat F SD 1.9 F 0.9 2.9 F 0.8
hFWHMimuscle F SD 2.1 F 0.7 3.8 F 1.0
hMR tempibolusu.l. 1.6 F 1.3 10.9 F 2.3 12.6 F 3.1
u.r. 1.4 F 1.1 12.6 F 3.1
b.l. 0.8 F 0.8 7.2 F 1.6 7.8 F 2.5
b.r. 0.9 F 0.7 8.3 F 2.5Tbolus (direct, top) 25.8 F 2.5 11.2 F 2.9 37.0 F 2.2
Flat fluctuations
(after fat
corrections)
0.18 F 0.17 0.29 F 0.19
NOTE: Width of the distribution: FWHM. u.l., upper left; u.r., upperright; b.l., bottom left; b.r., bottom right. Also the fluctuations in the fat
are shown.
Cancer Research
Cancer Res 2005; 65: (13). July 1, 2005 5878 www.aacrjournals.org
Cancer Research. on September 20, 2020. © 2005 American Association forcancerres.aacrjournals.org Downloaded from

In the prostate glands the MR temperatures are higher, probablydue to both higher temperatures and perfusion increase. This is inaccordance with direct temperature measurements in the urethraon occasion of heat treatments of prostate cancer, yieldingminimum values near 41jC, which is 1jC to 2jC higher than inmuscle (46).In the bladder we found even higher MR temperatures (mean, >7
MR-deg). Because of the variable filling of the bladder during theheat treatment, we identified these variables as artificially high. Aconstant bladder filling must be adhered (via a catheter) to achievereliable MR temperatures of the bladder. In this case, a directmeasurement by a thermistor in the catheter seems easier.The mean MR temperatures hTMRi in the specified tumor ROIs
correlate with directly measured reference temperatures anddepend in a reasonable and statistically relevant manner onvarious variables, in particular on the clinical response (Table 2).We conclude that the hTMRi of these tumors are useful tocharacterize the heat treatments in at least the same way asinvasive or minimal-invasive thermal data published earlier(1, 3, 46). Because a three-dimensional MR-temperature distribu-tion represents more complete information than temperaturemeasurements in points or along scan lines, hTMRi should be evena better predictor. This has to be validated in a larger number ofpatients.For further improvements of the analysis, we have to include
the perfusion, which can be determined by contrast mediastudies. For the majority of tumors, the perfusion change underheating is small, indicating an agreement of MR and realtemperatures. Some tumors—probably a limited percentage—willreact (in both directions), and this must be addressed either bycomplementary perfusion measurements or by other additional
considerations. MR temperature might even be a better predictorfor clinical outcome than real temperature because perfusiondecrease is typically associated with necrotic regions, which arenegative prognostic factors, whereas perfusion increase mightintensify the effectiveness by improving reoxygenation or druguptake.It is also useful to include other temperature-dependent MR data
sets. The T1 relaxation time is a suitable candidate to provideadditional information because it indicates the temperatureincrease in fat and depends less on perfusion (49). As thedependency on perfusion is different for T1 and phases (PFS),both observables together incorporate information about perfusionchanges induced by hyperthermia.All in all, we have shown the feasibility of noninvasive MR
thermography for deep hyperthermia in the pelvis. The applicationfor lower extremities is straightforward with the same procedure.In the abdominal region (e.g., the liver), motion is a severedisturbing factor and must be compensated with dedicatedtechniques (e.g., navigation).The MR data of various sequences under hyperthermia contain
much more information than discussed in this article, and mightprovide valuable insight into tumor physiology and biology. Furtherresearch on this innovative field is strongly desirable.
Acknowledgments
Received 11/9/2004; revised 3/9/2005; accepted 4/19/2005.Grant support: Deutsche Forschungsgemeinschaft, grant Wl 8/1-1 and Wu 235/1-1.The costs of publication of this article were defrayed in part by the payment of page
charges. This article must therefore be hereby marked advertisement in accordancewith 18 U.S.C. Section 1734 solely to indicate this fact.
We thank Paul Turner (BSD Medical Corp.) for his excellent cooperation andfruitful discussions.
References1. Rau B, Wust P, Tilly W, et al. Preoperative radio-chemotherapy in locally advanced recurrent rectalcancer: regional radiofrequency hyperthermia correlateswith clinical parameters. Int J Radiat Oncol Biol Phys2000;48:381–91.
2. Van der Zee J. Heating the patient: a promisingapproach. Ann Oncol 2002;13:1173–84.
3. Wust P, Gellermann J, Harder C, et al. Rationale forusing invasive thermometry for regional hyperthermiaof pelvic tumors. Int J Radiat Oncol Biol Phys 1998;41:1129–37.
4. Wust P, Hildebrandt B, Sreenivasa G, et al. Hyperther-mia in a combined treatment of cancer. Lancet Oncol2002;3:487–97.
5. Harima Y, Nagata K, Harinma K, et al. A randomizedclinical trial of radiation therapy versus thermoradio-therapy in stage III cervical carcinoma. Int J Hyper-thermia 2001;17:97–105.
6. Hildebrandt B, Wust P, Rau B, Schlag PM, Riess H.Regional hyperthermia for rectal cancer. Lancet 2000;356:771–2.
7. Van der Zee J, Gonzalez Gonzales D, et al. Comparisonof radiotherapy alone with radiotherapy plus hyperther-mia in locally advanced pelvic tumors: a prospective,randomised, multicentre trial. Lancet 2000;355:1119–25.
8. Behnia B, Suthar M, Webb AG. Closed-loop feedbackcontrol of phased-array microwave heating usingthermal measurements from magnetic resonance imag-ing. Magn Reson Eng 2002;15:101–10.
9. Kowalski M, Behnia B, Webb AG, et al. Optimization ofelectromagnetic phased-arrays for hyperthermia viamagnetic resonance temperature estimation. IEEETrans Biomed Eng 2002;49:1229–41.
10. Bremer C, Kreft G, Filler T, Reimer P. Accuracy of
non-enhanced MRI to monitor histological lesion sizeduring laser-induced interstitial thermotherapy. EurRadiol 2002;12:237–44.
11. McDannold N, Hynynen K, Jolesz F. MRI monitoringof the thermal ablation of tissues: effects of longexposure times. J Magn Reson Imaging 2001;13:421–7.
12. Bar NK, Schulz T, Puccini S, Schirmer T, Kahn T,Busse H. MRT-gestutzte laserinduzierte thermoablationbei lebertumoren—klinische aspekte und konzept einesuberwachungssystems. Z Med Phys 2003;13:209–13.
13. Heisterkamp J, Matheijssen NAA, van Hillegersberg R,et al. Accuracy of MR phase mapping for temperaturemonitoring during interstitial laser coagulation (ILC) inthe liver at rest and simulated respiration. Magn ResonMed 1999;41:919–25.
14. Botnar RM, Steiner P, Dubno B, Erhart P, vonSchulthess GK, Debatin JF. Temperature quantificationusing the proton frequency shift technique: in vitro andin vivo validation in an open 0.5 tesla interventional MRscanner during RF ablation. J Magn Reson Imaging2001;13:437–44.
15. Chen JC, Moriarty JA, Derbyshire JA, et al. Prostatecancer. MR imaging and thermometry during micro-wave thermal ablation—initial experience. Radiology2000;214:290–7.
16. Hynynen K, Pomeroy O, Smith DN, et al. MRimaging-guided ultrasound surgery of fibroadenomasin the breast: a feasibility study. Radiology 2001;219:176–85.
17. McDannold N, Hynynen K, Wolf D, Wolf G,Jolesz F. MRI evaluation of thermal ablation oftumors with focused ultrasound. J Magn ResonImaging 1998;8:91–100.
18. Parker DL, Smith V, Sheldon P, Crooks LE, Fussell L.Temperature distribution measurements in two-dimen-sion NMR imaging. Med Phys 1983;10:321–5.
19. Delannoy J, Chen CN, Turener R, et al. Noninvasivetemperature imaging using diffusion MRI. Magn ResonMed 1991;19:333–9.
20. Samulski TV, MacFall J, Zhang Y, et al. Noninvasivethermometry using magnetic resonance diffusion imag-ing: potential for application in hyperthermic oncology.Int J Hyperthermia 1992;8:819–29.
21. De Poorter J, De Wagter C, De Deene Y, et al.Noninvasive MRI thermometry with the proton reso-nance frequency (PRF) method: in vivo results in humanmuscle. Magn Reson Med 1995;33:74–81.
22. Kuroda K, Oshio K, Chung AH, et al. Temperaturemapping using the proton chemical shift: a chemicalshift selective phase mapping method. Magn Reson Med1997;38:845–51.
23. Kuroda K, Oshio K, Chung AH, Hynynen K, Jolesz FA.Temperature mapping using the water proton chemicalshift: a chemical shift selective phase mapping method.Magn Reson Med 1997;38:845–51.
24. Fried MP, Morrison PR, Hushek SG, Kernahan GA,Jolesz FA. Dynamic T1-weighted magnetic resonanceimaging of interstitial laser photocoagulation in theliver: observations on in vivo temperature sensitivity.Lasers Surg Med 1996;18:410–19.
25. Young IR, Hand JW, Oatridge A, et al. Modeling andobservation of temperature changes in vivo using MRI.Magn Reson Med 1994;32:358–69.
26. Gellermann J, Wlodarczyk W, Feussner A, et al.Methods and potentials of MR-tomograph to monitor-ing radiofrequency hyperthermia in a hybrid system. IntJ Hyperthermia. In press 2005.
27. De Poorter J, De Wagter C, De Deene Y, et al. Theproton-resonance-frequency-shift method comparedwith molecular diffusion for quantitative measurementof two-dimensional time-dependent temperature distri-bution in a phantom. J Magn Reson 1994;B103:234–41.
Regional Hyperthermia under MR Monitoring
www.aacrjournals.org 5879 Cancer Res 2005; 65: (13). July 1, 2005
Cancer Research. on September 20, 2020. © 2005 American Association forcancerres.aacrjournals.org Downloaded from

28. Peters RD, Hinks RS, Henkelmann RM. Ex vivotissue-type independence in proton-resonance fre-quency shift MR thermometry. Magn Reson Med 1998;40:454–9.
29. Quesson B, de Zwart JA, Moonen CTW. Magneticresonance temperature imaging for guidance of ther-motherapy. J Magn Reson Imaging 2000;12:525–33.
30. Young IR, Hajnal JV, Roberts IG, et al. An evaluationof the effects of susceptibility changes on the waterchemical shift method of temperature measurement inhuman peripheral muscle. Magn Reson Med 1996;36:366–74.
31. Wlodarczyk W, Boroschewski R, Hentschel M, et al.Fast 3D monitoring of small temperature changes forhyperthermia using magnetic resonance. Magn ResonImaging 1998;8:165–74.
32. Wlodarczyk W, Hentschel M, Wust P, et al.Comparison of magnetic resonance methods for map-ping of small temperature changes. Phys Med Biol1999;44:607–24.
33. Vogl TJ, Weinhold N, Mack MG, et al. Verification ofMR thermometry by means of an in vivo intralesion,fluoroptic temperature measurement for laser-inducedthermotherapy of liver metastases. RoFo Fortschr GebRontgenstr Neuen Bildgeb Verf 1998;169:182–8.
34. Carter DL, MacFall JR, Clegg ST, et al. Magneticresonance thermometry during hyperthermia for hu-man high-grade sarcoma. Int J Radiat Oncol Biol Phys1998;40:815–22.
35. Peller M, Loffler R, Baur A, et al. MRT-gesteuerteregionale Tiefenhyperthermie. Radiologe 1999;39:756–63.
36. Peller M, Reinl HM, Weigel A, et al. T1 relaxation timeat 0.2 Tesla for monitoring regional hyperthermia:feasibility study in muscle and adipose tissue. MagnReson Med 2002;47:1194–201.
37. Wust P, Gellermann J, Seebass M, et al. Teilkorper-hyperthermie mit einem radiofrequenz-multiantennen-applikator unter on-line kontrolle in einem 1,5 TMR-tomographen. Fortschr Rontgenstr 2004;176:363–74.
38. Gellermann J, Wlodarczyk W, Ganter H, et al. Apractical approach to perform the thermography in ahyperthermia/MR hybrid system—validation in ananthropomorphous phantom. Int J Radiat Oncol BiolPhys 2005;61:267–77.
39. Hildebrandt B, Wust P, Drager J, et al. Regional pelvichyperthermia as an adjunct to chemotherapy (oxalipla-tin, folinic acid, 5-fluorouracil) in pre-irradiated patientswith locally recurrent rectal cancer—a pilot study. Int JHyperthermia 2004:20:359–69.
40. Wust P, Fahling H, Helzel T, et al. Design and test ofmulti-amplifier systems with phase and amplitudecontrol. Int J Hyperthermia 1998;14:459–77.
41. Tilly W, Wust P, Rau B, et al. Temperature data andspecific absorption rates in pelvic tumours: predictivefactors and correlations. Int J Hyperthermia 2001;17:172–88.
42. Wust P, Stahl H, Loffel J, Seebass M, Riess H, Felix R.Clinical, physiological and anatomical determinants for
radiofrequency hyperthermia. Int J Hyperthermia 1995;11:151–67.
43. Van der Zee J, Peer-Valstar JN, Rietveld PJ, de Graaf-Strukowksa L, van Rhoon GC. Practical limitations ofinterstitial thermometry during deep hyperthermia.Int J Radiat Oncol Biol Phys 1998;40:1205–12.
44. Sneed PK, Dewhirst MW, Samulski T, Blivin J,Prosnitz LR. Should interstitial thermometry be usedfor deep hyperthermia. Int J Radiat Oncol Biol Phys1998;40:1015–7.
45. Issels R, Prenninger SW, Nagele A, et al. Ifosfamideplus etoposide combined with regional hyperthermia inpatients with locally advanced sarcomas: a phase IIstudy. J Clin Oncol 1990;8:1818–29.
46. Tilly W, Gellermann J, Graf R, et al. Regionalhyperthermia in conjunction with definitive radiother-apy against recurrent or locally advanced prostatecancer T3 pN0 M0. Strahlenther Onkol 2005;181:35–41.
47. Wust P, Nadobny J, Seebass M, et al. Influence of pa-tient models and numerical methods on predicted powerdeposition patterns. Int J Hyperthermia 1999;15:519–40.
48. Le Bihan D, Breton E, Lallemand D, Aubin M-L,Vignaud J, Laval-Jeantet M. Separation of diffusion andperfusion in intravoxel incoherent motion MR imaging.Radiology 1988;168:497–505.
49. Peller M, Kurze V, Loeffler R, et al. Hyperthermiainduces T1 relaxation and blood flow changes intumors. A MRI thermometry study in vivo . Magn ResonImaging 2003;21:545–51.
Cancer Research
Cancer Res 2005; 65: (13). July 1, 2005 5880 www.aacrjournals.org
Cancer Research. on September 20, 2020. © 2005 American Association forcancerres.aacrjournals.org Downloaded from

2005;65:5872-5880. Cancer Res Johanna Gellermann, Waldemar Wlodarczyk, Bert Hildebrandt, et al. Recurrent Rectal Carcinoma in a 1.5 Tesla Hybrid SystemNoninvasive Magnetic Resonance Thermography of
Updated version
http://cancerres.aacrjournals.org/content/65/13/5872
Access the most recent version of this article at:
Cited articles
http://cancerres.aacrjournals.org/content/65/13/5872.full#ref-list-1
This article cites 46 articles, 1 of which you can access for free at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://cancerres.aacrjournals.org/content/65/13/5872To request permission to re-use all or part of this article, use this link
Cancer Research. on September 20, 2020. © 2005 American Association forcancerres.aacrjournals.org Downloaded from