Upload
others
View
4
Download
0
Embed Size (px)
Citation preview
Nonenhanced MR Angiography1
Mitsue Miyazaki, PhDVivian S. Lee, MD, PhD While nonenhanced magnetic resonance (MR) an-giographic methods have been available since theearliest days of MR imaging, prolonged acquisition
times and image artifacts have generally limited their usein favor of gadolinium-enhanced MR angiographic tech-niques. However, the combination of recent technical ad-vances and new concerns about the safety of gadolinium-based contrast agents has spurred a resurgence of interestin methods that do not require exogenous contrast mate-rial. After a review of basic considerations in vascularimaging, the established methods for nonenhanced MRangiographic techniques, such as time of flight and phasecontrast, are considered and their advantages and disad-vantages are discussed. This article then focuses on newtechniques that are becoming commercially available, suchas electrocardiographically gated partial-Fourier fast spin-echo methods and balanced steady-state free precessionimaging both with and without arterial spin labeling. Chal-lenges facing these methods and possible solutions areconsidered. Since different imaging techniques rely on dif-ferent mechanisms of image contrast, recommendationsare offered for which strategies may work best for specificangiographic applications. Developments on the horizoninclude techniques that provide time-resolved imaging forassessment of flow dynamics by using nonenhanced ap-proaches.
� RSNA, 2008
1 From the Department of MRI, Toshiba Medical ResearchInstitute USA, 990 Corporate Woods Pkwy, Vernon Hills,IL 60061 (M.M.); and Department of Radiology, New YorkUniversity Medical Center, New York, NY (V.S.L.). Re-ceived August 24, 2007; revision requested November 7;revision received November 30; accepted January 29,2008; final version accepted February 21. Address cor-respondence to M.M. (e-mail: [email protected] ).
V.S.L., who is not an employee of or consultant toToshiba, had control of inclusion of any data andinformation that might present a conflict of interest forM.M., who is an employee of Toshiba.
� RSNA, 2008
REVI
EWS
AND
COM
MEN
TARY
�ST
ATE
OFTH
EAR
T
20 Radiology: Volume 248: Number 1—July 2008
Note: This copy is for your personal non-commercial use only. To order presentation-ready copies for distribution to your colleagues or clients, contact us at www.rsna.org/rsnarights.
Magnetic resonance (MR) angio-graphic techniques can be di-vided into two categories: con-trast material–enhanced and nonenhancedMR angiography. Since its introduction in1994 by Prince (1), first-pass contrast-enhanced MR angiography with gadolin-ium-based contrast material has seenwidespread acceptance. The approachhas benefited from many technical ad-vances, including strategies to synchro-nize arrival of the bolus of contrast ma-terial with MR acquisition (2–4), mov-ing bed technology for multistationstudies such as peripheral MR angiogra-phy (5,6), shortened acquisition timeswith parallel imaging (7), and k-spacesharing methods such as time-resolvedimaging of contrast kinetics, or TRICKS,
for “time-resolved” MR angiographic ac-quisitions (8).
Among the nonenhanced techniquesthat have been available for many years,three-dimensional (3D) time-of-flight(TOF) MR angiography remains themainstay of intracranial arterial evalua-tion. For peripheral MR angiography,flow is oriented craniocaudally, and two-dimensional (2D) TOF has been estab-lished as an accurate method to diagnoseperipheral vascular disease. However,long acquisition times are needed to im-age from the abdominal aorta to pedalarteries with transverse sections. The re-quirement for section positioning orthog-onal to the direction of flow has precludedapplication of TOF methods in areas ofcomplex geometry such as the thoracicaorta or renal arteries. Phase-contrastimaging is less commonly used to produceangiographic images because of its rela-tively long acquisition times (9–12). Untilrecently, other nonenhanced methods,such as arterial spin labeling (ASL) (13–15), have been confined to research ap-plications.
Several factors contribute to a renais-sance of interest in nonenhanced MR an-giographic methods. Improvements inMR hardware and software, including thewidespread availability of parallel imaging(16,17), have helped reduce acquisitiontimes and made some methods clinicallypractical. Moreover, the recent associa-tion between high doses of gadolinium-based contrast material for MR angiogra-phy and the debilitating and occasionallylife-threatening entity, nephrogenic sys-temic fibrosis (18–20), originally knownas nephrogenic fibrosing dermopathy,has made it imperative that patients withmoderate to severe renal insufficiencyand vascular disease have nonen-hanced alternatives for angiography.Much of the research on nonenhancedMR angiographic techniques origi-nates in Japan, driven by the relativelyhigh costs and limitations on dosing ofcontrast material there (21). It is alsoimportant to note that nonenhancedMR angiography can play a useful roleas a supplement to gadolinium-en-hanced MR angiography, particularlywhen the contrast-enhanced methodsfail or have serious artifacts (22).
The purpose of this article is to in-form the clinical imager about new hori-zons in the field of nonenhanced MRangiography. The focus is on arterio-graphic applications, reserving venogra-phy for separate consideration. We be-gin by summarizing general principles ofvascular MR imaging, reviewing the es-tablished nonenhanced methods such asTOF and phase-contrast MR angiogra-phy (23), and then discussing in greaterdetail newer strategies for MR angiogra-phy that do not require exogenous con-trast material, concentrating on electro-cardiographically (ECG)-gated partial-Fourier fast spin echo (FSE) and balancedsteady-state free precession (SSFP) (alsoreferred to as balanced fast field echo;true fast imaging with steady-state pre-cession, or true FISP; fast imaging em-ploying steady-state acquisition, or FIESTA;true SSFP; among others) with ASL. Fi-nally, the article concludes with a sum-mary of possible strategies for nonen-hanced alternatives in specific MR an-giographic applications and considerationof future directions.
Summary of General Principles ofVascular MR Imaging
Prior to discussing nonenhanced MRangiographic methods, some relevantunderlying principles governing angio-graphic imaging are reviewed.
Arterial and Venous Flow PatternsPeak systolic flow in arterial vessels typ-ically occurs 150–200 msec followingthe R wave of ECG tracings. The delaybetween peak systolic flow and ventric-ular contraction lengthens as the pulse
Published online10.1148/radiol.2481071497
Radiology 2008; 248:20–43
Abbreviations:ASL � arterial spin labelingECG � electrocardiographyFSE � fast spin echoMIP � maximum intensity projectionSSFP � steady-state free precession3D � three-dimensionalTOF � time of flight2D � two-dimensional
Essentials
� Improvements in MR hardwareand software, coupled with con-cerns about the safety of gado-linium-based contrast agents,have contributed to a renaissanceof interest in nonenhanced MRangiography.
� Time-of-flight MR is widely usedfor intracranial angiography and,in some centers, for carotid anddistal peripheral MR angiography.
� Electrocardiographically (ECG)-gated 3D partial-Fourier fast spin-echo (FSE) methods rely on sub-traction of systolic from diastolicacquisitions for angiography andare particularly well suited to pe-ripheral MR angiographic applica-tions.
� Balanced steady-state free preces-sion (SSFP) without arterial spinlabeling (ASL) can be performedwith ECG gating for thoracic aor-tic MR angiography and with bothECG gating and navigator-gatedfree breathing for whole-heartcoronary artery MR angiography.
� ASL with either balanced SSFP orpartial-Fourier FSE relies on spintagging to generate image con-trast and can be used in a varietyof applications, including pulmo-nary, carotid, renal, and distalperipheral MR angiography.
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
Radiology: Volume 248: Number 1—July 2008 21
wave moves distally toward the extrem-ities because of the compliance of thearterial structures (24,25). While peaksystolic velocity ranges from 70 to 100cm/sec in the abdominal aorta, it is usu-ally much lower in the peripheral ves-sels, ranging from 30 to 50 cm/sec in thefemoral artery compared with 10–20cm/sec in the dorsalis pedis (26). Thepulse waveform varies across the vascu-lar system. The reversal of arterial flowdue to diastolic filling of the coronaryarteries can be seen throughout the tho-racic aorta. For other arteries, the ap-pearance of the velocity waveform of anartery depends on vessel wall compli-ance and whether the artery feeds ahigh- or low-resistance structure. Forexample, lower extremity arteries sup-ply high-resistance muscle beds, result-ing in the triphasic appearance of theirvelocity waveforms. The triphasic ap-pearance is dampened in diabetic pa-tients with calcified, attenuated, or ste-notic vessels (25,27). In contrast, ves-sels such as the internal carotid arteryand renal artery that supply low-resis-tance vascular beds have a high forwardflow during diastole. Venous flow doesnot demonstrate pulsatility. Rather, itsslow flow varies with respiration as neg-ative intrathoracic pressure acceleratesvenous return to the chest.
T1 and T2 of Blood Compared with OtherTissuesArterial and venous blood have rela-tively long T1 relaxation times in vivo.The values depend on the oxygenationstatus of the blood. For arterial blood,T1 times of 1200 msec are typicallycited at 1.5 T (28), although exact val-ues depend on hematocrit level, oxygen-ation, and temperature. Venous T1 val-ues do not differ substantially from ar-terial T1 times. T1 values generallyincrease at higher magnetic fieldstrengths. For example, the T1 of brainparenchyma increases by 25%–40% at3 T (29), while on average, T1 relax-ation times are 21% longer for kidneycortex, liver, and spleen (30). T2 relax-ation times depend strongly on oxygen-ation. Arterial blood T2 relaxationtimes at 1.5 T are typically around 250msec (31,32), while venous blood T2
values are shorter, at about 30 msec foran oxygen saturation of 30% (32). Rel-evant to peripheral MR angiographicimaging techniques with T2 weighting,it has been observed that deep veinshave longer T2 times compared withsuperficial veins (33,34).
Key Characteristics and ImagingRequirements across MR AngiographicApplicationsOf the angiographic applications, carotid,peripheral, renal, and coronary MR an-giography exemplify the different chal-lenges of vascular imaging. For carotidMR angiography, the small size of the ves-sels combined with the clinical need todifferentiate between fine grades of ste-nosis demands high spatial resolution onthe order of 1 mm or less. At the sametime, for contrast-enhanced methods,rapid venous enhancement limits the win-dow for venous-free carotid MR angiogra-phy.
For peripheral MR angiography, theextensive anatomic coverage desired—typically at least 80 cm to as much as140 cm from the renal arteries to thetoes—requires efficient imaging tech-niques so that multiple stations can beimaged during a short examination pe-riod. Spatial resolution is particularlyimportant for visualizing small vessels.Patency of pedal arteries may be thedetermining factor for revascularizationversus amputation in patients with limb-threatening ischemia (35,36). The flowpatterns in the peripheral vessels canalso be complex. Both differences inatherosclerotic disease and hyperemiaassociated with foot ulcers can causedifferent rates of enhancement for twoextremities. Retrograde filling of proxi-mally occluded vessels can result in de-layed cephalad flow patterns of somearterial structures. In these settings, dy-namic imaging that provides temporalinformation about arterial flow can beclinically valuable (37). Additionally, theclose proximity of paired veins along-side peripheral arteries can make inter-pretation of MR angiographic findings achallenge unless venous signal is sup-pressed.
For the renal arteries, imaging withcertain nonenhanced techniques can be
particularly challenging because of thedifferent orientations of the renal arter-ies and their branches relative to theaorta and renal artery motion with res-piration. Similar challenges face appli-cations of MR angiography to the tho-racic aorta and subclavian arteries inthe evaluation of thoracic outlet syn-drome or in upper-extremity MR an-giography. Spatial resolution demandsfor renal MR angiography are also high,particularly for evaluation of possible fi-bromuscular dysplasia or other branch-vessel disease. Like for carotid arteries,rapid venous enhancement also re-stricts the window of acquisition forhigh-quality, arterially selective, con-trast-enhanced MR angiography.
Figure 1
Figure 1: Schematic of TOF MR angiographicprinciples. Stationary protons exposed to repeatedradiofrequency excitation pulses lose signal be-cause of saturation. Arrival of fresh protons resultsin increased signal intensity, particularly whenthere is complete replacement of protons in thesection between each excitation pulse. Mz � mag-netization, TR � repetition time.
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
22 Radiology: Volume 248: Number 1—July 2008
Finally, for the coronary arteries,minimizing motion artifacts requires ac-quisition during a limited period of thecardiac and respiratory cycles. High im-age contrast for the visibility of the cor-onary arteries requires suppression of
myocardial tissue and coronary venoussignal. Moreover, high spatial resolu-tion is critical to resolving clinically im-portant differences between mild, mod-erate, and severe stenoses.
TOF MR Angiographic Techniques
The most commonly used nonenhancedMR angiographic technique has beenTOF imaging (38–42), developed in thelate 1980s. TOF angiography relies onthe differences in exposure to radiofre-quency excitation between in-plane orin-slab stationary protons and the bloodprotons flowing into the section or slab(Fig 1). Stationary protons in the imag-ing section become relatively saturatedwith repeated excitation pulses and pro-duce low signal intensity. Inflowingblood protons in arteries and veins havenot experienced the excitation pulses,are not saturated, and therefore gener-ate high signal intensity. For selectiveimaging of arteries, saturation bandsare applied on the venous side of imag-ing sections to null signal from the ve-nous flow. Flow-compensation gradi-ents, consisting of additional positive-and negative-lobed gradients applied inone or more directions, reduce flow-related dephasing.
The contrast between inflowing ar-teries and background tissue in TOFMR angiography depends on certain im-aging parameters. Longer repetitiontimes allow for inflow of arterial pro-tons, but at the expense of increasedimaging times. With thinner sections,shorter repetition times can be used,although the gain in time with shorterrepetition time is offset by the need toimage more sections for the same ana-tomic coverage; typically repetition timesfor 2D imaging range from 25 to 50msec. The higher the flip angle thegreater the suppression of backgroundtissue and the greater the signal fromthe fully magnetized inflowing arterialprotons, provided flow is sufficientlyfast for all spins to be completely re-placed in a section with each excitation.Flip angles can vary from 25° to 60°,depending on the application.
Acquisitions can be performed byusing 2D or 3D methods, dependingon the spatial resolution and the ex-tent of the vascular territory to be im-aged. Today, the most common clini-cal application of TOF angiography isthe examination of intracranial vessels(38,39), for which 3D methods arepreferable to achieve high-spatial-resolution isotropic imaging (Fig 2). Incontrast, for peripheral MR angiogra-phy, the extensive anatomic coveragedesired makes 3D imaging impracti-cal. In clinical practice, 2D TOF an-giography is still used for evaluation oftibial and pedal arteries and has beenshown to be as accurate as conven-tional angiography for the diagnosis ofstenosis and occlusion in multicenterstudies (43–46) (Fig 3).
Limitations of TOF imaging includethe saturation of protons in vesselswithin the imaging section or slab, par-ticularly in 3D imaging, in general, or in2D imaging, where flow lies within theplane of imaging. Improvements to en-hance inflow effects in intracranial 3DTOF include tilted optimized nonsat-urating excitation, or TONE (47), whichuses progressively increasing flip anglesthrough the slab to compensate for sat-uration of blood flowing in the slab (Fig2), and multiple overlapping thin slabacquisition, or MOTSA, which repre-
Figure 2
Figure 2: Intracranial 3D TOF imaging in a35-year-old man with a history of headaches.Maximum intensity projection (MIP) demon-strates a pial arteriovenous malformation. Imagingwas performed by using magnetization transferand tilt optimized nonsaturated excitation to im-prove sensitivity to flow. (Image courtesy of Dr E.Knopp, New York University Medical Center.)
Figure 3
Figure 3: (a) Two-dimensional TOF peripheral MR angiography compared with (b) conventional angiog-raphy in a patient with peripheral vascular disease. (a) Sagittal MIP demonstrates patent, reconstituted dorsa-lis pedis (arrow) and correlates well with (b) the lateral view (arrow). Because a is an MIP, overlapping tissuesobscure visualization of the posterior tibial and lateral plantar arteries. On source MR angiograms, both ves-sels are well seen, comparable to digital subtraction angiograms.
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
Radiology: Volume 248: Number 1—July 2008 23
sents a hybrid of 2D and 3D methods(48,49). Application of magnetizationtransfer pulses improves depiction of in-tracranial vessels by further suppress-ing the brain parenchyma signal (47,50,51) on the basis of differences in T2relaxation times between free unboundwater protons (blood) and protonsbound to macromolecules (brain). Itshould also be noted that with TOFmethods, the focus is on flow-dependentluminal imaging. Visualization of thevessel wall is limited, as compared, forexample, to gated FSE images.
In the lower extremities, whereflow varies with the cardiac cycle, im-age contrast on TOF MR angiogramscan be enhanced by systolic gating.Limitations of 2D imaging of the lowerextremities include saturation of in-plane flow, such as at the origin of theanterior tibial arteries on transverseimages, which causes pseudostenosison MR angiograms (Fig 4). Typically,2D TOF imaging for applications suchas carotid and peripheral angiographyis performed by using traveling satu-ration bands to ensure venous nulling.In the extremities, implementationwith a caudal saturation band pre-cludes visualization of vessels that maybe filled in a retrograde manner (Fig5). More generally, with 2D TOF im-aging, sections must be positionedperpendicular to the direction of flow,which can be challenging in imagingthe thoracic aorta or the renal arter-ies. In most cases, 2D TOF imaging ofthe extremities has been supplantedby contrast-enhanced imaging for itsgreater speed, anatomic coverage,and time-resolved capabilities (37).
Phase-Contrast MR AngiographicTechniques
Phase-contrast MR angiography usespairs of bipolar or flow-compensatedand uncompensated gradient pulses togenerate flow-sensitive phase images(9,11,12,52). With phase-contrastMR imaging, phase data are used toreconstruct either velocity-encodedflow-quantification images or MR an-giographic images. For phase-contrastMR angiography, voxel signal intensity
(SI) reflects the absolute velocity ofvoxels (v) and is calculated as:
SI � �vx2 � vy2 � vz2 .
So, by definition, signal intensity is alwayspositive, independent of the direction offlow. To produce MR angiographic im-ages with flow sensitivity in three direc-tions, acquisitions need to be repeatedfour times: one with flow uncompensatedand three with different flow-compensa-tion directions (53). Phase-contrast MRangiography has the advantage of highsensitivity to turbulent flow that can beassociated with vascular stenoses and in-herently low background signal (Fig 6).
For flow quantification, velocity-en-coded images are generated by usingthe net phase shift, computed by sub-tracting the phase shifts generated bythe two (flow-encoded and flow-com-pensated) acquisitions. On velocity-en-coded images, the signal intensity on theimage is directly proportional to thephase shift accumulated, where phaseshift ranges from 180° to �180°. Posi-tive phase shifts appear with increasingbrightness, while negative phase shiftshave increasing darkness. The maxi-mum velocity measurable that corre-sponds to a phase shift of 180° is auser-defined parameter, referred to asencoding velocity, or Venc. For flowquantification applications, where ve-locities exceed the Venc, velocity aliasingwill occur. Phase-contrast MR angiogra-phy is more tolerant to mild velocityaliasing because of the way in which thevoxel signal intensities are calculated.
In the late 1990s, phase-contrast MRangiography demonstrated great promise
Figure 4
Figure 4: In-plane saturation inanterior tibial artery mimics steno-sis at 2D TOF acquisitions in ahealthy volunteer. Bilateral proxi-mal anterior tibial artery narrowing(arrows) seen on (a) 2D TOF im-age is not seen on (b) gadolinium-enhanced MR angiogram.
Figure 5
Figure 5: Retrograde filling of right peronealartery (arrow) on (b) cronal conventional angio-gram is not detected on (a) coronal MIP from 2DTOF MR angiography because with the TOFmethod, a traveling distal saturation band used tosuppress venous signal also inadvertently sup-pressed the retrograde filling peroneal artery. (Re-produced, with permission, from reference 37.)
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
24 Radiology: Volume 248: Number 1—July 2008
in a wide range of applications, includingrenal MR angiography (55–61), periph-eral MR angiography (53,62), and portalvenography (63). For example, coronal
2D phase-contrast MR angiographicmethods for three-station evaluation ofthe lower extremities—aortic bifurca-tion to tibioperoneal trunk—have beenused with an 80-mm-thick section, 3Dflow-encoding with Venc of 30 cm/sec inthe iliac arteries and of 20 cm/sec in thefemoral and popliteal arteries, and twosignals acquired, which resulted in im-aging times of 4–7 minutes per sta-tion, or an overall acquisition time of20–30 minutes. In a study of 115 pa-tients with 253 atherosclerotic le-sions, the sensitivity of phase-contrastMR angiography with this protocolwas 95%, specificity was 90%, posi-tive predictive value was 90%, andnegative predictive value was 96%(53,62).
Although recent technical develop-ments using undersampling methods toshorten acquisition times promise tomake phase-contrast MR angiographymore clinically practical (64,65), therelatively long acquisition times of mostcurrently available phase-contrast MRangiographic sequences preclude their
routine use except for specific applica-tions. Low-spatial-resolution phase-con-trast MR angiography is commonly usedas a scout sequence for extracranial ca-rotid MR angiography. As a supplemen-tal sequence to diffusion- and perfusion-weighted imaging, Liu et al (66) demon-strated the utility of a 2D phase-contrastMR angiographic acquisition for theevaluation of stroke prognosis. Prince etal (61) have advocated the supplemen-tal use of 3D phase-contrast MR angiog-raphy to distinguish between mild andmoderate or severe renal artery steno-sis (Fig 6). Iseda et al (67) used 3Dphase-contrast MR angiography simi-larly to help characterize physiologicallysignificant carotid artery stenoses. As asupplement to MR angiographic meth-ods, flow quantification with 2D phase-contrast imaging, an application distinctfrom MR angiography, is potentiallyvaluable for estimating flow and pres-sure gradients across stenoses in thecarotid arteries (68), peripheral arter-ies (69,70), and renal arteries (71–77),as well as supplementing MR angio-
Figure 6
Figure 6: (a) Axial 3D phase-contrast imagedepicts bright signal in the initial part of the left renalartery stenosis, where flow is accelerating, and thereis complete signal dropout beginning at the mostsevere part of the stenosis and extending for 1 cmdistally (arrow). (b, c) Corresponding 3D gadolini-um-enhanced MR angiograms in (b) coronal and(c) transverse views show a widely patent aorto–bi-iliac graft and severe left renal artery stenosis (arrow).The signal dropout from spin dephasing in a indi-cates there is a pressure gradient across the stenosis.(Modified, with permission, from reference 54.)
Figure 7
Figure 7: Three-dimensional partial-Fourier FSE imaging with systolic and diastolic acquisition. Eachsection (S1, S2, . . . Sn) is imaged in one single-shot acquisition. One trigger delay (d1) is timed for systole forone 3D acquisition, while a second delay (d2) is timed for diastole. Acquisitions are performed every other orevery third heartbeat. A short tau inversion-recovery (STIR) pulse can be used for improved fat suppres-sion. To generate a bright-blood angiogram, systolic images (where arterial flow appears dark) are sub-tracted from diastolic images. A � arteries, RF � radiofrequency, V � veins. (Modified, with permis-sion, from reference 85.)
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
Radiology: Volume 248: Number 1—July 2008 25
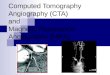
Figure 8
Figure 8: ECG preparatory scan to determine appropriate ECG delay time for systolic and diastolic triggering times; scan is performed prior to 3D acquisition. (a)Sequence diagram shows repeated 2D single-shot partial-Fourier acquisitions (Acq), each acquired with progressively longer trigger delay times (D1, D2, . . . D5) follow-ing the R-wave of the ECG tracing. (b) Single-shot images from selected delay times show typical results of ECG preparatory scan. For pulmonary angiography in thisexample, a systolic trigger of around 200 msec would result in desired flow void, and diastolic triggering gives bright-blood images at a delay of 700 msec. RF � radio-frequency, STIR � short tau inversion recovery. (Modified, with permission, from reference 85.)
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
26 Radiology: Volume 248: Number 1—July 2008
graphic evaluation such as in thoracicdissection (78) and coarctation (79),subclavian steal syndrome, intracranialischemia (80), central pulmonary arter-ies (81), and intracranial vascular mal-formations (82).
ECG-gated 3D Partial-Fourier FSESequence
One of the two newer methods that isdemonstrating promise for clinical use asa nonenhanced MR angiography tech-nique was first described in principle inthe 1980s by Wedeen et al (83) and Meuliet al (84) using an ECG-gated spin-echosequence. Recent improvements in theapproach, including use of single-shotpartial-Fourier FSE sequences (also re-ferred to as single-shot FSE, half-Fourierrapid acquisition with relaxation en-hancement, or fast asymmetric FSE) haveshortened the acquisition times and havemade this method clinically feasible onmodern MR systems, with resulting earlycommercial availability on some systems(85,86). In this section, we introduce thereader to the principles of this up-and-coming technique in some detail, discussapplications, and consider its limitations.
Principles of the TechniqueThis nonenhanced MR angiographic tech-nique relies on an ECG-gated 3D partial-Fourier FSE sequence, which is trig-gered for systolic and diastolic acquisi-
tions. The method relies on loss ofsignal, or flow void, as a result of fastarterial flow during systole. In contrast,during diastole, the slow flow in arteriescauses them to have high signal inten-sity on T2-weighted images. Because ofits relatively slow flow, venous blood isbright during both systole and diastole.Bright-blood MR angiography is thenachieved by subtracting systolic from di-astolic images (Fig 7). Interestingly, asimilar nonenhanced approach for MRangiography can also be achieved withgradient-echo imaging by using ECGgating and uncompensated gradients toaccentuate flow voids during systole andflow-compensated gradients to increasesignal in arteries during diastole (87).However, longer acquisition times forcomparable spatial resolution limit ap-plication of this method compared withFSE approaches.
Synchronization with the cardiac cy-cle can be achieved with ECG gating orperipheral pulse wave gating. To keepacquisition times reasonable, the 3D se-quence is typically implemented witheach partition acquired in a single shot(Fig 7). To allow sufficient T1 recovery,the repetition time for these gated ac-quisitions is typically every two to threeheartbeats (R-R intervals). The trigger-ing time is the same for all partitions.The acquisition time for each 3D imagedepends on the number of partitions orsections and is typically 90 seconds to 3minutes. Performance of the systolicand diastolic 3D acquisitions continu-ously and without interruption mini-mizes misregistration and motion arti-facts on subtracted images for anoverall acquisition times of about 3–6 min-utes. Concepts essential to successfulbright-blood MR angiographic images withthis technique are discussed next (85,86).
First, a T2 blurring effect in thephase-encoding direction at FSE-typesequences is related to the sampling ofmultiple echoes at different echo times(88). If the vessels are oriented perpen-dicular to the phase-encoding direction,as in peripheral MR angiography, theT2-blurring effect results in undesirablevessel blurring artifacts.
Second, to maximize differences be-tween systolic and diastolic images, re-
Figure 9
Figure 9: Spoiler gradients, representing ex-tended applications of gradients to dephase mag-netization, in the readout direction. Original �readout gradient in conventional partial-FourierFSE implementation. Spoiler � readout gradientwith additional spoiler gradients to improve sensi-tivity to slow flow in the readout direction in 3DECG-gated partial-Fourier FSE MR angiography. Ifthe signal difference between diastolic and systolicflow is small, strong spoiler gradients (larger grayareas) are applied. RF � radiofrequency. (Modi-fied, with permission, from reference 86.)
Figure 10
Figure 10: Nonenhanced MR angiography of the aorta in 32-year-old female volunteer with 3D ECG-gatedpartial-Fourier FSE (repetition time/effective echo time msec, four R-R intervals/30; 180° flip angle). (a)Source image and (b) MIP of diastolically triggered images obtained by using a trigger delay of 600 msec andecho train length of 67 in two separate shots, which resulted in 335-msec acquisition window per shot. Eight3-mm sections were acquired and interpolated to 16 1.5-mm sections. Phase-encoding directions werecraniocaudal and anteroposterior. Total scan time was about 3 minutes with an intermittent breathhold tech-nique. (Image courtesy of J. Urata, Saiseikai Kumamoto Hospital, Japan.)
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
Radiology: Volume 248: Number 1—July 2008 27
duce T2 blurring, and minimize motion-related artifacts, the total data samplingduration during each heartbeat shouldbe as short as possible. If each partitionis acquired in a single shot, a short in-terecho train spacing is desirable. Forexample, if the echo train length is 70with parallel imaging, an interecho trainspacing of 5 msec results in an acquisi-tion time of 350 msec per heartbeat.Although this time exceeds the typicalduration of systolic flow, the careful de-termination of a triggering time for peaksystolic flow, combined with use of cen-tric reordering, can help to preserve thedesired flow voids with a single-shotFSE sequence. Alternatively, data foreach partition can be collected in twoshots, which results in sharper imagesby reducing the data sampling windowtime. However, the scan time will dou-ble that of a single-shot method. Appli-cation of parallel imaging has allowedshorter data sampling periods, with ad-vantages of more precise imaging dur-ing systole and reduced T2 blurring.
Third, with a rectilinear k-space fill-ing, centric ordering results in intrinsi-cally less flow dephasing in the phase-en-coding direction compared with the read-out direction (89). As discussed in moredetail below, depending on the applica-tion, the orientation of the readout or fre-quency-encoding direction relative to thevessels of interest can be selected to opti-mize arterial signal. For the relativelyslower moving protons in the peripheralarteries, the readout direction can be ori-ented in the direction of flow and flow-spoiling gradient pulses can be applied inthe readout direction to increase the flow-dephasing effect during systole. Flow-spoiling gradient pulses accentuate thedifferences in signal between systolic anddiastolic phases without affecting slowerflowing venous blood and the stationarybackground signals.
Last, additional prepulses can beused in conjunction with the 3D partial-Fourier FSE method to achieve differenttypes of image contrast. For example,use of a short tau inversion-recoverymethod can be used to achieve fat-sup-pressed images (85,86).
Before performance of systolic anddiastolic 3D ECG-gated partial-Fourier
FSE acquisitions, one or two additionalpreparatory steps can be helpful. First,an “ECG-prep scan” that produces 2Dimages at incremental triggering timesof arbitrary steps can be used to find thetrigger delay for systole, when arteriesare black blood (flow voids), and dias-tole, when arteries are bright (85)(Fig 8). A second 2D preparatory scancan determine the amount of flow-spoiling gradient pulses that cause thebest selective dephasing of the arteriesof interest, particularly in slow-flowingarteries. The operator uses these pre-
paratory scans to define parameters forthe 3D acquisition (86) (Fig 9).
Applications of 3D ECG-gated FSESpecific aspects of the implementation of3D ECG-gated FSE images vary with theapplication. Imaging of the thoracic aortaand the peripheral arteries are consid-ered next. Application of a partial-FourierFSE technique for carotid MR angiogra-phy can be challenging because venoussignal can appear on subtracted imagesdue to the relatively fast flow of the jugu-lar veins. For renal MR angiography, the
Figure 11
Figure 11: Nonenhanced and contrast material– enhanced MR angiography in 58-year-old man with typeB aortic dissection. (a) Conventional nonenhanced black-blood ECG-triggered FSE image (three R-R inter-vals/80, 180° flip angle) with a double inversion recovery FSE sequence (inversion time, 550 msec), (b)source image, and (c) MIP image from nonenhanced 3D ECG-gated FSE (four R-R intervals/30, 180° flipangle); and (d) source image and (e) MIP image from contrast-enhanced 3D MR angiography show a throm-bosed false lumen and an ulcer-like projection (arrowhead). Areas of high signal intensity are observed in thefalse lumen in b (arrow), suggesting stagnant fluid collection not communicating with the true lumen. Withnonenhanced methods, mural abnormality is not well depicted on subtracted images; source images must beviewed to evaluate the vessel wall. (Modified, with permission, from reference 21.) (Image a courtesy of J.Urata, Saiseikai Kumamoto Hospital, Japan.)
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
28 Radiology: Volume 248: Number 1—July 2008
orthogonal directions of flow in the aortaand renal arteries present challenges forthe FSE method. Therefore, for nonen-hanced carotid and renal MR angio-
graphic acquisitions, balanced SSFP withASL may be preferable (see below).
Thoracic aorta.—The fast-flowingblood in the thoracic aorta consistently
produces a flow void (black blood) dur-ing systole and a high signal (brightblood) during diastole (85). For the tho-racic aorta, the phase-encoding direc-tion should be oriented parallel to thedirection of flow (craniocaudal) with theapplication of presaturation bands supe-rior and interior to avoid wraparoundartifacts. Also, since venous enhance-ment is not seriously detrimental to im-age quality, these acquisitions can beperformed with a single diastolic acqui-sition.
Typical nonenhanced MR imagesof the aortic arch by using gated 3DFSE methods are presented in Figure10. In a prospective study of 75 pa-tients referred for thoracic aortic MRangiography (34 with dissection, 27with aneurysm, four with arterial oc-clusion, 10 with surgical bypass), im-age quality of the nonenhanced imageswas excellent in 45, satisfactory in 25,and poor in five patients. In all 34cases of dissection, the intimal flapwas consistently visualized (21). Fig-ure 11 compares three methods:black-blood partial-Fourier FSE, non-enhanced 3D ECG-gated FSE, and ga-dolinium-enhanced MR angiography ina patient with a type B aortic dissec-tion.
Peripheral MR angiography with flowspoiling and flow compensation.—Un-like thoracic aortic applications, the fre-quency encoding or readout gradient forperipheral MR angiography is orientedin the direction of flow to improve sys-tolic flow spoiling. Additional readoutgradient pulses can be added to provideflow spoiling or flow compensation asneeded for optimal systolic flow void im-aging (86).
Figure 12 shows typical diastolic-and systolic-triggered images and theresulting arteriogram generated by sub-traction of systolic images from diastolicimages. In this case, flow spoiling of�10% (or partial-flow compensation)was used in the iliac to thigh region tocompensate for the fast flow of blood.Vessels with slower flowing blood suchas the calf (Figs 13, 14), pedal (Fig 15),and hand (Fig 16) arteries are usuallyimaged with this approach by usingstronger flow-spoiling pulses to differen-
Figure 12
Figure 12: Nonenhanced MR angiography of the pelvis and thighs in a 34-year-old healthy male volunteerwith 3D ECG-gated partial-Fourier FSE. (a) Diastolic and (b) systolic-triggered images are subtracted to pro-duce (c) MR angiogram (MIP). Flow spoiling of �10% (or partial-flow compensation) was used in the read-out (craniocaudal) direction to compensate for the fast flow of blood.
Figure 13
Figure 13: Peripheral MR angiography in a patient with claudication. (a) Nonenhanced 3D ECG-gatedpartial-Fourier FSE acquisition and (b) gadolinium-enhanced MR angiogram with a time-resolved approachto achieve optimal arterial enhancement. Both images show bilateral severe disease of the calf arteries. Fre-quency-encoding (FE ) direction is craniocaudal. (Image courtesy of R. Lim, New York University MedicalCenter.)
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
Radiology: Volume 248: Number 1—July 2008 29
tiate systolic arterial signal from dia-stolic signal.
To date, of the three studies (90–92)evaluating flow-spoiled ECG-gated 3DFSE for peripheral MR angiography inclinical subjects, two have been publishedonly in abstract form. Although prelimi-nary, these results reflect a range of expe-riences with the 3D FSE method. Intheir initial clinical study in 2002, Urataet al (90) found that the ECG-gated FSEmethod was comparable to gadolinium-enhanced MR angiography in 24 of 44regions, while 15 were inferior and fivewere superior when tested in a total of56 regions (18 iliac, 20 femoral, and 18calf area) in 26 patients diagnosed tohave or suspected of having arterial oc-clusive disease. To avoid overestimationof stenoses, the investigators in thisstudy (90) suggested that diastolic im-ages, which depict both arteries andveins, always be evaluated in addition tosubtracted MIP images. Nakamura et al(92) used a similar strategy in theirstudy of 13 patients with 56 diseasedsegments and compared MR angiogra-phy with 16-detector computed tomo-graphic (CT) angiography; they foundthat the MR method resulted in a sensi-tivity of 94%, a specificity of 94%, andan accuracy of 94% for the detection of50% or greater stenosis (Fig 17).
In a separate study, Lim et al (91)compared the nonenhanced method inthe distal station (calf and pedal arteries)with conventional bolus-chase imagingand 3D time-resolved contrast-enhancedMR imaging in 36 patients, where the ref-erence standard was a combined consen-sus interpretation of all three sequences.When all subjects were studied, the non-contrast technique demonstrated accu-racy of 79.4% (1083 of 1364), sensitivityof 85.4% (437 of 512), and specificity of75.8% (646 of 852), with a high negativepredictive value of 92.3% (646 of 700).Serious artifacts lead to poor diagnosticconfidence in 17 patients (47.2%). Amongpatients with satisfactory diagnostic confi-dence, accuracy, sensitivity, and negativepredictive value were 92.2% (661 of 717),92.4% (158 of 171), and 97.5 (503 of 516),respectively (Figs 13, 14). One limitation ofthe study was that only the subtracted MIPimages were evaluated.
Figure 14
Figure 14: MIP from calf MR angiography in 79-year-old man with left leg claudication. Left: ECG-gatedFSE image (two R-R intervals/49, 101° flip angle) shows severely diseased left popliteal artery (solid arrow)with distal occlusion; proximal occlusion of trifurcation vessels, including the posterior tibial artery (solidarrowhead); and severe stenosis of proximal anterior tibial artery (open arrowhead). Collateral supply to bothanterior and posterior tibial arteries (open arrows) and clear depiction of focal stenoses of right proximal ante-rior tibial artery and left mid anterior tibial artery (thin solid arrow) are noted. Right: Gadolinium-enhanced MRangiogram confirms findings. (Image courtesy of R. Lim, New York University Medical Center.)
Figure 15
Figure 15: Digital arterial MIP in a 37-year-old healthy male volunteer. Foot images acquired in a proneposition by using a quadrature knee coil. Nonenhanced MR angiogram with 3D ECG-gated partial-FourierFSE (three R-R intervals/30, 180° flip angle, 192 � 192 matrix interpolated to 384 � 384). For slower flow ofthe arteries of the feet, stronger flow-spoiling pulses, 35% in this case, are used to differentiate systolic arterialsignal from diastolic signal. (Image courtesy of I. Fujita, Saitama City Hospital, Japan.)
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
30 Radiology: Volume 248: Number 1—July 2008
Clearly, additional data in patientswith peripheral artery disease are neededto evaluate the practical use of this tech-nique in the clinical setting.
LimitationsThe ECG-gated 3D FSE method has theadvantage of not requiring intravenouscontrast material. Disadvantages includethe longer scan times compared withthose of contrast-enhanced methods. Foreach acquisition, the nonenhancedmethod requires 1–3 minutes, comparedwith the contrast-enhanced 3D gradient-echo sequences that require only 15–25seconds. As will be discussed in FutureDirections, the implementation of parallelimaging will shorten acquisition times andimprove image quality. Another limita-tion of this method is that on subtractionimages, vessel wall abnormalities can bemissed. Review of source images is neces-sary to visualize abnormalities such as in-tramural hematoma and aortic dissec-tions with slow flow.
The most important technical chal-lenge limiting the robustness of themethod across patients with varying de-grees of disease is imperfect timing ofthe triggered acquisitions. Inappropri-ate selection of the systolic trigger delayleads to suboptimal flow voids on sys-tolic images and resulting overestima-tion of stenosis and underestimation ofvessel length on subtracted datasets.This problem is exacerbated by relianceon subtraction images for evaluation ofstenosis. Two other technical issues in-clude improving sensitivity to vesselswith varying flow patterns, particularly
distal to a stenosis, or in collateralvessels. Additionally, the relatively longsampling window during each cardiaccycle (typically 325 msec per partitionwithout parallel imaging) results in de-graded image quality due to motionartifacts and blurring. Higher parallelimaging factors, particularly at highermagnetic field strengths, may helpovercome these problems by reducingthe number of echoes per partitionand consequently reducing vessel blur-ring by reducing T2-blurring effectsand minimizing motion-related arti-facts. Finally, patients with arrhyth-
Figure 16
Figure 16: Nonenhanced MR angiogram of thehands and forearms in a healthy volunteer with 3DECG-gated partial-Fourier FSE. Additional flowspoiling was used to achieve sensitivity to slowerflowing arteries in the hand. (Image courtesy ofJian Xu, Siemens and New York University Medi-cal Center.)
Figure 17
Figure 17: Comparison of three-station nonenhanced MR angiography with 16-detector CT angiographyin a 64-year-old male patient with bilateral atherosclerotic disease. (a) ECG-gated 3D partial-Fourier FSE MRangiogram obtained for three stations by using flow-spoiling pulses of 0, �5%, and �10% in iliac, femoral,and calf regions, respectively. Note the depiction of collateral vessels achieved with parallel imaging and reso-lution of 256 � 256 matrix interpolated to 512 � 512 (three R-R intervals/80, 160° flip angle, parallel factorof two, 4-mm section thickness and 2 mm after interpolation, and 37 � 37 cm field of view) and (b) contrast-enhanced CT angiogram in the same subject. (Image courtesy of K. Nakamura, Kyoritsu Tobata Hospital,Japan.)
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
Radiology: Volume 248: Number 1—July 2008 31
mias, particularly tachyarrhythmias,can be problematic and may also ben-efit from shorter acquisition windows.
Balanced SSFP without ASL
Principles of TechniqueAlthough initially described by Carr in1958 (93), balanced SSFP sequenceshave enjoyed a recent resurgence of in-terest across a wide range of applica-tions (94). The technique lends itselfwell to angiographic applications be-cause image contrast is determined byT2/T1 ratios, which produce bright-blood imaging without reliance on in-flow. The technique can therefore takeadvantage of recent advances in hard-ware that permit short repetition timesof less than 3–4 msec and with use ofhigh flip angles can produce high-signal-to-noise ratio MR angiographic imagesthat are suitable for parallel imaging.With balanced SSFP, both the arteriesand the veins have high signal intensity,and therefore most MR angiographicapplications utilize additional prepara-tory pulses to selectively enhance arter-ies (see section on coronary arteries be-low). Additionally, with renal MR angio-graphic applications, most methods alsorely on saturation bands over kidneysand inferior vena cava to reduce venoussignal and fat suppression to null theotherwise high signal of fat in these im-ages (95). Brittain et al (96) have re-cently shown that at 3 T, the greatersensitivity to oxygenation differences al-lows for better venous suppression withlonger repetition time for SSFP MR an-giography.
Two main applications of balancedSSFP without ASL MR angiographyhave been gaining acceptance—coro-nary MR angiography and thoracic aor-tic MR angiography.
ApplicationsCoronary MR angiography.—Among themost popular applications of balancedSSFP is its use with coronary MR an-giography (97). Most commonly, 3DSSFP coronary MR angiographic tech-niques have been implemented by us-ing thin slabs and breath-hold acquisi-
tions (97–100), thin-slab navigator-gated acquisitions (99) and, morerecently, whole-heart acquisitionsduring navigator-gated free breathing(101). To improve coronary arteryconspicuity, these sequences are typi-cally implemented by using T2 prepa-ration to suppress myocardial and ve-nous signal (98,102) and fat-suppres-sion pulses. Sakuma et al (101)demonstrated successful completionof MR angiography in 34 of 39 pa-tients, with average imaging times of13.8 minutes � 3.8 (standard devia-tion). In their experience, the overallsensitivity for detecting significant ste-nosis was 82% and specificity was91% (Fig 18). Defining acquisitionwindows during periods of minimalcoronary motion in diastole is criticalto the quality of the resulting images,although a recent study (103) sug-gested that patients with high heartrates may benefit from systolic gating.Sequences can be implemented withCartesian or radial sampling, and re-sults suggest reduced image artifactswith radial methods (102). The highsignal-to-noise ratio of balanced SSFPsequences lends itself well to parallelimaging; a recent study showed feasi-
bility of breath-hold whole-heart coro-nary MR angiography by using a 32-channel coil with high parallel factors(104). The advantage of these meth-ods is that both the coronary lumenand the vessel wall are visualized. Forimaging of the vessel lumen only, ASLhas been proposed in conjunction withbalanced SSFP for coronary MR an-giography (105,106).
Thoracic aortic MR angiography.—Without the necessity for venous or fatsuppression, combined with the fastflow of blood in the thoracic aorta, tho-racic MR angiography is perfectly suitedto balanced SSFP without ASL. Whenimplemented with ECG gating and trig-gered for diastolic acquisitions, 3D MRangiography can be achieved with respi-ratory triggering in acquisition times of5–10 minutes with use of parallel imag-ing (Fig 19).
LimitationsBalanced SSFP without ASL can bemore difficult to implement successfullyunder certain conditions. The sequenceis susceptible to field inhomogeneities,such as at air-tissue interfaces or in thepresence of metallic implants. To im-prove homogeneity, localized shimming
Figure 18
Figure 18: Reformatted 3D SSFP whole-heart coronary MR angiography (4.6/2.3; 90° flip angle; navigatorgated with fat saturation and T2 preparation) in a 42-year-old man with normal coronary arteries. (a) Left ante-rior oblique whole-heart angiogram with curved multiplanar reformatting clearly depicts the right coronaryartery (RCA) and left circumflex (LCX) arteries. (b) Oblique axial whole-heart coronary MR angiogram withcurved multiplanar reformatting shows the left main coronary artery, left anterior descending (LAD) artery,proximal RCA, and LCX arteries. (Reproduced, with permission, from reference 101.)
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
32 Radiology: Volume 248: Number 1—July 2008
may be necessary, which is typically notrequired with FSE methods. Addition-ally, without ASL, these sequences arenot specific for arteries or veins. The
addition of spin labeling or other sup-pression methods such as T2-prepara-tion pulses is necessary to produce ve-nous-free arteriograms.
ASL Imaging
Frequently used for perfusion measure-ments in the brain and elsewhere, ASLfor use with MR angiography can beusefully combined with fast imagingmethods such as balanced SSFP andpartial-Fourier FSE options. This sec-tion describes the principles of ASL foruse with MR angiography, considers arange of clinical applications, and con-cludes with a discussion of techniquelimitations.
Principles of TechniqueIn its earliest versions, ASL angiographygenerally relied on the spin tagging up-stream of the arteries of interest by us-ing an inversion pulse to generate imagecontrast (13–15,107,108). For exam-ple, Nishimura et al (13) obtained twoimages for subtraction, one with an in-version pulse limited to the upstreamslab and a second with a nonselectiveinversion so that upstream tissue wasinverted on only one acquisition. After ashort fixed time delay after the tagging,the tagged blood flows into the area ofinterest and the imaging can proceed.The time delay depends on the distancebetween the tagged and imaged areasand the rate of blood flow. The timedelay also affects the signal, since longerdelays result in less difference betweeninverted and noninverted signal becauseof T1 recovery. If this process is re-peated, with alternate acquisition of thetagged and nontagged images and twosets subtracted, the result will be abright-blood angiogram with no back-ground signal (Fig 20).
Bright-blood ASL imaging can alsobe produced by using a single acquisi-tion with a combination of a spatiallynonselective inversion recovery pulseand a spatially selective tag pulse (109)(Fig 21). The nonselective tag pulse in-verts the magnetization of the entirearea of imaging. The spatially selectivetagging pulse, again applied upstream ofthe arteries of interest, reverts thoseprotons to full magnetization. The spa-tially selective tagging pulse can be ap-plied in any orientation to mark specifi-cally the target vessels. A fixed time de-lay between tagging and imaging serves
Figure 19
Figure 19: MR angiography of the thoracic aorta in a 37-year-old man with recurrent aortic coarctation(arrow). Thin-section MIPs with (a) cardiac and respiratory-triggered balanced SSFP (259/1.4, 90° flip angle,parallel imaging factor of two, acquisition time of 6.5 minutes) without contrast material and (b) gadolinium-en-hanced 3D gradient-echo imaging. (Image courtesy of Monvadi B. Srichai, New York University Medical Center.)
Figure 20
Figure 20: Schematic for ASL-based MR angiography by using tag-on and tag-off images illustrates tag-ging (dashed box) applied to the chest, over the heart. During the interval, tagged blood moves to the desiredimaging region, carotid arteries in this example (curved arrow). Subtracted images produce MR angiogramsof carotid arteries, with all background tissue suppressed. This approach can be implemented by using par-tial-Fourier FSE or balanced SSFP readout techniques. FT � Fourier transform.
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
Radiology: Volume 248: Number 1—July 2008 33
two purposes. First, it allows the selec-tively tagged protons to reach the imag-ing region. Second, certain backgroundtissues in the imaging region can be se-lectively suppressed by imaging at theirnull point. For example, a delay time ofabout 550 msec can result in nulling ofbackground venous blood signal in theimaging volume.
For regions in which the back-ground tissues have a range of T1 relax-ation times, the application of a singleinversion time may be insufficient fornulling. In these cases, implementingthe tagged and untagged versions en-ables reliable suppression of back-ground signal with subtraction (Fig 20)(15,108).
Initially implemented by using read-out techniques such as segmented turbofast low-angle shot (turbo FLASH) orecho planar imaging, early results ofASL MR angiography were promising.For example, using a TOF subtractionmethod with turbo FLASH, Prasad et al(108) demonstrated that renal MR an-giography could be performed in 22 sec-onds by using 10–20-mm-thick sectionsand no ECG gating. In a pig model, sen-sitivity for detecting stenosis was 100%compared with that of conventional an-giography, with specificity varying from78% to 94%, depending on the defini-tion for significant stenosis (50% or70%). More recently, ASL methods havebeen implemented with two fast imagingmethods that have the advantage ofhigher signal-to-noise ratios compared tothose of previous methods: balancedSSFP and partial-Fourier FSE. Publishedliterature on these methods is limited, aswill be reviewed below; however, earlyresults are promising.
ASL with balanced SSFP.—The combi-nation of ASL with tagged and untaggedbalanced SSFP provides bright-blood,venous-free angiographic images withhigh signal-to-noise ratios (94,110,111).This approach is particularly well suitedto evaluation of vessels such as the renaland carotid arteries, because the se-quence is flow compensated in all threedirections and therefore minimizes sen-sitivity to flow artifacts.
ASL with partial-Fourier FSE.—Asan alternative to balanced SSFP, partial-
Fourier FSE methods can also be usedin conjunction with ASL. The SE-basedmethods have the advantage of less sen-sitivity to susceptibility artifacts com-pared with balanced SSFP. PulmonaryMR angiography with ASL methodstherefore benefits from the use of par-tial-Fourier FSE readout. For all partial-
Fourier FSE methods (see below), im-proved vascular signal is attained bycardiac triggering for diastolic imaging.
Applications of ASLPulmonary MR angiography.—Early re-sults reporting the application of ASLwith partial-Fourier FSE to 2D and 3D
Figure 21
Figure 21: Schematic for ASL-based MR angiography by using nonselective and selective tagged pulses.Imaging after an appropriate inversion time (TI ) results in nulling of background signal, which has experi-enced only the single nonselective inversion pulse (A). The tagged region (B ), upstream of the imaging area,has experienced both inversion pulses and retains full longitudinal magnetization. During the inversion time,tagged blood flows downstream into the desired imaging region. Unlike the approach shown in Figure 20, thisASL method can be performed by using a single acquisition and can be implemented by using partial-FourierFSE or balanced SSFP readout. Greadout � readout in frequency-encoding gradient, RF � radiofrequency.
Figure 22
Figure 22: Nonenhanced pulmonary MR angiography in a 26-year-old female volunteer by using ASL withalternating acquisitions with tag-on and tag-off and partial Fourier FSE (five R-R intervals/80, 180° flip angle,intermittent breathhold technique). (a) Spatially selective tagging was performed by using a sagittal slab overthe heart and imaging in the coronal plane to include the main pulmonary arteries bilaterally (ASL methoddepicted in Fig 20). Background signal was canceled out by the subtraction of tag-on and tag-off images.(b, c) Images show the effect of different inversion times of (b) 800 msec and (c) 1700 msec. (Image courtesyof F. Tateishi, Kumamoto Central Hospital, Japan.)
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
34 Radiology: Volume 248: Number 1—July 2008
pulmonary MR angiography have beenreported in abstract form (109,112).The imaging method uses a spatially se-lective tagging pulse and a nonselectiveinversion pulse as shown in Figure 22.The tag is applied by using a sagittalband across the heart. During the delaytime, that tagged blood from the hearttravels into the lungs. Then, the pulmo-nary arteries are imaged by using acoronal 3D partial-Fourier FSE acquisi-tion. Background signal is canceled outby subtraction of two acquisitions, onewith the tag on and a second without thetag. The delay time determines the pul-monary vasculature depicted and can bemanipulated to produce perfusion-typeimages (see Other Applications of ASLbelow). For pulmonary MR angiogra-phy, it is also possible to implement ASLby using a modified approach (109),whereby a spatially selective inversionpulse is applied in the area of interest,say in the coronal plane over the chest.Then, after an appropriate delay timefor inflow, that same region is imaged.Although background signal is presentin the chest wall and mediastinum, thedepiction of the pulmonary vessels withthis single acquisition can be excellent(Fig 23).
Carotid MR angiography.—Fast-flow-ing carotid arteries can be depicted byusing balanced SSFP with ASL and com-bined with parallel imaging. In one im-plementation reported in abstract form,a nonselective inversion pulse and selec-tive inversion pulse over the myocar-dium are applied in quick succession.After an inversion time selected to allowthe tagged myocardial blood to fill thecarotid arteries, the tagged protons areimaged by using a balanced SSFP se-quence (113) (Fig 24). Clinical testing ofthis method in patients is needed.
Renal MR angiography.—The bal-anced SSFP sequence is fully flow com-pensated in all three directions; there-fore, complex orientation of the aorta rel-ative to the renal arteries can be welldepicted by using the technique (Fig 25).For renal MR angiography, similar work(111) has been reported by using a real-time navigator echo during free breath-ing, where both a tag-on and tag-off ac-quisition were used. Spuentrup et alused a cylindrical (pencil beam) 2D se-lective inversion pulse to tag the supra-renal aorta and a 350–450-msec delayfrom labeling to data acquisition, with a122-msec acquisition to produce bright-blood renal MR angiography by using
balanced SSFP (111). In the initial clini-cal experience in eight healthy subjectsand seven patients with renal artery ste-nosis, with subtraction of two naviga-tor-gated data sets, results were compa-rable to contrast-enhanced MR angio-graphic images (111).
Distal-extremity MR angiography.—ASL with partial-Fourier FSE provides analternative approach to ECG-gated 3Dpartial-Fourier FSE imaging. An exam-ple in the hand is shown in Figure 26.Acquisition of one tag-on and one tag-off scan (Fig 20), followed by the sub-traction, eliminates background signaland improves visualization of small ves-sels in the hand and fingers. In Figure26a, tagging at the wrist is used to showarteries in the whole hand. The tech-nique can be modified to study the detailof even smaller vessels in the fingers(Fig 26b) by tagging the palm.
Other applications of ASL.—In ad-dition to being used to produce angio-grams, ASL can provide quantitativeand physiologic data about blood flow.The method has been validated forquantitative brain perfusion (for recent
Figure 23
Figure 23: Nonenhanced pulmonary MR angiography in a 28-year-old female volunteer by using modifiedASL approach and partial-Fourier FSE (five R-R intervals/80; 180° flip angle; inversion time, 800 msec withintermittent breathhold technique). (a) A spatially selective inversion pulse is applied in the coronal plane overthe chest and after a delay time for inflow, the same region is imaged. (b) Signal in the pulmonary vessels oncoronal MIP derives from the fresh untagged spins entering the slab. Note that signal from the background(muscle and fat) remains. (Image courtesy of F. Tateishi, Kumamoto Central Hospital, Japan.)
Figure 24
Figure 24: Nonenhanced carotid MR angio-gram in a 34-year-old male volunteer by usingASL with balanced SSFP and parallel imaging(5/2.5; 120° flip angle; inversion time, 900 msec;peripheral pulse gating; parallel imaging factor,two). Alternating acquisitions with tag-on andtag-off (Fig 19) are used. Note that strong sensitiv-ity to susceptibility with balanced SSFP causessignal loss in the subclavian arteries. (Image cour-tesy of Yuichi Yamashita, Toshiba.)
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
Radiology: Volume 248: Number 1—July 2008 35
reviews, see references 114,115). Mea-surement of blood velocity is also possi-ble with ASL. For example, by knowingthe distance between the tagged and im-aging slabs and the total duration oftime between application of the tag andcollection of the image (inversion recov-ery time plus effective echo time), themean blood velocity can be determined(109,116).
ASL methods can also be used to ob-tain noncontrast perfusion-like imagesoutside the brain by varying the timedelays between tagging and imaging,such as in the kidneys (108,117), lungs(118,119), and portal veins (120,121).Figure 27 illustrates a series of pulmonaryMR angiographic images by using a rangeof time delays, from 300 to 2500 msec,following tagging of the heart blood. Fordelay times of 300–1000 msec, blood canbe seen to flow from the pulmonary arter-ies to lung parenchyma, while after delaytimes of more than 1500 msec, blood be-gins to exit the lung parenchyma, causingdecreasing signal.
LimitationsAll techniques that rely on ASL for visu-alization of vessels share certain limita-tions. Because the technique relies onthe replacement of blood in the imagingvolume with tagged blood, the methodrequires reasonably high arterial veloc-ity for success. In peripheral arteries,where blood velocity is slower, the timeneeded to replace the blood in the imag-ing volume can approach that of T1 re-covery times for blood, resulting in loss
of the tagging effect. Multiple, separate,thinner-slab acquisitions may be neces-sary and therefore less efficient. Also,with selective tagging pulses for ASLMR angiography, flow direction is pre-sumed. For applications such as periph-eral MR angiography where flow rever-sal is sometimes encountered, this tech-nique can be limited (akin to the problemof TOF with traveling saturation bands).Limitations of standard ASL methodsthat require subtraction of tagged anduntagged datasets include longer acqui-sition times and the potential for motionbetween acquisitions to cause artifacts.
When implemented with ASL, par-tial-Fourier FSE and balanced SSFPmethods have different advantages anddisadvantages. To make bright-blood–tagged images with partial-Fourier FSE,the readout should be made during dias-tole, which lengthens the acquisition time,compared with balanced SSFP images,which can be acquired at any time with-out cardiac gating. On the other hand,balanced SSFP is much more stronglyaffected by susceptibility, comparedwith partial-Fourier FSE methods. Fortortuous vessels or those with branchesin different directions, the SSFP tech-niques may be preferable because thesequences are intrinsically flow com-pensated in three directions.
Summary of Applications for DifferentVascular Territories
From the above discussion, clearly thedifferences in key characteristics and
imaging requirements of different MRangiographic applications demand dif-ferent nonenhanced strategies. A sum-mary of possible strategies for nonen-hanced MR angiography in different ar-terial territories is provided in theTable.
Future Directions
Imaging at field strengths higher thanthe conventional 1.5 T, such as with the
Figure 25
Figure 25: Nonenhanced renal MR angiogram in a 27-year-old male volunteer by using ASL with balancedSSFP (5.0/2.5; 120° flip angle; inversion time, 1100 msec; parallel imaging factor, two). Selective and nonse-lective tagging approach (Fig 20) was used for aortic inflow with an inferior presaturation pulse to eliminatevenous flow. Acquisition was performed with respiratory triggering for a total scan time of 4 minutes. FrontalMIP is shown. (Image courtesy of J. Takahashi, Toranomon Hospital, Japan.)
Figure 26
Figure 26: Nonenhanced MR angiograms ofthe hand and digits in a 27-year-old male volun-teer by using ASL and partial-Fourier FSE (threeR-R intervals/80; 180° flip angle; inversion time,600 msec). Alternating acquisitions with tag-onand tag-off (Fig 20) were used to image (a) thewhole hand by applying the tag on the wrist and(b) the digits by applying the tag on the palm. (Imagecourtesy of J. Isogai, Hasuda Hospital, Japan.)
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
36 Radiology: Volume 248: Number 1—July 2008
Figure 27
Figure 27: Perfusion-like images of the lungs in a 28-year-old female volunteer by using ASL technique with partial-Fourier FSE. Images acquired across a range ofincreasing inversion times (TI ) by using a sagittal tagging slab. Increasing inversion time allows the tagged blood to travel further into the periphery of the lungs. Notethat background signal is canceled out by the subtraction of tag-on and tag-off images.
Suggested Nonenhanced MR Angiographic Techniques
MR Angiographic Application MR Method Notes*
Intracranial 3D TOF TONE and MOTSA improve sensitivity to slower flowCarotid ASL with 3D balanced SSFP or partial-Fourier FSE,
alternatively 2D or 3D TOF. . .
Thoracic aorta ECG-gated 3D partial-Fourier FSE alternatively 3D balancedSSFP
No flow spoiling, balanced SSFP can also be performed with ASL
Pulmonary ECG-gated 3D partial-Fourier FSE alternatively ASL with 3Dpartial-Fourier FSE
Triggering in diastole
Coronary ECG-gated 3D balanced SSFP Breath hold alternatively navigator-free breathingAbdominal aorta or renal ASL with 3D balanced SSFP alternatively phase contrast Multidirectional flow pattern favors SSFP over gated FSEPeripheral ECG-gated 3D partial-Fourier FSE with flow spoiling or flow
compensation alternatively 2D TOF with travelingsaturation bands
Customize degree of flow spoiling or compensation at each station
Hand and foot ASL with 3D balanced SSFP or partial-Fourier FSE Partial-Fourier FSE depicts morphology, ASL is a function of blood flowFlow quantification Phase contrast . . .
* MOTSA � multiple overlapping thin slab acquisition, TONE � tilt optimized nonsaturated excitation.
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
Radiology: Volume 248: Number 1—July 2008 37
increasingly available 3-T systems, hasdifferent benefits and drawbacks for thevarious nonenhanced MR techniques.Longer T1 relaxation times inherentlybenefit ASL methods by prolonging theduration of tagging effects. However, ifperformed in conjunction with balancedSSFP methods, these advantages maybe offset by the increased susceptibilityat higher field strengths with balancedSSFP. On the other hand, improved ar-terial-venous contrast at 3 T can beachieved with balanced SSFP sequencesby use of longer repetition time, whichresults in less conspicuous venous signalintensity on peripheral MR angiograms,and with the advantages of facilitatinghigher spatial resolution and reduced
bandwidths (33,96). For partial-FourierFSE methods, specific absorption ratelimitations may limit the use of full 180°refocusing pulses and result in reducedimage contrast and signal-to-noise ra-tios. Nevertheless, the intrinsically highersignal-to-noise ratio at 3 T does lend itselfwell to the use of parallel imaging.
Implementation of parallel imagingcan be particularly beneficial to nonen-hanced MR angiographic methods byreducing acquisition times and conse-quently decreasing undesirable blurringand motion artifacts. Most applicationsof parallel imaging suffer a trade-off ofreduced signal for shorter scan times;however, partial-Fourier FSE with par-allel imaging allows for compensating
benefits that include a reduction in T2blurring. With shorter acquisition times,multistation imaging with nonenhancedmethods becomes feasible. An exampleof whole-body nonenhanced MR angiog-raphy with high parallel imaging factorsis presented in Figure 28.
Last, a promising direction on thehorizon is the development of time-re-solved imaging techniques with nonen-hanced MR angiographic methods, par-ticularly the ECG-gated partial-FourierFSE method (122) and ASL with SSFP(123). Time-resolved methods may be-come possible with higher order parallelimaging implemented with undersam-pling techniques that use methods suchas radial imaging to vastly shorten ac-
Figure 28
Figure 28: Nonenhanced whole-body MR angiography at 1.5 T in a 39-year-old healthy male volunteer by using 3D ECG-gated partial-Fourier FSE (three R-R inter-vals/30; 180° flip angle; intermittent breathhold; total acquisition time, approximately 3 minutes per station). Images obtained with (a) a whole-body coil without parallelimaging and (b) 128-element coils with parallel imaging factor of six to eight (by implementation in both phase-encoding and section directions) in upper body and ab-domen. Note less blurring in b (inset), compared with a (inset). (Image courtesy of Nobuyasu Ichinose, Toshiba, Japan.)
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
38 Radiology: Volume 248: Number 1—July 2008
quisition times (124). Use of incrementaltrigger delay times may allow improvedsensitivity to a wider range of flow veloci-ties and resemble time-resolved contrast-enhanced MR angiography (Fig 29). Ini-tial data suggest that delays in enhance-ment on the time-resolved images mayreflect the severity of stenosis in periph-eral vascular disease (92), a promisingindication of advances to come in nonen-hanced MR angiography.
Glossary
arterial spin labeling, or ASL
MR imaging technique where protonsin a specific region, typically in a bloodvessel upstream of the imaging field ofview, experience an inversion pulseand are thereby “tagged.” After a fixedinterval, or delay time, when thetagged protons have traveled into thefield of view, imaging is performed.Variations on this approach can alsobe performed to suppress undesiredbackground signal through additionalnonselective inversion pulses.
balanced steady-state free precession,or SSFPA gradient-echo sequence frequently usedin cardiovascular applications wheresignal intensity does not depend onblood flow but rather on the ratio of T2to T1 relaxation times; blood is typicallybright. Also referred to as fast imagingemploying steady-state acquisition, orFIESTA, true fast imaging with steady-state precession, or true FISP, balancedfast field echo, or balanced FFE.
fast spin echo, or FSEA spin-echo sequence that uses multi-ple 180° refocusing pulses to generatea number of spin echoes per radiofre-quency excitation. The number of spinechoes is referred to as the echo trainlength, and the time between consec-utive echoes is the echo train spac-ing.
flow compensationTechnique designed to reduce the signalloss or dephasing caused by blood mov-ing with constant velocity. The methodrelies on specially designed positive andnegative gradients applied in the direc-
tion of blood flow. Also referred to asgradient moment nulling.
inversion pulseA 180° radiofrequency pulse that servesto invert the longitudinal magnetization.Inversion pulses are used as prepulsesfor sequences such as short tau inver-sion recovery (STIR) that are designedto null signal from fat. They are alsoused in ASL sequences where protonsused for imaging are selectively “tagged”by using inversion pulses.
magnetization transferThe transfer of energy between free, un-bound water protons and protons boundto macromolecules that results in differ-ences in T2 relaxation times. Magnetiza-tion transfer is used to suppress back-ground tissue, such as brain parenchyma,to allow greater conspicuity of vessels.
multiple overlapping thin-slabacquisition, or MOTSAA TOF angiographic method that usesmultiple thin 3D slabs, which slightlyoverlap, so that the resulting overall 3Dangiogram has less signal saturationthan would occur with a single-volume3D acquisition.
parallel imagingA technique for undersampling k-spaceby using coil sensitivity profiles, whichresults in substantial reductions in ac-quisition times at a cost of reduced sig-nal-to-noise ratios.
partial FourierA term used to refer to incomplete fill-ing of k-space by using a reduced num-ber of phase-encoding steps to shortenacquisition times.
phase-contrast angiographyA technique for generating MR angio-grams that relies on the accumulation ofphase differences as moving protonstravel through magnetic field gradients.
short tau inversion recovery, or STIRA fat-suppression technique that uses aninversion recovery pulse with an inver-sion time selected to null the signal fromfat.
Figure 29
Figure 29: Time-resolved nonenhanced MR angiograms in a 62-year-old male patient with arteriosclero-sis obliterans at occlusion of the left external artery by using 2D single-shot partial-Fourier FSE (three R-Rintervals/80 effective, 180° refocusing flip angle) with incremental delay times. Selected images are depictedfrom a series acquired with delay time increments of 10 msec and subtraction of systolic images from diastolicimages. From late systolic to diastolic phases, images show normal flow in the right iliac artery, whereas theleft iliac artery shows delay in flow due to stenosis. (Image courtesy of Dr. K. Nakamura, Kyoritsu Tobata Hos-pital, Japan.)
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
Radiology: Volume 248: Number 1—July 2008 39
spatially selective excitation pulsesRadiofrequency pulses that are applied tospecific regions of the body so as to resultin excitation of only protons in those re-gions, without affecting the remainder ofthe protons in the field of view.
spoiler gradientsExtended application of gradients todephase magnetization. In the case ofECG-gated 3D partial-Fourier FSE se-quences, the spoiler gradients are usedto enhance differences between arterialand venous blood signal.
tilt optimized nonsaturated excitation, orTONETechnique used for intracranial TOFMR angiography to compensate for sat-uration of blood flowing into the imagingslab by using progressively increasingflip angles to image protons that havemoved deeper into the slab.
time-of-flight angiographyMR angiography technique based on thedifferences between protons in station-ary tissue, which are saturated by re-peated radiofrequency excitations andthe high signal from fresh unsaturatedprotons that move into the imaging slabbetween each excitation pulse.
time-resolved angiographyA term used to refer to repeated MRangiographic acquisitions that depictthe temporal changes related to the ar-rival and passage of blood through thearterial and venous systems.
References1. Prince MR. Gadolinium-enhanced MR aor-
tography. Radiology 1994;191:155–164.
2. Wilman AH, Riederer SJ, King BF, DebbinsJP, Rossman PJ, Ehman RL. Fluoroscopi-cally triggered contrast-enhanced three-di-mensional MR angiography with ellipticalcentric view order: application to the renalarteries. Radiology 1997;205:137–146.
3. Earls JP, Rofsky NM, DeCorato DR, KrinskyGA, Weinreb JC. Breath-hold single-dosegadolinium-enhanced three-dimensionalMR aortography: usefulness of a timing ex-amination and MR power injector. Radiol-ogy 1996;201:705–710.
4. Kita M, Mitani Y, Tanihata H, et al. Moving-
table reduced-dose gadolinium-enhancedthree-dimensional magnetic resonance an-giography: velocity-dependent method withthree-phase gadolinium infusion. J MagnReson Imaging 2001;14:319–328.
5. Ho KY, Leiner T, de Haan MW, KesselsAG, Kitslaar PJ, van Engelshoven JM. Pe-ripheral vascular tree stenoses: evaluationwith moving-bed infusion-tracking MR an-giography. Radiology 1998;206:683–692.
6. Meaney JF, Ridgway JP, Chakraverty S, etal. Stepping-table gadolinium-enhanceddigital subtraction MR angiography of theaorta and lower extremity arteries: pre-liminary experience. Radiology 1999;211:59–67.
7. Sodickson DK, McKenzie CA, Li W, WolffS, Manning WJ, Edelman RR. Contrast-en-hanced 3D MR angiography with simulta-neous acquisition of spatial harmonics: apilot study. Radiology 2000;217:284–289.
8. Korosec FR, Frayne R, Grist TM, MistrettaCA. Time-resolved contrast-enhanced 3DMR angiography. Magn Reson Med 1996;36:345–351.
9. Wildermuth S, Debatin JF, Huisman TA,Leung DA, McKinnon GC. 3D phase con-trast EPI MR angiography of the carotidarteries. J Comput Assist Tomogr 1995;19:871–878.
10. Miller S, Schick F, Duda SH, et al. Gd-enhanced 3D phase-contrast MR angiogra-phy and dynamic perfusion imaging in thediagnosis of renal artery stenosis. Magn Re-son Imaging 1998;16:1005–1012.
11. Dumoulin CL, Yucel EK, Vock P, et al. Two-and three-dimensional phase contrast MRangiography of the abdomen. J Comput As-sist Tomogr 1990;14:779–784.
12. Dumoulin CL, Souza SP, Walker MF,Wagle W. Three-dimensional phase con-trast angiography. Magn Reson Med 1989;9:139–149.
13. Nishimura DG, Macovski A, Pauly JM,Conolly SM. MR angiography by selectiveinversion recovery. Magn Reson Med 1987;4:193–202.
14. Edelman RR, Siewert B, Adamis M, Gaa J,Laub G, Wielopolski P. Signal targetingwith alternating radiofrequency (STAR)sequences: application to MR angiography.Magn Reson Med 1994;31:233–238.
15. Wielopolski PA, Adamis M, Prasad P, GaaJ, Edelman R. Breath-hold 3D STAR MRangiography of the renal arteries using seg-mented echo planar imaging. Magn ResonMed 1995;33:432–438.
16. Sodickson DK, Manning WJ. Simultaneousacquisition of spatial harmonics (SMASH):
fast imaging with radiofrequency coil ar-rays. Magn Reson Med 1997;38:591–603.
17. Pruessmann KP, Weiger M, ScheideggerMB, Boesiger P. SENSE: sensitivity encod-ing for fast MRI. Magn Reson Med 1999;42:952–962.
18. Cowper SE, Robin HS, Steinberg SM, SuLD, Gupta S, LeBoit PE. Scleromyxoe-dema-like cutaneous diseases in renal-dial-ysis patients. Lancet 2000;356:1000–1001.
19. Sadowski EA, Bennett LK, Chan MR, et al.Nephrogenic systemic fibrosis: risk factorsand incidence estimation. Radiology 2007;243:148–157.
20. Grobner T. Gadolinium: a specific triggerfor the development of nephrogenic fibros-ing dermopathy and nephrogenic systemicfibrosis? Nephrol Dial Transplant 2006;21:1104-1108. [Published correction appearsin Nephrol Dial Transplant 2006;21:1745.]
21. Urata J, Miyazaki M, Wada H, Nakaura T,Yamashita Y, Takahashi M. Clinical evalua-tion of aortic diseases using nonenhancedMRA with ECG-triggered 3D half-FourierFSE. J Magn Reson Imaging 2001;14:113–119.
22. Lee VS, Martin DJ, Krinsky GA, Rofsky NM.Gadolinium-enhanced MR angiography: ar-tifacts and pitfalls. AJR Am J Roentgenol2000;175:197–205.
23. Lohan DG, Saleh R, Nael K, Krishnam M,Finn JP. Contrast-enhanced MRA versusnonenhanced MRA: pros and cons. ApplRadiol 2007;36(suppl):3–15.
24. Kanda T, Nakamura E, Moritani T, YamoriY. Arterial pulse wave velocity and risk fac-tors for peripheral vascular disease. EurJ Appl Physiol 2000;82:1–7.
25. Rose SC. Noninvasive vascular laboratoryfor evaluation of peripheral arterial occlu-sive disease. II. Clinical applications:chronic, usually atherosclerotic, lower ex-tremity ischemia. J Vasc Interv Radiol2000;11:1257–1275.
26. Fronek A, Coel M, Berstein EF. Quantita-tive ultrasonographic studies of lower ex-tremity flow velocities in health and dis-ease. Circulation 1976;53:957–960.
27. Toursarkissian B, Mejia A, Smilanich RP,Schoolfield J, Shireman PK, Sykes MT.Noninvasive localization of infrainguinal ar-terial occlusive disease in diabetics. AnnVasc Surg 2001;15:73–78.
28. Parker DL, Tsuruda JS, Goodrich KC, Al-exander AL, Buswell HR. Contrast-en-hanced magnetic resonance angiography ofcerebral arteries: a review. Invest Radiol1998;33:560–572.
STATE OF THE ART: Nonenhanced MR Angiography Miyazaki and Lee
40 Radiology: Volume 248: Number 1—July 2008
29. Bernstein MA, Huston J 3rd, Lin C, GibbsGF, Felmlee JP. High-resolution intracra-nial and cervical MRA at 3.0T: technicalconsiderations and initial experience. MagnReson Med 2001;46:955–962.
30. de Bazelaire CM, Duhamel GD, RofskyNM, Alsop DC. MR imaging relaxationtimes of abdominal and pelvic tissues mea-sured in vivo at 3.0 T: preliminary results.Radiology 2004;230:652–659.
31. Barth M, Moser E. Proton NMR relaxationtimes of human blood samples at 1.5 T andimplications for functional MRI. Cell MolBiol (Noisy-le-grand) 1997;43:783–791.
32. Wright GA, Hu BS, Macovski A. 1991 I.I.Rabi Award. Estimating oxygen saturationof blood in vivo with MR imaging at 1.5 T. JMagn Reson Imaging 1991;1:275–283.
33. Brittain JH, Olcott EW, Szuba A, et al.Three-dimensional flow-independent pe-ripheral angiography. Magn Reson Med1997;38:343–354.
34. Gronas R, Kalman PG, Kucey DS, WrightGA. Flow-independent angiography for pe-ripheral vascular disease: initial in-vivo re-sults. J Magn Reson Imaging 1997;7:637–643.
35. Pomposelli FB, Kansal N, Hamdan AD, etal. A decade of experience with dorsalispedis artery bypass: analysis of outcome inmore than 1000 cases. J Vasc Surg 2003;37:307–315.
36. Hughes K, Domenig CM, Hamdan AD, etal. Bypass to plantar and tarsal arteries: anacceptable approach to limb salvage. J VascSurg 2004;40:1149–1157.
37. Hahn WY, Hecht EM, Friedman B, BabbJS, Jacobowitz GR, Lee VS. Distal lowerextremity imaging: prospective comparisonof 2-dimensional time of flight, 3-dimen-sional time-resolved contrast-enhancedmagnetic resonance angiography, and 3-di-mensional bolus chase contrast-enhancedmagnetic resonance angiography. J Com-put Assist Tomogr 2007;31:29–36.
38. Masaryk TJ, Laub GA, Modic MT, Ross JS,Haacke EM. Carotid-CNS MR flow imaging.Magn Reson Med 1990;14:308–314.
39. Laub GA. Time-of-flight method of MR an-giography. Magn Reson Imaging Clin N Am1995;3:391–398.
40. Kaufman JA, McCarter D, Geller SC, WaltmanAC. Two-dimensional time-of-flight MR an-giography of the lower extremities: arti-facts and pitfalls. AJR Am J Roentgenol1998;171:129–135.
41. Li W, Zhang M, Sher S, Edelman RR. MRangiography of the vascular tree from theaorta to the foot: combining two-dimen-
sional time-of-flight and three-dimensionalcontrast-enhanced imaging. J Magn ResonImaging 2000;12:884–889.
42. Nelemans PJ, Leiner T, de Vet HC, vanEngelshoven JM. Peripheral arterialdisease: meta-analysis of the diagnosticperformance of MR angiography. Radiology2000;217:105–114.
43. Owen RS, Carpenter JP, Baum RA, PerloffLJ, Cope C. Magnetic resonance imaging ofangiographically occult runoff vessels in pe-ripheral arterial occlusive disease. N EnglJ Med 1992;326:1577–1581.
44. McCauley TR, Monib A, Dickey KW, et al.Peripheral vascular occlusive disease: accu-racy and reliability of time-of-flight MR an-giography. Radiology 1994;192:351–357.
45. Carpenter JP, Baum RA, Holland GA,Barker CF. Peripheral vascular surgerywith magnetic resonance angiography asthe sole preoperative imaging modality. JVasc Surg 1994;20:861–869; discussion869–871.
46. Baum RA, Rutter CM, Sunshine JH, et al.Multicenter trial to evaluate vascular mag-netic resonance angiography of the lowerextremity. American College of RadiologyRapid Technology Assessment Group.JAMA 1995;274:875–880.
47. Atkinson D, Brant-Zawadzki M, Gillan G,Purdy D, Laub G. Improved MR angiography:magnetization transfer suppression with vari-able flip angle excitation and increased reso-lution. Radiology 1994;190:890–894.
48. Blatter DD, Parker DL, Robinson RO. Ce-rebral MR angiography with multiple over-lapping thin slab acquisition. Radiology1991;179:805–811.
49. Parker DL, Yuan C, Blatter DD. MR angiog-raphy by multiple thin slab 3D acquisition.Magn Reson Med 1991;17:434–451.
50. Pike GB, Hu BS, Glover GH, Enzmann DR.Magnetization transfer time-of-flight mag-netic resonance angiography. Magn ResonMed 1992;25:372–379.
51. Miyazaki M, Kojima F, Ichinose N, OnozatoY, Igarashi H. A novel saturation transfercontrast method for 3D time-of-flight mag-netic resonance angiography: a slice-selec-tive off-resonance sinc pulse (SORS) tech-nique. Magn Reson Med 1994;32:52–59.
52. Dumoulin CL. Phase contrast MR angiogra-phy techniques. Magn Reson Imaging ClinN Am 1995;3:399–411.
53. Steffens JC, Link J, Muller-Hulsbeck S,Freund M, Brinkmann G, Heller M. Cardiac-gated two-dimensional phase-contrast MRangiography of lower extremity occlusive
disease. AJR Am J Roentgenol 1997;169:749–754.
54. Zhang H, Prince MR. Renal MR angiogra-phy. Magn Reson Imaging Clin N Am 2004;12:487-503, vi.
55. Meyers SP, Talagala SL, Totterman S, et al.Evaluation of the renal arteries in kidneydonors: value of three-dimensional phase-contrast MR angiography with maximum-intensity-projection or surface rendering.AJR Am J Roentgenol 1995;164:117–121.
56. de Haan MW, Kouwenhoven M, ThelissenRP, et al. Renovascular disease in patientswith hypertension: detection with systolicand diastolic gating in three-dimensional,phase-contrast MR angiography. Radiology1996;198:449–456.
57. De Cobelli F, Mellone R, Salvioni M, et al.Renal artery stenosis: value of screeningwith three-dimensional phase-contrast MRangiography with a phased-array multicoil.Radiology 1996;201:697–703.
58. Duda SH, Schick F, Teufl F, et al. Phase-contrast MR angiography for detection ofarteriosclerotic renal artery stenosis. ActaRadiol 1997;38:287–291.
59. De Cobelli F, Vanzulli A, Sironi S, et al.Renal artery stenosis: evaluation withbreath-hold, three-dimensional, dynamic,gadolinium-enhanced versus three-dimen-sional, phase-contrast MR angiography.Radiology 1997;205:689–695.
60. Hahn U, Miller S, Nagele T, et al. Renal MRangiography at 1.0 T: three-dimensional(3D) phase-contrast techniques versus gad-olinium-enhanced 3D fast low-angle shotbreath-hold imaging. AJR Am J Roentgenol1