Embed Size (px)
Citation preview
Nonclinical Studies SubcommitteeAdvisory Committee for Pharmaceutical
Science
Introduction & FDA Objectives
Gaithersburg HiltonDecember 14, 1999
T:\NCSS\121499.PPT
Nonclinical Studies Subcommittee
Functions: To provide advice on improved scientific
approaches to nonclinical drug development A means to foster scientific collaboration
among FDA, industry, academia, and the public
Scientific Advances & Opportunities
Genomics/proteomics Information technology High throughput technologies Mechanistic knowledge
Cancer, inflammation, cell signalling, etc.
Artificial intelligence Noninvasive imaging
An example of accelerating scientific information and technology:
Safety Assessment
Toxicology in the last millennium~~ B.C. knowledge & use of poisons
1500’s Exptl. physiology, toxic vs therapeutic dose-response (Paracelsus)
1600 Compound microscope1600-1700 Anatomic microscopy (Hooke, Malphigi, van Leeuwenhoek)
1700’s Comparative anatomy (Hunter, Cuvier); Occupational toxicology (Ramazzini); Environmental cancer (Potts)
1800’s Exptl. physiology & toxicolgy (CO, strychnine, curare)Chemical teratogenesis (St. Hilare) Cellular pathology (Virchow, 1860’s)
1900’s Modern regulatory toxicolgy Cell biochemistry and molecular biology
Toxicology in the last half century~~ 1906/1938 Food and Drug Acts; first flight
1940s Chemical carcinogenesis (Millers) & mutagenesis (Auerbach); DNA is the genetic material
1950 DNA structure; Clinical chemistry (serum biomarkers); Biochemistry (e.g., Krebs cycle); current approach tosystemic toxicity evaluation
1960 Toxicology as a discipline (SOT)Thalidomide, teratogensis testing
1970 EPA, OSHA formed; man on moon1970’s Genetic toxicology testing; EMS (19070; TSCA (1978)
1980’s Genetic engineering; oncogenes; noninvasive imaging
1990’s Molecular damage response and defense Genome sequenced; era of genetic links to disease; high-throughput genetic tools
Current “Biomarkers” of Systemic Toxicity
Markers of: Cellular integrity (AST, ALT, etc.) Homeostasis (BUN, electrolytes,cell type, etc.) Morpohologic evidence of damage Host defense responses
Behavior/appearance/body weight of organism
Current approach to safety evaluation
Clinical Chemistry/Hematology Markers of cellular integrity (AST, ALT, etc.) Markers of homeostasis (BUN, electolytes, etc.) Alterations in circulating cell populations
Histopathology Visible morphologic or staining change Host defense cell infiltration
Behavior/appearance/body weight of organism Special tests: cancer, mutation, reproduction,
neurotoxicology, immunotoxicology, etc.
Some Opportunities for New/Improved Toxicological Practices
Damage-specific responses Objective biochemical assays for host-defense cell
signaling and infiltration Better biomarkers of integrity/homeostasis
e.g., troponins Biochemical markers of cell death In vivo genetic markers of mutational damage,
oncogene activation, and suppressor inactivation Noninvasive technologies “Humanized” and/or transgenic animals Cell culture & microengineering
Molecular Evolution of Defense Systems
Systems have evolved to protect and repair each major function
Defense systems are often inducible
Molecules often evolve from function to repair
Key defense systems are conserved
Understanding these systems will provide the next generation of surrogate biomarkers for monitoring damage to cells and tissues
Some Damage- or Agent-Inducible Genes
Damage TypeFunctional Class /Inducer Class Example GenesProtein structure Protein denaturation HSP70, clpBDNA integrity DNA damage dinD, recA, GADD153Oxidative Protectants Redox balance katG, soi28, GSTGrowth Control Cell proliferators FOS, JUN DNA damage Metal Inducible Toxic metals merRXenobiotic Inducible Xenobiotics CYP1A1, CYP2E1
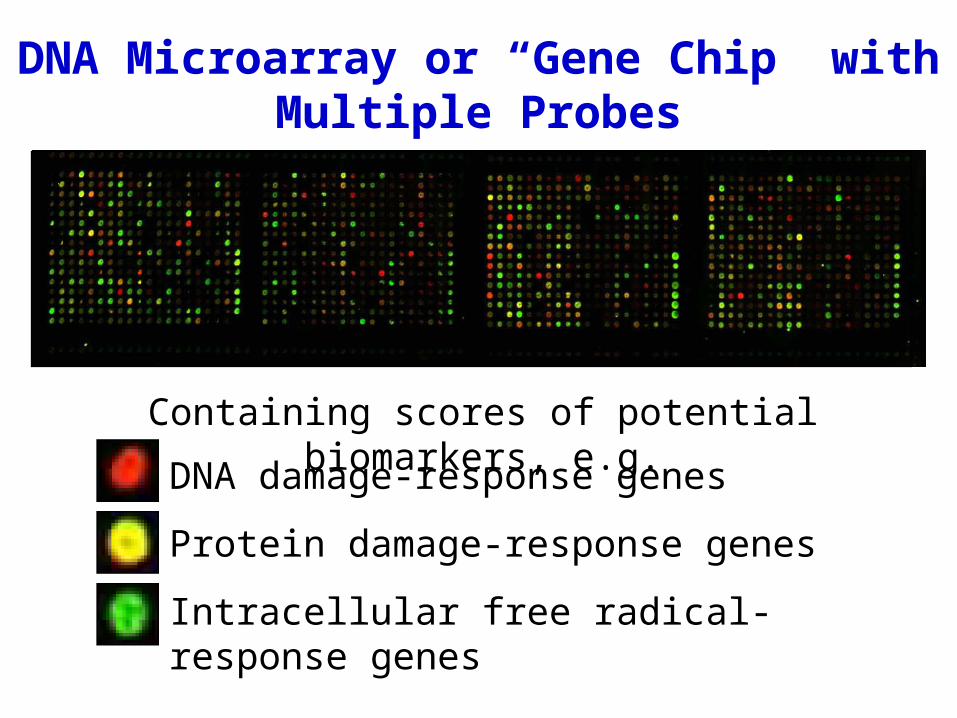
DNA damage-response genes
Protein damage-response genes
Intracellular free radical-response genes
DNA Microarray or “Gene Chip” with Multiple Probes
Containing scores of potential biomarkers, e.g.
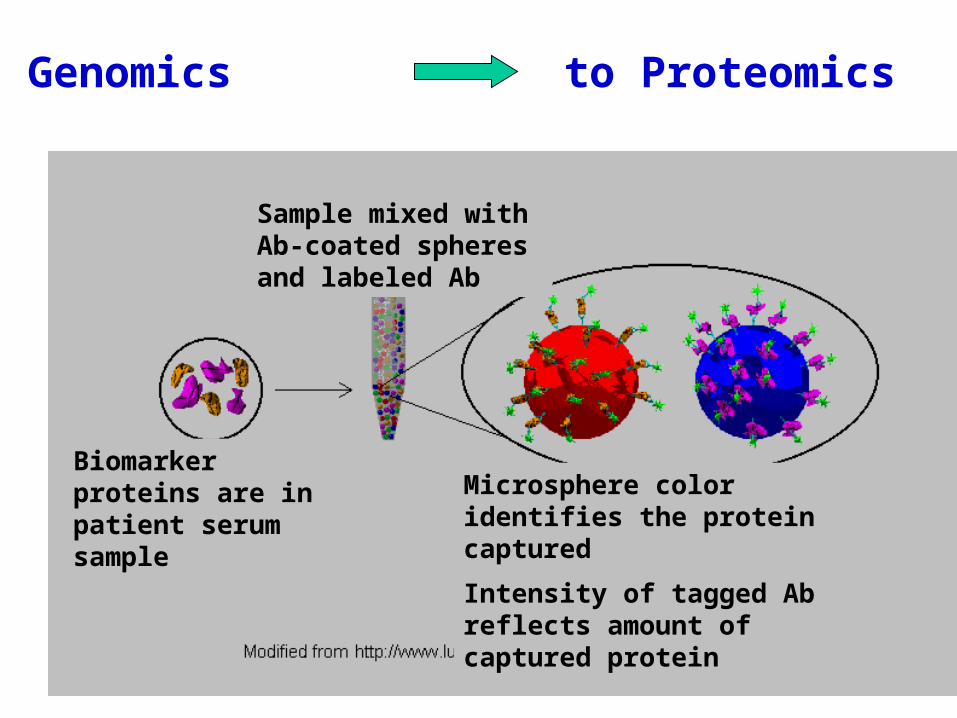
Genomics to Proteomics
Microsphere color identifies the protein captured
Intensity of tagged Ab reflects amount of captured protein
Sample mixed with Ab-coated spheres and labeled Ab
Biomarker proteins are in patient serum sample
What do we need to know?
Relationship of endpoint to health
Relationship to outcomes in established
assays
Relationship between laboratory models
and man
Reproducibility, accuracy, sensitivity,
robustness
Application of Safety Biomarkers to Human Studies
• Secreted proteins that are upregulated following toxic insult
• Tissue/organ-specific proteins that signal loss of cellular integrity
• Inaccessible upregulated membrane proteins that bind specific non-invasively monitorable probes
Biochemical Markers of Pathology
Damage/Insult Defense Response
Cell death Caspase-mediated cell death
Cell death/tissue damage Chemokine/cytokine-mediated
inflammatory response
Foreign/damaged protein Immune responses/NK receptor
Better biomarkers of cell integrity and homeostasis
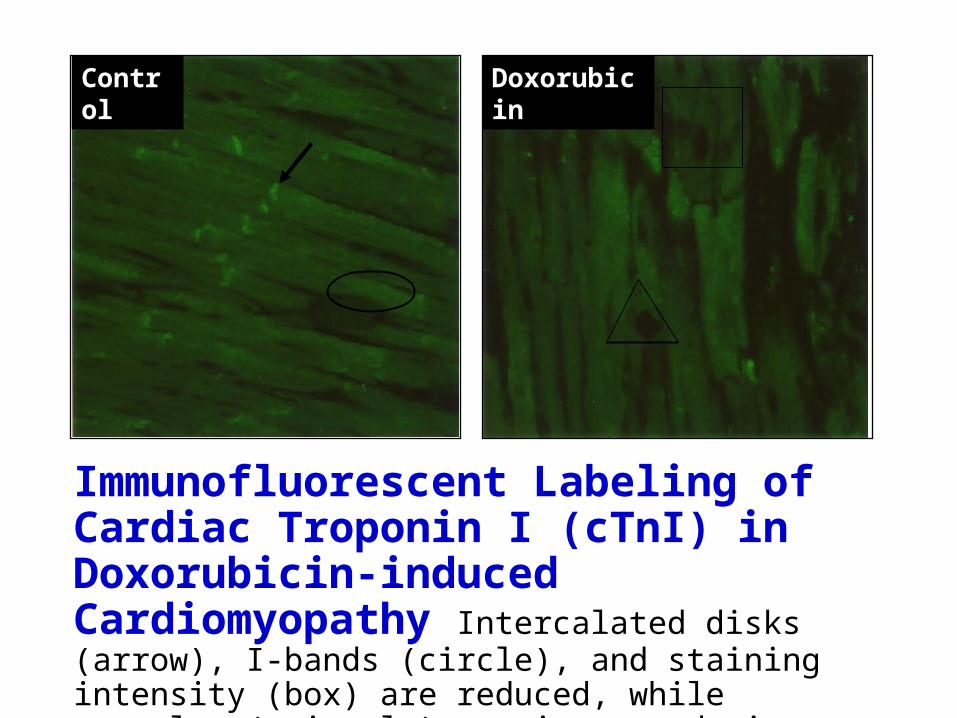
Immunofluorescent Labeling of Cardiac Troponin I (cTnI) in Doxorubicin-induced Cardiomyopathy Intercalated disks (arrow), I-bands (circle), and staining intensity (box) are reduced, while vacuoles (triangle) are increased in DXR- treated animals.
Control Doxorubicin
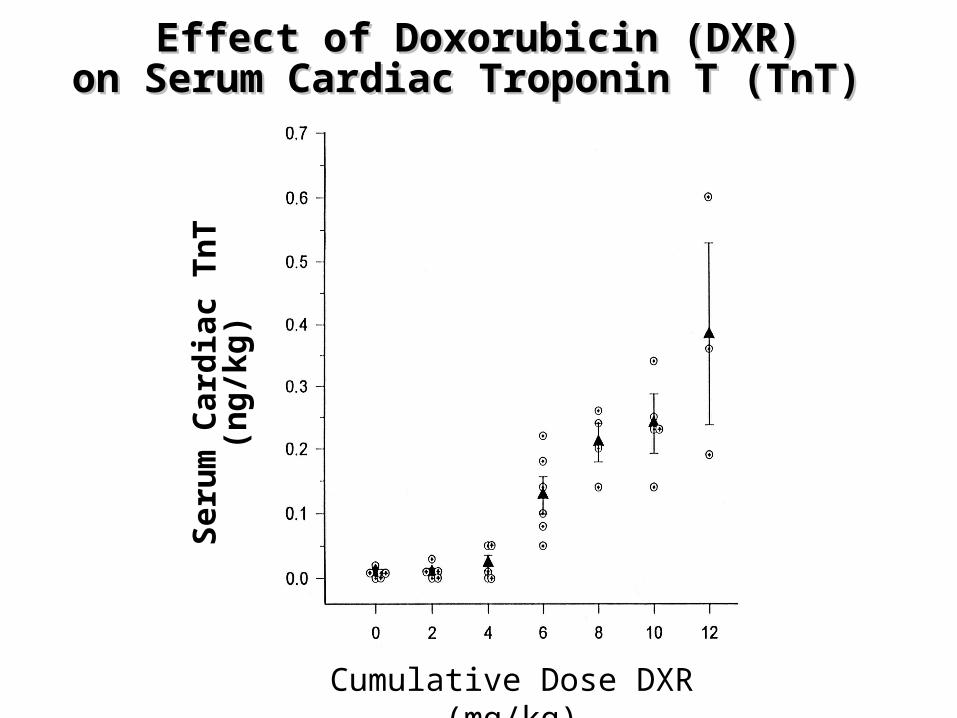
Effect of Doxorubicin (DXR)Effect of Doxorubicin (DXR)on Serum Cardiac Troponin T (TnT)on Serum Cardiac Troponin T (TnT)
Cumulative Dose DXR (mg/kg)
Ser
um
Car
dia
c T
nT
(ng/
kg)
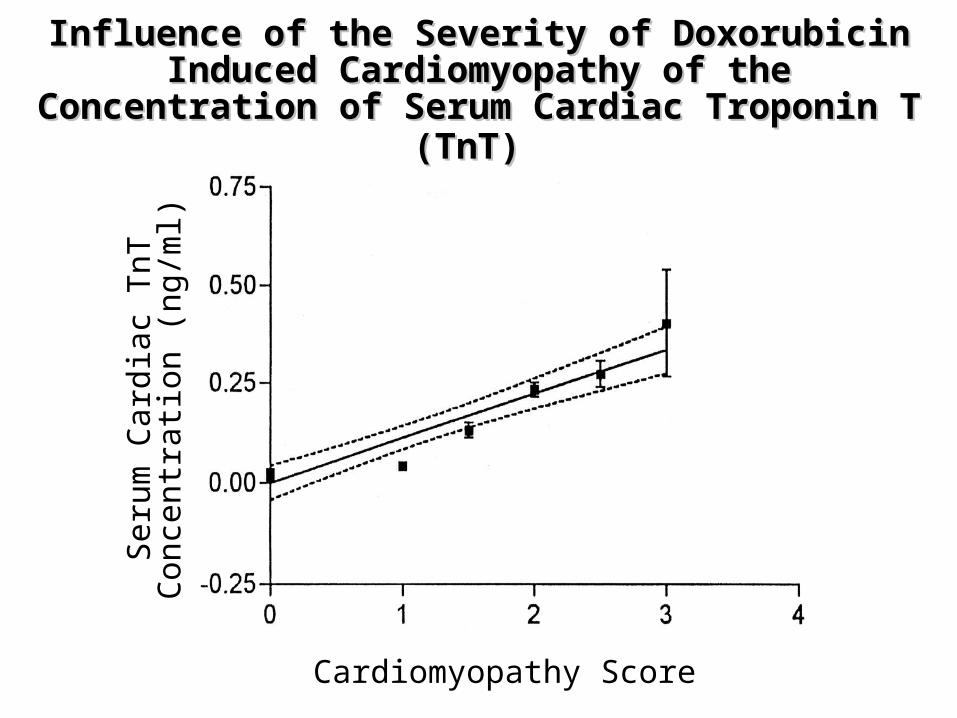
Influence of the Severity of Doxorubicin Induced Influence of the Severity of Doxorubicin Induced Cardiomyopathy of the Concentration of Serum Cardiomyopathy of the Concentration of Serum
Cardiac Troponin T (TnT)Cardiac Troponin T (TnT)
Cardiomyopathy Score
Ser
um C
ardi
ac T
nTC
once
ntra
tion
(ng/
ml)
How to focus resources among opportunities?
ACPS Nonclinical Studies Subcommittee:• Identify and recommend focus areas
• Identify experts in focus areas; form expert working groups (EWGs) with nominations from:• Federal Register announcements (Public)• FDA and “Stakeholders” (Collaborators)• Professional Societies
• Steering committee to collaborative projects• Support workshops and facilitate reports
Potential collaborators
FDA CDER CBER
Industry PhRMA BIO
Academia Public Institutions
Objectives1. To recommend approaches and mechanisms
to improve: Nonclinical information for effective drug
development Predictivity of nonclinical tests for human
outcomes Linkage between nonclinical and clinical
studies
and
2. To facilitate collaborative approaches to advancing the scientific basis of drug development and regulation
History and Next Steps NCSS Subcommittee meeting 8/31/99
– Define objectives and operating principles– Define focus areas– Discuss initial focus areas and mechanisms for
implementation– Define operating structure
ACPS meeting 9/24/99– ACPS endorsed concept
Select initial focus areas Form EWGs EWGs identify collaborators and identify
resources
![Nonclinical Safety Assessment of Biotherapeutics 11... · o ICH S9 [Nonclinical evaluation for anticancer pharmaceuticals] o ICH M3(R2) [Guidance on nonclinical safety studies for](https://img.pdfslide.us/doc/110x75/5f733d0766c4e466827990be/nonclinical-safety-assessment-of-biotherapeutics-11-o-ich-s9-nonclinical-evaluation.jpg)




























