Embed Size (px)
Citation preview
Non-Opioid Alternatives to Pain Management
Krysta Baack, PharmD, BCPS
Emergency Medicine Pharmacy Clinical Coordinator
Emergency Medicine Pharmacy PGY2 Residency Program Director
Nebraska Medicine
No actual or potential conflicts of interestUnlabeled and/or investigational use of some drugs will be discussed
(non-FDA labeled indications)
Objectives
1. Examine the different types of pain syndromes
2. Identify non-opioid options for treating different pain syndromes
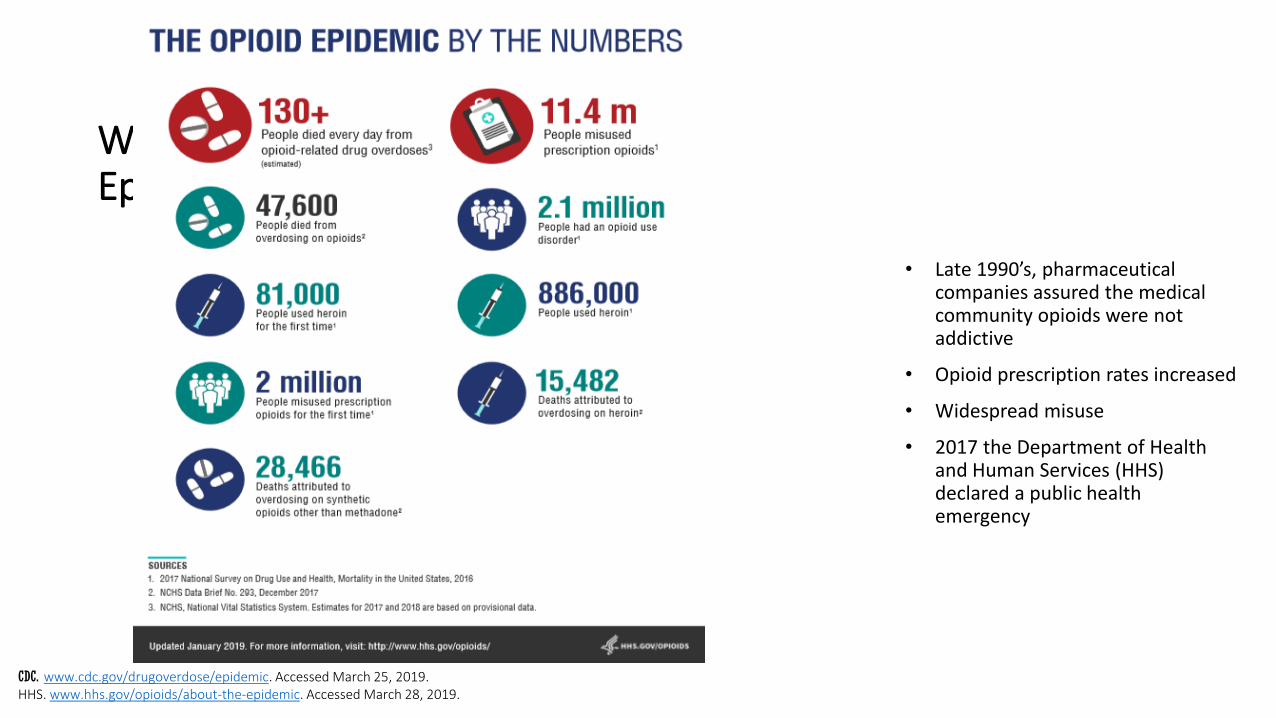
What is the Opioid Epidemic?
• Late 1990’s, pharmaceutical companies assured the medical community opioids were not addictive
• Opioid prescription rates increased
• Widespread misuse
• 2017 the Department of Health and Human Services (HHS) declared a public health emergency
CDC. www.cdc.gov/drugoverdose/epidemic. Accessed March 25, 2019.HHS. www.hhs.gov/opioids/about-the-epidemic. Accessed March 28, 2019.
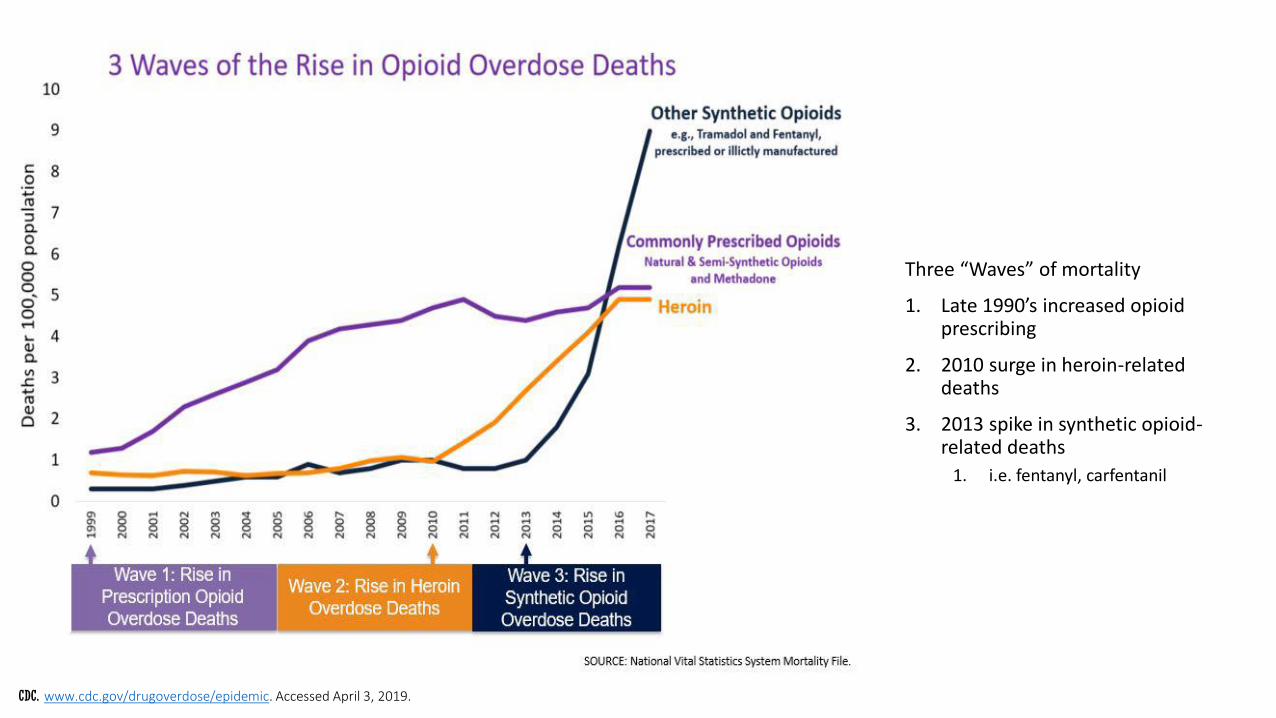
Opioid-related deaths
Three “Waves” of mortality
1. Late 1990’s increased opioid prescribing
2. 2010 surge in heroin-related deaths
3. 2013 spike in synthetic opioid-related deaths
1. i.e. fentanyl, carfentanil
CDC. www.cdc.gov/drugoverdose/epidemic. Accessed April 3, 2019.
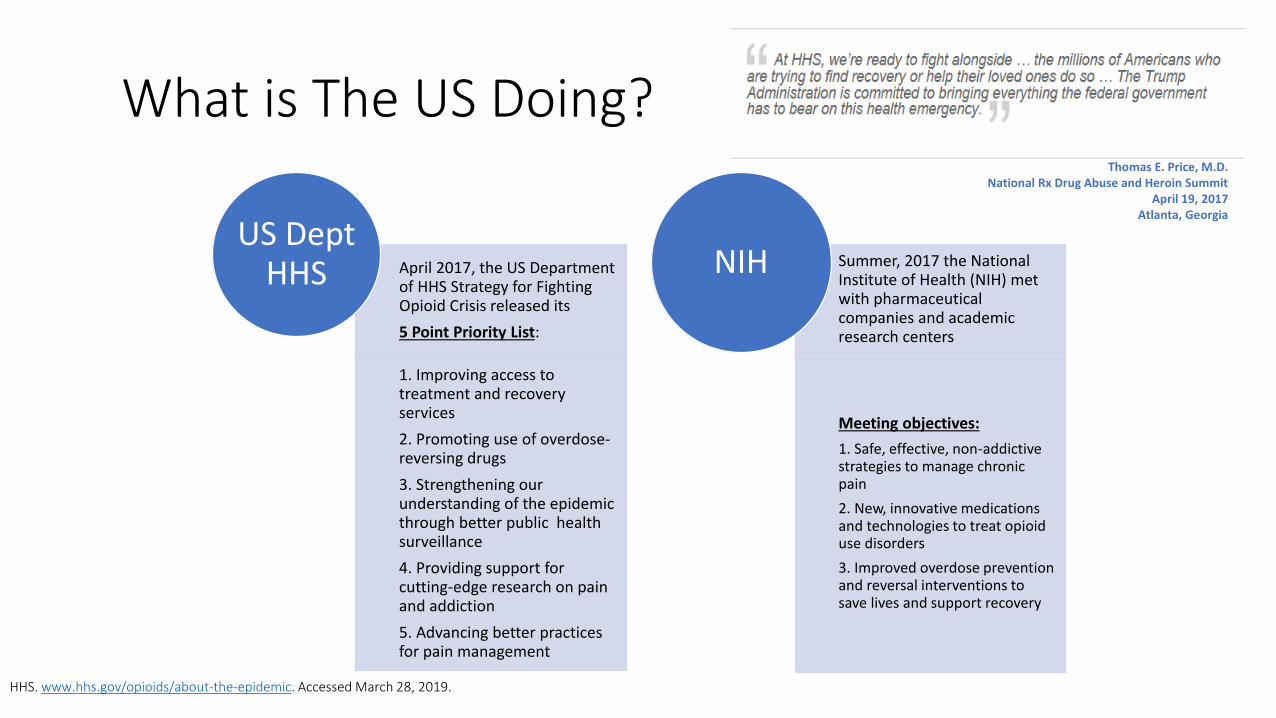
What is The US Doing?
April 2017, the US Department of HHS Strategy for Fighting Opioid Crisis released its
5 Point Priority List:
1. Improving access to treatment and recovery services
2. Promoting use of overdose-reversing drugs
3. Strengthening our understanding of the epidemic through better public health surveillance
4. Providing support for cutting-edge research on pain and addiction
5. Advancing better practices for pain management
US Dept HHS
Summer, 2017 the National Institute of Health (NIH) met with pharmaceutical companies and academic research centers
Meeting objectives:
1. Safe, effective, non-addictive strategies to manage chronic pain
2. New, innovative medications and technologies to treat opioid use disorders
3. Improved overdose prevention and reversal interventions to save lives and support recovery
NIH
HHS. www.hhs.gov/opioids/about-the-epidemic. Accessed March 28, 2019.
Thomas E. Price, M.D.National Rx Drug Abuse and Heroin Summit
April 19, 2017Atlanta, Georgia
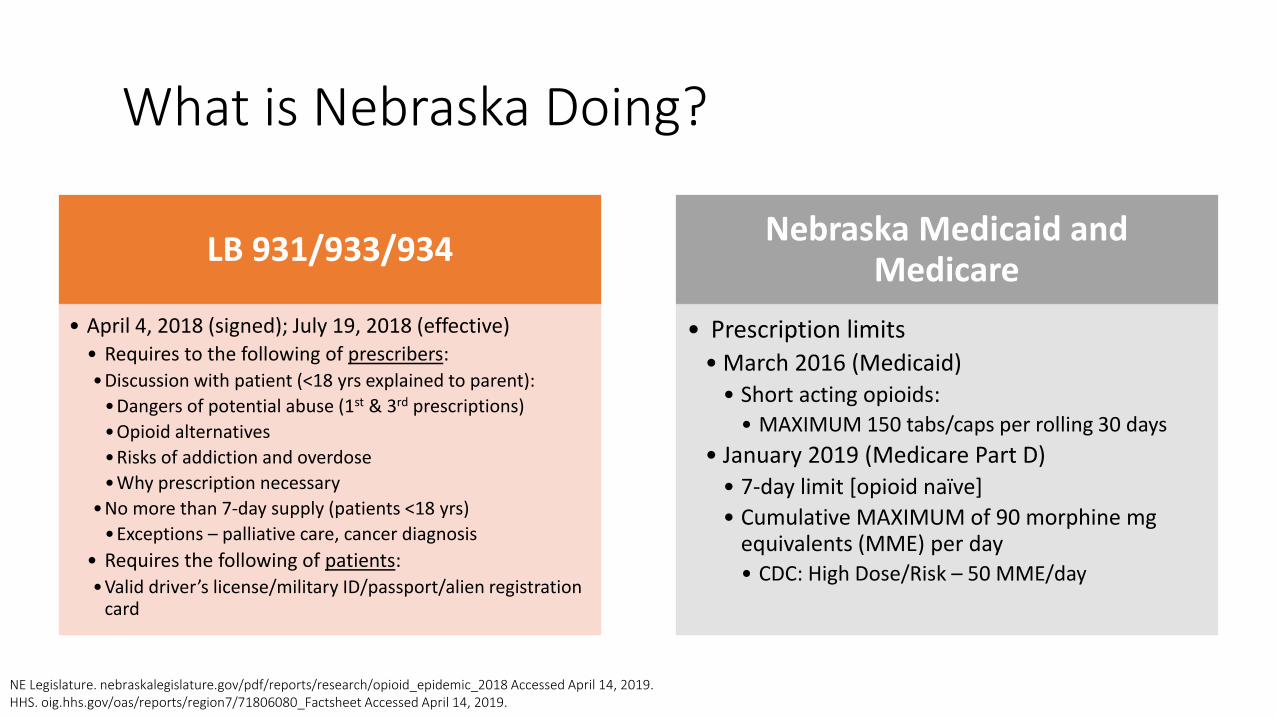
What is Nebraska Doing?
LB 931/933/934
• April 4, 2018 (signed); July 19, 2018 (effective)• Requires to the following of prescribers:•Discussion with patient (<18 yrs explained to parent):
•Dangers of potential abuse (1st & 3rd prescriptions)
•Opioid alternatives
•Risks of addiction and overdose
•Why prescription necessary
•No more than 7-day supply (patients <18 yrs)
•Exceptions – palliative care, cancer diagnosis
• Requires the following of patients:•Valid driver’s license/military ID/passport/alien registration
card
Nebraska Medicaid and Medicare
• Prescription limits• March 2016 (Medicaid)
• Short acting opioids: • MAXIMUM 150 tabs/caps per rolling 30 days
• January 2019 (Medicare Part D)• 7-day limit [opioid naïve]
• Cumulative MAXIMUM of 90 morphine mg equivalents (MME) per day• CDC: High Dose/Risk – 50 MME/day
NE Legislature. nebraskalegislature.gov/pdf/reports/research/opioid_epidemic_2018 Accessed April 14, 2019.HHS. oig.hhs.gov/oas/reports/region7/71806080_Factsheet Accessed April 14, 2019.
How can Pharmacists Help?KNOW THE ALTERNATIVES!
Common Pain Syndromes Presenting to the Emergency Department
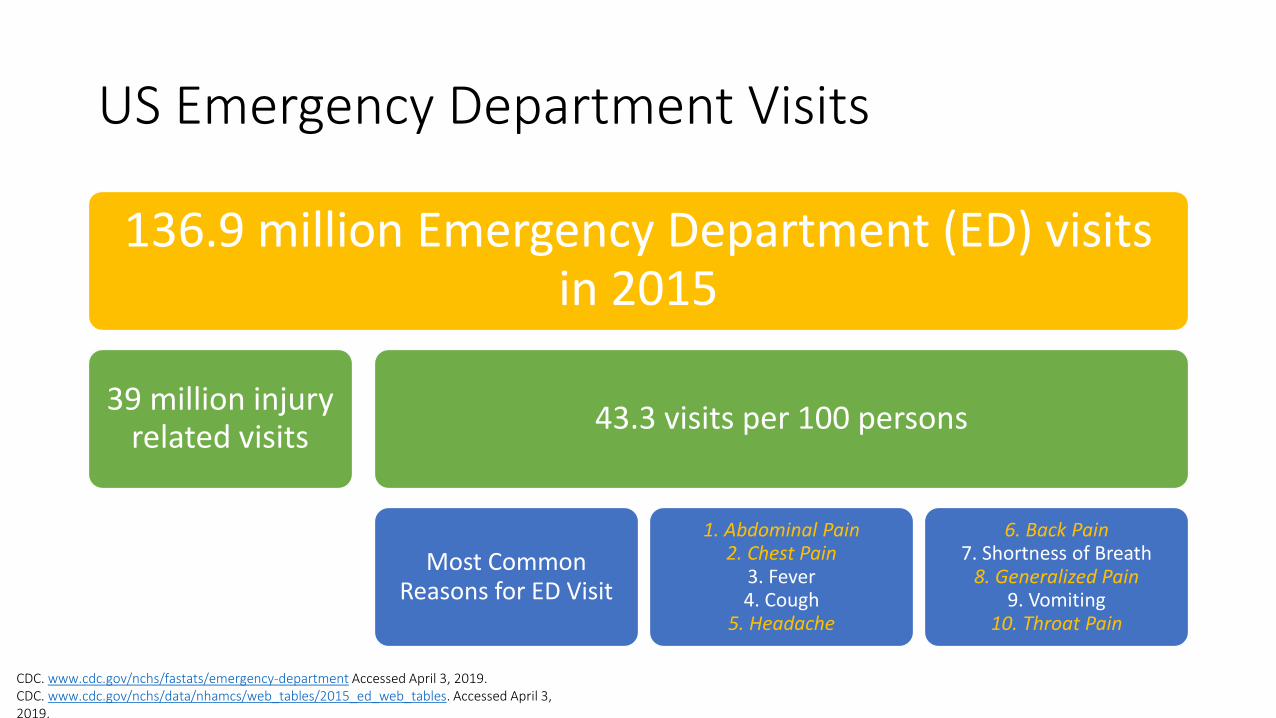
US Emergency Department Visits
136.9 million Emergency Department (ED) visits in 2015
39 million injury related visits
43.3 visits per 100 persons
Most Common Reasons for ED Visit
1. Abdominal Pain2. Chest Pain
3. Fever4. Cough
5. Headache
6. Back Pain7. Shortness of Breath
8. Generalized Pain9. Vomiting
10. Throat Pain
CDC. www.cdc.gov/nchs/fastats/emergency-department Accessed April 3, 2019.CDC. www.cdc.gov/nchs/data/nhamcs/web_tables/2015_ed_web_tables. Accessed April 3, 2019.
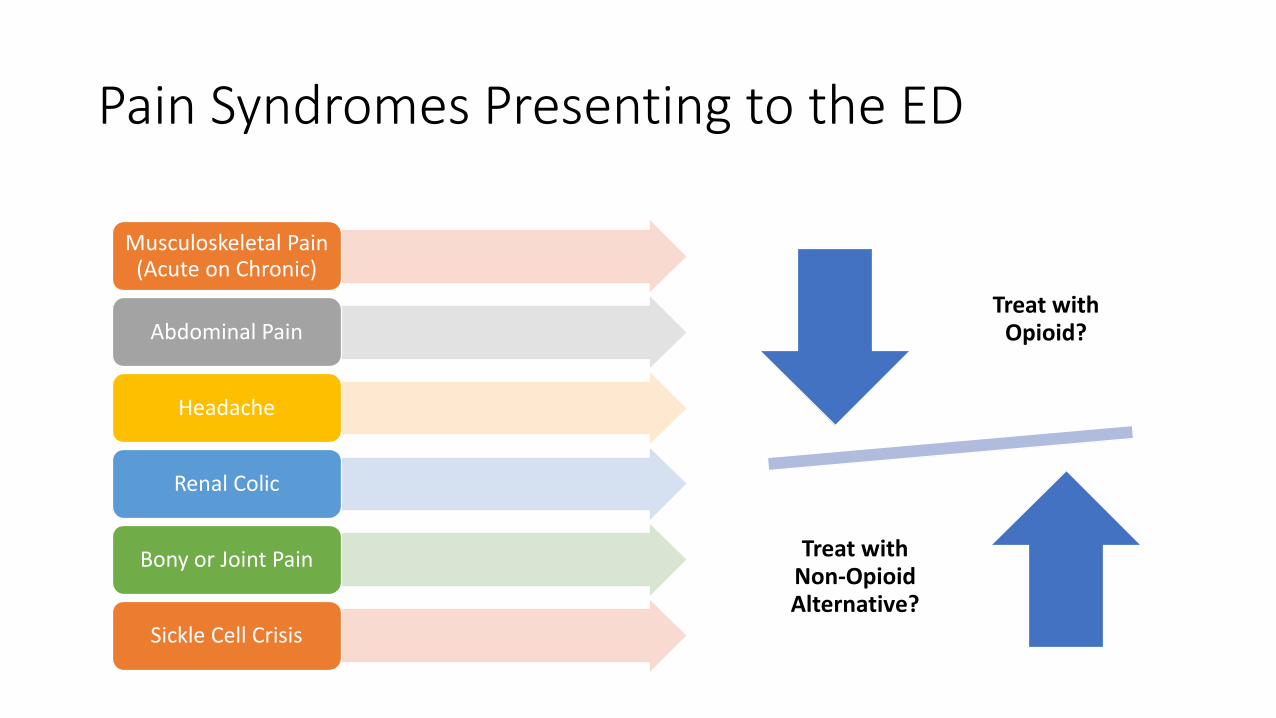
Pain Syndromes Presenting to the ED
Musculoskeletal Pain (Acute on Chronic)
Abdominal Pain
Headache
Renal Colic
Bony or Joint Pain
Sickle Cell Crisis
Treat with Opioid?
Treat with Non-Opioid Alternative?
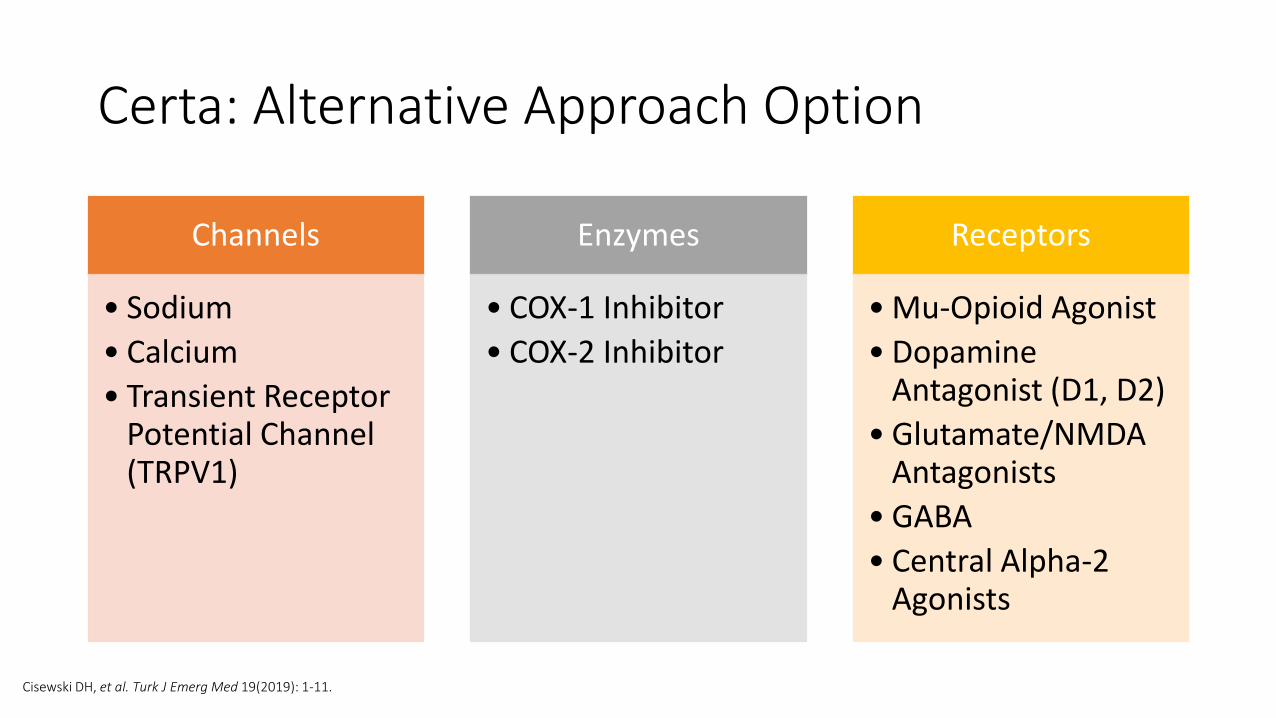
Certa: Alternative Approach Option
Channels
• Sodium
• Calcium
• Transient Receptor Potential Channel (TRPV1)
Enzymes
• COX-1 Inhibitor
• COX-2 Inhibitor
Receptors
• Mu-Opioid Agonist
• Dopamine Antagonist (D1, D2)
• Glutamate/NMDA Antagonists
• GABA
• Central Alpha-2 Agonists
Cisewski DH, et al. Turk J Emerg Med 19(2019): 1-11.
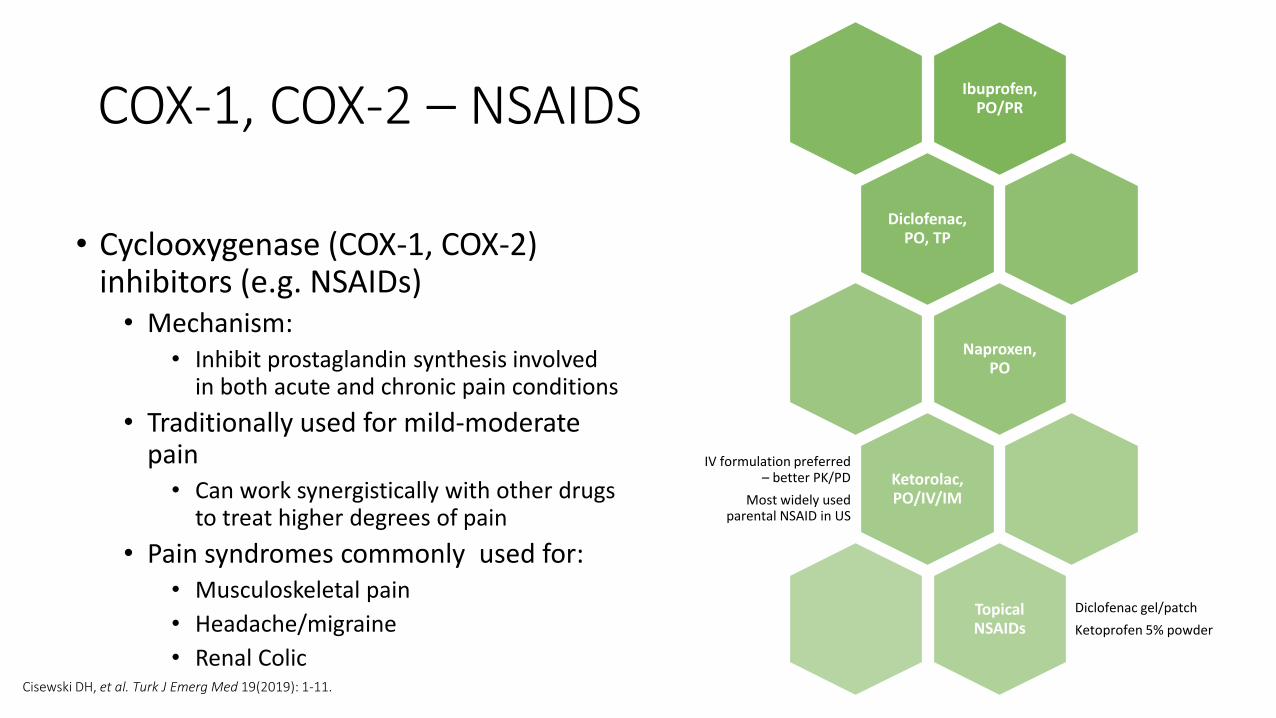
COX-1, COX-2 – NSAIDS
• Cyclooxygenase (COX-1, COX-2) inhibitors (e.g. NSAIDs)• Mechanism:
• Inhibit prostaglandin synthesis involved in both acute and chronic pain conditions
• Traditionally used for mild-moderate pain • Can work synergistically with other drugs
to treat higher degrees of pain
• Pain syndromes commonly used for:• Musculoskeletal pain
• Headache/migraine
• Renal Colic
Ibuprofen, PO/PR
Diclofenac, PO, TP
Naproxen, PO
Ketorolac, PO/IV/IM
IV formulation preferred – better PK/PD
Most widely used parental NSAID in US
Topical NSAIDs
Diclofenac gel/patch
Ketoprofen 5% powder
Cisewski DH, et al. Turk J Emerg Med 19(2019): 1-11.
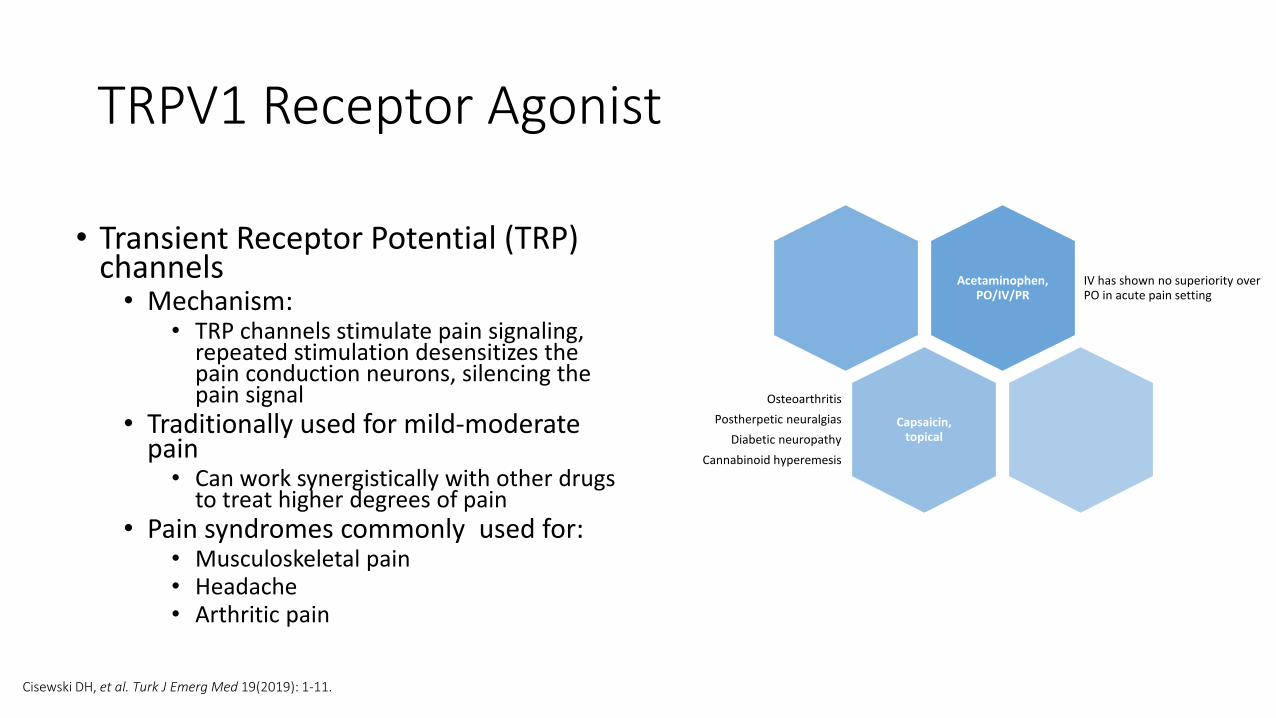
TRPV1 Receptor Agonist
• Transient Receptor Potential (TRP) channels• Mechanism:
• TRP channels stimulate pain signaling, repeated stimulation desensitizes the pain conduction neurons, silencing the pain signal
• Traditionally used for mild-moderate pain • Can work synergistically with other drugs
to treat higher degrees of pain• Pain syndromes commonly used for:
• Musculoskeletal pain• Headache• Arthritic pain
Acetaminophen, PO/IV/PR
IV has shown no superiority over PO in acute pain setting
Capsaicin, topical
Osteoarthritis
Postherpetic neuralgias
Diabetic neuropathy
Cannabinoid hyperemesis
Cisewski DH, et al. Turk J Emerg Med 19(2019): 1-11.
capsaicin• Primary pungent ingredient in hot chili
peppers
• Used topically (OTC patches, lotions and creams)
• Indications for use:
Clinical Pharmacology. www.clinicalpharmacology.com. Accessed April 3, 2019.
Sodium Channel Blockers
• Local anesthetic agents (e.g. lidocaine, bupivacaine)• Mechanism:
• Non-competitive inhibition of nerve signal dissemination
• Nerve blocks (regional anesthesia)• Infiltration of peripheral nerves creating localized
analgesic relief • Efficacy enhanced when used in combination• Pain syndromes commonly used for:
• Localized procedures (i.e. laceration repairs, abscess drainage, chest tube placement)
• Fractures and reductions• Headache/migraine
Lidocaine, ID/IV
Bupivacaine, ID
Cisewski DH, et al. Turk J Emerg Med 19(2019): 1-11.
Trigger Point Injections
• Trigger Points: palpable, tense bands of skeletal muscle fibers • When compressed – local and referred pain
• Sensitized nerve endings/fibers (nociceptors) can cause dysfunctional nerve endplates thus leading to pain • Disruption of trigger points mechanically by needle or local anesthetic results in relaxation and/or
lengthening of the muscle fibers
• Local vasodilation, dilution, and removal of the accumulated nociceptive substrates (i.e. acetylcholine)
• Treatment Options:• Local anesthetic or dry needling injections• Found to be helpful with:
• Headaches, lower back pain, other musculoskeletal pain syndromes
• How?• Direct visualization of trigger point(s) and/or nerve region(s) via ultrasound
Wong CSM and Wing SHS. Anesthesiol Res Pact 2012; 2012:492-452.
Off-Label Use of Lidocaine
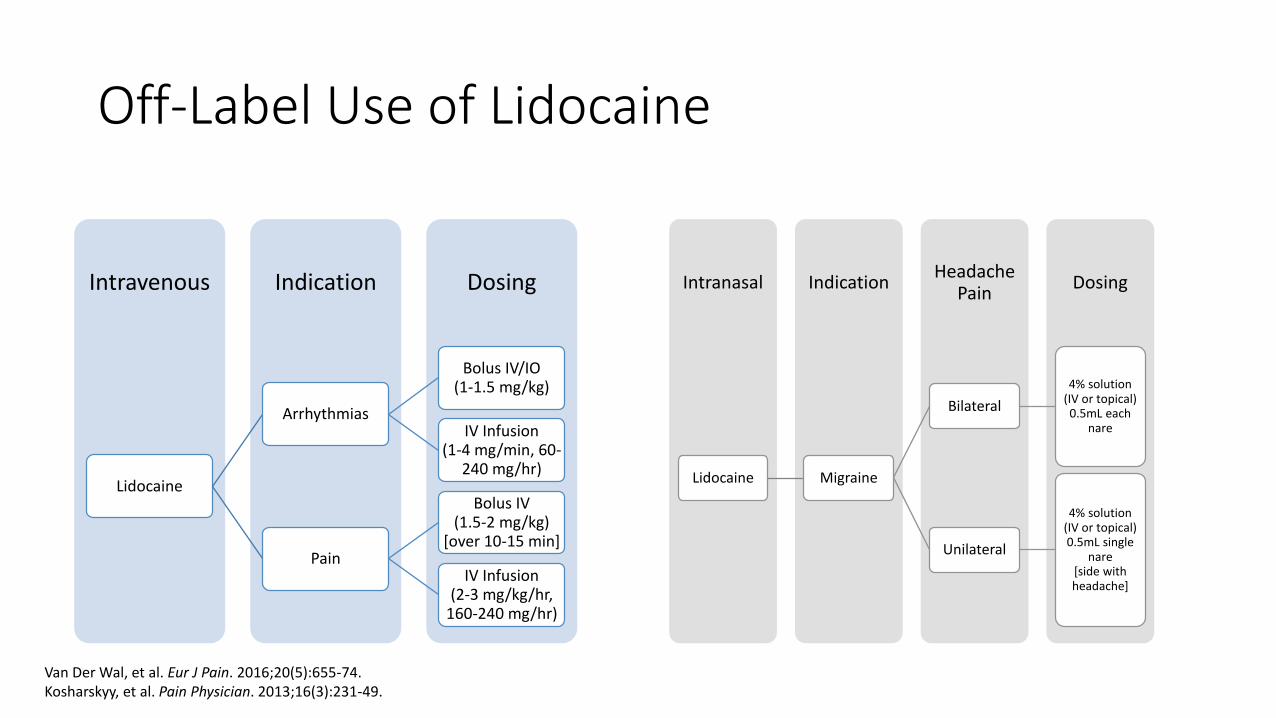
DosingIndicationIntravenous
Lidocaine
Arrhythmias
Bolus IV/IO (1-1.5 mg/kg)
IV Infusion (1-4 mg/min, 60-
240 mg/hr)
Pain
Bolus IV (1.5-2 mg/kg)
[over 10-15 min]
IV Infusion (2-3 mg/kg/hr,
160-240 mg/hr)
DosingHeadache
PainIndicationIntranasal
Lidocaine Migraine
Bilateral
4% solution (IV or topical) 0.5mL each
nare
Unilateral
4% solution (IV or topical) 0.5mL single
nare[side with headache]
Van Der Wal, et al. Eur J Pain. 2016;20(5):655-74.Kosharskyy, et al. Pain Physician. 2013;16(3):231-49.
Local Anesthetic Toxicity
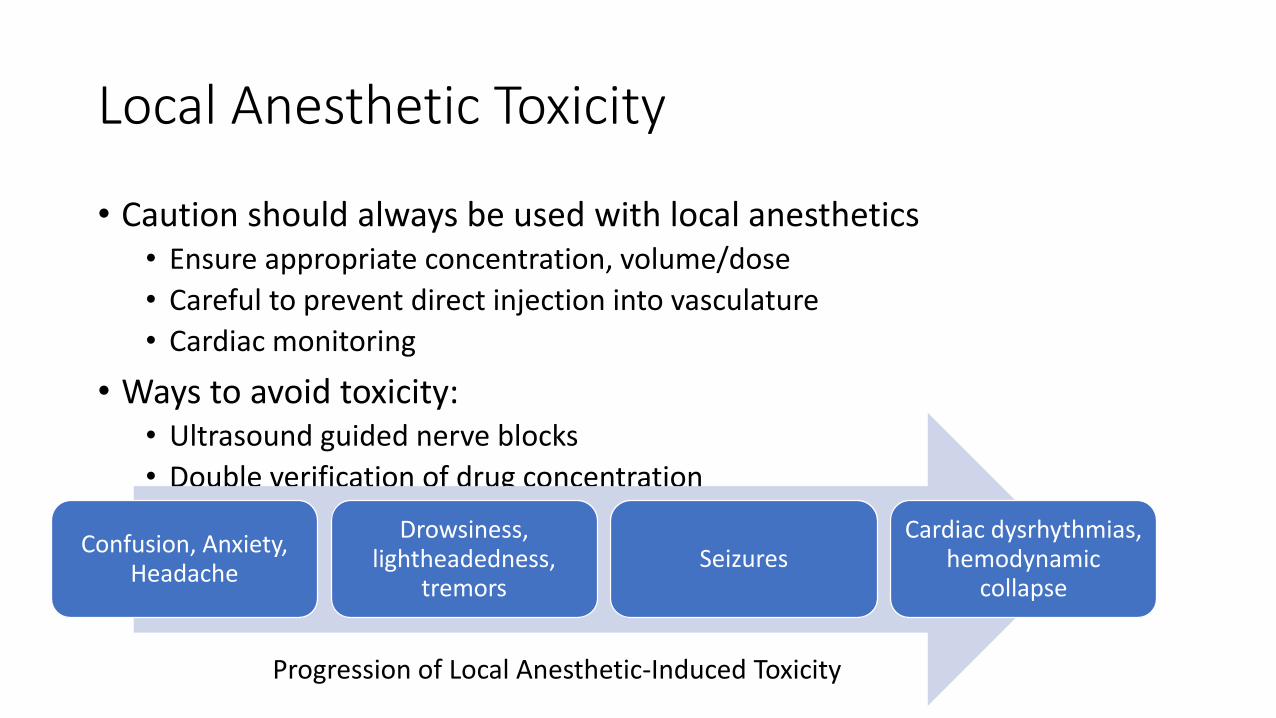
• Caution should always be used with local anesthetics• Ensure appropriate concentration, volume/dose
• Careful to prevent direct injection into vasculature
• Cardiac monitoring
• Ways to avoid toxicity:• Ultrasound guided nerve blocks
• Double verification of drug concentration
Confusion, Anxiety, Headache
Drowsiness, lightheadedness,
tremorsSeizures
Cardiac dysrhythmias, hemodynamic
collapse
Progression of Local Anesthetic-Induced Toxicity
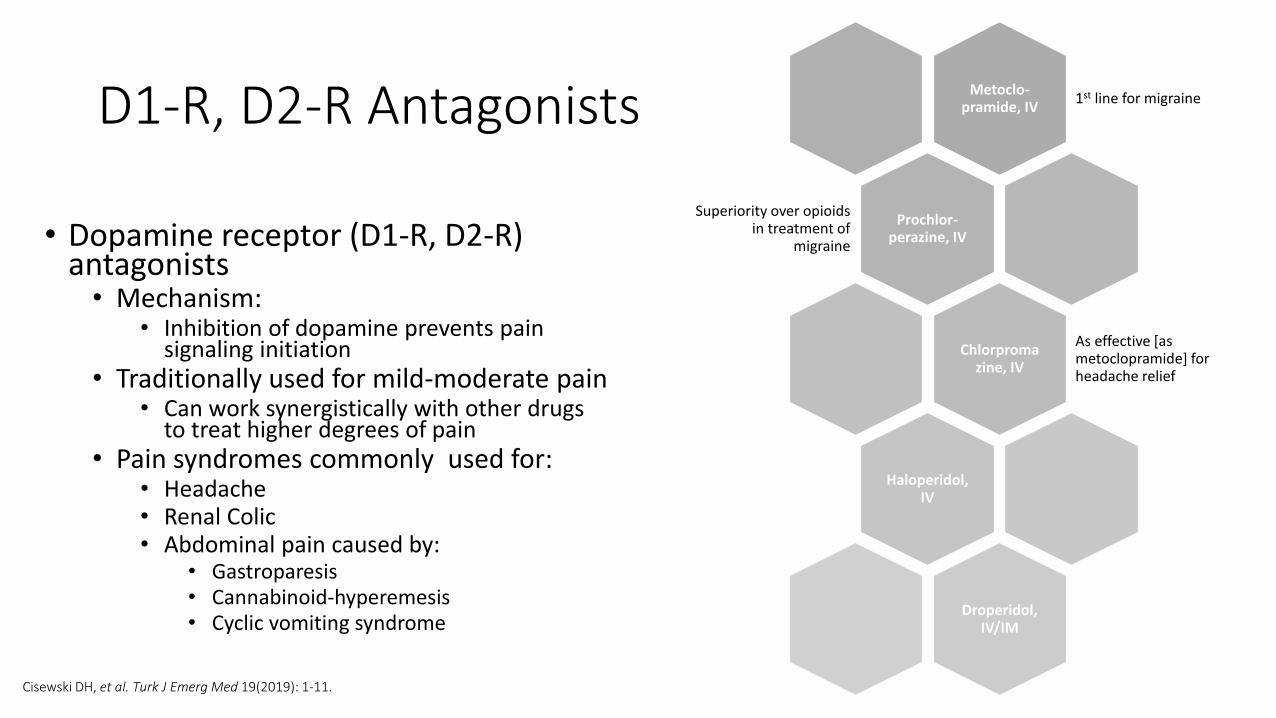
D1-R, D2-R Antagonists
• Dopamine receptor (D1-R, D2-R) antagonists• Mechanism:
• Inhibition of dopamine prevents pain signaling initiation
• Traditionally used for mild-moderate pain • Can work synergistically with other drugs
to treat higher degrees of pain• Pain syndromes commonly used for:
• Headache• Renal Colic• Abdominal pain caused by:
• Gastroparesis• Cannabinoid-hyperemesis • Cyclic vomiting syndrome
Metoclo-pramide, IV
1st line for migraine
Prochlor-perazine, IV
Superiority over opioids in treatment of
migraine
Chlorpromazine, IV
As effective [as metoclopramide] for headache relief
Haloperidol, IV
Droperidol, IV/IM
Cisewski DH, et al. Turk J Emerg Med 19(2019): 1-11.
Droperidol
• Butyrophenone derivative, structurally similar to haloperidol, with potent central dopamine antagonism • More potent antiemetic than antipsychotic properties (as compared to haloperidol)• BLACK BOX WARNING (2001)
• QT prolongation and torsade de pointes
• 2.5-5 mg IV or IM dosing• With lower dosing, adverse events reported are rare
• Extrapyramidal symptoms and sedation most common• Cardiac side effects rarely reported with lower dosing
• Cardiac monitoring • Baseline EKG
• Onset of action ~3-10 minutes (IV or IM)• Peak effect ~30 minutes • Duration of action ~2-4 hours
Clinical Pharmacology. www.clinicalpharmacology.com. Accessed April 10, 2019.Thomas MC, et al. Ann Pharmacother 2015 Feb; 49(2):233-40.
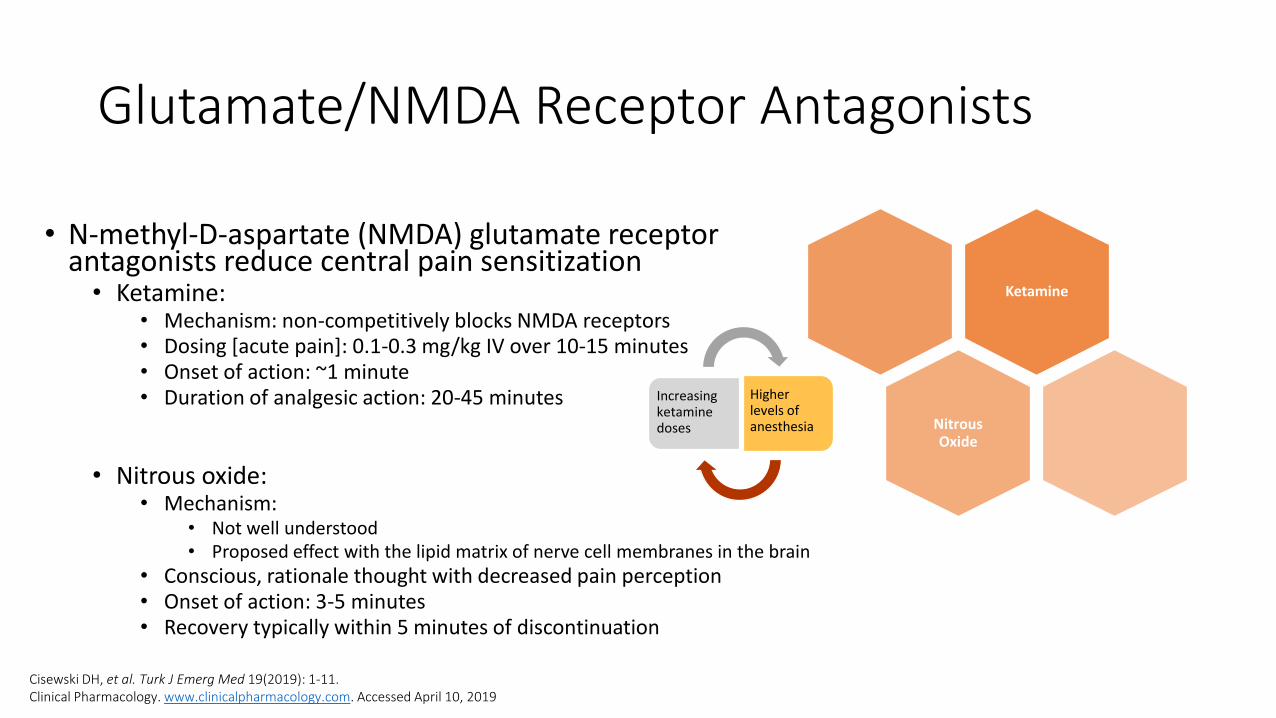
Glutamate/NMDA Receptor Antagonists
• N-methyl-D-aspartate (NMDA) glutamate receptor antagonists reduce central pain sensitization • Ketamine:
• Mechanism: non-competitively blocks NMDA receptors• Dosing [acute pain]: 0.1-0.3 mg/kg IV over 10-15 minutes • Onset of action: ~1 minute• Duration of analgesic action: 20-45 minutes
• Nitrous oxide:• Mechanism:
• Not well understood• Proposed effect with the lipid matrix of nerve cell membranes in the brain
• Conscious, rationale thought with decreased pain perception• Onset of action: 3-5 minutes• Recovery typically within 5 minutes of discontinuation
Ketamine
Nitrous Oxide
Cisewski DH, et al. Turk J Emerg Med 19(2019): 1-11.Clinical Pharmacology. www.clinicalpharmacology.com. Accessed April 10, 2019
Increasing ketamine doses
Higher levels of anesthesia
GABA receptor Agonist
• Gamma-aminobutyric acid (GABA) receptor agonist
• Propofol• Mechanism: Inhibition of the NMDA subtype of glutamate
receptors by channel-gating modulation and agonistic activity of gamma-aminobutyric acid (GABA) receptors
• Enhanced inhibitory synaptic transmission of GABAA receptor agonism
• Dosing [sub-anesthetic dosing]:• 30-40 mg IV x 1, repeating boluses of 10 mg every 3-5 minutes until
pain relief (MAX 120 mg)• Onset of action: ~30-60 seconds• Duration of action: dependent on infusion time; 3-5 minutes
• Indications:• Refractory migraine pain
• Cautions:• Needs continuous pulse oximetry and cardiac monitoring • Needs to be administered in setting in which advanced airway
management is immediately available
Propofol
Cisewski DH, et al. Turk J Emerg Med 19(2019): 1-11.Clinical Pharmacology. www.clinicalpharmacology.com. Accessed April 10, 2019
Serotonin (5HT-1) receptor Agonist
• Serotonin receptor agonists• Mechanism: prevents pain signal transmission by
inhibiting calcitonin gene-related peptide release
• Used in the treatment of headache (migraine and/or cluster headaches)• Can work synergistically with other drugs to treat higher
degrees of pain
• Sumatriptan Dosing:• 6mg SubQ, can repeat in 1 hr if symptoms persist
(MAX 12 mg/24 hrs)
• Cautions:• Paresthesia, flushing, palpitations, drowsiness• American Headache Society: incidence of cardiac side
effects extremely low
Sumatriptan
Cisewski DH, et al. Turk J Emerg Med 19(2019): 1-11.
Calcium Channel Blockers [Anticonvulsants]
• Mechanism: • Reduce central pain sensitization by preventing voltage-gated
postsynaptic neurotransmitter release
• Gabapentin and pregabalin• Pregabalin – increased potency and binding affinity [compared
to gabapentin]
• Indications:• Neuropathic pain
• Post-herpetic and diabetic
• Fibromyalgia
• Cautions/Precautions:• Adverse effects: dizziness, ataxia, peripheral edema, nystagmus,
tremor, angioedema, weight gain • Use with caution in elderly and renal impairment • Do not use in combination with opioids as there is an
enhancement of euphoric effects
Gabapentin
Pregabalin
Cisewski DH, et al. Turk J Emerg Med 19(2019): 1-11.
Other AntiEpileptic Drugs
Valproic Acid• Mechanism:
• Not well understood• Increases CNS concentrations of GABA through
inhibition of enzymes that catabolize GABA and block the reuptake of GABA into nerve endings
• May suppress repetitive neuronal firing through inhibition of voltage-gated sodium channels
• Indications:• Diabetic neuropathy (PO)• Refractory migraine (IV)
• Dosing:• Diabetic neuropathy: increasing titration of PO• Refractory migraine: 500-1000mg IV
• Caution if patient already taking topiramate for migraine prevention
Levetiracetam• Mechanism:
• Not well understood• Varying theories and differences in in-vitro
versus in vivo studies
• Indication:• Few case reports of success in refractory
migraine (IV)
• Dosing:• Refractory migraine: 500-1000mg IV
Rozen TD. Continuum (Minneap Minn) 2015; 21(4): 1004-1017.
Magnesium Sulfate
• Mechanism:• Antagonism of NMDA receptors• Blockade of peripheral neuromuscular transmission through
inhibition of acetylcholine release by motor nerve impulses• Combination?
• Indication:• Refractory migraine
• May work synergistically with other drugs in typical migraine cocktail
• Dosing:• 500-1000mg IV over 30-60 minutes
• Caution if infused too quickly; can cause hypotension
Rozen TD. Continuum (Minneap Minn) 2015; 21(4): 1004-1017.Clinical Pharmacology. www.clinicalpharmacology.com. Accessed April 10, 2019
Magnesium
Dexmedetomidine
• Mechanism: selective, centrally acting alpha2adrenoceptor agonist with sympatholytic, sedative and analgesic properties • Blunts sympathetic response thus causes analgesia
• Indication:• Post-operative pain
• Used synergistically with other agents• Shown to decrease opioid consumption and decrease
opioid-related side effects• Prolongs duration of local anesthetic blockade • Shorter time to anesthesia onset
• Dosing:• 0.5-1 mcg/kg IV• 1-2 mcg/kg intra-nasal
Dexmedetomidine
Cisewski DH, et al. Turk J Emerg Med 19(2019): 1-11.
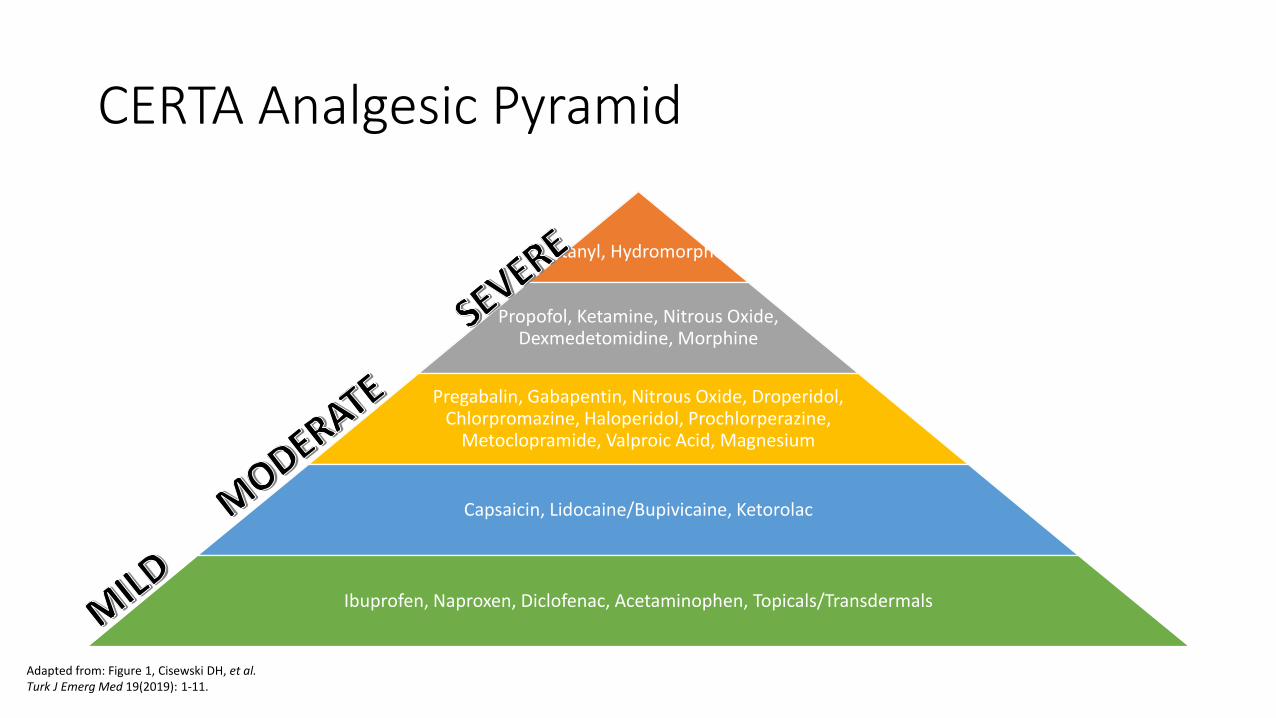
CERTA Analgesic Pyramid
Fentanyl, Hydromorphone
Propofol, Ketamine, Nitrous Oxide, Dexmedetomidine, Morphine
Pregabalin, Gabapentin, Nitrous Oxide, Droperidol, Chlorpromazine, Haloperidol, Prochlorperazine,
Metoclopramide, Valproic Acid, Magnesium
Capsaicin, Lidocaine/Bupivicaine, Ketorolac
Ibuprofen, Naproxen, Diclofenac, Acetaminophen, Topicals/Transdermals
Adapted from: Figure 1, Cisewski DH, et al.Turk J Emerg Med 19(2019): 1-11.
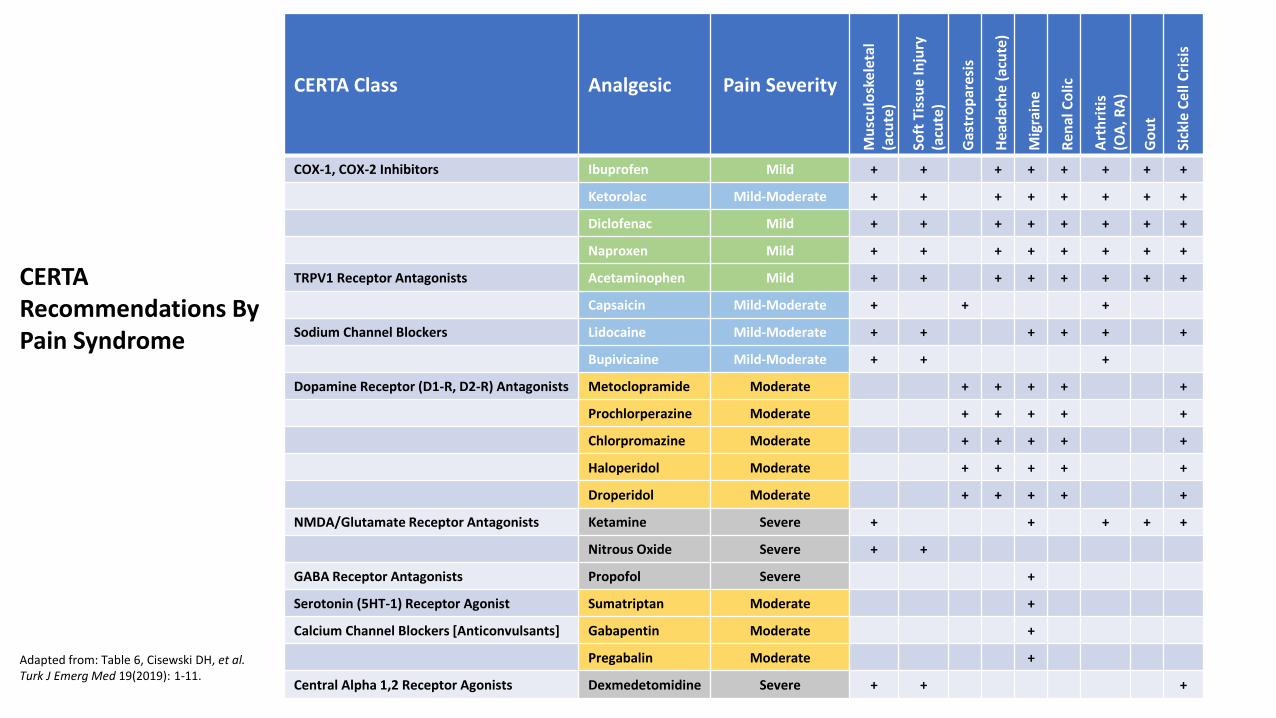
CERTA Class Analgesic Pain Severity
Mu
scu
losk
elet
al
(acu
te)
Soft
Tis
sue
Inju
ry
(acu
te)
Gas
tro
par
esis
Hea
dac
he
(acu
te)
Mig
rain
e
Ren
al C
olic
Art
hri
tis
(OA
, RA
)
Go
ut
Sick
le C
ell
Cri
sis
COX-1, COX-2 Inhibitors Ibuprofen Mild + + + + + + + +
Ketorolac Mild-Moderate + + + + + + + +
Diclofenac Mild + + + + + + + +
Naproxen Mild + + + + + + + +
TRPV1 Receptor Antagonists Acetaminophen Mild + + + + + + + +
Capsaicin Mild-Moderate + + +
Sodium Channel Blockers Lidocaine Mild-Moderate + + + + + +
Bupivicaine Mild-Moderate + + +
Dopamine Receptor (D1-R, D2-R) Antagonists Metoclopramide Moderate + + + + +
Prochlorperazine Moderate + + + + +
Chlorpromazine Moderate + + + + +
Haloperidol Moderate + + + + +
Droperidol Moderate + + + + +
NMDA/Glutamate Receptor Antagonists Ketamine Severe + + + + +
Nitrous Oxide Severe + +
GABA Receptor Antagonists Propofol Severe +
Serotonin (5HT-1) Receptor Agonist Sumatriptan Moderate +
Calcium Channel Blockers [Anticonvulsants] Gabapentin Moderate +
Pregabalin Moderate +
Central Alpha 1,2 Receptor Agonists Dexmedetomidine Severe + + +
Adapted from: Table 6, Cisewski DH, et al.Turk J Emerg Med 19(2019): 1-11.
CERTA Recommendations By Pain Syndrome
Opioid-Free Days
• Maimonides Medical Center (Brooklyn, NY)• >130,000 ED visits/year • >100 bed ED• Academic medical center
• 48 residents (emergency medicine)• >40 FTE ED attending physicians • 1 PGY2 emergency medicine pharmacy resident
• Trialed an “Opioid-Free” 8-hour Shift • 17 patients included (pain chief complaint)
• 12 acute pain and 5 chronic pain
• Utilized CERTA strategies to manage pain• Majority of patients treated with IV ketorolac and oral ibuprofen • One patient required rescue opioid therapy
Cohen V, et al. Am J Health-Syst Pharm 2015; 72:2080-2086.
Opioid Stewardship
• Emergency Department • ED Opioid Stewardship Team
• Resident completed MUE to evaluate current prescribing rates and trends
• Changing EMR defaults with opioid prescriptions [discharge]
• Creating provider “report cards” for opioid prescribing habits/trends
• Opioid Alternative Pocket Cards for providers
• Enhanced resident education
• Ongoing resident projects to evaluate the impact of our changes
• All Hospital• Acute Pain Steering Committee• Pain Stewardship Pharmacist
• EMR reports for pharmacist review
• EMR MME Calculator [discharge prescriptions]
• Updated order-sets
• Removal of combo-opioids
• Removal ability to order both PO and IV opioids
• Scheduled acetaminophen and NSAIDs
• 48 hour stop time for all IV opioids (some exceptions)
• Enhanced staff education• Encourage patients to set realistic pain-goal
expectationsSustained patient satisfaction scores despite opioid reduction strategies
Nebraska Medicine
Summary
1. Numerous different pain syndromes have been studied examining different non-opioid treatment strategies with positive outcomes
2. Consider utilizing a CERTA pain management approach
3. Consider different opioid stewardship strategies at your institution/place of work to decrease opioid utilization and help combat the Opioid Crisis
Assessment Questions
• Which of the following is NOT in the top 10 reasons for ED presentation?
A. Abdominal Pain
B. Headache
C. Chest Pain
D. Dental Pain
E. None of the above
Assessment Questions
• Which of the following is NOT in the top 10 reasons for ED presentation?
A. Abdominal Pain
B. Headache
C. Chest Pain
D. Dental Pain
E. None of the above
Assessment Questions
• Which of the following is NOT considered a non-opioid option for pain management?A. Propofol
B. Ketamine
C. Fentanyl
D. Dexmedetomidine
E. All of the above
Assessment Questions
• Which of the following is NOT considered a non-opioid option for pain management?A. Propofol
B. Ketamine
C. Fentanyl
D. Dexmedetomidine
E. All of the above
References
• Centers for Disease Control and Prevention. www.cdc.gov/drugoverdose/epidemic. Accessed March 25, 2019.
• Centers for Disease Control and Prevention. www.cdc.gov/nchs/fastats/emergency-department Accessed April 3, 2019.
• Centers for Disease Control and Prevention. www.cdc.gov/nchs/data/nhamcs/web_tables/2015_ed_web_tables. Accessed April 3, 2019.
• Clinical Pharmacology [database online]. Tampa, FL: Gold Standard, Inc.; 2019. www.clinicalpharmacology.com. Updated October 2016. Accessed April 3, 2019.
• Clinical Pharmacology [database online]. Tampa, FL: Gold Standard, Inc.; 2019. www.clinicalpharmacology.com. Updated July 2015. Accessed April 10, 2019.
• Clinical Pharmacology [database online]. Tampa, FL: Gold Standard, Inc.; 2019. www.clinicalpharmacology.com. Updated July 2016. Accessed April 10, 2019.
• Clinical Pharmacology [database online]. Tampa, FL: Gold Standard, Inc.; 2019. www.clinicalpharmacology.com. Updated August 2016. Accessed April 10, 2019.
• Clinical Pharmacology [database online]. Tampa, FL: Gold Standard, Inc.; 2019. www.clinicalpharmacology.com. Updated March 2019. Accessed April 10, 2019.
• Cohen V, Motov S, Rockoff B, et al. Development of an opioid reduction protocol in an emergency department. Am J Health-Syst Pharm 2015; 72:2080-2086.
• Department of Health and Human Services. www.hhs.gov/opioids/about-the-epidemic. Accessed March 28, 2019.
• Department of Health and Human Services. https://oig.hhs.gov/oas/reports/region7/71806080_Factsheet.pdf. Accessed April 14, 2019.
• Cisewski DH and Motov SM. Essential pharmacologic options for acute pain management in the emergency setting. Turk J Emerg Med 19(2019): 1-11.
• Van Der Wal, et al. The in vitro mechanisms and in vivo efficacy of intravenous lidocaine on the neuroinflammatory response in acute and chronic pain. Eur J Pain. 2016;20(5):655-74.
• Kosharskyy, et al. Intravenous infusions in chronic pain management. Pain Physician. 2013;16(3):231-49.
• NE Legislature. nebraskalegislature.gov/pdf/reports/research/opioid_epidemic_2018 Accessed April 14, 2019.
• Rozen TD. Emergency department and inpatient management of status migrainosus and intractable headache. Continuum (Minneap Minn) 2015; 21(4): 1004-1017.
• Thomas MC, Musselman ME, and Shewmaker J. Droperidol for the treatment of acute migraine headaches. Ann Pharmacother 2015 Feb; 49(2):233-40.
• Wong CSM and Wing SHS. A new look at trigger point injections. Anesthesiol Res Pact 2012; 2012:492-452.
Non-Opioid Alternatives to Pain Management
Krysta Baack, PharmD, BCPS
Nebraska Medicine














![Original Article Tocilizumab infusion therapy normalizes ... Papers...sALS patients, but previous anti-inflammatory approach with the cyclooxygenase-2 (COX-2) inhibitor celecoxib [8]](https://img.pdfslide.us/doc/110x75/60f96bbd0ba77f202104e787/original-article-tocilizumab-infusion-therapy-normalizes-papers-sals-patients.jpg)




![Colon, Rectal, and Anal Cancers¬¬13...(NSAIDs) such as sulindac (Clinoril, nonspecific COX-1 [cyclo-oxygenase-1] and COX-2 inhibitor) and celecoxib (Celebrex, COX-2 inhibitor) has](https://img.pdfslide.us/doc/110x75/5e8a4462b031bf73bf0f6eae/colon-rectal-and-anal-13-nsaids-such-as-sulindac-clinoril-nonspecific.jpg)