Embed Size (px)
Citation preview

Non-invasive Magnetic Resonance Myelography in Spontaneous Spinal
Cerebrospinal Fluid (CSF) Leak
Adam Liudahl, MDDiagnostic Radiology Resident
Bruno Policeni, MDStaff Neuroradiologist
Toshio Moritani, MDStaff Neuroradiologist
Aristides A. Capizzano, MDStaff Neuroradiologist
University of Iowa Hospitals & Clinics, Iowa City, IA
Control #479; eEdE-231

Financial Disclosures
• Authors have no financial disclosures to report
Outline
• Background• Anatomy • Review of available imaging modalities• Studies in the literature• Case Examples
Spontaneous Spinal CSF Leak
• Alternatively, Spontaneous intracranial hypotension, Cerebral spinal fluid (CSF) leak, spontaneous CSF hypovolemia.
• Syndrome consisting of a constellation of neurological symptoms (most commonly postural or orthostatic headache) and a CSF leak within the spinal axis

Spontaneous Spinal CSF Leak
• Exact cause unknown. *CSF leaks can occur from iatrogenic causes and uncommonly from intradural osteophyte leading to spinal dural tear.
• Possible cause is structural weakness of the spinal meninges, but likely multifactorial.
• CSF leak size is variable ranging from minimal amount during Valsalva to large amounts in paraspinal regions.

Spontaneous Spinal CSF Leak
• No large scale study examining incidence or prevalence
• Estimated at 5 per 100,000 in 2003/04 study• Female predominance, M:F of 2:1.1 • Typically in 30-50 years of age; peak incidence
around 40 years old
Definition/Diagnostic Criteria
Definition: Symptomatic leakage of CSF.Diagnostic criteria for headache attributed to spontaneous intracranial hypotension (SIH), according to International Classification of Headache Disorders, 3rd edition (ICHD-3):
A) any headache fulfilling criteria B through DB) low CSF pressure (<60 mm H20) and/or evidence of CSF leakage on imagingC) headache has developed in temporal relation to the low CSF pressure or CSF leakage, or has led to its discoveryD) not better accounted for by another ICHD-3 diagnosis
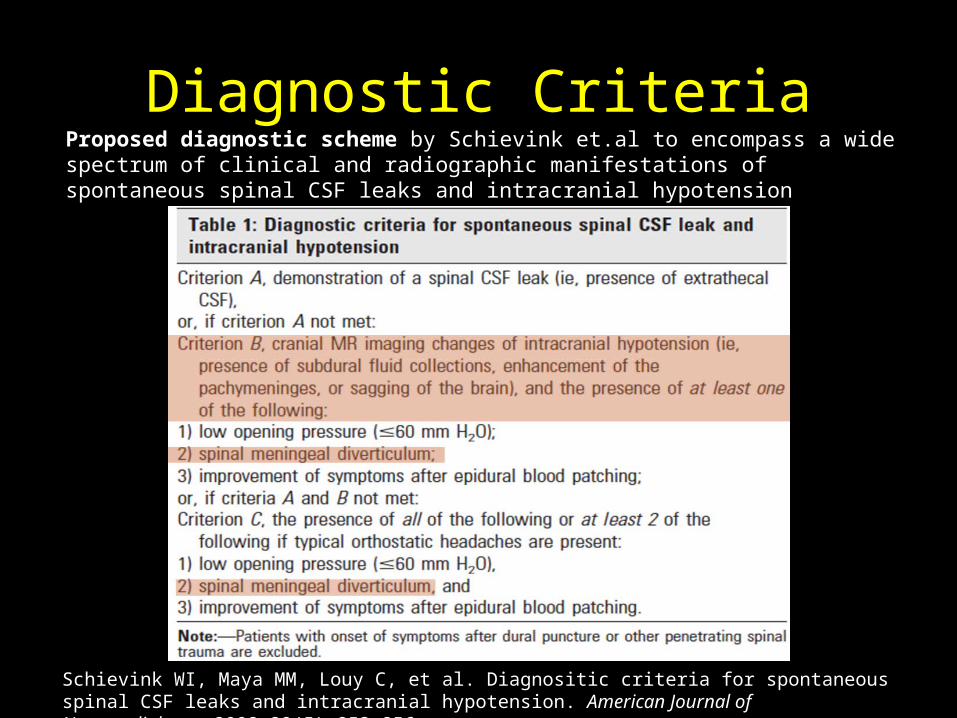
Diagnostic CriteriaProposed diagnostic scheme by Schievink et.al to encompass a wide spectrum of clinical and radiographic manifestations of spontaneous spinal CSF leaks and intracranial hypotension
Schievink WI, Maya MM, Louy C, et al. Diagnositic criteria for spontaneous spinal CSF leaks and intracranial hypotension. American Journal of Neuroradiology, 2008;29(5):853-856.
Treatment
• Conservative treatment– Bedrest, hydration and analgesics
• Epidural blood patch– Autologous blood or Fibrin glue sealant– Simple mass effect (both) & clotting (blood)– “Directed” patch more efficacious
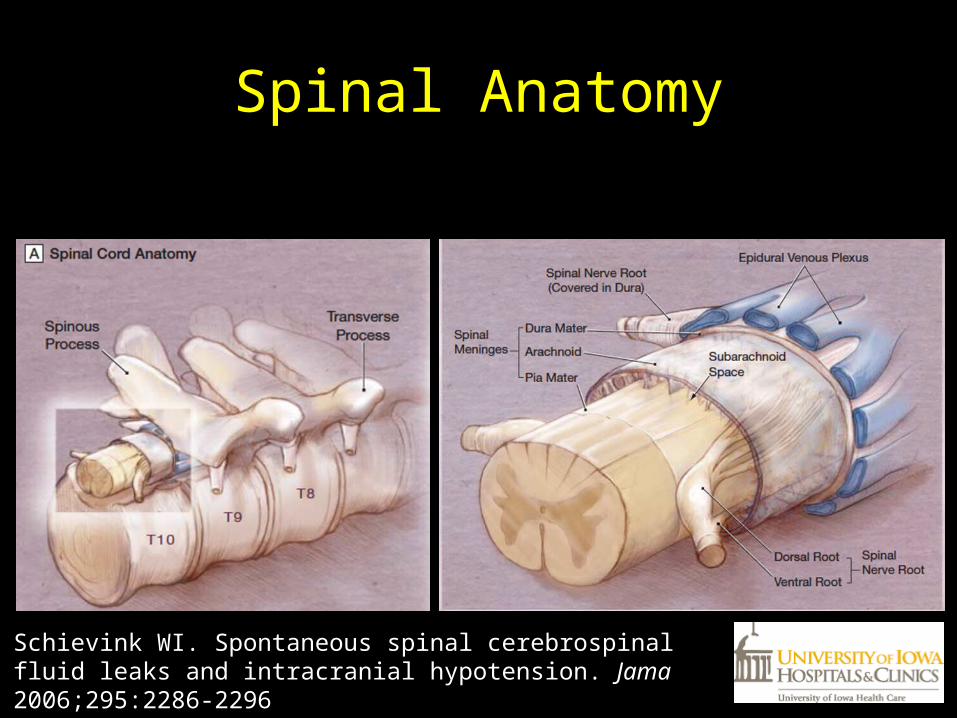
Spinal Anatomy
Schievink WI. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. Jama 2006;295:2286-2296
CSF hydrodynamics- Traditional Model
• CSF produced by choroid plexuses
• Flow from ventricles to subarachnoid spaces
• Resorbed by arachnoid villi
- New Model
• CSF produced and resorbed by the entire CSF-interstitial fluid unit
• Choroid plexuses, arachnoid villi and lymphatics have minor roles
• Formation and resorption occurs across walls of CNS blood capillaries
• CSF volume depends on hydrostatic and osmotic forces between capillaries and CSF-interstitial fluid unit
Monroe-Kellie hypothesis: the sum of the volumes of intracranial blood, CSF and cerebral tissue must remain constant.
Imaging options
• CT myelography• Radioisotope cisternography• Non-invasive MR myelography• Suggestive MR brain findings • Conventional Spinal MR
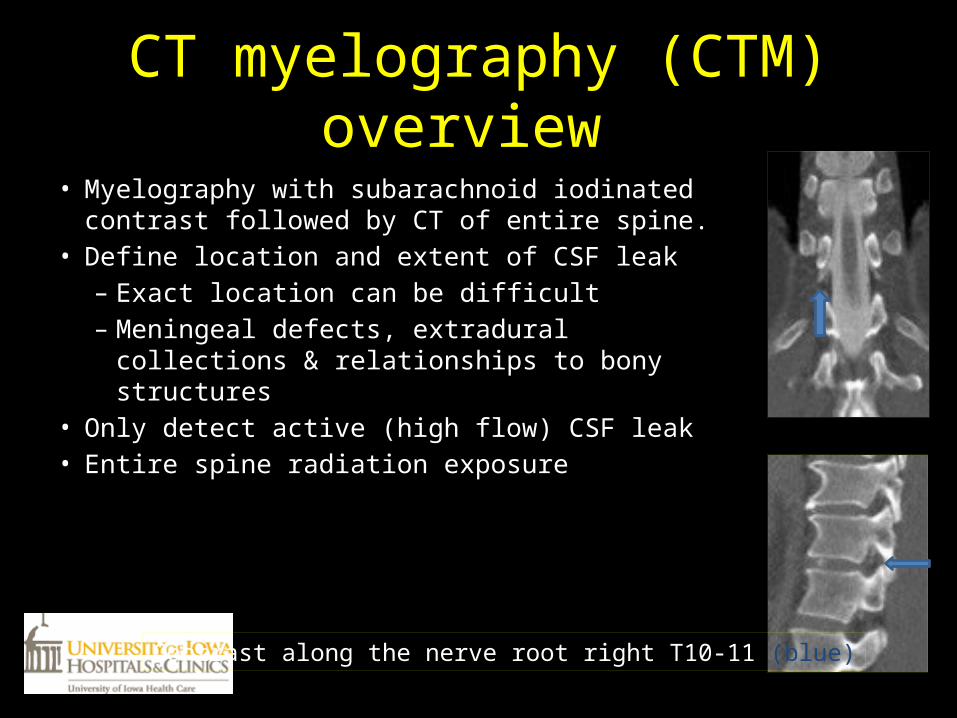
CT myelography (CTM) overview
• Myelography with subarachnoid iodinated contrast followed by CT of entire spine.
• Define location and extent of CSF leak– Exact location can be difficult– Meningeal defects, extradural collections
& relationships to bony structures• Only detect active (high flow) CSF leak• Entire spine radiation exposure
Contrast along the nerve root right T10-11 (blue)
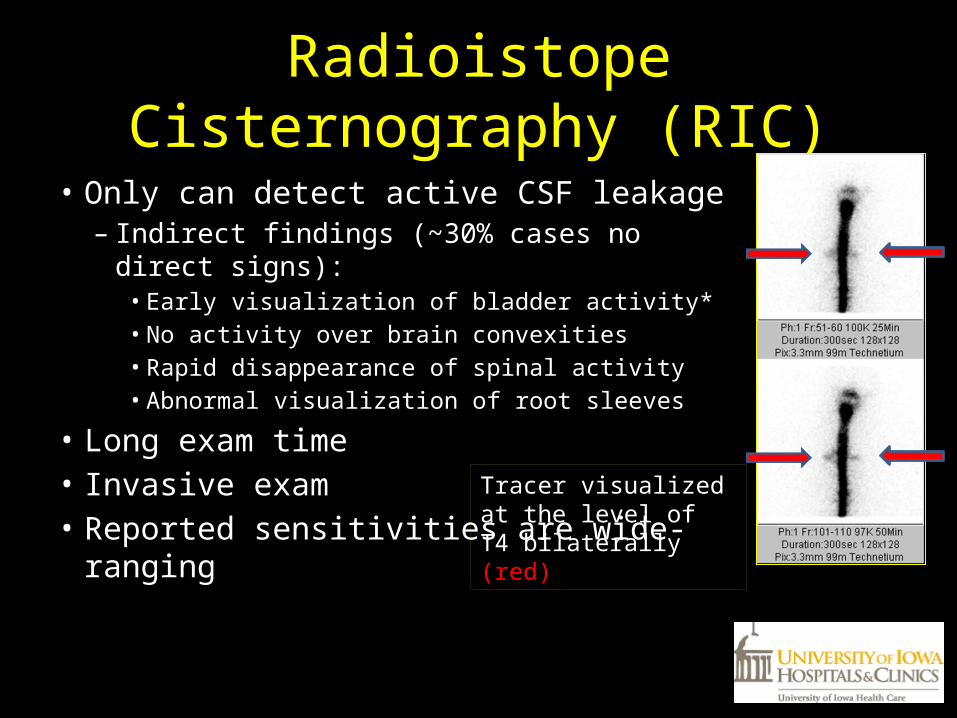
Radioistope Cisternography (RIC)
• Only can detect active CSF leakage– Indirect findings (~30% cases no direct
signs): • Early visualization of bladder activity*• No activity over brain convexities• Rapid disappearance of spinal activity• Abnormal visualization of root sleeves
• Long exam time• Invasive exam• Reported sensitivities are wide-ranging
Tracer visualized at the level of T4 bilaterally (red)

Non-Invasive MR myelography (MRM)
• T2 weighted images are the basic sequence in visualization of potential CSF leak. However, T2 with fat saturation or STIR is need to detect small fluid collections.
• MR myelography using heavily T2 weighted 3 D sequence (SPACE or HASTE with fat saturation) shows site as well as orientation of CSF leak channel
• Enhance CSF signal by suppressing adjacent tissue signal
• Leak may appear as CSF space expansion around nerve root sleeves
Normal MRM

Indirect MRI Brain Findings• Subdural fluid collections (white)• Pachymeningeal enchancement (blue)• Brain sagging (green)• Venous structure engorgement (yellow)• Pituitary hyperemia (red)

MR Spine Findings
• Spine fluid collection• C1-C2 sign• Floating dural sac sign• Dural enhancement/Dilated epidural veins• Meningeal diverticulum/Perineural cysts• Pseudomeningocele
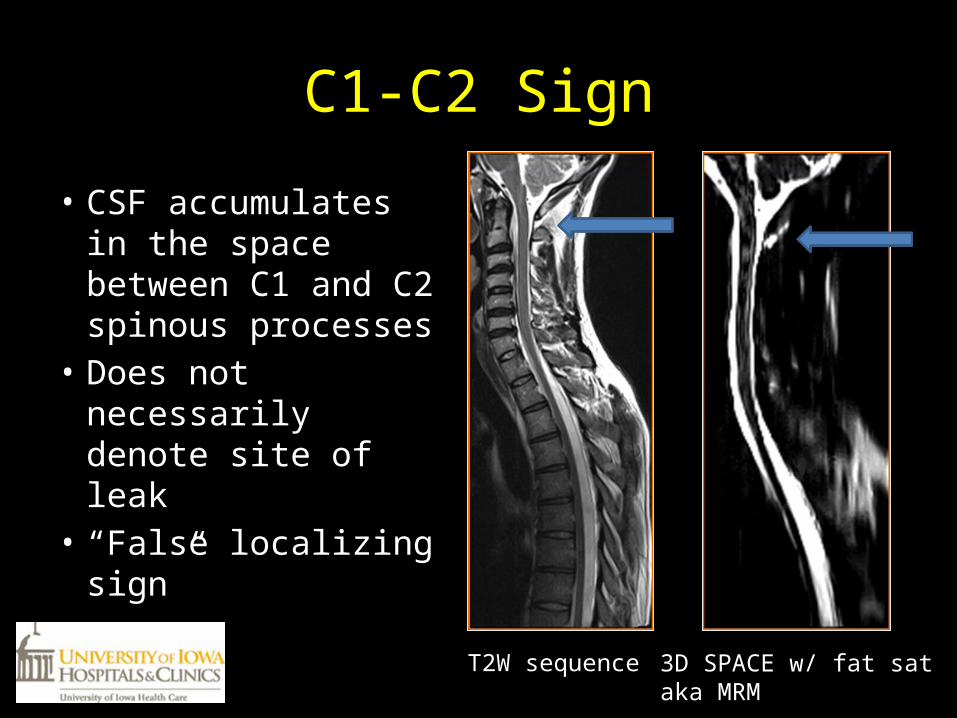
C1-C2 Sign
• CSF accumulates in the space between C1 and C2 spinous processes
• Does not necessarily denote site of leak
• “False localizing sign”
3D SPACE w/ fat sataka MRM
T2W sequence
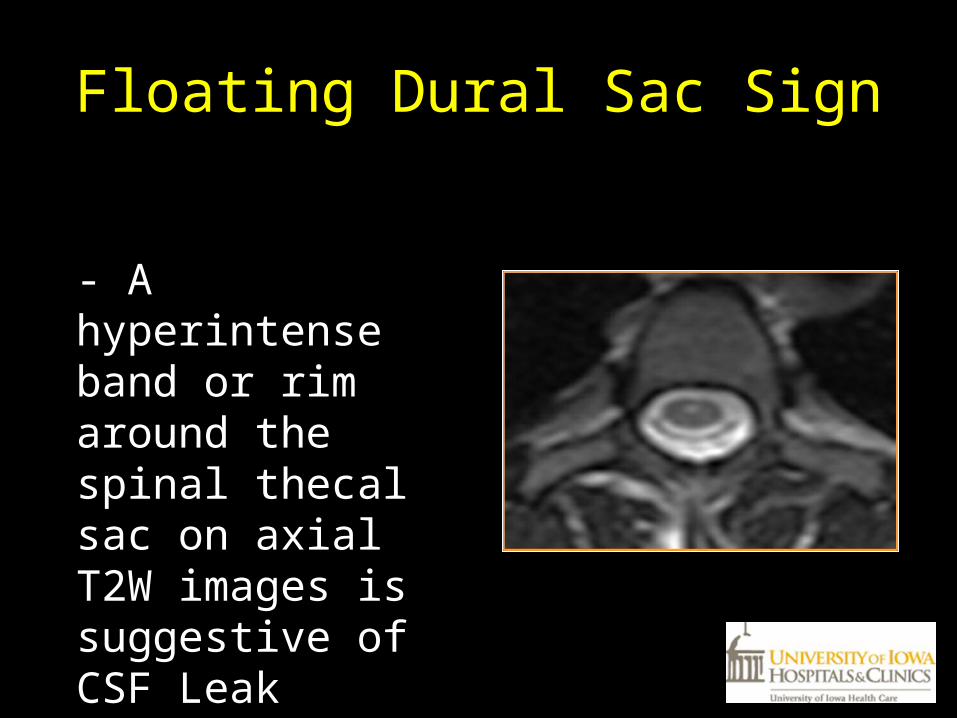
Floating Dural Sac Sign
- A hyperintense band or rim around the spinal thecal sac on axial T2W images is suggestive of CSF Leak
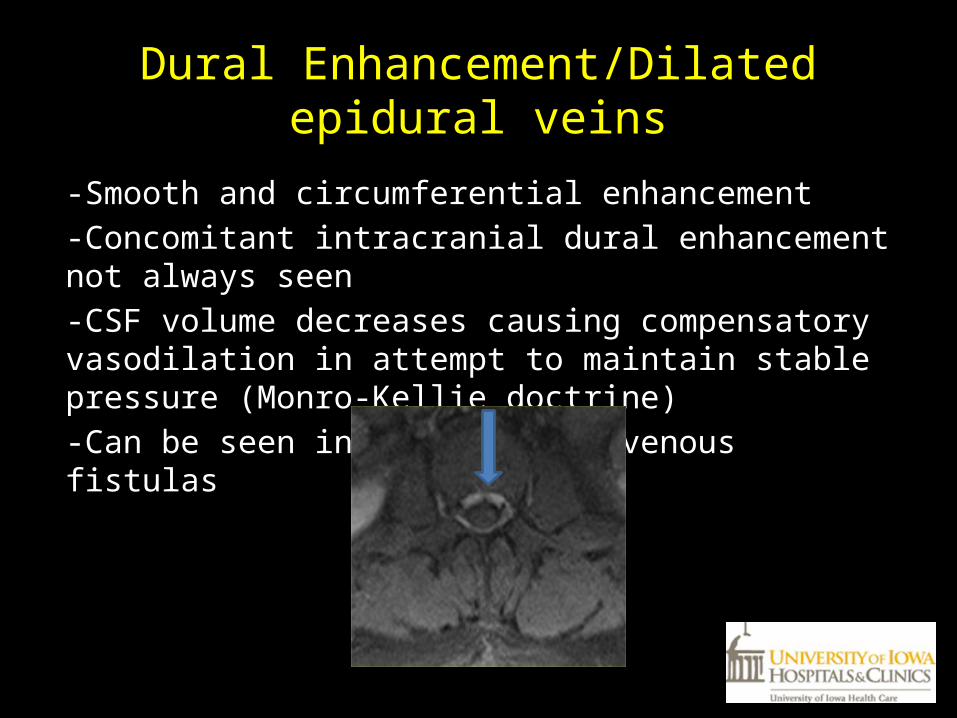
Dural Enhancement/Dilated epidural veins
-Smooth and circumferential enhancement-Concomitant intracranial dural enhancement not always seen -CSF volume decreases causing compensatory vasodilation in attempt to maintain stable pressure (Monro-Kellie doctrine)-Can be seen in dural arteriovenous fistulas

Meningeal diverticulum/ Perineural cyst
T3-T4
- May predispose to rupture/CSF leak- Proposed areas of dural weakness
Multiple perineural cystson 3D HASTE (right). Axial T2 weighted image showing right perineural cyst at T3-T4 (left).

Right T2-T3 CSF Leak
Young female who presented with headache. 3D SPACE myelogram demonstrates right T2-T3 CSF leak (blue) and multiple meningeal cysts/diverticula (yellow)
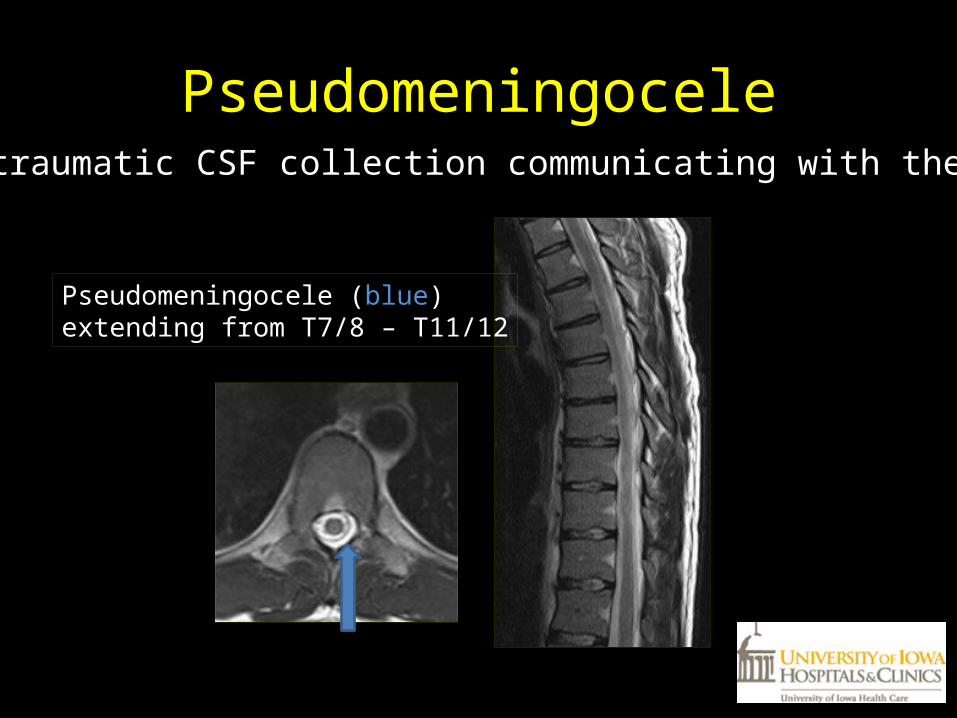
Pseudomeningocele- Post-traumatic CSF collection communicating with thecal sac
Pseudomeningocele (blue) extending from T7/8 – T11/12
Non-Invasive MR Studies From The Literature
• Tomoda, et al. (2008)– 27 patients– Comparison made to radioisotope cisternography (RIC)
• Wang, et al. (2009)– 19 patients– Comparison to computed tomographic myelography
(CTM)
• Yoo, et al. (2008)– 15 patients– Comparison made to radioisotope cisternography (RIC)
Tomoda, et al. (2008)
• Retrospective study involving 27 patients• 3D FSE MR myelography with RIC– 1.5T; TR 6000ms; TE 203.7 ms
• Conclusion: 3D FSE MRM useful in spinal CSF leak detection and may be initial test of choice
Tomoda Y, Korogi Y, Aoki T, et al. Detection of cerebrospinal fluid leakage: initial experience with three-dimensional fast spin-echo magnetic resonance myelography. Acta Radiologica 2008;49:197-203
Wang, et al. (2009)
• Prospective study with 19 patients• SSFSE (Heavily T2W) MRM compared to CTM– 1.5 T
• Results (detection rates did not differ)– Along nerve roots (84% v 74%, p = 0.25)– High cervical retrospinal (32% v 16%, p = 0.13)– Epidural CSF collection (89% v 79%, p = 0.20)
• Conclusion: MRM accurate in CSF leak localization and alternative to CTM
Wang Y-F, Lirng J-F, Fuh J-L, et al. Heavily T2-weighted MR myelography vs CT myelography in spontaneous intracranial hypotension. Neurology 2009;73:1892-1898
Yoo, et al. (2008)
• 15 patients• 2D TSE compared to RIC– 1.5 T; TR 8000ms; TE 1000ms
• Results – Agreement among two readers between MRM & RIC
(kappa = 0.634 & 0.444)• Conclusion: MRM can be used as screening tool
Yoo H-M, Kim S, Choi C, et al. Detection of CSF leak in spinal CSF leak syndrome using MR myelography: correlation with radioisotope cisternography. American Journal of Neuroradiology 2008;29:649-654
Non-Invasive MR Myelography
• Consists of the following spinal sequences– Sagittal T2, Sagittal T1– Axial T2, Axial Diffusion, Axial STIR – 3D Haste or 3D SPACE Myelogram*– Sagittal and Axial T1 fat-suppression post contrast
• TR 3000.00ms; TE 430.00ms*

Ex #1; + RIC, - MR (not MRM)
Radioisotope cisternography images (below) demonstrating multilevel thoracic and lumbar spinal CSF leaks.
Multiple axial T2 images in at different levels (right) in this same patient which do not show signs of spinal CSF leak.

Ex #2; + RIC, - MR initially, +MRM
R
T2 weight axial
Radioisotope cisternographyPatient with right sacral CSF leak which is not well demonstrated on initial conventional MR spine. Patient brought back for dedicated CSF leak protocol.Positive on RIC imaging.
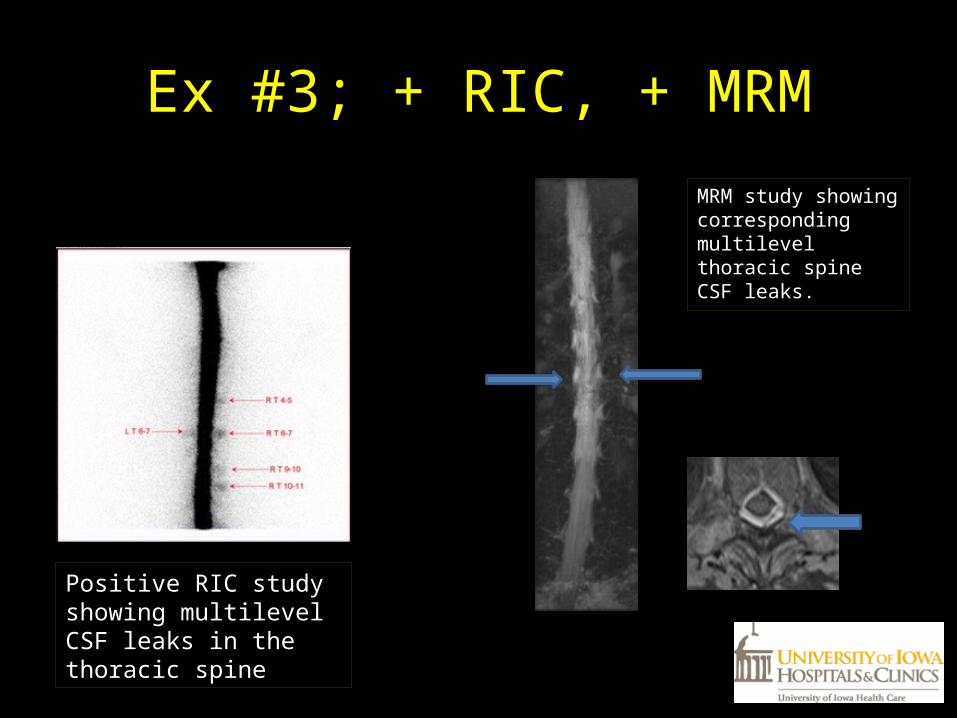
Ex #3; + RIC, + MRM
MRM study showing corresponding multilevel thoracic spine CSF leaks.
Positive RIC study showing multilevel CSF leaks in the thoracic spine
Summary/Conclusion
• Non-invasive magnetic resonance myelography is a first-line tool for diagnosing spinal cerebrospinal leaks in spontaneous intracranial hypotension.
References• 1. Schievink WI. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. Jama
2006;295:2286-2296• 2. Tomoda Y, Korogi Y, Aoki T, et al. Detection of cerebrospinal fluid leakage: initial experience with
three-dimensional fast spin-echo magnetic resonance myelography. Acta Radiologica 2008;49:197-203• 3. Wang Y-F, Lirng J-F, Fuh J-L, et al. Heavily T2-weighted MR myelography vs CT myelography in
spontaneous intracranial hypotension. Neurology 2009;73:1892-1898• 4. Yoo H-M, Kim S, Choi C, et al. Detection of CSF leak in spinal CSF leak syndrome using MR
myelography: correlation with radioisotope cisternography. American Journal of Neuroradiology 2008;29:649-654
• 5. Schievink WI, Maya MM, Louy C, et al. Diagnositic criteria for spontaneous spinal CSF leaks and intracranial hypotension. American Journal of Neuroradiology 2008;29(5):853-856.
• 6. Chikly B, Quagheber J. Reassessing cerebral fluid (CSF) hydrodynamics: A literature review presenting a novel hypothesis for CSF pathology. Journal of Bodywork & Movement Therapies 2013;17:344-354
• 7. Medina JH, Abrams K, Falcone S, et al. Spinal Imaging Findings in Spontaneous Intracranial Hypotension. American Journal of Roentgenology 2010;195:459-464
• 8. Amoozegar F, Guglielmin D, Hu W, Chan D, Becker WJ. Spontaneous intracranial hypotension: recommendations for management. The Canadian Journal of Neurological Sciences 2013;40(2):144-157
• 9. Thomas D, Menda Y, Graham M. Radionuclide Cisternography in Detecting Cerebrospinal Fluid Leak in Spontaneous Intracranial Hypotension: A Series of Four Case Reports. Clinical Nuclear Medicine 2009;34(7)410-416.
• 10. Hosoya T, Hatazawa J, Sato S, et al. Floating Dural Sac Sign is a Sensitive Magnetic Resonance Imaging Finding of Spinal Cerebrospinal Fluid Leakage. Neurologia Medico-Chirurgica 2013;53(4):207-212.


























![CEREBRAL CIRCULATION AND CEREBROSPINAL FLUID [CSF]](https://img.pdfslide.us/doc/110x75/56814ee4550346895dbc77ad/cerebral-circulation-and-cerebrospinal-fluid-csf.jpg)
