Embed Size (px)
Citation preview

Non-Accidental Trauma: Recognition Gudrun Mirick Mueller, MD
12/15/18

I have no disclosures related to this presentation. Special thanks to Dale Jarka, MD for clinical images and radiographs.
12/15/18

Why this lecture? Recognition!
• MSK injuries 2nd most common manifestation after soft tissue & bruising
• 1/3 of abused children are eventually seen by an orthopaedic surgeon
• The orthopaedic surgeon (esp. pediatric orthopaedist) often the first physician to recognize signs of NAT
• Families will often not present to the same ER twice, -> only ONE opportunity
12/15/18

CAPTA: Child Abuse Prevention & Treatment Act (amended 2003):
"any recent act or failure to act, on the part of the parent or
caregiver, which results in death or serious physical or emotional harm, sexual abuse or exploitation, or an act or failure to act which
presents an imminent risk of serious harm"
• Physical abuse: non-accidental physical injury (NAT) • Psychological abuse: emotional abuse, verbal abuse or mental
injury • Neglect: the failure to provide for the child's basic needs -
physical, emotional or educational
12/15/18

Types of Abuse
• Neglect: 78%
• Physical: 18%
• Sexual: 9%
• Psychological: 8%
12/15/18

Child Abuse & Neglect – Incidence
• Difficult to determine
• DHHS estimation - 1/100 (16% physical)
• Greatest risk: • First born • Unplanned • Premature • Stepchildren • Handicapped: esp cerebral palsy

Child Abuse & Neglect – Perpetrators
• Single-parent homes • Often young (mid 20’s) • W/O high school diploma • Living at or below poverty level • Difficulty coping w/ stressful
situations • Lack of social support
system • Drug use • Personal history of abuse

Child Abuse & Neglect – Perpetrators
• National Child Abuse and Neglect Data System:
• 37% unspecified
• 25% father/stepfather or boyfriend of mother
• 19% mother, stepmother or girlfriend of father
• 5% nonrelated caregiver
• Up to 10% had > 1 abuser National Children’s Advocacy Data, 2015

Child Abuse & Neglect – Victims
• Most common in infants/toddlers (demanding, defenseless & non-verbal)
• National Child Abuse and Neglect Data System: • < 1 yr 49%
• 1-2 yr 19%
• 3-12 yr 18%
• 13-20 yr 14%

Differential Diagnosis
• True accidental injury
• Osteogenesis imperfecta (OI)
• Osteopenia of prematurity
• Scurvy
• Rickets
• Disuse osteopenia (ex: non-ambulatory patients)
• Chronic disease: liver and kidney
• Leukemia/lymphoma
12/15/18

Presentation of NAT- History
• Vague
• Incomplete or contradictory details
• Delay in seeking care
• Injury not consistent w/ developmental stage (e.g. femur fx in non-ambulatory infant)
• Presence vs absence of witness
• History of previous injury

Presentation of NAT- Examination
• Must be thorough, esp under age 3 yrs
• Examination of skin, including hidden areas: • Burns - present in 10-25%
• Immersion-type • Bruises - present in 50 – 75%
• Bruising in abnormal locations (buttocks, perineum, trunk, back of head, back of legs)
• Bite marks • Present in different stages of healing

Presentation of NAT- Radiographic Eval
• >70% of NAT under 1 yr have multiple fx's in different stages of healing
• Many fx's carry low specificity for abuse individually
• No fx on its own can distinguish between NAT & AT
• No typical diaphyseal fracture pattern - specifically spiral fx’s
• Salter-Harris fractures uncommon, except for distal humerus

Presentation of NAT- Skeletal Survey
• AP views of all bones of appendicular bones
• AP/lat views of skull • Lat view of T & L spine • Separate lat view of C spine • AP view of chest • AP view of abdomen
• AP view of pelvis • AP femur • AP humerus • May include coned-down view of
joints (e.g. ankle) • Bilateral oblique view of ribs

Presentation of NAT- Further Radiologic Eval
• “Babygrams” not sufficient for diagnosis – detail lost at periphery
• CT scanning
• Frequently necessary to evaluate other injuries (intracranial, solid organ)
• CT scanning may confirm subtle fractures
• 3D CT’s may be more easily understood by lay juries
• Bone scan also useful adjunct – highly sensitive

Specificity of Fx’s for NAT - High
• Classic metaphyseal lesion: “corner fractures”
• Multiple rib fractures, especially posteromedial
• Scapular fractures
• Sternal fractures
• Clavicular fractures • Especially in very young children

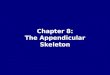
Classic Metaphyseal Fracture/Lesion (CML)
• Fracture plane dissects on metaphyseal side along zone of provisional calcification, tearing it off, usually incompletely
• At periphery, it extends slightly into metaphysis, due to tight attachment of periosteum at level of physis
7moF: “fell off bed” - Brought in 36 hrs later - Admitted for 2 days for w/u - Eventually cleared - Treated in spica cast

Multiple Rib Fractures
• Rib fractures in children < 3yrs have positive predictive value of 95% as indicator of NAT
• Posteromedial rib fractures can only be caused when chest is squeezed A & P, levering posteromedial ribs over transverse processes
• However children w/ NAT more likely to have a single rib fx (one study – avg. 1.2/child)
• In same study, rib fx’s were only skeletal injury in 29%

Multiple Rib Fractures

Rib Fractures – Rabbit Study
• Simultaneous pressure on chest & back caused multiple posteromedial rib fractures
• The same did NOT occur when the back was laid flat against a board & the chest compressed anteriorly
• Ruling out PM rib fractures as a result of chest compressions during CPR.

Specificity of Fx’s for NAT - Moderate
• Multiple fractures
• Fractures in various stages of healing
• Physeal separations
• Vertebral body fractures & separations
• Digital fractures
• Complex skull fractures

Multiple Fractures/Fractures of Various Ages
• Only moderately specific for NAT
• When multiple fx’s w/o history of trauma, high index of suspicion necessary
• Dx of NAT can be make when highly specific injuries are among injuries identified, whether soft tissue or bony
• Though fx’s such as CML/corner fractures or posteromed rib fx’s are highly specific, low-specificity long-bone fx’s are very common

Fracture Healing Time Frame
Process markedly accelerated in infants:
• By 1 week: resolution of ST swelling • By 2 weeks: new sub-periosteal bone formation • 2 – 3 week time:
• Immature or soft callus present • Loss of fx line definition
• By 3 weeks: mature or hard callus

Fracture Healing - Callus
• Intra-articular fx’s: • Do not show callus, as no periosteum
present • Periosteal elevation & reaction seen
more proximally/distally away from the joint
• As trauma in NAT tends to be repetitive & w/o medical Rx, callus tends to be abundant.
• Callus may be markedly delayed in osteopenic patients (poor nutrition, Vit D or Ca deficiencies)

Physeal Separations
• Often overlooked • Images frequently misinterpreted (not familiar or comfortable w/
pediatric imaging) • Since epiphysis not ossified/only slightly ossified, displacement
may not be apparent to casual observer

Distal Humeral Physeal Separations
• Fracture commonly misinterpreted as a dislocation
• Dislocations do NOT occur in infant elbow
• Majority of cases: distal epiphysis moves medially & posteriorly
• Confirmation can be obtained w/ U/S or MR

Head Injury in NAT
• Most common cause of death & disability in childhood
• 3rd leading cause of death in children < 1 yr
• < 1 yr: 95% of intracranial injuries were caused by NAT
• Reported mortality w/ head trauma is 10% • 5X that of childhood leukemia • 18X that of childhood brain tumors

Skull Fractures in NAT
• Can be the only evidence of NAT
• Infants - most NAT skull fx's are simple linear fx's
• Older children - depressed NAT skull fx's are more prominent
• Important to be familiar w/ various sutures, synchondroses & fissures that may be present throughout the developmental stages

Skull Fractures in NAT (cont’d)
• Can be difficult to interpret
• Must differentiate from vascular grooves and accessory sutures
• 3D CT scan very helpful

Other Non-MSK Injuries in NAT
• Traumatic brain injury accounts for the majority of death and disability in NAT
• Denver 1996-2002: 7% of trauma admissions were NAT-related (265 of 3705)
• 9% of NAT pts had visceral injury: • 71% solid organ - did not require surgery (liver most frequent) • 50% hollow organ – half required urgent surgery (most common
requiring surgery: duodenum, jejunum & ilium)

Visceral Injuries in NAT
• Hollow organ injuries is rare in pediatric blunt trauma secondary to other mechanisms
• In accidental blunt injuries, the force is dispersed over a larger body surface area, compared to the fist or foot of assailant
• These children may have high ISS – involve trauma service

Mimics of NAT – Osteogenesis Imperfecta
• Complexity & variability in OI make differentiation from NAT challenging
• HOWEVER: rib fractures generally occur in the more severe/obvious types and are usually lateral
• Corner fractures/CMLs are highly suspicious: • Type 2 collagen predominates in epiphyseal cartilage • Type 1 collagen is not present in the physis
• Thus the most fragile portion of the OI bone is the midshaft
• Keep in mind that OI is rare, especially the 5-10% of patients w/ negative OI workup
• Lab testing may be required for diagnosis

Mimics of NAT
• Primary non-Hodgkins Lymphoma • May present with pain or pathological fracture • Full radiographic workup • Requires biopsy
• Disuse osteopenia
• Rickets • Dietary: Vitamin D deficiency • Metabolic: Unable to absorb GI vitamins
12/15/18

Role of Orthopaedic Surgeon in NAT
• Recognition is first priority
• Medical personnel are mandated reporters • In Minnesota, done by county of child’s residence
• Only suspicion is required, not certainty
• Inform family of duty to notify pertinent authorities
• Tell them that every patient w/ this history or fracture at this age goes through the same process
• It should come across as routine standard of care without implication of guilt

Role of Orthopaedic Surgeon in NAT
• Most large hospitals have a CPS or SCAN team and may include: • Social workers • Nurses • Pediatrician • Access to consultants (neurosurgeon, orthopaedist, general
surgeon or urologist)
• Abuse estimated to recur in 30-50% left unreported - 5% of those will result in death

Conclusions
• Abuse is second to SIDS as cause of death in ages 1-5 months and second to accidental trauma in children > 1 year
• Awareness the most critical component in making the diagnosis
• Abuse may be missed if only searching for high-specificity fractures!
• Corner metaphyseal fractures • Posteromedial rib fractures • Be suspicious!

Thank you!
12/15/18




![[PPT]Appendicular Skeleton Pectoral Girdle and Upper … · Web viewAPPENDICULAR SKELETON PECTORAL GIRDLE AND UPPER LIMB PECTORAL GIRDLE scapula humerus clavicle CLAVICLE sternal](https://img.pdfslide.us/doc/110x75/5b1c49a87f8b9a2d258f98c3/pptappendicular-skeleton-pectoral-girdle-and-upper-web-viewappendicular-skeleton.jpg)