Embed Size (px)
Citation preview
NOAK: Differentialindikationen,oder sind alle gleich?
Prof.Dr.med.Carl-Erik DempfleIMD - Gerinnungszentrum Mannheim
Akademische Lehrambulanz derMedizinischen Fakultät Mannheimder Universität Heidelberg
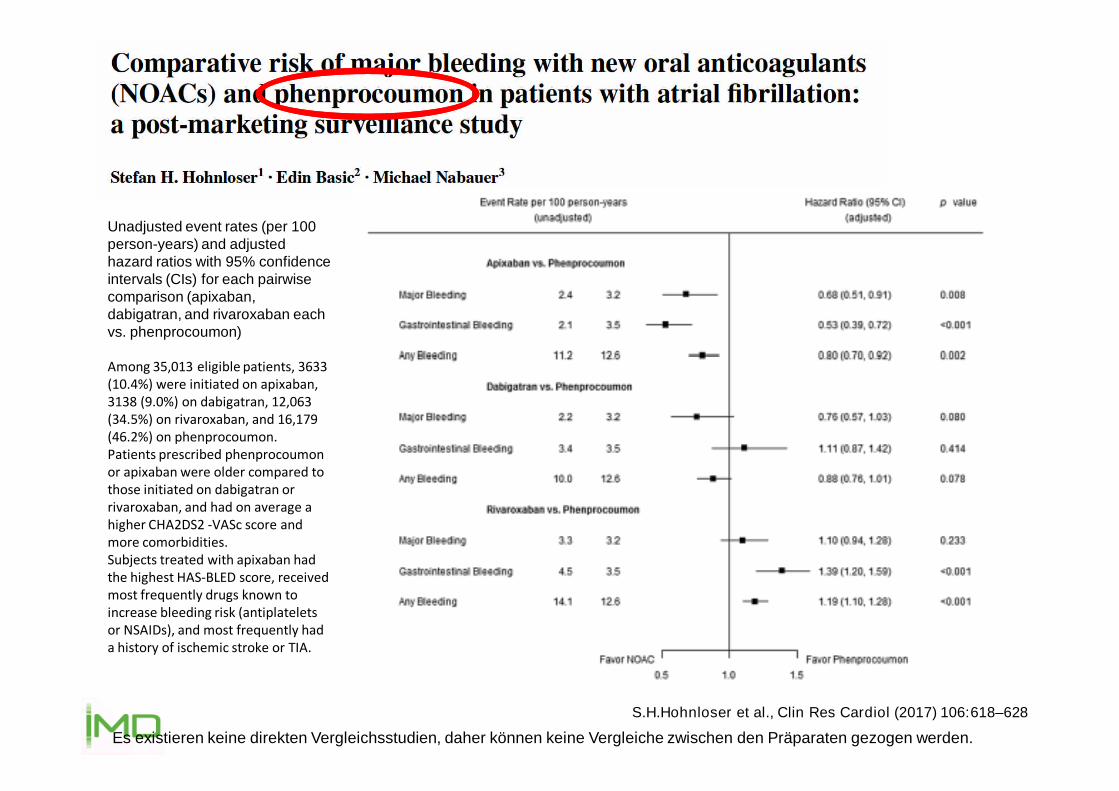
S.H.Hohnloser et al., Clin Res Cardiol (2017) 106:618–628
Unadjusted event rates (per 100person-years) and adjustedhazard ratios with 95% confidenceintervals (CIs) for each pairwisecomparison (apixaban,dabigatran, and rivaroxaban eachvs. phenprocoumon)
Among 35,013 eligible patients, 3633(10.4%) were initiated on apixaban,3138 (9.0%) on dabigatran, 12,063(34.5%) on rivaroxaban, and 16,179(46.2%) on phenprocoumon.Patients prescribed phenprocoumonor apixaban were older compared tothose initiated on dabigatran orrivaroxaban, and had on average ahigher CHA2DS2 -VASc score andmore comorbidities.Subjects treated with apixaban hadthe highest HAS-BLED score, receivedmost frequently drugs known toincrease bleeding risk (antiplateletsor NSAIDs), and most frequently hada history of ischemic stroke or TIA.
Es existieren keine direkten Vergleichsstudien, daher können keine Vergleiche zwischen den Präparaten gezogen werden.

S.Själander et al., Thrombosis Research 167 (2018) 113–118
Es existieren keine direkten Vergleichsstudien, daher können keine Vergleiche zwischen den Präparaten gezogen werden.
Nationwide retrospective cohort studybased on Swedish quality registries.37,174 patients were instituted onwarfarin, 6574 on dabigatran, 8323 onrivaroxaban and 12,311 on apixaban.
In warfarin treated patients, the time intherapeutic range was 71.4%.
This study showed no differencebetween apixaban, dabigatran, orrivaroxaban compared to high TTRwarfarin treatment regarding strokeprevention. However, fewer bleedingevents were seen for apixaban anddabigatran, but not for rivaroxaban.
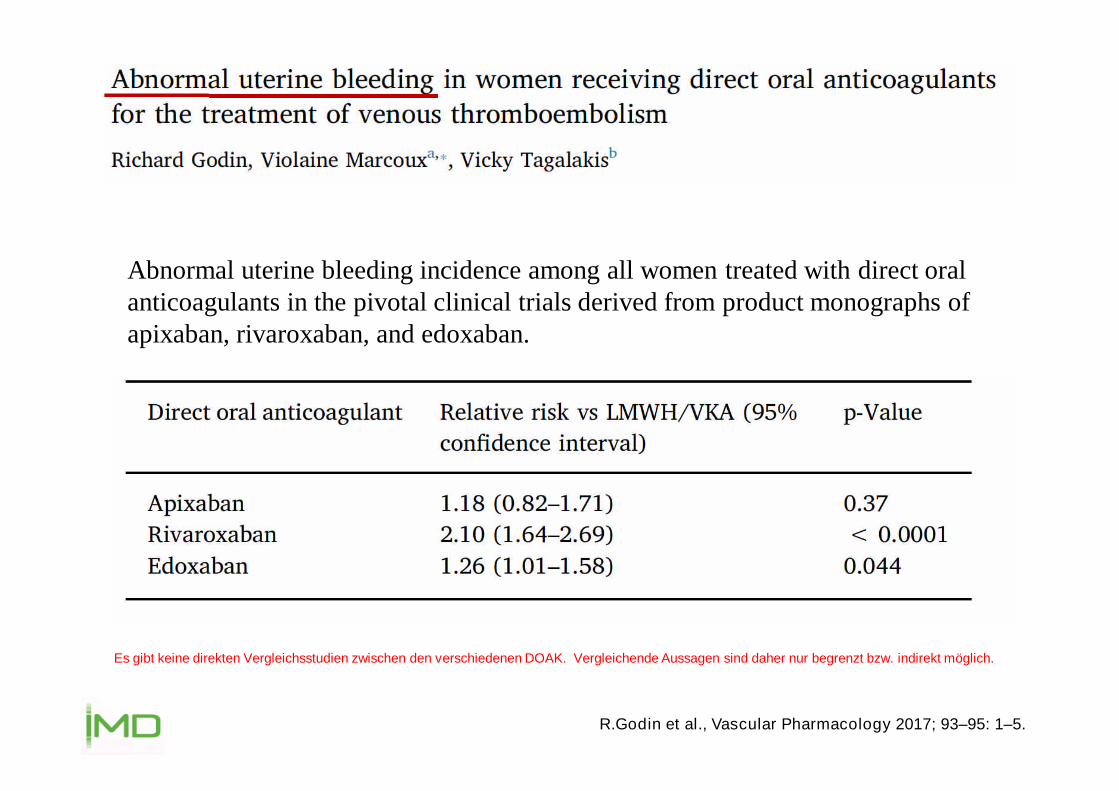
R.Godin et al., Vascular Pharmacology 2017; 93–95: 1–5.
Abnormal uterine bleeding incidence among all women treated with direct oralanticoagulants in the pivotal clinical trials derived from product monographs ofapixaban, rivaroxaban, and edoxaban.
Es gibt keine direkten Vergleichsstudien zwischen den verschiedenen DOAK. Vergleichende Aussagen sind daher nur begrenzt bzw. indirekt möglich.

A.H.E.M.Maas et al., Maturitas 2015; 82: 355-359
All reported adverse events of abnormal uterine bleeding to theWHO adverse event database Vigilyze https://vigilyze.who-umc.org
Es gibt keine direkten Vergleichsstudien zwischen den verschiedenen DOAK. Vergleichende Aussagen sind daher nur begrenzt bzw. indirekt möglich.

A.H.E.M.Maas et al., Maturitas 2015; 82: 355-359
All reported adverse events of abnormal uterine bleeding to theWHO adverse event database Vigilyze https://vigilyze.who-umc.org
Concomitant long-term use of a NOACwith acetylsalicylic acid or otherantiplatelet drugs should be avoided.
Es gibt keine direkten Vergleichsstudien zwischen den verschiedenen DOAK. Vergleichende Aussagen sind daher nur begrenzt bzw. indirekt möglich.

•K.Booyawat et al., Blood. 2017;130(24):2603-2609
Rivaroxaban
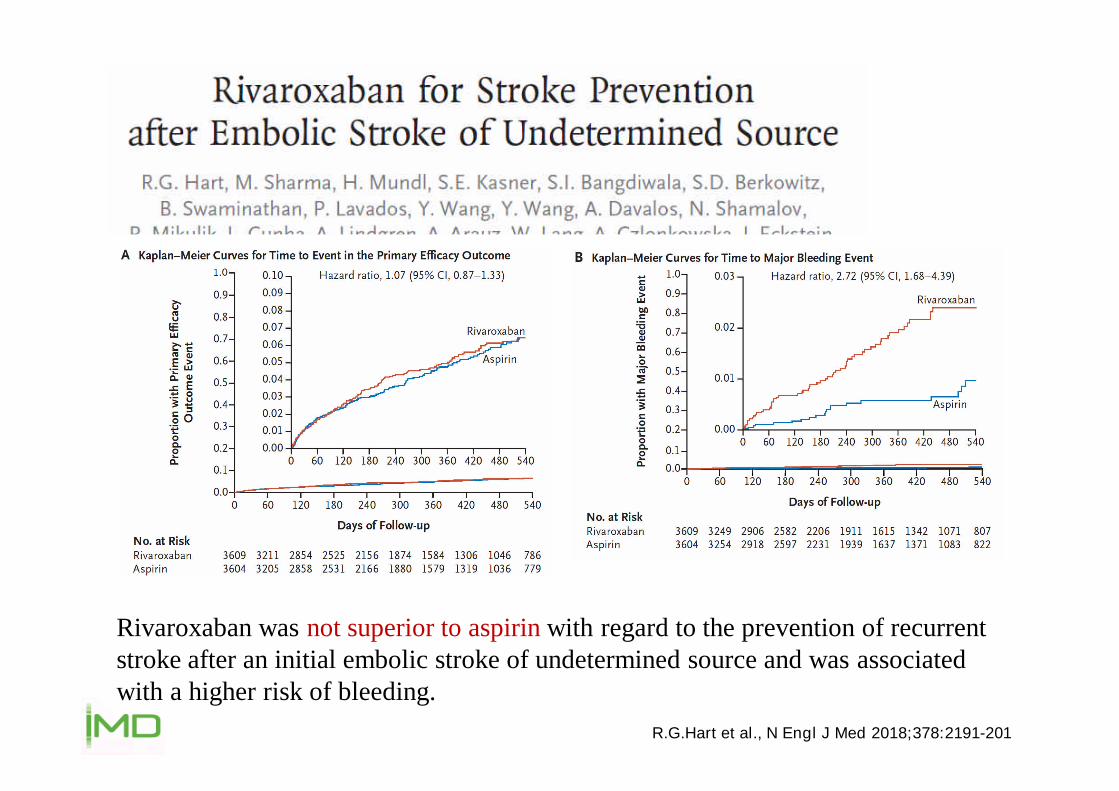
R.G.Hart et al., N Engl J Med 2018;378:2191-201
Rivaroxaban was not superior to aspirin with regard to the prevention of recurrentstroke after an initial embolic stroke of undetermined source and was associatedwith a higher risk of bleeding.
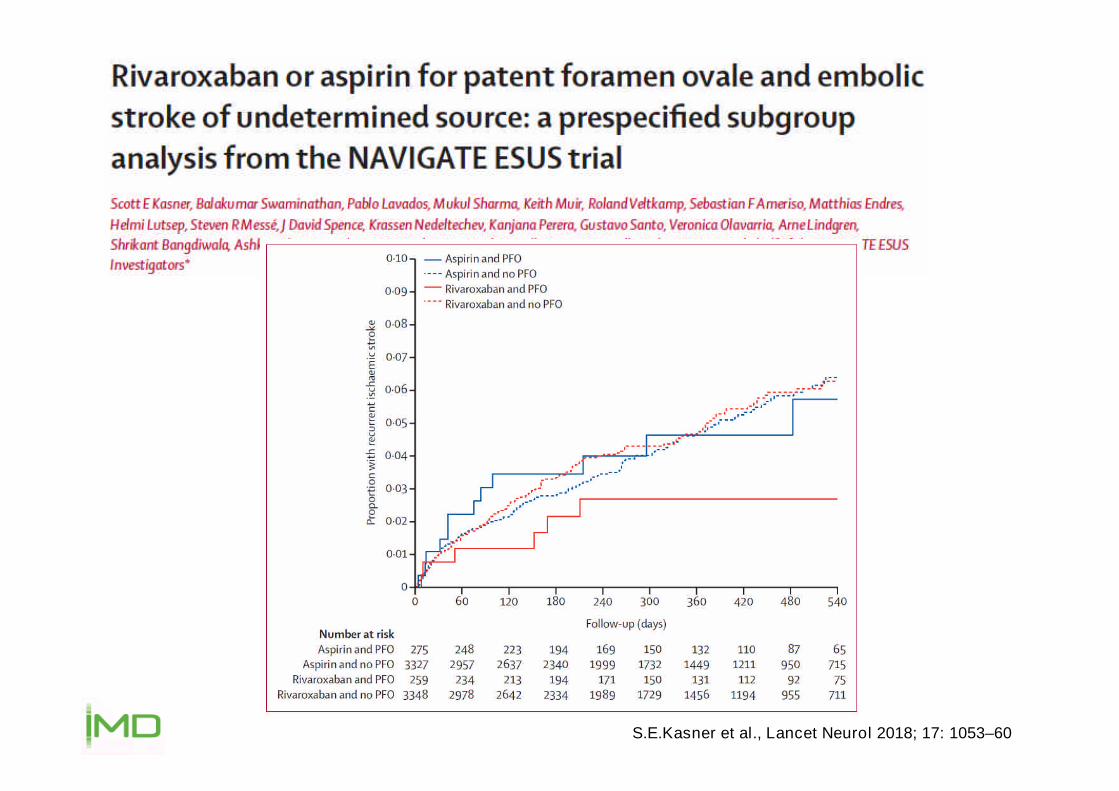
S.E.Kasner et al., Lancet Neurol 2018; 17: 1053–60

S.E.Kasner et al., Lancet Neurol 2018; 17: 1053–60
Among patients with ESUS who have PFO, anticoagulationmight reduce the risk of recurrent stroke by about half...
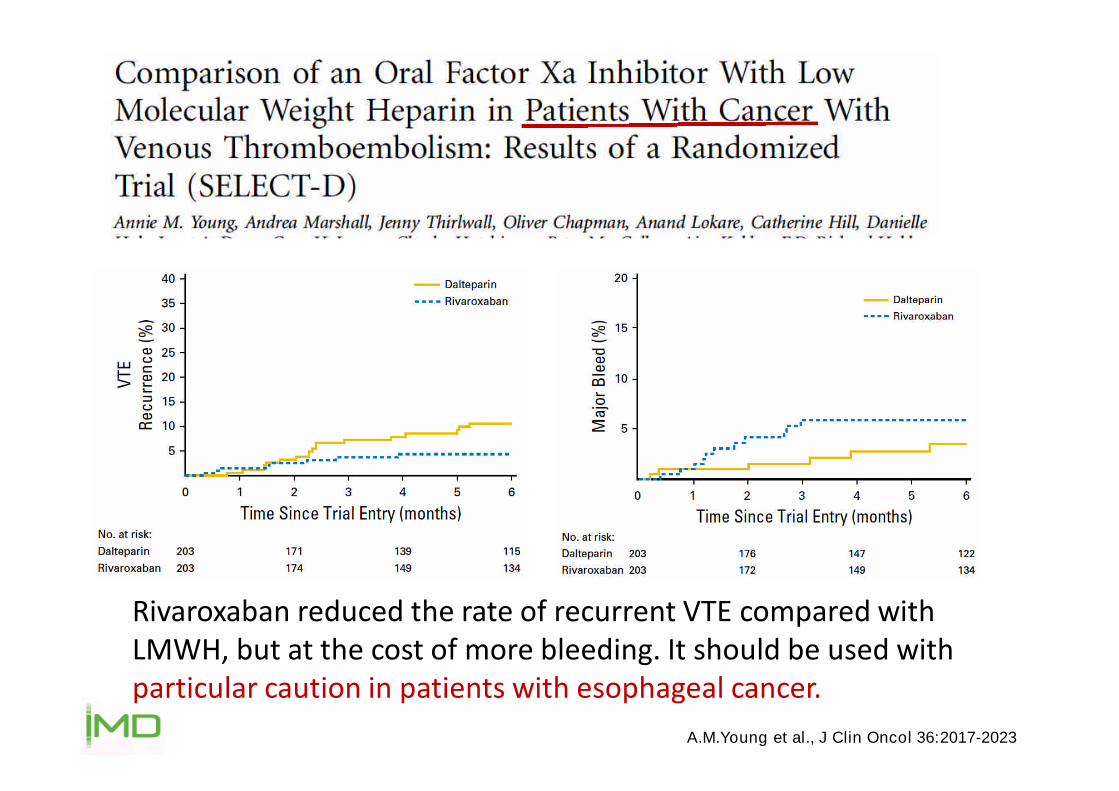
A.M.Young et al., J Clin Oncol 36:2017-2023
Rivaroxaban reduced the rate of recurrent VTE compared withLMWH, but at the cost of more bleeding. It should be used withparticular caution in patients with esophageal cancer.

The primary efficacy outcome was recurrent venous thromboembolism.
The EINSTEIN Investigators, N Engl J Med 2010;363:2499-510
Langzeit-Sekundärprophylaxe: Rivaroxaban vs. Placebo

Bleeding
p<0.001(for superiority)
HR, 0.1895% CI, 0.09–0.39
p<0.001
EINSTEIN-EXT:Primary efficacy outcomes and Major/CRNM bleeding
*Primary efficacy outcome. Recurrent VTE includes fatal PE. Furthermore, PE was considered to be the cause of death ifĚĞĂƚŚ�ĐŽƵůĚ�ŶŽƚ�ďĞ�ĂƩ ƌŝďƵƚĞĚ�ƚŽ�Ă�ĚŽĐƵŵĞŶƚĞĚ�ĐĂƵƐĞ�ĂŶĚ�W��ĐŽƵůĚ�ŶŽƚ�ďĞ�ĐŽŶĮ ĚĞŶƚůLJ�ƌƵůĞĚ�ŽƵƚ͘ �ΏWƌŝŵĂƌLJ�ƐĂĨĞƚLJ�ŽƵƚĐŽŵĞ͘
Efficacy Safety
HR=NA
p=0.11
n=42 n=8 n=7 n=36n=0 n=4
Bauersachs R et al. N Engl J Med 2010;363:2499–2510.
HR, 5.1995% CI, 2.3–11.7
Dose was rivaroxaban 20mg daily
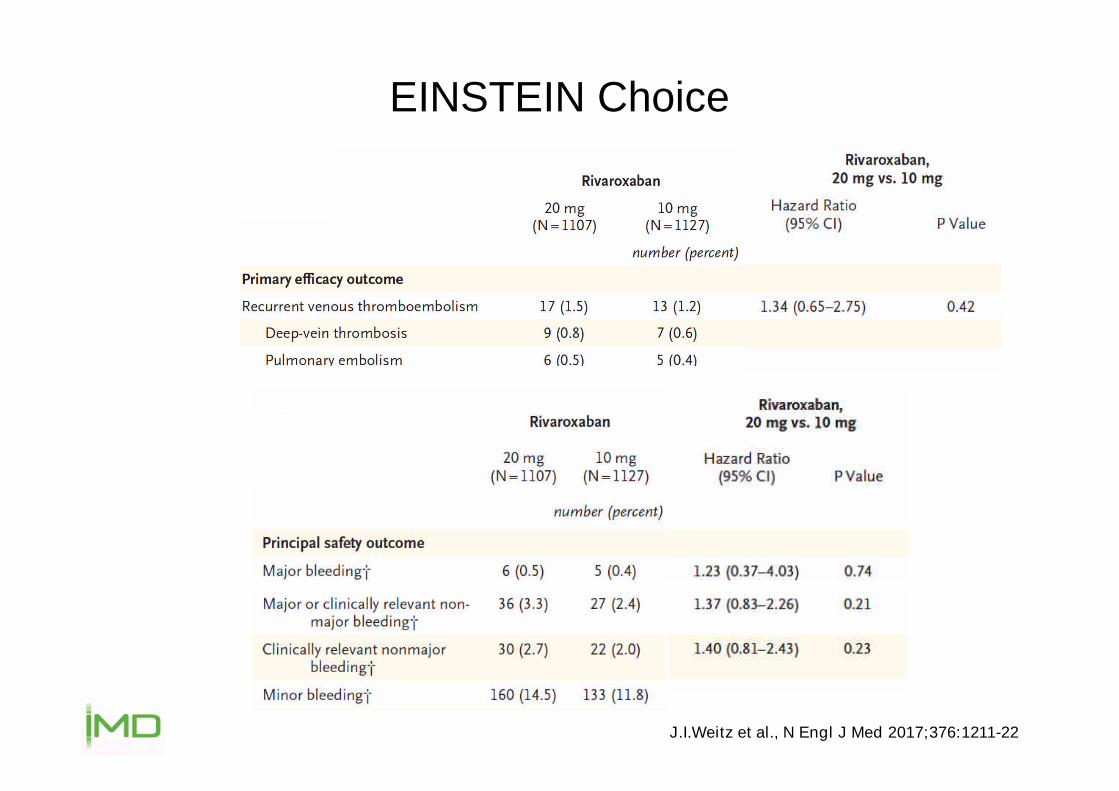
EINSTEIN Choice
J.I.Weitz et al., N Engl J Med 2017;376:1211-22
VTE-Sekundärprophylaxe mit Xarelto
Langfristige VTE-Sekundärprophylaxemit Xarelto 20 mg ODER 10 mgtäglich, abhängig vom Risikoprofil
• APS, PC-Mangel, AT-Mangel,hom. FVL, hom. PTH G20210A,kombinierte Thrombophilien
eher 20 mg täglich
• Het. FVL, het. PTH G20210A eher 10 mg täglich
S.S.Anand et al., Lancet 2018; 391: 219–29
S.J.Connolly et al., Lancet 2018; 391: 205–18
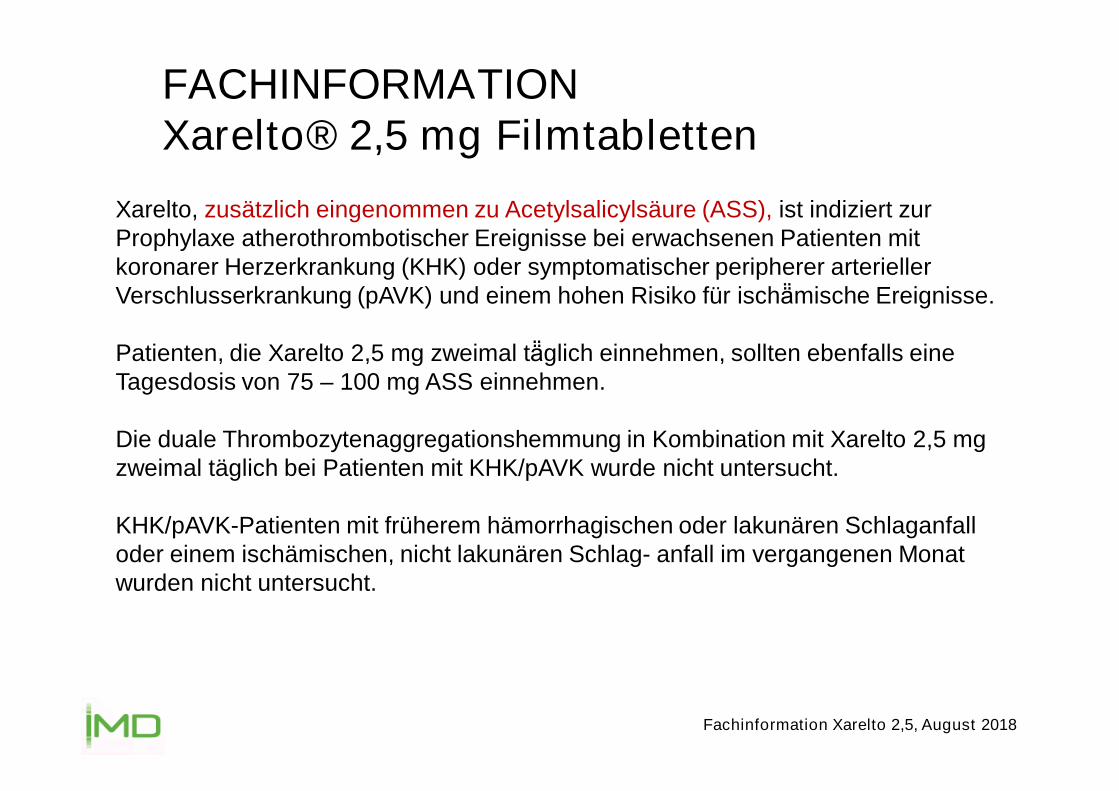
FACHINFORMATIONXarelto® 2,5 mg Filmtabletten
Fachinformation Xarelto 2,5, August 2018
Xarelto, zusätzlich eingenommen zu Acetylsalicylsäure (ASS), ist indiziert zurProphylaxe atherothrombotischer Ereignisse bei erwachsenen Patienten mitkoronarer Herzerkrankung (KHK) oder symptomatischer peripherer arteriellerVerschlusserkrankung (pAVK) und einem hohen Risiko für ischä̈mische Ereignisse.
Patienten, die Xarelto 2,5 mg zweimal tä̈glich einnehmen, sollten ebenfalls eineTagesdosis von 75 – 100 mg ASS einnehmen.
Die duale Thrombozytenaggregationshemmung in Kombination mit Xarelto 2,5 mgzweimal täglich bei Patienten mit KHK/pAVK wurde nicht untersucht.
KHK/pAVK-Patienten mit früherem hämorrhagischen oder lakunären Schlaganfalloder einem ischämischen, nicht lakunären Schlag- anfall im vergangenen Monatwurden nicht untersucht.
Xarelto 2 x täglich 2,5 mg PLUS ASS 100 mg täglich.
NICHT Eliquis 2 x 2,5 mg !

S.Harder; Journal of Clinical Pharmacology, 2012;52:964-975
Rivaroxaban

A.S.De Vriese et al., Am J Kidney Dis. 2018; 66(1):91-98
A 10-mg dose of rivaroxaban in hemodialysis patientswithout residual kidney function results in drug exposuresimilar as published for 20 mg in healthy volunteers.
Apixaban

Die empfohlene Dosis zur verlängerten Prophylaxe von rezidivierenden
TVT und LE ist ausschließlich Apixaban 2,5 mg 2 x täglich. G.Agnelli et al., N Engl J Med 2013;368:699-708
Langzeit-Sekundärprophylaxe: Apixaban vs. Placebo

Die empfohlene Dosis zur verlängerten Prophylaxe von rezidivierenden
TVT und LE ist ausschließlich Apixaban 2,5 mg 2 x täglich. G.Agnelli et al., N Engl J Med 2013;368:699-708
Langzeit-Sekundärprophylaxe: Apixaban vs. Placebo

AMPLIFY-EXT: Efficacy outcomes
*Primary efficacy outcome. Patients who were lost to follow-up were classified as having had a primary outcome event.†Prespecified secondary outcome.RR=relative risk.
p<0.001(for superiority, each dose)
RR (95% CI):
p<0.001RR (95% CI):
Recurrent VTE or VTE-Related Death†Recurrent VTE or All-Cause Death*
2.5 mg:0.33
(0.22–0.48)
5 mg:0.36
(0.25–0.53) 2.5 mg:0.19
(0.11–0.33)
5 mg:0.20
(0.11–0.34)
n=96 n=32 n=34 n=73 n=14 n=14
Pat
ien
tsw
ith
eve
nt,
%
Die empfohlene Dosis zur verlängerten Prophylaxe von rezidivierendenTVT und LE ist ausschließlich Apixaban 2,5 mg 2 x täglich. Agnelli G et al. N Engl J Med 2013;368:699–708.

AMPLIFY-EXT: Major and CRNM bleeding
Agnelli G et al. N Engl J Med 2013;368:699–708.
p=NS
RR (95% CI):
Bleeding
n=4n=2 n=1 n=22 n=27 n=35
2.5 mg:0.49
(0.09–2.64)
5 mg:0.25
(0.03–2.24)
2.5 mg:1.20
(0.69–2.10)
5 mg:1.62
(0.96–2.73)
p=NS
RR (95% CI):
*Primary safety outcome
Pat
ien
tsw
ith
eve
nt,
%
Die empfohlene Dosis zur verlängerten Prophylaxe von rezidivierendenTVT und LE ist ausschließlich Apixaban 2,5 mg 2 x täglich.

VTE-Sekundärprophylaxe mit Eliquis
Langfristige VTE-Sekundärprophylaxe: nur Eliquis 2 x 2,5 mgvorgesehen
Problem bei Hochrisiko-Patienten (APS, ...) ?

X.Wang et al., J Clin Pharmacol. 2015 Aug 31. doi: 10.1002/jcph.628
Apixaban 5 mg
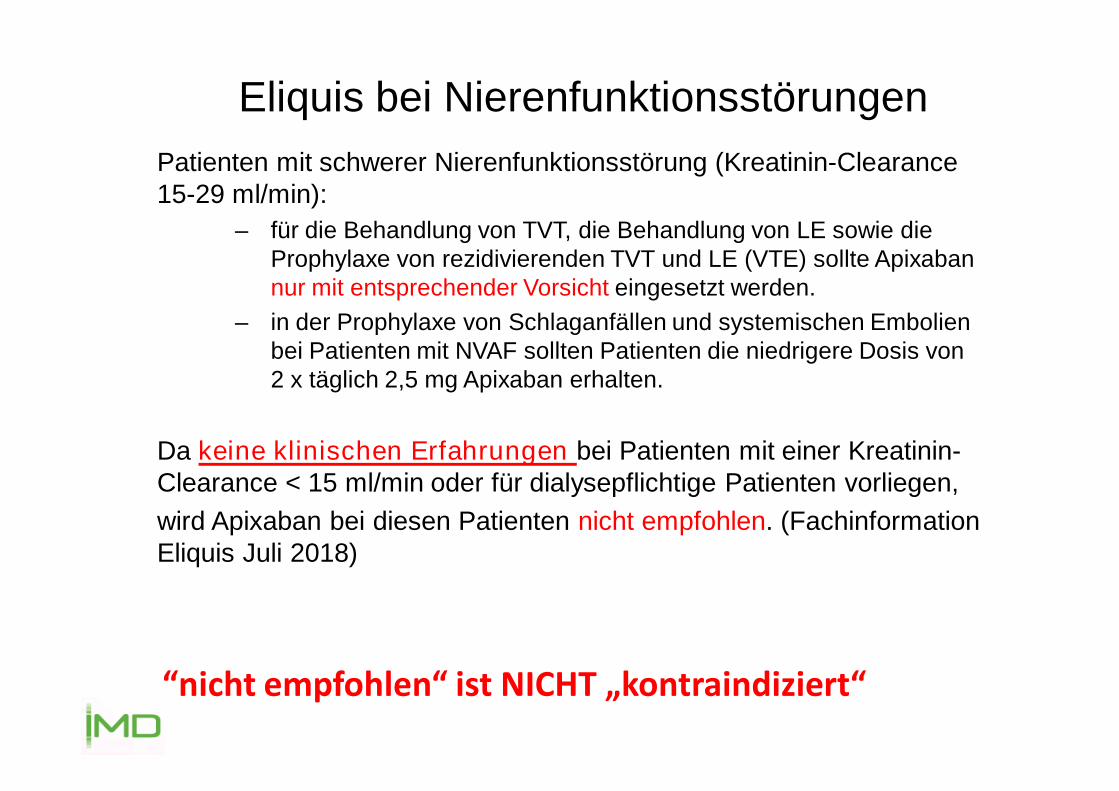
“nicht empfohlen“ ist NICHT „kontraindiziert“
Patienten mit schwerer Nierenfunktionsstörung (Kreatinin-Clearance15-29 ml/min):
– für die Behandlung von TVT, die Behandlung von LE sowie dieProphylaxe von rezidivierenden TVT und LE (VTE) sollte Apixabannur mit entsprechender Vorsicht eingesetzt werden.
– in der Prophylaxe von Schlaganfällen und systemischen Embolienbei Patienten mit NVAF sollten Patienten die niedrigere Dosis von2 x täglich 2,5 mg Apixaban erhalten.
Da keine klinischen Erfahrungen bei Patienten mit einer Kreatinin-Clearance < 15 ml/min oder für dialysepflichtige Patienten vorliegen,
wird Apixaban bei diesen Patienten nicht empfohlen. (FachinformationEliquis Juli 2018)
Eliquis bei Nierenfunktionsstörungen

R.Chokesuwatanaskul et al., Pacing Clin Electrophysiol. 2018;41:627–634.
Compared to VKAs, apixaban was significantly associated with reduced risk of majorbleeding (pooled OR, 0.42; 95% CI: 0.28–0.61)
When meta-analysis was limited only to studies in patients with ESRD on dialysis, thepooled OR of major bleeding was 0.27 (95% CI: 0.07–0.95).
There was no significant difference in risk of thromboembolic events in advanced CKDor ESRD patients on apixaban versus VKAs (pooled OR, 0.56; 95% CI: 0.23–1.39)
... 1,291 advanced CKD/ESRD patients who received apixaban ...
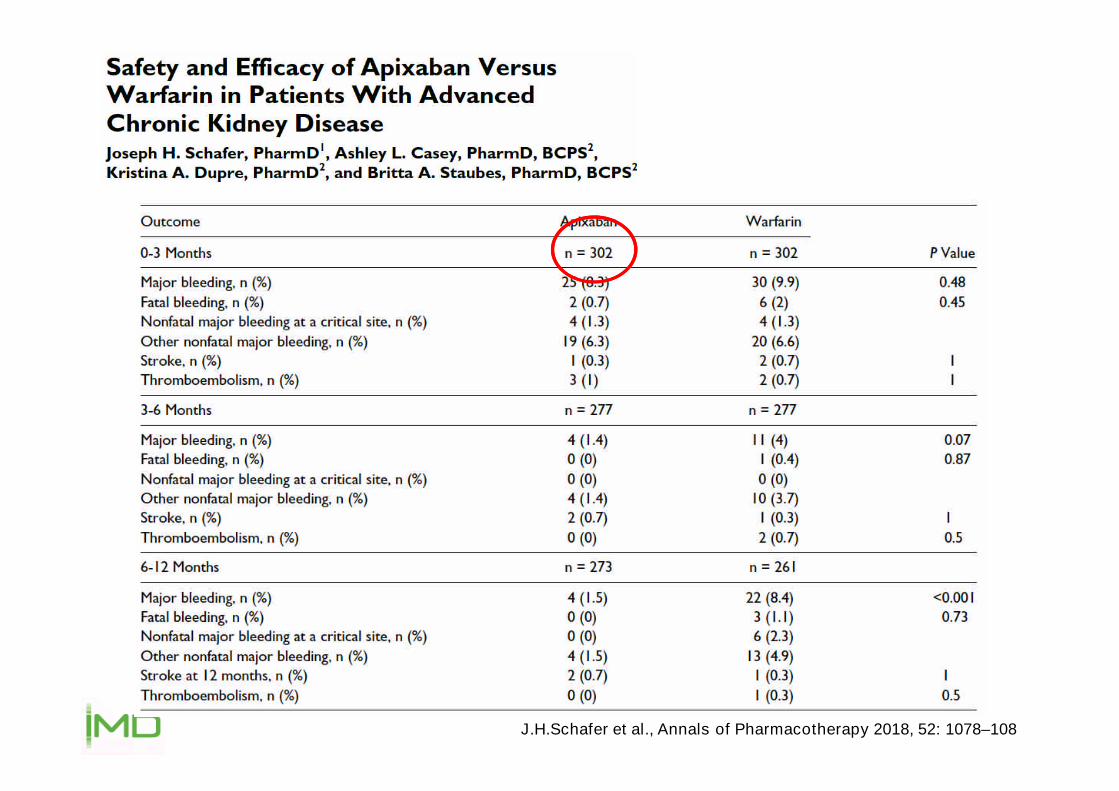
J.H.Schafer et al., Annals of Pharmacotherapy 2018, 52: 1078–108

D.Reed et al., Res Pract Thromb Haemost. 2018;2:291–298.
Compared to warfarin, our findings suggest that apixaban is a safe and effectivealternative in patients with ESRD maintained on dialysis, with apixaban patientsexperiencing fewer bleeding events than warfarin patients.
... apixaban (n=74) or warfarin (n=50) ...
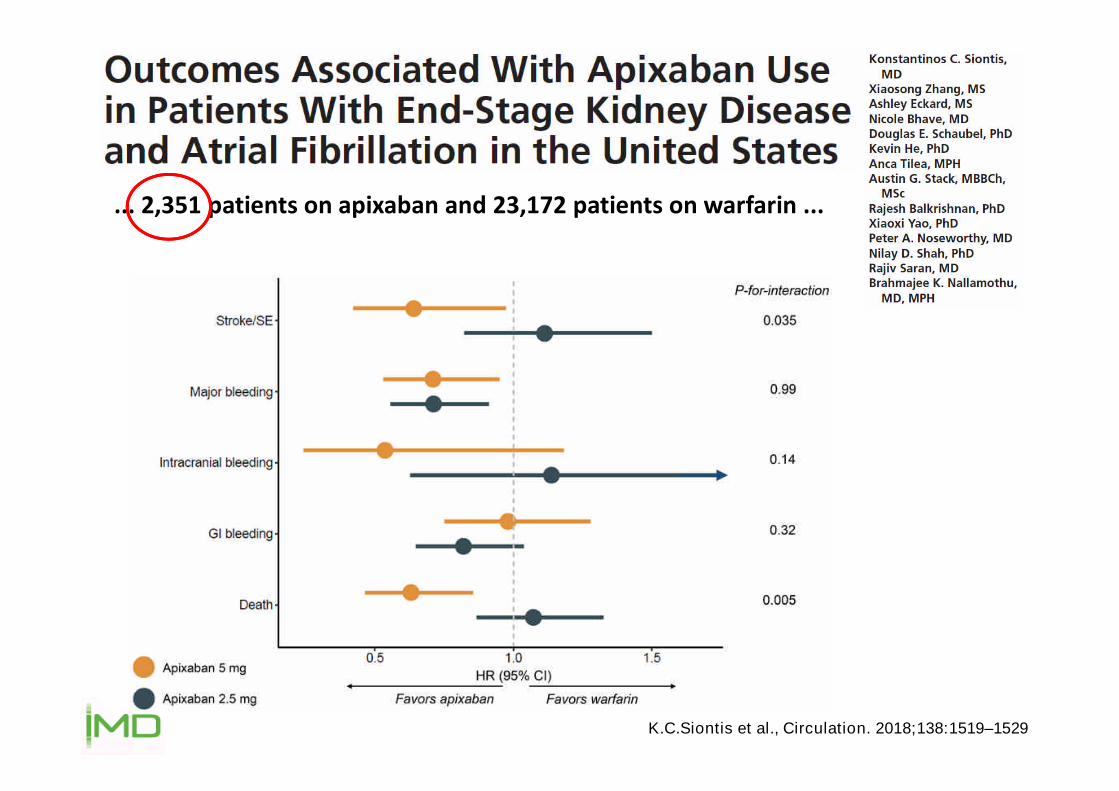
K.C.Siontis et al., Circulation. 2018;138:1519–1529
... 2,351 patients on apixaban and 23,172 patients on warfarin ...

Kommende Studien
RENAL-AF:Apixaban 2 x 5 mg vs. Warfarin INR 2-3 bei niereninsuffizientenPatienten mit Hämodialyse
AXADIA:Apixaban 2 x 2,5 mg vs. Phenprocoumon bei Patienten mit ESRD


Edoxaban
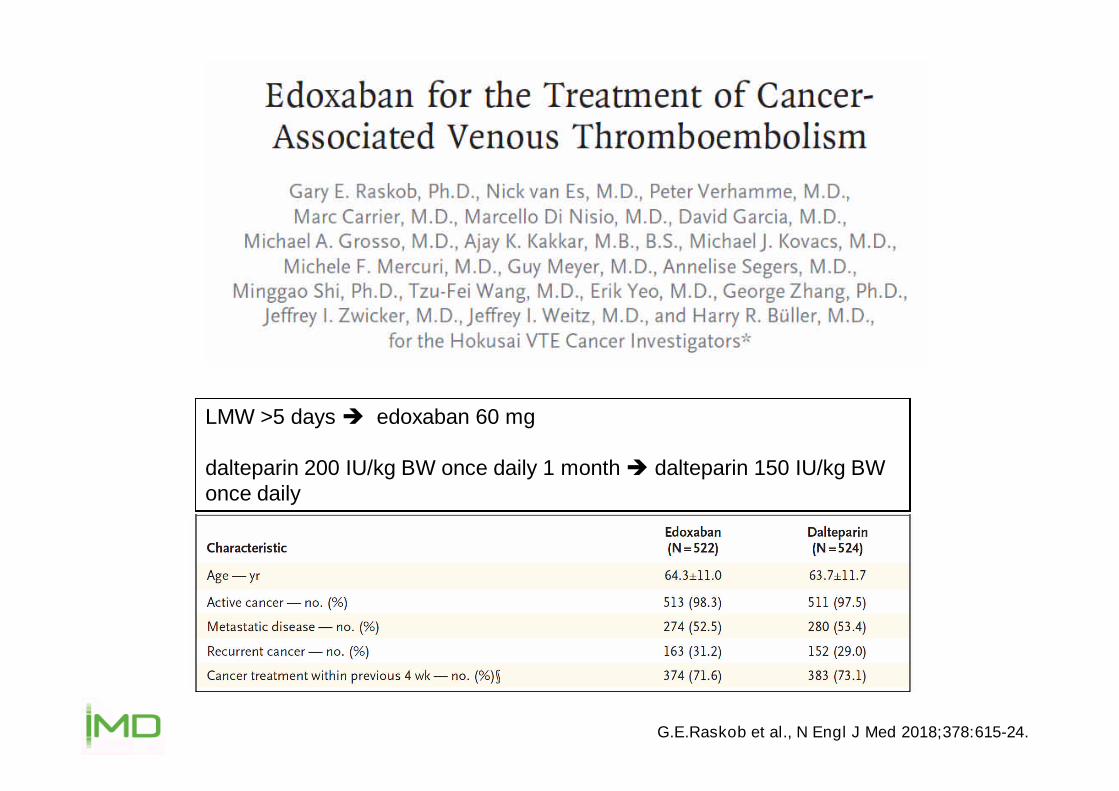
G.E.Raskob et al., N Engl J Med 2018;378:615-24.
LMW >5 days edoxaban 60 mg
dalteparin 200 IU/kg BW once daily 1 month dalteparin 150 IU/kg BWonce daily

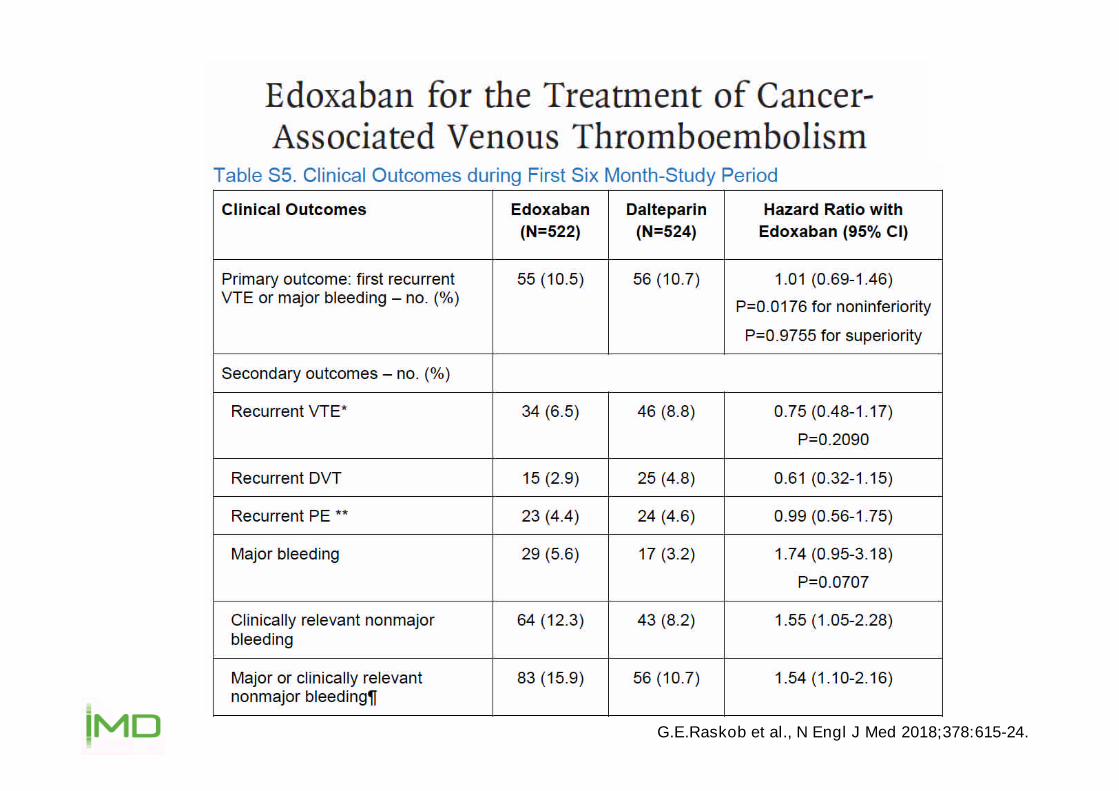
G.E.Raskob et al., N Engl J Med 2018;378:615-24.

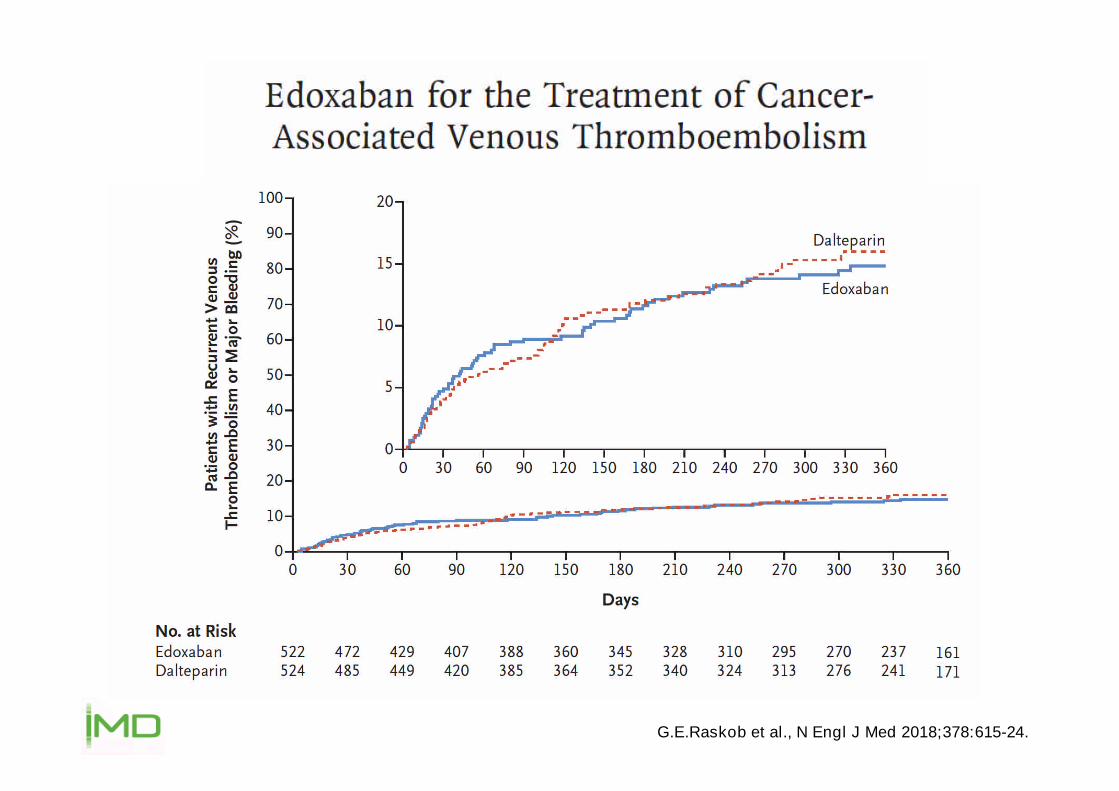
G.E.Raskob et al., N Engl J Med 2018;378:615-24.

G.E.Raskob et al., N Engl J Med 2018;378:615-24.
G.E.Raskob et al., N Engl J Med 2018;378:615-24.
G.E.Raskob et al., N Engl J Med 2018;378:615-24.
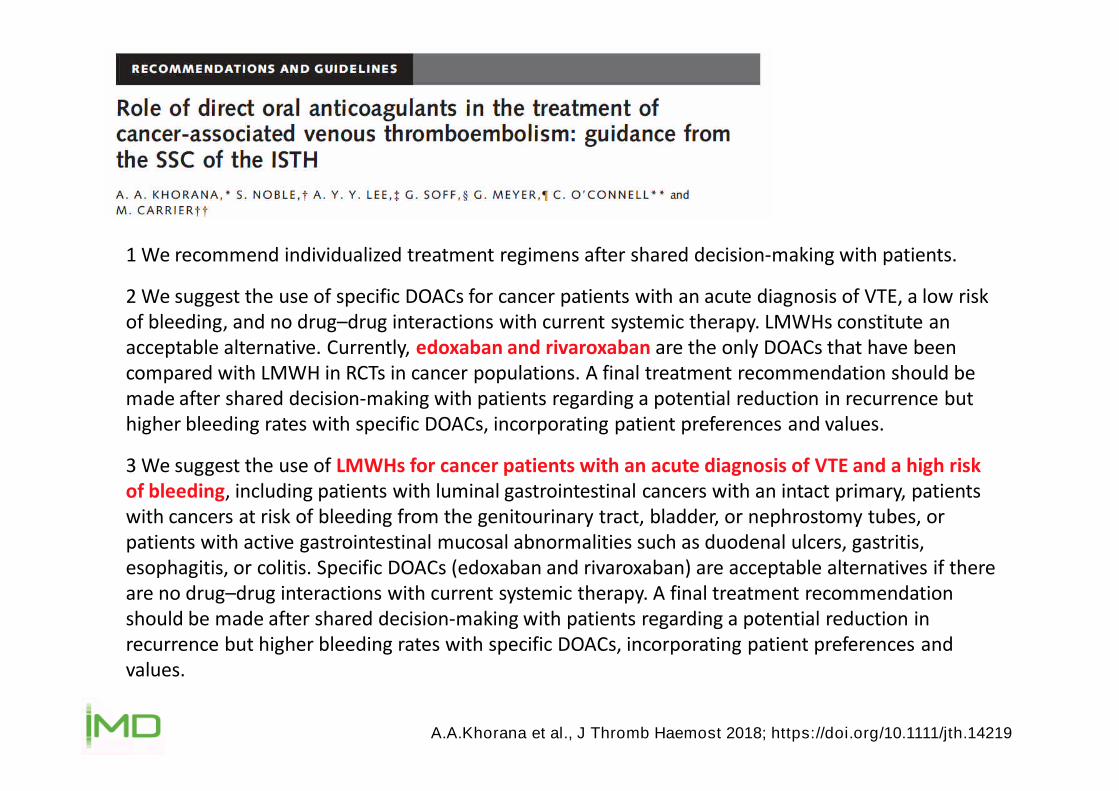
A.A.Khorana et al., J Thromb Haemost 2018; https://doi.org/10.1111/jth.14219
1 We recommend individualized treatment regimens after shared decision-making with patients.
2 We suggest the use of specific DOACs for cancer patients with an acute diagnosis of VTE, a low riskof bleeding, and no drug–drug interactions with current systemic therapy. LMWHs constitute anacceptable alternative. Currently, edoxaban and rivaroxaban are the only DOACs that have beencompared with LMWH in RCTs in cancer populations. A final treatment recommendation should bemade after shared decision-making with patients regarding a potential reduction in recurrence buthigher bleeding rates with specific DOACs, incorporating patient preferences and values.
3 We suggest the use of LMWHs for cancer patients with an acute diagnosis of VTE and a high riskof bleeding, including patients with luminal gastrointestinal cancers with an intact primary, patientswith cancers at risk of bleeding from the genitourinary tract, bladder, or nephrostomy tubes, orpatients with active gastrointestinal mucosal abnormalities such as duodenal ulcers, gastritis,esophagitis, or colitis. Specific DOACs (edoxaban and rivaroxaban) are acceptable alternatives if thereare no drug–drug interactions with current systemic therapy. A final treatment recommendationshould be made after shared decision-making with patients regarding a potential reduction inrecurrence but higher bleeding rates with specific DOACs, incorporating patient preferences andvalues.
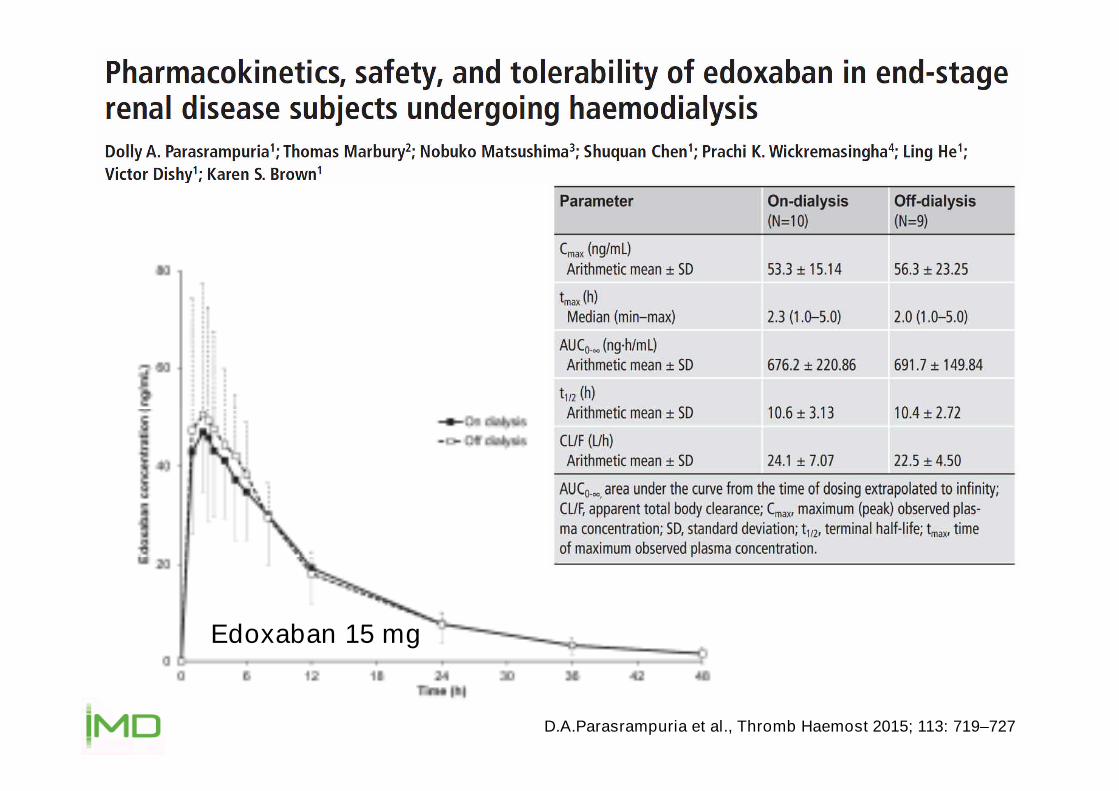
D.A.Parasrampuria et al., Thromb Haemost 2015; 113: 719–727
Edoxaban 15 mg
Dabigatran

54th Ann Mtg of the American Society of Hematology (ASH), Atlanta, 8 - 11 Dec 2012 (Poster)

International Stroke Conference 2015; Nashville, Poster CT P28
Idarucizumab
• Bindungsaffinität für Dabigatran ~350 mal höher als die Bindung vonDabigatran zu Thrombin
• keine prokoagulatorische oder antikoagulatorische Wirksamkeit
• intravenöse Applikation, sofortiger Wirkeintritt
• Standard-Dosis 5 g
Glund S et al. AHA 2013; abstract 17765;van Ryn J. AHA 2012; Presentation 9928; van Ryn J et al. Circulation 2012;126:A9928
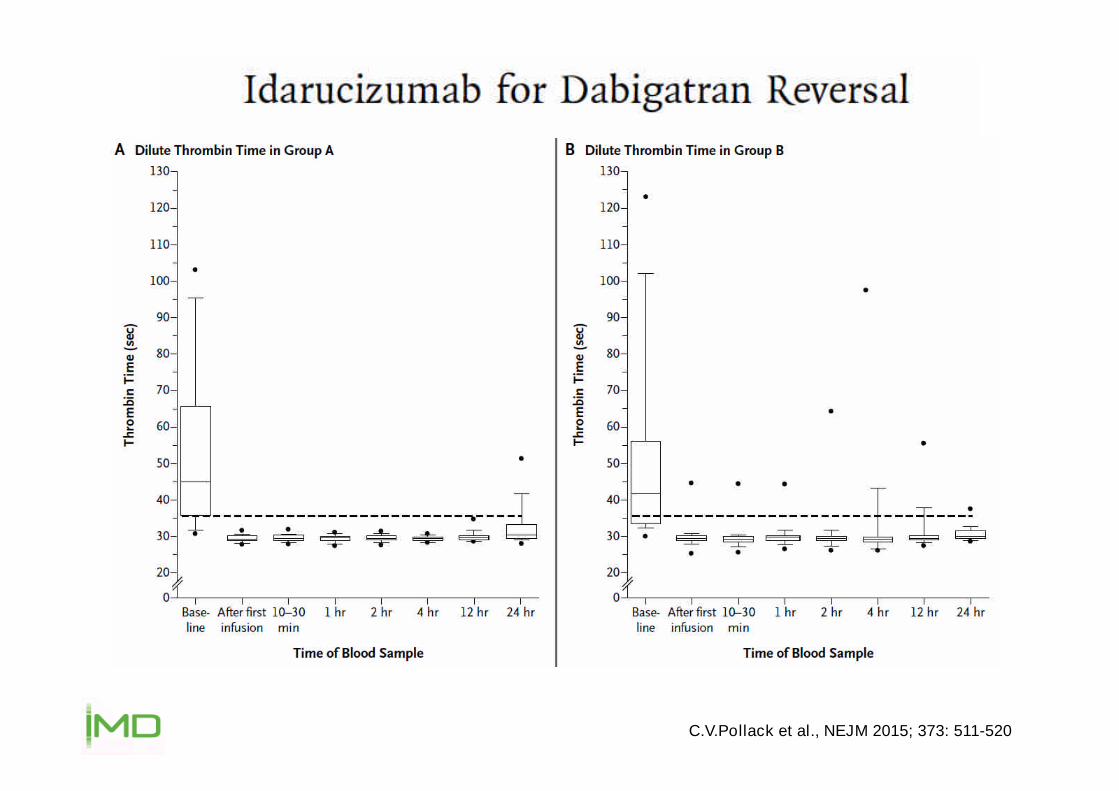
C.V.Pollack et al., NEJM 2015; 373: 511-520
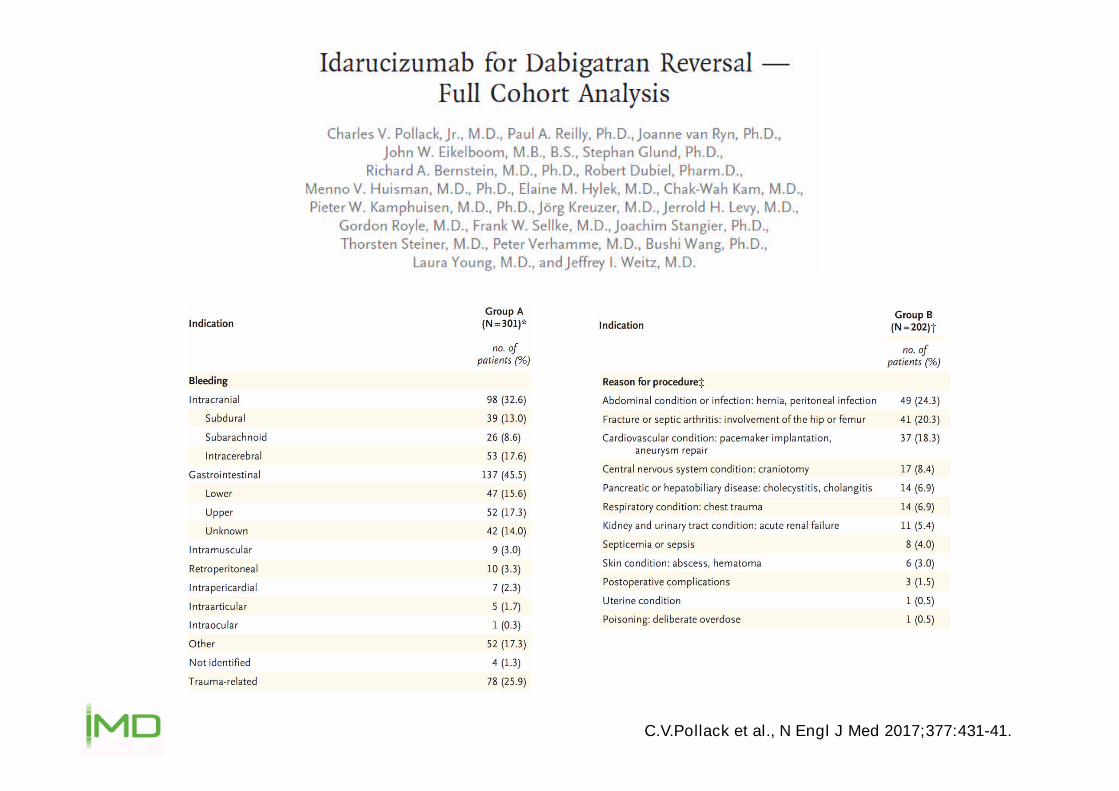
C.V.Pollack et al., N Engl J Med 2017;377:431-41.

C.V.Pollack et al., N Engl J Med 2017;377:431-41.
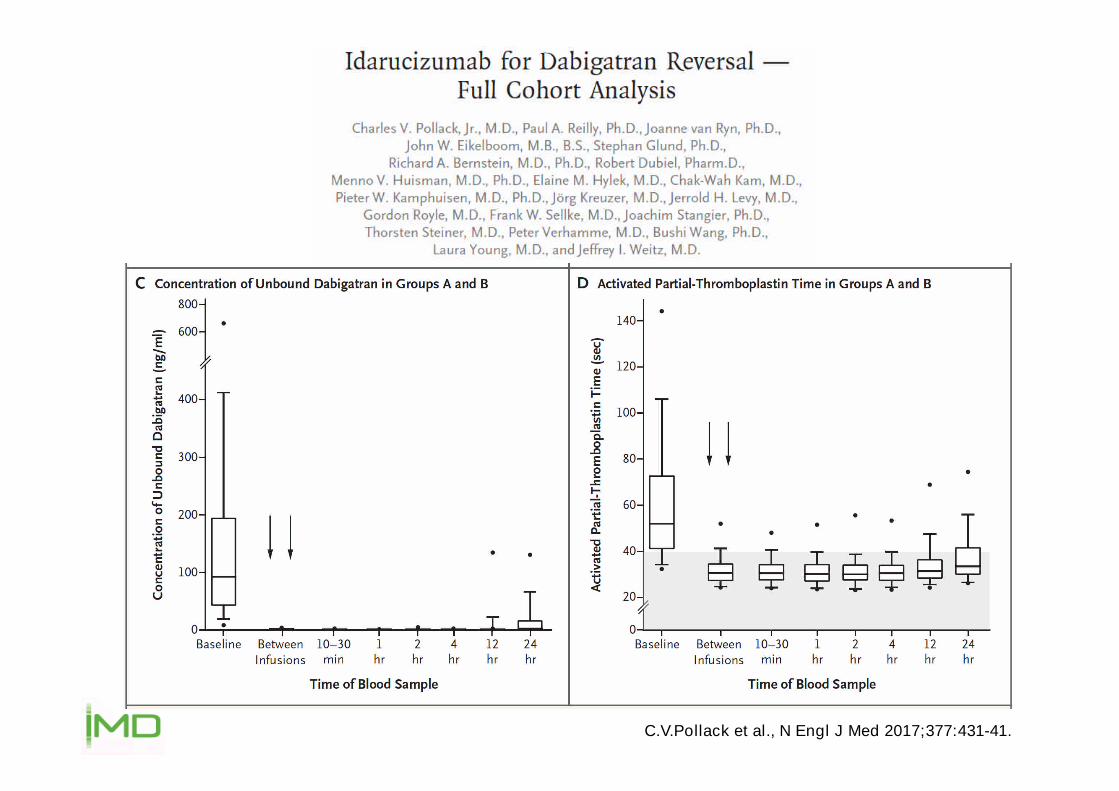
C.V.Pollack et al., N Engl J Med 2017;377:431-41.

Dabigatran nach Idarucizumab
Glund S et al. ASH 2014, San Francisco Dec 06-09; Blood 124 (21): Abstract 334
Zeit nach Infusionsende (Std.)
747260483626242220181614121086420-2
dTT
(s)
80
75
70
65
60
55
50
45
40
35
30
45–64 Jahre (n=12), Dabigatranetexilat 220 mg BID
+ Idarucizumab 5 g
Oberer Normalwert
Mittlerer Basiswert
Ende der Idarucizumab-Infusion (5-min)
DabigatranIdarucizumab
WiederbeginnDabigatran
Spitzen-spiegel
Talspiegel

Five minutes after the administration of 5 g idarucizumab, weinitiated systemic intravenous thrombolysis with alteplase (6 mginjection bolus followed by 54 mg over 60 minutes).
We treated the patient with an intravenous bolus of 5 g idarucizumabgiven for 5 minutes to antagonize the anticoagulant effect ofdabigatran. Immediately afterward, intravenous thrombolysis with 69mg r-tPA, equivalent to 0.9 mg r-tPA/kg body weight was initiated.






























