Embed Size (px)
DESCRIPTION
Zirconium and porcelain fused to metal
Citation preview

38 Australasian Dentist
Restoration of heavily-filled, fractured, worn or congenitally malformed teeth is
very commonly achieved through use of the full coverage crown. Similar restorations are used as the abutments for conventional fixed bridgework and so it is easy to see why they have become the most widely prescribed of all indirect restorations.
For many years, gold was the only realistic option when crowning molar and premolar teeth, and restorations of this type continue to provide superb long-lasting service for many patients. Full gold crowns exhibit great strength, allow relatively minimal tooth preparation and demonstrate excellent biocompatibility together with minimal damage to opposing teeth. Gold’s great strength, combined with its ductility, permits the use of knife-edge mar-gins and cross-sectional thicknesses as low as 1mm. Indeed, the full gold crown continues to set the standard by which other full coverage restorations are judged, and many experienced practitioners continue to favour the use of gold for the restoration of lower first and second molars because of the considerable occlusal loading placed on these teeth. The gold crown’s only real drawback is its appearance, which is considered unacceptable by many patients. The desire for an aesthetic solution led firstly to the development of the porcelain-fused-to-metal
(PFM) restoration and ultimately to the various all-ceramic types that are available today.
While there is no doubting the success of pressed ceramics such as Empress (Ivoclar Vivadent) when used to restore the anterior segment, the use of all-ceramic materials to restore posterior teeth has, to date, been some-what more problematic. It would probably be fair to say that there have been a number of false dawns in the shape of systems that prom-ised much and were certainly aesthetic, but in the end simply did not provide consistent durability.
However, with the appearance of zirco-nium-based systems there does, at last, seem to be a credible all-ceramic alternative to the dominant PFM restoration and the remainder of this article compares the various characteris-tics and properties of the two restorations.
Porcelain-fused-to-metal restorations
PFM restorations were introduced in 1962 following the development of porcelains ther-mally compatible with dental alloys during firing. It was now possible for porcelains to be fired successfully onto metal substructures, so successfully in fact that, around the world, PFM restorations still comprise over three-quarters of all indirect restorations.
Dr David Penn
Comparing porcelain-fused-to-metal versus zirconium-based restorations Dr David Penn examines the pros and cons of porcelain-fused-to metal versus zirconium-based restorations.
By Dr David Penn
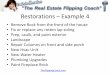
Figure 1. The “greying” effect of an implant fixture and root filled 2.1 needed an all ceramic solution in both abutment type and crown/veneer material to produce an outstanding aesthetic result.
clinical Article AwAiting cPD Point APProvAl from the DentAl BoArD.
Please refer to our website for updates: www.australasiandentist.com.au

Australasian Dentist 39
Aesthetics As alluded to in the introduction, there is less and less justification for using the PFM restoration to restore anterior teeth given the availability of highly aesthetic, translucent, sufficiently strong pressed ceramic systems. These days, anterior PFM restorations are usually reserved for the following situations: 1. In patients exhibiting excessive
occlusal loading, tooth wear, brux-ism, etc, or where insufficient interocclusal clearance exists to accommodate porcelain. Here, a palatal metal surface is highly beneficial because of its resistance to fracture
2. Where the degree of tooth discol-ouration to be masked is such that the restoration’s inherent opacity becomes an advantage. Clearly, the major role of the PFM restora-tion is in the posterior segments and their continued widespread use is testimony to their longev-ity and durability.1 When planned and executed properly, the PFM restoration is capable of providing a highly acceptable aesthetic out-come, although without due care and attention all too many appear lifeless and unnatural. The most common cause of this is inadequate tooth preparation, leaving the tech-nician without enough space for sufficient thickness for veneering ceramic to block out the colour and opacity of the metal substructure. The result is either a dull, opaque appearance or an overbuilt contour, or a combination of both of these . For PFM restorations to have any
chance of appearing life-like, suffi-cient tooth structure (at least 1.5mm) must be removed to accommodate both metal and ceramic. This degree of reduction is also necessary to ensure that the porcelain is fully sup-ported by the underlying metal core.2 As dentists we are constantly walking a tightrope between, on the one hand, under-preparation and, on the other, removing too much tooth structure, which may compromise retention and can lead to pulp damage. The fact that countless PFM restorations have been placed using improperly mixed zinc phosphate cement undoubtedly adds insult to injury, compounding the assault on the pulp.
Two other aesthetic concerns with PFMs are:
1. Long-term colour stability It is quite common for PFM restora-tions to become lighter over time
as the superficial stains placed by the technician to characterise the appearance are gradually dissolved by patients’ consumption of acidic drinks and foods
2. Exposure of restoration margins Even if the margins of PFM restorations are placed slightly subgingivally, it is usually only a matter of time before the gingival tissues recede and the dark, unattractive, margins become visible (Figure 2). It is possible to mitigate this somewhat by trimming back the margin of the metal coping slightly, thus allowing the incorpora-tion of an all-ceramic margin (Figure 3a). All this is relative though, and exposed PFM restoration margins that are visible when the patient smiles are never attractive (Figure 3b)
Tooth wear Older PFM restorations were veneered using large-particle size ceramic materials and these are known to
cause wear of the opposing dentition, an effect exacerbated whenever occlu-sal grinding of the ceramic is carried out and the surface is left unglazed. The smaller particle size of current ceramics has greatly reduced such wear, although whenever possible, unglazed, roughly finished porcelain surfaces should be avoided.
Metal sensitivity There have been many reports in the literature of gingival reactions to various elements . In PFM restoration copings – in particular Nickel and Beryllium.
Restoration design PFM restorations are extremely ver-satile and have been modified to act as retainers for a variety of designs of ‘conventional’ bridgework. The use of precision attachments and stress breakers has enabled long-lasting bridgework to be placed in less than optimal clinical situations.
Cementation Cement formulations have evolved significantly over the years from zinc phosphate, through polycarboxylate, glass ionomer resin, resin and resin-modified glass ionomers (RMGI), to the most recent resin cements combined with self-etch primer. In general, RMGI cements, e.g. FujiCem (GC) and RelyX Luting Plus (3M Espe), are best for routine use because of their potential for fluoride release, moderate strength and ease of use. In situations where high strength is required, such as crown preparations with inadequate retentive properties, then resin-based composite cements such as Panavia F (Kuraray), Multilink (Ivoclar Vivadent) and RelyX Unicem (3M Espe) are recommended.
Dealing with failure PFM restorations can fail in a number of different ways. ‘Primary’ failure is where the restoration itself fails, for example through complete or partial loss of the porcelain. This can happen through faulty laboratory procedures or, more likely, because of crack prop-agation within the porcelain induced over time by excessive occlusal load-ing and/or unsupported veneering porcelain. It may be possible to repair/replace the lost porcelain by means of products such as CoJet silicate ceramic surface treatment system (3M Espe), which, if successful, provides an eco-nomical alternative to replacing the
Figure 2. These PFM restorations have been successful for 15 years but their opacity and lifeless appearance in tandem with the root exposure had the patient seeking a more aesthetic option.
Figure 3b. These long standing PFM restorations have only failed for aesthetic reasons
Figure 3a. 360 degree all ceramic margins offer significantly improved aesthetics but require more aggressive tooth preparation.
clinical

40 Australasian Dentist
restoration. In many cases though, the restoration will require replacement.
‘Secondary’ failures include the crown coming off because of inad-equate retention form; caries and peri-odontal disease, both of which may arise due to poor marginal fit and/or poor emergence profile, which results in plaque accumulation. Again, it may be possible to adjust and repair the situation but more often than not the restoration will need to be replaced.
Removal of a well-retained PFM restoration is usually best achieved by sectioning the crown using a bur such as Midway’s fine crosscut Beaver bur (Dentsply) either alone or in conjunc-tion with a crown remover. When the tooth has been root-filled (or the crown is being removed to permit root canal treatment), the latter option is usually the most sensible as it is all too easy to fracture the already weak-ened tooth.
Zirconium-based restorations While PFM restorations offer the pos-sibility of a more aesthetic appearance than gold (at least in the eyes of some), they are nevertheless something of a compromise and for many people the ideal posterior crown would be all-ceramic and capable of withstanding heavy occlusal forces.
This ideal is now within reach in the shape of a new generation of resto-rations utilising internal copings made
from zirconium ceramic. Zirconium oxide is a polycrystalline material with a tetragonal structure partially stabilised with yttrium oxide yielding an almost total absence of structural porosities (Figure 7). This structure results in great strength and fracture resistance (>900MPa) and examples include Cercon (Dentsply), Lava (3M), Procera Zirconia (Nobel Biocare) and the newer generation Calypso PFZ ( Southern Cross)
As with the PFM restorations, great care must be taken in planning, correct case selection3 and tooth prep-aration – for example, zirconia-based restorations also require enough clear-ance to permit sufficient thickness of core and veneering ceramics, and the ideal margin design is a 360º deep chamfer. For these restorations to function correctly, the porcelain must be fully supported and be of adequate thickness.
Other comparisons with PFM res-torations include the following:
AestheticsThe newer generation zirconium-based restorations ( Calypso SCDL) are generally considered to be superior to PFM restorations, given ideal room for the veneering ceramic. While the zirconium substructure is opaque, it is nevertheless much lighter in colour and therefore masking it is less of a problem than with a PFM restoration. Some systems use a very white coping
material while, increasingly, manu-facturers are offering multiple-shaded copings. As with the PFM restoration, it is possible for the technician to trim the coping back in order to cre-ate a more natural cervical margin. For this reason it is likely that if and when gingival recession occurs, the resulting visible margin will be less offensive than the exposed margin of a PFM restoration. (Figure 4)
Given that zirconia-based restora-tions use similar veneering ceramics to PFM restorations, they are likely to behave similarly to the latter in terms of long-term colour stability and opposing tooth wear. If the underlying zirconium core is exposed as result of occlusal adjustment then it is thought this would have a very damaging effect on opposing teeth, as it is both hard and abrasive
BiocompatibiltyZirconium-based restorations appear to induce little in the way of a gin-gival reaction, a clear advantage over the PFM restoration. One negative biological aspect, however, is the pos-sibility of pulpal damage brought on as a result of the need for considerable tooth reduction
ApplicationsGiven zirconium’s great strength, it can also be used for the substructures of fixed bridges, with current recom-mendations allowing spans of up to six units. This varies with each particular system, each manufacturer recommending a maximum span for its own material.
Currently, though, precision attachments and stress-breaking components are not available and this therefore limits to some extent the scope of zirconium-based bridgework u Cementation – as with PFM
restorations, RMGI cements are recommended for routine use and resin-based composite cements for situations where retention is compromised
u Dealing with failure – failures of zirconium-based restorations are similar in nature to those occurring with PFM restorations but in comparison are more trou-blesome to deal with because of a) the intrinsic nature of the zirconium core, and; b) the fact that the restoration is likely to be more effectively bonded to tooth structure than a PFM restoration. For example, the zirconium core is extremely hard and difficult to
clinical
Figure 4c: Cemented crowns demonstrate improved emergence profile, morphology and masking ability of Calypso PFZ
Figure 4b: The original gold posts and cores and remaining dentine are difficult to mask
Figure 4a: These In-Ceram crowns were placed more than 10 years ago but have failed for aesthetic reasons only.

Australasian Dentist 41
clinical
Dr David Penn is in private practice in Sydney, Australia, and is managing director of Southern Cross Dental Laboratories (Australia).
remove and, at the same time, cre-ating very high temperatures that can clearly damage the tooth’s pulp. It is strongly advised to use burs specifically designed for this task such as the Great White Z diamond zirconia cutting bur (SS White) or the Magic Touch 6/018PF-blue diamond bur (Strauss Diamond Instruments Inc) along with the use of ample coolant dur-ing the cutting process. As with PFM restorations, first
create a groove in the porcelain and cut through the hard ceramic before using an instrument to remove the crown. These difficulties are com-pounded when multi-unit restorations are involved. There is no easy way to deal with these situations and the old adage ‘prevention is better than cure’ is extremely pertinent – thorough treatment planning, case selection and clinical execution is essential.
conclusion PFM restorations have provided many years of excellent service but they nevertheless do have drawbacks. Zir-conium-based crowns may prove to be
the answer but only time will tell if they exhibit similar levels of durabil-ity as the PFM restoration.4 In general terms, zirconium-based restorations tend to have better aesthetics, more acceptable marginal appearance and reduced soft tissue reaction. Long-term colour stability and effect on opposing teeth are likely to be similar to that seen in PFM restorations, as the external ceramic materials are similar.5
Prostheses requiring precision attachments or stress breakers are currently best made with PFM resto-rations. As always, any restoration, whichever type used and comprising however many units, requires thor-ough planning, careful clinical tech-nique and excellent communication between dentist and laboratory. u
references1. Christensen, G. Longevity of posterior
dental restorations. J Am Dent Assoc, 2005: Vol 136, No 2, 201-203
2. Christensen,G. Frequently encountered errors in tooth preparations for crowns. J Am Dent Assoc
3. Della Bona, A and Kelly, JR The clinical success of all ceramic restorations. J Am Dent Assoc, 2008 Vol 139, No suppl_4, 8S-13S
4. Sailer I, Feher A, Filser F, et al. Prospec-tive clinical study of zirconia posterior fixed partial dentures: 3-year follow-up. Quintessence Int 2006;37(9):685–93
5. Donovan, T E : Factors Essential for Suc-cessful All-Ceramic Restorations J Am Dent Assoc, 2008: Vol 139, No suppl_4, 14S-18S
1. The new generation PFZ crowns exhibit greater flexural strength than conventional PFM crowns.
2. PFZ crowns can be finished with knife edge margins
3. Given an ideal preparation, PFZ crowns are now considered to be more aesthetic than PFM crowns.
4. Crown preparations for PFZ crowns are identical to those of conventional PFM crowns
5. The weakest part of the PFZ crown and most common area for failure is the union between the veneering ceramic and the zirconia coping
6. PFZ crowns are suitable for patients with bruxism, espe-cially in the posterior segment
7. Diamond Burs are ideal to remove PFZ crowns
8. The selection of either type of restoration does not guaran-tee the long term vitality of the pulp
9. Porcelain buccal shoulders generally improve the aesthetic properties of PFM crowns
10. Cracks do not propagate through to the veneering ceramic in PFM because of the tooth preparation performed
11. Zirconia is an ideal material for porcelain veneers when attempting to mask dark dentine
12. Both PFM and PFZ crowns now can achieve aesthetics simi-lar to other crown types such as e.Max or Procera Alumina
CPD Quiz: True or False
Figure 5. 3 unit Calypso PFZ bridge displaying excellent aesthetics and marginal integrity
Figure 6. The latest PFZ crowns use zirconia blocks of varying colours and opacities and are then dipped in special dyes to match most shade guides. The specifically designed venering ceramics are far more translucent and can generally produce excellent aesthetics in 0.6mm thickness (over a 0.6mm zirconia coping) meaning a reduction of at least 1.2mm is critical for success.