Embed Size (px)
Citation preview

HISTORY 42-year-old white man.
CHIEF COMPLAINT: Hypertension discovered in routine insurance
examination.
PRESENT ILLNESS: At age 22 a “slight” elevation in blood pressure was
noted on a military discharge physical examination. Since then he has gained
30 pounds, continued to smoke one package of cigarettes a day and has no
regular program of exercise. In the past he has noted mild dyspnea on exertion
and occasional headaches in the evening.
There is no history of heart murmur, renal disease, diabetes, or chest pain.
Proceed
36-1

PRESENT ILLNESS (continued): He has had no history of weakness,
polyuria, syncope, paroxysmal sweating, palpitations or abdominal pain. He
takes no drugs. His cholesterol has never been measured.
FAMILY HISTORY: An older brother has hypertension. His father also had
hypertension and died suddenly of a “heart attack.”
Question: Based on this history, what is your initial diagnostic impression?
36-2

Answer: The patient probably has primary (essential) hypertension.
In well over 90% of patients, hypertension is primary. This patient has no
historical clues to a secondary cause. With a positive family history, primary
hypertension is even more likely. Secondary causes of hypertension should
still be considered. In most cases, they may be excluded by the history,
physical examination and simple laboratory tests.
Question: What are the major causes of secondary hypertension?
36-3

Answer: The major causes of secondary hypertension include:
I. Adrenal
– Pheochromocytoma
– Hyperaldosteronism
– Cushing’s syndrome
II. Renal
– Parenchymal disease
– Vascular (e.g., arterial stenosis)
– Obstructive uropathy
III. Exogenous
– Drugs (e.g., NSAIDS, steroids, birth control pills)
IV. Coarctation of the aorta
Question: Has the history excluded any of these diagnoses?
36-4

Answer: Most of the causes of secondary hypertension have been virtually
excluded by the history.
Pheochromocytoma is usually associated with “spells.” A convenient mnemonic
is the 6 “P’s”–pheochromocytoma, paroxysms, perspiration, postural
hypotension, palpitations and pain (headaches). Obesity is uncommon, weight
gain is rare. Hyperaldosteronism is frequently associated with polyuria and
weakness. Cushing’s syndrome is primarily excluded by physical examination
and laboratory tests.
Proceed
36-5

There is no history to suggest glomerulonephritis, urinary infections or
obstructive uropathy. Physical examination is also important to detect some
causes of renal hypertension.
There is no history of drug use. If the patient were a woman, she should be
closely questioned about birth control pills.
Coarctation is best excluded by physical examination. In addition, there is no
history of murmur.
Question: How do you interpret the patient’s complaint of headache?
36-6

Answer: It is not uncommon for patients with hypertension to complain
of headache, tinnitus and nosebleeds, but these symptoms are not of
diagnostic value, as they are no more frequent in hypertensive patients than in
the general population.
The headache associated with severe hypertension is classically occipital in
location and is present upon awakening in the morning.
Questions: 1. What risk factors for coronary artery disease have been identified
by the history?
2. How do you interpret the patient’s dyspnea?
36-7

Answers: 1. Hypertension, smoking, and a positive family history are all risk factors for
coronary artery disease in this patient.
2. His exertional dyspnea may reflect his weight gain, smoking, poor physical
fitness and/or left ventricular dysfunction.
PHYSICAL SIGNS
a. GENERAL APPEARANCE - Normal appearing, moderately obese man.
Question: How is this patient’s general appearance helpful in excluding
secondary causes of hypertension?
36-8

Answer: The general appearance makes Cushing’s syndrome unlikely (no
“buffalo hump,” centripetal obesity, striae, or change in hair pattern). Rarely,
pheochromocytoma may be associated with neurofibromatosis, and coarctation
of the aorta with Turner’s syndrome.
Proceed
36-9

PHYSICAL SIGNS (continued)
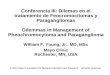
b. JUGULAR VENOUS PULSE - The CVP is estimated to be 5 cm H2O.
Question: How do you interpret the jugular venous pulse?
1.0 SECOND
S1 S2
JUGULAR
VENOUS
PULSE
ECG
PHONO
LOWER LEFT
STERNAL EDGE
36-10

Answer: The CVP and jugular venous pulse are normal.
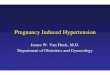
c. ARTERIAL PULSE - (BP = 170/110 mm Hg, right arm, lying)
Questions:
1. How do you interpret the blood pressure and arterial pulse?
2. What additional information concerning the blood pressure and arterial
pulses is required?
CAROTID
ECG
PHONO
LOWER LEFT
STERNAL EDGE S2
S1
36-11

Answers: 1. There is systolic and diastolic hypertension. The carotid pulse contour
is normal.
2. The blood pressure should be recorded in both arms lying and standing. It
should also be recorded in the legs, and the upper and lower extremity
pulses should be simultaneously palpated.
The blood pressure measured in the left arm, lying, was also
170/110 mm Hg. It did not change upon standing. Postural hypotension
may be seen in renovascular disease and pheochromocytoma, and its
absence is a significant negative finding.
The blood pressure is normally higher in the legs. In this patient, the
pressure measured with an appropriate size thigh cuff was 190/112 mm Hg.
In addition, simultaneous palpation of the upper extremity and femoral
pulses demonstrated no femoral decrease or delay. These observations
exclude coarctation of the aorta.
Proceed
36-12

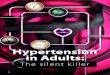
d. PRECORDIAL MOVEMENT
Question: How do you interpret the apical impulse?
5th ICS
MIDCLAVICULAR
LINE
APEXCARDIOGRAM
ECG
36-13

Answer: The left ventricular impulse is sustained, but not displaced. There
is an abnormally prominent atrial filling wave (arrow). The sustained impulse is
consistent with ventricular hypertrophy from chronic hypertension. The
palpable presystolic impulse reflects enhanced left atrial contraction against a
poorly compliant left ventricle.
Proceed
36-14

e. CARDIAC AUSCULTATION
Question: How do you interpret the acoustic events at the apex?
PHONO-APEX
LOW FREQUENCY
APEXOCARDIOGRAM
36-15

36-16
Answer: The first and second heart sounds are normal. A fourth heart
sound is present (arrow). It is the acoustic equivalent of the palpable presystolic
movement of the apex impulse (broken arrow).
e. CARDIAC AUSCULTATION (continued)
Question: How do you interpret the acoustic events at the upper left
sternal edge?
UPPER LEFT STERNAL EDGE
ECG
EXPIRATION INSPIRATION
1
2L
1 1 2
A2 P2 A2
P2 .06 sec

Answer: There is a normal inspiratory splitting of the second sounds of .04
seconds. The aortic component is increased in intensity due to the high aortic
closing pressure. The increase in A2 is also well heard at the upper right
sternal edge.
Palpation of the abdomen revealed no masses, and on auscultation no bruits
were heard.
Question: What is the significance of these latter observations?
36-17

Answer: Palpation and auscultation of the abdomen are important in the
search for secondary causes of hypertension. Polycystic kidneys, if present
are frequently palpable. Abdominal and/or flank bruits suggest renal artery
stenosis. An enlarged urinary bladder may be seen with obstructive uropathy.
These findings are not present in this patient.
f. PULMONARY AUSCULTATION
Question: How do you interpret the acoustic events in the pulmonary lung
fields?
Proceed
36-18

36-19
g. FUNDOSCOPIC EXAMINATION - LEFT EYE
Question: How do you interpret these funduscopic findings?
Answer: In all lung fields, there are normal vesicular breath sounds.

Answer: The fundus shows a normal optic disk and mild hypertensive
vascular changes with a diminished arteriovenous (AV) ratio of 1/2
(normal = 4/5) and focal arteriolar spasm (arrow). The latter may imply rapidly
progressive and/or secondary forms of hypertension. Although significant
AV nicking (broken arrow) and increased arteriolar light reflex (white arrow)
are also present, the latter changes are arteriolar-sclerotic (reflecting chronicity
of the disease) and are not directly related to the degree of hypertension
or prognosis.
There are several systems for grading hypertensive funduscopic findings. One
such system follows. The increasingly severe changes to be described are
directly related to prognosis. This patient has grade II hypertensive retinopathy
by this classification.
Proceed
36-20

36-21
KEITH-WAGNER-BARKER GRADING SYSTEM
FOR HYPERTENSIVE RETINOPATHY
GRADE I Arteriolar Narrowing
GRADE II More Pronounced Generalized Narrowing
Plus Focal Areas of Narrowing
GRADE III Increased Severity of Grade II Changes
Plus Hemorrhages and Exudates
GRADE IV All of the Above Plus Papilledema
Proceed

36-22
g. FUNDOSCOPIC EXAMINATION (continued) - LEFT EYE
Question: How do you interpret this fundus from another patient?

36-23
Answer: The fundus is normal.
g. FUNDOSCOPIC EXAMINATION (continued) - LEFT EYE
Question: How do you interpret this fundus from still another patient?

36-24
Answer: This fundus shows papilledema (arrow), generalized and focal
arteriolar spasm (broken arrow), flame-shaped hemorrhages (white arrow) and
cotton-wool exudates (red arrow) - Grade IV hypertensive retinopathy.
ELECTROCARDIOGRAM
Question: How do you interpret this ECG?
III II aVR
V6 V5 V4 V3 V2 V1
aVF aVL I
V2 - 6 1/2 Standard

Answer: There is normal sinus rhythm and left ventricular hypertrophy as
evidenced by an increased QRS voltage, intrinsicoid delay and ST-T
wave changes.
CHEST X RAYS
Question: How do you interpret these chest X rays?
LATERAL PA
36-25

Answer: The pulmonary vasculature is normal. On the PA film there is a
prominent aortic knob (arrow). The cardiothoracic ratio is normal. In contrast to
ventricular dilation, it is common for concentric ventricular hypertrophy to occur
without an increase in cardiothoracic ratio.
In the lateral film, the inferoposterior prominence of the cardiac silhouette
(arrow) suggests some degree of left ventricular enlargement.
Question: Based in the history, physical examination, ECG and X rays,
what is your diagnostic impression?
36-26

Answer: This patient has significant hypertension with resulting left
ventricular hypertrophy and funduscopic changes. In patients with less
significant hypertension, the average of three blood pressure determinations
taken on separate occasions is necessary to establish the diagnosis.
In men between the ages of 35 and 50, with a positive family history and with
no evidence to suggest a secondary cause, hypertension is almost always
primary. It is, nonetheless, necessary for the physician to consider secondary
causes of hypertension, even though patients with potentially curable causes
make up less than 1% of all hypertension.
Question: What routine laboratory work should be obtained in this patient?
36-27

Answer: Routine tests that are recommended for hypertensive patients
include a urinalysis, BUN or creatinine and serum potassium. These tests are
obtained to screen for renal disease and hyperaldosteronism. In this patient,
they were normal.
In addition, risk factors for coronary artery disease should be determined. This
patient’s total cholesterol was elevated and his high density lipoprotein (HDL)
cholesterol was low, indicating an increased risk for coronary artery disease.
His triglycerides and fasting blood glucose were normal.
Question: Are additional laboratory tests indicated to rule out secondary
causes of hypertension and further evaluate this patient?
36-28

Answer: In this patient expensive screening tests for rare, curable
secondary causes of hypertension are unwarranted, as the history, physical
examination and simple laboratory tests have indicated that their presence is
unlikely. Thyroid studies might be helpful to rule out hyperthyroidism.
Echocardiography may be indicated in selected patients to define the anatomy
and function of the left ventricle.
Question: What are your therapeutic recommendations for this patient?
36-29

Answers: The goal of therapy should be to achieve blood pressure control
with the simplest, least costly program with the fewest side effects. The
therapeutic steps to be taken include:
1. Patient Education: He should be informed of the risk of his disease, the
benefits of therapy, and the likely need for lifelong serial blood pressure
assessment and treatment. Most patients can be instructed in how to take
their own blood pressure.
2. Diet: He should restrict salt, alcohol, cholesterol and saturated fat intake
and lose weight.
Proceed
36-30

36-31
Answers (continued):
3. Habits: He should stop smoking. After his blood pressure is controlled and
an exercise test is performed, he should consider a graded
exercise program.
4. Drug therapy: His initial therapy might include a beta-adrenergic blocker or
a low dose thiazide diuretic. Angiotensin converting enzyme (ACE)
inhibitors and calcium channel blocking agents may also be considered for
initial drug therapy in certain patients depending on age, race, associated
medical conditions and social background. If concomitant non-
pharmacologic therapy is successful in lowering the blood pressure,
medication may be reduced or eliminated.
Question: What is the mechanism of antihypertensive action of
thiazide diuretics?

Answer: The initial antihypertensive effect of thiazide diuretics relates to a
decrease in intravascular volume and, thereby, cardiac output. With continued
use, however, the cardiac output returns to control levels despite a continuing
antihypertensive effect. This long term antihypertensive action of thiazides is
related to their natriuretic effect and resultant decrease in arteriolar smooth
muscle sodium content and tone.
Proceed
36-32

The patient was initially treated with 25 mg of hydrochlorothiazide each
morning. The dose was increased to 50 mg due to an inadequate therapeutic
response. This therapy, coupled with his weight loss and sodium restriction,
resulted in an average blood pressure of 130/80 mm Hg sitting and standing.
Repeat laboratory studies revealed the potassium to be normal and the BUN,
fasting blood glucose, serum triglycerides and uric acid to be mildly elevated.
Question: What changes in his regimen are indicated?
36-33

Answer: Mild increases in BUN, triglycerides, glucose and uric acid are
common with high-dose thiazide therapy. Mild changes are not an indication to
modify treatment. Mild decreases in potassium are similarly not a cause for
concern in the patient without heart disease. With heart disease or with severe
hypokalemia, potassium supplementation with potassium chloride may be
indicated. Alternatively, a potassium sparing diuretic may be used.
Question: How should the patient be treated if there is an inadequate
response to high-dose diuretic therapy?
36-34

Answer: A second drug such as an ACE-Inhibitor may be added. ACE-
inhibitors or Angiotensin Receptor Blockers (ARBs) are indicated in
hypertensive patients with elevated serum glucose levels.
Other antihypertensive drugs include beta-blockers, vasodilators and CNS
active agents. These are outlined in the next slide.
Proceed
36-35

36-36
Proceed for Summary
VASODILATORS
ACE Inhibitors
Angiotensin-II Antagonists
Calcium Channel Blockers
Alpha 1 ( Beta) Blockers
Hydralazine / Minoxidil
CNS ACTIVE AGENTS
Clonidine

SUMMARY
Primary hypertension affects a very significant percent of the adult population.
It is often associated with a positive family history. In those who experience a
recent significant increase in blood pressure or refractory hypertension,
secondary causes should be sought.
The majority of patients with primary hypertension are asymptomatic. Hence,
detection is difficult, and the patient must be educated regarding the need for
long-term treatment. An initial observation of hypertension should be confirmed
by at least two additional determinations at least a week apart.
There are several variations of primary hypertension including labile, “white
coat,” isolated systolic hypertension and pre-hypertension. Labile hypertension
is a blood pressure that is quite variable from day-to-day. White coat
hypertension is hypertension only in the clinician’s office. Isolated systolic
hypertension is common in the elderly and is a systolic pressure of > 139
mmHg in the presence of a diastolic pressure of < 90 mmHg. Pre-hypertension
is a blood pressure of 120-139 / 80-89 mmHg. These patients should be
followed closely, as they are at higher risk for developing sustained
hypertension.
Proceed 36-37

SUMMARY (continued)
The need for medical treatment is determined not only by the level of blood
pressure, but also by risk factors such as age, sex, family history, smoking,
dyslipidemia and diabetes, as well as the presence or absence of damage to
the vessels of the heart, brain, kidney and eye (target organs). Anti-
hypertensive treatment should be initiated immediately not only in patients with
blood pressures of 170/90 mm Hg or more, but also in patients with lesser
degrees of hypertension who are diabetic or have evidence of target organ
damage.
Therapy in these patients as well as those with milder disease reduces the risk
for subsequent target organ damage, reduces the risk for sudden death from
aortic dissection, and may reduce the mortality from myocardial infarction. The
optimal goal of therapy is BP < 120/80 mm Hg.
Proceed
36-38

SUMMARY (continued)
In most cases, extensive metabolic and renal studies are unwarranted. In
addition, the history, physical examination and simple routine laboratory work
most often identify the very small subset of patients in whom additional studies
are indicated.
Maintenance of ideal weight, salt restriction and medication are the
cornerstones of initial medical therapy. The key to effective treatment,
however, is patient education. The patient should be advised of all correctable
risk factors for atherosclerotic cardiovascular disease and of the extreme
importance of long-term therapy and follow-up.
If hypertension remains undetected and/or untreated, serious disability and/or
death from stroke, renal failure, dissecting aortic aneurysm, congestive heart
failure or myocardial infarction are the usual sequelae. If detected early and
effectively treated, the risk of developing these complications is comparable to
the nonhypertensive patient.
36-39

36-40
PATHOLOGY
A typical autopsy specimen from a patient with untreated hypertension. There
is severe symmetrical thickening of the left ventricular wall measuring
approximately 25 mm (normal = 9-11 mm). The right ventricular wall thickness
is normal.
Proceed for Case Review
LEFT RIGHT
POSTERIOR
ANTERIOR

36-41
To Review This Case of
Moderate Primary Hypertension:
The HISTORY is typical in that the patient is asymptomatic, or has only
mild symptoms, and there are no historical clues to a secondary cause of
hypertension. The family history is positive for hypertension. Additional risk
factors (smoking and positive family history) for the development of
atherosclerotic cardiovascular disease are present.
PHYSICAL SIGNS:
a. The GENERAL APPEARANCE reveals the patient to be overweight,
without evidence of endocrinologic or other causes of hypertension.
b. The JUGULAR VENOUS PULSE is normal in mean pressure and
wave form.
c. The carotid and peripheral ARTERIAL PULSES are normal, and the
blood pressures in both upper and lower extremities reveal systolic and
diastolic hypertension. These findings exclude coarctation of the aorta.
Proceed

d. PRECORDIAL MOVEMENT reveals a nondisplaced, sustained systolic
impulse reflecting the afterloaded, hypertrophied left ventricle, and a
presystolic impulse due to an enhanced atrial contraction against the
thickened ventricle.
e. CARDIAC AUSCULTATION at the base reveals an enhanced A2 due to
augmented aortic root pressure. The second sound splits normally.
At the apex there is a fourth heart sound, the acoustic equivalent of the
palpable apical presystolic movement. The absence of abdominal and flank
bruits is an important negative finding, as they are commonly heard with
renal artery stenosis.
f. PULMONARY AUSCULTATION reveals normal vesicular breath sounds
in all lung fields.
g. FUNDUSCOPIC examination reveals arteriolar narrowing and focal
spasm (Grade II hypertensive retinopathy).
Proceed
36-42

The CHEST X RAYS show a slightly prominent aortic knob and
suggest left ventricular enlargement.
LABORATORY DATA show normal renal function, electrolytes and
uric acid. The results do not suggest a secondary cause of hypertension. The
total cholesterol is elevated with a low HDL cholesterol, indicating an increased
risk for coronary heart disease.
TREATMENT consists of weight reduction, salt restriction and
antihypertensive medication. A majority of hypertensive patients will require
multiple drug therapy. The treatment of his additional risk factors for coronary
artery disease includes the cessation of smoking, weight loss, restriction of
alcohol, cholesterol and saturated fats, and a graded exercise program after a
baseline exercise stress test. Careful follow-up of treatment and continuing
patient education and encouragement are mandatory.
36-43