Embed Size (px)
Citation preview

27/02/2015
1
Opiate Use Disorders and Pain in the elderly: Integrating care with the pain specialist
Gabriel Paulian M.D
Christopher Ong, M.D
Yuliet Sanchez, M.D
Uma Suryadevara, M.D
No disclosures for any of the speakers!

27/02/2015
2
Where’s the pain?

27/02/2015
3
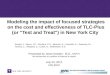
Algorithm for a general approach to the assessment of chronic nonmalignant pain
ROBERT P. JACKMAN, MD, JANEY M. PURVIS, MD, Cascades East Family Medicine Residency Program, Oregon Health and Science University, Klamath Falls, Oregon
BARBARA S. MALLETT, MD, Spinal Diagnostics, Tualatin, Oregon
Am Fam Physician. 2008 Nov 15;78(10):1155-1162.
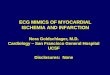
WHO Step Ladder Approach

27/02/2015
4

27/02/2015
5
Are opiates indicated in my patient?
Influences on therapeutic decisions:
Outcomes during prior therapies
Pain severity and course
Age and medical comorbidities
Reasonable alternatives
Likelihood of addiction/abuse/diversion
Critical outcomes
Pain relief
Function - physical and psychosocial
Side effects
Drug-related behaviors: abuse, addiction, pseudoaddiction, diversion
If they are indicated: what are the possible outcomes

27/02/2015
6
Barriers to Opioid Therapy
Patient-related factors
• Fear of addiction
System factors
• Availability in pharmacies
Clinician-related factors
• Poor knowledge of pain management, opioid pharmacology and chemical dependency
• Fear of regulatory oversight

27/02/2015
7
Opioid Therapy: what are my options?
Immediate-release preparations Used mainly :
opioid naïve patients
acute pain
dose finding during initial treatment of chronic pain
“rescue” dosing (breakthrough pain )
Can be used for long-term management in select patients
Dose limit?
Duration of opioid therapy—lifetime?
Tolerance
Hyperalgesia
Opioid Therapy: what else do I need to know?

27/02/2015
8
Opioid Therapy: Side Effects
Common
Constipation
Somnolence, mental clouding
Less common
Nausea -Sweating
Myoclonus -Amenorrhea
Pruritus -Sexual dysfunction
Urinary retention -Headache
Opioid Therapy
Scenario 1:
67 y/o F with PMHx of chronic knee pain secondary to severe DJD managed with OXYCODONE/APAP 5/325 1 tab po QID

27/02/2015
9

27/02/2015
10
Opioid Therapy
Scenario 2:
72 y/o M with PMHx of low back pain secondary to failed back surgery managed with METHADONE 10 mg po Q 8 hrs
Opioid Therapy

27/02/2015
11

27/02/2015
12
Psychiatric Comorbidities
Depression is present in more than 50% of patients with chronic pain.
Severity of pain is a strong predictor of worsening depression and health-related quality of life outcomes.
Treatment options in the context of pain: Medications (SSRIs, anxiolytics, TCAs), CBT, Complementary and alternative treatment, Lifestyle changes
Psychiatric Comorbidities: Depression
Chronic pain is an important risk factor for suicide.
Suicide Risk assessment tools in patients with pain.
Consider other treatment options if patient is at a higher risk for suicide or depression: A delicate balance!

27/02/2015
13
Psychiatric comorbidities: Anxiety
Treatment in the context of pain: Antidepressants (SNRIs, TCAs) psychological treatments, other anxiolytics.
Benzodiazepines: The main actions are hypnotic, anxiolytic, anticonvulsant, myorelaxant, and amnesic.
Adverse effects in elderly from Benzodiazepines: psychomotor impairment, occasionally paradoxical excitement, falls and fractures, intellectual and cognitive impairment.
Some Important Data:
2004 to 2008: 111% increase in the estimated number of emergency department visits involving nonmedical use of opioid analgesics.
2004 to 2008: 89% increase in such visits for benzodiazepines.
From 2007-2011: Opioid prescribing rates increased 32 percent. 2010 data: Opioid analgesics were involved in 75% of pharmaceutical overdose deaths.
cdc.gov

27/02/2015
14
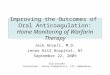
Benzodiazepines
Data from the National Vital Statistics System multiple cause-of-death file: Benzodiazepines were involved in 31% of opioid-analgesic poisoning deaths in 2011, up from 13% in 1999.
Prescribing Benzodiazepines with Opiates is DANGEROUS!
Alternatives for Benzodiazepines
Substance Use Disorders: Another Comorbidity
Pain
Chronic pain
Physical dependence
Tolerance
Addiction
Pseudoaddiction
Hyperalgesia
Opioid induced hyperalgesia

27/02/2015
15
Substance Use Disorder
Addiction
Chronic pain and depression can predispose to benzoabuse and dependence
Risk increases with age and more common among patients on multiple medications
Commonly used questionnaires are less sensitive in the elderly
Opioid Use screening tools
SOAPP (Screener and Opioid Assessment for Patients with Pain-Revised)
ORT (Opioid Risk Tool)
DIRE (Diagnosis, Intractability, Risk, Efficacy Tool)
SISAP (Screening Instrument for Substance Abuse Potential)

27/02/2015
16
Ongoing assessment tools:
COMM (Current Opioid Misuse Measure)
ABC (Addiction Behaviors Checklist)
Chabal 5-Point Checklist
PMQ (Pain Medication Questionnaire)
PDUQ (Prescription Drug Use Questionnaire)
PADT (Pain Assessment and Documentation Tool)
Working together
Treatment options like CBT, Relaxation therapy and group therapy.
Treat pain and psychiatric comorbidities together.
Multidisciplinary treatment approach: best approach for pain management.