Embed Size (px)
Citation preview
N M E T H 5 2 7 , F A L L 2 0 1 3
T E A M P R I S T I N E
Diabetic Mobile Application
Implementation
Si Feng, Dennis Kan, Kristine Kim, Mark Moon
D i a b e t i c M o b i l e A p p I m p l e m e n t a t i o n 2
Diabetic Mobile Application Implementation
ABSTRACT
Background & Goals: Fosters Health System (FHS) is a large non-profit healthcare organization. Fosters’ current diabetic management performance is below national average. Dr. Brock Jim, the Chief Medical Informatics Officer (CMIO) of FHS, is committed to implement a new clinical diabetic management application to connect patients and clinicians together to improve diabetic care management. Technology: The new diabetic mobile application was selected based on integrating new technology with patient-centered care and clinician management needs to ensure better-coordinated diabetic care. Training and technical support will be available to facilitate the process. Implementation: Tina Turner, the project leader appointed by Dr. Jim, will lead a team of experts to implement the new application. Readiness of diabetic patient population and all clinicians involved will be accessed during preparation period. Data will be collected through Beta-testing stage to make the app ready to go live. The focus of the “Go-Live” process is educating all the participants and troubleshooting for potential problems. Re-evaluation will occur throughout all stages to make necessary adjustments. Conclusion: The purpose of this case study is to simulate the process of acquiring and implementing a new diabetic mobile application in FHS and identify any potential barriers and concerns involved in this process.
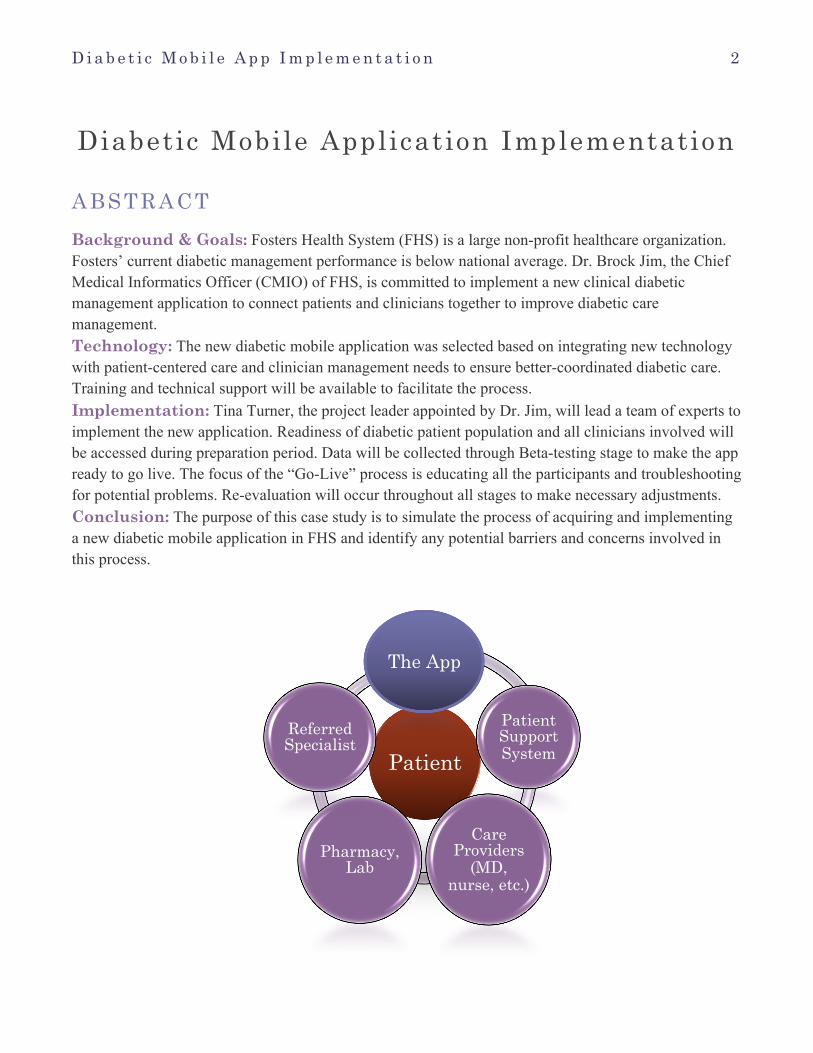
Patient
The App
Patient Support System
Care Providers
(MD, nurse, etc.)
Pharmacy, Lab
Referred Specialist
D i a b e t i c M o b i l e A p p I m p l e m e n t a t i o n 3
INTRODUCTION According to American Diabetes Association (2013), about 26 million Americans (18.8 million diagnosed plus 7 million undiagnosed) 20 years of age and older, have diabetes, and another 79 million people in the United States have pre-diabetes (i.e., elevated levels of blood glucose that are not high enough to meet the diagnostic criteria for diabetes). With more than 1 billion smartphones and 100 million tablets around the world, these devices can be valuable tools in diabetes management (Eng & Lee, 2013). In addition to this, with the advent of wireless communications, there are no longer barriers of space and time between healthcare providers and patients. Health care providers can work along side with their patients to guide them through each step of care. Fosters Health System is planning to implement a new mobile application for diabetes management.
This mobile application will be implemented throughout the Fosters Health System in both inpatient and outpatient settings. Dr. Jim, the Chief Medical Informatics Officer (CMIO) of Fosters, will be appointing a project manager to lead a team of experts to select and implement a mobile diabetes management application. The application system will involve only Type II adult diabetic patients at this stage of implementation. If the implementation process was successful with this patient population, the application will expand its patient population base to all diabetic patients (include all Type I, Type II, and Gestational diabetic patients) in later versions. The application will also include patients’ support systems (family members and caregivers), and clinicians (physicians, nurse practitioners, nurses, pharmacists, lab technicians, registered dietitians, and all other care providers involved in patients’ care). Health care providers can use the application to help patients with health-related behavioral changes, medication regimen management, caregiver concerns, and other diabetes management-associated issues. The project team will first choose the appropriate mobile application and technology requirement for the system. They will need to assess the readiness of diabetic patient population and all the care providers involved during preparation period. They will gather all the necessary information in Beta-testing stage to help improve the prototype and make it ready to go live. During the “Go-Live” process, the implementation team will focus on educating all the participants and troubleshooting the potential problems related to new application. Re-evaluation will occur all throughout the implementing process to monitor progress and make necessary adjustments.
BACKGROUND Fosters Health System (FHS) is a non-profit healthcare organization that provides care for 2 hospitals, 1 physician group, 20 outpatient clinics, 3 long-term care facilities and 1 home health agency in Washington state.
Based on the system-wide standard Electronic Medical Record (EMR), there are approximately 2000 diabetic patients in the Fosters Health System. According to public and internal data, at the Fosters Health System, the current diabetic management performance is poor. About three-quarters of the diabetes patients at FHS have HbA1c over 8.1%. The Board of Directors was very disappointed with the report and asked the executive management to develop a strategy plan to improve the quality of diabetic management. Since Fosters’ vision is to empower patient with
D i a b e t i c M o b i l e A p p I m p l e m e n t a t i o n 4
coordinated care to achieve the best quality health outcomes through new innovations, CMIO Dr. Jim, came forward with the idea of implementing a mobile diabetes management application to connect patients and clinicians together to improve diabetic care. He is prepared to appoint Tina Turner, an experienced RN who has worked in Fosters’ Diabetic clinic for over 15 years and a Master’s in passing CIPCT (Clinical Informatics & Patient-Centered Technologies) student at the University of Washington, as the project leader. Tina will lead a team of experts, include IT specialists, clinical educators, program evaluators, and research clinicians.
Fosters’ Chief Financial Officer (CFO), Mr. Green, has gathered enough funds from the Fosters Health System Innovation Funding, Implementation Project Grant from American Diabetes Association, and community fundraisings. Based on the financial proposal for the new diabetic application system, the current funding should support the acquisition and implementation plan over a 2-year time period.
STRATEGIC GOALS The Fosters Health System is committed to its mission of providing the best possible care in a cost effective, efficient manner while maintaining a patient-friendly and compassionate environment. To fulfill this mission, the Fosters Health System will:
1. Pioneer a patient and healthcare provider partnership in the accountability of diabetes management by providing access to an easily downloadable smartphone application for diabetic patients by October of 2014.
2. Promote patient initiative in the management for care of diabetes with the implementation of daily blood glucose tracking system, food diary entry system, list of medications, and medication refill reminders.
3. Maintain or reduce HbA1c levels below 7% in 20% of patients by a 25% increase in adherence and decrease late medication refills by June of 2015.
4. Continue to update the application with software maintenance and informatics support for patients and healthcare providers with any new features or changes that are added to the application.
5. Improve diabetes outcomes by creating a platform with current patient related medical information that is accessible to all different healthcare providers that is up-to-date and accurate.
TECHNOLOGY
A c q u i s i t i o n P r o c e s s Finding a sophisticated application that met the needs of the Foster Health System requirements for diabetes management was the most important goal, yet the application had to be functional and intuitive for patients. Tina Turner, project manager, started a small committee to facilitate the acquisition of a diabetes management. Tina brought in the pharmacy managers of both outpatient and inpatient settings, the lead information technology specialist, a couple physicians from the family medicine clinic, and the
D i a b e t i c M o b i l e A p p I m p l e m e n t a t i o n 5
Chief Financial Officer. Tina wanted to make sure the application was geared towards the ultimate goal of patient care; money was not the main factor in the decision, yet the cost had to be reasonable. The committee met for many weeks browsing different options that were available on the “App Store” for several different smartphone software platforms. The current applications that were offered and marketed through a third party company didn’t offer exactly what the Foster Health System was looking for. One app that looked promising with all the functional capability and data management for diabetic patients was not exactly user friendly. In other cases, apps that were extremely user friendly did not have all the functional capabilities the Fosters Health System needed to implement in order to manage a chronic illness. Along with the disappointment of not having all the features that were necessary, contracting with a third party company was not a cost-effective option. Many start-up software companies were asking for hundreds of thousands to millions of dollars for setting up the application within the Foster Health System. It did not seem reasonable to the committee to set up an application that didn’t meet the needs of the patients and the Health System itself. It seemed that innovation was the only real option that would facilitate the goals of patient care. If the Fosters Health System was about to spend hundreds of thousands of dollars, it seemed most sensible to recruit a team of developers, artists, and engineers to create an application that met the needs of the Foster Health System and user friendly interface for the patient population.
S o f t w a r e R e q u i r e m e n t s The team of web developers has worked diligently to create an application that is easily downloadable among all mobile devices such as smartphones and tablet computers. The list of common smartphone platforms includes: Apple iOS 3.0 and above, Android version 2.3 and above (Gingerbread and above), Blackberry 10, and Windows Phone (Mobile). For the tablet market, the list includes: Android, Blackberry OS, Apple iOS, and Windows.
S o f t w a r e u p d a t e s Updates will be announced in the application through a notification system, which lists all changes that affect the user.
T r a i n i n g f o r H e a l t h c a r e P r o v i d e r s
I n f o r m a t i o n a l m e e t i n g The clinic’s IT specialist plans on having convenient informational meetings that are open to all healthcare providers in the clinic. This will include a PowerPoint presentation of screen shots of the capabilities of the application. With updates to the application, there will be meetings to inform all healthcare providers of the new advancements along with a question & answer session to remove any confusion.
C o m p u t e r - b a s e d t r a i n i n g ( C B T ) The web developers have worked with the IT specialist to create a succinct, yet informative computer based learning experience that is accessed through the clinic’s website. This training is
D i a b e t i c M o b i l e A p p I m p l e m e n t a t i o n 6
available to all healthcare providers and the patients of the clinic as a reference. New CBT’s will be released and accessible with any new advancements or updates to the application.
I n c l u d e d i n f o r m a t i o n i n t h e p r e s e n t a t i o n Appointment reminders, inputting blood glucose levels, graphing blood glucose trends, medication management/refill reminders, insulin refill requests, logging entries in the food diary, and the patient’s personal diabetes management journal (including integration of photos for wound progression).
T e c h n i c a l S u p p o r t With the release of the application, the IT specialist(s) will be available during clinic hours as a resource for healthcare providers to assist with technical issues. The specialist(s) will be able to answer questions through e-mail or through phone calls. The following list provides examples of tasks that the IT specialist(s) will be able to assist healthcare providers with:
P a s s w o r d r e t r i e v a l If any provider or patient forgets his/her username or password for the application, the specialist(s) will be able to retrieve the information using any security information that is inputted by the user.
A p p o i n t m e n t r e m i n d e r s IT specialist(s) will be able to e-mail out a weekly schedule for physicians and nursing staff for the upcoming diabetes management appointments.
N o t i f i c a t i o n s t o p h a r m a c y Notifications for prescription refills will be filtered to seamlessly integrate into an automatic refill program for each patient utilizing the refill feature.
C o n s o l i d a t i o n o f f o o d j o u r n a l IT specialist(s) will facilitate the use of the food journal portal that is available for all health care providers taking part in the diabetes management of any patient using the application.
G e n e r a l a s s i s t a n c e The specialist(s) will be able for general assistance and questions regarding the application during business hours in which the clinic is open.
Dr. Jim realizes that the implementation of new technology can be a very dangerous choice. Although younger generations may see the benefit of such advancements, older generations may not be open to the change of using a mobile device to assist with their diabetes management. Dr. Jim has to make sure that each type of provider in the clinic is able to understand the benefits and be knowledgeable about the component of the application that is directly related to their field.

D i a b e t i c M o b i l e A p p I m p l e m e n t a t i o n 7
IMPLEMENTATION
P r e p a r a t i o n Dr. Jim was tasked with searching for a project manager who would be in charge on making this new application implementation happen. Tina Turner, a nurse at one of Fosters’ diabetes clinics and a graduate student studying health informatics, was sought after for this role. Tina quickly said yes, for this role satisfied her both financially and academically. Tina has decided to implement this new application at the adult diabetic clinics first. Preparation for the go live day was fairly extensive with the consideration of a multidisciplinary approach. Tina has selected “champions” from different disciplines to aid in the deployment of this new application. The groups that champions represented included adult patients and their caretakers, clinicians such as Dr. Stephanie Moro, who is an endocrinologist, Theodore Rooting, who is a family nurse practitioner, and Arnold Palmar, who is a seasoned diabetes nurse as well as a diabetes educator. These three clinicians have director contact with the diabetes patients and families within Fosters Health System. There was representation from ancillary departments such as Jacob Black from laboratory, Vanessa Humanlog who is a pharmacist, Samantha Yumtree who is a registered dietitian, Regina Simmons who is a physical therapist, Milly Blanks from the occupational therapy division, Lanky Segg who is a podiatrist, and Phyllis Redd, a wound care specialist. There were also a few family members and patients that sat on this team. Champions represent their group and are experts of their field for the implementation team. Their knowledge and input are very important in the success of this application as they are and will be the end users of the application. It is the champions that addressed what they need in this application to make it efficiently functional. During the course of the planning process, multiple disciplines voiced their input of what futures they want in the application. The clinicians desired to have the capability for patients to relay blood glucose levels and their current insulin pump settings. Melody Mellitus, who is a long-standing patient of the clinic, wanted to have a directory of who to call when they need help. Vanessa Humanlog suggested having a feature for patients and their caregivers to be able to reorder insulin. Samantha Yumtree wanted to have a food diary as part of the application for patients that count carbohydrates. Lanky Segg and Phyllis Redd would like to see a feature where patients can take pictures of their current wounds and track their progression.
B e t a T e s t After the team had decided what features where needed, the design team developed a beta version where selected few were able to test out. The beta testing period was for 2 months and comprise of end users in different age groups (18-75 years of age) in only 3 of our clinics. The implementation team has decided to use different age group to gather horizontal data, for the patients at different points of their lifespan. After their two months of beta testing, an evaluation process followed which looked at accessibility, components of user friendliness, features that they would like to see, as well as how it interfaced with our current system. A number of changes occurred such as debugging, adding appointment reminders, and working out some interface issues.
A YouTube video was created to promote this app and was released to the public. Promotions were released onto our website as well as to the local diabetic foundation’s website. There was also Computer Based Training (CBT) for clinicians on how to retrieve data using their application. By the end of the CBT, clinicians were able to retrieve data that patients have inputted, review medications and lab results, and communicate with other clinicians and patients.

D i a b e t i c M o b i l e A p p I m p l e m e n t a t i o n 8
D i s a p p o i n t i n g P a t i e n t E n g a g e m e n t “I cannot believe this data-----only 3 patients!” exclaimed Dr. Jim, the CMIO. A week has passed since the beta test launch of the mobile diabetes application on October 1, 2013. To his disappointment, Dr. Jim, CMIO, has noticed that only 3 patients out of 80 sample diabetic patients (3.8%) in the health system are actively using the mobile diabetes management application. Dr. Jim called Tina, Project Manager, and discussed seriousness of this result. “Tina, well-done for the project! However, data are telling us a challenge. Needless to mention the top management, this way low participation is not acceptable. All of our efforts and valuable resources can end up with just wastes. Please find causes of this poor outcome and bring me a solution to bolster patients’ engagement. That is a key to success…” said Dr. Jim. ‘... what went wrong…’ Tina was frustrated as well and discouraged by the poor outcome. Tina decided to review the implementation process thoroughly, at the same time requesting her project team to research about significant contributing factors for successful diabetes management tools. Challenged, but she and her team members determined to drive a success for the implementation of mobile diabetes management application.
P r o m o t i n g P a t i e n t E n g a g e m e n t Initially, Tina and the project team reviewed the beta test and implementation step by step, but they could not find something that negatively affected the little participation. After the thorough review and further research, Tina and the project team realized that patient education is a key to successful implementation and the little participation was related to promotion, not technical malfunction or other user issues. Tina and the project team identified a number of ways to promote and educate the use of diabetes management application, which includes utilizing all clinicians related to diabetes care as a channel to promote patients’ participation and the websites and blogs of Fosters Health System. Further, the project team sought a consultation from the marketing department of the health system in regard to effective ways and strategies for successful promotion of the application. The project team produced a comprehensive marketing plan, and Dr. Jim approved it for execution.
“Tina, it is encouraging…active users of the application is increasing,” said Arnold, the diabetes nurse and educator. It has been three weeks since the vigorous marketing for the application throughout the health system. A number of active users among beta-users increased from 3 (4%) to 37 (46%), and new active users are increasing by 1 to 3 individuals per day. Besides, Tina and the project team members began receiving positive and encouraging comments from patients and colleges. Confident with this improvement and engagement, Tina and her project team is moving forward to a successful Go-Live.
“ G o L i v e ” Since there is not a period of low census within our targeted population, Arnold Palmer suggested that a random date where to be selected, December 1, 2013. Tina Turner has specific goals of transition our current method of reporting and communication with the clinicians and patients to the new application within 6 months of the Go Live date.
Tina Turner decided to have a designated Go Live Educator to address the new application. Go Live Educators such as Harriet McGonagall who recruited to perform one-on-one education sessions with patients during their clinic visits. Education entailed introduction of this new add and its functionality.
D i a b e t i c M o b i l e A p p I m p l e m e n t a t i o n 9
Since this is considered to be a replacement tool, there should not be additional education that patients and families will have to learn. The education shouldn’t take more than 10 minutes. Yet “new patient’s education is much more extensive,” says McGonagall since they ask a lot of questions and need reinforcement with other concepts of their care such as how often to report the blood glucose or what an HbA1c is. Educating new patients would take “30 minutes or sometimes an hour if they are new to this type of technology, and I am the only educator at this time within the clinic” said McGonagall.
R e - e v a l u a t i o n In March 2014, one quarter has passed and the diabetic app has been a success. Tina Turner and other members of the original implementation group performed a re-evaluation process. The purpose of the re-evaluation is multifaceted. Arnold Palmar wanted to first evaluate if our end users are satisfied with the rollout of the new application. Comments such as “I Love this app” or “This helps better managing my illness and it is quick nifty” were common during the evaluation process. Clients stated that it formed a better communication loop as well as better management of their disease. Empirically, clients having better control of their diabetes management demonstrated an improved outcome as evidenced by 65% of the clients now having HbA1c less than 7.0%. This statistical analysis is important, as it is one of the criteria that are required for a grant, which is funding this initiative. Jacob Black from laboratory suggested implementing a new protocol to have patients to check their blood glucose via point of care testing before, during, and after a meal for having more data for his end. Black also suggested to have a few patients come into the laboratory for blood work if any occasions of blood glucose being above 250.
CONCLUSION In this case study, FHS acquired and implemented a new diabetic mobile application to encourage patient engagement and improve quality of care in diabetes management. After Beta-testing and patient engagement evaluations, the overall process of implementation was successful. The case study also would help identify any potential barriers and concerns in the implementation process. However, the current result is only focused on adult Type II diabetic patients in FHS in a short period of time and the long-term result is unknown. Therefore, continuous evaluation and application improvements are still needed in the process. Effective communication and consistent performance measurements are important for long-term successful implementation and quality of care improvement in diabetes management.
SYNOPSIS The diabetic clinic within Fosters Health Systems (FHS) faced the ever so frustrating dilemma of mismanaged diabetes. Dr. Brock Jim tasked newly appointment project manager Tina Turner recruits teams of experts throughout different disciplines to develop a diabetic management mobile application. The implementation team embarks on a rocky journey in finding an application that is suitable for their clinic. From brainstorming, to implementation, and even beta testing, the team experienced many difficulties and quickly realized that implementing something as simple as an application is not as easy
D i a b e t i c M o b i l e A p p I m p l e m e n t a t i o n 1 0
as they thought. In the end, their work triumphed and ultimately, enabled patients to take charge of their own diabetic care.
INTENDED LEARNER AUDIENCE 1. Informatics students who will be studying the acquisition and implementation of mobile clinical
applications in a large medical group. 2. Hospital administrators who will be involved in the selection and implementation of mobile
clinical applications. 3. IT personnel who are going to be involved in the planning of a mobile clinical application
development and operation. . 4. Clinicians who are involved in the acquisition and implementation of diabetic management
systems.
LEARNING OBJECTIVES
1. Students will be able to identify character, traits, and desired knowledge that a project manager will seek in order to form an effective implementation team.
2. The students need to understand the complexity of having all different types of healthcare providers become knowledgeable with the functions and software of the application in order to facilitate patient usage.
3. The students should be able to identify the potential barriers when implementing a new diabetic clinical mobile application in Fosters Health System.
4. The students will be able to identify contributing factors to successful mobile diabetes management tools that result in improved diabetic management outcomes.
5. The students should be able to identify the issue with confidentiality when launching a smartphone application.
TEACHING NOTE
T e a c h i n g N o t e f o r O b j e c t i v e 1 The goal for this objective is to have students be able to identify how to form a successful implementation team or any team for that matter. The step to implementing anything is to form a team. Students must determine what the function of this team should be. Suggestion that the implementation team should be tasked with, planning, coordinating, managing the budget as well as all aspects of such system. No doubt, we should incorporate the mission and vision within the purpose of their specific team as well. Once a purpose is determined, students will need to decide whom specifically on the team. In order to form a purposeful team, students must ask the question what is the purpose of having a certain person on your team. Who do they represent, what expertise do they bring, and most importantly, do they fit into
D i a b e t i c M o b i l e A p p I m p l e m e n t a t i o n 1 1
the current team dynamic. Other aspect that the students may suggest is how being in the implementation will benefit their future. By determined if there are positive aspects, there is an added interest and investment in being a part of this team.
Different disciplines that are suggested to be in a medical informatics implementation team are to have the subject matter experts that are affected by an application. For example since this case student focus on diabetes management, subject matter included endocrinologist, diabetes specialist, nutritionist, pharmacies, clinical informaticist, information technology, and so on. Please note that more subject matter experts may be included what this application expands. For example, wound care experts may not be included at first if there are no aspect on wound care directly relation. Yet, wound care experts may be included in later improvements on an application if there are aspects of wound care management such as taking pictures of leg wounds and sending them to their providers.
The reason for a team is the idea of sharing ideas and to tackle a large task, which is too large for one person to manage. That being said, team dynamics is very important in completing a project and making it successful. Something that will help with team dynamics is to find a common ground. This could be either through working in the same location, same area, or even having the same vision and future goals. Another aspect that will help with team dynamics is to have current team members be involved with the selection process, which will show value to current team members and for them to select their future team members. Tips for Resolving the Case Problem:
• Think about using tools to help select a team such as a logics test or the Myer-Briggs personality test.
• What questions would you ask if you were interviewing for new team members? To have a successful team, one must be invested in what they do. Getting involved in the interviewing process can be one way.
T e a c h i n g N o t e f o r O b j e c t i v e 2
The students need to understand the complexity of having all different types of healthcare providers become knowledgeable with the functions and software of the application in order to facilitate patient usage.
Despite all the different smartphone software platforms that are available, all users will experience the same functionality with a smartphone application. Students should recognize that the application has to be exactly the same to use in order for healthcare providers to have a simple experience in managing care for each patient. To help patients with the application, each health care provider needs to be well versed with the software. Are the computer based training sessions a good idea? How often should the health system provide a CBT before healthcare providers become tired of this mode of sharing information where they just click through the information screens instead of actually learning and watching? Should there be time limitations on the CBT in order to make sure we do not lose the attention of the CBT users? For example, if a patient went to see their primary care physician and started asking questions about pharmacy refill notifications is that the responsibility of the primary care physician or the pharmacist?
D i a b e t i c M o b i l e A p p I m p l e m e n t a t i o n 1 2
The idea behind implementing a system is making sure that there is a technological tool that is helpful in managing diabetes and easy to use. Although a pharmacist may be responsible for dispensing diabetic medication, they cannot dispense medication without a prescription from the doctor. In essence, healthcare providers work as a team to help manage a diabetic patient and the same idea carries through with this scenario. All healthcare providers should be well versed with the basic functions of the application and should be able to teach their patients how to use it. Tips for Resolving the Case Problem:
• Have the class discuss current options for computer based training or other forms of technology used for training. What are the benefits and drawbacks of each form used for training purposes?
• This is a good time to think about positives and negatives associated with launching an application for patients to use. What are some technological issues that might be a problem associated with both the provider and the patient?
• Have the students to think of different ways to train all users (patients and healthcare providers) how to use the application.
T e a c h i n g N o t e f o r O b j e c t i v e 3 The students should be able to identify the potential barriers when implementing a new diabetic clinical mobile application in Fosters Health System.
The students should first have a brief overview of why Fosters Health System needs to implement this new diabetic clinical mobile application. The current clinical performance of Fosters’ diabetic management is at a critical level and in desperate need of new innovations to improve quality of care. This mobile application technology will revolutionize healthcare by encouraging patients to be more involved in their own diabetic management and have easy access to clinicians. It also provides the opportunity for clinicians to monitor patients’ care progress and interact with patients to guide them through their plans of care. However, this application implementation process potential barriers with patients’ accessibility and confidentiality issue. The application would require both patients and clinicians to have at least daily access of a mobile device. This might be difficult to achieve with patients who do not have access to a mobile device and Internet connection or are not familiar with the new technology. Since this application is connected to the Fosters Health System EMR and involved in physician-patient privileged information exchange, privacy is also a big concern during implementation. Patient’s records must be kept confidential at all times; otherwise it will cause enormous issues in Fosters Health System. In addition, resistance to change among patients and providers might prevent the new application to succeed. This new innovation requires change in behavior and attitude with diabetic management, which could be uncomfortable for some people. Tips for Resolving the Case Problem:
• First, let the class address why Fosters Health System is implementing a new diabetic mobile application and give a brief overview of how the application is going to be utilized.
• Then, let students engage in-group discussion to brainstorm potential barriers when implementing the app and then provide rationales for those barriers.
T e a c h i n g N o t e f o r O b j e c t i v e 4 The students need to identify contributing factors to successful mobile diabetes management tools that result in improved diabetic management.
D i a b e t i c M o b i l e A p p I m p l e m e n t a t i o n 1 3
While there is potential to improve diabetes management by utilizing mHealth, implementation of the advanced technology itself does not guarantee a success of outcome. A recent study discovered that a half (50%) of enrollees to a mobile diabetes management program dropped out of the program due to a number of reasons (Katz, Mesfin, & Barr, 2012). Therefore, it is important for the students to identify contributing factors that lead to a successful implementation of effective mobile diabetes management applications. Such contributing factors are complex and interrelated, which include cell phone factors, diabetes management applications factors, support staff factors, patient factors, case manager factors, and primary care providers factors (Katz, Mesfin, & Barr, 2012). The biggest contributing factor is engagement of patients. For example, diabetes management application factors include frequency of messages, reminders, ease of access to the application, and interface. Message content should be appropriate for the patient population and provide relevant information according to the individual patient’ condition in order to keep the patient engaged in this long-term diabetes management. No matter how elegant and sophisticated the application may be, what is most important is the outcome of the patient that greatly depends on the patient’s behavioral change in his or her daily living. From acquisition, to development, and to implementation, engaging patients as end users is a key for successful implementation. In the development of diabetes management application, developers and all stakeholders involved in such development should always remember this engagement of patient as a top priority.
The second biggest contributing factor to the success is strong support to diabetic patients, healthcare providers, clinicians, and other stakeholders. During go-live events and implementation, a variety of issues arise, which can be technical or human-related, from simple questions like how to access to the application and to the complex questions like how to transfer the patient’s information to EHRs. Constant and strong support for all stakeholders, particularly patients, is most crucial. Without this strong and timely support, the implementation process cannot motivate interested patients and other stakeholders. The strong support enhances participation and meaningful use of the technology. The scope of this support is beyond technical issues. It includes clinical aspects for an effective diabetes management. The single most effective factor for successful diabetes management is patient teaching. This concept should align with the support.
The success of implementation of mHealth application also depends on a number of contributing factors that make the whole process of implementation effective and productive. To name a few, the contributing factors are: organizing an effective team and identifying a champion(s), determining a clear project scope and realistic expectations, establishing and instituting a concrete project plan, creating an appropriate environment, understanding an organization’s culture and not underestimating user resistance, allocating sufficient resources, providing adequate training, and establishing strong working relationship with vendors (Wager, Lee, & Glaser, 2013, pp. 241-270). In this case scenario, particularly, a broad group of champions was actively involved in the project, including patients and their caregivers, Dr. Stephanie Moro, an endocrinologist, Theodore Rooting, a family nurse practitioner, and Arnold Palmar, who is a RN and diabetes educator. Dr. Jim (CMIO) was such a great sponsor for the project, demonstrating continued interests and support for the project. The project manager Tina Turner and her project team were very solid and effective, which functioned an indispensable vehicle to successfully implement the diabetes management application. The students should understand all these contributing factors are interrelated.
D i a b e t i c M o b i l e A p p I m p l e m e n t a t i o n 1 4
Tips for Resolving the Case Problem: • First, let the class discuss how the initially low patient engagement improved after the review
and its follow-up implementation, identifying contributing factors for the improvement. • Also, let the students engage in-group discussion to identify contributing factors that led the
whole process of implementation of the mobile diabetes management application successful.
T e a c h i n g N o t e f o r O b j e c t i v e 5 The students should be able to identify the issue with confidentiality when launching a smartphone application.
Technology paves the way in tracking patient-related medical information. The electronic health records revolutionized the way that patient information is kept and accessed. With technology advancing, there is always someone trying to outwit the safety features to hack into existing system to access personal information for ulterior motives. This is a valid concern for developing an application that stores personal medical information. The application is supposed to be used as a tool to help patients monitor their blood sugar and progress of their chronic disease. In the hands of the wrong person, what can be done with this personal information? Is this even a valid concern for patients who are concerned about the safety of their personal information? What sort of personal data would this application store that would make the patient vulnerable if the information was hacked or accessed by a third party? The purpose of this exercise is to understand the patient’s perspective; any concern is considered valid and therefore should be respected. Even though the idea of getting information hacked may be a far-fetched idea, there are many patients who believe in confidentiality is an important issue. Some patients may readily take a risk with personal information to utilize a tool for healthcare while other patients may be greatly paranoid that the U.S. government will use their information for tracking purposes. Needless to say, there is a great variety of patients and a broad spectrum of ideas concerning confidentiality. In order to ease the concerned patient, what are some ways to relieve their concern about releasing personal medical information through an application? What sort of mechanisms for patient confidentiality can be initiated when developing the application? What sort of capabilities does a smartphone have to protect the user and the contents of its information? Tips for Resolving the Case Problem:
• The class should discuss the pros and cons of putting in personal medical data into a smartphone application. Do the benefits outweigh the negative aspects or is it the other way around?
• Have the class discuss measures that the software developers can add in as a measure of patient confidentiality. Do legal matters come in? Who is responsible if the data is accessed?
DISCUSSION QUESTIONS 1. What are some ways to address and resolve issues regarding team conflicts? 2. How do you choose a go-live date that is conducive to your current situation? 3. Who do you choose to be on a beta testing group and why? 4. What are significant contributing factors for successful implementation of mobile disease
management tools like a diabetes management application in this case? 5. What are contributing factors that make a whole process of health information technology
project successful?
D i a b e t i c M o b i l e A p p I m p l e m e n t a t i o n 1 5
6. How can mHealth, in particular, a mobile diabetes management application enhance patient’s engagement in care and contribute to patient’s behavioral changes?
7. How can an effective project team for mHealth be built and developed? 8. What are some other options of training for healthcare providers that would be effective? 9. At what point should the distinction be made between healthcare fields that one type of provider
may not be responsible for the other healthcare provider’s expertise with the application? 10. What types of technical problems will patients experience with the launch of a smartphone
application? 11. How do we deal with the very concerned or paranoid patients about confidentiality? Is there a
way to convince someone of utilizing the application to receive the benefits?
D i a b e t i c M o b i l e A p p I m p l e m e n t a t i o n 1 6
REFERENCES
American Diabetes Association (ADA). (2013). Standards of medical care in diabetes - 2013. Diabetes Care, 36(Suppl. 1), S11-S66. doi:10.2337/dc13-S011
Eng, D. S., & Lee, J. M. (2013). The promise and peril of mobile health applications for diabetes and endocrinology. Pediatric Diabetes. 14(4):231–8.
Katz, R., Mesfin, T., & Barr, K. (2012). Lessons from a community-based mHealth diabetes self-management program: “It’s not just about the cell phone”. Journal of Health Communication, 17:67–72, doi: 10.1080/10810730.2012.650613
Rosenfield, D., Hebert, P.C., Stanbrook, M.B., MacDonald, N.E., & Flegel, K. (2011, June). Being Smarter with Smartphones. CMAJ, 183(18):133-137. Retrieved from http://www.cmaj.ca/content/183 18/E1276.short
Treja, A., Mehta, N.B., Jain, A.K., Ishwaran, H., Avital, M., & Fishleder, A.J. (2008). Satisfaction with Web-Based Training in an Integrated Healthcare Delivery Network: Do Age, Education, Computer Skills and Attitudes Matter? SMC, 8(48):240-248. Retrieved from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2575204/
Wager, K. A., Lee, F. W., & Glaser, J. P. (2013). Health Care Information Systems: A practical approach for health care management (3rd ed.). San Francisco, CA: Jossey-Bass.