Embed Size (px)
Citation preview

NLP Planned Orthopaedic Surgery for Adults- Health Inequalities and Equalities Impact Assessment
NLP P lanned Orthopaedic Su rgery
fo r Adu l t s Health Inequalities and Equalities
Impact Assessment
Author: Sue Clegg and Clive Caseley
Date: December 2019

The Fold Space,
20 Clyde Terrace
London SE23 3BA
REG VAT GB 858230025
Registered in England Company
Number 05358457
Registered office:
24 Old Bond Street, London W1S 4AP
+44 207 017 2011 [email protected]
www.vervecommunications.co.uk
CONTENTS
1. EXECUTIVE SUMMARY 3
ABOUT THIS REPORT 3
APPROACH 4
MAIN IMPACTS AND MITIGATIONS 4
2. BACKGROUND 6
3. THE NEED FOR AN HEALTH INEQUALITIES AND EQUALITY IMPACT ASSESSMENT 8
HEALTH INEQUALITIES 8
EQUALITY IMPACT ASSESSMENT 8
FULFILLING THE REQUIREMENTS 9
4. PROTECTED CHARACTERISTIC GROUPS 10
5. VERVE COMMUNICATIONS 11
6. OVERVIEW OF THIS REPORT 12
7. CURRENT ARRANGEMENTS FOR PLANNED ORTHOPAEDIC SURGERY FOR
ADULTS IN NCL 14
THE NEED FOR CHANGE 15
7.1.1 Waiting lists 15 7.1.2 NHS targets 15 7.1.3 Cancellations 15
7.1.4 Increase in demand 15 7.1.5 Variation in patient experience 15
8. PROPOSED FUTURE ARRANGEMENTS FOR PLANNED ORTHOPAEDIC SURGERY
FOR ADULTS IN NCL 16
SERVICE LOCATIONS AND PROVIDER PARTNERSHIPS 17
PATIENT PATHWAYS 18
8.2.1 Pathway for patients requiring an overnight stay 18 8.2.2 pathway for day case patients 18
MITIGATIONS BUILT INTO THE MODEL 18
9. CHANGE POINTS ARISING FROM THE PROPOSALS 20
SERVICE MODEL CHANGES 20
PATHWAY CHANGES 22
10. METHODOLOGY 23
HOW PREVIOUS WORK FED INTO PHASE 2 23
PHASE 2 23
STAKEHOLDER WORKSHOP 27
11. POPULATION DENSITIES OF THE SCOPED IN GROUPS 29
The Fold Space,
20 Clyde Terrace
London SE23 3BA
REG VAT GB 858230025
Registered in England Company
Number 05358457
Registered office:
24 Old Bond Street, London W1S 4AP
+44 207 017 2011 [email protected]
www.vervecommunications.co.uk
THE POPULATION OF NCL 29
PEOPLE AGED 65+ 29
DISABILITY 30
GENDER REASSIGNMENT 31
RACE 31
CARERS 34
SOCIO-ECONOMIC DEPRIVATION 34
12. FINDINGS 36
THE IMPACTS OF CHANGE PROVISION 36 12.1.1 Service model changes 36
12.1.2 Pathway changes 38
DISCUSSION OF THE IMPACTS OF THE CHANGES 39 12.2.1 Locations of care provision 40
12.2.2 Changes to reduce cancellations 45 12.2.3 Changes to manage complicated and deteriorating patients 46 12.2.4 Rehabilitation services available 7 days a week 46
12.2.5 Changes to improve the care pathway 47
13. CONCLUSIONS 48
RECOMMENDATIONS FROM THE INTEGRATED HEALTH INEQUALITIES AND EQUALITY
IMPACT ASSESSMENT FOR THE CONSULTATION PHASE 48 13.1.1 Recommendation 1 – Focus on positive steps to tackle inequality 48
13.1.2 Recommendation 2 – Prioritising people for whom equalities impacts are likely
to be highest 49 13.1.3 Recommendation 3 – Targeted approaches to engagement where
necessary 50 13.1.4 Recommnedation 4 - Ensuring follow-through 50
RECOMMENDATIONS FROM THE MOTT MACDONALD TRAVEL ANALYSIS 50

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
3
1. EXECUTIVE SUMMARY
ABOUT THIS REPORT
This Integrated Health Inequality and Equality Impact Assessment (HIEIA) forms part of an
Integrated Impact Assessment to support consultation on proposals for change to planned
orthopaedic surgery for adults in North Central London (NCL) and surrounding areas.
When major changes to NHS services are proposed there are statutory requirements derived from
the Equality Act 2010 to consider equalities and health inequalities.
For those commissioning or providing public services, there are two principle duties:
1. Meet the Public Sector Equality Duty (PSED)
2. To take account of the likely implications for changes to services or the location or access
arrangements for groups or individuals protected under the Act.
An Equality Impact Assessment (EIA) is part of a structured process to meeting these duties and
taking equality of opportunity into consideration when proposing changes to services.
To fulfil these requirements North London Partners in health and care (NLP) has commissioned two
independent pieces of work to examine the effects the changes might have on groups of
people sharing protected characteristics:
● This HIEIA report looks at whether there are any health or other inequalities which are
likely to arise from the changes to the provision of planned orthopaedic surgery for adults
in NCL.
● A separate, but linked, report by Mott MacDonald considers the travel implications of the
changes, which includes demographic profiling of local people who might be required
to travel for planned orthopaedic surgery and hence identifies some groups sharing
protected characteristics under the Act or experiencing social deprivation, and a
detailed review of modes of travel and transport identifying potential barriers and
mitigations for these groups.
This report concludes that generally the changes are likely to have positive impacts for all
patients, and for some scoped-in groups in particular. Sixteen positive impacts were identified
and one negative impact. The negative impact arises from proposed changes to the location of
some services in future. Some early ideas for mitigations are offered in the final chapter.
This report was produced independently by Verve Communications. It complements and draws
on analysis undertaken to inform the travel assessment and will be supplemented by further work
during and following public consultation.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
4
APPROACH
The purpose of this report is to:
● Identify any positive or negative impacts for NCL residents within protected characteristic
groups resulting from proposed changes
● Make recommendations for the consultation period
● Offer initial thoughts on mitigations.
To achieve this, a structured approach was taken to understanding which groups would be
impacted as a direct consequence of the changes to the service model and to defining
‘change points’ within the new model and proposed service locations which enabled a
prioritised set of impacts (both positive and negative) to be identified for more detailed
consideration:
● The starting point was nine protected characteristics groups protected under the Act,
and NLP also chose to scope in people with caring responsibility and deprived
communities to ensure that inequalities derived from these characteristics were also
reflected.
● From this, a longer-list was developed to consider differential impacts which may be
relevant (e.g. for people experiencing physical access as distinct from other groups
within the disability protected characteristic who may have specific health conditions
related to surgery or visual impairments). This led to 30 identified sub-categories.
● Detailed review of the proposed model and an understanding of specific groups and
communities who may be disproportionately impacted derived from population data,
enabled sixteen key ‘change points’ to be identified.
● Through a facilitated process involving patient representatives, service managers and
front-line clinicians, the groups most likely to be impacted was developed from the wider
group and tested with stakeholders and the NLP equalities lead. Through this process six
broad groups were identified as priorities for assessment.
MAIN IMPACTS AND MITIGATIONS
Impacts due to the following are considered in depth in this report:
● Proposed change of some locations of care provision
● Proposed changes likely to reduce cancellations
● Proposed changes to management of complex or deteriorating patients
● Proposed changes to rehabilitation following surgery
● Proposed changes to streamline the care pathway.
Recommendations for engagement during the consultation phase are made to ensure that:
● Mitigations are considered and patients and stakeholders asked to propose solutions to
potential negative impacts
● Prioritising engagement with people for whom impacts are likely to be highest
NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
5
● Targeted approaches to engagement of specific cohorts of patients
● Engagement with providers supports them to understand impacts and develop solutions.
NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
6
2. BACKGROUND
North London Partners in health and care (NLP) is proposing changes to the way in which
planned surgery for adults requiring planned orthopaedic surgery is delivered. The changes will
affect residents of Barnet, Camden, Enfield, Haringey and Islington, as well as small numbers of
patients from other areas who travel to north central London (NCL) for orthopaedic surgery.
Demand for planned orthopaedic operations for adults has been growing and the NHS is
struggling to offer treatment in a timely way to patients. As well as growth in demand planned
surgery is frequently cancelled due to emergency care taking priority, especially in winter.
The hospitals across north central London have worked together to find a new way to organise
planned orthopaedic surgery for adults which will greatly improve care for local people. The
changes aim to ensure equity of access to high quality care, address unwarranted variation in
the quality of care, increase capacity for planned orthopaedic operations, reduce cancellations
and make better use of the money available for this kind of care.
The review team led an engagement process between August and October 2018, during which
there was extensive involvement by residents, patients and individuals and groups bringing the
views of service users, local third sector organisations, equalities groups and north London’s
diverse communities.
During this phase, a desktop equalities review (Initial Equalities Analysis) was undertaken. This
considered potential impacts on groups sharing protected characteristics defined by the Equality
Act 2010 based on the geography and demographics of the north central London population
and the existing patient pathway. Its purpose was to inform development of the service model.
This paper builds on findings in both the engagement report and the desktop review which can
be found here:
● https://www.northlondonpartners.org.uk/downloads/plans/Adult-elective-orthopaedic-
review/End%20of%20engagement%20papers/North%20London%20Partners%20Review%2
0Group_Summary%20of%20Engagement%20Evaluation.pdf
● https://www.northlondonpartners.org.uk/downloads/plans/Adult-elective-orthopaedic-
review/End%20of%20engagement%20papers/North%20London%20Partners%20EIA%20sc
oping%20for%20engagement%20Final.pdf
Between November 2018 and January 2020, the model was developed and considered by both
the north central London Joint Overview and Scrutiny Committee and the Joint Commissioning
Committee of the NCL clinical commissioning groups (CCGs).
During the summer of 2019, providers were invited to make proposals for delivery of the agreed
model and an options appraisal process was undertaken to develop and evaluate options to be
taken forward to consultation.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
7
The review team is currently planning a consultation exercise, which it is anticipated will
commence early in 2020. This document will inform that process.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
8
3. THE NEED FOR AN HEALTH INEQUALITIES AND EQUALITY
IMPACT ASSESSMENT
HEALTH INEQUALITIES
The King’s Fund and Nuffield Trust published a report1 in 2017 which made recommendations for
the successful implementation of the five NHS Sustainability and Transformation Plans for London.
In response the Mayor of London developed a six test framework for major hospital
reconfiguration2; Test 1 relates to health inequalities and the prevention of ill health:
“The impact of any proposed changes on health inequalities has been fully considered
at an STP level. The proposed changes do not widen health inequalities and, where
possible, set out how they will narrow the inequalities gap. Plans clearly set out proposed
action to prevent ill-health.”
The work reported herein has considered the proposed changes to planned orthopaedic surgery
for adults in north central London in light of this requirement and discusses health inequalities
alongside potential inequalities for protected characteristic groups.
The five other Mayor of London tests are considered elsewhere.
EQUALITY IMPACT ASSESSMENT
Since the Equality Act 20103 has been law, public bodies are required to take account of the
needs of specific groups of people. In doing so, they can treat some groups differently – or more
favourably - in order to promote equality.
This aspect of the law (which also applies to employment practice) aims to ensure that services
are designed to meet the needs of everyone in the community and that people already at risk of
unequal treatment or outcomes, for example in health or educational attainment, are not further
disadvantaged by the actions of public service organisations.
When major changes to NHS services are proposed there are statutory requirements derived from
the Act to consider equalities and health inequalities.
For those commissioning or providing public services, there are two principle duties:
1. Meet the Public Sector Equality Duty (PSED), which means to consider, or have “due regard”
to their responsibilities to:
● Eliminate unlawful discrimination, harassment and victimisation and other conduct
prohibited by the Act
1 Sustainability and transformation plans in London, an independent analysis of the October 2016 STPs
(completed in March 2017) 2 https://www.london.gov.uk/what-we-do/health/champion-and-challenge/mayors-six-tests 3 https://www.legislation.gov.uk/ukpga/2010/15/contents/enacted

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
9
● Advance equality of opportunity between people who share a protected characteristic
and those who do not
● Foster good relations between people who share a protected characteristic and those
who do not.
2. To take account of the likely implications for changes to services or the location or access
arrangements for groups or individuals protected under the Act.
An Equality Impact Assessment (EIA) is part of a structured process to meeting these duties and
taking equality of opportunity into consideration when proposing changes to services.
The principal components are:
● Review and analysis of the potential impacts of proposed changes, including
experience, accessibility and outcomes
● Identification of priority groups or communities protected under the Act who might
experience differential (especially adverse) impact
● Ensuring that the views of such groups are heard, and their interests are considered in
drawing up plans and making decisions
● Identification and implementation of mitigating actions which might address inequality
when changes are made and in future access and service delivery.
FULFILLING THE REQUIREMENTS
To fulfil the requirements for the consideration of health inequalities and equality impacts NLP has
commissioned two independent pieces of work to examine the effects the proposed changes
might have on groups of people sharing protected characteristics:
● This HIEIA report looks at whether there are any health or other inequalities which are
likely to arise from the proposed changes to the provision of planned orthopaedic
surgery for adults in NCL.
● A separate but linked report by Mott MacDonald considers the travel implications of the
proposed changes, which includes demographic profiling of local people who might be
required to travel for orthopaedic surgery and hence identifies some groups sharing
protected characteristics under the Act or experiencing social deprivation, and a
detailed review of modes of travel and transport identifying potential barriers and
mitigations for these groups. Where relevant the key findings from the travel impact
analysis are highlighted in this report.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
10
4. PROTECTED CHARACTERISTIC GROUPS
The nine protected characteristics listed in the 2010 Act are:
● Age
● Disability
● Gender reassignment
● Marriage and civil partnership
● Pregnancy and maternity
● Race
● Religion or belief
● Sex (gender)
● Sexual orientation
The report also considers two other groups who could be disadvantaged by the proposed
changes:
● Carers
● People affected by economic deprivation

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
11
5. VERVE COMMUNICATIONS
Verve Communications Limited (Verve) is an independent full-service agency which supports NHS
organisations in delivering transformation and change. Over the past several years Verve have
supported NHS service configurations, institutional and major programmes of clinical change.
Verve has experience in successfully completing equalities impact assessments and can call on a
team of specialists to bring relevant expertise and insight.
This document has been produced independently by Verve and it represents our own analysis
and advice.
We are grateful for the assistance and support provided by NLP colleagues and the Mott
MacDonald team.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
12
6. OVERVIEW OF THIS REPORT
This document reports on Stage 2 of a three-stage assessment process to develop an Integrated
Health Inequalities and Equality Impact Assessment (HIEIA) to ensure any decisions made will
advance quality and ensure fairness by removing barriers, engaging patients and community.
Stage 1 was a desktop review4 the output of which was a rapid scoping report which identified
potentially impacted groups. It was used to inform pre-consultation engagement activities in the
summer and autumn of 2018.
Stage 2 builds on Stage 1 and looks explicitly at the impact of the proposed model of care and
the proposed location of services. The output, this report, delivers an initial HIEIA identifying
positive and negative impacts resulting from the proposed changes and makes
recommendations for the consultation stage; it also offers some initial thoughts on mitigations to
reduce negative impacts.
Stage 3 will take place after the consultation period and will build upon the previous two stages.
It will deliver a revised and final integrated HIEIA, which will reflect the results of the public
consultation. The report will offer an updated mitigations schedule and suggest next steps.
The three stages are summaries below.
4 https://www.northlondonpartners.org.uk/downloads/plans/Adult-elective-orthopaedic-
review/End%20of%20engagement%20papers/North%20London%20Partners%20EIA%20scoping%20for%20enga
gement%20Final.pdf
COMPLETED
Stage 1
August 2018
•Desktop review
•Examined the groups likely to be affected by any proposed changes to planned orthopaedic care for adults
•Used to guide the development of proposals and related engagment
THIS REPORT
Stage 2
December 2019
•Initial Integrated Health Inequality and Equality Impact Assessment
•identify any positive or negative impacts for NCL residents within protected characteristic groups resulting from proposed changes
•makes recommendations for the consultation period
•offers initial thoughts on mitigations
TO FOLLOW
Stage 3
Post-consultation
•Revised Final Integrated Health Inequalities and Equalities Impact Assessment
• revisits the stage 2 in light of feedback from the consultation
•refines recommendations for mitigation
•suggests next steps
NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
13
Figure 1 The scope of each stage
The objective for this work is to identify any positive or negative impacts for NCL residents within
protected characteristic groups, carers and those from areas of economic deprivation, resulting
from the proposed changes to the delivery of planned orthopaedic services for adults.
The report will describe the current arrangements for planned orthopaedic surgery for adults and
will go on to outline the proposed changes to model of care. The change points in the proposed
model will be identified. The methodology for considering scoped-in and scoped out groups is
discussed, together with the methods used for identifying potential impacts of service changes
on the scoped-in groups. The population densities of the scoped-in groups in NCL are given.
The findings section tabulates the positive and negative aspects of each change point for
scoped-in groups, and then discusses the impacts in more detail.
The final section of the report presents our conclusions and recommendations for the next phase
of the work. A list of recommendations made in the Mott MacDonald travel report is also
included.
NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
14
7. CURRENT ARRANGEMENTS FOR PLANNED
ORTHOPAEDIC SURGERY FOR ADULTS IN NCL
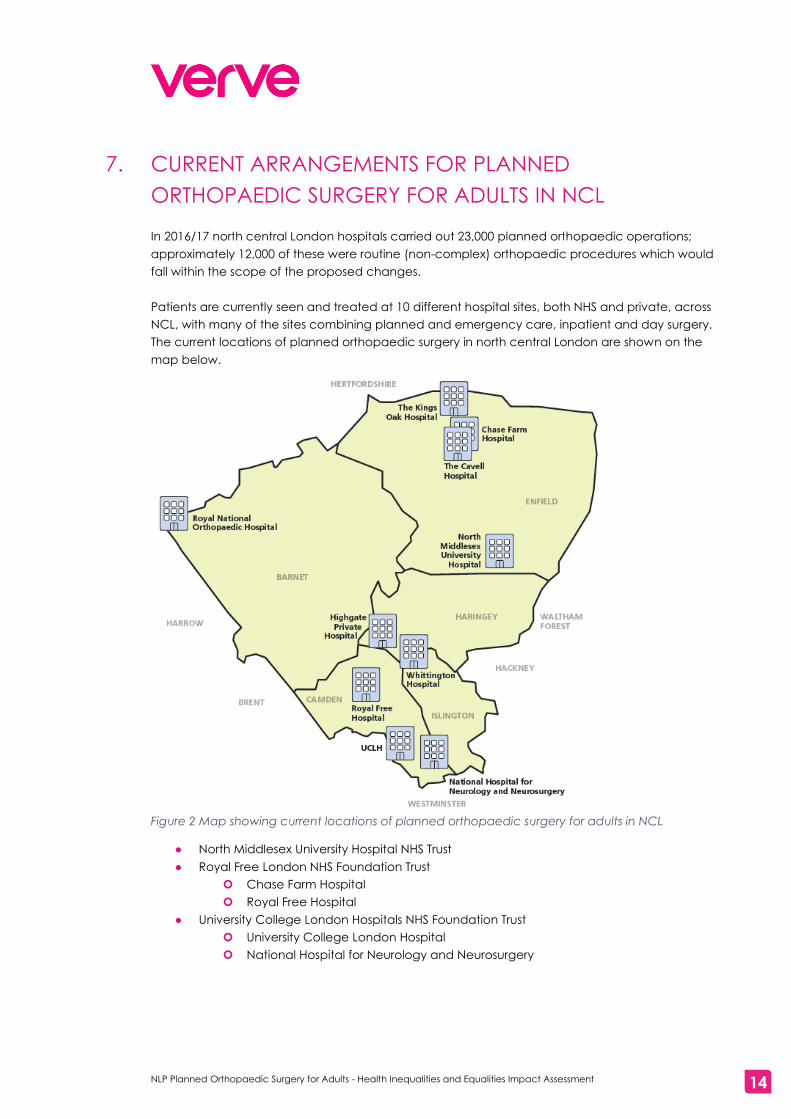
In 2016/17 north central London hospitals carried out 23,000 planned orthopaedic operations;
approximately 12,000 of these were routine (non-complex) orthopaedic procedures which would
fall within the scope of the proposed changes.
Patients are currently seen and treated at 10 different hospital sites, both NHS and private, across
NCL, with many of the sites combining planned and emergency care, inpatient and day surgery.
The current locations of planned orthopaedic surgery in north central London are shown on the
map below.
Figure 2 Map showing current locations of planned orthopaedic surgery for adults in NCL
● North Middlesex University Hospital NHS Trust
● Royal Free London NHS Foundation Trust
Chase Farm Hospital
Royal Free Hospital
● University College London Hospitals NHS Foundation Trust
University College London Hospital
National Hospital for Neurology and Neurosurgery
NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
15
● Whittington Health NHS Trust
● Royal National Orthopaedic Hospital NHS Trust
● The Cavell Hospital (BMI Healthcare)
● Highgate Private Hospital (Aspen)
● The Kings Oak Hospital (BMI Healthcare)
Within current arrangements, Barnet Hospital offers outpatient appointments, but does not offer
orthopaedic surgery
THE NEED FOR CHANGE
Although the current provision of planned orthopaedic surgery for adults in NCL is of good
quality, improvements were identified to enhance patient experience and improve health
outcomes.
7.1.1 WAITING LISTS
In January 2019 there were 10,500 patients on waiting lists for planned orthopaedic surgery; there
was a 24% increase in the numbers of patients waiting for surgery between January 2018 and
January 2019.
7.1.2 NHS TARGETS
The NHS expects 92% of patients to have started treatment within 18 weeks of referral by their GP;
however, on average, between January 2018 and January 2019, only 79% of patients referred for
planned orthopaedic surgery in NCL started treatment within 18 weeks, with some hospitals falling
as low as 65% in winter months.
7.1.3 CANCELLATIONS
In 2018/19 530 orthopaedic operations were cancelled across NCL, 96% of which were cancelled
on the day of surgery. This equates to ten cancellations a week. The main reason for
cancellations were the demands of emergency cases which can result in beds not being
available or staff being called away at short notice.
7.1.4 INCREASE IN DEMAND
The demand for planned orthopaedic surgery for adults, such as hip and knee replacements, is
expected to increase by around 9.5% by 2029. The current arrangements would find it very
challenging to meet this increase in demand and waiting lists could increase.
7.1.5 VARIATION IN PATIENT EXPERIENCE
There are variations between hospitals in terms of time spent in hospital, infection rates and the
number of patients needing revision surgery.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
16
8. PROPOSED FUTURE ARRANGEMENTS FOR PLANNED
ORTHOPAEDIC SURGERY FOR ADULTS IN NCL
The proposed changes to arrangements for planned orthopaedic surgery for adults in NCL have
been clinically driven and co-created with local people and NHS staff with the aim of improving
patient experience and outcomes and ensuring a service fit for the future.
A joined-up approach to planned orthopaedic surgery for adults in NCL is proposed. This should
ensure that NCL residents have timely access to consistent, high-quality, orthopaedic surgery,
regardless of where they live in the area.
Two partnerships have been formed by local NHS trusts – with North Middlesex University Hospital
(North Mid) working with The Royal Free London and University College London Hospital (UCLH)
and Whittington Health working together. The partnerships would be overseen by a network of
health professionals who will ensure that, regardless of where patients receive care, it is of a
consistently high standard. These new partnerships would deliver a new improved service.
The proposed service would have:
● Two NHS hospitals with dedicated operating theatres and beds, for patients who need to
stay overnight after their operation
● A choice of NHS hospitals for those needing day surgery
● Within each partnership, a choice of NHS hospitals for outpatient appointments
● Improved education classes for patients so they understand their operation and what to
do to before surgery to support their recovery afterwards
● Appointments would be with a named surgeon, who, with their surgical team, would stay
with patients throughout their care, regardless of where it takes place
● Rehabilitation support for patients after their surgery
● Access to high dependency or intensive care units for patients who need additional care
after their surgery
● Care coordinators to support patients with conditions such as dementia or a learning
disability to understand their care and where it might take place
● More complex surgery would continue at the Royal National Orthopaedic Hospital, a
super-specialist centre
● Patients with other complex medical conditions, such as haemophilia, will have their
surgery at the hospital which specialises in their condition
● Emergency orthopaedic care would continue at all local hospitals with an Accident and
Emergency department

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
17
SERVICE LOCATIONS AND PROVIDER PARTNERSHIPS
The proposed service locations and provider partnerships are shown in the map below:
Figure 3 Map showing proposed service locations and provider partnerships

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
18
PATIENT PATHWAYS
8.2.1 PATHWAY FOR PATIENTS REQUIRING AN OVERNIGHT STAY
Figure 4 Patient pathway for those needing an overnight stay
8.2.2 PATHWAY FOR DAY CASE PATIENTS
Figure 5 Patient pathway for day case patients
MITIGATIONS BUILT INTO THE MODEL
Comprehensive early engagement with patients influenced NLP’s thinking and ensured that
some mitigations for concerns were built into the proposed model at an early stage. The analysis
in this report takes this work into account and acknowledges that a great deal of work has
already been undertaken to ensure that equalities considerations are central to the proposed
model.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
19
The concerns and mitigations are shown in the table below.
Concerns raised: Influence on thinking:
Patient experience:
o Patients with vulnerabilities might find it
difficult to travel to, and find their way
around, different hospitals
o Clinical delivery model: Inclusion of care
co-ordination function
o Options appraisal: Scored section on
patients with vulnerabilities within the
patient experience section
Continuity of care:
o Location of pre-operative assessments
and post-operative care/rehabilitation
were a concern
o Clinical delivery model is specific about
which organisation is responsible for pre-
operative assessment and patient
education sit in the pathway
o Options appraisal: providers asked to give
detailed consideration of how they will
deliver both pre-operative assessment
and patient education in their proposals
Patients with complex needs:
o It was not clear where patients with
complex needs would have their surgery
o Clinical delivery model: To include an
essential requirement for all planned
orthopaedic surgery centres for adults to
have an HDU
o Options appraisal: Assessment of
proposals around inclusion of HDU, case-
mix and managing clinical complexity
Integration:
o Contributors stressed the importance of
joined-up working
o Integrated IT systems were also important
o Clinical delivery model: To include a
section on digital requirements
o Options appraisal: IT and digital
considerations are included as part of the
deliverability score
Travel:
o There were repeated comments
suggesting that an in-depth transport
analysis should be considered
o Clinical delivery model: To include a
section on travel and transport
arrangements
o Options appraisal: A detailed travel
analysis will need to be carried out and
published as part of the public
consultation
Table 1 Inbuilt mitigations

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
20
9. CHANGE POINTS ARISING FROM THE PROPOSALS
A number of ‘change points’ have been identified in the proposals. ‘Change points’ are the
elements of the proposed model of care that will be different for patients in future, if the
proposals are implemented, when compared with the current arrangements.
The tables below show service model and pathway changes being proposed, together with a
description of each change and the expected outcomes of the changes.
SERVICE MODEL CHANGES
Change Description Expected outcome
360 patients will
change location
from UCLH
360 patients who would have gone
to UCLH would in future go to the
Whittington for day surgery
Reduced cancellations
and waiting times
360 patients will
change location
from the
Whittington
350 patients who would have gone
to the Whittington would in future
go to UCLH for inpatient care
Reduced cancellations
and waiting times
400 patients will
change location
from the North
Middlesex
400 patients who would have gone
to the North Middlesex would in
future go to Chase Farm for
inpatient care
Reduced cancellations
and waiting times
80 NHS funded
private sector
patients will change
location
80 NHS funded patients who would
have received day surgery in
private sector provision5 would,
over time, have their surgery at
UCLH
Consistent high quality
integrated care.
1020 NHS funded
private sector
patients will change
location
1020 NHS funded patients who
would have received day surgery in
private sector provision would, over
time, have their surgery at Chase
Farm instead.
Consistent high quality
integrated care.
560 NHS funded
private sector
patients would
change location
560 NHS funded patients who would
have received inpatient care in
private sector provision would, over
time, have their surgery at Chase
Farm instead.
Consistent high quality
integrated care.
40 NHS funded
private sector
patients would
change location
40 NHS funded patients who would
have received inpatient care in
private sector provision would, over
time, have their surgery at UCLH
instead
Consistent high quality
integrated care.
225 patients
referred to RNOH
for non-specialist
care could change
location
225 patients referred to RNOH for
non-specialist care could be
suitable for treatment at Chase
Farm instead
Patients will be able to
access the right treatment
at the right time with
minimal delays
75 patients referred
to RNOH for non-
75 patients referred to RNOH for
non-specialist care could be
Patients will be able to
access the right treatment
5 The private sector hospitals referred to are Cavell, Kings Oak and Highgate Hospitals

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
21
Change Description Expected outcome
specialist care
could change
location
suitable for treatment at UCLH
instead
at the right time with
minimal delays
Ring fenced beds There will be dedicated inpatient
beds for patients requiring in-patient
care
Reduced cancellations
related to orthopaedic
trauma/non-orthopaedic
admissions, reduced
waiting times, reduced
infection rates, high
quality consistent care,
reduced revision rates and
readmissions
Dedicated theatres Dedicated theatre space able to
operate 7 days a week
Increased capacity,
reduced cancellations,
reduced waiting times,
reduced infection rates,
high quality consistent
care, reduced variation in
care, reduced revision
rates and readmissions
High Dependency
Unit6
A minimum level 2 high
dependency care available at all
sites carrying out surgery
Ability to manage
complicated and
deteriorating patients
safely and effectively on
site minimising the need
for transfer
Ability to manage
deteriorating
patients
Systems and processes in place to
effectively manage patients who
require more intensive treatment
including transfer to intensive care
Early identification of
patients who are likely to
require additional medical
support to enable care
plans to be initiated.
Patients receiving the right
care are the right time
through immediate
referral to the most
appropriate hospital that
meets their clinical need.
Robust pathways in place
to transfer patients to high
dependency or intensive
care
Senior overnight
medical cover
Medical cover 24/7 including
overnight provision on site
The needs of patients who
deteriorate unexpectedly
or who require more
complex intervention can
be safely and effectively
managed without transfer
improving patient
experience
Rehabilitation
services 7 days a
week
Ability to mobilise patients 7 days a
week
Providing effective
intervention, improving
6 Quality of care for all patients will be improved by the addition of HDUs

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
22
Change Description Expected outcome
experience and reducing
length of stay
Table 2 Service model changes
PATHWAY CHANGES
Change Description Expected outcome
NCL wide
Multidisciplinary
Team working
(MDT)
Robust structures in place to share
clinical learning and provide
specialist advice and support
regarding individual patients
Improving patient safety
and effectiveness leading
to reduced revision rates,
readmissions and
decreased length of stay
Care co-ordinators Care co-ordinator roles in place to
support patients in navigating the
system and accessing the right care
and support at the right time
Improved patient
experience and
effectiveness of care
resulting in decreased
length of stay and the risk
of readmission
Consistent referral
pathways and
criteria
NCL wide referral processes and
criteria to ensure care constancy
across NCL
Equitable care that ensure
all patients across NCL
receive the same high
quality access to services
Standardised
patient education
and information
NCL wide approach to pre- and
post-operative information and
patient education
Ensuring all patients
receive the same high
quality information and
advice
Consistent
approach to pre-
operative
assessment
Standardise NCL wide pre-
operative assessment practices and
protocols
NCL wide assessment
practices will ensure
clinical and social issues
are identified early and
needs based care plans
implemented
Surgeons follow the
patient7
Surgeons will follow the patient from
local hospital to planned
orthopaedic surgery centre to
ensure there is consistency of care
Improving patient
experience
Table 3 Pathway changes
7 This is not a change per se, as patients currently see the same surgical team pre-operatively and for
operations, however, patients were concerned that receiving care in different locations might mean different
surgical teams would do their operations. Reassurance about continuity of care is likely to improve patient
experience.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
23
10. METHODOLOGY
HOW PREVIOUS WORK FED INTO PHASE 2
From August to October 2018 the NLP Programme Team talked to over six hundred people (a
combination of NCL NHS service users and stakeholders). People were specifically targeted for
engagement exercise based on the Stage 1 Desktop Review Equalities Impact Assessment.
People took part in thirteen workshops alongside potential service providers to develop ideas for
how the services could work in the future. Groups represented in the workshops included:
● Older people
● People from different ethnic backgrounds
● People with physical disabilities
● People with learning disabilities
● People with mental health conditions
● Women
● People from areas affected by socio-economic deprivation
● People who had undergone/were undergoing gender reassignment
Those involved in the options appraisal groups (who made up 50% of the panel) also contributed
to this phase.
The findings from these workshops have been integrated into this stage of the Integrated Health
Inequalities and Equality Impact Assessment.
PHASE 2
For the current phase (Phase 2) of the Integrated Health Inequalities and Equality Impact
Assessment no engagement with patients was undertaken. The aim of this work was to identify
positive and negative impacts resulting from proposed changes in the model of care delivery for
planned orthopaedic surgery for adults, particularly for people in protected characteristic
groups, carers and those affected by deprivation. Specifically, the work sought to identify which
groups needed to be ‘scoped-in’ for the consultation exercise and the following Phase 3
Integrated Health Inequalities and Equality Impact Assessment report.
A methodical approach was taken to understanding which groups would be impacted as a
direct consequence of the changes to the service model. This would ensure that specific
detailed analysis of impact (both positive and negative) was focused on those who would
experience change.
NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
24
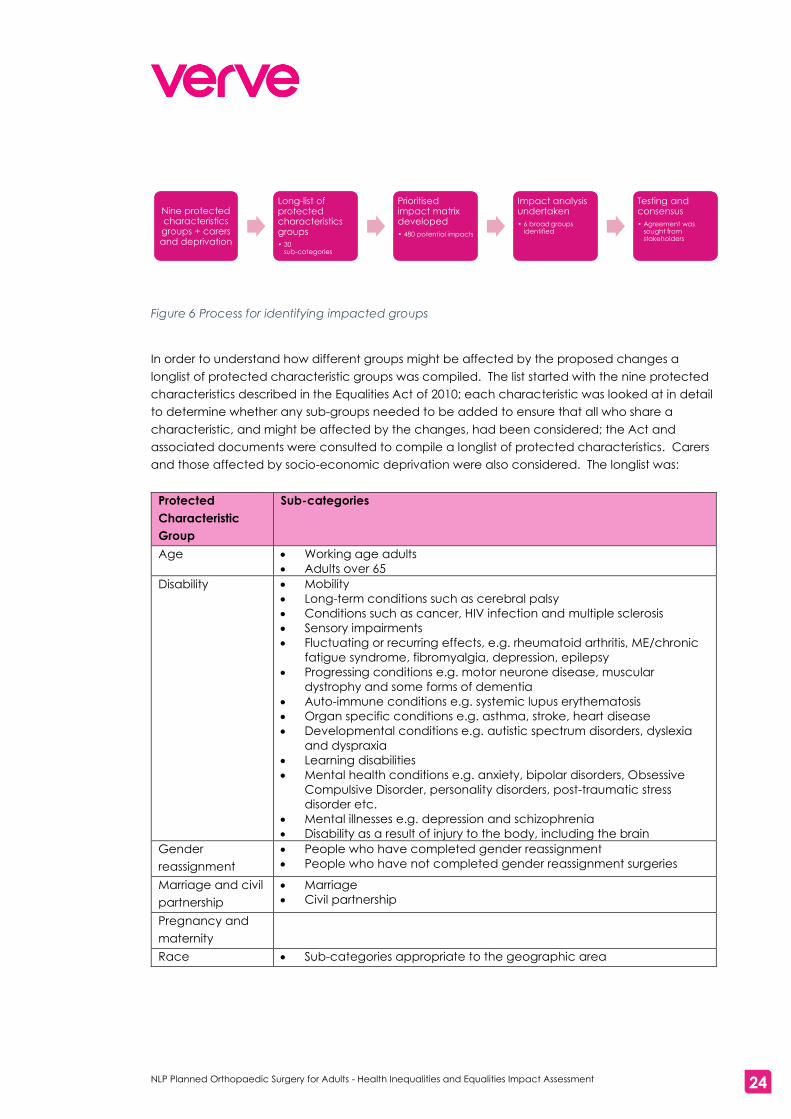
Figure 6 Process for identifying impacted groups
In order to understand how different groups might be affected by the proposed changes a
longlist of protected characteristic groups was compiled. The list started with the nine protected
characteristics described in the Equalities Act of 2010; each characteristic was looked at in detail
to determine whether any sub-groups needed to be added to ensure that all who share a
characteristic, and might be affected by the changes, had been considered; the Act and
associated documents were consulted to compile a longlist of protected characteristics. Carers
and those affected by socio-economic deprivation were also considered. The longlist was:
Protected
Characteristic
Group
Sub-categories
Age • Working age adults
• Adults over 65
Disability • Mobility
• Long-term conditions such as cerebral palsy
• Conditions such as cancer, HIV infection and multiple sclerosis
• Sensory impairments
• Fluctuating or recurring effects, e.g. rheumatoid arthritis, ME/chronic
fatigue syndrome, fibromyalgia, depression, epilepsy
• Progressing conditions e.g. motor neurone disease, muscular
dystrophy and some forms of dementia
• Auto-immune conditions e.g. systemic lupus erythematosis
• Organ specific conditions e.g. asthma, stroke, heart disease
• Developmental conditions e.g. autistic spectrum disorders, dyslexia
and dyspraxia
• Learning disabilities
• Mental health conditions e.g. anxiety, bipolar disorders, Obsessive
Compulsive Disorder, personality disorders, post-traumatic stress
disorder etc.
• Mental illnesses e.g. depression and schizophrenia
• Disability as a result of injury to the body, including the brain
Gender
reassignment
• People who have completed gender reassignment
• People who have not completed gender reassignment surgeries
Marriage and civil
partnership
• Marriage
• Civil partnership
Pregnancy and
maternity
Race • Sub-categories appropriate to the geographic area
Nine protected characteristics groups + carers and deprivation
Long-list of protected characteristics groups
• 30 sub-categories
Prioritised impact matrix developed
• 480 potential impacts
Impact analysis undertaken
• 6 broad groups identified
Testing and consensus
• Agreement was sought from stakeholders

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
25
Protected
Characteristic
Group
Sub-categories
Religion or belief • Sub-categories appropriate to the geographic area
Sex • Male
• Female
Sexual orientation • Consider whether to include sub-categories
Carers • Adults caring for adults (either could be patient)
• Adults caring for children with extra needs (adult would be patient)
• Young carers caring for adults (adult would be patient
• Paid carers
Socio-economic
deprivation
Table 4 Longlist of protected characteristics and other groups to consider
The long-list comprised 30 categories/sub-categories to consider.8
A ‘prioritised impact matrix’ was developed, allowing each of the 30 categories to be considered
against all the 16 service model and pathway change points (see section 7, above). Effectively,
the matrix showed service change points in columns and protected characteristics and
sub/groups as rows, giving a 30x16 table. Each of the 480 cells was considered in terms of
whether a service change was likely to affect a category or sub-category differentially or
disproportionately compared with the general population. Each cell was given a value of High,
Medium or Low for potential impact. High or Medium impacts could be positive or negative; a
Low impact indicated that little or no impact was likely.
Three expert analysts completed the matrix separately.
An example of a cell from one analysist’s matrix is given below:
Changes →
Ring fenced beds
Service Model or Pathway →
Service Model
Protected Characteristic
Sub-category
Disability Long-term conditions
High (positive) - fewer cancellations beneficial - can plan better e.g. when to stop medications pre surgery etc
Figure 7 Example of analytical matrix cell
8 We acknowledge that it is likely that people could fall into more than one category or sub-category in the
list above, however, it is beyond the scope of this exercise to consider the effects of intersectionality.
Analyst’s notes on the
effect of ring fenced
beds for people with
long-term conditions
– here the analyst has
said that a High
(positive) impact is
likely as fewer
cancellations mean
better planning is
possible etc.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
26
The analysts then came together to compare their views. Where differences of opinion occurred,
the analysts debated their positions until agreement was reached. In the rare instances when
agreement could not be reached the higher or highest level of impact was the final outcome
(for example, if 2 analysts assessed a cell as being High and one assessed as Medium, and
agreement could not be reached, the final impact assessment for that cell would be High).
A master matrix was produced showing the agreed cell values for all 480 cells from which a
shortlist of scoped in protected characteristics and sub-categories was developed, to include all
characteristics and sub-categories for whom the analysts had assigned High or Medium impacts.
It was also decided to combine some of the sub-categories where the impacts were similar or
identical across the matrix.
Scoped in
groups
Sub-categories To include
Age Adults over 65
Disability Mobility
Long-term conditions • Long-term conditions such as cerebral
palsy
• Conditions such as cancer, HIV infection
and multiple sclerosis
• Fluctuating or recurring effects, e.g.
rheumatoid arthritis, ME/chronic fatigue
syndrome, fibromyalgia, depression,
epilepsy
• Progressing conditions e.g. motor neurone
disease, muscular dystrophy and some
forms of dementia
• Auto-immune conditions e.g. systemic
lupus erythematosis
• Organ specific conditions e.g. asthma,
stroke, heart disease
• Disability as a result of injury to the body,
including the brain
Sensory impairments
Developmental and
learning disabilities
• Developmental conditions e.g. autistic
spectrum disorders, dyslexia and
dyspraxia
• Learning disabilities
Mental health conditions
and mental illnesses
• Mental health conditions e.g. anxiety,
bipolar disorders, obsessive compulsive
disorder, personality disorders, post-
traumatic stress disorder etc.
• Mental illnesses e.g. depression and
schizophrenia
Gender
reassignment
• Include people who have/have not
completed gender reassignment
surgeries
Race • Describe potential differential needs of
some ethnic groups and note where
NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
27
Scoped in
groups
Sub-categories To include
there are geographic hotspots – look for
impacts based on travel
Carers • Adults caring for adults
(either could be
patient)
• Adults caring for
children with extra
needs (adult would be
patient)
• Young carers caring for
adults (adult would be
patient)
Socio-
economic
deprivation*
Table 5 Shortlist of scoped in groups
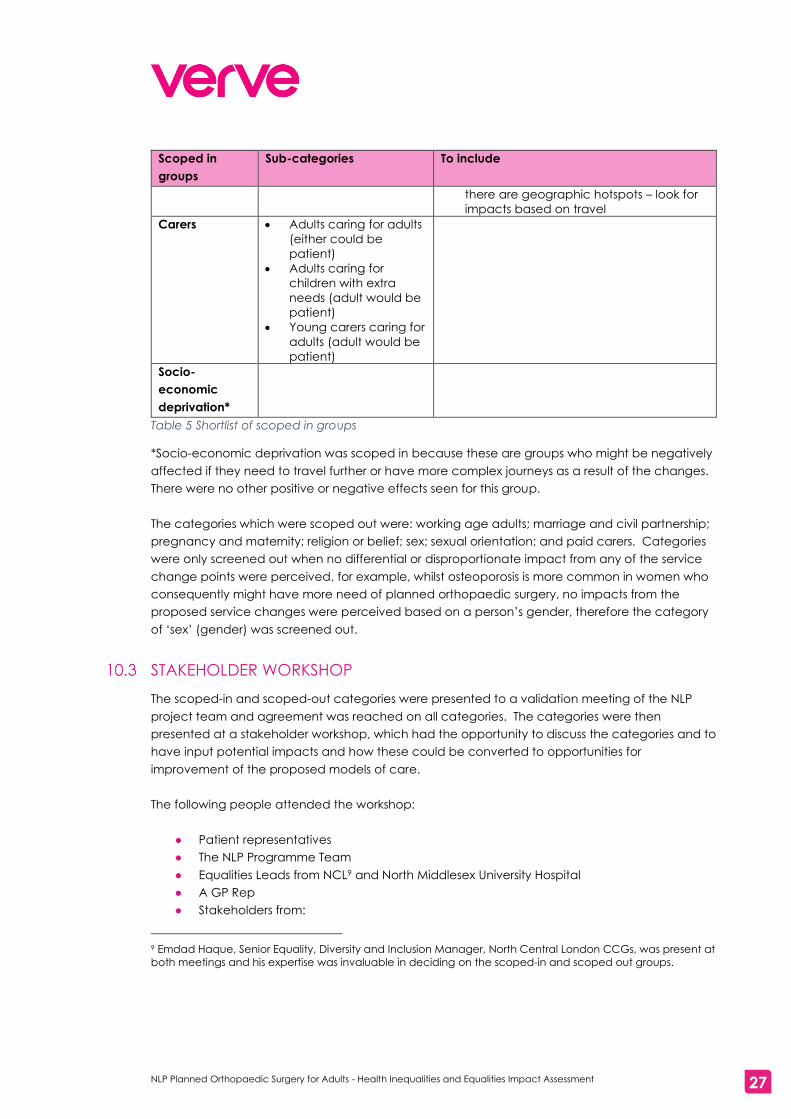
*Socio-economic deprivation was scoped in because these are groups who might be negatively
affected if they need to travel further or have more complex journeys as a result of the changes.
There were no other positive or negative effects seen for this group.
The categories which were scoped out were: working age adults; marriage and civil partnership;
pregnancy and maternity; religion or belief; sex; sexual orientation; and paid carers. Categories
were only screened out when no differential or disproportionate impact from any of the service
change points were perceived, for example, whilst osteoporosis is more common in women who
consequently might have more need of planned orthopaedic surgery, no impacts from the
proposed service changes were perceived based on a person’s gender, therefore the category
of ‘sex’ (gender) was screened out.
STAKEHOLDER WORKSHOP
The scoped-in and scoped-out categories were presented to a validation meeting of the NLP
project team and agreement was reached on all categories. The categories were then
presented at a stakeholder workshop, which had the opportunity to discuss the categories and to
have input potential impacts and how these could be converted to opportunities for
improvement of the proposed models of care.
The following people attended the workshop:
● Patient representatives
● The NLP Programme Team
● Equalities Leads from NCL9 and North Middlesex University Hospital
● A GP Rep
● Stakeholders from:
9 Emdad Haque, Senior Equality, Diversity and Inclusion Manager, North Central London CCGs, was present at
both meetings and his expertise was invaluable in deciding on the scoped-in and scoped out groups.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
28
NCL
UCLH
Royal Free Hospital
● Mott MacDonald team
● Verve team
The agenda of the workshop was:
● Introduction to the workshop
● Setting the scene – the review so far
● What are equalities analyses and why do we do them?
● Travel analysis – what is being looked at and early findings
● Equalities Impact Assessment – potential impacts from proposed changes to the service
model and care pathway
● Opportunities for improvement already in the proposed models
● Looking for further opportunities for improvement
● Table discussions on how specific potential impacts could be converted into
opportunities for improvement
● Feedback on the table discussions
● Closing statements
Potential opportunities for improvement, or mitigations, suggested during the Stakeholder
Workshop are presented in section 13.1.1
This HIEIA builds on an extensive pre-consultation engagement exercise and previous desktop
review, as described in Section 10.1.
These exercises involved engagement with groups sharing protected characteristics and were
key to setting the scope and method for this stage. During these exercises, sections (a) and (c) of
the public sector equality duty were considered. These relate to having due regard to the need
to eliminate discrimination, harassment and victimisation (section (a)) and to foster good relations
(section (c)).
Nothing in the responses to pre-consultation engagement indicated issues relevant to these
aspects of the duty. However, we note that NLP intend to ensure within the consultation period
that this is tested further, and we would expect to include any relevant findings and proposed
mitigations in our final report.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
29
11. POPULATION DENSITIES OF THE SCOPED IN GROUPS
This section gives the population of NCL and the demographics of the scoped in groups
discussed in section 10. The maps also show the locations of NHS and private hospitals in NCL, for
reference.
THE POPULATION OF NCL
The estimated resident population of NCL in 2019 is approximately 1.5 million. Over the next
decade the NCL population is expected to increase by 9%10
The following map11 shows population density in NCL and surrounding areas
Map 1 Population density of NCL and surrounding areas
PEOPLE AGED 65+
The 2019 estimate of NCL residents aged over 65 is 182,00012, with an expected increase to
234,000 in the next ten years.
The map below shows the population density of people aged 65 and over in NCL and
surrounding areas. The data is derived from ONS Mid-year population estimates, 2018.
10 GLA 2017 based housing led population projections 11 The maps in this section were prepared by Mott MacDonald for the associated travel analysis for this project 12 GLA 2017 based housing led population projections

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
30
Map 2 Population density of residents aged 65+ in NCL and surrounding areas
DISABILITY
A survey13 has estimated that 14% of people aged 16-74 in the inner London regions live with
disabilities. The estimate of the NCL population in 2017/18 living with disabilities in 211,00014.
The map below shows the population density of people with long term health problems and
disabilities in NCL and surrounding areas. The data is derived from people reporting that they
had long-term health problems or disabilities in the 2011 Census.
13 2017/18 Family Resource Survey 14 2017/18 estimated calculated by the Public Health Knowledge and Intelligence team applying regional
prevalence to NCL boroughs.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
31
Map 3 Population density of people with long term health problems and disabilities in NCL and
surrounding areas
GENDER REASSIGNMENT
At present there are no official estimates of the numbers of people who have undergone, or are
undergoing, gender reassignment either nationally or locally.
RACE
GLA 2016 based population projections show approximately 62% (943,000 people) of the NCL
population are from White ethnic groups; there is a lot of diversity amongst the rest of the
population, with 191,000 people being from Black ethnic groups, 94,000 describing themselves as
being in a ‘mixed’ ethnic group and 217,000 being from Asian ethnic groups15. The 2011 Census
showed that there were 70,324 Turkish people living in NCL.
The following maps show the population densities for White people, Black people, Asian people
and Turkish people. The data used to produce the maps is from the 2011 Census.
15 GLA 2016 based population projections

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
32
Map 4 Population density of White people in NCL and surrounding areas
Map 5 Population density of Black people living in NCL and surrounding areas

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
33
Map 6 Population density of Asian people living in NCL and surrounding areas
Map 7 Population density of Turkish people living in NCL and surrounding areas
NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
34
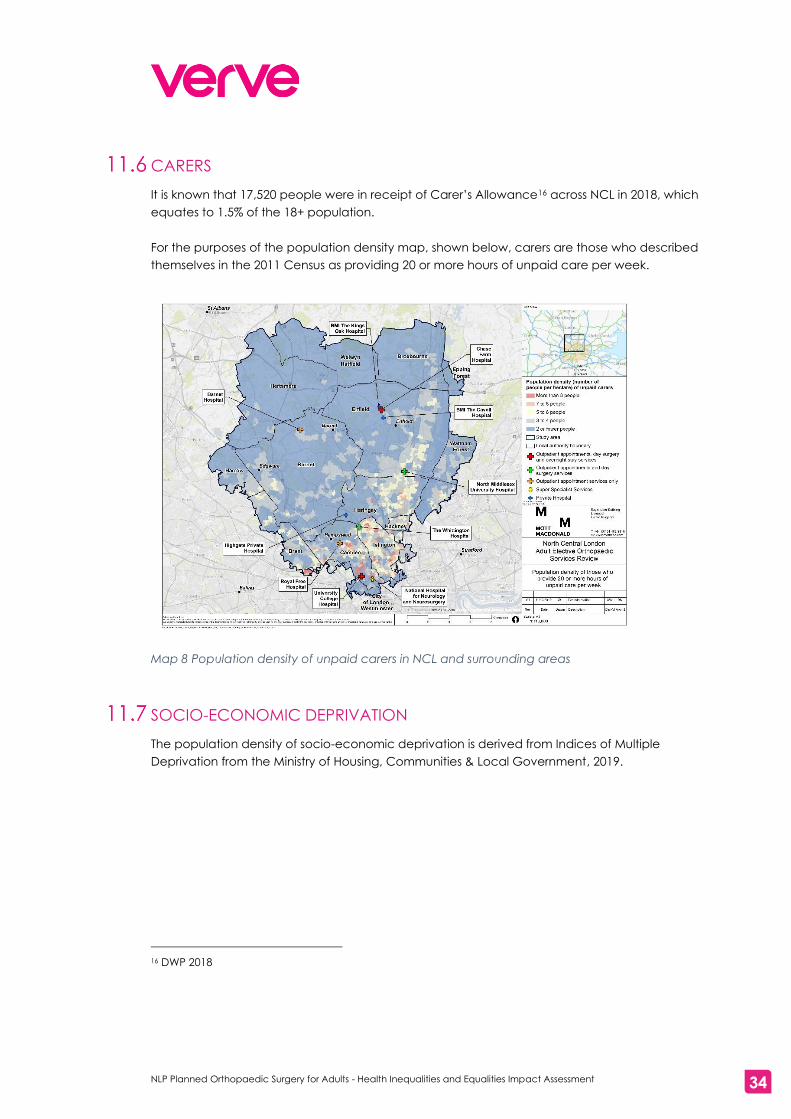
CARERS
It is known that 17,520 people were in receipt of Carer’s Allowance16 across NCL in 2018, which
equates to 1.5% of the 18+ population.
For the purposes of the population density map, shown below, carers are those who described
themselves in the 2011 Census as providing 20 or more hours of unpaid care per week.
Map 8 Population density of unpaid carers in NCL and surrounding areas
SOCIO-ECONOMIC DEPRIVATION
The population density of socio-economic deprivation is derived from Indices of Multiple
Deprivation from the Ministry of Housing, Communities & Local Government, 2019.
16 DWP 2018

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
35
Map 9 Population density of socio-economic deprivation in NCL and surrounding areas

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
36
12. FINDINGS
This section of the report will discuss impacts of the proposed service change points (see section
7, above) in relation to the scoped-in groups outlined in section 9, above.
It is important to stress that impacts are analysed and described to enable the programme team
to consider them and develop a response as the programme progresses. Negative impacts are
not, in themselves, static – but should be seen as opportunities for further refinement of the
model. The consultation offers an ideal opportunity, in partnership with affected groups, to seek
the views of stakeholders in order to find suitable mitigations.
Both POSITIVE and NEGATIVE impacts are examined in the table. We have identified:
16 POSITIVE IMPACTS
1 NEGATIVE IMPACT
The section starts with a table showing where medium and high impacts of change might be
expected, and whether these are positive or negative impacts; there is then a discussion of what
the impacts are likely to be.
THE IMPACTS OF CHANGE PROVISION
The following tables show the proposed change points, their expected outcomes and our
evaluation of where High or Medium, positive or negative impacts might occur. Low impacts are
not shown as it is expected that there would be little or no impact.
12.1.1 SERVICE MODEL CHANGES
Change Expected outcome Impacts
Changes of location
Improved clinical outcomes
including reduced
cancellations, decreased
waiting times, reduced
infection rates, decreased
revisions and readmissions.
The delivery of at-scale
orthopaedic surgery at
dedicated facilities would
result in consistently excellent
clinical interventions across
end-to-end pathways.
Consistent high quality
integrated care in NHS
provision for those moving
Potential for positive or
negative impacts
depending on where
patients live as journey
times may be shorter or
longer.17
HIGH POSITIVE impacts
for all patients, including
scoped in groups, re
reduction of
cancellations and
waiting times etc.
HIGH POSITIVE impacts
for people with
disabilities who have
17 It should be noted that patients can choose which partnership they are referred to for care, and they could
choose to go to a hospital which is geographically further from them.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
37
Change Expected outcome Impacts
from NHS funded private
sector care to NHS care.
Access to the right treatment
at the right time for those who
have been mis-referred to
RNOH for non-specialist care,
and who could be suitable for
NHS care in NCL
carers. More choice
would be available for
carers to stay overnight
with those they care for.
Currently UCLH offers this
facility and the
proposed changes
would see Chase Farm
having this provision too.
POSITIVE impacts for
people moving from NHS
funded private sector
provision into NHS
provision as they will
have access to
consistent high quality
integrated care
delivered by the NHS.
POSITIVE impacts for
those mis-referred to
RNOH for non-specialist
care as they would not
experience delays in
treatment arising from
mis-referral.
HIGH NEGATIVE impacts
possible for people with
disabilities (learning
disabilities, autistic
spectrum disorders etc),
carers and those
affected by socio-
economic deprivation
and some ethnic groups
who might have to travel
to different hospitals for
surgery, with potentially
more complex or longer
journeys.
Dedicated (ring fenced) beds for
patients requiring in-patient care
Reduced cancellations
related to orthopaedic
trauma/non-orthopaedic
admissions, reduced waiting
times, reduced infection rates,
high quality consistent care,
reduced revision rates and
readmissions
MEDIUM/HIGH POSITIVE
impacts for all patients,
especially for those with
disabilities, carers and
those affected by socio-
economic deprivation
Dedicated theatre space able to
operate 7 days a week
Increased capacity, reduced
cancellations, reduced
waiting times, reduced
infection rates, high quality
MEDIUM/HIGH POSITIVE
impacts for all patients,
especially for those with
disabilities, carers and
NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
38
Change Expected outcome Impacts
consistent care, reduced
variation in care, reduced
revision rates and readmissions
those affected by socio-
economic deprivation
A minimum level 2 high
dependency unit available
Ability to manage
complicated and
deteriorating patients safely
and effectively on site
minimising the need for
transfer
MEDIUM/HIGH POSITIVE
impacts for all patients,
especially for those with
other health conditions
or disabilities which
might cause medical
complexity
Systems and processes in place
to effectively manage
deteriorating patients/those who
require more intensive treatment
including transfer to intensive
care
Early identification of patients
who are likely to require
additional medical support to
enable care plans to be
initiated.
Patients receiving the right
care are the right time
through immediate referral to
the most appropriate hospital
that meets their clinical need.
Robust pathways in place to
transfer patients to Intensive
care
MEDIUM/HIGH POSITIVE
impacts for all patients,
especially for those with
other health conditions
or disabilities which
might cause medical
complexity
Senior overnight medical cover
giving medical cover 24/7 on site
The needs of patients who
deteriorate unexpectedly or
who require more complex
intervention can be safely and
effectively managed without
transfer improving patient
experience
MEDIUM/HIGH POSITIVE
impacts for all patients,
especially for those with
other health conditions
or disabilities which
might cause medical
complexity
Rehabilitation services 7 days a
week
Providing effective
intervention, improving
experience and reducing
length of stay
MEDIUM/HIGH POSITIVE
impacts for all patients,
especially for those with
other health conditions
or disabilities which
might cause medical
complexity
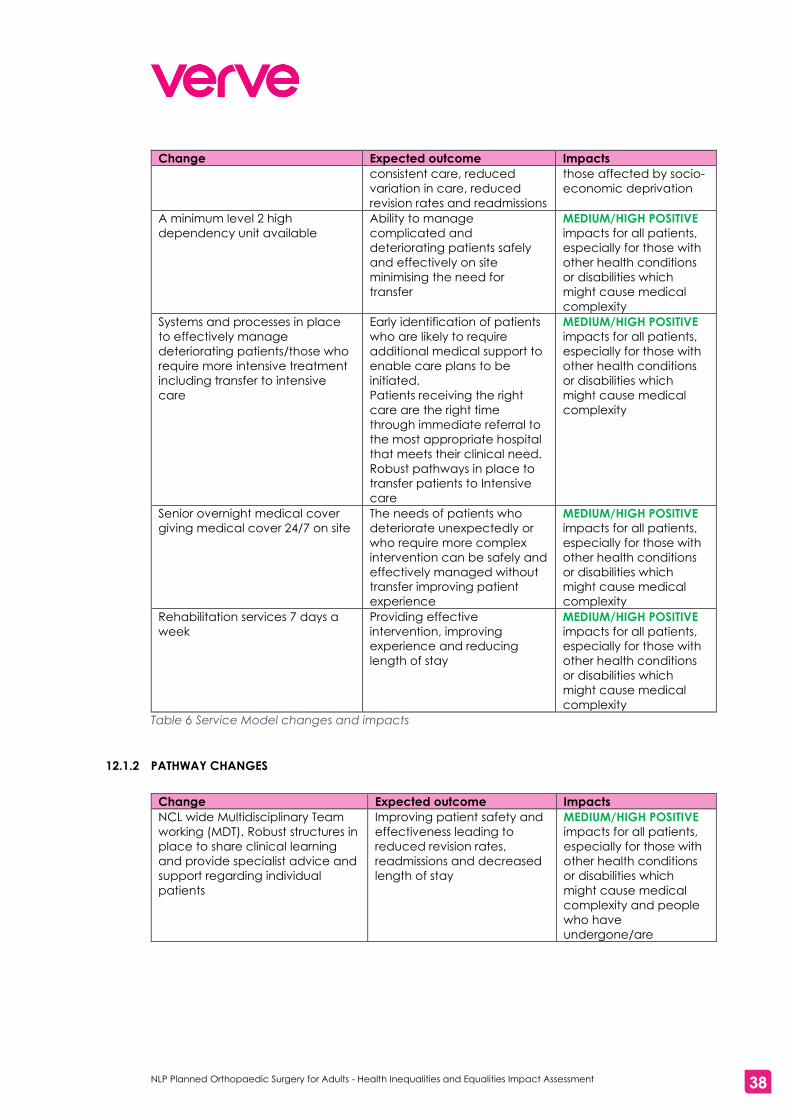
Table 6 Service Model changes and impacts
12.1.2 PATHWAY CHANGES
Change Expected outcome Impacts
NCL wide Multidisciplinary Team
working (MDT). Robust structures in
place to share clinical learning
and provide specialist advice and
support regarding individual
patients
Improving patient safety and
effectiveness leading to
reduced revision rates,
readmissions and decreased
length of stay
MEDIUM/HIGH POSITIVE
impacts for all patients,
especially for those with
other health conditions
or disabilities which
might cause medical
complexity and people
who have
undergone/are

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
39
Change Expected outcome Impacts
undergoing gender
reassignment
Care co-ordinator roles in place to
support patients in navigating the
system and accessing the right
care and support at the right time
Improved patient experience
and effectiveness of care
resulting in decreased length
of stay and the risk of
readmission
MEDIUM/HIGH POSITIVE
impacts for all patients,
especially those over the
age of 65, people with
disabilities, carers and
those affected by socio-
economic deprivation
Consistent referral pathways and
criteria
Equitable care that ensure all
patients across NCL receive
the same high quality access
to services
MEDIUM POSITIVE
impacts for all patients,
NCL wide approach to pre- and
post-operative information and
patient education
Ensuring all patients receive
the same high quality
information and advice
MEDIUM POSITIVE
impacts for all patients,
especially those over the
age of 65 and those with
disabilities
Standardise NCL wide pre-
operative assessment practices
and protocols
NCL wide assessment
practices will ensure clinical
and social issues are
identified early and needs
based care plans
implemented
MEDIUM/HIGHPOSITIVE
impacts for all patients,
especially those with
disabilities and for
people who have
undergone/are
undergoing gender
reassignment
Surgeons will follow the patient
from base hospital to planned
orthopaedic surgery centre to
ensure there is consistency of care
Improving patient experience MEDIUM/HIGHPOSITIVE
impacts for all patients,
especially those with
disabilities and for
people who have
undergone/are
undergoing gender
reassignment
Table 7 Pathway changes and impacts
As the table above shows, we estimate that there could be some negative impacts for some
groups in relation to the re-location of services, however, the intended outcomes of the re-
location of services (reduction of waiting times and fewer cancellations) are seen as highly
positive outcomes for all patients, including some specific scoped in groups; the availability of
space for carers to stay with patients at Chase Farm is also a high positive impact.
For all other proposed changes, we estimate there will be medium or high positive impacts for all
patients and have identified scoped-in groups where the impact is likely to be most beneficial.
DISCUSSION OF THE IMPACTS OF THE CHANGES
The service change points cluster under five headings: locations of care provision; changes to
reduce cancellations; changes to manage complicated and deteriorating patients;

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
40
rehabilitation services; and changes to improve the care pathway. Each will be discussed below
in relation to positive or negative benefits for particular scoped-in groups.
12.2.1 LOCATIONS OF CARE PROVISION
The service changes proposed will rationalise the locations where adults receive planned
orthopaedic surgery, and consolidate surgery requiring an overnight stay onto two sites.
In the past planned orthopaedic surgery for adults was available in ten locations across the NCL
patch. The new service model proposes two sites for inpatient care (i.e. procedures requiring an
overnight stay) and four sites for day surgery (i.e. procedures not requiring an overnight stay).
All patients would experience a significant improvement in their care and to achieve this, some
patients would have surgery in a different hospital in future, when compared to current
arrangements.
Day surgery: For example, shoulder, hand and foot surgery
● 360 patients a year who would currently go to UCLH would have their surgery at
Whittington Hospital instead.
● 80 patients a year, who would currently have NHS care in a private hospital, would over
time have their surgery at UCLH instead.
● 1020 patients a year, who would currently have NHS care in a private hospital, would
over time have their surgery at Chase Farm instead.
Overnight stay: For example, hip and knee surgery
● 400 patients who would currently go to North Mid. would have their surgery at Chase
Farm instead.
● 360 patients who would currently go to Whittington Hospital would have their surgery at
UCLH instead.
● 560 patients who would currently have NHS care in a private hospital, would over time
have their surgery at Chase Farm instead.
● 40 patients who currently have NHS care in a private hospital would over time have their
surgery at UCLH instead.
● 225 patients referred to the RNOH for non-specialist care could be suitable for treatment
at the Chase Farm instead.
● 75 patients referred to the RNOH for non-specialist care could be suitable for treatment
at UCLH instead.
Two things should be noted here: first, the patients enumerated above are future patients, not
people who would have to changes location part way through their care; second, for those
requiring inpatient care, generally, only one or two visits to the hospital where operations are
done are needed.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
41
Travelling to a different location may have positive or negative impacts for patients, depending
on the start point for their journey and which partnership they choose for their care; for some
people journeys may be shorter or easier, but for others journeys could be more complex, more
costly or longer. Mott MacDonald’s work reports in detail the potential impacts of changes of
location and travel time for the scoped in groups18.
Mott MacDonald assessed the following potential impacts:
● Longer journey times – high likelihood, moderately adverse –increase in journey time
expected for the majority of residents across NCL, but likely to be around 15 minute
increase
● Availability of public transport – high likelihood for northern partnership (North
Middlesex/Royal Free London) with moderately adverse effects; medium likelihood for
southern partnership (UCLH/Whittington Health) with minor adverse effects
● Additional travel costs – high likelihood, moderate adverse effects, especially for more
deprived communities, those with long term conditions and some BAME groups
● Cost and availability of parking – medium likelihood, minor adverse effects
For a full description of methodology and discussion of the impacts of change, together with
suggested mitigations, please see Mott MacDonald’s report.
Mott MacDonald have produced the following demographic information about the people who
are most likely to be affected by the movement of care provision (see the Mott MacDonald
report on transport issues for an explanation of their methodology):
18 PLACEHOLDER for link to MM report
NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
42
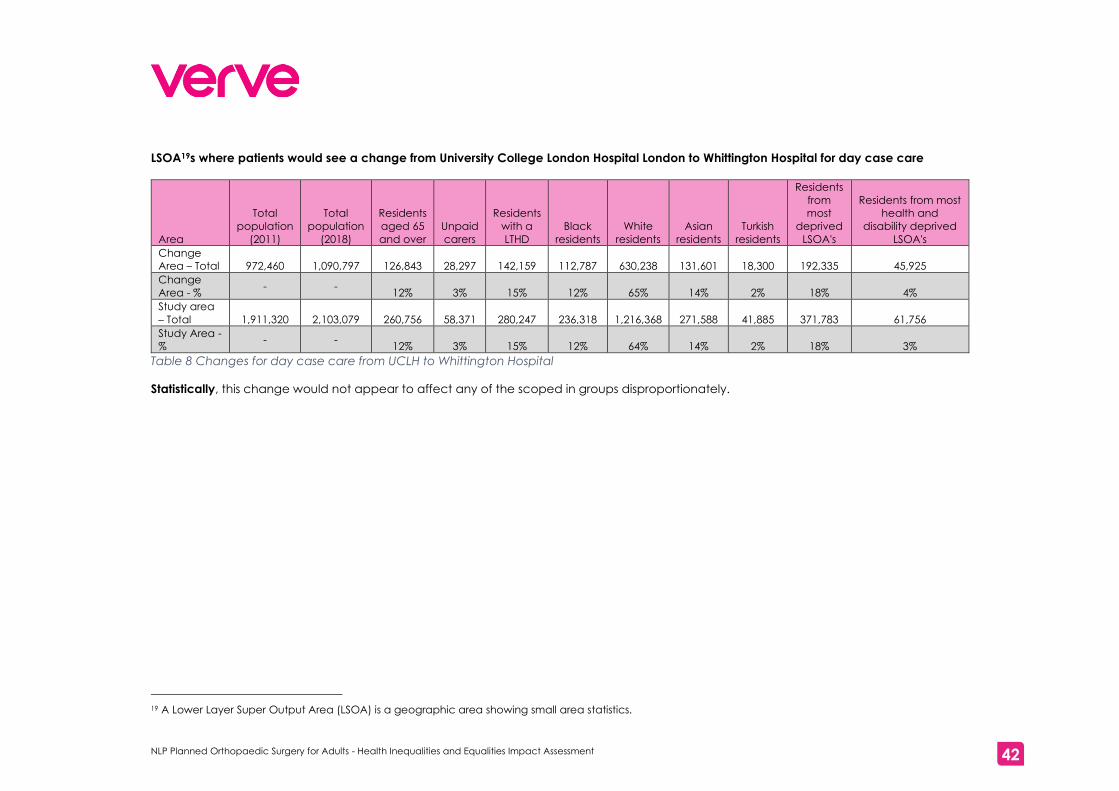
LSOA19s where patients would see a change from University College London Hospital London to Whittington Hospital for day case care
Area
Total
population
(2011)
Total
population
(2018)
Residents
aged 65
and over
Unpaid
carers
Residents
with a
LTHD
Black
residents
White
residents
Asian
residents
Turkish
residents
Residents
from
most
deprived
LSOA's
Residents from most
health and
disability deprived
LSOA's
Change
Area – Total 972,460 1,090,797 126,843 28,297 142,159 112,787 630,238 131,601 18,300 192,335 45,925
Change
Area - % - -
12% 3% 15% 12% 65% 14% 2% 18% 4%
Study area
– Total 1,911,320 2,103,079 260,756 58,371 280,247 236,318 1,216,368 271,588 41,885 371,783 61,756
Study Area -
% - -
12% 3% 15% 12% 64% 14% 2% 18% 3%
Table 8 Changes for day case care from UCLH to Whittington Hospital
Statistically, this change would not appear to affect any of the scoped in groups disproportionately.
19 A Lower Layer Super Output Area (LSOA) is a geographic area showing small area statistics.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
43
LSOAs where patients would change from Whittington Hospital to University College London Hospital for inpatient care
Area
Total
population
(2011)
Total
population
(2018)
Residents
aged 65
and over
Unpaid
carers
Residents
with a
LTHD
Black
residents
White
residents
Asian
residents
Turkish
residents
Residents
from
most
deprived
LSOA's
Residents from most
health and
disability deprived
LSOA's
Change
Area - Total 519,418 571,474 65,387 15,114 75,921 66,709 340,956 59,413 13,263 122,735 33,796
Change
Area - % - -
11% 3% 15% 13% 66% 11% 3% 21% 6%
Study area
– Total 1,911,320 2,103,079 260,756 58,371 280,247 236,318 1,216,368 271,588 41,885 371,783 61,756
Study Area -
% - -
12% 3% 15% 12% 64% 14% 2% 18% 3%
Table 9 Changes for inpatient care from Whittington Hospital to UCLH
Statistically, the biggest effect of this change would be for residents living in the most deprived areas and those with the most health and
disability deprivation.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
44
LSOAs where patients would change from North Middlesex University Hospital to Chase Farm Hospital for inpatient care
Area
Total
population
(2011)
Total
population
(2018)
Residents
aged 65
and over
Unpaid
carers
Residents
with a
LTHD
Black
residents
White
residents
Asian
residents
Turkish
residents
Residents
from
most
deprived
LSOA's
Residents from most
health and
disability deprived
LSOA's
Change
Area - Total 347,525 376,934 43,893 11,742 54,838 71,052 198,627 39,234 18,420 143,491 11,292
Change
Area - % - -
12% 3% 16% 20% 57% 11% 5% 38% 3%
Study area
– Total 1,911,320 2,103,079 260,756 58,371 280,247 236,318 1,216,368 271,588 41,885 371,783 61,756
Study area -
% - -
12% 3% 15% 12% 64% 14% 2% 18% 3%
Table 10 Changes for inpatient care from North Middlesex University Hospital to Chase Farm Hospital
Statistically, the biggest effect of this change would be for Black people, Turkish people and those affected with social deprivation.
NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
45
We believe there are four specific scoped-in groups who are potentially impacted by a change
in the location of their care, depending upon the start-point for their journey and their choice of
partnership:
Disability
Although it might be expected that patients with mobility issues would be negatively affected by
changes in location if longer or more complex journeys to hospitals were necessary, in fact they
are more likely to be eligible for patient transport than some other groups, so any changes could
be mitigated for many members of this group. There is, however, further consideration of impact
necessary for those with a physical disability who may not access patient transport services.
For those choosing Chase Farm for inpatient care there could be benefits for people who have
carers, as provision could be made for carers to stay overnight, which is likely to reduce anxiety
and allow their carer to be involved in their day-to-day care. This provision is currently available
at UCLH, so the proposals would offer more choice for people with carers.
There could be negative impacts for people who might struggle in new environments, for
example, those with sensory impairments and people with learning difficulties. Some potential
mitigations, raised at the stakeholder workshop, will be discussed in the next chapter.
Carers
Longer, more complex or more costly journeys are likely to have high negative impacts on carers,
whether they are the patient or caring for someone who is a patient. For carers who are patients
finding cover whilst they attend appointments can be difficult, and potentially costly, so the
shortest time away from home is beneficial.
Socio-economic deprivation
For those affected by socio-economic deprivation more costly journeys would be problematic.
Some people, depending on whether they are claiming certain benefits, are able to claim back
taxi fares to appointments. However, having enough money to pay the fare and then claim
back could cause problems.
Ethnicity
Mott MacDonald’s analysis shows that Turkish people and Black people could be particularly
impacted by the movement of services from North Middlesex University Hospital to Chase Farm
because of the location where they are likely to live. The Travel Analysis report discusses this in
more detail.
12.2.2 CHANGES TO REDUCE CANCELLATIONS
Ring fenced beds for planned orthopaedic surgery and dedicated theatres for operations would
both have the effect of reducing cancellations of appointments, improving waiting times,
reducing infection rates and reducing revision rates and readmissions.
These service changes were seen to be beneficial for all patients, with positive benefits for the
following groups:

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
46
Disability and gender reassignment - medications
A particular benefit of reducing cancellations was identified for people whose condition requires
them to take regular medications. Some surgical procedures require patients to stop taking
medications for a specified time before going to hospital. If their operation is cancelled, they will
have to stop their medications a second time.
Disability - anxiety
Reductions in cancellations were identified as being particularly beneficial for people who might
be anxious about going to hospital for an operation, for example people with developmental
and learning difficulties, mental health problems and mental illnesses, and those with sensory
impairments, who might have worked with carers or others to go to hospital on a particular day.
Similarly, reductions in waiting times would also be beneficial for people in this category.
Carers - disruption
For carers who are patients making plans for care provision in their absence can be complex; a
cancellation of an operation would be very disruptive for them.
Socio-economic deprivation - costs
Cancellations could be costly for people affected by socio-economic deprivation, for example,
for people on zero-hours contracts. Reducing waiting times and cancellations is likely to be
highly beneficial for this group in terms of less loss of income and fewer wasted journeys.
12.2.3 CHANGES TO MANAGE COMPLICATED AND DETERIORATING PATIENTS
Having robust systems in place to manage complicated and deteriorating patients, including
having onsite HDU facilities in centres offering inpatient planned orthopaedic surgery and having
24/7 medical cover would be beneficial for all patients, particularly for those with underlying
medical conditions and disabilities.
Disability - planning
There are likely to be high positive impacts for people with long term conditions and complex co-
morbidities. People’s needs could be planned for and their conditions managed without the
need to transfer to another hospital if they deteriorate.
12.2.4 REHABILITATION SERVICES AVAILABLE 7 DAYS A WEEK
By providing rehabilitation services 7 days a week patient will be able to be mobilised quickly.
This is likely to reduce the length of stay in hospital and improve patient experience. Patients with
disabilities are likely to have high positive benefits.
Disability – reducing length of stay
For many people with disabilities, particularly those who might be anxious about being in hospital,
having rehabilitation services available 7 days a week is likely to help them to return home to a
less stressful environment more quickly.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
47
12.2.5 CHANGES TO IMPROVE THE CARE PATHWAY
Six of the changes identified are designed to improve the care pathway for patients: NCL wide
Multidisciplinary Team working; care co-ordinators; patients seeing the same surgeon and/or
surgical team throughout their care; consistent referral pathways; standardised patient
education and information; a consistent approach to pre-operative assessment.
Whilst the changes to the care pathway are likely to improve the quality of care for all patients,
there are some groups for whom the impacts are likely to be medium or highly positive.
Disabilities
For people who have complex needs having consistency in the care pathway is likely to be
highly beneficial. Having robust learning structures in place is likely to enhance staff
understanding of patients’ potential needs, for example how to help patients with sensory
impairments or developmental difficulties. Care co-ordinators are likely to have high positive
impacts for those with disabilities by helping them to understand the system and how to navigate
it.
Adults over 65
This group of patients is likely to gain medium benefit from standardised patient information, so
that they understand what is going to happen and what they need to do to maximise the benefit
of their operation. Further, this group could also benefit from care co-ordinators helping them to
navigate the care pathway.
Gender reassignment
For people in this category, disclosure of their gender reassignment can be worrying. Having
consistency across the care pathway would be highly beneficial. MDTs could provide specialist
advice to colleagues; care co-ordinators could provide information for patients and being
assured that they would see the same surgical team throughout is likely to reduce anxiety and
improve patient experience.
Socio-economic deprivation
For people who might anxious about loss of earnings or the cost of journeys to and from hospital
care co-ordinators are likely to have a high positive impact if they can provide information about
what support is available.
Carers
When a carer is a patient there is likely to be anxiety about how they can ‘fit in’ pre-operative
assessments, surgery and post-operative recovery with as little disruption to their caring duties as
possible. Care co-ordinators could have a high positive impact by helping carers to understand
how long the process is likely take and what support is available to them.
The findings from this phase of the work will be used to help formulate consultation engagement
plans. During the consultation practical mitigations will be explored with the scoped in priority
groups.
NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
48
13. CONCLUSIONS
The objective of this phase of the health inequalities and equality impact assessment was to
identify where changes to the provision of planned orthopaedic surgery for adults in NCL might
have positive or negative impacts on protected characteristic groups, carers and those affected
by socio-economic deprivation.
Overall, for all patients, there are likely to be positive impacts on patients’ health by reductions to
waiting times, having fewer cancellations, reducing infection rates and reducing revision rates
and readmissions.
The report has shown that generally the changes are likely to have positive impacts for all
patients, and for some scoped-in groups in particular.
There are some potentially negative impacts arising from changes to the location of the services
in future, however, there are also some positive impacts from the location changes.
RECOMMENDATIONS FROM THE INTEGRATED HEALTH INEQUALITIES AND
EQUALITY IMPACT ASSESSMENT FOR THE CONSULTATION PHASE
The work in this phase of the EIA was designed to feed into the consultation phase. The
consultation will involve engagement with residents across the catchment seeking to:
● Understand whether the options are supported and perceptions about benefits and
concerns
● Identify a schedule of mitigations to reduce any negative impacts identified.
In conducting the consultation, we recommend the following:
13.1.1 RECOMMENDATION 1 – FOCUS ON POSITIVE STEPS TO TACKLE INEQUALITY
Stakeholders should be invited to consider, critique and co-design current and planned
mitigations for negative impacts identified in this report.
A stakeholder workshop held to validate the scoped-in groups for this element of the health
inequalities and equality impact assessment suggested several mitigations. These could be used
to develop especially valuable insight if incorporated into discussion guides for deliberative
workshops and/or other qualitative approaches:
● Volunteers who can help people with sensory impairments to navigate hospitals,
particularly in sites which they are unused to
● For people who have sensory impairments, learning disabilities, autistic spectrum
disorders or anxiety, a visit to an unfamiliar site ahead of an appointment could be
arranged to allow them to become familiar with the environment
● Co-ordination between GP and learning disability nurses at hospitals would be helpful for
people with learning disabilities
NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
49
● Ways to transfer information on support needs between GP and hospital, and different
hospitals in the partnership
● Improve training for hospital staff on how to find support for those who need it, and know
how to ask patients what care they need
● Ensure that patients know what their patient journey is likely to be, including which
hospitals they will visit, and how many appointments they are likely to have
● Ensuring that carers are involved when the person they care for is a patient
● Ensuring that patients know what help there is for them
● Ensuring patients and carers know that they can ask for changes to appointment or
surgery times to better fit their needs
● Planning procedures to best help people with long term conditions, for example putting
people with diabetes first on operating lists to cause least disruption to their medications
● For people with lower literacy levels using picture diagrams
● For those with little or no English, ensuring adequate interpreting services are available
● Training staff in basic British Sign Language
● Utilising the skills of staff who already work in our hospitals to draw on their language skills
● Support patient choice at referral so that they can choose the most convenient
partnership for the surgery they will require
Further work with stakeholders could identify more mitigations.
13.1.2 RECOMMENDATION 2 – PRIORITISING PEOPLE FOR WHOM EQUALITIES IMPACTS ARE LIKELY
TO BE HIGHEST
During the public consultation stage (which will commence in January 2020) the views of groups
and individuals should be sought to generate potential mitigations for specifically identified
negative impacts, and to ensure that potentially negative impacts have not been overlooked.
We would recommend that the following scoped-in groups are consulted:
● Carers, including:
Carers who might be patients themselves
Those who care for people who might be patients
Young people who care for a person who might be a patient
● People affected by socio-economic deprivation
● Black and minority ethnic communities, in particular the following groups, who are highly
represented in Haringey and where current patterns of provision suggest may be likely to
have surgery at a different site in future:
People from Turkish backgrounds
People from Black African and Black Caribbean backgrounds
● People who have had/are in the process of having gender reassignment surgery
● Previous patients who fall into any of the scoped-in groups discussed in this report.
We believe that by asking individuals, and groups representing the scoped-in groups, what
worked for them and where there could have been improvements a robust schedule of
mitigations can be created.

NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
50
13.1.3 RECOMMENDATION 3 – TARGETED APPROACHES TO ENGAGEMENT WHERE NECESSARY
We also recognise that targeted approaches to engagement may be necessary to reach some
of these groups, and recommend that the following are considered:
● Telephone interviews for members of the groups who may find it difficult to attend
meetings and events and tend to be under-represented in face-to-face engagement
exercises, specifically:
o People with physical disabilities and access challenges
o Carers
● Engagement through national or regional representative bodies and/or trusted networks
of people where relatively small numbers of individuals sharing protected characteristics
are resident across the entire footprint, specifically:
o People who have had/are in the process of having gender reassignment
surgery.
13.1.4 RECOMMNEDATION 4 - ENSURING FOLLOW-THROUGH
We recommend the consultation evaluation report should contain discrete summaries of:
● The views of scoped in groups and communities especially those identified as priorities
(see Recommendations 2 and 3)
● The views on potential mitigations with a view to exploring their feasibility and practical
implementation with providers, including – but not limited to - those identified through this
EIA (see Recommendation 1).
RECOMMENDATIONS FROM THE MOTT MACDONALD TRAVEL ANALYSIS
For completeness, we include here some recommendations from the Mott MacDonald travel
analysis:
● Existing transport schemes which could help patients unable to attend hospital
appointments by public transport due to a medical condition should be more widely
promoted, including ensuring that GPs and other referrers have the right information to
support patients
● More generally, clearer information should be provided about transport options,
including public transport and car travel
● Care co-ordinators could support patients in working out travel and access issues
● Hospital sites could consider having rooms set aside for overnight accommodation for
those who have long or difficult journeys, or who have difficulty getting home, for
example, due to adverse weather conditions
● Consideration could be given to staggering admissions to reflect the distance patients
are travelling to hospitals
● Patients should be made aware that they can ask for appointment times to suit their
commitments and travel needs
NLP Planned Orthopaedic Surgery for Adults - Health Inequalities and Equalities Impact Assessment
51
● Hospital trusts, local councils and transport providers could work together to ensure that
their local strategies are joined up and promote local accessibility
● Trusts should consider whether there are any actions they could take to improve transport
for patients, for example, at Chase Farm there is a charity run minibus to pick patients up
from existing bus stops and take them to the main entrance
● A continuous review of accessibility through a travel plan should be considered,
including understanding current travel arrangements via patient engagement and
understanding best practice in other Trusts and hospitals
Fuller versions of the recommendations, travel time analysis and methodology can be found in
the Mott MacDonald report.