Embed Size (px)
Citation preview
NIVOLUMAB IN
HODGKIN LYMPHOMA
Dra. Shirley Quintana Truyenque
Médico Oncólogo
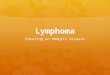
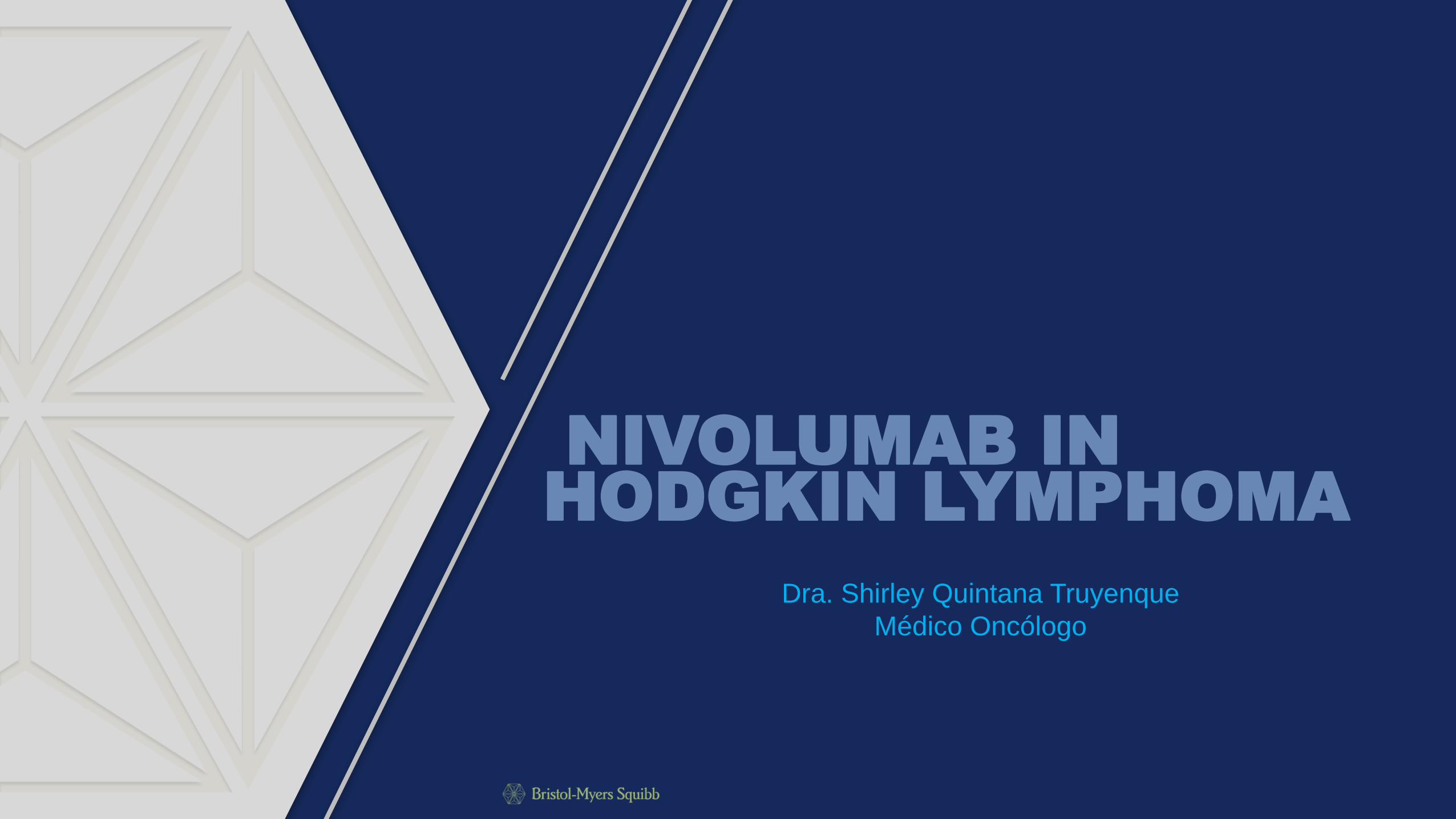
GLOBOCAN 2012: Hodgkin Lymphoma Incidence
and Mortality
ASR, age standardized ratio; EU, European Union; HL, Hodgkin lymphoma; US, United States. 1. King RL et al. Adv Anat Pathol. 2014;21:12-25. 2. GLOBOCAN 2012: http://globocan.iarc.fr/Pages/fact_sheets_population.aspx. Accessed October 12, 2016. 3. Townsend W et al. Lancet. 2012;380:836-847. 4. National Cancer Institute. http://seer.cancer.gov/statfacts/html/hodg.html. Accessed October 12, 2015. 5. Bosetti C et al. Ann Oncol. 2009;20:767-774.
• HL accounts for 12%–30% of all malignant lymphomas1
• Incidence has remained mostly unchanged during
the past 2 decades3
• HL incidence was stable in the US from 2002 to 20124
• HL mortality was stable in the US from 2002 to 20124
• HL mortality marginally declined in the EU from 1992 to 20025
0.0
0.5
1.0
1.5
2.0
2.5
3.0
Global EU US France Germany Japan
Estim
ate
d A
SR
s p
er
100,0
00
Incidence
HL Statistics2
Global EU US France Germany Japan
New cases (estimated, 2012) 65,950 12,431 8,601 1,757 2,017 1,061
Incidence* (estimated, 2012) 0.9 2.2 2.5 2.6 2.2 0.5
Deaths
(estimated, 2012) 25,469 2694 1,295 305 296 148
Mortality rate* (estimated, 2012) 0.3 0.3 0.3 0.3 0.2 0.1
* Estimated ASRs per 100,000. Both sexes, all ages.
Mortality rate
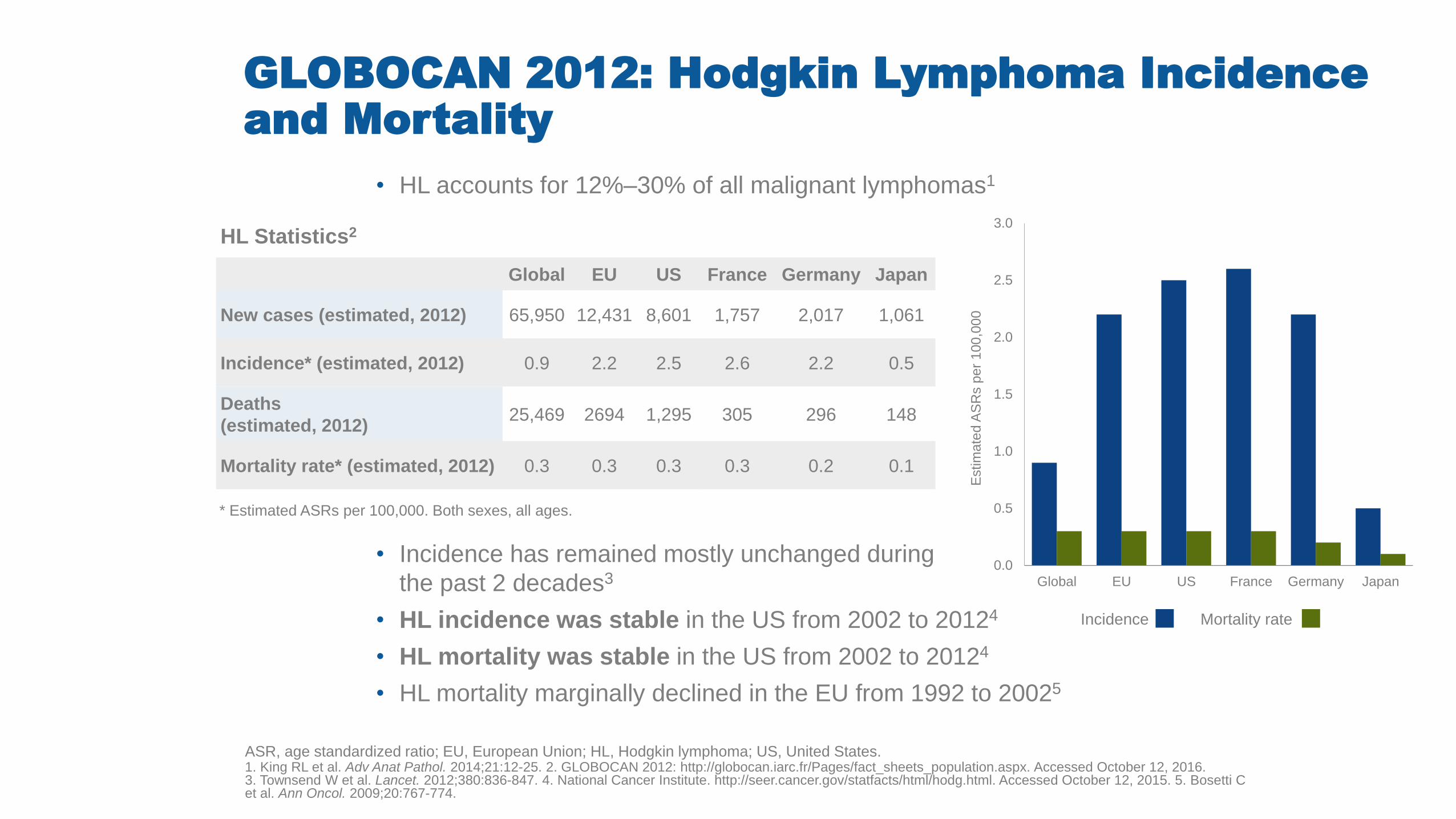
Hodgkin Lymphoma
BCL6, B-cell lymphoma 6 protein; CD, cluster of differentiation; cHL, classical Hodgkin lymphoma; HL, Hodgkin lymphoma; NLPHL, nodular lymphocyte-predominant Hodgkin lymphoma; PAX-5, paired box 5. 1. Eichenauer DA et al. Ann Oncol. 2011;22(suppl 6):vi55-vi58. 2. NCCN Guidelines®. HL. V3. 2016. 3. King RL et al. Adv Anat Pathol. 2014;21:12-25. 4. American Cancer Society. http://www.cancer.org/cancer/hodgkindisease/detailedguide/hodgkin-disease-what-is-hodgkin-disease. Accessed October 12, 2016. 5. Küppers R. Nat Rev Cancer. 2009;9:15-27. 6. Eberle FC et al. Cancer. 2009;15:129-137.
• HL is traditionally mai divided into 2 n categories1-3:
• HL tumors tend to contain a mixture of inflammatory cells5
• Patient prognosis differs among the cHL subtypes, with lymphocyte-depleted and
mixed cellularity subtypes having worse prognoses6
• CD20+, CD30-, CD45+, CD79a+,
BCL6+, PAX-5+; CD3-, CD15-
NLPHL is characterized by
lymphocyte-predominant cells
(popcorn cells), which are variants of Reed-
Sternberg cells4
• Nodular sclerosing: 60%–80%
• Mixed cellularity: 15%–30%
• Lymphocyte-rich: ~5%
• Lymphocyte-depleted: <1%
• CD20- (majority), CD30+, CD15+, PAX-5+
(weak); CD3-, CD45-, CD79a-
cHL is characterized by
Reed-Sternberg cells2
~95% cHL2-4 ~5% NLPHL1,2
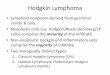
Inflammatory Microenvironment in Hodgkin
Lymphoma
APRIL, A proliferation-inducing ligand; BCMA, B-cell maturation antigen; CCL, CC chemokine ligand; CD, cluster of differentiation; HL, Hodgkin lymphoma; IL, interleukin; NGF, nerve growth factor; PD1, programmed cell death 1; PDL1, programmed death ligand 1; RS, Reed-Sternberg; TH, T helper cell; Treg, regulatory T cells; TARC, Thymus and Activation-Regulated Chemokine; TGF, transforming growth factor; TNF, tumor necrosis factor; TRKA, tyrosine kinase receptor type 1. 1. Küppers R. J Clin Invest. 2012;122:3439-3447. 2. Küppers R. Nat Rev Cancer. 2009;9:15-27.
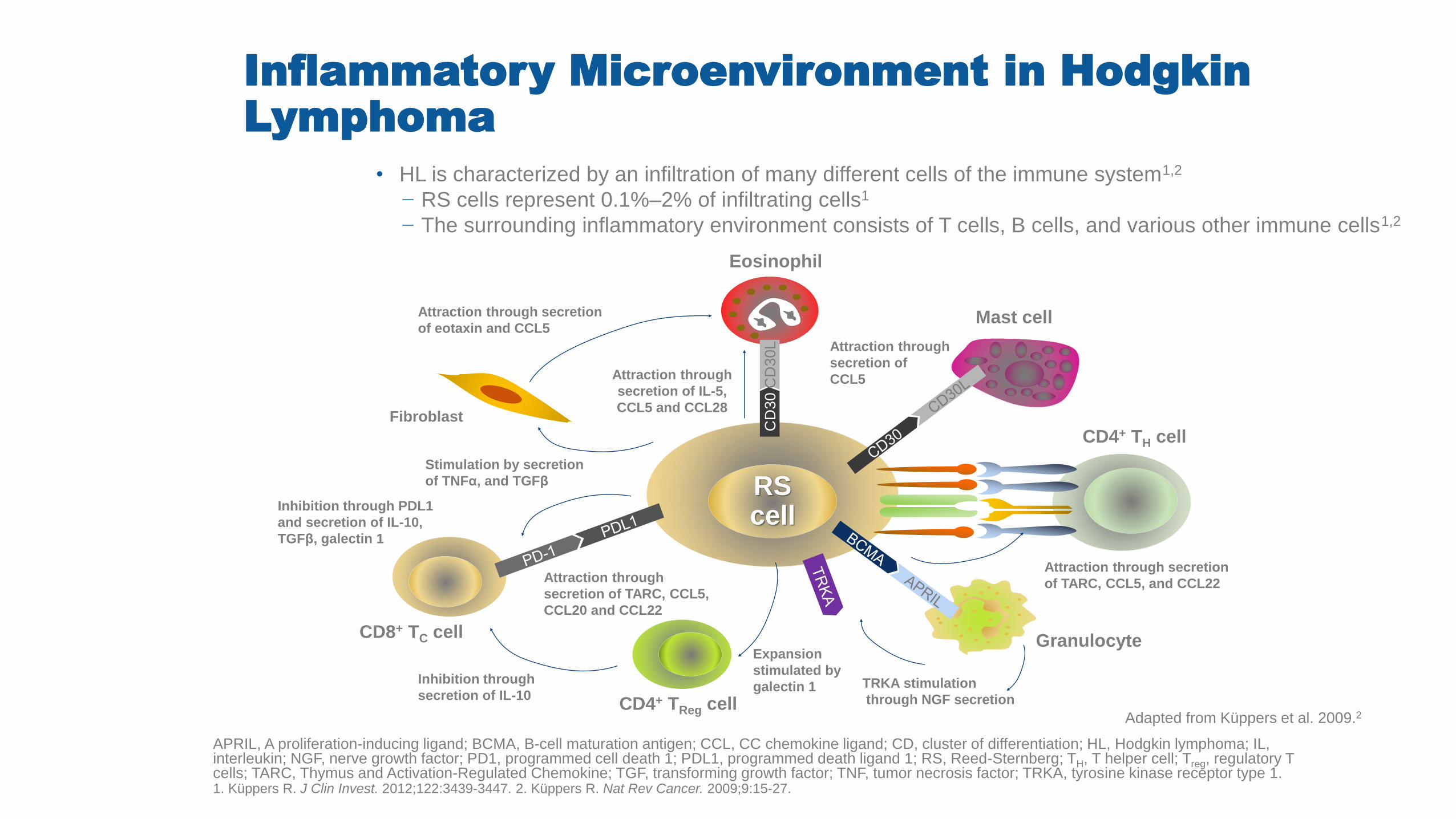
• HL is characterized by an infiltration of many different cells of the immune system1,2
− RS cells represent 0.1%–2% of infiltrating cells1
− The surrounding inflammatory environment consists of T cells, B cells, and various other immune cells1,2
Adapted from Küppers et al. 2009.2
RS cell
Mast cell
CD4+ TH cell
Eosinophil
Granulocyte
CD4+ TReg cell
CD8+ TC cell
Fibroblast
Attraction through secretion
of eotaxin and CCL5
Attraction through
secretion of IL-5,
CCL5 and CCL28
Stimulation by secretion
of TNFα, and TGFβ
Inhibition through PDL1
and secretion of IL-10,
TGFβ, galectin 1
Attraction through
secretion of TARC, CCL5,
CCL20 and CCL22
Inhibition through
secretion of IL-10
Expansion
stimulated by
galectin 1 TRKA stimulation
through NGF secretion
Attraction through secretion
of TARC, CCL5, and CCL22
CD
30
CD
30
L
Attraction through
secretion of
CCL5
Stage Distribution and Survival in Hodgkin
Lymphoma
HL, Hodgkin lymphoma. 1. National Cancer Institute. Hodgkin lymphoma. http://seer.cancer.gov/statfacts/html/hodg.html. Accessed October 11, 2016.
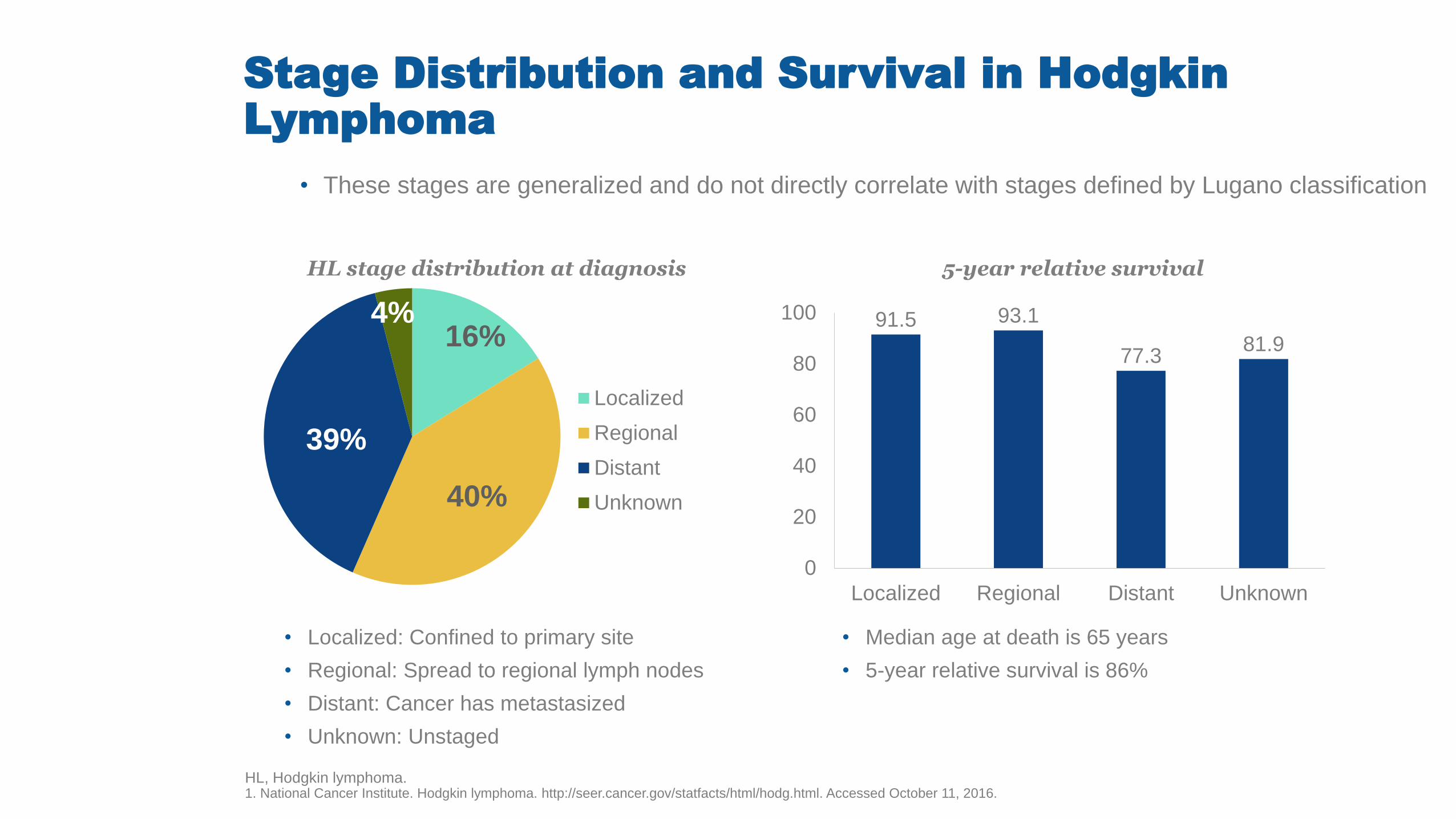
• These stages are generalized and do not directly correlate with stages defined by Lugano classification
• Localized: Confined to primary site
• Regional: Spread to regional lymph nodes
• Distant: Cancer has metastasized
• Unknown: Unstaged
• Median age at death is 65 years
• 5-year relative survival is 86%
HL stage distribution at diagnosis 5-year relative survival
16%
40%
39%
4%
Localized
Regional
Distant
Unknown
91.5 93.1
77.3 81.9
0
20
40
60
80
100
Localized Regional Distant Unknown
IPS and Prognosis in Advanced-Stage Hodgkin
Lymphoma
FFP, freedom from progression; HL, Hodgkin lymphoma; IPS, International Prognostic Score; OS, overall survival. 1. Hasenclever D et al. N Engl J Med. 1998;339:1506-1514. 2. Moccia AA et al. J Clin Oncol. 2012;30:3383-3388.
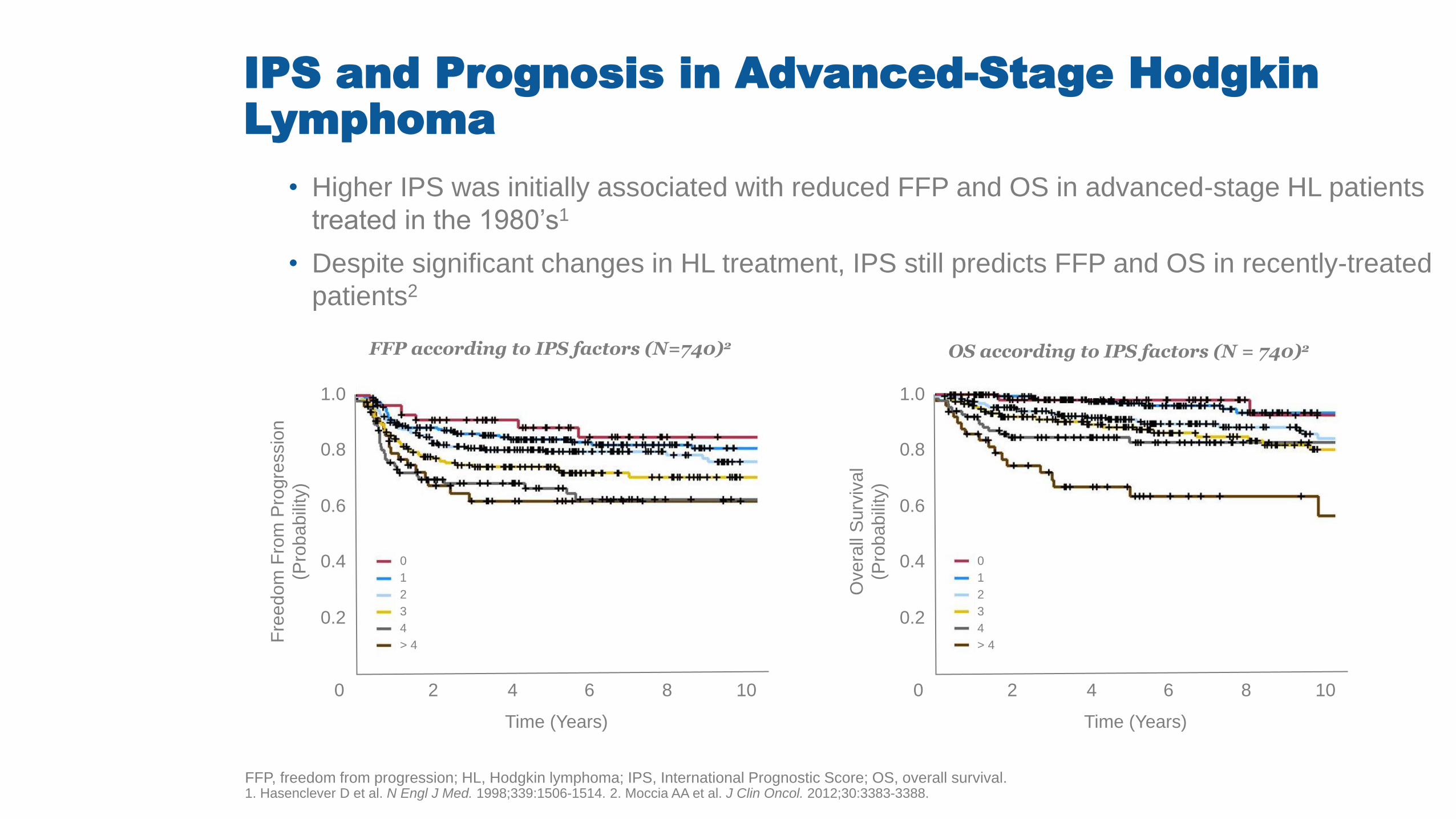
• Higher IPS was initially associated with reduced FFP and OS in advanced-stage HL patients
treated in the 1980’s1
• Despite significant changes in HL treatment, IPS still predicts FFP and OS in recently-treated
patients2
OS according to IPS factors (N = 740)2 FFP according to IPS factors (N=740)2
1.0
0.8
0.6
0.4
0.2
0 2 4 6 8 10
Time (Years)
Fre
edom
Fro
m P
rogre
ssio
n
(Pro
babili
ty)
0
1
2
3
4
> 4
1.0
0.8
0.6
0.4
0.2
0 2 4 6 8 10
Time (Years)
Overa
ll S
urv
ival
(Pro
babili
ty)
0
1
2
3
4
> 4
6
7
8
9
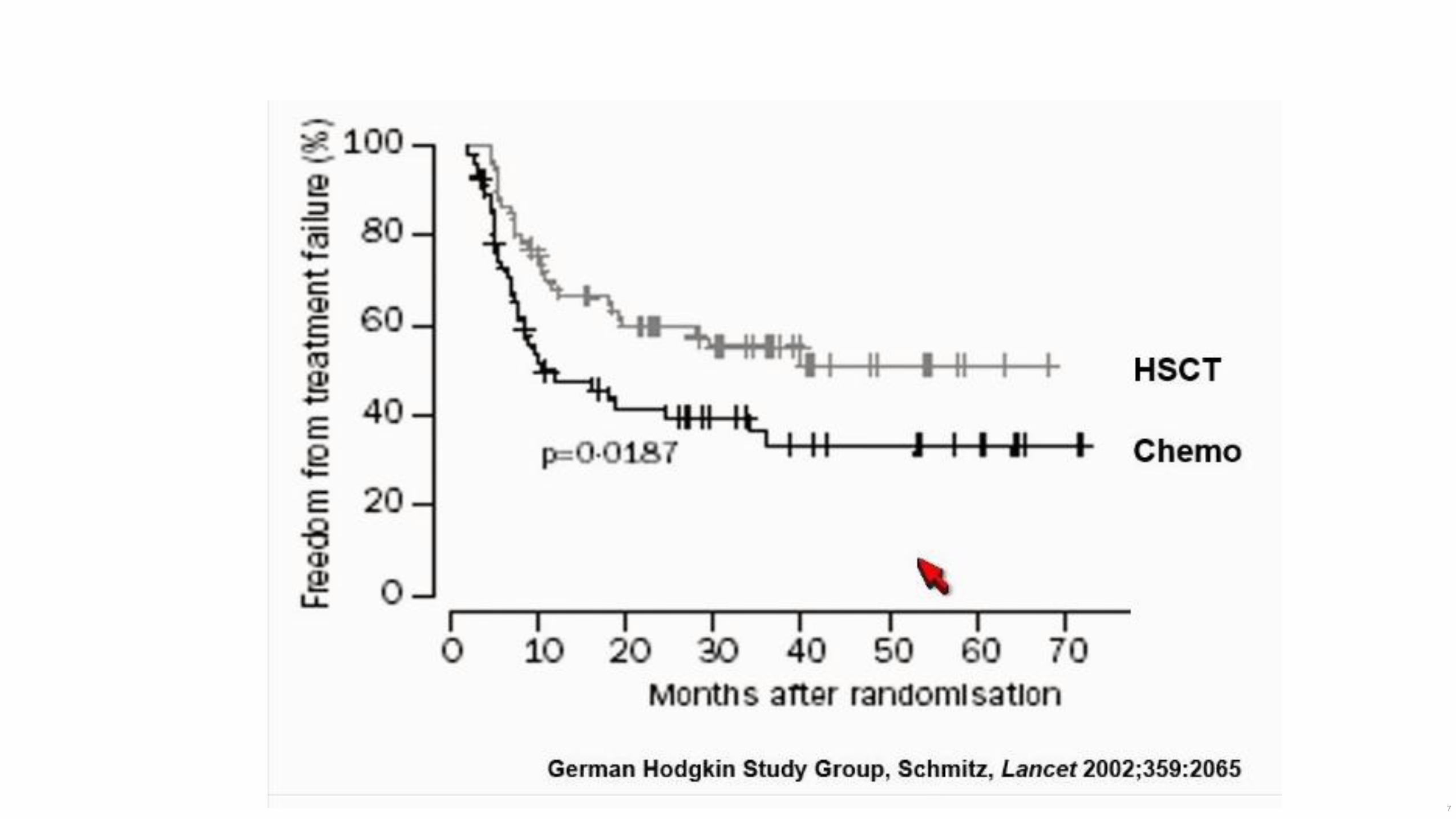
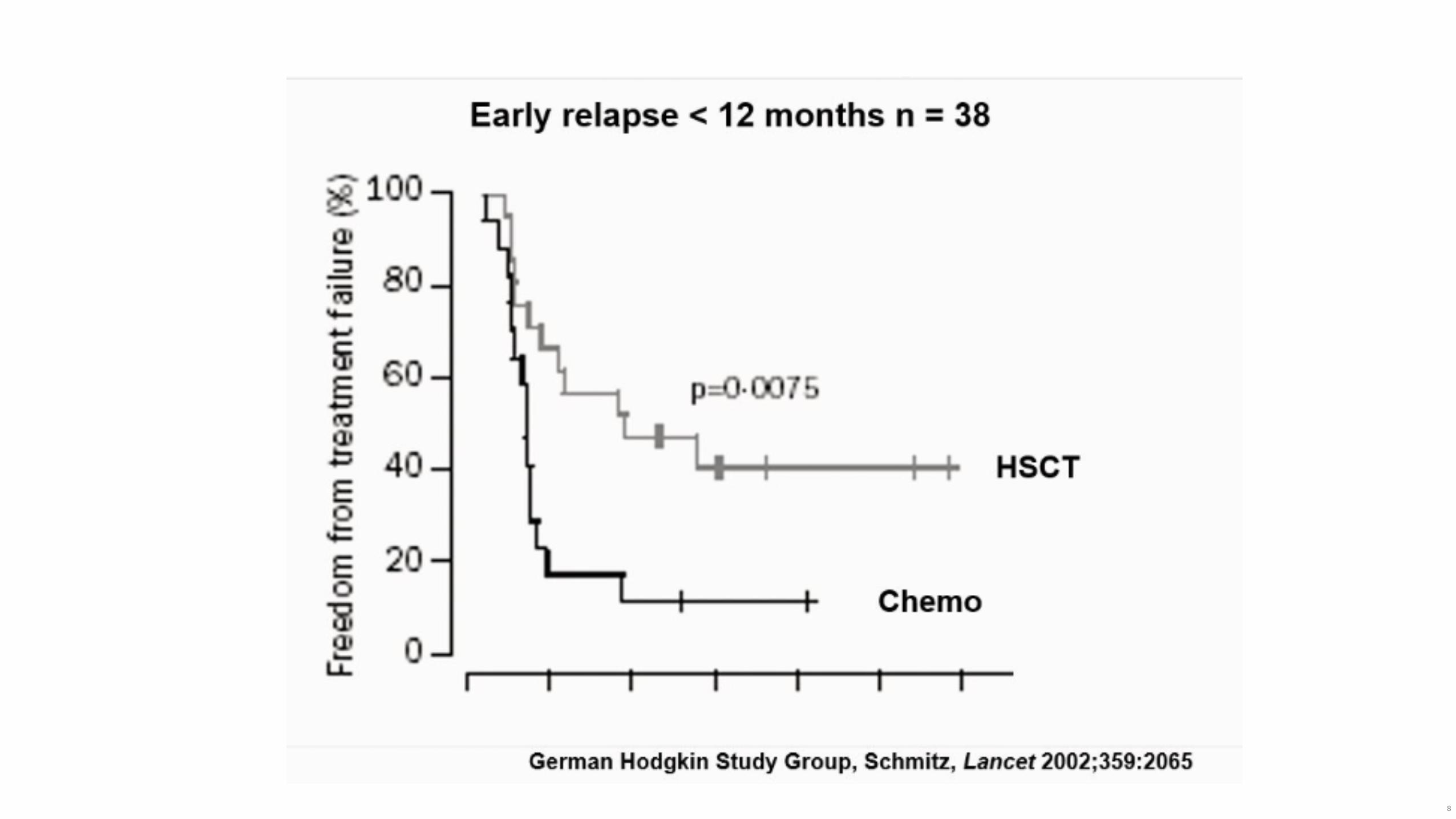
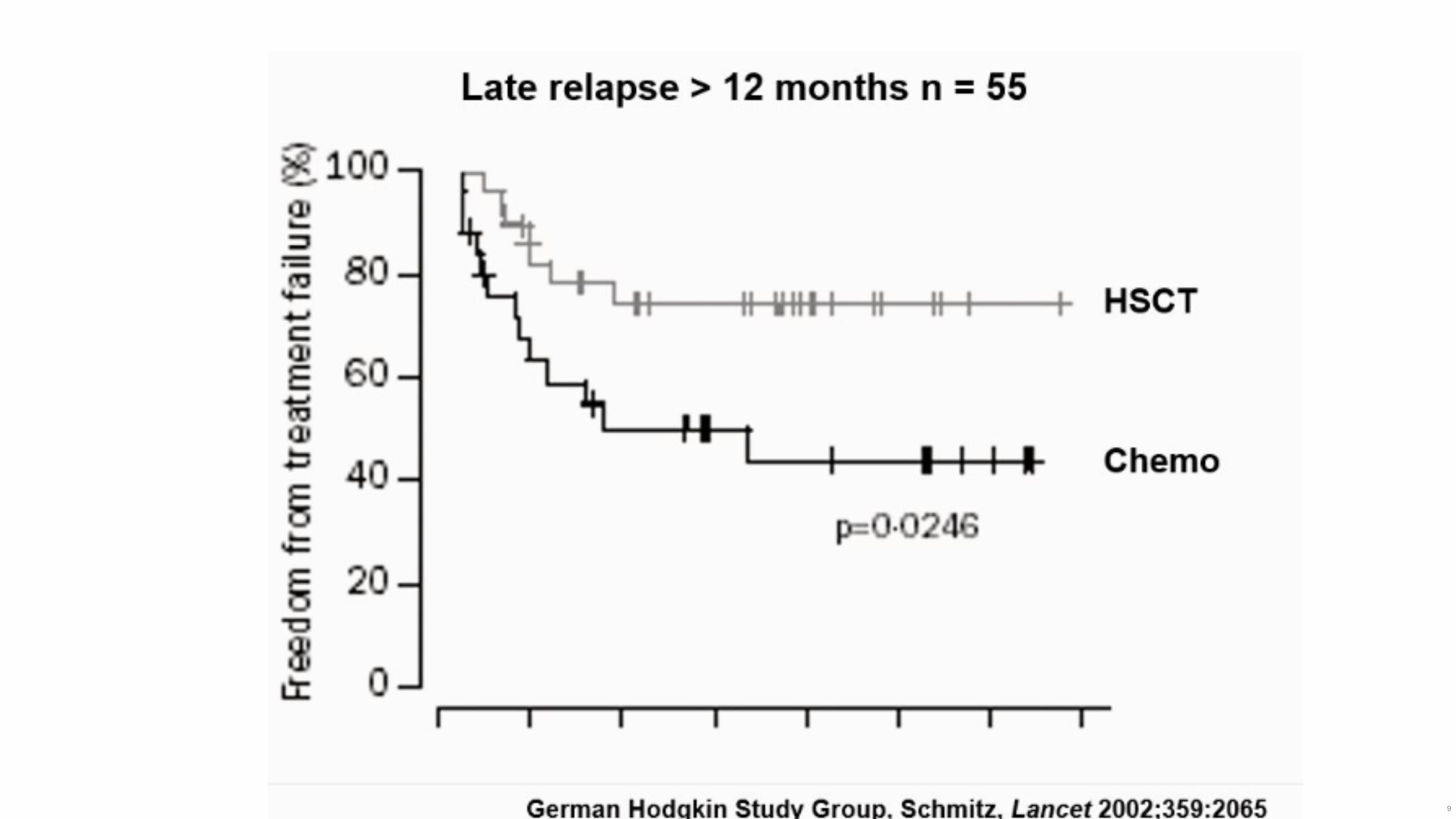
• LH: LHc,( 95%), NLPHL (5%)
• Alta respuesta a quimioterapia, mayoría están curados con actuales guías de
tratamiento
• SG a 5 años
• EC I – II : 90%
• EC III : 84 %
• EC IV :65%.
• 30% de los pacientes son refractarios/recaen a la primera línea de tratamiento. (Auto
TPH)
• Aproximadamente el 30% de los pacientes con Auto TPH recaen.
• Fuente: American Cancer Society Website
10
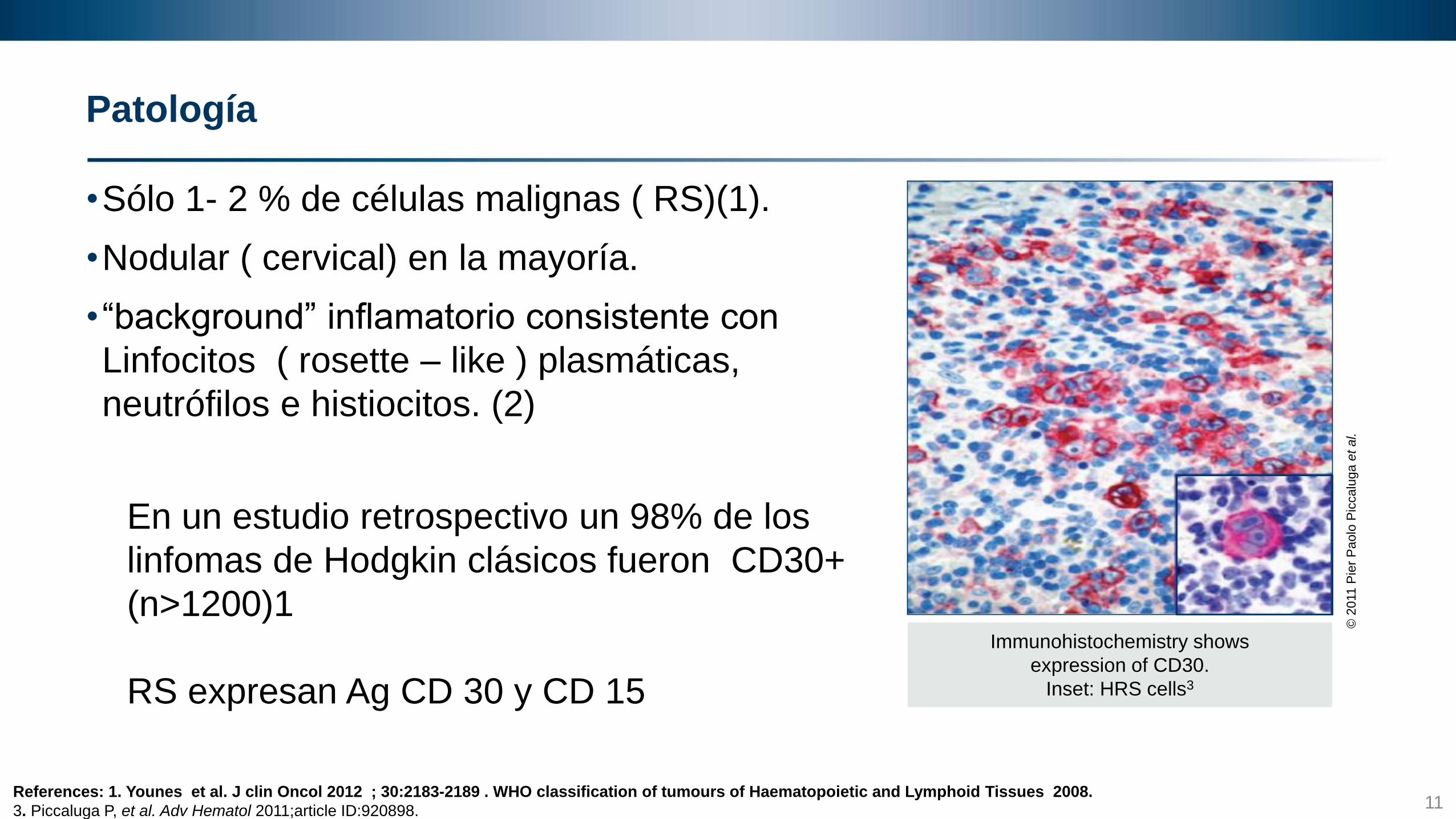
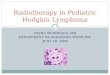
Patología
•Sólo 1- 2 % de células malignas ( RS)(1).
•Nodular ( cervical) en la mayoría.
•“background” inflamatorio consistente con
Linfocitos ( rosette – like ) plasmáticas,
neutrófilos e histiocitos. (2)
En un estudio retrospectivo un 98% de los
linfomas de Hodgkin clásicos fueron CD30+
(n>1200)1
RS expresan Ag CD 30 y CD 15
Immunohistochemistry shows
expression of CD30.
Inset: HRS cells3
© 2
011
Pie
r P
ao
lo P
icca
lug
a e
t a
l.
11 References: 1. Younes et al. J clin Oncol 2012 ; 30:2183-2189 . WHO classification of tumours of Haematopoietic and Lymphoid Tissues 2008.
3. Piccaluga P, et al. Adv Hematol 2011;article ID:920898.
12
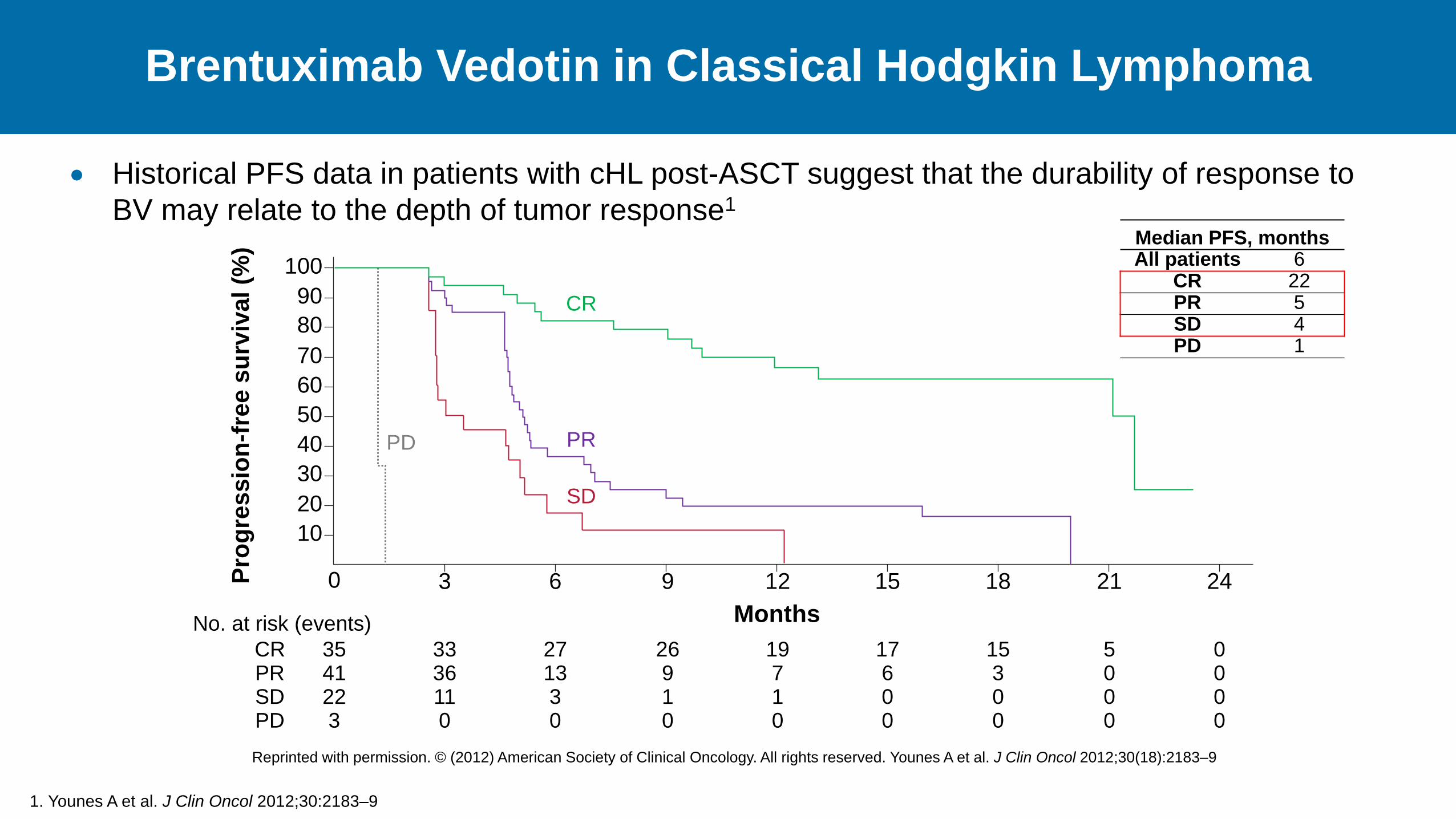
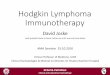
Brentuximab Vedotin in Classical Hodgkin Lymphoma
1. Younes A et al. J Clin Oncol 2012;30:2183–9
Historical PFS data in patients with cHL post-ASCT suggest that the durability of response to
BV may relate to the depth of tumor response1
Median PFS, months All patients 6
CR 22 PR 5 SD 4 PD 1
0 3 6 9 12 15 18 21 24
10
20
30
40
50
60
70
80
90
100 P
rog
ress
ion
-fre
e s
urv
ival (%
)
35 33 27 26 19 17 15 5 0 CR 41 36 13 9 7 6 3 0 0 PR 22 11 3 1 1 0 0 0 0 SD 3 0 0 0 0 0 0 0 0 PD
Months
CR
PR
SD
PD
No. at risk (events)
Reprinted with permission. © (2012) American Society of Clinical Oncology. All rights reserved. Younes A et al. J Clin Oncol 2012;30(18):2183–9
PD-1 CHECKPOINT
INHIBITORS:
MECHANISM OF
ACTION
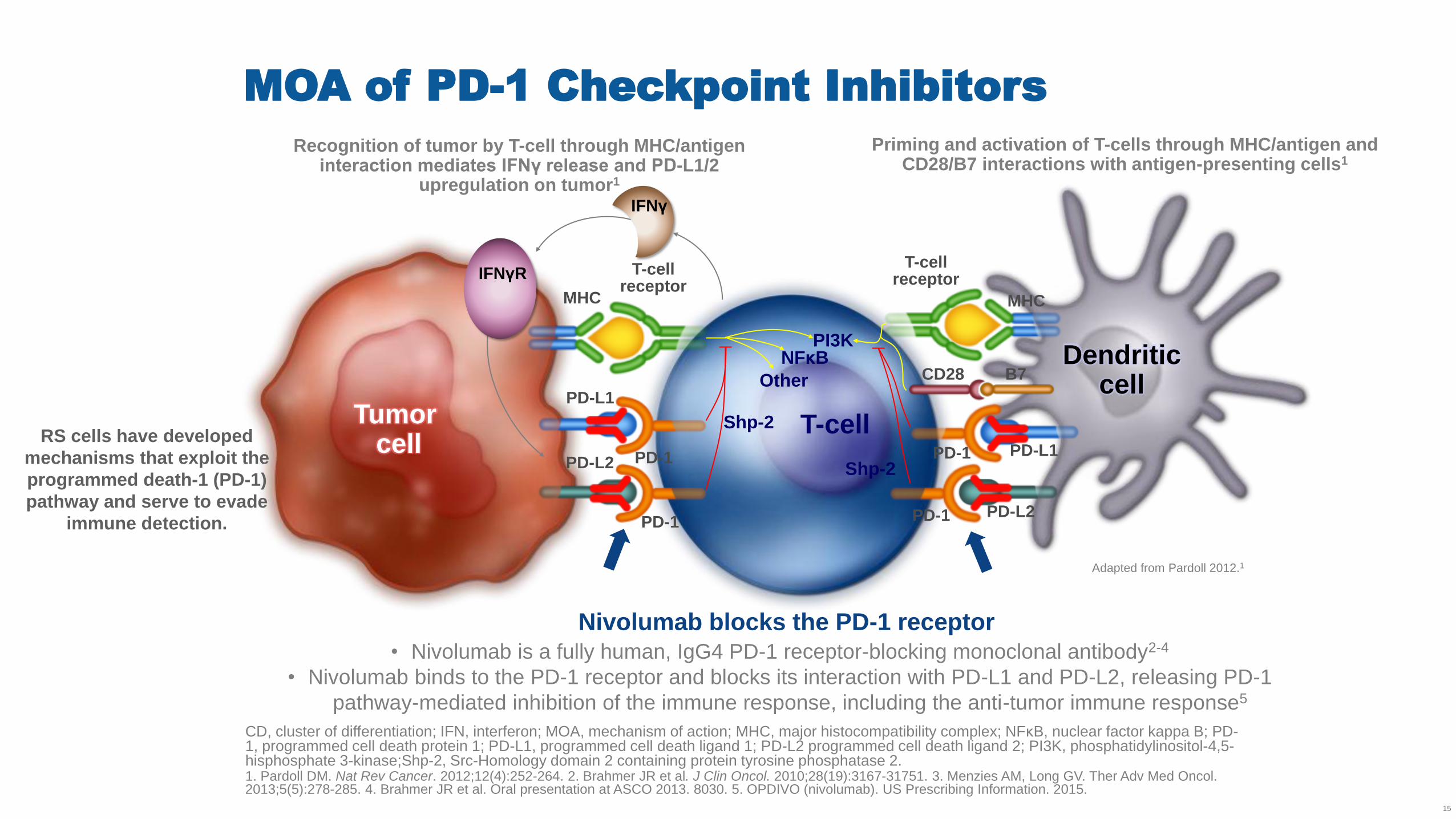
MOA of PD-1 Checkpoint Inhibitors
CD, cluster of differentiation; IFN, interferon; MOA, mechanism of action; MHC, major histocompatibility complex; NFκB, nuclear factor kappa B; PD-1, programmed cell death protein 1; PD-L1, programmed cell death ligand 1; PD-L2 programmed cell death ligand 2; PI3K, phosphatidylinositol-4,5-hisphosphate 3-kinase;Shp-2, Src-Homology domain 2 containing protein tyrosine phosphatase 2. 1. Pardoll DM. Nat Rev Cancer. 2012;12(4):252-264. 2. Brahmer JR et al. J Clin Oncol. 2010;28(19):3167-31751. 3. Menzies AM, Long GV. Ther Adv Med Oncol. 2013;5(5):278-285. 4. Brahmer JR et al. Oral presentation at ASCO 2013. 8030. 5. OPDIVO (nivolumab). US Prescribing Information. 2015.
15
Priming and activation of T-cells through MHC/antigen and CD28/B7 interactions with antigen-presenting cells1
Recognition of tumor by T-cell through MHC/antigen interaction mediates IFNγ release and PD-L1/2
upregulation on tumor1
Adapted from Pardoll 2012.1
• Nivolumab is a fully human, IgG4 PD-1 receptor-blocking monoclonal antibody2-4
• Nivolumab binds to the PD-1 receptor and blocks its interaction with PD-L1 and PD-L2, releasing PD-1
pathway-mediated inhibition of the immune response, including the anti-tumor immune response5
MHC
PD-L1
PD-1 PD-1
PD-1 PD-1
Nivolumab blocks the PD-1 receptor
T-cell receptor
T-cell receptor
PD-L1 PD-L2
PD-L2
MHC
CD28 B7
T-cell
NFκB
Other
PI3K Dendritic
cell Tumor
cell
IFNγ
IFNγR
Shp-2
Shp-2
RS cells have developed
mechanisms that exploit the
programmed death-1 (PD-1)
pathway and serve to evade
immune detection.
CheckMate 205 Update With Minimum 12-Month Follow-Up:
A Phase 2 Study of Nivolumab in Patients With
Relapsed/Refractory Classical Hodgkin Lymphoma
John Timmerman,1 Andreas Engert,2 Anas Younes,3 Armando Santoro,4 Philippe Armand,5
Michelle Fanale,6 Graham P. Collins,7 Voravit Ratanatharathorn,8 John Kuruvilla,9
Jonathon B. Cohen,10 Kerry J. Savage,11 Marek Trneny,12 Jan Paul de Boer,13 Margaret Shipp,14 Scott
Rodig,15 Pier Luigi Zinzani,16 Kazunobu Kato,17 Anne Sumbul,17 and Stephen Ansell,18 on behalf of
the CheckMate 205 Investigators
1University of California, Los Angeles, CA, USA; 2University Hospital of Cologne, Cologne, Germany; 3Memorial Sloan Kettering Cancer Center, New
York, NY, USA; 4Humanitas Cancer Center – Humanitas University, Rozzano–Milan, Italy; 5Dana-Farber Cancer Institute, Boston, MA, USA; 6University of Texas MD Anderson Cancer Center, Houston, TX, USA; 7Oxford Cancer and Haematology Centre, Churchill Hospital, Oxford, UK;
8Barbara Ann Karmanos Cancer Institute, Detroit, MI, USA; 9Princess Margaret Cancer Centre and University of Toronto, Toronto, Canada; 10Winship
Cancer Institute—Emory University, Atlanta, GA, USA; 11British Columbia Cancer Agency, Vancouver, Canada; 12Charles University in Prague and
General University in Prague, Prague, Czech Republic; 13LLPC-HOVON Netherlands Cancer Institute, Amsterdam, Netherlands; 14Dana Farber
Cancer Institute, Boston, MA, USA; 15Brigham and Women's Hospital, Boston, MA, USA; 16Institute of Hematology “Seràgnoli”, University of
Bologna, Bologna, Italy; 17Bristol-Myers Squibb, Princeton, NJ, USA; 18Mayo Clinic, Rochester, MN, USA
Presented at the 58th Annual Meeting and Exposition of the American Society of Hematology; San Diego, CA; December 5, 2016
1110
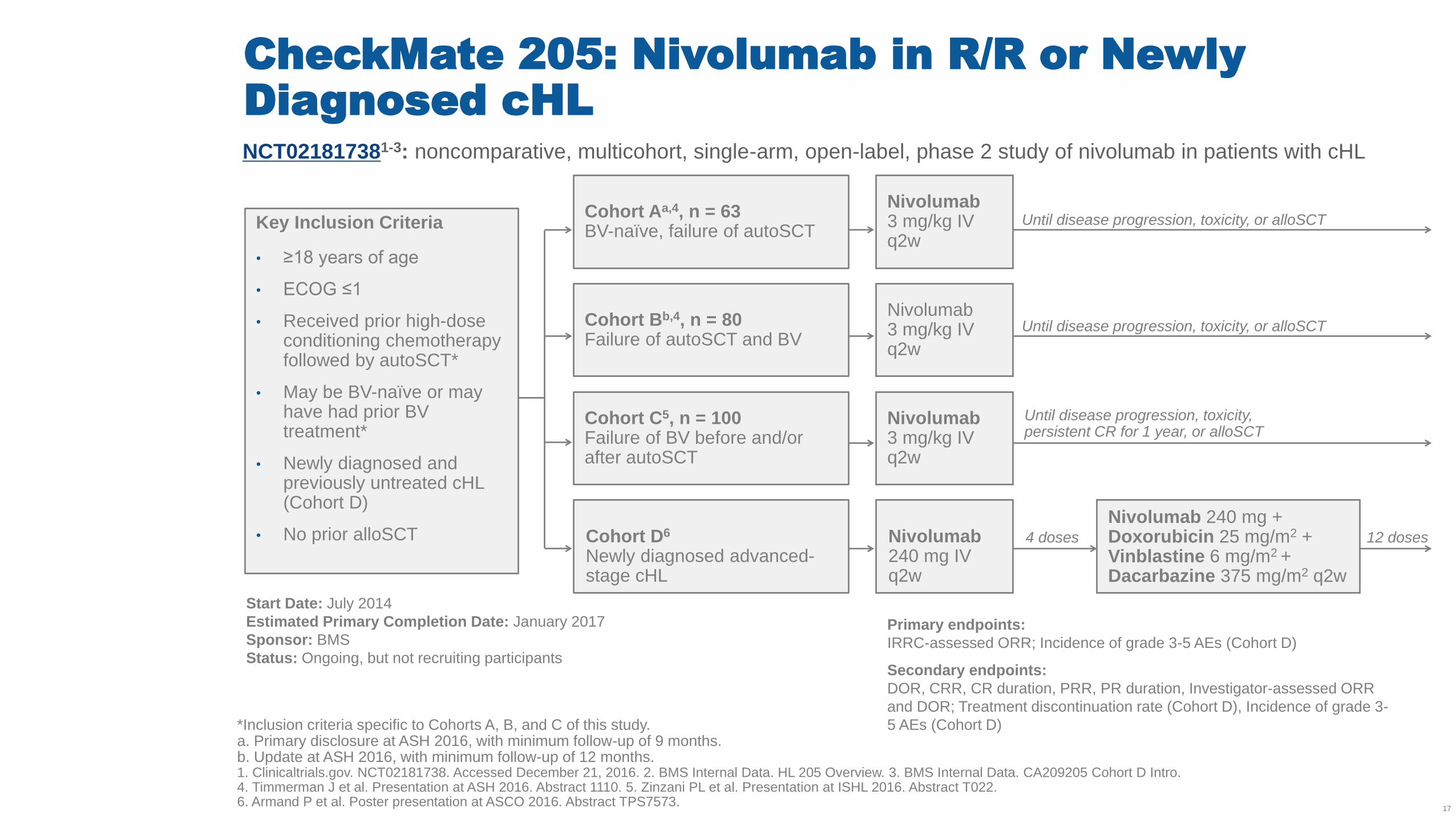
CheckMate 205: Nivolumab in R/R or Newly
Diagnosed cHL
*Inclusion criteria specific to Cohorts A, B, and C of this study. a. Primary disclosure at ASH 2016, with minimum follow-up of 9 months. b. Update at ASH 2016, with minimum follow-up of 12 months. 1. Clinicaltrials.gov. NCT02181738. Accessed December 21, 2016. 2. BMS Internal Data. HL 205 Overview. 3. BMS Internal Data. CA209205 Cohort D Intro. 4. Timmerman J et al. Presentation at ASH 2016. Abstract 1110. 5. Zinzani PL et al. Presentation at ISHL 2016. Abstract T022. 6. Armand P et al. Poster presentation at ASCO 2016. Abstract TPS7573.
17
NCT021817381-3: noncomparative, multicohort, single-arm, open-label, phase 2 study of nivolumab in patients with cHL
Key Inclusion Criteria
• ≥18 years of age
• ECOG ≤1
• Received prior high-dose conditioning chemotherapy followed by autoSCT*
• May be BV-naïve or may have had prior BV treatment*
• Newly diagnosed and previously untreated cHL (Cohort D)
• No prior alloSCT
Cohort Aa,4, n = 63 BV-naïve, failure of autoSCT
Cohort Bb,4, n = 80 Failure of autoSCT and BV
Cohort C5, n = 100 Failure of BV before and/or after autoSCT
Cohort D6 Newly diagnosed advanced-stage cHL
Nivolumab 3 mg/kg IV q2w
Nivolumab 3 mg/kg IV q2w
Nivolumab 3 mg/kg IV q2w
Primary endpoints:
IRRC-assessed ORR; Incidence of grade 3-5 AEs (Cohort D)
Secondary endpoints:
DOR, CRR, CR duration, PRR, PR duration, Investigator-assessed ORR
and DOR; Treatment discontinuation rate (Cohort D), Incidence of grade 3-
5 AEs (Cohort D)
Start Date: July 2014
Estimated Primary Completion Date: January 2017
Sponsor: BMS
Status: Ongoing, but not recruiting participants
Until disease progression, toxicity, or alloSCT
Until disease progression, toxicity, or alloSCT
Nivolumab 240 mg IV q2w
Nivolumab 240 mg + Doxorubicin 25 mg/m2 + Vinblastine 6 mg/m2 + Dacarbazine 375 mg/m2 q2w
12 doses 4 doses
Until disease progression, toxicity, persistent CR for 1 year, or alloSCT
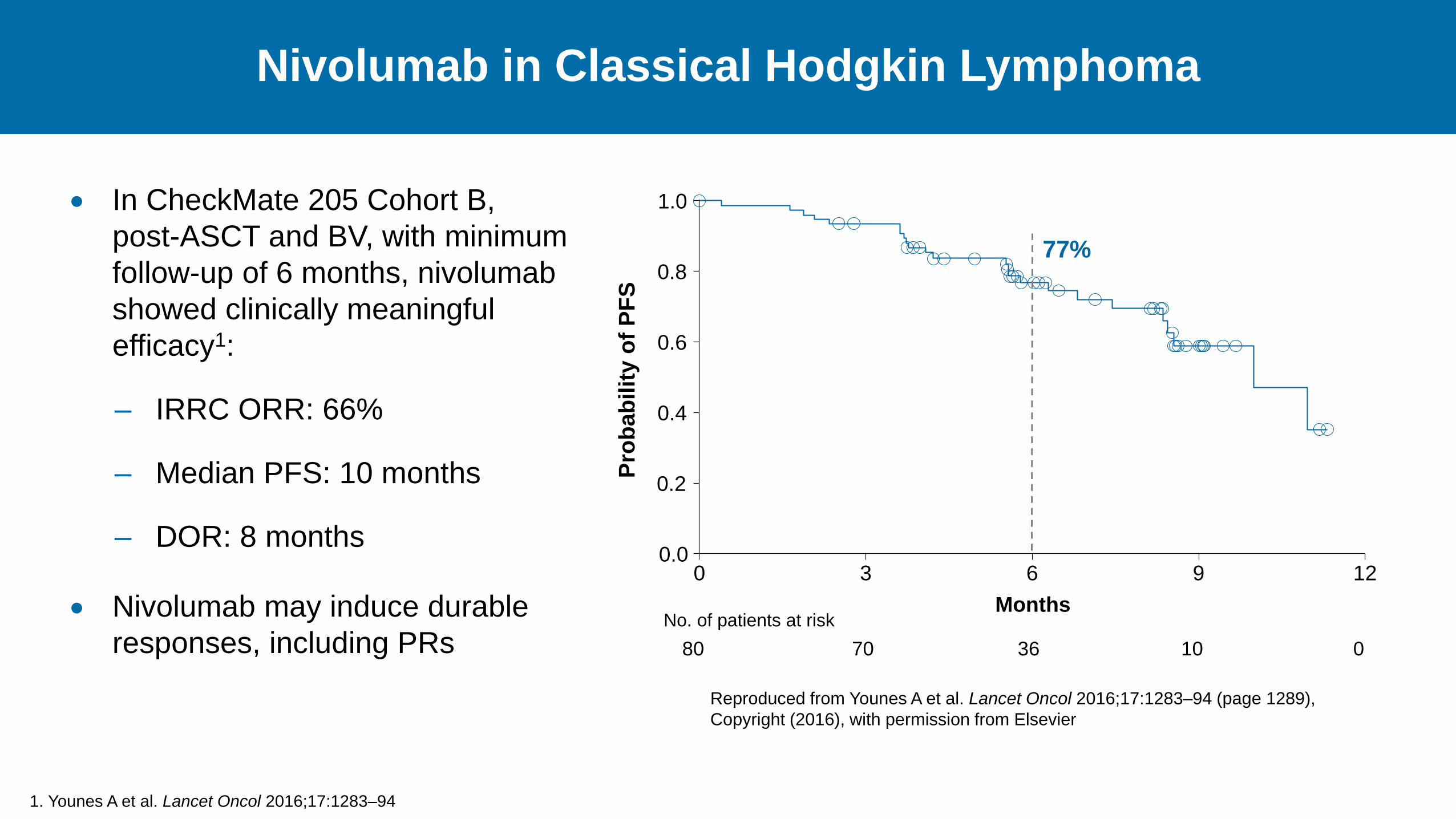
Nivolumab in Classical Hodgkin Lymphoma
1. Younes A et al. Lancet Oncol 2016;17:1283–94
In CheckMate 205 Cohort B,
post-ASCT and BV, with minimum
follow-up of 6 months, nivolumab
showed clinically meaningful
efficacy1:
– IRRC ORR: 66%
– Median PFS: 10 months
– DOR: 8 months
Nivolumab may induce durable
responses, including PRs
Months
1.0
0.8
0.6
0.4
0.2
0.0
Pro
bab
ilit
y o
f P
FS
0 3 6 9 12
77%
80 70 36 10 0
No. of patients at risk
Reproduced from Younes A et al. Lancet Oncol 2016;17:1283–94 (page 1289),
Copyright (2016), with permission from Elsevier
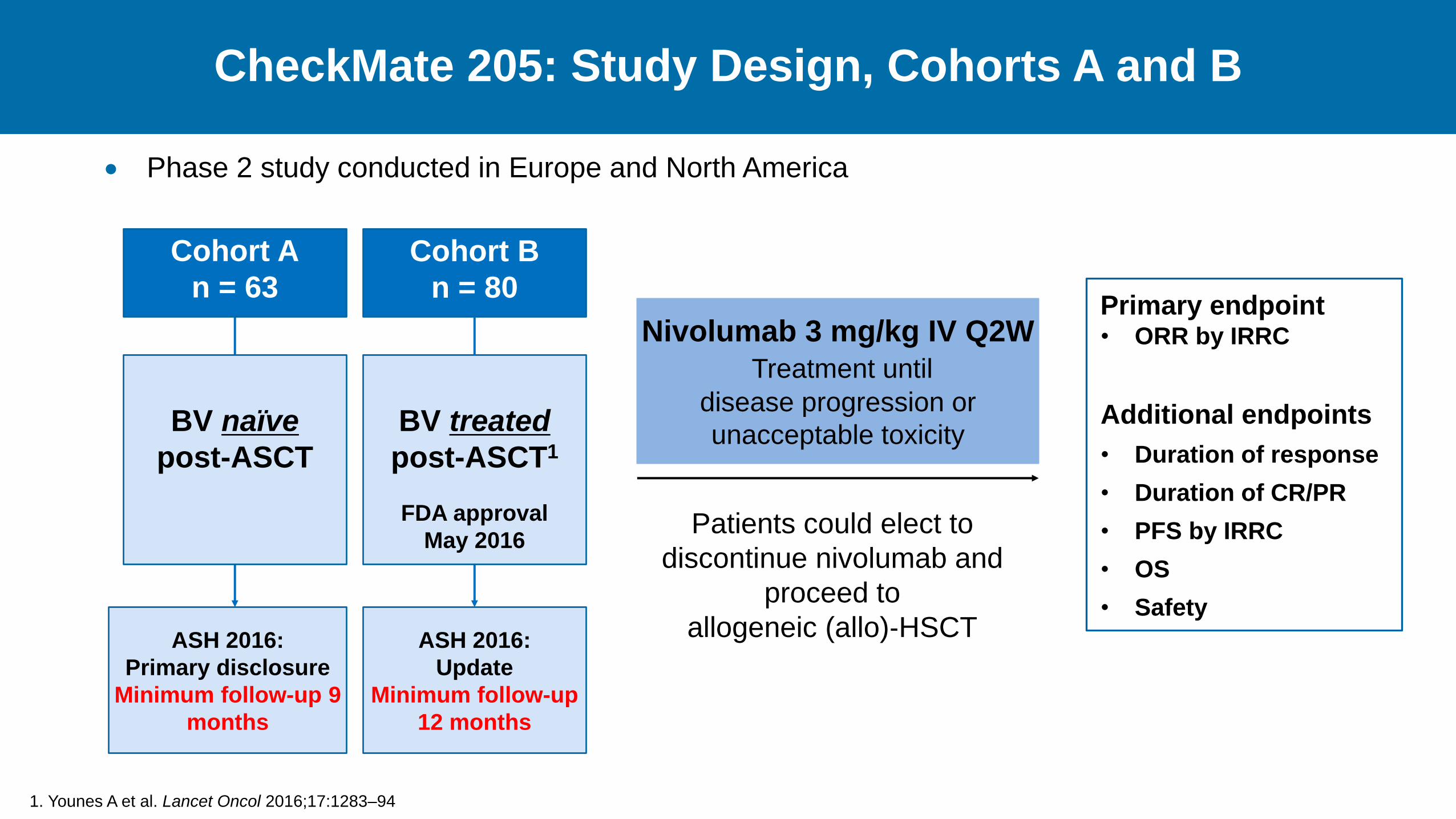
CheckMate 205: Study Design, Cohorts A and B
Primary endpoint • ORR by IRRC
Additional endpoints
• Duration of response
• Duration of CR/PR
• PFS by IRRC
• OS
• Safety
1. Younes A et al. Lancet Oncol 2016;17:1283–94
Nivolumab 3 mg/kg IV Q2W
Treatment until
disease progression or
unacceptable toxicity
Patients could elect to
discontinue nivolumab and
proceed to
allogeneic (allo)‐HSCT
Cohort B
n = 80
Cohort A
n = 63
BV naïve
post-ASCT
BV treated
post-ASCT1
FDA approval
May 2016
ASH 2016:
Primary disclosure
Minimum follow-up 9
months
ASH 2016:
Update
Minimum follow-up
12 months
Phase 2 study conducted in Europe and North America
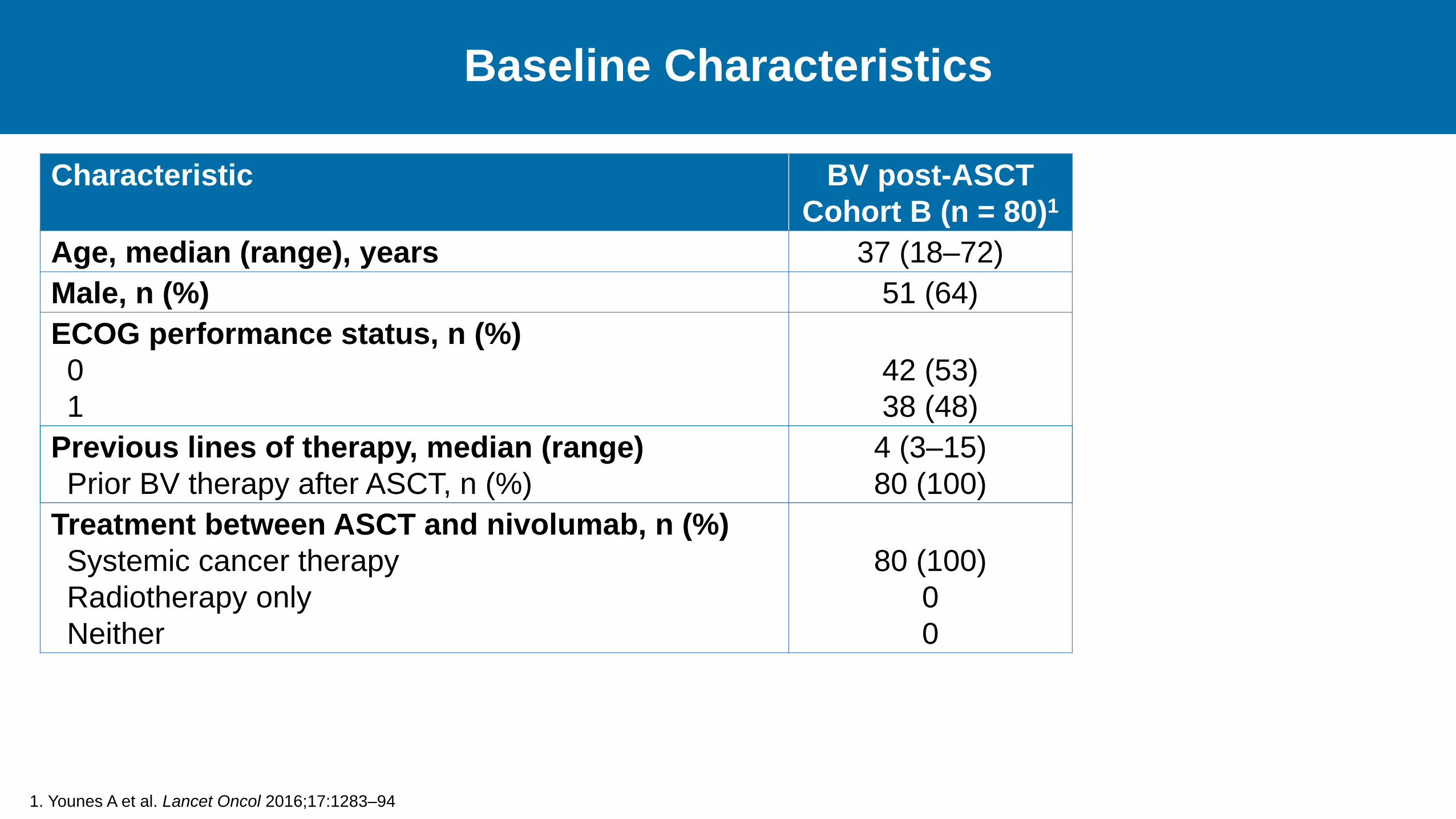
Baseline Characteristics
Characteristic BV post-ASCT
Cohort B (n = 80)1
Age, median (range), years 37 (18–72)
Male, n (%) 51 (64)
ECOG performance status, n (%)
0
1
42 (53)
38 (48)
Previous lines of therapy, median (range)
Prior BV therapy after ASCT, n (%)
4 (3–15)
80 (100)
Treatment between ASCT and nivolumab, n (%)
Systemic cancer therapy
Radiotherapy only
Neither
80 (100)
0
0
1. Younes A et al. Lancet Oncol 2016;17:1283–94
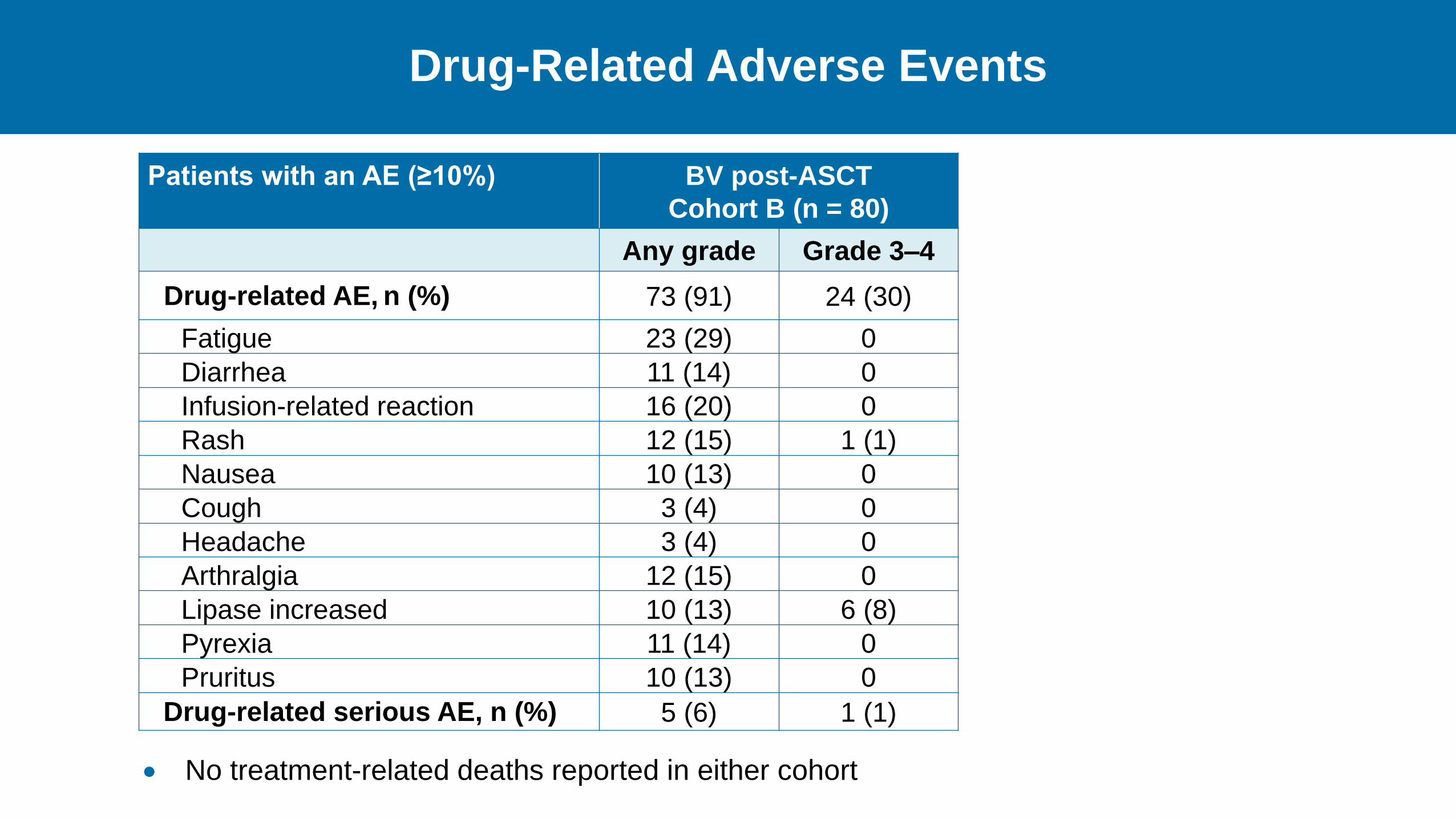
Drug-Related Adverse Events
Patients with an AE (≥10%) BV post-ASCT
Cohort B (n = 80)
Any grade Grade 3–4
Drug-related AE, n (%) 73 (91) 24 (30)
Fatigue 23 (29) 0
Diarrhea 11 (14) 0
Infusion-related reaction 16 (20) 0
Rash 12 (15) 1 (1)
Nausea 10 (13) 0
Cough 3 (4) 0
Headache 3 (4) 0
Arthralgia 12 (15) 0
Lipase increased 10 (13) 6 (8)
Pyrexia 11 (14) 0
Pruritus 10 (13) 0
Drug-related serious AE, n (%) 5 (6) 1 (1)
No treatment-related deaths reported in either cohort
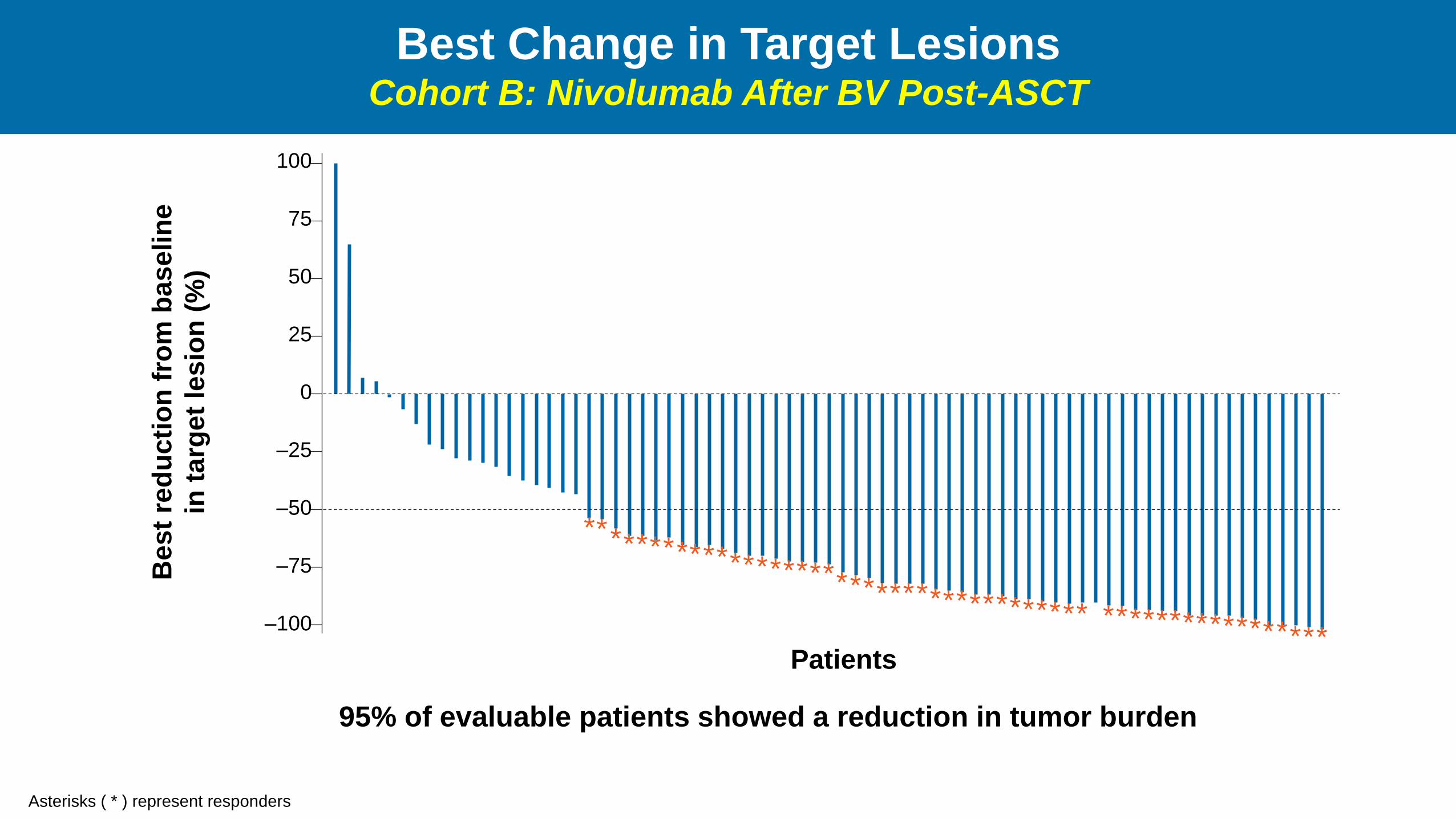
Best Change in Target Lesions Cohort B: Nivolumab After BV Post-ASCT
Asterisks ( * ) represent responders
95% of evaluable patients showed a reduction in tumor burden
Best
red
ucti
on
fro
m b
aselin
e
in t
arg
et
lesio
n (
%)
* * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * –100
–75
–50
–25
0
25
50
75
100
Patients
* * * * *
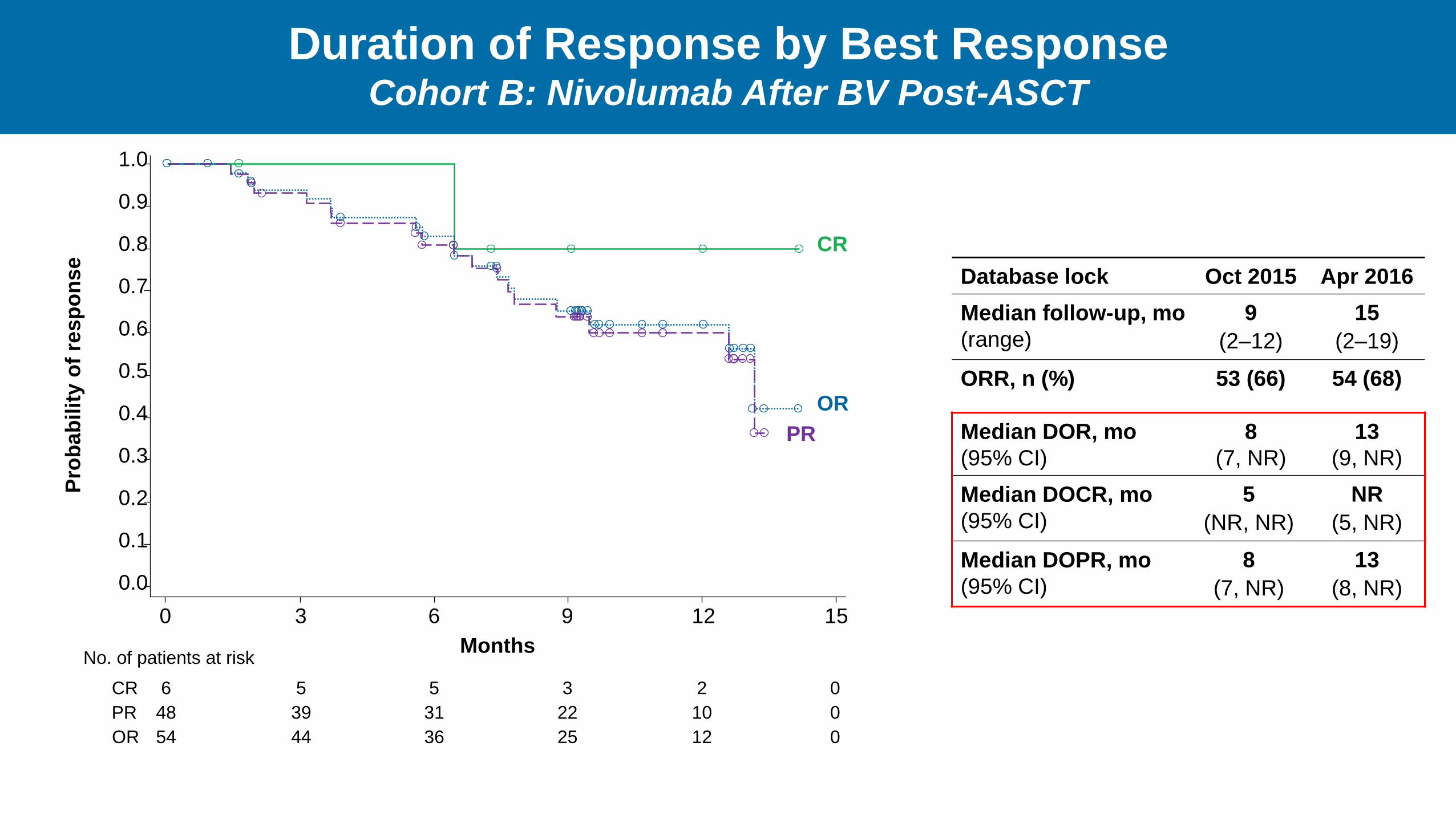
Duration of Response by Best Response Cohort B: Nivolumab After BV Post-ASCT
OR
CR
PR
0 3 6 9 12 15
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pro
bab
ilit
y o
f re
sp
on
se
Months
6 5 5 3 2 0
48 39 31 22 10 0
54 44 36 25 12 0
No. of patients at risk
CR
PR
OR
Database lock Oct 2015 Apr 2016
Median follow-up, mo
(range)
9
(2–12)
15
(2–19)
ORR, n (%) 53 (66) 54 (68)
Median DOR, mo
(95% CI)
8
(7, NR)
13
(9, NR)
Median DOCR, mo
(95% CI)
5
(NR, NR)
NR
(5, NR)
Median DOPR, mo
(95% CI)
8
(7, NR)
13
(8, NR)
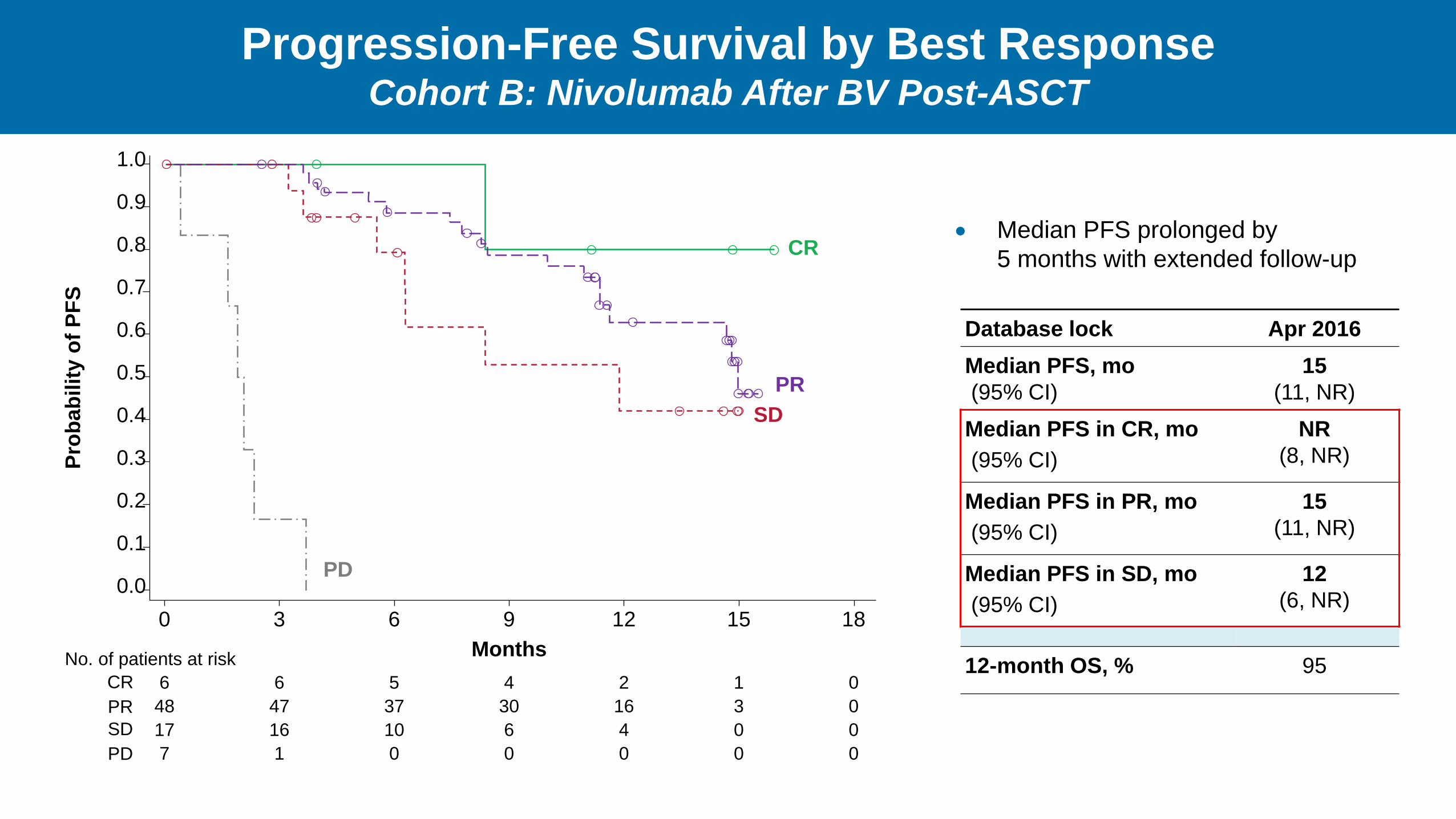
Progression-Free Survival by Best Response Cohort B: Nivolumab After BV Post-ASCT
CR
PR
SD
PD
18 0 3 6 9 12 15
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pro
bab
ilit
y o
f P
FS
Months
0 6 6 5 4 2 1
0 48 47 37 30 16 3
0 17 16 10 6 4 0
0 7 1 0 0 0 0
No. of patients at risk
CR
PR
SD
PD
Database lock Apr 2016
Median PFS, mo
(95% CI)
15
(11, NR)
Median PFS in CR, mo
(95% CI)
NR
(8, NR)
Median PFS in PR, mo
(95% CI)
15
(11, NR)
Median PFS in SD, mo
(95% CI)
12
(6, NR)
12-month OS, % 95
Median PFS prolonged by
5 months with extended follow-up
0
10
20
30
40
50
60
70
80
90
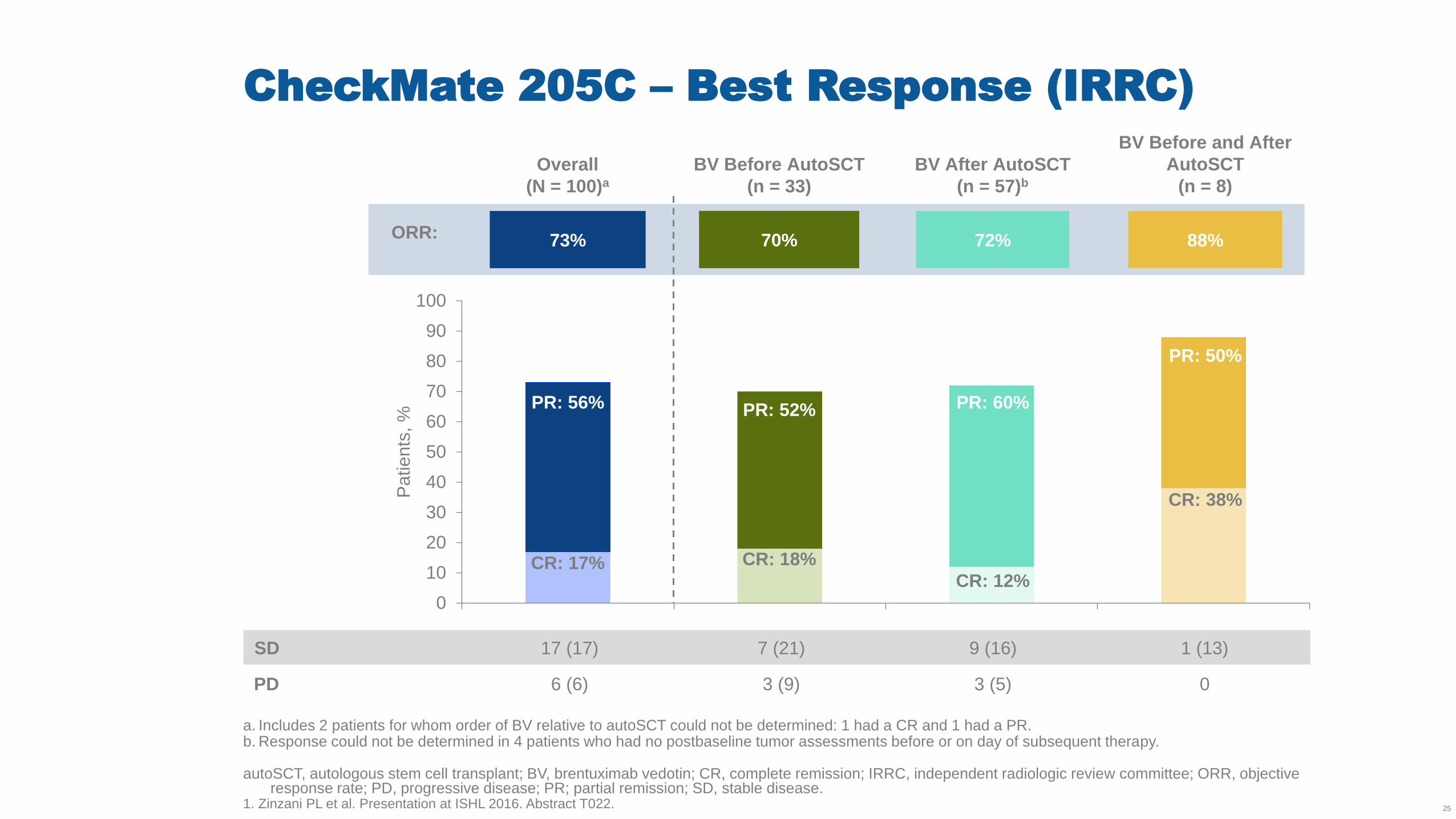
100
Patients
, %
73% 70% 72% 88%
CR: 17%
PR: 56%
CR: 18%
PR: 52%
CR: 12%
PR: 60%
PR: 50%
CR: 38%
BV Before and After
AutoSCT
(n = 8)
Overall
(N = 100)a
BV Before AutoSCT
(n = 33)
BV After AutoSCT
(n = 57)b
CheckMate 205C – Best Response (IRRC)
a. Includes 2 patients for whom order of BV relative to autoSCT could not be determined: 1 had a CR and 1 had a PR. b. Response could not be determined in 4 patients who had no postbaseline tumor assessments before or on day of subsequent therapy. autoSCT, autologous stem cell transplant; BV, brentuximab vedotin; CR, complete remission; IRRC, independent radiologic review committee; ORR, objective
response rate; PD, progressive disease; PR; partial remission; SD, stable disease. 1. Zinzani PL et al. Presentation at ISHL 2016. Abstract T022. 25
SD 17 (17) 7 (21) 9 (16) 1 (13)
PD 6 (6) 3 (9) 3 (5) 0
ORR:
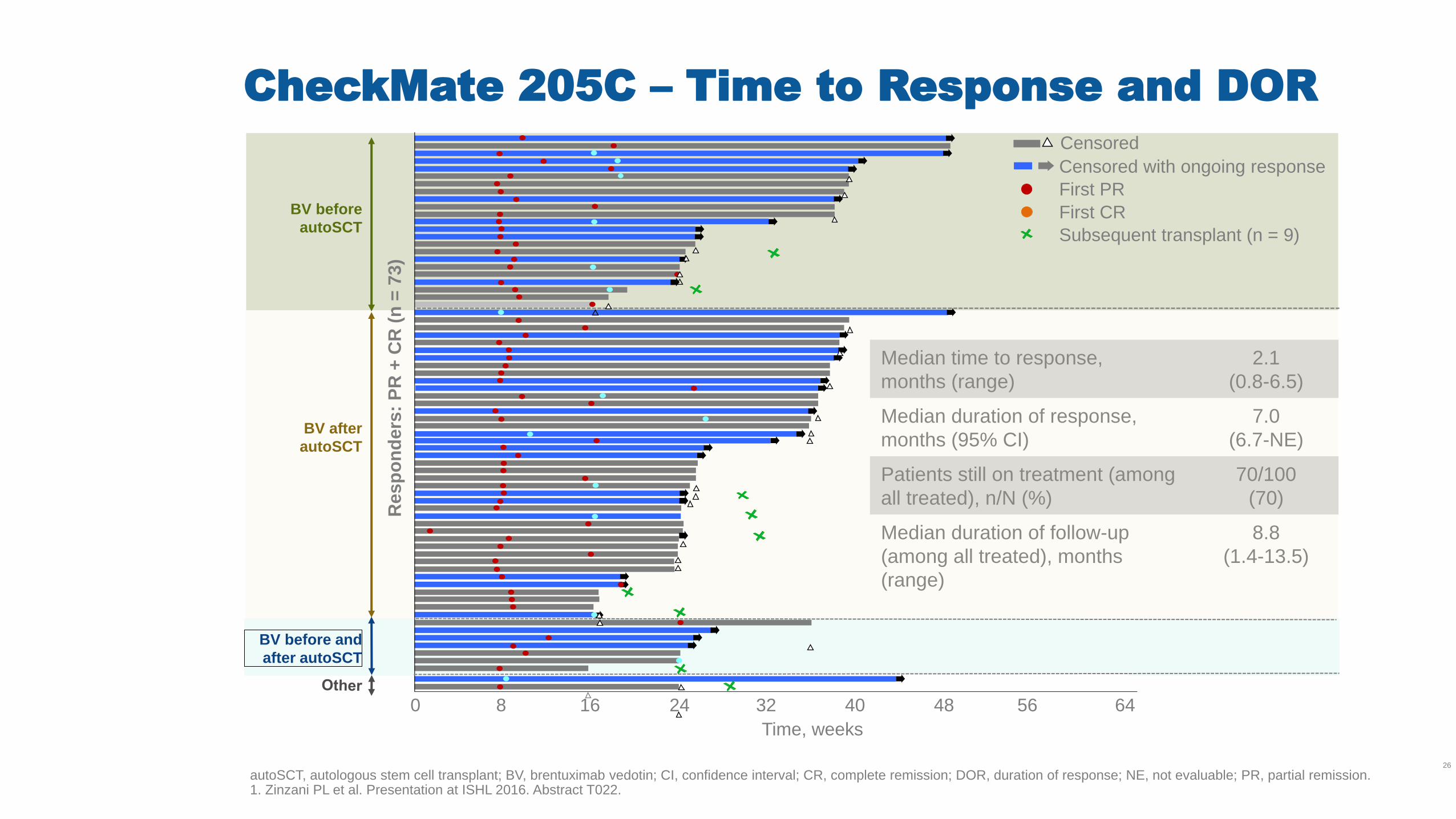
CheckMate 205C – Time to Response and DOR
autoSCT, autologous stem cell transplant; BV, brentuximab vedotin; CI, confidence interval; CR, complete remission; DOR, duration of response; NE, not evaluable; PR, partial remission. 1. Zinzani PL et al. Presentation at ISHL 2016. Abstract T022.
26
Median time to response,
months (range)
2.1
(0.8-6.5)
Median duration of response,
months (95% CI)
7.0
(6.7-NE)
Patients still on treatment (among
all treated), n/N (%)
70/100
(70)
Median duration of follow-up
(among all treated), months
(range)
8.8
(1.4-13.5)
BV before and
after autoSCT
Time, weeks
BV after
autoSCT
0 64 56 48 40 32 24 16 8
Resp
on
ders
: P
R +
CR
(n
= 7
3)
BV before
autoSCT
Censored with ongoing response
First PR
First CR
Subsequent transplant (n = 9)
Censored
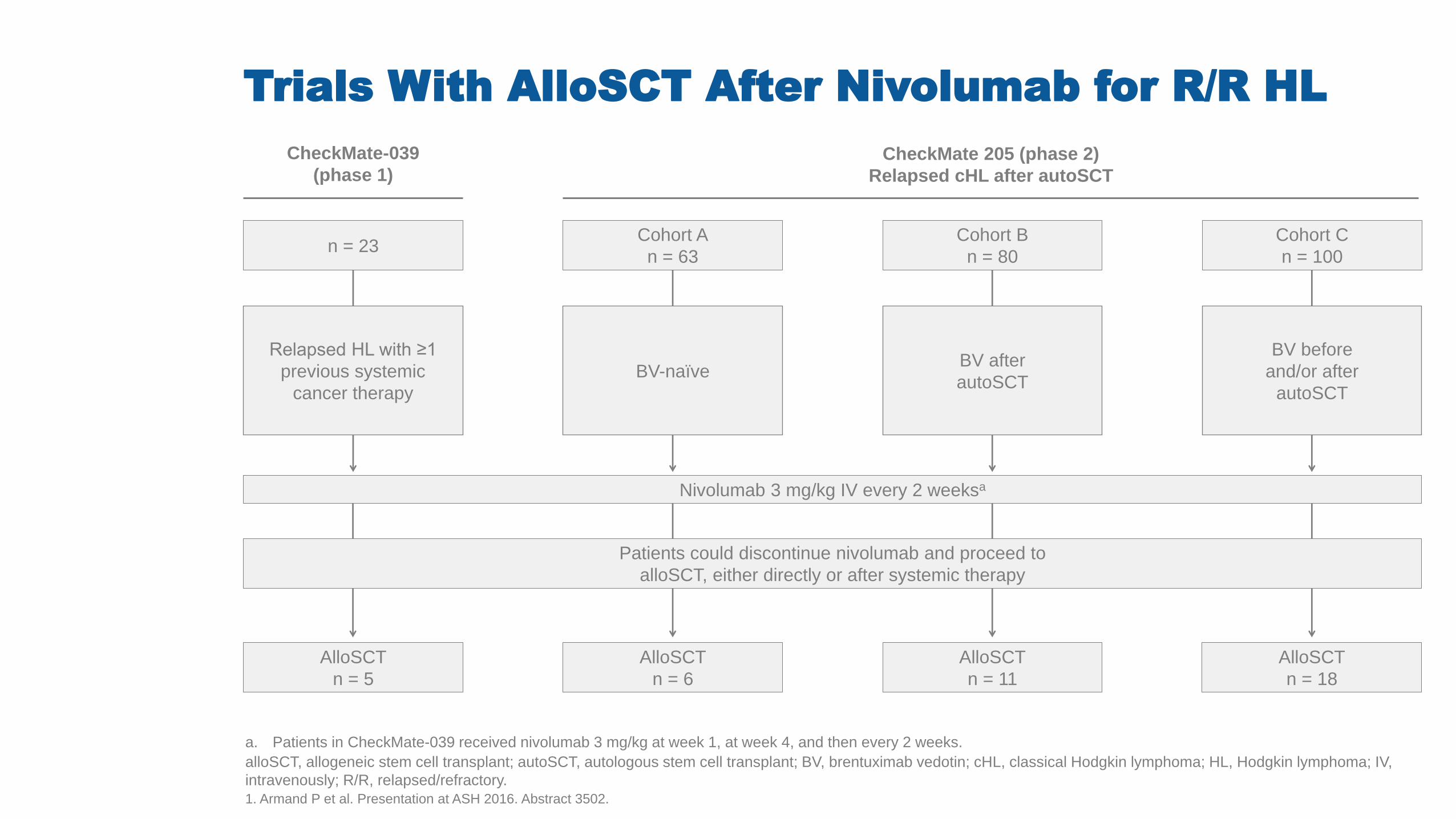
Trials With AlloSCT After Nivolumab for R/R HL
a. Patients in CheckMate-039 received nivolumab 3 mg/kg at week 1, at week 4, and then every 2 weeks.
alloSCT, allogeneic stem cell transplant; autoSCT, autologous stem cell transplant; BV, brentuximab vedotin; cHL, classical Hodgkin lymphoma; HL, Hodgkin lymphoma; IV,
intravenously; R/R, relapsed/refractory.
1. Armand P et al. Presentation at ASH 2016. Abstract 3502.
CheckMate-039
(phase 1)
Nivolumab 3 mg/kg IV every 2 weeksa
Patients could discontinue nivolumab and proceed to
alloSCT, either directly or after systemic therapy
AlloSCT
n = 5
CheckMate 205 (phase 2)
Relapsed cHL after autoSCT
Cohort A
n = 63
Cohort B
n = 80
Cohort C
n = 100
AlloSCT
n = 6
AlloSCT
n = 11
AlloSCT
n = 18
BV-naïve
BV before
and/or after
autoSCT
BV after
autoSCT
n = 23
Relapsed HL with ≥1
previous systemic
cancer therapy
Conclusion
En pacientes no tratados previamente con BV y tratados con BV,
Nivolumab demostró:
• Alta ORR (68%)
• Respuestas duraderas y PFS independientemente de la
profundidad de la respuesta, incluso en pacientes con PR o SD
• Un perfil de seguridad aceptable.
Nivolumab ofrece una opción de tratamiento favorable para los
pacientes con linfoma de Hodgkin que progresa después de ASCT
LOCAL APPROVAL MAY
BE REQUIRED BEFORE
EXTERNAL USE. REFER
TO LOCAL GUIDELINES.
Table of Contents
PD-1 Checkpoint
Inhib i tors : MOA
Pseudo-Progression as
Response to Immuno-
Oncology Therapies
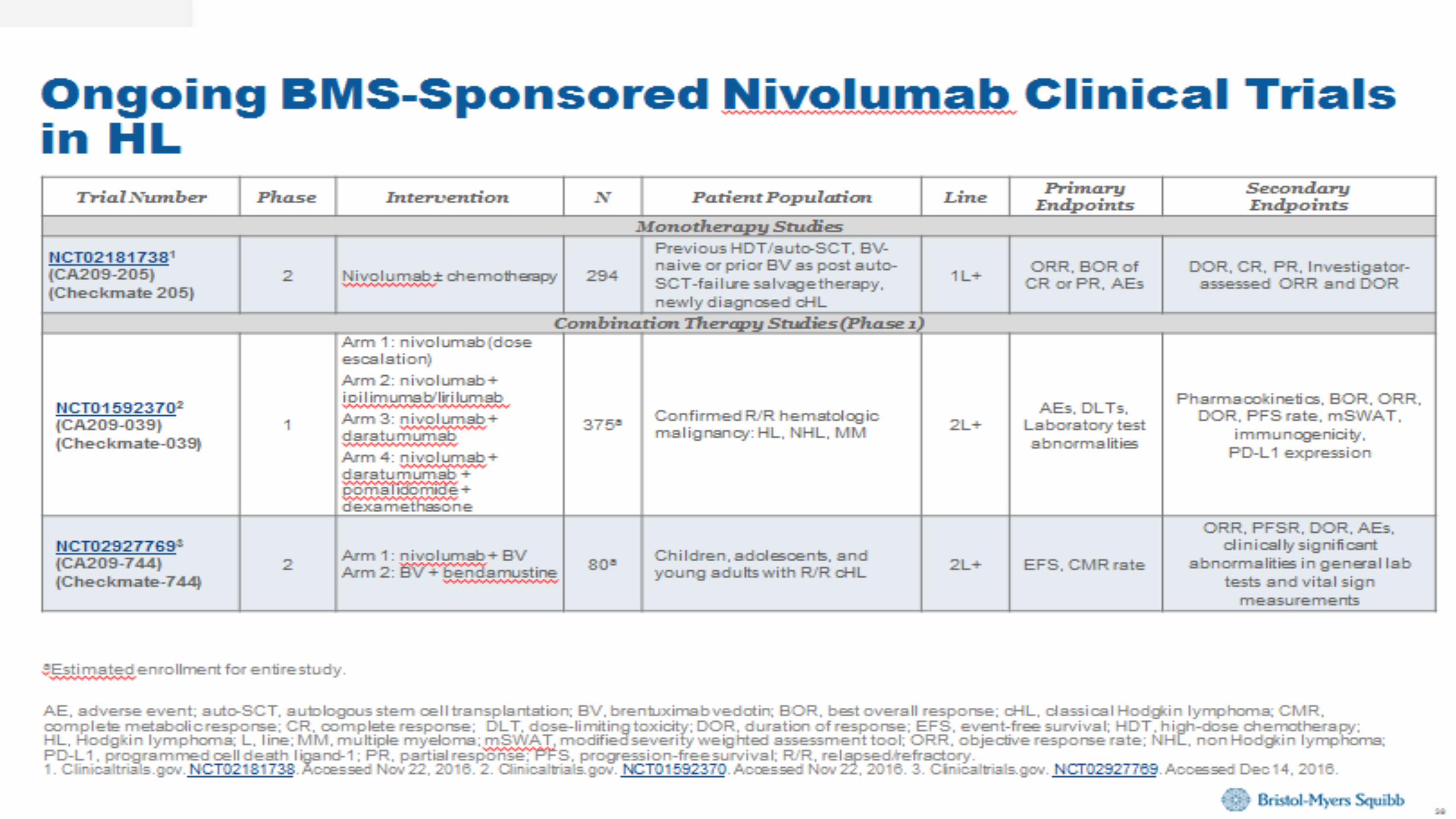
Nivolumab: Ongoing
BMS-Sponsored Clinical
Trials
CTLA-4 Checkpoint
Inhib i tors : MOA
Nivolumab: ISRs
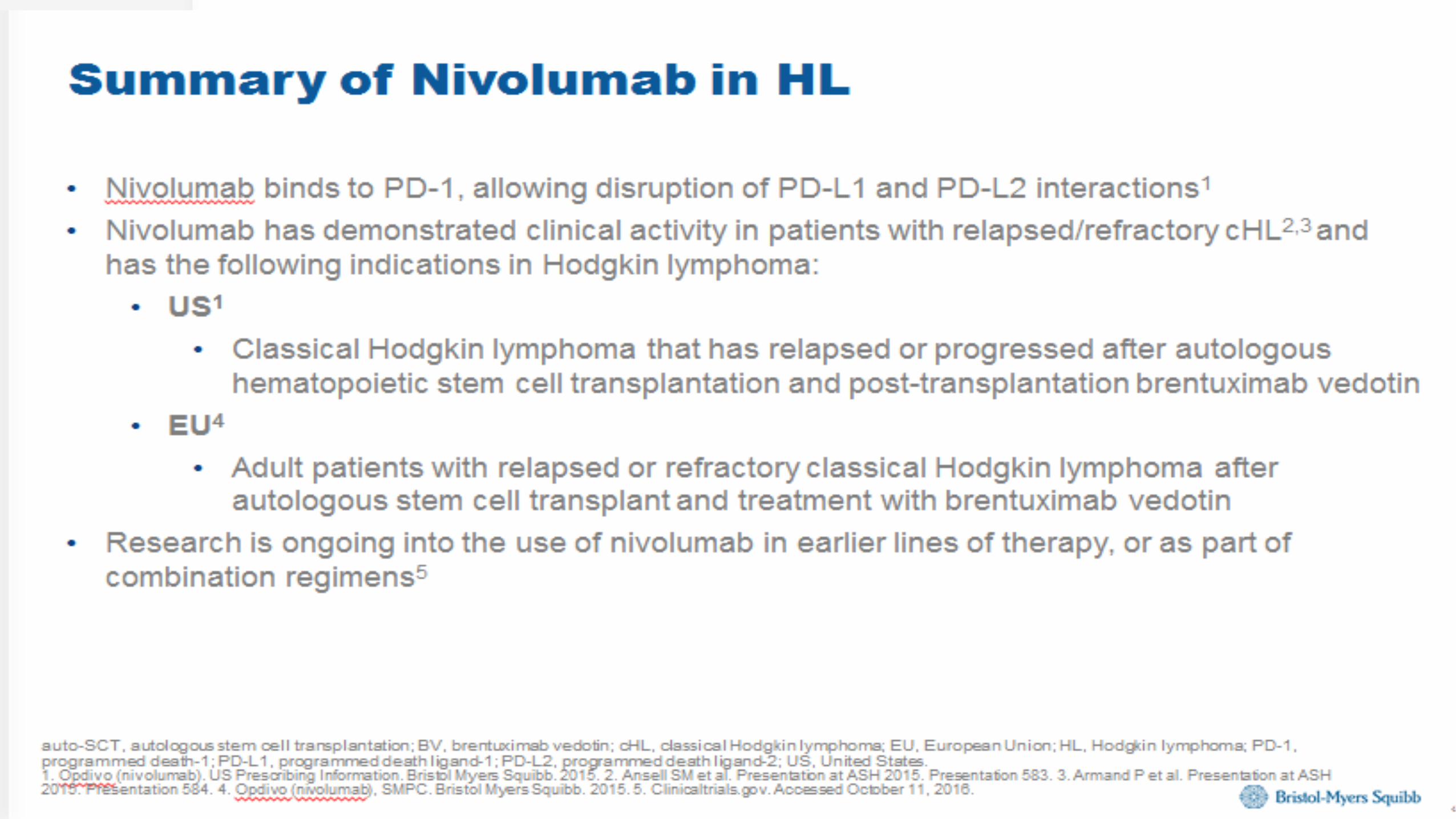
Summary
29
LOCAL APPROVAL MAY
BE REQUIRED BEFORE
EXTERNAL USE. REFER
TO LOCAL GUIDELINES.
Table of Contents
PD-1 Checkpoint
Inhib i tors : MOA
Pseudo-Progression as
Response to Immuno-
Oncology Therapies
Nivolumab: Ongoing
BMS-Sponsored Cl in ical
Tr ia ls
CTLA-4 Checkpoint
Inhib i tors : MOA
Nivolumab: ISRs
Summary
30
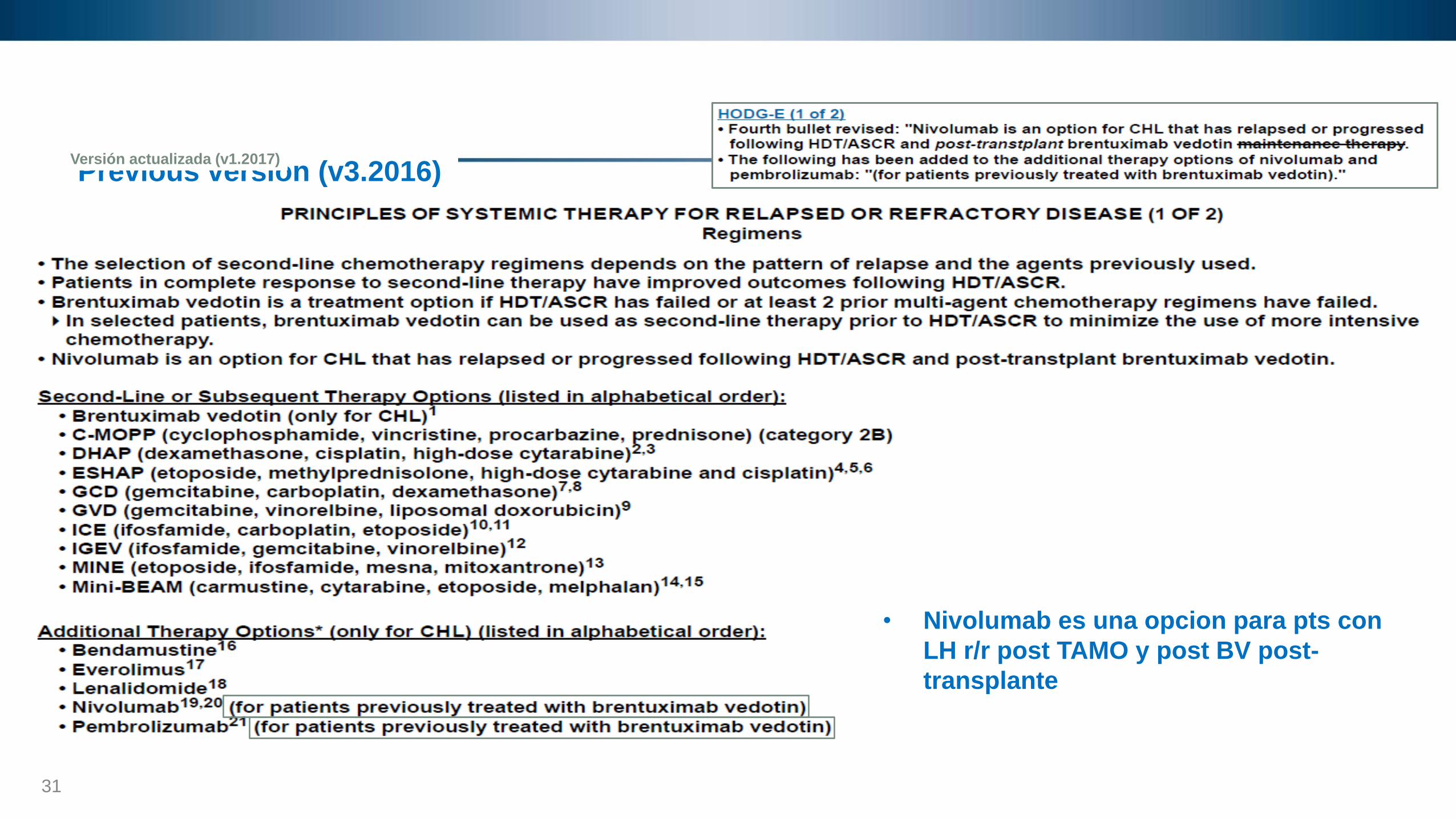
Previous version (v3.2016)
31
HODG-E Versión actualizada (v1.2017)
• Nivolumab es una opcion para pts con
LH r/r post TAMO y post BV post-
transplante
CASO CLÍNICO:
LINFOMA DE HODGKIN R/R
Filiación
• Varón de 39 años, químico-farmaceútico.
– Elabora productos con soda caústica e hipoclorito de sodio.
– Contacto TBC (+) (hermano con TBC en dos años de tratamiento)
• Antecedentes: DM2 (2014) en tto. con Metformina.
• No antecedentes oncológicos.
• Antecedente familiar: tía materna con cáncer de mama.
Cuadro Clínico:
• TE: 3 m.
– Síntomas principales: tos productiva en incremento, disnea, sudoración vespertina, hiporexia, baja de peso (15 kilos).
• Examen físico: ECOG 1
– Adenopatías en hemicuello derecho (G II) de hasta 2 cm.
– Pulmones: roncos bilaterales.
FI: Octubre 2014
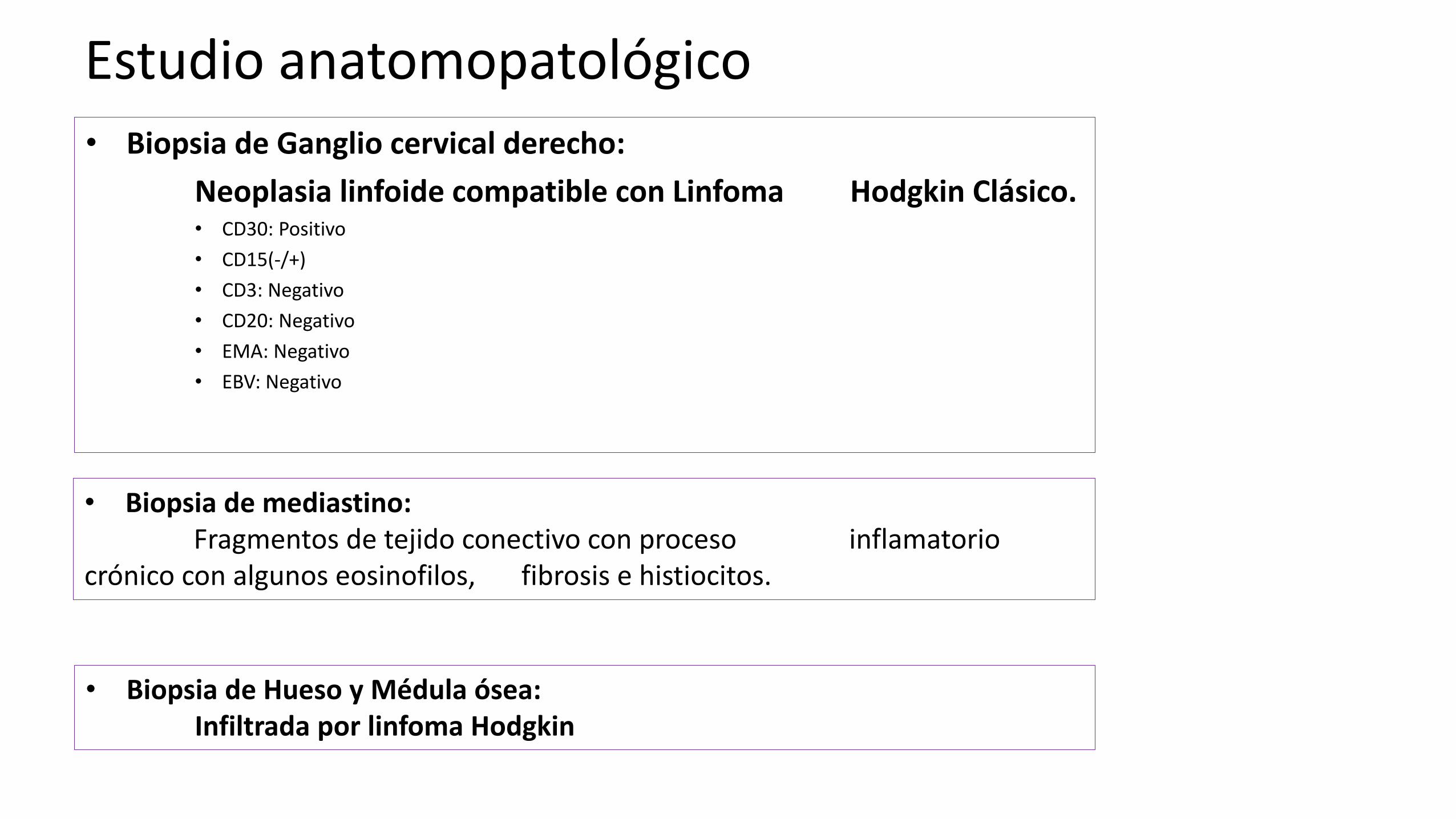
Estudio anatomopatológico • Biopsia de Ganglio cervical derecho:
Neoplasia linfoide compatible con Linfoma Hodgkin Clásico. • CD30: Positivo
• CD15(-/+)
• CD3: Negativo
• CD20: Negativo
• EMA: Negativo
• EBV: Negativo
• Biopsia de mediastino: Fragmentos de tejido conectivo con proceso inflamatorio crónico con algunos eosinofilos, fibrosis e histiocitos.
• Biopsia de Hueso y Médula ósea: Infiltrada por linfoma Hodgkin
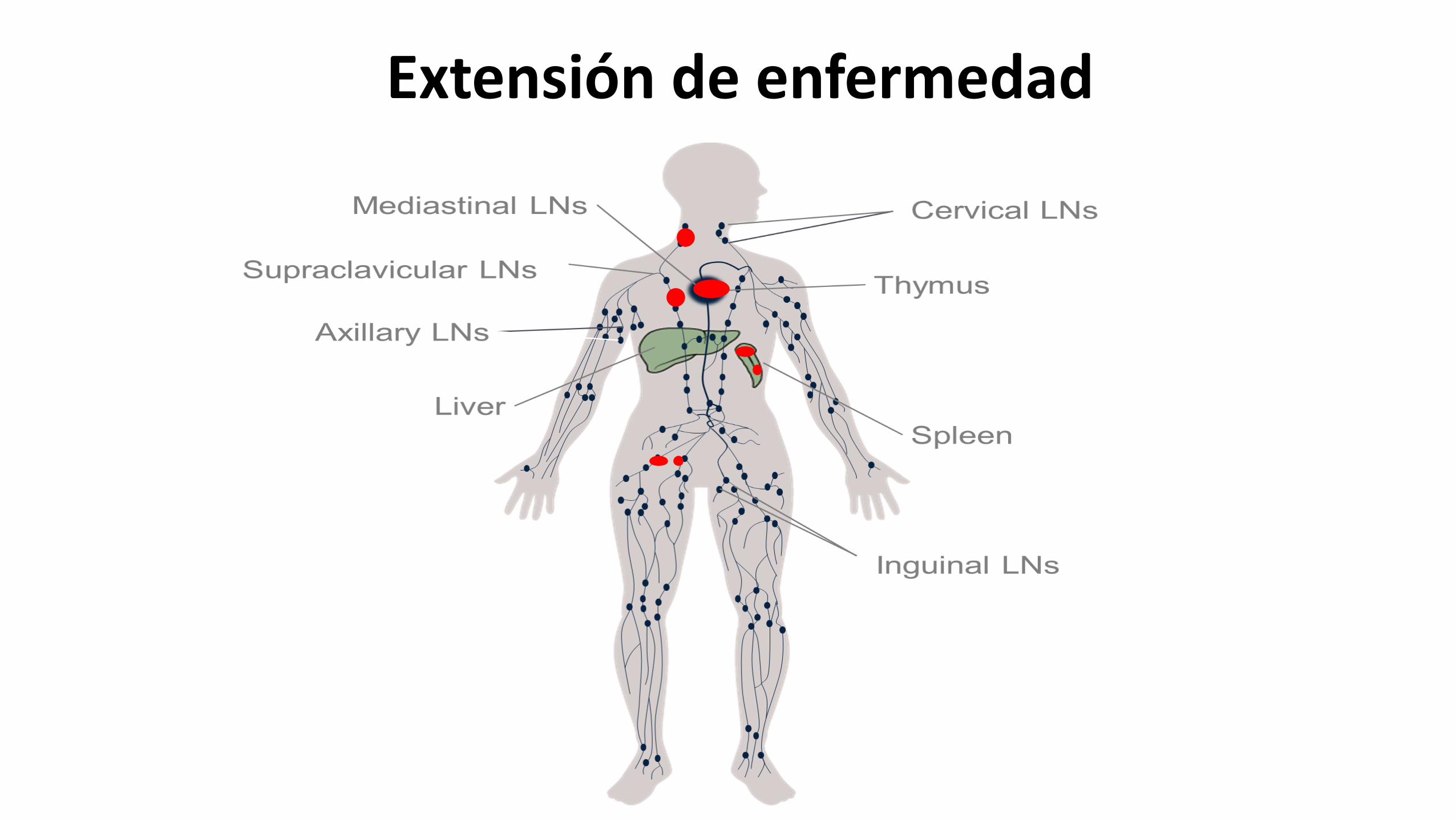
Extensión de enfermedad
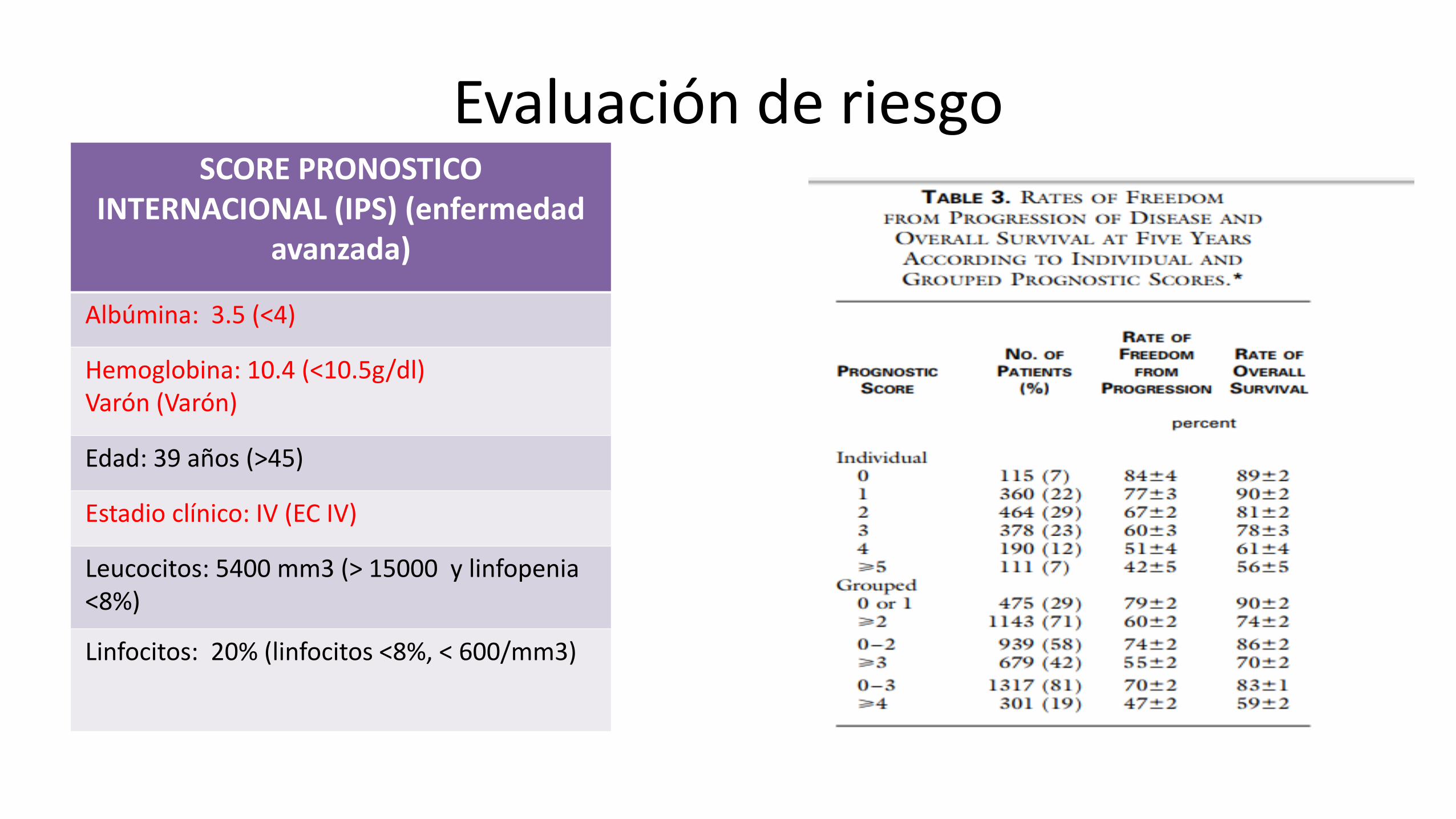
Evaluación de riesgo SCORE PRONOSTICO
INTERNACIONAL (IPS) (enfermedad avanzada)
Albúmina: 3.5 (<4)
Hemoglobina: 10.4 (<10.5g/dl) Varón (Varón)
Edad: 39 años (>45)
Estadio clínico: IV (EC IV)
Leucocitos: 5400 mm3 (> 15000 y linfopenia <8%)
Linfocitos: 20% (linfocitos <8%, < 600/mm3)
DIAGNÓSTICO: Linfoma de Hodgkin clásico EC IV B IPS AR
Tratamiento:
• Dic 2014- May 2015: Inicia tratamiento con ABVDX 6 con respuesta parcial.
• Jun 2015 - Nov 2015: ICE X 4 con enfermedad estable al inicio y luego progresión de enfermedad.
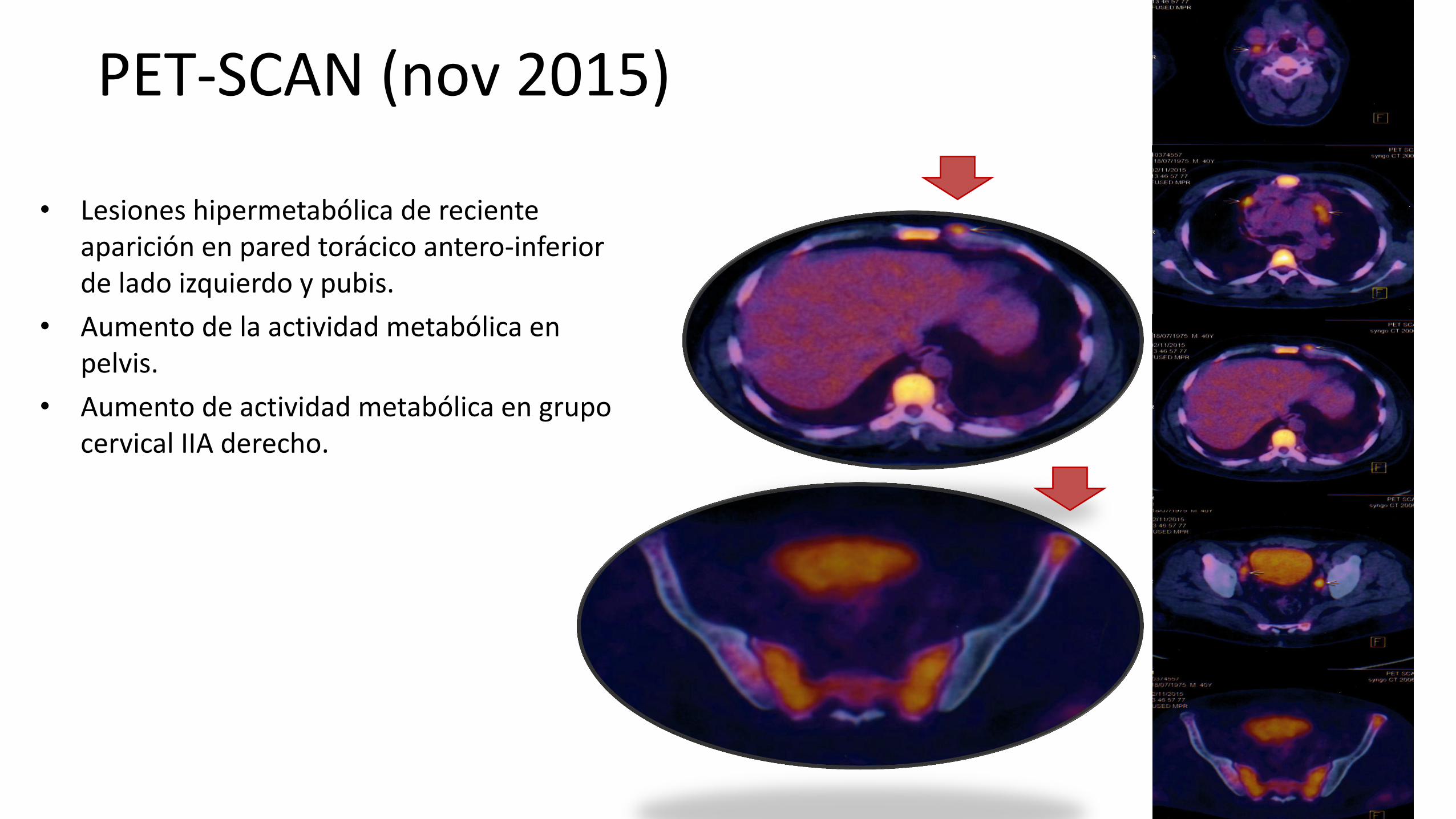
PET-SCAN (nov 2015)
• Lesiones hipermetabólica de reciente aparición en pared torácico antero-inferior de lado izquierdo y pubis.
• Aumento de la actividad metabólica en pelvis.
• Aumento de actividad metabólica en grupo cervical IIA derecho.
Tratamiento de 3° línea:
• Dic 2015- May 2016: Brentixumab 1.8 mg/kg c/3 sem con mejoría clínica y estabilización de la enfermedad.
– Crecimiento clínico de adenopatía cervical derecha hasta 3 cm.
– Nódulos subcutáneos en región anterior de tórax (1x1cm)
– Dolor en tórax superior derecho que se irradia a brazo.
– VSG 75 mm/h (aumento)
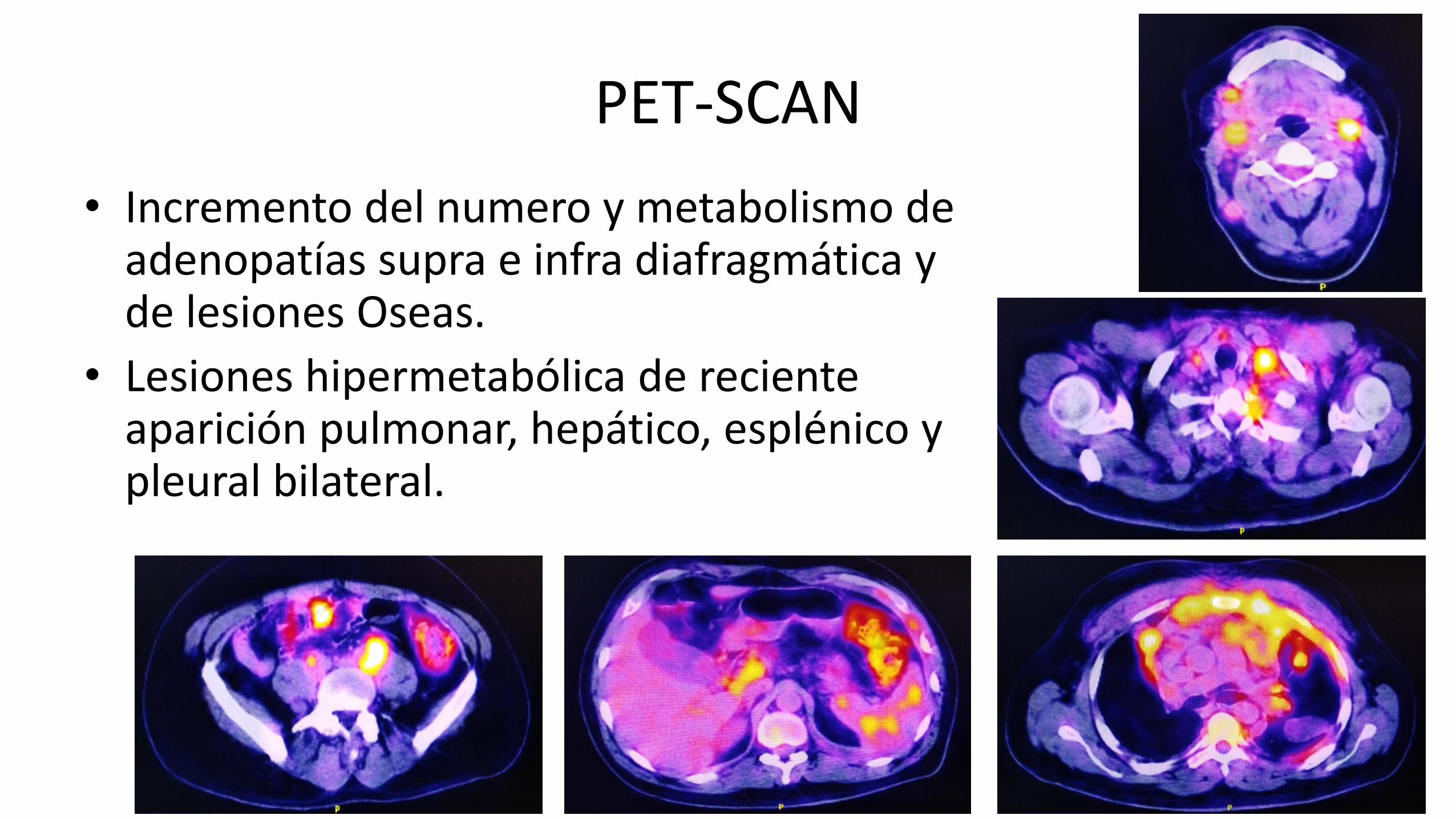
PET-SCAN
• Incremento del numero y metabolismo de adenopatías supra e infra diafragmática y de lesiones Oseas.
• Lesiones hipermetabólica de reciente aparición pulmonar, hepático, esplénico y pleural bilateral.
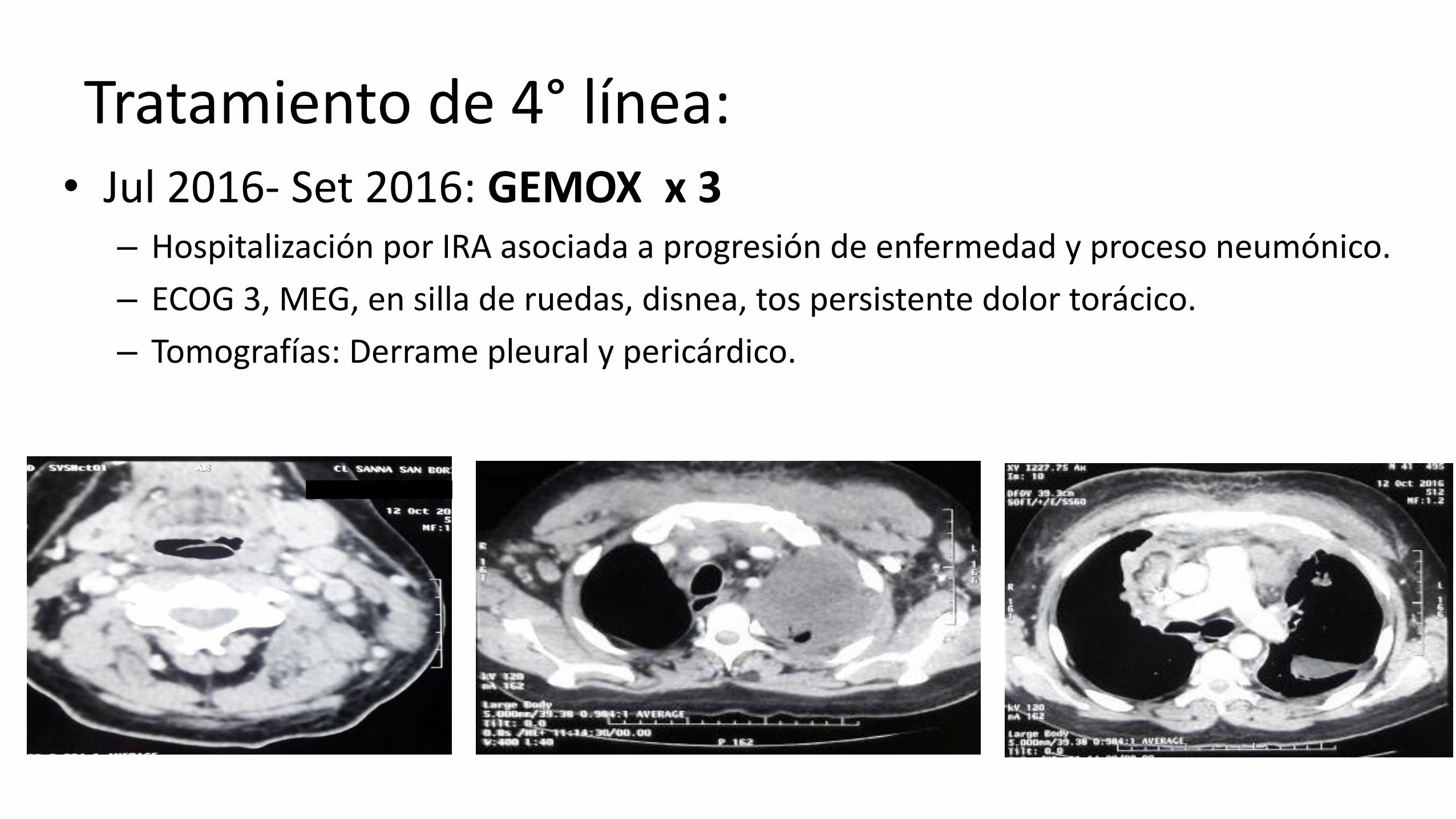
Tratamiento de 4° línea: • Jul 2016- Set 2016: GEMOX x 3
– Hospitalización por IRA asociada a progresión de enfermedad y proceso neumónico.
– ECOG 3, MEG, en silla de ruedas, disnea, tos persistente dolor torácico.
– Tomografías: Derrame pleural y pericárdico.
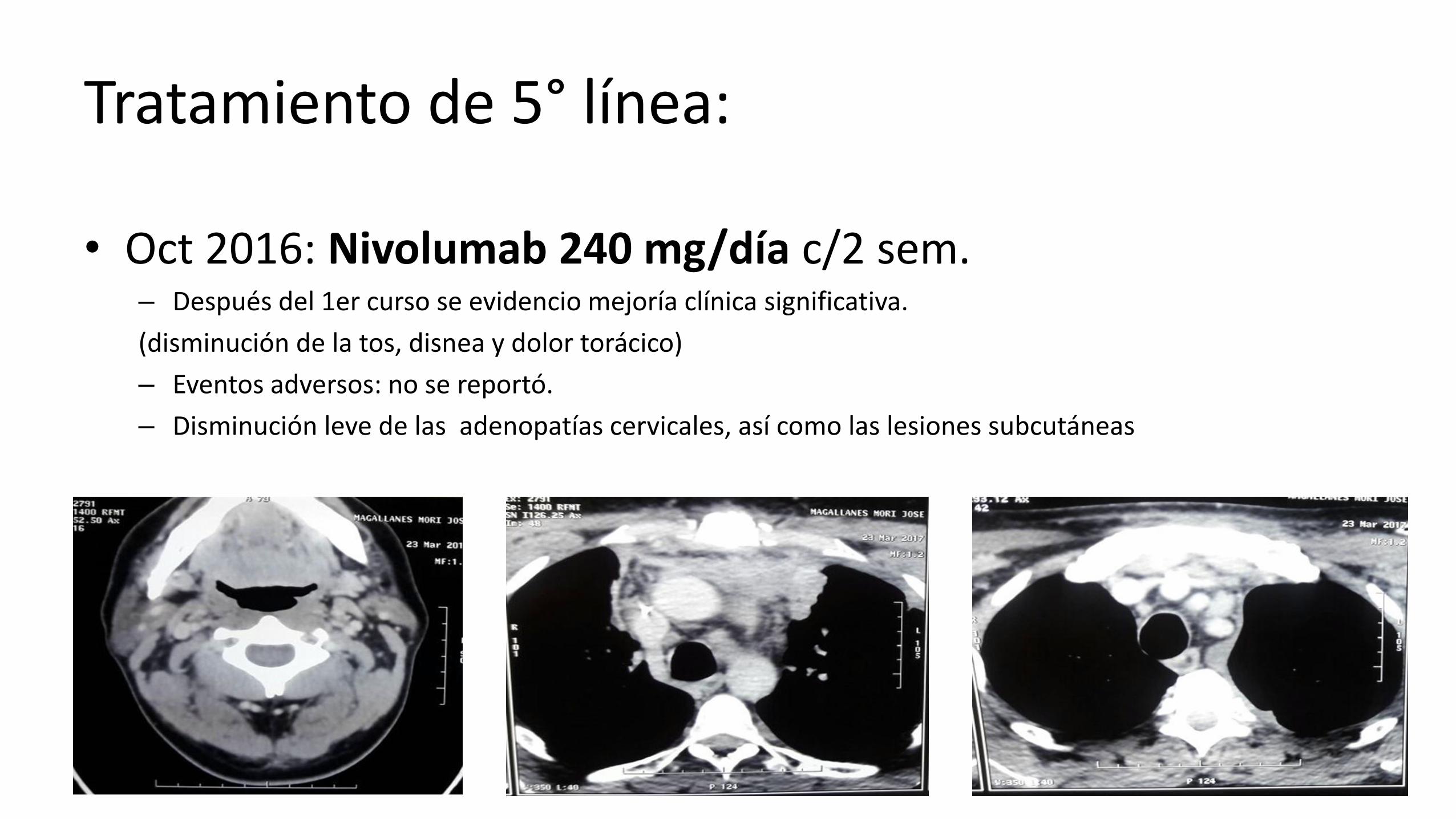
Tratamiento de 5° línea:
• Oct 2016: Nivolumab 240 mg/día c/2 sem. – Después del 1er curso se evidencio mejoría clínica significativa.
(disminución de la tos, disnea y dolor torácico)
– Eventos adversos: no se reportó.
– Disminución leve de las adenopatías cervicales, así como las lesiones subcutáneas
Tratamiento de 5° línea: NIVOLUMAB
Hasta la actualidad ha recibido 24 cursos – Después del primer curso se evidencio mejoría clínica significativa.
– Eventos adversos: disminución de peso, dolor articular esporádico, tendencia al llanto (Sd. Depresivo)
– Clínicamente no se palpan adenopatías y lesiones subcutáneas en resolución.
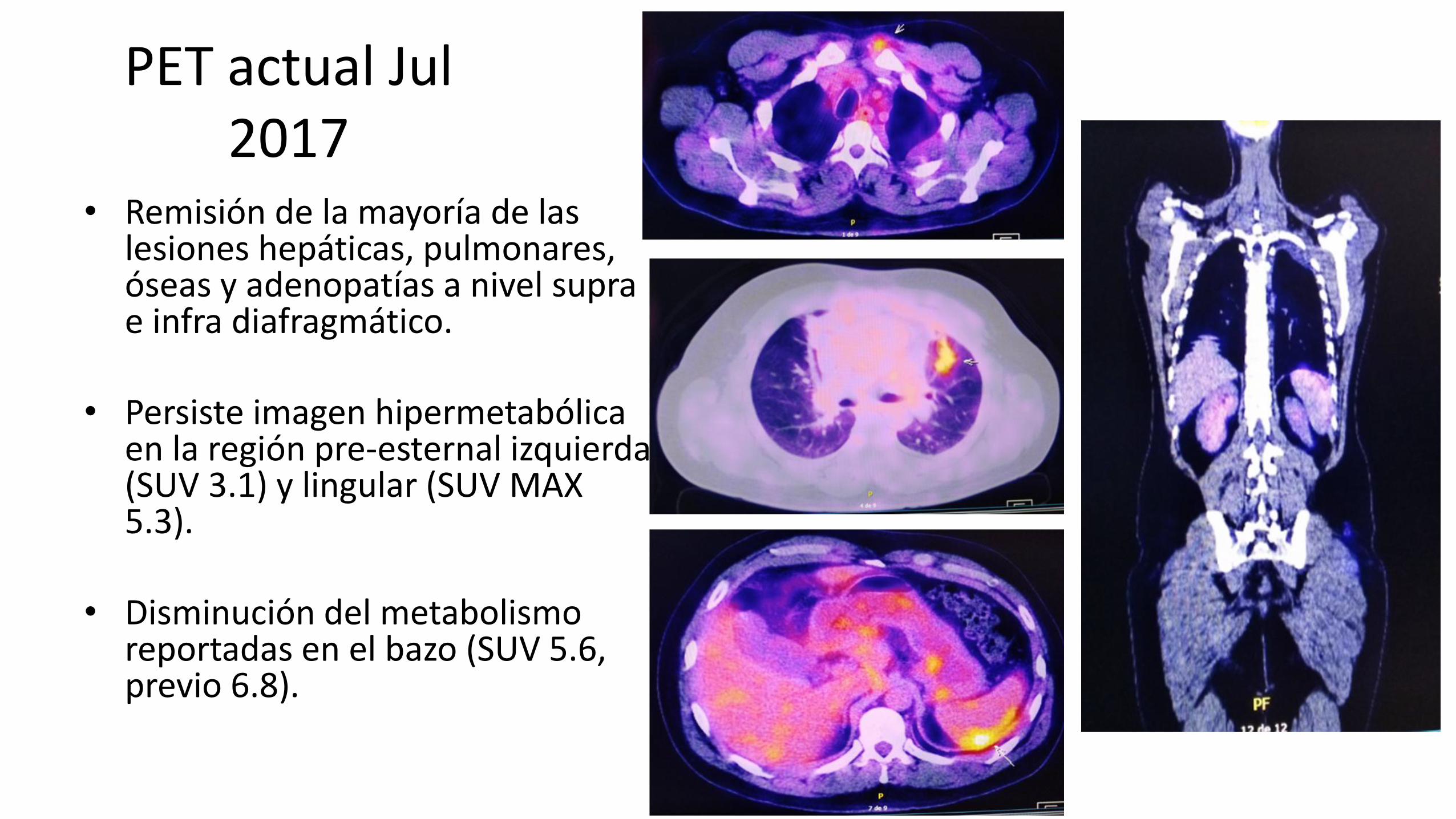
PET actual Jul 2017
• Remisión de la mayoría de las lesiones hepáticas, pulmonares, óseas y adenopatías a nivel supra e infra diafragmático.
• Persiste imagen hipermetabólica
en la región pre-esternal izquierda (SUV 3.1) y lingular (SUV MAX 5.3).
• Disminución del metabolismo
reportadas en el bazo (SUV 5.6, previo 6.8).
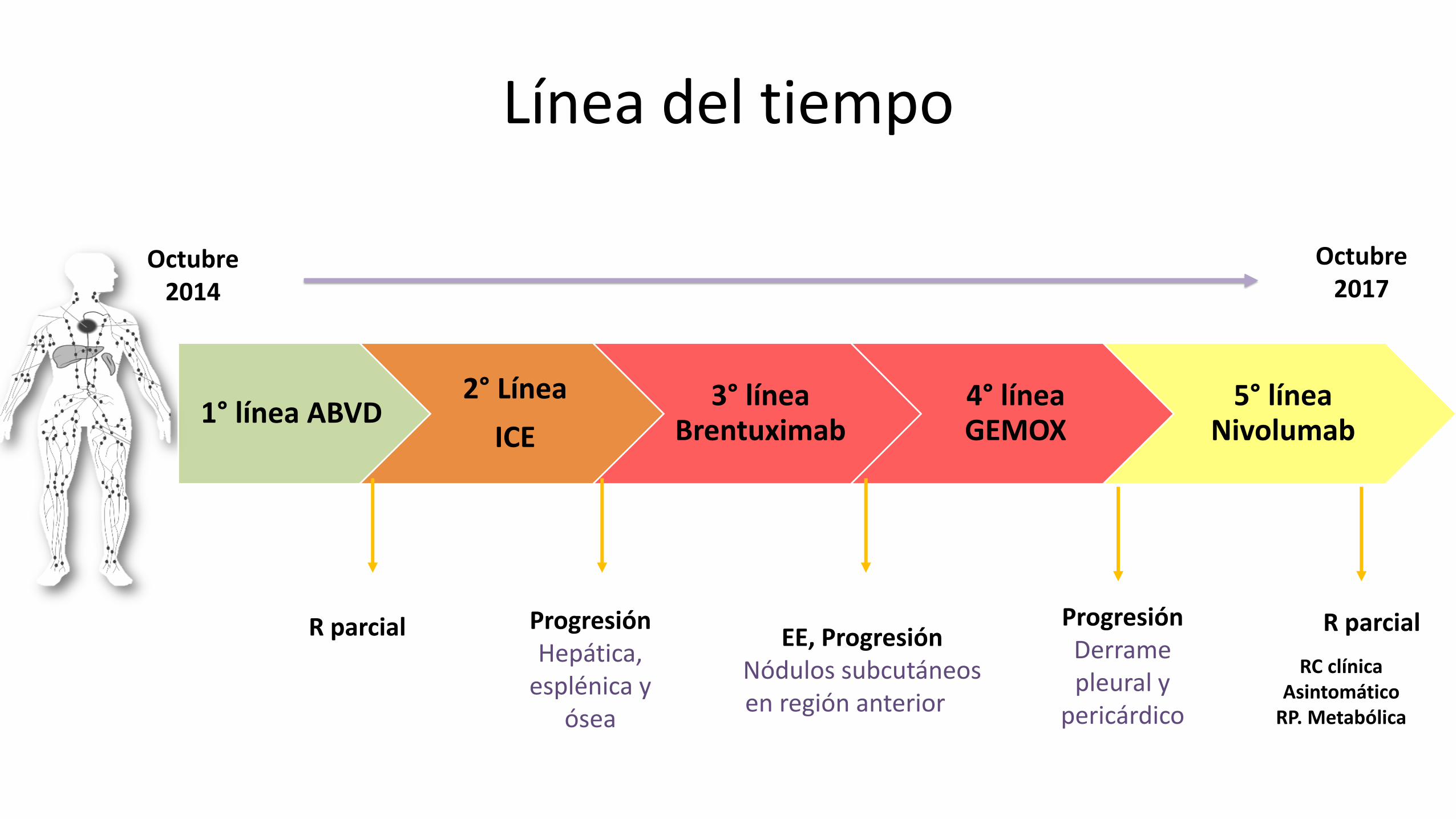
Línea del tiempo
1° línea ABVD 2° Línea
ICE
3° línea Brentuximab
4° línea GEMOX
5° línea Nivolumab
Octubre 2014
R parcial Progresión Hepática,
esplénica y ósea
Octubre 2017
EE, Progresión Nódulos subcutáneos en región anterior de
tórax
Progresión Derrame pleural y
pericárdico
R parcial
RC clínica Asintomático
RP. Metabólica
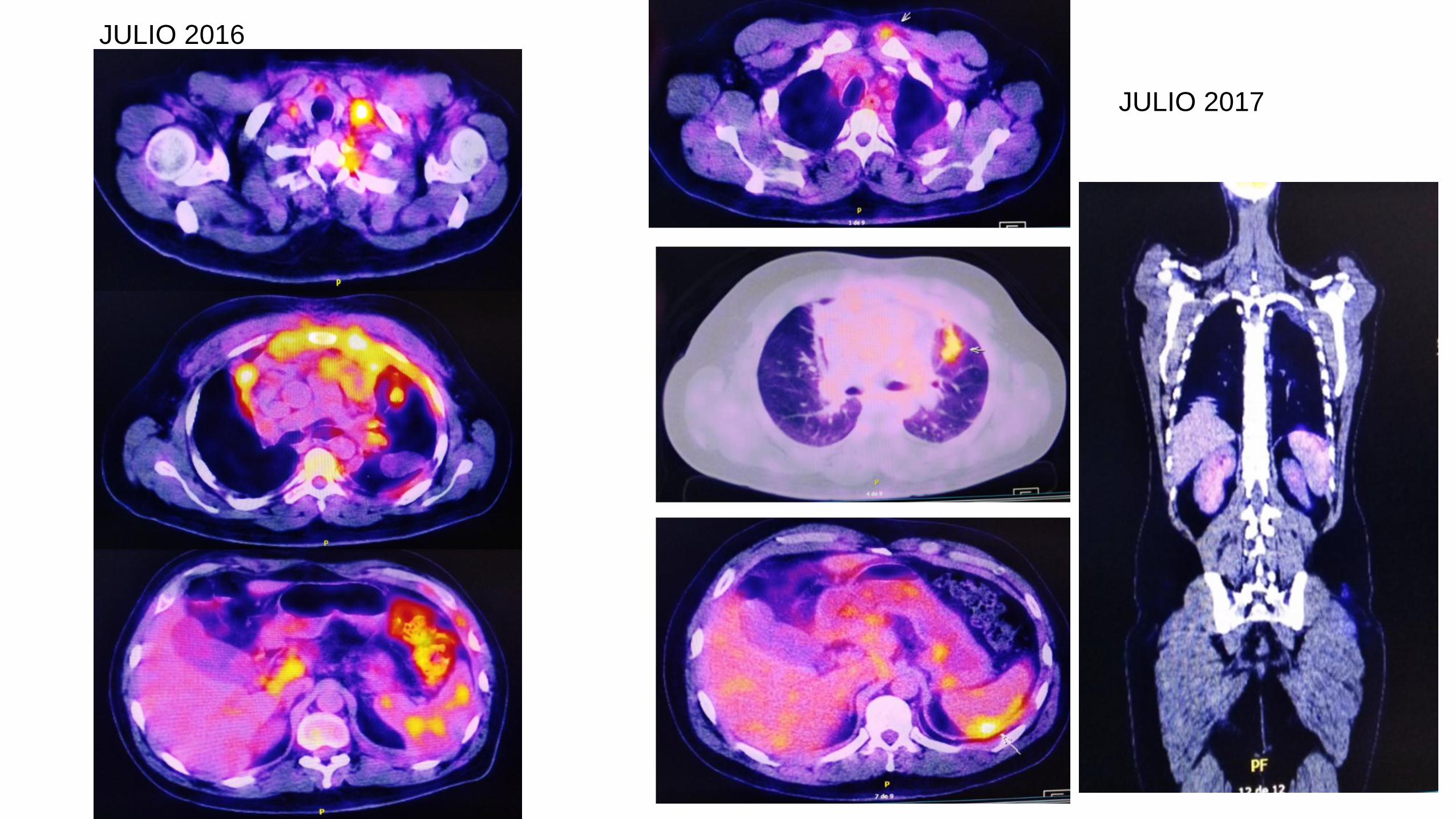
JULIO 2016
JULIO 2017