Embed Size (px)
Citation preview

1
NHSN and Public Reporting
Linda R. Greene, RN,MPS,CIC
Manager Infection Prevention
Highland Hospital
Rochester, NY
linda_ [email protected]

2
Objectives
• Describe challenges and opportunities related to pay for
performance and pay for reporting
• Identify changes to NHSN definitions for 2015
• Apply definitions to case scenarios
• Interpret NHSN data and illustrate ways it can be used to drive
improvement using the current evidence

3

4

5
Reported Measures

Who Gets HAIs? 1/25 on any given day in U.S.
hospitals; many are older adults
Magill SS, et al. NEJM 2014

How Big of a Problem are Healthcare
Associated Infections (HAIs) in the U.S.?
• Point Prevalence Survey;
National Healthcare Safety
Network (NHSN) N=183
hospitals, 2011
• Patients at risk = 11,282
– 452 (4.0%) with > one HAI
– Distribution by site – see pie chart
– C. difficile = 70% of GI infections
• Nationwide estimates:
– 648,000 patients with 721,800
HAIs/year
Magill SS et al. NEJM 2014;370:1198-208

8
HHS Action Plan

9

10

11
Challenges

12
Hospital Compare
U.S. National Benchmark = 1
Central line-associated bloodstream infections (CLABSI)
State
My Hospital

13
HAC Reduction

14
NHSN
TAP Reports
5 Star System

15

16
NHSN Data is Important
• Surveillance vs. Clinical Definitions
• Future move to algorithmic surveillance
• CMS validation
• Many changes in 2015 . Will become the new baseline year.

17
General Changes
Infection Window Period*†
Date of Event*
Present on Admission (POA) Infections*†
Healthcare-Associated Infections(HAI)*†
Repeat Infection Timeframe (RIT)*†
Secondary BSI Attribution Period*†
Pathogen assignment*†
*Does not apply to VAE, LabID Event Surveillance
†Does not apply to SSI Surveillance

18
NHSN
NHSN Course
Slides Posted
NHSN Webinar

19
No Longer Used
• Gap days
• Date last element was met

20
Infection Window Period
Infection Window Period
A 7 day period during which all site-specific infection
criterion must be met. It includes the date of the first
positive diagnostic test, that is an element of the site-
specific criterion, 3 calendar days before and 3 calendar
days after
For site-specific criterion that do not include a diagnostic test, the
first documented localized sign or symptom that is an element of
the infection criterion will be used

21
Example
Infection Window Period
Diagnostic test examples:
Laboratory specimen collection
Imaging test
Procedure or exam
Localized sign and/or symptom examples:
Diarrhea
Site specific pain
Purulent exudate

22
Date of Event
The date the first element used to meet the CDC NHSN site-specific
infection criterion occurs for the first time within the seven day infection
window period
Fever
Positive cultureDate
of Infection
2015

23
Date of Event

24
Present on Admission (POA) vs. Healthcare-Associated Infection
(HAI)
Present on Admission - date of event* occurs on the day of
admission or the day after admission.
The POA time period continues to include the day of admission, 2 days
before and the day after admission.
Healthcare-Associated Infection - the date of event* occurs on or
after the 3rd calendar day of admission.
POA

25
Repeat Infection Timeframe (RIT)
• A 14-day timeframe during which no new infections of
the same type are reported
• The date of event is Day 1 of the 14-day Repeat
Infection Timeframe
• Additional pathogens identified are added to the event

26
RIT
The RIT will apply at the level of specific type of infection with the
exception of Bloodstream Infection (BSI), Urinary Tract Infection (UTI)
and Pneumonia (PNEU) where the RIT will apply at the major type of
infection
• Patients will have no more than one BSI (e.g., LCBI1, LCBI2, MBI-LCBI1etc.)
• Patients will have no more than one UTI (e.g., SUTI, ABUTI)

27

28
Test Your Knowledge
Mrs. X is admitted to your hospital on Oct 1st . A
urinary catheter is inserted at that time. On Oct 3rd,
she spikes a temp of 38.2. The next day, a urine
culture is sent which grows 100,00 ecoli.
Is this an HAI?
Why or why not?

29
Another One
Mr. Y developed a CAUTI on 11/01/14 which grew 100,000
pseudomonas
On 11/13/14, he has a second urine culture sent which grows
100,000 proteus. How is this classified?
1. Not a new CAUTI- no further data is added to NHSN
2. New CAUTI- Different organism
3. Not a new CAUTI, but add proteus to the pathogen list of the
pre-existing infection.

30
Definitions
Secondary Bloodstream Infection (BSI) Attribution Period
The period in which a positive blood culture must be collected to
be considered as a secondary bloodstream infection to a primary
site infection.
The period is 14 – 17 days in length depending upon the date of
event

31
Blood Culture Ecoli

32
Secondary BSI
Secondary bloodstream infections may be attributed to a primary
site infection as per the Secondary BSI Guide of the BSI event
protocol
Blood culture pathogen matches at least one organism found in
the site-specific infection culture used to meet the primary site
infection criterion
OR
The positive blood culture is an element used to meet the
primary site infection criterion

33
Pathogen Assignment
Pathogen Assignment
Additional eligible pathogens identified within a Repeat Infection
Window are added to the event
Pathogens exclusions for specific infection definitions (e.g., UTI,
PNEU)* also apply to secondary bloodstream infection pathogen
assignment
Excluded pathogens must be attributed to another primary site-specific
infection as either a secondary BSI or identified as a primary BSI

34
Pathogen Assignment
BSI pathogens may be assigned to more than
one infection source
Assigned as a secondary BSI pathogen to a site-specific
infection (e.g., UTI) and assigned as an additional
pathogen to a primary BSI event

35

36
New CAUTI Definition
Definitional Changes:
The Urinary Tract Infections (UTI) definitions will no longer
include:
Symptomatic UTI (SUTI) criteria 2 and 4 due to removal of
the following elements:
• Colony counts of less than 100,000 CFU/ml
• Urinalysis results
• Urine cultures that are positive only for yeast, mold,
dimorphic fungi, or parasites
• Uropathogen List for Asymptomatic Bacteremic UTI (ABUTI)

37
CAUTI
What These Changes Mean for Facilities Reporting UTIs to
NHSN in 2015
Only urine cultures with a colony count of at least 100,000
CFU/ml for at least one bacteria will be used to meet NHSN UTI
criteria.
Only bacteria will be accepted as causative organisms of UTI.
ABUTI criteria will use the same pathogen list as SUTI.

38
Question
Mrs. X is admitted to your unit on 11/6/2014. She has a PICC
line in place and a urinary catheter is inserted.
On 11/10/2014 she spikes a temperature of 38.5, the physician
orders blood and urine cultures. Both the blood and urine grow
1,000 candida.
How do you classify this infection?
1. CAUTI with secondary BSI
2. Primary BSI and CAUTI
3. CLABSI only

39
SSI Definition
Infection Present at Time of Surgery
Infection present at time of surgery (PATOS) will be a new field on the SSI Event form. PATOS denotes that an infection is present at the start of, or during, the index surgical procedure (in other words, it is present preoperatively).
PATOS doesn’t apply if there is a period of wellness between the time of a preoperative condition and surgery.
The infection must be noted/documented preoperatively or found intra-operatively in a pre-operative or intraoperative note.

40
SSI Continued
The patient does not have to meet the NHSN definition of an SSI
at the time of the primary procedure but there must be surgeon
notation that there is evidence of infection or abscess present at
the time of surgery.

41
PATOS
Only select PATOS = YES if it applies to the depth of SSI that is
being attributed to the procedure (e.g., if a patient had evidence
of an intra-abdominal infection at the time of surgery and then
later returns with an organ space SSI the PATOS field would be
selected as a YES.
If the patient returned with a superficial or deep incisional SSI
the PATOS field would be selected as a NO).

42
Question
19 year old patient admitted with an acute abdomen, to OR for
XLAP with finding of an abscess due to ruptured appendix, and
an APPY is performed. Patient returns 2 weeks later and meets
criteria for an organ space IAB SSI.
How would you mark the PATOS field?
1.Yes
2. No

43
Question
Patient is admitted with a ruptured diverticulum and the surgeon
notes that there are multiple abscesses in the intra abdominal
space. Patient returns 3 weeks later and meets criteria for a
superficial SSI ?
How would you mark the PATOS field?
1. Yes
2. No

44
SSI
Diabetes Documented
Along with the current NHSN definition of diabetes, assignment
of the discharge ICD-9 codes in the 250 to 250.93 range will be
acceptable for use to answer YES to this diabetes field question.
Change in “Scope” Field Reporting Instruction
The reporting instruction for answering the SCOPE risk factor
field will be updated. The instruction regarding the extension of a
scope site will be removed. New instruction in the Table of
Instructions will be: Check Y if the NHSN operative procedure
was coded as a laparoscopic procedure performed using a
laparoscope/robotic assist, otherwise check N.

45

46

47
MRSA/ VRE Continued
• MDRO and CDI LabID Event reporting for facility-wide inpatient
(FacWideIN) will also require location-specific surveillance for
that same organism in each emergency department(s) (pediatric
and adult) and 24-hour observation location(s).
• Facilities participating in FacWideIN LabID Event reporting will be
required to map and report outpatient LabID Events from emergency
departments and 24-hour observation locations for the same
organism and LabID Event type (i.e., All Specimens or Blood
Specimens only). This means facilities will no longer assign the
admitting inpatient location to LabID Events when specimens are
collected in the emergency department or 24-hour observation
location on the same calendar day as inpatient admission.

48
VAE
Combining possible / probable VAP
Ability to enter episodes of mechanical ventilation
Pathogen reporting and secondary bloodstream attribution
specific to pneumonia 1 will not be allowed

49
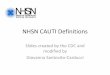
VAE Surveillance Definition Algorithm Summary
Patient on mechanical ventilation > 2 days
Baseline period of stability or improvement, followed by sustained period of worsening oxygenation
Ventilator-Associated Condition (VAC)
General evidence of infection/inflammation
Infection-Related Ventilator-Associated Complication (IVAC)
Positive results of microbiological testing
Possible or Probable VAP
• Respiratory status component
• Additional evidence
• Infection / inflammation component
No CXR needed!

50
Case 1
50
MV Day Min
PEEP
Min
FiO2
1 8 100
2 7 70
3 6 50
4 6 70
5 5 60
6 6 50
7 6 70
8 5 80
9 5 50
10 5 50
54 yr old male admitted to the ICU transferred on ventilator from the ED. Review vent settings below to see if VAE criteria are met. If so, on what day?1. No VAC2. Day 43. Day 74. Day 8

51
Case 2
51
54 yr old male admitted to the ICU transferred on ventilator from the ED. Would the criteria be met with these settings? If so, on what day?1. No VAC2. Day 43. Day 74. Day 8
MV
Day
Min
PEEP
Min
FiO2
1 8 100
2 7 70
3 6 50
4 6 70
5 5 50
6 6 50
7 6 70
8 5 80
9 5 50
10 5 50

52
The Data
Our job is to turn data into meaningful information which can be
used by care providers to improve outcomes
Let’s look at this scenario:

53
Which answer(s) best describes this data?
1. Both the CAUTI rate and the SIR are higher statistically
higher than the NHSN mean
2. The rate difference is due to chance
3. Only 14% of like ICU’s reporting to NHSN have a higher
infection rate


55

56
Evidence Based Practices
Look at the evidence
Conduct a gap analysis
Evaluate what processes are already in place

57
Recent Guidelines
Only 2 recommendations with
high level of Evidence:
1.Do not ROUTINELY use antiseptic
catheters to prevent CAUTI
((quality of evidence: I).
2. Do not treat asymptomatic
bacteriuria in catheterized
patients except before invasive
urologic procedures
(quality of evidence: I).

58
Appropriate Indications for Catheter Use
Appropriate Indications
Patient has acute urinary retention or obstruction
Need for accurate measurements of urinary output in critically ill patients.
Perioperative use for selected procedures:
•urologic surgery or other surgery on contiguous structures of genitourinary
tract,
•anticipated prolonged surgery duration (removed in post-anesthesia unit),
•anticipated to receive large-volume infusions or diuretics in surgery,
•operative patients with urinary incontinence,
•need to intraoperative monitoring of urinary output.
To assist in healing of open sacral or perineal wounds in incontinent patients.
Requires prolonged immobilization (e.g., potentially unstable thoracic or lumbar
spine)
To improve comfort for end of life care if needed.
Gould C, et al. Infect Control Hosp Epidemiol 2010;31:319-26.

59
Driving Performance
Most CAUTIs occur from day 7-10
Yeast is the primary pathogen in 30% of the CAUTIs
Most patients are transferred out of the ICU with a catheter
Which of the following actions would not be a first step?
• 1) Institute nurse driven removal protocols, automatic stop
orders ,etc.
• 2) Ensure catheters are inserted for appropriate indications
• 3) Develop a competency program to ensure all care providers
insert urinary catheters aseptically
• 4) Develop culturing guidelines

60
SSIs

61

62

63

64
Changes
2008
Wash and clean area around incision site using appropriate antiseptic agent( A- 2).
Control blood glucose level during the immediate postoperative period for patients undergoing cardiac surgery (AI).
2014
Use alcohol-containing pre-operative skin preparatory agents if no contraindication exists ( New- 1 High)
Maintain post-operative blood glucose ≤ 180 mg/dL.
Cardiothoracic surgical procedures (A-I; NEW=HIGH)
Non-cardiac procedures [Dronge Arch Surg 2006; Golden Diabetes care 1999; Olsen MA JBoneJoint Surg Am 2008] (NEW= 2 MODERATE)

65
Changes
2008
Maintain normothermia (temperature higher than 36oC) immediately after colorectal surgery – previous unresolved
Impervious plastic wound protectors-not discussed
2014
Maintain normothermia(temperature > 35.5 °C) during the perioperative period.
(NEW= 1 HIGH)
Impervious plastic wound protectors in gastrointestinal and biliary tract surgery (NEW= 1 HIGH)

66
Changes
2008
Maintaining oxygenation with supplemental oxygen during and after colorectal procedures (unresolved issue)
Routine screening for MRSA or routine attempts to decolonize surgical patients with an antistaphylococcal agent in the preoperative setting (unresolved issue)
2014
Maintaining oxygenation with
supplemental oxygen during and
following colorectal procedures
(NEW)
Special populations: recommended
for use in locations and/or populations
within the hospital with unacceptably
high SSI rates despite implementation
of the basic SSI prevention
strategies:
Screen for Staphylococcus aureus
and/or decolonize surgical patients
with an anti-staphylococcal agent in
the pre-operative setting

67
Changes
• Check list- not discussed
• Not addressed
• Use the WHO check list (1)
• Optimize tissue oxygenation by
administering supplemental
oxygen during and immediately
following procedures requiring
mechanical ventilation

68
Changes - Antibiotics
2008
• Administer prophylaxis within 1
hour before incision
• Discontinue prophylaxis within
24 hours after surgery
2014
Although guidelines suggest stopping the antimicrobial agent within 24 hours of surgery, there is no evidence that agents given after closure contribute to efficacy, and they do contribute to increased resistance
Weight dose antibiotics

69
CMS Final Rule for Value Based Purchasing 2017:
Remove from measure set the following process measures as “topped-
out”:
SCIP-Inf-2: Prophylactic Antibiotic Selection for Surgical Patients
SCIP-Inf-3: Prophylactic Antibiotic Discontinued Within 24 Hours After
Surgery End Time
SCIP-Inf-9: Urinary Catheter Removed on Postoperative Day 1 or
Postoperative Day 2

70
Unresolved Issues
1. Preoperative bathing with chlorhexidine-containing products.
•Preoperative bathing with agents such as chlorhexidine has been shown to reduce bacterial colonization of the skin. Several studies have examined the utility of preoperative showers, but none has definitely proven that they decrease SSI risk. Six randomized controlled trials evaluating the use of 4% chlorhexidine gluconate were included in a Cochrane review, with no clear evidence of benefit noted. It should be noted that several of these studies had methodological limitations and were conducted several years ago. Thus, the role of preoperative bathing in SSI prevention is still uncertain.
•To gain the maximum antiseptic effect of chlorhexidine, adequate levels ofCHG must be achieved and maintained on the skin. Typically, adequate levels are achieved by allowing CHG to dry completely.

71
Safety – More than a Model
71
Patient
Leadership
Communication
Teamwork
Managing Behavioral
Choices
Organizational Learning
System Design

72
Different Direction
• Contextual Journey
• INSIDE OUT
• Observe then define
• Observation for
understanding
• Anthropology foundation
• Solutions are uncovered,
guided by insiders, those
directly involved-creates
ownership
• Traditional Journey
• OUTSIDE IN
• Define, then observe
• Observation for compliance
• Manufacturing foundation
• Solutions are pre-defined, guided
by outsiders, those indirectly
involved-buy-in
Our New Journey

73
The Bottom Line
Many changes for 2015
Moving toward clearer definitions and data that can easily be
retrieved from the medical record
Surveillance data is important to drive performance
improvement and assure the accuracy of reported data

74
Difficult Job
http://youtu.be/Pk7yqlTMvp8