Embed Size (px)
Citation preview

NHS GEMS Annual Report 2005-2006
DESCRIPTION OF OOH SERVICES
As a result of the implementation of the new GMS contract in April 2004 where the GPs within Glasgow opted out of providing out of hours care, responsibility for the provision of Primary Care Medical Service during the out of hours period transferred to NHS Greater Glasgow (Primary Care Division) on 1 July 2004. All staff TUPE transferred to NHS Greater Glasgow and the service continued with no major changes. Recent reorganisation within Glasgow has resulted in NHS GEMS becoming a self managed unit with the Emergency Care and Medical Specialties Directorate (Acute) within Glasgow with effect form 1 April 2006. The first point of contact for patients in the OOH period is by telephone to NHS 24, either by telephoning NHS 24 directly or telephoning their GP surgery number. The clinical consultation service for ambulant patients is delivered from six PCECs NHS GEMS have six Primary Care Emergency Centres (PCECs) open weekend day time and every evening until midnight. Two PCECs are open overnight. The PCECs are staffed with sessional GPs supported by traditional nursing roles.
The Patient Transport Service supports the service for ambulant patients and consists of 5 ten-seater minibuses which are tracked at all times from the NHS GEMS centre (Cowglen) and fitted with panic alarms for staff.
Within the past two years GP registrars have been introduced to the service to allow them to gain experience of working in the in the out of hours period in a supervised environment. Approximately 40 registrars are accommodated and are required to attend 120 hours of supervised training. NHS GEMS has now completed the training and consolidated practice for 10 Minor Illness Nurse Practitioners. These nurse practitioners are now currently working in some of the PCECs and an evaluation of their practice is ongoing. NHS GEMS has extremely good links with Community Psychiatric Services (CPNs). The out of hours CPN team is located within the NHS GEMS hub at Cowglen. NHS GEMS also works closely with the Learning Disability Service which has a dedicated on call service working harmoniously with NHS GEMS . Since the establishment of NHS GEMS eleven years ago it became clear that dental emergencies were a significant proportion of out of hours calls. We have worked with our dental colleagues to define the issue and NHS Glasgow has established Glasgow Emergency Dental Service. This service is linked through the NHS GEMS IT system to NHS 24, allowing direct referral of patients to the dental hospital out of hours. Dental nurses are now available to provide triage at the dental hospital and discussion is taking place as to the best site for this triage.
1
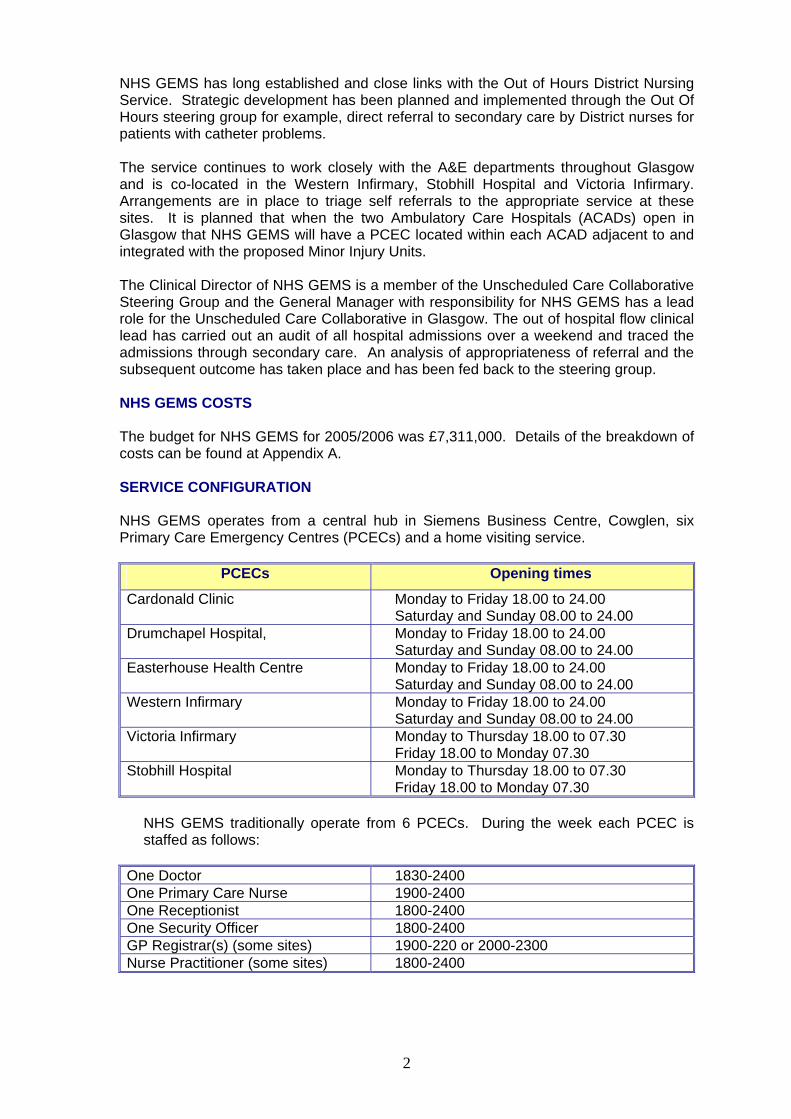
NHS GEMS has long established and close links with the Out of Hours District Nursing Service. Strategic development has been planned and implemented through the Out Of Hours steering group for example, direct referral to secondary care by District nurses for patients with catheter problems. The service continues to work closely with the A&E departments throughout Glasgow and is co-located in the Western Infirmary, Stobhill Hospital and Victoria Infirmary. Arrangements are in place to triage self referrals to the appropriate service at these sites. It is planned that when the two Ambulatory Care Hospitals (ACADs) open in Glasgow that NHS GEMS will have a PCEC located within each ACAD adjacent to and integrated with the proposed Minor Injury Units. The Clinical Director of NHS GEMS is a member of the Unscheduled Care Collaborative Steering Group and the General Manager with responsibility for NHS GEMS has a lead role for the Unscheduled Care Collaborative in Glasgow. The out of hospital flow clinical lead has carried out an audit of all hospital admissions over a weekend and traced the admissions through secondary care. An analysis of appropriateness of referral and the subsequent outcome has taken place and has been fed back to the steering group. NHS GEMS COSTS The budget for NHS GEMS for 2005/2006 was £7,311,000. Details of the breakdown of costs can be found at Appendix A. SERVICE CONFIGURATION NHS GEMS operates from a central hub in Siemens Business Centre, Cowglen, six Primary Care Emergency Centres (PCECs) and a home visiting service.
PCECs Opening times
Cardonald Clinic Monday to Friday 18.00 to 24.00 Saturday and Sunday 08.00 to 24.00
Drumchapel Hospital, Monday to Friday 18.00 to 24.00 Saturday and Sunday 08.00 to 24.00
Easterhouse Health Centre Monday to Friday 18.00 to 24.00 Saturday and Sunday 08.00 to 24.00
Western Infirmary Monday to Friday 18.00 to 24.00 Saturday and Sunday 08.00 to 24.00
Victoria Infirmary Monday to Thursday 18.00 to 07.30 Friday 18.00 to Monday 07.30
Stobhill Hospital Monday to Thursday 18.00 to 07.30 Friday 18.00 to Monday 07.30
NHS GEMS traditionally operate from 6 PCECs. During the week each PCEC is staffed as follows:
One Doctor 1830-2400 One Primary Care Nurse 1900-2400 One Receptionist 1800-2400 One Security Officer 1800-2400 GP Registrar(s) (some sites) 1900-220 or 2000-2300 Nurse Practitioner (some sites) 1800-2400
2

Stobhill and Victoria Infirmary sites remain open midnight till 0730am. The staffing level is: One Doctor 2400-0700 One Receptionist 2300-0730 One Security Officer 2300-0730
HOME VISITING Midweek evenings (Monday-Friday) - 5 cars (1 doctor / 1 driver) - 1800-2400 Cars are based at the following sites Cardonald, Drumchapel, Easterhouse, Stobhill and Victoria and visit mainly in that geographical area. If there are no visits to perform the home visiting doctor will see patients at the sites Overnight Home Visiting 2400-0730 3 Cars One car based at Stobhill and Victoria site and one based in west of the city. The two site based cars - if there are no calls pending the cars will return to sites and the doctor will see patients. IT LINKS Patient details are transferred directly via an electronic link to each PCEC from NHS 24. There is no appointment system at the PCECs. Patients are asked to attend as soon as possible. This system works well with the intention of all patients being seen within 30 minutes of arrival. Details of home visiting calls traditionally were sent to cars electronically by our hub controller. This IT link is now non functional and is a significant risk to the organisation and to patient care/safety. A bid has been constructed and this requires to be ratified and new IT installed as soon as possible. Currently details of home visits are telephoned to cars with the risk of loss of important information. TIME STRATIFICATION The organisation’s key performance indicators are set by the time stratification assigned to each call by NHS 24. NHS GEMS continually monitor compliance to response times set by NHS 24. TRANSPORT NHS GEMS own five mini buses. Patients who do not have their own transport can be transported to and from sites on request. Five mini buses are co-ordinated from the hub.
3

KEY PERFORMANCE INDICATORS
NHS GEMS – GREATER GLASGOW
1. A nurse or doctor should assess patients within 30 minutes of arrival at the Primary Care Emergency Centre.
2. NHS GEMS will respond to house visits within the time stratification assigned by
NHS 24:
Dual Response 98% Priority 1 – ASAP within 1 hour 98% Priority 2 - < 1 hour 100% Priority 3 - < 2 hours 100% Priority 4 - < 4 hours 100%
3. Hospital referrals are appropriate. (No more than 5% of hospital referrals would be
challenged at review.) 4. The treatment prescribed by the doctor is appropriate for diagnosis (no more than
5% of these treatments would be challenged at review.) 5. 100% of GP bags will be fully stocked and available for each home visit session. 6. 100% of patients Call Sheets for Out of Hours consultations must be sent to the
patient’s registered GP by 8am the following morning or by 8am on Monday following weekends or Tuesday following public holidays.
7. a. 100% of complaints should be acknowledged to within 3 working days of
receipt. b. 90% of complaints should be investigated and responded to within 20
working days. c. 100% of situations where a written response cannot be made with 20
working days the complainant should be sent a letter containing an apology reason for delay and expected timescale for response.
STAFFING
During the period of transfer from NHS GEMS the Co-op to NHS GEMS and the implementation of the new GP out of hours contract our impression was that a significant number of contracted GPs would either reduce their number of sessions for NHS GEMS or stop working for NHS GEMS altogether. Our intention therefore was to explore the route of a mixed economy with both contracted GPs and salaried GPs. It became clear however that the core number of general practitioners acting as contracted GPs did not significantly alter during this transition period. In addition, a significant number of previous GP registrars, who for the first time had received structured out of hours training within NHS GEMS, were keen to work for the service on a contracted basis following their registrar year. There is also a significant pool of locum general practitioners (non principals) within the Glasgow area who are pursuing portfolio careers and sessional work within NHS GEMS is popular. Practitioners like to be able to vary their commitment depending on life circumstances rather than commit to a fixed number of sessions per week. This has to date worked well for us and this summer and winter sessions have been filled easily. The implications of employing salaried GPs have been explored and at present we feel there would be no advantage to NHS GEMS in pursuing this route.
4

STAFFING [cont’d] The fee structure was well established pre 2004 and we have not been required to substantially increase fees although an 18% increase was applied to the GP sessional rate in the spring of 2005. This was as a result of an agreed “freeze” on sessional rates in the run up to the transfer of the Co-op to NHS GEMS when our rates were considerably lower than neighbouring Health Board areas. Pressure over the Festive period, due to higher rates being offered in neighbouring Health Boards led to NHS GEMS increasing their rates last year following agreement at Chief Executive level. The agreement was to approach but not leapfrog neighbouring Health Boards as long as those neighbouring Health Boards did not institute pay rises which would widen the gap even further. This agreement worked well and all sessions were filled. NHS GEMS has always had a significant nursing input at Primary Care Centres. Our Primary Care nurses continue to function and to significantly add quality to the service offered within the Primary Care Emergency Centres. In addition we have trained 10 NHS GEMS Nurse Practitioners with the aim that these practitioners will become autonomous practitioners. Our aspiration is that our GNPs will be able to assess patients, come to a management plan decision, prescribe and discharge. Our nurses have completed an accredited course at Caledonian University and we also had input into the design of the course. This has allowed a substantial period of consolidation within the service. Succession planning however is a problem. Full evaluation of this service is ongoing to demonstrate value for money and to ensure that the service meets clinical governance standards. There is an opportunity to improve the skill mix and in particular the educational pathway that has been established could lead to training opportunities for existing acute services staff as ACADs approach. We have, within our service, a well established out of hours Community Psychiatric Nursing Service. This service is available from 8.30pm until 9.30am Monday-Friday and from 4pm until 9am at weekends. The CPN service will take calls directly from NHS 24or from NHS GEMS and offer telephone advice to new and known patients. They will also visit patients at home or see patients at a Primary Care Centre. The service is also responsive to requests from A&E to assess patients with psychiatric problems, for example attempted suicide. This service has been established for many years and is an example of a situation where a patient will be seen by the most appropriate professional in the most appropriate place at the most appropriate time. The CPN service also arranges follow up by day and has a direct link to the various resource centres within Glasgow. The service also has access to the computer database of patients known to Mental Health Services. Although funded through Mental Health the service is sited in our NHS GEMS hub and is recognised as an integral part of the service. We work closely with our Community Pharmacist colleagues and have a system in place which allows the pharmacist to contact the NHS GEMS doctor at the nearest Primary Care Emergency Centre should the pharmacist require advice on a patient presenting with a minor ailment. Should the pharmacist feel that a patient presenting requires a face-to-face contact with a doctor then the pharmacist can write a short note and send the patient directly to the Primary Care Emergency Centre. Should the pharmacist wish to speak to a GP for advice a system is in place to allow contact with the GP in the nearest PCEC. Each PCEC has one receptionist, one security officer, one primary care nurse (until midnight). Our hub has three controllers until midnight when this reduces to two. We have two team leaders who are responsible for the service during operational hours. A small management team share a 1 in 4 rota from home in case of emergency or situations, which the team leader cannot handle. This consists of the Clinical Director, the Operations Manager, and two medical advisors. NHS GEMS currently employ the following staff May 2006 (most are part time):
5
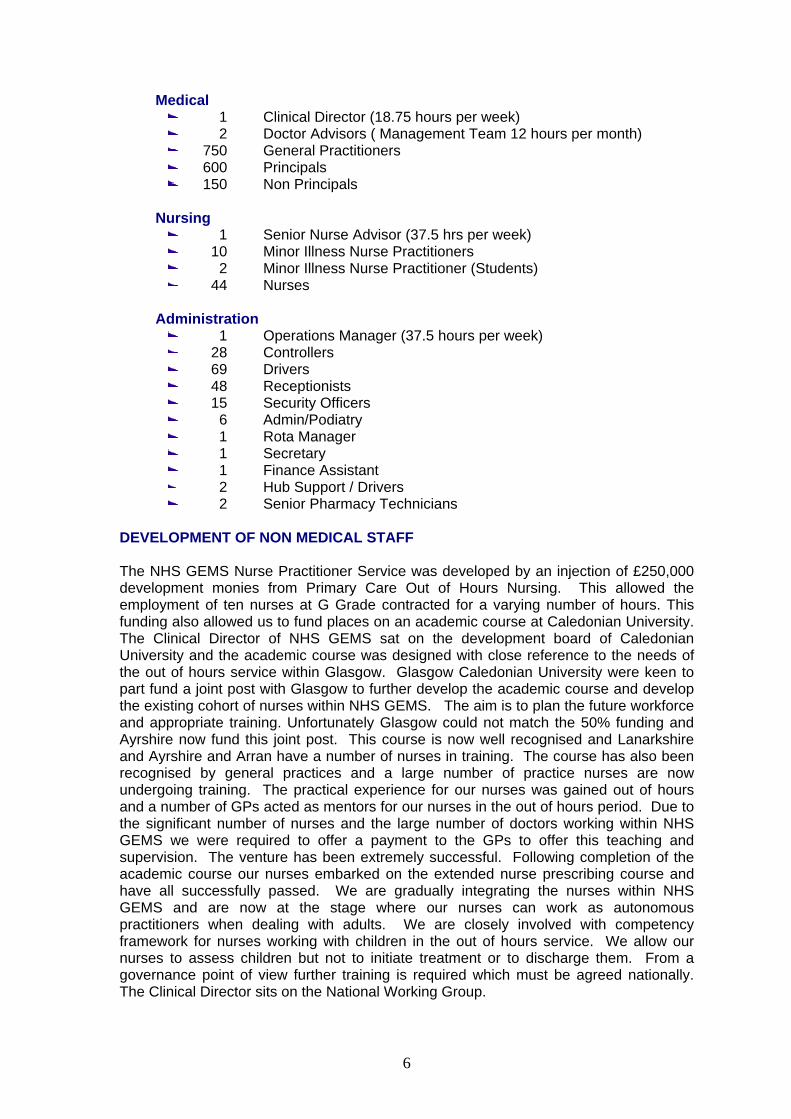
Medical
1 Clinical Director (18.75 hours per week) 2 Doctor Advisors ( Management Team 12 hours per month) 750 General Practitioners 600 Principals 150 Non Principals
Nursing 1 Senior Nurse Advisor (37.5 hrs per week) 10 Minor Illness Nurse Practitioners 2 Minor Illness Nurse Practitioner (Students) 44 Nurses
Administration
1 Operations Manager (37.5 hours per week) 28 Controllers 69 Drivers 48 Receptionists 15 Security Officers 6 Admin/Podiatry 1 Rota Manager 1 Secretary 1 Finance Assistant 2 Hub Support / Drivers 2 Senior Pharmacy Technicians
DEVELOPMENT OF NON MEDICAL STAFF The NHS GEMS Nurse Practitioner Service was developed by an injection of £250,000 development monies from Primary Care Out of Hours Nursing. This allowed the employment of ten nurses at G Grade contracted for a varying number of hours. This funding also allowed us to fund places on an academic course at Caledonian University. The Clinical Director of NHS GEMS sat on the development board of Caledonian University and the academic course was designed with close reference to the needs of the out of hours service within Glasgow. Glasgow Caledonian University were keen to part fund a joint post with Glasgow to further develop the academic course and develop the existing cohort of nurses within NHS GEMS. The aim is to plan the future workforce and appropriate training. Unfortunately Glasgow could not match the 50% funding and Ayrshire now fund this joint post. This course is now well recognised and Lanarkshire and Ayrshire and Arran have a number of nurses in training. The course has also been recognised by general practices and a large number of practice nurses are now undergoing training. The practical experience for our nurses was gained out of hours and a number of GPs acted as mentors for our nurses in the out of hours period. Due to the significant number of nurses and the large number of doctors working within NHS GEMS we were required to offer a payment to the GPs to offer this teaching and supervision. The venture has been extremely successful. Following completion of the academic course our nurses embarked on the extended nurse prescribing course and have all successfully passed. We are gradually integrating the nurses within NHS GEMS and are now at the stage where our nurses can work as autonomous practitioners when dealing with adults. We are closely involved with competency framework for nurses working with children in the out of hours service. We allow our nurses to assess children but not to initiate treatment or to discharge them. From a governance point of view further training is required which must be agreed nationally. The Clinical Director sits on the National Working Group.
6

We are in discussion with the Ambulance Service but have not as yet developed any paramedic integration within NHS GEMS. We have an in house pharmacy service to ensure adequate medication supplies are available within our PCECs sites and in doctors’ bags.
This is professionally supported by the Clinical Director within community pharmacy and directly managed by the Senior Nurse advisor in NHS GEMS. We have two medical support nurses / senior pharmacy technicians who work Monday to Friday to support the home visiting driver service and our six PCECs.
Equipment currently available at our PCEC sites:
26 Doctor Bags, 16 Resuscitation bags for the Home visiting service. 6 Resuscitation Trolleys within the PCECs
The PCECs have drug and equipment stocks (agreed to minimum and maximum stock levels depending on our formulary). PATIENT EXPERIENCE NHS GEMS the Co-op was formed eleven years ago. At that time the steering group included membership from the Local Health Council. The establishment of the out of hours Co-op was discussed widely within the community and was welcomed. The feedback throughout the years from the Health Council has been extremely positive. Local Health Council has always sat on the NHS GEMS Quality Assurance Group that was previously known as the Deputising Sub Committee. This group now has two lay representatives and meets quarterly to discuss statistics and complaints. Patient Satisfaction Questionnaires presented during our recent QIS visit, November 2005 were extremely positive. Through the LHCC structure Out Of Hours was discussed at all local planning meetings as development plans were implemented. A series of meetings have been held to develop a primary care strategy within Glasgow over the last five years. Out Of Hours care featured at each meeting and feedback was obtained and suggestions for development taken on board and fed into the planning process. Our most recent event was at Celtic Park in November 2005 at which over 400 delegates attended. This represented many stakeholders including NHS 24, Acute Services, voluntary agencies, patient representation, LHCC, committee members etc. Feedback from this was collated and sent to all delegates and relevant agencies and was fed into the planning process. A further event is scheduled for November 2006 targeted at the elderly population. This is being co-ordinated by NHS Glasgow Public involvement/Patient Focus department and will explain the role of the NHS GEMS Nurse Practitioner in terms of the OOH service regarding availability and usage. The aim is to discuss with patient’s representatives, NHS 24 and other stakeholders including Social Work Department. A move from Lightburn Hospital to Easterhouse Health Centre for our PCEC involved significant public consultation in autumn 2004/spring 2005. The service was moved successfully.
7

Gaps in the current service have been identified. In particular there is a lack of service for patients with addiction in the out of hours period. The Community Addiction Teams within Glasgow have been established on a 9-5 basis Monday-Friday. Patients with addiction problems telephoning out of hours have only the option of attending the Primary Care Emergency Centre. We feel that the most appropriate professional would not necessarily be a general practitioner and are in discussion with Addiction Services on this matter. ACTIVITY
Calendar year 2004 2005 2006* [January-June]
Advice 47221 55821 34015
CMH 6663 6421 2732
DN0 1759 1993 813
HV 30752 31344 14007
PCC 92961 94895 43183
Speak to GP 7043 9573 5331
Other 44618 31030 2237
Total 231017 231077 102318
CMH = Community Mental Health DN = District Nurse HV = Home Visits PCC = Primary Care Centre
The activity is consistent year on year with no significant increase or decrease. It should be noted however that the number of “Speak to GP” calls is significantly increased from 2004-2005. Part of this is due to the volume of untriaged calls being taken from NHS 24 during this period. YEAR TO 31/3/06 31.3.05 31.3.06
Total number of patient contacts with out of hours service
231,997 233,227
Number of patient phone calls completed as NHS 24 advice only with no further action required
84,070 82,838
Number of patient phone calls completed as GP advice only
8,539 9,061
Number of patient phone calls completed as other local OOH staff advice only.
5.306 5,246
Number of patient contacts who received a home visit by a GP
31.135 30.747
Number of patient contacts who received a home visit from another health care professional
2,439 2,310
Number of patient contacts treated at OOH primary care emergency centres
79,083 76,731
Number of patient contacts that bypassed NHS 24 or local triage and self presented at OOH primary care emergency centre (WALK INS)
17,636 16,294
Number of patients who were provided with transport during OOH period.
3,943 4,698
Total number of A&E attendances during primary care out of hours period.
146,842 148,098
8

NHS GEMS WINTER PLANNING 2005/2006 Planning for peak periods of activity over the festive period and during the winter months began early in 2005 (July). NHS GEMS participated in National Winter Planning meetings and contributed to strategy. The following paragraphs summarise the planning assumptions and document activity and lessons learned. “NHS GEMS Winter Planning 2005/2006” was produced in July 2005 and is reported in full. 1. REVIEW OF STATISTICS FROM 2004-05
The review enabled us to look closely at each day of the holiday and examine numbers of patients referred to NHS GEMS on an hour by hour basis. The statistics show actual time of referral but not actual time of attendance at NHS GEMS. We also have statistics available as far back as 1999 and have addressed these in our planning. Only one festive period when Christmas was day 2 of holiday. The main learning points were:
Early morning period was less busy than anticipated. Only one GP in Primary Care Centres mid to late evening (except Victoria). No influenza epidemic. Weather favourable. GP sessions were filled late due to initially under-pricing. Extra NHS 24 triage sessions requested at a late stage. Due to this timing,
these sessions required to be offered at a higher pay rate. This caused discontent amongst staff who had already contracted to work sessions.
NHS GEMS doctors triaged significant numbers of untriaged calls sent from NHS 24. The total number of calls triaged by NHS GEMS was 2,376.
2. ANTICIPATED DIFFERENCES THIS YEAR 2005-06
Four day break covering different actual days. Day 2 is Christmas and New Year’s Day (as opposed to day 1 last year). Due to the potential for NHS 24 call back we need to plan to staff relatively
higher later in the day. 3. PLAN FOR EACH DAY
Day 1: Christmas Eve and Hogmanay will be staffed as a normal Saturday staffing level. Day 2: Christmas Day is anticipated to be busier than usual as it falls on second day of a holiday. We will therefore increase our staffing complement to allow two “ back-up “GPs throughout the whole day and one”back-up” GP overnight. We will have a peripatetic GP in the call centre throughout the day. In anticipation of NHS 24 call back, the GP can move to the busiest site or carry out house calls as well as dealing with some untriaged calls if required. Day 2: New Year’s Day. This will be staffed at a higher level than Christmas Day as it is traditionally busier and as it is day 2 of the holiday it will be staffed higher than last year. The peripatetic GP will be engaged on similar basis to Christmas Day. Day 3 & Day 4 of both weeks will be staffed to a high level equivalent to last year with increased staffing levels, compared to last year, towards the end of the day.
9

Extra doctors could be employed as peripatetic GPs dealing with untriaged calls from NHS 24 and being available for flexible deployment to sites (all cars being utilised) should the need arise. Recruitment of such GPs will require to be carried out at same time as original rota bids. ie from mid September.
4. ROTAS
The rotas matched activity to doctors available throughout the holiday period. It is extremely difficult to find doctors at short notice so we have to anticipate the possible worst case scenario – although NHS 24 performance and influenza epidemic are difficult to quantify, extra back up and peripatetic doctors are a safety net. Peripatetic GPs will be utilised by NHS 24 for untriaged calls.
5. RATES OF PAY
The first day of the holiday will be paid to doctors as a public holiday rate equivalent to that paid over the four-day Easter break time. We anticipate difficulties filling these sessions and to counteract this offer a higher rate of pay than a normal Saturday (which would not be attractive). Days 3 and 4 of both holidays will be paid at the same rate as Boxing Day last year. Christmas and New Year rates are equivalent to last year. There has been agreement at the OOH operational group to avoid substantial increases in the hourly rate compared to last year. On this basis the rates quoted are thought to be competitive.
6. NHS 24
At a recent meeting of West of Scotland Out of Hours Co-ordinating Group, the Chief Executive of NHS 24 reported on a recent meeting with Chief Executives of Health Boards. It is recognised that NHS 24 are highly unlikely to be able to deliver fully over the festive period due to various reasons including recruitment. It is anticipated therefore that call-back will be a major feature and the Chief Executive has asked that NHS Boards recognise that there will be a gap in service. It has been agreed that it is the NHS Board who will be accountable for this gap in service. It is therefore our responsibility to have plans in place to meet this gap.
Last year we invited doctors to triage within NHS GEMS and we suggest that we should invite doctors for the four day period over the festive period. This year we would suggest that on day 3 and 4 of the holiday we anticipate a very large call volume and require 70 hours of doctor time to perform triage function throughout the day each day. The doctors would work approximately six-hour sessions. The pay rate should be the same as that paid to our GP advisor. In addition we suggest the doctors throughout the day be employed initially as triagers but should the need arise move them to sites as an extra pair of hands. This system worked well last year. On Hogmanay and Christmas Eve we anticipate a normal, perhaps slightly busier Saturday. It would not be our intention to recruit GPs to help with triage at this time but were we to do so then the cost would be the same as our GP advisor per hour and the GPs would be involved in six-hour sessions. Anticipating that NHS 24 may require from NHS GEMS on this day we would suggest four extra doctors to undergo triage, which is 24 hours per day.
10

Christmas Day is traditionally difficult to recruit to fill sessions. We would suggest the employment of two extra doctors on this day who should be peripatetic in that they could assist with triage or be moved to sites or house visiting if required. This would help us cope with any potential late shift of calls due to excessive call back. As NHS GEMS will be unable to provide substantial triage support it is hoped that NHS 24 will be able to staff up on Christmas Day, which will be the quietest of the eight-day holiday. New Year’s Day we anticipate will be busy and suggest two extra doctors offering triage. In addition to doctor triage we employed nurse triage last year and at an early stage we would suggest writing to the nurses involved asking them to perform a triage function over this holiday period. The Nurse Advisor will take this forward. The pay rate to nurses should be a national one and should be agreed by NHS 24 across all sites. It was brought to our attention last year that the nurses were relatively unhappy in that they were performing the same task as a doctor but being paid significantly smaller amounts.
7. INFLUENZA IMMUNISATION
NHS GEMS should encourage staff to be immunised for influenza vaccination. This can be done through Occupational Health in the Health Board or through the patient’s own general practitioner. We will write to staff encouraging this.
8. PUBLICITY
Through the Health Board Winter Planning Groups the usual local documentation should be prepared and sent out for public information over the festive period.
A joint letter should be sent at an early stage from the GP Sub Committee and NHS GEMS NHS reminding GPs of their contractual obligation to remain available for patients up to 6pm on 23 December and 30 December and for the three day period between Christmas and New Year holidays.
9. NHS GEMS NURSE PRACTITIONERS In October an exercise will be carried out to determine where and when our nurse practitioners would be of most value to us over the festive period. The consolidation period will not yet have been completed but the nurses could prove a valuable resource during the festive period. Should sites become excessively busy then nurses could help in the initial triage of patients. If NHS 24 and our own triage arrangements are unable to cope with the volume of calls then patients may be asked to attend centres untriaged. Plans should be put in place now to determine nursing availability over this period. Patients would be seen initially by nursing staff at the PCECs.
11

10. NURSING HOME TEAM
An approach has been made to the lead consultant with a view to having a Nursing Home Team available during day 4 of the holiday. This could remove significant pressure from NHS 24 and NHS GEMS. It is doubtful if existing assisting general practices could be persuaded to cover homes over this festive period but this suggestion will also be made.
Attached is our predicted workload over the festive period, which has been calculated following examination of previous years’ workload.
11. COSTS
The cost of allocating peripatetic GPs last year was met by NHS 24 and we would seek additional funding this year. We have increased staffing levels later in the day at several sites due to the effects of call back last year. We will be seeking additional funding from NHS 24 this year and are confident that the cost of any additional GP triage sessions will be met by NHS 24.
12. RECRUITMENT OF DEPUTIES
We anticipate difficulty filling all sessions. Pay rates may become an issue as other boards have yet to publish their rates, although there is a level of agreement at OOH Operational Group. We have negotiated with a German recruitment agency and hope to introduce 2 doctors in September and October with a view to engaging over the festive period. WORKLOAD REPORT - FESTIVE PERIOD 2005/2006
Planning began in July 2005. Excellent co-operation at National level between out of hours providers, NHS 24, Scottish Executive. NHS GEMS received support from Primary Care Division in developing Winter Plan. Intervention at NHS Board Chief Executive level allowed a realistic competitive pay scale for doctors to be achieved in co-operation with other Health Board areas. Staffing levels were determined using previous year’s statistics and learning. Analysis of hourly call rates at each PCEC in previous years informed need to increase staffing levels at particular times. NHS 24 requested that NHS GEMS take untriaged calls over the festive period. NHS GEMS established a rota for untriaged calls based on previous year. The doctor rota was full by end of November. This reflected the realistic pay rates and the increased pool of doctors due to last year’s registrars becoming NHS GEMS deputies. NHS 24 introduced a Simul-8 modelling tool which attempted to inform out of hours providers of predicted workload.
12

STATISTICS
The comparable days are days 3 and 4 of holiday period with a breakdown at Appendix B.
CHRISTMAS
Day 3 (03)
Day 3 (04)
Day 3 (05)
Day 4 (03)
Day 4 (04)
Day 4 (05)
House Visits
263 223 228 228 220 281
PCEC Attendance
944 721 993 663 671 1,132
Triaged at NHS GEMS
- 408 391 - 577 580
NEW YEAR -2006
Day 3 (04)
Day 3 (05)
Day 3 (06)
Day 4 (04)
Day 4 (05)
Day 4 (06)
House Visits
276 269 266 269 203 288
PCEC Attendance
849 769 1,181 616 710 1,088
Triaged at NHS GEMS
- 518 474 - 599 500
SIMUL 8 prediction of untriaged calls to be passed to NHS GEMS was: 1,421 Actual calls passed: 3,526 At 10 calls per hour per GP NHS GEMS had built in a capacity of 4,480 At New Year 62% of contacts with NHS 24 resulted in a face to face contact at NHS GEMS NHS. SIMUL 8 predicted 46% face to face contacts. Of New Year Day 4 - PCEC contacts up 47% compared to 2005. SIMUL 8 AS PREDICTOR OF OOH WORKLOAD
TOTAL CALLS UNTRIAGED TO PARTNERS
HOME VISITS PCEC
CHRISTMAS SIMUL 8
Actual SIMUL 8 Actual SIMUL 8 Actual SIMUL 8 Actual
7,722 6,049 817 1,626 1,293 861 2,644 * 2,891 NEW YEAR
SIMUL 8
Actual SIMUL 8 Actual SIMUL 8 Actual SIMUL 8 Actual
7,554 6,663 604 1,900 1,335 953 2,723 * 3,245
* Excludes self presenting patients
13

TOTAL FACE TO FACE CONSULTATIONS
CHRISTMAS PCEC HOME VISITS
2003 2,769 939 2004 2,348 745 2005 2,891
*3,395 861
* Includes self presenting patients
NEW YEAR
PCEC HOME VISITS
2004 2,844 1,015 2005 2,572 879 2006 3,245
*3,729 953
* Includes self presenting patients
Lessons Learned From Festive Period 2005/06: 1. Increased workload requires high medical staffing by OOH provider 2. Need to try to increase home care advice and reduce un-necessary attendance at
OOH provider 3. Glasgow may struggle to find manpower to continue to provide such a high volume
of untriaged calls and we look to NHS 24 to improve nurse advisor staffing levels urgently.
4. We ask NHS 24 to improve the priority allocation to home visits as too many calls
passed inappropriately as high priority during the busy festive period–meaning OOH providers cannot meet own KPIs and operationally causes difficulties.
5. NHS 24 Satellite centres reported as working well with much better co-operation
and clinical feedback resulting in high motivation to reach mutual aspirations. Glasgow do not have satellite centres.
6. Working with partners, not only NHS 24 but NHS as a whole has been extremely
rewarding this year. The overall picture is that NHS 24 met all KPIs. NHS 24 staff report high morale and a well organised festive period in comparison to last year. OOH providers stress that the workload was higher than last year with providers at times stretched due to the volume of attendances and house calls. Good planning and extreme hard work and commitment by all OOH staff resulted in a clinically safe service coping with more contacts than ever before.
14
ONGOING TRIAGE NHS 24 has requested ongoing triage from NHS GEMS through to March 2007. Therefore seven sessions of triage are provided every Saturday. This provides capacity to deal with 400 untriaged calls. WINTER PLAN A robust winter plan was produced by Primary Care Division. JOINT PLANNING Excellent relationship has been established with NHS 24, which allows joint planning for Easter and holiday weekends. July 2006 will be a particular challenge with depletion of GP workforce during the traditional holiday period. CLINICAL AND HEALTHCARE GOVERNANCE Due to the transfer of NHS GEMS the co-op to NHS GEMS as part of the Primary Care Division it has been challenging to become embedded into governance structure. Traditionally NHS GEMS the co-op reported to the Deputising Sub Committee of the Area Medical Committee. On transfer to NHS GEMS this committee was disbanded and NHS GEMS reported into Primary Care Clinical Governance Committee. During the period of re-organisation within NHS Glasgow it has indeed been difficult to engage in a co-ordinated governance agenda. Significant events, statistics, guidelines, changes of policy, practice, complaints handling and IR1 reporting are all the responsibility of NHS GEMS management team and the responsibility of the Clinical Director. The Clinical Director sits in Primary Care Clinical Governance Committee and reports directly to the Chair of the Committee. The previous Deputising Sub Committee was a robust quarterly scrutinisation of GESM and NHS 24 statistics and of complaints. This group was re-established October 2005 as NHS GEMS Quality Assurance Group and the minutes sent to Primary Care Clinical Governance Committee. The group has GP, A&E, nursing, LMC, CPN, NHS 24 and lay representation. COMPLAINTS A total of 23 complaints handled April 05 - March 06 (compared to 22 handled April 04 - March 05), all with local resolution. Learning points are disseminated throughout the organisation in a structured way and documented in each complaint file. SEA Significant events are actioned by NHS GEMS Management Team. Significant clinical events would be sent to Clinical Governance Committee. There have been no significant events in this period. INCIDENT REPORTS There is a robust system for IR1 reporting with local actions being implemented by NHS GEMS Management Team. IR1 forms are sent centrally and included in central recording.
15
HEALTH AND SAFETY All NHS GEMS sites are Health Board owned premises and full risk assessment has taken place. INFORMATION TECHNOLOGY NHS GEMS is linked to NHS 24 IT. Systems and all data are transferred electronically. NHS GEMS uses the Knightowl system at hub and in PCECs. Information is dispatched from the hub to in car IT technology known as *. Knightowl is a system that preceded Adastra versions 2 and 3. It has some benefits over these systems in report generation. It is the intention of NHS GEMS to convert to Adastra version 3 at the earliest opportunity. This would allow clinicians to enter data at the time of consultation. EMERGENCY CARE SUMMARY NHS GEMS can access ECS. This system provided details:
Demographics Repeat prescribing Acute prescribing Allergies
This was rolled out in NHS GEMS November 2005. QUALITY IMPROVEMENT SCOTLAND (QIS) QIS submission was prepared in Autumn 2005 and visit took place November 2005. NHS GEMS was assessed s Level 3 - “largely compliant with standards”. An action plan has been submitted to address areas of the service which are not yet fully compliant. Level 3 was regarded as a most satisfactory outcome by the Clinical Governance Committee. STAFF GOVERNANCE All staff undergo Disclosure checks and have staff induction and training on joining the service. Currently work is underway to ensure Personal Development Planning takes place. This is challenging in a service where the majority of staff are part time and have other daytime jobs. All doctors working for NHS GEMS have an annual appraisal under the National GP Appraisal Scheme. FINANCIAL GOVERNANCE Financial Governance is the responsibility of the Primary Care Division, Director of Finance. Day to day financial management is devolved to NHS GEMS Management Team. Superannuation regulations regarding out of hours income have been clarified in year and this has led to guidance being issued by NHS GEMS/PCD Finance to all GPs and locums. NHS GEMS session rate is now a gross rate, which includes the employer’s superannuation contribution.
16
17
FUTURE DEVELOPMENTS Closer working/integration with NHS 24. In other health board areas satellite centres have been established with NHS 24 triage function becoming a local board responsibility. This system is reported as working well. NHS Glasgow is keen to explore similar integration with NHS 24. Closer working/integration with Clyde PCECs During 2006/2007 NHS GEMS will work with Clyde PCEC to establish a plan for integration of the two services. Development of feedback to clinicians A challenge to all OOH organisations is to establish a robust system of feedback to clinicians on clinical cases. A robust method of feedback of problematic cases does exist but we are exploring ways to feedback on a routine basis. Move to Acute Division From April 2006 NHS GEMS will be sited within the Acute Division of the re-organised NHS Board. This will present challenges as we form and establish new relationships.

APPENDIX A
18
SUMMARY OF NHS GEMS COST SBREAKDOWN OF ACTIVITY OVER CHRISTMAS PERIOD
2003/04 2004/05 Before
the date of transfer of
responsibilities
2004/05 From the date of transfer of
responsibilities
2005/06 2006/07
£000
000
£000
Budget £0000
Actual £000
Financial Year budget
£000
Actual spend to July 2006
£000
Current Year projection
£000 Total cost of OOH services in the board area (this includes the board contribution and the contribution made by GP OOH organisations).
5,840
1,947
Contribution by GP OOH organisations to the cost of OOH services, eg co-operatives etc
4,523
1,508
Contribution by the board to the cost of OOH services
1,317
347
4,905
7,311
7,282
7,872
2,625
7,872

APPENDIX A [cont’d]
BREAKDOWN OF COSTS
2005/06 Direct service provision Budget £000 Actual £000
Total OOH capital costs 0 0
Total OOH revenue costs 7,311 7,744
How these revenue costs are made up.
Salaries (ie all board directly employed staff) 2,637 2,812
Sessional staff payments for OOH work 3,980 4,175
Premises 217 227
Patient Transport 104 100
Staff Transport/Travel 21 21
IT revenue (ie investment of OOH, eg software) 35 107
Staff education, training and development 9 2
Depreciation 0 0
Management and administration costs 260 262
Drugs and medical supplies 20 9
Other revenue costs 28 11
Total OOH costs to boards for services provided by GP practices who have not opted out of providing OOH services.
7,311
7,726
Total OOH costs for services provided by other OOH service providers, excluding GP practices that have not opted out of OOH service provision.
0
18
19

20
FUNDING OF PRIMARY CARE OOH SERVICES 2005/06
Budget £000
Actual £000
Unified budget (OOH contribution) 1,833 1,833
PMS allocation (OOH contribution) 0 0
GP fees 6% claw back 3,300 3,300
OOH development fund 1,800 1,800
Other funding for OOH 378 349
Total funding for OOH services 7,311 7,282
APPENDIX A [cont’d]

BREAKDOWN OF ACTIVITY OVER CHRISTMAS PERIOD
24/12/2005 25/12/2005 26/12/2005 27/12/2005 Total Home Visits 208 15% 144 16% 228 14% 281 13% 861
Advice 324 23% 291 33% 433 26% 553 26% 1601 PCECs 679 47% 396 45% 839 51% 977 47% 2891
Speak to Doctor 156 11% 24 3% 96 6% 202 10% 478 Other 67 5% 18 2% 51 3% 82 4% 218
Total From NHS 24 1434 100% 873 100% 1647 100% 2095 100% 6049 CPNs/ Direct
Access 12 10 25 17 64 Walkins 128 16% 67 14% 154 16% 155 14% 504
Total PCECs 807 463 993 1132 3395 Total Contacts 1574 950 1826 2267 6617
The figures above show the disposition of all contacts handled by NHS 24 over the four day Christmas period The figures below show the untriaged calls passed to us by NHS 24 and the disposition of the calls triaged by our own GPs. These
figures are a sub set of the figures above and should not be added. Home Visits 48 11% 13 6% 24 6% 31 5% 116
Advice 139 31% 82 41% 118 30% 251 43% 590 PCECs 252 56% 103 51% 247 63% 288 50% 890 Other 15 3% 3 1% 2 1% 10 2% 30
Total Untriaged 454 100% 201 100% 391 100% 580 100% 1626 Card 87 30 103 130 Drum 112 58 126 170 East 95 54 150 167 Stob 182 140 218 232 Vic 248 152 288 323
West 60 22 103 100 Total 784 55% 456 #REF! 988 #REF! 1122 #REF! 3350
APPENDIX B
21

22
BREAKDOWN OF ACTIVITY OVER CHRISTMAS PERIOD [cont’d]
31/12/2005 01/01/2006 02/01/2006 03/01/2006 Total Home Visits 194 13% 205 17% 266 14% 288 14% 953
Advice 345 24% 300 25% 468 24% 586 29% 1699 PCECs 695 48% 574 48% 1050 53% 926 45% 3245
Speak to Doctor 141 10% 92 8% 118 6% 180 9% 531 Other 78 5% 30 2% 62 3% 65 3% 235
Total From NHS 24 1453 100% 1201 100% 1964 100% 2045 100% 6663
CPNs/ Direct Access 22 20 15 13 70 Walkins 99 12% 92 14% 131 11% 162 15% 484
Total PCECs 794 666 1181 1088 3729
Total Contacts 1574 1313 2110 2220 7217
The figures above show the disposition of all contacts handled by NHS 24 over the four day New Year period The figures below show the untriaged calls passed to us by NHS 24 and the disposition of the calls triaged by our own GPs. These figures
are a sub set of the figures above and should not be added. Home Visits 29 6% 53 12% 32 7% 29 6% 143
Advice 146 30% 141 32% 138 29% 239 48% 664 PCECs 306 62% 235 54% 300 63% 226 45% 1067 Other 9 2% 7 2% 4 1% 6 1% 26
Total Untriaged 490 100% 436 100% 474 100% 500 100% 1900
APPENDIX B

23










![Draft NHS Model Complaints Handling Procedure [word version]library.nhsggc.org.uk/media/263263/nhsggc-complaints... · Web viewDraft NHS Model Complaints Handling Procedure [word](https://img.pdfslide.us/doc/110x75/60e065363c8ec162db186f93/draft-nhs-model-complaints-handling-procedure-word-version-web-view-draft-nhs.jpg)