Embed Size (px)
Citation preview

The NHS Outcomes Framework 2015/16
December 2014

Title: The NHS Outcomes Framework 2015/16
Author: NHS Group, Department of Health FN-NHSG-NHSCPS-17185
Document Purpose: Policy
Publication date: December 2014
Contact details: NHS Outcomes Framework, NHS Group, Department of HealthRoom 234, Richmond House79 WhitehallLondon SW1A [email protected]
You may re-use the text of this document (not including logos) free of charge in any format or medium, under the terms of the Open Government Licence. To view this licence, visit www.nationalarchives.gov.uk/doc/open-government-licence/
© Crown copyright
Published to gov.uk, in PDF format only.
www.gov.uk/dh
Contents
Introduction 2
Background 3
Assessing NHS England’s progress using the NHS Outcomes Framework 5
Clinical Commissioning Group Outcome Indicator Set 5
Reviewing the NHS Outcomes Framework 6
Review process for the NHS Outcomes Framework 2015/16 6
Next steps on the NHS Outcomes Framework 6
Changes across each domain 7
Domain 1 8
Domain 2 10
Domain 3 12
Domain 4 15
Domain 5 17
NHS Outcomes Framework – at a glance 19

2 The NHS Outcomes Framework 2015/16
Introduction
1. The NHS Outcomes Framework, alongside the Adult Social Care and Public Health Outcomes Frameworks, sits at the heart of the health and care system. The NHS Outcomes Framework:
• provides a national overview of how well the NHS is performing;
• is the primary accountability mechanism, in conjunction with the mandate, between the Secretary of State for Health and NHS England; and
• improves quality throughout the NHS by encouraging a change in culture and behaviour focused on health outcomes not process.
2. The NHS Outcomes Framework was developed in December 2010, following public consultation, and has been updated annually. Refreshing the NHS Outcomes Framework allows it to become a tool which reflects the current landscape of the health and care system, and to be better suited to approach the many challenges that the system faces.
3. This document sets out the updated NHS Outcomes Framework for 2015/16. It is being published alongside the mandate to NHS England for 2015/16. It is also accompanied by a Technical Appendix which provides detailed information about the indicators still being developed for the framework.
4. This year’s refresh of the NHS Outcomes Framework is on a larger scale than previous years. As part of this review we engaged with stakeholders over the summer, and have published a summary of what we heard and the Department’s response alongside this document.
Background 3
Background
5. The NHS Outcomes Framework is a set of 68 indicators which measure performance in the health and care system at a national-level. It is not intended to be an exhaustive list of health indicators. Rather, it has been designed to be a set of outcomes that together form an overarching picture of the current state of health and care services in England. This also means that the NHS Outcomes Framework must remain parsimonious so as not to undermine the rationale for the framework, as a whole, in providing a focus for accountability and improvement.
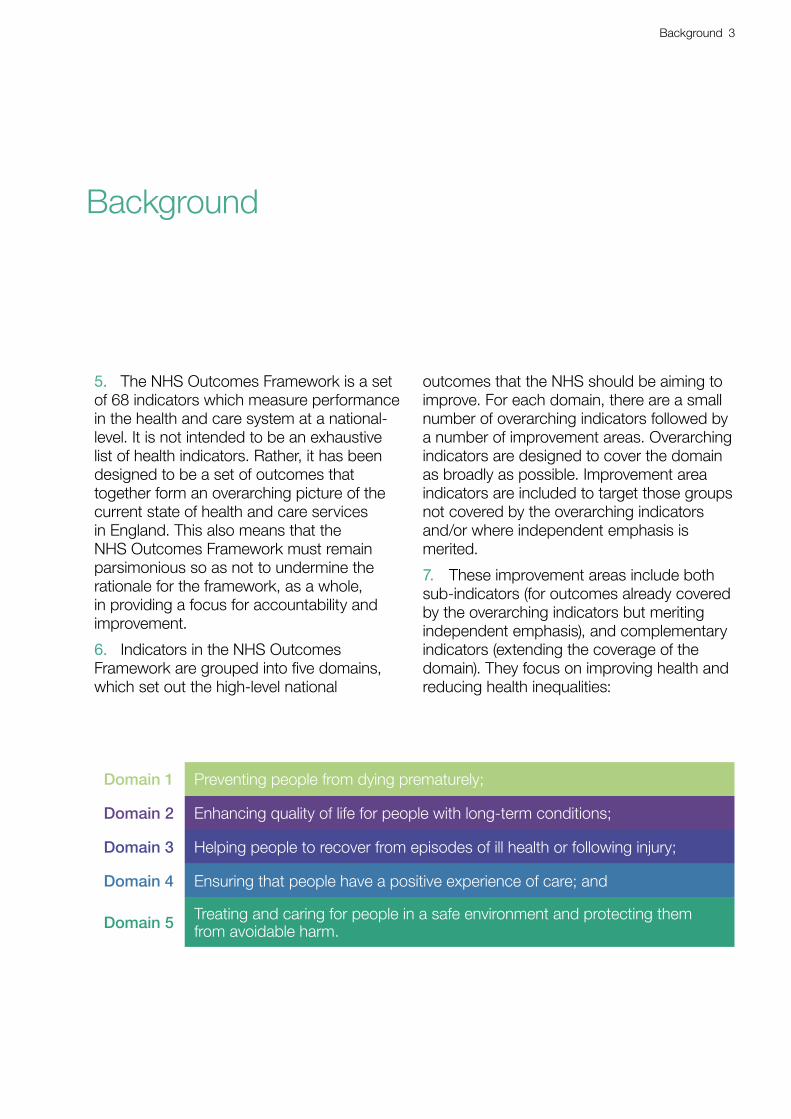
6. Indicators in the NHS Outcomes Framework are grouped into five domains, which set out the high-level national
outcomes that the NHS should be aiming to improve. For each domain, there are a small number of overarching indicators followed by a number of improvement areas. Overarching indicators are designed to cover the domain as broadly as possible. Improvement area indicators are included to target those groups not covered by the overarching indicators and/or where independent emphasis is merited.
7. These improvement areas include both sub-indicators (for outcomes already covered by the overarching indicators but meriting independent emphasis), and complementary indicators (extending the coverage of the domain). They focus on improving health and reducing health inequalities:
Domain 1 Preventing people from dying prematurely;
Domain 2 Enhancing quality of life for people with long-term conditions;
Domain 3 Helping people to recover from episodes of ill health or following injury;
Domain 4 Ensuring that people have a positive experience of care; and
Domain 5 Treating and caring for people in a safe environment and protecting them from avoidable harm.
4 The NHS Outcomes Framework 2015/16
8. Each year since the NHS Outcomes Framework was first published in 2010, the Department of Health has been improving the framework by refining existing indicators and developing new indicators. These changes have helped improve the scope and coverage of the NHS Outcomes Framework, alignment with the mandate to NHS England,1
and alignment with the two other outcomes frameworks – the Public Health Outcomes Framework (PHOF)2 and the Adult Social Care Outcomes Framework (ASCOF).3
9. The Public Health Outcomes Framework and the Adult Social Care Outcomes Framework reflect the different delivery systems and accountability models for public health and adult social care but have the same overarching aim of improving the outcomes that matter to people. The Department continues to work to align the frameworks to encourage collaboration and integration, both in terms of how shared and complementary indicators are presented across all three frameworks, and through an increased and more systematic use of shared and complementary indicators.
10. These three outcomes frameworks are supported by Education Outcomes, which set the education and training outcomes for the health and care system as a whole. Education Outcomes have an enabling role across the whole system and aim to measure progress in education, training and workforce development and the consequential impact on the quality and safety of services for patients and service users.
1 https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/256406/Mandate_14_15.pdf
2 https://www.gov.uk/government/publications/healthy-lives-healthy-people-improving-outcomes-and-supporting-transparency
3 https://www.gov.uk/government/publications/adult-social-care-outcomes-framework-2014-to-2015

Assessing NHS England’s progress using the NHS Outcomes Framework 5
Assessing NHS England’s progress using the NHS Outcomes Framework
11. The NHS Outcomes Framework forms an essential part of the way in which the Secretary of State for Health holds NHS England to account. It has been designed to be the primary assurance mechanism to assess the progress of NHS England at a national level, meaning that the limited number of indicators and the type of data collected by them must represent the NHS service users, and the challenges faced by the NHS, as effectively as possible.
12. As a part of this, the NHS Outcomes Framework plays a key role in assessing progress against the mandate to NHS England,4 a document published by the Department of Health which sets out the key objectives for NHS England.
13. The mandate is structured around the five domains of the NHS Outcomes Framework and as such, progress against objectives in the mandate is assessed using the NHS Outcomes Framework. Furthermore, there is an objective in the mandate for NHS England to demonstrate progress against the five domains and all of the indicators in the NHS Outcomes Framework including, where possible, by comparing our services and outcomes with the best in the world.
14. It is then for NHS England, working with Clinical Commissioning Groups and others, to determine how best to deliver improvements against the mandate and how they do this is set out in their annual business plan.5
4 https://www.gov.uk/government/publications/nhs-mandate-2014-to-2015
5 The latest version of the business plan can be seen at: http://www.england.nhs.uk/wp-content/uploads/2013/04/ppf-1314-1516.pdf
15. The Department of Health holds NHS England to account and is continually reviewing progress against the mandate objectives, and this is informed by data from the NHS Outcomes Framework. In assessing NHS England’s progress, success will be measured not only by the average level of improvement but also by progress in reducing health inequalities and unjustified variation. Each year, the Secretary of State publishes an annual assessment of NHS England’s progress.6.
Clinical Commissioning Group Outcomes Indicator Set
16. NHS England has developed the Clinical Commissioning Group Outcomes Indicator Set (CCG OIS) to support the NHS Outcomes Framework. The CCG Outcomes Indicator Set comprises NHS Outcomes Framework indicators that can be measured at CCG level as well as additional indicators developed by NICE and HSCIC. These provide clear, comparative information to support CCGs, and Health and Wellbeing Boards identify local priorities and demonstrate progress on improving outcomes, as well as delivering public transparency about local health services.
6 The first annual assessment was published in July 2014 and can be seen here: https://www.gov.uk/government/publications/nhs-england-assessment-of-performance
6 The NHS Outcomes Framework 2015/16
Reviewing the NHS Outcomes Framework
Review process for the NHS Outcomes Framework 2015/16
17. The changes that we have made to the NHS Outcomes Framework this year (described in the subsequent chapter of this document) have been informed by advice received by the Outcomes Framework Technical Advisory Group (OFTAG) and engagement with stakeholders held in the summer. This stakeholder engagement was in the form of feedback from the events themselves, as well as written responses received to the document which set out our proposed changes, which was published online.7
18. To see how your feedback has shaped this year’s refresh of the NHS Outcomes Framework, please see the accompanying document entitled NHS Outcomes Framework 2015-16: What we heard and the Government’s response.
Next steps on the NHS Outcomes Framework
19. Within the Department of Health, work is underway to look at how the three outcomes frameworks (the Public Health, Adult Social Care and NHS Outcomes Frameworks) collectively provide an overview of the health
7 https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/341391/14-07-30_NHS_Outcomes_Framework_Stakeholder_Engagement_Document.pdf
and care system, and how they could be improved. Feedback we received on the future role of outcomes frameworks will be used to inform this work, and in the future we would expect to carry out a larger refresh of all three frameworks.
Changes across each domain 7
20. This section of the document describes the changes being made to the NHS Outcomes Framework for 2015/16. Changes are shown in green in the table for each domain, and are explained in the text below each table. The table also indicates which indicators are shared with the Public Health Outcomes Framework (PHOF) or the Adult Social Care Outcomes Framework (ASCOF).
21. We intend to identify key health inequalities measures, based on NHS Outcomes Framework indicators, following the stakeholder engagement exercise over the summer. These will be integral to assessing NHS England’s progress using the NHS Outcomes Framework. We are progressing work on this set with a view to publishing the outcome before the NHS Outcomes Framework takes effect in April 2015.
22. A small number of new indicators have been added, but overall changes have been kept to a minimum, in line with the stable mandate to NHS England for 2015/16. The accompanying Technical Appendix provides further details on all changes to the framework.
23. There are no longer any placeholder indicators in the NHS Outcomes Framework – all indicators are either live or in development. Indicators in development are shown in italics.
Changes across each domain

8 The NHS Outcomes Framework 2015/16
Domain 11. Preventing people from dying prematurelyOverarching indicators
1a Potential years of life lost (PYLL) from causes considered amenable to healthcare
i Adults ii Children and young people
1b Life expectancy at 75
i Males ii Females
1c Neonatal mortality and stillbirths
Improvement areas
Reducing premature mortality from the major causes of death
1.1 Under 75 mortality rate from cardiovascular disease (PHOF 4.4*)
1.2 Under 75 mortality rate from respiratory disease (PHOF 4.7*)
1.3 Under 75 mortality rate from liver disease (PHOF 4.6*)
1.4 Under 75 mortality rate from cancer (PHOF 4.5*)
i One- and ii Five-year survival from all cancers
iii One- and iv Five-year survival from breast, lung and colorectal cancer
v One- and vi Five-year survival from cancers diagnosed at stage 1&2 (PHOF 2.19**)
Reducing premature death in people with mental illness
1.5 i Excess under 75 mortality rate in adults with serious mental illness (PHOF 4.9*)
ii Excess under 75 mortality rate in adults with common mental illness
iii Suicide and mortality from injury of undetermined intent among people with recent contact from NHS services (PHOF 4.10**)
Reducing deaths in babies and young children
1.6 i Infant mortality (PHOF 4.1*)
ii (previously 1.6.iii) Five-year survival from all cancers in children
Reducing premature death in people with a learning disability
1.7 Excess under 60 mortality rate in adults with a learning disability

Changes across each domain 9
Children and young people
Change made: Move indicator 1.6.ii ‘Neonatal mortality and stillbirths’ to become overarching indicator 1c.
Why we made this change: Neonatal mortality is not covered by the existing overarching indicators 1a, ‘Potential years of life lost (PYLL) from causes considered amenable to healthcare’, or 1b, ‘Life expectancy at 75’. It has therefore been moved to become an overarching indicator for the domain to reflect this.
Cancer survival
Change made: Add two new in development indicators for one- and five-year survival from cancers diagnosed at stages 1 and 2 (1.4.v and 1.4.vi).
Why we made this change: Indicators 1.4.i ‘One’ and ii. ‘Five-year survival from breast, lung and colorectal cancer’ are likely to suffer from lead time bias (the measure of survival can be improved by diagnosing earlier without postponing mortality) and length bias (the measure of survival can be improved by diagnosing a higher proportion of less aggressive cancers rather than postponing mortality) – the Technical Appendix to this document provides a more detailed explanation. Measuring survival at stages 1 and 2 provides us with more complete information to facilitate an assessment of cancer survival outcomes.
Mental health
Change made: Add a new in development indicator 1.5.ii for ‘excess under 75 mortality rate in adults with common mental illness’.
Why we made this change: It is estimated that 6 million people in the UK have a common mental illness.8 In addition, people with common mental illness have a mortality rate over 1.7 times that of the general population. The Government’s mandate to NHS England has an objective for NHS England to work towards parity of esteem for physical and mental health, and this indicator would sit alongside the existing indicator for excess mortality among patients with serious mental illness to measure progress towards this goal. This indicator is part of a commitment to improving the coverage of mental health indicators which has formed a key part of this review.
Change Made: Add a new in development indicator 1.5.iii for ‘suicide and mortality from injury of undetermined intent among people with recent contact from NHS services’.
Why we made this change: The Department believes that the NHS has a role in preventing suicide and increasing access to mental health services for those at risk. There is evidence that the NHS can influence outcomes in suicide when they have had contact with people beforehand. For example, effective care planning prior to discharge from hospital, early follow-up appointments and health professionals ensuring the adverse events that preceded the admission have been addressed could all reduce suicides. Currently the NHS Outcomes Framework does not capture suicides, apart from those in contact with secondary mental health services (indicator 1.5.i).
8 IAPT three-year report: the first million patients (2012) p.12 http://www.iapt.nhs.uk/silo/files/iapt-3-year-report.pdf
10 The NHS Outcomes Framework 2015/16
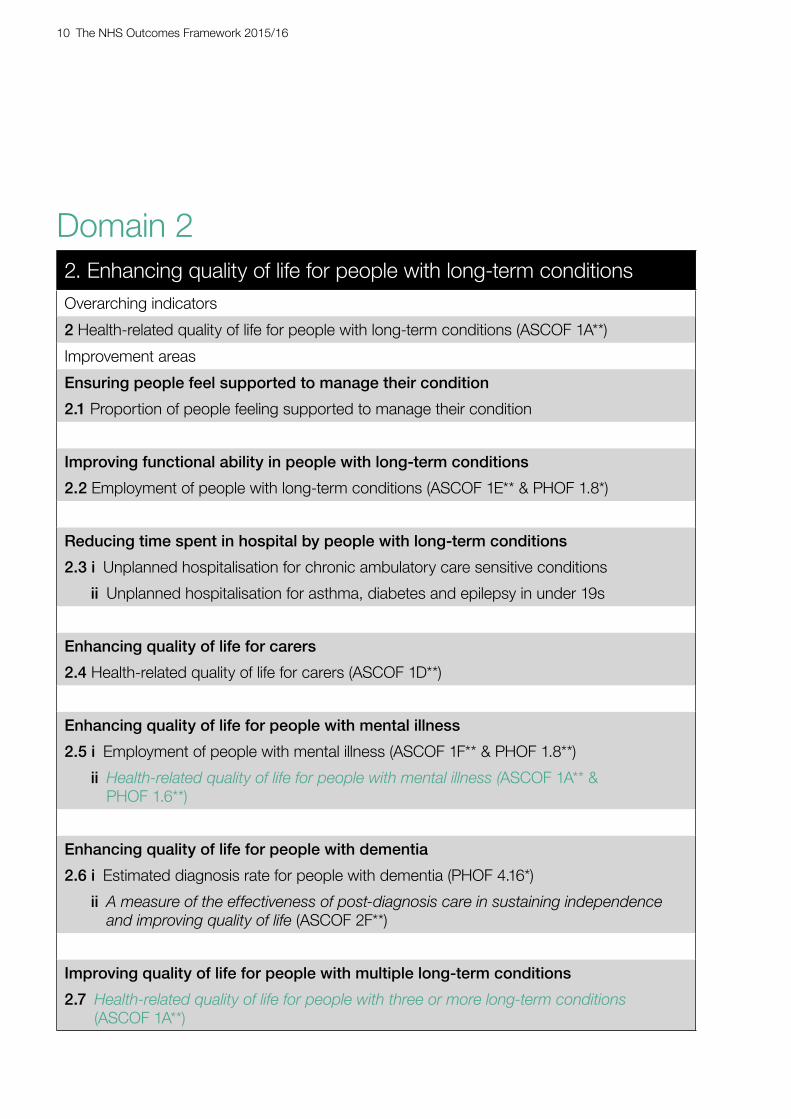
Domain 22. Enhancing quality of life for people with long-term conditionsOverarching indicators
2 Health-related quality of life for people with long-term conditions (ASCOF 1A**)
Improvement areas
Ensuring people feel supported to manage their condition
2.1 Proportion of people feeling supported to manage their condition
Improving functional ability in people with long-term conditions
2.2 Employment of people with long-term conditions (ASCOF 1E** & PHOF 1.8*)
Reducing time spent in hospital by people with long-term conditions
2.3 i Unplanned hospitalisation for chronic ambulatory care sensitive conditions
ii Unplanned hospitalisation for asthma, diabetes and epilepsy in under 19s
Enhancing quality of life for carers
2.4 Health-related quality of life for carers (ASCOF 1D**)
Enhancing quality of life for people with mental illness
2.5 i Employment of people with mental illness (ASCOF 1F** & PHOF 1.8**)
ii Health-related quality of life for people with mental illness (ASCOF 1A** & PHOF 1.6**)
Enhancing quality of life for people with dementia
2.6 i Estimated diagnosis rate for people with dementia (PHOF 4.16*)
ii A measure of the effectiveness of post-diagnosis care in sustaining independence and improving quality of life (ASCOF 2F**)
Improving quality of life for people with multiple long-term conditions
2.7 Health-related quality of life for people with three or more long-term conditions (ASCOF 1A**)

Changes across each domain 11
Mental health
Change made: Add new in development indicator 2.5.ii for ‘health-related quality of life for people with mental health illness’.
Why we made this change: This indicator provides a more comprehensive measure of health-related quality of life for people with mental illness which goes beyond what is shown by the existing indicator 2.5.i ‘employment of people with mental illness’. Alongside the new indicator for excess mortality in people with common mental illness in Domain 1, this change is part of our commitment to improve the coverage of mental health indicators in the NHS Outcomes Framework.
People with multiple long-term conditions
Change made: Add a new improvement indicator 2.7 (health-related quality of life for people with three or more long-term conditions).
Why we made this change: Specialisation of medical care is important in providing world standard care to patients. However, it is also important that patients are treated as a whole person. 30% of people over 75 are living with more than one health condition, and amongst the general population people that have 2 or more conditions outweigh those who only have one. Including an indicator to measure the health related quality of life for people with multiple long term conditions was welcomed by stakeholders as an important addition to the NHS Outcomes Framework.
12 The NHS Outcomes Framework 2015/16
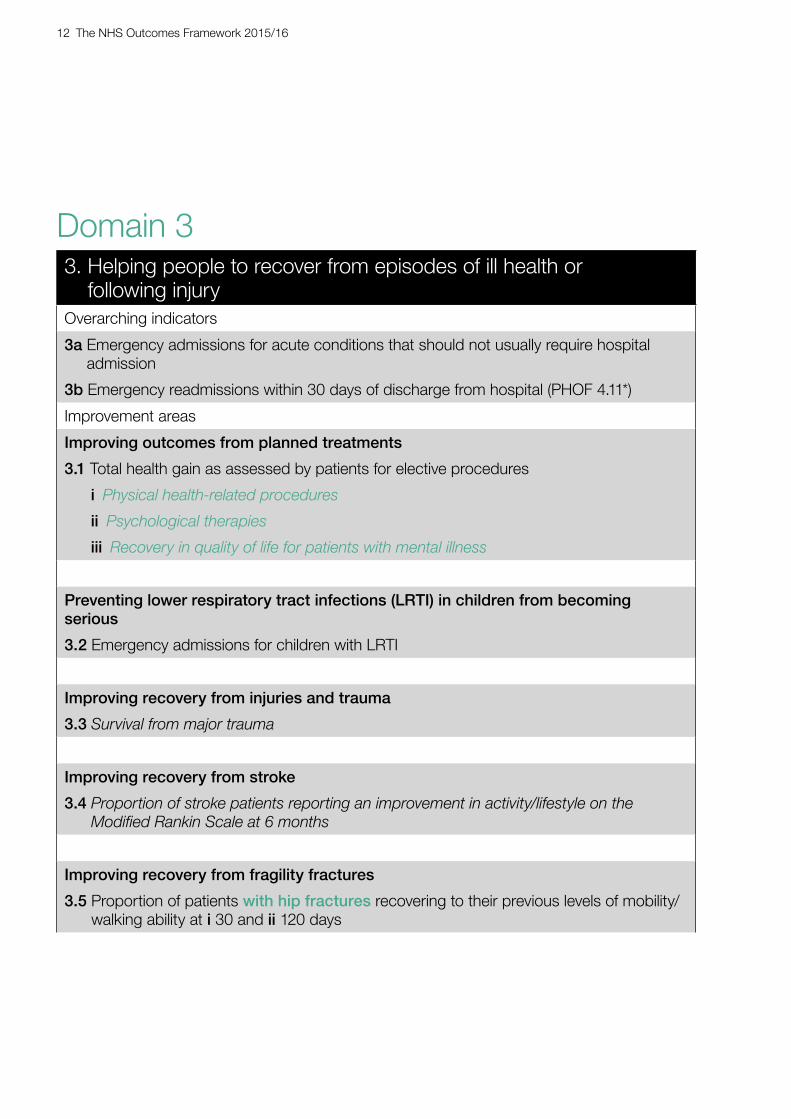
Domain 33. Helping people to recover from episodes of ill health or
following injuryOverarching indicators
3a Emergency admissions for acute conditions that should not usually require hospital admission
3b Emergency readmissions within 30 days of discharge from hospital (PHOF 4.11*)
Improvement areas
Improving outcomes from planned treatments
3.1 Total health gain as assessed by patients for elective procedures
i Physical health-related procedures
ii Psychological therapies
iii Recovery in quality of life for patients with mental illness
Preventing lower respiratory tract infections (LRTI) in children from becoming serious
3.2 Emergency admissions for children with LRTI
Improving recovery from injuries and trauma
3.3 Survival from major trauma
Improving recovery from stroke
3.4 Proportion of stroke patients reporting an improvement in activity/lifestyle on the Modified Rankin Scale at 6 months
Improving recovery from fragility fractures
3.5 Proportion of patients with hip fractures recovering to their previous levels of mobility/walking ability at i 30 and ii 120 days

Changes across each domain 13
Helping older people to recover their independence after illness or injury
3.6 i Proportion of older people (65 and over) who were still at home 91 days after discharge from hospital into reablement / rehabilitation service (ASCOF 2B[1]*)
ii Proportion offered rehabilitation following discharge from acute or community hospital (ASCOF 2B[2]*)
Dental health
3.7 i Decaying teeth (PHOF 4.02**)
ii Tooth extractions in secondary care for children under 10
Mental health
Change made: Consolidate the existing Patient Reported Outcomes Measures (PROMs) indicators 3.1.i-v from five into two: physical and mental health related procedures.
Why we made this change: Patient Reported Outcome Measures (PROMs) are a way of measuring recovery as reported by patients themselves. We have reduced the existing PROMs measures from five to two for two reasons: firstly, to ensure that the framework remains as succinct as possible, and secondly, to align further with the Government’s agenda to put mental health on par with physical health. Therefore, rather than there being four indicators for physical health and one for mental health, there is one for each.
Change made: Add new in development indicator 3.1.iii ‘recovery in quality of life for patients with mental health problems’.
Why we made this change: The current indicator 3.1 relates to IAPT services, a primary care intervention. This new proposed indicator will measure recovery for people receiving secondary mental health services.
Fragility fractures
Change made: Change the wording of existing indicator 3.5 to specify that the indicator measures ‘proportion of patients with hip fractures recovering to their previous levels of mobility/walking ability at 30/130 days’.
Why we made this change: Currently, the indicator is described as referring to patients recovering from fragility fractures, but it is compiled only from hip fracture data. The wording has been changed to more accurately reflect this. No other changes have been made to this indicator.
Dental health
Including indicators for dental health fills a significant gap in coverage of the NHS Outcomes Framework, with 29.9 million unique visits to NHS commissioned dentistry services in the 24 months prior to August 2014.9
Change made: Add new in development indicator 3.7.i for ‘decaying teeth’.
9 http://www.hscic.gov.uk/catalogue/PUB11625

14 The NHS Outcomes Framework 2015/16
Why we made this change: This indicator is designed to measure an improvement of quality of life for people with dental disease, comparing improvement in oral health over long periods of time for patients who regularly visit the dentist.
Change made: Add new in development indicator 3.7.ii ‘Tooth extractions in secondary care for children under 10’.
Why we made this change: Where the above indicator 3.7.i would measure outcomes for people regularly visiting the dentist, this indicator provides a proxy measure for the health outcomes of children who do not regularly visit the dentist. Avoidable tooth extracts are often the consequence of the failure to provide preventative interventions such as brushing advice and fluoride varnishes, or early-stage restorative interventions such as fillings. With the right interventions, children should almost never need to undergo dental care procedures under general anaesthetic.

Changes across each domain 15
Domain 44. Ensuring that people have a positive experience of care
Overarching indicators
4a Patient experience of primary care
i GP services
ii GP out-of-hours services
iii NHS dental services
4b Patient experience of hospital care
4c Friends and family test
4d Patient experience characterised as poor or worse
i Primary care
ii Hospital care
Improvement areas
Improving people’s experience of outpatient care
4.1 Patient experience of outpatient services
Improving hospitals’ responsiveness to personal needs
4.2 Responsiveness to in-patients’ personal needs
Improving people’s experience of accident and emergency services
4.3 Patient experience of A&E services
Improving access to primary care services
4.4 Access to i GP services and ii NHS dental services
Improving women and their families’ experience of maternity services
4.5 Women’s experience of maternity services
Improving the experience of care for people at the end of their lives
4.6 Bereaved carers’ views on the quality of care in the last 3 months of life
16 The NHS Outcomes Framework 2015/16
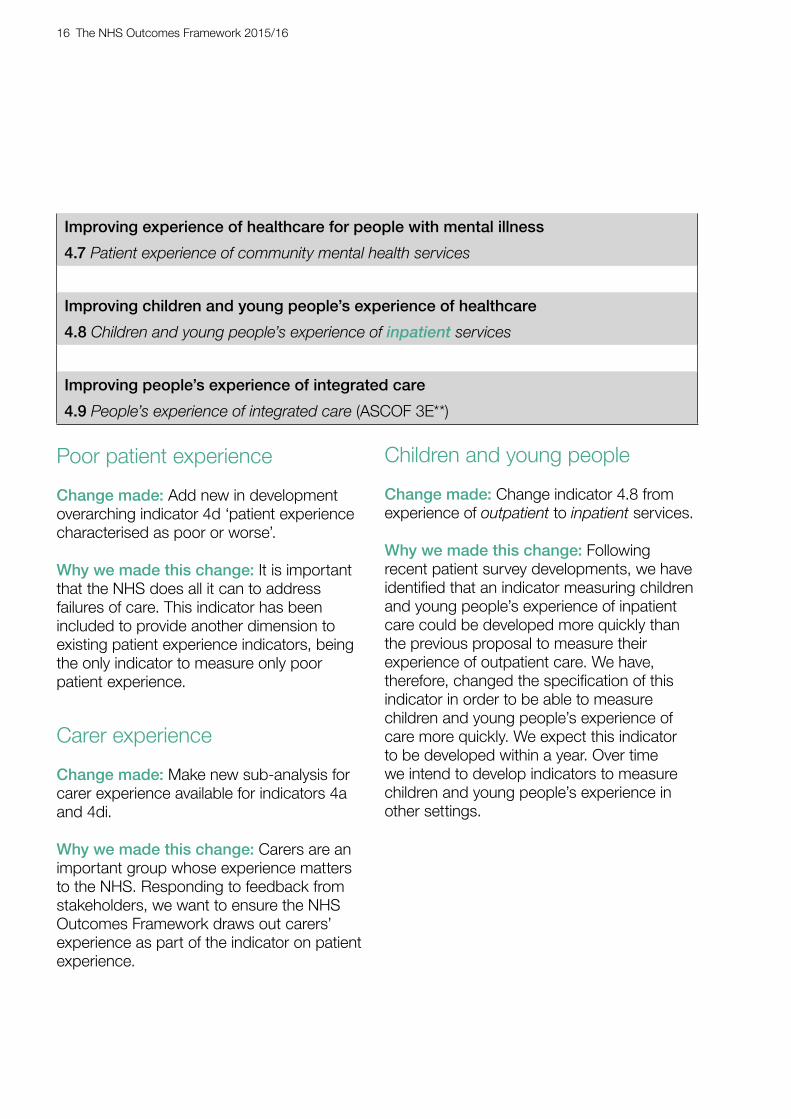
Improving experience of healthcare for people with mental illness
4.7 Patient experience of community mental health services
Improving children and young people’s experience of healthcare
4.8 Children and young people’s experience of inpatient services
Improving people’s experience of integrated care
4.9 People’s experience of integrated care (ASCOF 3E**)
Poor patient experience
Change made: Add new in development overarching indicator 4d ‘patient experience characterised as poor or worse’.
Why we made this change: It is important that the NHS does all it can to address failures of care. This indicator has been included to provide another dimension to existing patient experience indicators, being the only indicator to measure only poor patient experience.
Carer experience
Change made: Make new sub-analysis for carer experience available for indicators 4a and 4di.
Why we made this change: Carers are an important group whose experience matters to the NHS. Responding to feedback from stakeholders, we want to ensure the NHS Outcomes Framework draws out carers’ experience as part of the indicator on patient experience.
Children and young people
Change made: Change indicator 4.8 from experience of outpatient to inpatient services.
Why we made this change: Following recent patient survey developments, we have identified that an indicator measuring children and young people’s experience of inpatient care could be developed more quickly than the previous proposal to measure their experience of outpatient care. We have, therefore, changed the specification of this indicator in order to be able to measure children and young people’s experience of care more quickly. We expect this indicator to be developed within a year. Over time we intend to develop indicators to measure children and young people’s experience in other settings.

Changes across each domain 17
Domain 55. Treating and caring for people in a safe environment and protecting them
from avoidable harmOverarching indicators
5a (previously 5c) Deaths attributable to problems in healthcare
5b Severe harm attributable to problems in healthcare
Improvement areas
Reducing the incidence of avoidable harm
5.1 Deaths from venous thromboembolism (VTE) related events
5.2 Incidence of healthcare associated infection (HCAI)
i MRSA
ii C. difficile
5.3 Proportion of patients with category 2, 3 and 4 pressure ulcers
5.4 Hip fractures from falls during hospital care
Improving the safety of maternity services
5.5 Admission of full-term babies to neonatal care (definition and quality statement amended)
Improving the culture of safety reporting
5.6 Patient safety incidents reported
Children and young people
Change made: Remove existing indicator 5.6 incidence of harm to children due to ‘failure to monitor’.
Why we made this change: This year, a piece of research was done on this indicator which sampled 1/6 of reported cases of failure to monitor (i.e. a patient’s condition has deteriorated and clinicians have not intervened) over a 6 month period. The results showed that only 3% of the reported cases were of the type of harm that was
intended to be measured. This indicator, therefore, had the potential to be seriously misleading, as the numbers reported would give no indication of the true figures.
The Department is committed to the measurement of patient safety for children and young people and the inclusion of such indicators in the NHS Outcomes Framework. The Department is now working to find an alternative measure, as a priority, as soon as possible.
18 The NHS Outcomes Framework 2015/16
Overarching indicators
Change made: Combine the National Learning and Reporting System (NRLS) based indicators into a single improvement area indicator for patient safety incidents reported.
Move previous overarching indicator 5c (Hospital deaths attributable to problems in care) to overarching indicator 5a.
Introduce a new overarching indicator 5b (Severe harm attributable to problems in care).
Why we made this change: Combining the NRLS-based indicators in to a single improvement area indicator for patient safety incidents reported reflects the fact that patient safety incident reporting is a measure of both patient safety and patient safety reporting culture. Therefore, the introduction of a new improvement area recognises that the NRLS indicators are not purely a measure of patient safety.
Hip fractures
Change made: Add new indicator 5.4 ‘Hip fractures from falls during hospital care’.
Why we made this change: 2,500 cases of hip fractures from falls during hospital care were recorded in 2012/13. Patients who are already ill have very poor outcomes and greatly extended lengths of stay.
Improving the safety of maternity services
Change made: Amend definition of admission to neonatal care to include only higher levels (1-3) of specialist neonatal care.
Why we made this change: Admission of a full term baby to a neonatal unit is used as proxy indicator for significant harm. The indicator currently includes all levels of specialist neonatal care (1 to 3) as well as low levels such as outreach visits by neonatal unit staff to babies managed in post-natal wards. These low levels of specialist care are provided differently in different trusts and inconsistently recorded in the Neonatal Research Database; while levels 1 to 3 are unambiguously defined as they require physical admission to a neonatal unit.
Change made: Amend the quality statement of indicator 5.5, ‘admission of full-term babies to neonatal care’ to reflect issues regarding the quality of the indicator. The quality statement will be available from the HSCIC indicator portal.10
Why we made this change: OFTAG have raised concerns regarding the quality of this indicator as a measure of patient safety outcomes. For example, it takes no account of several important confounders e.g. changes in the supply of neonatal care units (an increase in supply is likely to lead to an increase in the value of the indicator that is not a reflection of worse outcomes) or the total number of births (affecting the demand for neonatal services).
10 https://indicators.ic.nhs.uk/webview/

NH
S O
utco
mes
Fra
mew
ork
– A
t a g
lanc
e 19
3 Ove
rarc
hing
indi
cato
rs
Hel
ping
peo
ple
to re
cove
r fro
m e
piso
des
of il
l hea
lth o
r fo
llow
ing
inju
ry
3a E
mer
genc
y ad
mis
sion
s fo
r acu
te c
ondi
tions
that
sho
uld
not u
sual
ly re
quire
ho
spita
l adm
issi
on
3b E
mer
genc
y re
adm
issi
ons
with
in 3
0 da
ys o
f dis
char
ge fr
om h
ospi
tal (
PH
OF
4.11
*)
Impr
ovin
g ou
tcom
es fr
om p
lann
ed tr
eatm
ents
3 .
1 To
tal h
ealth
gai
n as
ass
esse
d by
pat
ient
s fo
r ele
ctiv
e pr
oced
ures
i P
hysi
cal h
ealth
-rela
ted
proc
edur
es
ii Ps
ycho
logi
cal t
hera
pies
iii
Rec
over
y in
qua
lity
of lif
e fo
r pat
ient
s w
ith m
enta
l illn
ess
Pre
vent
ing
low
er re
spira
tory
trac
t inf
ectio
ns (L
RTI
) in
child
ren
from
bec
omin
g se
rious
3.
2 E
mer
genc
y ad
mis
sion
s fo
r chi
ldre
n w
ith L
RTI
Impr
ovin
g re
cove
ry fr
om in
jurie
s an
d tra
uma
3.3
Surv
ival
from
maj
or tr
aum
a
Impr
ovin
g re
cove
ry fr
om s
troke
3.
4 Pr
opor
tion
of s
troke
pat
ient
s re
porti
ng a
n im
prov
emen
t in
activ
ity/li
fest
yle
on th
e M
odifi
ed R
anki
n Sc
ale
at 6
mon
ths
Impr
ovin
g re
cove
ry fr
om fr
agili
ty fr
actu
res
3 .
5 P
ropo
rtion
of p
atie
nts
with
hip
frac
ture
s re
cove
ring
to th
eir p
revi
ous
leve
ls o
f m
obilit
y/w
alki
ng a
bilit
y at
i 30
and
ii 1
20 d
ays
Hel
ping
old
er p
eopl
e to
reco
ver t
heir
inde
pend
ence
afte
r illn
ess
or in
jury
3.
6 i P
ropo
rtion
of o
lder
peo
ple
(65
and
over
) who
wer
e st
ill at
hom
e 91
day
s
afte
r dis
char
ge fr
om h
ospi
tal i
nto
reab
lem
ent /
reha
bilit
atio
n se
rvic
e
(A
SC
OF
2B[1
]*)
ii
Pro
porti
on o
ffere
d re
habi
litat
ion
follo
win
g di
scha
rge
from
acu
te o
r
c
omm
unity
hos
pita
l (A
SC
OF
2B[2
]*)
Enh
anci
ng q
ualit
y of
life
for p
eopl
e w
ith lo
ng-te
rm
cond
ition
s 2 O
vera
rchi
ng in
dica
tors
2
Hea
lth-re
late
d qu
ality
of l
ife fo
r peo
ple
with
long
-term
con
ditio
ns (A
SC
OF
1A**
)
Impr
ovem
ent a
reas
E
nsur
ing
peop
le fe
el s
uppo
rted
to m
anag
e th
eir c
ondi
tion
2.1
Pro
porti
on o
f peo
ple
feel
ing
supp
orte
d to
man
age
thei
r con
ditio
n
Impr
ovin
g fu
nctio
nal a
bilit
y in
peo
ple
with
long
-term
con
ditio
ns
2.2
Em
ploy
men
t of p
eopl
e w
ith lo
ng-te
rm c
ondi
tions
(AS
CO
F 1E
**
PH
OF
1.8*
) &
Red
ucin
g tim
e sp
ent i
n ho
spita
l by
peop
le w
ith lo
ng-te
rm c
ondi
tions
2.
3 i U
npla
nned
hos
pita
lisat
ion
for c
hron
ic a
mbu
lato
ry c
are
sens
itive
con
ditio
ns
ii U
npla
nned
hos
pita
lisat
ion
for a
sthm
a, d
iabe
tes
and
epile
psy
in u
nder
19s
Enh
anci
ng q
ualit
y of
life
for c
arer
s 2.
4 H
ealth
-rela
ted
qual
ity o
f life
for c
arer
s (A
SC
OF
1D**
)
Enh
anci
ng q
ualit
y of
life
for p
eopl
e w
ith m
enta
l illn
ess
2.5
i Em
ploy
men
t of p
eopl
e w
ith m
enta
l illn
ess
(AS
CO
F 1F
** &
PH
OF
1.8*
*)
ii H
ealth
-rela
ted
qual
ity o
f life
for p
eopl
e w
ith m
enta
l illn
ess
(AS
CO
F 1A
** &
P
HO
F 1.
6**)
Pre
vent
ing
peop
le fr
om d
ying
pre
mat
urel
y 1 Ove
rarc
hing
indi
cato
rs
1a P
oten
tial y
ears
of l
ife lo
st (P
YLL)
from
cau
ses
cons
ider
ed a
men
able
to
heal
thca
re
i A
dults
ii C
hild
ren
and
youn
g pe
ople
1b
Life
exp
ecta
ncy
at 7
5
i M
ales
ii F
emal
es
1c N
eona
tal m
orta
lity
and
stillb
irths
Impr
ovem
ent a
reas
Red
ucin
g pr
emat
ure
mor
talit
y in
peo
ple
with
men
tal i
llnes
s 1.
5 i E
xces
s un
der 7
5 m
orta
lity
rate
in a
dults
with
ser
ious
men
tal i
llnes
s (P
HO
F 4.
9*)
ii Ex
cess
und
er 7
5 m
orta
lity
rate
in a
dults
with
com
mon
men
tal i
llnes
s
iii
Sui
cide
and
mor
talit
y fro
m in
jury
of u
ndet
erm
ined
inte
nt a
mon
g pe
ople
with
rece
nt c
onta
ct fr
om N
HS
serv
ices
(PH
OF
4.10
**)
Red
ucin
g m
orta
lity
in c
hild
ren
1.
6 i I
nfan
t mor
talit
y (P
HO
F 4.
1*)
i i Fi
ve y
ear s
urvi
val f
rom
all
canc
ers
in c
hild
ren
Red
ucin
g pr
emat
ure
mor
talit
y fro
m th
e m
ajor
cau
ses
of d
eath
1 .
1 U
nder
75
mor
talit
y ra
te fr
om c
ardi
ovas
cula
r dis
ease
(PH
OF
4.4*
) 1.
2 U
nder
75
mor
talit
y ra
te fr
om re
spira
tory
dis
ease
(PH
OF
4.7*
) 1 .
3 U
nder
75
mor
talit
y ra
te fr
om li
ver d
isea
se (P
HO
F 4.
6*)
1.4
Und
er 7
5 m
orta
lity
rate
from
can
cer (
PH
OF
4.5*
)
i O
ne- a
nd ii
Fiv
e-ye
ar s
urvi
val f
rom
all
canc
ers
i ii O
ne- a
nd i
v Fi
ve-y
ear s
urvi
val f
rom
bre
ast,
lung
and
col
orec
tal c
ance
r v
One
- and
vi F
ive-
year
sur
viva
l fro
m c
ance
rs d
iagn
osed
at s
tage
1&2
(
PH
OF
2.19
**)
Red
ucin
g pr
emat
ure
deat
h in
peo
ple
with
a le
arni
ng d
isab
ility
1.
7 Ex
cess
und
er 6
0 m
orta
lity
rate
in a
dults
with
a le
arni
ng d
isab
ility
4 Ove
rarc
hing
indi
cato
rs
Ens
urin
g th
at p
eopl
e ha
ve a
pos
itive
exp
erie
nce
of c
are
4a P
atie
nt e
xper
ienc
e of
prim
ary
care
i G
P s
ervi
ces
ii G
P O
ut-o
f-hou
rs s
ervi
ces
iii N
HS
den
tal s
ervi
ces
4 b P
atie
nt e
xper
ienc
e of
hos
pita
l car
e 4c
Frie
nds
and
fam
ily te
st
4d P
atie
nt e
xper
ienc
e ch
arac
teris
ed a
s po
or o
r wor
se
i.
Prim
ary
care
ii. H
ospi
tal c
are
Impr
ovem
ent a
reas
Impr
ovin
g pe
ople
’s e
xper
ienc
e of
out
patie
nt c
are
4.1
Pat
ient
exp
erie
nce
of o
utpa
tient
ser
vice
s
Impr
ovin
g ho
spita
ls’ r
espo
nsiv
enes
s to
per
sona
l nee
ds
4.2
Res
pons
iven
ess
to in
-pat
ient
s’ p
erso
nal n
eeds
Impr
ovin
g ac
cess
to p
rimar
y ca
re s
ervi
ces
4.4
Acc
ess
to i
GP
ser
vice
s an
d ii
NH
S d
enta
l ser
vice
s
Impr
ovin
g w
omen
and
thei
r fam
ilies
’ exp
erie
nce
of m
ater
nity
ser
vice
s 4.
5 W
omen
’s e
xper
ienc
e of
mat
erni
ty s
ervi
ces
Impr
ovin
g th
e ex
perie
nce
of c
are
for p
eopl
e at
the
end
of th
eir l
ives
4.
6 B
erea
ved
care
rs’ v
iew
s on
the
qual
ity o
f car
e in
the
last
3 m
onth
s of
life
Impr
ovin
g ex
perie
nce
of h
ealth
care
for p
eopl
e w
ith m
enta
l illn
ess
4.7
Patie
nt e
xper
ienc
e of
com
mun
ity m
enta
l hea
lth s
ervi
ces
Impr
ovin
g ch
ildre
n an
d yo
ung
peop
le’s
exp
erie
nce
of h
ealth
care
4.
8 C
hild
ren
and
youn
g pe
ople
’s e
xper
ienc
e of
inpa
tient
ser
vice
s
Impr
ovin
g pe
ople
’s e
xper
ienc
e of
acc
iden
t and
em
erge
ncy
serv
ices
4.
3 P
atie
nt e
xper
ienc
e of
A&
E s
ervi
ces
Impr
ovin
g pe
ople
’s e
xper
ienc
e of
inte
grat
ed c
are
4.
9 Pe
ople
’s e
xper
ienc
e of
inte
grat
ed c
are
(AS
CO
F 3E
**)
Red
ucin
g th
e in
cide
nce
of a
void
able
har
m
5.1
Dea
ths
from
ven
ous
thro
mbo
embo
lism
(VTE
) rel
ated
eve
nts
5.2
Inci
denc
e of
hea
lthca
re a
ssoc
iate
d in
fect
ion
(HC
AI)
i M
RS
A
ii
C. d
iffic
ile
5 .3
Prop
ortio
n of
pat
ient
s w
ith c
ateg
ory
2, 3
and
4 p
ress
ure
ulce
rs
5.4
Hip
frac
ture
s fro
m fa
lls d
urin
g ho
spita
l car
e
Impr
ovin
g th
e sa
fety
of m
ater
nity
ser
vice
s 5.
5 A
dmis
sion
of f
ull-t
erm
bab
ies
to n
eona
tal c
are
Trea
ting
and
carin
g fo
r peo
ple
in a
saf
e en
viro
nmen
t and
pr
otec
ting
them
from
avo
idab
le h
arm
5 O
vera
rchi
ng in
dica
tors
5a D
eath
s at
tribu
tabl
e to
pro
blem
s in
hea
lthca
re
5b S
ever
e ha
rm a
ttrib
utab
le to
pro
blem
s in
hea
lthca
re
Impr
ovem
ent a
reas
NH
S O
utco
mes
F r
amew
ork
2015
/16
at a
gla
nce
Alig
nmen
t with
Adu
lt S
ocia
l Car
e O
utco
mes
Fra
mew
ork
(AS
CO
F) a
nd/o
r P
ublic
Hea
lth O
utco
mes
Fra
mew
ork
(PH
OF)
*
Indi
cato
r is
shar
ed
**
Indi
cato
r is
com
plem
enta
ry
Indi
cato
rs in
ital
ics
are
deve
lopm
ent
in
Enh
anci
ng q
ualit
y of
life
for p
eopl
e w
ith d
emen
tia
2.6
i Est
imat
ed d
iagn
osis
rate
for p
eopl
e w
ith d
emen
tia (P
HO
F 4.
16*)
ii
A m
easu
re o
f the
effe
ctiv
enes
s of
pos
t-dia
gnos
is c
are
in s
usta
inin
g
i
ndep
ende
nce
and
impr
ovin
g qu
ality
of l
ife (A
SC
OF
2F**
)
Impr
ovin
g D
enta
l Hea
lth
3.7
i D
ecay
ing
teet
h (P
HO
F 4.
02**
)
ii
Impr
ovem
ent A
reas
Impr
ovin
g th
e cu
lture
of s
afet
y re
porti
ng
5 .6
Pat
ient
saf
ety
inci
dent
s re
porte
d
Impr
ovin
g qu
ality
of l
ife fo
r peo
ple
with
mul
tiple
long
-term
con
ditio
ns
2.7
Hea
lth-re
late
d qu
ality
of l
ife fo
r peo
ple
with
thre
e or
mor
e lo
ng-te
rm c
ondi
tions
(A
SC
OF
1A**
)
Toot
h ex
tract
ions
in s
econ
dary
car
e fo
r chi
ldre
n un
der 1
0

© Crown copyright 2014 2903144 Produced by Williams Lea for the Department of Health





























