Embed Size (px)
Citation preview
NHS England South Region Standard Operating Procedure for Urgent Dental Care Hubs (UDCH) during the COVID-19
Pandemic
This document should be reviewed weekly as the current situation develops.
Version Control
Revision date
New version number
Summary of changes
29/04/20 7.0 Induction (computer system section)
Triage
Prescribing
Cleaning of Surgery
Safe Working
Addition of appendix for further info on PPE
30/04/20 7.1 Amendments to Prescribing section
20/05/20 7.2 Inclusion of anosmia symptom
Triage section: significant risk of medical deterioration
Incident learning form embedded
Inclusion of PPE table
Amendment to additional info on PPE in appendices
Addition of PPE diagrams in appendices
Addition of secondary triage flow chart and references in appendices
Addition of pain management document in appendices
27/05/20 7.3 Medical emergencies appendix
Removed option of gloves for patient (hand sanitising remains)
Inclusion of option to take patient’s temperature according to hub risk assessment
Minor amendment to diagram 1
Clarification in Workforce section by inclusion of all specialties
03/06/20 7.4 Minor amendment to patients abroad section
Inclusion of additional information about staff risk assessments
10/06/20 7.5 Removal of paragraph referring to cessation of routine care
Amendment to statement on mouthwash
Removal of reference to air conditioning use
Respirators for AGPs in PPE section
17/06/20 7.6 Inclusion of diagram 1a
01/07/20 7.7 Modification of diagram 1a
Change to requirement for hubs to issue analgesia and antimicrobials
05/08/20 7.8 Removed inconsistency in PPE guidance
Added HPT contact details
Urgent Dental Care Hubs SOP v7.8 05/08/20 2
Contents
Version Control .......................................................................................................... 1
Introduction and Principles ......................................................................................... 3
Staff Induction ............................................................................................................ 7
Patient Pathway ......................................................................................................... 9
Triage ....................................................................................................................... 13
Prescribing ............................................................................................................... 20
Record Keeping ....................................................................................................... 25
Cleaning of Surgery.................................................................................................. 25
Safe Working ............................................................................................................ 27
Appendices .............................................................................................................. 36
Feedback template ................................................................................................... 47
Health Protection Team Contact Details .................................................................. 47
References and Further Guidance ........................................................................... 48
Urgent Dental Care Hubs SOP v7.8 05/08/20 3
Introduction and Principles
Purpose The following Standard Operating Procedure (SOP) is applicable in the planning and operating of Urgent Dental Care Hubs (UDCHs) during the COVID-19 Pandemic across the South East region of England, including Kent, Surrey, Sussex, Hampshire and Isle of Wight, Buckinghamshire, Oxfordshire and Berkshire. This SOP aims to encourage a consistent approach towards urgent dental problems across the region, recognising the importance of staff and patient safety in this time while still enabling access to urgent care when patients cannot manage their symptoms themselves. It is essential to minimise the number of patients accessing these centres to reduce the risk of transmission of COVID-19 to staff and patients, avoid unmanageable or inappropriate demand and to conserve available PPE supplies. This SOP sets out the provision of urgent dental services to be implemented from the above date. In addition, there is further information available in the Issue 3 Preparedness Letter for dental care 25 March 2020 and Issue 4 Preparedness Letter of 15 April 2020. Key Principles:
Flexible arrangements, rapidly developing;
Care limited to emergencies and urgent dental care;
Best interests of patients;
Protecting the local population;
Protecting NHS frontline staff including the dental team;
Dental teams to keep up to date with current guidance;
All patients who will benefit from and need urgent dental treatment will be able to access it and those whose needs do not meet the criteria will be advised to self-manage.
Dental Treatment in Primary Care All practices, either individually or collaboratively, are to establish a remote urgent dental care service, providing advice by telephone or other appropriate means for their patients with urgent needs during usual contracted hours and, wherever possible, treating with:
Advice Analgesia Antimicrobial means where appropriate
Urgent Dental Care Hubs SOP v7.8 05/08/20 4
In NHS England and NHS Improvement South East, to provide the best urgent care service needs to our patients in this unprecedented time, we would like to remind all practices which provide services for the NHS that they are to remain open or be remotely accessible (i.e. accessible just via telephone) to provide advice and prescribing by a dentist during normal working hours to offer a priority first tier triage for all emergency and urgent patients. The advice you offer may also be to patients you have not seen in your practice before and who have not recently seen a dental professional.
Patients who are abroad:
If you have a patient abroad whom you have seen before you can give advice;
If you have a patient abroad whom you have not seen before you should not give advice.
Emergency (these patients should be directed to A&E):
Life threatening emergencies, e.g. airway restriction or breathing/ swallowing
difficulties due to facial swelling Uncontrollable dental haemorrhage following extractions that cannot possibly
be dealt with within the Urgent Dental Care Hub; Rapidly increasing swelling around the throat or eye which causes immediate
threat to life; Trauma to head and neck to include dental arches that requires maxillofacial
services. Urgent primary dental care:
Trauma such as dento-alveolar injuries or avulsion of a permanent tooth Oro-facial swelling that is significant and worsening but does not present
realistic threat to life Post extraction haemorrhage that the patient cannot control by local
measures but does not present realistic threat to life Dental conditions that have resulted in acute and severe systemic illness Severe dental and facial pain: that is pain that cannot be controlled by the
patient following self-help advice or the use of appropriate antimicrobials. Fractured teeth or tooth with pulpal exposure Dental and soft tissue infections without systemic involvement/effect. Oro-dental conditions that are likely to exacerbate systemic medical
conditions Suspected oral cancer.
Each patient should be assessed and managed on their own merit, taking into
account the patient’s best interests, professional judgement, local UDC
arrangements and the prioritisation of the most urgent care needs.
Urgent Dental Care Hubs SOP v7.8 05/08/20 5
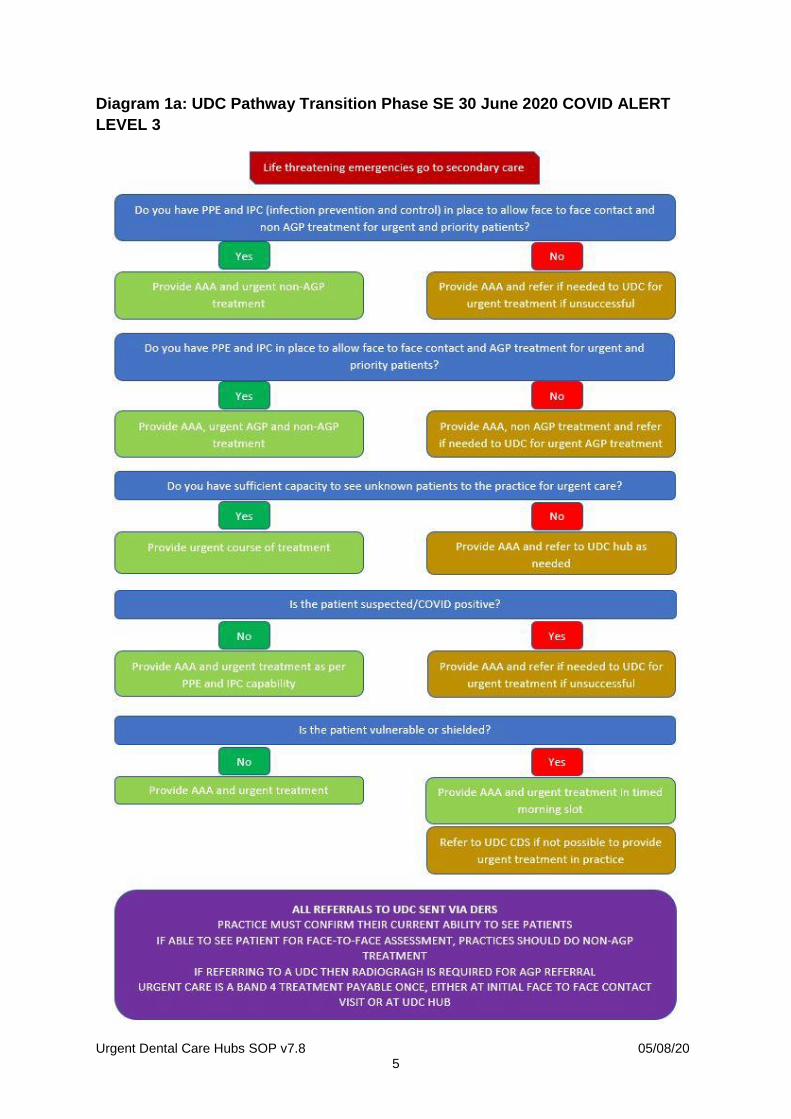
Diagram 1a: UDC Pathway Transition Phase SE 30 June 2020 COVID ALERT
LEVEL 3
Urgent Dental Care Hubs SOP v7.8 05/08/20 6
Possible list of treatments which could be provided include:
1. Assessment and Diagnosis Examination, assessment and advice; Radiographic examination and radiological report;
2. Interventive Treatments
Aerosol generating procedures (AGPs) should be avoided unless absolutely necessary as per the Issue 3 Preparedness Letter. For a list of aerosols see the Chief Dental Officer of Scotland’s letter on AGPs. A risk assessment should be undertaken, on a case by case scenario, using clinical judgement to consider the risks of aerosol generation versus unnecessary tooth extraction e.g. a pulpectomy on an anterior tooth. Further information can be found at the British Endodontic Society.
Dressing of teeth and palliative treatment; Re-implantation of an avulsed, luxated or subluxated permanent tooth
following trauma with any necessary endodontic treatment being delayed until aerosol generating procedure (AGP) avoidance has been removed
No surgical extraction of teeth where possible to minimise aerosol; Provision of post-operative care including treatment of infected sockets; Urgent treatment for acute conditions of the gingivae or oral mucosa,
including treatment for pericoronitis or for ulcers and herpetic lesions, and any necessary oral hygiene instruction in connection with such treatment;
Incising an abscess; Other treatment immediately necessary as a result of trauma.
Urgent Dental Care Hubs SOP v7.8 05/08/20 7
Staff Induction
Urgent care dental hubs will be set up and staffed initially by staff already employed by the practice for NHS contracted work. A rota will be developed to set out the clinic schedule and staff booked. When new staff will be working in the practice then a local induction should be used and recorded, see below.
RECORD OF INDUCTION
NAME: DESIGNATION: Induction carried out by:
Date and Sign on completion
See appendices for a declaration template for the items below:
Appropriate indemnity insurance
GDC registration
Hold a valid NHS Performer number & EDI pin
Up-to-date Hep B status
Up-to-date IRMER CPD
Hold a DBS
Up-to-date BLS and medical emergencies CPD Check when attending hub for the first time:
Photo ID checked, e.g. driving licence or passport
Display name on PPE, e.g. sticky label Practice specific:
Nursing arrangements
Toilets
Staff facilities, incl. changing and lockers
PPE in line with current guidance for COVID-19 (see Issue 3 Preparedness Letter and PHE guidance)
Emergency drugs/resus equipment location
Prescription pads location and local pharmacy arrangements
Medical history form and process Policies:
Health and safety policies and regulations, including COSHH
Cross infection control procedures to HTM-0105 standard
Sharps injury protocol
Radiation protection – local rules
Radiograph processing
Waste disposal
Local children and vulnerable adults safeguarding arrangements
Urgent Dental Care Hubs SOP v7.8 05/08/20 8
Fire policy
Accident book location
Information governance
Practice NHS complaints policy Surgery:
Start and end of session checklists
Use of equipment (switch on, switch off etc)
Location of clinical equipment and materials
Isolation switches location
Aspirator maintenance procedure
Equipment line management
Autoclaves and decontamination room Computer system:
Data protection
Use of personal DERS login. The South East DERS login normally used will be functional in all South East hubs.
Basic use of system and clinical notes
Sending off electronic FP17
Access to patient records, including paper, or any other patient identifiable information in practice
Keeping Staff Safe Government guidance for business and employers is found here. All staff should be risk assessed on an ongoing basis to protect them and keep possible cases, household contacts, staff who should be shielded, or those at increased risk, away from work. It is recommended that the risk assessment is carried out by a line manager, supervisor or designated senior manager within the Urgent Dental Care Hub. It should be carried out in a one to one consultation in a sensitive manner taking into consideration staff well-being and any concerns that the staff member may have. NHSE/I have produced a Risk Assessment Tool and Risk Reduction Framework that can be used as part of the risk assessment process. The outcome of the risk assessment should be documented for each staff member and any necessary workplace adjustments made as required. In line with government advice, it is recommended that as part of risk assessment, dental providers review resource requirements for service operations and commitments. Where appropriate, this should allow staff to stay at or work from home to avoid non-essential travel and contact; or to participate in local workforce redeployment efforts in line with local arrangements. COVID-19 guidance around social distancing and good hygiene practice should be promoted as far as possible in the workplace.

Urgent Dental Care Hubs SOP v7.8 05/08/20 9
For further guidance see the National COVID-19 guidance and standard operating procedure.
Patient Pathway
General dental practices are responsible for providing urgent dental care, limited to advice, analgesia and anti-microbials, where appropriate, as well as triage for any patient who contacts them (this must not be restricted to patients who normally attend the practice). This includes a COVID assessment of the patient, either individually or by a local collaborative arrangement amongst practices. A COVID assessment for patients will be completed at first stage triage firstly by the General Dental Practitioner or local Out Of Hours Emergency Dental Services . Triage at second stage facilitated through the dental electronic referral system (DERS) followed by contact with the patient remotely by a dentist working for the UDCH prior to any potential face to face clinical assessment in the UDCH.
General dental practices and CDS services remain first line as per Issue 3 Preparedness Letter and Issue 4 preparedness letter providing:
o Advice o Analgesics o Anti-microbials (as appropriate)
Existing dental Out Of Hours services will remain operational providing the three A as above.
Initial contact is carried out in primary care which will involve determining the patient COVID status (Hot or Cold) and patient category (1-4- see Issue 3 Preparedness Letter) and triaging as per pathway (see diagram 1).
If an appointment is required, the patient will be referred through DERS for further triage and where appropriate an appointment with the appropriately skilled clinician in the UDCH. A triage will take place by a dentist who will attempt to provide appropriate advice before potentially scheduling an appointment (see below).
UDCHs triage in real time, up to 7 days per week (hours to be confirmed, dependent on demand). There is no target time to see the patient.
Recommend that operating clinicians are appropriately skilled to carry out the necessary treatment, for example oral surgery procedures should be performed in order to ensure swift care delivery, to reduce risk, and avoid the need for re-attendance or further issues.
Urgent Dental Care Hubs SOP v7.8 05/08/20 10
Triage Within UDCHs The expectation is that face to face contacts within UDCHs are kept to a minimum. In doing so, non-essential contact and travel is reduced, cross-infection risks are minimised and essential PPE is protected. The patient pathway for the UDCH is considered to have two broad stages – remote management and face-to-face management. As far as possible, patients should be managed remotely and exit the pathway at the end of this stage. Those patients who cannot be managed remotely will enter the face-to-face stage of the pathway Issue 4 preparedness letter. Following electronic referral (DERS) to the UDCH, the triaging dentist will have a responsibility to conduct a further, detailed triage prior to consideration of any face to face appointment. Hub services are expected to have also followed the SOP outlined in Section 4.1 of COVID-19 Urgent Dental Care SOP. Video conferencing is an extremely useful tool, particularly in relation to the assessment of swellings. If, following this stage of triage, it is found that the patient can in fact be managed remotely, the patient should be given the appropriate advice, analgesia or antibiotics (as appropriate) and discharged on DERS. A comprehensive discharge summary should also be provided to the referring dentist detailing the reason that the referral has been rejected and providing any advice that is required for their further management of the patient. A face to face contact must only be made following this triage and conduction of risk assessment on an individual basis for each patient and it is confirmed that the patient cannot be managed remotely. If the electronic referral to the UDCH does not contain all relevant information to confirm the urgent nature of the referral, the triaging dentist can decide whether to reject the referral or to proceed and discover further information directly from the patient. Referrals should only be rejected or returned for more information if the dentist at the UDCH decides that there is no risk to the patient by delaying their treatment. The triager at the UDCH should ensure that any referrals rejected or returned clearly specify the reason why and note that the referral will be reconsidered if further detail entered by the referrer substantiates this. Where multiple incomplete or inappropriate referrals are repeatedly received from the same practice, even after advice issued on the returned/rejected referrals, the dentist leading the UDCH should consider a direct approach to the practice provider and if that fails, to inform NHS England South East, quoting relevant URNs at [email protected].

Urgent Dental Care Hubs SOP v7.8 05/08/20 11
Diagram 1: NHS England South East region urgent dental care pathway
All patients to be treated as potentially ‘hot’.
Urgent Dental Care Hubs SOP v7.8 05/08/20 12
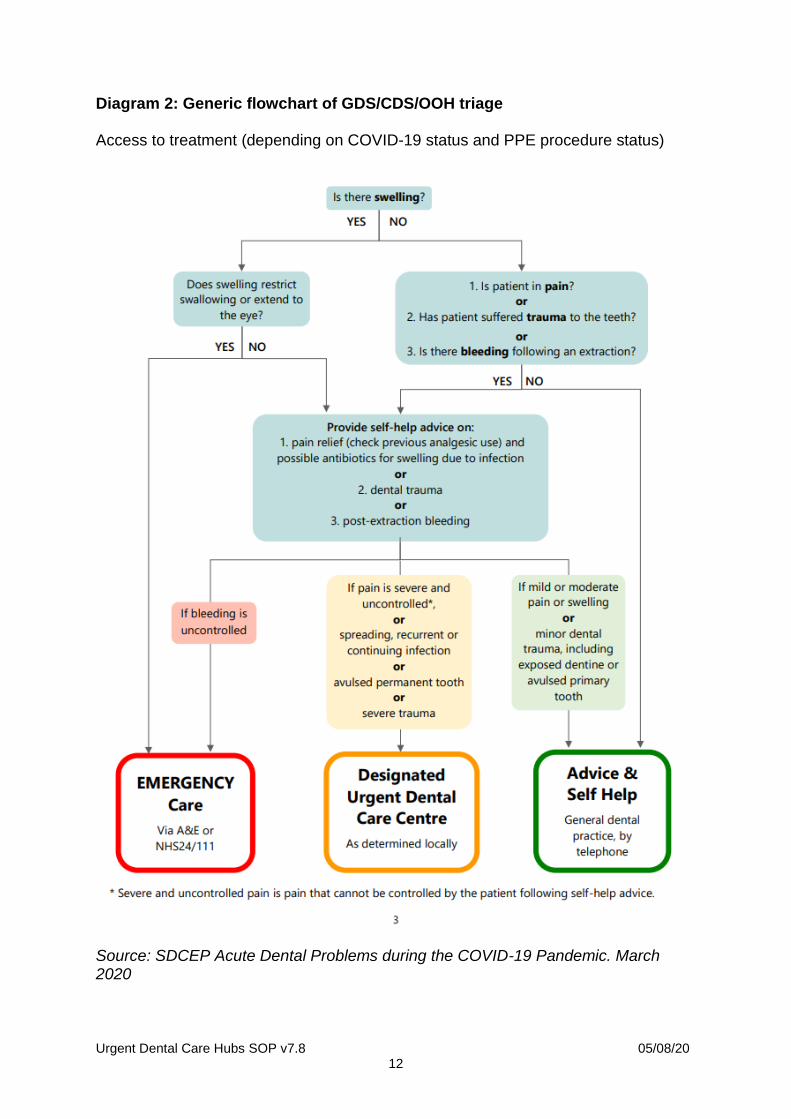
Diagram 2: Generic flowchart of GDS/CDS/OOH triage Access to treatment (depending on COVID-19 status and PPE procedure status)
Source: SDCEP Acute Dental Problems during the COVID-19 Pandemic. March 2020
Urgent Dental Care Hubs SOP v7.8 05/08/20 13
Triage
Definition of need:
P1 - Requires immediate treatment on the day Directed to UDCH or secondary care depending on severity P2 – Treatment ideally within 24 hours Directed to UDCH for management P3 Non-Urgent - Dental emergency that can be treated in GDS or CDS and can be managed once routine care resumes Two week rule (suspected oral cancer) The two week pathway via DERS should be utilised for all non-traumatic lesions that have been present for over three weeks. See NICE guidelines: https://www.nice.org.uk/guidance/ng12 P1 Requires immediate treatment on the day, Directed to UDCH or secondary care depending on severity Referral to dental facility in community care and or hospital unit depending on patient needs and severity of dental issue and skill mix at UDCH For example:
Oral facial dental infection with swelling / pyrexia / airway risk
Bleeding of dental origin that the patient cannot control
Trauma of the facial skeleton (usually requiring maxillo-facial input)
Trauma to teeth requiring urgent management that has defined timeline. (tooth avulsion)
P2 Treatment ideally within 24 hours, directed to UDCH for management Referral to dental facility in community for management For example:
Dental infection that if not treated would escalate to level P1.
Severe pericoronitis that cannot be managed by analgesics/antibiotics/self-care.
Localised swelling without pyrexia that can be managed by local dental measures.
Dental infection that can be treated by removal of a tooth or extirpation of pulp if appropriate on balance of risk assessment, aerosol generation etc.
Dental trauma of the teeth and supporting structures that can be managed in outpatient facilities.
Urgent Dental Care Hubs SOP v7.8 05/08/20 14
Orthodontic Emergencies causing trauma – if attempts have been made to resolve the cause of the ulceration (see P3) and if the trauma is still continuous, severe and causing ulceration.
Patients with significant risk of deteriorating medically may need an assessment at a UDC hub (CDS) prior to the following:
cardiac care - valve replacement and heart surgery.
high risk medication-related osteonecrosis of the jaw (MRONJ).
patients undergoing planned active oncology treatment.
These may be treated in CDS hubs or in secondary care or a mixture of both dependent upon the results of a virtual multi-disciplinary team (led by secondary care or CDS).
For example, where a patient is at significant risk of MRONJ and a Consultant requests a thorough dental assessment with remedial dental treatment where required prior to commencement of drug therapy, this would fall under the criteria of “oro-dental conditions that are likely to exacerbate systemic medical conditions”. A referral on the UDC hub pathway should be made selecting “Medication Related Osteonecrosis” ensuring full medical history and medication are detailed and upload a copy of the Consultant’s letter and any recent x-rays. The UDC hub (CDS) will carry out an examination and for medically complex patients for whom they would usually seek advice, including higher risk patients who are being treated with anti-resorptive or anti-angiogenic drugs for the management of cancer, consideration should be given to holding a virtual multi-disciplinary team following the examination to consult an oral surgery/special care dentistry specialist with regards to treatment planning. Any treatment that is required may be carried out in the UDC hub and/or oral surgery team in secondary care dependent upon the virtual MDT outcome. Full guidance can be found here https://www.sdcep.org.uk/wp-content/uploads/2017/04/SDCEP-Oral-Health-Management-of-Patients-at-Risk-of-MRONJ-Guidance-full.pdf.
Guidance on management of adults with cancer:
UKMi_QA_Cancer-in
-dental-patients_update-Nov-2019.pdf
P2 services to have close liaison with hospital units. P3 Non-Urgent, Dental emergency that can be treated in GDS or CDS and can be managed once routine care resumes For example:
Mild or moderate pain: that is, pain not associated with an urgent care condition and that responds to over the counter medications.
Minor dental trauma.
Urgent Dental Care Hubs SOP v7.8 05/08/20 15
Post extraction bleeding that the patient is able to control using self-help measures.
Loose or displaced crowns, bridges or veneers.
Fractured or loose-fitting dentures and other appliances including orthodontics;
o If the ulceration is due to part of an orthodontic appliance, patients should be advised to contact their orthodontist for advice. Further information for dentists and patients may be accessed via the BOS website https://www.bos.org.uk
o If the ulceration is due to a fractured tooth or filling, advice includes purchase of a temp filling kit when someone next visits a pharmacy.
Fractured posts; fractured, loose or displaced fillings. Treatments normally associated with routine dental care bleeding gums. Dealing with a patient with an urgent dental condition All patients at UDCHs will be treated as potentially COVID-19 positive, however those who answer yes to the following questions may be at higher risk and will be treated at different times or different locations.
1. Do you have a new or continuous dry cough? 2. Is temperature above 37.8? 3. Have you been diagnosed with COVID-19? 4. Have you or a member of your household been told to self-isolate? 5. Have you suffered a loss of, or change in, your normal sense of smell or taste
(anosmia)? If the patient has COVID-19 symptoms or is self-isolating, then they will be directed to an appropriate site.
Management of Aerosol Generating Procedures (AGP)
High-speed dental drills are accepted as AGPs. Using high-speed drills to open an access cavity or surgical high-speed drills to undertake surgical extraction of a tooth/root will necessitate use of enhanced PPE. Particular care should be taken to avoid surgical extractions at this time. Where it is necessary to remove bone, slow handpieces should be used with irrigation to reduce the risk. The use of 3-in-1 syringes, ultrasonic scalers or other pieces of dental equipment powered by air compressor should be avoided at this time. If, however, they are used as an adjunct to treatment with high-speed drills, staff will already have donned PPE for AGPs. A risk assessment should be undertaken considering the risks of aerosol generation for extirpation versus unnecessary tooth extraction.
Urgent Dental Care Hubs SOP v7.8 05/08/20 16
To reduce cross contamination, consider:
Rubber dam should be used where possible to reduce aerosol. After placing rubber dam decontaminate the operative field with sodium hypochlorite.
Access into the pulp chamber only without instrumentation of the root canal system.
. Alternative treatments to be considered:
Dental extractions.
Dressings only with caries removal.
Using hand excavation.
Avoid endodontic procedures.
Avoid use of ultrasonic scaler. Advice on Managing Dental Pain The delivery of advice on managing dental pain requires suitable training. Patients who are waiting for dental appointments might require basic advice on the effective management of their dental pain. Give the patient the following advice on the use of self-help measures, including appropriate analgesia to relieve pain.
Avoid stimuli that precipitate or worsen the pain such as hot or cold foods or cold air.
Holding cooled water or crushed ice around the tooth can help some types of dental pain.
Severe pain from the mouth or teeth sometimes feels worse when lying flat; therefore, try lying propped up as this might ease the pain.
Use painkillers that have successfully provided pain relief for you in the past without adverse effects.
Avoid taking aspirin as a painkiller if there is bleeding.
Ensure patients are reminded to follow the directions on the packet for advice on precautions in some medical conditions e.g. patients with asthma should avoid non-steroid anti-inflammatories.
Advise the patient to call back if symptoms persist or worsen. See Scottish Dental Clinical Effectiveness Programme – Drugs for the Management of Dental Problems During COVID-19 Pandemic
SDCEP-MADP-COVI
D-19-drug-supplement-080420.pdf
See appendix on managing acute dental pain within COVID-19 AAA triaging.

Urgent Dental Care Hubs SOP v7.8 05/08/20 17
Shielded Groups As far as possible, the management of these patient groups should be carried out remotely and invasive treatment delayed. The referrals will specifically identify those patients who are shielded (Individuals at the highest risk of severe illness from COVID-19 who are advised to shield themselves and stay at home for 12 weeks) and patients at increased risk. The DERS referral pathway will contain specific questions in drop down format in order to identify these patients. The system is therefore reliant on the input of specific and accurate information from the referring dentist to ensure reliable identification. Following input of this information, the algorithm will ensure that shielded patients (defined in guidance) in particular are separated from other patient groups by directing these patients to the local CDS services. The patient’s GP and/or other dedicated health and social care professionals should be consulted as necessary to arrange face-to-face care in a way that aligns with the patient’s overall care needs and minimises contact risk. Where appropriate, urgent dental care may be provided on a domiciliary visit by a dedicated dental team. If there is limited capacity for domiciliary care provision, consideration should be given to prioritising patients at highest risk (i.e. shielded patients). In the event that a dental team identifies a shielded patient or patient at increased risk as having possible COVID-19 symptoms, refer to a medical practitioner for further assessment.
Urgent Dental Care Hubs SOP v7.8 05/08/20 18
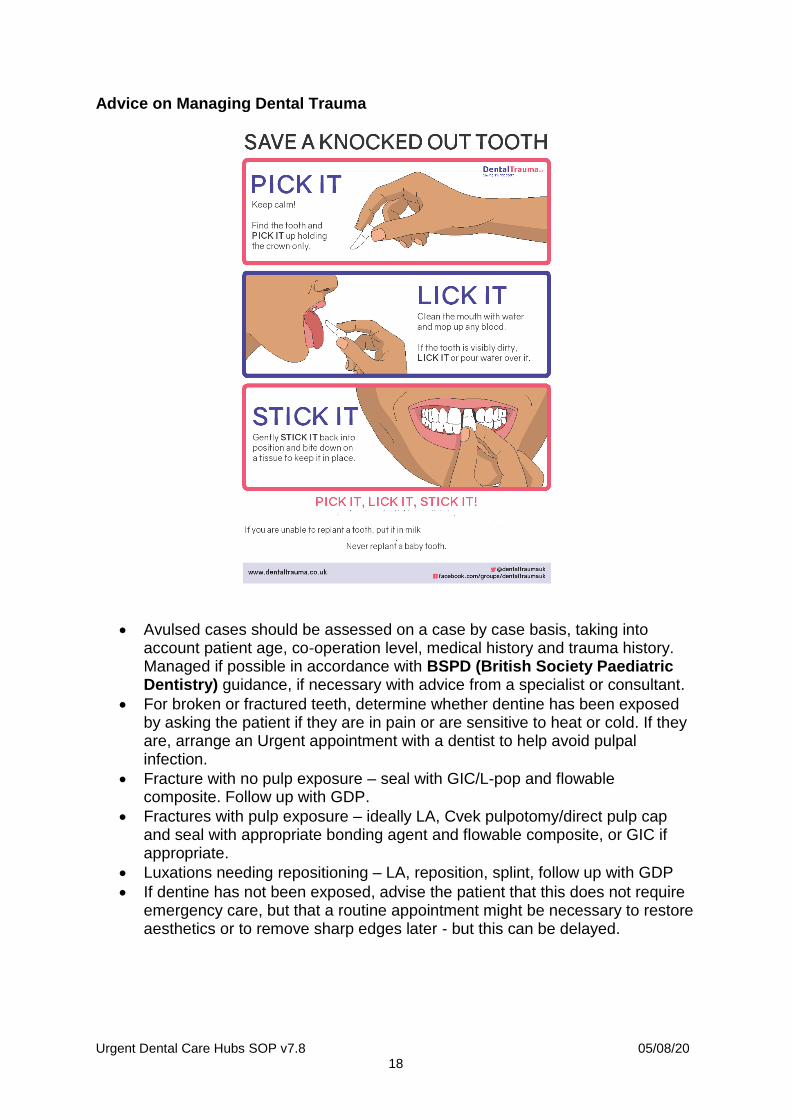
Advice on Managing Dental Trauma
Avulsed cases should be assessed on a case by case basis, taking into account patient age, co-operation level, medical history and trauma history. Managed if possible in accordance with BSPD (British Society Paediatric Dentistry) guidance, if necessary with advice from a specialist or consultant.
For broken or fractured teeth, determine whether dentine has been exposed by asking the patient if they are in pain or are sensitive to heat or cold. If they are, arrange an Urgent appointment with a dentist to help avoid pulpal infection.
Fracture with no pulp exposure – seal with GIC/L-pop and flowable composite. Follow up with GDP.
Fractures with pulp exposure – ideally LA, Cvek pulpotomy/direct pulp cap and seal with appropriate bonding agent and flowable composite, or GIC if appropriate.
Luxations needing repositioning – LA, reposition, splint, follow up with GDP
If dentine has not been exposed, advise the patient that this does not require emergency care, but that a routine appointment might be necessary to restore aesthetics or to remove sharp edges later - but this can be delayed.
Urgent Dental Care Hubs SOP v7.8 05/08/20 19
Advice on Managing Post-Extraction Bleeding Patients who have had extractions during the past week might require basic advice on the management of bleeding from the extraction area.
Ascertain that no anticoagulant medication is currently being taken.
Give the patient the following advice on the use of self-help measures to stop the bleeding.
Blood-stained saliva is normal after dental extractions.
Make a small pad with a clean cotton handkerchief or kitchen towel and dampen it slightly with water.
Rinse the mouth once only with warm (not hot) water to get rid of the blood. Place the damp pad over the socket area and bite firmly.
If there are no opposing teeth hold the pad firmly on the socket.
Maintain this while sitting upright quietly for 20 minutes and then check. Repeat once if necessary.
After the bleeding has stopped, remain rested and as upright as possible.
Do not drink alcohol.
Do not disturb the blood clot in the socket.
Advise the patient to re-contact the service if these self-help measures prove inadequate.
Orthodontic advice British Orthodontic Society (BOS) COVID-19 Orthodontic Emergencies Protocol (25th March 2020) can be found here: https://www.bos.org.uk/COVID19-BOS-Advice/COVID19-BOS-Advice
Urgent Dental Care Hubs SOP v7.8 05/08/20 20
Prescribing
Introduction Where patients cannot come to a dental surgery, dental professionals may be asked to provide advice remotely and to work with patients to defer the need for active treatment using pain control and antimicrobial treatment. The basic principles of the GDC’s guidance on remote consultation and prescribing apply (see GDC Guidance on remote consultations and prescribing).
You must make an appropriate assessment of your patient’s condition, prescribe within your competence and keep accurate records.
You must have an understanding of your patient’s current health and medication, including any relevant medical history, in order to prescribe medicines safely.
You must only prescribe medicines to meet the identified dental needs of your patients.
You should only use remote means to prescribe medicines for dental patients if there is no other viable option and it is in their best interests.
In the specific circumstances of COVID-19, the key requirement is to make an appropriate risk assessment. That risk assessment should be recorded by the dentist and should take into account the infection risk of COVID-19, both from and to the patient, as well the apparent seriousness of the need for treatment and the extent to which it has been possible to make a clinical assessment via telephone/video consultation. Patients should have access to the 3A’s such as Advice, Analgesia and Antimicrobials and should not be advised to contact 111 as this is inappropriate. With the exception of patients that consider they have COVID-19 and require advice relating to COVID-19 symptoms (and not for dental advice), patients should not be advised to contact 111 and you should manage them yourself or refer to the hub if their system cannot be controlled. National guidance National guidance can be found at: https://www.fgdp.org.uk/news/open-letter-prescribing-antibiotics-during-covid-19-%C2%A0
Urgent Dental Care Hubs SOP v7.8 05/08/20 21
Procedure Antibiotics still need to be prescribed appropriately for the patient’s condition and should follow choice, dose and duration of antibiotic recommended in FGDP(UK) or SDCEP guidance.
FGDP(UK): Antimicrobial Prescribing for General Dental Practitioners
SDCEP: Drug prescribing for dentistry
SDCEP: Drugs for the Management of Dental Problems During COVID-19 Pandemic
The dental AMS toolkit also includes patient information leaflets that could be used to provide or reinforce key messages to patients.
Antibiotics should be prescribed in the following situations:
If it is considered that the patient has a bacterial infection which requires antibiotics. This would include the treatment of acute apical or periodontal abscess and acute pericoronitis, necrotising ulcerative gingivitis/periodontitis.
after discussion with the patient about the benefits and risks associated with the treatment options offered.
with advice on what to do if symptoms continue to progress.
with consideration of a follow-up call to the patient after a few days to check how their infection has responded to the antibiotics.
Consider prescribing an antibiotic if there is any swelling even if it is only localised. In these situations, the prescription has a prophylactic role as ideal treatment which could be incisional drainage, extraction or opening the tooth up cannot be carried out.
Antibiotics should not be prescribed in the following situations:
Because of a patient request.
Routinely as part of a pathway to care.
Acute pulpitis should still be managed only with painkillers with regimes described above – refer to analgesic advice section. Prescribing antibiotics is inappropriate as they are of no clinical benefit in managing dental pain from this inflammatory issue.
Pain on biting in the absence of swelling should be treated with pain killers only.
Urgent Dental Care Hubs SOP v7.8 05/08/20 22
Provision of a prescription
During the current COVID-19 pandemic it may be appropriate to use a remote medium to prescribe analgesics and antimicrobials for patients. Pharmacists can supply medication through remote prescribing provided they receive a physical prescription within 72 hours. This applies to prescription only medication.
Confirm patient details and obtain consent (or follow principles of the Mental Capacity Act 2005).
Explain how the remote prescription process will work and what to do if the patient has any concerns.
Explain that prescription will only be provided if it is safe to do so.
Explain that it is not safe to prescribe without sufficient information about the patient’s health or if remote care is unsuitable to meet their needs.
Explain it may be unsafe if relevant information is not shared with other healthcare providers involved in their care.
If it is unsafe to prescribe then signpost to other appropriate services; see above triage SOP.
Issuing the prescription by a GDP If DERS is unavailable, you should follow the protocol below omitting the sections where you are required to input data into DERS/REGO. You must contact the pharmacy using the following website address to find their telephone number: https://www.nhs.uk/service-search/find-a-pharmacy Use your practice nhs.net account to send the prescription once you have confirmed the email address with the pharmacy. An e-mail sent from or to a non-nhs.net e-mail address which contains patient identifiable information could constitute an information governance breach. Prescribing via DERS
1. Log onto DERS with your normal log in details. 2. Add in the patient details, i.e. name, address, telephone number DOB to
create a record and URN for the patient. 3. Check medical history, medications, allergies, any contraindications and
interactions. 4. Answer the prompts as to the patients COVID-19 status – this is important. If
the patient or a member of their family is symptomatic or self-isolating, they MUST not attend the pharmacy to collect the medication and must arrange for someone else to collect it.
5. Shielded patients should also be advised to ask someone else to pick up the prescription. In some cases, the pharmacy may also deliver, but this will incur an additional charge to the patient and is up to the patient to arrange.
6. Follow normal prescription guidelines and give patient any advice relevant to the medication prescribed.
Urgent Dental Care Hubs SOP v7.8 05/08/20 23
7. Select Prescription Pathway from the drop-down menu. Follow the prompts on the screen to create a record of the prescription. Select the appropriate medication, dose, route and frequency. Ensure items below have been completed.
a. Check the opening times of the patient’s preferred pharmacy you are sending the script to via their profile on the NHS website (https://www.nhs.uk/service-search/find-a-pharmacy) as some pharmacies may have needed to close because of COVID-19 related illness. Try to select the pharmacy local to the patient (after discussion with the patient as to which one they would like to use).
b. You should telephone the pharmacy to confirm they have current access to their pharmacies NHS net mail shared account and to alert them that a dental prescription will be sent. Agree whether this is necessary each time a dental prescription is sent.
c. Select the pharmacy from the list on DERS/REGO screen and then transmit the prescription to the pharmacy.
8. Send the referral. The system will save the referral in the prescribing tab visible from the front screen.
a) The dentist should then write an identical FP10D and sign it prior to posting or otherwise delivering it to the pharmacy. Please remember to sign and print the prescribers name clearly, along with GDC number, as well as using the practice stamp showing the provider contract number if appropriate.
b) To help manage patient expectations:
When you have sent the email to the pharmacy, contact your patient and advise them when to go to the pharmacy. This should ideally be 3 hours after the sending of e-mail to allow for dispensing, however if the patient has a large swelling, medication should be collected and taken as soon as possible.
Remind the patient to check pharmacy opening times before travelling.
Some pharmacies may be extremely busy and therefore enforcing social distancing, and in addition their workloads may result in some pharmacies having 2-3-hour queues at peak times. The patient or whoever collects the medication must be made aware to tell the pharmacist they have come to collect a dental prescription which has arrived via the pharmacy nhs.net shared email account and will be available in their inbox. They should advise the pharmacist this is not via the usual method that GPs use (EPS) but from a dentist.
c) It is the dentist’s responsibility to post the original hand-written prescription (FP10D) to the pharmacy by FIRST CLASS POST to arrive within 3 working days. The pharmacy address can be found on the DERS/REGO screen or on the NHS UK website (link shown above). It is a legal requirement to ensure the prescription arrives at the pharmacy within 72 hours. https://bnf.nice.org.uk/guidance/emergency-supply-of-medicines.html
d) Give an email address on an enclosure in the envelope with the FP10D prescription to which, the pharmacy can acknowledge receipt of the prescription original.
Urgent Dental Care Hubs SOP v7.8 05/08/20 24
9. Ask the patient to contact you if they are unable to obtain the prescription. 10. All pharmacies have been advised to accept dental prescriptions via these
mechanisms, under the “urgent supply at the request of a prescriber” as included in the pharmacy’s terms of service. It is also a requirement that pharmacies have access to their nhs net mail shared account. Dentists can refer pharmacies to their Local Pharmaceutical committee website where this information has been posted. Dentists experiencing difficulties with a specific pharmacy which cannot be resolved locally can email [email protected]. Dentists should send any other queries on this process, not relating to the use of DERS to [email protected].
Record keeping
All records to be kept in accordance with guidelines to include justification for remote prescription (see Record Keeping section of this document).
Make an entry of any prescription in the prescription log.
Keep a record of paper prescription sent and confirmation of receipt by pharmacy.
Keep a record of the URN associated with the prescription for entering onto patients notes. Await confirmation of receipt by pharmacy.
Follow up The patient should be advised that antibiotics will not be effective immediately but if their condition does not improve, they should seek further dental advice. Stock of analgesia and antimicrobials at UDCHs Hubs are no longer required to hold or issue analgesia and antimicrobials and should issue prescriptions as per NHS Regulations.
Urgent Dental Care Hubs SOP v7.8 05/08/20 25
Record Keeping
Record keeping and treatment claims will be carried out using the UDCHs’ own software systems. A word document can be uploaded as per below.
Example clinical
record template.docx
Cleaning of Surgery
It is accepted that local guidance may exist with NHS Trusts which deviates from the information given here. The surgery should be cleaned at the start of the day before seeing any patients (see step by step guide of what to clean). Staff cleaning surgeries must be trained on the appropriate materials and equipment to use when cleaning a surgery. Staff that undertake cleaning do not need to be a dental registrant, but they must have been trained on the correct use of the products and the flow of cleaning (please see section below which outlines cleaning process to be followed). They must also ensure they are wearing the appropriate PPE to undertake the cleaning (gloves, fluid resistant surgical mask (Type IIR FRSM), eye protection and plastic apron). Cleaning Ideally, use disposable wipes which are chlorine based at 1,000ppm av.cl, to clean and disinfect all hard surfaces, the floor, chairs, door hands and any reusable non-invasive equipment. If disposable wipes are not available use disposable cloths, paper roll, mop heads, to clean and disinfect all hard surfaces or floor or chairs or door handles or reusable non-invasive care equipment following one of the 2 options below:
● use either a combined detergent disinfectant solution at a dilution of 1000 parts per million (ppm) available chlorine (av.cl.)
● or a neutral purpose detergent followed by disinfection (1000 ppm av.cl.) You should follow manufacturer’s instructions for dilution, application and contact times for all detergents and disinfectants as these will differ across each product.
Urgent Dental Care Hubs SOP v7.8 05/08/20 26
Step by step cleaning guide
● Clean all reusable equipment and surfaces systematically and ensure that you regularly change wipes or rinse out the cloth in the detergent disinfectant solution throughout the process below: Ensure the whole chair is cleaned from top to base unit.
● Clean the light on the dental chair thoroughly. ● Clean the foot pedals. ● Clean the dental stools. ● Clean the outside of any material containers used during the procedure.
Where possible dispense materials prior to the episode of care and minimise containers on surfaces.
● When cleaning the surfaces, work systematically from the top or furthest away point.
● Clean wall cabinets, then work surfaces, then base cabinets. ● Clean the handles on units/ cupboards. ● Clean the computers. ● Clean the taps. ● Clean the hand wash basins. ● Wipe down the paper towel dispenser. ● Wipe down the alcohol gel and soap dispensers. ● Clean the door handle. ● Clean the light switches. ● Other items which are not disposable. ● Clean the outside of the door handle.
Once outside of the surgery any cloths and mop heads used must be disposed of as single use items and not re-used, even if they are designed for multiple uses. The detergent disinfectant should be emptied, and the mop bucket thoroughly cleaned paying particular attention to the outside and the underside of the bucket. Ensure enough solution is available for the full session.
Urgent Dental Care Hubs SOP v7.8 05/08/20 27
Safe Working
Hub location
Each local UDC system will involve provision of necessary face-to-face treatment at a number of specific, designated sites in a way that allows appropriate separation (through physical or temporal measures, eg zones, sessions/appointment times) and treatment of all patients.
UDC hubs have been set up as either GDS or CDS to see: 1. Patients who are possible or confirmed COVID-19 patients – including
patients with symptoms (new, persistent cough or high temperature), or those living in their household: (“Hot” sessions in the CDS/GDS)
2. Patients who are shielded – those at the highest risk of severe illness from COVID-19: (CDS)
3. Patients who are at increased risk of severe illness from COVID-19. (CDS)
4. Patients who do not fit one of the above categories (GDS).
The surgery should be readily accessible, ideally ground floor direct access if possible.
Precautions should be taken to avoid ‘Shielding’ patients or ‘at risk’ patients from coming into contact with other patients.
The hub should have one/two surgeries allocated to treatment of patients.
There must be a separate Local Decontamination Unit (LDU) present at the hub. The LDU should ideally have a washer-disinfector in place.
There should be adequate car parking facility at the hub in case the patient has to wait in a car prior to being seen (minimise use of waiting areas). If the patient is accompanied their companion should also wait in the car for the duration of the appointment (where possible), or outside the hub observing social distancing.
The location will have appropriate signage.
The clinical location will not be advertised in order to avoid walk in contact. Preparation of the hub
Waiting rooms and reception areas should allow for 2 metre separation. The care environment should be kept clean and clutter free. All non-essential items including toys, books and magazines should be removed from reception and waiting areas.
Urgent dental care surgeries into two categories depending on whether the treatment includes aerosol generating procedures (AGPs) or not. AGPs should be avoided where possible.
All urgent dental care centres will follow standard infection control precautions (SICPs) necessary to reduce the risk of transmission of infectious agents from both recognised and unrecognised sources. In dental settings, there is guidance from HTM01-05 and NICE describing infection prevention and control measures that should be used by all staff, in all settings, always, for all patients.
Urgent Dental Care Hubs SOP v7.8 05/08/20 28
Hand hygiene and respiratory/cough hygiene
Hand hygiene, washing thoroughly with soap and water, is essential to reduce the transmission of infection. All dental staff and patients/carers should decontaminate their hands with alcohol-based hand rub when entering and leaving urgent dental care services.
Hand hygiene must be performed immediately before every episode of direct patient care and after any activity or contact that potentially results in hands becoming contaminated, including the removal of PPE, equipment decontamination and waste handling.
Respiratory and cough hygiene should be observed by staff and patients/carers. Disposable tissues should be available and used to cover the nose and mouth when sneezing, coughing or wiping and blowing the nose – ‘Catch it, bin it, kill it’. Hand hygiene should be performed after disposing of the tissue.
Any procedures should be carried out with a single patient and only staff who are needed to undertake the procedure present in the room with the doors shut. Dental care professionals working in urgent care settings should be trained in all aspects of infection prevention and control (IPC) and fully familiar with HTM01 05 for decontamination.
Training should include donning (putting on) and doffing (taking off) PPE.
Cleaning staff should also be trained in IPC measures. Personal protective equipment This section details the minimum standard of PPE to be donned. During periods of widespread community transmission of COVID-19 dentists should use PPE to treat patients based on the type of urgent care they are providing. In effect, there is now an assumption that all patients present a risk of transmission of the virus. Non-AGP treatment of all patients involves compliance with standard infection control procedures. This will ensure there is no contact or droplet transmission of COVID-19. Eye protection, disposable fluid-resistant surgical mask, disposable apron and gloves should be worn. (Level 2 PPE) For AGP treatment, to prevent aerosol transmission disposable, fluid-repellent surgical gown (or waterproof long-sleeved protective apron), gloves, eye protection (faceshield or visor) and an FFP3 respirator should be worn by those undertaking or assisting in the procedure. (Level 3 PPE)
Urgent Dental Care Hubs SOP v7.8 05/08/20 29
Respirators for AGP
The HSE has stated that FFP2 and N95 respirators (filtering at least 94% and 95% of airborne particles respectively) offer protection against COVID-19 and so may be used if FFP3 respirators are not available. These respirators offer protection against AGPs, are recommended by the World Health Organization and are used routinely in other countries by dentists for AGPs.
Operators who are unable to wear respirators e.g. due to facial hair, religious head coverings should wear alternatives such as hoods.
All respirators need to be fit tested and checked. Providers are reminded to exercise caution as some reusable masks contain latex. Risk reduction of droplet contamination can be undertaken by using high-speed suction and use of rubber dam. Filtering face piece (FFP3) respirators for AGPs FFP3 respirators must be:
Fit-tested on all healthcare staff who may be required to wear an FFP3 respirator to ensure an adequate seal/fit according to the manufacturers’ guidance;
Fit-checked (according to the manufacturers’ guidance) by staff every time an FFP3 respirator is donned to ensure an adequate seal has been achieved;
Compatible with other facial protection used – i.e. protective eyewear – so that this does not interfere with the seal of the respiratory protection; regular prescription glasses are not considered adequate eye protection;
Disposed of and replaced if breathing becomes difficult, the respirator is damaged or distorted, the respirator becomes obviously contaminated by respiratory secretions or other body fluids, or if a proper face fit cannot be maintained; in effect this may mean that FFP3s may be worn once for dental AGPs and then discarded as clinical waste (hand hygiene must always be performed after disposal);
FFP3s should be removed outside the dental surgery where AGPs have been generated in line with doffing protocol.
In exceptional circumstances it may be acceptable to use an FFP3 mask for a session. Such exceptional circumstances should be risk assessed and this risk assessment and the rationale for any decision taken should be documented by the UDC Clinician.
In the unlikely scenario that FFP3 masks are used for a session they must be shielded from ‘splatter’ with a fluid resistant surgical mask or visor to protect the respirator from droplets; a session ends when the healthcare worker leaves the care setting/exposure environment; PPE should be disposed of after each session or earlier if damaged, soiled, or uncomfortable.
Urgent Dental Care Hubs SOP v7.8 05/08/20 30
Preparing for clinical care
Follow standard infection control guidelines (see cleaning section) to set up surgery ensuring surfaces are as clear as possible.
Ensure further equipment is available in clean decontamination area.
Remove non-essential items from surgeries and waiting areas e.g. impression machines/books/magazines
Assess equipment (kit) required for type of urgent care appointment from patient triage notes.
The two members of the clinical team in surgery put on COVID-19 full PPE.
Donning of appropriate PPE should be in “clean” area. See guidance.
The runner (third staff member) is to put on PPE then check COVlD-19 full PPE is correctly donned on the clinical surgery team.
Consider completing notes in an alternative area post treatment.
Staff should wear footwear that can be wiped down post treatment.
The runner will remain outside of surgery door (or by hatch if available) and pass through any additional equipment that may be required during urgent care appointment. If additional equipment is required, the runner is to remove gloves, apply gel hand sanitiser and don new gloves.
Treatment of patients in the hub
Patient should stay outside the hub until instructed by a member of the team to enter (respecting social distancing).
Wherever possible patients should be brought in on their own – carers should not be allowed except in exceptional circumstances.
Only nurse and dentist in clinic area during treatment.
On entering the building ask the patient to sanitise their hands. Ensure you remain at the safe social distancing (2 metres) from the patient.
Consider whether taking the patient’s temperature would add value to your assessment, if so this should be taken by the runner.
Escort the patient to reception and if the patient is a charge payer, the patient must pay the urgent treatment fee of £22.70. Ideally this should have been paid on the phone prior to the patient attending. documentation should have been pre-prepared at this point for the patient to review by sight and pay the fee (if required). The patient should not touch any of the documents; you may need to read out the document/information to a patient so they can confirm the details.
The patient should then be taken to the surgery and asked to be seated in the dental chair; ideally, they should not touch any door or item other than the dental chair.
Once in the surgery the nurse and dentist should confirm the medical history of the patient directly verbally.
Examine the patient.
Following on from examination, ensure consent to treatment is given by the patient and recorded on the computer.
Urgent Dental Care Hubs SOP v7.8 05/08/20 31
If possible, the patient should rinse with 0.2 % povidone-iodine mouthrinse or alternatively a mouthwash of 1ml to 8ml diluted hydrogen peroxide for 1min, or peroxyl (1.5% hydrogen peroxide) prior to treatment can be considered.
Avoid use of the spittoon and ensure disposable cardboard receiver dish or plastic cup is in place.
Provide treatment as needed.
Give verbal post op instructions to the patient. Confirm the patient has understood these as no document/leaflet will be offered.
If required, dispense analgesics or if necessary, antimicrobials to the patient.
Nurse directs the patient to the door and calls for the runner who escorts the patient through reception observing the 2 metre social distancing rules.
Patient should leave the premises and the cleaning of the area can then commence.
Following treatment
Patient is escorted by the runner out of the clinic.
The runner (in Level 2 PPE and remaining outside of surgery) receives dirty instruments from clinical team in surgery, takes instruments to decontamination room and remains in PPE to follow standard decontamination process; removing gloves, gel/wash hands and applying new gloves as required.
Clinical team in surgery should remove gloves and apron/gown/coverall and dispose in clinical waste stream, wash hands and leave surgery, shutting door behind them
Outside surgery door, reusable visors (and goggles if worn as well) must be removed from back of head and dropped into designated box and disposable items (mask, some visors) are to be removed from back of head and disposed of in clinical waste bag (bin in corridor), gel hands
See guidance and PHE video.
Following an AGP, the surgery should not be re-entered for at least an hour to allow virus to settle (see COVID-19: Guidance and standard operating procedure urgent dental care systems in the context of coronavirus V 1, 15 April 2020)
Should the environment have negative pressure isolation then this time can be reduced to 20 minutes
Windows to the outside in neutral pressure rooms can be opened.
Record time of re-entry on laminated sheet on surgery door
At the appropriate time put on Level 2 PPE and re-enter surgery. Follow standard infection control guidelines to clean surgery paying particular attention to door handles and patient contact points. See step by step cleaning guide section.
Prepare for next patient in Level 2 PPE
Repeat after each patient
If no AGPs have been generated in the surgery, then cleaning can commence in the normal timeframe (20 minutes).

Urgent Dental Care Hubs SOP v7.8 05/08/20 32
At the end of the day
Infection control procedures for cleaning and closing of the surgery should be followed with particular vigilance to cleaning door handles, switches, chairs work surfaces or anything else that the patient may come into contact with.
Uniforms should be cleaned daily and at the end of the day put in a plastic bag to transport home. The plastic bag should be disposed of in the household waste stream.
It is acceptable to place uniforms in a washable pillowcase or similar provided that this is transported home in a plastic bag which is disposed in the household waste stream.
A team debrief should take place at the end of each day to look at lessons learned and any improvements that can be made to the process will be shared and implemented. As the pathway matures the frequency of debrief may be reduced.
Personal protective equipment (PPE) for
COVID-19 urgent dental care settings
Waiting room/ reception No clinical treatment
Runner/decon nurse No clinical treatment
Dental surgery Non AGP treatment
Dental surgery Treatments involving AGP’s
Good hand hygiene Yes Yes Yes Yes
Disposable gloves No Yes Yes Yes
Disposable plastic apron
No Yes Yes No
Disposable gown* No No No Yes*
Fluid-resistant surgical mask (FRSM) Type IIR
Yes Yes Yes No
Filtering face piece (FFP3) respirator
No No No Yes

Urgent Dental Care Hubs SOP v7.8 05/08/20 33
* Fluid-resistant gowns (or long-sleeved waterproof apron) must be worn during
aerosol generating procedures (AGPs). If non-fluid-resistant gowns are used, a disposable plastic apron should be worn underneath.
** Eye protection ideally should be disposable. If polycarbonate safety
glasses/goggles or equivalent are used, they should be disinfected in line with manufacturers’ guidance. Visor or face shield needs to cover the forehead, extend below the chin and wrap around the side of the face.
Eye protection/visor or face shield **
No Yes Yes Yes
Urgent Dental Care Hubs SOP v7.8 05/08/20 34
Additional equipment needed to meet the requirements of this SOP
Apron.
Disposable surgical gown/coverall.
Emergency drug supply should be present and checks of kits should have been undertaken.
Eye protection: face visor or goggles.
FFP3 respirator masks and associated training and fit testing.
Fluid resistant (Type IIR) surgical mask (FRSM).
Full face re-usable visor (or other suitable eye protection).
Gloves, normal nitrile gloves.
Hand sanitiser.
Surgical gloves. Workforce An appropriate team, approved on the National Performer List with a diverse range of skills, is required to deliver care within the UDCH including:
GDPs competent to provide care within this SOP.
Access to a clinician with appropriate oral surgery skills on a rostered frequent basis.
Appropriate links with other specialist support e.g. Special Care Dentistry, Orthodontics, Paediatric Dentistry, Restorative Dentistry, Periodontics and Endodontics.
Access to clinicians and/or specialists experienced with trauma (e.g. paediatric specialists).
Incident Management and Learning Each UDHC is responsible for developing its own incident management plan to deal with medical emergencies in the context of the COVID-19 pandemic. Below is a template for use in reflection and information sharing following incidents that may take place at UDCHs:
Learning from
Incidents template.docx
Urgent Dental Care Hubs SOP v7.8 05/08/20 35
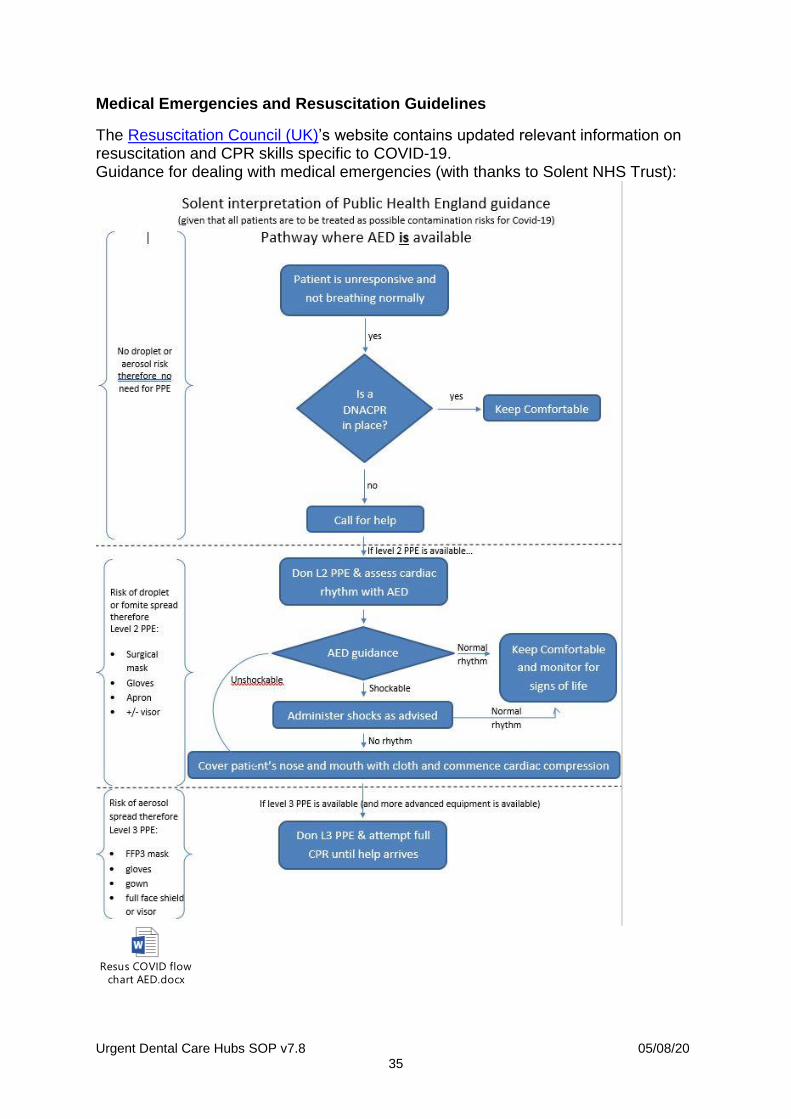
Medical Emergencies and Resuscitation Guidelines
The Resuscitation Council (UK)’s website contains updated relevant information on resuscitation and CPR skills specific to COVID-19. Guidance for dealing with medical emergencies (with thanks to Solent NHS Trust):
Resus COVID flow
chart AED.docx

Urgent Dental Care Hubs SOP v7.8 05/08/20 36
Appendices
Additional information relating to PPE
In times of severe PPE shortage, FFP2 masks may be used as an alternative to
Type IIR FRSMs. When used without a face fit test, an FFP2 mask will afford a
similar level of protection to a Type IIR FRSM.

Urgent Dental Care Hubs SOP v7.8 05/08/20 37
Antibiotics Don’t Cure Toothache poster
NHS Antibiotics
Dont Cure Toothache dental pain relief poster.pdf
Urgent Dental Care Hubs SOP v7.8 05/08/20 38
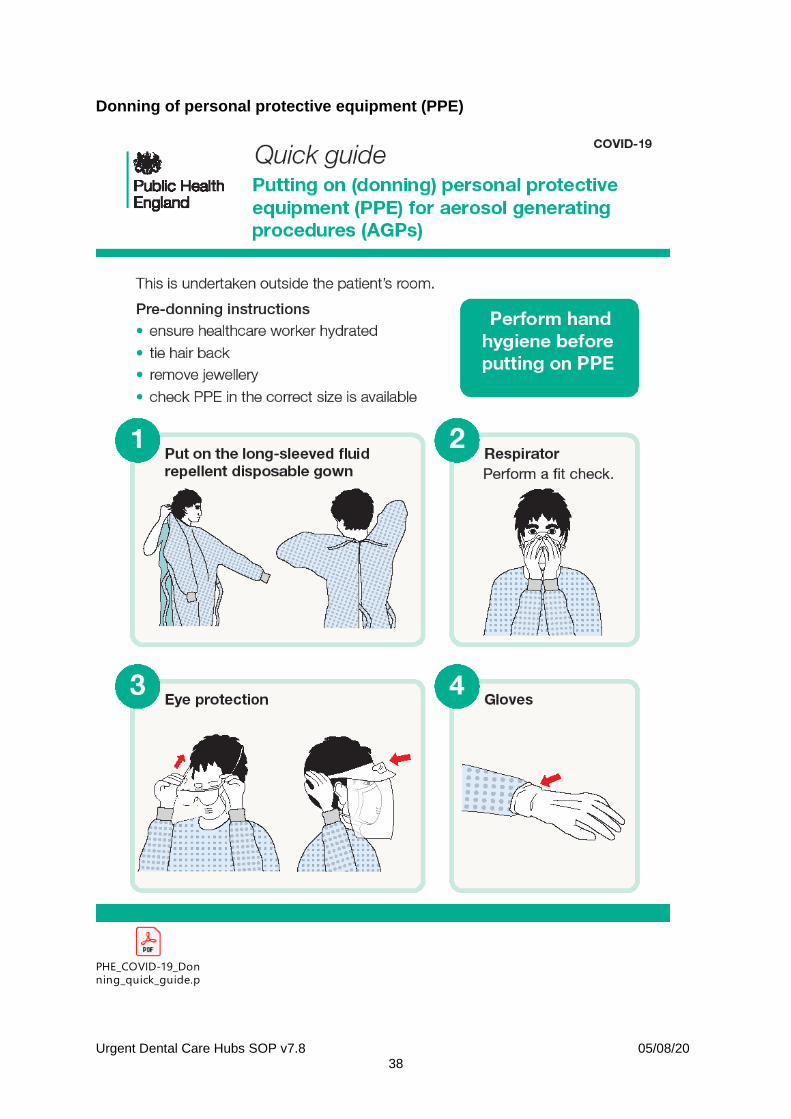
Donning of personal protective equipment (PPE)
PHE_COVID-19_Don
ning_quick_guide.pdf
Urgent Dental Care Hubs SOP v7.8 05/08/20 39
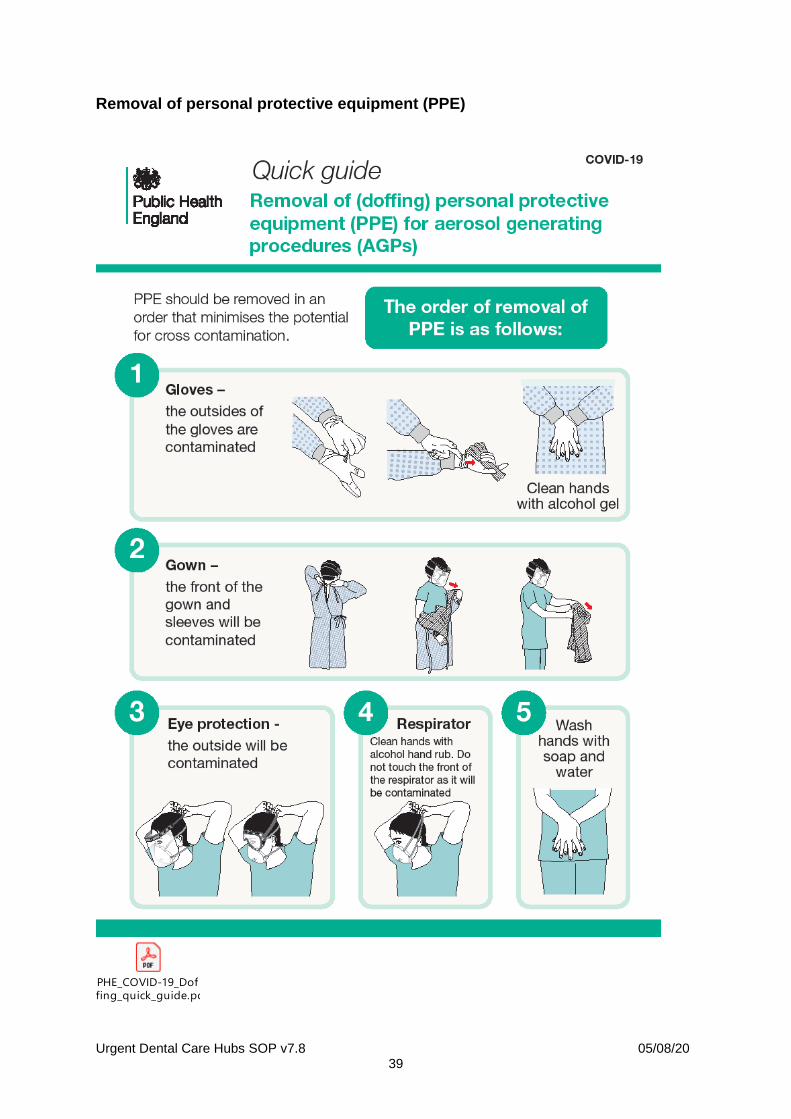
Removal of personal protective equipment (PPE)
PHE_COVID-19_Dof
fing_quick_guide.pdf
Urgent Dental Care Hubs SOP v7.8 05/08/20 40
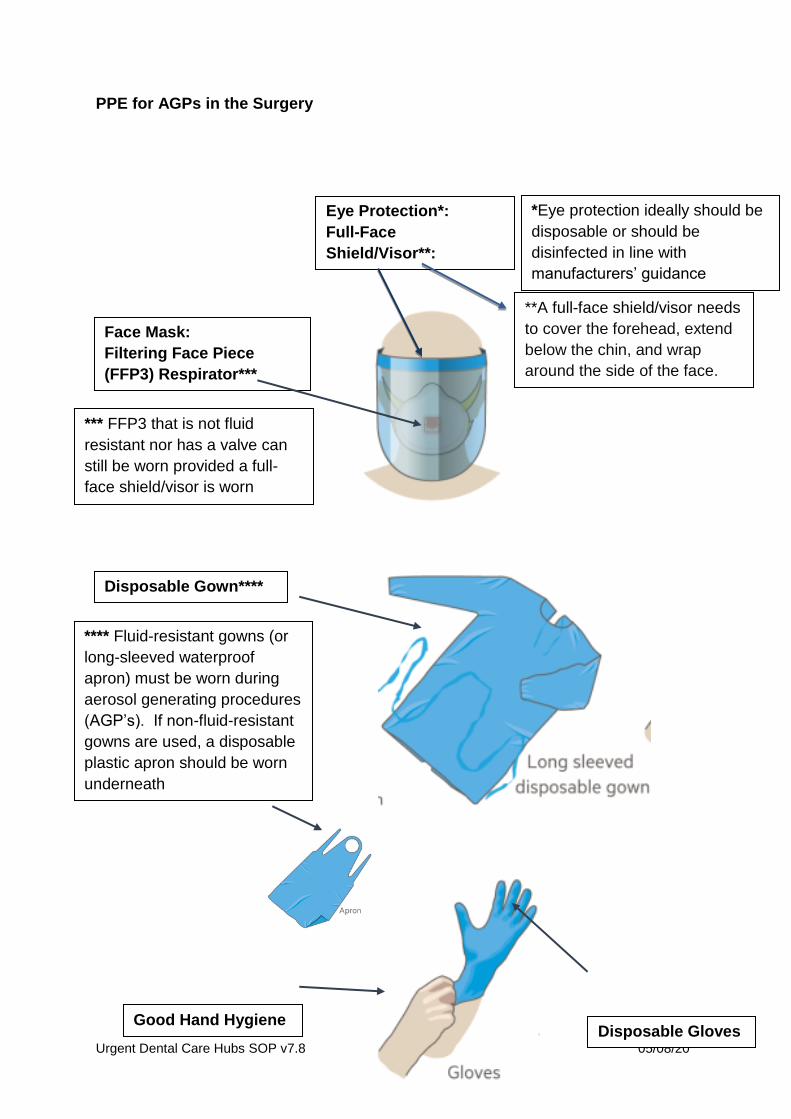
PPE for AGPs in the Surgery
Eye Protection*:
Full-Face
Shield/Visor**:
*Eye protection ideally should be
disposable or should be
disinfected in line with
manufacturers’ guidance
Face Mask:
Filtering Face Piece
(FFP3) Respirator***
*** FFP3 that is not fluid
resistant nor has a valve can
still be worn provided a full-
face shield/visor is worn
Disposable Gown****
**** Fluid-resistant gowns (or
long-sleeved waterproof
apron) must be worn during
aerosol generating procedures
(AGP’s). If non-fluid-resistant
gowns are used, a disposable
plastic apron should be worn
underneath
Good Hand Hygiene Disposable Gloves
**A full-face shield/visor needs
to cover the forehead, extend
below the chin, and wrap
around the side of the face.
Urgent Dental Care Hubs SOP v7.8 05/08/20 41
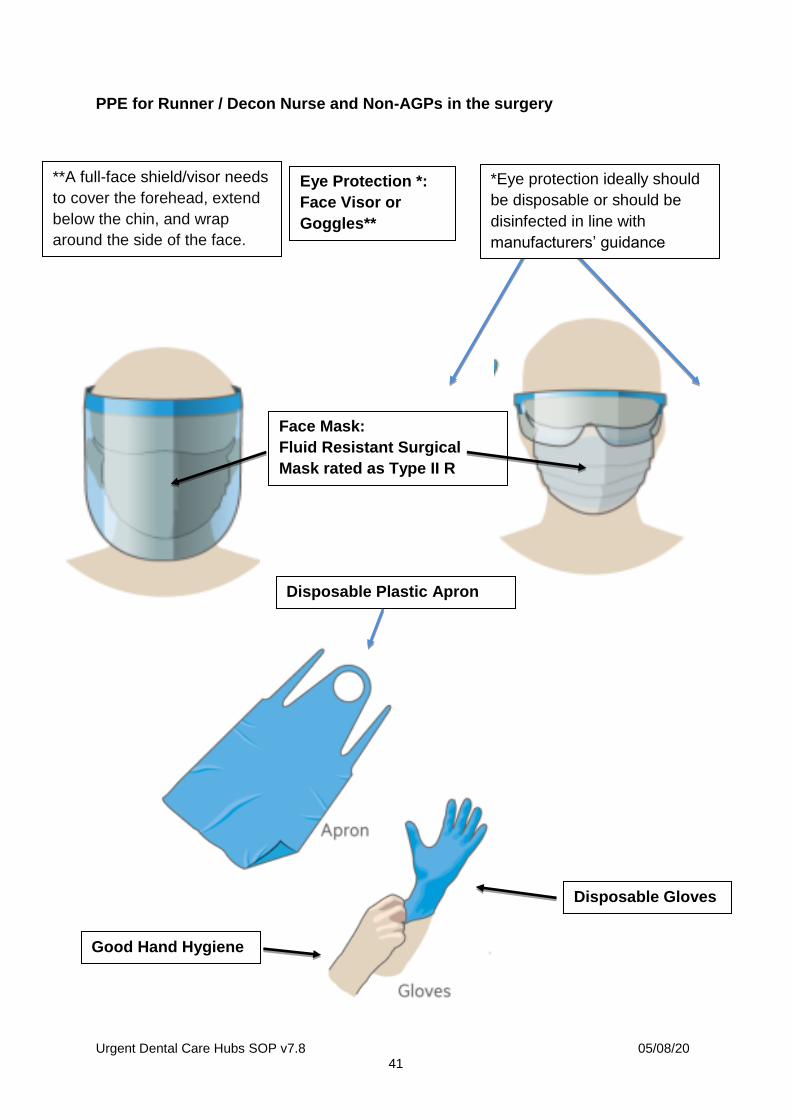
PPE for Runner / Decon Nurse and Non-AGPs in the surgery
Eye Protection *:
Face Visor or
Goggles**
Face Mask:
Fluid Resistant Surgical
Mask rated as Type II R
Disposable Plastic Apron
*Eye protection ideally should
be disposable or should be
disinfected in line with
manufacturers’ guidance
Good Hand Hygiene
Disposable Gloves
**A full-face shield/visor needs
to cover the forehead, extend
below the chin, and wrap
around the side of the face.
Urgent Dental Care Hubs SOP v7.8 05/08/20 42
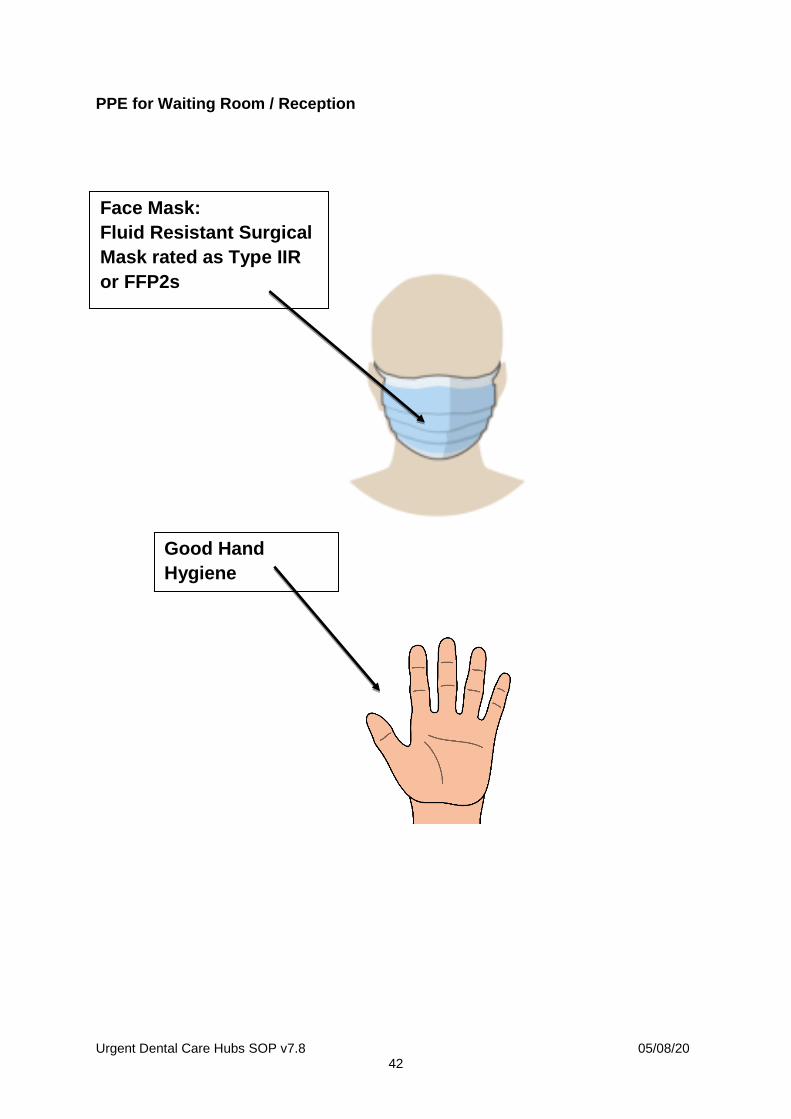
PPE for Waiting Room / Reception
Face Mask:
Fluid Resistant Surgical
Mask rated as Type IIR
or FFP2s
Good Hand
Hygiene

Urgent Dental Care Hubs SOP v7.8 05/08/20 43
Urgent Dental Care Hubs SOP v7.8 05/08/20 44
Secondary triage flow chart references
Note: open embedded PDF to click on URLs.
Flow chart PDF file (open for access to URLs):
Flow Chart for
structuring decision making at Secondary Triage in UDCs ~ May 2020v3.pdf
Urgent Dental Care Hubs SOP v7.8 05/08/20 45
PHE video: removal and disposal of PPE
https://www.youtube.com/watch?v=oUo5O1JmLH0&feature=youtu.be
Using a FFP3 respirator
Frequently Asked Questions on wearing PPE
Frequently_asked_q
uestions_on_wearing_PPE_v1.pdf
Recommended PPE for primary, outpatient and community care by setting,
NHS and independent sector
T2_Recommended_
PPE_for_primary_outpatient_and_community_care_by_setting_poster.pdf
Management of acute dental pain in adults within the AAA triaging necessary
with COVID-19
AAA Guidance doc
on Pain and AB management for triagers in Covid 19 - ver6.pdf
Urgent Dental Care Hubs SOP v7.8 05/08/20 46
Declaration Template
Dear
Thank you for agreeing to work in the Urgent Dental Clinic in the South East of
England.
Please can you read below, tick the boxes and sign the form. Please email to XXX
I confirm that I have:
Valid indemnity insurance
GDC registration with no fitness to practice
restrictions
On NHS National Performer List
Up-to-date Hep B status
Up-to-date IRMER
DBS check
Up-to-date BLS and medical emergency
training
PIN Number for FP17 transmissions
Name
Signature (electronic)
Date
Declaration
template.docx
Urgent Dental Care Hubs SOP v7.8 05/08/20 47
Feedback template
A group will meet weekly to consider any changes to this document. If you would
like to suggest any changes or additions then please complete the following
document and e-mail to [email protected].
Feedback
template.docx
Health Protection Team Contact Details
Dental practices in SE region can contact the Health Protection Team (HPT) for any
queries relating to Health Protection (e.g. procedure for the practice if there is a staff
member reporting COVID-19 symptoms) or to alert the HPT if they have two or more
confirmed cases of COVID-19 in their practice.
The HPT contact details are as follows:
Non-urgent enquires:
Kent: [email protected]
Hampshire & IoW: [email protected]
Surrey & Sussex: [email protected]
Thames Valley: [email protected]
Urgent enquiries: contact 0344 225 3861 between 9am and 5pm and select:
Option 1 for Kent
Option 2 for Hampshire and IoW
Option 3 for Surrey & Sussex
Option 4 for Thames Valley
Urgent Dental Care Hubs SOP v7.8 05/08/20 48
References and Further Guidance
1. SDCEP guidance – describes protocols for management of acute dental care
problems during COVID-19 pandemic: http://www.sdcep.org.uk/wp-content/uploads/2013/03/SDCEP+MADP+Guidance+March+2013.pdf
2. FGDP guidance – prescribing standard operating procedure: https://www.fgdp.org.uk
3. British National Formula – Dental Practitioner’s Formulae, drug interactions, indications, contra-indications and doses: https://bnf.nice.org.uk/guidance/emergency-supply-of-medicines.html
4. Chief Dental Officer’s Letter of Preparedness to practice in primary care – current guidance stating routine dentistry is ceased as of 25th March 2020: https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/03/issue-3-preparedness-letter-for-primary-dental-care-25-march-2020.pdf
5. Chief Dental Officer: Issue 4 Preparedness Letter for Primary Dental Care 15 April 2020: https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/03/C0282-covid-19-dental-preparedness-letter-15-april-2020.pdf
6. COVID-19 guidance and standard operating procedure: Urgent dental care systems in the context of coronavirus: https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/04/C0282-covid-19-urgent-dental-care-sop.pdf
7. British Endodontic Society – Guidelines on urgent endodontic procedur:
https://britishendodonticsociety.org.uk/wp-content/uploads/2020/03/BES-Emergency-Protocol-FINAL-DOCUMENT-29-MARCH-2020.pdf
8. General Dental Council – Guidance on remote consultations and prescribing:
https://www.gdc-uk.org/docs/default-source/guidance-documents/high-level-principles-remote-consultations-and-prescribing.pdf
9. NHS England – Coronavirus SOP for primary care settings:
https://www.england.nhs.uk/publication/coronavirus-standard-operating-procedures-for-primary-care-settings/
10. Mental Capacity Act:
http://www.legislation.gov.uk/ukpga/2005/9/contents
11. British Orthodontic Society – Management of orthodontic emergencies during COVID-19: https://www.bos.org.uk/Portals/0/Public/docs/Advice%20Sheets/COVID19%20FACTSHEETS/Flow%20and%20Protocol.pdf
Urgent Dental Care Hubs SOP v7.8 05/08/20 49
12. Chief Dental Officer of Scotland letter on Aerosol Generating Procedures –
explains what procedures are aerosol generating: https://www.fgdp.org.uk/sites/fgdp.org.uk/files/editors/2020.03.18%20CDO%20Scotland%20COVID-19%20letter%20on%20remuneration%20and%20AGPs.pdf
13. British Association of Oral & Maxillofacial Surgeons: https://www.baoms.org.uk/professionals/omfs_and_covid-19.aspx
14. Resuscitation Council UK: Statements on COVID-19 CPR and Resuscitation:
https://www.resus.org.uk/media/statements/resuscitation-council-uk-statements-on-covid-19-coronavirus-cpr-and-resuscitation/



























