Embed Size (px)
DESCRIPTION
Marjo-Riitta J ä rvelin , MD, MSc , PhD, Paediatrician Professor and Chair in Life-Course Epidemiology. Identifying causal pathways in longitudinal analysis using structural equation modelling. NFBC 1966 – 1986 Northern Finland Birth Cohorts. Ralph and Eve Seelye Charitable Trust, - PowerPoint PPT Presentation
Citation preview

NFBC 1966 – 1986Northern Finland Birth Cohorts
Marjo-Riitta Järvelin, MD, MSc, PhD, PaediatricianProfessor and Chair in Life-Course Epidemiology
Identifying causal pathways in longitudinal analysis using structural equation modelling
Ralph and Eve Seelye Charitable Trust, Liggins Institute Trust
EurHealthAging

Main points of presentation• Life course epidemiology:
Why longitudinal approaches? General issues (philosophy), re-cap of study
designs
• Statistical models: Practical approach – how do you plan your analyses?
Introduction into methodology (examples: weight, BP)
• In Practice - FTO gene and obesity
- Gene clusters (encoding nicotinic acetylcholine receptor subunits / dopamine metabolism), life
course and smoking behaviour
• Potential biases: Missing data, measurement error

Life course epidemiologyAnalytical issues
• Life course epidemiology involves the study of how health is related to factors operating at different stages earlier in life or across generations.
• Essentially, aim is to relate a ‘distal’ outcome to various exposures that are temporally ordered and also may:• belong to different dimensions (biological, social ...hierarchical... )• change over time (when repeated observations are involved)• be causally related
• Approach not that new but possible only when data are available over relevant periods. However, completeness, quality and coverage are variable – methodological challences (new ”dawn” of longitudinal epuidemiology)

GENOTYPE Health/DiseaseAdverse trait
Maternal genotype
Paternal genotype
Environments
prenatal postnatal childhood adult
malnutritionstressDiseaseSmokingDrinking
diseasehealth education
diet smokingexercise alcohol
marital statushousingsocioeconomic statusHealth behaviour
TO SUMMARISE : Determinants of health over the lifecourse (DEVELOPMENTAL PLASTICITY)
KEY Q: WHAT ARE THE RELATIVE ROLES OF GENETIC AND ENVIRONMENTAL FACTORS? DoHAD = Developmental Origins of Health and Disease
Sustainable communities and places
Examples
Accumulation of positive and negative effects on health and wellbeing
Healthy Standard of LivingPrevention

Tens of different phenotypes have been associated with deviant foetal growth (birth weight, BW) and other pregnancy
related factors by now - analyses are demanding
Foetal growth/ maternal health
Birth weight – as a marker
Musculo-skeletal, dental health
Asthma, atopy, lung function, infections,
Immune system
Metabolic disease and
intermediate disease markers ; BP, LIPIDS
Schizophenia, mental disorders
Behavioural disorders
ADHD
Health Behaviour, personality,
cognitive function
Reproduction, abortions, PCOS, males
Development and Disabilities
[CP, epilepsy, intelligence]Prediction - Paula’s interest!

Longitudinal settings – key issuesfrom analyses point of view
1) Design of the Study - nature of the data (binary/continuous; accuracy)
2) Longitudinal outcome measures– Linear mixed models to deal with correlated
measurements and to allow for individual variation [Growth, blood pressure models, for example]
3) Longitudinal exposures/several exposures over the life-course– ’Life-course epidemiology’

Statistical models (life-course)Aim is to :• relate a distal outcome to factors arising at earlier ages and/or
earlier generations
Standard multivariable regression approach (example next):• regress the distal outcome on all these factors. This:
• gives estimates of effect for each factor, holding the others constant (re-cap – standard linear regression)
• not adequate approach to address the aim if we are interested in the web of relations surrounding that exposure
Multivariate joint regression approach:• specify the joint distribution(interrelationships) of all the
variables in the diagram. That is, define a multivariate (as opposed to multivariable) model that corresponds to the causal diagram (Greenland & Brumback, 2005)

8
Oulu
STUDIES ON BLOOD PRESSURE - Northern Finland 1966 and 1986 Birth Cohort (NFBC)
Programme Whole population in the area
in 1966 604 000
in 1986 630 000
Study populations
1) Women (parents) and births with expected dates of delivery for year 1966 (N=12,231) and between (thesis in 1969)
2) 1 July 1985 and 30 June 1986 (N= 9479)
~ 13
00 k
m

NFBC 1966 AND 1986 – milestones in data collection
12-16gw birth 1y 7 8 14-16 24-29 31 46 (clinics ongoing)
NFBC1966n=12231 96%
NFBC 1986N=947999%
Profs. P Rantakallio, A-L Saukkonen, A-L Hartikainen, M-R Jarvelin

Example: Association between birth weight and adult SBP at age 31 years in the NFBC1966
A multivariable regression approach (standard)
Variable β (SE)
Model 1 (unadjusted)
BW (kg) -7.13 (3.04)
Model 2 (adjusted for gender)
BW (kg) -5.92 (2.73)
gender (male vs. female) 13.94 (2.54)
Model 3(adjusted for gender and BMI at 31y)
BW (kg) -6.72 (2.63)
gender (male vs. female) 12.04 (2.53)
BMI31 (kg/m2) 0.78 (0.24)

Statistical models (life-course)Aim is to :• relate a distal outcome to factors arising at earlier ages
and/or earlier generations.Standard multivariable regression approach:• regress the distal outcome on all these factors. This:
• gives estimates of effect for each factor, holding the others constant
• not adequate approach to address the aim if we are interested in the web of relations surrounding that exposure.
Multivariate joint regression approach (example):• specify the joint distribution (interrelationships) of all the
variables in the diagram (”spider diagram”). That is, define a multivariate (as opposed to multivariable) model that corresponds to the causal diagram (Greenland & Brumback, 2005). (in the next slide BP=Blood Pressure, BMI=Body Mass Index)

Maternal Smoking at the 2nd Month of
Pregnancy
Maternal Pre-
Pregnancy BMI
Parity
Family SES at Birth
BMI at Birth
Gestational Age
GenderAlcohol
Use at Age 31 Years
DISTAL PHENOTYPE
–BP, BMI..
SES at Age 31 Years
BMI at Age 14 Years
GENE- FTO
Physical Activity at Age
31 Years
Alcohol Use at Age 14 Years
Smoking at Age 14 Years
Maternal Age
Smoking at Age 31
Years
Physical Activity at
Age 14 Years
Family SES at Age 14
Years
Diet at Age 31 Years
Maternal Blood Pressure During
Pregnancy
Prenatal Birth Childhood Adolescence Adulthood
1. ”Spider diagram” challenge -
life-course analyses of FTO using path analysis (SEM)

Two approaches:
a) Structural Equation Models (SEMs, Bollen, 1989; Skrondal & Rabe-Hensketh,2003):general family of multivariate models that include pathanalysis, factor analysis, latent growth models, . . .
b) Chain Graph models (Cox & Wermuth, 1996; Edwards,2000):
In specific settings the two approaches overlap
.
Multivariate joint regression models

How to begin with the analyses? - Think of relevant variables
- Build your model piece by piece
- Simple example first of complex model
Maternal BMI
Maternal smoking
Parity
SES
Birth weight
Gestational age
Gender
BMI at 14y
Alcohol useSmoking
BMI AT 31Y
BLOOD PRESSURE
Genetic effects
SES
Submodel 1Submodel 2

Example: Association between birth weight and adult SBP in the NFBC1966
A path model approach
Consider a model where one of the explanatory factors,adult BMI, is also an intermediate outcome:
Gender
BW (kg)
BMI 31y (kg/m2) SBP (mmHg) 31y

A path model approachModel specification
The algebraic specification corresponding to this diagram isa set of simultaneous equations. Assuming linear relations:
BMI31 = α1 + β11gender + β12BW + e1
SBP31 = α2 + β21gender + β22BW + β23BMI31 + e2

A path model approachResults (β, unit= kg/m2 for BMI at 31y or mmHg for SBP at 31y)
Variable β (SE)
Model for BMI31 (kg/m2)
BW (kg) 0.47 (0.11)
gender (male vs. female) 0.97 (0.11)
Model for SBP31 (mmHg)
BW (kg) -6.35 (1.98)
gender (male vs. female) 12.20 (2.58)
BMI31 (kg/m2) 0.77 (0.23)
BMI31 is an ‘endogenous’ variable: it is a dependent and also an explanatory variable.

A path model approachGraphical results with β (unit= kg/m2 for BMI or mmHg for SBP)
Birth weight and gender have both a direct and an indirect effect on adult SBP
Variable β (SE)
Model for BMI31 (kg/m2)
BW (kg) 0.47 (0.11)
gender (male vs. female)
0.97 (0.11)
Model for SBP31 (mmHg)
BW (kg) -6.35 (1.98)
gender (male vs. female)
12.20 (2.58)
BMI31 (kg/m2) 0.77 (0.23)
Gender
BW (kg)
BMI 31y (kg/m2)
SBP (mmHg) 31y
0.97
0.47
0.77
12.20
-6.35

A path model approachDirect and indirect effects
Birth weight and gender have both direct and indirecteffects on adult SBP.
Their indirect effects can be quantified by multiplying theregression coefficients along the indirect pathway.
• indirect effect of BW:1 kg in BW → BMI at 31→ SBP at 31: 0.47 × 0.77= 0.37• direct effect of BW:1 kg in BW → SBP at 31: -6.35
These should be added to make up the total, i.e. marginal,effect -5.98 (0.37+(-6.35)).

Standard multivariable regression vs. path analysis
Variable β (SE)
Standard multivariable regression (adjusted for gender and BMI31)
BW (kg) -6.72 (2.63)
Path analysis
BW (kg)
direct effect -6.35 (1.98)
indirect effect 0.37 (0.14)
total effect -5.98 (1.96)
• Multivariable regression provides a direct effect estimate of the association conditional on all the other variables in the model (past and future, no order time-wise)
• Causality not addressed, i.e. no information on possible mediation (indirect effects) on the causal pathway.

Adjusted for perinatal factors: sex, gestational age, parental social class, parity, maternal height and pre-pregnancy weight, maternal smoking during pregnancy
Jarvelin et al. Hypertension, 44:838-846, 2004
122.5
123.5
124.5
125.5
126.5
127.5
128.5
129.5
130.5
<2500 -2999 -3499 -3999 -4499 >=4500
SBP [mmHg]
p < 0.03
Systolic blood pressure (mmHg, 95% CI) at 31 years and birth weightfor WHOLE COHORT (solid line) and for SINGLETONS (dotted line),
N=5960
Birth weight [g]

Another ”look” with full data - path analysis approach: Blood pressure levels in adulthood - draw a figure! Web of variables during the life course – which variables to choose?
Maternal BMI
Maternal age
Maternal smoking
Parity
SES
Prenatal Birth Adolescence Adulthood
Birth weight
Gestational age
Gender
BMI at 14y
Alcohol use
Smoking
BMI at 31y
BLOOD PRESSURE
Genetic effects
SES

More Complex analyses: MODELLING STRATEGY - EXAMPLENorthern Finland Birth Cohort 1966
- To identify sensitive periods growth and relative impact of growth and other factors (e.g. Genetic factors)
• Population-based birth cohort, N=12231• Recruitment
– Pregnant mothers living in the provinces of Oulu and Lapland
– Expected delivery date in 1966
• Data collection:– Maternal background and pregnancy data– Follow-ups at 1y, 14y and 31y
• Clinical examination and postal questionnaires at 31y including DNA samples (N=5753)
24 gw birth 1y 14y 31yhttp://kelo.oulu.fi/NFBC

A more complex setting: Analytical strategy
1) Select relevant variables and order them along the life course
2) Select outcomes (intermediate and distal) based on your hypothesis and data (chronological order etc.)
Maternal age
Maternal BMI
Parity
Family SES
Birth weight
Gestational age
Gender
Alcohol use at 31y
Smoking at 31y
BMI at 31y BP at 31y
Genetic effects
SES at 31y
Maternal smoking
Maternal BP
BMI growth velocity birth-AP
BMI growth velocity AP-
AR
BMI growth velocity 11-
15y
Physical activity at 31y
Diet at 31y
Prenatal Birth Adolescence AdulthoodInfancy Childhood
AP=adiposity peak; AR=adiposity rebound

Typical change in infant/child BMI
BMI at AP
Age at AP
BMI at AR
AP = adiposity peak AR = adiposity rebound
Age at AR

A more complex setting: Analytical strategy
1) Select relevant variables and order them along the life course
2) Select outcomes (intermediate and distal) based on your hypothesis and data (chronological order etc.)
Maternal age
Maternal BMI
Parity
Family SES
Birth weight
Gestational age
Gender
Alcohol use at 31y
Smoking at 31y
BMI at 31y BP at 31y
Genetic effects
SES at 31y
Maternal smoking
Maternal BP
BMI growth velocity birth-AP
BMI growth velocity AP-
AR
BMI growth velocity 11-
15y
Physical activity at 31y
Diet at 31y
Prenatal Birth Adolescence AdulthoodInfancy Childhood
AP=adiposity peak; AR=adiposity rebound

3) Test associations in your submodels (Chi square tests, correlation coefficients, regression analyses) and specify if the associatios are linear / non-linear (nature of assoc)
4) Think of biologically plausible pathways and combine the submodels into one pathway model
5) Run path analyses and use different goodness of fit indices to evaluate the model fit
6) Omit variables and paths that do not seem necessary, allow some variables to correlate, add relevant paths etc to improve model fit
7) Rerun the modified model
A more complex setting: Analytical strategy

Modelling scheme:

Summary and conclusions
• Strong evidence that BW is inversely associated with adult BP, taking into account postnatal growth and several other factors along the causal pathway
• Postnatal growth especially from AR onwards is positively associated with adult BP
• BMI growth between AP-AR (in females) and AR-11y (in males) also negatively directly associated with adult BP, i.e. slow growth during these periods is associated with higher adult BP regardless of growth later in life

Model estimation
Inference is based on the multivariate likelihood function; the maximum likelihood approach
Software: in Stata, MPlus, LISREL, Amos, SAS and R (but for less general models).

Path modelAssessment
i) With no missing values: same results by fitting separateunivariate regression models
ii) Goodness of fit can be judged using several indices andcriteria:
• Chi-square test on the correlation matrix• SRMR: Standardized root mean square residual• RMSEA:Root Mean Square Error of Approximation• CFI: Comparative Fit Index
iii) However model could be biased e.g. because of:• unaccounted confounding factors (Hernan et al, 2002)• model misspecification: e.g. due to interactions,non-linearities.• poor data quality
iv) Points above valid more generally
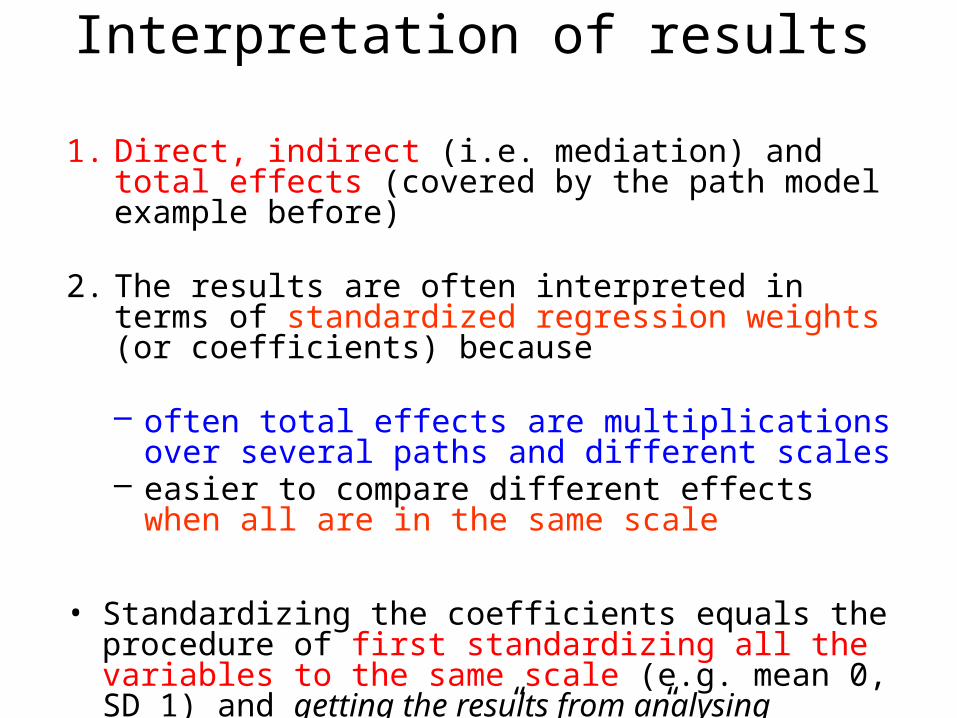
Interpretation of results
1. Direct, indirect (i.e. mediation) and total effects (covered by the path model example before)
2. The results are often interpreted in terms of standardized regression weights (or coefficients) because
– often total effects are multiplications over several paths and different scales
– easier to compare different effects when all are in the same scale
• Standardizing the coefficients equals the procedure of first standardizing all the variables to the same scale (e.g. mean 0, SD 1) and getting the results from analysing standardized variables ”SCALING”..

Standardized regression weights
• For continuos covariates:
bSTDYX=b*SD(X)/SD(Y)
= the change in Y in Y SD units for a standard deviation change in X
• For binary covariates:bSTDY=b/SD(Y)
= the change in Y in Y SD units when X changes from 0 to 1

Standardized regression weightsExample
Height Y: Mean(Y)=164.7, SD(Y)=6.3Weight X: Mean(X)=64.9, SD(X)=11.9
height=a + b*weight +e
b=0.17: – one kg increase in weight increases height by 0.17cm
bSTDYX=0.17*11.9/6.3=0.32 – a SD change in X (11.9 kg) increases Y by 0.32 Y SD
units, i.e. 0.32*6.3cm=2.02cm

Model estimation
Inference is based on the multivariate likelihood function; the maximum likelihood approach
Software: in Stata, MPlus, LISREL, Amos, SAS and R (but for less general models).

Potential biasesOur interpretation of results obtained from a multivariatemodel depends on the appropriateness of the assumedstructure and the quality of the available data.
We cannot interpret the estimated effects as causal withoutconsidering whether:
• conceptual model is correct; need to ask questions like
Are there any unaccounted confounding factors? Are the measures of effect specified on the correct scale?
• the quality of the data is satisfactory: Are the data affected by:
1) measurement error?2) systematic missingness?

Rubin’s classification (1987):
MCAR: missing completely at random;MAR: missing at random;MNAR: missing not at random
If missingness is assumed to be MAR,one approach isMultiple Imputation (MI). Its aim is to integrate the‘substantive’ model likelihood over the missing values.
In practice MI consists of an imputation step and ananalytical step which are repeated m times (for stability andassessment of precision).
Missing data bias

• allows the joint estimation of complex relationships
• assumptions underlying these relationships -althoughmostly untestable- are all explicit
• allows dealing with measurement error directly (alsocan deal with misclassification within the sameframework)
• allows dealing with missing values directly (assumption of MAR)
• assuming model is correct, gives estimates of directand indirect effects
Disease mechanisms.... With reservations
Advantages of a multivariate approach -

• heavily structured
• estimated direct and indirect effects may be grossly biased (and difficult)
• other approaches (e.g. marginal structural models -Hernan et al, Epidemiology, 2004) make fewerparametric assumptions (especially regardingunmeasured confounders) and therefore are morerobust (but could be less efficient if the equivalent SEMwere correct)
Disadvantages of a multivariate approach

These analytic strategies open new ways of understanding better disease mechanisms
Need for a very careful interplay of:
1) subject-knowledge2) data gathering across different sources – time periods3) model specification and fitting to deal with:
Structure: Quality:temporal associations measurement error‘causal’ association missing values
proxy variables
4) sensitivity analyses on the less developed sections5) comparisons across different studies – REPLICATION!
Summary, message...

Smoking and Blood Pressure
• Several studies show lower BP in smokers (Leone 2011. Cardiol Res Pract 2011: 264894)
• BUT, in the long run, smoking increases arterial stiffness thus partly contributing to rising BP (Leone 2011. Cardiol Res Pract 2011: 264894)

CHRNA - GENE CLUSTER ENCODES NICOTINIC ACETYLCHOLINE RECEPTOR SUBUNITS
TTC12-ANKK1-DRD2 – DOPAMIN METABOLISM, LINKED WITH NICOTININ USE, DEPENDENCIES
Pathways leading to smoking behaviour – reference with blood pressure

To catch-up: many types of changes in genome - single-nucleotide polymorphisms (SNPs), tandem repeats, copy number of variation (CNV), inversions, deletions
DNA molecule 1 differs from DNA molecule 2 at a single base-pair location (a C/T polymorphism)Sugar-phosphate backbone; rangs are nucleotide base pairs (C combines with G, A with T)
A = adenineT = thymineC = cytosineG = guanine
ATG CTG..“sentences”=genes
Gene -> proteins



after further adjustment for multiple testing, power issue
after adjustment for sex, BMI,PCs

Smoking at 14
Maternal smoking during
pregnancy
TTC12-rs10502172[G] CHRNA3-rs1051730[A]
Family SES at 14
SEX (F vs M)
Prenatal family SES
Maternal marital status at birth
High Novelty seeking
SES at 31
SBP at 31
Shared genetics between smoking and SBP
Smoking at 31

Conclusions and Future aspects
• Some evidence for an association between variants in the CHRNA5-CHRNA3-CHRNB4 and SBP (in smokers)
• Replication needed – CARTA – consortium; Mendelian randomization approach
• Lifecourse analyses

Maternal Smoking at the 2nd Month of
Pregnancy
Maternal Pre-
Pregnancy BMI
Parity
Family SES at Birth
BMI at Birth
Gestational Age
GenderAlcohol
Use at Age 31 Years
DISTAL PHENOTYPE
-BMI
SES at Age 31 Years
BMI at Age 14 Years
GENE- FTO
Physical Activity at Age
31 Years
Alcohol Use at Age 14 Years
Smoking at Age 14 Years
Maternal Age
Smoking at Age 31
Years
Physical Activity at
Age 14 Years
Family SES at Age 14
Years
Diet at Age 31 Years
Maternal Blood Pressure During
Pregnancy
Prenatal Birth Childhood Adolescence Adulthood
1. ”Spider diagram” challenge -
life-course analyses of FTO using path analysis (SEM)

Direct, indirect and total effects of FTO on adult BMI (standardized beta values)• Direct effect: 0.04
• Indirect effects of the FTO variant to adult BMI:– FTO-mat.BMI-BMI31: 0.03*0.095=0.003– FTO-mat.BMI-BBMI-BMI14-BMI31: 0.03*0.155*0.08*0.529=0.002– FTO-BBMI-BMI14-BMI31: 0.018*0.08*0.529=0.001– FTO-BMI14-BMI31: 0.026*0.529=0.014– Total indirect: 0.003+0.002+0.001+0.014=0.020
• Total effect: 0.02+0.04=0.06
0.095
0.5290.08
0.026
0.03
0.175
0.018
0.155
0.04
0.25
0.16

Direct, Indirect and Total Effects of FTO-rs9939609 on Body Mass Index (BMI) During the Life Course in the Northern Finland Birth
Cohort 1966 (adjusting for all other factors). Note – SES, physical activity, maternal parity had large effects
Abbreviations: BMI, body mass index; CI, confidence interval., BMI log transformed
Effect of FTO-rs99309609 P value Change in the mean level of
BMI (g/m2), per A-allele change
95% CI
Total 5.0x10-5 371 185, 570
Total indirect (via …) 0.02 121 19.6, 227
Direct 0.001 239 89.6, 396

Acknowledgements… OULUM JarvelinA TaanilaA PoutaA-L Harti-KainenM LeinonenJ VeijolaA RuokonenM IsohanniM SavolainenK-H Hertzig
HelsinkiL PalotieT PaunioJ EkelundE NymanH Mannila
KuopioJ Pekkanen+team
UppsalaA Rodriquez
CopenhagenJ OlsenT Sörensen
LONDON/UKP ElliottL CoinJ ChambersM LevinA BlakemoreJ KoonerU SovioP O’ReillyD PillasM McCarthyD CanoyG Davey SmithT FraylingG Schumann
LilleP Froquel S CauchiN Boutia-Naji
AthensC Bakoula +team
BergenE Heiervang
TampereSuvi Virtanen
LAF NelsonS SmalleyJ McCoughC SabattiS Service
BonnDLichterman
Dallas
AustraliaMcGrathL PalmerL CoinE Hypponen
BostonJ HirschhornM DalyH Lyon
NEW ZEALANDW CaulfieldW SchierdingJ O’Sullivan P Davies et al..
























![1966-1975 [WMEAT 1966-1975 185668]](https://img.pdfslide.us/doc/110x75/577cc16d1a28aba7119302de/1966-1975-wmeat-1966-1975-185668.jpg)



