Embed Size (px)
Citation preview

Non Adherence of CML Patients Results From Our Global Survey
SHARF GIORA
EBMT Swiss Nurses Working Group
Zurich- 23/11/2013

Confidential & Proprietary. Not For Public Distribution. Do Not Copy. 2
What we will cover »
The story so far
Adherence Levels
Influencers of Adherence
Demographics & Treatment
Beliefs & Motivation
Strategies for Adherence

CML Advocates Network: global network of leukemia patient groups
http://www.cmladvocates.net
Public directory of Chronic Myeloid Leukemia groups
“Social media platform” to have advocates collaborate
Build skills, coordinate campaigns, build partnerships, share knowledge
Founded 2007 by 4 advocates 82 patient organisations
in 66 countries

CML has turned from a lethal into a chronic disease in the last 15 years
15 years ago, surviving 5 years had a chance of 50:50
Today, When treated according to guidelines and high adherence, survival is close to general population
Side effects are still a problem
Psycho-oncology services often not offered
The lion is in the cage, but adherence is a serious issue

Where we are now
• The launch of imatinib, a BCR-ABL kinase inhibitor, transformed the treatment of CML, and indeed the face of oncology as a whole
• 2nd generation products, nilotinib and dasatinib, are designed to manage instances of imatinib resistance
TKIs have revolutionis
ed CML treatment so people can live longer
However, non-
adherence is a key issue in
CML
There is a clear link between
adherence and
survival rates
• Adherence is a complex and multifactorial issue, especially in medical conditions that require long-term therapy such as chronic phase CML
• A combination of internal and external factors may lead to reduced patient adherence to long-term therapies
• Both the HAMMERSMITH study and the ADAGIO study highlighted the importance of patient compliance in regards to achieving optimal treatment response
• Missing more than 2-3 daily doses each month can negatively impact response
Long Term Adherence to Imatinib Alex Bazeos et al, ASH 2009

We aimed to replace “gut feeling” by extensive solid data to better understand the problem:
Understand patient behaviours associated with adherence
And Help identify the ‘true’ issues behind non-adherence
Explore cultural influence and difference on adherence
Support development of physician and patient tools to improve adherence and improve patient outcomes

Our research was truly global: 12 languages, 2546 CML patients from 79 countries
Sample: Total of 2546 respondents
Global reach
Methodology •Online - Recruited by patient associations online & via other methods
•Paper & Pen (France, Germany, Italy) – Recruited by physicians at consultations
•CML patients over 18 years old, currently taking oral medication for CML
•Fieldwork – Started on CML World Day, 22/9 2012 – 30th January 2013
2151
395
Paper
Online
Countries with >30 respondents Countries with base <30 respondents

We used the validated Morisky Adherence Scale to classify patients into adherence levels
Questions: Forget medication
Miss for other reason
Stopped because felt worse Forgot when travelling Taken yesterday? Stop when under control Inconvenience How often having difficulty to remember
Low: 21 %
Medium: 47 %
High: 33 %
Adherence score classifies patients into
adherence groups:

Confidential & Proprietary. Not For Public Distribution. Do Not Copy. 9
Adherence Levels

Serbia
USA
Lebanon Venezuela
Poland
Russian Federation
Australia
France (Online)
Argentina
UK
France (Paper & Pen)
Philippines
Czech Republic
India
Italy (Online) Italy (Paper & Pen)
Finland
Israel
Netherlands
Thailand
Mexico
Slovenia
Germany (Online) Germany (Paper & Pen)
5
10
15
20
25
30
35
40
45
5 15 25 35 45 55 65 75 85
USA and Serbia stand out through the proportion missing doses, both accidentally & intentionally
% M
isse
d o
n P
urp
ose
in las
t ye
ar
% Missed Accidentally / Due to Circumstance in last year
“Above global average for missed
doses”
Global Average
Global
Average
“Below global average for missed
doses”

Slovenia stands out as the most adherent country via the Morisky scale
Adherence by Market - Proportion Classified as High %
F1/ base = all respondents (n=2546) Low (n=528), Medium (n=1185), High (n=833) - Please answer ‘yes’ or ‘no’ to each question based on your personal experience with your CML medication. F2/ base = all respondents (n=2546) Low (n=528), Medium (n=1185), High (n=833) - How often do you have difficulty remembering to take all your medications?
+
N.B. Higher sample size = more likelihood of a sig.
diff.

Venezuela & Australia have the lowest proportion of adherent patients according to the Morisky scale
Adherence by Market - Proportion Classified as High %
F1/ base = all respondents (n=2546) Low (n=528), Medium (n=1185), High (n=833) - Please answer ‘yes’ or ‘no’ to each question based on your personal experience with your CML medication. F2/ base = all respondents (n=2546) Low (n=528), Medium (n=1185), High (n=833) - How often do you have difficulty remembering to take all your medications?
_
_

Half have missed a dose accidentally in the last year. 2 in 10 have decided to miss a dose
Missed a dose accidentally in last month %
3 (average
doses missed in last
month)
Decided to miss a dose in last month %
8% of the sample missed both accidently and on purpose in the last month
+ Yes: Ser., USA, other Cen. & Lat. Am.
+Yes: Ser., USA
Missed a dose accidentally in last year %
11.3 (average
doses missed in last year)
Decided to miss a dose in last year %
17% of sample missed both accidently and on purpose in the last year
+ Yes: Ser., USA, other Cen. & Lat. Am.
+ Yes: USA, Russ

74% believe they take their CML medication exactly as prescribed, but 19% of them missed a dose last month
Self rated adherence (rated 1-5) %
+ Neth., Slov., Thai., It. (paper)
BUT: 19% of those who claim to always take medicine as prescribed, had in fact missed a
dose accidently in the last month. Gap between perception & reality.

Imatinib seems to be linked with higher adherence, Nilotinib is more prevalent in the low adherence group
B3a / base-all respondents (n=2546) Low (n=528), Medium (n=1185), High (n=833) - Which medication do you take for your CML currently? B3a/B6 / base=all respondents (n=2546) - Which medication do you take for your CML currently? What CML treatments, if any, did you have before you began to take the one you are currently taking?
Current Medication %
Nilotinib
Imatinib
Dasatinib
Other (incl. ponatinib) + don’t know

Nilotinib has fewer high adherers than the other two therapies
B3a / base-all respondents (n=2546) Low (n=528), Medium (n=1185), High (n=833) - Which medication do you take for your CML currently?
Current Medication vs. Levels of Adherence %
+
Nilotonib
+
Nilotonib

Those with low adherence are more likely to take their medication 2 x day & do so in the evening
Time of day that take medication %
B4a / base=all respondents (n=2546) Low (n=528), Medium (n=1185), High (n=833) - How many times a day do you take your CML medication? B4b / base=all respondents (n=2546) Low (n=528), Medium (n=1185), High (n=833) - When during the day do you usually take your CML medication?
Low adherers are also aware that the doses they miss most are their evening doses (34%)
How many times take medication % / Av.
Av. 1.3
Av. 1.3
Av. 1.4
Av. 1.3
M, H
H
M, H H
L, M L
L, M
H, M
H
H

Those within the low adherence group have a younger age profile vs. the other groups
14
12
18
17
20
18
21
20
15
20
10
14
14
12
19
17
19
19
11
7
18
16
28
20
Male / 18-40
Female / 18-40
Male / 41-55
Female / 41-55
Male / 56+
Female / 56+
Age / Gender %
A1 / base=all respondents (n=2546) Low (n=528), Medium (n=1185), High (n=833) – How old are you? A2 / base=all respondents (n=2546) Low (n=528), Medium (n=1185), High (n=833) – What is your gender?
Total High Medium Low
M, H
H H
H
L
L
L, M
L
Young
er
Old
er

Forgetting & routine interruption primary reasons for accidental, side effects for intentional non-adherence
Reason for missing accidentally % (n=1283)
C2d / n=1283 - Which circumstances led to a missed dose of your medication? C5 / n=491 - Why did you decide to miss a dose of your medication? C6 / n=126 - Which side effect(s) were you hoping to avoid by intentionally missing one or more doses of your medication?
Reason for deciding to miss % (n=491)
Whilst accidental missing is more linked to memory, purposeful missing of doses is more related to physical symptoms

My health depends on my CML medication
I have been told I need to take every dose of my CML treatment or the treatment may not work
I worry if I miss a dose of my CML medication
I worry about the long term effects of my CML medication
Having to take my CML medication worries me
My CML medication impacts my work life
My CML medication impacts my social life
My CML medication disrupts my life
It is ok to miss a few doses of my CML medication every now and then
I find it difficult to swallow my CML medication
I find it difficult to open / close the CML medication packages
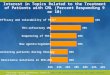
Low adherence group worries more about QOL and long term side effects, and is not clear about consequences Attitudes towards CML treatment by adherence groups (top 3 box%)
C8 / base=all respondents (n=2546). Low (n=528), Medium (n=1185), High (n=833) When thinking about your CML medication, please indicate the extent to which you agree with each of the following statements? (Please indicate for each item below on a scale of 1-7 where 1=strongly disagree and 7=strongly agree)
H, M
H, M
H, M
H, M
H, M
H, M
H, M
H
H, M
L
H, M
H
H
H
H
H

Joint responsibility: Adherence is strongly influenced by doctor-patient relationship
High adherence group is more likely to discuss missing a dose with their physicians
High adherence group is more satisfied with info received from HCPs & HCPs is perceived to be approachable
Accidentally HIGH LOW „Yes always“ 83 % 47 %
Intentionally HIGH LOW „Yes always“ 85 % 48 %
Info received HIGH LOW „Very satisfied“ 69 % 45 % „Not satisfied at all“ / „Somewhat dissatisfied“ 4 % 16 %
HCP is approachable HIGH LOW „Very approachable“ 73 % 53 % „Not very approachable“ 7 % 14 %

What can patients groups do?
Improve communication on adherence between patients and physicians
Raise the profile of adherence issues in the community - patient information, meetings, doctors, relatives, industry!
Support with routines, provide reminders.

Reminders from family members & pill dispensers are primary tools used, followed by electronic reminders
Tool Usage (%)
Possible future niche in mobile applications for over ¼ of patients
E2 base = all respondents (n=2546) Below is a list of tools that could help you to remember to take your CML medication. For each item, please indicate whether you already use such a tool, or if you would use the tool if it were available

Conclusion
Patients do not want to be patients. Daily drug taking reminds them that they are sick.
"This is cancer! Of course my patient is taking his medicine" is mostly a misled assumption.
There are risk groups like younger patients, longer time on
treatment, Taking the drug twice a day that need special attention.
There are intentional and non-intentional mechanisms of non-adherence. Physicians and patient groups need to address them jointly.

Thank you! To the CML patients in 79 countries that participated. To the CML patient organisations supporting the survey. The Workgroup: Giora Sharf, Verena Hoffmann, Felice Bombaci, Mina Daban, Fabio Efficace, Joëlle Guilhot, Jana Pelouchová, Euzebiusz J. Dziwinski, Jan de Jong, Anthony Gavin, Jan Geissler Our Partners: German CML Study Group, GIMEMA Italy, French FI LMC Group
Come and visit our poster at ASH