Embed Size (px)
Citation preview

Newborn Screening for
Congenital Hypothyroidism
QLD Update
Paediatric Society of Queensland Meeting 201820th October 2018
Dr Tony HuynhPaediatric Endocrinologist – Queensland Children’s Hospital
Chemical Pathologist – Mater Pathology

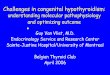
Thyroid hormone synthesis
Thyroid hormone synthesis secretion and major signaling pathways in
thyrocytes. AC, adenylyl cyclase; cAMP, cyclic AMP; DAG,
diacylglycerol; DEHAL1, iodotyrosine dehalogenase 1; DIT,
diiodotyrosine; DUOX, dual oxidase 2; DUOXA2, dual oxidase
maturation factor 2; KCNQ1 and KCNE2, potassium channel subunits;
MCT8, monocarboxylate transporter 8; MIT, monoiodotyrosine; NIS,
sodium/iodide symporter; PDS, pendrin (SLC26A4, solute carrier
26A4); PKA, protein kinase A; PLC, phospholipase C; TG,
thyroglobulin; TPO, thyroid peroxidase; TSH, thyrotropin; TSHR, TSH
receptor.
Cherella CE and Wassner AJ. Int J Pediatr Endocrin 2017

Congenital causes of hypothyroidism

Congenital hypothyroidism
• One of the most common preventable causes
of intellectual impairment world-wide
• Increasing incidence detected by NBS
– 1:4000 in mid-1970s to 1:2000 by 2010
– Due to lowering of TSH cut-offs (identifying milder
cases); more births in populations with higher
incidence
• Inverse relationship between age of treatment
initiation and IQ
Klein AH et al. J Pediatr 1972, Ford G and LaFranchi SH. Best Res Clin Endocrinol Metab 2014; Corbetta C et al. Clin Endocrinol 2009.

History of NBS in Australia
• 1960s: Phenylketonuria
• 1970s: Congenital hypothyroidism
– Primary TSH strategy
• Recent advances
– MS-based techniques for IEM
– Genetic analysis
• Different state-based practices
• CAH recently approved by DoH
– Not yet implemented in QLD

Newborn Screening Unit
QLD Maternity Hospitals (2017) – approximately 61000 births
Public – 61
Private - 18

Pathology Queensland – NBS TSH screen
Notification algorithm up to 2018TFT repeated two weeks after birth
for all babies <1500g and again at
four week in those <1000g.

Pathology Queensland – NBS TSH screen

• Frequency of results throughout QLD
- TSH 14-29 mIU/L: 43 cases
- TSH ≥ 30 mIU/L: 36 cases
- 45 confirmed cases of CH
• Confirmation of cases usually via laboratory
staff proactively chasing up follow-up tests
• Missed cases from 2-tier system
NBS TSH statistics - 2016

Case 1
• 3 week old male neonate
– Presentation with severe stridor and concerns about airway
obstruction
– Also vomiting, decreased feeds
• Parents from South Sudan
• Non-consanguineous marriage
• 3 year-old brother with congenital hypothyroidism – aetiology
unknown
• Term baby, SVD, good Apgars, no antenatal issues, maternal
medical history unremarkable
• “Lump in neck” noted at birth – for monitoring

• NBS TSH
– TSH result flagged abnormal result (>14mIU/L)
• Designated contact person notified via usual channels
• Follow-up did not occur
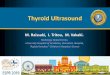
Supplementary Figure 1. Radiological investigations of the proposita at three weeks of age. (A) Magnetic Resonance Imaging of the neck showing
significant enlargement and extension of the thyroid gland, and (B) Tc-99m pertechnetate thyroid scan demonstrating significantly increased
radiotracer uptake.
A B
Case 1
Watanabe Y et al. A Novel Mutation in the TG Gene (G2322S) Causing Congenital Hypothyroidism in a Sudanese Family: A Case Report. BMC Medical Genetics 2018

• Parents from India – non-consanguineous, first
baby, no maternal or family history of thyroid
issues
• D3 abnormal screen (TSH 17mIU/L)
• Parents contacted D17 but not aware of urgency
• Recollection on D30 (TSH 16 mIU/L)
• Parents not contacted about abnormal result
• TFTs at 7 weeks (TSH 31mU/L, FT4 7.4 pmol/L)
Final diagnosis: Lingual thyroid
Case 2

Discussion points
• 2 missed cases in 18 months
• Implementation of new notification process– All TSH ≥ 14 mIU/L now requires formal TFT
• Process of identifying clinical leads within each hospital– Private hospitals more challenging
• Email system from the NSU– Paediatric clinician
– NSU
– QCH – [email protected], Endocrine nurse, Tony Huynh
• Development of Clinical Form

Clinical Feedback
• Closing the NBS loop
– Final diagnosis
– Improved clinician-
laboratory
interactions
– Guide TSH cut-off
– Research
• Establish contact
database