Embed Size (px)
Citation preview

New vaccines for Tuberculosis
Current and future perspectives
Jelle Thole
Tuberculosis Transmission

Tuberculosis in the worldAccording to latest WHO data, in 2006:
14.4 million prevalent cases of TB 9.2 million new cases, 0.7 million in HIV-positive
people 1.7 million TB-related deaths, 0.2 million in HIV-
positive people 0.5 million case of multidrug-resistant cases (MDR-
TB)
Drug resistance and TB/HIV co-infection are keybarriers to progress

Estimated numbers of new cases, 2006
No estimate0–999
10 000–99 999100 000–999 999
1 000 000 or more
1000–9999
Estimated number of new TBcases (all forms)
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the WorldHealth Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or
boundaries.Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
© WHO 2006. All rights reserved

Worldwide Distribution of New TB Cases, 2006
New TB cases per 100,000 population in 2006
No estimate0-24
50-99
100-299
300 or more
25-49

TB/HIV Coinfection
TB is the most common presenting illness among peopleliving with HIV on ARV treatment worldwide
TB is the leading cause of death among HIV positiveindividuals in Africa
85% of 217,000 people that died of HIV associated TB in2006 people lived in Sub-Saharan Africa
At least 1/3 of the 33.2 million people living with HIV arealso infected with TB and have a greater risk ofdeveloping TB disease (5-10 % annually)

Estimated HIV prevalence in new TB
cases, 2006
No estimate
0–4
20–49
50 or more
5–19
HIV prevalence in
TB cases, (%)
The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on th e part of the World Health
Organization concerning the legal status of any country, territo ry, city or area or of its authorities, or concerning the delimi tation of its frontiers or boundaries.
Dotted lines on maps represent approximate border lines for whic h there may not yet be full agreement.
! WHO 2006. All rights reserved

Drug Resistance: Multidrug-resistant TB (MDR-TB) Drug-resistant TB is widespread and found in all 81
countries recently surveyed by WHO. Multidrug-resistant TB (MDR-TB) does not respond to the
standard six month treatment using first line-drugs (i.e.resistant to isoniazid and rifampicin).
MDR-TB can take up to two years to treat with drugs thatare more toxic, and 100 times more expensive.
WHO estimates 500,000 new cases and 110,000 deathseach year
Highest rates in countries of the former Soviet Union andChina

Extensively Drug-Resistant TB (XDR-TB)
Extensively drug-resistant TB (XDR-TB) is defined as MDR-TB plusresistance to any fluoroquinolone and any of the second-line anti-TBinjectable drugs: amikacin, kanamycin or capreomycin).
40,000 new cases of XDR-TB each year 45 countries with at least one confirmed case of XDR The true scale of the problem remains unknown in some pockets of
the world. Only six countries in Africa—the region with the highest incidence
of TB in the world--were able to provide drug resistance data forthe latest WHO surveillance report.
Other countries in the region could not conduct surveys becausethey lack the equipment and trained personnel needed to identifydrug-resistant TB.
MDR-TB and XDR-TB are highly lethal in people living with HIV --studies show case fatality rates of over 90%.


Calmette & Guérin(1906-1921) Attenuated M. bovis First used in 1921 1928 recommended
for wide spread useby League of nations
Widespread use after1945
Most widely usedvaccine
BCG Vaccine

AERAS GLOBAL TB VACCINE FOUNDATION
British School ChildrenBritish School ChildrenBritish School Children
S. India (Madanapalle)USA (Georgia & Alabama)S. India (Chingleput)USA (Georgia Children)
USA (Chicago Infants)Puerto Rico (Gen. Pop.)
N. American Indians
Brazil (Sao Paolo)Argentina (Buenos Aires)Brazil (Belo Horizonte)Cameroon (Yaounde) Canada (Manitoba Indians)
Surinam (Rangoon)Sri Lanka (Colombo)Colombia (Cali)Argentina (Santa Fe)
Togo (Lome)Thailand
Indonesia (Jakarta)
Vaccine Efficacy (%)-900 -500 -300 -100 0 20 40 60 70 80 90 Population
Variable Efficacy of BCG vs. Pulmonary TB
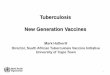
Genealogy of BCG vaccines
Brosch et alPNAS, 2007,104: 5596

Variable efficacy of BCG
Genetic variation in BCG strains Genetic variation in populations Differences in virulence between TB strains (eg.
Beijing) Protection against endogenous infection but not
exogenous re-infection Interference by non-tuberculous mycobacteria (eg.
M.avium) Interference by concurrent parasitic infection (Th2
–induction)

Current vaccines against TB
One vaccine, BCG,reduces risk of severepediatric TB disease
Variable protectionagainst adult pulmonaryTB, which accounts formost TB worldwide
Risk of disseminatedBCG in HIV positiveinfants

Exposure to infectious particles
No Infection (70%) Infection (30%)
Early Progression
1-2 years (5%)
Resistance
(
95%)
Late Progression
Lifetime (5%)
Resistance (95%)
Preventionof Latency
Differential Vaccines
Prevention ofReactivation
(Improved)prevention ofinfection and
disease
Therapeutic Vaccines

New TB Vaccines
Identify “protective” immune response duringinfection and disease
Identify antigens involved Design a vaccine capable of inducing a
protective response
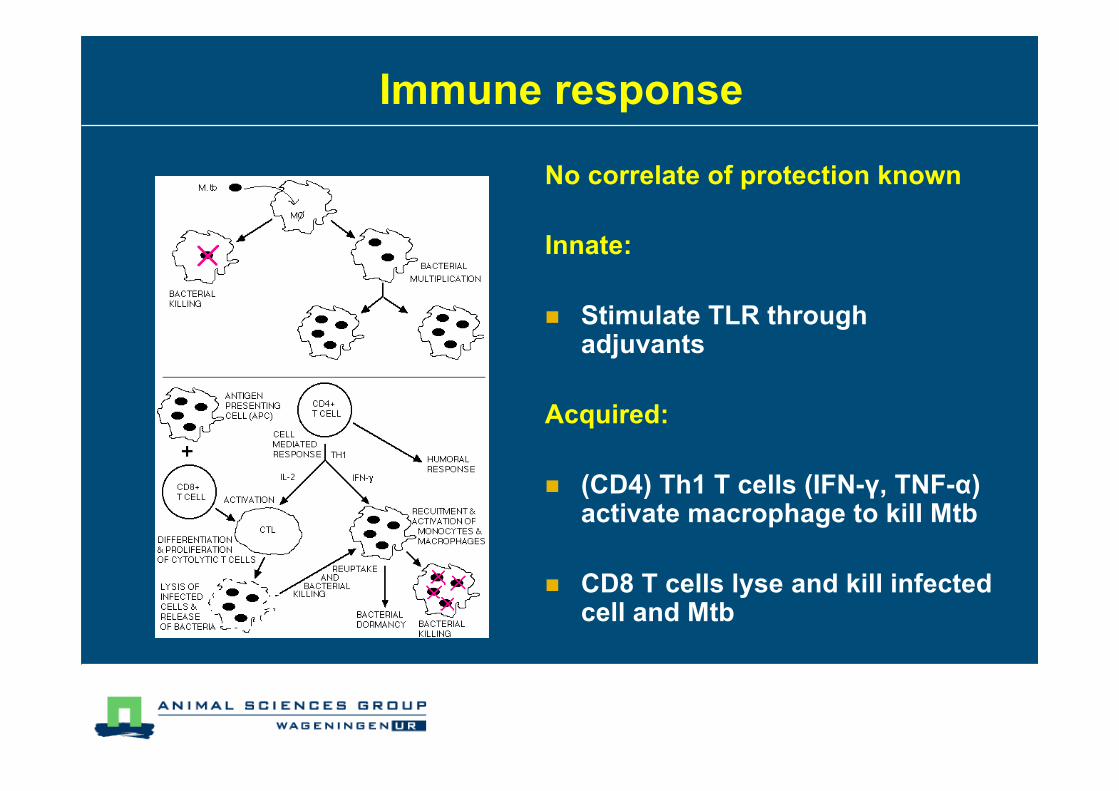
Immune response
No correlate of protection known
Innate:
Stimulate TLR throughadjuvants
Acquired:
(CD4) Th1 T cells (IFN-γ, TNF-α)activate macrophage to kill Mtb
CD8 T cells lyse and kill infectedcell and Mtb

Classes of Antigens
Secreted:Antigen85
ESAT6
CPF10
Latency:DosR:
Rv2029
HSP16Resuscitation:Rv3407
Stress :HSP65
HSP70
HSP16
RD antigens notpresent in BCG:
ESAT6
TB10.4
Glycolipids:
SGL

Recent adjuvants in TB
MPLA from S. Minnesotaplus QS21 from soap barktree in oil or liposomes
TLR4 signalling,
Depot
GSKBioAS01B/AS02
Antimicrobial peptide,KLK, withimmunostimulatory
oligonucleotide, ODN1a,
TLR9 signalling,
APC,
Depot
IntercellIC31
SSI
Origin
dimethyldioctadecylammonium bromide (DDA),and trehalose 6,6’-dibehenate (TDB)
TLR ?
Depot
What
DDA/TDB
VaccineNonclin Phase IIIPhase I Phase II

Design of new vaccines Improve BCG
Adding antigens from RD regions (eg. ESAT6) Overexpression of antigens (Ag85) Engineering phagosome escape (Hly, Pfo)
Attenuate M.tuberculosis Deleting essential genes (eg. Phop, auxotrophic mutants)
(Viral) vector based MVA, Adenovirus, rBCG
Subunit antigens combined with adjuvants Secreted antigens (Ag85, ESAT6, TB10.4) Strong immunogens (Rv1196, Rv0125) Latency antigens (hsp16, DosR etc) Adjuvants (IC31, AS02/1B, DDA/TDB)

NLUKFRITESGEBEDKCH
SenegalGambiaEthiopiaSouth Africa
TB-VACDesign and testing of vaccine candidates against
tuberculosis: identification, development, andclinical studies
Consortium of 29 European + 4 African Partners 1-1-2004 - 31-12-2008 17 mE EC FP6, and 1.8 mSF OFES

Project overview

Discovery and Preclinical Development
5 new vaccine candidates (live and subunit) 15 candidate surrogate markers 3 candidate adjuvant molecules Preclinical animal models
Vaccine efficacy immunogenicity Safety Post-exposure
> 50 publications; >10 IP

BCG::RD1
BCG::RD1 gives betterprotection
Overcomes inhibition ofprotection to BCG afterpre-exposure to M.avium
BCG::RD1 more virulentthan BCG in SCID


Protective Capacity rBCG ΔureC-HlyChallenge “Beijing“ (200 CFU 120 d post vaccination)
0 50 100 150 200 2502
3
4
5
6
naiveBCG PasteurBCG P ΔureC-Hly
time post challenge [day]
log
CFU
Bei
jing
/ lun
g
* Δ log = 2.3
* Δ log = 2.1
Δ log =2.3Δ log = 2.1
Grode et al., J Clin Invest. 2005 Sep;115(9):2472-9.

M. tuberculosis::PhoP
Signal Transduction Systems enable bacteria to detectenvironmental stimuli and respond to them
P
ATP
ADP
11 TCSs in M. tuberculosis
limited number of TCS when comparedwith other bacteria
Sensor Protein
Transcription Factor
Attenuation by deletion of PhoP gene

Nonparametric Survival PlotKaplan-Meier Method
Time post-challenge (days)
0 20 40 60 80 100 120 140 160 180 200
% s
urv
iva
l
0
20
40
60
80
100
M. Tb/PhoP
M. microti/RD1
BCG-MVA/85-FP/85
DNA-BCG
rHly/ureC BCG
TT-LAM/L3
BCG
Saline
SurvivalSurvival
- BCG
- Mtb PhoP
- BCG MVA/85A - FP/85A
- Saline
Survival of guinea pigs up to 26 weeks post high-dose (500CFU) aerosolchallenge

Geneva meeting: WHO, Aeras, EMEA, FDA

CryoTEM picture of LipoVac liposomesCryoTEM picture of LipoVac liposomes
Cationic liposomes+
Immunomodulator
Stable formulation based on
DDA/TDB – a novel adjuvant for theefficient induction of both cell-mediated
and humoral immune responses

Long-term immune responses and protection
with Ag85B-ESAT6 in DDA/TDB
Frequency of IFN- ! producing cells*
Months post immunisation
0 2 4 6 8 10 12 14
Sp
ots
/10
6 c
ells
0
250
500
750
1000
Spleen
Naive
BCG LipoV
ac
Lo
g1
0 C
FU 3.0
3.5
4.0
4.5
5.0
Log10 CFU in lungs
Naive BCG LipoVac
Log10 C
FU
4.0
4.5
5.0
5.5
6.0
*measured by ELISPOT after restimulation with vaccine (Ag85B -ESAT-6) antigen
Naive BCG DDA/TDB

Product development teams for 6 vaccines GMP production of 2 vaccines 3 vaccines in phase I/IIa trials 3 new vaccines entering down stream
development One adjuvant entering clinical trials
(DDA/TDB) Capacity in 2 new African clinical trial sites
(AHRI, Ethiopia; Ledantec, Senegal)
Downstream development

Diablerets Feb 08
Discovery
Pre-clinicalefficacy
GMP-Production
Non-clinicalsafety
IND
file
Effective protection(mice , g-pigs, N-hu Prim)
Lot consistency-
- FormulationIncl. neonatal.
TOXstudies
As RQ
by RA
Ph1 Trials Safety / immunogenicityadults (in area of production)
PPDneg
BCGprimed
LTBI ortreated
TB
HIVinfected
Ph2a- Safety / immunogenicity ados. + infants
Adults/Ados Infants[Formulation.
Bridg.]Interference
studies
HIV posados/infants
2009-10
Ph1-Safety / immunogenicityadults (high endemicity area)
PPD neg &BCG primed
LTBI
Phase IIb Phase III
Adults/ados infant Adults/ados infants
ProductDevelopmentTeam (PDTs)
Diablerets Feb 08
Pre-clinicalefficacy
GMP-Production
TOXstudies
IND
file
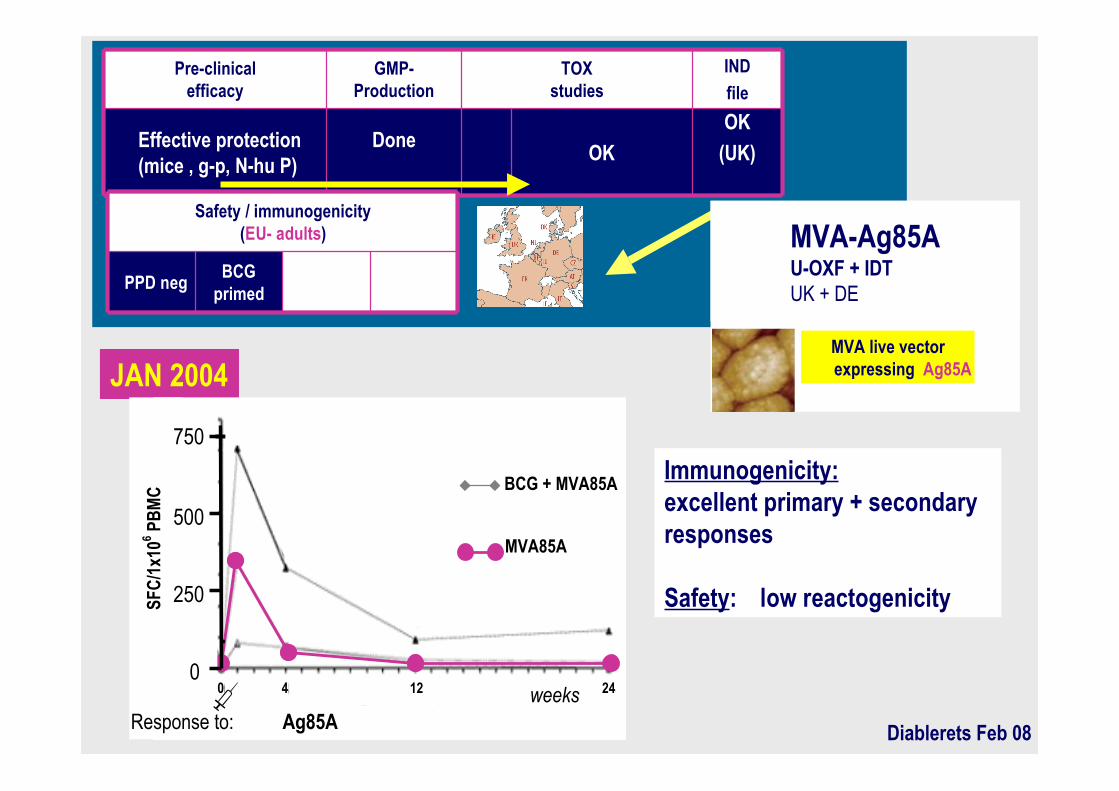
Effective protection(mice , g-p, N-hu P)
DoneOK
OK
(UK)
Safety / immunogenicity(EU- adults)
PPD negBCG
primed
JAN 2004
Immunogenicity:excellent primary + secondaryresponses
Safety: low reactogenicity
0 4 12 24
MVA85A
0
250
500
750
SFC
/1x1
06 PB
MC
Response to: Ag85Aweeks
MVA-Ag85AU-OXF + IDTUK + DE
MVA live vector expressing Ag85A
BCG + MVA85A

Diablerets Feb 08
Ph2a-Safety / immunogenicity ados. + infants (AFR)
Ados/ InfantsAge de-
escalationDose
escalationInterference
studiesHIV infectedados/infants
Ph1- Safety / immunogenicity(AFR- adults)
PPD neg &BCG primed
LTBI HIV infected
Phase 2b AFR Phase 3 AFR
AdosInfants2008-12
Ados 2009- Adults 2009-12
Safety / immunogenicity(EU- adults)
PPD negBCG
primedLTBI or
treated TBHIV
infected
MVA-Ag85AU-OXF + IDTUK + DE
MVA live vector expressing Ag85A
JAN 2008
Pre-clinicalefficacy
GMP-Production
TOXstudies
IND
file
Effective protection(mice , g-p, N-hu P)
DoneOK
OK
(UK)

Diablerets Feb 08
Ph1-Safety / immunogenicity(AFR- adults)
PPD neg &BCG primed
LTBI
Pre-clinicalefficacy
(mice , g-p, N-hu P)
GMP-Production
Pre-clinicalsafety
IND
file
Effective protection
++Done- DK
(several lots)
neonatal mice
OKTOX
studies
OK
OK(NL, UK)
Safety / immunogenicity(EU- adults)
PPD negBCG
primedLTBI
Ag85B-ESAT6+ IC31 (H1)SSI + Intercell
ESAT-6Ag85B
Ethiopia
JAN 2008
Immunogenicity: good primary responseSafety: low reactogenicity
-2 0 6 12 320
250
500
750
Ag85B ESAT6 H1
IFNγ
SFU
/ 106
PB
MC
-2 0 6 12 32-2 0 6 12 32weeks
IFNγ ELISPOT
Resp. to:

Diablerets Feb 08
Trials Status Funding source
Phase 1 –trial(s) in PPD neg Done 04-05 - USA/BE GSK
Phase 1- trial(s) in PPD pos(BCG or latent TB)
Done 05-06 - CH TB-VAC & GSK
Phase 1 – trial(s) in HIV pos Planned 08 - CH GSK & TB-VAC
Completed & on-going trials – USA + Europe
Mtb72F + AS-02M72+AS02 or M72+AS01GSKBE
Ra35TbH9 39 kDaRa12
M72- AS01
Pre-clinicalefficacy
M, GP, NHP
GMP-Production
TOXstudies
IND
++ Doneseveral lots
OK OK
JAN 2008

Diablerets Feb 08
Trials Status Funding source
Phase 1 –trial(s) in PPD neg Done 04-05 - USA/BE GSK
Phase 1- trial(s) in PPD pos(BCG or latent TB)
Done 05-06 - CH TB-VAC & GSK
Phase 1 – trial(s) in HIV pos Planned 08 - CH GSK & TB-VAC
Completed & on-going trials – USA + Europe
Mtb72F + AS-02M72+AS02 or M72+AS01GSKBE
Ra35TbH9 39 kDaRa12
M72- AS01
Pre-clinicalefficacy
M, GP, NHP
GMP-Production
TOXstudies
IND
++ Doneseveral lots
OK OK
• Highly immunogenic in BCG-primedand Mtb-exposed individuals(boosting)
• Vaccine shown to be safe withacceptable local reactogenicity inBCG-primed individuals
JAN 2008

Diablerets Feb 08
Candidate -vaccines
DeveloperInitial cGMPProduction
RegulatoryAssessm.
Phase IPPD-
Phase I/IIIn PPD+
Clinical Trialsin PPD+ andHIV exposed
MVA-Ag85A,
(VV, Pr-b)UOXF Done (lot1) Done (lot1)
On-going2003-4
UOXF
Mtb72fhybrid
recAg +AS02
GSKbio Done (lot1) Done (lot1)InitiatedFeb 2004
USA
Ag85B-ESAT6
recAg + IC31
SSIplanned
TB-VAC CANDIDATE VACCINES WP6 M- 0

Planned 2007Done 2007Done 2007MP-
VPM/BPRrBCG-UreC-
Hly
2007
Ethiopia
2007
Leiden09/ 2005Leiden
Done(lot1)Done 2004SSI
Ag85B-ESAT6
recAg +IC31
2007Lausanne
2005
UOXF
Clinical Trials in
PPD+ & HIV+
09-2005Lausanne
2004-5
UOXF
Clinical Trialsin PPD+
InitiatedFeb 2004
USA
On-going2003-4
UOXF
Phase I
Clinical Trials
Pre-PDTexploratorymeetings
UNIZAR
INSERM/ULB
Mtb- PhoP
HBHA
2007EthiopiaDone (lot1)Done (lot1)GSKbio
Mtb72fhybrid
recAg +AS02
2006
Senegal
The Gambia
South Africa
Done (lot1)Done (lot1)UOXFMVA-
Ag85A,
(VV, Pr-b)
RegulatoryAssessm.
Initial cGMP
ProductionDeveloper
Candidate -vaccines
TBVAC CANDIDATE VACCINESWP6 M-42

website: www.tb-vac.org

TuBerculosis VaccineInitiative (TBVI)
Foundation to facilitate European effortstowards the development of new TB vaccines
5 March 2008

TBVI Activities
Facilitate Discovery, Preclinical and Early clinical TBvaccine development
Responsibility and Ownership of candidate vaccine withindividual project partners
Guide and Advice on development by tailor made productdevelopment teams (PDT)
Stimulate late clinical development through productdevelopment partnerships
TBVI Industry/EDCTP/AERAS/PDP
Discovery Preclinical ClinicalPhase I/IIa Phase IIb/III License/
Phase IV
Product development teams

TBVAC Vaccine Pipeline
+CNRSGL
TBDIPASBCG-RD1
+IPLHBHA
+UNIZARMtb-PhoP
+MPIIB/VPM
BCG-ΔureA-Hly
+SSI85B-ESAT6-
IC31
+GSKBIOM72-
AS01B
+UOXFMVA85A
PDTWhoVaccine Discovery Nonclin Phase IIIPhase I Phase II

Global pre and non clinical developmentpipeline
As of March 2008:• 10 Priming, Pre-exposure candidates• 17 Boosting, Pre-exposure candidates• 12 Post-exposure – immunotherapy candidates
Nine additional candidates scheduled forclinical trials in 2008 according to sponsors

TB vaccines in clinical trials
Subunit fusion protein of Ag85Band TB10.4 in IC31 adjuvant, toboost BCG
SSI85B-TB10.4in IC31(HyVAC4)
Recombinant BCG overexpressingAg85B, to replace BCG
UCLArBCG-Ag30
Detoxified Fragmented MTB, totreat latently infected individuals
ArchivelPharma
RUTI
Crucell
SSI
GSKBio
UOXF
Origin
Recombinant adenovirus35expressing Ag 85A, 85B, 10.4 toboost (recombinant)BCG
Subunit fusion protein of Ag85Band ESAT6 in IC31 adjuvant, toboost BCG
Subunit fusion protein of Rv1196and Rv0125 in ASO1B adjuvant , toboost BCG
Recombinant vaccinia expressingAg85A, to boost BCG
What
rAd35-Ag85A,85B,TB10.4
85B-ESAT6
in IC31(Hyb1)
M72 in
AS01B
MVA85A
Vaccine Nonclin Phase IIIPhase I Phase II

ImprovedBCG
rBCG-HlyrBCG-PFOMtb-PhoP
Future TB vaccinesLe
vel o
f Pro
tect
ion
BoostMVA85A
72MH1
HyVac4Ad35/Ag85A
B,TB10.4
1950 2000 2020 2025 2030 2050
LatencyDosR
Rv3409
STOP-TB/MDG:less than1 case/million in2050

Summary and Future challenges
More TB vaccine candidates than ever before,and prospect of new vaccine between 2015-2020
Keep pipeline filled with second and thirdgeneration vaccines Vaccines (latent bacteria, improved protection) Delivery (systems/adjuvants, applications (needless)
and routes eg. ID, mucosal) Preclinical models to select for clinical development
Biomarkers and correlates of protection (Global) clinical site development