Embed Size (px)
Citation preview

Researcher ClaimsMeningoccocal Vaccine is a
"Potential Time Bomb"
By Katherine Joyce Smith
Investigative journalist Jonathan Eisenslammed the meningococcal vaccina-tion campaign today as a "potentialtime bomb" for the health of vaccinerecipients.
Quoting from the package insert sup-plied by Chiron Corporation, manufac-turer of the MeNZB vaccine, theAuckland based researcher stated thatthe company acknowledged thatbecause it had not conducted"prospective trials" of the vaccine,there was no evidence that the vaccinewould prevent vaccine recipients fromcontracting meningoccocal disease.
That means that instead of vaccinating a sizeablegroup of volunteers and following their progress
to see whether or not they developed meningo-coccal disease, the company merely assumedthat the vaccine would be effective because itincreased the level of antibodies against themeningococcal bacteria in approximately 75% ofthose vaccinated in the trials on the vaccine.
According to Mr Eisen, this lack of evidence that
What Your Doctor Will Never Tell You
October-November 2004Volume 4 Number 1Price $NZ 4.95
Vaccine Maker Admits NZMeningococcal Vaccine
May Not Work Ð and CouldBe Dangerous
I n t h i s i s s u e• Dr Mike Godfrey: The Meningitis andlack of Vitamin C hypothesis • 16,000 “adverse events” in UK, 12deaths, from meningococcal vaccine • DPT and autism epidemic: the undeni-able relationship• Polio Vaccine/cancer connection• MMR and autism: More proof• Link between vaccines and diabetesestablished• The great Thimerosal coverup • Concerns over “fraudulent medicalresearch”: Unravelling the public trust• Doctors 3rd leading cause of death inUS – Journal of the AMA• Dissent in medicine: Doctors at lastspeak the truth about vacccines
SPECIAL VACCINEISSUE

the vaccine would protect against meningoccocaldisease essentially means that the vaccine is still"experimental".
In addition to concerns that the vaccine may notprotect against meningococcal disease, Eisenalso pointed to short-comings in the clinical trialsperformed prior to the provisional licensing of thevaccine. One of the most seri-ous shortcomings was that thehealth of vaccine recipientswas monitored only for "up to"seven days after each injec-tion.
Eisen pointed out that such asshort follow-up period for vac-cine recipients meant that thetrial could only identify theshort term side effects of thevaccine; longer term riskswould not be identified prior tothe vaccine being adminis-tered into over a million youngNew Zealanders in the mass vaccination cam-paign.
Chiron's datasheet for the MeNZB vaccineacknowledges that MeNZB's "parent vaccine"(Menbvac – used in Norway) had been linked toserious adverse reactions including anaphylaticreactions (life threatening allergic reactions),haematuria (blood in urine), Guillaine-Barre syn-drome (a neurological disorder that may includeparalysis), and myalgic encephalitis (otherwiseknown as ME or chronic fatigue syndrome).
According to Chiron, these side effects were"very rare", but no data on their frequency wasgiven.
Eisen pointed out that in some cases it can takeyears for serious long term side effects of vac-cines to become apparent, citing the case of thevaccine designed to prevent meningitis (andother infections) caused by the bacteriahaemophilus influenzae. This vaccine was intro-duced to New Zealand in 1991 and was creditedwith a reduction in bacterial meningitis caused bythis organism (which commonly lives in the backof the nose and throat without causing disease.)However, a study of published in 2002 in themedical journal Autoimmunity showed that thevaccine was responsible for a 26% increase in
diabetes in the 100,000 children who receivedthe vaccine as part of a clinical trial.
Significantly, it was not until 3-4 years after thevaccine that the most of the vaccine-relatedcases of diabetes were diagnosed.
"The fact that this vaccine remains on the NewZealand market, despite thefact that it is known to causediabetes in some childrenspeaks volumes about thecompetence of the peopledetermining public health poli-cy in New Zealand." Eisensaid, adding out that the infor-mation handouts for parentson immunisation produced bythe Ministry of Health did notdisclose the fact that theHaemophilus influenzae vac-cine increased the risk of achild developing diabetes.
"My concern is that every baby, child and teenag-er who receives the MeNZB vaccine is an unwit-ting guinea pig in one of the largest medicalexperiments in our nation's history", Eisen stated.
"The Ministry of Health has largely succeeded inmanipulating the media coverage of meningococ-cal disease to create a public panic in whichrational discussion of the risks and benefits ofthis vaccine has been stymied. People areunderstandably frightened of meningococcal dis-ease, given its ability to maim or kill people withastonishing rapidity, and the graphic pictures thatthey have seen of people suffering from this dis-ease increase that fear."
"However, this is just one side of the picture. TheMinistry of Health itself acknowledges thataround one in five people naturally carries thebacteria that can cause meningococcal diseasein the back of their nose and throat – without
There is a lack of Safety and Efficacy stud-ies on vaccine damage. There are no controlgroup studies. Authorities consider that "tonot vaccinate" is unethical and so haverefused to study unvaccinated volunteers. Ifcontrol studies were done according to hon-est science, vaccination would be outlawed.
"My concern is thatevery baby, child andteenager who receivesthe MeNZB vaccine isan unwitting guinea pigin one of the largestmedical experimentsin our nation's history.”

becoming ill. It is only a tiny minority of peoplewho actually develop meningococcal disease. Atno point is the MoH investigating why that is thecase."
"Meningococcal disease is associated with over-crowded housing, exposure to cigarette smoke,and poor nutrition which impairs immunity tomany diseases in addition to increasing suscepti-bility to meningococcal disease. Why aren't par-ents being informed about the link between nutri-tional deficiencies such as iron and vitamin Cdeficiency and passive smoking – and meningo-coccal disease, so that they can take the appro-priate actions to protect their children's health?Instead, the Ministry of Health is largely ignoringthe factors known to increasethe risk of meninigococcal dis-ease (and other infections) andseems intent on stampedingparents with emotional black-mail into allowing their childrento be vaccinated with an inade-quately tested vaccine thatmay not even work."
"What's more, if the MeNZBvaccine does have seriouslong term side effects, thehealth of a whole generation ofNew Zealanders will have beenput at risk. We simply cannotafford as a nation to gamblewith the health of our nation'sfuture by allowing this massvaccination programme to pro-cede."
"It is vital to remember that even amongPolynesian children (who are at the highest riskof developing meningococcal disease of any eth-nic group) the vast majority of children will neverget meningococcal disease. However, every sin-gle person who is vaccinated with the MeNZBvaccine is vulnerable to the as yet unknown risksof this vaccine. It is of great concern to me thatthe MeNZB vaccine contains aluminium hydrox-ide, which was identified as being carcinogenic inanimal tests as far back as 1975. Cancer alreadykills more New Zealand children than any otherdisease. I don't believe that it makes good senseto inject babies, children or teenagers with aknown carcinogen when cancer is already such aserious public health problem in this country, for
adults and children alike."
"I believe the Ministry of Health is seriously mis-guided in promoting this vaccine as the best wayto reduce the incidence of meningococcal dis-ease. I encourage parents and young people tothink carefully about the risks of this vaccine,read the package insert supplied by the manu-facturer and ensure that they make an informedchoice about this vaccine."
THE FULL TEXT OFJONATHAN EISEN’S REPORT:
The manufacturer of the newmeningococcal vaccine cur-rently being introduced intoNew Zealand has admittedthat ”complete protectionagainst infection caused by theNew Zealand strain (of thebacteria) cannot be guaran-teed.”
In the “package insert”designed to provide guidelinesfor doctors and nurses admin-istering the vaccine, the CHI-RON company also admits thatthe vaccine has a high rate ofpossible side effects.
Moreover, it says that muchcrucial data about the performance of the vac-cine, as well as data on “contraindications”(where it should not be used) are incomplete.
Specifically:
• While the insert says that “the population at riskshould be vaccinated with MeNZB to preventserious systemic disease” it concedes that “dataon concomitant use of other vaccines are not yetavailable.” This means that if a person gets oneor more other vaccines at or around the sametime as the MeNZB vaccine, there are no data onpossible adverse outcomes.
• The vaccine also “has not been evaluated inpersons with thrombocytopenia (low bloodplatelet count) or bleeding disorders.”
“The Ministry ofHealth itself acknowl-edges that aroundone in five peoplenaturally carries thebacteria that cancause meningococ-cal disease in theback of their noseand throat – withoutbecoming ill.”

• ”As with all injectable vaccines, appropriatemedical treatment and supervision should alwaysbe readily available in the rare case of an ana-phylactic event (life threatening allergic reaction)following administration of a vaccine.” The com-pany neglects to provide any data on these kindsof events.
• “MeNZB has not been specifically evaluated inthe immunocompromised. Individuals with com-plement deficiencies and individuals with func-tional or anatomical asplenia (problems with orabsence of a spleen) may mount an immuneresponse to MeNZB; however, the degree of pro-tection that would be afforded is unknown.”
• “Any acute infection andfebrile illness (an illnesswith an associated fever)is reason for delaying theuse of MeNZB exceptwhen, in the opinion ofthe physician,withholdingthe vaccine entails agreater risk.” In otherwords, inasmuch as themanufacturer does notactually have any mean-ingful data on risks andbenefits, it’s up to thedoctor’s “educatedguess” as to whether ornot to vaccinate a sick child or infant. More: “Aminor illness such a temperature of less than38.5 detgrees such as a minor upper respiratoryinfection, is not usually reason to postponeimmunisation.” However, in that such an infectionmay or may not be an indication of someone whois “immunocompromised” (a contraindication forthe vaccine; remember that there is “no data” onthis) the reader is left wondering about thisapparent contradiction in the directions.
• “There are no adequate data from the use ofMeNZB in pregnant women.”
• “Information on the safety of the vaccine duringlactation is not available.”• “The degree and quality of the cellular immuneresponse is not yet established.”
• “Clinical efficacy (whether it works or not): Noprospective efficacy trials have been performedwith MeNZB.” In other words, the company hasno idea as to whether or not the vaccine actually
does what they say it should do.
• “Adverse Reactions from Clinical Studieswith the Norwegian parent vaccine, Menbvac,an OMV vaccine manufactured with a strainfrom a different sero-(sub)type (B:15:P1.7,16 )
For MenBvac further adverse events were report-ed including anaphylactic reactions, flu-likesymptoms, haematuria (blood in the urine),Guillain-Barre Syndrome (neurological disorderthat may include paralysis), myalgicencephalomyelitis/chronic fatigue syndrome(akaME). All these reactions were very rare (no datasupplied) and occured in adolescents and/or
adults. Additional infor-m a t i o n : A l t h o u g hMenBvac is the parentvaccine of MeNZB theabove mentionedadverse events ofMenBvac may not nec-essarily be expected tohappen with MeNZB (noreason or data speci-fied).TRANSLATION: Theseare some of the adversereactions to the parentstrain (Norwegian vac-cine) from which the
New Zealand vaccine was developed. We don’tknow what the reactions to the NZ strain will be,and this is the reason:
“Adverse reactions (to the vaccine in the trialperiod) were collected on the day of vaccina-tion and each day following for up to 7 days.”
TRANSLATION:This means is that the NZ vac-cine, which is related to the Norwegian vac-cine, may or may not have a similar adversereaction profile – nobody knows yet and theMinistry of Health is not waiting to find outbefore it releases the vaccine for use in NewZealand.
Moreover, the company followed up the trialsubjects ) only about 1000 people) for onlyabout a week, even though some “adversereactions” don’t begin to show up until manyweeks or months later (or even years withsome vaccines, like the cancer connection tothe polio vaccine).
"The Ministry of Health haslargely succeeded in manip-ulating the media coverageof meningococcal disease tocreate a public panic inwhich rational discussion ofthe risks and benefits of thisvaccine has been stymied.

Finally, we come to aluminium hydroxide, an“adjuvant” in the vaccine. This was shown asfar back as 1975 to be a possible carcinogen(cancer-causing agent) by US Bureau ofBiologics and the US Food and DrugAdministration).
The fact is that the MeNZB vaccine is still highlyexperimental, despite what the Ministry of Healthis telling the people of New Zealand, which is thatthe vaccine will prevent meningoccocal meningi-tis, is safe and well trialled.
“This vaccine has been safely used in clinical tri-als in Auckland with a range ofage groups, including babies andadults.”
The MoH is not telling the peopleof New Zealand that we are pay-ing a vaccine company $200 mil-lion to experiment on our childrenwith the possibility of long lasting“adverse consequences” like can-cer, diabetes and other serious ill-nesses down the track.
A Precedent
With the bandwagon rolling alongon the new meningitis vaccine, itmay be instructive to consider thefollowing, which links an earliervaccine for meningitis to a marked increase indiabetes.
The prestigious peer reviewed journalAutoimmunity (August 2002 Vol. 35 (4), pp. 247-253} recently published an article by Dr. J. BartClassen, an immunologist at ClassenImmunotherapies, and David Carey Classen, aninfectious disease specialist at the University ofUtah, proving a causal relationship between thehemophilus vaccine and the development ofinsulin dependent diabetes. The data is particu-larly disturbing because it indicates the risksof the vaccine exceeds the benefit. The find-ings are expected to allow many diabetics toreceive compensation for their injuries.
The study followed over 100,000 children whohad been randomized in a large clinical trial toreceive 1 or 4 doses of the hemophilus vaccineand over 100,000 unvaccinated children. After 7
years the group receiving 4 doses of the vaccinehad a statistically significant, 26% elevated rateof diabetes, or an extra 54 cases/100,000 chil-dren, compared to children who did not receivethe vaccine.
By contrast immunization against hemophilus isexpected to prevent only 7 deaths and 7 to 26cases of permanent disability per 100,000 chil-dren immunized. The study showed that almostall of the extra cases of diabetes caused by thevaccine occurred between 3-4 years after vacci-nation. Furthermore the paper provides new dataproving the vaccine causes diabetes in mice and
reviews data from 3 smallerhuman studies, which all had sim-ilar results to the current study, butwere too small to reach statisticalsignificance.
"Our results conclusively provethere is a causal relationshipbetween immunization schedulesand diabetes. We believe immu-nization schedules can be madesafer," stated Dr. Bart Classen.
The Classens' research is alreadybecoming widely accepted. Anindependent group ofresearchers working at a presti-gious Swedish medical centerrecently published a paper
(Annals . N.Y. Acad Sci. 958: 293-296, 2002) sup-porting their findings. Last year doctors attendinga conference of the American College forAdvancement in Medicine overwhelminglyagreed that vaccines can cause chronic diseasessuch as diabetes.
Conclusion
“The medical authorities keep lying. Vaccinationhas been a disaster on the immune system. Itactually causes a lot of illnesses. We are actual-ly changing our genetic code through vaccina-tion...100 years from now we will know that thebiggest crime against humanity was vaccines."
– Guylaine Lanctot, MD, author of Medical Mafia
After critically analyzing literally ten's of thou-sands of pages of the vaccine medical literature,
FACT: A 1992study published inThe AmericanJournal ofE p i d e m i o l o g yshows that childrendie at a rate 8times greater thannormal within threedays after getting aDPT vaccination.

Dr. Viera Scheibner concluded that "there is noevidence whatsoever of the ability of vaccines toprevent any diseases. To the contrary, there is agreat wealth of evidence that they cause seriousside effects." Dr. Classen, a notable medicalresearcher has stated, "My data proves that thestudies used to support immunization are soflawed that it is impossible to say if immunizationprovides a net benefit to anyone or to society ingeneral.
"This question can only be determined by properstudies which have never been performed. Theflaw of previous studies is that there was no long-term follow up and chronic toxicity was not lookedat.”
The continued denial and suppression of the evi-dence against vaccines only perpetuates the"myths" of their "success" and, more importantly,their negative consequences on our children andsociety. Aggressive and comprehensive scientificinvestigation into adverse vaccine events is clear-ly warranted, yet immunization programs contin-ue to expand in the absence of such research.
Concerns over vaccine adverse effects and con-flicts of interest led the American Society ofPhysicians and Surgeons to issue a Resolution toCongress calling for a "moratorium on vaccinemandates and for physicians to insist upon trulyinformed consent for the use of vaccines."
Approved by unanimous vote at the AAPSOctober 2000 annual meeting, the resolution
noted the "increasing numbers of mandatorychildhood vaccines, to which children aresubjected without information about potentialadverse side effects" ; the fact that "safety test-ing of many vaccines is limited and the data areunavailable for independent scrutiny, so thatmass vaccination is equivalent to human experi-mentation and subject to the Nuremberg Code,which requires voluntary informed consent"; andthe fact that "the process of approving and'recommending' vaccines is tainted withconflicts of interest."
In an October 1999 statement to Congress, BartClassen, M.D., M.B.A., founder and CEO ofClassen Immunotherapies and himself a devel-oper of vaccine technologies, stated, "It is clearthat the government's immunization policiesare driven by politics and not by science."
FACT: In The New England Journal of Medicine(July 1994) a study found that over 80% of chil-dren under 5 years of age who had contractedwhooping cough had been fully vaccinated(immunised).
FACT: The death rate from common infectiousdiseases such as tuberculosis, whooping cough,measles and diptheria had declined by over 90%BEFORE the introduction of vaccination. (1)
FACT: A 1992 study published in The AmericanJournal of Epidemiology shows that children dieat a rate 8 times greater than normal within threedays after getting a DPT vaccination.
FACT: Many children develop serious conditionsas a result of vaccination. How many?Unfortunately, it is impossible to know for surebecause only a small fraction (less than 10%) ofall "adverse reactions" are ever reported. (2)
Long-term adverse reactions to vaccinesmay include:
Arthritis: This is a known risk of the rubellaportion of the MMR vaccine. The risk is higher inand women and adolescent girls.(3)
New Zealand vaccinations are not compulsory.Children DO NOT have to be vaccinated in order to goto daycare or school. Know your rights. Inform your-self about the pros and cons of any and all vaccinesbefore you decide. ItÕs your decision.
Website addresses of some of the new generation of honest professionals:
Dr D Duffy: www.duffyslaw.com Dr J. Mercola: www.mercola.cola Dr. Leo Rebello www.aidsalternativa.orgPatrick Quanten http://www.activehealthcare.co.ukRath Foundation Drug Barons:http://www.dr-rath-foundation.orgDr Robert Anderson: www.psrg.org.nz or [email protected] information re: Genetic Engineering, radiation and fluorida-tion.Visit the Soy website at soyonlineservice.co.nzWestonprice An organization, promoting good living with goodeating www.westonaprice.org .Chris Reiger of Pacific Health and Fitness Centre for latest listof food aditives codes: http://www.foodadditives.org.nz/ Cause and prevention of cot death:Dr T James Sprott OBE www.cotlife2000.co.nz Fraudulent Medicine www.pnc.com.au/~cafmrTAAP (The Autism Autoimmunity Project) www.TAAP.info and"TAAP into the truth!"Vaccines: redflagsweekly.com

Diabetes: According to the NZ Medical Journal(24/05/96), Insulin Dependent Diabetesincreased by 60% in NZ children after a massvaccination campaign using a genetically engi-neered Hepatitis B vaccine.
Autism: This once rare (but now common) braindisorder has been linked to the MMR vaccine byseveral independent researchers and doctorsand published in peer-reviewed medical journalslike The Lancet and The Journal of Adverse DrugReactions. Dr Mary Megson and others havealso linked the DPT vaccine to this distressingcondition. Autism can ruin a childÕs ability to learnand develop normal relationships.
Asthma: British researcher Dr Michael Odentfound that children who were vaccinated with theDPT vaccine were four times more likely to devel-op asthma than children who were not injectedwith this vaccine.
Cancer: The polio vaccine has been implicatedin some brain cancers where the presence of acancer-causing virus (SV-40) contaminating thevaccine has been confirmed. (Surprisingly therehas never been a study comparing the health ofvaccinated vs unvaccinated people, and themedical establishment refuses to conduct one Ðon ÒethicalÓ grounds.)
FACT: Some vaccines such as the rubella(MMR) (4), the Hepatitis A vaccine(5) amongothers, are cultured on cells from aborted humanfoetuses.
FACT: Many vaccines do not prevent diseasevery effectively, despite what youÕve been told. Inthe USA where 98% of children are vaccinated,children (and adults) still develop measles,whooping cough and other "vaccine preventable"diseases. A massive outbreak of whoopingcough occurred in Holland in 1998, despite thefact that over 90% of the population had beenvaccinated against it.
Researcher Ron Law writes:
"My understanding was that there were approx20 deaths a year due to meningococcal B until Ilooked at the latest data just released by theMOH... and note that this was during the big roll
out of the so-called MeNZB (vaccine) and thedreadful picture of the two kiddies in hospital wesaw on TV and in the newspapers. I don't recall asingle headline to the effect that in 2003 therewere only 13 deaths – down on 2002 which inturn was down on 2001 which was the peakyear...
How will the MOH explain the fact that thefatality rate has dropped BEFORE introduc-tion of the vaccine? Even the incidence hasdropped.
On page 7 of the above report the authors liewhen saying that the epidemic can be expectedto take another 10 years to run its natural coursewithout intervention...(the MOH) should be pro-moting honest Public Health information..."
And Ron’s further research goes on to state:"Note that only about 72% of all (potential) caseswill be targeted by the vaccine... which has a 75%success rate regarding inducing antibodies... thismeans that only 0.72 x 0.75 have a chance ofbeing protected from meningitis per se by thevaccine... that's about 50% ... so that makes thebenefits way less than being touted by official-dom." And if that’s not all get this:
Now, given that data from 1998–2002 shows thatMaori and Pacific children make up 65–69 per-cent of all meningococcal cases in the groupaged 0–4 years, I would say that if you are notMaori nor Pacific Islander or poor (and thereforepoorly nourished) the chances of the vaccinebeing of any benefit what so ever are bugger all...why bother with the downside – i.e. the risks dueto the vaccine?"
F A C T :According to the NZ Ministry ofHealth (Immunisation Handbook,2002), the Norwegian “parent” vac-cine of the current MeNZB vaccinewas never distributed nationally inNorway, partly, they say, because itwas “ineffective”.

Meningitis Vaccine:
The Horror Story gets worse!
These reports below from the international pressconfirm the dangers of the vaccine that we havebeen concerned about for the past few weeks.Decide for yourselves whether we were wrong inwarning you of the dangers your children face insubmitting to this treatment.
The debate as to the safety of the MeNZB vac-cine continues to heat up as the news hits NewZealand that the Chiron corporation, the maker ofthe vaccine, also made a meningococcal vaccinefor the UK that resulted in thousands of "adverseevents" and several deaths.
Here are some follow-up stories to give you anidea of what happened in the UK after Chiron (themanufacturer of the new New Zealand meningo-coccal vaccine) "rolled out" another inadequatelytested and now PROVEN dangerous meningo-coccal vaccine.
Is the NZ vaccine safe? Was it adequately test-ed? Will it even work? The manufacturer is notsaying, nor can they when the follow-up on thetest "subjects" only lasted "up to seven days" fol-lowing the jab.
What sort of a risk are you prepared to take insubmitting to this treatment. Decide for yourself.Meningitis advisers funded by drug firms:http://observer.guardian.co.uk/uk_news/story/0,6903,363705,00.html
Doctors accuse drug firms of 'disease mon-gering':http://www.telegraph.co.uk/news/main.jhtml?xml=/news/2004/08/29/ndocs29.xml&sSheet=/news/2004/08/29/ixnewstop.html
Deaths spark meningitis jab fears:ht tp: / /news.bbc.co.uk/2/h i /uk_news/pol i -tics/897968.stm
Meningitis Vaccine under Scrutiny in UK:http://www.chiroweb.com/archives/18/22/05.html
Safety fears over meningitis vaccine:http://news.bbc.co.uk/2/hi/health/787570.stm
RELATED ARTICLES
UK firm tried HIV drug on orphans:http://observer.guardian.co.uk/international/story/0,6903,1185305,00.html http://www.indymedia.org.uk/en/2004/04/289007.html
Vaccines and the media:http://www.vaccinetruth.org/vaccines_and_the_media.htm
Vaccine underScrutiny in UK
Agency Finds More Than 16,000 AdverseReactions Since Last Year
by Michael Devitt, Associate Editor
http://www.chiroweb.com/archives/18/22/05.html
Last November, the British government instituteda mass national immunization program designedto vaccinate all children under 18 against menin-gitis C, a rare but potentially fatal brain disease.
A series of government documents obtained byThe Observer, a British newspaper, has revealedthat more than 16,000 adverse reactions possiblylinked to two vaccines have been reported inthe past 10 months, including 12 deaths thatoccurred in people after being vaccinated.
The vaccines in question, Meningitec andMeninjugate, are designed to offer protectionfrom meningitis C, which strikes approximately
Bulk copies of this issue of WHATYOUR DOCTOR WILL NEVER TELLYOU (10 or more) are available for$NZ4.95each (prepaid by cheque,please) from:
THE FULL COURT PRESSPO BOX 44-128AUCKLAND, NZ

1,500 people in the United Kingdom every year.The disease causes an inflammation of the mem-branes that surround the brain and spinal cord; itcan also lead to hearing loss, kidney failure,brain damage or limb amputation. The diseaseoccurs most frequently in young children, withsymptoms including high fever, severeheadaches, nausea, rashes and neck stiffness.About 10% of those infected with meningitis C diefrom the disease.
Since the immunization program began inNovember 1999, it has been under review by theMedicines Control Agency (MCA) and theCommittee on Safety of Medicines (CSM), whichuse a system called the Yellow Card Scheme toreport possible adverse reactions to drugs andvaccines. Under the scheme, doctors, pharma-cists, coroners and dentists are advised to submitsuspected adverse reactions to pharmaceuticalsor new vaccines to the MCA or CSM - even if theyare not completely sure whether the vaccinecaused the reaction. The MCA and CSM, in turn,investigate all causes of death and assess YellowCard reports to determine any safety issues thatmay be associated with a new drug or vaccine.
According to the Committee on Safety ofMedicines, more than 15 million doses of thevaccines have been distributed in the U.K.Statistical analyses conducted by the BritishDepartment of Health, claim the vaccine hasreduced the number of meningitis cases by asmuch as 85 percent, particularly among childrenaged 15-17 and infants less than a year old.
Figures compiled by The Observer, however,appear to contradict those published by the gov-ernment. According to their statistics, there hasbeen only an 18 percent drop in the total numberof meningitis cases, from 713 cases during thefirst eight months of 1999 to 587 through thesame time frame this year. Moreover, in parts ofLondon, East Anglia and the West Midlands,there has even been a rise this year in the num-ber of people diagnosed with the disease.
The Observer also reported that as of August 29,MCA and CSM had received 7,742 Yellow Cardreports associated with the meningitis C vaccine,with symptoms ranging from headaches anddizziness to vomiting and convulsions. Althougheach report corresponded to one patient, manyreports listed more than one reaction (for
instance, nausea and headache), bringing thetotal number of adverse reactions that may havebeen caused by the vaccine to 16,527 - approxi-mately one reaction for every 907 doses given.In addition to the adverse reactions, 12 deathsoccurring in people who had been recently vacci-nated have been reported to the CSM. Seven ofthe deaths were a result of sudden infant deathsyndrome (SIDS); one patient died of a convul-sion 10 days after being vaccinated.
While those numbers are high, the actualnumbers may be much higher. TheDepartment of Health estimates that only 10-15 percent of reactions are reported using theYellow Card Scheme. Based on that estima-tion, the actual number of people experienc-ing adverse reactions to the meningitis vac-cine could be in the tens of thousands.
Health officials have downplayed those numbers,insisting that the vaccine has saved lives and pre-vented disabilities. A statement released by CSMand the Joint Committee on Vaccination andImmunisation in August said that "the balance ofrisk and benefit is overwhelmingly favourable"and that "there is no suggestion that this vaccinehas led to any deaths."
As worried parents and lawmakers seek a peace-ful conclusion, the situation has angered parentsacross the U.K. and has caused some people tocall for a halt to the immunization program untilmore tests have been conducted.
"I am not convinced by government reassur-ances," said Isabella Thomas, a member ofJustice Awareness Basic Support, a vaccinationsupport group. "We are receiving daily calls fromparents whose children have had serious reac-tions. We believe the government introduced it fartoo quickly."
Adam Finn, a pediatric expert at SheffieldChildren's Hospital, added that the vaccine wassafe, but that it had induced adverse reactions ina number of children. Finn also said that the gov-ernment has a duty to give the public all relevantinformation about the vaccine. "The public hassufficient intelligence to make the decision forthemselves," he said. "The way to get them toaccept it is to tell the whole story."

Vaccinations:The Overlooked Factors
Autism Research Review International, 1998, Vol. 12, No. 1
Bernard Rimland, Ph.D.Autism Research Institute4182 Adams AvenueSan Diego, CA 92116
Vaccinations, like motherhood and apple pie,have long been regarded as taboo topics, beyondcriticism. No more. The publication in The Lancetof the article by Andrew Wakefield and associ-ates, providing a well-documented mechanismfor the long suspected role of MMR vaccines incausing autism, has raised an international furor.
I began to suspect a link between the DPT vacci-nation and autism as early as in the mid 1960s,based on letters from and interviews with manyparents. Our Form E-3 parent questionnaire, dat-ing from 1967, asked parents about their chil-dren's reaction to the DPT shot. H. L. Coulter andB. L. Fisher state, in their excellent book, DPT:Shot in the Dark (1985), "The phenomenon ofearly infantile autism was first observed and dis-cussed by physicians in the early 1940s, a fewyears after the pertussis vaccine became morewidely used in the United States .... The parallelto certain areas of pertussis vaccine damage isstriking" (p. 123).
Dr. Michael Odent, writing in theJournal of the American MedicalAssociation (1994), claims a fivetimes higher rate of asthma inpertussis-immunised childrencompared to non-immunisedchildren. He is also quoted in theI n t e r n a t i o n a l Va c c i n a t i o nNewsletter (Sept. 1994):
"Immunised children havemore ear infections andspend more days in hospital."
Meningitis – or Scurvy?by Dr Mike Godfrey
One must accept that despite high rates of asymptomaticcarriage in adult populations some persons have died with-in hours of diagnosis whilst others have self-limiting dis-eases. The death rate was 23 in 2001 dropping to 18 andthen 13 by 2003. Thus the so-called epidemic may alreadybe waning even before the vaccination campaign. It isknown that exposures to cigarette smoke, alcohol, low ironlevels, poor living conditions and certain genetic factors areall conducive to increased infection rates. However, thisdoes not explain why some get a severe or fatal haemor-rhagic infection.
The features of meningococcal sepsis include a severecapillary leak syndrome and disseminated intravascularcoagulation or clots. It is possible that this could effectivelybe acute haemorrhagic scurvy and eminently amenable toappropriate therapy. The 1940-70s literature supports thiswith parenteral ascorbic acid (AA) capable of destroyingdiphtheria, tetanus, salmonella, gas gangrene (clostridium)and meningococcal endotoxins.
Prof. Clemetson's 1989 3 volume texbook on Vit.C showedwhy bacterial toxin-induced mortality increases with AAdepletion. Other researchers have confirmed that non-sur-vivors from meningitis having oxidised whatever AAreserves they had to neutralize bacterial toxins, sufferedacute, lethal scurvy.
AA levels in the spinal fluid of meningitis patients has beennegatively correlated with the outcome of patients withbacterial meningitis and thus, its depletion also may be anindicator of a bad prognosis.
Up to 15% of the population may be scorbutic(<0.2mg/100ml serum) and thus at increased risk of bacte-rial endotoxin toxicity as would many of the impoverishedand nutrient-deficient South Auckland populations. Thelatent scorbutic state can then be converted into frankscurvy by infections (and even vaccines), and under suchconditions hemorrhagic phenomena are frequent. All of thepatho-physiological features of haemorrhagic and throm-botic conditions found in bacterial meningitis are seen inAA deficiency states.
It could therefore surely be appropriate to administer thissafe and cheap therapy concurrently with antibiotics toeveryone suspected of this disease. Indeed, it is possiblyonly when the liver is overwhelmed by bacterial toxin that afulminating haemorrhagic disease ensues.
However, for maximum effectiveness continuous AA infu-sions at 0.7G/Kg/ or more/24hrs may be required. Thewhole reason for a vaccine is to prevent severe diseaseand/or deaths but surely if we have a cheap, safe effectiveway of making the disease comparatively trivial, therewould hardly be a need for a vaccine.
Finally, if parents are persuaded to allow their children tobe vaccinated, they ought to preload them with AA for atleast a week before and a week after to help them copewith the vaccine toxins.

Readers of the Autism Research ReviewInternational (ARRI) are well aware of theautism-vaccine controversy (see ARRI 10/4,10/1, 9/3, 9/2, 9/1, 6/3), but until now the massmedia have been kept largely in the dark. InBritain, where there has been an epidemic ofautism, with hundreds of families registering forprojected class-action law suits, some newspa-pers have been devoting half-page or larger arti-cles to the controversy.
Dr. Wakefield and his courageous collaboratorshave endured a torrent of criticism and abusefrom those dedicated to silencing anyone chal-lenging the sacred-cow status of vaccines. Thefact is, vaccines are not nearly as safe, nor any-where near as effective, as vaccination propo-nents claim.
Dr. Wakefield's opponents argue, quite specious-ly, that he is confusing asso-ciation with causation, andthat the autism link may bemerely "coincidental."
I find it doubly ironic that thevaccine advocates accuseWakefield of this elementaryerror in logic. That very argu-ment was used just aswrongly – against vaccina-tions – by the opponents ofEdward Jenner when heintroduced vaccination toEurope. (It was used earlierin Asia.) Jenner's observa-tion that milkmaids exposedto pox-infected cows devel-oped a resistance to small-pox was attributed to coinci-dence. Fortunately for today's vaccine propo-nents, Jenner's critics did not succeed in dis-missing his observations as merely "coinci-dence."
The second irony is that the critics who accuseDr. Wakefield of confusing association with cau-sation are guilty of doing that very thing – delib-erately, not mistakenly – while trying to influencepublic policy, by claiming that vaccines causesteep declines in the incidence of disease whenthere is good evidence that the decline was oftendue to other factors – that is, to coincidence.
In their reply to Wakefield's article, "Vaccineadverse effects: causal or coincidental?," R.T.Chen and F. DeStephano (Lancet 2/28/98) pres-ent a table implying that the incidence of a num-ber of diseases was enormously reduced by vac-cinations. In fact, judging from data presented byNeil Z. Miller in his book Vaccines, are They Safeand Effective?, the reductions Chen andDeStephano cite are often coincidental ratherthan causal. In the case of measles, the deathrate did drop precipitously over a period of fourdecades, but the death rate fell 95% before themeasles vaccine was introduced! In the case ofpolio, the death rate had dropped 60% from itspeak in the 1920s and '30s before the vaccinesarrived in the 1950s. There is considerable evi-dence that the claims of benefit for other vaccines(e.g., pertussis, tetanus) are also greatly inflated.
There is an enormous amount of credible evi-dence that vaccines can anddo cause harm. In responseto what was seen as acause-and-effect relation-ship with sudden infantdeath syndrome (SIDS), theJapanese government, in1979, ordered the postpone-ment of routine DPT shotsuntil after the age of two."SIDS has virtually disap-peared from Japan (Neil Z.Miller, Immunization:Theoryvs. Reality (1996).)
In an article titled, "The DarkSide of Immunizations?,"Science News (November22, 1997) reported findingsby scientists implicating the
rise in diabetes and asthma to vaccines, andthese allegations are just the tip of a very largeiceberg. (The medical establishment's ferociousdefense of vaccines as irrefutably safe and bene-ficial somehow reminds me of the Titanic.)
I am not saying that vaccinations are withoutvalue. I am saying that their benefits have beenoverstated, and their dangers dismissed muchtoo carelessly.
QUESTIONS. The Black Death is estimated tohave killed one third of the population of Europebefore it subsided. Why did it subside? Largely
The Black Death is esti-mated to have killed onethird of the population ofEurope before it sub-sided. Why did it subside?Largely because theimmune system is a mar-velously adaptable instru-ment which learned, natu-rally, how to cope with theplague.

because the immune system is a marvelouslyadaptable instrument which learned, naturally,how to cope with the plague.
Interesting though it is that one out of three diedof the plague, it is even more interesting that twoout of three lived. Why?
Although the headlines alarmed us all whensome people died as a result of the swine flu vac-cine and some people died when exposed toLegionnaire's disease, it is even more interestingthat most people survived. Why?Why are some children injuredby MMR shots and others not?
The answer is that people arevery different, in many ways. Partof the difference is genetic.Another part is environmental.
We can't do much about thegenetic part right now, but wecan do a lot about each person'ssusceptibility to disease, includ-ing vaccine-induced disease, bydealing intelligently with the envi-ronment.
TOXIC EXPOSURE. It is nosecret that our environment is loaded with toxins,many of which greatly impair not only the brainbut also the immune system. Lead, mercury, pes-ticides, and solvents all can create havoc with theimmune system. There is of course a huge litera-ture on this topic. Two excellent recent books are:Our Toxic World: Who is Looking After ourKids by H. E. Buttram, M.D., and Richard Piccolo(1996), and Is This Your Child's World? by DorisRapp, M.D. (1997).
NUTRITION. In my view, the most important, andby far the most feasible, approach to preventingdamage by toxins of all kinds, including the toxinsin vaccines (vaccines contain mercury, aluminumand formaldehyde, in addition to germs) is to helpthe child's developing, immature immune systemby providing generous amounts of the nutrientsthe body needs if it is going to be able to protectitself from a dangerous, toxin-laden world.
In his book Every Second Child (1981), ArchieKalokerinos, an Australian physician, tells us thatthe death rate among the aborigine children he
was assigned to help was an astounding 50%!His investigation showed these deaths to beassociated with vaccinations, and he found thechildren's diets to be severely deficient in vitaminC. By merely administering vitamin C (100 mg permonth of age), he dropped the death rate to near-ly zero.
In my view, and in the view of many others whohave studied these problems, every mother-to-be, starting well before conception, should be
taking significant (several gramsa day, at least) amounts of vita-min C, and every child shouldalso be given supplements--especially in view of the stresson the immune system imposedby vaccines.
But vitamin C is by no means theonly nutrient that should be sup-plemented if the immune systemis to develop and function effec-tively. Nutrients known to beeffective in autism, vitamin B6and DMG, have been shown inlaboratory studies to enhanceimmune function. The mineralszinc and selenium, both implicat-
ed in many cases of autism, are critical inimmune function.
Nutrition is the single most important determinantof immune function, according to world authorityR. K. Chandra, who specifically mentions zinc,selenium, iron, copper, vitamins A, C, E, B6, andfolic acid.
The message is very clear: mothers should takea high quality, broad-spectrum vitamin and min-eral supplement before conception, and duringpregnancy and lactation. And every child shouldalso be getting extra nutrients through mother'smilk or along with food, if the immune system isto develop properly. The cost of not doing so maybe very high.
Science News(November 22,1997) reported find-ings by scientistsimplicating the risein diabetes and asth-ma to vaccines, andthese allegations arejust the tip of a verylarge iceberg.

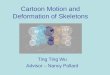
VAERS:(REPORTED VACCINEADVERSE REACTIONS) IN US1999-2002
AdverseReactionsReported Age 0-6
HospitalizationReported Age 0-6
DeathsReportedAge 0-6
DPT16,544
1,631394
HEP13,363
1,840642
Flu 419
4111
Hib22463
3,224843
MMR18,680
1,736110
OPV22,915
2,868 866
Total94,384
9,6042,866
As of the end of 2002, the VAERS system con-tained 244,424 total reports of possible reactionsto vaccines, including 99,145 emergency roomvisits, 5,149 life-threatening reactions, 27,925hospitalizations, 5,775 disabilities, and 5,309deaths[2], according to data compiled by Dr.Mark Geier, a vaccine researcher in SilverSpring, Md. The data represents roughly 1 billiondoses of vaccines, according to Geier. Dr. J.Anthony Morris, former Chief Vaccine ControlOfficer at the US Federal Drug Administrationagrees that such evidence has great bearing onthe entire vaccination question saying, "There isa great deal of evidence to prove that immuniza-tion of children does more harm than good."
Cancer-causingMonkey Virusesand the PolioVaccine
Americans have been told repeatedly thatHIV/AIDS is the first time a monkey virus hasjumped species to cause a new epidemic calledAIDS.
But the rarely-publicized truth is that a cancer-causing monkey viruses jumped species a halfcentury ago when contaminated polio vaccineswere given to millions of people on the planet,including half the U.S. population of that era.
In the early 1960's it was discovered that somelots of polio vaccines manufactured on rhesusmonkey kidney tissue during the period 1955 to1963 were contaminated with a monkey viruscalled SV40 (Simian[monkey] virus #40). This pri-mate virus was quickly proven to cause variouscancers in experimental animals. However, tothis day, U.S. government officials still insist thereis no absolute proof that SV40 causes humancancer.
Despite the lack of government interest in SV40in human cancer for three decades, genetic andimmunologic studies by independent researchersover the past decade indicate this virus is clearlyassociated with human cancer, such as rapidly-fatal cancers of the lung (mesothelioma), bonemarrow cancer (multiple myeloma), brain tumorsin children, and other forms of cancer.
A Washington Times report (09/21/03) indicates"Some of the polio vaccine given to millions ofAmerican children from 1962 until 2000 couldhave been contaminated with a monkey virus thatshows up in some cancers, according to docu-ments and testimony to be delivered to a Housecommittee Wednesday.
The vaccine manufacturer said such claims don'thave any validity,' and the Centers for DiseaseControl and Prevention (CDC) agrees.Documents set to be delivered to the HouseSubcommittee on Human Rights and Wellnessappear to show that the original "seeds" used toproduce the Sabin [oral] vaccine could havebeen tainted with SV40; that the company that

manufactured the vaccine, Wyeth Lederle, mayhave used Rhesus monkeys – which are morelikely to carry the disease – rather than theAfrican Green monkeys it says it used, accordingto company documents; and that the companymay not have performed all of the screening testsrequired."
Stanley P Kops is a lawyer who represents chil-dren and adults damaged by polio vaccines. Hehas documentation indicating that the polio virus"seeds" from which the oral vaccine is made arestill not proven to be free of SV40.
In his article entitled "Oral polio vaccine andhuman cancer: a reassessment of SV40 as acontaminant based upon legal documents",appearing in the journal Anticancer Research(November 2000), Kops states: "In litigationinvolving the Lederle oral polio vaccine, the man-ufacturer's internal documents failed to revealsuch removal [of SV40] in all of the seeds. Theabsence of confirmatory testing of the seeds, aswell as testimony of a Lederle manager, indicatethat this claim of removal of SV40 and the testingfor SV40 in all the seeds cannot be fully substan-tiated.These legal documents and testimony indi-cate that the scientific community should not becontent with prior assumptions that SV40 couldnot have been in the oral polio vaccine.
Only further investigation by outside scientificand independent researchers who can review thetest results claimed in the January 1997 meetingand who can conduct their own independent eval-uations by testing all the seeds and individualmono-valent pools will assure that SV40 has notbeen present in commercially sold oral poliovirusvaccine manufactured by Lederle."
More information on Kops, SV40, and polio litiga-tion can be found at www.sv40cancer.com
More than 600 million doses of polio vaccinewere sold by Lederle from 1963 to 1999. On Jan.1, 2000, the CDC recommended injections of aninactivated killed polio vaccine (IPV) that elimi-nates the risk of spreading the disease, unlike theoral live polio vaccine that had been used fordecades. This prompted Lederle to get out of thepolio vaccine business, and the last batch ofOrimune was produced on Dec. 31, 1999.
For anyone who still thinks that vaccine makersand government health officials are always yourfriend, I would highly recommend a just-pub-lished book titled AIDS. The Virus and theVaccine: The True Story of a Cancer-CausingMonkey Virus, Contaminated Polio Vaccine,and the Millions of Americans Exposed, by
Three books youshould read as
soon as you can:SUPPRESSED INVENTIONSAND OTHER DISCOVERIES by Jonathan EisenRRP $29.95
The classic, controversial bestseller that details hun-dreds of products, technologies and medical cures thathave been suppressed over the last 100 years.
THE CANCER PREVENTIONHANDBOOK by Katherine SmithRRP $29.95
What your doctor and cancer society don’t want you toknow. Details many everyday carcinogens found in thehome and office (medicines, too) you may not be awareof, and non-toxic replacements you should know about.
The GE Selloutby Jonathan EisenRRP $9.95
GE is biowarfare with another name. Learn about thisdangerous technology and why the government is hellbent on literally forcing it down your throat.
PEOPLE POWERby Jonathan EisenRRP $14.95How to make the government listen to you, for achange. The definitive book on Direct Democracy andBinding Citizens Initiated Referenda.
Please rush me the following books:[ ] Suppressed Inventions ($29.95)
[ ] Cancer Prevention Handbook ($29.95)
[ ] The GE Sellout ($9.95)
[ ] People Power ($14.95)
Please add $4 per book for p/h. All orders are prepaidonly. Sorry, no credit cards.TOTAL AMOUNT ENCLOSED: $________
Name .......................................................................
Address ...................................................................
City/Town .................................................................

Debbie Bookchin and Jim Schumacher. The bookexplores the history of the polio vaccine, the con-tamination problems with SV40 , the ensuing vac-cine-related cancer problems, and the govern-ment's cover-up of the problem over the pastthree decades.
Few people realize how dangerous vaccines canbe and how complicated the process of vaccinemanufacture really is, particularly when vaccinesare made on living animal or human cells.Contamination with bacteria and viruses andtheir elimination from the final product are con-stant problems during the process.There are alsorecent suspicions that the laboratory media usedto feed and nourish the cell cultures upon whichthe virus is grown may also be a source of con-tamination.
For further details on the dangers of vac-cines, see "Are Vaccines Causing MoreDiseases than they are Curing?"(www.whale.to/v/cantwell.html)
Rense.com
Death By LethalVaccineInfection By Christine Colebeck 9-17-4
Today is my daughter's sweet 16th birthday butwe will not be celebrating.
Instead I will light a candle and when I blow it outI will make a wish in my daughter's memory. Mywish is for all mother's worldwide, that you willeducate yourselves and that you make informedchoices so that you may prevent unnecessarytragedy and be spared from my pain.
Laura's Story
After 41 weeks of pregnancy, on July 27th, 1986,a perfect and healthy little baby, Laura Marie,made her entrance into the world. We were wel-comed home by family and friends anxiouslywaiting to meet the new family member. Theyshowered her with so many beautiful, little tiny,pink dresses, we joked that she would never beable to wear them all in one lifetime.
Our lives changed completely and now revolvedaround stroller walks in the park, visiting friends,changing diapers, night feedings and shopping
for more little pink dresses. We were parents now,we had a family and life was absolutely perfect.
I took Laura for several baby check-ups at thepediatrician. She was a kind and gentle olderwoman. At 3 months old, the pediatrician wasvery pleased with Laura's development andweight gain and vaccinated her with DPT OPV. Ididn't even question her, I knew that all myfriend's babies had this same vaccine and "allgood mothers" vaccinated their children to pro-tect them. I left the pediatrician's office andwalked home.
Laura was very fussy, which was unusual. Shewas crying loudly all the way home in the stroller.When we got home, I realized she had urinatedso heavily she wet everything in the stroller. Thenher cry turned into screaming and she developeda fever, her leg was very swollen and red, and felthot. I called the pediatrician who told me this was"normal" and to give her Tempra. I gave her babyTempra and I felt better, the pediatrician hadassured me this was normal.
Laura continued to scream and I could no longerconsole her. My every instinct told me this wasnot normal but I was young with my first child andtrusted the doctor. I could not hold Laura in myarms because she screamed louder as anymovement of her leg seemed to cause her terri-ble pain. I put her in the swing and she cried her-self to sleep. I was so relieved, the Tempra wasworking and the doctor must have been right. Ibegan to feel silly for all my worrying. A short timelater, Laura woke up screaming and spent theevening screaming and sleeping on and off.
She had no appetite and nothing made her stopcrying. Finally it was bedtime and she cried in hercrib, until she fell asleep. She had never criedherself to sleep before and I felt very bad for let-ting her but if I held her, she screamed louder. Myhusband came home from work and I told himabout everything that had happened that day.Laura was sleeping soundly in her crib and wewere both relieved that she seemed to be feelingbetter and decided not to worry... I should haveworried.
In the morning I awoke and was startled to real-ize my husband had slept in for work. I immedi-ately knew something was wrong and the worryfrom the previous night came rushing back to me.I quickly ran to her crib, with a feeling of dread.She did not look right. I closed my eyes tight andopened them again, and considered the possibil-ity that this was a dream, but when I opened myeyes she looked dead.

I went into shock and after that, much of this dayremains a blur. I touched her and she was verywarm. I screamed for my husband to call 911.
I watched as he performed CPR, my body wasfrozen and I couldn't move. He tried to revive ourchild to no avail. He was shouting for me to openthe door for the paramedics, I was temporarilyjolted back to reality and I went and opened thedoor. I could now move but couldn't speak. I juststood there numbly shaking my head, feelingcompletely helpless as dozens of paramedics,police and firemen rushed past me into ourhome. I didn't cry, and I wanted to scream at themto leave her alone but I couldn't speak. She wason the floor and they were shocking her tiny body,in the little bedroom with the yellow painted wallsand clown wallpaper. I stood there praying in myhead that they would just leave her alone, thatthey would get out of her bedroom and that Iwould wake up from this horrible dream.
Then I heard someone saying there was a faintpulse and I suddenly felt hopeful. She was rushedfrom the house in an ambulance. It was then thatthe homicide detectives led us into another roomand the interrogation began.
They decided that my husband and I needed tobe questioned in separate rooms. I immediatelyrealized they suspected that we had done this toour child. We all know that perfect children do notsuddenly die for no reason. I was silent, I hadalready decided in my own mind that this wassomehow all my fault and although I wasn't quitesure what I had done to kill her, I was convincedthat I had somehow caused this to happen.Perhaps, I was being punished by god for a sin orperhaps it happened because I had let her cryherself to sleep that night. The fact remained thatmy child was dead and "good mothers" do nothave dead children.
My husband began to protest loudly about theline of questioning and he demanded we betaken immediately to the hospital, to see ourchild. The detectives finally took us to the hospi-tal and put us in the "bad news room." The doc-tor came and insisted we sit down before hespoke to us. He began telling us that they hadtried this and that and then finally he said thewords that would echo in my ears for a lifetime:
"She is dead."
The pediatrician whom I so respected andadored broke down and cried when I gave her thenews on the phone. She went back and forthdefending the vaccine that she was told was safe,and blaming it for killing my child and those who
told her it was safe.
She then told me that she also had anotherpatient, an infant boy, die after this same vacci-nation.
Then the detectives took us home for more ques-tions, often repeating the same questions sever-al times until they grew tired of asking them. Thequestions constantly centered around ourinvolvement, then they searched the house anchecked for signs of forced entry. My husbandrepeatedly told them that he thought the vaccinehad killed our child and told them over and overabout her unusual behavior since she was vacci-nated.
Everyone we knew arrived at our house. I madecoffee and tidied the house, like it was any otherday and we were having "guests". Shock is astrange and wonderful thing and of course youdon't know you are in it.
My parents finally insisted on taking me to theirhouse for a few days, while my husband and hisfriends had the horrendous task of packing up thenursery because I couldn't stand to look at it anylonger. The room I had so lovingly made was nowempty and a source of great pain.
Several days later, after the funeral and the tinywhite coffin that was so small my husband car-ried it alone, I finally came out of shock andallowed myself to cry a river. I cried for all thethings I would never do with my daughter. All theballet classes I would never take her to, the wed-ding I would never attend, the grandchildren Iwould never know and all the dreams I wouldnever realize with her. I cried for all that was andall that would never be. There was an emptinessinside of me that threatened to swallow me upwhole, as I fell into the depths of grief during thedarkest days of my life.
The detectives eventually became satisfied thatwe had not harmed our daughter in any way andthe investigation into her death ended. We werethen left without answers.
The doctors did not want to talk about her deathbeing related in any way to the vaccine and, oneafter the other, refused to answer our many ques-tions. I was repeatedly told that vaccines were for"the greater good." I was even told that loss of lifethrough immunization was "expected" in the waragainst disease but these losses were consid-ered to be at "acceptable" levels. However, thisdid not feel very acceptable or good to me as amother with empty arms that ached for my child.The coroner finally told us months later that the

cause of death was determined to be "SIDS"(sudden infant death syndrome), meaning "noknown cause," and refused to release a copy ofthe autopsy report to us.
It took almost a year for us to obtain this reportand to our great horror, we realized that theautopsy summery was copied directly from thevaccine product monograph under the heading"Contraindications" as follows:
"Sudden infant death syndrome has been report-ed following administration of vaccines containingDiphtheria, tetanus toxoids, and pertussis vac-cine. However, the significance of these reports isnot clear. One common factor is the age whereprimary immunization was done between the ageof 2 to 6 months, a period where most suddeninfant death syndromes are found to 1occur witha peak incidence being at 2 to 4 months."
There was no toxicology testing performed andthe pediatrician never filed an adverse vaccinereaction report with health authorities. I laterlearned that most vaccine-induced deaths in thiscountry are listed as SIDS and SIDS statistics areNOT included in vaccine adverse reaction data,even if a child dies only a few hours after receiv-ing inoculation. This data is presented to physi-cians and the public to reassure them that vac-cines are safe.
The government's own literature advises thatthere has been little or no testing in the area ofvaccine safety or efficacy. Essentially, our chil-dren are the test. According to their literature,immunization is "the most cost effective" way toprevent disease. Nowhere in their literature doesit claim to be the safest. We are trading our chil-dren's lives to save the government money. Weare told that the benefits outweigh the risks butmany of the diseases that we vaccinate for arenot even life threatening; however, the vaccineitself has the potential to kill.
Vaccines kill at a much higher rate than we areled to believe. We play vaccine roulette with ourchildren's lives and we never know which childwill fall victim next.
If the odds are 1 in 500 thousand for death, 1 in100 thousand for permanent brain injury, 1 in1700 for seizures and convulsions or one in 100for adverse reaction, are you willing to take thatchance? Are any odds acceptable enough toconvince you to gamble with your child's life?
I can assure you that death from vaccination isneither quick nor painless. I helplessly watchedmy daughter suffer an excruciatingly slow death
as she screamed and arched her back in pain,while the vaccine did as it was intended to do andassaulted her immature immune system. The poi-sons used as preservatives seeped through hertiny body, overwhelming her vital organs one byone until they collapsed. It is an image that willhaunt me forever and I hope no other parent everhas to witness it.
A death sentence considered too inhumane forthis county's most violent criminals was handeddown to my beautiful, innocent, infant daughter,death by lethal injection.
Today, on my daughter's birthday, I will grieve notonly for the loss of my own child but for all theinnocent children for which the benefits of vac-cines do not outweigh the risks and are unneces-sarily sentenced to death by lethal injection,under the guise of "the greater good." The truewar is not against disease; we have somehowbecome our own worst enemy by putting our faithin science instead of nature. Today, I call on allmothers across the world to join me in putting anend to this senseless slaughter of our most pre-cious resource, our children.
Commentary by Dawn Richardson
http://www.vaccineinfo.net/PROVE
Dear PROVE Members
I am forwarding this ... as a tribute to baby Lauraand all the other children who have been injuredor killed by a vaccine so that parents can learnanother side to the vaccine story.
When I was almost 8 months pregnant with oneof my daughters, I had volunteered to go to theTravis County Morgue with Karin Schumacherwho, for years before she went to Law School,ran the NVIC news-list. Karin asked me to helpher go through autopsy reports of infants listed asSIDS deaths and look at vaccination information.I will never forget the experience. We sat there inthis basement buried in infant autopsy reports asmy own baby kicked and turned inside of me.
Here were two of our observations: 1) A highlydisproportionate amount of SIDS deaths clus-tered at 2, 4, and 6 months – which are the verytimes infants are vaccinated. If vaccines hadnothing to do with these, the numbers shouldhave been randomly spread throughout the first 6months of life. Not so. I challenge the naysayersto go to any morgue in the country and to be hon-est and see what I'm talking about.

2) It was shocking at how rare it was for the vac-cine information to be recorded and how littleinvestigating into the cause of death of thesebabies was actually done. It floored me that thewhen the vaccine information was even men-tioned, it was often so incomplete. Medical exam-iners routinely missed asking for this indispensa-ble information and failed to note the correlationof the date when the child died to even raise thequestion.
One of the things that struck me when readingChristine's story ... is that here we are 16 yearslater and so many doctors are still downplayingand denying the risks of vaccines and healthybabies are still dying after being vaccinated.
One of the most offensive things that SenatorFrist has in his vaccine bill which shields the drugcompanies from all liability when a vaccineinjures or kills someone is that he is proposingthat the federal government increase the amountof money that a parent receives from the govern-ment compensation program when their child iskilled by a vaccine.(http://www.senate.gov/%7Efrist/Contact/con-tact.html.) Parents are not willing to be bought offwith this blood money. Elected officials like Fristwho want to eliminate the financial responsibilityof the drug companies altogether and throw abone to parents that the government will paythem more if the government mandated vaccinekills their kid need to be voted out of Congress.
The key to change is education. Fortunately, theInternet allows parents to educate parents.Please stop for a quiet moment after reading thenote and say a prayer for all the babies whoselives were ended before they even got a chanceto really start ... and then take the time to forwardthis on to other parents.
Sincerely, Dawn Richardson President, PROVE
http://www.vaccineinfo.net/national_issues/oppose_Frist_bill_s2053.htm
Senator Frist's Vaccine Bill S 2053
Dr. Mercola's Comment:
I strongly urge you to forward this particular pieceto everyone – parents, expecting parents, womenin their childbearing years, and anyone who mayknow such individuals – and ask them to forwardit on, too. One of the greatest powers of theInternet is that we can spread important informa-tion quickly; another is that we are not (yet!)restricted from doing so by government or corpo-
rate bodies.
Laura's tragic story is, sadly, anything but new.For years, as you can see via the links below orby searching on Mercola.com, I have warnedagainst vaccines, as have other credentialedphysicians. The good they may do is over-whelmed by the harm they inflict, from the traumaof being stuck with endless needles to inflictingthe very disease they are supposed to guardagainst to, as this story shows, death.
http://www.mercola.com/article/vaccines/death.htm
There are alternate and vastly safer methods thatall begin with a truly healthy diet as outlined in my Eating Plan; of course, drug manufacturers andthe government they have purchased don't wantyou to believe that the foods you consume andthe habits you adopt are the primary solution toestablishing immunity to diseases and livinglonger. They want you to believe that their phar-maceuticals, including vaccines, are essential toyour existence, and your children's.
http://www.mercola.com/nutritionplan/index.htm
Their wealth relies on your dependency, and sothey will do everything to crush the notion of "nat-ural" - meaning they don't profit from it, and youtake back the control - health. They will spendthree billion dollars this year alone in advertise-ments for their pharmaceuticals, preying onunsuspecting consumers' hopes and fears withthese carefully crafted campaigns. Apparently,they will not even stop at killing our children tofeed their greed.
Again, I encourage you to check out the linksbelow, and to use the powerful search feature onMercola.com, using terms such as "vaccine" or"pharmaceutical manufacturer," to find out howthe corporate medical establishment is puttingyour life and the lives of those you love at risk –and how to take back your health.
Related Articles:
http://www.mercola.com/2001/aug/18/vaccine_myths.htm
http://www.mercola.com/2002/jul/31/hoax.htm
Dispelling Vaccination Myths http://www.mercola.com/2002/mar/30/mercury_vaccine.htm
Mercury Poisoning from Vaccines http://www.mercola.com/2002/jul/31/hoax.htm
Pharmaceutical Advertising: Another 3 Billion Dollar Hoax http://www.mercola.com/2002/feb/2/vaccine_insanity.htm

The Dark Side ofImmunizations
“A controversial hypothesis suggests thatvaccines may abet diabetes, asthma.Epidemiological studies hint at a possiblelink between vaccinations and immunesystem disruption.”
FROM: Science News 22 November 97
"Bart Classen, a Maryland physician, pub-lished data showing that diabetes ratesrose significantly in New Zealand followinga massive hepatitis B vaccine campaign inyoung children, and that diabetes ratesalso went up sharply in Finland after threenew childhood vaccines were introduced."
In fall 1997, two influential professional maga-zines featured articles asking the question: Hasthe decrease of infectious diseases in childhoodthrough the mass use of vaccines been replacedwith an increase in chronic diseases such as dia-betes and asthma? The Economist , a presti-gious international magazine read by world lead-ers in government, business and public policy,and Science News , a magazine read by bothhealth care professionals and the general public,explored the reported links between vaccinesand chronic diseases in their November 22, 1997issues.
Their conclusion was that there indeed appearedto be a connections between some vaccines andchronic illness in later life. This conclusion cor-roborated an earlier study in the NZ Journal ofMedicine which found a connection between theHepB vaccine and juvenile diabetes.
We need to learn a lot more about vaccine &diabetes connection – asthma & vaccine connec-tion – SIDS & autism and vaccine connection –"Shaken Baby Syndrome": the vaccination link.
US Congressman callsfor criminal penaltiesfor thimerosal coverup
A US Congressman is calling for criminal penal-ties for any government agency that knew aboutthe dangers of thimerosal in vaccines and didnothing to protect American children.Congressman Dan Burton (R-Indiana) duringCongressional Hearing:
"You mean to tell me that since 1929, we've beenusing Thimerosal, and the only test that you knowof is from 1929, and every one of those peoplehad mennigitis, and they all died?" For nearly anhour, Burton repeatedly asked FDA and CDC offi-cials what they knew and when they knew it.(Thimerosal contains a related mercury com-pound called ethyl mercury. Mercury is a toxicmetal that can cause immune, sensory, neurolog-ical, motor, and behavioral dysfunctions.)
Sources:
J. Barthelow ClassenClassen Immunotherapies6517 Montrose AvenueBaltimore, MD 21212
Patricia M. GravesDepartment of EpidemiologyUniversity of Colorado Health Sciences CenterDenver, CO 80210
Joan T. HarmonNational Institute of Diabetes and Digestive and KidneyDiseasesBuilding 45, Room 5AN1845 Center DriveBethesda, MD 20892-6600
Ronald E. LaPorteGraduate School of Public HealthUniversity of PittsburghRoom A529Pittsburgh, PA 15261
Howard L. WeinerCenter for Neurologic DisordersBrigham and Women's Hospital77 Avenue Louis PasteurBoston, MA 02115

MMR HAS STRONGASSOCIATION WITHAUTISM – U.S.RESEARCHBy John von Radowitz The IndependentAugust 9, 2002
http://news.independent.co.uk/uk/health/story.jsp?story=322755
New evidence suggesting a link between the measles,mumps and rubella (MMR) vaccine and autism emergedyesterday from the United States.
Scientists at Utah State University found a strong associa-tion between the MMR jab and an auto-immune reactionthought to play a role in autism.
The team, led by Dr Vijendra Singh, analysed blood sam-ples from 125 autistic children and 92 children without thedevelopmental disorder. The researchers found a "signifi-cant increase" in the level of MMR antibodies in theautistic children. Part of the measles component of the vac-cine caused an unusual anti-measles response in 75 of theautistic children, but not in the normal children.
More than 90 per cent of the autistic samples that showedan immune response to MMR were also positive for anti-bodies thought to be involved in autism. These antibodiesattack the brain by targeting the basic building blocks ofmyelin, the insulating sheath that covers nerve fibres. DrSingh suggested that auto-immune response might be theroot cause of autism.
The US scientists, who report their findings in the Journalof Biomedical Science, concluded: "Stemming from this evi-dence, we suggest that an inappropriate antibody responseto MMR, specifically the measles componentthereof, might be related to pathogenesis of autism."
Dr Singh published previous work indicating a link betweenMMR and autism, concentrating on the brain's reaction. Hehas argued for years that autism can be traced to an auto-immune reaction centred on the brain. MMR fears havebeen blamed for a dip in the number of children being vac-cinated between December and March.
The pressure group Jabs (justice, awareness and basicsupport), which wants parents to have the option of givingtheir children single injections, said the research strength-ened its case.
Jonathan Harris, its West Midlands spokesman, said: "Ireally feel there's a very, very strong case now for sus-pending MMR use while further investigations are carriedout. At the moment parents only have the choiceof MMR or nothing. We think that's irresponsible of theDepartment of Health."
EXPERTS DIFFER WHILECHILDREN CONTINUE TOSUFFER AUTISM
By Kathy SinnottIrish ExaminerJuly 26, 2002
http://www.examiner.ie/pport/web/opinion/Full_Story/did-sgSd9bGREwpTA.asp
Over the past couple of years, we have seen medicalauthorities and medical correspondents reaching a notguilty verdict on the MMR causing autism. They justify thison the basis of scientific evidence. Maybe it's time thepublic understood this term. Scientific evidence is 100%evidence. Does the public realise that, by this definition, wecannot be sure that smoking causes lung cancer?
Maybe it's time to note that there are other types of evi-dence:
First, there is laboratory evidence. For example, there's thefact that our leading cell pathologist has discovered that avirus is causing a new type of ulceration in the bowels ofchildren that regressed into autism, that the offending virusis a measles virus and that the sequenced DNA of this virusis that of the vaccine strain of measles, not wild measles.
There is clinical evidence, that of physicians treating thesechildren. Physicians who, because they recognise and treatthe viral, heavy metal, and fungal overloads experienced bythese children, are successfully improvingthese childrens' lives.
Then there is anecdotal evidence. For example, on theHope Project Helpline, we have heard hundreds of autismonset stories from parents and the vast majority of theseimplicate the MMR, and others the DPT vaccine in autism.
Lastly, there is the eyewitness evidence of frightened par-ents who have watched their beautiful children slip awayinto the quagmire of autism within weeks of the MMR.
It is a sad fact that the only evidence that seems acceptablein this debate (can you call something as lopsided as theMMR controversy in Ireland a debate?) is 100% scientificevidence. Hard and damning laboratory evidence seems tobe ignored, clinical evidence is excused, anecdotal evi-dence ridiculed as scare-mongering and parental eyewit-ness evidence cannot be accepted by our guardians ofdrug safety, the Irish Medicines Board.
So what will happen? For the time being, susceptible chil-dren and teenagers will continue to develop AutisticSpectrum disorders, bowel disease, eating disorders andbipolar, to name but a few, in ever increasing numbers.
Eventually, the decision will be taken out of the hands of ourmedical guardians and Minister for Health and Children. AHigh Court judge will listen to all the types of evidence andhe or she will make a legal decision on the balance of prob-ability, 51% that the MMR caused the plaintiff to becomeautistic.
Following a number of these decisions, a tribunal will beheld and we will finally be able to understand how medicalauthority, money and politics allowed thousands of Irishchildren to be sacrificed to the requirements of100% "scientific evidence".

http://www.nzherald.co.nz/storydisplay.cfm?storyID=3572104&thesection=news&thesubsection=general
Concern mounts overfraudulent medicalresearch 13.06.2004By DIANA McCURDY
Be wary next time you read about a medical breakthroughor a miracle drug. New research has found that scientistsare disturbingly selective when reporting the results of clin-ical trials.
Many scientists cherry-pick favourable results. Otherschange tack when unexpected or interesting resultsemerge, breaching research protocols.
A research team led by Oxford University academic An-Wen Chan analysed 102 trials and found that researchersfailed to fully report almost two-thirds of the results relatingto potentially harmful outcomes.
Half of the results relating to the effectiveness of a treat-ment were not made fully public.
Many researchers also failed to adhere to basic researchprotocol. Scientists are supposed to specify their mainobjectives - or "primary outcomes" - before beginning a trialto protect against selective reporting.
However, in 62 per cent of cases, researchers changed theprimary outcomes in their published reports.
In one published trial, the assessment of pain intensityshifted from being a primary outcome to being unspecified.In another, researchers introduced new primary outcomesthat were not mentioned in their initial outline.
"The reporting of trial outcomes is not only frequentlyincomplete, but also biased and inconsistent with proto-cols," the team reported in the Journal of the AmericanMedical Association. "Published articles, as well as reviewsthat incorporate them, may therefore be unreliable andoverestimate the benefits of intervention."
It's a disturbing prospect. Ultimately, clinical trials influencewhich drugs your doctor prescribes - and which drugsPharmac funds.
"The worst possible situation for patients, healthcare pro-fessionals and policy-makers occurs when ineffective orharmful interventions are promoted," the team says. "But itis also a problem when expensive therapies, which arethought to be better than cheaper alternatives, are not trulysuperior."
Many researchers seem oblivious to the potential bias intheir published reports. Eighty-six per cent of respondentsto the Oxford study denied the existence of unreported out-comes despite clear evidence to the contrary.
Auckland University Clinical Trials Research Unit (CTRU)director Anthony Rodgers describes the team's findings asa "wake-up call", but not surprising.
This study is not the first to cast suspicion upon potentialbias in medical research, he says.
In an effort to counter the problem, pressure is mounting forcompulsory registration of trials.
In New Zealand, there is no definitive register of clinical tri-als. Some researchers sign up with off-shore registers butit is not compulsory to do so.
Rodgers is among a group of academics agitating for acompulsory register to be set up in New Zealand. "[It will]basically keep researchers honest and make sure trials getpublished in the way they were planned and inconvenientthings don't get pushed under the carpet."
CTRU research fellow Andrew Jull says registers also helpto stop bias from creeping into common medical practice.
When clinicians or government funding agencies want toassess the merits of a drug, they turn to reviews of pub-lished trials. Those reviews give an overview of all researchinto a particular treatment or condition.
But there is a growing concern that non-publication of sometrials is skewing results. Australian research has found thattrials with a positive outcome are three times more likely tobe published than those with a negative outcome, so thepublic frequently doesn't see unfavourable or inconvenientfindings.
"So if your trial finds that something doesn't work or, alter-natively, it doesn't find a result full stop, then it is apparent-ly more difficult to get it published," Jull says.
Failure to publish can have dangerous - even lethal - con-sequences.
When a recent review of antidepressant trials looked atpublished and unpublished research it found that severaldrugs that seemed beneficial for children actually appearedto cause more harm than good when all published andunpublished research was taken into account.
An even more alarming example occurred in the 1980s andearly 1990s when thousands died while using an approvedheart attack medication. It was not until 1993 that a trialconducted 13 years earlier was published, along with itsevidence of a higher death rate.
Today, failure to publish is increasingly viewed as a form of

scientific misconduct. But overcoming journal editors' pref-erence for positive results can be difficult.
Such is the extent of the problem that a journal has beenestablished to cater specifically for negative findings - theJournal of Negative Results in Biomedicine.
Jull says that when journal editors' bias toward positiveresults is combined with the potentially biased reporting ofresearchers, it creates a very real danger we will develop askewed perception of how effective certain drugs are.
Efforts have already been made to conquer the problem.The major medical journals now subscribe to the Consortstatement, which provides strict guidelines for unbiasedtrial reporting. The journal editors have also agreed to try tocounter their bias toward positive trials.
More people within the health profession are recognisingthat they should take into account the results of unpub-lished trials in their treatment reviews. The CochraneCollaboration, which was established in 1993 to providesystematic reviews of health research, now uses both pub-lished and unpublished data.
Jull believes making it compulsory to register clinical trialswould greatly improve public access to results.
"Before you are allowed to proceed, you must register [yourtrial] with a database that's accessible to all," he says. "Sowhen people reviewing evidence make a decision whethera treatment works or not, they have access to all the evi-dence and not just the published evidence."
More than 500 applications for clinical trials have gone toresearch ethics committees in New Zealand in the past fiveyears. It is not known how many were later withdrawn andhow many have languished unpublished.
Jull says ethics committees have a duty to ensure trialresults become public. "If it is unpublished, there is thepotential that, even with the best will, prescribers can bemisled, and that can have disastrous effects."
At the moment, there is little official interest in setting up aNew Zealand register, but Jull believes it would be a simple,cheap exercise to set one up online. Researchers couldenter their own details over the internet.
"It's probably easier than in a lot of other countries becausewe have ethics committees that work to a single operationalstandard. No clinical trial can proceed without ethics com-mittee approval. It would be relatively simple for the ethicscommittees to say: Is this registered?"
As well as combating potential bias, a New Zealand regis-ter of trials would help scientists to keep tabs on localresearch, making collaboration easier and preventing dupli-cation, Jull says. Patients and clinicians could also use theregister to track down trials in which they could participate.
Doctors Are The ThirdLeading Cause ofDeath in the US,Killing 250,000 PeopleEvery Year – JAMA The July 28th (2000) issue of the Journal of the AmericanMedical Association (JAMA) is the best article I have everseen written in the published literature documenting thetragedy of the traditional medical paradigm.
JAMA admits: ConventionalMedicine is the 3rd LeadingCause of Death in the U.S.
In a mind boggling article published by The Journal of theAmerican Medical Association - Vol. 284. No. 4 - July 28,2000 the research finally admits to mainstream that theyare killing 250,000 Americans per year. They estimate thefigure to be low and say remember these are only the deathfigures, not the adverse side effects associated with dis-ability or discomfort. Complete article is on the web site.
12,000 - unnecessary surgery7,000 - medication errors in hospital 20,000 - other errors in hospitals80,000 - nosocomial infections in hospitals106,000 - adverse effects of medications
Many believe the US has the best health care in the world,but look at more JAMA stats. Of 13 countries the US rank-ings are terrible. (Countries in order of their average rank-ing - Japan, Sweden, Canada, France, Australia, Spain,Finland, Netherlands, U.K., Denmark, Belgium, US, andGermany.)
A child who developed severe epilepsy after receiving theMMR jab has been found to have measles virus from thevaccine in his brain. The results of tests conductedrecently have been revealed by the 13-year-old boy'smother. She says that she has decided to go public inorder to push the Government to take the plight of chil-dren allegedly damaged by the three-in-one measles,mumps and rubella vaccination more seriously. Scientistssay that the implications of the discovery are difficult toassess without further research. However, it raises newquestions about the triple inoculation, which has beendogged by controversy since Andrew Wakefield, a formerconsultant at the Royal Free Hospital in London,<http://www.telegraph.co.uk/news/main.jhtml?xml=/news/2001/01/21/nmmr21.xml>linked it with a new syndromeof bowel disease and autism in children.

Doctors SpeakOut on VaccinesEven the WHO (World Health Organisation) has admitted,disease and mortality rates in Third World countries haveno direct correlation with immunisation procedures or med-ical treatment, but they are closely related to the standardof hygiene and diet. A 1973 issue of Scientific Americanrevealed the same finding : that "over 90% of all contagiousdisease was eliminated by vastly improved water systems,sanitation, living conditions and transportation of food."Mass vaccinations did not appear on the scene until a cen-tury after the decline in infectious diseases started (1850-1940), but inoculations were, and still are given full credit. –Susan DeSimone
"Up to 90% of the total decline in the death rate of childrenbetween 1860-1965 because of whooping cough, scarletfever, diphtheria, and measles occurred before the intro-duction of immunisations and antibiotics." ---Dr. ArchieKalokerinos, M.D.
"The mechanics of vaccination to build immunity, on theother hand, is quite unnatural. Rather than space exposureto a relatively minuscule level of micro-organisms in agradual manner, massive quantities of antigens are intro-duced into the body through a series of vaccinations thatare given right in a row over a short period of time. All vac-cines, with the exception of the OPV (oral polio vaccination)are injected directly into the bloodstream, by-passing themucosal immune system known as the secretory IgA. Thesecretory IgA is the first in a series of defensive levels with-in the immune system. It serves as a buffer, filteringmicrobes so that the impact of these invading organismsis greatly reduced once it reaches the bloodstream.The IgAallows the antigen to be removed in the same manner inwhich it arrived - through the mucosal barrier - by sneez-ing, coughing and sweating. So a vaccine that has beeninjected "gives the body no warning, no generalised inflam-matory response, no chance to recognise, duplicate ordefend itself against future challenges from typical anti-gens." – Dr. Robert Mendelsohn, How to Raise a HealthyChild In Spite of Your Doctor.
A recent topical example: the diphtheria case, and the"fear" created by this one, extremely mild, case in anunvaccinated child. Dr Ossi Mansoor, a principal doctorregarding vaccination policy, stated on Radio Pacific, "Thefigures we have are that in the 1920s there were 800deaths every year" (from diphtheria). Yet the New ZealandGovernment's statistics show the average yearly numberwas below 100, also that the average death rate per 10,000mean of population fell from 6.08 to 0.20 before the use ofthe diphtheria vaccine. – Southland Times 30-Sep-1998
"I've been practicing for 40 years, and in the past 10
years the children have been sicker than ever."--Dr DorisJ.Rapp, paediatric allergist.
"Measles, mumps, rubella, hepatitis B, and the wholepanoply of childhood diseases are a far less serious threatthan having a large fraction (say 10%) of a generationafflicted with learning disability and/or uncontrollableaggressive behaviour because of an impassioned crusadefor universal vaccination... Public policy regarding vaccinesis fundamentally flawed. It is permeated by conflicts ofinterest. It is based on poor scientific methodology (includ-ing studies that are too small, too short, and too limited inpopulations represented), which is, moreover, insulatedfrom independent criticism. The evidence is far too poorto warrant overriding the independent judgements ofpatients, parents, and attending physicians, even if thiswere ethically or legally acceptable."
– Association Of American Physicians & Surgeons
"If you want the truth on vaccination you must go to those
Vaccine-DiabetesConnection
In the May 24, 1996, New ZealandMedical Journal, J. Barthelow Classen,MD, a former researcher at the U.S.National Institutes of Health (NIH) andthe founder and CEO of ClassenImmunotherapies in Baltimore, report-ed that juvenile diabetes increased 60per cent following a massive hepatitisB vaccination campaign for babies sixweeks or older in New Zealand from1988 to 1991. In the October 22, 1997,Infectious Diseases in Clinical Practice,Classen showed that Finland's inci-dence of diabetes increased 147 percent in children under five after threenew vaccines were introduced in the1970s, and that diabetes increased 40per cent in children aged 5 to 9 afterthe addition of the MMR and Hib vac-cines in the 1980s. He concluded that"the rise in IDDM [juvenile onset dia-betes] in the different age groups cor-related with the number of vaccinesgiven."

who are not making anything out of it. If doctors shot at themoon every time it was full as a preventive of measles andgot a shilling for it, they would bring statistics to prove it wasa most efficient practice, and that the population would bedecimated if it were stopped." – Dr Allinson
"To pass our examinations and get qualified, we mustaccept what our teachers tell us. In other words, we mustcultivate what Josh Billings called 'A well-balanced mind –one that will balance in any direction required.'"
– Major R. Austin M.R.C.S., L.R.C.P
"The greatest threat of childhood diseases lies in the dan-gerous and ineffectual efforts made to prevent themthrough mass immunisation. There is no convincing scien-tific evidence that mass inoculations can be credited witheliminating any childhood disease."
– Dr. Robert Mendelsohn, M.D.
"I think that no person would permit anybody to get close tothem with an inoculation if they would really know how theyare made, what they carry, what has been lied to themabout them and what the real percent of danger is of con-tracting such a disease which is minimal."
– Dr. Eva Snead
"There are significant risks associated with every immuni-sation and numerous contraindications that may make itdangerous for the shots to be given to your child...There isgrowing suspicion that immunisation against relativelyharmless childhood diseases may be responsible for thedramatic increase in autoimmune diseases since massinoculations were introduced. These are fearful diseasessuch as cancer, leukaemia, rheumatoid arthritis, multiplesclerosis, Lou Gehrig's disease, lupus erthematosus, andthe Guillain-Barre syndrome." – Dr. Mendelsohn, M.D.
"Probably 20% of American children-one youngster in five-– suffers from 'development disability'. This is a stupefyingfigure... We have inflicted it on ourselves.. 'developmentdisabilities' are nearly always generated by encephalitis.And the primary cause of encephalitis in the USA and otherindustrialised countries is the childhood vaccination pro-gram.To be specific, a large proportion of the millions of USchildren and adults suffering from autism, seizures, mentalretardation, hyperactivity, dyslexia, and other shoots orbranches of the hydraheaded entity called 'developmentdisabilities', owe their disorders to one or another of thevaccines against childhood diseases."
– Harris Coulter, PhD
"It is pathetic and ludicrous to say we ever vanquishedsmallpox with vaccines, when only 10% of the populationwas ever vaccinated." – Dr. Glen Dettman
"There is no evidence that any influenza vaccine thus fardeveloped is effective in preventing or mitigating any attackof influenza. The producers of these vaccines know thatthey are worthless, but they go on selling them anyway."
– Dr. J. Anthony Morris (formerly Chief Vaccine ControlOfficer at the US Food and Drug Administration)
"There is a great deal of evidence to prove that immunisa-tion of children does more harm than good." – Dr. J.Anthony Morris (formerly Chief Vaccine Control Officer atthe US Food and Drug Administration.)
"There is insufficient evidence to support routine vaccina-tion of healthy persons of any age." – Paul Frame, M.D.,Journal of Family Practice
"Official data shows that large scale vaccination has failedto obtain any significant improvement of the diseasesagainst which they were supposed to provide protection"
– Dr. Sabin, developer of Polio vaccine
"All vaccination has the effect of directing the three valuesof the blood into or toward the zone characteristics of can-cer and leukaemia...Vaccines do predispose to cancer andleukaemia."
– Professor L.Vincent - founder of Bioelectronics
"Many here voice a silent view that the Salk and Sabin PolioVaccines, being made from monkey kidney tissue, hasbeen directly responsible for the major increase inleukaemia in this country."
– Dr F. Klenner, M.D.
"Even to this day, the government, the FDA is refusing touse the sophisticated biotechnology to evaluate the con-taminants in the vaccines such as the polio vaccines thatthey are administering. I think (people) would be appalledthat some of the vaccines that are currently being used arestill laced with viruses."
– Leonard Horowitz., D.M.D., M.A., M.P.H.
WHAT YOUR DOCTOR WILL NEVERTELL YOU is published 4 times a year (orsometimes less frequently) by The Full CourtPress. Subscriptions are $29.95 (as a dona-tion/koha) for 10 issues. If you are unable topay, please let us know.
Editors: Katherine Joyce Smith andJonathan Eisen
Mailing address:
The Full Court PressPO Box 44-128AucklandNew Zealand