Embed Size (px)
Citation preview
New users of benzodiazepines: implications for elder patient safety
G. Bartlett, PhDFamily MedicineMcGill University
Outline
Benzodiazepine use in the elderly Objectives of study Methods Population & data sources Results – new users vs non-users Results – predictors of new use Conclusions, Limitations Future Directions
Benzodiazepines - review
Sedative/hypnotics:
hypnotic, anxiolytic, anticonvulsant, muscular relaxant, amnesic
high efficacy, rapid onset of action, low toxicity
unique among psychotropics for multiple indications and relative safety compared with other sedative/hypnotics
Concerns about Benzodiazepines
psychomotor impairment
paradoxical excitement
tolerance, dependence and withdrawal effects with long term use
injuries from falls
Concerns about Benzodiazepinesfor the Elderly
Due to changes that occur with normal aging, elderly demonstrate increased sensitivity to:
psychomotor impairment memory impairment rebound or withdrawal effects interactions with other
medications/conditions

Use of Benzodiazepines:Why the Elderly?
insomnia can be a “pathological” feature associated with age
anxiety due to other illnesses more likely to suffer acute grief
reactions fewer complications with
benzodiazepines than with tricyclic anti-depressants and anti-psychotics
Risk from injuries from falls for benzodiazepines still in dispute
Physicians may be prescribing benzodiazepines perceived to be safer to higher risk patients
Pre-existing risk factors may be cause confounding in published studies
What risk factors for falls are present before a benzodiazepine is prescribed?
Why are we still discussing benzodiazepine safety?
Methods
All patients >65 years with no benzodiazepine script in baseline year
Risk factors for falls assessed in baseline year: age & sex clinical characteristics disabilities & impairments prior hospitalizations prior health care use use of other prescription medication.
5 years of follow-up until first benzodiazepine script dispensed – product name identified

Benzodiazepines available in QC
Triazolam (Halcion) Midazolam (Versed) – IV only Alprazolam (Xanax) Bromazepam (Lectopam) Lorazepam (Ativan) Oxazepam (Serax) Nitrazepam (Mogadon) Temazepam (Restoril) Clobazam (Frisium) Clonazepam (Rivotril) Diazepam (Valium) Flurazepam (Dalmane) Chlordiazepoxide (Librium) Clorazepate* (Traxene)
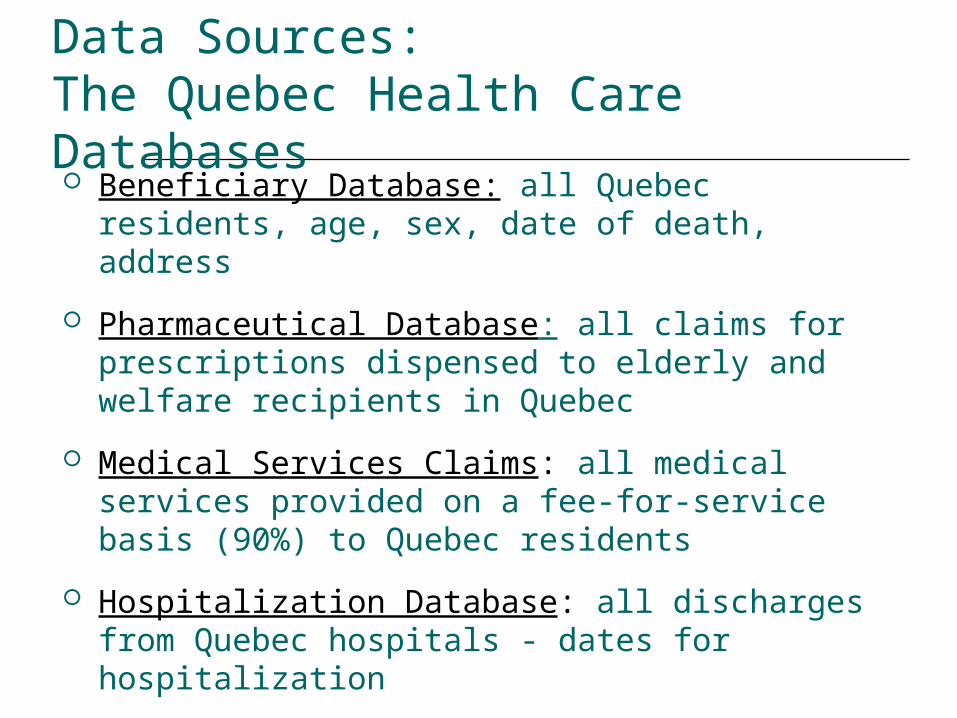
Data Sources: The Quebec Health Care Databases Beneficiary Database: all Quebec residents, age,
sex, date of death, address
Pharmaceutical Database: all claims for prescriptions dispensed to elderly and welfare recipients in Quebec
Medical Services Claims: all medical services provided on a fee-for-service basis (90%) to Quebec residents
Hospitalization Database: all discharges from Quebec hospitals - dates for hospitalization
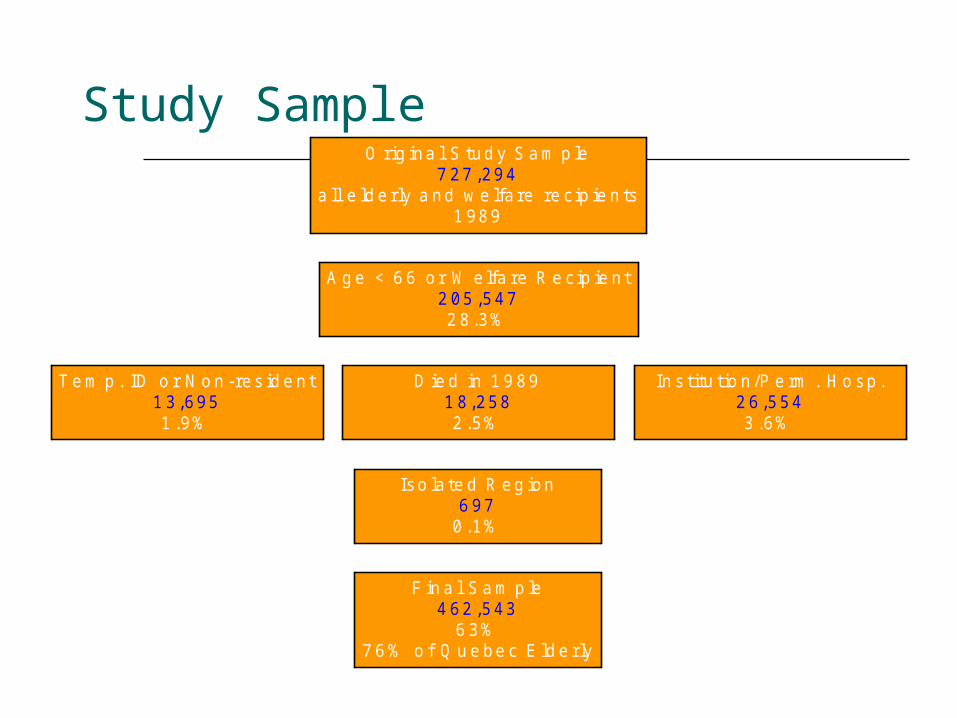
Study Sample
T e m p . ID o r N o n -res id e n t1 3 ,6951 .9%
F in a l S a m p le4 62 ,543
6 3%7 6 % o f Q u e be c E ld e rly
Iso la te d R eg ion6 97
0 .1%
D ie d in 1 9 891 8,2582 .5%
In s titu t io n /P e rm . H o sp .2 6 ,5543 .6%
A g e < 6 6 o r W e lfa re R e cip ie n t2 05 ,5472 8.3%
O rig ina l S tud y S a m p le7 27 ,294
a ll e ld erly a nd w e lfa re re cip ie n ts1 989
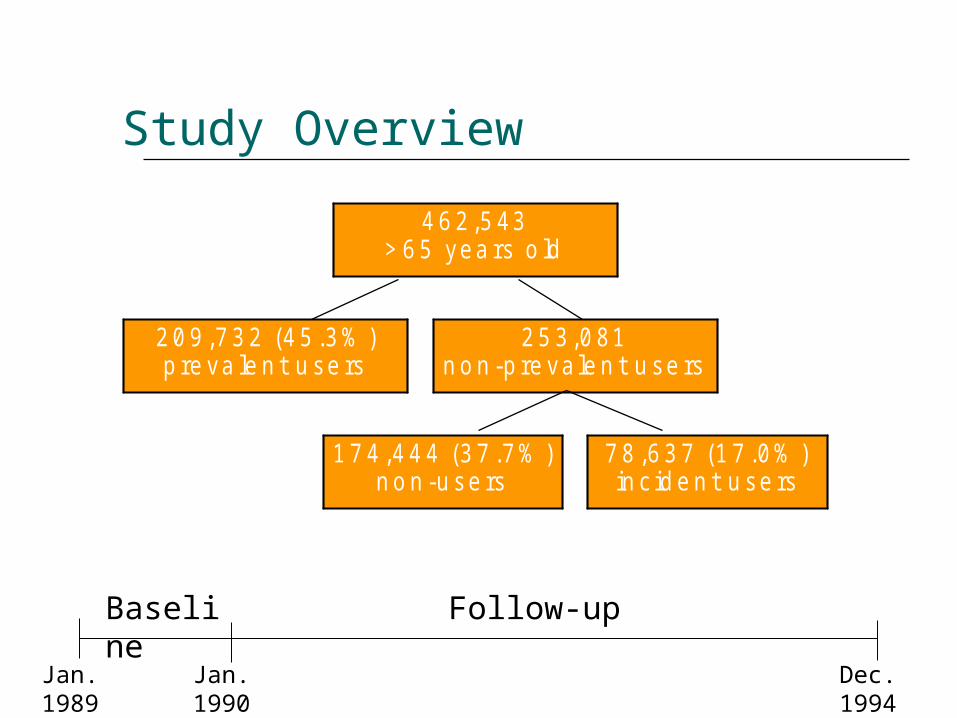
Study Overview
2 0 9 ,7 3 2 (4 5 .3 % )p re va le n t u se rs
1 7 4 ,4 4 4 (3 7 .7 % )n o n -u se rs
7 8 ,6 3 7 (1 7 .0 % )in c id e n t u se rs
2 5 3 ,0 81n o n -p re va le n t u se rs
4 6 2 ,5 43> 6 5 yea rs o ld
Jan. 1989 Jan. 1990 Dec. 1994
Baseline Follow-up
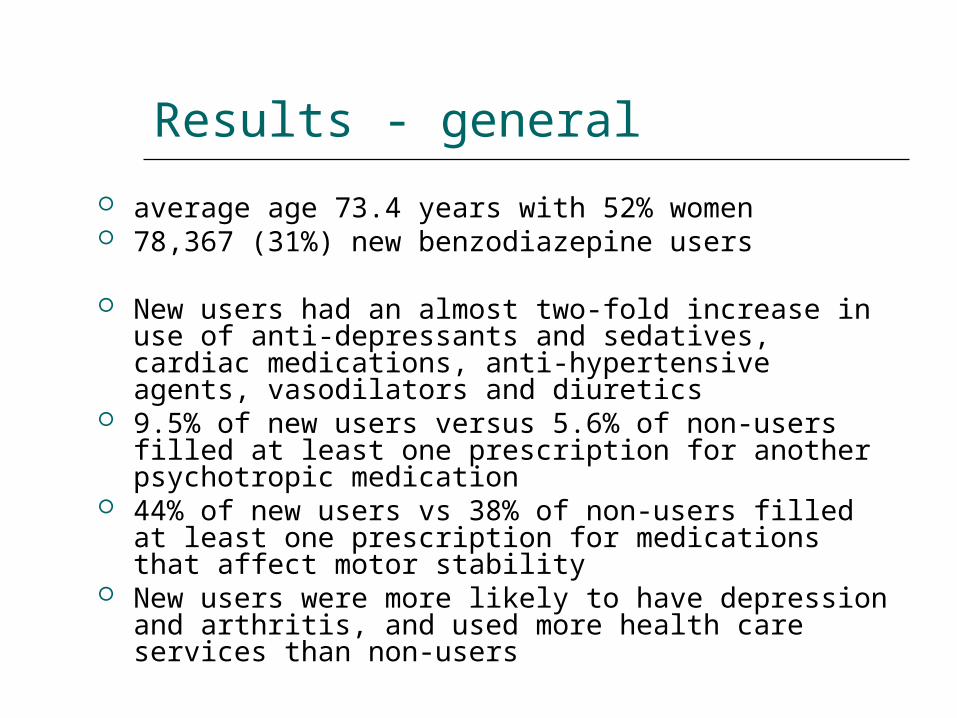
Results - general
average age 73.4 years with 52% women 78,367 (31%) new benzodiazepine users
New users had an almost two-fold increase in use of anti-depressants and sedatives, cardiac medications, anti-hypertensive agents, vasodilators and diuretics
9.5% of new users versus 5.6% of non-users filled at least one prescription for another psychotropic medication
44% of new users vs 38% of non-users filled at least one prescription for medications that affect motor stability
New users were more likely to have depression and arthritis, and used more health care services than non-users
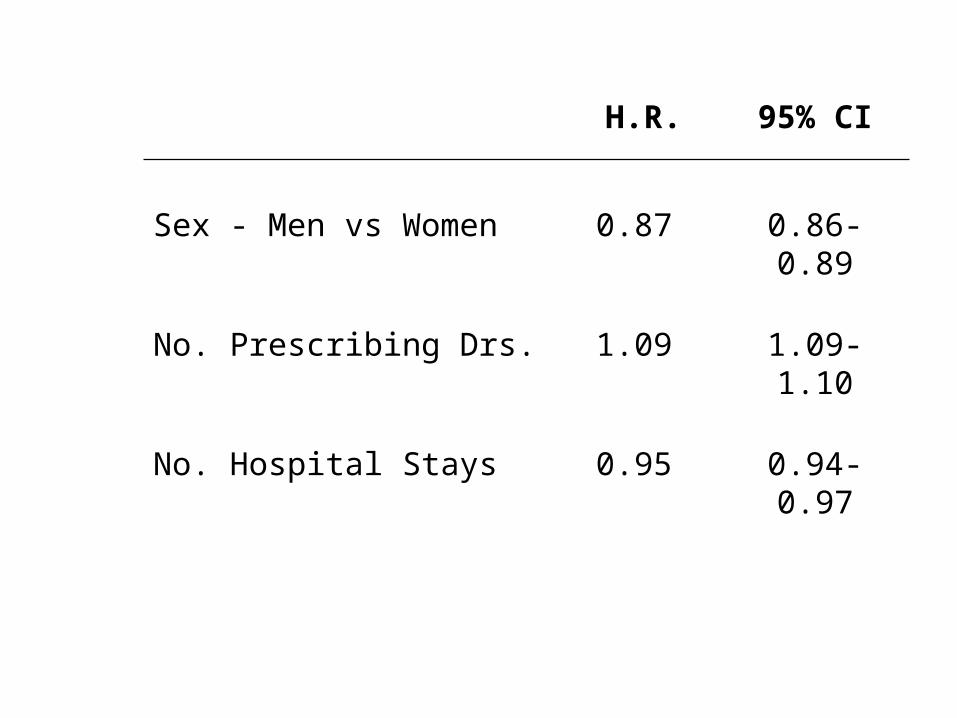
H.R. 95% CI
Sex - Men vs Women 0.87 0.86-0.89
No. Prescribing Drs. 1.09 1.09-1.10
No. Hospital Stays 0.95 0.94-0.97
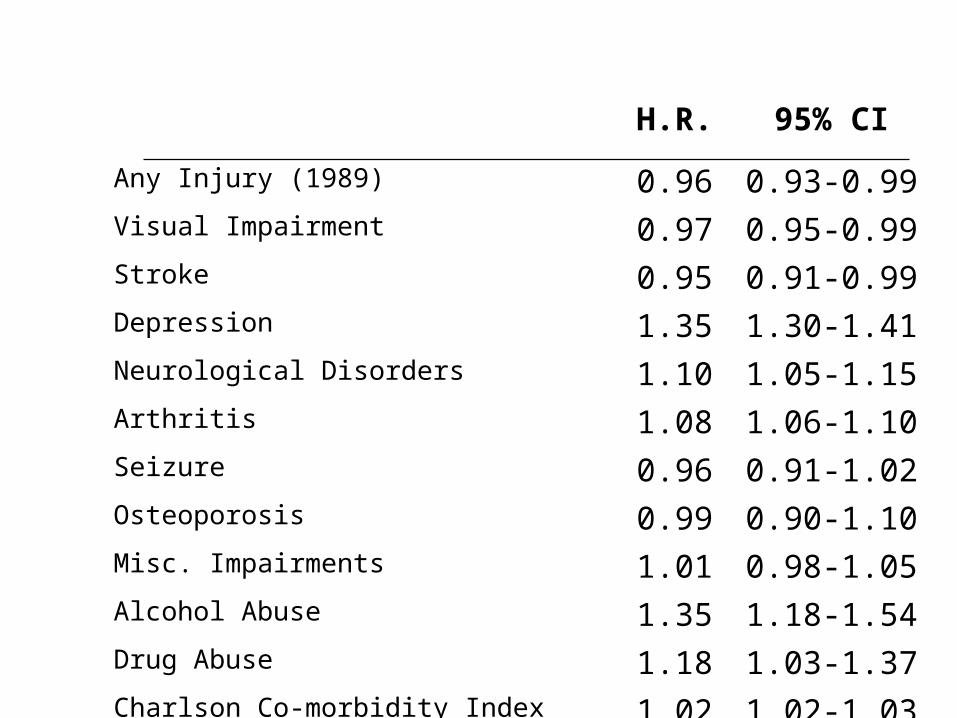
H.R. 95% CI
Any Injury (1989) 0.96 0.93-0.99Visual Impairment 0.97 0.95-0.99Stroke 0.95 0.91-0.99Depression 1.35 1.30-1.41Neurological Disorders 1.10 1.05-1.15Arthritis 1.08 1.06-1.10Seizure 0.96 0.91-1.02Osteoporosis 0.99 0.90-1.10Misc. Impairments 1.01 0.98-1.05Alcohol Abuse 1.35 1.18-1.54Drug Abuse 1.18 1.03-1.37Charlson Co-morbidity Index 1.02 1.02-1.03
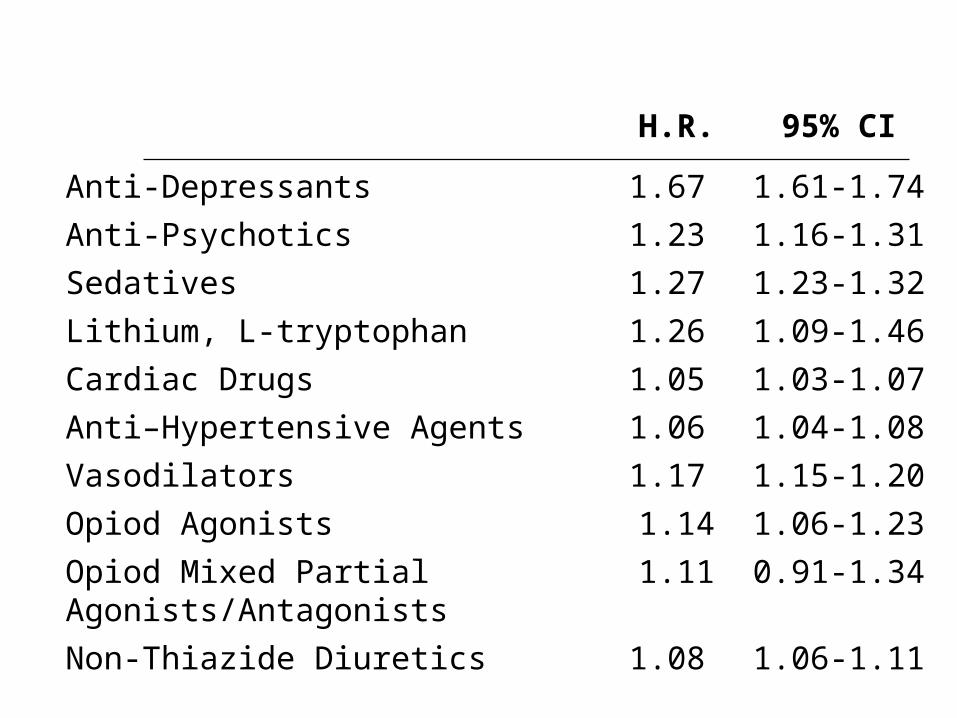
H.R. 95% CI
Anti-Depressants 1.67 1.61-1.74
Anti-Psychotics 1.23 1.16-1.31
Sedatives 1.27 1.23-1.32
Lithium, L-tryptophan 1.26 1.09-1.46
Cardiac Drugs 1.05 1.03-1.07
Anti–Hypertensive Agents 1.06 1.04-1.08
Vasodilators 1.17 1.15-1.20
Opiod Agonists 1.14 1.06-1.23
Opiod Mixed Partial Agonists/Antagonists
1.11 0.91-1.34
Non-Thiazide Diuretics 1.08 1.06-1.11
Results – product specific
decreased risk of starting oxazepam and flurazepam for older ages
women were more to be new users of the majority of the benzodiazepines except temazepam and flurazepam
each additional prescribing physician seen increased by risk of new use by 5-15%
having an fall injury decreased risk for lorazepam (HR=0.93, p=0.01) and diazepam (HR=0.86, p=0.04) and an increased probability for chlordiazepoxide (HR=1.34, p=0.04)
Results – disabilities and impairments depression was strongly associated with new use
except triazolam and temazepam -particularly strong for alprazolam (HR=1.98, p<0.0001) and clonazepam (HR=2.46, p<0.0001)
weaker but consistently positive increased risk for arthritis
neurological disorders (including dementia and Parkinson’s disease) and clonazepam (HR=2.24, p<0.0001);
alcohol abuse and both oxazepam (HR=1.55 p=0.001) and chlordiazepoxide (HR=12.1, p<0.0001)
drug abuse with bromazepam (HR=2.34, p=0.0008).
Results – disabilities and impairments strongest and most consistent associations
were seen for use of anti-depressants as well as other psychotropic medications (anti-psychotics and non-benzodiazepine sedatives, lithium or l-tryptophan)
filling a prescription for an anti-depressant significantly increased risk varying from a 23% increase for diazepam (HR=1.23) to more than tripling the hazard for clonazepam (HR=3.13)
use of anti-psychotics, other sedatives, and lithium or l-tryptophan increased risk by more than double for new clonazepam and flurazepam use and over five times for clonazepam (HR=5.19, p<0.0001).

Conclusions
Factors associated with new benzodiazepine use vary considerably among the individual products
Physicians appear to be “channeling” new users based on own criteria – not necessarily evidence based
Any research on risk needs to account for these factors by individual products
Limitations
under-diagnosis and under-reporting of the treatment of certain diseases
anxiety and insomnia were often not coded in the database making it difficult to assess the association between these diagnoses and benzodiazepine use
proxy measure of use (dispensed prescription)
no prescription information available during hospitalization

Future Directions
Why benzodiazepines are chosen by physicians – are other risk factors accounted for?
Role of risk in guidelines recommendations…
Methods to reduce risk of falls – smart alerts?
Investigations of risk from falls – are other risk factors accounted for?
Is dose adjusted for in high risk patients?







![Analytical methods for determination of benzodiazepines. A ... · receptor (BZ receptor), because it can affect the ability to bind benzodiazepines [5,13,14]. Benzodiazepines act](https://img.pdfslide.us/doc/110x75/5e14ec7c8625516a950995fb/analytical-methods-for-determination-of-benzodiazepines-a-receptor-bz-receptor.jpg)