Embed Size (px)
Citation preview
New (U.S.) Lipid Guidelines (The Good and Bad)
Robert A. Vogel, MDClinical Professor of MedicineUniversity of Colorado Denver
Disclosures: National Coordinator ODYSSEY Trial (Sanofi)

ATP-3 ATP-4
Patient Risk
Lipid Profile
Meds to improve lipid profile,
Lifestyle
Patient Risk
Statins, Lifestyle
RCTs
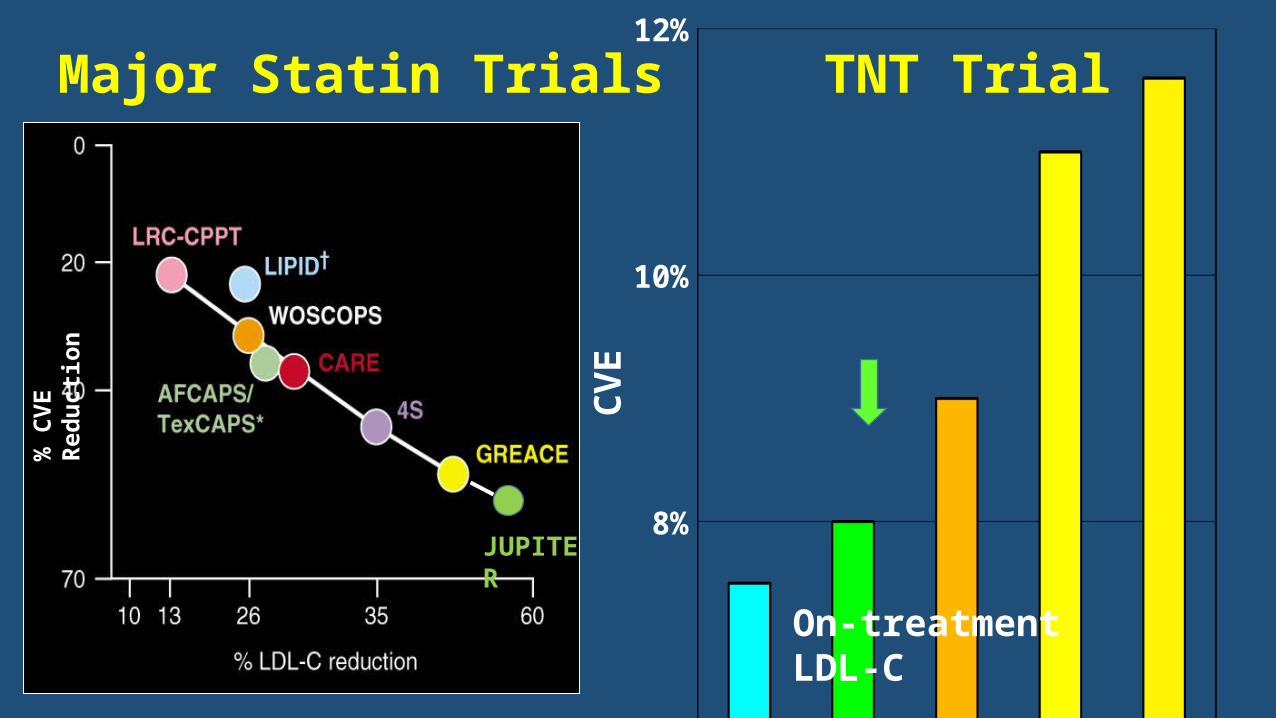
Major Statin Trials TNT Trial
54 70 83 97 1226%
8%
10%
12%
CVE
On-treatment LDL-C
JUPITER
% C
VE R
educ
tion

Dal-Outcomes: Incidence of the Primary End Point (CHD Death, Nonfatal MI, USA, Cardiac Arrest)
Schwartz GG et al. N Engl J Med 2012. DOI: 10.1056/NEJMoa1206797
Years
Prim
ary
End
Poin
t (%
)
HDL-C: ↑33%, LDL-C: no ∆
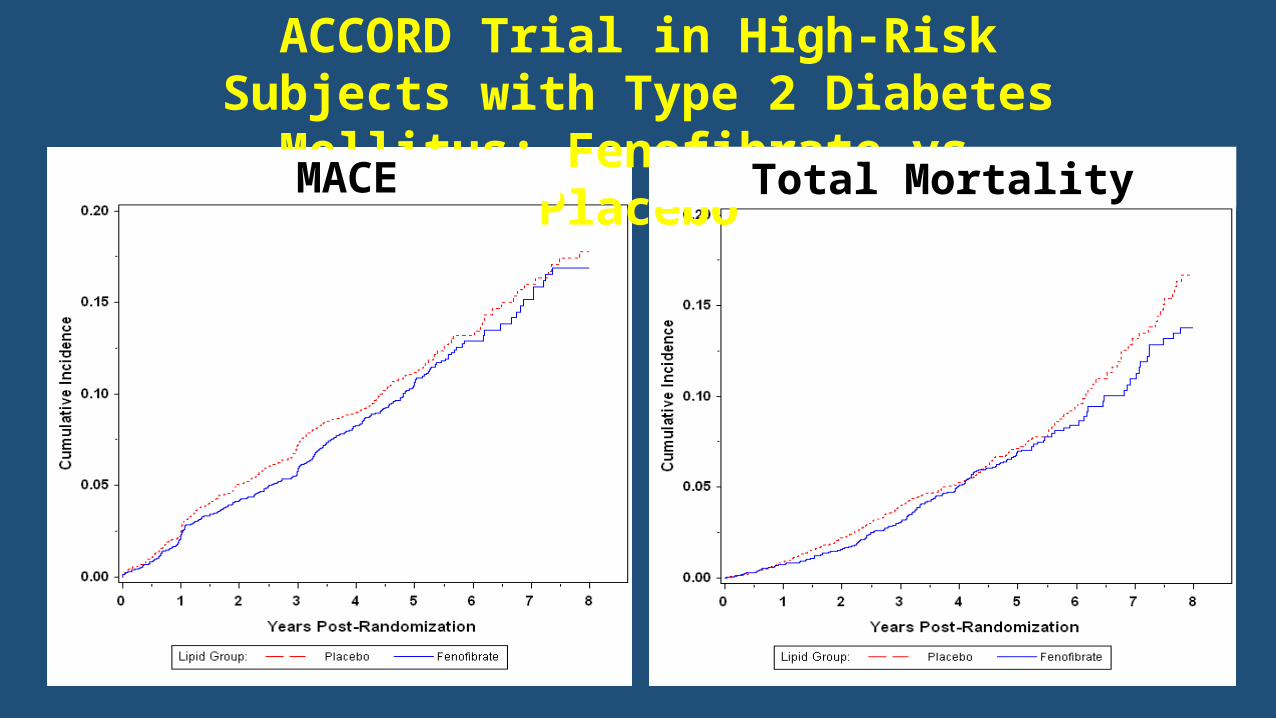
ACCORD Trial in High-Risk Subjects with Type 2 Diabetes Mellitus: Fenofibrate vs. Placebo
MACE Total Mortality
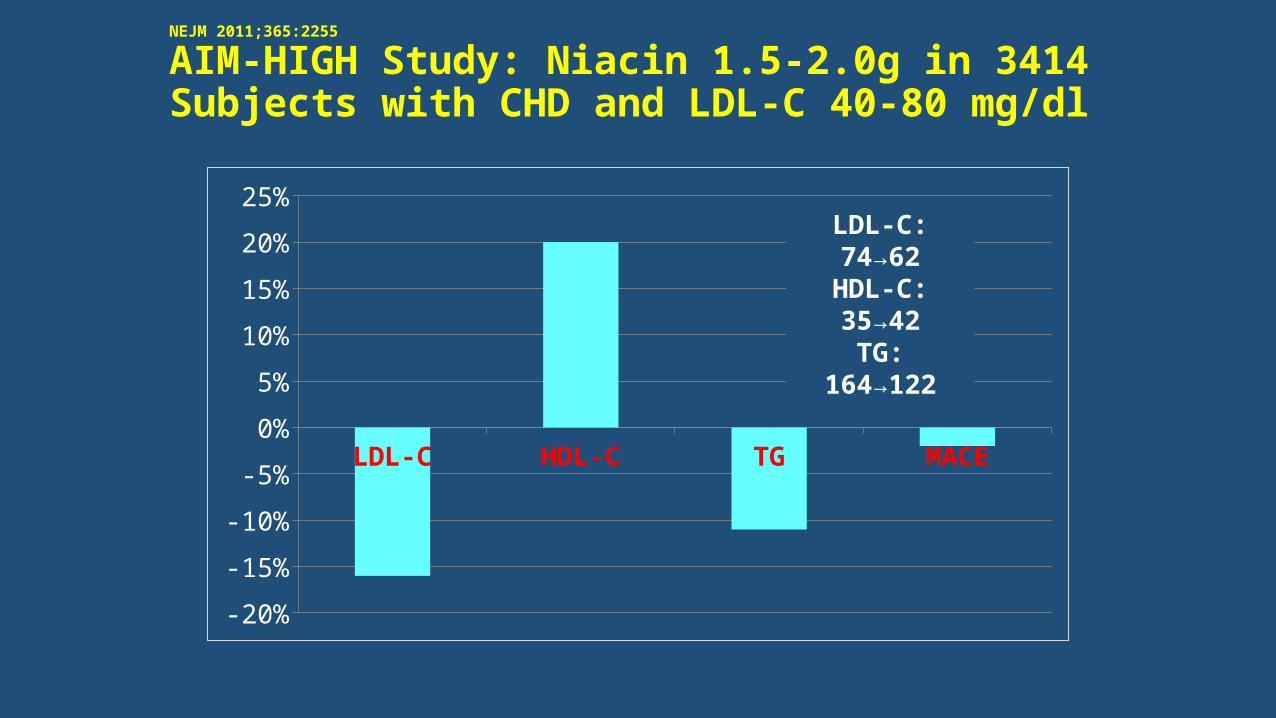
NEJM 2011;365:2255
AIM-HIGH Study: Niacin 1.5-2.0g in 3414 Subjects with CHD and LDL-C 40-80 mg/dl
LDL-C HDL-C TG MACE
-20%
-15%
-10%
-5%
0%
5%
10%
15%
20%
25%LDL-C: 74→62HDL-C: 35→42TG: 164→122
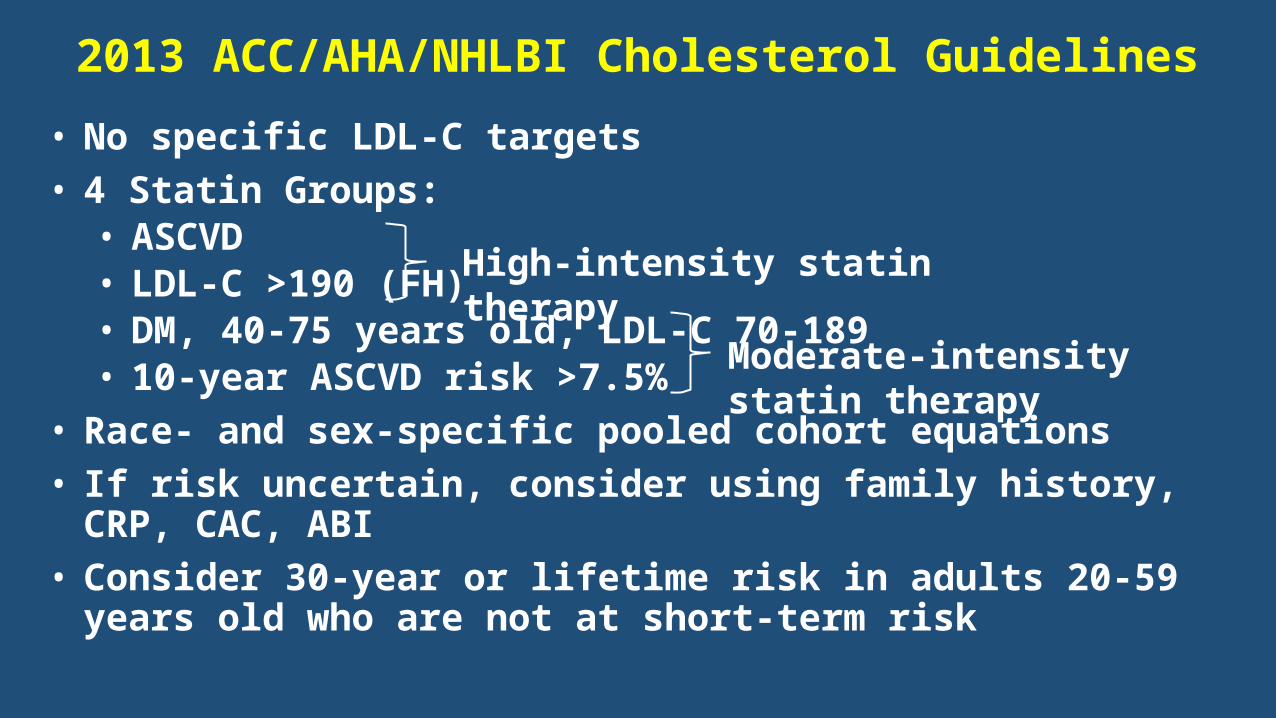
2013 ACC/AHA/NHLBI Cholesterol Guidelines• No specific LDL-C targets• 4 Statin Groups:• ASCVD• LDL-C >190 (FH)• DM, 40-75 years old, LDL-C 70-189• 10-year ASCVD risk >7.5%
• Race- and sex-specific pooled cohort equations• If risk uncertain, consider using family history, CRP, CAC, ABI• Consider 30-year or lifetime risk in adults 20-59 years old who are not at
short-term risk
High-intensity statin therapy
Moderate-intensity statin therapy
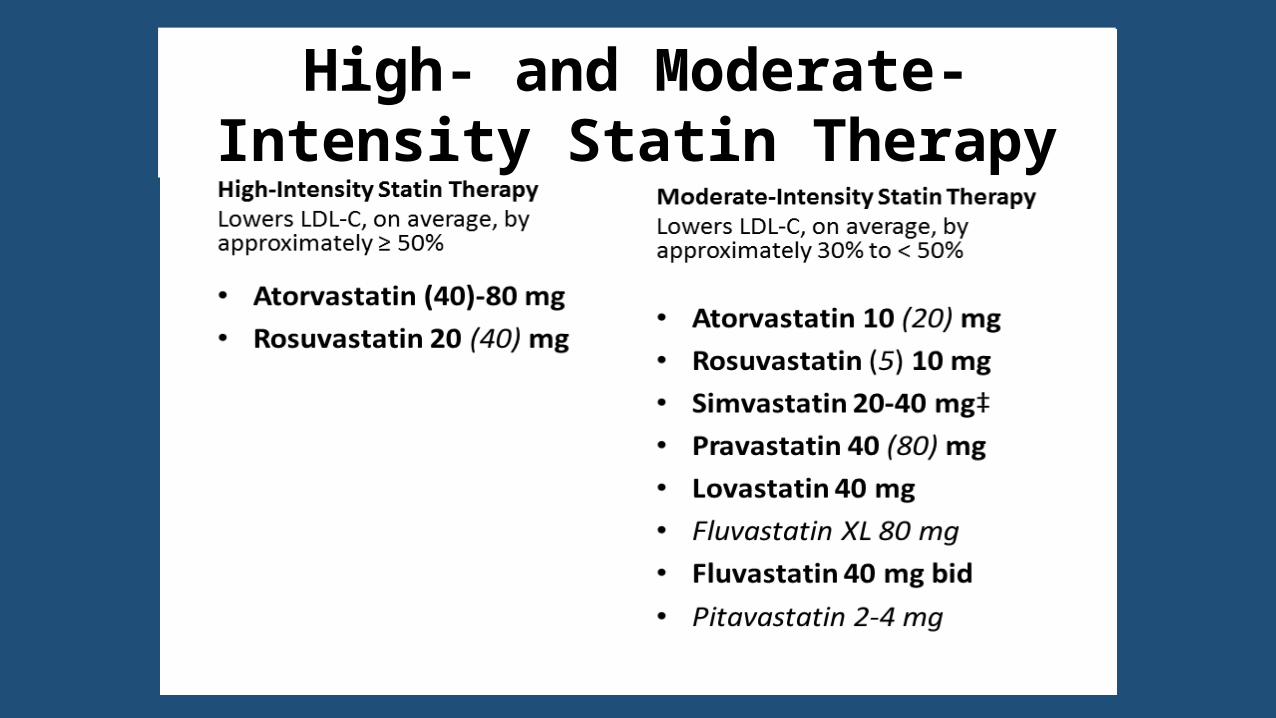
High- and Moderate-Intensity Statin Therapy

Q: Why have the guidelines been changed?
A: Because the data don’t support LDL-C treatment goals.
Q: How do you judge treatment if you don’t consider on-treatment LDL-C?
A: By statin usage and dose

Pooled Cohort Equation vs. FRS 10-Year CHD/ASCVD Event Rates for a nonsmoking, non diabetic, non
hypertensive male with TC 200 mg/dl, HDL 45 mg/dl, and SBP 130 mmHg
Age 40 Age 50 Age 60 Age 700%2%4%6%8%
10%12%14%16%18%20%
PCE ASCVD Risk FRS CHD Risk
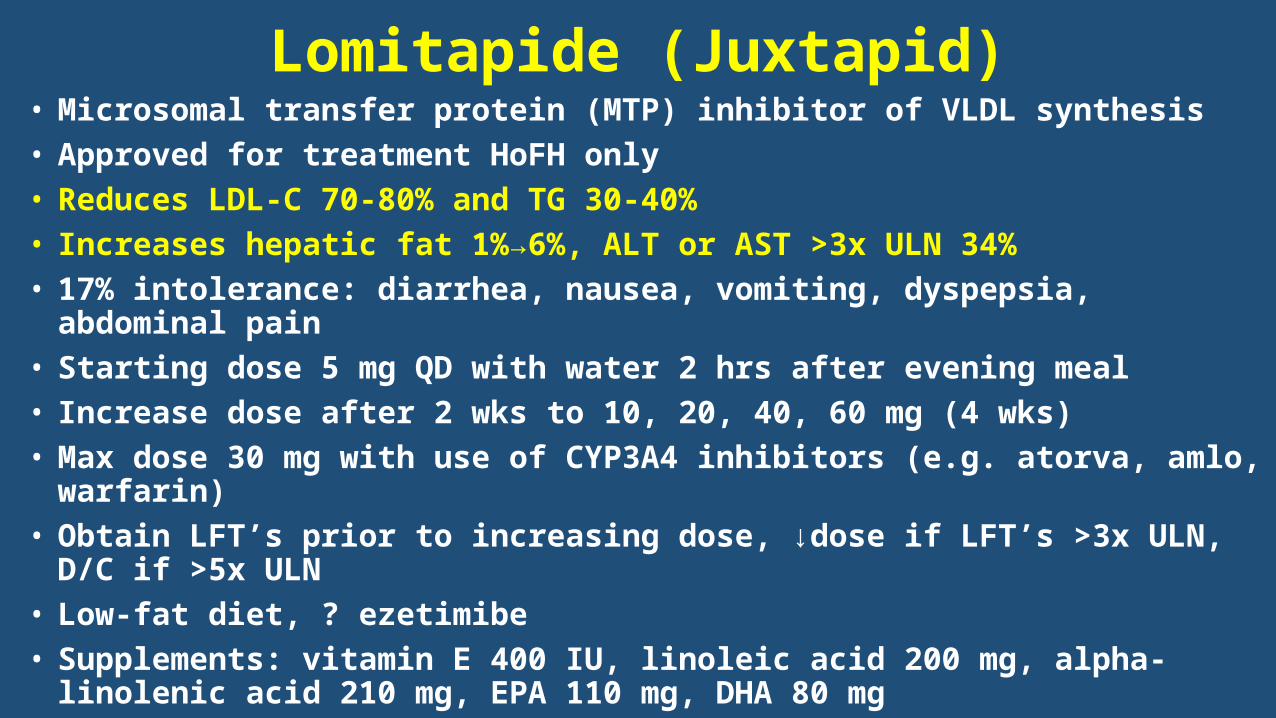
Lomitapide (Juxtapid)• Microsomal transfer protein (MTP) inhibitor of VLDL synthesis• Approved for treatment HoFH only• Reduces LDL-C 70-80% and TG 30-40%• Increases hepatic fat 1%→6%, ALT or AST >3x ULN 34%• 17% intolerance: diarrhea, nausea, vomiting, dyspepsia, abdominal pain• Starting dose 5 mg QD with water 2 hrs after evening meal• Increase dose after 2 wks to 10, 20, 40, 60 mg (4 wks)• Max dose 30 mg with use of CYP3A4 inhibitors (e.g. atorva, amlo, warfarin) • Obtain LFT’s prior to increasing dose, ↓dose if LFT’s >3x ULN, D/C if >5x ULN• Low-fat diet, ? ezetimibe• Supplements: vitamin E 400 IU, linoleic acid 200 mg, alpha-linolenic acid 210
mg, EPA 110 mg, DHA 80 mg

Mipomersen (Kynamro)• Antisense oligonuclide (ASO) to ApoB messenger RNA• Approved for treatment HoFH only• Weekly 200mg S.C. injections• Reduces LDL-C 25 – 65%, Lp(a) 25%• Increases hepatic fat: 12% LFT’s >3x ULN, 3% >5x ULN
(LFT monitoring required)• 84% injection site reactions, 30% flu-like symptoms 2 days
post injection

13
13
LDL-R Synthesis, Cycling, and Degradation
Degradation of LDL-R
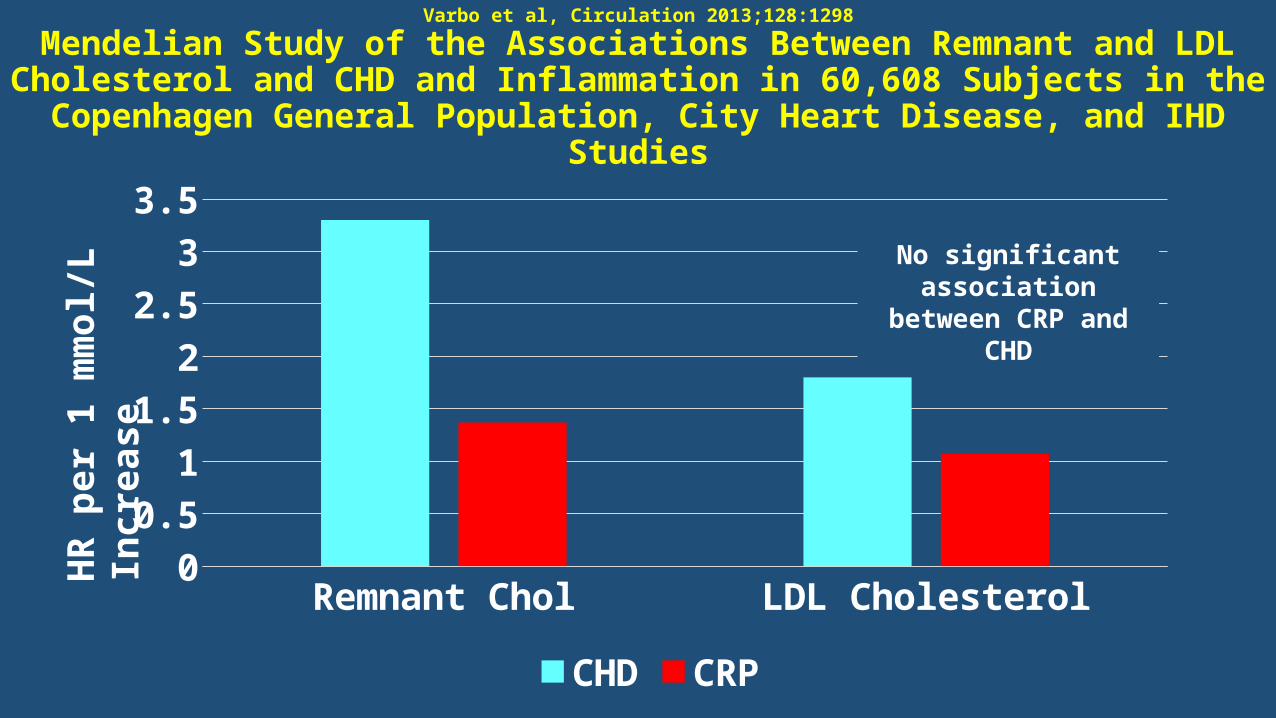
Varbo et al, Circulation 2013;128:1298
Mendelian Study of the Associations Between Remnant and LDL Cholesterol and CHD and Inflammation in 60,608 Subjects in the
Copenhagen General Population, City Heart Disease, and IHD Studies
Remnant Chol LDL Cholesterol0
0.5
1
1.5
2
2.5
3
3.5
CHD CRP
HR
per 1
mm
ol/L
Incr
ease
No significant association between CRP and CHD

2014 Lipid Management
• Evaluate disease not lipid profile risk
• Use statins at evidence-based dosage
• Lifestyle is important
• PCSK9 and Apo C-III inhibitors are promising