Embed Size (px)
Citation preview

Review
10.1517/17460440802105938 © 2008 Informa UK Ltd ISSN 1746-0441 565
New tuberculosis drug development: targeting the shikimate pathway Senta M Kapnick & Ying Zhang † Johns Hopkins University, Department of Molecular Microbiology & Immunology, Bloomberg School of Public Health, Baltimore, MD 21205, USA
Background : Tuberculosis (TB) remains a leading cause of morbidity and mortality worldwide, yet no new drugs have been developed in the last 40 years. Objective : The exceedingly lengthy TB chemotherapy and the increasing emergence of drug resistance complicated by HIV co-infection call for the development of new TB drugs. These problems are further compounded by a poor understanding of the biology of persister bacteria. Methods : New molecular tools have offered insights into potential new drug targets, particularly the enzymes of the shikimate pathway, which is the focus of this review. Results/conclusion : Shikimate pathway enzymes, especially shikimate kinase, may offer attractive targets for new TB drug and vaccine development.
Keywords: drug development , Mycobacterium tuberculosis , shikimate kinase , shikimate pathway
Expert Opin. Drug Discov. (2008) 3(5):565-577
1. Introduction
Tuberculosis (TB) is a disease whose history is intimately intertwined with that of humans. The relationship between the two represents the ultimate infectious disease encounter and subsequent attempts at control and eventual elimination. At one time, TB killed more people than any other disease [1] , shaping human history by its ability to infiltrate any home and every life. In the late 17th century, John Bunyan wrote in his book, The Life and Death of Mr. Badman : “The captain of all these men of death that came against him to take him away, was the Consumption, for it was that that brought him down to his grave” [2] . Although TB has acquired many names over centuries of human coexistence – Consumption, the White Plague, phthisis, and Wasting Disease to name a few, its persistence as one of the great pandemics is reflected by the fact that among the numerous infectious diseases caused by bacterial pathogens today, TB remains the leading cause of morbidity and mortality worldwide with nearly 2 million deaths each year [3] . It is estimated that 2 billion people are latently infected with the Mycobacterium tuberculosis bacillus, the etiologic agent of tuberculosis, and 1 in 10 of those people will develop active disease in their lifetime. With 8.8 million new cases in 2005 [3] , TB maintains a stronghold on its pandemic status.
The steady increase in TB prevalence rates and the emergence of drug-resistant strains emphasizes the urgent need for new drugs effective in treating the disease in the context of a new epidemiology that is at least partially a reflection of HIV co-infection, drug resistance, immigration, and globalization. It is estimated that 40 million people worldwide are infected with HIV, and approximately one-third of those individuals are co-infected with the tubercle bacillus [4] . Mortality rates in these HIV–TB co-infected individuals are estimated to be five times higher than those with TB infection alone [5-7] . HIV–TB co-infection also presents new problems for management of pharmacologic interactions, as
1. Introduction
2. TB chemotherapy
3. The problem of persisters
4. Current TB drug targets
5. The shikimate pathway
6. Shikimate kinase
7. Drug development based on
the shikimate pathway
8. Vaccine development based on
the shikimate pathway
9. Expert opinion
Exp
ert O
pin.
Dru
g D
isco
v. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
S.A
Lib
119
257
on 1
0/24
/12
For
pers
onal
use
onl
y.

New tuberculosis drug development: targeting the shikimate pathway
566 Expert Opin. Drug Discov. (2008) 3(5)
those with active TB and HIV are at increased risk for developing drug resistance [8,9] . In addition, the weakened immune system of HIV-infected individuals allows for reactivation of latent TB infection and/or re-infection [10] , sometimes increasing the risk of TB by 100-fold [11,12] .
The emergence of drug-resistant strains also represents a significant hurdle for TB control and elimination goals. Although improved sanitation and the use of the Bacillus Calmette-Guerin vaccine initially lowered TB rates through-out the world [10] , these techniques are no longer staving off the disease. Significant drug resistance has developed in a very short period of time. In every country surveyed by the World Health Organization (WHO), strains resistant to at least one drug were found, and WHO estimates that there are ∼ 450,000 new cases of multi-drug-resistant (MDR) TB every year [13] . MDR TB is defined as resistance to at least isoniazid (INH) and rifampin (RIF), and requires extensive, expensive, chemotherapy for up to 2 years with second-line drugs [3] . The rapidly rising prevalence of extensively drug-resistant (XDR) TB, representing a virtually untreatable disease, only compounds the problem. XDR TB is defined as resistance to INH and RIF plus resistance to two main second-line drugs, a fluoroquinolone and any one of the aminoglycosides (capreomycin, amikacin, kanamycin) [3] . However, TB drug resistance and current limitations in susceptibility testing are not all that render MDR/XDR TB an increasing threat. In certain subgroups, accelerated progression of the disease is being observed. Investigations by the Centers for Disease Control and Prevention (CDC) between 1988 and 1992 found a dramatic shortening of the median weeks from diagnosis to death among co-infected HIV–MDR TB patients [14] . The more recent XDR TB outbreak in South Africa, in which 52 of 53 HIV–TB co-infected individuals died within 16 days [15] , further emphasizes the dire need for new antitubercular drugs.
2. TB chemotherapy
2.1 Brief history of TB chemotherapy Sixty years ago there were no drugs to cure TB, and no new drugs have been developed in the last 40 years [16] . The history of TB chemotherapy began in 1943, when Schatz and Waksman isolated streptomycin (SM), the first effective TB drug [17] . Soon after, the British Medical Research Council performed the first ever randomized clinical trial proving the drug’s efficacy [18] but resistance to SM was quickly observed [19] . It was later found that addition of para-aminosalicylic acid (PAS) to SM prevented drug resistance, thus establishing the important principle of drug combination that today forms the basis for the treatment of not only TB but also other infectious diseases such as HIV–HAART and even cancer. The addition of INH to the SM/PAS regimen in the 1950s was found to effectively cure TB patients in 18 – 24 months. The discovery of RIF in the 1960s and its subsequent use in combination
with INH further shortened treatment to 9 months [18] . In the 1970s and 1980s, reevaluation of pyrazinamide (PZA) in combination with INH and RIF led to the current 6 month TB chemotherapy. Since 1991, directly observed therapy – short course (DOTS) has been the recommended standard TB chemotherapy by WHO. DOTS requires 6 months to complete, consisting of a 2-month initial phase of daily administration of INH, RIF, PZA, and ethambutol (EMB), followed by the continuation phase of 4 months of INH and RIF. DOTS has a cure rate up to 95% and is extremely cost-effective [3] . However, MDR TB strains are posing significant problems for this current treatment regimen. DOTS-plus, a treatment regimen designed for MDR TB patients involving the addition of second-line drugs to the standard DOTS program, is extremely expensive and can last for up to 2 years [13] , in addition to having significant toxic side effects [20] .
2.2 Problems with current TB therapy DOTS therapy is lengthy and toxic, and therefore the development of secondary drug resistance is at least partially owing to poor patient compliance. Significant side effects include hepatitis, dyspepsia, arthralgia, and exanthema [21] . The impact of these side effects is responsible for patient-initiated treatment termination in ∼ 23% of cases [20] . Drug combination therapy is vital for the prevention of drug resistance; nonetheless, the lengthy regimen is increasing noncompliance and subsequent drug resistance development. Clearly, the problem lies not in the treatment principle but in the drugs themselves. TB therapy is exceptionally long when compared with other bacterial infection treatment regimens, most of which are cured with a maximum of 14 days of antibiotic treatment [22] . Chlamydia infections are cured with one pill, and pneumococcal infections in 1 week. M. tuberculosis represents an anomaly with regard to treatment. The problem of lengthy TB treatment is thought to be owing to phenotypic resistance or tolerance, a mechanism not unique to M. tuberculosis [23,24] , present in persister bacteria formed in response to environmental stresses as in stationary phase, dormant state, and biofilms [25] . With the exception of RIF and PZA, which only kill a portion of persister bacilli, current antitubercular drugs are mainly effective against actively growing bacilli populations [26] . This lack of effective drugs active for dormant or persister populations represents a major problem in TB treatment.
3. The problem of persisters
3.1 The need for lengthy therapy 3.1.1 The Mitchison hypothesis The Mitchison hypothesis describes four bacterial popula-tions and can partially explain the current need for lengthy combination therapy. The first population is actively growing and is killed by INH, RIF, SM, and EMB.
Exp
ert O
pin.
Dru
g D
isco
v. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
S.A
Lib
119
257
on 1
0/24
/12
For
pers
onal
use
onl
y.

Kapnick & Zhang
Expert Opin. Drug Discov. (2008) 3(5) 567
Semi-dormant populations consist of two subpopulations: those undergoing spurts of metabolism targeted by RIF and those in an acid environment targeted by PZA. The use of PZA to target semi-dormant populations not killed by other antitubercular drugs shortens TB therapy from 9 months to 6 months. The fourth and final population described by the Mitchison hypothesis is the dormant bacterial population. No drugs target this population and herein lies the problem with current TB drugs [26] .
3.1.2 The Yin and Yang model A second and more recent model, the Yin and Yang model [27] , describes the mycobacterial life cycle and the effects of traditional and more recent drugs on the mixed populations. This model depicts a more dynamic bacterial population consisting of growing and nongrowing subpopulations in a range of varying metabolic states and continuously changing. In the growing populations (Yang), there is a small proportion of slow-growing bacteria known as persisters (Yin). The active growers are effectively killed or inhibited by INH, RIF, EMB, and SM. As the actively growing population enters the stationary phase, they become the minority in the population as more and more persisters form. In the Yin and Yang model, the persister population is also composed of various subpopulations in flux. In addition to killing active growers, RIF, moxifloxacin, gatifloxacin, and diarylquinoline R207910 (J compound) also kill a portion of these persister subpopulations, whereas other persisters in acidic pH are killed by PZA. Still, upon removal of anti-biotics, other persister subpopulations not killed by current antitubercular drugs can revert to active growers. These are known as reverters, and can once again become susceptible to INH and RIF in their active states during the continuation phase of treatment. The Yin and Yang model helps explain the current continued need for 6-month therapy regimens – after a 2-month treatment with INH, RIF, EMB, and PZA, some of the persisters revert to growing forms and thus can be killed by INH and RIF in the subsequent 4 months of treatment [27] . This model, which addresses dynamic subpopulations, helps to explain the need for such lengthy treatment and may have implications for developing more effective treatment strategies.
3.2 Classes of persisters The value of further understanding the persister switch cannot be emphasized enough because the phenotypic resistance of nonreplicating persisters represents the major problem for current TB therapy. Persisters were first studied in staphylococcal bacteria [28] , and although recently there is considerable research being performed in this area [29-32] , little is currently known about the mechanisms of M. tuberculosis persistence. However, two classes of persisters have been proposed [31] . Type I persisters appear to emerge slowly nearing the end of the stationary phase of bacterial growth. Type II persisters appear to undergo a
reversible metabolic switch, allowing them to materialize spontaneously [33] . This switch between normal and type II persister cells is observed under conditions of environmental change, such as stress or the presence of antibiotics, thus potentially conferring a selective advantage [25] . In addition, persister states may have increased occurrence among specific antibiotics, as has been observed in Escherichia coli populations when a β -lactam antibiotic or genetic mutation-induced SOS response has the potential to stop bacterial cell division [30] . Thus, the antibiotic can potentially become an extracellular stimulus facilitating bacterial survival. When antibiotics have already unsuccessful bactericidal or bacteriostatic effects against persister populations, as is the case with current TB drugs, persister switches may be further favored [31] .
3.3 Persister switch mechanisms 3.3.1 Toxin–antitoxin modules The mechanism governing this persister switch is still not understood. However, it has been suggested that the frequency of this switch may be partially controlled by the expression of toxins [34,35] . Toxin–antitoxin (TA) modules, originally described as factors ensuring episomal stability [36] , have been identified among the genes induced in persister populations [37] . The toxins inhibit transcription and trans-lation by several mechanisms, and are neutralized by labile antitoxins [33] . Evidence of the role of TA modules in persistence was recently provided by description of the HipA protein expression in E. coli , where cells overexpressing TA modules HipA and RelE form increased persisters [34] . These characterizations contribute significantly to the bacterial stress models, furthering our understanding of phenotypic drug tolerance mechanisms. However, a recent study showed that overexpression of other unrelated toxic proteins, such as heat-shock protein DnaJ and protein PmrC, have also been shown to cause increased formation of persisters [38] . Therefore, TA modules may not be the sole mediators of persister formation.
3.3.2 PhoU as a persistence switch A new persister gene, phoU , has recently been identified, where inactivation of the E. coli phoU gene leads to increased susceptibility to both antibiotics and stress conditions owing to a defect in forming persisters [39] . In this model of persister formation, PhoU serves as a global metabolic repressor, suppressing cellular metabolism on a comprehensive level thus promoting persister formation. In M. tuberculosis , which is notorious for its persistence, there are two PhoU homologs, PhoY1 and PhoY2. PhoY2 appears to be the equivalent of E. coli PhoU as its mutation caused increased susceptibility to TB drugs and stresses (W Shi and Y Zhang, unpublished). As PhoU is a ubiquitous protein present in both Gram-negative and Gram-positive bacteria, this switch may represent a potential persister drug target in many bacterial species [39] .
Exp
ert O
pin.
Dru
g D
isco
v. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
S.A
Lib
119
257
on 1
0/24
/12
For
pers
onal
use
onl
y.

New tuberculosis drug development: targeting the shikimate pathway
568 Expert Opin. Drug Discov. (2008) 3(5)
4. Current TB drug targets
Current antitubercular drugs primarily target cellular processes involved in bacterial growth and are either bacteriostatic or bactericidal. These include cell wall synthesis inhibitors, nucleic acid synthesis inhibitors, protein synthesis inhibitors, and energy inhibitors. With the exception of RIF and PZA, these drugs are highly effective against actively replicating cells and are considerably less potent against persisters [22] . Both persistent bacterial populations and patient noncompliance owing to lengthy therapy must be taken into consideration when developing new antimycobacterial drugs. The need for improved understanding of in vivo TB biology is essential for new drug development.
From the isolation of the H37Rv strain of M. tuberculosis in 1905 to the completion of the complete genome sequence in 1998 [40] , advances in molecular microbiology techniques have made the primary sequence of potential drug targets accessible. However, the sequence is only the beginning. Perhaps more challenging is identifying which of the 4,400 M. tuberculosis genes are essential, and which represent novel drug targets [41] . New drugs with novel mechanisms of action are needed to avoid the cross-resistance problem and, more importantly, to kill persister TB populations [22] . Recent advances in molecular tools make possible the identification of targets essential for survival and persistence whose inhibition is likely to shorten therapy. Various new drug targets and drug candidates have been recently reviewed [27] . This article will focus on the shikimate pathway as an attractive new drug target.
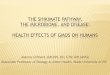
5. The shikimate pathway
The shikimate pathway involves seven enzymatic steps in the biosynthesis of the chorismate end product ( Figure 1 ), which in turn serves as the precursor for the synthesis of the aromatic amino acids, folates, ubiquinones, mycobactins, menaquinones, and napthoquinones ( Figure 2 ). Pathway essentiality has been proven in culture using mutants whose growth is completely inhibited without the provision of aromatic supplements [42] . Genomic studies demonstrating shikimate pathway essentiality in bacteria, fungi, algae, parasites, and higher plants make enzymes of the shikimate pathway attractive targets for drug development [43-45] . In fact, the pathway has been targeted in plants and apicomplexan parasites [46] , where Plasmodium falciparum and Toxoplasma gondii inhibition is observed in the presence of a known 5-enolpyruvylshikimate 3-phosphate (EPSP) synthase inhibitor, the herbicide glyphosate [47] . For almost three decades, there has been substantial interest in the shikimate pathway enzymes as a potential drug target in bacteria [48] . Through comparison of human and bacterial genomes, the ability to elucidate pathways essential in bacteria and not in humans allows for identification of drug
targets that can potentially decrease antimicrobial compound toxicity. Aromatic compound biosynthesis through the shikimate pathway is an attractive target for drug develop-ment because it is not present in mammals, which derive their aromatic compounds from their diet, making these potential targets considerably less toxic in humans [43] .
Perhaps one of the most important advances in the field of microbial physiology and metabolism occurred in the 1950s, when Bernard Davis explained pathway mechanisms by blocking biosynthetic steps in E. coli mutants [49] . Davis devised the common method of determining the order of reaction steps in a pathway using the principle that a mutant blocked in any given step accumulates the substrate of the blocked reaction. The substrates thus become a growth factor for a nearby mutant blocked at the earlier step. In this way, the biochemical pathway is determined [50] . Based on Davis’ work, the origin of the atoms making up shikimic acid was elucidated: phosphoenolpyruvate (PEP) and D -erythrose-4-phosphate (E4P) [51] . Davis’ initial work foreshadowed what we now know as the field of molecular genetics.
It was not until the early 1990s that the specific study of the shikimate pathway in M. tuberculosis began [52] , and the availability of the M. tuberculosis genome sequence [40] allowed for the identification of a homologous gene cluster encoding shikimate pathway enzymes ( Table 1 ). The cluster consists of the aroD gene (Rv2537c) encoding type II 3-dehydroquinate (DHQ) dehydratase, aroB (Rv2538c) encoding DHQ synthase, aroK (Rv2539c) encoding type I shikimate kinase (SK), and finally the aroF gene (Rv2540c) encoding chorismate synthase. The remaining three enzyme homologs are the aroG (Rv2178c) encoding the 3-deoxy- D -arabino-heptulosonate 7-phosphate (DAHP) synthase enzyme, aroE (Rv2552c) encoding shikimate-5-dehydrogenase (SD), and aroA (Rv3227) encoding 5-enoylpyruvylshikimate 3-phosphate (EPSP) synthase [43] .
The seven-step biosynthesis pathway of aromatic rings in bacteria begins with the substrates PEP E4P ( Figure 1 ) [48] . PEP and E4P undergo a stereospecific aldol-like conden-sation, catalyzed by DAHP synthase (encoded by the aroG gene), to form DAHP. The second step, catalyzed by DHQ synthase ( aroB ), converts DAHP to 3-dehydroquinate [53] . This step involves the committed formation of the carbo-cyclic ring precursor of the benzene ring in aromatic amino acids, folic acids, and numerous secondary metabolites. The third step is catalyzed by DHQ dehydratase, formerly known as dehydroquinase ( aroD ), and leads to the formation of 3-dehydroshikimate (DHS) [54] . This dehydration reaction introduces the first double bond to the aromatic ring. The fourth step in the shikimate pathway involves a reversible conversion of DHS to form shikimate [43] , from which the pathway derives its name. This NADPH-dependent reduction is catalyzed by the SD enzyme, encoded by the aroE gene [55] .
Exp
ert O
pin.
Dru
g D
isco
v. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
S.A
Lib
119
257
on 1
0/24
/12
For
pers
onal
use
onl
y.

Kapnick & Zhang
Expert Opin. Drug Discov. (2008) 3(5) 569
The fifth step marks the beginning of the second half of the shikimate pathway, where the reaction involving the shikimate substrate is catalyzed by SK, encoded by the aroK gene, to yield shikimate-3-phosphate (S3P) [56] . This is achieved through the transfer of a phosphate from the ATP co-substrate to the carbon 3-hydroxyl group to form the S3P product. The sixth and seventh steps in the pathway involve the condensation of S3P, through EPSP synthase ( aroA ), to yield EPSP [57] , followed by the addition of a second double bond into the aromatic ring,
catalyzed by chorismate synthase ( aroF ), to form the pathway end product, chorismate [43] .
6. Shikimate kinase
Although all seven homologs of the shikimate pathway have been identified in the M. tuberculosis genome, the SK ( aroK ) enzyme in particular may represent a potentially efficacious target in TB drug development. aroK is an essential gene whose inactivation leads to loss of viability [42] , providing
Phosphoenolpyruvate (PEP)+
HO O
O P
CH2 H2O
3-Deoxy-D-arabino-heptulosonate7-phosphate synthase
(DAHP synthase)EC: aroGMT: aroG
Pi NAD+ NAD+ + Pi
O
HO
H
H OH
OH
H
H2C–O–P
CH2
COO-
3-Dehydroquinate synthase(DHQ synthase)
EC: aroBMT: aroB 3-Dehydroquinate
(DHQ)
3-Dehydroquinate(DHQ dehydratase)
EC: aroDMT: aroD
H2O
3-Deoxy-D-arabino-heptulosonate 7-phosphate(DAHP)
ADP ATP NADP+ NADPH + H+
D-erythrose 4-phosphate (E4P)
Shikimate kinase(SK)
EC: aroK, aroLMT: aroK
Shikimate 3-phosphate(S3P)
PEP
Pi
Shikimate(SKH)
5-Enolpyruvylshikimate 3-phosphate synthase(EPSP synthase)
EC: aroAMT: aroA
5-Enolpyruvylshikimate 3-phosphate(EPSP)
Chorismate(CHA)
Chorismate synthase(CS)
EC: aroCMT: aroF
Pi
Shikimate dehydrogenase(SD)
EC: aroEMT: aroE
3-Dehydroshikimate(DHS)
COO-OH
OH
OH
O
COO-
HO
OH
OH
COO-
OH
OH
O
COO-
P O
OH
OH
O
COO-
COO-
OH
O CH2P
COO-
COO-
OH
CH2O
H
H OH
OH
H2C–O–P
CHO
Figure 1 . The shikimate pathway in M. tuberculosis [43,96] . Exp
ert O
pin.
Dru
g D
isco
v. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
S.A
Lib
119
257
on 1
0/24
/12
For
pers
onal
use
onl
y.

New tuberculosis drug development: targeting the shikimate pathway
570 Expert Opin. Drug Discov. (2008) 3(5)
evidence for the essentiality of shikimate pathway. Only when a second copy of the aroK gene is present could the disruption of the original chromosomal gene allow continued survival, despite presence of exogenous p -aminobenzoate and aromatic amino-acid supplements [42] .
The aroK (Rv2539c) gene is 531 base pairs long, coding for 176 amino acids with a theoretical molecular mass of 18.58 kDa [56] . In 2001, the first of cloning and over-expression of functional M. tuberculosis SK was published [58] . The three-dimensional structure of the enzyme complexed with shikimate was reported in 2004 ( Figure 3 ) [59,60] .
SK uses ATP in the fifth reaction of the pathway to catalyze the phosphorylation of the 3-hydroxyl group of shikimic acid, yielding S3P. SK represents one of two non-constitutively produced enzymes in the shikimate pathway, the latter being the DAHP synthase enzyme of the first step in the pathway [43] . In the E. coli model, two different forms catalyze this reaction: SKI, encoded by the aroK gene [61] and SKII, encoded by the aroL gene [62,63] .
The differences in the two gene products in E. coli lie in their biologic roles. SKII in E. coli appears to be involved in the shikimate pathway and is controlled by a negative feedback mechanism, mediated by the presence of tyrosine and tryptophan [64] . The role of SKI, however, is not clear, and may be unrelated to the shikimate pathway in E. coli organisms. The reason for the presence of two enzymes is not known but it has been suggested that the shikimate substrate may be a branch-point intermediate for another pathway [65] . In contrast to the E. coli bacterium, genome sequencing has revealed that M. tuberculosis has only one SK-encoding gene ( aroK ), and the gene shares a greater degree of homology with the E. coli aroK SKI enzyme (38% identity at the protein level) than the aroL SKII enzyme (28% identity) [56] .
Although few inhibition studies have been performed involving the M. tuberculosis SK (MtSK) enzyme [66] , the elucidation of the crystal structure of MtSK [59,67] has
Mycobactins, menaquinones &napthoquinones
Isochorismate
Shikimate pathwayAnthranilate
Phenylalanine
Prephenate
4-Amino-4-deoxy chorismate
Chorismate(CHA)
p-aminobenzoic acid
Tyrosine
p-dehydroxybenzoate
FolatesUbiquinones
Tryptophan
O
OHCH2
HN
H2N
O
OHCH2
NH2
O
OH
OH
CH2
H2N
COO-
COO-
OH
O CH2
Figure 2 . The shikimate pathway end product, chorismate, is the common precursor for the downstream biosynthesis of mycobactins, menaquinones, napthoquinones, aromatic amino acids, folates, and ubiquinones [43] .
Exp
ert O
pin.
Dru
g D
isco
v. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
S.A
Lib
119
257
on 1
0/24
/12
For
pers
onal
use
onl
y.

Kapnick & Zhang
Expert Opin. Drug Discov. (2008) 3(5) 571
allowed for the detailed study of the enzyme and related target-ligand interactions [60,68-70] . Among the specific SK interfaces studied has been the role of the ADP/Mg 2+ complex in creating the correct geometry to complete the phosphoryl transfer essential for the formation of S3P [59,71] . SK is a member of the same structural family of nucleoside monophosphate (NMP) kinases, which contain the three CORE, LID, and NMP-binding domains [72] . These domains mediate the MtSK–shikimate interaction and allow for conformational changes on substrate binding [59,68] .
Three functional motifs have also been described among the enzyme’s α / β folds: the Walker A and Walker B motifs, and an adenine-binding loop [73] . A phosphate-binding loop (P-loop), formed by the Walker A motif between the β 1 and α 1 folds, creates a hole which houses ADP and stabilizes the transition state through hydrogen bond donation [74] . MtSK inhibition through the ATP-binding site has been proposed; however, a potential weakness in this strategy may be that a similar binding site can be found in many P-loop kinases [75] , thus decreasing specificity.
Table 1 . The shikimate pathway enzymes in M. tuberculosis .
Pathway enzyme M. tuberculosis homologs
Structural information
Role Status and inhibition studies
1. DAHP synthase aroG (Rv2178c) 253 ± 25 kDa [82] (probable pentamer in solution) 1389 bp 462 amino acids
Catalyzes fi rst committed step in pathway
Type II MT DAHP synthase 3D structure determined [90] ; fi rst mechanism-based inhibitors synthesized [73]
2. DHQ synthase aroB (Rv2538c) 38.1 kDa [86] 1089 bp 362 amino acids
Essential for ring-containing compound synthesis
MT DHQ synthase crystal structure complete [109] , mechanism studies underway [43] ; carbocyclic phosphonate (DAHP analogue) inhibition studies [110] for further catalysis understanding needed
3. DHQ dehydratase aroD (Rv2537c) 15.8 kDa [43] 444 bp 147 amino acids
Introduction of fi rst double bond to aromatic ring
MT crystal structure complete [111] ; inhibitory action observed in series of previously known inhibitors [93]
4. Shikimate dehydrogenase
aroE (Rv2552c) 27.2 kDa [84] 810 bp 269 amino acids
Reversible conversion of DHS and NADPH to shikimate
E. coli , Haemophilus infl uenzae structures resolved [112,113] ; DHS analogue series shows some competitive inhibition in reverse reaction only [114]
5. Shikimate kinase aroK (Rv2539c) 18.58 kDa [56] 531 bp 176 amino acids
Marks beginning of second half of pathway
3D structure of SK–shikimate complex elucidated [59] ; proposed cyclopentenyl structures as shikimic acid analogue [66]
6. EPSP synthase aroA (Rv3227) 46.43 kDa [58] 1353 bp 450 amino acids
Penultimate step introducing second PEP into pathway
Crystal structure determination studies underway [43] ; current target of herbicide glyphosate [115] , effi cacy in mice against pathogenic protozoans [47] but variation in bacterial enzyme inhibition [116]
7. Chorismate synthase aroF (Rv2540c) 41.76 kDa [88] 1206 bp 401 amino acids
Final step introducing second double bond into aromatic ring yielding chorismate synthase
Crystallographic analysis performed [117] ; unique reduced fl avin mononucleotide dependence suggested target for drug development [97]
DAHP: 3-Deoxy- D -arabino-heptulosonate 7-phosphate; DHQ: 3-Dehydroquinate; DHS: 3-Dehydroshikimate; EPSP: 5-Enolpyruvylshikimate 3-phosphate; MT: Mycobacterium tuberculosis ; NADPH: Nicotinamide adenine dinucleotide phosphate; PEP: Phosphoenolpyruvate; SK: Shikimate kinase.
Exp
ert O
pin.
Dru
g D
isco
v. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
S.A
Lib
119
257
on 1
0/24
/12
For
pers
onal
use
onl
y.

New tuberculosis drug development: targeting the shikimate pathway
572 Expert Opin. Drug Discov. (2008) 3(5)
These studies in molecular dynamics are providing insight into the structural complexities of specific enzymes. Knowledge about molecule behavior deduced from observed structural flexibility in target-ligand interactions provides information that may allow for the design of specific inhibitors that target ATP or shikimate binding sites, preventing reaction catalysis by inhibiting conformational changes [56] . The availability of the structure of MtSK may also allow drug design to focus on specific or competitive enzyme inhibitors, and further evaluate alternative binding affinities in the enzyme folds and functional motifs of the MtSK enzyme.
7. Drug development based on the shikimate pathway
The development of drugs targeting the shikimate pathway enzymes offers the potential benefit of cross-species potency, making them attractive, marketable, and cost- effective agents ( Table 1 ) [76] . The first efficacious shikimate pathway enzyme inhibitor with antimicrobial activity was (6S) -6-fluoroshikimate [77] , thought to inhibit p -aminobenzoic acid generation [78] , which serves as a substrate for down-stream folate biosynthesis [79] . However, mutations in mecha-nisms of drug uptake occurred causing the rapid development of resistance specific to (6S) -6-fluoroshikimate [80,81] .
All the enzymes of the M. tuberculosis shikimate pathway have been characterized to some degree [82-88] . However, the number of studies investigating M. tuberculosis crystal structures and mechanisms of action vary from enzyme to enzyme. For example, although the crystal structure of the E. coli DAHP synthase, the first enzyme of the shikimate pathway, has been known for some time [89] , only recently has the preliminary M. tuberculosis DAHP synthase three-dimensional structure
ADP
Shikimate
Figure 3 . M. tuberculosis shikimate kinase complexed with shikimate and ADP [69] .
been elucidated [90] . In addition, differences among enzymes between bacteria also make the process of shikimate enzyme characterization a slow and laborious process. This became especially evident in studies investigating the third enzyme of the pathway. DHQ dehydratase has two classes in E. coli – type I and type II, implicated in chorismate bio-synthesis and quinate catabolism, respectively [91] . By contrast, M. tuberculosis has only one type II DHQ dehydratase enzyme in the shikimate pathway [87] . Differences among shikimate pathway enzymes, however, may allow for the focused design of specific inhibitors of the type I or type II DHQ dehydratases. In fact, type II selective inhibitors mimicking a transition state in this reaction have been synthesized in the past [92] . More recently, studies involving analogues of (1R, 3R, 4R) -1,3,4-trihydroxycyclohex-5-en-1-carboxylic acid, a known DHQ dehydratase inhibitor, have demonstrated some successful inhibition of M. tuberculosis DHQ dehydratase [93] .
The crystal structure of the fourth enzyme of the M. tuberculosis shikimate pathway, shikimate dehydrogenase, is yet to be elucidated. However, insights into the chemical and kinetic mechanisms of the enzyme have recently been published [83,84] . By contrast, substantially more work has been performed on the fifth and sixth enzymes of the pathway: SK and EPSP [56,57,59,60,69,94] . Two small molecular inhibitors against Helicobacter pylori shikimate kinase have recently been identified through high-throughput screening: 3-methoxy-4-{[2-({2-methoxy-4-[(4-oxo-2-thioxo-1,3- thiazolidin-5-ylidene)methyl]phenoxy}methyl)benzyl]oxy}benzaldehyde and 5-bromo-2-(5-{[1-(3,4-dichlorophenyl)- 3,5-dioxo-4-pyrazolidinylidene]methyl}-2-furyl)benzoic acid. The first is a noncompetitive inhibitor of shikimate and MgATP, and the second is a competitive inhibitor of shikimate and noncompetitive inhibitor of MgATP [95] . Molecular modeling was also performed to evaluate the mechanisms of inhibition for future inhibitor design. In addition, the commercial herbicide glyphosate, an inhibitor of EPSP synthase, is already available and widely used [46] . However, further studies are needed to investigate controversial conformational changes undergone by EPSP synthase on inhibitor binding before new compounds targeting this enzyme are seen [96] . The final enzyme of the shikimate pathway, chorismate synthase, also represents a potential target for drug development. Unique to this final and flavin-dependent enzyme of the shikimate pathway is the stringent requirement for stereospecific elimination [97] , making chorismate synthase another attractive target for drug development.
The enzymes of the shikimate pathway have attracted significant interest but considerable work remains to be done before potent and safe inhibitors are developed. The availability of bacterial genome sequences and advances in crystallography and molecular genetic tools have significantly aided the identification of new targets for antibiotic development.
Exp
ert O
pin.
Dru
g D
isco
v. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
S.A
Lib
119
257
on 1
0/24
/12
For
pers
onal
use
onl
y.

Kapnick & Zhang
Expert Opin. Drug Discov. (2008) 3(5) 573
8. Vaccine development based on the shikimate pathway
It has been determined that M. tuberculosis strains defective in their amino-acid biosynthesis pathways demonstrate varying degree of attenuation [98,99] . Thus, in addition to providing new targets for drug development, the shikimate pathway is also of increasing interest in vaccine development. The M. tuberculosis aroA gene, coding for EPSP synthase enzymes, has been of particular interest. Deletion of the shikimate pathway gene, aroA encoding EPSP synthase, renders virulence attenuation in strains of Salmonella [100] , and has already been exploited in the development of vaccines that elicit a protective response [101] . In addition, Listeria monocytogenes mutants with deletions in the aroA (EPSP synthase), aroB (DHQ synthase), and aroE (SD) have demonstrated significant attenuation in mice and still elicited a protective T-cell response [102] . Other studies involving the inactivation of aro genes in Shigella flexneri [103] , Pasteurella multocida [104] , the Streptococcus suis swine strain [105] , and Salmonella typhimurium and S. typhi species [106,107] have met with some success, suggesting that inactivation of shikimate pathway genes may also be useful in M. tuberculosis vaccine development.
9. Expert opinion
Recent advances in genome sequencing and molecular biology of mycobacteria have made it possible to identify essential key targets for drug development. Among the essential genes that have been identified and could serve as drug targets are components of the shikimate pathway, especially SK ( aroK ). Significant progress has been made in terms of the biochemical, molecular genetic, and structural characterization of the shikimate pathway enzymes [43] . All of these are important for understanding the physiology of the tubercle bacillus and may provide useful information when choosing drug targets in target-based drug screens. We may indeed to identify inhibitors for shikimate pathway enzymes, including SK, in target-based screens. However, the field of TB drug development has evolved recently from previously focusing on identifying inhibitors or compounds that are active against actively growing bacilli including MDR TB to identifying drug candidates that kill nonreplicating persisters and shorten the therapy.
Given aroK or other shikimate enzyme inhibitors are identified based on target-based screens, there may still be problems with compound penetration and activity against whole organisms, in vivo PK/PD profiles, toxicity, and in vivo antituberculosis activity, in particular activity against persisters. It is now well known that there are serious limitations to the target-based approach [22,108] . An alternative is the use of whole cell based screens to identify possible inhibitors of the shikimate pathway in M. tuberculosis using compounds that mimic shikimate pathway intermediates or
the chorismate end product. Whole cell based screens can be performed under different screening conditions. In particular, ageing, hypoxia, and acidic pH conditions that facilitate persister formation would be desirable for identifying compounds active against persisters. Given that shikimate pathway inhibitors have in vitro and in vivo activity against M. tuberculosis , it is unlikely that the inhibitors would be used alone, i.e., they will have to be used in combination with current TB drugs like PZA, RIF, and INH for treatment. To become a much-needed new TB drug, it will be vital for inhibitors of the shikimate pathway enzymes, including aroK , to shorten TB chemotherapy when used in combination with PZA, RIF, and INH.
The choice of the target for drug development is obviously critical. The shikimate pathway may provide attractive drug targets, as its end product chorismate is the common precursor for the downstream biosynthesis of many essential products for the cell including mycobactins, menaquinones, napthoquinones, aromatic amino acids, folates, and ubiquinones. However, the importance of the target may vary according to different selection conditions. For example, aroK is an essential gene that is required for in vitro growth in lab culture media but it may or may not be essential under other growth conditions. It is becoming increasingly clear that a drug that hits a single target in the cell may have significant limitations. It will therefore be important to evaluate aroK inhibitors with other drugs under different conditions to determine the optimal drug combination for cidal and sterilizing activity.
Besides potentially offering useful targets for drug development, shikimate pathway mutants may also be good TB vaccine candidates. aroA mutants have already been used as attenuated vaccines with other bacterial species, especially Salmonella , and have shown some protective efficacy in clinical trials [101] .
In summary, shikimate pathway enzymes, especially SK ( aroK ), may indeed offer attractive targets for new TB drug and vaccine development. However, the target-based screen-ing approach may have limitations, and whole cell based screens with shikimate pathway intermediate mimics, especially under conditions that facilitate persister forma-tion, may be needed to identify compounds active not only for growing bacteria but more importantly for persisters. Shikimate pathway inhibitors will have to be used together with current TB drugs for more effective treatment. Recent progress in combinatorial chemistry, molecular genetics, and structural and systems biology may facilitate more efficient development of new drug candidates that target the shikimate pathway.
Declaration of interest
YZ acknowledges the support by NIH grant AI44063, Basic Research (973) Program (2005CB523102) and Changjiang Scholar Program, China.
Exp
ert O
pin.
Dru
g D
isco
v. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
S.A
Lib
119
257
on 1
0/24
/12
For
pers
onal
use
onl
y.

New tuberculosis drug development: targeting the shikimate pathway
574 Expert Opin. Drug Discov. (2008) 3(5)
Bibliography 1. Dubos R, Dubos J. The white plague:
tuberculosis, man, and society. New Brunswick: Rutgers University Press; 1987
2. Bunyan J. The Life and Death of Mr. Badman. London: Hesperus Press; 2007
3. World Health Organization. The World Health Organization Global Tuberculosis Program. 2007 . Available from: http://www.who.int/tb/en/
4. McShane H. Co-infection with HIV and TB: double trouble. Int J STD AIDS 2005 ; 16 : 95 -101
5. Oursler K, Moore R, Bishai W, et al. Survival of patients with pulmonary tuberculosis: clinical and molecular epidemiologic factors. Clin Infect Dis 2002 ; 34 : 752 -9
6. Elliot A, Halwiindi B, Hayes R, et al. The impact of human immunodefi ciency virus on mortality of patients treated for tuberculosis in a cohort study in Zambia. Trans R Soc Trop Med Hyg 1995 ; 89 : 78 -82
7. Chaisson RE, Schecter GF, Theuer CP, et al. Tuberculosis in patients with the acquired immunodefi ciency syndrome. Clinical features, response to therapy, and survival. Am Rev Respir Dis 1987 ; 136 (3): 570 -4
8. Vernon A, Burman W, Benator D, et al. Acquired rifamycin monoresistance in patients with HIV-related tuberculosis treated with once-weekly rifapentine and isoniazid. Tuberculosis Trials Consortium. Lancet 1999 ; 353 (9167): 1843 -7
9. March F, Garriga X, Rodriguez P, et al. Acquired drug resistance in Mycobacterium tuberculosis isolates recovered from compliant patients with human immunodefi ciency virus-associated tuberculosis. Clin Infect Dis 1997 ; 25 (5): 1044 -7
10. Frothingham R, Stout JE, Hamilton CD. Current issues in global tuberculosis control. Int J Infect Dis 2005 ; 9 (6): 297 -311
11. Sepkowitz KA, Raffalli J, Riley L, et al. Tuberculosis in the AIDS era. Clin Microbiol Rev 1995 ; 8 (2): 180 -99
12. Perriens JH, Colebunders RL, Karahunga C, et al. Increased mortality and tuberculosis treatment failure rate among human immunodefi ciency virus (HIV) seropositive compared with HIV seronegative patients with pulmonary tuberculosis treated with “standard” chemotherapy in Kinshasa, Zaire. Am Rev Respir Dis 1991 ; 144 (4): 750 -5
13. World Health Organization. Stop TB Partnership. 2007 . Available from: http://www.who.int/mediacentre/factsheets/fs104/en/index.html
14. Castro K. Extensively drug resistant TB (XDR-TB) late breaking update. CDC DTBE All Hands Meeting; 2006 October 15
15. Gandhi NR, Moll A, Sturm AW, et al. Extensively drug-resistant tuberculosis as a cause of death in patients co-infected with tuberculosis and HIV in a rural area of South Africa. Lancet 2006 ; 368 (9547): 1575 -80
16. Mitchison DA. The diagnosis and therapy of tuberculosis during the past 100 years. Am J Respir Crit Care Med 2005 ; 171 (7): 699 -706
17. Schatz A, Bugie E, Waksman SA. Streptomycin, a substance exhibiting antibiotic activity against gram-positive and gram-negative bacteria. Proc Soc Exp Biol Med 1944 ; 55 : 66 -9
18. Fox W, Ellard GA, Mitchison DA. Studies on the treatment of tuberculosis undertaken by the British Medical Research Council tuberculosis units, 1946-1986, with relevant subsequent publications. Int J Tuberc Lung Dis 1999 ; 3 (10 Suppl 2): S231 -79
19. Waksman SA, Reilly HC, Schatz A. Strain specifi city and production of antibiotic substances. V. Strain resistance of bacteria to antibiotic substances, especially to streptomycin. Proc Natl Acad Sci USA 1945 ; 31 (6): 157 -64
20. Schaberg T, Rebhan K, Lode H. Risk factors for side-effects of isoniazid, rifampin and pyrazinamide in patients hospitalized for pulmonary tuberculosis. Eur Respir J 1996 ; 9 (10): 2026 -30
21. Awofesoa N. Anti-tuberculosis medication side-effects constitute a major factor for poor treatment adherence. Bulletin of the World Health Organization; 2006
22. Zhang Y. The magic bullets and tuberculosis drug targets. Ann Rev Pharmacol Toxicol 2005 ; 45 : 529 -64
23. Shah D, Zhang Z, Khodursky A, et al. Persisters: a distinct physiological state of E. coli. BMC Microbiol 2006 ; 6 : 53
24. Massey RC, Buckling A, Peacock SJ. Phenotypic switching of antibiotic resistance circumvents permanent costs in Staphylococcus aureus. Curr Biol 2001 ; 11 (22): 1810 -4
25. Kussell E, Kishony R, Balaban NQ, et al. Bacterial persistence: a model of survival in
changing environments. Genetics 2005 ; 169 (4): 1807 -14
26. Mitchison DA. The action of antituberculosis drugs in short-course chemotherapy. Tubercle 1985 ; 66 (3): 219 -25
27. Zhang Y. Advances in the treatment of tuberculosis. Clin Pharmacol Ther 2007 ; 82 (5): 595 -600
28. Bigger J. Treatment of staphylococcal infections with penicillin. Lancet 1944 ; ii : 497 -500
29. Klapper I, Gilbert P, Ayati BP, et al. Senescence can explain microbial persistence. Microbiology 2007 ; 153 (Pt 11): 3623 -30
30. Miller C, Thomsen LE, Gaggero C, et al. SOS response induction by beta-lactams and bacterial defense against antibiotic lethality. Science 2004 ; 305 (5690): 1629 -31
31. Balaban NQ, Merrin J, Chait R, et al. Bacterial persistence as a phenotypic switch. Science 2004 ; 305 (5690): 1622 -5
32. Byrne ST, Gu P, Zhou J, et al. Pyrrolidine dithiocarbamate and diethyldithiocarbamate are active against growing and nongrowing persister Mycobacterium tuberculosis. Antimicrob Agents Chemother 2007 ; 51 (12): 4495 -7
33. Warner DF, Mizrahi V. Tuberculosis chemotherapy: the infl uence of bacillary stress and damage response pathways on drug effi cacy. Clin Microbiol Rev 2006 ; 19 (3): 558 -70
34. Korch SB, Henderson TA, Hill TM. Characterization of the hipA7 allele of Escherichia coli and evidence that high persistence is governed by (p)ppGpp synthesis. Mol Microbiol 2003 ; 50 (4): 1199 -213
35. Korch SB, Hill TM. Ectopic overexpression of wild-type and mutant hipA genes in Escherichia coli: effects on macromolecular synthesis and persister formation. J Bacteriol 2006 ; 188 (11): 3826 -36
36. Gerdes K, Rasmussen PB, Molin S. Unique type of plasmid maintenance function: postsegregational killing of plasmid-free cells. Proc Natl Acad Sci USA 1986 ; 83 (10): 3116 -20
37. Keren I, Shah D, Spoering A, et al. Specialized persister cells and the mechanism of multidrug tolerance in Escherichia coli. J Bacteriol 2004 ; 186 (24): 8172 -80
38. Vazquez-Laslop N, Lee H, Neyfakh AA. Increased persistence in Escherichia coli
Exp
ert O
pin.
Dru
g D
isco
v. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
S.A
Lib
119
257
on 1
0/24
/12
For
pers
onal
use
onl
y.

Kapnick & Zhang
Expert Opin. Drug Discov. (2008) 3(5) 575
caused by controlled expression of toxins or other unrelated proteins. J Bacteriol 2006 ; 188 (10): 3494 -7
39. Li Y, Zhang Y. PhoU is a persistence switch involved in persister formation and tolerance to multiple antibiotics and stresses in Escherichia coli. Antimicrob Agents Chemother 2007 ; 51 (6): 2092 -9
40. Cole ST, Brosch R, Parkhill J, et al. Deciphering the biology of Mycobacterium tuberculosis from the complete genome sequence. Nature 1998 ; 393 (6685): 537 -44
41. Duncan K. Identifi cation and validation of novel drug targets in tuberculosis. Curr Pharm Des 2004 ; 10 (26): 3185 -94
42. Parish T, Stoker NG. The common aromatic amino acid biosynthesis pathway is essential in Mycobacterium tuberculosis. Microbiology 2002 ; 148 (Pt 10): 3069 -77
43. Ducati RG, Basso LA, Santos DS. Mycobacterial shikimate pathway enzymes as targets for drug design. Curr Drug Targets 2007 ; 8 (3): 423 -35
44. Starcevic A, Akthar S, Dunlap WC, et al. Enzymes of the shikimic acid pathway encoded in the genome of a basal metazoan, Nematostella vectensis, have microbial origins. Proc Natl Acad Sci USA 2008 ; 105 (7): 2533 -7
45. Bentley R. The shikimate pathway – a metabolic tree with many branches. Crit Rev Biochem Mol Biol 1990 ; 25 (5): 307 -84
46. Coggins J. The shikimate pathway as a target for herbicides. In: Dodge A, editor, Herbicides and plant metabolism. Cambridge: Cambridge University Press; 1989
47. Roberts F, Roberts CW, Johnson JJ, et al. Evidence for the shikimate pathway in apicomplexan parasites. Nature 1998 ; 393 (6687): 801 -5
48. Coggins JR, Abell C, Evans LB, et al. Experiences with the shikimate-pathway enzymes as targets for rational drug design. Biochem Soc Trans 2003 ; 31 (Pt 3): 548 -52
49. Davis BD. Aromatic biosynthesis. I. The role of shikimic acid. J Biol Chem 1951 ; 191 (1): 315 -25
50. Davis BD, Mingioli ES. Aromatic biosynthesis. VII. Accumulation of two derivatives of shikimic acid by bacterial mutants. J Bacteriol 1953 ; 66 (2): 129 -36
51. Srinivasan PR, Shigeura HT, Sprecher M, et al. The biosynthesis of shikimic acid from D-glucose. J Biol Chem 1956 ; 220 (1): 477 -97
52. Garbe T, Jones C, Charles I, et al. Cloning and characterization of the aroA gene from Mycobacterium tuberculosis. J Bacteriol 1990 ; 172 (12): 6774 -82
53. Srinivasan PR, Rothschild J, Sprinson DB. The enzymic conversion of 3-deoxy- D -arabino-heptulosonic acid 7-phosphate to 5-dehydroquinate. J Biol Chem 1963 ; 238 : 3176 -82
54. Mitsuhashi S, Davis BD. Aromatic biosynthesis. XII. Conversion of 5-dehydroquinic acid to 5-dehydroshikimic acid dy 5-dehydroquinase. Biochem Biophys Acta 1954 ; 15 (1): 54 -61
55. Yaniv H, Gilvarg C. Aromatic biosynthesis. XIV. 5-Dehydroshikimic reductase. J Biol Chem 1955 ; 213 (2): 787 -95
56. Pereira JH, Vasconcelos IB, Oliveira JS, et al. Shikimate kinase: a potential target for development of novel antitubercular agents. Curr Drug Targets 2007 ; 8 (3): 459 -68
57. Levin JG, Sprinson DB. The enzymatic formation and isolation of 3-enolpyruvylshikimate 5-phosphate. J Biol Chem 1964 ; 239 : 1142 -50
58. Oliveira JS, Pinto CA, Basso LA, et al. Cloning and overexpression in soluble form of functional shikimate kinase and 5-enolpyruvylshikimate 3-phosphate synthase enzymes from Mycobacterium tuberculosis. Protein Expr Purif 2001 ; 22 (3): 430 -5
59. Pereira JH, de Oliveira JS, Canduri F, et al. Structure of shikimate kinase from Mycobacterium tuberculosis reveals the binding of shikimic acid. Acta Crystallogr D Biol Crystallogr 2004 ; 60 (Pt 12 Pt 2): 2310 -9
60. Dhaliwal B, Nichols CE, Ren J, et al. Crystallographic studies of shikimate binding and induced conformational changes in Mycobacterium tuberculosis shikimate kinase. FEBS Lett 2004 ; 574 (1-3): 49 -54
61. Lobner-Olesen A, Marinus MG. Identifi cation of the gene (aroK) encoding shikimic acid kinase I of Escherichia coli. J Bacteriol 1992 ; 174 (2): 525 -9
62. Millar G, Lewendon A, Hunter MG, et al. The cloning and expression of the aroL gene from Escherichia coli K12. Purifi cation and complete amino acid
sequence of shikimate kinase II, the aroL-gene product. Biochem J 1986 ; 237 (2): 427 -37
63. DeFeyter RC, Pittard J. Purifi cation and properties of shikimate kinase II from Escherichia coli K-12. J Bacteriol 1986 ; 165 (1): 331 -3
64. Ely B, Pittard J. Aromatic amino acid biosynthesis: regulation of shikimate kinase in Escherichia coli K-12. J Bacteriol 1979 ; 138 (3): 933 -43
65. Weiss U, Edwards J. The biosynthesis of aromatic compounds. New York: John Wiley and Sons; 1980
66. An M, Toochinda T, Bartlett PA. Five-membered ring analogues of shikimic acid. J Org Chem 2001 ; 66 (4): 1326 -33
67. Gu Y, Reshetnikova L, Li Y, et al. Crystallization and preliminary X-ray diffraction analysis of shikimate kinase from Mycobacterium tuberculosis in complex with MgADP. Acta Crystallogr D Biol Crystallogr 2001 ; 57 (Pt 12): 1870 -1
68. Gu Y, Reshetnikova L, Li Y, et al. Crystal structure of shikimate kinase from Mycobacterium tuberculosis reveals the dynamic role of the LID domain in catalysis. J Mol Biol 2002 ; 319 (3): 779 -89
69. Dias MV, Faim LM, Vasconcelos IB, et al. Effects of the magnesium and chloride ions and shikimate on the structure of shikimate kinase from Mycobacterium tuberculosis. Acta Crystallogr Sect F Struct Biol Cryst Commun 2007 ; 63 (Pt 1): 1 -6
70. Hartmann MD, Bourenkov GP, Oberschall A, et al. Mechanism of phosphoryl transfer catalyzed by shikimate kinase from Mycobacterium tuberculosis. J Mol Biol 2006 ; 364 (3): 411 -23
71. Matte A, Tari LW, Delbaere LT. How do kinases transfer phosphoryl groups? Structure 1998 ; 6 (4): 413 -9
72. Vonrhein C, Schlauderer GJ, Schulz GE. Movie of the structural changes during a catalytic cycle of nucleoside monophosphate kinases. Structure 1995 ; 3 (5): 483 -90
73. Walker JE, Saraste M, Runswick MJ, et al. Distantly related sequences in the alpha- and beta-subunits of ATP synthase, myosin, kinases and other ATP-requiring enzymes and a common nucleotide binding fold. EMBO J 1982 ; 1 (8): 945 -51
74. Smith CA, Rayment I. Active site comparisons highlight structural similarities
Exp
ert O
pin.
Dru
g D
isco
v. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
S.A
Lib
119
257
on 1
0/24
/12
For
pers
onal
use
onl
y.

New tuberculosis drug development: targeting the shikimate pathway
576 Expert Opin. Drug Discov. (2008) 3(5)
between myosin and other P-loop proteins. Biophys J 1996 ; 70 (4): 1590 -602
75. Leipe DD, Koonin EV, Aravind L. Evolution and classifi cation of P-loop kinases and related proteins. J Mol Biol 2003 ; 333 (4): 781 -815
76. Brown J, Warren P. Antibiotic discovery: is it all in the genes? Drug Discov Today 1998 ; 3 : 564 -66
77. Davies GM, Barrett-Bee KJ, Jude DA, et al. (6S)-6-fl uoroshikimic acid, an antibacterial agent acting on the aromatic biosynthetic pathway. Antimicrob Agents Chemother 1994 ; 38 (2): 403 -6
78. Bornemann S, Ramjee MK, Balasubramanian S, et al. Escherichia coli chorismate synthase catalyzes the conversion of (6S)-6-fl uoro-5-enolpyruvylshikimate-3-phosphate to 6-fl uorochorismate. Implications for the enzyme mechanism and the antimicrobial action of (6S)-6-fl uoroshikimate. J Biol Chem 1995 ; 270 (39): 22811 -5
79. Green JM, Merkel WK, Nichols BP. Characterization and sequence of Escherichia coli pabC, the gene encoding aminodeoxychorismate lyase, a pyridoxal phosphate-containing enzyme. J Bacteriol 1992 ; 174 (16): 5317 -23
80. Jude DA, Ewart CD, Thain JL, et al. Transport of the antibacterial agent (6S)-6-fl uoroshikimate and other shikimate analogues by the shikimate transport system of Escherichia coli. Biochim Biophys Acta 1996 ; 1279 (2): 125 -9
81. Ewart CD, Jude DA, Thain JL, et al. Frequency and mechanism of resistance to antibacterial action of ZM 240401, (6S)-6-fl uoro-shikimic acid. Antimicrob Agents Chemother 1995 ; 39 (1): 87 -93
82. Rizzi C, Frazzon J, Ely F, et al. DAHP synthase from Mycobacterium tuberculosis H37Rv: cloning, expression, and purifi cation of functional enzyme. Protein Expr Purif 2005 ; 40 (1): 23 -30
83. Magalhaes ML, Pereira CP, Basso LA, et al. Cloning and expression of functional shikimate dehydrogenase (EC 1.1.1.25) from Mycobacterium tuberculosis H37Rv. Protein Expr Purif 2002 ; 26 (1): 59 -64
84. Zhang X, Zhang S, Hao F, et al. Expression, purifi cation and properties of shikimate dehydrogenase from Mycobacterium tuberculosis. J Biochem Mol Biol 2005 ; 38 (5): 624 -31
85. Oliveira JS, Mendes MA, Palma MS, et al. One-step purifi cation of 5-enolpyruvylshikimate-3-phosphate synthase enzyme from Mycobacterium tuberculosis. Protein Expr Purif 2003 ; 28 (2): 287 -92
86. de Mendonca JD, Ely F, Palma MS, et al. Functional characterization by genetic complementation of aroB-encoded dehydroquinate synthase from Mycobacterium tuberculosis H37Rv and its heterologous expression and purifi cation. J Bacteriol 2007 ; 189 (17): 6246 -52
87. Garbe T, Servos S, Hawkins A, et al. The Mycobacterium tuberculosis shikimate pathway genes: evolutionary relationship between biosynthetic and catabolic 3-dehydroquinases. Mol Gen Genet 1991 ; 228 (3): 385 -92
88. Dias MV, Borges JC, Ely F, et al. Structure of chorismate synthase from Mycobacterium tuberculosis. J Struct Biol 2006 ; 154 (2): 130 -43
89. Shumilin IA, Kretsinger RH, Bauerle RH. Crystal structure of phenylalanine-regulated 3-deoxy- D -arabino-heptulosonate-7-phosphate synthase from Escherichia coli. Structure 1999 ; 7 (7): 865 -75
90. Webby CJ, Lott JS, Baker HM, et al. Crystallization and preliminary X-ray crystallographic analysis of 3-deoxy- D -arabino-heptulosonate-7-phosphate synthase from Mycobacterium tuberculosis. Acta Crystallogr Sect F Struct Biol Cryst Commun 2005 ; 61 (Pt 4): 403 -6
91. Gourley DG, Shrive AK, Polikarpov I, et al. The two types of 3-dehydroquinase have distinct structures but catalyze the same overall reaction. Nat Struct Biol 1999 ; 6 (6): 521 -5
92. Frederickson M, Parker EJ, Hawkins AR, et al. Selective inhibition of type II dehydroquinases. J Org Chem 1999 ; 64 (8): 2612 -3
93. Sanchez-Sixto C, Prazeres VF, Castedo L, et al. Structure-based design, synthesis, and biological evaluation of inhibitors of Mycobacterium tuberculosis type II dehydroquinase. J Med Chem 2005 ; 48 (15): 4871 -81
94. Filgueira de Azevedo W Jr, Canduri F, Simoes de Oliveira J, et al. Molecular model of shikimate kinase from Mycobacterium tuberculosis. Biochem Biophys Res Commun 2002 ; 295 (1): 142 -8
95. Han C, Zhang J, Chen L, et al. Discovery of Helicobacter pylori shikimate kinase inhibitors: bioassay and molecular modeling. Bioorg Med Chem 2007 ; 15 (2): 656 -62
96. Marques MR, Pereira JH, Oliveira JS, et al. The inhibition of 5-enolpyruvylshikimate-3-phosphate synthase as a model for development of novel antimicrobials. Curr Drug Targets 2007 ; 8 (3): 445 -57
97. Dias MV, Ely F, Palma MS, et al. Chorismate synthase: an attractive target for drug development against orphan diseases. Curr Drug Targets 2007 ; 8 (3): 437 -44
98. Smith DA, Parish T, Stoker NG, et al. Characterization of auxotrophic mutants of Mycobacterium tuberculosis and their potential as vaccine candidates. Infect Immun 2001 ; 69 (2): 1142 -50
99. Hondalus MK, Bardarov S, Russell R, et al. Attenuation of and protection induced by a leucine auxotroph of Mycobacterium tuberculosis. Infect Immun 2000 ; 68 (5): 2888 -98
100. Hoiseth SK, Stocker BA. Genes aroA and serC of Salmonella typhimurium constitute an operon. J Bacteriol 1985 ; 163 (1): 355 -61
101. Dilts DA, Riesenfeld-Orn I, Fulginiti JP, et al. Phase I clinical trials of aroA aroD and aroA aroD htrA attenuated S. typhi vaccines; effect of formulation on safety and immunogenicity. Vaccine 2000 ; 18 (15): 1473 -84
102. Stritzker J, Janda J, Schoen C, et al. Growth, virulence, and immunogenicity of Listeria monocytogenes aro mutants. Infect Immun 2004 ; 72 (10): 5622 -9
103. Cersini A, Salvia AM, Bernardini ML. Intracellular multiplication and virulence of Shigella fl exneri auxotrophic mutants. Infect Immun 1998 ; 66 (2): 549 -57
104. Scott PC, Markham JF, Whithear KG. Safety and effi cacy of two live Pasteurella multocida aro-A mutant vaccines in chickens. Avian Dis 1999 ; 43 (1): 83 -8
105. Fittipaldi N, Harel J, D’Amours B, et al. Potential use of an unencapsulated and aromatic amino acid-auxotrophic Streptococcus suis mutant as a live attenuated vaccine in swine. Vaccine 2007 ; 25 (18): 3524 -35
106. Marsden MJ, Vaughan LM, Fitzpatrick RM, et al. Potency testing of a live, genetically attenuated vaccine for salmonids. Vaccine 1998 ; 16 (11-12): 1087 -94
Exp
ert O
pin.
Dru
g D
isco
v. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
S.A
Lib
119
257
on 1
0/24
/12
For
pers
onal
use
onl
y.

Kapnick & Zhang
Expert Opin. Drug Discov. (2008) 3(5) 577
107. Stocker BA. Auxotrophic Salmonella typhi as live vaccine. Vaccine 1988 ; 6 (2): 141 -5
108. Projan SJ. Why is big Pharma getting out of antibacterial drug discovery? Curr Opin Microbiol 2003 ; 6 (5): 427 -30
109. Carpenter EP, Hawkins AR, Frost JW, et al. Structure of dehydroquinate synthase reveals an active site capable of multistep catalysis. Nature 1998 ; 394 (6690): 299 -302
110. Widlanski T, Bender SL, Knowles JR. Dehydroquinate synthase: the use of substrate analogues to probe the late steps of the catalyzed reaction. Biochemistry 1989 ; 28 (19): 7572 -82
111. Gourley DG, Coggins JR, Isaacs NW, et al. Crystallization of a type II dehydroquinase from Mycobacterium tuberculosis. J Mol Biol 1994 ; 241 (3): 488 -91
112. Michel G, Roszak AW, Sauve V, et al. Structures of shikimate dehydrogenase
AroE and its Paralog YdiB. A common structural framework for different activities. J Biol Chem 2003 ; 278 (21): 19463 -72
113. Ye S, Von Delft F, Brooun A, et al. The crystal structure of shikimate dehydrogenase (AroE) reveals a unique NADPH binding mode. J Bacteriol 2003 ; 185 (14): 4144 -51
114. Baillie AC, Corbett JR, Dowsett JR, et al. Inhibitors of shikimate dehydrogenase as potential herbicides. Biochem J 1972 ; 126 (3): 21P
115. Steinrucken HC, Amrhein N. The herbicide glyphosate is a potent inhibitor of 5-enolpyruvyl-shikimic acid-3-phosphate synthase. Biochem Biophys Res Commun 1980 ; 94 (4): 1207 -12
116. Herrmann KM, Weaver LM. The shikimate pathway. Ann Rev Plant Physiol Plant Mol Biol 1999 ; 50 : 473 -503
117. Dias MV, Ely F, Canduri F, et al. Crystallization and preliminary X-ray crystallographic analysis of chorismate synthase from Mycobacterium tuberculosis. Acta Crystallogr D Biol Crystallogr 2004 ; 60 (Pt 11): 2003 -5
Affi liation Senta M Kapnick & Ying Zhang † † Author for correspondence Johns Hopkins University, Department of Molecular Microbiology & Immunology, Bloomberg School of Public Health, 615 N Wolfe Street, Baltimore, MD 21205, USA Tel: +1 410 614 2975 ; Fax: +1 410 955 0105 ; E-mail: [email protected]
Exp
ert O
pin.
Dru
g D
isco
v. D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
S.A
Lib
119
257
on 1
0/24
/12
For
pers
onal
use
onl
y.