Embed Size (px)
Citation preview
New Paradigms for Quality Management in Radiation Therapy
M. Saiful Huq, Ph.D., FAAPM, FInstP Professor and DirectorDepartment of Radiation Oncology
University of Pittsburgh Cancer Institute ; UPMC Cancer CentersPittsburgh, Pennsylvania, USA
Acknowledgment
Members of TG100
• M. Saiful Huq (Chair)• Peter B. Dunscombe• Benedick A. Fraass• John P. Gibbons• Geoffrey S. Ibbott• Sasa Mutic
• Ellen D. Yorke (Vice Chair)• Arno Mundt (MD)• Jatinder R. Palta• Frank Rath (Industrial
engineer)• Bruce R. Thomadsen• Jeffrey F. Williamson
AAPM Summer School 2011Saiful Huq - New Paradigms for QM in RT 2
Outline
• Why do we need a new paradigm for QM?
• What is this new paradigm?
• Example application of the new paradigm
AAPM Summer School 20113Saiful Huq - New Paradigms for QM in RT
Disclaimer
• Data presented here has not yet been approved by the Therapy Physics Committee of the AAPM and thus does not have official AAPM endorsement
AAPM Summer School 20114Saiful Huq - New Paradigms for QM in RT
What is on a cancer patient’s mind?
• Safety
• Radiation therapy accident article published in NY Times
AAPM Summer School 20115Saiful Huq - New Paradigms for QM in RT
Listen to this story ……. January 24, 2010
AAPM Summer School 20116Saiful Huq - New Paradigms for QM in RT
The Radiation BoomRadiation Offers New Cures, and Ways to Do Harm
Sunday, January 24, 2010
Scott Jerome-Parks
Saiful Huq - New Paradigms for QM in RT AAPM Summer School 20116
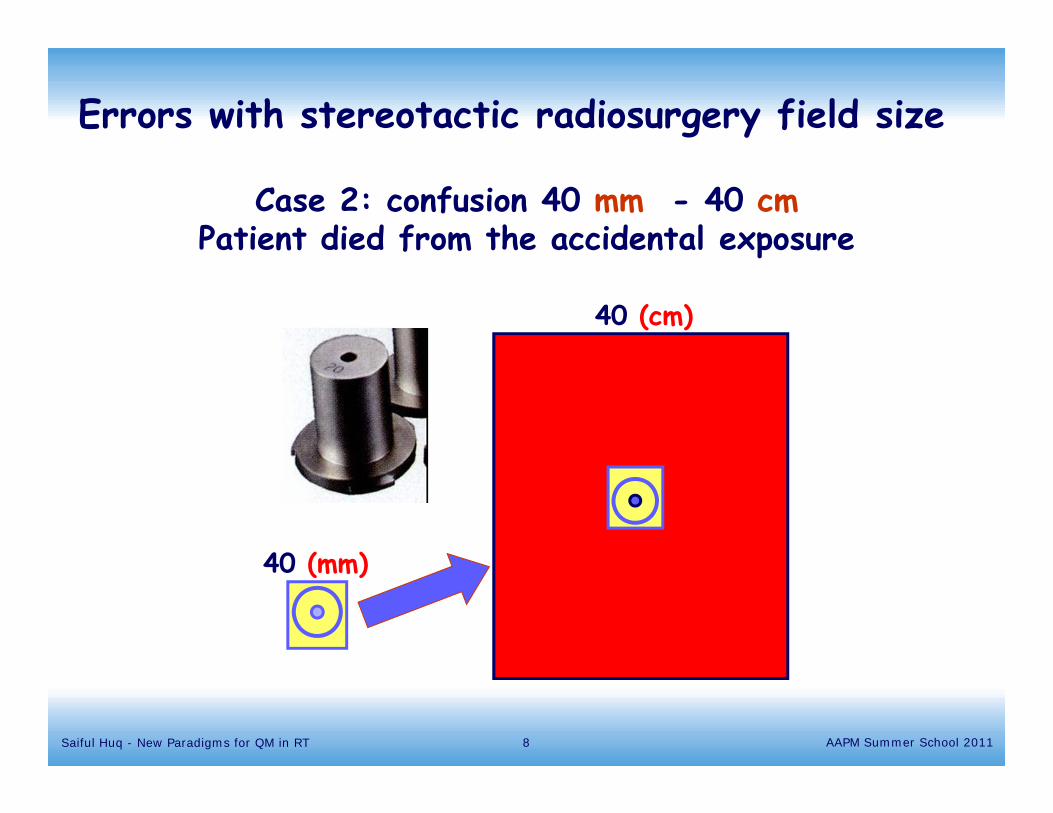
Case 2: confusion 40 mm - 40 cmPatient died from the accidental exposure
40 (mm)
40 (cm)
Errors with stereotactic radiosurgery field size
Saiful Huq - New Paradigms for QM in RT AAPM Summer School 20118
Can current QM standards prevent such events and meet the safety standards of new clinical
challenges?
Failure of QM:
• Insignificant errors in dose to the target
• Major events that can injure or kill patients
Main goal of QM:
• Patients will receive the prescribed treatment correctly
AAPM Summer School 20119Saiful Huq - New Paradigms for QM in RT
Current quality management standards and their focus
• Focus of current QM/QA guidelines measure functional performances of radiotherapy equipment by
measurable parameters set tolerances at desirable but achievable values
• QA/QC programs are prescriptive
• Example: AAPM TG-40, TG-142 recommendations
AAPM Summer School 201110Saiful Huq - New Paradigms for QM in RT
Examples of current QA paradigms: annual calibration of linac
that is it could have been spent checking things with a higher likelihood of failure
• The annual QA takes several days to complete
• If everything checks out, the effort was mostly wasted
• If some problem was found, how long had it been wrong?
• If the problem was significant then a daily check should be in place to prevent it
AAPM Summer School 201111Saiful Huq - New Paradigms for QM in RT
Example: IMRT QA
• This is certainly something that we would want to have correct
• We measure fluence maps for IMRT QA
AAPM Summer School 201112Saiful Huq - New Paradigms for QM in RT
• However, if the system has been commissioned, and then used correctly, why would this be wrong for the patient?
• If you worry about the leaf movement, even if the fluence map indicates correct movement for the first day of treatment, why do you think it might be correct in a week?
• Are there problems found this way? Almost never
• Do need QA for leaf movement, maybe daily
AAPM Summer School 201113Saiful Huq - New Paradigms for QM in RT
• What do we do? Find another location that satisfies the test criteria
• Do we make a patient go repeat planning because the test results did not satisfy the acceptable criteria?
• Why do we do this?
AAPM Summer School 201114Saiful Huq - New Paradigms for QM in RTSaiful Huq - New Paradigms for QM in RT
Problems with current QA paradigm
• These examples suggest that QA as performed currently might not be the optimal use of a physicist’s time
• Just performing all the recommended QA might not provide protection against events
AAPM Summer School 201115Saiful Huq - New Paradigms for QM in RT
The problem
• Lack of adequate guidance for resource allocation The premise: If it can be checked, check it That is…..everything
• RT QA guidance is focused on equipment performance even though most RT events have resulted from human performance failures rather than equipment failure
• Lack of adequate personnel
AAPM Summer School 201116Saiful Huq - New Paradigms for QM in RT
The problem
• Pressure on medical physicists to implement new technologies
• Lack of guidance on how to implement these technologies
• Delays in publishing QA protocols for emerging technologies
AAPM Summer School 201117Saiful Huq - New Paradigms for QM in RT
Where are the resources and time to do it all?
What should a time starved physicist do?
What to Do?
18Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
2008
2008
2009
Recent reports
19Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
2000
How safe is safe: Risk in radiotherapy (RT)
Ford and Terezakis; Red Journal 78, 321-322, 2010
• Rate of serious injury in RT is 1000 times higher
• Rate of misadministration in RT is 0.2 % ( 1 in 600)
• Rate of serious injury: airline accidents is 1 in 10 million
16,000 times lower than that of RT
• In reality no one knows
• Risk profiles of anesthesia: similar to airline industry
20Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
• As technology & processes change Retrospective approaches are not
sufficient All-inclusive QC checks may not be
feasible Develop proactive approaches to
anticipation of failure modes Evaluate risks from each failure mode
ICRP 112 Conclusions and recommendations
21Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Prospective risk assessment
• Before introducing a new technology or technique figure out, through a formal process, what could go wrong and what the consequences might be
22Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Application of risk-based analysis methods to radiotherapy quality management
AAPM’s TG 100
• Charge Identify a structured QA program approach that balances
patient safety and quality versus resources commonly available and strike a good balance between prescriptiveness and flexibility
After the identification of the hazard analysis for broad classes of radiotherapy develop the framework of the QA program
23Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
ICRP 112 definition of risk
• “Risk can be regarded as some function of the probability of an event’s occurring and the severity of the consequences for the patient should the event occur”
24Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Risk assessment
• Many risk assessment and analysis tools/techniques exist in industry
• These tools can be easily adapted to RT to enhance safety and quality of treatment process
• Risk assessment is the process of analyzing the hazards involved in a process
• TG100 used some of these tools to develop new guidelines for RT QM
25Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
TG100 risk analysis methodology
Use IMRT as a case study
• FMEA (Failure Modes and Effects Analysis)
• Fault Tree Analysis
• Process Mapping (Tree)
• Establishment of a risk based QM program
26Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Process Tree
• Visual illustration of the physical and temporal relationships between the different steps of a process that demonstrates the flow of these steps from process start to process end
TG100 risk analysis methodology
27Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011

Patient database information entered
Immobilization and positioning
CT simulation
Other pre-treatment imaging
Transfer images and other DICOM data
Initial treatment planning directive
RTP anatomy contouring
Treatment planning
Plan approval
Plan preparation
Initial tx(Day 1)
Subsequent tx(Day N)
End of txStart of tx
Example: IMRT process tree
28Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
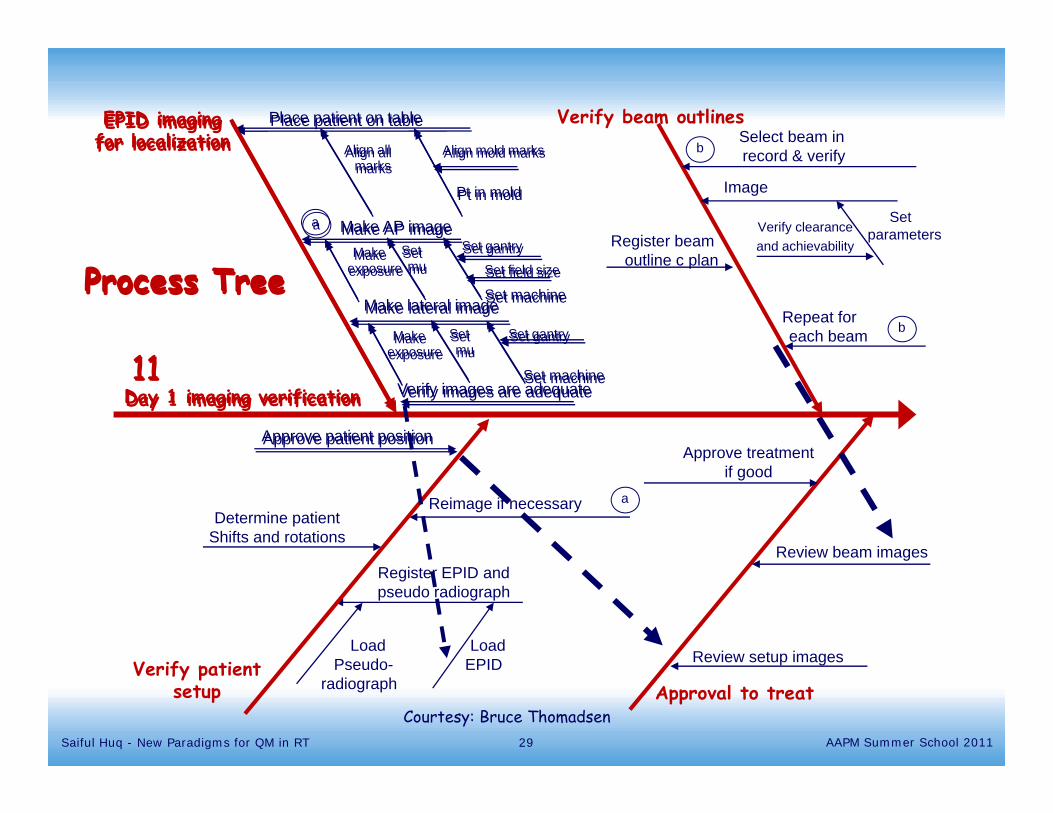
Verify patientsetup
Register EPID andpseudo radiograph
LoadEPID
LoadPseudo-
radiograph
Determine patientShifts and rotations
Reimage if necessary a
Verify beam outlinesSelect beam in record & verify
Image
SetparametersVerify clearance
and achievabilityRegister beamoutline c plan
Repeat for each beam b
b
Approval to treat
Review setup images
Review beam images
Approve treatmentif good
Day 1 imaging verification
EPID imagingfor localization
Place patient on table
Align mold marks
Pt in mold
Align allmarks
Make AP imageSetmu
Set gantryMakeexposure Set field size
Set machineMake lateral image
Setmu
Set gantryMakeexposure
Set machineVerify images are adequate
Approve patient position
a
11
Process Tree
Day 1 imaging verification
EPID imagingfor localization
Place patient on table
Align mold marks
Pt in mold
Align allmarks
Make AP imageSetmu
Set gantryMakeexposure Set field size
Set machineMake lateral image
Setmu
Set gantryMakeexposure
Set machineVerify images are adequate
Approve patient position
a
11
Process Tree
Courtesy: Bruce Thomadsen29Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011

Day 1 imaging verification
EPID imagingfor localization
Place patient on table
Align mold marks
Pt in mold
Align allmarks
Make AP imageSet
muSet gantryMake
exposure Set field size
Set machineMake lateral image
Setmu
Set gantryMakeexposure
Set machineVerify images are adequate
Verify patientsetup
Register EPID andpseudo radiograph
LoadEPID
LoadPseudo-
radiograph
Determine patientShifts and rotations
Reimage if necessary
Approve patient position
a
a
Verify beam outlinesSelect beam in record & verify
Image
SetparametersVerify clearance
and achievabilityRegister beamoutline c plan
Repeat for each beam b
b
Approval to treat
Review setup images
Review beam images
Approve treatmentif good
11
Process Tree
Courtesy: Bruce Thomadsen30Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
FMEA
• Assess potential risks involved in the process
• FMEA assesses the likely hood of errors in a process and considers the effects of such error
TG100 risk analysis methodology
31Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
IMRT failure modes and effects analysis
What could possibly go wrong (potential failure mode)
How could that happen (what are the causes that result in a failure mode)
What effects would such a failure produce (potential effects of failure)
The overall risk of each identified failure mode is then scored and prioritized according to RPN
A good FMEA then identifies corrective actions to prevent failure from reaching the patient
• FMEA looks at each process and at each step asks the questions:
32Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
• First day of Tx: Patient maybe positioned incorrectly relative to the isocenter
Example of FMEAFailure mode:
• Tx machine or simulator laser misalignment• Therapist error due to inattention• Poor instruction or setup documentation in the chart• Inadequate immobilization• Organ motion or tumor growth
Causes of failure:
• The magnitude of the displacement from planned isocenter• Tx technique (stereotactic, 3D conformal or large fields)• Proximity of critical structures and when in the course of tx the
error was detected
Consequences: severity depends on:
33Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Steps to perform a quantitative FMEA
• Identify all of the potential causes for each FM
• Determine the impact of each FM on the outcome of the process
• Identify all possible failure modes (FM)
• Establish a risk based QM program
34Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
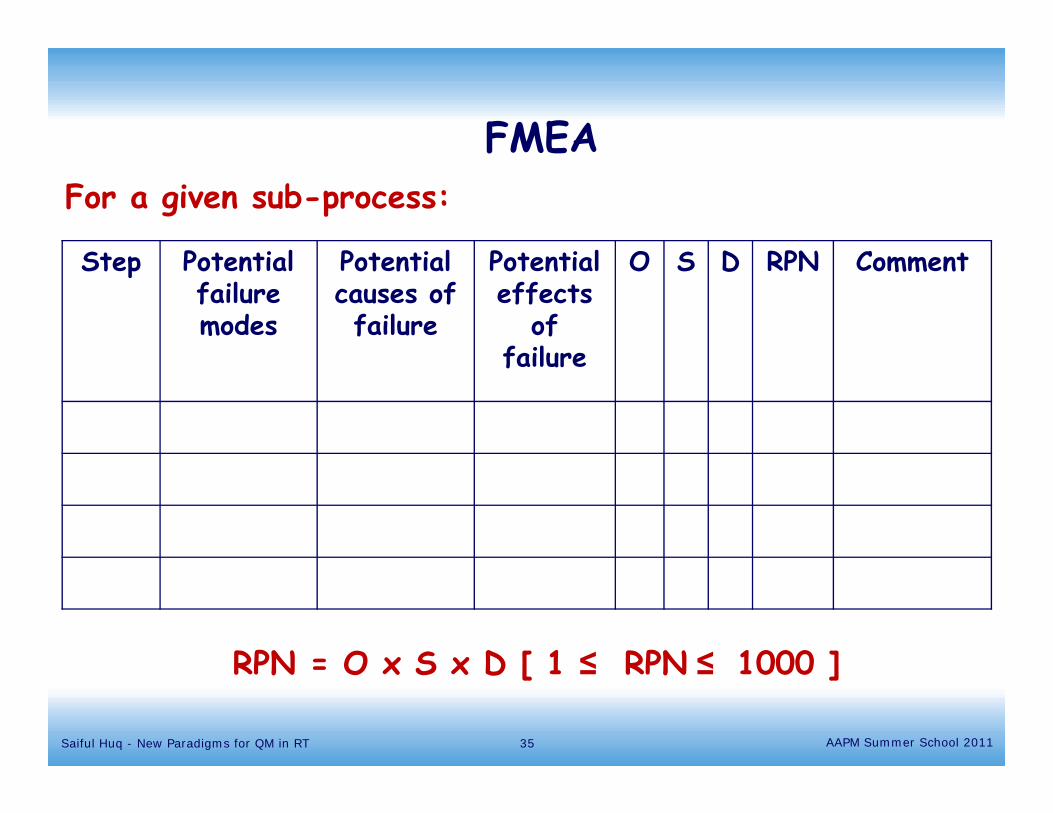
Step Potential failure modes
Potential causes of failure
Potential effects
of failure
O S D RPN Comment
FMEAFor a given sub-process:
RPN = O x S x D [ 1 ≤ RPN ≤ 1000 ]
AAPM Summer School 2011Saiful Huq - New Paradigms for QM in RT 35
What are O, S and D’s?
• O : Probability that a specific cause will result in a failure mode
• S: Severity of the effects resulting from a specific failure mode if it is not detected or corrected
• D: Probability that the failure will not be detected
• Risk priority number RPN = O*S*D
• For O, S and D one assigns values from 1 to 10.
• TG100 has developed scales for O,S, and D indices that are tied to radiotherapy outcomes and observations
36Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
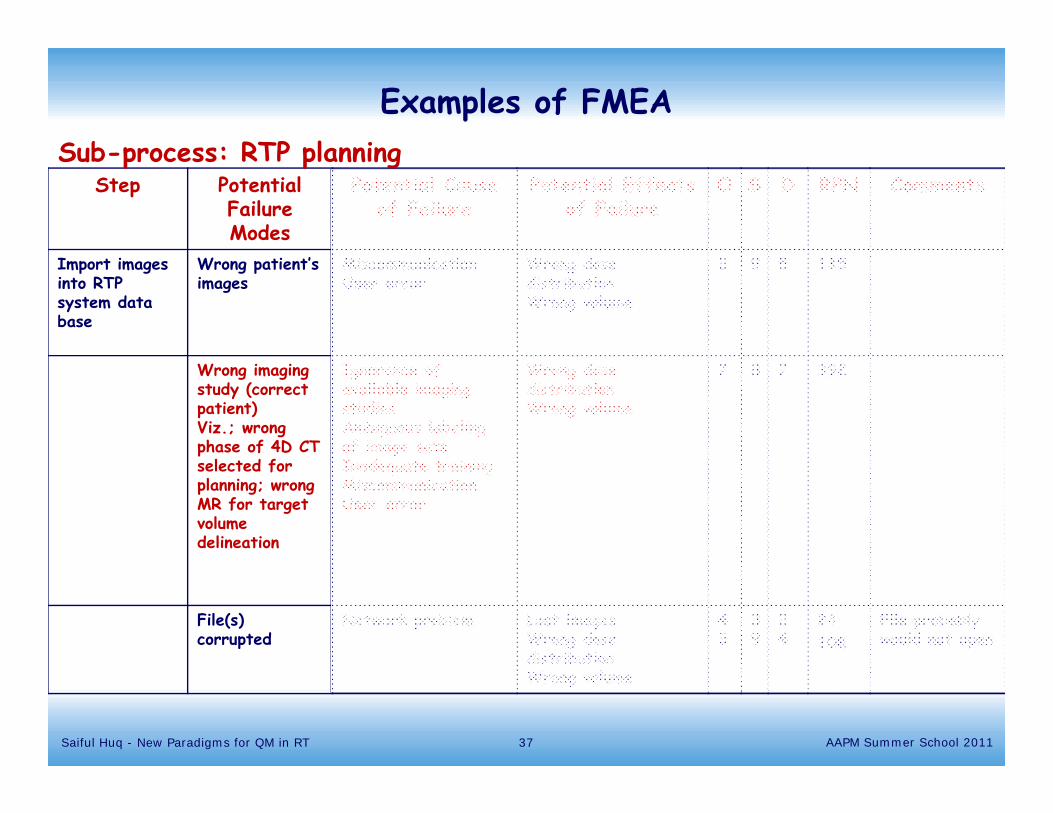
Examples of FMEA
Step Potential Failure Modes
Potential Cause of Failure
Potential Effects of Failure
O S D RPN Comments
Import images into RTP system data base
Wrong patient’s images
MiscommunicationUser error
Wrong dose distributionWrong volume
3 9 5 135
Wrong imaging study (correct patient)Viz.; wrong phase of 4D CT selected for planning; wrong MR for target volume delineation
Ignorance of available imaging studiesAmbiguous labeling of image setsInadequate training MiscommunicationUser error
Wrong dose distributionWrong volume
7 8 7 392
File(s) corrupted
Network problem Lost imagesWrong dose distributionWrong volume
43
39
24
24108
File probably would not open
Sub-process: RTP planning
37Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
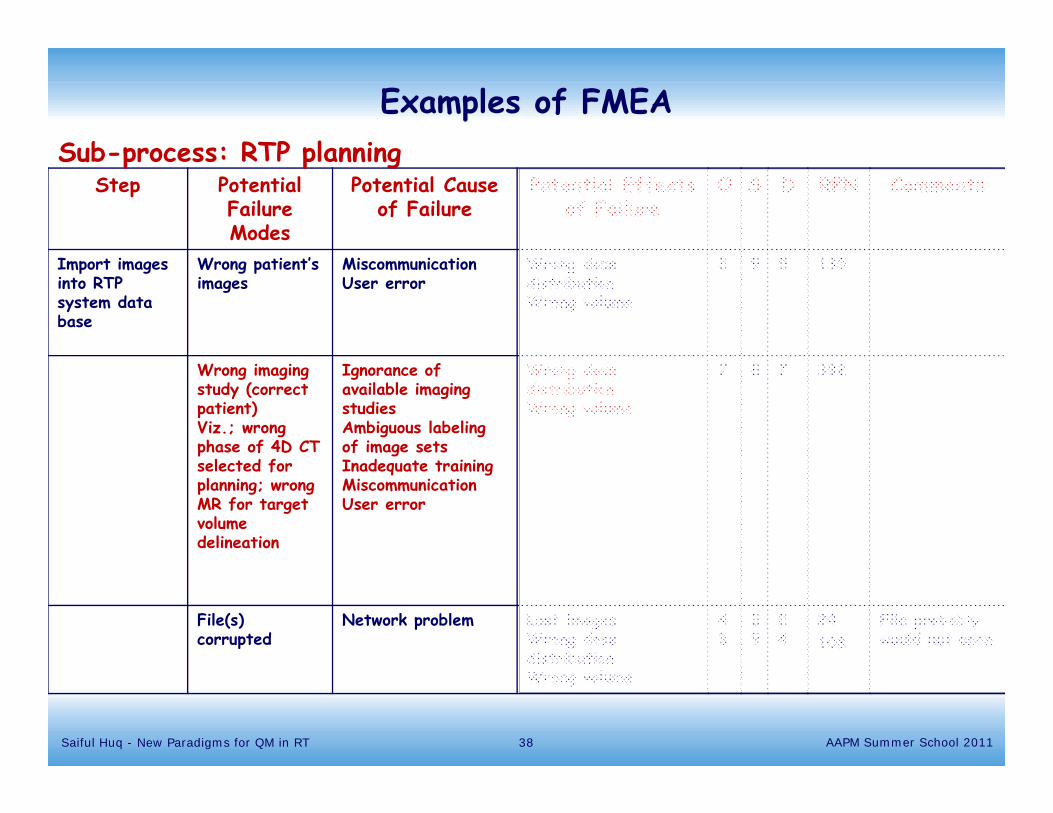
Examples of FMEA
Step Potential Failure Modes
Potential Cause of Failure
Potential Effects of Failure
O S D RPN Comments
Import images into RTP system data base
Wrong patient’s images
MiscommunicationUser error
Wrong dose distributionWrong volume
3 9 5 135
Wrong imaging study (correct patient)Viz.; wrong phase of 4D CT selected for planning; wrong MR for target volume delineation
Ignorance of available imaging studiesAmbiguous labeling of image setsInadequate training MiscommunicationUser error
Wrong dose distributionWrong volume
7 8 7 392
File(s) corrupted
Network problem Lost imagesWrong dose distributionWrong volume
43
39
24
24108
File probably would not open
Sub-process: RTP planning
38Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
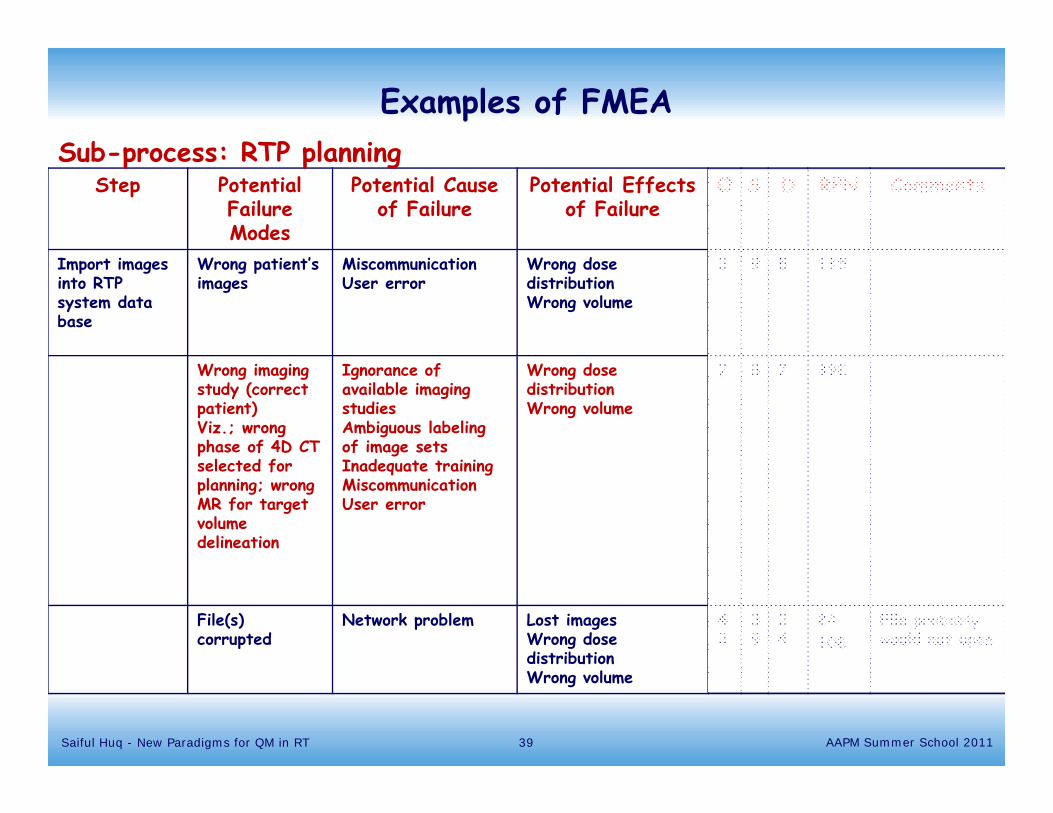
Examples of FMEA
Step Potential Failure Modes
Potential Cause of Failure
Potential Effects of Failure
O S D RPN Comments
Import images into RTP system data base
Wrong patient’s images
MiscommunicationUser error
Wrong dose distributionWrong volume
3 9 5 135
Wrong imaging study (correct patient)Viz.; wrong phase of 4D CT selected for planning; wrong MR for target volume delineation
Ignorance of available imaging studiesAmbiguous labeling of image setsInadequate training MiscommunicationUser error
Wrong dose distributionWrong volume
7 8 7 392
File(s) corrupted
Network problem Lost imagesWrong dose distributionWrong volume
43
39
24
24108
File probably would not open
Sub-process: RTP planning
39Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
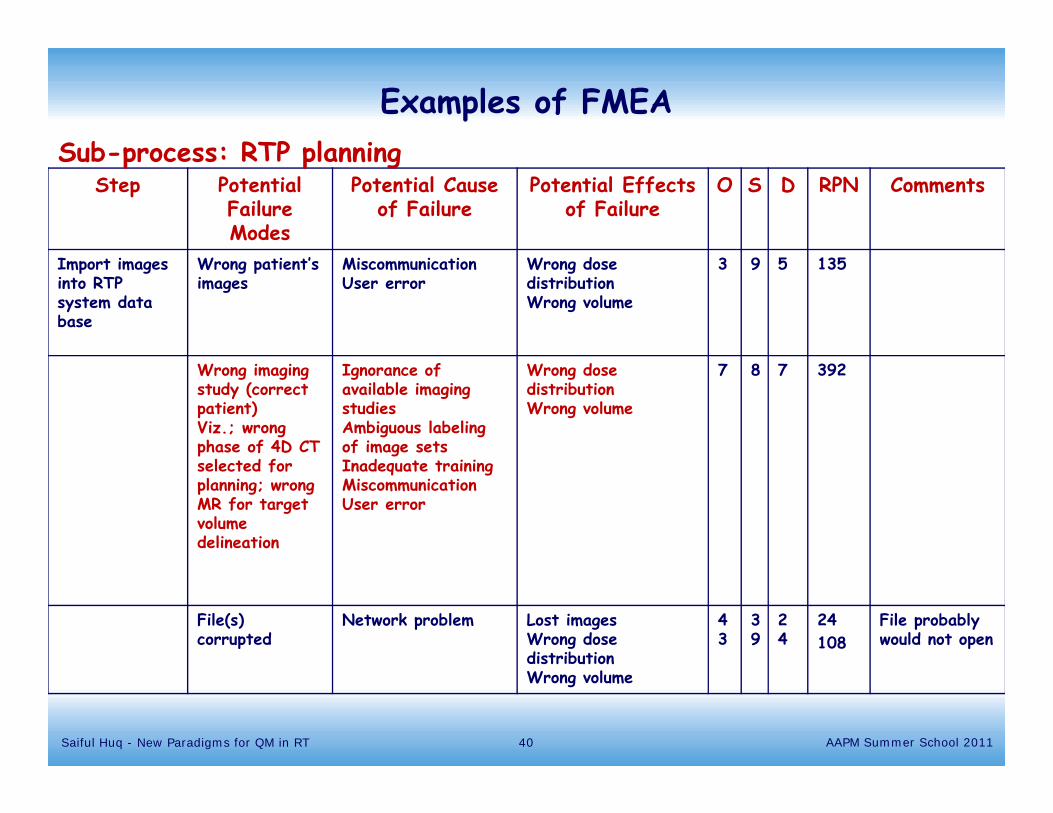
Examples of FMEA
Step Potential Failure Modes
Potential Cause of Failure
Potential Effects of Failure
O S D RPN Comments
Import images into RTP system data base
Wrong patient’s images
MiscommunicationUser error
Wrong dose distributionWrong volume
3 9 5 135
Wrong imaging study (correct patient)Viz.; wrong phase of 4D CT selected for planning; wrong MR for target volume delineation
Ignorance of available imaging studiesAmbiguous labeling of image setsInadequate training MiscommunicationUser error
Wrong dose distributionWrong volume
7 8 7 392
File(s) corrupted
Network problem Lost imagesWrong dose distributionWrong volume
43
39
24
24108
File probably would not open
Sub-process: RTP planning
40Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
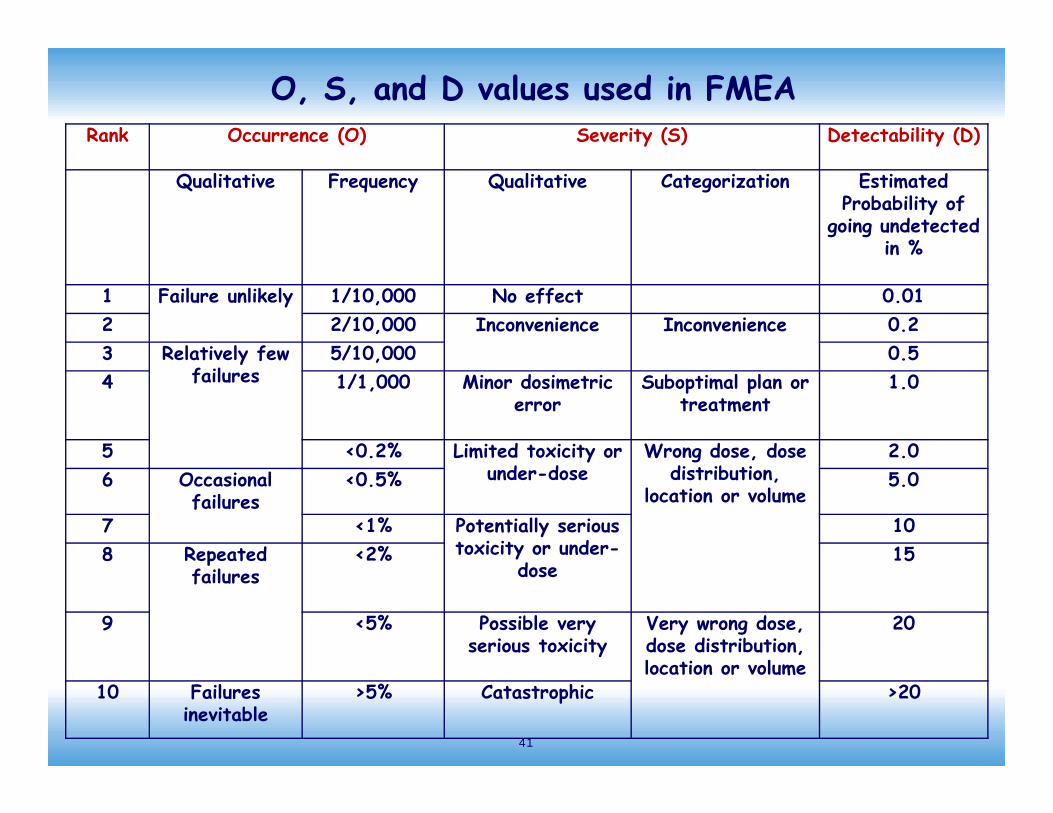
O, S, and D values used in FMEARank Occurrence (O) Severity (S) Detectability (D)
Qualitative Frequency Qualitative Categorization Estimated Probability of
going undetected in %
1 Failure unlikely 1/10,000 No effect 0.012 2/10,000 Inconvenience Inconvenience 0.23 Relatively few
failures5/10,000 0.5
4 1/1,000 Minor dosimetric error
Suboptimal plan or treatment
1.0
5 <0.2% Limited toxicity or under-dose
Wrong dose, dose distribution,
location or volume
2.06 Occasional
failures<0.5% 5.0
7 <1% Potentially serious toxicity or under-
dose
108 Repeated
failures<2% 15
9 <5% Possible very serious toxicity
Very wrong dose, dose distribution, location or volume
20
10 Failures inevitable
>5% Catastrophic >20
41
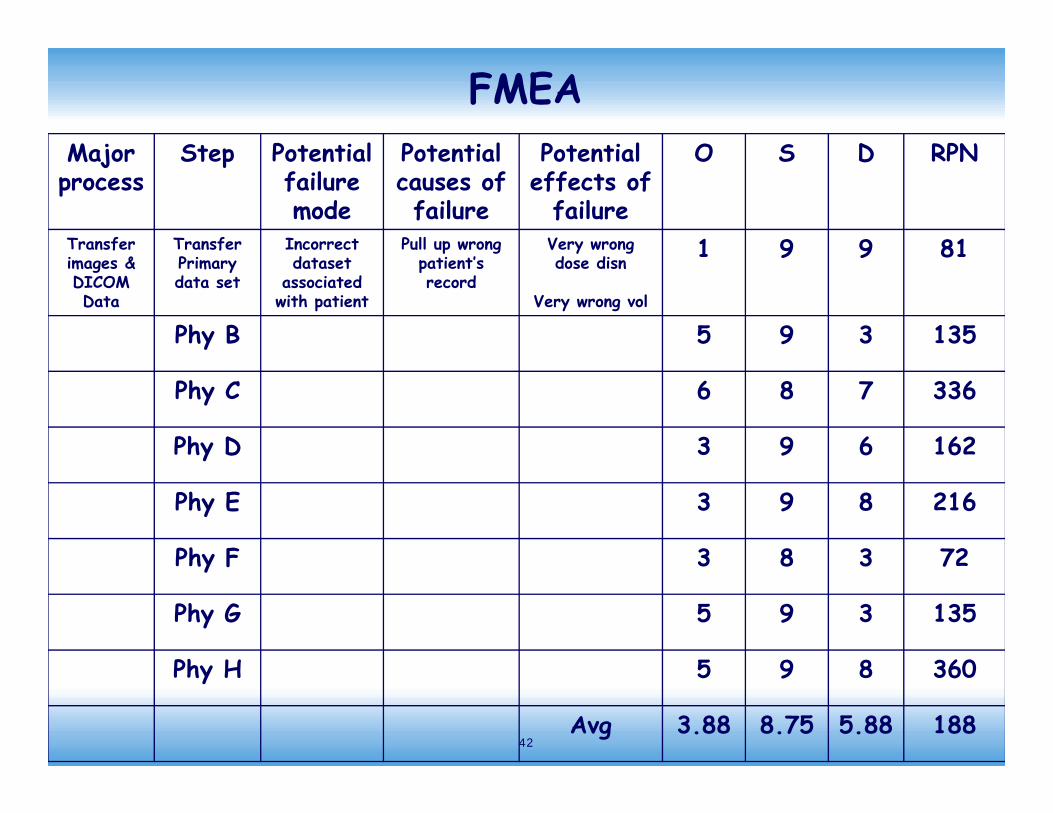
Major process
Step Potentialfailure mode
Potentialcauses of failure
Potential effects of
failure
O S D RPN
Transfer images & DICOM Data
Transfer Primary data set
Incorrect dataset
associated with patient
Pull up wrong patient’s record
Very wrong dose disn
Very wrong vol
1 9 9 81
Phy B 5 9 3 135
Phy C 6 8 7 336
Phy D 3 9 6 162
Phy E 3 9 8 216
Phy F 3 8 3 72
Phy G 5 9 3 135
Phy H 5 9 8 360
Avg 3.88 8.75 5.88 188
FMEA
42
FMEA results• 91 steps
• Individual RPNs ranged from 2 to 720
• Average RPNs ranged from 19 to 388. We designed our QM program based upon average RPN
• The top 20% of the failures had average RPN greater than 179
• 216 possible failure modes with many causes associated with them
43Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
FMEA- mark process map
• Shows if potential failures are uniformly distributed through the processes or clustered
• If clustered, should consider the major step as a hazard
• Prioritize the potential failure modes based on RPN and severity function
• Mark the highest rank steps on the process map
44Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
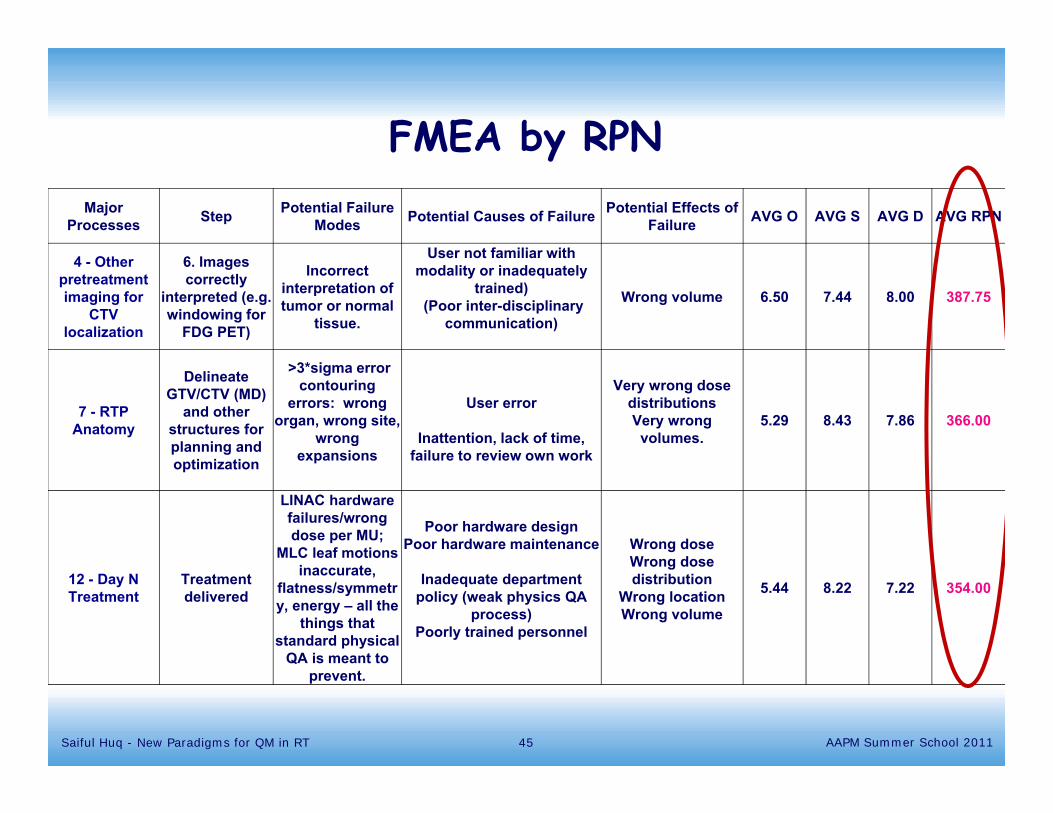
Major Processes Step Potential Failure
Modes Potential Causes of Failure Potential Effects of Failure AVG O AVG S AVG D AVG RPN
4 - Other pretreatment imaging for
CTV localization
6. Images correctly
interpreted (e.g. windowing for
FDG PET)
Incorrect interpretation of tumor or normal
tissue.
User not familiar with modality or inadequately
trained)(Poor inter-disciplinary
communication)
Wrong volume 6.50 7.44 8.00 387.75
7 - RTP Anatomy
Delineate GTV/CTV (MD)
and other structures for planning and optimization
>3*sigma error contouring
errors: wrong organ, wrong site,
wrong expansions
User error
Inattention, lack of time, failure to review own work
Very wrong dose distributionsVery wrong
volumes. 5.29 8.43 7.86 366.00
12 - Day N Treatment
Treatment delivered
LINAC hardware failures/wrong dose per MU;
MLC leaf motions inaccurate,
flatness/symmetry, energy – all the
things that standard physical
QA is meant to prevent.
Poor hardware design Poor hardware maintenance
Inadequate department policy (weak physics QA
process)Poorly trained personnel
Wrong dose Wrong dose distribution
Wrong locationWrong volume
5.44 8.22 7.22 354.00
FMEA by RPN
45Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
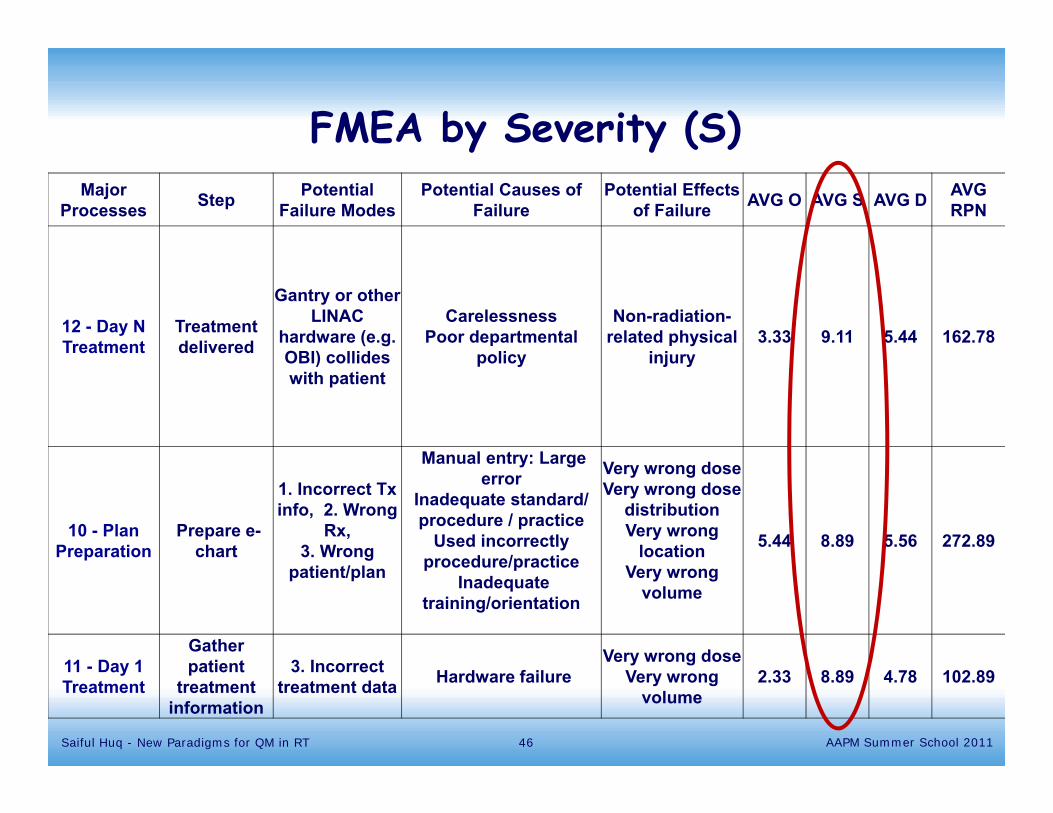
Major Processes Step Potential
Failure ModesPotential Causes of
FailurePotential Effects
of Failure AVG O AVG S AVG D AVG RPN
12 - Day N Treatment
Treatment delivered
Gantry or other LINAC
hardware (e.g. OBI) collides with patient
Carelessness Poor departmental
policy
Non-radiation-related physical
injury3.33 9.11 5.44 162.78
10 - Plan Preparation
Prepare e-chart
1. Incorrect Txinfo, 2. Wrong
Rx, 3. Wrong
patient/plan
Manual entry: Large error
Inadequate standard/ procedure / practice
Used incorrectly procedure/practice
Inadequate training/orientation
Very wrong dose Very wrong dose
distributionVery wrong
locationVery wrong
volume
5.44 8.89 5.56 272.89
11 - Day 1 Treatment
Gather patient
treatment information
3. Incorrect treatment data Hardware failure
Very wrong dose Very wrong
volume2.33 8.89 4.78 102.89
FMEA by Severity (S)
46Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
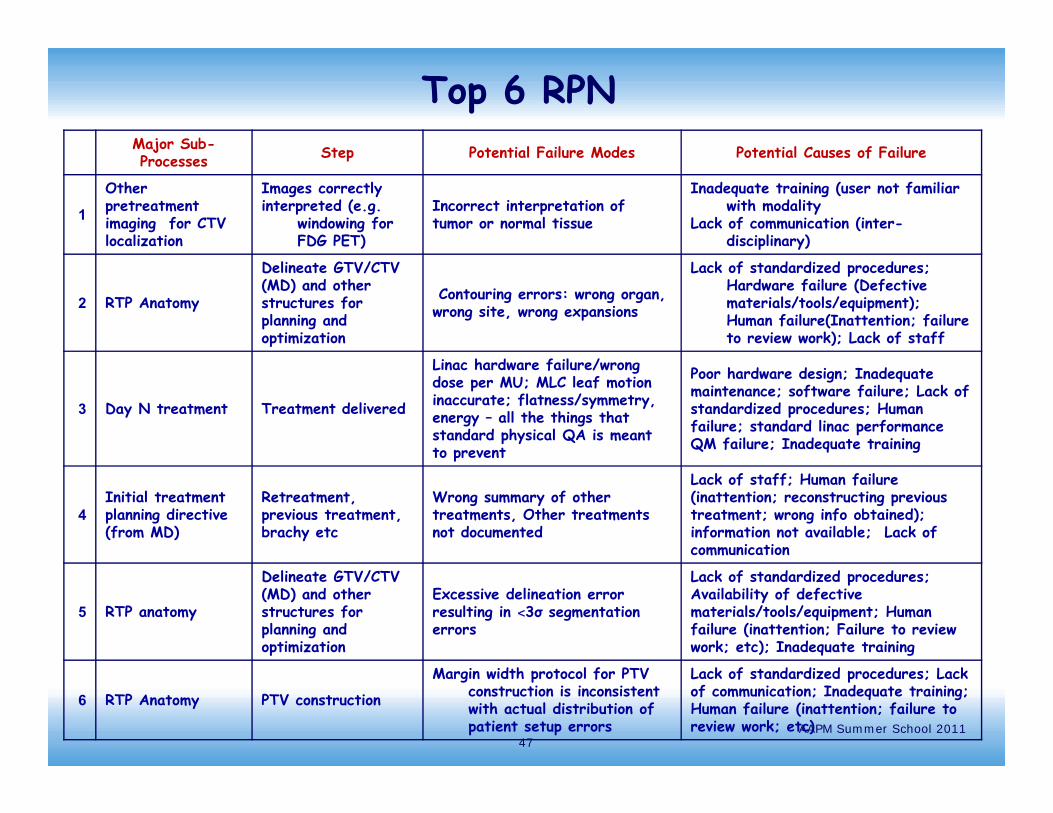
Top 6 RPNMajor Sub-Processes Step Potential Failure Modes Potential Causes of Failure
1
Other pretreatment imaging for CTV localization
Images correctlyinterpreted (e.g.
windowing for FDG PET)
Incorrect interpretation of tumor or normal tissue
Inadequate training (user not familiar with modality
Lack of communication (inter-disciplinary)
2 RTP Anatomy
Delineate GTV/CTV (MD) and other structures for planning and optimization
Contouring errors: wrong organ, wrong site, wrong expansions
Lack of standardized procedures; Hardware failure (Defective materials/tools/equipment); Human failure(Inattention; failure to review work); Lack of staff
3 Day N treatment Treatment delivered
Linac hardware failure/wrong dose per MU; MLC leaf motion inaccurate; flatness/symmetry, energy – all the things that standard physical QA is meant to prevent
Poor hardware design; Inadequate maintenance; software failure; Lack of standardized procedures; Human failure; standard linac performance QM failure; Inadequate training
4Initial treatment planning directive (from MD)
Retreatment, previous treatment, brachy etc
Wrong summary of other treatments, Other treatments not documented
Lack of staff; Human failure (inattention; reconstructing previous treatment; wrong info obtained); information not available; Lack of communication
5 RTP anatomy
Delineate GTV/CTV (MD) and other structures for planning and optimization
Excessive delineation error resulting in ˂3σ segmentation errors
Lack of standardized procedures; Availability of defective materials/tools/equipment; Human failure (inattention; Failure to review work; etc); Inadequate training
6 RTP Anatomy PTV construction
Margin width protocol for PTV construction is inconsistent with actual distribution of patient setup errors
Lack of standardized procedures; Lack of communication; Inadequate training; Human failure (inattention; failure to review work; etc)AAPM Summer School 2011
47
Successful treatment
Imaging and diagnosis
12 Subsequenttreatments
Chart filing
Immobilization equipment fabricated
Immobilization equipment documented,labeled, and stored
Immobilization forImaging study
Set up data documented
Time out
Positioning
Imaging (port films, CBCT, etc) 27
Documentation
Treatment 3
Treatment 3
Documentation
Immobilization equipment documented,labeled, and stored
Scheduling
Approveplan 7, 20
7 RTP anatomycontouring
1 Patient database information entered
Data into electronic Database 22
Data into written chart 22
Review of patient medical history
Immobilization equipment fabricated
Import and fuse images 16
MD: delineateGTV/CTV 2,5
PTV construction
Edit density map for artifacts
Delineate ROIs and planning structures
Indicate motion/uncertainty Management 13, 14
Specify registration goals 23, 38
Specify protocol for delineating target and structures 17
Specify images for target/structure delineation 11
Specify dose limits and goals 26
Suggest initial guidelines for treatment parameters
Enter prescriptionAnd planning constraints 18, 21, 45
Setup fields
Setup dose calc parameters
Optimization/Dose calculation 12, 31
Evaluate plan 10, 28
6 Initial treatmentplanning directive
8 Treatment planning
2 Immobilizationand positioning
3 CT simulation
9 Planapproval
11 Initial treatment
Patient Identified
Special Instructions (pacemakers, allergies, preps, etc.) 9
Account for previous treatmentsor chemotherapy 4
Motion management 8
Tx Unit operationand calibration 3Information on
Previous orconcomitant treatment 22
Protocol for delineationof targets 17
Patient ID
Treatment Site
Treatment settings
Imaging
Motion Management 8
Protocol for PTVMargin 6
Specify PTV Margin
Select Images 25
4D imaging correct 13
OptimizationROI 33, 44
Optimizationsettings 45
Treatment accessories 24
Boolean operations 29, 46
Changes noted 32, 34
Patient information 35
Monitor Pt/Tx 37, 43
Monitor Pt/Tx 37, 43
Specify ROI for optimization 19
Treatment settings
Positioning
Pt prep 35
Changes correct 40, 42Run leaf sequencer
Pt changes noted 42
Imaging Studies
Patient prepped (contrast, tattoos, BBs etc.)
Treatment accessories 24
4 Other imaging
Patient informedOf imaging requirements
Images Interpreted 1
Position patient
Make images
5 Transferimages
TransferOther datasets
Transfer CTDataset 41
Create case
4D representation
Save patient
Calculate doseto optimization pointsand dose distribution 12, 31
Heterogeneity correction 30
Evaluate leaf sequencer
Evaluate deliverysystem limitations
Complete formalprescription 36
Manual data entry and plan modification 39
Specify treatment course
Delivery protocols
Scheduling
Automatic data entry and plan modification
Prepare DRR and other images
Check version ofplan and patient ID
Annotate localization anatomy
Order fields
Prepare paper chart
Prepare electronic chart 15
Transfer patient data to treatment delivery 15
Define localization imaging
10 Planpreparation
Enter demographics
Patient PositionRecorded in database
Patient information
Tx Unit operationand calibration 3
Process tree (map) I wouldn’t try to read it…will hurt your eyes
48Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Successful treatment
Imaging and diagnosis
12 Subsequenttreatments
Chart filing
Immobilization equipment fabricated
Immobilization equipment documented,labeled, and stored
Immobilization forImaging study
Set up data documented
Time out
Positioning
Imaging (port films, CBCT, etc) 27
Documentation
Treatment 3
Treatment 3
Documentation
Immobilization equipment documented,labeled, and stored
Scheduling
Approveplan 7, 20
7 RTP anatomycontouring
1 Patient database information entered
Data into electronic Database 22
Data into written chart 22
Review of patient medical history
Immobilization equipment fabricated
Import and fuse images 16
MD: delineateGTV/CTV 2,5
PTV construction
Edit density map for artifacts
Delineate ROIs and planning structures
Indicate motion/uncertainty Management 13, 14
Specify registration goals 23, 38
Specify protocol for delineating target and structures 17
Specify images for target/structure delineation 11
Specify dose limits and goals 26
Suggest initial guidelines for treatment parameters
Enter prescriptionAnd planning constraints 18, 21, 45
Setup fields
Setup dose calc parameters
Optimization/Dose calculation 12, 31
Evaluate plan 10, 28
6 Initial treatmentplanning directive
8 Treatment planning
2 Immobilizationand positioning
3 CT simulation
9 Planapproval
11 Initial treatment
Patient Identified
Special Instructions (pacemakers, allergies, preps, etc.) 9
Account for previous treatmentsor chemotherapy 4
Motion management 8
Tx Unit operationand calibration 3Information on
Previous orconcomitant treatment 22
Protocol for delineationof targets 17
Patient ID
Treatment Site
Treatment settings
Imaging
Motion Management 8
Protocol for PTVMargin 6
Specify PTV Margin
Select Images 25
4D imaging correct 13
OptimizationROI 33, 44
Optimizationsettings 45
Treatment accessories 24
Boolean operations 29, 46
Changes noted 32, 34
Patient information 35
Monitor Pt/Tx 37, 43
Monitor Pt/Tx 37, 43
Specify ROI for optimization 19
Treatment settings
Positioning
Pt prep 35
Changes correct 40, 42Run leaf sequencer
Pt changes noted 42
Imaging Studies
Patient prepped (contrast, tattoos, BBs etc.)
Treatment accessories 24
4 Other imaging
Patient informedOf imaging requirements
Images Interpreted 1
Position patient
Make images
5 Transferimages
TransferOther datasets
Transfer CTDataset 41
Create case
4D representation
Save patient
Calculate doseto optimization pointsand dose distribution 12, 31
Heterogeneity correction 30
Evaluate leaf sequencer
Evaluate deliverysystem limitations
Complete formalprescription 36
Manual data entry and plan modification 39
Specify treatment course
Delivery protocols
Scheduling
Automatic data entry and plan modification
Prepare DRR and other images
Check version ofplan and patient ID
Annotate localization anatomy
Order fields
Prepare paper chart
Prepare electronic chart 15
Transfer patient data to treatment delivery 15
Define localization imaging
10 Planpreparation
Enter demographics
Patient PositionRecorded in database
Patient information
Tx Unit operationand calibration 3
Process tree (map) I wouldn’t try to read it…will hurt your eyes
49Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Successful treatment
Imaging and diagnosis
12 Subsequenttreatments
Chart filing
Immobilization equipment fabricated
Immobilization equipment documented,labeled, and stored
Immobilization forImaging study
Set up data documented
Time out
Positioning
Imaging (port films, CBCT, etc) 27
Documentation
Treatment 3
Treatment 3
Documentation
Immobilization equipment documented,labeled, and stored
Scheduling
Approveplan 7, 20
7 RTP anatomycontouring
1 Patient database information entered
Data into electronic Database 22
Data into written chart 22
Review of patient medical history
Immobilization equipment fabricated
Import and fuse images 16
MD: delineateGTV/CTV 2,5
PTV construction
Edit density map for artifacts
Delineate ROIs and planning structures
Indicate motion/uncertainty Management 13, 14
Specify registration goals 23, 38
Specify protocol for delineating target and structures 17
Specify images for target/structure delineation 11
Specify dose limits and goals 26
Suggest initial guidelines for treatment parameters
Enter prescriptionAnd planning constraints 18, 21, 45
Setup fields
Setup dose calc parameters
Optimization/Dose calculation 12, 31
Evaluate plan 10, 28
6 Initial treatmentplanning directive
8 Treatment planning
2 Immobilizationand positioning
3 CT simulation
9 Planapproval
11 Initial treatment
Patient Identified
Special Instructions (pacemakers, allergies, preps, etc.) 9
Account for previous treatmentsor chemotherapy 4
Motion management 8
Tx Unit operationand calibration 3Information on
Previous orconcomitant treatment 22
Protocol for delineationof targets 17
Patient ID
Treatment Site
Treatment settings
Imaging
Motion Management 8
Protocol for PTVMargin 6
Specify PTV Margin
Select Images 25
4D imaging correct 13
OptimizationROI 33, 44
Optimizationsettings 45
Treatment accessories 24
Boolean operations 29, 46
Changes noted 32, 34
Patient information 35
Monitor Pt/Tx 37, 43
Monitor Pt/Tx 37, 43
Specify ROI for optimization 19
Treatment settings
Positioning
Pt prep 35
Changes correct 40, 42Run leaf sequencer
Pt changes noted 42
Imaging Studies
Patient prepped (contrast, tattoos, BBs etc.)
Treatment accessories 24
4 Other imaging
Patient informedOf imaging requirements
Images Interpreted 1
Position patient
Make images
5 Transferimages
TransferOther datasets
Transfer CTDataset 41
Create case
4D representation
Save patient
Calculate doseto optimization pointsand dose distribution 12, 31
Heterogeneity correction 30
Evaluate leaf sequencer
Evaluate deliverysystem limitations
Complete formalprescription 36
Manual data entry and plan modification 39
Specify treatment course
Delivery protocols
Scheduling
Automatic data entry and plan modification
Prepare DRR and other images
Check version ofplan and patient ID
Annotate localization anatomy
Order fields
Prepare paper chart
Prepare electronic chart 15
Transfer patient data to treatment delivery 15
Define localization imaging
10 Planpreparation
Enter demographics
Patient PositionRecorded in database
Patient information
Tx Unit operationand calibration 3
Process map marking I wouldn’t try to read it…will hurt your eyes
50Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Fault tree
• FMEA helps lay out the fault tree
• Fault tree helps an individual or a dept see which steps in their practice are not covered by QM and visualize potential locations for effective QM measures
• The RPN and S values direct attention to the errors most in need of remedy
• Every step needs some QM to block the effects of failure from affecting the patient
51Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Errorin data
Errorin QC
Error in data input
Errorin QC
Error in Calculation algorithm
Errorin QC
Error in prescription
Errorin QC
Error in calculation
Errorin QA
Error in Calculated value for patient
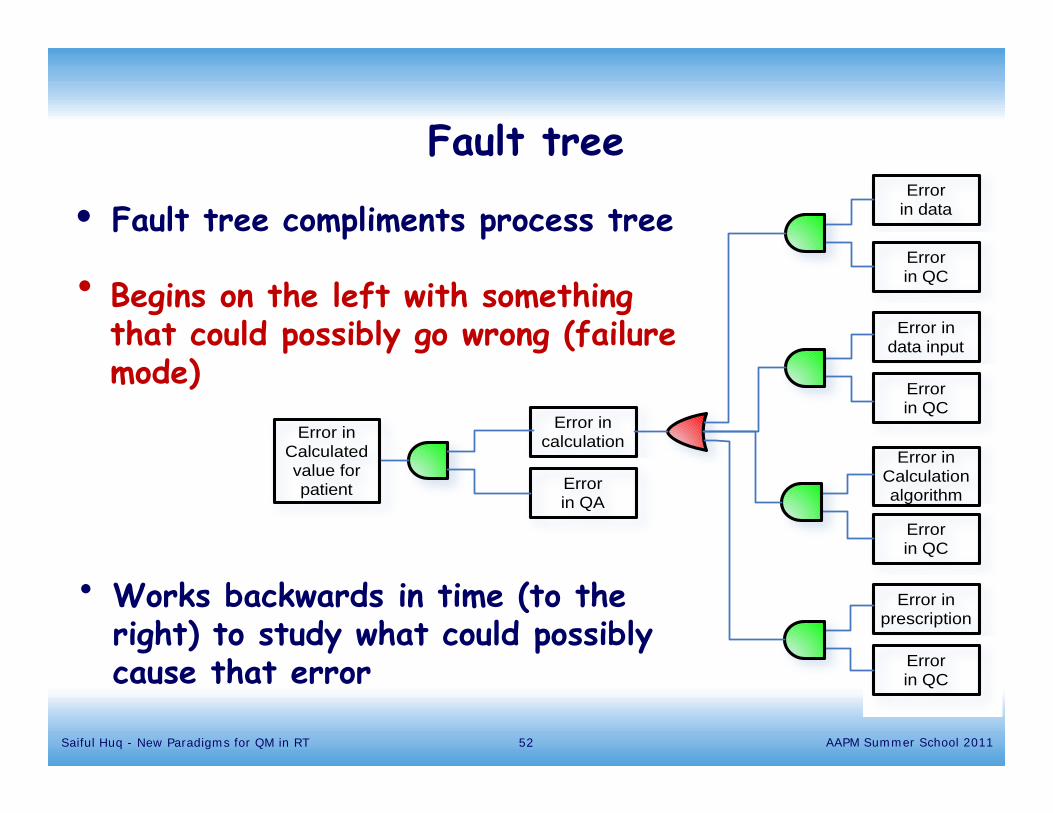
• Fault tree compliments process tree
• Begins on the left with something that could possibly go wrong (failure mode)
• Works backwards in time (to the right) to study what could possibly cause that error
Fault tree
52Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
TG10053Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011

M. Saiful Huq – Recommendations of TG100 54
Human failure18%
Lack of standardized procedures
18%Inadequate
training15%
Inadequate resources
13%
Hardware/software failures
13%
Lack of communication
11%
Design failure4%
Commissioning 4%
Others4%
Causes of failure
Rocky Mountain Chapter meeting Feb 6, 2010
Most commonly cited causes of high risk
failures
• Human factors Inadequate training Miscommunication within and between departments
• Lack of consistent procedural guidelines• Lack of attention by people performing task• Time pressure• People as well as linacs, need to be “commissioned”
55Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Training Program !!
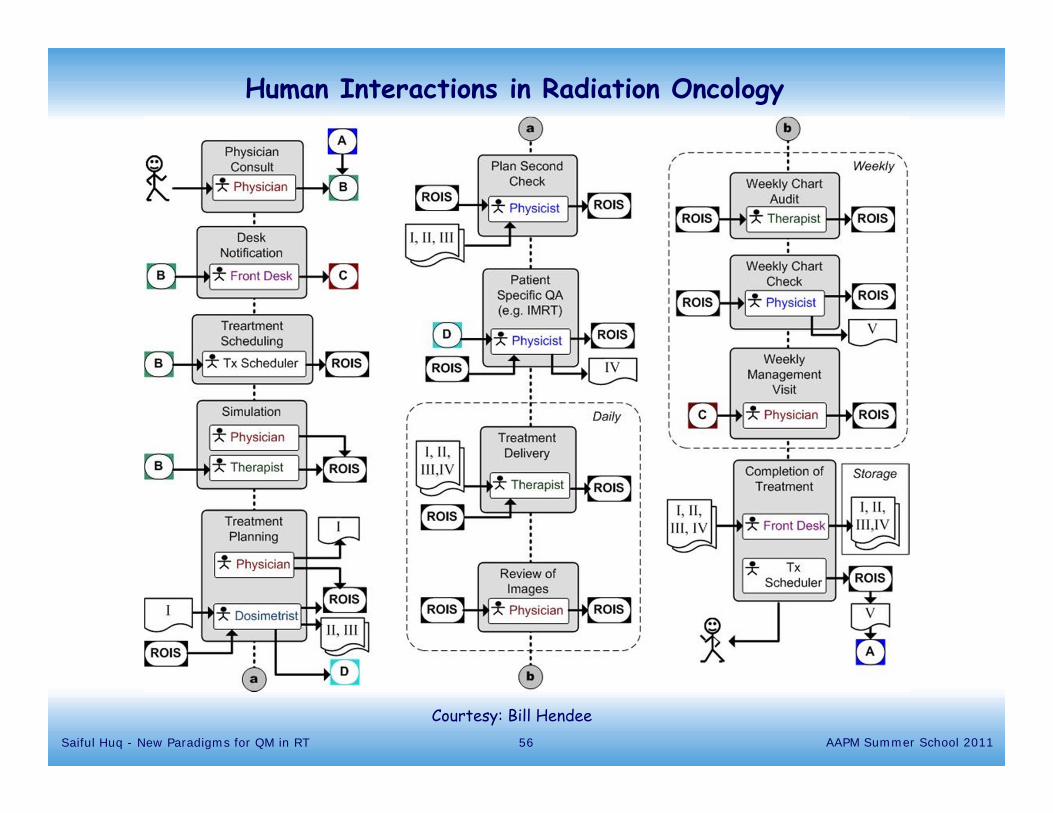
Human Interactions in Radiation Oncology
Courtesy: Bill Hendee56Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Design of QM program
• Use the FTA and FMEA risk and process oriented information to design a QM program for the process being investigated
• Example Sub-process: RTP anatomy Step: Delineate GTV/CTV and other structures FM: › 3σ contouring error, wrong organ, site, or expansions RPN = 366 Rank: #2
57Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
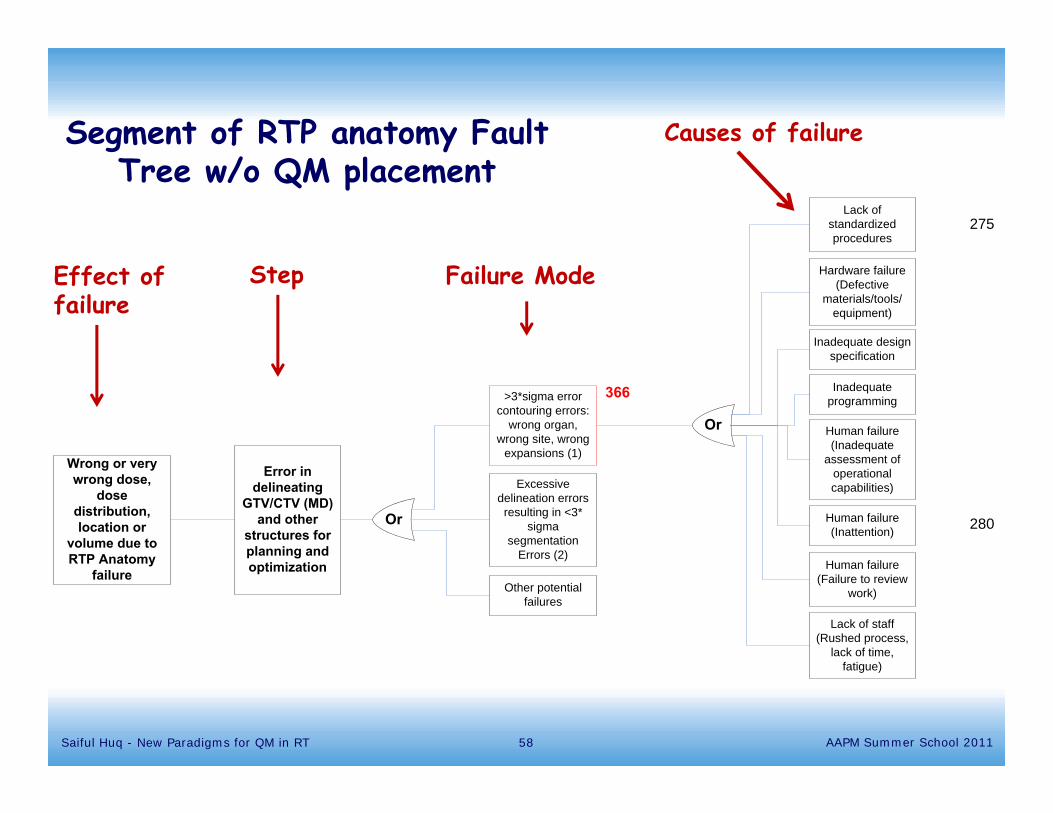
Or
Error in delineating
GTV/CTV (MD) and other
structures for planning and optimization
>3*sigma error contouring errors:
wrong organ, wrong site, wrong
expansions (1)
Lack of standardized procedures
Hardware failure (Defective
materials/tools/equipment)
Inadequate design specification
Human failure (Inadequate
assessment of operational capabilities)
Inadequate programming
Lack of staff (Rushed process,
lack of time, fatigue)
Excessive delineation errors resulting in <3*
sigma segmentation
Errors (2)
Other potential failures
Or
Wrong or very wrong dose,
dose distribution, location or
volume due to RTP Anatomy
failure
275
280Human failure (Inattention)
Human failure (Failure to review
work)
366
Segment of RTP anatomy Fault Tree w/o QM placement
Step Failure Mode
Causes of failure
Effect of failure
58Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
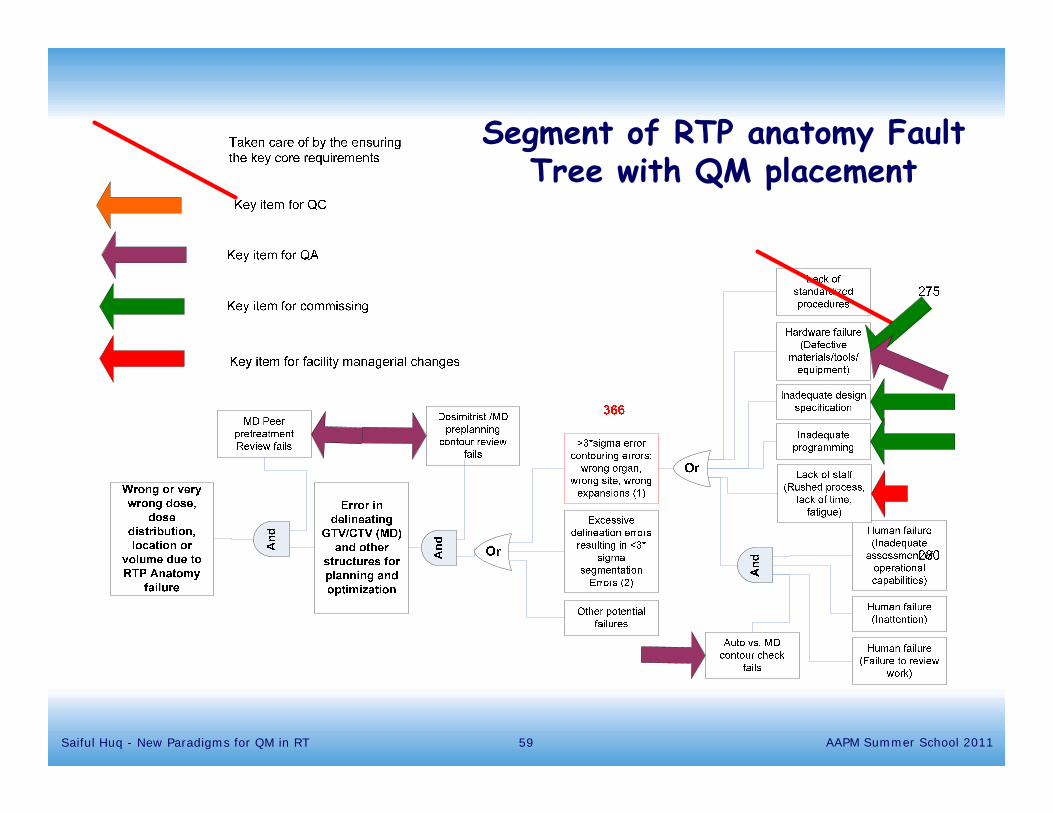
Segment of RTP anatomy Fault Tree with QM placement
59Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
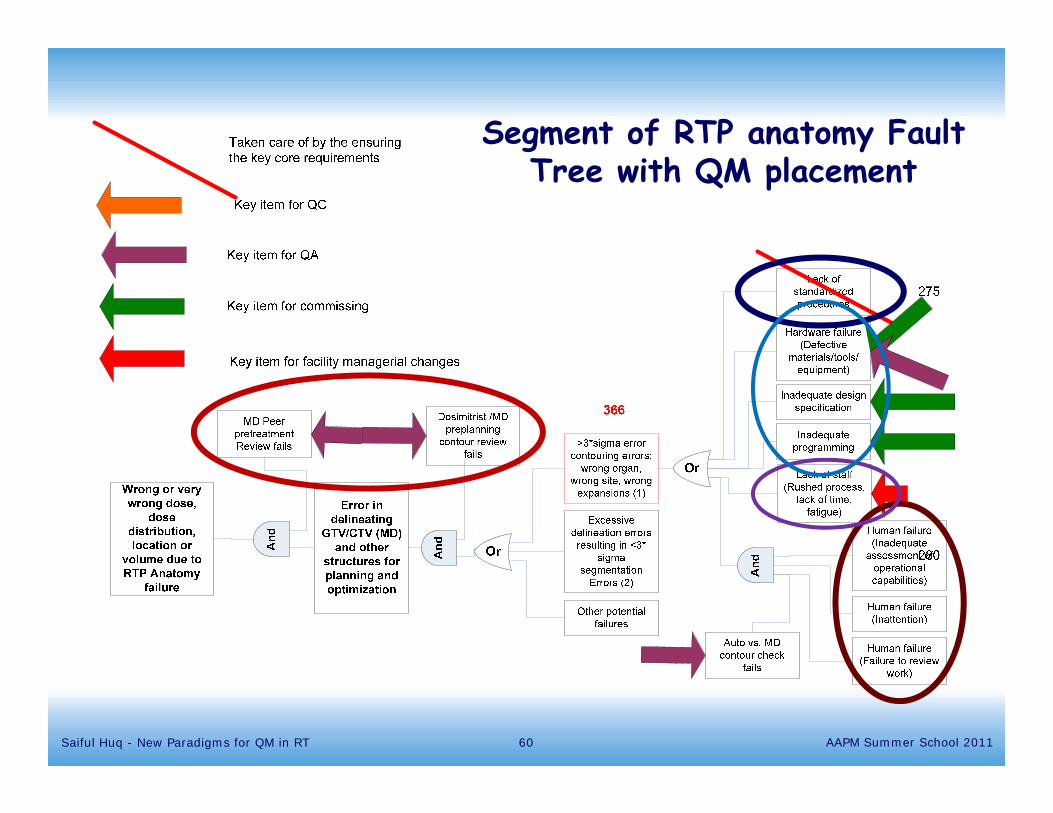
Segment of RTP anatomy Fault Tree with QM placement
60Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Challenges in the implementation of new QM paradigm
• Performing the FMEA analyses require skills gained from experience in such analysis
• Large institutions may have the resources to go through this, but a small, community hospital will not
• That being said, the greatest advantage is to analyze your situation
61Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Guidance to clinical physicists
• Each facility should consider its own needs for addressing potentially hazardous situations
• Assessing risks and performance effectiveness, appropriate QM can be designed to use resources most effectively
• Involve the entire team of professionals in the development of FMEA and QM process
• We expect that the high risk steps and common failure modes identified in the TG100 exercise are relevant to a clinical physicist’s institution
62Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Recommendations• Form a multidisciplinary team consisting of radiation
oncologists, medical physicists, dosimetrists, therapists, nurses, engineers
• This team should be responsible for the development of a FMEA-based risk aware QM program
• Priority for FMEA-based effort should be given to high-risk procedures, high severity procedures, new procedures and those that are resource intensive
• FMEA-based methodology be adopted as an ongoing activity aimed towards continuous process improvement
63Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Recommendations• Future AAPM task groups undertake FMEA-based
analysis of important clinical processes
• AAPM establish a website with model FMEAs for various procedures as those analysis are developed
• AAPM should also develop web based training tools to train the medical physics community on an ongoing basis on the newly developed FMEAs for various procedures
64Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Conclusions• TG100 approach provides a concrete demonstration of
how to supplement the TG40 device centered approach with a holistic process-centered approach that considers the interactions between the network of devices, staff and processes that are required to perform radiation therapy
• TG100 analysis also provides specific guidance as to where in radiation therapy planning and delivery process the highest risk events are located
65Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
66
It is useful to report all accidents before consequences appear
Our job is not to prevent errors, but to keep the errors from injuring the patients.
Lucian Leape
It is impossible to make anything foolproof because fools are so ingenious.
Artur Bloch, Murphy’s law
Courtesy: Josef NovotnySaiful Huq - New Paradigms for QM in RT AAPM Summer School 2011

Acknowledgment
Special thanks to Professor Bruce Thomadsen from University of Wisconsin for providing some of the slides for this presentation
AAPM Summer School 2011Saiful Huq - New Paradigms for QM in RT 67
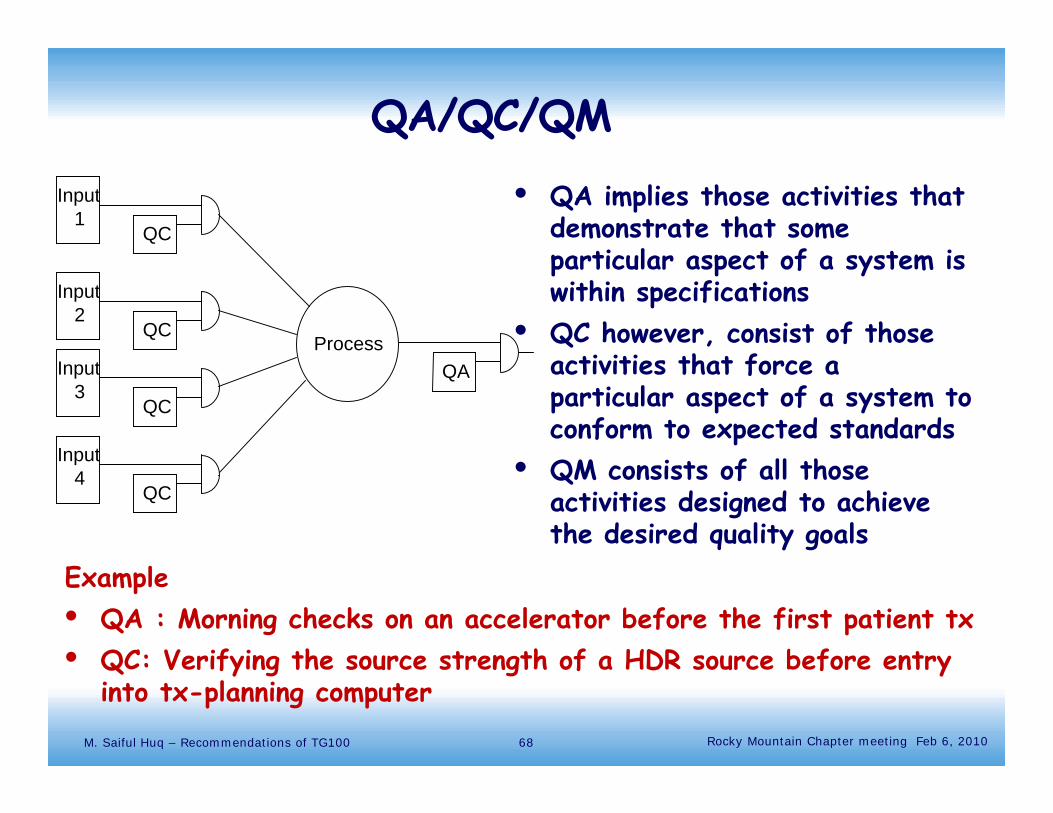
QA/QC/QM
• QA implies those activities that demonstrate that some particular aspect of a system is within specifications
• QC however, consist of those activities that force a particular aspect of a system to conform to expected standards
• QM consists of all those activities designed to achieve the desired quality goals
68M. Saiful Huq – Recommendations of TG100
Process
Input
QC
Input
QC
Input
QC
Input
QC
1
2
3
4
QA
Example• QA : Morning checks on an accelerator before the first patient tx• QC: Verifying the source strength of a HDR source before entry
into tx-planning computerRocky Mountain Chapter meeting Feb 6, 2010
Patient specific IMRT QA-assumptions for MLC
• The MLC shapes used for each patient cover the range of leaves and positions used in all patients
• The sensitivity of the plans tested during one day or week is adequate to detect problems with MLC function that could affect other patient plans already under treatment
• The frequency of the new patient specific IMRT QA provides sufficient MLC checks to prevent MLC delivery errors from persisting long enough to exceed the geometric and dosimetric accuracy goals over a course of IMRT
69Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Definitions
• Quality: • Those product features that meets the needs of the patient,
including rational medical, psychological, and economic goals and the professional and economic needs of the caregivers and the institution
• A clinical process tat is designed to realize cancer treatments that conforms with nationally accepted standards of practices and specifications
• Freedom from errors and mistakes
• Failure: Not meeting the desired level of quality is Failure.
70Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Definitions
• Errors: Failures consisting of acts, either of commission or omission, that incorrectly execute the intended action required by the process
• Mistakes: Failures due to incorrect intentions or plans, such that even if executed as intended, would not achieve the goal
• Near Miss: A situation resulting from a failure that would have compromised quality of the patient’s treatment had it not been detected or corrected.
71Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
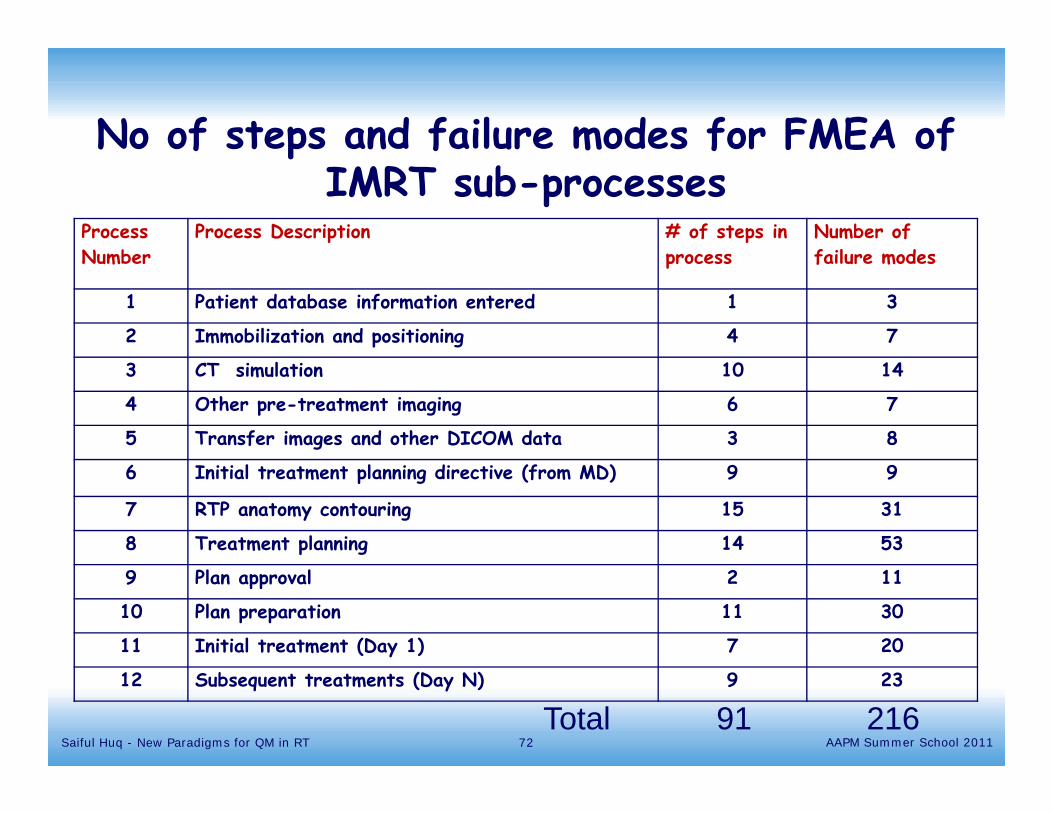
Process Number
Process Description # of steps in process
Number of failure modes
1 Patient database information entered 1 3
2 Immobilization and positioning 4 7
3 CT simulation 10 14
4 Other pre-treatment imaging 6 7
5 Transfer images and other DICOM data 3 8
6 Initial treatment planning directive (from MD) 9 9
7 RTP anatomy contouring 15 31
8 Treatment planning 14 53
9 Plan approval 2 11
10 Plan preparation 11 30
11 Initial treatment (Day 1) 7 20
12 Subsequent treatments (Day N) 9 23
No of steps and failure modes for FMEA of IMRT sub-processes
Total 91 21672Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
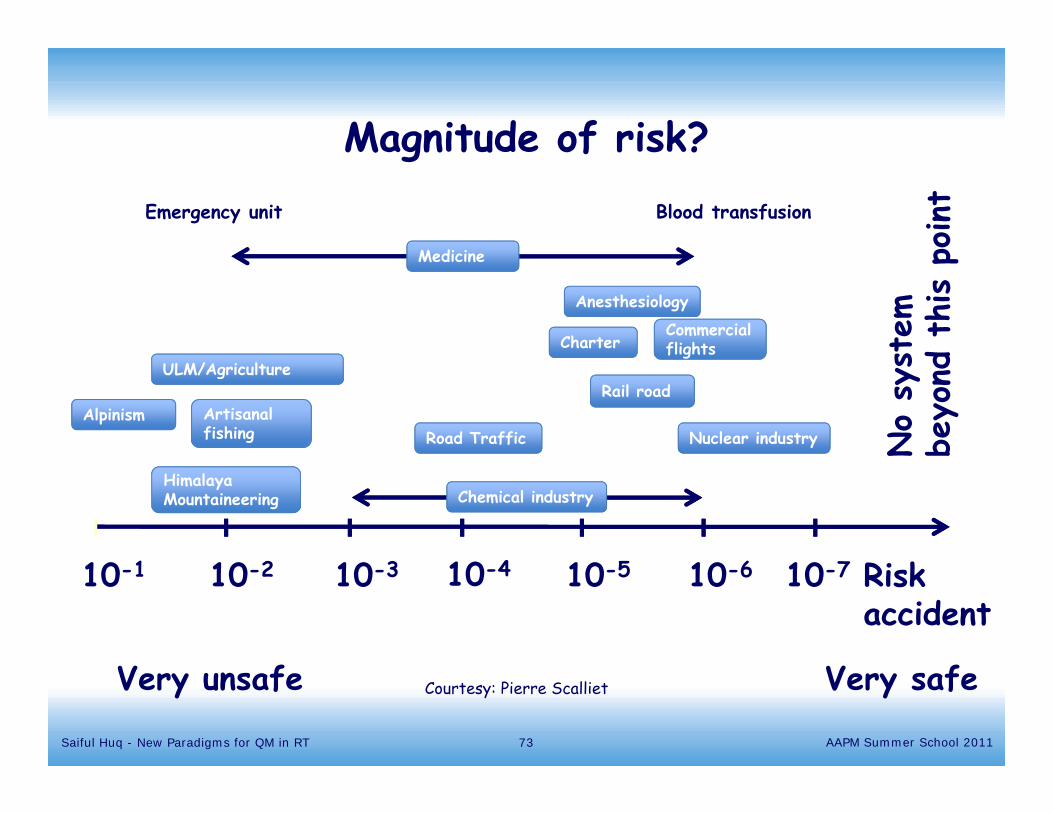
10-1
Alpinism Artisanal fishing Road Traffic Nuclear industry
10-2 10-3 10-4 10-5 10-6 Risk accident
10-7
Chemical industry
ULM/AgricultureRail road
Commercial flightsCharter
Medicine
Emergency unit Blood transfusion
Very safeVery unsafe
No
syst
em
beyo
nd t
his
point
Magnitude of risk?
Anesthesiology
Himalaya Mountaineering
Courtesy: Pierre Scalliet
73Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
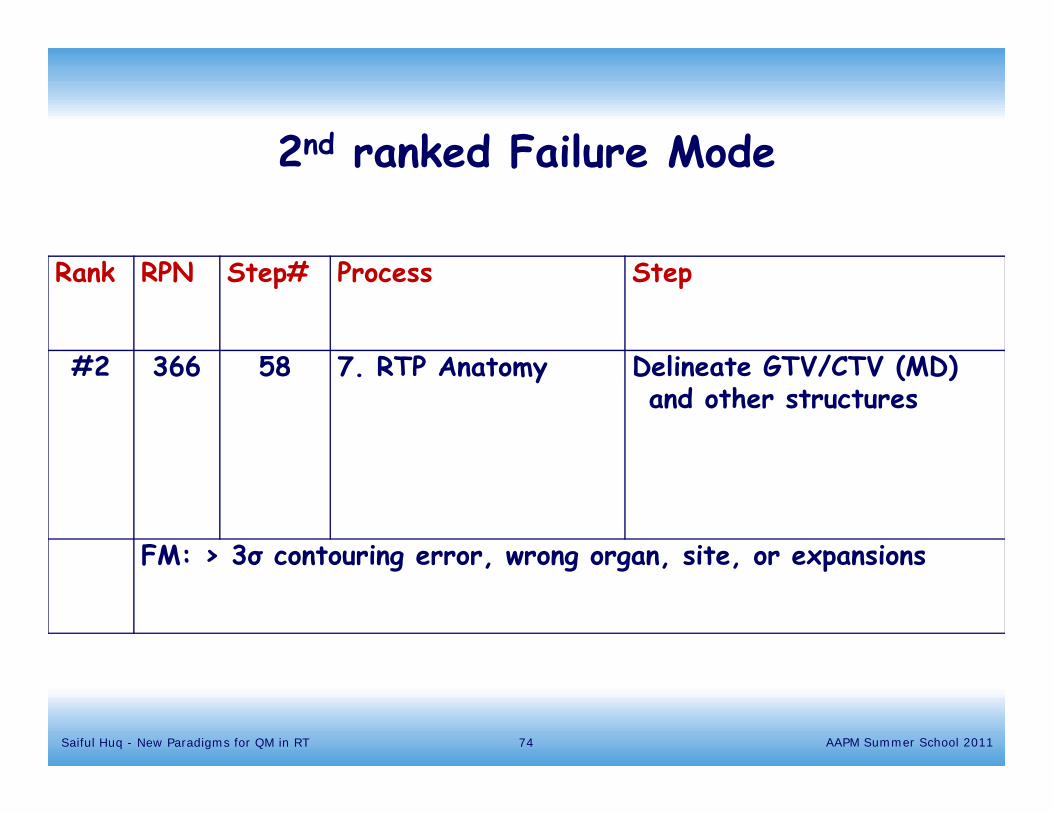
Rank RPN Step# Process Step
#2 366 58 7. RTP Anatomy Delineate GTV/CTV (MD) and other structures
FM: > 3σ contouring error, wrong organ, site, or expansions
2nd ranked Failure Mode
74Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
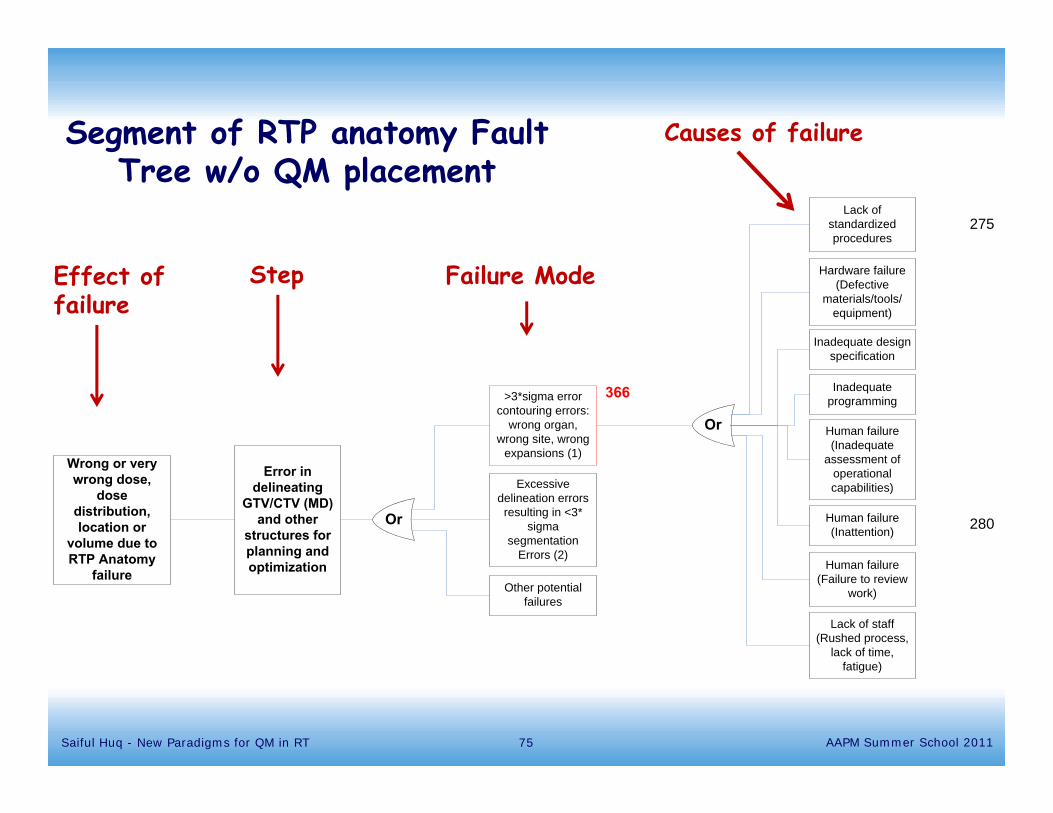
Or
Error in delineating
GTV/CTV (MD) and other
structures for planning and optimization
>3*sigma error contouring errors:
wrong organ, wrong site, wrong
expansions (1)
Lack of standardized procedures
Hardware failure (Defective
materials/tools/equipment)
Inadequate design specification
Human failure (Inadequate
assessment of operational capabilities)
Inadequate programming
Lack of staff (Rushed process,
lack of time, fatigue)
Excessive delineation errors resulting in <3*
sigma segmentation
Errors (2)
Other potential failures
Or
Wrong or very wrong dose,
dose distribution, location or
volume due to RTP Anatomy
failure
275
280Human failure (Inattention)
Human failure (Failure to review
work)
366
Segment of RTP anatomy Fault Tree w/o QM placement
Step Failure Mode
Causes of failure
Effect of failure
75Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
Training program !!
76Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
• Highlighted the need to make patient safety a high priority
• Priority has focused on identifying and reducing preventable events
• Adapt tools of ultra safe systems such as aviation industries ?
Institute of Medicine, 2000
77Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
2008
2008
2009
Recent reports
78Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
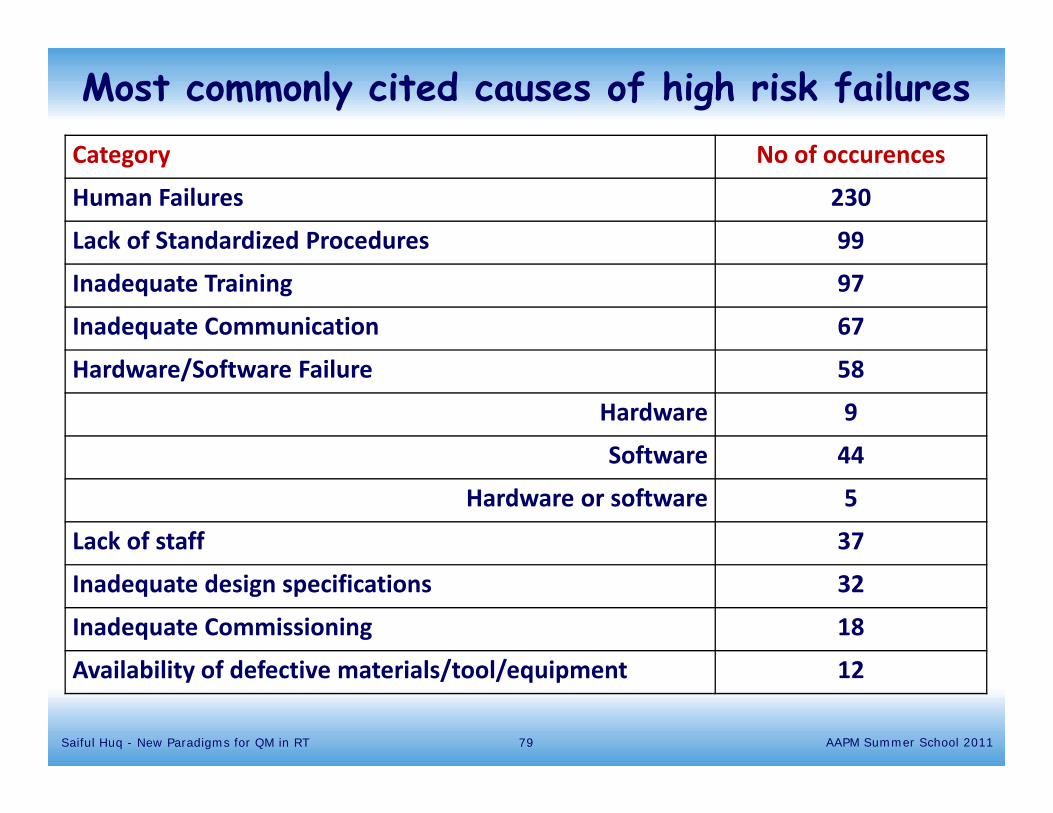
Category No of occurences
Human Failures 230
Lack of Standardized Procedures 99
Inadequate Training 97
Inadequate Communication 67
Hardware/Software Failure 58
Hardware 9
Software 44
Hardware or software 5
Lack of staff 37
Inadequate design specifications 32
Inadequate Commissioning 18
Availability of defective materials/tool/equipment 12
Most commonly cited causes of high risk failures
79Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
TG100 methodology for designing QM program in radiation therapy
• Prioritize the potential failure modes based on RPN and severity function
• Mark the highest rank steps on the process map
• Mark the same highest ranked steps on the fault tree
• Select QM intervention placement
• Establish the goals of the QM program
• Select appropriate QM tools
80Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011
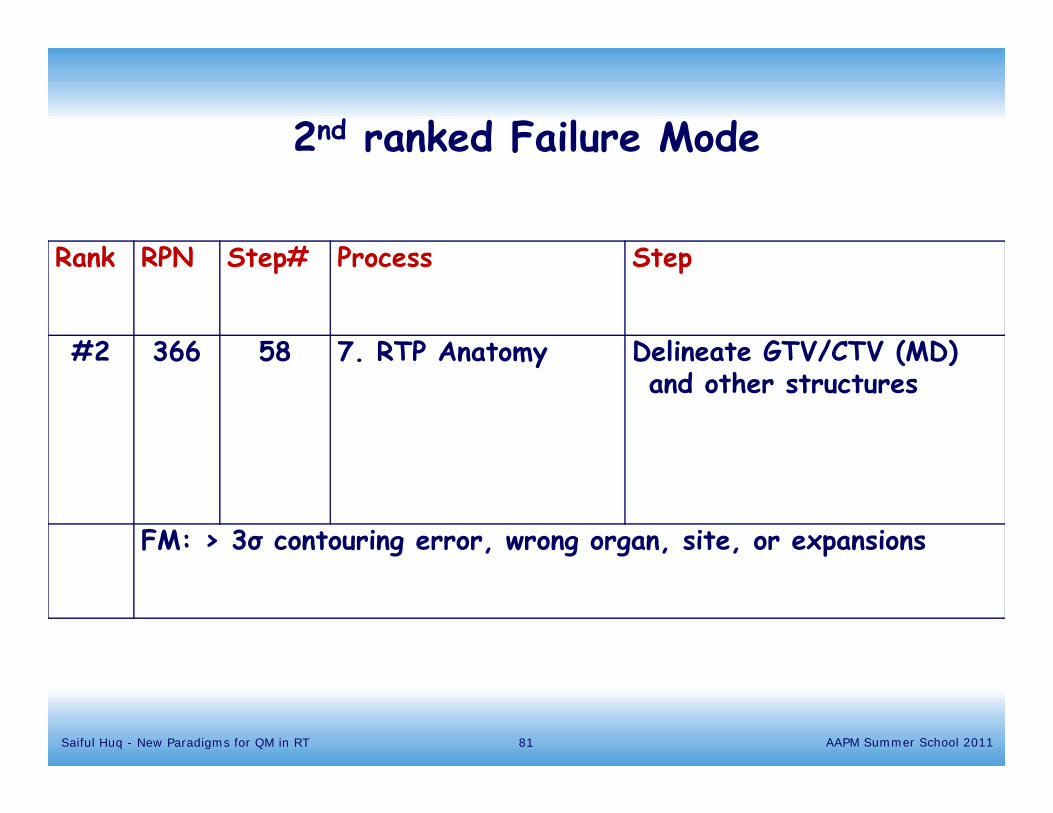
Rank RPN Step# Process Step
#2 366 58 7. RTP Anatomy Delineate GTV/CTV (MD) and other structures
FM: > 3σ contouring error, wrong organ, site, or expansions
2nd ranked Failure Mode
81Saiful Huq - New Paradigms for QM in RT AAPM Summer School 2011