Embed Size (px)
Citation preview

New Modalities in Diabetes DiagnosisPresented By:
Kristin J. Brown, MSIVDr. William M. Scholl College of Podiatric Medicine
July 2011
Image source: http://www.nsinc.org/what-we-treat.php

Who Should Be Tested?According to the ADA1:• Overweight/obese adults
• BMI >25• Who have one or more
additional risk factors
• At age 45 years• Repeat testing every 3 yrs• If pre-diabetic, test every
year.

Methods of Diagnosis Source: ADA’s “Standards of Medical Care”1

HbA1c vs. FPG & OGTT1
≥6.5 diagnose DM Disadvantages
Higher in cost Limited availability
for testing. Can be altered in
patients with anemia and hemoglobinopathies.
Benefits Fasting not required Greater pre-analytical
stability than FPG Less vulnerable to
alterations than FPG during stress & illness.

FPG1
Studies have shown the FPG test has a specificity exceeding 96%, but it is only 50% sensitive.2

FPG & OGTT1
OGTT has been shown to have a sensitivity of 73% and specificity of 80%.2
Both FPG and OGTT are invasive, fasting exams that suffer from poor reproducibility.2

www.ngsp.org3
Click icon to add picture
HbA1c Assay Interferences
“If your diabetes patient has a hemoglobin variant, your lab should use one of the methods that does not show interference from the variant, thus producing an accurate A1C result.”

Complications Diabetes complications1,4:
CVD** PVD Nephropathy Retinopathy Neuropathy
Peripheral and autonomic Hearing loss Stroke HTN
Image source: http://www.netheryeye.com/OurServices/DiabeticRetinopathy.aspx

Neuropathy1,4
One of the most common late complications of DM.
Leading cause of non-traumatic amputations in the US.
Has a role in other late complications of diabetes. Neuropathic ulcerations!
Increases risk of mortality.

Neuropathy Etiology
AGE’s (Advanced Glycation End products)5
Increased in hyperglycemia & oxidative stress Sugars cross-link with other proteins Contribute to segmental demyelination and
interact with nitric oxideneronal apoptosis.
Excess sugars and proteins broken down by the Maillard reaction5: Creates AGE’s
Image source: http://www.artistaday.com/?p=5717/

AGE’s Increased in skin collagen in those with
neuropathy.5
Especially pentosidine and cross-lines These when excited with near-
UV and blue light.fluoresce
Image source: http://thegist.dermagist.com/how-to-increase-collagen-and-elastin-production

AGE’s First screened via punch biopsy that
often times required a suture for closure.2
Now studies using near infrared (NIR) technologies.2
Non-invasive Portable & immediate results Readings corrected for intrinsic
fluorescence parameters. (dark vs. light skin, etc.)Image source: http://www.punchbiopsycpt.com/what-is-a-punch-biopsy

Studies M.N. Ediger, B. Olson, and J Maynard.
“Noninvasive Optical Screening for Diabetes.” Journal of Diabetes Science & Technology. 2009;3(4):776-780.6
Retrospective cohort of 2,793 subjects All identified as naïve & at risk based on the
ADA’s Standard of Care Guidelines. Compared FPG, HbA1c, and OGTT to SIF.
OGTT at 2hr 75g was considered the baseline. Results

Studies J.D. Maynard et al. “Noninvasive Type 2
Diabetes Screening”. Diabetes Care. 2007;30(5):1120-1124.7
351 subjects with one or more DM risk factors. Ages 21-86 years Compared HbA1c, FGT, SIF vs. OGTT 84 pts had AGT (OGTT >140 mg/dL) Results

Studies B.N. Conway et al. “Skin Intrinsic
Fluorescence Correlates with Autonomic and Distal Symmetrical Polyneuropathy in Individuals with Type 1 Diabetes.” Diabetes Care. 2011;34:1000-1005.5
111 people with DM1 Mean age 49 years Determined if CDSP and autonomic neuropathy
associated with SIF vs. HbA1c. Results

Scout DS by VeraLight8
Image source: http://www.veralight.com/SCOUT_Video.html

Scout DS by VeraLight8
Image source: http://www.veralight.com/SCOUT_Video.html

Scout DS by VeraLight8
≥50 =diabetic<50 =normal
Image source: http://www.veralight.com/SCOUT_Video.html

Corneal Confocal Microscopy
“A rapid, non-invasive technique that enables a prospective and reiterative evaluation of the human cornea at high magnification [1-2 µm resolution].”9
Utilizes confocal optics, which allows examination of a focused point.9
Coronal sections of the cornea. Can visualize corneal epithelium, Bowman’s membrane
(nerve-complex), stroma, and endothelium. Even better than histopathological exams!9
Fun fact: The cornea is the most densely innervated part of the human body!9

Corneal Confocal Microscopy Cont… The cornea contains C and Aδ fibers.9
Reminder: C fibers are large, unmyelinated fibers responsible for slow, aching pain. Aδ cause fast, sharp pain.
Those fibers account for the majority of symptoms in diabetic neuropathy, and have been shown to be damaged first.9

Study M. Tavakoli, et al. “Corneal Confocal
Microscopy: A novel noninvasive test to diagnose and stratify the severity of human diabetic neuropathy.” Diabetes Care. 2010;33(8):1792-1797.10
110 DM and 17 healthy pts. Assessed on NDS, QST, NCV (sural &
peroneal), NCCA, CCM. Results

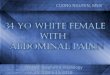
Image source: M. Tavakoli, et al. “Corneal Confocal Microscopy: A novel noninvasive test to diagnose and stratify the severity of human diabetic neuropathy.” Diabetes Care. 2010;33(8):1792-1797.O5
normal
moderate
mild
severe

Conclusion Skin Intrinsic Fluorescence and Corneal Confocal
Microscopy are two technologies at the forefront of diabetic and diabetic neuropathy diagnosis.
They are non-invasive techniques that give immediate results, and have been shown by multiple studies to be superior to other techniques.
While they aren’t seen widely now, you will probably see them soon…

Image source: http://www.nsinc.org/what-we-treat.php
Thank you.Questions?

References1. American Diabetes Association. “Standards of Medical Care in Diabetes-2010.” Diabetes
Care. 2010:33(supplement 1):511-561.2. Hull, E., et al. “Noninvasive, optical detection of diabetes: model studies with porcine skin.”
Optics Express. 2004;12(19):4496-4509.3. Centers for Disease Control & Prevention. “Harmonizing Hemoglobin A1C Testing.” Accessed
online July 12th, 2011. http://www.ngsp.org/bground.asp4. American Diabetes Association website. “Living with Diabetes: Complications.” Accessed
online July 10, 2011. http://www.diabetes.org/living-with-diabetes/complications/5. Conway, B.N. et al. “Skin Intrinsic Fluorescence Correlates with Autonomic and Distal
Symmetrical Polyneuropathy in Individuals with Type 1 Diabetes.” Diabetes Care. 2011;34:1000-1005.
6. Ediger, M.N., B. Olson, and J Maynard. “Noninvasive Optical Screening for Diabetes.” Journal of Diabetes Science & Technology. 2009;3(4):776-780.
7. Maynard, J.D. et al. “Noninvasive Type 2 Diabetes Screening”. Diabetes Care. 2007;30(5):1120-1124.
8. VeraLight Website. “The VeraLight Scout DS.” Accessed online July 10th, 2011. http://www.veralight.com/products.html
9. Hossain, P., A. Sachdev, and R. Malik. “Early detection of diabetic peripheral neuropathy with corneal confocal microscopy.” The Lancet. 2005;366:1340-1342.
10. Tavakoli, M. et al. “Corneal Confocal Microscopy: A novel and noninvasive test to diagnose and stratify the severity of human diabetic neuropathy.” Diabetes Care. 2010;33(8):1792-1797.
11. Malik, R.A. et al. “Corneal Confocal Microscopy: a non-invasive surrogate of nerve fibre damage and repair in diabetic patients.” Diabetologia. 2003;46:683-688.