Embed Size (px)
DESCRIPTION
New
Citation preview
Management of Bleeding in Oral Surgery
Presented by : P. Santosh, IV BDS.Guided By: Dr. Ramesh, MDS.,
Department of Oral and Maxillofacial Surgery
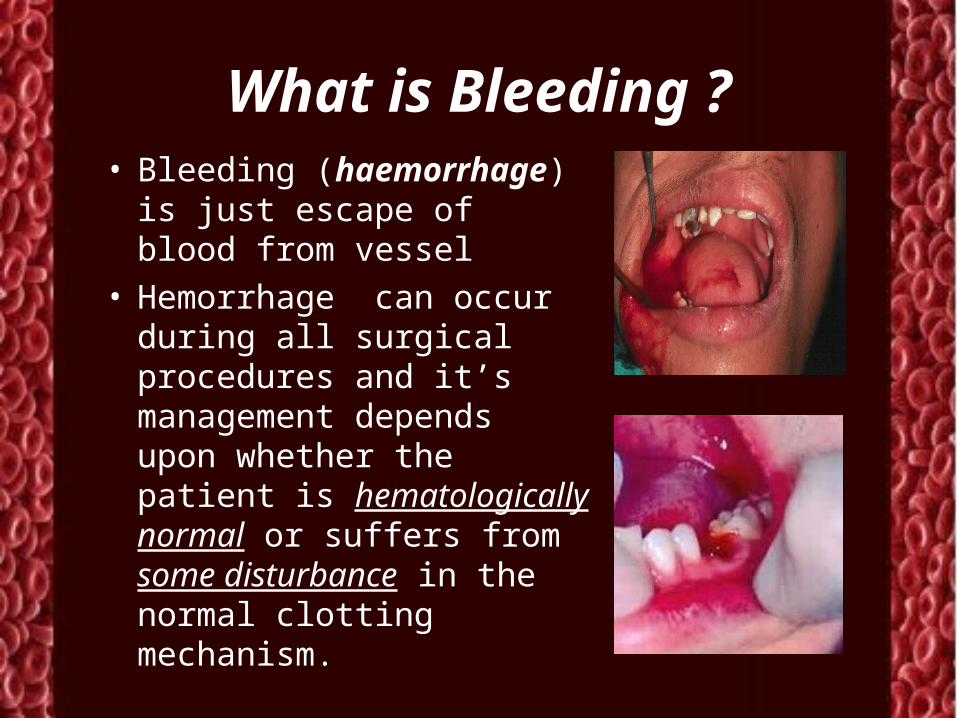
What is Bleeding ?• Bleeding (haemorrhage)
is just escape of blood from vessel
• Hemorrhage can occur during all surgical procedures and it’s management depends upon whether the patient is hematologically normal or suffers from some disturbance in the normal clotting mechanism.
What causes Bleeding in oral surgery ?
• Hemorrhage following Oral Surgical procedures can occur due to local (soft tissue or bone) or systemic causes. (heriditary conditions such as hemophilia, Von Willebrand’s disease)
• In healthy patients the postoperative bleeding is mainly due to local causes.
Local causes …
• Soft tissue i.e arterial, venous, or capillary in nature.
• Venous blood is dark red in color and flows steadily and heavily
• Arterial bleeding is bright red and spurting in nature.
• Bone• Bone appears to
bleed in case of injury to inferior alveolar artery, or from central vascular lesions (Hemangioma or Vascular malformation)
Systamic causes…
• 1. hereditary conditions ( Hemophilia)
• 2. thrombocytopenia
• 3. Leukemias
• 4. uncontrolled hypertension
• 5. oral anticoagulants like Aspirin or Warfarin
• 6. Chronic Liver disease
• 7. Vitamin k deficiency
Classification of hemorrhageAmerican College of Surgeons' Advanced Trauma Life
Support (ATLS)
• Class I Hemorrhage involves up to 15% of blood volume.
• Class II Hemorrhage involves 15-30% of total blood volume. Volume resuscitation with crystalloids is all that is typically required.
• Class III Hemorrhage involves loss of 30-40% of circulating blood volume.. Fluid resuscitation with crystalloid and blood transfusion are usually necessary
• Class IV Hemorrhage involves loss of >40% of circulating blood volume. Aggressive resuscitation is required to prevent death.
Types of hemorrhage…Primary Heamorrhage
: This occurs during the
surgery, as a result of injury like cutting or laceration of the artery or bleeding from bone.
This also occurs when surgery is done in an infected area with a lot of granulation tissue.
• Reactionary Hemorrhage This type of bleeding occurs
within a few hours after surgery.
Patients who have unknowingly disturbed / dislodged the clot are also prone for this type of bleeding.
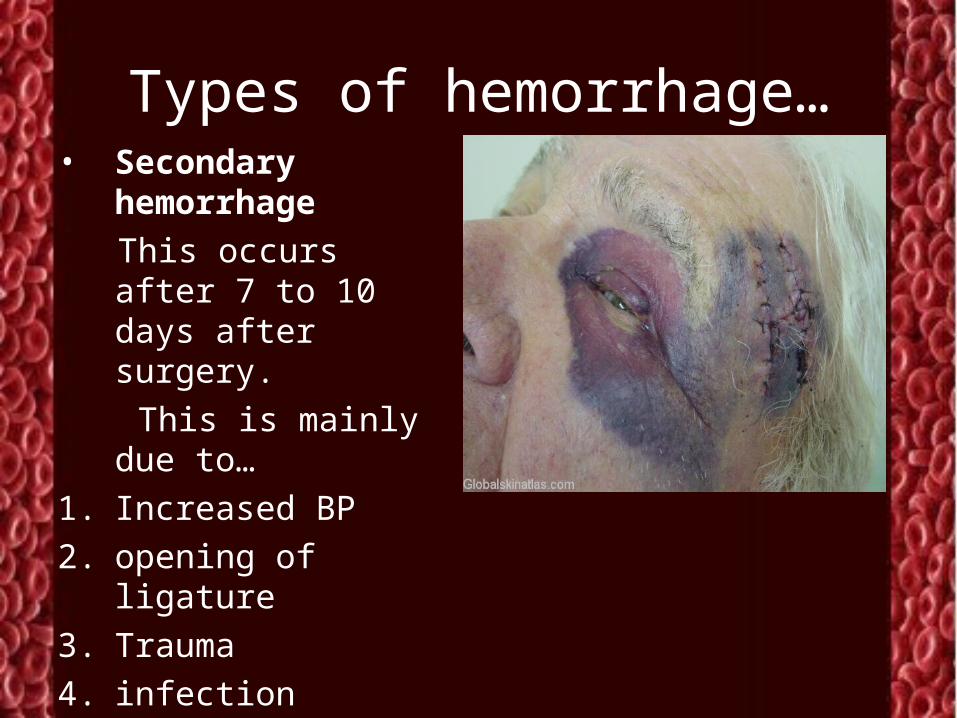
Types of hemorrhage…• Secondary
hemorrhage
This occurs after 7 to 10 days after surgery.
This is mainly due to…
1. Increased BP
2. opening of ligature
3. Trauma
4. infection
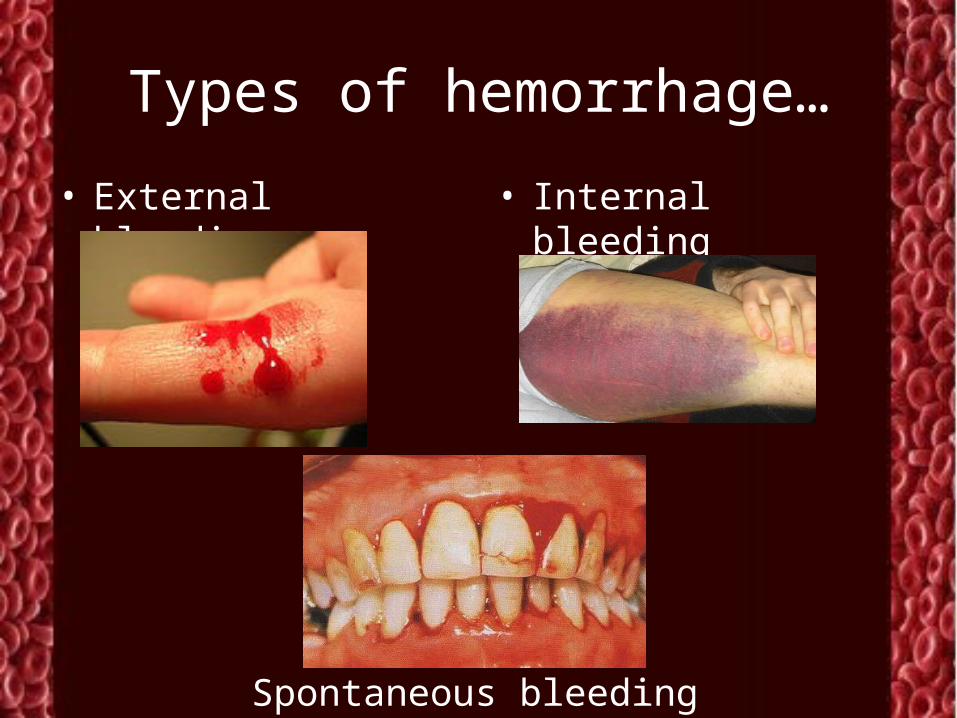
Types of hemorrhage…
• External bleeding • Internal bleeding
Spontaneous bleeding
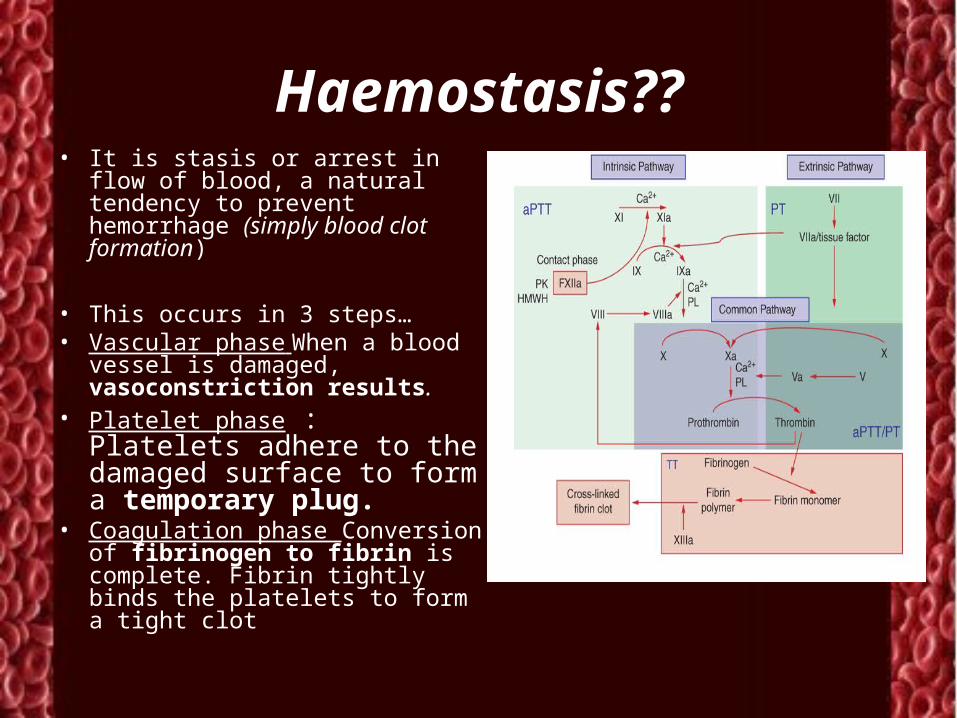
Haemostasis??• It is stasis or arrest in flow of
blood, a natural tendency to prevent hemorrhage (simply blood clot formation)
• This occurs in 3 steps…• Vascular phase When a blood
vessel is damaged, vasoconstriction results.
• Platelet phase : Platelets adhere to the damaged surface to form a temporary plug.
• Coagulation phase Conversion of fibrinogen to fibrin is complete. Fibrin tightly binds the platelets to form a tight clot
Clinical Evaluation of patient
• History:• Family history of bleeding?• Complication during
previous surgery?• History of hematuria, easy
brusing,epistaxis, menorrahgia?
• History of cancer or collagen vascular diseases diagnosed?
• Any drug or medication patient is on?
• Examination• Anemia• Petechial spots?• Echymosis or
telengestesia?• Spleen, Liver
enlargement?• Singns of liver failure?• Bleeding in synovial
joints? ( hereditary coagulopathies)
Lab Reports…
• PLATELET COUNT• BLEEDING TIME (BT)• PROTHROMBIN TIME (PT)• PARTIAL THROMBOPLASTIN TIME (PTT)• THROMBIN TIME (TT)• Others …• HB- TC- DLC -CT – ESR – PCR • Screening test for Blood Guucose and HIV infection
Lab reports
• BT : 2-8 min.PROVIDES ASSESSMENT OF PLATELET COUNT AND FUNCTION
• CT : 2-5 mins to rule out related disorders
• PT: 20- 40 secs. Measures Effectiveness of the Extrinsic Pathway
• PTT : 25- 40 secs.Measures Effectiveness of the Intrinsic
Pathway
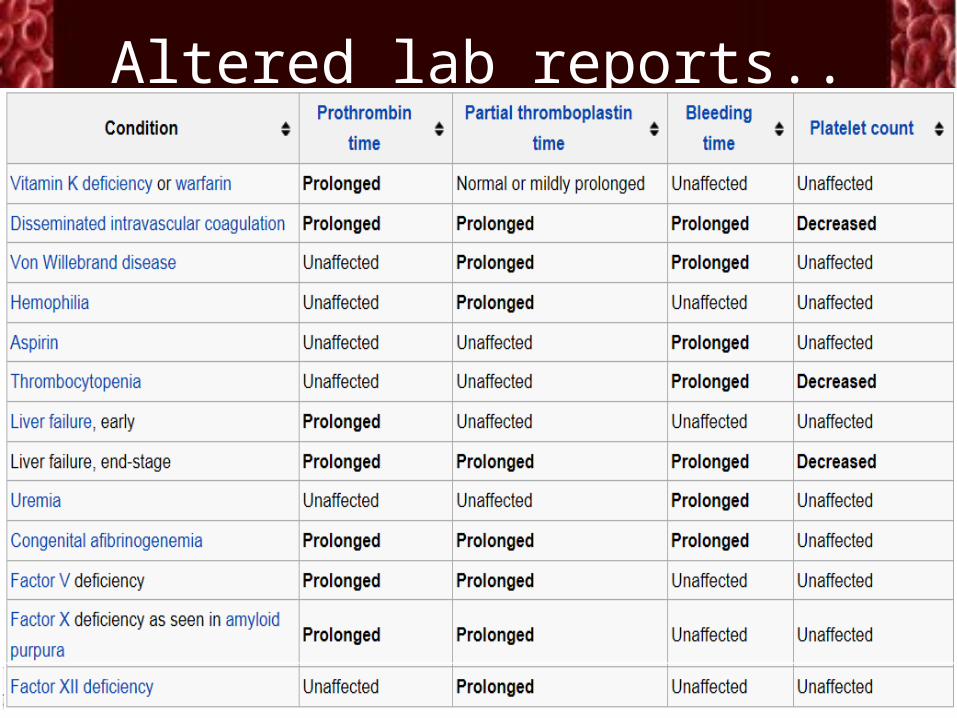
Altered lab reports..
Platelets 100,000 - 400,000 cell/ cu mm
< 100,000 Thrombocytopenia
50,000 - 100,000 Mild Thrombocytopenia
< 50,000 Severe Thrombocytopenia
WBC 7000-11000 cells/cu mm
RBC 4-6 lakh cells / cu mm
Management of Primary Hemorrhage in Normal patients
The management of bleeding during surgery (Primary bleeding) can be achieved by the following means:
1.Mechanical methods
2.Thermal agents
3.Chemical methods
4.Systemic agents
5.Ligation of related blood vessels
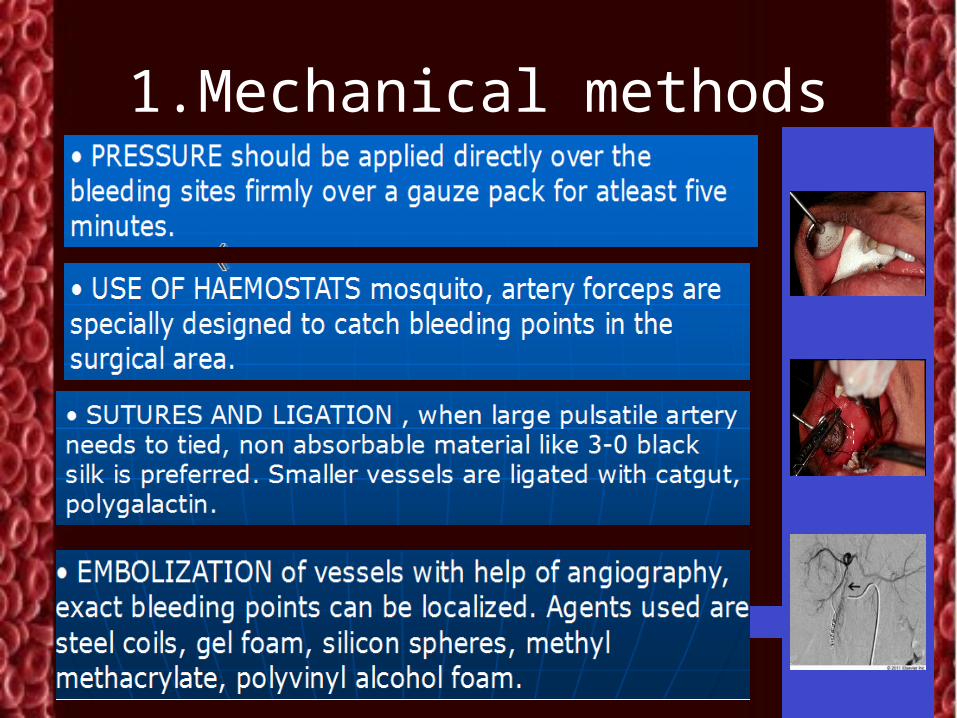
1.Mechanical methods
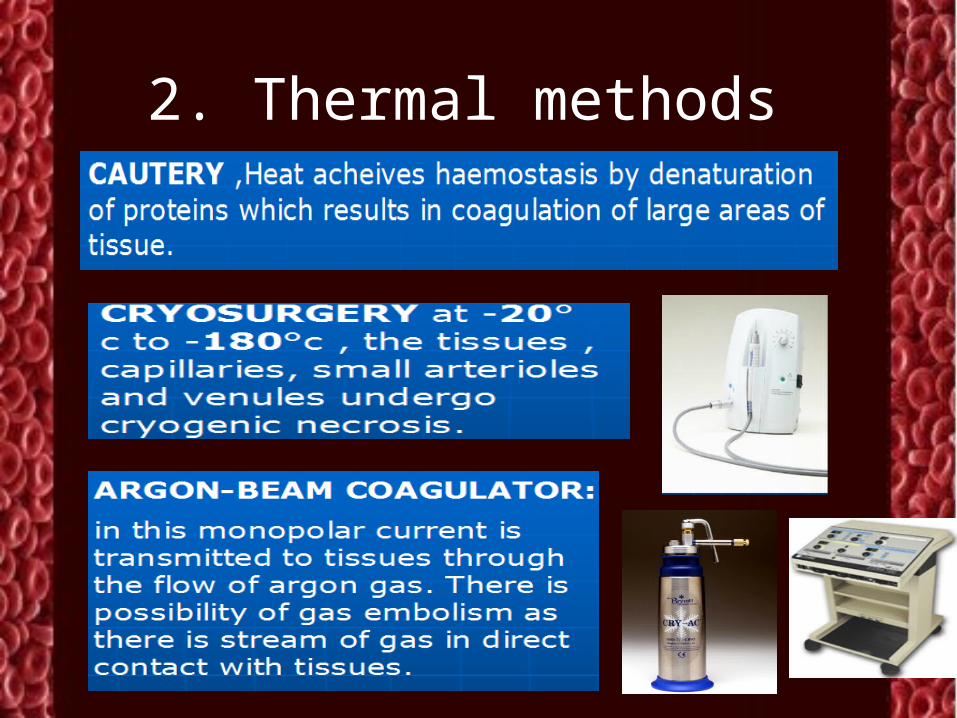
2. Thermal methods

3. Chemical methods
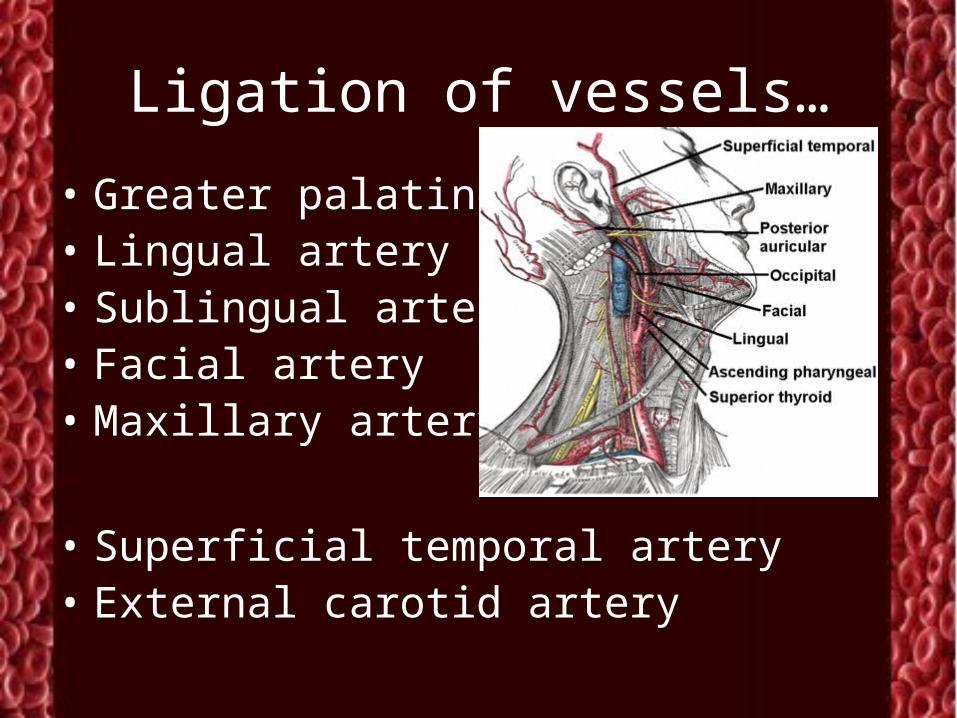
Ligation of vessels…
• Greater palatine• Lingual artery• Sublingual artery• Facial artery• Maxillary artery
• Superficial temporal artery• External carotid artery
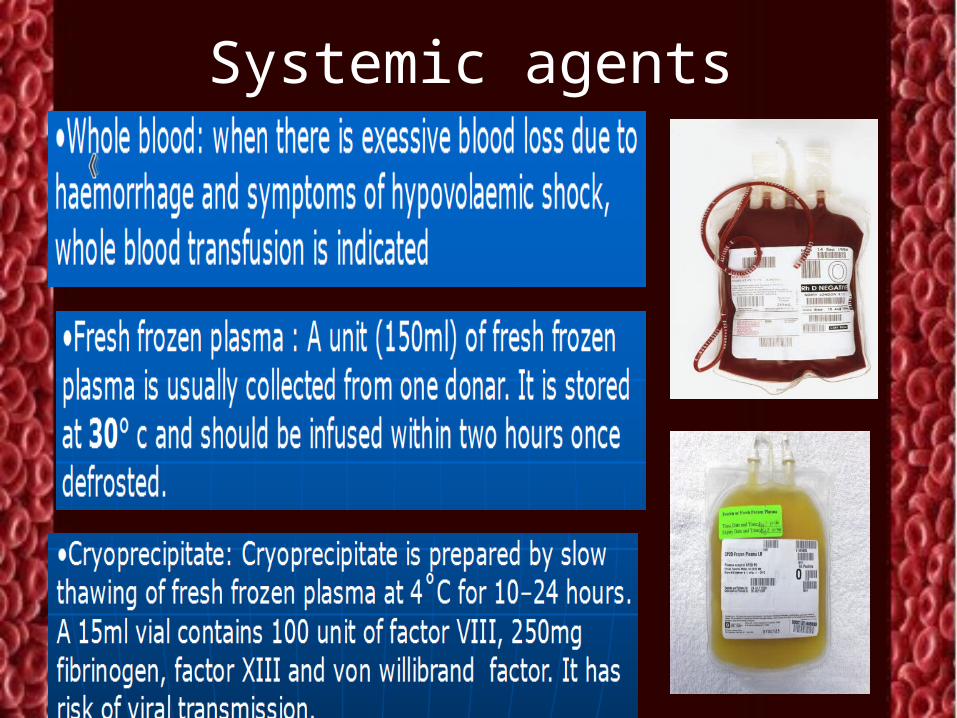
Systemic agents
Hemophilia management
• Deficiency of factor VIII ( hemophilia A) or IX (hemophilia A) or hemophilia.
Management in special patients
• Haemphilia A, von Willebrands disease• Patient on Anti- Coagulant therapy• Uncontrolled Hypertensive patient• End stage liver disease
Early diagnosis:
Identification of systemic problem and referral for physician's advice.
Use of local hemostatic aids after controlling systemic effects of the disease is helpful
Classification of coagulation disorders
• Congenital X-linked Haemophilia A and B • Autosomal Von Willebrand disease Factor II, V, VII, X, XI and
XIII deficiencies Combined II, VII, IX and
X deficiency • Hypofibrinogenaemia and
Dysfibrinogenaemia• Acquired Liver failure
• Increased consumption• Coagulation activation
– Disseminated intravascular coagulation (DIC)
• Immune-mediated – Acquired haemophilia
and von Willebrand syndrome
• Drug-induced• Inhibition of function
– Heparins – Lepirudin
• Inhibition of synthesis – Warfarin
Hemophilia management• Factor VIII concentrate.• Desmopressin (0.3 micro gm/ kg diluted in 100ml saline
given in 30 mins)• Tranaxemic acid (3-4 gm Tb or 0.5- 1 mg IV)• Episilon aminicaproic acid (5mg – 1mg 8th hourly)• AVOID• Complicated surgeries• IV injections in severe cases• Check• INR value 2-3 , PT 20-22 secs is check and treatment is
done on patient on warffarn. • Stop aspirin prior to extractions for 5 days.• Always check BP values for a hypertensive patient.
Von Willebrands disease
• It is most commonly inherited disorder, occurs due to deficiency of von willebrands factor. (synthesised by endothelial cells and megakaryocytes always bound to F VII as a complex. )
• Most patients with von Willebrand disease have type 1 vWD which is characterised by a quantitative decrease in a normal functional protein.
• Patients with type 2 disorders inherit vWF molecules which are functionally abnormal
Von Willebrands disease
• Investigations reveal:• Reduced activity of vWF and factor VIII,
and a prolongation of the bleeding time• Management:• The vasopressin receptor agonist DDAVP
raises the vWF and factor VIII levels by 3-4-fold, which is useful in arresting bleeding in patients with Von Willibrands disease and mild or moderate haemophilia A
Liver diseases..
• There is reduced hepatic synthesis, e.g. of factors V, VII, VIII, IX, X, XI, prothrombin and fibrinogen. Thrombocytopenia may occur secondary to hypersplenism in portal hypertension. In cholestatic jaundice there is reduced vitamin K absorption, leading to deficiency of factors II, VII, IX and X
Small note on Complications…
• Shock (hypovolumic)
• Infection transfer during transfusion
• Exsanguination ( complete loss of blood)
• Death of patient
______________________________



](https://img.pdfslide.us/doc/110x75/577cc1011a28aba71191ebaa/11040-microsoft-powerpoint-11040-microsoft-powerpoint-securtization-compatibility.jpg)





![New Microsoft PowerPoint Presentation.ppt [Read …media.mycrowdwisdom.com.s3.amazonaws.com/aaop/Resources/...Microsoft PowerPoint - New Microsoft PowerPoint Presentation.ppt [Read-Only]](https://img.pdfslide.us/doc/110x75/5f798734ccfe2c3952073dc2/new-microsoft-powerpoint-read-mediamycrowdwisdomcoms3amazonawscomaaopresources.jpg)