Embed Size (px)
Citation preview
New Mexico Human Services Department
Encounter Quality:Lessons from New Mexico
Mark Pitcock, Deputy Director, Medical Assistance DivisionSeptember 10, 2013

New Mexico Managed Care
2
• 1997 SALUD• 2005 Behavioral Health• 2008 Coordination of Long‐Term Services• 2014 Centennial Care
NOTE: All New Mexico MCOs are required to operate statewide.

Encounter Processing
• MCO submits encounters to New Mexico’s fiscal agent– Professional, institutional and dental encounters to the FA’s translator
– Pharmacy to the FA’s PBM system
• Fiscal agent adjudicates the encounters and generates error reports for the MCOs
• Encounters are available in the MMIS for inquiry and in the data warehouse for analysis and ad hoc reporting
3

Encounter Fundamentals
• Use standard formats (X12 837, NCPDP)• Make sure you can identify the provider
– NPI: Blessing and curse– Provider network file
• Apply appropriate edits• Insist on an MCO paid amount• Provide a void/adjustment process using standard formats
4

Encounter Fundamentals (cont.)
• Include encounter‐related contract requirements with teeth– Submit at least 90% of claims within 30 calendar days and 99% within 60 calendar days of the date of adjudication
– Meet accuracy requirements by submitting encounters with no more than a 3% error rate per invoice type
– Liquidated damages: 2% of monthly capitation payment
5

Ongoing Challenges
• Federal Mandates (NPI, 5010, ICD‐10)• COBA interface• Periodic re‐procurements (adding new MCOs which may or may not have a clue)
• Internal MCO issues (e.g., conversion to a new claims system)
• Sub‐capitated arrangements (e.g., dental, transportation)
6

2014: New Frontiers for New Mexico• Requiring submission of encounters for non‐claim based services such as care coordination
• Requiring submission of encounters for denied claims
• Requiring submission of encounters for Medicare claims paid by a member’s Special Needs Plan or Medicare Advantage Plan for which there is no Medicaid obligation
7
Leveraging Data For Better Managed Care OutcomesMESC 2013September 10, 2013
Managing Managed Care PlansNeeds
• Many States lack the resources, capacity and analytics necessary for actively managing members assigned to Managed Care Organizations (Managing the managed care plans!)
• States require improved means for tracking and understanding the quality of care received by their members and ensure efficient use of limited financial resources
• As states continue transitioning members from Fee-for-Service to managed care, they need a variety of comparisons for MCO performance, including validating managed care is equal or better than FFS
• Encounter data that is “clean” and “correct” is a must – including those encounters which were denied by the MCO
• The trend toward moving more vulnerable and complex members into managed care (e.g. dual eligibles, 1915c waivers, etc.) creates more emphasis in managing managed care plans
• HEDIS is only part of the equation
• Trust…but verify

Managing Managed Care PlansOpportunities
• Understand quality of health care delivered across the state
• Reduce benefit costs
• Provide trend analysis
• Leverage “big data” and today’s modern visualization tools
• Assist in setting MCO rates
• Monitor MCO effectiveness
• Identify discrepancies between FFS vs. Managed Care
• Compare MCOs to peers for performance and outcomes
• Identify opportunities of rewarding well-run MCOs with additional members

Xerox Customer Driven Approach
October 24, 201311
Dreaming Session AnalyticsScenarios
Medical/PharmaDomain Assets
Prioritized Scenarios& Define Workflows with Impact
Customer pilots
Prototyping
Multiple iterations
Client Workshop
Managing Managed Care PlansTypes of Advanced Analytics
• Compare MCOs for disparity in care for Native Americans compared to other demographics
• Compare MCOs for higher utilization of the emergency room
• Compare provider network adequacy between MCOs. Specifically, are participants getting equal access to a PCP in each managed care organization
• Compare MCOs for hospital stay readmissions
• Compare MCOs with chronic condition utilization forecasting
• Geographically visualize hot spots or specific pockets of disease in the state
• Visualize delays in visits to PCP after a member is released from the hospital
• Risk adjust to view how results may vary

Managing Managed Care PlansVisually compare MCOs with higher utilization of the emergency room
• Visualization of trends occurring with avoidable ER visits
• Question answering e.g. “which geographic areas have a rising trend in avoidable ER visits?”
• Determination of causes for high ER incidence – e.g. few well-check visits, high PCP panel rates?
• Perspectives into risk for chronic conditions of diabetes, asthma, and heart disease
• How do MCO’s compare against each other in avoidance?

Emergency Room Utilization• Number of ER visits and cost/utilization ratio
• Determine avoidable ER visits
• Determine frequent ER users
• Data source: NM Medicaid MMIS data
• Time Period: 1/1/2009 - 12/31/2012
• Population: All NM Medicaid SALUD! MCO members

Emergency Room UtilizationQuick Facts:
• Average ER visit charge is about $1750 and the average paid amount is $700
• MCO1 is relatively small but has the highest normalized ER utilization rate
• The normalized utilization ratio is calculated as the total number of ER visits/1,000 member months (using HEDIS specs as basis)
• The average utilization rate per 1,000 member months is 47; the national rate of ER encounters per 1,000 member months has been reported as 68.3
• Spike on ER visits in Oct 2009 due to a frantic flu season that peaked that month
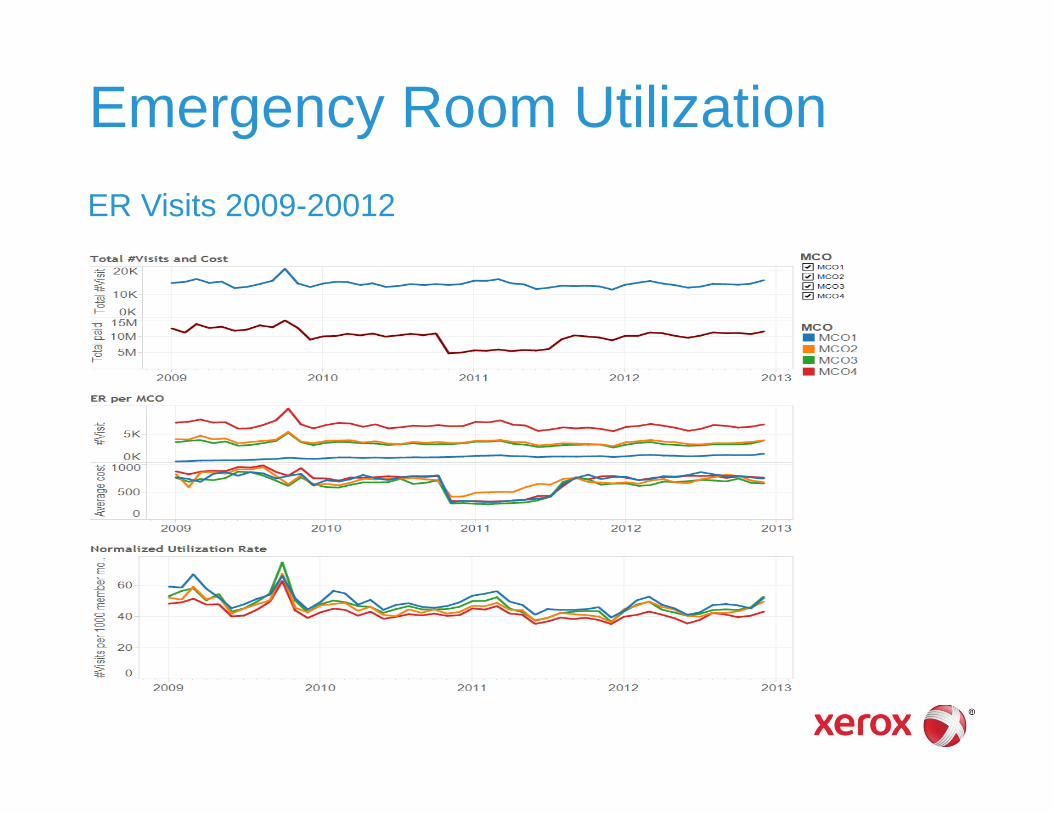
Emergency Room UtilizationER Visits 2009-20012
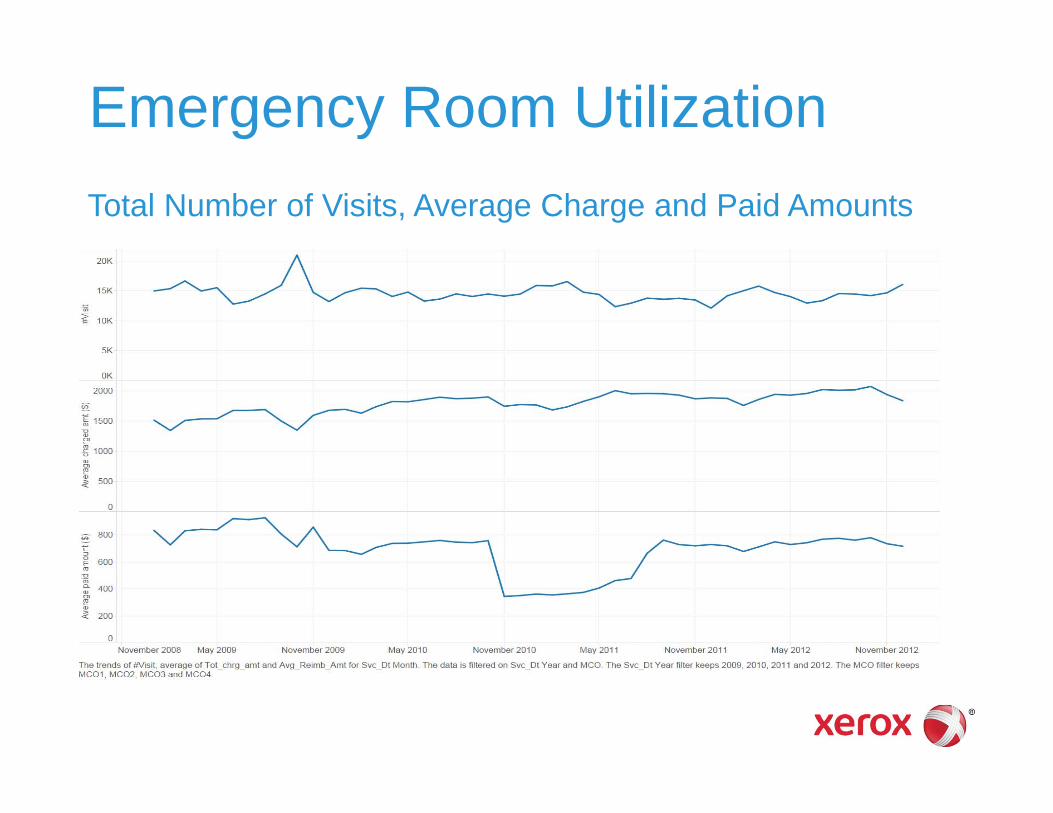
Emergency Room UtilizationTotal Number of Visits, Average Charge and Paid Amounts

Emergency Room UtilizationER Visits and Paid Amount
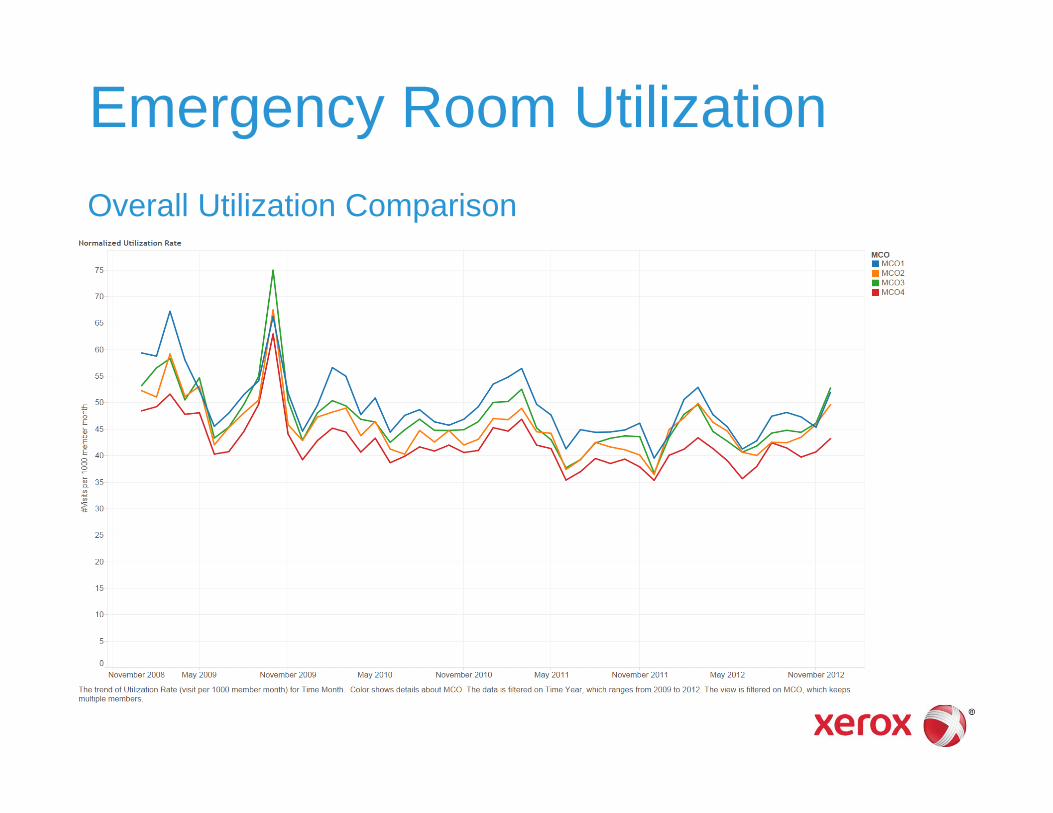
Emergency Room UtilizationOverall Utilization Comparison
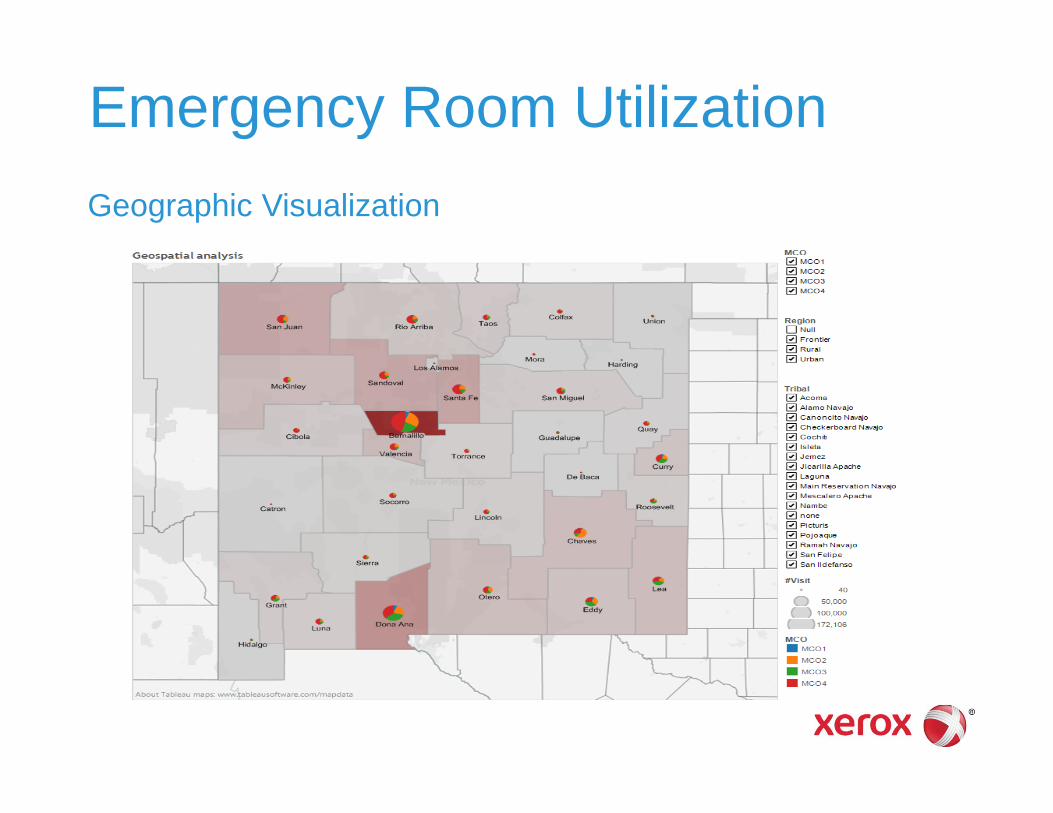
Emergency Room UtilizationGeographic Visualization
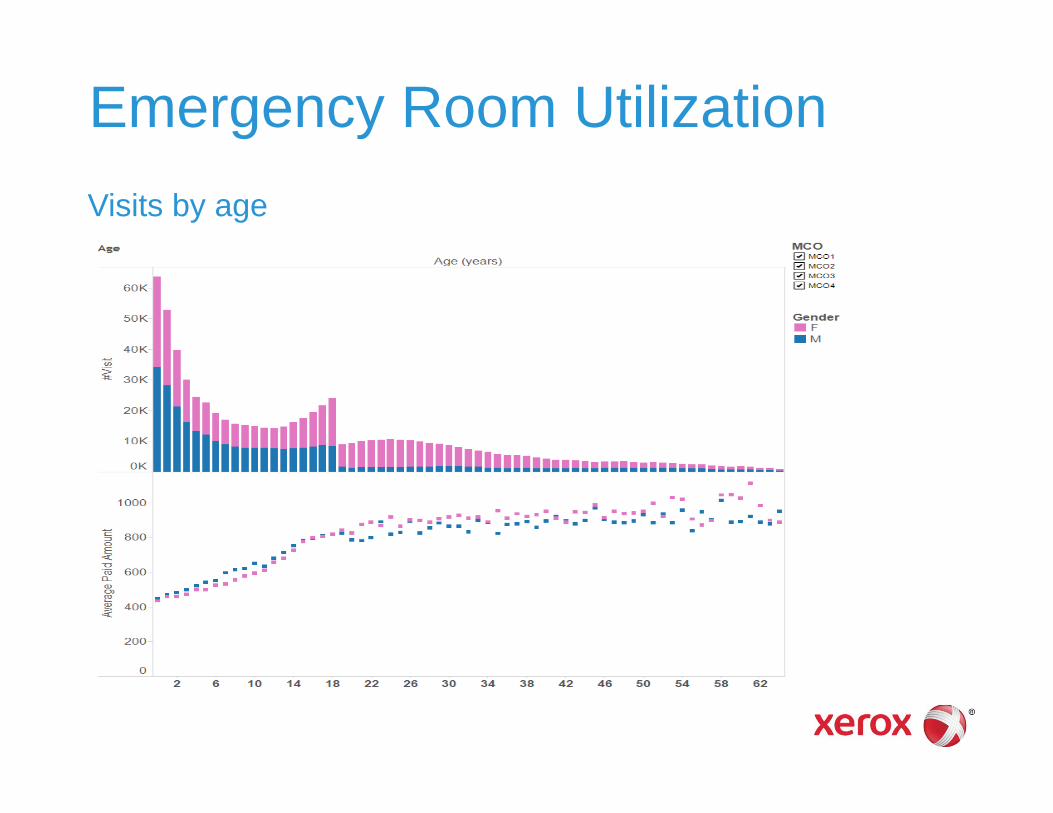
Emergency Room UtilizationVisits by age

Emergency Room UtilizationAvoidable by Age
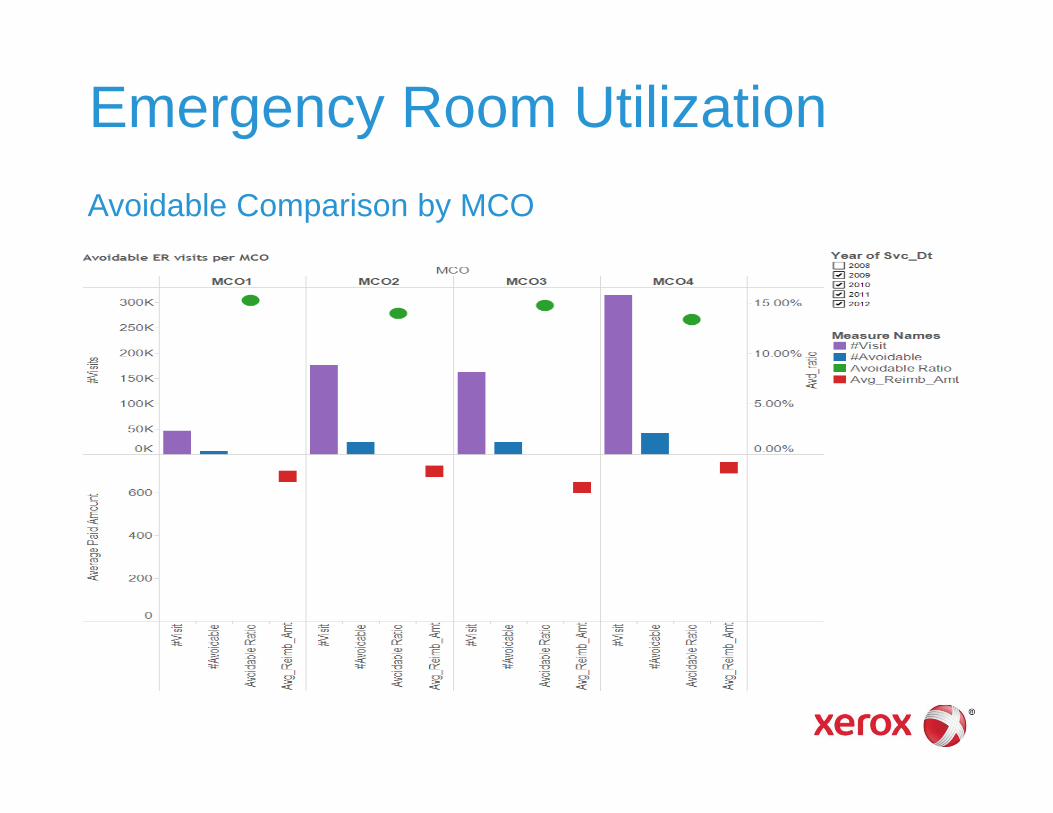
Emergency Room UtilizationAvoidable Comparison by MCO
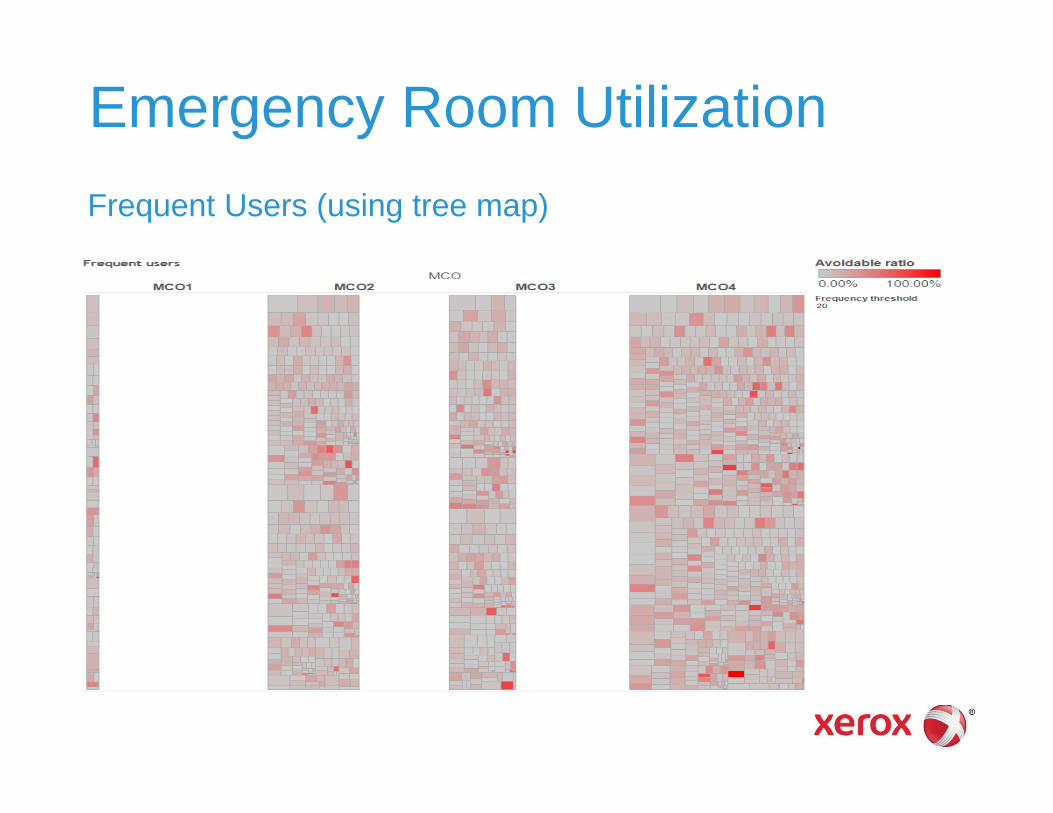
Emergency Room UtilizationFrequent Users (using tree map)

Emergency Room UtilizationFrequent Users (drill down)


Program Integrity Analyticsin Medicaid Managed Care
2013 Medicaid Enterprise Systems Conference
Cathie OttDirector, Program & Payment IntegrityHealth Care AuthorityAugust 2013
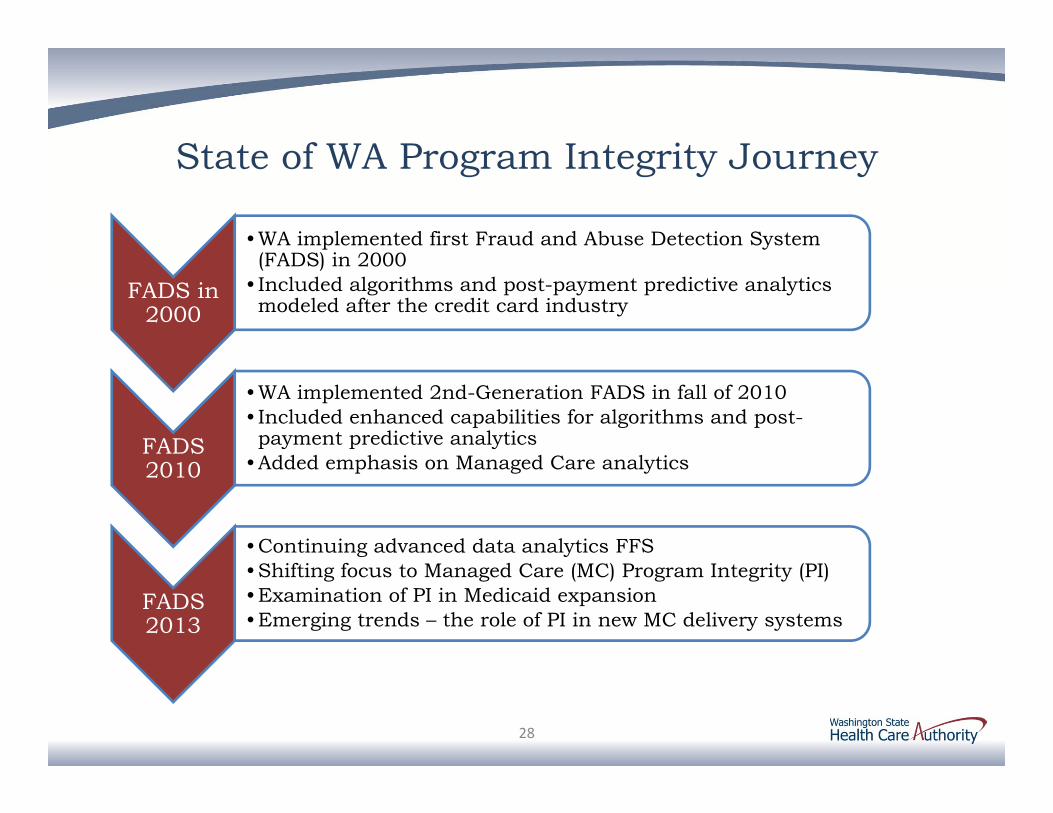
State of WA Program Integrity Journey
FADS in 2000
•WA implemented first Fraud and Abuse Detection System (FADS) in 2000
• Included algorithms and post-payment predictive analytics modeled after the credit card industry
FADS 2010
•WA implemented 2nd-Generation FADS in fall of 2010 • Included enhanced capabilities for algorithms and post-payment predictive analytics
•Added emphasis on Managed Care analytics
FADS 2013
•Continuing advanced data analytics FFS•Shifting focus to Managed Care (MC) Program Integrity (PI)•Examination of PI in Medicaid expansion•Emerging trends – the role of PI in new MC delivery systems
28
WA Managed Care Trends In September 2011, HCA conducted a joint procurement
for Healthy Options (Medicaid managed care), Basic Health plan, and SSI population
Five plans were successful bidders, including three Managed Care Organizations new to WA Medicaid
Application of care management principles and new competition among MCOs produced significant savings to the state
The addition of SSI blind and disabled population in July 2012 increased managed care enrollment to over 70% of the current Medicaid caseload
Managed care is the primary coverage vehicle for the WA Medicaid expansion population in 2014
Healthcare reform trends introduce new models along the managed care continuum
29
Fraud, Waste and Abuse Basics The fraud triangle – why individuals or
organizations commit fraud
1. Pressure: typically comes from some financial need or desire
2. Opportunity: system weakness or lack of controls (historically healthcare fraud has been relatively easy)
3. Rationalization: the basis by which the perpetrator is able to excuse the behavior
These remain the same in managed care but the oversight changes
30
Pressure
RationalizationOpportunity

What is required for effective MC PI?
MC PI includes oversight of the MCO and its administration as well as oversight of MCO provider and client behavior
Three things needed for effective fraud, waste and abuse detection
Effective tools to detect fraud early
Ability to act quickly
Tools to spot new areas of fraud as they emerge
For MC, effective fraud, waste and abuse detection and prevention requires strong collaboration between healthcare policy, compliance, internal audit, claims processing, legal and contract compliance
31
WA Managed Care Program Integrity (PI) Initiative
Introduced in 2012, the MC PI Initiative examines the application of existing advanced analytic capabilities to Encounter Data (ED)
WA ED is collected in standard HIPAA transaction formats and available in Data Warehouse. Initial analytic focus was on data quality
ED Validity: the extent to which encounter data actually means what you think it means; is it actionable?
ED Reliability: The extent to which data are consistent and mean the same thing from across providers and plans
PI analytics continue concurrent with ED Workgroup examining a set of supporting goals
32

WA Managed Care Program Integrity (PI) Initiative
Initial analytics provided actionable results
Duplicate maternity/delivery payments (MCO and FFS)
Capitation payments made after client’s date of death
Client with no encounter services reported within a year
Outstanding issue for WA is determination of the disposition of actionable overpayments identified using ED
33

WA Managed Care ED Workgroup Goals include:
Operationalize a detailed ED validation process with routine monitoring
Develop a set of production reports for tracking quality and timeliness of ED
Coordinate with MCO to understand their claims processing systems, edits, and encounter data submission processes
Recommend necessary improvements and/or add service level agreements and amend plan contracts as needed
Research the value of conducting sample audits of encounters
Develop initiatives that use ED and shifts data quality from a theoretical to an immediate need.
34






























