Embed Size (px)
Citation preview

Research ArticleNew Insights into the Hepcidin-Ferroportin Axis and IronHomeostasis in iPSC-Derived Cardiomyocytes from Friedreich’sAtaxia Patient
Alessandra Bolotta ,1,2 Provvidenza Maria Abruzzo ,1,2 Vito Antonio Baldassarro ,3
Alessandro Ghezzo ,1 Katia Scotlandi,4 Marina Marini ,1,2 and Cinzia Zucchini 1
1Department of Experimental, Diagnostic and Specialty Medicine, Bologna University, 40126 Bologna, Italy2IRCCS Fondazione Don Carlo Gnocchi, 20148 Milan, Italy3Interdepartmental Centre for Industrial Research in Health Sciences and Technologies (ICIR-HST), University of Bologna,40064 Ozzano, Bologna, Italy4CRS Development of Biomolecular Therapies, Experimental Oncology Laboratory, Orthopedic Rizzoli Institute, 40136 Bologna, Italy
Correspondence should be addressed to Provvidenza Maria Abruzzo; [email protected]
Received 11 September 2018; Accepted 4 December 2018; Published 27 March 2019
Guest Editor: Giorgos Sakkas
Copyright © 2019 Alessandra Bolotta et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work isproperly cited.
Iron homeostasis in the cardiac tissue as well as the involvement of the hepcidin-ferroportin (HAMP-FPN) axis in this process andin cardiac functionality are not fully understood. Imbalance of iron homeostasis occurs in several cardiac diseases, includingiron-overload cardiomyopathies such as Friedreich’s ataxia (FRDA, OMIM no. 229300), a hereditary neurodegenerativedisorder. Exploiting the induced pluripotent stem cells (iPSCs) technology and the iPSC capacity to differentiate into specificcell types, we derived cardiomyocytes of a FRDA patient and of a healthy control subject in order to study the cardiac ironhomeostasis and the HAMP-FPN axis. Both CTR and FRDA iPSCs-derived cardiomyocytes express cardiac differentiationmarkers; in addition, FRDA cardiomyocytes maintain the FRDA-like phenotype. We found that FRDA cardiomyocytes show anincrease in the protein expression of HAMP and FPN. Moreover, immunofluorescence analysis revealed for the first time anunexpected nuclear localization of FPN in both CTR and FRDA cardiomyocytes. However, the amount of the nuclear FPN wasless in FRDA cardiomyocytes than in controls. These and other data suggest that iron handling and the HAMP-FPN axisregulation in FRDA cardiac cells are hampered and that FPN may have new, still not fully understood, functions. These findingsunderline the complexity of the cardiac iron homeostasis.
1. Introduction
Iron is a trace metal essential for numerous biological pro-cesses. Its homeostasis is finely regulated, since both ironexcess and deficiency are potential detrimental. In fact, ironexcess favors the formation of oxygen radicals, while irondeficiency impairs enzyme functionality affecting oxygenmetabolism. It has been demonstrated that the dysregulationof iron homeostasis is involved in different pathological con-ditions, including cancer, anemia, neurodegenerative disor-ders, and cardiac diseases [1]. Iron deficiency was found to
occur in heart failure patients, independently of normalsystemic iron concentration, causing morphological andfunctional mitochondrial alterations and consequently ATPdepletion [2]. These dysfunctions, in turn, impair cardiaccontractility and relaxation. Ironically, cardiomyopathy canbe induced also by systemic iron overload, as in hereditaryhemochromatosis (HH) and β-thalassemia, and by iron mis-distribution in the cellular organelles, as in Friedreich’s ataxia(FRDA) [3]. Iron excess causes an alteration of systolic anddiastolic functions through the decrease of L-type channelactivity, essential for the heart contraction. In addition, at
HindawiOxidative Medicine and Cellular LongevityVolume 2019, Article ID 7623023, 11 pageshttps://doi.org/10.1155/2019/7623023

the cellular level, iron misdistribution in cellular organelles,such as the mitochondria, can damage the cells throughoxygen radical production. Cardiomyocytes, being endowedof poor antioxidant defenses, are more susceptible to reac-tive species of oxygen (ROS) damage via Fenton andHeiber-Weiss-typereactions [3, 4]. Iron homeostasis is reg-ulated by several proteins involved in the iron uptake,transport, storage, and export. These proteins cooperatewith ferrireductases, ferroxidases, and chaperones to regu-late the cellular iron trafficking and to limit the unboundlabile iron pool (LIP), potential source of ROS. Iron existswithin heme molecules such as hemoglobin and cytochromesor in iron-sulfur cluster- (ISC-) containing proteins suchas succinate dehydrogenase; moreover, nonheme/non-ISCiron-containing proteins are present in the cells [5]. Non-heme iron is transported into the cells by iron-bindingproteins, such as transferrin. Cellular uptake of iron fromtransferrin is initiated by the binding of transferrin totransferrin receptor 1 (TFRC). TFRC is a transmembraneprotein that assists iron uptake through receptor-mediatedendocytosis of iron-loaded transferrin [5]. In addition, ironchaperones such as frataxin, a nuclear-encoded protein local-ized into the mitochondrial matrix, act as iron sensor andstorage proteins as well as iron chaperons during cellularFe-S cluster biosynthesis [6].
In iron homeostasis, a central regulatory mechanism isthe binding of the hormone hepcidin (HAMP) to the ironexporter ferroportin (FPN). FPN is the only iron-exportingprotein localized in the cell membrane; it was independentlydiscovered by three different groups [7–9]. The FPN struc-ture has not been completely defined; it is characterized by9-12 transmembrane domains (TMs), organized into twosix-helix halves, which are connected by a large cytoplasmicloop between the 6th and the 7th domain [10, 11]. Further-more, whether the functional form of FPN is monomeric ordimeric remains an open question. Genetic and biochemicalevidences support the dimeric form [12]. However, differentgroups reported that FPN is a monomer, and that, in thisform, it is able to bind HAMP [13, 14]. Regulation of FPNoccurs at multiple levels, transcriptional, posttranscriptional,and posttranslational. FPN expression is regulated at thetranscriptional level by hypoxia inducible factor-2alpha(HIF2α) in response to hypoxia and inflammation; more-over, it is induced by iron heme and other metals. Posttran-scriptionally, FPN synthesis is regulated by iron regulatoryproteins (IRPs), which bind to an iron responsive element(IRE) located in its 5′UTR. In addition, posttranslational reg-ulation of FPN is mediated by HAMP. HAMP binds FPNand triggers its internalization, ubiquitination, and subse-quent lysosomal degradation [10, 11].
At systemic level, circulating HAMP is synthesized by theliver, where it is induced in iron overloading conditions andis inhibited by iron deficiency due to anemia, hypoxia, inef-fective erythropoiesis, and inflammation [10, 11]. HAMP isalso expressed in the heart, brain, kidney, and placenta [15];in these tissues, its role is less defined, but it is likely involvedin iron handling. HAMP expression is regulated by differentmembers of the TGF-β superfamily, including BMP (bonemorphogenetic protein) receptors, associated BMP ligands,
and the cytoplasmic SMAD transcription factor [16]. More-over, it is been shown that Atoh8 (atonal bHLH transcriptionfactor 8) contributes to hepcidin regulation in response toiron levels by interacting with Id1 proteins [17]. Cardiacexpression of HAMP is induced in response to hypoxia andinflammation [18]. Upregulation of HAMP occurs in heartischemia [19], while its downregulation was described in amouse model of dilated cardiomyopathy [20]. Moreover,Hsieh et al. [21] showed that apoptosis was induced by theknockdown of HAMP by siRNA in human cardiomyocytestreated with ferrous iron. Anomalies of HAMP-FPN axisaffect the heart functionality. Mouse cardiac FPN knockoutsshow dilated cardiomyopathy and iron deposits in cardio-myocytes [22]. In addition, it has been shown that HAMPknockout at the cardiac level leads to an increase in cardiacFPN; moreover, HAMP loss or HAMP unresponsivenessis associated to cardiac hypertrophy and apoptosis [23]. Inaddition, heart autoptic tissue of FRDA patients revealedmacrophagic inflammatory infiltrate with high levels ofHAMP and iron deposits [24]. To the mechanisms of ironuptake, transport, storage, and export mentioned above,one should add those that regulate the utilization of ironand its correct subcellular distribution. Noteworthy, a stillunderestimated subcellular compartment involved in irontrafficking is the nucleus, where iron-sulfur clusters associ-ated with DNA repair enzymes [25] and transcription factorshave been described [26]. Iron transporters and storageproteins, such as the divalent metal transporter 1 (DMT1),lactoferrin, and ferritin, are associated to the nucleus [27].
The deregulation of iron compartmentalization is veryoften associated with neurodegenerative pathologies such asFriedrich’s ataxia, a progressive neurodegenerative disordercharacterized by degeneration of central and peripheral ner-vous systems and associated with hypertrophic cardiomyop-athy and iron deposits [28]. Cardiomyopathy and subsequentcardiac failure is the most common cause of death in FRDApatients [29], where expanded GAA repeats in intron 1 ofthe frataxin gene (FXN) cause its partial deficit [30]. Physio-logical functions of frataxin involve iron binding and storage,biogenesis of heme and iron-sulfur clusters, and iron sensing;data suggest that further—still undetermined—functions arepresent. Frataxin depletion results in mitochondrial dysfunc-tion, mitochondrial iron accumulation, and ROS production[5, 31]. In this context, the complex relationship between themitochondrial aberrations, iron imbalance and frataxin dys-function, has contributed to the difficulty of deciphering themolecular mechanisms underlying the iron homeostasisimbalance and consequently of identifying effective therapeu-tic molecules to mitigate the cardiac hypertrophy. Moreover,the lack of a model that can recapitulate the phenotypic andgenotypic characteristics of FRDA contributes to the poorknowledge of the underlying mechanisms of this disease.
Aim of the present study is to generate and character-ize iPSC-derived cardiomyocytes as a cellular model toexplore the HAMP-FPN axis and investigate the ironhomeostasis in FRDA cardiac phenotype. Differentiation ofiPSC-derived cardiomyocytes was monitored by cardiac geneanalysis with real-time PCR and evaluation of cardiac pro-teins by cytofluorimetric and immunofluorescence methods.
2 Oxidative Medicine and Cellular Longevity

2. Material and Methods
2.1. Human-Induced Pluripotent Stem Cells (hiPSCs).HumaniPSCs derived from a healthy subject and from a FRDApatient were obtained from the NIGMS Human GeneticCell Repository at the Coriell Institute for Medical Research:(GM 23280∗A and GM23404∗B, respectively) and gener-ated through fibroblast reprogramming according to theYamanaka method [32]. Table S1 reports genotypic andphenotypic features of the subjects.
2.2. Cardiomyocyte Derivation from hiPSCs. Differentiationof hiPSCs in cardiomyocytes was performed according tothe GiWi method by Lian et al. [33]. The detailed protocoland the timeline of cardiac differentiation are reported inFigure S1.
2.3. Flow Cytometric Analysis. For cytometric analysis, wellswere washed with PBS 1x and cardiomyocytes were dissoci-ated with trypsin-EDTA 0.25% and then fixed in 1% parafor-maldehyde for 20min at room temperature and 90% coldmethanol for 15min. Cells (0 5 × 106) were centrifuged andthe pellet incubated with primary anti-troponin T (TNNT2)antibody (Thermo Fisher Scientific, Waltham, MD) over-night at 4°C in a buffer containing 5% BSA and 1% TritonX-100 in PBS. Secondary antibody (Alexa Fluor 488 Goatanti-mouse IgG1) was added, and the samples were incu-bated for 30min at room temperature, after which the nucleiwere stained with DAPI. Samples were acquired using aFACSCalibur instrument and analyzed with the CellQuestsoftware (Becton Dickinson, Italy). The primary and second-ary antibody and the dilutions used are listed in Table S2.
2.4. Immunostaining Analysis. Cardiomyocytes were washedwith PBS 1x and were dissociated with trypsin-EDTA0.25% and then seeded on 0.1% gelatin-coated coversplis at1 × 105cells/mL. After two days, the cells were fixed in 4%paraformaldehyde for 15min at room temperature. Theprimary and secondary antibody and the dilutions used arelisted in Table S2. Cardiomyocytes were incubated overnightat 4°C with the primary antibody in a buffer containing 5%nonfat dry milk and 0.4% Triton X-100 in PBS. Cells werewashed three times for 5min in PBS 1x. Subsequently, thecardiomyocytes were incubated with the secondary antibodyfor 20min at room temperature, followed by nuclear stainingwith mounting medium containing DAPI (Santa CruzBiotechnology, DBA, Italy). Images of cardiomyocytes wereobtained using a fluorescence microscope (Leica DMLB FluoMS15062).
2.5. RNA Isolation and cDNA Synthesis. Total RNA wasextracted with TRIzol™ reagent (Invitrogen, Milan, Italy)following the manufacturer’s instructions. RNA quality wasmeasured by evaluation of 28S and 18S rRNA band sharp-ness after denaturing electrophoresis. RNA purity and con-centration were assessed by spectrophotometer evaluation(Ultrospec 3000, Pharmacia Biotech, Cambridge, UK) at 230,260, and 280nm. Reverse transcription (800ng of RNA tem-plate) was performed in a final volume of 20μL using theiScript cDNA Synthesis Kit (Bio-Rad, Hercules, CA) following
the manufacturer’s instructions. The cDNA thus obtained wasstored at -20°C and used for qRT-PCR analysis.
2.6. Quantitative RT-PCR Analysis. Quantitative RT-PCRwas performed according to Abruzzo et al. [34] in aBio-Rad CFX96 real-time thermal cycler using the SsoAd-vanced™ SYBR® Green Supermix (Bio-Rad Laboratories,Hercules, CA). The primer sequences for target and house-keeping genes (β-actin, GAPDH) are listed in Table S3.Primers were designed with PRIMER3 and AMPLIFYsoftware and, whenever possible, were designed as to spanan exon-exon junction. All primers were purchased fromSigma-Aldrich (St. Louis, MO). Data were analyzed withthe software CFX Manager software (Bio-Rad Laboratories,Hercules, CA), by using the 2−ΔΔCT method [35]; data werenormalized with the housekeeping genes β-actin andGAPDH; primer efficiency in the real-time PCR reactionwas between 95% and 105% [36].
2.7. Bioinformatic Analysis of Ferroportin Protein Sequence.In order to evaluate whether a nuclear localization signal(NLS) is present in FPN, its protein sequence was analyzedby cNLS Mapper, a freely available software (http://nls-mapper.iab.keio.ac.jp/cgi-bin/NLS_Mapper_form.cgi). cNLSis a bioinformatic tool useful to predict the NLS specific forthe αβ importin pathway; it yields the NLS scores (levels ofNLS activities). Four NLS profiles are calculated: class 1/2,class 3, class 4, and bipartite NLSs. cNLS Mapper extractsputative NLS sequences with a score equal to or more thanthe selected cutoff score. Each amino acid residue at eachposition within an NLS class yields a score that sums up inorder to characterize the entire NLS activity. Higher scores(8, 9, or 10) indicate the exclusive localization in the nucleus;scores 7 or 8 indicate a partial localization in the nucleus;scores 3, 4, or 5 suggest that the protein is localized both inthe nucleus and in the cytoplasm. Scores 1 or 2 define theexclusive localization in the cytoplasm [37].
2.8. Confocal Analysis of Ferroportin. Confocal microscopywas used to study the presence of the FPN in the nuclei ofiPSC-derived cardiomyocytes. Sections were scanned witha Nikon Ti-E fluorescence microscope coupled to an A1Rconfocal system and the NIS-Elements AR 3.2 software. Adiode laser system with 405 wavelength output, air-cooledargon-ion laser system with 488 wavelength output, andyellow diode-pumped solid-state laser system with 561wavelength output were used. Images were acquired withoil immersion 60x with an optical resolution of 0.18 micron,2x scanner zoom, and 1024 × 1024 pixel resolution. All the zstacks were collected in compliance with optical section sep-aration (z interval) values suggested by the NIS-Elements AR3.2 software. Three random fields per sample were acquired,containing at least 10 cells per sample. Stacks were 0.850μmfor a total of 14 images. 3D images were analyzed by theImaris software (Bitplane, Concord, MA). The algorithm ofthe software is able to detect the nuclei, marked by DAPI,and create an isosurface on the blue fluorescence. Then, thegreen fluorescence, corresponding to the total FPN signal,
3Oxidative Medicine and Cellular Longevity

was quantified only inside the nuclei isosurfaces. In addition,the volume of each nucleus was measured and analyzed.
2.9. Western Blot Analysis. Cardiomyocytes were lysed in50mM Tris-HCl (pH8.0), 150mM NaCl, NP-40 1%, andprotease inhibitor mix (Roche, Sigma-Aldrich, Saint Louis,MO). Protein concentration was determined using Bradfordprotein assay (Bio-Rad Laboratories, Hercules, CA). 45μgof protein samples was solubilized in Laemmli buffer 4x(200mM Tris-HCl, pH6.8, 5% SDS, 25% glycerol, 0.04%bromophenol blue, and 5% beta-mercaptoethanol) for 1 hin ice bath. Precast gradient gels (Mini-PROTEAN TGXstain-free protein gel, 4-15% polyacrylamide) (Bio-Rad Lab-oratories, Hercules, CA) were used. Mini-PROTEAN TGXgels contain trihalo compounds, which, in the presence ofUV light, react with tryptophan residues producing fluores-cence, proportional to the total protein amount of the sam-ple. Gels were electroblotted onto nitrocellulose membranes(pore sizes: 0.45μm). Membranes were exposed to UV lightin order to visualize the protein band integrity and the effi-ciency of transfer. After blocking in Tris-buffered saline(TBS 1x) containing 0.1% Tween-20 (TBS-T), nonfat milk5%, and 1% BSA for 1 h at room temperature, membraneswere probed overnight at 4°C with the primary antibodiesand then washed three times with TBS-T and incubatedwith rabbit-IgG HRP-conjugated secondary antibody, dis-solved in blocking buffer for 1 hour at room temperature.Details about primary and secondary antibodies used arelisted in Table S2. Finally, membranes were incubated withECL chemiluminescent reagent (Western Bright ECL HRPsubstrate, Advansta, CA, USA) and exposed to an X-rayfilm (Aurogene s.r.l., Rome, Italy). Densitometric analysiswas performed by means of Bio-Rad Gel Doc 2000. Densityof specific protein bands was normalized to the β-actin band.
2.10. Statistical Analysis. For quantitative RT-PCR, statisticalanalysis was performed by the CFX Manager software(Bio-Rad Laboratories, Hercules, CA) and qbase plus(http://www.biogazelle.com/). For Western blot, the statis-tical analysis was performed by Student’s t-test. A value ofp < 0 05 was considered statistically significant.
3. Results
3.1. Cardiomyocyte Differentiation from hiPSCs. The differ-entiation of cardiomyocytes (CMs) from iPSCs was success-fully repeated four times. Movies SM1 and SM2, reported inthe Supplementary Materials, show beating CMs from bothcontrol and FRDA cultures. Notably, some of the beatingareas found in cardiomyocyte cultures derived from FRDAiPSCs were unsynchronized, in contrast with the remarkablesynchronization of control cardiomyocyte cultures.
3.2. Cardiomyocyte Characterization. The characterizationof cardiomyocyte differentiation was obtained by evaluat-ing the synthesis of four heart-specific genes: GATA4, atranscription factor specific for the cardiac lineage; SIRPA,a nonreceptorial tyrosine protein-phosphatase, exclusivelyexpressed on the surface of hiPSC-derived cardiomyocytes[38]; and TNNT2 and actinin 2, two cardiac structural
proteins. Messenger RNAs from control and FRDA CMsand iPSCs were compared by qRT-PCR and results areshown in Figure 1(a) as the average of four independentdifferentiation procedures. Cardiac-specific genes were sig-nificantly upregulated in CMs with respect to iPSCs inboth control and FRDA samples.
Moreover, TNNT2 protein was evaluated by FACS anal-ysis in CMs (Figure 1(b)). FACS analysis showed that the effi-ciency of CM differentiation from iPSCs was 80-90%.
Finally, the immunofluorescence analysis demon-strated that TNNT2 costained with the heavy myosin chain(MF20) proteins (Figure 1(c)) in both control and FRDACMs. TNNT2 fluorescence suggests that both control andFRDA CMs display the typical sarcomeric organization.
3.3. Maintenance of the FRDA-Like Phenotype in iPSCs andCMs. To determine whether FRDA iPSCs and CMs main-tained the FRDA-like phenotype, the gene expression ofFXN was analyzed. As expected, the expression of FXN genein FRDA iPSCs was about 30% of control iPSCs (Figure 2).Moreover, cardiac differentiation did not alter the patholog-ical phenotype; the expression of FXN in FRDA CMs wasabout 55% with respect to control. An average of fourindependent experiments is shown.
3.4. TFRC Gene Expression Is Upregulated in FRDA CMs. ThemRNA abundance of the key iron homeostasis-related geneswas assessed in control and FRDA CMs by qRT-PCR. Dataare shown in Figure 3 as the average of four independentdifferentiation procedures. The expression of transferrinreceptor (TFRC) was significantly increased in iPSC-CMsFRDA. Moreover, also the mRNA levels of HAMP, FPN,and ATOH8, a transcription factor involved in HAMP regu-lation, showed a trend to increase. No relevant difference wasevidenced in the expression of FTH1 gene.
3.5. Protein Expression of HAMP and FPN Is Increased inFRDA CMs. To validate gene expression data, the proteinamount of HAMP and FPN by Western blot was evaluatedin whole lysates of both CTR and FRDA CMs. A representa-tive image and the densitometric analysis of the bands areshown in Figures 4(a) and 4(b); the average of three indepen-dent differentiation experiments is reported. A significantincrease of HAMP and FPN (about 2.5 and 2.0 times, respec-tively) was found in FRDA CMs compared to controls. Itshould be noted that FPN antibody detects two bands, atabout 72 kDa and 62 kDa, respectively, both of which weremore intense in FRDA CMs with respect to controls. Rosset al. [39] described two FPN bands, at ~65 and ≈55 kDa,respectively, in T-REx™/FPN-V5 cells and demonstrated thatthe heavier isoform was glycosylated.
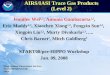
3.6. FPN Nuclear Localization in iPSC-Derived CMs. FPNprotein localization and expression was assessed by immu-nostaining using confocal microscopy. Figure 5(a) clearlydemonstrates a nuclear localization of FPN in both CTRand FRDA CMs. Moreover, the analysis of FITC fluorescenceintensity (Figure 5(b)) showed that (i) the amount of FPNwas significantly lower in the nuclei from FRDA CMs com-pared to controls and (ii) decrease was stronger when
4 Oxidative Medicine and Cellular Longevity

normalized to the volume of the nucleus, which (iii) is greaterin FRDA CMs than in control. Since the nuclear localizationof FPN had not been previously described, we used the cNLSMapper software to identify, if present, nuclear localizationsignals (NLS) in the FPN protein sequence (NP_055400).This analysis revealed three predicted bipartite nuclearlocalization sequences: a sequence of 29 aa in 223 position
(LWKVYQKTPALAVKAGLKEEETELKQLNL) with 3.3score, a sequence of 32 aa (WLRRKCGLVRTGLISGLAQL-SCLILCVISVF) in 362 position with 3.1 score, and finallya sequence of 29 aa (KAGLKEEETELKQLNLHKDTEPK-PLEGTH) in 236 position with 3.8 score (Figure 5(c)). TheNLS score analysis suggests that FPN can be localized in boththe nucleus and cytoplasm.
0400800
120016002000
Fold
chan
ge
GATA4
CTRiPSCs
FRDAiPSCs
CTRCMs
FRDACMs
CTRiPSCs
FRDAiPSCs
CTRCMs
FRDACMs
CTRiPSCs
FRDAiPSCs
CTRCMs
FRDACMs
CTRiPSCs
FRDAiPSCs
CTRCMs
FRDACMs
0 05
10152025 SIRPA
Fold
chan
ge
50100150200250300
Fold
chan
ge
TNNT2
050
100150200250300350 Actinin 2
Fold
chan
ge⁎⁎⁎⁎
⁎⁎
⁎⁎
⁎⁎ ⁎⁎⁎⁎
(a)
100 101 102 103 104100 101 102 103 104100 101 102 103 104100 101 102 103 104
0
40
80
120
160
200
FL1-H
Cou
nts
0
40
80
120
160
200
FL1-H
Cou
nts
M1
M2
0
40
80
120
160
200
FL1-H
Cou
nts
M1
M2
0
40
80
120
160
200
FL1-H
Cou
nts
M1
M2
CTR CMs NC M1 = 2,91% M1 = 94,65 %
M2 = 52,99 %
CTR CMs FRDA CMs NC M1 = 2,93 %M2 = 0,02 %
FRDA CMs M1 = 90,94 %M2 = 51,97 %
M1
(b)
CTR CMs
TNN
T2M
F 20
DA
PIM
erge
FRDA CMs
(c)
Figure 1: Characterization of CTR and FRDA iPSCs and iPSC-derived CMs. (a) Gene expression of four specific cardiac genes, GATA4,SIRPA, TNNT2, and actinin 2 characterized by qRT-PCR. Data were normalized with two housekeeping genes, β-actin and GAPDH; foreach gene, the normalized expression value of CTR iPSCs was set to 1, and all other gene expression data were reported to that sample.PCR was run in triplicate; data are from four independent differentiation experiments and are expressed as mean ± SEM. ∗p < 0 05; ∗∗p <0 01. (b) A representative flow cytometer analysis of CTR and FRDA CMs stained with TNNT2. NC negative control was stained withsecondary antibody only; M1: percentage of TNNT2-positive CMs; M2: percentage of CMs highly positive to TNNT2. (c) A representativeimmunofluorescence image of CTR and FRDA CMs. TNNT2 is stained in green; heavy myosin chain (MF 20) is stained in red; the nucleiare stained with DAPI (blue). Scale bar 50 μm.
5Oxidative Medicine and Cellular Longevity

4. Discussion
In the present study, we describe some relevant features ofiron homeostasis in iPSC-derived cardiomyocytes from onehealthy control and one FRDA-affected patient. Cardiomyo-cytes were shown to fully express cardiac differentiationmarkers. Both FRDA iPSCs and CMs maintained the patho-logical phenotype, characterized by low levels of frataxinmRNA; however, frataxin expression in FRDA CMs wasnot as reduced as in iPSCs relative to control CMs. A similarresult was reported by Hick et al. [40], who ascribed such dif-ference to the reduced number of GAA repeats in the CMbeating areas with respect to iPSCs of the same subject. Spon-taneously beating areas were observed at 9-12 days from thestart of the induction procedure, but FRDA beating areaswere desynchronized, in agreement with similar resultsreported by Hick et al. [40].
Several studies pointed out the importance of ironhomeostasis in the cardiac tissue; however, to date, the localregulation of iron in cardiomyocytes has not been fully char-acterized. In particular, the HAMP-FPN axis seems to be cru-cial for heart function [15, 22, 23]. Cardiac iron dysregulationwas described in several disorders including FRDA, which ischaracterized by iron maldistribution within subcellularcompartments, leading to mitochondrial iron accumulationand cytosolic iron depletion [5, 28, 41]. In the present study,cardiomyocytes were derived from CTR and FRDA humaniPSCs in order to study some features of iron homeostasis,focusing the attention to the HAMP-FPN axis. This cellularmodel was already exploited by Lee et al. [42] to study thegene and protein expression of a group of iron-handling pro-teins in FRDA. To our knowledge, iron distribution withinthe cell compartments has not yet been evaluated in theiPSC-derived CM cellular model. The lack of such evaluationis a limitation of the present study, but this issue will beaddressed in future research.
In the present study, a number of iron homeostasis-related genes and proteins were found to be dysregulated inFRDA CMs. Elevated HAMP expression has been alreadydescribed in FRDA autoptic heart tissues [24], but theauthors attributed HAMP overexpression to macrophagicinflammatory infiltrate. On the contrary, our results suggestthat the increase in HAMP content is due to its overexpres-sion in FRDA CMs.
In turn, HAMP downregulates the cellular amount ofFPN, causing its lysosomal degradation [10, 11]. At variancewith the expected decrease of FPN levels, HAMP upregulationin FRDA CMs was not accompanied by a decrease in FPN,rather a significant increase of FPN (protein) was observed.
In a different context, both FPN and HAMP werefound to be significantly decreased in brain tissue of Alz-heimer’s disease patients, where oxidative stress is knownto occur [43].
Our data show that the upregulation of HAMP and FPNin FRDA CMs is accompanied by the upregulation of TFRC.Huang et al. [44] found a decrease of FPN and an increase ofTFRC in the heart of a conditional frataxin knockout (mutant)mice. It is difficult to compare our in vitro data with this study,which makes use of an animal model, where a complex inter-play between local and systemic iron homeostasis takes place,and where frataxin expression is almost completely abolished.It is our opinion that our observations may reflect a dysregu-lation of these iron-handling proteins in FRDA CMs. Since itis known that oxidative stress affects FRDA neuronal and car-diac cells [45], it is possible that FPN loses its responsiveness toHAMP downregulation owing to the oxidation of key cysteineresidues located in the HAMP- and FPN-interacting sites[46–48]. It can be envisioned that these cysteine residuesare not oxidized in a “normal” low iron context, where oxida-tive stress is not present and HAMP downregulates FPN inorder to avoid a further iron depletion. However, in the cyto-plasm of FRDA cardiomyocytes, an unusual concurrence oflow iron concentration AND oxidative stress is present, whichwould favor the inability of HAMP to downregulate FPN andto avoid iron leakage. Obviously, this is only one out of severalother hypotheses, and further investigations need to be carriedout for its validation or disproval.
The presence of FPN in the nuclei of CTR and FRDACMs was demonstrated in this study for the first time. Thisfinding suggests that FPN, traditionally considered as a trans-membrane protein, could play a role in the maintenance ofnuclear iron homeostasis. Henle et al. [49] described spe-cific iron-binding sites on DNA. Moreover, other proteinsinvolved in iron cellular trafficking, such as the divalent metaltransporter 1 (DMT1), lactoferrin, and ferritin [27], havebeen found in the nuclear compartment. It is possible thatthe nuclear localization of FPN underscores a protective rolefrom excess free iron in the nuclear compartment. Surpris-ingly, we found a lesser amount of nuclear FPN in FRDA car-diomyocytes with respect to controls, a result that seems tosupport the finding of DNA oxidative stress markers(8-OXO-dg) in FRDA patients [50]. On the other hand, thefact that FPN is less abundant in the nuclei of FRDA CMsthan in controls is not necessarily in contradiction with theincrease in both mRNA and protein FPN in FRDA
Fold
chan
ge
0
0.5
1
1.5
CTR iPSCs FRDA iPSCs CTR CMs
FXN
⁎⁎⁎
⁎
FRDA CMs
Figure 2: Evaluation of the FRDA-like phenotype in iPSCs andCMs. qRT-PCR of FXN gene expression in both CTR and FRDAiPSCs and CMs. Data were normalized with two housekeepinggenes, β-actin and GAPDH; the normalized FXN expression valueof CTR iPSCs was set to 1, and all other gene expression datawere reported to that sample. Data are from four independentdifferentiation experiments and are expressed as mean ± SEM.∗p < 0 05; ∗∗∗p < 0 001.
6 Oxidative Medicine and Cellular Longevity

TFRC
Fold
chan
ge
0
0.5
1
1.5
2
2.5
CTR CMs0
0.5
1
1.5
2
2.5
3
3.5 HAMP
Fold
chan
ge
Fold
chan
ge
Fold
chan
ge
Fold
chan
ge
0
0.5
1
1.5
2
2.5FPN
0
0.5
1
1.5
2
2.5ATOH8
0
0.5
1
1.5
2
2.5FTH1
FRDA CMs CTR CMs FRDA CMs CTR CMs FRDA CMs
CTR CMs FRDA CMsCTR CMs FRDA CMs
⁎⁎⁎
Figure 3: Gene expression of proteins involved in iron homeostasis in CTR and FRDA CMs. Expression levels of TFRC, HAMP, FPN,ATOH8, and FTH1 genes in CTR and FRDA CMs evaluated by qRT-PCR. Data were normalized with two housekeeping genes, β-actinand GAPDH; for each gene, the normalized expression value of CTR CMs was set to 1, and all other gene expression data were reportedto that sample. Data are from four independent differentiation experiments and are expressed as mean± SEM. ∗∗∗p < 0 001.
0
0.2
0.4
0.6
0.8
HA
MP/�훽
-Act
in
HAMP
�훽-Actin
28 kDa
42 kDa
CTR CMs FRDA CMs
⁎⁎
(a)
⁎
72 kDa
42 kDa
62 kDa FPN
�훽-Actin
CTR CMs FRDA CMs
0
1
2
3
4
5
FPN
/�훽-A
ctin
(b)
Figure 4: Protein expression of HAMP and FPN. (a) A representative Western blot image of HAMP expression. The band densities wereanalyzed by densitometry and normalized to β-actin. Histogram showing means ± StdDev of HAMP/β-actin. (b) A representativeWestern blot image of FPN expression. The band densities were analyzed by densitometry and normalized to β-actin. Histogram showingmeans ± StdDev of FPN/β-actin. Data are from three independent differentiation experiments. ∗p < 0 05; ∗∗p < 0 01.
7Oxidative Medicine and Cellular Longevity

CTR CMs FRDA CMs
(a)
0
200
400
600
800
Nuc
lear
fluo
resc
ence
inte
nsity
CTR CMs FRDA CMs Nuc
lear
fluo
resc
ence
inte
nsity
/Av
erag
e nuc
lear
vol
ume
0
0.5
1
1.5
CTR CMs FRDA CMs 0
400
800
1200
1600
Aver
age n
ucle
i vol
ume
CTR CMs FRDA CMs
⁎⁎⁎ ⁎⁎⁎ ⁎⁎⁎
(b)
223
236
362
3.3
3.8
3.1
Pos.
Pos.
Sequence
Sequence
Predicted bipartite NLS
Predicted monopartite NLS
Score
Score
Predicted NLSs in query sequence
1 3 5 8 10Exclusively cytoplasmiclocalization
Both nuclear andcytoplasmic localization
Partially Nuclearlocalization
Exclusively Nuclearlocalization
FPNScore values
(c)
Figure 5: FPN nuclear localization in iPSC-derived CMs. (a) A representative confocal microscopy 3D image projection of FITC-stained FPN(green) protein expression in both CTR and FRDA CMs; the nuclei are counterstained with DAPI (blue). Scale bar equal 10 μm. (b) (i)Quantitative analysis of nuclear FITC fluorescence intensity in both CTR and FRDA CMs, (ii) quantitative analysis of nuclear FITCfluorescence intensity normalized to the average nuclear volume in both CTR and FRDA CMs, and (iii) average nuclear volume in bothCTR and FRDA CMs; ∗∗∗p < 0 001. (c) Bioinformatic analysis of FPN (NP_055400), using cNLS Mapper, predicted three bipartite NLSwith a score value >3 indicating that the protein localizes both in the nucleus and in the cytoplasm.
8 Oxidative Medicine and Cellular Longevity

cardiomyocytes, since Western blots were carried out inwhole cell lysates, which include cytoplasmic FPN. A limita-tion of the present study is the lack of quantification of cyto-plasmic FPN, either by confocal microscopy (which wouldrequire the delimitation of cell boundary by a specific stain-ing) or by subcellular fractioning. This will be addressed byfuture studies.
The regulation of FPN distribution among the differentsubcellular compartments is a relevant issue, not yet affordedby researchers; in fact, the presence of 9-12 transmembranedomains supports its localization in the plasma membraneand its role of iron exporter and makes less likely a cytoplas-mic and a nuclear localization. Thus, the nuclear localizationof FPN we document here needs to be discussed not only interms of novel FPN function(s), but also within the contextof membrane and organelle trafficking and of final destina-tion of proteins characterized by hydrophobic domains call-ing for a plasma membrane localization.
Finally, the presence of the enlarged nuclei, which wasdescribed here to occur in FRDA cardiomyocytes, has beenreported in other cardiac pathologies, such as in hypertro-phic and in dilated cardiomyopathy [51]. These morpholog-ical data need to be further investigated.
5. Conclusions
Cardiomyocytes derived from iPSCs retained the FRDA-likephenotype. Important alterations in the expression of HAMPand FPN, two proteins that play pivotal roles in cardiac ironhomeostasis, are described here. Moreover, a novel nuclearlocalization of FPN in cardiomyocytes is reported, whichsuggests a potential new physiological function of this pro-tein. These findings may have important implications in theunderstanding of cardiac iron homeostasis in both physio-logical and pathological conditions, such as FRDA. In partic-ular, FRDA cardiomyocytes appear to be unable to exploitHAMP-operated regulation of FPN, which might be one ofthe reasons why iron distribution within the cell is impaired,thus leading to increase in the free iron pool. This, togetherwith the defective assembly of mitochondrial proteins, wouldlead to chronic oxidative stress in FRDA cardiac cells. Aspointed out by many authors [52–54], oxidative stress doesnot only lead to cell damage and apoptosis but also plays arole in adverse remodeling and contractile dysfunctions, asseen in FRDA patients.
Abbreviations
ATOH8: Atonal BHLH transcription factor 8BMPs: Bone morphogenetic proteinsCMs: CardiomyocytesDMT1: Divalent metal transporter 1FACS: Flow cytometryFPN: FerroportinFRDA: Friedreich’s ataxiaFTH1: Ferritin heavy chain 1FXN: Frataxin geneGAPDH: Glyceraldehyde-3-phosphate dehydrogenaseHAMP: Hepcidin
HH: Hereditary hemochromatosishiPSCs: Human-induced pluripotent stem cellsIF: ImmunofluorescenceIREs: Iron regulatory elementsIRPs: Iron regulatory proteinsISC: Iron-sulfur clusterLIP: Labile iron poolMF 20: Myosin heavy chainNLS: Nuclear localization signalROS: Reactive oxygen speciesTFRC: Transferrin receptor 1TNNT2: Cardiac troponin TTMs: Transmembrane domains.
Data Availability
The data used to support the findings of this study are avail-able from the corresponding author upon request.
Disclosure
The funding organizations had no role in the study design,data collection and analysis, decision to publish, or prepara-tion of the manuscript.
Conflicts of Interest
Authors declare the absence of conflicts of interest. Theauthors hereby declare that they have no financial relation-ships to disclose in relation to this article.
Authors’ Contributions
Marina Marini and Cinzia Zucchini share coseniorship.
Acknowledgments
This work has been supported by a grant from the AISA(Italian Association of Patients with Ataxic Syndrome)and by a grant from the “Fondazione Luisa Fanti Melloni,”University of Bologna, Italy. The authors would like tothank Dr. Filippo Fortuna for believing in this research andfor supporting it in any possible way and Dr. Martina Rossifor her help.
Supplementary Materials
Supplementary 1. Table S1: phenotypic data of control sub-ject and FRDA patient from which iPSCs were generated byCoriell Institute Repositories. Table S2: list of primary andsecondary antibodies used in cytofluorimetry (FACS),immunofluorescence (IF), and Western blot (WB) analysis.Table S3: primer sequences and amplicon length of the genesanalyzed by real-time PCR in iPSC-derived cardiomyocytes.β-Actin and GADPH were used as housekeeping genes.
Supplementary 2. Figure S1: timeline of iPSC-derived cardio-myocyte differentiation protocol.
Supplementary 3. SM1: CTR cardiomyocytes.
Supplementary 4. SM2: FRDA cardiomyocytes.
9Oxidative Medicine and Cellular Longevity

References
[1] R. Gozzelino and P. Arosio, “Iron homeostasis in health anddisease,” International Journal of Molecular Sciences, vol. 17,no. 1, 2016.
[2] M. F. Hoes, N. Grote Beverborg, J. D. Kijlstra et al., “Iron defi-ciency impairs contractility of human cardiomyocytes throughdecreased mitochondrial function,” European Journal of HeartFailure, vol. 20, no. 5, pp. 910–919, 2018.
[3] S. Dev and J. L. Babitt, “Overview of iron metabolism in healthand disease,” Hemodialysis International, vol. 21, Supplement1, pp. S6–S20, 2017.
[4] E. Gammella, S. Recalcati, I. Rybinska, P. Buratti, and G. Cairo,“Iron-induced damage in cardiomyopathy: oxidative-dependent and independent mechanisms,” Oxidative Medi-cine and Cellular Longevity, vol. 2015, Article ID 230182,10 pages, 2015.
[5] D. J. R. Lane, A. M. Merlot, M. L.-H. Huang et al., “Cellulariron uptake, trafficking and metabolism: key molecules andmechanisms and their roles in disease,” Biochimica et Biophy-sica Acta (BBA) - Molecular Cell Research, vol. 1853, no. 5,pp. 1130–1144, 2015.
[6] K. C. Kondapalli, N. M. Kok, A. Dancis, and T. L. Stemmler,“Drosophila frataxin: an iron chaperone during cellular Fe-Scluster bioassembly,” Biochemistry, vol. 47, no. 26, pp. 6917–6927, 2008.
[7] S. Abboud and D. J. Haile, “A novel mammalianiron-regulated protein involved in intracellular iron metabo-lism,” Journal of Biological Chemistry, vol. 275, no. 26,pp. 19906–19912, 2000.
[8] A. Donovan, A. Brownlie, Y. Zhou et al., “Positional cloningof zebrafish ferroportin1 identifies a conserved vertebrateiron exporter,” Nature, vol. 403, no. 6771, pp. 776–781,2000.
[9] A. T. McKie, P. Marciani, A. Rolfs et al., “A novel duodenaliron-regulated transporter, IREG1, implicated in the basolat-eral transfer of iron to the circulation,” Molecular Cell, vol. 5,no. 2, pp. 299–309, 2000.
[10] H. Drakesmith, E. Nemeth, and T. Ganz, “Ironing out ferro-portin,” Cell Metabolism, vol. 22, no. 5, pp. 777–787, 2015.
[11] D. M. Ward and J. Kaplan, “Ferroportin-mediated iron trans-port: expression and regulation,” Biochimica et BiophysicaActa, vol. 1823, no. 9, pp. 1426–1433, 2012.
[12] I. De Domenico, D. M. Ward, G. Musci, and J. Kaplan, “Evi-dence for the multimeric structure of ferroportin,” Blood,vol. 109, no. 5, pp. 2205–2209, 2007.
[13] E. Pignatti, L. Mascheroni, M. Sabelli, S. Barelli, S. Biffo, andA. Pietrangelo, “Ferroportin is a monomer in vivo in mice,”Blood Cells, Molecules, and Diseases, vol. 36, no. 1, pp. 26–32,2006.
[14] A. E. Rice, M. J. Mendez, C. A. Hokanson, D. C. Rees, andP. J. Bjorkman, “Investigation of the biophysical and cell bio-logical properties of ferroportin, a multipass integral mem-brane protein iron exporter,” Journal of Molecular Biology,vol. 386, no. 3, pp. 717–732, 2009.
[15] D. Vela, “Balance of cardiac and systemic hepcidin and its rolein heart physiology and pathology,” Laboratory Investigation,vol. 98, no. 3, pp. 315–326, 2018.
[16] P. J. Schmidt, “Regulation of iron metabolism by hepcidinunder conditions of inflammation,” Journal of BiologicalChemistry, vol. 290, no. 31, pp. 18975–18983, 2015.
[17] L. Kautz, D. Meynard, A. Monnier et al., “Iron regulates phos-phorylation of Smad1/5/8 and gene expression of Bmp6,Smad7, Id1, and Atoh8 in the mouse liver,” Blood, vol. 112,no. 4, pp. 1503–1509, 2008.
[18] U. Merle, E. Fein, S. G. Gehrke, W. Stremmel, and H. Kulaksiz,“The iron regulatory peptide hepcidin is expressed in the heartand regulated by hypoxia and inflammation,” Endocrinology,vol. 148, no. 6, pp. 2663–2668, 2007.
[19] G. Simonis, K. Mueller, P. Schwarz et al., “The iron-regulatorypeptide hepcidin is upregulated in the ischemic and in theremote myocardium after myocardial infarction,” Peptides,vol. 31, no. 9, pp. 1786–1790, 2010.
[20] L. Zhang, D. Lu, W. Zhang et al., “Cardioprotection by Hepc1in cTnTR141W transgenic mice,” Transgenic Research, vol. 21,no. 4, pp. 867–878, 2012.
[21] Y. P. Hsieh, C. H. Huang, C. Y. Lee, C. Y. Lin, and C. C. Chang,“Silencing of hepcidin enforces the apoptosis in iron-inducedhuman cardiomyocytes,” Journal of Occupational Medicineand Toxicology, vol. 9, no. 1, p. 11, 2014.
[22] S. Lakhal-Littleton, M.Wolna, C. A. Carr et al., “Cardiac ferro-portin regulates cellular iron homeostasis and is important forcardiac function,” Proceedings of the National Academy of Sci-ences, vol. 112, no. 10, pp. 3164–3169, 2015.
[23] S. Lakhal-Littleton, M. Wolna, Y. J. Chung et al., “An essentialcell-autonomous role for hepcidin in cardiac iron homeosta-sis,” Elife, vol. 5, 2016.
[24] A. H. Koeppen, R. L. Ramirez, A. B. Becker et al., “The patho-genesis of cardiomyopathy in Friedreich ataxia,” PLoS One,vol. 10, no. 3, article e0116396, 2015.
[25] Y. Wu and R. M. Brosh, “DNA helicase and helicase-nucleaseenzymes with a conserved iron-sulfur cluster,” Nucleic AcidsResearch, vol. 40, no. 10, pp. 4247–4260, 2012.
[26] A. S. Fleischhacker and P. J. Kiley, “Iron-containing transcrip-tion factors and their roles as sensors,” Current Opinion inChemical Biology, vol. 15, no. 2, pp. 335–341, 2011.
[27] K. J. Thompson, M. G. Fried, Z. Ye, P. Boyer, and J. R. Connor,“Regulation, mechanisms and proposed function of ferritintranslocation to cell nuclei,” Journal of Cell Science, vol. 115,Part 10, pp. 2165–2177, 2002.
[28] S. Michael, S. V. Petrocine, J. Qian et al., “Iron andiron-responsive proteins in the cardiomyopathy of Frie-dreich’s ataxia,” Cerebellum, vol. 5, no. 4, pp. 257–267, 2006.
[29] A. Y. Tsou, E. K. Paulsen, S. J. Lagedrost et al., “Mortality inFriedreich ataxia,” Journal of the Neurological Sciences,vol. 307, no. 1-2, pp. 46–49, 2011.
[30] V. Campuzano, L. Montermini, M. D. Molto et al., “Frie-dreich’s ataxia: autosomal recessive disease caused by an intro-nic GAA triplet repeat expansion,” Science, vol. 271, no. 5254,pp. 1423–1427, 1996.
[31] M. Pandolfo, “Iron metabolism and mitochondrial abnormal-ities in Friedreich ataxia,” Blood Cells, Molecules and Diseases,vol. 29, no. 3, pp. 536–547, 2002.
[32] K. Takahashi and S. Yamanaka, “Induction of pluripotentstem cells from mouse embryonic and adult fibroblast culturesby defined factors,” Cell, vol. 126, no. 4, pp. 663–676, 2006.
[33] X. Lian, J. Zhang, S. M. Azarin et al., “Directed cardiomyocytedifferentiation from human pluripotent stem cells by modulat-ing Wnt/β-catenin signaling under fully defined conditions,”Nature Protocols, vol. 8, no. 1, pp. 162–175, 2012.
[34] P. M. Abruzzo, M. Marini, A. Bolotta et al., “Frataxin mRNAisoforms in FRDA patients and normal subjects: effect of
10 Oxidative Medicine and Cellular Longevity

tocotrienol supplementation,” BioMed Research International,vol. 2013, Article ID 276808, 9 pages, 2013.
[35] K. J. Livak and T. D. Schmittgen, “Analysis of relativegene expression data using real-time quantitative PCR andthe 2(-delta delta C(T)) method,” Methods, vol. 25, no. 4,pp. 402–408, 2001.
[36] M. W. Pfaffl, “A new mathematical model for relative quanti-fication in real-time RT-PCR,” Nucleic Acids Research,vol. 29, no. 9, pp. 45e–445, 2001.
[37] S. Kosugi, M. Hasebe, N. Matsumura et al., “Six classes ofnuclear localization signals specific to different bindinggrooves of importin α,” Journal of Biological Chemistry,vol. 284, no. 1, pp. 478–485, 2008.
[38] N. C. Dubois, A. M. Craft, P. Sharma et al., “SIRPA is a specificcell-surface marker for isolating cardiomyocytes derived fromhuman pluripotent stem cells,” Nature Biotechnology, vol. 29,no. 11, pp. 1011–1018, 2011.
[39] S. L. Ross, K. Biswas, J. Rottman et al., “Identification of anti-body and small molecule antagonists of ferroportin-hepcidininteraction,” Frontiers in Pharmacology, vol. 8, p. 838, 2017.
[40] A. Hick, M. Wattenhofer-Donze, S. Chintawar et al., “Neuronsand cardiomyocytes derived from induced pluripotent stemcells as a model for mitochondrial defects in Friedreich’sataxia,” Disease Models & Mechanisms, vol. 6, no. 3, pp. 608–621, 2013.
[41] H. Puccio, D. Simon, M. Cossée et al., “Mouse models for Frie-dreich ataxia exhibit cardiomyopathy, sensory nerve defectand Fe-S enzyme deficiency followed by intramitochondrialiron deposits,” Nature Genetics, vol. 27, no. 2, pp. 181–186,2001.
[42] Y.-K. Lee, P. W.-L. Ho, R. Schick et al., “Modeling ofFriedreich ataxia-related iron overloading cardiomyopathyusing patient-specific-induced pluripotent stem cells,” PflügersArchiv - European Journal of Physiology, vol. 466, no. 9,pp. 1831–1844, 2014.
[43] A. Raha, R. Vaishnav, R. Friedland, A. Bomford, andR. Raha-Chowdhury, “The systemic iron-regulatory proteinshepcidin and ferroportin are reduced in the brain in Alzhei-mer’s disease,” Acta Neuropathologica Communications,vol. 1, no. 1, p. 55, 2013.
[44] M. L.-H. Huang, E. M. Becker, M. Whitnall, Y. S. Rahmanto,P. Ponka, and D. R. Richardson, “Elucidation of the mecha-nism of mitochondrial iron loading in Friedreich’s ataxia byanalysis of a mouse mutant,” Proceedings of the National Acad-emy of Sciences, vol. 106, no. 38, pp. 16381–16386, 2009.
[45] M. Perdomini, A. Hick, H. Puccio, and M. A. Pook, “Animaland cellular models of Friedreich ataxia,” Journal of Neuro-chemistry, vol. 126, Supplement 1, pp. 65–79, 2013.
[46] X. B. Liu, F. Yang, and D. J. Haile, “Functional consequences offerroportin 1 mutations,” Blood Cells, Molecules, and Diseases,vol. 35, no. 1, pp. 33–46, 2005.
[47] A. Fernandes, G. C. Preza, Y. Phung et al., “The molecularbasis of hepcidin-resistant hereditary hemochromatosis,”Blood, vol. 114, no. 2, pp. 437–443, 2009.
[48] J. B. Jordan, L. Poppe, M. Haniu et al., “Hepcidin revisited,disulfide connectivity, dynamics, and structure,” Journal ofBiological Chemistry, vol. 284, no. 36, pp. 24155–24167, 2009.
[49] E. S. Henle, Z. Han, N. Tang, P. Rai, Y. Luo, and S. Linn,“Sequence-specific DNA cleavage by Fe2+-mediated Fentonreactions has possible biological implications,” Journal of Bio-logical Chemistry, vol. 274, no. 2, pp. 962–971, 1999.
[50] J. B. Schulz, T. Dehmer, L. Schols et al., “Oxidative stress inpatients with Friedreich ataxia,” Neurology, vol. 55, no. 11,pp. 1719–1721, 2000.
[51] P. A. Harvey and L. A. Leinwand, “The cell biology of disease:cellular mechanisms of cardiomyopathy,” The Journal of CellBiology, vol. 194, no. 3, pp. 355–365, 2011.
[52] M. Seddon, Y. H. Looi, and A. M. Shah, “Oxidative stress andredox signalling in cardiac hypertrophy and heart failure,”Heart, vol. 93, no. 8, pp. 903–907, 2007.
[53] D. B. Sawyer, “Oxidative stress in heart failure: what are wemissing?,” The American Journal of the Medical Sciences,vol. 342, no. 2, pp. 120–124, 2011.
[54] H. Tsutsui, S. Kinugawa, and S. Matsushima, “Oxidative stressand heart failure,” American Journal of Physiology-Heart andCirculatory Physiology, vol. 301, no. 6, pp. H2181–H2190,2011.
11Oxidative Medicine and Cellular Longevity

Stem Cells International
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Disease Markers
Hindawiwww.hindawi.com Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwww.hindawi.com Volume 2013
Hindawiwww.hindawi.com Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwww.hindawi.com Volume 2018
PPAR Research
Hindawi Publishing Corporation http://www.hindawi.com Volume 2013Hindawiwww.hindawi.com
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwww.hindawi.com Volume 2018
Journal of
ObesityJournal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwww.hindawi.com Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwww.hindawi.com Volume 2018
Diabetes ResearchJournal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Research and TreatmentAIDS
Hindawiwww.hindawi.com Volume 2018
Gastroenterology Research and Practice
Hindawiwww.hindawi.com Volume 2018
Parkinson’s Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwww.hindawi.com
Submit your manuscripts atwww.hindawi.com