Embed Size (px)
Citation preview

SYMPOSIUM: SOCIAL PAEDIATRICS
New insights into airpollution and children’shealthJonathan Grigg
AbstractAir pollution remains a major threat to children’s health. In high-income
countries, most outdoor air pollution is from fossil fuel combustion, and
most indoor pollution is from cooking and environmental tobacco smoke
(ETS). Outdoor pollution in medium- and low-income countries is a mix of
fossil-fuel, solid fuel (e.g. coal) and biomass (wood), and indoor pollution
is from biomass smoke, solid fuels and ETS. Over the last decade, new data
suggest that both biomass smoke and ETS increases the vulnerability of
children to bacterial pneumonia, and that fossil-fuel and biomass smoke
impair children’s neurocognitive development. Further research is needed
to establish biological plausibility for these associations.
Keywords air pollution; biomass; children; environmental tobacco
smoke; fossil-fuel; neurocognitive impairment; pneumonia
Children are especially vulnerable to the adverse effects of envi-
ronmental pollution. Pollutants are either inhaled, or ingested, or
absorbed through the skin. There are many potential environ-
mental threats to children’s health, and for most the evidence base
is unclear. For example, teasing out the independent effect of
a single chemical amongst thousands of compounds is nearly
impossible. For chemicals, regulatory agenciesmust therefore take
a precautionary approach i.e. to not wait for definitive proof to
protect children’s health. One area where causal association, is
certain, yet exposure of children still occurs, is air pollution. A
previous review in this journal of the effects of traffic-derived air
pollution, focused on inhalable particulatematter (PM less than 10
microns in aerodynamic diameter; PM10), and addressed lung
growth and prevalence of respiratory symptoms. The aim of this
review is to focus on new insights into the adverse effects of air
pollution, both indoor and outdoor, on children’s health.
Traffic-derived air pollution
Recent studies suggest that inhalation of traffic-derived pollutants
has non-respiratory effects on the developing nervous system.
Franco Suglia et al, estimated the exposure of 202 school-age
children to black carbon (i.e. traffic-derived soot) at the home
address, and found that black carbon was independently associ-
ated with decreases in a range of neurocognitive variables such as
vocabulary, and composite intelligence quotient. To date, the
mechanism that links deposition of black carbon PM in the lung to
Jonathan Grigg MD is Professor of Paediatric Respiratory and
Environmental Medicine at the Centre for Paediatrics in the Blizard
Institute, Barts and the London School of Medicine, London, UK.
Conflict of interest: none.
PAEDIATRICS AND CHILD HEALTH 22:5 198
impairment of brain function is unclear. Indeed, the possibility of
a confounding variable (e.g. noise) cannot be excluded. However,
there are proof-of-concept studies suggesting that airway PM
affects brain function. For example, Yokota et al instilled diesel
exhaust PM into the nose of 2-week old infant rats once a week for
4 weeks and found that PM-treated animals showed a lower
avoidance performance than control animals given sham-instil-
lation. Furthermore, therewas a trend for levels of dopamine in the
medial mammillary nucleus of the brain to be lower in the PM-
treated animals. Histological examination of the brain showed
no evidence that PM had penetrated into the nervous system e
suggesting that this effect was mediated by indirect mechanisms.
The effect of maternal inhalation of traffic-derived pollution on
the developing fetus has been identified in recent studies with
sufficient power to detect independent effects. In a study of over
70,000 singleton births in Canada, Brauer et al estimated exposure
to air pollution at mothers’ residence and found that living within
50mof amain roadwas associatedwith a 22%increase in low-birth
weight.Whenexposure to air pollutantswasmodelled individually,
all air pollutants other than ozone, were associated with small for
gestational age. An effect of air pollution on preterm birth was also
founde albeit only for PM2.5. Similarly in a US study, Wihelm and
Ritz reported an association betweenmodelled exposure ofmothers
to traffic-derived PM- and risk for preterm birth and term low-birth
weight. How PM impacting in the lungs of mothers could influence
the developing fetus is unclear. A possible mechanism is that PM
alters the pattern of cytokines in the maternal and fetal circulation.
Some evidence for this phenomenon was recently provided by
Latzin et al who studied a birth cohort of 265 healthy term-born
neonates and found that mean PM10 over the last 3 months of
pregnancy was associated with increased interleukin-1 beta in cord
blood. In summary, although the evidence base is limited these
epidemiological associations are of concern and establishing bio-
logical plausibility in animal models is urgently needed.
Indoor air pollution
Indoor air pollutants either penetrate into the home from the
outside or are generated within the home. In high-income
countries, penetrating indoor pollution is mainly from traffic-
derived emissions. Thus both PM and vehicular-emitted gases
such as nitrogen dioxide (NO2) are higher in homes near main
roads than those near to less heavily used roads. For example,
Esplugues et al found higher concentrations of NO2 in homes
located on streets with a high frequency of vehicle traffic. The
major sources of indoor-generated air pollutants are cooking and
parental smoking e and both sources produce PM and NO2.
PM in homes with smokers is up to 15 mg/m3 higher than non-
smoking homes. Although there is substantial body of evidence
showing that exposure of children to passive environmental
tobacco smoke (ETS) is associated with increased respiratory
symptom prevalence e including cough and wheeze, there has
always been the question whether exposure of children to
secondhand smoke causes asthma. Strong evidence for a causal
link between ETS and asthma has recently been provided by
a systematic review of data from eight cohort studies. This meta-
analysis showed that the adjusted predicted relative risk for
a secondhand smoke effect on incident asthma is 1.33 (95% CI,
1.14e1.56) e an association strongest in school-age children.
� 2011 Elsevier Ltd. All rights reserved.

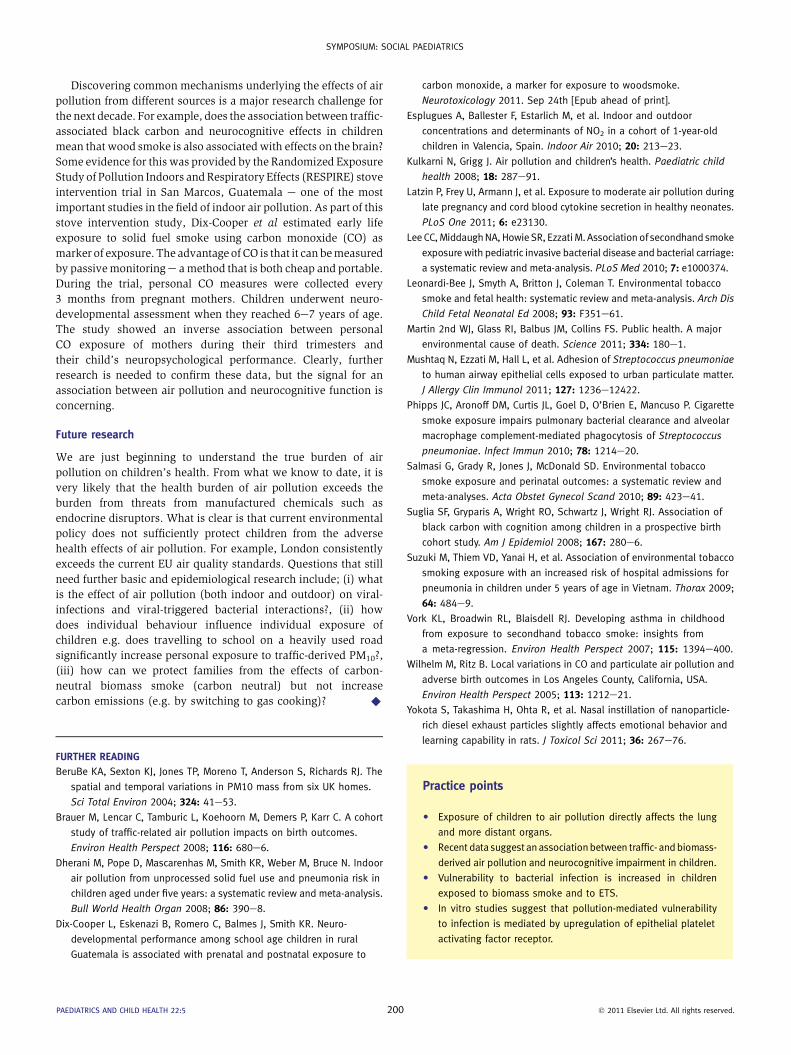
Figure 1 Pneumococci adhering to a monolayer of alveolar epithelial cells
imaged by scanning electron microscopy. Bacteria are bead-like
structures. Adherence is mediated by epithelial platelet activating factor
receptor interacting with ligands in the bacterial cell wall.
SYMPOSIUM: SOCIAL PAEDIATRICS
The effect of maternal ETS exposure on perinatal outcomes is less
obvious. In a recent systematic review and meta-analysis,
Salmasi et al identified publications covering 48,439 ETS-
exposed women and 90,918 unexposed women and found that
ETS-exposed infants weigh less, with a trend towards increased
low-birth weight. Using a similar approach, Leonardi-Bee et al
reported that exposure of non-smoking pregnant women to ETS
reduces mean birth weight by at least 33 g, and increases the risk
of birth weight below 2500 g by 22%. Since both ETS and traffic-
derived emissions have components in common, such as
carbonaceous PM, these data also provide indirect support for an
association between traffic-derived PM and birth weight (dis-
cussed above).
Another important area on the global scale is the interaction
between ETS and vulnerability to infection. In a recent meta-
analysis Lee et al assessed the association between ETS and
invasive bacterial disease in children. They found a consistent
association between invasive meningococcal and Hib disease
with the adjusted odds ratio (OR) for meningococcal disease of
1.2 (1.5e2.6). For invasive pneumococcal disease the OR was
positive, but not significant. An explanation for this non signifi-
cant finding is that pneumococcal pneumonia, although the
major cause of bacterial pneumonia in children is frequently
associated with negative blood cultures. The strongest evidence
that ETS is a major vulnerability factor for pneumococcal pneu-
monia was provided by a study from Vietnam. Suzuki et al
assessed hospital admissions for pneumonia among children
aged less than 5 years in the previous 12 months in a population-
based cross-sectional survey that included all residents of 33 in
a central area of Vietnam. Exposure to ETS was associated with
hospital admissions for pneumonia (OR 1.55, 95% CI, 1.25
e1.92). This OR may seem relatively low, but since the preva-
lence of ETS in Vietnam was 70%, it was estimated that 28% of
childhood pneumonia in this community is attributable to ETS
with 44,000 excess hospital admissions in young children per
year. Biological plausibility for this association was provided by
Phipps et al who exposed mice to cigarette smoke for 5 weeks
then instilled S. pneumoniae into the airway. Smoke-exposed
mice had increased lung bacterial load at both 24 and 48 h
after infection, and more clinical illness. Even more important on
the global scale, is the association between exposure to biomass
and coal smoke (e.g. wood, coal) and infection. Dherani et al in
a meta-analysis and systematic review found an overall pooled
OR of 1.78 (95% CI, 1.45e2.18) for exposure of children to solid
fuel smoke and risk of pneumonia in young children. It is now
widely accepted by policy makers that reduction of household
indoor air pollution from solid fuels would represent a major
contribution to the prevention deaths in young children living in
low-income countries. Indeed, these data have contributed to the
realization than indoor air pollution is a major environmental
cause of death for both women and young children. In response
to this, the United Nations Foundation launched the Global
Alliance for Clean Cookstoves e which aims for 100 million
homes to adopt clean stoves by 2020. In 2011, Hillary Clinton
made this initiative a major part of her Global Partnerships
Initiative.
Since both ETS and indoor solid fuel pollution are associated
with pneumonia in young childrene could traffic-derived PM also
increase vulnerability to infection? Bacterial pneumonia is
PAEDIATRICS AND CHILD HEALTH 22:5 199
relatively uncommon in high-income countries as are, fortunately,
deaths. Since it is difficult to perform adequately powered epide-
miological studies into air pollution and infection in high-income
countries, studies suggesting biological plausibility become more
important. For example, my group recently developed a model for
the effect of PM on the adherence of pneumococci to lower airway
epithelial cells (Figure 1). Adherence of bacteria to airway lining
cells is a prerequisite step for establishing invasive disease, and
environmental factors that upregulate adhesion are putative
vulnerability factors for bacterial pneumonia. We found that both
PM10 from a UK city (where most pollution is from traffic), and
from Accra (a city with a mix of traffic-derived and solid fuel
PM10), up-regulated pneumococcal adhesion to lower airway
epithelial cells in vitro. Furthermore,we found that themechanism
for both fossil-fuel PM and mixed source PM was the same, i.e.
upregulation of the ligand for pneumococcal adhesion on the
surface of epithelial cells e the platelet activating factor receptor
(PAFR). PAFR, by chance, happens to express proteins that
interact with proteins in the pneumococcal cell wall. Pneumococci
therefore adhere to this receptore and are thenmoved into the cell
as the receptor is internalized. In vitro studies comparing the
effects of ETS, biomass PM and traffic-derived PM may therefore
help to clarify whether there are commonmechanisms underlying
the association between air pollution and bacterial infection. From
our data, we hypothesize that children exposed to high levels of air
pollution (biomass, fossil-fuel and ETS) constitutively express
increased levels of PAFR in their lower airway epithelial cells. By
linking in vitro observations to valid markers of vulnerability
in vivo (such as PAFR expression) it may be possible to generate
sufficient data for policy makers to act on the presumption that
traffic-derived PM increases pneumonia vulnerability without
waiting for expensive and difficult-to-perform epidemiological
studies.
� 2011 Elsevier Ltd. All rights reserved.
Practice points
C Exposure of children to air pollution directly affects the lung
and more distant organs.
C Recent data suggest an associationbetween traffic- andbiomass-
derived air pollution and neurocognitive impairment in children.
C Vulnerability to bacterial infection is increased in children
exposed to biomass smoke and to ETS.
C In vitro studies suggest that pollution-mediated vulnerability
to infection is mediated by upregulation of epithelial platelet
activating factor receptor.
SYMPOSIUM: SOCIAL PAEDIATRICS
Discovering common mechanisms underlying the effects of air
pollution from different sources is a major research challenge for
the next decade. For example, does the association between traffic-
associated black carbon and neurocognitive effects in children
mean that wood smoke is also associatedwith effects on the brain?
Some evidence for this was provided by the Randomized Exposure
Study of Pollution Indoors andRespiratory Effects (RESPIRE) stove
intervention trial in San Marcos, Guatemala e one of the most
important studies in the field of indoor air pollution. As part of this
stove intervention study, Dix-Cooper et al estimated early life
exposure to solid fuel smoke using carbon monoxide (CO) as
marker of exposure. The advantage of CO is that it can bemeasured
by passivemonitoringe amethod that is both cheap and portable.
During the trial, personal CO measures were collected every
3 months from pregnant mothers. Children underwent neuro-
developmental assessment when they reached 6e7 years of age.
The study showed an inverse association between personal
CO exposure of mothers during their third trimesters and
their child’s neuropsychological performance. Clearly, further
research is needed to confirm these data, but the signal for an
association between air pollution and neurocognitive function is
concerning.
Future research
We are just beginning to understand the true burden of air
pollution on children’s health. From what we know to date, it is
very likely that the health burden of air pollution exceeds the
burden from threats from manufactured chemicals such as
endocrine disruptors. What is clear is that current environmental
policy does not sufficiently protect children from the adverse
health effects of air pollution. For example, London consistently
exceeds the current EU air quality standards. Questions that still
need further basic and epidemiological research include; (i) what
is the effect of air pollution (both indoor and outdoor) on viral-
infections and viral-triggered bacterial interactions?, (ii) how
does individual behaviour influence individual exposure of
children e.g. does travelling to school on a heavily used road
significantly increase personal exposure to traffic-derived PM10?,
(iii) how can we protect families from the effects of carbon-
neutral biomass smoke (carbon neutral) but not increase
carbon emissions (e.g. by switching to gas cooking)? A
FURTHER READING
BeruBe KA, Sexton KJ, Jones TP, Moreno T, Anderson S, Richards RJ. The
spatial and temporal variations in PM10 mass from six UK homes.
Sci Total Environ 2004; 324: 41e53.
Brauer M, Lencar C, Tamburic L, Koehoorn M, Demers P, Karr C. A cohort
study of traffic-related air pollution impacts on birth outcomes.
Environ Health Perspect 2008; 116: 680e6.
Dherani M, Pope D, Mascarenhas M, Smith KR, Weber M, Bruce N. Indoor
air pollution from unprocessed solid fuel use and pneumonia risk in
children aged under five years: a systematic review and meta-analysis.
Bull World Health Organ 2008; 86: 390e8.
Dix-Cooper L, Eskenazi B, Romero C, Balmes J, Smith KR. Neuro-
developmental performance among school age children in rural
Guatemala is associated with prenatal and postnatal exposure to
PAEDIATRICS AND CHILD HEALTH 22:5 200
carbon monoxide, a marker for exposure to woodsmoke.
Neurotoxicology 2011. Sep 24th [Epub ahead of print].
Esplugues A, Ballester F, Estarlich M, et al. Indoor and outdoor
concentrations and determinants of NO2 in a cohort of 1-year-old
children in Valencia, Spain. Indoor Air 2010; 20: 213e23.
Kulkarni N, Grigg J. Air pollution and children’s health. Paediatric child
health 2008; 18: 287e91.
Latzin P, Frey U, Armann J, et al. Exposure to moderate air pollution during
late pregnancy and cord blood cytokine secretion in healthy neonates.
PLoS One 2011; 6: e23130.
Lee CC,MiddaughNA, Howie SR, EzzatiM. Association of secondhand smoke
exposure with pediatric invasive bacterial disease and bacterial carriage:
a systematic review and meta-analysis. PLoS Med 2010; 7: e1000374.
Leonardi-Bee J, Smyth A, Britton J, Coleman T. Environmental tobacco
smoke and fetal health: systematic review and meta-analysis. Arch Dis
Child Fetal Neonatal Ed 2008; 93: F351e61.
Martin 2nd WJ, Glass RI, Balbus JM, Collins FS. Public health. A major
environmental cause of death. Science 2011; 334: 180e1.
Mushtaq N, Ezzati M, Hall L, et al. Adhesion of Streptococcus pneumoniae
to human airway epithelial cells exposed to urban particulate matter.
J Allergy Clin Immunol 2011; 127: 1236e12422.
Phipps JC, Aronoff DM, Curtis JL, Goel D, O’Brien E, Mancuso P. Cigarette
smoke exposure impairs pulmonary bacterial clearance and alveolar
macrophage complement-mediated phagocytosis of Streptococcus
pneumoniae. Infect Immun 2010; 78: 1214e20.
Salmasi G, Grady R, Jones J, McDonald SD. Environmental tobacco
smoke exposure and perinatal outcomes: a systematic review and
meta-analyses. Acta Obstet Gynecol Scand 2010; 89: 423e41.
Suglia SF, Gryparis A, Wright RO, Schwartz J, Wright RJ. Association of
black carbon with cognition among children in a prospective birth
cohort study. Am J Epidemiol 2008; 167: 280e6.
Suzuki M, Thiem VD, Yanai H, et al. Association of environmental tobacco
smoking exposure with an increased risk of hospital admissions for
pneumonia in children under 5 years of age in Vietnam. Thorax 2009;
64: 484e9.
Vork KL, Broadwin RL, Blaisdell RJ. Developing asthma in childhood
from exposure to secondhand tobacco smoke: insights from
a meta-regression. Environ Health Perspect 2007; 115: 1394e400.
Wilhelm M, Ritz B. Local variations in CO and particulate air pollution and
adverse birth outcomes in Los Angeles County, California, USA.
Environ Health Perspect 2005; 113: 1212e21.
Yokota S, Takashima H, Ohta R, et al. Nasal instillation of nanoparticle-
rich diesel exhaust particles slightly affects emotional behavior and
learning capability in rats. J Toxicol Sci 2011; 36: 267e76.
� 2011 Elsevier Ltd. All rights reserved.





























