Embed Size (px)
Citation preview
The Growing Crisis in Attracting andKeeping Direct Support Workers and HomeProviders, and What We Can Do About it.
Bob James, Executive Director, Community Developmental Services/Region VIII
If you speak with anyone who is involved in the developmental disabilities ser-vice system you will soon be talking about the shortage of people to do the work.This is true whether you’re speaking with a family needing services, a legislatorfunding them, the director of the agency providing them, or the direct supportprofessional (DSP) working overtime to deliverthem. Turnover has reached 50%; vacancies are at anall-time high, and new hires are often rushed intoservice with insufficient training. And it is projectedto get steadily worse over the coming decades.
It is a national crisis. A recent report by the U.S.Department of Health and Human Services statesthat “Between 2003 and 2020, H.H.S.anticipates thatthe number of DSP’s needed to provide for thegrowth of long term support services for individualswith ID/DD (Intellectual Disabilities/DevelopmentalDisabilities) will increase by…37%. This increase willbe largely due to population increases, increases in lifeexpectancy among persons with ID/DD, aging of fam-ily caregivers, and expansion of home and community-based services. This increasein demand will be occurring at a time when the labor supply of adults age 18-39years, who traditionally have filled these jobs is expected to increase only by 7%.”If we look at women age 22-44, a more accurate reflection of our workforce, the fig-ures are even worse. And after 2020 the gap increases at an even faster rate.
A COLLABORATIVE EFFORT BY THE
DISABILITIES RIGHTS CENTER, INSTITUTE ON DISABILITY, AND NH COUNCIL ON DEVELOPMENTAL DISABILITIES
SUSAN COVERT, EDITOR
W e l c o m e
to the Fall Issue of the
Rap Sheet. Direct support
professionals are the glue
that holds our social
service system together.
These are the workers who
support people with
disabilities to live at home
and to be active
community members. With
increasing demands for
direct supports and a
diminishing workforce,
New Hampshire’s
community-based system
is facing a crisis. In this
issue we look at what
we can do to turn
things around.
D I R E C T C A R E I N T H E G R A N I T E S T A T E
The Latest in Disability Research, Advocacy, Policy, and Practice Fall Issue 2007
N e w H a m p s h i r e
RAP Sheet
( C o n t i n u e d o n n e x t p a g e )
Sa
ra L
eav
itt
Bob James, Executive Director forCommunity Developmental Services

2
( C o v e r s t o r y c o n t i n u e d )
Clearly, we have a problem on our hands that willrequire a comprehensive, long-range solution, similarto the successful drive to end the wait list for develop-mental services. The viability of our service system andthe dream of community inclusion for all are at risk ifwe fail to rise to the challenge. Without a substantialinvestment of resources there simply will be too fewpeople to operate the system.
Fortunately, we know what is needed. Here are fivestrategies that address the needs of both direct supportprofessionals who hold staff positions and home pro-viders who provide residential care for someone livingin their home:
1. Establish a minimum livable wage and benefitpackage. We must make wages competitive withbusiness and industry (since we are competing withthem for workers) and figure out how to offer ben-efits, especially health coverage, to our workforce– including our home providers. The legislatureshould establish a reasonable package and fund it.
2. Invest seriously in training. It is important that newstaff and home providers receive a full training andorientation before starting on the job, and supportonce they are in it. There are some very successfultraining practices that we can learn from. I know ofone agency that requires applicants to successfullycomplete 24 hours of training before being selectedas a home provider. This has resulted in high qual-ity, long lasting placements. Another provides aclinical consultant to help work through problemsituations. It is equally important that staff be givenopportunities for professional growth and advance-ment. On-line initiatives like the College of DirectSupport provide new avenues for training DSP’s andhome providers – while giving them a means of ad-vancement. (In addition to training opportunities,the Internet has the potential to open new lines ofcommunication and reduce the isolation felt bysome staff and home providers.) The National Alli-ance for Direct Support Professionals has developeda national credentialing program for DSP’s. Utiliz-
ing these (or other) exemplary training practices ona statewide basis would improve the quality of serviceswhile attracting and keeping our more motivatedworkers. A review of the training provided through-out the state would be a first step in making system-wide improvements. Substantially increased fundingfor training – and for the staff time to participate –would be a sound investment.
3. Greatly expand the practice of involving DSP’s andhome providers in decision making. Often over-shadowed by the focus on wages and benefits, thisis a “best practice” that lies at the heart of job sat-isfaction and has the potential to significantly re-duce staff turnover. Our most successful examples oflongevity occur in situations where the DSP’s orhome provider’s judgment is trusted and relied upon,where relationships are characterized by respect,and the worker has a personal connection with theindividual served. This is often the case with con-sumer-directed services, an innovation that is rapidlygaining in popularity in New Hampshire. Here isone solution that requires little or no additionalfunding – just a vigorous championing of best prac-tices that are currently happening. For example, oneresidential agency includes a home provider on ev-ery hiring committee – including those for seniormanagers.
4. Sponsor a statewide recruitment campaign. Astrong public relations campaign would do twothings: it would advance the cause of inclusion whilecreating a positive image for the work we do. If weactually implement the recommendations above, wecan truly say “Work to change your community one personat a time. Inclusion for all. It’s a career – not just a job.” Aconsulting firm could develop a PR campaign for areasonable one-time cost; getting the message outby maximizing use of the web, public service an-nouncements, and donated air time could signifi-cantly improve staff recruitment. Area Agencies canexpand the use of scholarships for graduating highschool students choosing a career in human services.

3
5. Coordinate state policy making. In the 1980’sand 1990’s, New Hampshire was steadily march-ing toward full community inclusion for peoplewith disabilities, and the state’s policies un-equivocally supported that direction. Idealisticpeople were drawn to join in the cause, andmany saw it as the new civil rights movement.“The dignity of risk” was considered a right fordisabled and non-disabled alike. This haschanged. The movement to make the everydaylives of people with disabilities more like thelives of everyone else has slowed significantly.Accountability and reporting, one-size-fits-allrules, and paperwork have increased. Jobs – directcare and otherwise – have become more bureau-cratic and less creative – and less attractive.Home providers are subject to increasingly in-trusive inspections and required home modifica-tions that don’t make sense to them. For in-stance, under newly proposed window sizeregulations, most of the existing homes in my re-gion fail, which means providers must agree tohave their windows enlarged or have the indi-vidual with disabilities removed from theirhome. On the one hand, New Hampshire iscommitted to a community-based system forelders and people with disabilities; yet on theother, it is developing regulations that seriouslyhamper that. This is because the state depart-ments and local officials who have a say in thesematters have differing views and have not beenable to agree on one consistent policy. Until thisis resolved, it will remain a significant obstacleto solving the workforce issues discussed here.
The growing crisis in finding and keeping qualifiedDSP’s and home providers can be solved. It will re-quire strong statewide leadership, a new compre-hensive strategy, and dedicated funding from thelegislature. To view these strategies as “nice, butbeyond our means” will result in the eventual break-down of services to our most vulnerable citizens.We really have no choice. In this case, the rightthing to do is also the only smart thing to do.
SB 138 Workforce Development Committee
Most people are aware that in the last legislative sessionNew Hampshire lawmakers passed Senate Bill 138 toaddress the wait list for developmental services. In additionto providing funding to reduce the wait list, SB138 alsoestablished a committee to develop a plan to address long-term workforce and related human resource issues. Thatcommittee held its first meeting on August 21, and itsrecommendations are due to the legislature by December 1,2007. The membership of the group was stipulated in thebill and is broadly representative. It consists of:
Matthew Ertas, Department of Health and Human Services(serving as chairperson)
Nancy Rollins, Department of Health and Human ServicesDiane Carignan, People First of New HampshireBeth Dixon, Kirsten Murphy, and Cathy Spinney of Area
Agency Board of DirectorsSusan Gunther, Bobbi Gross, and Michael Umali from
Family Support CouncilsEllen Edgerly, New Hampshire Brain Injury AssociationGordon Allen, New Hampshire Council on Developmental
DisabilitiesMike Skibbie, Disabilities Rights CenterDavid Hagner, Institute on Disability – University of New
HampshireDennis Powers, Community Support NetworkDeborah Hopkins, Private Provider Network
The plan must:
1. Provide for annual or periodic salary increases for allArea Agency and provider agency staff, in addition todirect support staff increases mandated elsewhere in thebill. In addition, direct support wages must be brought atleast to parity with Mental Health Worker I positions atNew Hampshire Hospital by July 1, 2011.
2. Provide for increased enhanced family care [homeprovider] rates and rate structure, in addition to thosemandated elsewhere in the bill.
3. Address whether and how free college tuitionprograms could be accessed.
4. Address whether and how affordable health insurancecould be offered to Area Agency and provider staff, andenhanced family care providers.
It will be up to the legislature to act on the recommen-dations in the plan.

4
Loving my work as a Direct Support ProfessionalRobin Carlson
I have truly found my purpose in life – for more than 22 yearsI have been a direct support professional. I began working inthe human services field just as Laconia State School was clos-ing and New Hampshire was beginning to build a communitysupports system. I felt I was part of a civil rights movement thatwas liberating citizens who for decades had been cast away. Asa new worker in New Hampshire’s developmental service sys-tem, I received training from national leaders in the disabilityfield. I learned about the systematic devaluation of people withdisabilities from Dr. Wolfensburger. John and Connie LyleO’Brien taught me about the importance of focusing on people’stalents rather than their deficits. I learned about positive behav-ioral supports from Herb Lovett and community capacity build-ing from John McKnight. From all these teachers I came tounderstand that people with disabilities are my equals and ifour society is to be whole, we need their contributions.
In 1989, while working for an area agency, I met Frank Caswell.As a young boy, Frank spent three and half years at LaconiaState School until his grandmother, appalled by the deplorableconditions, took him out the institution. Life for Frank contin-ued to be difficult. When I first met Frank he had returned tohis hometown after 17 years of wandering across the countryand living on the streets. He was an extremely isolated manwho allowed no one in his life except his sister, Patricia. As hissupport worker, it took me a solid year to gain his trust anddevelop a relationship. We got to know each other better asneighbors living in separate apartments in a big house. Whenmy husband and I bought our first home and got ready to move,Frank decided he would like to live with us. Seventeen yearslater we are still together.
I believe our success is rooted in the value-based trainings Ireceived early in my career. This training inspired me to alignmyself with people who needed a strong voice for justice. I alsowas immersed in a person-centered culture working with otherswho held the same vision of building an inclusive community.In helping people with disabilities achieve their personal goalsand creating accepting communities, the role of the direct supportprofessional is pivotal. While my work has been personally reward-ing, the pay has never been adequate. I have seen many dedicateddirect support professionals leave the field because they couldnot earn a living wage. While moving into management positionsoffers better pay, this is something that not all direct supportprofessionals have the ability or even the desire to do.
In order to ensure quality community supportsto people with disabilities, New Hampshireneeds an effective direct support professionalworkforce. To accomplish this, workers musthave access to value-based training, connec-tions to local and national associations thatpromote professionalism and respect for directsupport, opportunities for career develop-ment, and the ability to earn a living wage.When New Hampshire truly invests in directsupport professionals, the outcome will be thecreation of a vibrant and tolerant culturewhere communities value and actively seekeveryone’s contributions. The sky is the limit.
As Frank’s support person, I measure successby the people Frank has allowed into his lifeand with whom he has mutual, respectful, andcaring relationships. When Frank had hisbirthday in July, thirteen people came to-gether to help him celebrate! Friends, family,and community are what make life worthwhilefor Frank and for me.
Robin Carlson is chairperson for the Planning Commit-tee for the 2007 Direct Support Professional Conference,an Institute on Disability Leadership Graduate, Work-shop Presenter, and state contact person for the NationalAlliance for Direct Support Professionals (NADSP).
Frank Caswell and his support person, Robin Carlson
5
New State Law provides for Medicaid Coverage ofDisposable Incontinence Supplies and an
Independent Review Process for All Items and ServicesCarol Stamatakis, Esq., New Hampshire Council on Developmental Disabilities
On July 3, 2007, Governor Lynch signed into lawHouse Bill 826, relative to coverage of services anditems under the Medicaid program. Effective Septem-ber 1, 2007, New Hampshire’s Medicaid program willcover incontinence supplies for adults, and new stan-dards will govern access to a wide array of medicalservices and items, including durable medical equipment.As stated in the bill, “It is the intent of the generalcourt to support persons with special health care needsand disabilities with coverage of medically necessaryservices and items under the medical assistance programso that they may live in their homes and communitiesas independently as possible and with the maximumability to be mobile and exercise self care.”
Rep. Tom Donovan of Claremont, prime sponsor ofHB 826, has worked for many years in human services.He has seen first hand how the lack of coverage formedically necessary items impacts the lives of those whoare unable to afford them. Motivated by the stories heheard from families, as well as the experiences of hisolder clients, Rep. Donovan introduced a bill to requireMedicaid coverage of disposable incontinence supplies.When he learned that the Department of Health andHuman Services (DHHS) was considering administra-tive rules that would make it more difficult for adultswith disabilities and elders to access some durablemedical equipment, Rep. Donovan expanded the scopeof his bill to include these items.
In the absence of explicit state laws, the DHHS hasused administrative rules to determine the extent ofMedicaid coverage for durable medical equipment andother services. At times this has resulted in denials ofitems and services that families and health care pro-viders believed were medically necessary. New rulesbeing proposed by DHHS raised concerns that therewould be increased denials for medically necessaryservices and items that could jeopardize the ability ofsome New Hampshire citizens to remain in their
homes. HB 826 provided an opportunity for the leg-islature to take a comprehensive look at how
coverage of medical equipment, supplies, and servicescould be a cost-effective alternative to institutional-ization and other expensive services. Passage of HB 826also underlined the State’s commitment to home andcommunity-based care. In addition to Rep. Donovan,co-sponsors of the bill included Rep. Daniel Eaton,(Cheshire 2); Rep. Frank Tupper, (Merrimack 6); Rep.Susan Emerson, (Cheshire 7); Sen. John Gallus, (Dis-trict 1); Sen. Martha Fuller Clark, (District 24); andSen. Iris Estabrook (District 21).
The legislation establishes an independent reviewprocess to allow access to those items or services nototherwise covered that are permitted under the federalMedicaid program and that meet certain objective cri-teria. While coverage of durable medical equipment isthe main focus of the legislation, it also includes anyitem or service that could be covered by Medicaidunder federal law. For example, an item not otherwisecovered would be allowed if a denial for coverage isclinically contraindicated; if it would prevent the needfor a more costly covered service or item, includingprevention of hospitalization or institutionalization; orif new scientific evidence supports the medical appro-priateness of the requested service or item.
The many telephone calls to legislators and the testi-mony of people with disabilities and families at thelegislative hearings were particularly compelling andconvinced policymakers of the critical need for thislegislation. Rep. Donovan commented, “I would havedone something on my own, but to have so manyadvocates and families behind me to help was bothhumbling and empowering.”
DHHS is working to develop rules and procedures toimplement the new law. Interim rules are expected tobe in place by the end of September. The developmentof final rules will include a process for prior authori-zation for incontinence supplies based on documenta-tion of medical need, applicable service limits, and aprocess to request an independent coverage review forother services and items.
6
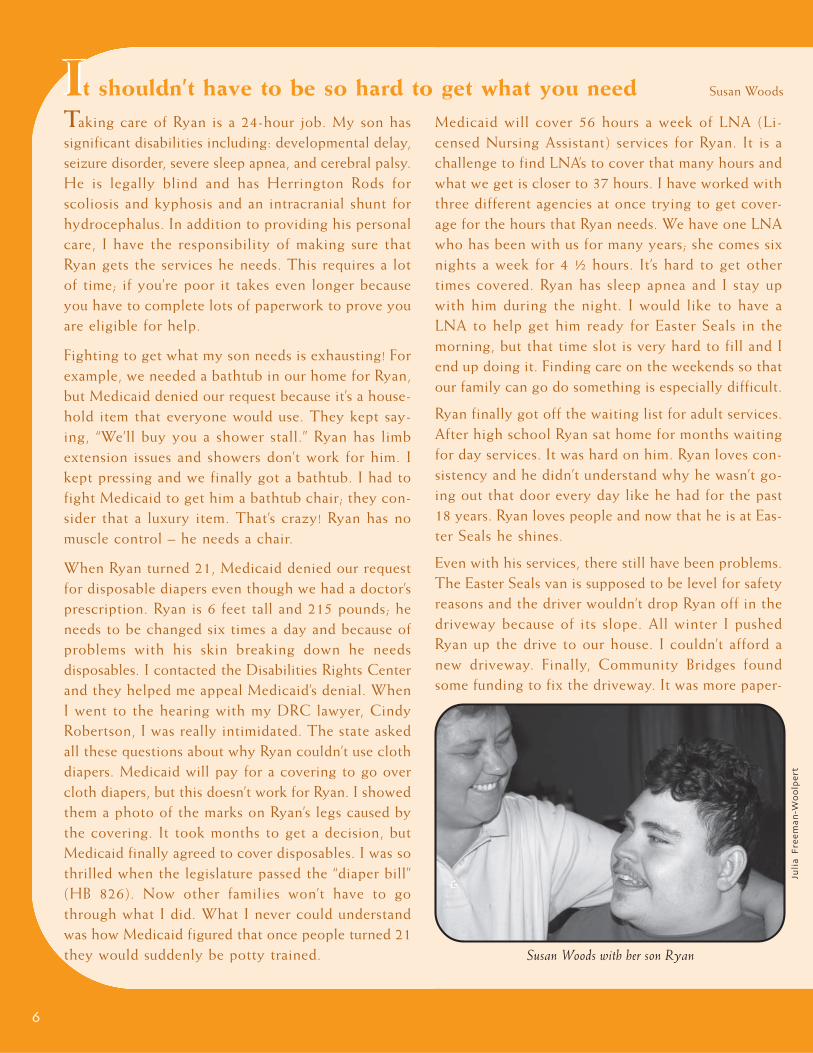
Taking care of Ryan is a 24-hour job. My son hassignificant disabilities including: developmental delay,seizure disorder, severe sleep apnea, and cerebral palsy.He is legally blind and has Herrington Rods forscoliosis and kyphosis and an intracranial shunt forhydrocephalus. In addition to providing his personalcare, I have the responsibility of making sure thatRyan gets the services he needs. This requires a lotof time; if you’re poor it takes even longer becauseyou have to complete lots of paperwork to prove youare eligible for help.
Fighting to get what my son needs is exhausting! Forexample, we needed a bathtub in our home for Ryan,but Medicaid denied our request because it’s a house-hold item that everyone would use. They kept say-ing, “We’ll buy you a shower stall.” Ryan has limbextension issues and showers don’t work for him. Ikept pressing and we finally got a bathtub. I had tofight Medicaid to get him a bathtub chair; they con-sider that a luxury item. That’s crazy! Ryan has nomuscle control – he needs a chair.
When Ryan turned 21, Medicaid denied our requestfor disposable diapers even though we had a doctor’sprescription. Ryan is 6 feet tall and 215 pounds; heneeds to be changed six times a day and because ofproblems with his skin breaking down he needsdisposables. I contacted the Disabilities Rights Centerand they helped me appeal Medicaid’s denial. WhenI went to the hearing with my DRC lawyer, CindyRobertson, I was really intimidated. The state askedall these questions about why Ryan couldn’t use clothdiapers. Medicaid will pay for a covering to go overcloth diapers, but this doesn’t work for Ryan. I showedthem a photo of the marks on Ryan’s legs caused bythe covering. It took months to get a decision, butMedicaid finally agreed to cover disposables. I was sothrilled when the legislature passed the “diaper bill”(HB 826). Now other families won’t have to gothrough what I did. What I never could understandwas how Medicaid figured that once people turned 21they would suddenly be potty trained.
Medicaid will cover 56 hours a week of LNA (Li-censed Nursing Assistant) services for Ryan. It is achallenge to find LNA’s to cover that many hours andwhat we get is closer to 37 hours. I have worked withthree different agencies at once trying to get cover-age for the hours that Ryan needs. We have one LNAwho has been with us for many years; she comes sixnights a week for 4 ½ hours. It’s hard to get othertimes covered. Ryan has sleep apnea and I stay upwith him during the night. I would like to have aLNA to help get him ready for Easter Seals in themorning, but that time slot is very hard to fill and Iend up doing it. Finding care on the weekends so thatour family can go do something is especially difficult.
Ryan finally got off the waiting list for adult services.After high school Ryan sat home for months waitingfor day services. It was hard on him. Ryan loves con-sistency and he didn’t understand why he wasn’t go-ing out that door every day like he had for the past18 years. Ryan loves people and now that he is at Eas-ter Seals he shines.
Even with his services, there still have been problems.The Easter Seals van is supposed to be level for safetyreasons and the driver wouldn’t drop Ryan off in thedriveway because of its slope. All winter I pushedRyan up the drive to our house. I couldn’t afford anew driveway. Finally, Community Bridges foundsome funding to fix the driveway. It was more paper-
IIt shouldn’t have to be so hard to get what you need Susan Woods
Juli
a F
ree
ma
n-W
oo
lpe
rt
Susan Woods with her son Ryan

7
work and I needed to find a contractor who would do arush job or the money would go away. Luckily, we did getit done.
Ryan is not on the waiting list for residential services.Community Bridges told me that Ryan has to stay in ourhome unless I can prove I can’t take care of him. I resentthat – I’ve been caring for Ryan for 23 years. While I don’twant Ryan to live anywhere else right now, there maycome a time when I physically just can’t do it anymore.I also would like to have somewhat of a life someday.
There is no out of home respite for someone like Ryan.He used to go to Crotched Mountain, but the statechanged their rules and made it so difficult that they nolonger do respite care. The last time I had a weekendaway was when Ryan was in the hospital. I needed thatbreak and needed time to do things with the rest of thefamily. I knew Ryan would be cared for, but I still wor-ried about him the whole time I was gone.
During the last several years, Ryan has had four or fivecase managers. They keep leaving. It’s very frustrating;as soon as I’d explain something to one case manager, Ihave to explain it all over again to a new person. It wearsyou down. We had one case manager who stayed for awhile, but wasn’t able to rearrange her hours so she couldfinish her degree. She recently left, the person whoreplaced her didn’t even stay two weeks and now wehave yet another case manager.
Fortunately, I’m really good at advocating for Ryan. Iknow what I want and I’m persistent. I feel badly for thepeople who don’t know what to do and just accept thatthis is the way it has to be. My advice is to talk withwhoever you need to talk to. If you need to bypass yourarea agency and go to the state, then go to the state.Don’t be afraid to go to your legislators or to the Gov-ernor. If you have a problem, write them and call them.If they don’t hear from families and individuals then theyhave no idea how difficult our lives can be.
I don’t understand why the state makes it so hard. Itshouldn’t have to be so hard to get what you need. Youshouldn’t have to always fight for it. It’s not like this isa joyride for us.
NH’s Direct SupportProfessional Conference:Past and PresentDavid Ouellette, New Hampshire Council onDevelopmental Disabilities
Thirteen years ago the New Hampshire Devel-opmental Disabilities Council, under the direc-tion of Al Robichaud, organized the state’s firstDirect Support Professional (DSP) conference.The intent of the conference was to recognizethe contribution of DSPs and offer training rel-evant to their work. The conference provideda forum where DSPs could share their ideas,concerns, and dreams. Participants also had theopportunity to make connections, relax, andre-charge their batteries! After all direct sup-port can be challenging, hard work.
DSPs have served on the conference planningcommittee from the begin-ning helping to ensurethat the conferencefulfills its mission toeducate, value andrespect the DSP inorder to change theworld to include allpeople. Barbara Wil-son, planning commit-tee member and DSP,created the conferencelogo – a tree with the words compassion, wisdom,and honor embedded in its leaves.
Over the years the DSP conference has beenfortunate to have great keynote speakers in-cluding: Don Shumway, Greg Galluzzo, FrancisKee Brunside, Rachel Simon, and Peter Leidy.Conference workshops have covered a widerange of topics including the history of LaconiaState School, sexuality, system change throughadvocacy, and building community. In responseto requests from conference attendees the con-ference now includes more DSP presenters who
( C o n t i n u e d o n p a g e 9 )
8
We cannot hold a torch to light another’s pathwithout brightening our own.
~ Ben Sweetland
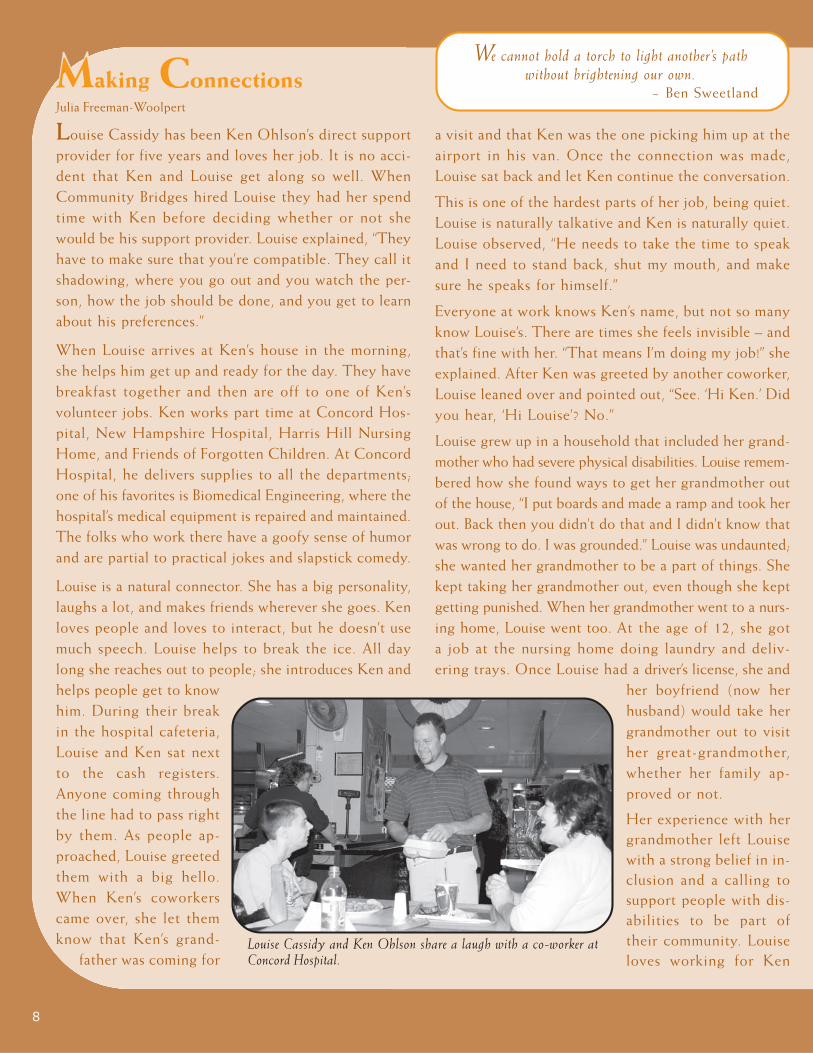
Louise Cassidy has been Ken Ohlson’s direct supportprovider for five years and loves her job. It is no acci-dent that Ken and Louise get along so well. WhenCommunity Bridges hired Louise they had her spendtime with Ken before deciding whether or not shewould be his support provider. Louise explained, “Theyhave to make sure that you’re compatible. They call itshadowing, where you go out and you watch the per-son, how the job should be done, and you get to learnabout his preferences.”
When Louise arrives at Ken’s house in the morning,she helps him get up and ready for the day. They havebreakfast together and then are off to one of Ken’svolunteer jobs. Ken works part time at Concord Hos-pital, New Hampshire Hospital, Harris Hill NursingHome, and Friends of Forgotten Children. At ConcordHospital, he delivers supplies to all the departments;one of his favorites is Biomedical Engineering, where thehospital’s medical equipment is repaired and maintained.The folks who work there have a goofy sense of humorand are partial to practical jokes and slapstick comedy.
Louise is a natural connector. She has a big personality,laughs a lot, and makes friends wherever she goes. Kenloves people and loves to interact, but he doesn’t usemuch speech. Louise helps to break the ice. All daylong she reaches out to people; she introduces Ken andhelps people get to knowhim. During their breakin the hospital cafeteria,Louise and Ken sat nextto the cash registers.Anyone coming throughthe line had to pass rightby them. As people ap-proached, Louise greetedthem with a big hello.When Ken’s coworkerscame over, she let themknow that Ken’s grand-
father was coming for
a visit and that Ken was the one picking him up at theairport in his van. Once the connection was made,Louise sat back and let Ken continue the conversation.
This is one of the hardest parts of her job, being quiet.Louise is naturally talkative and Ken is naturally quiet.Louise observed, “He needs to take the time to speakand I need to stand back, shut my mouth, and makesure he speaks for himself.”
Everyone at work knows Ken’s name, but not so manyknow Louise’s. There are times she feels invisible – andthat’s fine with her. “That means I’m doing my job!” sheexplained. After Ken was greeted by another coworker,Louise leaned over and pointed out, “See. ‘Hi Ken.’ Didyou hear, ‘Hi Louise’? No.”
Louise grew up in a household that included her grand-mother who had severe physical disabilities. Louise remem-bered how she found ways to get her grandmother outof the house, “I put boards and made a ramp and took herout. Back then you didn’t do that and I didn’t know thatwas wrong to do. I was grounded.” Louise was undaunted;she wanted her grandmother to be a part of things. Shekept taking her grandmother out, even though she keptgetting punished. When her grandmother went to a nurs-ing home, Louise went too. At the age of 12, she gota job at the nursing home doing laundry and deliv-ering trays. Once Louise had a driver’s license, she and
her boyfriend (now herhusband) would take hergrandmother out to visither great-grandmother,whether her family ap-proved or not.
Her experience with hergrandmother left Louisewith a strong belief in in-clusion and a calling tosupport people with dis-abilities to be part oftheir community. Louiseloves working for Ken
MMaking ConnectionsJulia Freeman-Woolpert
Louise Cassidy and Ken Ohlson share a laugh with a co-worker atConcord Hospital.

9
conduct workshops on how to provide quality services. Atevery conference, DSPs have the opportunity to discuss theissues and challenges that affect their work. In their confer-ence evaluations participants consistently report that the DSPconference provided them with information and networkingopportunities that they would not otherwise have had.
While the DSP conference has gone through manytransformations, the outcomes have remained the same– education, networking, and renewal. The conferenceoffers an opportunity for DSP’s to improve themselves andgive the people they support a better quality of life. The2007 DSP Conference – Goals: Yours, Mine, and Ours – will beheld on October 26th and 27th at the Grand Summit Resortin Bartlett. Kathy Bates, Tracy Cintron, and Jim Piet will bethe keynote presenters. The conference registration fee is$50 and includes all workshops and meals. To reserve aroom call the Grand Summit Hotel directly at 1-888-554-1900; be sure to mention that you are attending the DSPConference. The deadline for hotel reservations is October5th and October 12th for conference registration. For moreinformation or to register contact David Ouellette at theNew Hampshire Council on Developmental Disabilities –271-3236 or by email at [email protected]
( C o n t i n u e d f r o m p a g e 7 )
This issue of the Rap Sheet is dedicated toLouise Cassidy and all those direct supportprofessionals whose care and dedicationmake such a positive difference in the livesof people with disabilities. On September15, 2007 Louise Cassidy was killed in acar accident. She was a loving wife,mother, grandmother, and caregiver. Shewill be greatly missed.
Support the Rap Sheet!
For the past three years, the Rap Sheet has provided an
in depth examination of issues affecting people with
disabilities and their families. The federal grant dollars
that have helped to finance the publication of the Rap
Sheet are drying up. We are asking for your support to
help ensure that we can continue to bring you the latest
in disability research, advocacy, policy, and practice.
To make an online donation, please go to: http://
www.drcnh.org/donate.htm, or send your check to the
Disabilities Rights Center, 18 Low Avenue, Concord,
NH 03301. Donations are tax deductible. Thank you!
and his family. She is proud to be part ofCommunity Bridges and feels their philosophyof providing support matches her own. Shealso noted, “Community Bridges has excellenttraining and it’s mandatory.” The agency’s train-ing covers a wide range of topics including:driver’s safety, CPR, and client rights.
Louise has considered leaving her job for onethat pays better, especially as she looks towardsretirement. She makes less than half of whatshe made when she worked at Blue Cross-BlueShield in customer service. “But,” she said, “Ihave a wonderful husband who is workingharder than he probably should so that I cancontinue doing this job. He says this is whatyou do; this is what makes you happy. Andwhen you’re happy, everyone’s happy.”
Asked if she would recommend direct supportas a profession, Louise answered, “You’d neverbe able to support yourself or a family on this,but yes, definitely! You get up in the morningand you are excited about going to work withthat person and what you can do that day tobe fun. You leave at the end of the day andyou know he’s had a good day and he’s happy.”
Louise looked over at Ken. “If you’re happy,I’m happy,” she said.

10
Special Needs Trusts (also called“Supplemental Needs Trusts”) are irre-vocable, discretionary trusts estab-lished by someone other than theperson who is the primary benefi-ciary of the trust. In most cases, aparent, other family member, or alegal guardian creates the trust for anindividual with a disability. The pri-mary purpose of the Special NeedsTrust is to enable the beneficiary toreceive or continue to receive Med-icaid and other benefits, while being
able to draw on the trust for items orservices that governmental benefitsdo not cover.
BACKGROUNDAlthough Special Needs or Supple-mental Trusts have been around fordecades, it was not until 1993 whenCongress recognized and affirmedtheir validity under the OmnibusBudget Reconciliation Act of 1993(OBRA ‘93) that they became widelypopular.
There are different types of SpecialNeeds Trusts. A “self-settled” trust isone where the source of the trust con-sists of funds (e.g. an inheritance, per-sonal injury settlement, retroactiveSocial Security Disability award) thatare owned or received by the indi-vidual with the disability who is to bethe trust’s primary beneficiary. Self-settled trusts contain a “pay-back”provision to reimburse the state forMedicaid advanced to the individualduring his or her lifetime. Pay-back
My Way Leslie Boggis, New Initiatives Manager, Area Agency of Greater Nashua, Inc.
Frank Sinatra claimed, “I did it my way!” Now manyindividuals and families in New Hampshire are singingthe same tune. They have requested the option to receiveservices their way, and the state of New Hampshire haslistened. More than eight years ago the Area Agency ofGreater Nashua, Inc., following the Medicaid guidelinesfor the state’s Division of Developmental Services, usedMedicaid funds to establish Consumer Directed Services(CDS) for individuals and families who want greatercontrol over how their services are delivered and a sayin how their support dollars are used.
CDS enables individuals and families to tailor supportsand services to meet their unique needs and interests.Our agency’s CDS program works hard to live up toits motto – Your Choice, Your Community, Your Home, YourWorker, Your Schedule!
A single mother in our region who was looking at ser-vices for her daughter after high school realized thatthe traditional 9:00-3:00 day program wasn’t going towork for her family or her daughter. She needed towork full time and her daughter requires 24-hour care.With support from CDS, this parent was able to designa program that includes essential personal care servicesfor her daughter, as well as, horseback riding, swim-ming, a variety of other community activities, and timeat home. She has recruited, trained, and continues to
manage the two employees who support her daughter.She sets the weekly schedule and, with the workers,plans activities that match her daughter’s needs andinterests. Working with the Area Agency, this mothersets the rates of pay for the workers and authorizesexpenditures from her daughter’s individual supportbudget. The Area Agency is the employer of record forher daughter’s workers and provides workman’s compen-sation insurance, benefits, liability coverage, payroll, andtax functions. Using the CDS option, this mother wasable to keep her job and had the opportunity to createan individualized program to meet her daughter’s needs.
Self-directed supports are a partnership between indi-viduals, families, and the Area Agency. The individualand family design services, oversee the supports, setschedules, and authorize payments. The Area Agencyprovides employer and payroll functions for anyworkers that are hired, offers education and supportto individuals and their families, and conducts over-sight required for regulatory compliance. Last but notleast, the Area Agency provides fiscal managementthrough monthly budget statements. Simply put, theindividual budget gives the individual and family a “fixedchecking account” to pay for services. The Area Agencywrites the checks that the individual and family autho-rize and keeps them informed about their ongoing
INTRODUCTION TO SPECIAL NEEDS TRUSTS

11
is required when the trust terminates;that is, when the beneficiary dies.
In the second type of trust, typicallycreated by a family member (a parentor grandparent), trust funds werenever owned or received by the ben-eficiary. This type, commonly calleda “third-party” trust does not requirea pay-back provision to the state.
The final type of trust, called a“pooled trust,” is managed by a not-for-profit corporation. These are
occasionally used by family memberswho do not want to serve as trustee,but more often these are establishedfor individuals who are 65 years ofage or older. In New Hampshire,Enhanced Life Options, a not-for-profit corporation located in Bed-ford, administers a pooled trust forpersons of all ages with disabilities.Pooled trusts are allowed to retain orwithhold a certain percentage (thisvaries from state to state) of theMedicaid pay-back; the retained funds
may be used to assist other benefi-ciaries in the pool whose needs aregreater than their individual trustresources.
HOW SPECIAL NEEDSTRUST WORKAlthough there are strict income andresource rules governing eligibilityfor SSI and Medicaid, a properlycrafted Special Needs Trust shouldallow an individual with a disability
( C o n t i n u e d o n p a g e 1 4 )
balance. This allows individuals and families to man-age the ebb and flow of life knowing they can’t over-draw their account.
At the Area Agency of Greater Nashua, Inc. over onehundred and fifty individuals with their families orallies have chosen to design and manage their ownsupports and services. Many individuals and their fami-lies opt to totally customize services, as did the motherin example above, while others use their budget topurchase services from traditional day or residentialprograms or arrange for a combination of traditionaland customized services. A former Laconia StateSchool resident who manages his own program had aworker with whom he was very close move out of thelocal area. While this worker was no longer availableto help with weekly grocery shopping and other sup-ports, the Area Agency recognized the importance ofhelping maintain this long-term friendship. A con-sumer directed option with individual budget controlwas used to support these friends spending time together;the individual’s independent living supports now arepurchased from a local vendor.
Parents with children under the age of twenty-one whohave chosen self-directed services have used funds forpersonal care and supports, behavioral consultations,
respite care, and home and vehicle modifications. Mostparents have used the self-directed service option tocustom tailor after school care to meet the needs andinterests of their child and to address the specificscheduling needs of their family. One mother designedan after school experience for her daughter that includedtherapeutic horseback riding, adaptive dance, and yoga.
The individual and family directed option goes beyondpaying for personal care or supporting participation incommunity activities. CDS has provided the opportu-nity for many individuals to pursue and maintain em-ployment that matches their talents and interests. Indi-viduals and families have used CDS to pay for workerswho consult with employers, provide supports on thejob, and assist in finding employment. A family whoused their personal network to secure employment fortheir daughter has a customized plan and individual bud-get that pays for a mentor who works with their daugh-ter on social skills, cooking, budgeting, and who alsoprovides consultation when needed to her employer.
Work, learning, personal care, recreation, and healthare all areas where individuals and families can customtailor supports and services to meet their unique needsand circumstances. With consumer directed services, in-dividuals and their families can say, “I did it my way!”
John MacIntosh, Esq. and Representative Ruth Bleyler
12
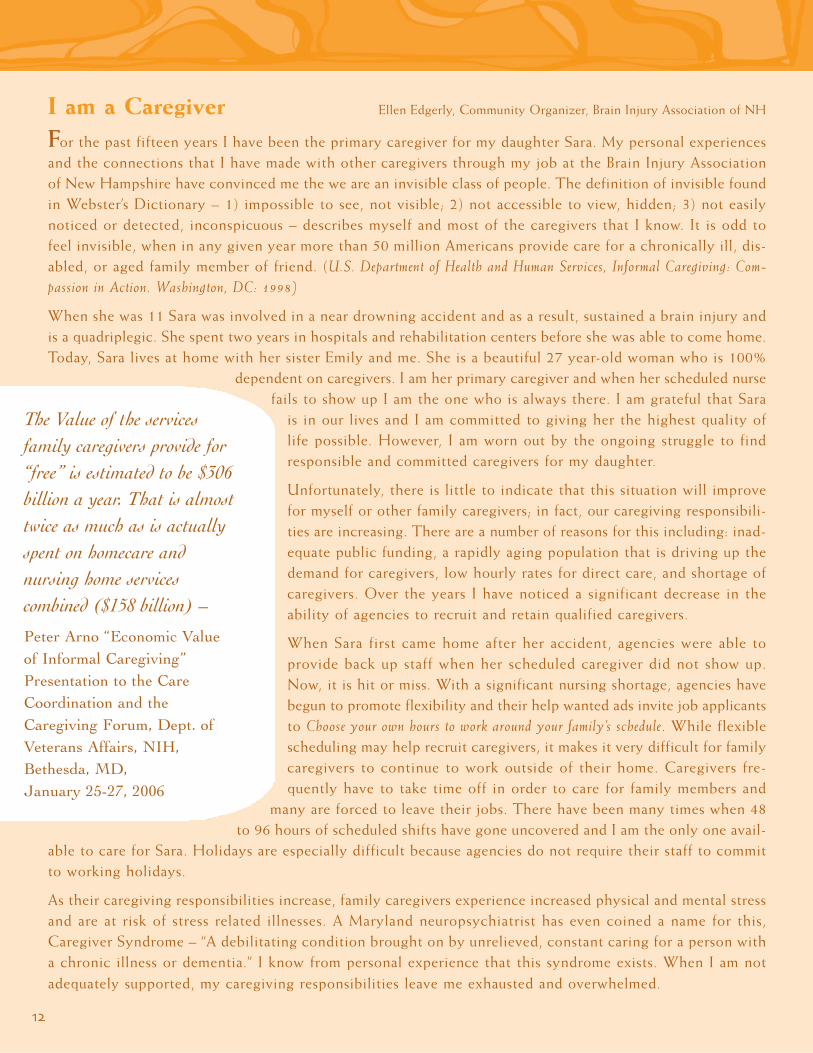
I am a Caregiver Ellen Edgerly, Community Organizer, Brain Injury Association of NH
For the past fifteen years I have been the primary caregiver for my daughter Sara. My personal experiencesand the connections that I have made with other caregivers through my job at the Brain Injury Associationof New Hampshire have convinced me the we are an invisible class of people. The definition of invisible foundin Webster’s Dictionary – 1) impossible to see, not visible; 2) not accessible to view, hidden; 3) not easilynoticed or detected, inconspicuous – describes myself and most of the caregivers that I know. It is odd tofeel invisible, when in any given year more than 50 million Americans provide care for a chronically ill, dis-abled, or aged family member of friend. (U.S. Department of Health and Human Services, Informal Caregiving: Com-passion in Action. Washington, DC: 1998)
When she was 11 Sara was involved in a near drowning accident and as a result, sustained a brain injury andis a quadriplegic. She spent two years in hospitals and rehabilitation centers before she was able to come home.Today, Sara lives at home with her sister Emily and me. She is a beautiful 27 year-old woman who is 100%
dependent on caregivers. I am her primary caregiver and when her scheduled nursefails to show up I am the one who is always there. I am grateful that Sara
is in our lives and I am committed to giving her the highest quality oflife possible. However, I am worn out by the ongoing struggle to findresponsible and committed caregivers for my daughter.
Unfortunately, there is little to indicate that this situation will improvefor myself or other family caregivers; in fact, our caregiving responsibili-ties are increasing. There are a number of reasons for this including: inad-equate public funding, a rapidly aging population that is driving up thedemand for caregivers, low hourly rates for direct care, and shortage ofcaregivers. Over the years I have noticed a significant decrease in theability of agencies to recruit and retain qualified caregivers.
When Sara first came home after her accident, agencies were able toprovide back up staff when her scheduled caregiver did not show up.Now, it is hit or miss. With a significant nursing shortage, agencies havebegun to promote flexibility and their help wanted ads invite job applicantsto Choose your own hours to work around your family’s schedule. While flexiblescheduling may help recruit caregivers, it makes it very difficult for familycaregivers to continue to work outside of their home. Caregivers fre-quently have to take time off in order to care for family members and
many are forced to leave their jobs. There have been many times when 48to 96 hours of scheduled shifts have gone uncovered and I am the only one avail-
able to care for Sara. Holidays are especially difficult because agencies do not require their staff to committo working holidays.
As their caregiving responsibilities increase, family caregivers experience increased physical and mental stressand are at risk of stress related illnesses. A Maryland neuropsychiatrist has even coined a name for this,Caregiver Syndrome – “A debilitating condition brought on by unrelieved, constant caring for a person witha chronic illness or dementia.” I know from personal experience that this syndrome exists. When I am notadequately supported, my caregiving responsibilities leave me exhausted and overwhelmed.
The Value of the servicesfamily caregivers provide for“free” is estimated to be $306billion a year. That is almosttwice as much as is actuallyspent on homecare andnursing home servicescombined ($158 billion) –
Peter Arno “Economic Valueof Informal Caregiving”Presentation to the CareCoordination and theCaregiving Forum, Dept. ofVeterans Affairs, NIH,Bethesda, MD,January 25-27, 2006
13
Over the years, I have found myself thinking about my fellowcaregivers. In particular, those who are trying to stay on an even keeland who are feeling that they have lost control. I want to share whatI have learned and that is the best way an individual can manage herlife is to realize that none of us – caregivers or not – really have anycontrol. An older woman, who is a loving caregiver to her grand-son, recently told me, “If you want to make your god smile, tell himyour life plans.”
I try to enjoy the simple blessings of my life, the smell of a beauti-ful autumn day or the laughter of my grandchildren. I also enjoysitting on the porch swing with Sara beside me in her wheelchairwatching the hummingbirds come to the feeders. George and I havebeen known to bundle Sara up at 1:00 in the morning and wheel heroutside to watch the awesomeness of an August meteor shower.
More importantly I have learned to take care of myself. I am com-mitted to being Sara’s caregiver for the long term. To stay healthyphysically and mentally, I need to occasionally put myself firstwithout feeling guilty. With all that said, please know that I therehave been times when I melt down and imagine getting in mymustang and driving off, but these times are few and far between.I also worry about caregiving responsibilities interfering with mywork. If I lose my job, then what will I do? How will I supportSara, Emily, and myself? OK Ellen, Stop. Remember the reality –we have no control.
Sara Edgerly enjoying time in the garden.
Ell
en
Ed
ge
rly
The Direct Care WorkforceInitiative is a program of the NewHampshire Community Loan Fund. Itsgoal is to improve the quality of low-wageparaprofessional direct care jobs so peopleneeding support can rely on theavailability of a stable, experiencedworkforce. The Initiative is particularlyinterested in developing alliances toadvance policy resulting in a higherquality of care and support for people whoare aging and living with disabilities inNew Hampshire’s communities. Bestpractices are tested at Quality CarePartners, a home care agency based inManchester. For more information,contact Terry Lochhead [email protected].
The Coalition of Caring –Statewide Caregiver ConferenceThis daylong conference will be heldNovember 3, 2007 at Springfield Collegein Manchester. The conference isdesigned for parents, spouses, adultchildren, and friends who are caregivers.Workshops include: Well Being of theCaregiver – Grief and Loss – FindingHumor In Your Life – SettingBoundaries – Legal and FinancialIssues.Conference registration is $20 andincludes lunch. Registration deadlineis October 22, 2007. Space is limited;so please register early.To obtain a Caregivers ConferenceRegistration Form, please contactEllen Edgerly by [email protected] ortelephone 603-332-9891.

14
to be eligible for Medicaid and SSI,even if he or she is the primary ben-eficiary of a trust worth thousands ofdollars. In general, a Special NeedsTrust should not be used for basicneeds such as food, clothing, andshelter. However, it may be used tosupplement care beyond what SSIand Medicaid provide. Expenses cov-ered by a Special Needs Trust mightinclude, among other things, dentalcare, therapies, therapeutic trips orvacations, home ownership, and com-panionship or support services.
In the 2007 legislation session Rep-resentative Ruth Bleyler introducedHB 273 to resolve a long-standingdisagreement between officials at theNew Hampshire Department of Healthand Human Services and trust attor-neys and families over whether thestate could treat distributions fromSpecial Needs Trusts more restric-tively for Medicaid eligibility thanother states which generally follow
( C o n t i n u e d f r o m p a g e 1 1 )
the SSI rules. The bill was passed bythe Legislature and the law, whichgoes into effect on November 1,2007 (Ch. Law 166, RSA 167:4(v)),will align New Hampshire’s distribu-tion rules with those of the rest ofthe country. In effect, the new lawprovides that if distributions fromSpecial Needs Trusts do not violatefederal SSI eligibility rules, then thedistributions will not be disqualifyingfor New Hampshire Medicaid either.This will ensure uniformity and pre-dictability for parents and trusteesgoing forward.
WHO CAN ESTABLISH ASPECIAL NEEDS TRUST?Oddly enough, the one person whocannot establish a Special NeedsTrust is the individual who is the pri-mary beneficiary. In general, SpecialNeeds Trusts must be established(“settled”) by a parent, grandparent,legal guardian, or court. The indi-vidual with the disability who is the
primary beneficiary must be underthe age of 65 (except for pooledtrusts) and must have a disability thatqualifies under the Social SecurityDisability standard. Again, if themonies comprising the trust are orwere those of the person with the dis-ability, it must contain a “pay-back”provision to the state. The funds orother assets not owned by the indi-vidual with the disability do not re-quire reimbursement to the state.
WHO NEEDS A SPECIALNEEDS TRUST?Special Needs Trusts are commonlyused when an individual with a dis-ability receives an unexpected “wind-fall” such as a retroactive Social Secu-rity Disability award, an inheritance,personal injury settlement, or otherlarge sum of money. Parents andgrandparents often use a SpecialNeeds Trust to plan for future finan-cial support for family members with
disabilities. In making decisionsthat will affect the future for aperson with disabilities, theimportance of maintaining Med-icaid eligibility cannot be over-stated. Not only is Medicaid animportant medical insuranceprogram for hospital care andother medical needs (includingmedications), under its various“waiver” programs Medicaid isalso the most significant methodby which people with disabilitiesreceive long-term care and resi-dential and vocational supports.Consequently, individuals withdisabilities and their familymembers should consult withlawyers about the utility of Spe-cial Needs Trusts.Governor Lynch signs into law HB 273.
15
The Family and Medical Leave Act: A Brief OverviewRose Wiant, Esq., Disabilities Rights Center
In 1993 Congress passed the Family and Medical Leave Act (FMLA) to enable employees to take time awayfrom work to deal with a personal illness, to care for a family member with an illness, or to care for a newchild. The FMLA is a means for employees to “balance the demands of the workplace with the needs offamilies” and is intended to “promote the stability and economic security of families.” The FMLA makes itpossible for an employee to take an unpaid, but job-protected, leave of absence for up to 12 weeks peryear.
To be eligible for FMLA leave, the employee must have worked for the employer for at least 12 months,although the 12 months do not necessarily need to be consecutive. Over the 12-month period immedi-ately preceding the leave, the employee must have worked at least 1,250 hours, not including paid vaca-tion or paid sick time. Finally, the employee must work for a covered employer, that is a private employerwith 50 or more employees or any public employer.
Generally speaking, an eligible employee is entitled to take FMLA leave to care for a new child or to address a“serious health condition.” A new child can be a newborn infant, a newly adopted child, or a newly placedfoster child. A serious health condition can pertain to the employee’s own health or to the health of afamily member. The FMLA enables the employee to take time off to deal with his or her own serioushealth condition or to care for a spouse, parent, son, or daughter who has a serious health condition.
Under the FMLA, a serious health condition is “an illness, injury, impairment or physical or mental healthcondition that involves a period of incapacity.” The period of incapacity could be a result of inpatient careor continuing treatment for a health condition lasting more than three days, pregnancy or prenatal care, achronic serious health condition that requires periodic visits to a healthcare provider, a permanent or long-term condition for which treatment might not be effective, or multiple treatments for a condition that wouldlikely result in more than three days of incapacity if not treated. Substance abuse treatment may be cov-ered. Unless there are complications, FMLA leave is not intended for conditions such as the flu or otherminor illnesses or routine dental work. Simply put, serious health conditions are those that are likely torequire professional treatment and a period of recuperation.
The employee must notify the employer of the need for FMLA leave and, when possible, provide 30-daysadvance notice prior to taking the leave. The employee needs to provide enough information related tothe reason for the leave so that the employer can determine whether the requested leave will qualify underFMLA. Generally, FMLA leave is unpaid. However, the employer must hold the employee’s job and mustmaintain the employee’s health insurance.
Upon return from FMLA leave, the employee can expect to return to his or her original position. If notthe same position, the employee must be restored to an equivalent job with equivalent pay and benefits.However, the employee must be able to perform the essential functions of the job. The FMLA makes itpossible for an employee to take time away from work to recuperate from an illness or to care for a familymember without fear of losing his or her job or of losing critical health insurance.
If you would like additional information about the FMLA, a good place to begin is the U.S. Departmentof Labor website (http://www.dol.gov/esa/whd/fmla/). Your employer also can provide information aboutyour rights and responsibilities under the FMLA.
Source: 29 U.S.C. § 2601 et seq.; 29 CFR § 825.

16
The Role of Paraprofessionals inSupporting Students with Disabilities Frank Sgambati, Institute on Disablity
As I travel the state working with teams that are collaborating to include students with special needs intoregular classrooms, I am always amazed at how much success depends upon the quality of involvement thatstudents have with paraprofessionals. Unfortunately, not all districts include paraprofessionals as full mem-bers of the student’s educational team or provide them with the training and support that they need. Instruc-tional assistants and other school paraprofessionals need to be recognized for the valuable role that they play.These members of the school community are typically the ones who spend the most time with special edu-cation students, including those whose needs are the most complex and challenging. Paraprofessionals oftenhave the greatest insight into the student and should be included in the planning process; their input andfeedback is crucial. Those schools where the teachers and team members, including paraprofessionals, plan togetherregularly and where paraprofessionals are routinely asked for their input and feedback create an environmentthat supports students’ success.
I have been working in education for more than 35 years. My introduction to the field - and probably mymost valuable learning experience - was working as a classroom assistant. I was fortunate to work with a teacherwho understood that our working as a team would benefit the whole class. The students in the room saw meas another teacher who was there to support all of them. Drawing from the lessons I’ve learned in my workin schools, and especially from the students I have worked with, I would like to share what I believe are bestpractices for paraprofessionals who are supporting students with disabilities in general education classrooms:
Best Practices for School ParaprofessionalsProvide support that helps the student to becomemore independent
Promote and facilitate social connections andfriendships
Be a resource for all students in the class and lessof a one-to-one aide
Support the student to be a fully participatingmember of the classroom community
Support the classroom teacher to be a teacher forall students, including those with special needs
Support the student to be actively involved in allaspects of the general education curriculum
Work with the team to promote collaboration andon going support between family and school
Seek out and take advantage of professional devel-opment and training opportunities
Without competent paraprofessionals, schools would struggle to include students with disabilities as valuedmembers of the school community. Paraprofessionals deserve recognition for their work and should be includedin the planning process.
PRESIDENTIAL CANDIDATE FORUMON EQUALITY, OPPORTUNITY, AND ACCESS
Friday November 2, 2007 — 8:30-4:00
Radisson Hotel Ballroom, Center of NH, 700 Elm Street, Manchester, NH
Hosted ByGranite State Independent Living
For more information visit our website: www.gsil.org
Or call (603) 228-9680 • 800-826-3700 • 888-396-3459 (TTY)
Co-hosted byNH Council on Developmental Disabilities • Disabilities Rights Center
NH Institute on Disability • NH Spinal Cord Injury Association • People First of NH
SSSSSAAAAAVVVVVE E E E E TTTTTHEHEHEHEHE
DDDDDAAAAATTTTTEEEEE
1717
College of Direct SupportsDavid Johnson, Director of Communications, Moore Center Services
Career opportunities in Direct Support are onthe rise. This is especially true in New Hamp-shire, the state that pioneered community-based care. With an increased demand for com-munity services, a greater number of directsupport professionals (DSPs) are needed.
Moore Center Services in Manchester recog-nizes the importance of attracting committed,compassionate, and competent personnel.Moore Center – a non-profit organization thatserves individuals with developmental disabilitiesand acquired brain disorders and older adults –credits its reputation as an innovator in humanservices to its exceptional team of direct supportprofessionals.
“There is no question that the lifeblood of ouragency is our Direct Support workforce,” saidPaul Boynton, President and CEO of Moore CenterServices. “Their hard work and dedication is criti-cal to the Moore Center and the clients we serve.”
To ensure that there is a qualified direct supportworkforce DSPs need access to advanced training. Aspart of its commitment to quality direct support,Moore Center Services offers training through itsCollege of Direct Support, an intensive, online cur-riculum developed by the University of Minnesota.This training is open to direct support professionalsacross the Granite State and has become a valuablestate-of-the-art teaching tool for New Hampshire’ssocial service agencies.
“It’s an excellent program,” observed Rachel Kingston,Direct of Individual Development Services for MooreCenter. “The College of Direct Support gives my staffa new perspective on the work they do. It makes themfeel even more professional.”
Recently, the College of Direct Support has offereda major incentive for those enrolled in the program.Completion of the curriculum now can be applied
towards a two-year Associates Degree in Human Ser-vices from the New Hampshire Community Techni-cal College at Manchester. In addition, many agen-cies offer wage increases or bonuses to staff memberswho complete courses through the College of DirectSupport.
While access to advanced training is one benefit ofa career in direct support, the real pay-off for directsupport professionals is the satisfaction of helpingothers and making a positive difference in someone’slife. “I enjoy the people here so much,” said HelenBennett, a DSP of 12 years who works in the MooreCenter Elders Day Program. “They give us muchmore than we give them.”
UNH student Nick Ho, who worked in the Eldersprogram over the summer, summed up the feelingsof many direct support professionals when he said,“This is the best job I have ever had.”
For more information about The College of DirectSupport, contact Scott Trudo at 603- 206-2816 [email protected].
Da
vid
Jo
hn
son
Pat Bolieau meets with Jillian Poole, Moore Center DSP and the 2007ANCOR (American Network of Community Options and Resources)DSP of the YEAR for NH
Consumer-Directed Personal Care Services
For over 26 years, Granite State Independent Living has provided consumer-directed personal care services toNew Hampshire residents. Consumer-directed models of home-and community-based long term care (LTC)services are at the forefront of LTC changes across the nation. Consumer-direction is rooted in the belief thatindividuals should have the power to decide the types of LTC services that they need, who will deliver theservices, and when and how the services are delivered. This premise is essential to independent living.
At the heart of the consumer-direction movement in LTC are personal care services. Non-medical in nature,personal care is assistance with activities of daily living, such as bathing, dressing, transferring from bed to chair,toileting, mobility, and nutrition assistance. It also includes housekeeping, cooking, shopping, and laundry.
Personal Care Service Options
Granite State Independent Living (GSIL) offers three options for personal care services: the Personal CareAttendant Program (PCA), the Personal Care Services Program (PCSP), and Independent Care Options (ICO).These programs are self-directed, giving consumers complete control over their personal care. Individuals selectand hire their own personal care workers, and decide how, when, and where their care is provided. GSIL PersonalCare Service Coordinators teach consumers or their designated representatives how to select, hire, and managepersonal care workers to meet their lifestyle needs.
While each program offers a similar scope of service, there are differences in eligibility requirements.
The Personal Care Attendant Program was GSIL’s first personal care program. Individuals who are eligible includethose who:
Are 18 years of age or older
Are their own legal guardian
Are able to self-direct their care
Are medically stable
Do not require 24-hour care
Are Medicaid eligible
Have a severe physical disability
Require a wheelchair for mobility
Require at least two hours of personal care servicesdaily
The PCA program assists individuals with tasks of daily living, such as bathing and dressing, toileting and grooming,housekeeping and cooking, nutrition assistance, mobility assistance, and errands and shopping
UNH Carsey Institute Studies Direct Care Workers
Direct care workers are known by many names:caregivers, direct support professionals, personal careattendants, homemakers, respite workers, home careaides, and companions. The work that they do – assis-tance with personal care, housekeeping, and running er-rands – helps older Americans and individuals withphysical or developmental disabilities to remain in thecommunity living in their own homes. Direct care workerearn low wages, have few benefits and little hope foradvancement. The majority of these workers are women.
The Carsey Institute at the University of New Hamp-shire is nationally recognized for its research on thechallenges facing families. The Institute has a particu-lar interest in low-income working women. Recently,the Carsey Institute’s faculty and staff have developedresearch capacity and expertise in the area of the Di-rect Care Workforce and the Aging Population. Theiranalyses will provide a better understanding of whodirect care workers are and the factors that are affect-ing the high turnover rate in this workforce.
18

In 2000 the option for consumer-directed personal care services was made available through the Home and Com-munity Based Services Waiver for the Elderly and Chronically Ill. Granite State Independent Living was oneof the first organizations to be certified by the state to provide these services. Individuals who are eligible thisprogram include those who:
Qualify for the Home and Community-Based Elderly and Chronically Ill (HCBC-ECI) Waiver program; and
Are able to direct their own care, or
Have an authorized personal care services representative who acts on his or her behalf to direct care.
The PSCP program offers assistance with the same tasks-of-daily living as the PCA program, but PCSPs can alsohelp consumers access their communities by driving them to and from appointments, visits, and other activities.
The newest addition to GSIL’s personal care program is Independent Care Options. While the other two personalcare options are restricted to individuals who are on a Medicaid program, Independent Care Options is availableto individuals who can or wish to pay for personal care services. Individuals who are eligible include those who:
Are 18 years of age or older
Are a New Hampshire resident
Can direct his or her own care, or
Have a personal care representative who acts on his or her behalf to direct care.
The Independent Care Options program provides services that are individually-tailored to meet consumers’lifestyles. Services include but are not limited to:
Basic personal care services
Assistance with accessing the community
Companionship
Respite Care
Chore services
Household Management Services
Granite State Independent Living currently serves over 400 consumers and acts as the “employer of record” forover 700 personal care workers in New Hampshire.
For more information about personal care services please call 603-228-9680 or visit the Long Term Supportssection of Granite State Independent Living’s website at www.gsil.org.
Jill Burke, Vice President of Long-Term Supports, Granite State Independent Living
In addition to its focus on direct caregivers, Carseyresearchers examine the economic status of workingwomen in New Hampshire and New England. TheCarsey Institute provides information to policy mak-ers, practitioners, the media, and the general public onissues concerning working women and family life andwork in rural America. For additional information visitwww.carseyinstitute.unh.edu
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
19
The RThe RThe RThe RThe RAP Sheet is a frAP Sheet is a frAP Sheet is a frAP Sheet is a frAP Sheet is a freeeeeeeeee
quartquartquartquartquarterly publicerly publicerly publicerly publicerly publicaaaaation;tion;tion;tion;tion;
ttttto subscribeo subscribeo subscribeo subscribeo subscribe
please cplease cplease cplease cplease contontontontontacacacacacttttt thethethethethe
DisabilitiesDisabilitiesDisabilitiesDisabilitiesDisabilities Right Right Right Right Rights Cs Cs Cs Cs Centententententer aer aer aer aer attttt
603-603-603-603-603-222222828282828-----04320432043204320432
20
Did you know? The ADA offers protections for familymembers and caregivers tooJames Fox, Esq., Disabilities Rights Center
It is well known that the American with Disabilities Act (ADA) protects people with disabilities from dis-crimination by public accommodations, public entities, and employers (so-called covered entities). But didyou know that the ADA also protects the associates of people with disabilities – family members, friends,caregivers – from discrimination based upon their known relationship or association with a person with adisability? Under the ADA, covered entities are not permitted to take adverse action against any individualbased upon an unfounded or stereotypical fear or belief centering on a third party’s disability. The ADA doesNOT require covered entities to make reasonable accommodations to a person without a disability who isan associate of a person with a disability.
Here are some examples:
An employer may not refuse to hire or promote a person because that person has a child witha disability and the employer has an unfounded belief that the caregiving responsibilities for thechild will mean problems with work attendance.
A restaurant may not refuse or provide substandard service to a person who has a friend whouses a service animal, due to a desire to exclude the person with the service animal.
An employer may not discriminate in hiring against a person who has a family member withAIDS, due to an unfounded belief that the person will themselves contract AIDS or infect otherswithin the workplace.
An employer may not refuse to hire a person who has a spouse with a disability due to anunfounded belief that health insurance coverage costs would go up.
An employer may not exclude an employee from a company’s family picnic based upon anunfounded belief that the employee’s child with autism will attend and be disruptive, or makethe other children uncomfortable.
A doctor’s office may not refuse to take on a new patient who has a spouse with a mental illnessbased upon an unfounded belief that the spouse will accompany the patient to appointments anddisrupt the office.
A law firm that allows its attorneys to take administrative leave to provide pro bono servicesmay not discriminate by refusing to allow an attorney to take this leave to provide pro bonoservices to people with mental illnesses, based on an unfounded belief that it will tarnish theimage of the firm.
For more information see “Questions and Answers about the Association Provision of the Americans withDisabilities Act” on the website of the Equal Employment Opportunity Commission here: www.eeoc.gov/facts/association_ada.html
If you find yourself in a situation where an adverse action has been taken against you based upon your associa-tion with a person with a disability, there are steps you can take to protect your rights. For more informationabout your rights and remedies, contact the Disabilities Rights Center at 1-800-834-1721, www.drcnh.org, or
the NH Commission for Human Rights, (603) 271-2767, www.nh.gov/hrc/.
ξ
21
DirDirDirDirDirececececect Ct Ct Ct Ct Cararararare Re Re Re Re Resouresouresouresouresourccccceseseseses
The Arc of the United StatesThe world’s largest grassroots organization of and for peoplewith intellectual and developmental disabilities.1010 Wayne Avenue, Suite 650Silver Spring, MD 20910(301) 565-3842 / (800) 433-5255 (toll free)www.thearc.org
Carsey Institute at UNHThe Carsey Institute, a nationally recognized research, isexamining factors affecting the high turnover rate in the directcare workforce.For additional information visitwww.carseyinstitute.unh.edu
College of Direct SupportAn internet-based college for direct support professionals.Educating a workforce of Direct Support Professionals –“Building Careers, Supporting Lives.”111 Center Park Drive, Suite 175Knoxville, TN 37922(865) 934-0221 / (877) 353-2767 (toll free)www.info.collegeofdirectsupport.com/In New Hampshire, Moore Center Services is the distributor forthe College of Direct Support: contact either Dave Jenkins orScott Trudo: 603.206.2818 orscott.trudo@moorecenter.
Direct Care Workforce InitiativeNH Community Loan Fund
The Initiative works to improve the quality of low-wageparaprofessional direct care jobs so people needing support canrely on the availability of a stable, experienced workforce.7 Wall St.Concord, NH 03301(603) 224-6669Contact: Terry Lochhead: [email protected]/programs/economic/workforce.html
National Alliance for Direct SupportProfessionals
A coalition of organizations and individuals committed tostrengthening the quality of human service support bystrengthening the direct support workforce.
New Hampshire affiliate:Laura LassinsLifeshare Inc.225 Eddy RoadManchester, NH 03102(603) 625-8825E-Mail: [email protected] www.nadsp.org
New Hampshire Family VoicesFamilies and Friends Speaking on Behalf of Children withSpecial Health Care Needs(603) 271-33451 / (800) 852-3345 (toll free)www.nhfv.org
Paraprofessional Healthcare InstitutePHI works to improve the lives of people who need home andresidential care – and the lives of the workers who providethat care.349 East 149th Street, 10th FloorBronx, NY 10451(718) 402-7766email: [email protected]/
Parent to Parent of New HampshireResources for Parents of Children with Special Needs(800)698-5465 (toll free)www.p2pnh.org
TASHEquity, Opportunity, and Inclusion for People with Disabilitiessince 19751025 Vermont Ave., Floor 7Washington, DC 20005(202) 263-5600www.tash.org/index.html
ABLE NHOver the past several months disability
advocates and family members from across
New Hampshire have come together to
create an independent advocacy organiza-
tion. Advocates Building Lasting Equality in
New Hampshire (ABLE NH) has recently
been incorporated and will be an affiliate
of the Arc of the United States. To become
a member of ABLE NH or for additional
information please contact Julia Freeman-
Woolpert at the Disabilities Rights Center
(603) 228-0432 or by email at
22
The Autism Mini-Series: 2007 DatesJoin experts on Autism Spectrum Disorders (ASD) for topicaldiscussions related to children with ASD, their families, and theirsystems of support. Each small group session is designed to beinformative, interactive, and filled with practical ideas forparenting and teaching.
Location for all Sessions: University of NH, Durham, NHCost: $30 eachDates & Topics:
Wednesday, October 17, 2007: Person CenteredPlanning (PCP) for Young Children with ASD
Time: 3pm – 5pmPresenter: Ann Dillon
Tuesday, October 23, 2007: Promoting Membership,Participation, and Learning for Students with ASD inthe General Education Classroom
Time: 4pm – 6pmPresenters: Michael McSheehan & Cheryl Jorgensen
Wednesday, November 14, 2007: Early Markers forChildren with ASD
Time: 3pm – 5pmPresenter: Ann Dillon
Introductory Training for FacilitatedCommunication (FC)
Will provide participants with a general overview of facilitatedcommunication, FC’s history, basic FC technique, determining FCcandidacy, and a review of research and best practices.
Date & Location: Tuesday, October 9, 2007:Institute on Disability, 56 Old Suncook Rd., Suite 2,Concord, NH
Time: 9am – 3:30pm Cost: $95Presenter: Pascal Cheng, M.Ed.,C.A.S.Life as a Paraprofessional
Comprehensive full-day workshops designed specifically for first-year or seasoned classroom paraprofessionals to present strategiesfor supporting students with challenging behavior.
Time: 9am – 3pm Cost: $90 eachPresenter: Cathy Apfel, M.EdDates & Locations:
Level I: Pre & Elementary SchoolTuesday, October 9, 2007: E.F. Lane, Keene, NHThursday, October 11, 2007: The Highlander Inn,Manchester, NHThursday, December 6, 2007: The Highlander Inn,Manchester, NH
Level II: Middle & High SchoolTuesday, November 6, 2007: Holiday Inn, Concord, NHThursday, November 8, 2007: E.F. Lane, Keene, NH
Strategies for Success SeriesTwo-hour sessions to explore academic and social successstrategies for students with disabilities.
Time: 3:30pm – 5:30pm Cost: $35 eachLocation: Institute on Disability, 56 Old Suncook Road,
Suite 2, Concord, NH 03301Presenters: Cathy Apfel, M.Ed., and Frank Sgambati, MSDates & Topics:
Tuesday, October 16, 2007: Positive Behavior Sup-port: Re-Thinking the Role of ContextTuesday, October 30, 2007 & Tuesday, November 13,2007: Foundations of Effective Classroom Manage-ment: A Guide for Success (Participants must attendboth sessions)Wednesday, November 14, 2007: Parents and Teach-ers Promoting Positive Relationships for Students withDisabilitiesThursday, December 6, 2007: Including Samuel:Strategies on How Schools Can Work for All KidsThursday, December 13, 2007: Teachers and Parapro-fessionals Working Together: Effective Methods ofSupervision and Support
Making Choice Real: Transforming LongTerm Systems of Support
One day conference outlining NH’s efforts to expand and enhance aperson-centered system for older adults and adults with disabilities.
Date & Location: Wednesday, October 24, 2007:Radisson Hotel, Center of NH, Manchester, NH
Time: 8:30am – 3:30pmCost: $50 (professionals); $25 (consumers & families)Presenters: Nancy Rollins, Director, Division of Commu-
nity Based Care Services, NH Dept. of Health &Human Services; Nicholas Toumpas, Acting Commis-sioner, NH Dept. of Health & Human Services; LisaAlecxih, Vice President, The Lewin Group
Building Bridges to the Social World:Strategies for Developing Social Competence
and Connections for Children with AutismFor children with labels of ASD, understanding and participatingin social interactions can be difficult and frustrating. CarolAnn
UPCOMING IODTRAINING AND EVENTS

23
Edscorn, an adult with Asperger’s Syndrome, and Cathy Apfel,M.Ed., team up to offer personal insights and strategies fordeveloping social awareness and competence.
Date & Location: Thursday, October 25, 2007:The Common Man, Plymouth, NH
Time: 8:30am – 3pm Cost: $99Presenters: CarolAnn Edscorn & Cathy Apfel, M.Ed.
Voices of Friendship: How Schools Can
Help or Hinder the Development of Social
RelationshipsWill help participants learn to identify the barriers to friendshipthat exist in many schools and classes, as well the wide variety ofstrategies that schools and families can use to facilitate thedevelopment of friendships.
Date & Location: Monday, October 29, 2007:The Common Man, Concord, NH
Time: 8:30am – 3pm Cost: $90Presenter: Carol Tashie
2007-2008 Autism Research to PracticeSeries
Understanding and Supporting Individuals with Autism andTheir Families
First Series Date & Location: Friday, November 2, 2007:Center of NH Radisson Hotel
Time: 8:30am – 3pm Cost: $125Title: Introduction to the SCERTS ModelPresenter: Amy Laurent, M.Ed., OTR/L
The Latest in Disability Research, Advocacy, Policy, and Practice Fall Issue 2007
N e w H a m p s h i r e
DISABILITIES RIGHTS CENTER, INC.18 Low Avenue, Concord, NH 03301-4971Voice and TDD: (603) 228-0432 1-800-834-1721 FAX: (603) 225-2077TDD access also through NH Relay Service: 1-800-735-2964 (Voice and TDD)E-mail: [email protected] Website: www.drcnh.org“Protection and Advocacy System for New Hampshire”
The Disabilities Rights Center is dedicated to eliminating barriers to the full and equal enjoyment of civil and other legal rights for people with disabilities.
INSTITUTE ON DISABILITY/UCED – UNIVERSITY OF NH10 West Edge Drive, Suite 101, Durham, NH 03824-3522Phone (Tel/TTY): (603) 862-4320 Fax: (603) 862-0555 Website: www.iod.unh.edu
Institute on Disability/UNH – Concord Institute on Disability/UNH – Manchester56 Old Suncook Road, Suite 2 340 Commercial Street, 2nd floorConcord, NH 03301 Manchester, NH 03101Phone (Tel/TTY): (603) 228-2084 Phone: (603) 628-7681
The Institute on Disability advances policies and systems changes, promising practices, education and research that strengthen communities andensure full access, equal opportunities, and participation for all persons.
NH COUNCIL ON DEVELOPMENTAL DISABILITIES21 South Fruit Street, Suite 22, Room 290Concord, NH 03301-2451Phone: (603) 271-3236 TTY/TDD: 1-800-735-2964 Website: www.nhddc.com
Dignity, full rights of citizenship, equal opportunity, and full participation for all New Hampshire citizens with developmental disabilities.
NH COUNCIL ON DEVELOPMENTAL DISABILITIES
21 South Fruit Street, Suite 22, Room 290Concord, NH 03301-2451RETURN SERVICE REQUESTED
This publication was supported solely by federal funding from grants from the Center for Mental Health Services, Substance Abuse and Mental Health ServicesAdministration; Centers for Medicare and Medicaid-Real Choice System Change; U.S. Department of Health and Human Services, Administration on DevelopmentalDisabilities and the Health Resources Services Administration; Maternal and Child Health Bureau; Office of Disability Employment Policy; U.S. Department of EducationDepartment of Rehabilitation Services and National Institute on Disability Rehabilitation and Research (NIDRR); US Department of Labor; and the Social SecurityAdministration.
The contents are solely the responsibility of the grantees and do not necessarily represent the official views of the federal grantors.
INSIDE THIS ISSUEThe Growing Crisis inDirect Care
New Legislation RegardingMedicaid Coverage
Consumer Directed Services
An Introduction to SpecialNeeds Trust
Personal Stories
RAP Sheet