Embed Size (px)
Citation preview

New Frontiers New Frontiers inin Neurotherapy Neurotherapy for for Multiple Sclerosis Multiple Sclerosis
Focus on the Foundation Role of Focus on the Foundation Role of Immunomodulation for Long-Term Efficacy, Immunomodulation for Long-Term Efficacy,
Safety, Neuronal Preservation, and Disability Safety, Neuronal Preservation, and Disability MitigationMitigation
Program ChairmanProgram Chairman
Bruce A. Cree, MD, PhD, MCRBruce A. Cree, MD, PhD, MCRAssistant Professor of NeurologyAssistant Professor of Neurology
Department of NeurologyDepartment of NeurologyUniversity of CaliforniaUniversity of California
San Francisco Multiple Sclerosis CenterSan Francisco Multiple Sclerosis CenterSan Francisco, CaliforniaSan Francisco, California
Investigations • Innovation • Clinical ApplicationInvestigations • Innovation • Clinical Application

Program FacultyProgram Faculty
BRUCE A. CREE, MD, PhD, BRUCE A. CREE, MD, PhD, MCRMCRAssistant Professor of NeurologyAssistant Professor of NeurologyDepartment of NeurologyDepartment of NeurologyUniversity of CaliforniaUniversity of CaliforniaSan Francisco Multiple Sclerosis San Francisco Multiple Sclerosis CenterCenterSan Francisco, CaliforniaSan Francisco, California MARK J. TULLMAN, MDMARK J. TULLMAN, MDAssistant Professor of NeurologyAssistant Professor of NeurologyDirector, Multiple Sclerosis Clinical Director, Multiple Sclerosis Clinical Care Care CenterCenterThe Neurological Institute of New The Neurological Institute of New YorkYorkColumbia University Medical CenterColumbia University Medical CenterNew York, New YorkNew York, New York
ROHIT BAKSHI, MD, FAANROHIT BAKSHI, MD, FAANAssociate Professor of Neurology & Associate Professor of Neurology & RadiologyRadiologyDirector, Laboratory for Director, Laboratory for Neuroimaging Neuroimaging ResearchResearchMS Center, Brigham & Women’s MS Center, Brigham & Women’s HospitalHospitalHarvard Medical SchoolHarvard Medical SchoolBoston, MABoston, MA
GUY J. BUCKLE, MD, MPHGUY J. BUCKLE, MD, MPHDirector of MS Clinical Care Partners Director of MS Clinical Care Partners Multiple Sclerosis CenterMultiple Sclerosis CenterBrigham and Women’s HospitalBrigham and Women’s HospitalAssistant Professor of NeurologyAssistant Professor of NeurologyHarvard Medical SchoolHarvard Medical SchoolBoston, MassachusettsBoston, Massachusetts

The Evidence for First Line The Evidence for First Line Therapy with Immune-Therapy with Immune-
Modulating AgentsModulating AgentsFrom Mechanisms to Therapy—Landmark From Mechanisms to Therapy—Landmark Trials, Long-Term Safety Data and Clinical Trials, Long-Term Safety Data and Clinical
ExperienceExperience
Investigations • Innovation • Clinical ApplicationInvestigations • Innovation • Clinical Application
Program ChairmanProgram ChairmanBruce A. Cree, MD, PhD, MCRBruce A. Cree, MD, PhD, MCR
Assistant Professor of NeurologyAssistant Professor of NeurologyDepartment of NeurologyDepartment of Neurology
University of CaliforniaUniversity of CaliforniaSan Francisco Multiple Sclerosis CenterSan Francisco Multiple Sclerosis Center
San Francisco, CaliforniaSan Francisco, California

OverviewOverview
► Mechanisms of action of first line Mechanisms of action of first line therapiestherapies
► Outcome measures in clinical trialsOutcome measures in clinical trials
► Comparison of landmark trialsComparison of landmark trials
► Longitudinal studies: what do they tell Longitudinal studies: what do they tell us?us?

Goals of TreatmentGoals of Treatment
► Reduce frequency of relapseReduce frequency of relapse
► Slow progression of disabilitySlow progression of disability
► Reduce MRI activityReduce MRI activity
► Prevent morbidity from symptoms and Prevent morbidity from symptoms and provide palliative careprovide palliative care
► Maintain adherenceMaintain adherence
► Provide long-term efficacy and safety Provide long-term efficacy and safety

TregTh2/Th3
MO
IL-4IL-5IL-6
IL-13TGF
B
HistamineProteases
TNFNAA, ATP
NOO2
5-HT
Mast Cell
IL-12
APC
Thp
CD4
CD40LCD40
IL-4 & IL-10
CD4APCThp
CD28B7
Th2/Th3
B7
CD40
MicrogliaCD40L
CD28
Th1Th17
B
Glutamate
TCD8
MMP-2/9
VCAM-1ICAM-1 VCAM-1
IFNTNFIL-17
IL-10TGF
Ab+C9neo
CD8
Mast Cell
T
Granutocyte
Complement
Monocyte
Pl
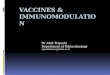
Figure courtesy of Dhib-Jalbut S, 2008
Immunopathogenesis of the MS LesionImmunopathogenesis of the MS Lesion
IFNTNFTh17
NOOi
TNFaMMP
LFA-1VLA-4Th1
Th17
Oligo
BBB
MCP-1MIP-1P-10
RANTES
Astrocyte
IL-23
Treg
CD4+CD25+
Myelin AgMicrobial Ag
HLA
Virus
TCR

IFN-IFN-: Activity: Activity
TH1+
RestingT cell
MMP
Activated (+)T cells
TH1+
TH1+
MMP
BBBBlood CNS
TNF-α IFN-γ
IL-2
TH1APC APC
IFN-β
IFN-β
MyelinproteinAntigen
TH1+
Adapted from Yong VW. Adapted from Yong VW. NeurologyNeurology. 2002;59:802-808.. 2002;59:802-808.

Glatiramer Acetate: ActivityGlatiramer Acetate: Activity
Adapted from Ziemssen T et al. J Neurol Sci. 2005;233:109-112.Adapted from Ziemssen T et al. J Neurol Sci. 2005;233:109-112.
BBB
GA-specificT cell
APC
GA
ther
apy
TH1 TH2
APC
Microglia
MHC
CNS Ag
TCR
Macrophage
Periphery CNS
TH2
MHC
GA
TCR
Neuroregeneration
Bystandersuppression
effect
Anti-inflammatory cytokines
Neurotrophins+ +
TCRIL-4
IL-10
BDNF

Low (0-1 attacks in 2 years)Low (0-1 attacks in 2 years)
Intermediate (2-4 attacks in 2 years)Intermediate (2-4 attacks in 2 years)
High (High (>> 5 in 2 years) 5 in 2 years)
Weinhenker B et al. Brain. 1989;112:1422Weinhenker B et al. Brain. 1989;112:1422
Long-Term DisabilityLong-Term DisabilityEffect of Early RelapsesEffect of Early Relapses
50504040303020201010
2020
00
00
4040
6060
8080
100100
Time from onset of MS (years)Time from onset of MS (years)
Per
cent
Pts
DS
S <
6P
erce
nt P
ts D
SS
< 6
p < 0.0001p < 0.0001

Number of Attacks, 1Number of Attacks, 1stst 2 years 2 years p <0.001p <0.001
Interval Between 1Interval Between 1stst 2 Attacks 2 Attacks p <0.001p <0.001
DSS at 2 yearsDSS at 2 years p < 0.001p < 0.001
DSS at 5 yearsDSS at 5 years p < 0.001p < 0.001
Development of DisabilityDevelopment of DisabilityEffect of Early Clinical Course Effect of Early Clinical Course
Clinical CharacteristicClinical Characteristic Significance*Significance*
* Controlled for age at onset, remitting at onset, cerebellar, cerebral* Controlled for age at onset, remitting at onset, cerebellar, cerebral
Weinshenker B et al. Weinshenker B et al. Brain. 1991;114 ( Pt 2):1045-56.Brain. 1991;114 ( Pt 2):1045-56.

Relapses in MSRelapses in MS
► Relapses are the most obvious evidence of Relapses are the most obvious evidence of inflammatory disease activity in RRMS inflammatory disease activity in RRMS
► Relapse frequency in typical untreated Relapse frequency in typical untreated RRMS populations enables treatment effect RRMS populations enables treatment effect to be rapidly assessable in a 12-month to be rapidly assessable in a 12-month clinical studyclinical study
Total number of relapses during the study periodTotal in-study person-years

Effect on Annualized Relapse Rates: Summary Effect on Annualized Relapse Rates: Summary of Phase III Trials – 2 years in-studyof Phase III Trials – 2 years in-study
35
% R
educ
tion
in r
elap
se r
ates
% R
educ
tion
in r
elap
se r
ates
30
25
20
15
10
5
0
31%
8 MIU qod8 MIU qodIFN beta-1bIFN beta-1b
P=0.0001
29%
4.4 MIU tiw4.4 MIU tiwIFN beta-1aIFN beta-1a
P<0.001
32%
8.8 MIU tiw8.8 MIU tiwIFN beta-1aIFN beta-1a
P<0.0001
29%
20 mg qd20 mg qdglatiramer acetateglatiramer acetate
P=0.055P=0.055
6 MIU qw6 MIU qwIFN beta-1aIFN beta-1a
P=0.04
18%
N.B.: Results are from separate clinical trialsJacobs et al. Ann Neurol. 1996;39:285; IFNB MS Study Group. Neurology. 1993;43:655; IFNB MS Study Group and University of British Columbia MS/MRI Analysis Group. Neurology. 1995;45:1277; Johnson et al. Neurology. 1995:45:1268; Johnson et al. Neurology. 1998;50:701; PRISMS Study Group. Lancet. 1998;352:1498; Rebif package insert.

Is MS All About Relapses? Is MS All About Relapses?
► Hypothesis: if relapses cause long-term Hypothesis: if relapses cause long-term disability then patients with frequent disability then patients with frequent relapses should be at higher risk for relapses should be at higher risk for disabilitydisability
► From the London Ontario natural history From the London Ontario natural history studies patients with frequent attacks studies patients with frequent attacks are at highest risk for future ambulatory are at highest risk for future ambulatory disabilitydisability
► Assumption: modifying the relapse rate Assumption: modifying the relapse rate will influence long-term disabilitywill influence long-term disability
Weinshenker et al. 1989 Brain 112:1419Weinshenker et al. 1989 Brain 112:1419

Proportion of Placebo Groups Proportion of Placebo Groups with Clinical Activity with Clinical Activity
Jacobs et al. Ann Neurol. 1996;39:285; IFNB MS Study Group. Neurology. 1993;43:655; IFNB MS Study Group and University of British Columbia MS/MRI Analysis Group. Neurology. 1995;45:1277; Johnson et al. Neurology. 1995:45:1268; Johnson et al. Neurology. 1998;50:701; PRISMS Study Group. Lancet. 1998;352:1498.
RelapsesRelapses EDSS EDSS ProgressProgress
IFNIFNββ-1b (3 year)-1b (3 year) 86%86% 39%39%
IFNIFNββ-1a (QW) (2 year)-1a (QW) (2 year) 77%77% 35%35%
IFNIFNββ-1a (TIW) (2 year)-1a (TIW) (2 year) 84%84% 38%38%
Glatiramer acetate (2 year)Glatiramer acetate (2 year) 73%73% 25%25%

How is Sustained Progression How is Sustained Progression Measured?Measured?
► Most clinical trials define progression by Most clinical trials define progression by comparing the change in EDSS from comparing the change in EDSS from baseline to study conclusion, and then baseline to study conclusion, and then confirmconfirm the change in EDSS at 3 or 6 the change in EDSS at 3 or 6 monthsmonths
► Does this measure of confirmed Does this measure of confirmed progression reflect permanent disability?progression reflect permanent disability?
► If so, then confirmed changes in EDSS If so, then confirmed changes in EDSS during the course of the trial should be during the course of the trial should be sustainedsustained by the end of the study by the end of the study

Does Sustained Disability Measure Does Sustained Disability Measure Permanent Disability?Permanent Disability?
► 50% of patients with a 1 point change, 50% of patients with a 1 point change, confirmed at 3 months will improve to a lower confirmed at 3 months will improve to a lower EDSSEDSS
► 33% of patients with a 1 point change, 33% of patients with a 1 point change, confirmed at 6 months, will improve to a lower confirmed at 6 months, will improve to a lower EDSSEDSS
► More stringent measures of change are harder More stringent measures of change are harder to demonstrate in 2-year trials because to demonstrate in 2-year trials because relatively few MS patients will progress relatively few MS patients will progress
► Conclusions: Conclusions: 6 months sustained EDSS change 6 months sustained EDSS change is more rigorous than a 3-month sustained is more rigorous than a 3-month sustained change, but neither is a good predictor of long change, but neither is a good predictor of long term disabilityterm disabilityLiu C & Blumhardt LD Liu C & Blumhardt LD J Neurol Neurosurg Psychiatry. 2000J Neurol Neurosurg Psychiatry. 2000;;68:450-7.68:450-7.

**1 EDSS point sustained for 1 EDSS point sustained for 6 months in 6 MIU qw phase III trial6 months in 6 MIU qw phase III trial and for and for 3 months 3 months in all other in all other phase III trials.phase III trials.
Jacobs et al. Ann Neurol. 1996;39:285; IFNB MS Study Group. Neurology. 1993;43:655IFNB MS Study Group and University of British Columbia MS/MRI Analysis Group. Neurology. 1995;45:1277Johnson et al. Neurology. 1995:45:1268; Johnson et al. Neurology. 1998;50:701PRISMS Study Group. Lancet. 1998;352:1498
Effect on Sustained Disability*: Effect on Sustained Disability*: Summary of Phase III TrialsSummary of Phase III Trials
40
Reduct
ion in
R
educt
ion in
su
stain
ed d
isabili
ty
sust
ain
ed d
isabili
ty
pro
gre
ssio
n (
%)
pro
gre
ssio
n (
%)
12%
22%
30%
NS
30
20
10
0
8.8 MIU tiw8.8 MIU tiwIFN beta-1aIFN beta-1a
4.4 MIU tiw4.4 MIU tiwIFN beta-1aIFN beta-1a
20 mg qd20 mg qdglatiramer acetateglatiramer acetate
p<0.05
p<0.05
p=NSp=NS
37%
6 MIU qw6 MIU qwIFN beta-1aIFN beta-1a
p=0.0229%
8 MIU qod8 MIU qodIFN beta-1bIFN beta-1b
p=NSp=NS

SummarySummary
► Relapses and disability progression represent Relapses and disability progression represent different but complimentary aspects of MS natural different but complimentary aspects of MS natural historyhistory
► Relapse rate reduction and the mean change in Relapse rate reduction and the mean change in EDSS are the most sensitive clinical outcome EDSS are the most sensitive clinical outcome measures in MS trialsmeasures in MS trials
► The generally accepted sustained change in EDSS The generally accepted sustained change in EDSS measure is not a reliable marker of long term measure is not a reliable marker of long term disability disability
► Phase III trials results showed:Phase III trials results showed: The interferons and glatiramer acetate modestly reduce the relapse The interferons and glatiramer acetate modestly reduce the relapse
raterate IFN beta-1a has a statistically significant impact on sustained IFN beta-1a has a statistically significant impact on sustained
disability progression over two yearsdisability progression over two years IFN beta-1a and glatiramer acetate have a statistically significant IFN beta-1a and glatiramer acetate have a statistically significant
impact on the mean EDSS over two yearimpact on the mean EDSS over two year

Are direct comparator studies Are direct comparator studies needed in MS or can we make needed in MS or can we make
valid conclusions from cross trial valid conclusions from cross trial comparisons?comparisons?

Cross Trial ComparisonsCross Trial ComparisonsRelative Efficacy (RR)Relative Efficacy (RR)
IFNIFNββ-1a-1a30 30 µµgg qwqw
IFNIFNββ-1b, -1b, 250 250 µµgg
qodqod
IFN IFN ββ-1a -1a 44 44 µµgg
tiwtiw
GA GA 20 mg20 mg
qdqd
Relapse rate (annualized)Relapse rate (annualized) -18%-18% -34%-34% -32%-32% -29%-29%
Relapse-Free (2 years)Relapse-Free (2 years) +42%+42% +95%+95% +100%+100% +36%+36%
Progression free Progression free -37%-37% -29%-29% -30%-30% -12%-12%
New T2 LesionsNew T2 Lesions -36%-36% -83%-83% -78%-78% -38%-38%
Gd+ LesionsGd+ Lesions -42%-42% -- -88%-88% -33%-33%
BODBOD - 4%- 4% -17%-17% -15%-15% -8%-8%

672 days (96 weeks)
IFNβ-1a
GA
Time to first relapse (days)Time to first relapse (days)
Hazard ratio (95% CI): 0.943 (0.74, 1.21) p = 0.643
0 100 200 300 400 500 600 700
0.00
0.25
0.50
0.75
1.00
Sur
viva
l dis
trib
utio
n fu
nctio
nS
urvi
val d
istr
ibut
ion
func
tion
The REGARD TrialThe REGARD TrialTime to First Relapse (1Time to First Relapse (1oo endpoint) endpoint)

The BEYOND TrialThe BEYOND TrialRelapse Risk (1Relapse Risk (1oo Endpoint) Endpoint)
►No significant difference in relapse risk between any groupNo significant difference in relapse risk between any group
Interferon beta-1bInterferon beta-1b 500 500 vs. vs. Interferon beta-1bInterferon beta-1b 250 250
Interferon beta-1b Interferon beta-1b 500500vs. Glatiramer acetatevs. Glatiramer acetate
Interferon beta-1b Interferon beta-1b 250250vs. Glatiramer acetatevs. Glatiramer acetate
Primary AnalysisPrimary Analysis
Sensitivity Analysis Sensitivity Analysis (no major protocol violations, (no major protocol violations,
100% of doses, post-hoc)100% of doses, post-hoc)
P-valuesP-values(one-sided)(one-sided)
P-valuesP-values(one-sided)(one-sided)
P=0.16P=0.16
P=0.73P=0.73
P=0.43P=0.43
P=0.29P=0.29
P=0.30P=0.30
P=0.18P=0.18
0.50.5 1.0 1.5 1.0 1.50.50.5 1.0 1.5 1.0 1.5

What can be learned from What can be learned from long-term follow up studies?long-term follow up studies?

Long-Term Follow UpLong-Term Follow Up
► Do long-term follow up studies Do long-term follow up studies adequately address medication safety?adequately address medication safety?
► Do long-term studies adequately Do long-term studies adequately address longitudinal efficacy?address longitudinal efficacy?
► Have methods of analysis for Have methods of analysis for longitudinal studies been optimized?longitudinal studies been optimized?

BiasBias ImpactImpact StrategyStrategy
AscertainmentAscertainmentModified therapeutic effect dependent Modified therapeutic effect dependent
on characteristics of participating on characteristics of participating patients.patients.
F/U must be as complete as possible F/U must be as complete as possible Directly compare baseline and on-Directly compare baseline and on-RCT characteristics of those RCT characteristics of those patients in LTF to those not in LTFpatients in LTF to those not in LTF
Informed Informed Therapeutic Therapeutic DecisionsDecisions
Inflated estimate of therapeutic benefit Inflated estimate of therapeutic benefit because patients doing well because patients doing well continue therapy whereas failing continue therapy whereas failing patients switch or stop therapy.patients switch or stop therapy.
MPR: Use percent of total possible MPR: Use percent of total possible time on therapy instead of time on therapy instead of absolute time to assess exposure.absolute time to assess exposure.
Treatment Treatment SelectionSelection
Modified therapeutic effect dependent Modified therapeutic effect dependent on patient selection characteristics.on patient selection characteristics.
Propensity Scoring: Adjust for the Propensity Scoring: Adjust for the propensity (i.e., likelihood) that a propensity (i.e., likelihood) that a particular treatment will be particular treatment will be selected based on available selected based on available patient characteristicspatient characteristics
Multiple TestingMultiple TestingIncreased risk of Type 1 error from the Increased risk of Type 1 error from the
use of multiple predictor variables use of multiple predictor variables and weighting schemesand weighting schemes
Create a single model and apply Create a single model and apply adjustments to p-values according adjustments to p-values according to the number of predictors tested to the number of predictors tested in the model.in the model.
Sources of Bias in LTFU StudiesSources of Bias in LTFU Studies

Glatiramer Acetate 15 year LTFUGlatiramer Acetate 15 year LTFU
Ford C et al. Mult Scler. 2010;16:342-50. Ford C et al. Mult Scler. 2010;16:342-50.

Glatiramer Acetate 15 year LTFUGlatiramer Acetate 15 year LTFU
Ford C et al. Mult Scler. 2010;16:342-50. Ford C et al. Mult Scler. 2010;16:342-50.

Glatiramer Acetate 15 year LTFUGlatiramer Acetate 15 year LTFU
► In a small cohort of patients followed for In a small cohort of patients followed for 15 years, glatiramer acetate was safe and 15 years, glatiramer acetate was safe and well toleratedwell tolerated
► 65% of continuously treated patients did 65% of continuously treated patients did not progress to SPMSnot progress to SPMS
► 41% of patients withdrawing from the 41% of patients withdrawing from the study did so because of disease study did so because of disease progressionprogression● Propensity scores were used to try to adjust Propensity scores were used to try to adjust
for differences between ongoing and for differences between ongoing and withdrawing patientswithdrawing patients
► EDSS at baseline predicts EDSS at 15 EDSS at baseline predicts EDSS at 15 yearsyears

IFN IFN ββ-1a (QW) LTFU Disposition-1a (QW) LTFU Disposition
Bermel R et al. Mult Scler. 2010 Feb 18. [Epub ahead of print]Bermel R et al. Mult Scler. 2010 Feb 18. [Epub ahead of print]
Complete 2-year follow-up(n=172)
Unascertained(n=36)
Ascertained for ASSURANCE(n=136; 79%)
Able to locate,Unable to contact
(n=13)
Unable to locate(n=23)
Living(n=122; 90%)
Deceased(n=14; 10%)
ICF and question booklet
completedLOCF

IFN IFN ββ-1a QW LTFU Outcomes-1a QW LTFU Outcomes
Bermel R et al. Mult Scler. 2010 Feb 18. [Epub ahead of print]Bermel R et al. Mult Scler. 2010 Feb 18. [Epub ahead of print]
Currently receiving IM IFN ß-1a (n=56)Currently receiving IM IFN ß-1a (n=56)Not currently receiving IM IFN ß-1a (n=66)Not currently receiving IM IFN ß-1a (n=66)
Pat
ient
s, %
Pat
ient
s, %
Pat
ient
s, %
Pat
ient
s, %
P=0.062P=0.062
EDSS MilestoneEDSS Milestone
P=0.326P=0.326P=0.114P=0.114
P=0.006P=0.006

IFN IFN ββ-1a QW LTFU Conclusions-1a QW LTFU Conclusions
► 79% of eligible patients were located for the 15 79% of eligible patients were located for the 15 year follow upyear follow up
► At 15 years, patients currently on IFN At 15 years, patients currently on IFN ββ-1a had -1a had less progression in EDSS scores than patients less progression in EDSS scores than patients not on IFN not on IFN ββ-1a -1a
► However, patients not currently on IFN However, patients not currently on IFN ββ-1a had -1a had higher baseline EDSS scores suggesting more higher baseline EDSS scores suggesting more severe baseline MSsevere baseline MS● Propensity scores were used to adjust for these Propensity scores were used to adjust for these
differencesdifferences
► Inferences with regard to association with lower Inferences with regard to association with lower EDSS and ongoing treatment were not made EDSS and ongoing treatment were not made
Bermel R et al. Mult Scler. 2010 Feb 18. [Epub ahead of print]

124124
125125
123123
5252
5858
5656IFNβ-1b 250 µg
IFNβ-1b 50 µg
Placebo
1988 1993
Pivotal Study (n=372)Pivotal Study (n=372)
LTF
2005
Cross-sectional investigation of:- clinical outcomes (disability, relapse rate)- imaging (brain and spinal MRI)- cognition and mood- QoL, resource use- lab parameter including NAb's and PgX
Patients under regular medical care - no trial
1990
IFN IFN ββ-1b LTFU Design-1b LTFU Design
Ebers G et al. presented at ECTRIMS, Madrid, Spain, September 2006: P666Ebers G et al. presented at ECTRIMS, Madrid, Spain, September 2006: P666Ebers G et al. presented at AAN, October 2006: M-3Ebers G et al. presented at AAN, October 2006: M-3

Event Rates and Long-Term EfficacyEvent Rates and Long-Term EfficacyClinical and Radiological EndpointsClinical and Radiological Endpoints
1.1. Need to demonstrate that the short-Need to demonstrate that the short-term event-rates are correlated with term event-rates are correlated with long-term outcome.long-term outcome.
2.2. Need to demonstrate that the short-Need to demonstrate that the short-term event-rates contribute term event-rates contribute independently to predicting outcome.independently to predicting outcome.
3.3. Need to demonstrate that therapies Need to demonstrate that therapies which reduce the event-rates, are also which reduce the event-rates, are also associated with improved long-term associated with improved long-term outcome.outcome.
Ebers G et al. presented at ECTRIMS, Madrid, Spain, September 2006: P666Ebers G et al. presented at ECTRIMS, Madrid, Spain, September 2006: P666Ebers G et al. presented at AAN, October 2006: M-3Ebers G et al. presented at AAN, October 2006: M-3

IFN IFN ββ-1b LTFU Adjusted OUtcome-1b LTFU Adjusted OUtcome
Any Variable + Any Exposure Weighting – Any Negative Outcome
EDSSp<0.001
1
Exposurep<0.001
2
HighLow
Ebers G et al. presented at ECTRIMS, Madrid, Spain, September 2006: P666Ebers G et al. presented at ECTRIMS, Madrid, Spain, September 2006: P666Ebers G et al. presented at AAN, October 2006: M-3Ebers G et al. presented at AAN, October 2006: M-3

Event Rates and Long-Term EfficacyEvent Rates and Long-Term EfficacyConclusionsConclusions
1.1. The LTF study demonstrates that the short-term The LTF study demonstrates that the short-term event-rate is correlated with long-term outcome.event-rate is correlated with long-term outcome.
2.2. The LTF study also demonstrates that the short-The LTF study also demonstrates that the short-term event-rate contributes independently to term event-rate contributes independently to predicting long-term outcome.predicting long-term outcome.
3.3. The LTF study provides convincing evidence that The LTF study provides convincing evidence that early initiation and sustained use of IFNearly initiation and sustained use of IFNββ-1b has a -1b has a beneficial impact on long-term outcome in MS.beneficial impact on long-term outcome in MS.
4.4. The analysis strategy employed provides a The analysis strategy employed provides a methodological framework for mitigating bias in methodological framework for mitigating bias in assessing long-term efficacy in other clinical trials assessing long-term efficacy in other clinical trials having similar non-randomized data.having similar non-randomized data.

► Disease modifying therapy seems favorably effect the Disease modifying therapy seems favorably effect the long-term course of MSlong-term course of MS
► Propensity score adjusted analysis and other statistical Propensity score adjusted analysis and other statistical methods for controlling biases inherent in long term, methods for controlling biases inherent in long term, unblinded studies are important statistical advances for unblinded studies are important statistical advances for interpreting these studiesinterpreting these studies
► Once the MS community agrees on the relevant Once the MS community agrees on the relevant covariates, these methods can be used to sort out some covariates, these methods can be used to sort out some of these issues without the cost (and ethical dilemmas) of these issues without the cost (and ethical dilemmas) posed by long-term placebo-controlled trials.posed by long-term placebo-controlled trials.
ConclusionsConclusions

The Emergence of The Emergence of Immunosuppressive Agents for MSImmunosuppressive Agents for MS
Safety, Efficacy, and Cautionary Notes—Safety, Efficacy, and Cautionary Notes—Patient Monitoring, Risks for Infection, and Patient Monitoring, Risks for Infection, and
Mechanisms of Action Mechanisms of Action
Mark J. Tullman, MDMark J. Tullman, MDAssistant Professor of NeurologyAssistant Professor of Neurology
Director, Multiple Sclerosis Clinical Care CenterDirector, Multiple Sclerosis Clinical Care CenterThe Neurological Institute of New YorkThe Neurological Institute of New York
Columbia University Medical CenterColumbia University Medical CenterNew York, New YorkNew York, New York
Investigations • Innovation • Clinical ApplicationInvestigations • Innovation • Clinical Application

Existing and Emerging MS TherapiesExisting and Emerging MS Therapies
20052005 2011201120062006 20072007 20102010 20122012 20132013
Injectables
IV
Generic Mitoxantrone (oncology) (MS)
Generic Mitoxantrone (oncology) (MS)
TysabriTysabri
Rebif
Filed
Approved In phase II
In phase III
Cladribine
AmpyraAmpyra
BG12
Teriflunomide
Laquinimod
Ocrelizumab
IV
Alemtuzumab
Oral
ExtaviaExtavia
Rebif
Betaseron
Copaxone
Avonex
Novantrone
Ampyra
Extavia
Tysabri
BG12Caldribine
Fingolimod
Ocrelizumab
TeriflunomideTeriflunomide
LaquinimodLaquinimod
AlemtuzumabAlemtuzumab
GenericMitoxantrone
(oncology) MS

Efficacy in Recent StudiesEfficacy in Recent Studies
► Annualized relapse rate 0.29-0.36 over 2 yearsAnnualized relapse rate 0.29-0.36 over 2 years► 58-61% relapse-free over 2 years58-61% relapse-free over 2 years► 79-81% without disability progression over 2 79-81% without disability progression over 2
yearsyears► 88.3% without disability progression over 96 88.3% without disability progression over 96
weeksweeks► 91.3% without disability progression over 96 91.3% without disability progression over 96
weeksweeks► 74% without disability progression over 3 years74% without disability progression over 3 years► 75% without EDSS progression 5 years after 75% without EDSS progression 5 years after
CIS onsetCIS onset► 13.3% 13.3% reductionreduction in MRI T2 lesion load over 3 in MRI T2 lesion load over 3
yearsyears► All in placebo, interferon, or glatiramer All in placebo, interferon, or glatiramer
acetate-treated patientsacetate-treated patients
Kappos L, et al. Lancet Neurol 2009; 8: 987–97; Giovannoni G, et al. N Engl J Med. 2010;362:416-426; CAMMS223 Trial Investigators. NEJM 2008;359:1786-1801; Kappos L et al. N Engl J Med. 2006;355:1124-40; Mikol et al. Lancet Neurol 2008; 7: 903–14

Prognostic SignsPrognostic Signs
► Favorable OutcomeFavorable Outcome● Female Female ● Younger age at onsetYounger age at onset● Little disability 5 Little disability 5
years after onset years after onset ● Optic neuritis as 1Optic neuritis as 1stst
attackattack
► Worse OutcomeWorse Outcome● MaleMale● Older age at onsetOlder age at onset● Frequent attacks Frequent attacks ● Short interval Short interval
between 1between 1stst 2 attacks 2 attacks● Incomplete recovery Incomplete recovery
from 1from 1stst attack attack● Cerebellar Cerebellar
involvement as 1involvement as 1stst symptomsymptom
● Rapidly accumulating Rapidly accumulating disabilitydisability
● Progressive disease Progressive disease from onsetfrom onset

Baseline Brain MRI Lesion NumberBaseline Brain MRI Lesion Number20-Year Clinical Status20-Year Clinical Status
Fisniku LK. Brain 2008;131:808-817.

Baseline Brain MRI Lesion NumberBaseline Brain MRI Lesion Number20-Year Clinical Status20-Year Clinical Status
Fisniku LK. Brain 2008;131:808-817.

Disease Free StateDisease Free State
Proportion Free of Clinical and MRI ActivityProportion Free of Clinical and MRI Activity
p < 0.0001
Hardova E, et al. Lancet Neurol 2009;8:254-60.
Natalizumab Placebo

AlemtuzumabAlemtuzumab
► Monoclonal humanized antibody directed Monoclonal humanized antibody directed against CD52 antigenagainst CD52 antigen
● CD52 antigen is a cell surface glycoprotein that CD52 antigen is a cell surface glycoprotein that is present on >95% of T lymphocytes, B is present on >95% of T lymphocytes, B lymphocytes, monocytes, and eosinophilslymphocytes, monocytes, and eosinophils
● Results in prolonged depletion of B cells, T cells, Results in prolonged depletion of B cells, T cells, and monocytesand monocytes
► Within an hour following a single 5- to 10-mg Within an hour following a single 5- to 10-mg dose, lymphocytes and monocytes are no dose, lymphocytes and monocytes are no longer detectable in circulationlonger detectable in circulation
► FDA-approved for B-CLLFDA-approved for B-CLLMuraro P, et al. Neurotherapeutics. 2007;4:676-692. Coles A, et al. J Neurol. 2006;253:98-108.Muraro P, et al. Neurotherapeutics. 2007;4:676-692. Coles A, et al. J Neurol. 2006;253:98-108.

CAMMS223 Trial Investigators. NEJM 2008;359:1786-1801.CAMMS223 Trial Investigators. NEJM 2008;359:1786-1801.
Month 0 Month 12Month 0 Month 12 Month 24 Month 24 Month 36 Month 36
107107 95 80 95 80 6666
108108 105 104 105 104 9292
108108 102 101 102 101 92922424
7777
2222
8888
IFNIFNββ-1a-1a44 mcg thw SC44 mcg thw SC
AlemtuzumabAlemtuzumab12 mg daily IV12 mg daily IV
AlemtuzumabAlemtuzumab24 mg daily IV24 mg daily IV

Alemtuzumab CAMMS223: Co-Alemtuzumab CAMMS223: Co-Primary Endpoints (36 months)Primary Endpoints (36 months)
CAMMS223 Trial Investigators. NEJM 2008;359:1786-1801.CAMMS223 Trial Investigators. NEJM 2008;359:1786-1801.

Alemtuzumab CAMMS223: Alemtuzumab CAMMS223: MRI OutcomesMRI Outcomes
CAMMS223 Trial Investigators. N Engl J Med. 2008;359:1786-1801.
P≤0.03 for both doses of alemtuzumab vs. IFN at m 0-12 and 0-24. P=NS at m 0-36
Months 0-12 0-24 0-36
n=91
n=96
n=100
n=75
n=96n=91
n=60
n=80
n=87
P=0.16
P=0.04
P=0.04
P=0.03
Months 0-36 12-36

Alemtuzumab CAMMS223: SafetyAlemtuzumab CAMMS223: Safety
► Principal AEs associated with alemtuzumab Principal AEs associated with alemtuzumab
included:included:
● Infusion reactionsInfusion reactions
● Mild-to-moderate infectionsMild-to-moderate infections
● AutoimmunityAutoimmunity• Immune thrombocytopenia in 6 of 216 patients Immune thrombocytopenia in 6 of 216 patients
(2.8%)(2.8%) including one deathincluding one death
• Thyroid disorders (28% vs. 3% for IFNThyroid disorders (28% vs. 3% for IFNββ-1a)-1a)
• 1 case of Goodpasture’s syndrome1 case of Goodpasture’s syndrome
CAMMS223 Trial Investigators. N Engl J Med. 2008;359:1786-1801. CAMMS223 Trial Investigators. N Engl J Med. 2008;359:1786-1801.

Alemtuzumab CAMMS223: SafetyAlemtuzumab CAMMS223: Safety
Infections, %IFN ß-1a(n=107)
Alem 12 mg
(n=108)
Alem 24 mg
(n=108)
Upper resp. infection* 27.1 44.4 50.9
Lower resp. infection* 1.9 11.1 13.9
Herpes simplex 2.8 8.3 8.3
Herpes zoster 0.9 1.9 5.6
Meningitis** 0 0 1.8
* P<0.001 alemtuzumab vs. IFN ** Listeria or viral meningitis
CAMMS223 Trial Investigators. N Engl J Med. 2008;359:1786-1801. CAMMS223 Trial Investigators. N Engl J Med. 2008;359:1786-1801.

Alemtuzumab: Alemtuzumab: Effects on the Immune SystemEffects on the Immune System
► B cells returned to B cells returned to normal within 3-6 normal within 3-6 monthsmonths
► Median recovery time Median recovery time for CD4+ T cells > for CD4+ T cells > 100 cells/100 cells/µL = 3 µL = 3 monthsmonths
► 6-9 months for CD4+ 6-9 months for CD4+ T cells > 200 cells/T cells > 200 cells/µLµL
► Median recovery time Median recovery time to baseline levels of to baseline levels of CD4+ T cells = 61 CD4+ T cells = 61 monthsmonths
Thompson S, et al. Thompson S, et al. J Clin Immunol 2010;30:99–105. J Clin Immunol 2010;30:99–105. Coles A, et al. J Neurol. 2006;253:98-108.Coles A, et al. J Neurol. 2006;253:98-108.

CladribineCladribine
► Synthetic purine nucleoside analogue prodrugSynthetic purine nucleoside analogue prodrug► Accumulates and is incorporated into the DNA of lymphocytes as Accumulates and is incorporated into the DNA of lymphocytes as
a result of a high ratio of deoxycytidinekinaseto 5' nucleotidase a result of a high ratio of deoxycytidinekinaseto 5' nucleotidase activityactivity
► Selectively induces apoptosis in dividing and non-dividing Selectively induces apoptosis in dividing and non-dividing lymphocyteslymphocytes
► Sustained reduction in lymphocyte subtypes (CD4+ T cells, CD8+ Sustained reduction in lymphocyte subtypes (CD4+ T cells, CD8+ T cells and B cellsT cells and B cells
► Relatively transient effects on other immune cells such as Relatively transient effects on other immune cells such as neutrophils and monocytesneutrophils and monocytes
► Reduces levels of pro-inflammatory chemokinesReduces levels of pro-inflammatory chemokines► Crosses the blood brain barrier - CSF concentration = 25% of Crosses the blood brain barrier - CSF concentration = 25% of
plasma (patients with no BBB compromise)plasma (patients with no BBB compromise)► FDA-approved for hairy cell leukemiaFDA-approved for hairy cell leukemia
Carson et al. Blood 1983;62:737–43; 2Beutler et al. Proc Natl Acad Sci USA 1996;93:1716–20. Rice et al.Neurology 2000;54:1145–55. Szczucinski et al. Acta Neurol Scand 2007;115:137–46Bartosik-Psujek et al. Acta Neurol Scand 2004;109:390–2. Liliemark.ClinPharmacokinet1997;32:120–3.

Dosing: 4-5 day courses at month 1 and 2 (3.50 mg/kg) or months 1-4 (5.25 mg/kg) and 2 additional monthly courses beginning at week 48
1326 patients
Placebo (n = 437)
Cladribine 3.50 mg/kg total dose; 4 courses (n = 433)
Cladribine 5.25 mg/kg total dose; 6 courses (n = 456)
48 96 Time (weeks) 0 60 72 84362413
MRI
Neurological examination
–4
X X X X
X X X X
95 16
X X X X
X X
44 52
X X
X X
Giovannoni G, et al. N Engl J Med. 2010;362:416-426.

CLARITY: Clinical OutcomesCLARITY: Clinical Outcomes
* P < 0.001
0.33 (0.29-0.38)
0.14* (0.12-0.17)
0.15*(0.12-0.17)
57.6%
54.5%
An
nu
aliz
ed r
elap
se
rate
(9
5% C
I)
60.9
79.7*
78.9*
Odds Ratio (95% CI)2.43 (1.81-3.27)
Odds Ratio (95% CI)2.53 (1.87-3.43)
Per
cen
t o
f re
lap
se-f
ree
pa
tie
nts
at
98 w
eeks
Placebo (n = 437)
Cladribine 3.50 mg/kg (n = 433)
Cladribine 5.25 mg/kg (n = 456)
Giovannoni G, et al. N Engl J Med. 2010;362:416-426.

CLARITY: Clinical OutcomesCLARITY: Clinical Outcomes
Placebo 437 424 399 373 355 333 315 304 3043.50 mg 433 424 407 389 379 364 355 347 3475.25 mg 456 447 425 404 388 375 363 350 350
Placebo
Cladribine 3.50 mg/kg 0.67 (0.48-0.93); P = 0.02
Cladribine 5.25 mg/kg 0.69 (0.49-0.96); P = 0.03
0 12 24 36 48 60 72 84 96
0
5
10
15
20
25
HR vs Placebo (95% CI)
Weeks
Pro
po
rtio
n w
ith
co
nfi
rme
d 3
-mo
nth
E
DS
S p
rog
ress
ion
(%
)
Time to Confirmed EDSS Progression
Giovannoni G, et al. N Engl J Med. 2010;362:416-426.

CLARITY: MRI OutcomesCLARITY: MRI Outcomes
0.12 0.11
All P < 0.001
87.9%
me
an
± S
E l
es
ion
s/p
ati
en
t/s
ca
n
0.91
85.7%
T1 Gadolinium-T1 Gadolinium-Enhancing LesionsEnhancing Lesions Active T2-Weighted LesionsActive T2-Weighted Lesions
1.43
0.38 0.33
73.4%
76.9%
1.72
0.43 0.38
74.4%
77.9%Combined Unique LesionsCombined Unique Lesions
Placebo (n = 437)
Cladribine 3.50 mg/kg (n = 433)
Cladribine 5.25 mg/kg (n = 456)
Giovannoni G, et al. N Engl J Med. 2010;362:416-426.

CLARITY: Safety and TolerabilityCLARITY: Safety and Tolerability
Preferred term, n (%) patientsPreferred term, n (%) patients PlaceboPlacebo(n = 435)(n = 435)
CladribineCladribine3.5 mg/kg3.5 mg/kg(n = 430)(n = 430)
CladribineCladribine5.25 mg/kg5.25 mg/kg(n = 454)(n = 454)
CladribineCladribineoveralloverall
(n = 884)(n = 884)
Herpes zoster 0 8 (1.9) 11 (2.4) 19 (2.1)
Herpes zoster oticus 0 0 1 (0.2) 1 (0.1)
Varicella 1 (0.2) 1 (0.2) 1 (0.2) 2 (0.2)
Any infection or infestation 188 (42.5) 205 (47.7) 222 (48.9) 427 (48.3)
Deaths 2 (0.5) 2 (0.5) 2 (0.4) 4 (0.5)
► 20 patients had 21 zoster events in the cladribine groups20 patients had 21 zoster events in the cladribine groups► All 21 cases were self-limiting and dermatomal; no cases were disseminatedAll 21 cases were self-limiting and dermatomal; no cases were disseminated► 3.2% of patients developing grade 3 or 4 lymphopenia at any time during the study 3.2% of patients developing grade 3 or 4 lymphopenia at any time during the study
developed zoster versus 1.8% of those that did notdeveloped zoster versus 1.8% of those that did not► 70% of patients with zoster had normal lymphocyte count or lesser grade lymphopenia 70% of patients with zoster had normal lymphocyte count or lesser grade lymphopenia
at the approximate time zoster developedat the approximate time zoster developed► Deaths - Placebo: Hemorrhagic CVA, suicide; cladribine 3.5 mg/kg: acute MI, pancreatic Deaths - Placebo: Hemorrhagic CVA, suicide; cladribine 3.5 mg/kg: acute MI, pancreatic
carcinoma; cladribine 5.25 mg/kg: drowning, pancytopenia/pneumonia then cardio-carcinoma; cladribine 5.25 mg/kg: drowning, pancytopenia/pneumonia then cardio-respiratory arrestrespiratory arrest
Giovannoni G, et al. N Engl J Med. 2010;362:416-426.

CLARITY: Safety and TolerabilityCLARITY: Safety and Tolerability
Preferred term, n (%)Preferred term, n (%) PlaceboPlacebo(n = 435)(n = 435)
CladribineCladribine3.5 mg/kg3.5 mg/kg(n = 430)(n = 430)
CladribineCladribine5.25 mg/kg5.25 mg/kg(n = 454)(n = 454)
CladribineCladribineoveralloverall
(n = 884)(n = 884)
During StudyDuring Study
MelanomaMelanoma 00 1(0.2)1(0.2) 00 1(0.2)1(0.2)
OvarianOvarian 00 1(0.2)1(0.2) 00 1 (0.1)1 (0.1)
PancreaticPancreatic 00 1 (0.2)1 (0.2) 00 1 (0.1)1 (0.1)
CervixCervix 00 00 1(0.2)1(0.2) 1(0.2)1(0.2)
During post-study During post-study surveillancesurveillance
ChoriocarcinomaChoriocarcinoma 00 00 1(0.2)1(0.2) 1(0.2)1(0.2)
MalignanciesMalignancies
Giovannoni G, et al. N Engl J Med. 2010;362:416-426.

CLARITY: Effects on Lymphocyte SubsetsCLARITY: Effects on Lymphocyte Subsets
Maximum Effects on CD4 and CD 19 Counts*Maximum Effects on CD4 and CD 19 Counts*
Weeks 0-48 Weeks 48-96Weeks 0-48 Weeks 48-96
3.5 5.25 3.5 5.253.5 5.25 3.5 5.25
mg/kg mg/kg mg/kg mg/kgmg/kg mg/kg mg/kg mg/kg
CD4 (week)CD4 (week)
Cells/µLCells/µL
CD19 (week)CD19 (week)
Cells/µLCells/µL
1616
391391
99
1818
1616
209209
1616
1414
7272
275275
5252
2727
7272
207207
5252
3131Add Reference
*Median values
Rieckmann P, et al. Presented at ECTRIMS, Düsseldorf, Germany, September 9-12, 2009. Poster #816.

Fingolimod (FTY720) Fingolimod (FTY720)
1. Brown B, et al. Ann Pharmacother. 2007;41:1660-1668. 2. Kappos L, et al. N Engl J Med. 2006;355:1124-1140. 3. Mullershausen F, et al. Presented at: ECTRIMS; October 11-14, 2007; Prague, Czech Republic. 4. Miron VE, et al. Presented at: ECTRIMS; October 11-14, 2007; Prague, Czech Republic. 5. Barske C, et al. Presented at: ECTRIMS; October 11-14, 2007; Prague, Czech Republic.
► Sphingosine-1-phosphate (S1P) receptor Sphingosine-1-phosphate (S1P) receptor modulatormodulator
► Sequesters circulating lymphocytes into Sequesters circulating lymphocytes into secondary lymphoid organssecondary lymphoid organs
● Peripheral reduction of CD3+, CD4+, CD8+, CD45RA+ Peripheral reduction of CD3+, CD4+, CD8+, CD45RA+ (naive T cells), CD45RO+ (memory T cells) and CD19+ cells(naive T cells), CD45RO+ (memory T cells) and CD19+ cells
● No effect on lymphocyte induction, proliferation, No effect on lymphocyte induction, proliferation, or memory functionor memory function
► May inhibit the production of IL-17May inhibit the production of IL-17► S1P receptors located within the CNSS1P receptors located within the CNS
● Fingolimod or deletion of S1P1 from neural cells reduces Fingolimod or deletion of S1P1 from neural cells reduces astrogliosis in EAEastrogliosis in EAE

1272 patients(1:1:1)
Clinic visits
Oral fingolimod 0.50 mg once daily (n = 425)
MRI
Oral fingolimod 1.25 mg once daily (n = 429)
Placebo once daily (n = 418)
Randomization Month 6 Month 12 Month 24
Kappos L, et al. N Engl J Med. 2010;362:387-401.

FREEDOMS: Primary Efficacy FREEDOMS: Primary Efficacy EndpointEndpoint
Annualized Relapse Rate at 24 monthsAnnualized Relapse Rate at 24 months
PlaceboPlacebo(n = 431)(n = 431)
FingolimodFingolimod0.5 mg0.5 mg
(n = 429)(n = 429)
FingolimodFingolimod1.25 mg1.25 mg(n = 420)(n = 420)
-54% vs Placebop < 0.001
-60% vs Placebop < 0.001
Kappos L, et al. N Engl J Med. 2010;362:387-401.

FREEDOMS: Disability DataFREEDOMS: Disability Data
Number at RiskFTY720 1.25 mg 429 401 373 356 344 332 322 305 165FTY720 0.50 mg 425 416 388 370 354 340 332 321 152Placebo 418 391 371 341 320 308 290 279 143
FTY720 1.25 mg (17%)†
Days on studyDays on study
90 180 270 360 450 540 630 720
5
10
15
20
25
30
Placebo (24%)
FTY720 0.50 mg (18%)*
Per
cen
t w
ith
3-m
on
th c
on
firm
ed
Per
cen
t w
ith
3-m
on
th c
on
firm
ed
ED
SS
pro
gre
ssio
nE
DS
S p
rog
ress
ion
FTY720 0.50 mg vs placebo HR 0.70P = 0.02 in time to disability Progression
FTY720 1.25 mg vs placebo HR 0.68P = 0.02 in time to disability Progression
* P = 0.03 vs placebo† P = 0.01 vs placebo
Kappos L, et al. N Engl J Med. 2010;362:387-401.
0

FREEDOMS: MRI EndpointsFREEDOMS: MRI Endpoints
T2 and Gadolinium-Enhancing Lesions at 24 MonthsT2 and Gadolinium-Enhancing Lesions at 24 Months
-82% P<0.001-74% P<0.001
Kappos L, et al. N Engl J Med. 2010;362:387-401.Kappos L, et al. N Engl J Med. 2010;362:387-401.

FREEDOMS: Brain VolumeFREEDOMS: Brain Volume
P≤0.03 for both doses of fingolimodvs. placebo at all time points
Kappos L, et al. N Engl J Med. 2010;362:387-401.Kappos L, et al. N Engl J Med. 2010;362:387-401.

Randomization Month 6 Month 12 Ongoing
Oral fingolimod 0.5 mg once daily and matchingweekly placebo injection IM
Optional extensionphase
Oral fingolimod 1.25 mg once daily and matchingweekly placebo injection IM
IFNβ-1a 30 µg IM once weekly andmatching daily oral placebo capsule Assessments
MRI
EDSS
Clinical visit
Cohen J, et al. N Engl J Med. 2010;362:412-415.

TRANSFORMS: TRANSFORMS: Primary Efficacy EndpointPrimary Efficacy Endpoint
Annualized Relapse Rate at 12 monthsAnnualized Relapse Rate at 12 months
IFNIFNββ-1a 30 µg IM-1a 30 µg IMonce weeklyonce weekly
(n = 431)(n = 431)
Oral fingolimodOral fingolimod0.5 mg0.5 mg
(n = 429)(n = 429)
Oral fingolimodOral fingolimod1.25 mg1.25 mg(n = 420)(n = 420)
-52% vs IFNβ-1a,p < 0.001
-38% vs IFNβ-1a,p < 0.001
Cohen J, et al. N Engl J Med. 2010;362:412-415.

TRANSFORMS: MRI EndpointsTRANSFORMS: MRI Endpoints
T2 and Gadolinium-Enhancing Lesions at 12 MonthsT2 and Gadolinium-Enhancing Lesions at 12 Months
Cohen J, et al. N Engl J Med. 2010;362:412-415.Cohen J, et al. N Engl J Med. 2010;362:412-415.
-42% vs. IFNß-1aP<0.001
-35% vs. IFNß-1aP=0.004
-55% vs. IFNß-1aP<0.001
-73% vs.IFNß-1a P<0.001

TRANSFORMS: Brain VolumeTRANSFORMS: Brain Volume
P < 0.001
Cohen J, et al. N Engl J Med. 2010;362:412-415.

Fingolimod: SafetyFingolimod: Safety
► Transient reduction in heart rate on initiation of Transient reduction in heart rate on initiation of treatmenttreatment
► Elevated blood pressureElevated blood pressure● ↑↑mean systolic BP (mean systolic BP (1.9 and 3.6 mm Hg for 0.5 1.9 and 3.6 mm Hg for 0.5
mg and 1.25 mg, respectively) and diastolic BP mg and 1.25 mg, respectively) and diastolic BP (0.7 and 2.1 mm HG for 0.5 and 1.25 mg, (0.7 and 2.1 mm HG for 0.5 and 1.25 mg, respectively)respectively)
► Elevated liver enzymesElevated liver enzymes● ↑↑LFTs ≥ 3 x ULN 8% for FTY720 0.5 mg, 10% for LFTs ≥ 3 x ULN 8% for FTY720 0.5 mg, 10% for
FTY720 1.25 mg, 1.2% for placebo, 2% for IFNß-FTY720 1.25 mg, 1.2% for placebo, 2% for IFNß-1a1a
► Macular edemaMacular edema● FREEDOMS - 7 cases in the 1.25 mg dose group FREEDOMS - 7 cases in the 1.25 mg dose group
(1.6%) and none in the 0.5 mg dose group(1.6%) and none in the 0.5 mg dose group● TRANSFORMS – 6 cases (4 in the 1.25 mg dose TRANSFORMS – 6 cases (4 in the 1.25 mg dose
group (1%) and 2 in the 0.5 mg dose group group (1%) and 2 in the 0.5 mg dose group (0.5%))(0.5%))
Kappos L, et al. N Engl J Med. 2010;362:387-401. Cohen J, et al. N Engl J Med. 2010;362:412-415.

Fingolimod: SafetyFingolimod: Safety
AE, n (%)AE, n (%)
FTY720 FTY720 0.5 mg 0.5 mg (n = 854)(n = 854)
FTY720FTY7201.25 mg1.25 mg(n = 849)(n = 849)
PlaceboPlacebo(n = 418)(n = 418)
IFNIFNß-1aß-1a(n = 431)(n = 431)
Skin Cancers
Basal cell carcinoma 7(0.8)7(0.8) 3(0.4)3(0.4) 3(0.7)3(0.7) 1(0.2)1(0.2)
Melanoma 3(0.4)3(0.4) 1(0.1)1(0.1) 1(0.2)1(0.2) 00
Bowen’s Disease 1 (0.1)1 (0.1) 00 00 00
Infections
Herpes infections 46(5.4)46(5.4) 48(5.7)48(5.7) 33(7.9)33(7.9) 12(2.8)12(2.8)
Malignancies and Herpes InfectionsMalignancies and Herpes Infections
Kappos L, et al. N Engl J Med. 2010;362:387-401. Cohen J, et al. N Engl J Med. 2010;362:412-415.

Fingolimod: SafetyFingolimod: Safety
► Two fatal infections in patients treated Two fatal infections in patients treated with FTY720 1.25 mg with FTY720 1.25 mg ● Herpes encephalitis Herpes encephalitis ● primary disseminated varicellaprimary disseminated varicella
► Hemorrhagic encephalitis in a patient Hemorrhagic encephalitis in a patient treated with FTY720 1.25 mgtreated with FTY720 1.25 mg
► Posterior reversible encephalopathy Posterior reversible encephalopathy syndrome in a patient treated with 5 mg syndrome in a patient treated with 5 mg in the phase 2 studyin the phase 2 study
Cohen J, et al. N Engl J Med. 2010;362:412-415; Kappos L et al. Cohen J, et al. N Engl J Med. 2010;362:412-415; Kappos L et al. N Engl J Med. 2006;355:1124-40; N Engl J Med. 2006;355:1124-40; Leypoldt F, et al. LK. Neurology 2009;72:1022-24. Leypoldt F, et al. LK. Neurology 2009;72:1022-24.

Normal range Normal range
Treatment duration (yrs), Treatment duration (yrs), mean mean ± SEM± SEM 1.9 1.9 ± 0.2± 0.2 --
Lymphocyte count (x 10Lymphocyte count (x 1099/L), /L), mean mean ± SEM± SEM 0.4 0.4 ± 0.1± 0.1 0.9-3.30.9-3.3
CD4 T cell count (cells/CD4 T cell count (cells/µL), µL), mean ± SEMmean ± SEM 78 78 ± 5.6± 5.6 700-1100700-1100
CD8 T cell count (cells/CD8 T cell count (cells/µL), µL), mean ± SEMmean ± SEM 149 149 ± 7.4± 7.4 500-900500-900
FTY720 1.25 mg (n = 16)FTY720 1.25 mg (n = 16)
Mehling M, et al. Neurology 2008;71:1261–1267

[PD5.006] Prolonged Reduction in Circulating [PD5.006] Prolonged Reduction in Circulating Lymphocytes after Discontinuation of FTY720 Lymphocytes after Discontinuation of FTY720 (Fingolimod): Possible Relationship to Duration of (Fingolimod): Possible Relationship to Duration of TherapyTherapy
Mark R. Keezer, Yves Lapierre, Igor Shames, David Mark R. Keezer, Yves Lapierre, Igor Shames, David Haegert, Amit Bar-Or, Jack Antel, Montreal, QC, Haegert, Amit Bar-Or, Jack Antel, Montreal, QC, Canada Canada
CONCLUSIONS/RELEVANCE: CONCLUSIONS/RELEVANCE: Peripheral lymphocyte Peripheral lymphocyte counts remained depressed beyond the currently counts remained depressed beyond the currently expected time period in 2 patients following cessation expected time period in 2 patients following cessation of long-term FTY720 therapy. Regional lymph node of long-term FTY720 therapy. Regional lymph node architecture was preserved in the one available architecture was preserved in the one available patient. Exploration of larger datasets will determine patient. Exploration of larger datasets will determine the true incidence of prolonged lymphopenia and the true incidence of prolonged lymphopenia and whether time to recovery of circulating lymphocytes whether time to recovery of circulating lymphocytes may provide a potential biomarker for guiding may provide a potential biomarker for guiding continued therapy. continued therapy. Category - MS and Related Diseases - Clinical ScienceCategory - MS and Related Diseases - Clinical Science
Presented at the AAN Annual Meeting 2010Presented at the AAN Annual Meeting 2010. .

Emerging Therapies:Emerging Therapies:Trading Efficacy for SafetyTrading Efficacy for Safety
► ? Impaired ? Impaired immune immune surveillance and surveillance and opportunistic opportunistic infectionsinfections
► Viral and other Viral and other infectionsinfections
► ? Malignancies? Malignancies► Long-lasting Long-lasting
effectseffects
► AutoimmunityAutoimmunity► TeratogenicityTeratogenicity► Rare, but serious Rare, but serious
infusion reactionsinfusion reactions► The UnknownThe Unknown

Natalizumab and the Risk of PMLNatalizumab and the Risk of PML

► Humanized monoclonal antibody directed against Humanized monoclonal antibody directed against CD11a affecting T-lymphocyte activation, CD11a affecting T-lymphocyte activation, migration, and reactivationmigration, and reactivation
► Evaluated in 4 randomized, double-blind, placebo-Evaluated in 4 randomized, double-blind, placebo-controlled trialscontrolled trials
► FDA-approved for psoriasis in 2003FDA-approved for psoriasis in 2003● At the time of approval, 2764 patients had been At the time of approval, 2764 patients had been
treatedtreated● 218 treated for 218 treated for ≥ 1 year≥ 1 year
Nijsten T, et al. Arch Dermatol 2009;145:1037-39.Nijsten T, et al. Arch Dermatol 2009;145:1037-39.

► October 2008: Label update to include PMLOctober 2008: Label update to include PML► February 2009: February 2009:
• FDA issued a Public Health Advisory and changed the label FDA issued a Public Health Advisory and changed the label to include a “black box” warning for PMLto include a “black box” warning for PML
– At the time, 48,000 patients treated with efalizumab, but At the time, 48,000 patients treated with efalizumab, but only 14,000 for > 1 year, 5,100 for > 2 years, and 1,900 for only 14,000 for > 1 year, 5,100 for > 2 years, and 1,900 for > 3 years> 3 years
• EMEA recommends suspension of marketingEMEA recommends suspension of marketing• Health Canada suspends marketingHealth Canada suspends marketing
► April 2009: April 2009: Genentech announced plans for a Genentech announced plans for a voluntary withdrawal from the U.S. market voluntary withdrawal from the U.S. market
Nijsten T, et al. Arch Dermatol 2009;145:1037-39.

Meaningful impactMeaningful impact
Disease CourseDisease Course
MRIMRI
? Better than ABCR? Better than ABCR
? Window of opportunity? Window of opportunity
ConvenienceConvenience
Benefits RisksBenefits Risks
Treatment Decisions: Treatment Decisions: Considering Benefits and RisksConsidering Benefits and Risks
Short-term safetyShort-term safety
Long-term safetyLong-term safety
PharmacovigilancePharmacovigilance
Post-approval studiesPost-approval studies
Pregnancy issuesPregnancy issues

The Long Haul: Optimizing Long-Term The Long Haul: Optimizing Long-Term Functional Status and Financial Functional Status and Financial
Outcomes in RRMS with Outcomes in RRMS with Immunomodulation TherapyImmunomodulation Therapy
What Do The Trials Teach Us?What Do The Trials Teach Us?
New Frontiers New Frontiers in in NeurotherapyNeurotherapy
Guy J. Buckle, MD, MPHGuy J. Buckle, MD, MPHDirector of MS Clinical Care Partners Multiple Sclerosis CenterDirector of MS Clinical Care Partners Multiple Sclerosis Center
Brigham and Women’s HospitalBrigham and Women’s HospitalAssistant Professor of NeurologyAssistant Professor of Neurology
Harvard Medical SchoolHarvard Medical SchoolBoston, MassachusettsBoston, Massachusetts

CNS = central nervous system.CNS = central nervous system.Compston A, et al. Compston A, et al. LancetLancet. 2002;359(9313):1221-1231. Frohman EM. . 2002;359(9313):1221-1231. Frohman EM. Med Clin N AmMed Clin N Am. 2003;87(4): . 2003;87(4): 867-897. Hogancamp WE, et al. 867-897. Hogancamp WE, et al. Mayo Clin Proc.Mayo Clin Proc. 1997;72(9):871-878. National Multiple Sclerosis Society. 1997;72(9):871-878. National Multiple Sclerosis Society. Who gets MS? http://www.nationalmssociety.org/about-multiple-sclerosis/who-gets-ms/index.aspx. Accessed Who gets MS? http://www.nationalmssociety.org/about-multiple-sclerosis/who-gets-ms/index.aspx. Accessed
January 8, 2009. January 8, 2009. Lage MJ, et al. Lage MJ, et al. WorkWork. 2006;27(2):143-151. 2006;27(2):143-151.
Epidemiology of MSEpidemiology of MS
► The most common chronic disease affecting the CNS in The most common chronic disease affecting the CNS in young adults young adults
► Approximately 400,000 cases in the United StatesApproximately 400,000 cases in the United States● Estimates range from 250,000 to 500,000Estimates range from 250,000 to 500,000
► The chances of developing MS are 1:1000 in the general The chances of developing MS are 1:1000 in the general populationpopulation
► Estimated 2.5 million cases worldwideEstimated 2.5 million cases worldwide
► Highest incidence in Caucasians Highest incidence in Caucasians
► Higher incidence in women (approximately 3:1)Higher incidence in women (approximately 3:1)
► MS strikes individuals between the ages 20-50, normally a MS strikes individuals between the ages 20-50, normally a time of peak productivitytime of peak productivity

Cardoso E, et al. Cardoso E, et al. Arq NeuropsiquiatrArq Neuropsiquiatr. 2006;64(3-B):727-730.. 2006;64(3-B):727-730.
Potential Triggers for MSPotential Triggers for MS
EnvironmentalFactors
InfectiousAgent
Genetic Predisposition
MSMSAbnormal Immunologic Response

National Multiple Sclerosis Society. http://www.nationalmssociety.org/about-multiple-sclerosis/what-we-know-about-ms/symptoms/index.aspx. Accessed February 21, 2010.
Clinical ManifestationsClinical Manifestations
► FatigueFatigue
► PainPain
► DepressionDepression
► Numbness/Numbness/paresthesiasparesthesias
► Cognitive dysfunctionCognitive dysfunction
► WeaknessWeakness
► SpasticitySpasticity
► Optic neuritisOptic neuritis
► Bladder dysfunctionBladder dysfunction
► Bowel dysfunctionBowel dysfunction
► Cerebellar Cerebellar dysfunctiondysfunction
► Sexual dysfunctionSexual dysfunction
► Gait abnormalitiesGait abnormalities
► Partial/complete Partial/complete paralysisparalysis

Age of Onset of MSAge of Onset of MS
Cardoso E, et al. Arq Neuropsiquiatr. 2006;64(3-B):727-730.
0
5
10
15
20
25
30
35
0-10 11-20 21-30 31-40 41-50 51-60
YearsYears
Pati
ents
(%
)Pati
ents
(%
)
Distribution of Patients According toDistribution of Patients According tothe Decade of Life of MS Symptoms Onsetthe Decade of Life of MS Symptoms Onset

EDSS = Expanded Disability Status Scale. Kurtzke JF. Neurology. 1983;33:1444-1452.
Progression of Disability: EDSSProgression of Disability: EDSS
8.0–8.5 = Confined to bed or chair8.0–8.5 = Confined to bed or chair
7.0–7.5 = Confined to wheelchair7.0–7.5 = Confined to wheelchair
6.0–6.5 = Walking assistance is needed6.0–6.5 = Walking assistance is needed
5.0–5.5 = Increasing limitation in ability to walk5.0–5.5 = Increasing limitation in ability to walk
4.0–4.5 = Disability is moderate4.0–4.5 = Disability is moderate
3.0–3.5 = Disability is mild to moderate3.0–3.5 = Disability is mild to moderate
2.0–2.5 = Disability is minimal2.0–2.5 = Disability is minimal
1.0–1.5 = No disability1.0–1.5 = No disability
0 = Normal neurologic exam0 = Normal neurologic exam
Increasing disease burden
10.0 = Death due to MS
9.0–9.5 = Completely dependent

Natural History of MS and Cost of Natural History of MS and Cost of MSMS
*Curve is based on an estimation of the decrease in cost for early treatment of about 40% at each range of EDSS
Burks J. J Manag Care Med. 2008;12(1):26-31. [Exhibit 8].Comi G. Neurol Sci. 2006;27:S8-S12.Kobelt G, et al. Neurology. 2006;66(11):1696-1702.
$0
$10,000
$20,000
$30,000
$40,000
$50,000
$60,000
$70,000
Severe EDSS > 6Moderate EDSS 4-6Mild EDSS < 4
CIS RRMS SPMSPre-clinical
Predicted Cost
Early Intervention*
MRI lesion activity
Clinical Threshold
Atrophy and Axonal Degradation
US
$ pe
r Y
ear
US
$ pe
r Y
ear

Weinshenker BG, et al. Weinshenker BG, et al. BrainBrain. 1989;112:1419-1428.. 1989;112:1419-1428.
Early RelapsesEarly RelapsesAffect Long-term DisabilityAffect Long-term Disability
Time from Onset of MS (years)
Low (0-1 attacks in 2 years)Intermediate (2-4 attacks in 2 years)High (≥5 in 2 years)
Pat
ient
s (%
)
5040302010
20
00
40
60
80
100
Actuarial analysis of disabilityActuarial analysis of disability——percentage of patients not having reached EDSS 6percentage of patients not having reached EDSS 6::difference between the groups is significant (difference between the groups is significant (P P < .0001). < .0001).

*In 224 placebo patients from the NMSS task force on clinical outcome assessment. EDSS = Expanded Disability Status Scale; NMSS = National Multiple Sclerosis Society.Lublin FD, et al. Neurology. 2003;61:1528-1532.
Relapses Can Result inRelapses Can Result inResidual Long-Term DisabilityResidual Long-Term Disability
Net Change in EDSS Score from before a Relapse to after a Relapse*Net Change in EDSS Score from before a Relapse to after a Relapse*
42% of patients had a residual deficit ≥0.5 point% of patients had a residual deficit ≥0.5 point28% had a residual deficit ≥1.0 point28% had a residual deficit ≥1.0 point
42.4% increase 0.5 or more
28.1% increase 1 or more
Nu
mb
er o
f S
ub
ject
s
1 37 4
8
20
86
32 33
148 5
1 20
20
40
60
80
100
-3.5 -2.5 -2.0 -1.5 -1.0 -0.5 0.0 0.5 1.0 1.5 2.0 2.5 3.5 4.0

Long-term Study Design in RRMSLong-term Study Design in RRMS
Copaxone® (glatiramer acetate injection)20,21
N=251 in original pivotal trial; 19 placebo patients of 251 in pivotal trial did not enter open-label extension, and 1 patient received 1 dose of COPAXONE® and never returned for evaluation. Therefore, 231 patients were included in the mITT analysis. The Ongoing cohort included 108 patients at 10 years and 100 patients at 15 years.
Avonex® (IFNβ-1a)9,23
Avonex®: N=301; 158 Avonex®, 143 placebo; subset (85 Avonex®, 87 placebo) followed for 2 years. 15-year retrospective follow-up: n=116; 15-year follow-up consisted of a questionnaire at year 15.
Betaseron® (IFNβ-1b)24,25
Betaseron®: N=372; 125 Betaseron® 1.6 MIU, 124 Betaseron® 8 MIU, 123 placebo.
16-year retrospective follow-up: n=328 identified patients (35 of these were deceased but included in the study as identified patients). LTFU data were obtained in an observational study consisting of a single-visit assessment or report at 16 years. At LTFU, 182/260 patients were not taking Betaseron®.
Rebif® (IFNβ-1a)26
N=560; 184 Rebif® 44 mcg, 189 Rebif® 22 mcg, 187 placebo; at end of year 2, 172 placebo patients randomized to 22 mcg (n=84) or 44 mcg (n=87); and double-blind study was continued to year 4.
LTFU data were obtained in an observational study consisting of a single-visit assessment 7-8 years after enrollment.
Tysabri® (natalizumab)27
N=942; Tysabri® 300 mg (n=627) or placebo (n=315).
Up to 15 years
2 yrs
15 years
5 yrs
16years
4 yrs
7-8 years
3yrs Key
Prospective study design
Retrospective follow-up
9.9. Jacobs LDJacobs LD, et al., et al. Ann Neurol. Ann Neurol. 1996;39:285-294. 1996;39:285-294. 20.20. Ford C, et al. WCTRIMS 2008. Abstract P44. Ford C, et al. WCTRIMS 2008. Abstract P44. 21.21. Ford CC, et al. Ford CC, et al. Mult Scler. Mult Scler. 2006;12:309-320. 2006;12:309-320. 23. 23. Bermel RA, et al. WCTRIMS 2008.Bermel RA, et al. WCTRIMS 2008. Abstract P14.Abstract P14. 24. 24. IFNIFNββ Study Group. Study Group. Neurology. Neurology. 1995;45:1277-1285. 1995;45:1277-1285. 25. 25. Ebers G, et al. AAN 2006. Ebers G, et al. AAN 2006. P01.079. P01.079. 26. 26. Kappos L, et al. Kappos L, et al. Neurology. Neurology. 2006;67:944-953. 2006;67:944-953. 27.27. O’Connor PW, et al. AAN 2007. O’Connor PW, et al. AAN 2007. P06.082.P06.082.

Ryan M, et al. J Manag Care Pharm. 2009;15(1)(Suppl S-b):S1-S17.
Data SupportingData SupportingLong-Term Use of DMTLong-Term Use of DMT
Disease Disease Duration Duration (Years)(Years)
Percentage Percentage Reaching Reaching EDSS 4EDSS 4
Percentage Percentage Reaching Reaching EDSS 6EDSS 6
GA 15-year LTFUGA 15-year LTFU >18.5>18.5 38%38% 18%18%
High-dose IFN-1aPRISMS 8
~13 26.8%26.8% 20%20%
IFN-1b 16 Year(> 80)
~20 Not reportedNot reported ~45%
Low-dose IFN-1a15-year 14.314.3 64%64% 32%32%

Scope of QoLScope of QoL
► Three important domains in lifeThree important domains in life● Physical functioningPhysical functioning● Psychosocial functioningPsychosocial functioning● Symptom-related phenomenonSymptom-related phenomenon

The Two Faces of Multiple SclerosisThe Two Faces of Multiple Sclerosis
MSRelapse
ProgressionMRI
SymptomsMobility
EmploymentDepression
FatigueCognition

HRQOL = Health-related quality of life. Petajan JH, et al. Ann Neurol. 1996;39(4):432-441. Motl R,W et al. Psychol Health Med. 2009;14(1)111-124.
Mobility and HRQOLMobility and HRQOL
► Improvement in strength and mobility Improvement in strength and mobility can lead to improved social interaction can lead to improved social interaction and emotional behaviorand emotional behavior
► Improved fitness in MS is associated Improved fitness in MS is associated with improved HRQOLwith improved HRQOL
► Physical activity is indirectly associated Physical activity is indirectly associated with improved depression, fatigue, pain, with improved depression, fatigue, pain, in individuals with MSin individuals with MS

Heesen C, et al. Mult Scler. 2008;14(7):988-991.
Multiple SclerosisMultiple Sclerosis
35
40
30
20
10
0
5
Walking
Power and Coordination of H
ands
Normal S
kin Sensations
Lack of Pain
Bladder Contro
l
Bowel Contro
l
Visual Function
Awakefulness and Alertness
Thinking and Memory
Firs
t R
ank
(%)
Firs
t R
ank
(%)
Speech
SwallowingMood
sexuality
25
15
MS >15 YearsMS <5 Years

Walking Impairment and Walking Impairment and Quality of LifeQuality of Life
► 64% of patients report difficulty walking64% of patients report difficulty walking► Impairment worsens with increasing EDSS severityImpairment worsens with increasing EDSS severity
Per
cent
Am
ong
Pat
ient
s w
ho
Per
cent
Am
ong
Pat
ient
s w
ho
Rep
orte
d W
alki
ng I
mpa
irmen
tR
epor
ted
Wal
king
Im
pairm
ent
Johanesson et al. J Neurol. 2007;254:767-773

Trends Across MS Clinical TrialsTrends Across MS Clinical TrialsAnnualized Relapse Rate (ARR)Annualized Relapse Rate (ARR)
Johnson1995
Polman2006
REGARD2007
BECOME2007
KapposTRANSFORMS
Jacobs1996
IFNββ-1b study
group,1993
PRISMS-21998
BEYOND2007
CAMMS2232008
3 years
HERMES2008
48 weeks
FORTE20081 year
CLARITY2009

Cost of MS RelapseCost of MS Relapse
► Reducing relapses is key to reducing costsReducing relapses is key to reducing costs• The number of relapses is a significant The number of relapses is a significant
predictor of total costpredictor of total cost► Cost of treating a relapse is difficult to Cost of treating a relapse is difficult to
calculatecalculate• Includes initial care, acute treatment costs, Includes initial care, acute treatment costs,
post-discharge services, daily cost of post-discharge services, daily cost of outpatient medicationsoutpatient medications
► In one study, using 2002 dollars, costs ranged In one study, using 2002 dollars, costs ranged from $243 to $12,870, depending on level of from $243 to $12,870, depending on level of management neededmanagement needed
► Cost estimates do not differentiate between Cost estimates do not differentiate between the different forms of MSthe different forms of MSMorrow TJ. J Neurol Sci. 2007;256(supp 1):S39-S44.
Grudzinski AN, et al. J Manag Care Pharm. 2000;6:19-24.O’Brien JA, et al. BMC Health Serv Res. 2003;3:17-29.

Medical Costs Per RelapseMedical Costs Per Relapse
ED = emergency department; IV = intravenous.O’Brien J, et al. BMC Health Serv Res. 2003;3(1):17-28.
TherapistsTherapistsConsultsConsults
Follow-Up Office VisitsFollow-Up Office VisitsSymptom-Related MedicationsSymptom-Related MedicationsFollow-Up Office VisitsFollow-Up Office Visits
Hospital readmissionsHospital readmissions
Nursing homeNursing home
Skilled nursingSkilled nursing
Home healthcareHome healthcare
RehabilitationRehabilitation
Outpatient follow-upOutpatient follow-upHome administrationHome administration
Post Discharge ServicesPost Discharge ServicesHospital day caseHospital day case
Hospital AdmissionHospital AdmissionIV MethylprednisoloneIV MethylprednisoloneSymptom-Related MedicationsSymptom-Related MedicationsEDEDEDED
Usual care physicianUsual care physicianUsual care physicianUsual care physicianUsual care physicianUsual care physician
Initial ContactInitial ContactInitial ContactInitial ContactInitial ContactInitial ContactHigh-Intensity EpisodeHigh-Intensity EpisodeModerate-Intensity EpisodeModerate-Intensity EpisodeLow-Intensity EpisodeLow-Intensity Episode
$12,870$1847$243

Whetton-Goldstein K, et al. Mult Scler. 1998;4(5):419-425. Pope GC, et al. Neurology. 2002;58(1):37-43. Kobelt G, et al. Neurology. 2006;66(11):1696-1702. Patwardhan MB, et al. Mult Scler. 2005;11(2):232-239. O’Brien JA, et al. J Neurosurg Psychiatry. 2006;77:918-926.
Economic ImplicationsEconomic Implications
► Annual cost of MS in the United States is estimated at Annual cost of MS in the United States is estimated at approximately $13.6 billion (in 1994 dollars)approximately $13.6 billion (in 1994 dollars)
► Total lifetime direct and indirect costs per patient are Total lifetime direct and indirect costs per patient are estimated at approximately $2.4 million (in 1994 dollars)estimated at approximately $2.4 million (in 1994 dollars)
► Mean annual direct and indirect costs per patient total Mean annual direct and indirect costs per patient total an estimated $47,215 (in 2004 dollars)an estimated $47,215 (in 2004 dollars)
► Mean direct healthcare costs incurred by insured Mean direct healthcare costs incurred by insured patients with MS are 2 to 3 times higher than those patients with MS are 2 to 3 times higher than those without MSwithout MS
► Direct correlation between cost (direct and indirect) and Direct correlation between cost (direct and indirect) and severity of disease has been well-establishedseverity of disease has been well-established
► Therapeutics that modify MS activity and severity can Therapeutics that modify MS activity and severity can result in both clinical and economic benefitsresult in both clinical and economic benefits

DMT = disease-modifying therapy.Kobelt G, et al. Neurology. 2006;66(11):1696-1702.
MS Cost DriversMS Cost Drivers
Sick Leave/Reduced Working Time (10%)
Early Retirement (34%)
Hospital Inpatient Care (3%)
Ambulatory Care (4%)
Tests (2%)
Other Drugs (6%)
Services (2%)
Adaptations (5%)
DMTs (22%)
Informal Care (12%)

DMTs = disease-modifying therapies.Kobelt G, et al. Neurology. 2006;66(11):1696-1702.
Costs of MS by Disease SeverityCosts of MS by Disease Severity
70,000
60,000
50,000
40,000
30,000
20,000
0
10,000
Mild EDSSMild EDSS<4.0<4.0
Moderate EDSSModerate EDSS4.0-6.04.0-6.0
Severe EDSSSevere EDSS>6.0>6.0
AllAllPatientsPatients
Indirect Costs
Direct Costs
Informal Care
Other Drugs
DMTs
Cos
t ($)
Cos
t ($)

Cost of CareCost of Care
Cost and functionalityCost and functionality
Adapted from: Kobelt G, Berg J, Atherly D et al. Neurology. 2006; 66:1696–1702.Adapted from: Kobelt G, Berg J, Atherly D et al. Neurology. 2006; 66:1696–1702.
* 2004 US Dollars Non-Drug Costs
EDSS ScoreEDSS Score
Approximate Mean Annual Cost*Approximate Mean Annual Cost*
MedicalMedicalUnpaid Unpaid
CaregiveCaregiver Timer Time
Lost Lost Work Work TimeTime
TotalTotal
MildMildEDSS 0 - 3.5EDSS 0 - 3.5
$3,106$3,106 $932$932 $9,938$9,938 $13,976$13,976
ModerateModerateEDSS 4.0 - 6.0EDSS 4.0 - 6.0
$5,100$5,100 $3,188$3,188 $22,950$22,950 $31,238$31,238
SevereSevereEDSS 6.5 - 9.5EDSS 6.5 - 9.5
$12,524$12,524 $12,524$12,524 $21,291$21,291 $46,339$46,339

AWP = average wholesale price.Prescott JD, et al. J Manag Care Pharm. 2007;13(1):44-52. CuraScript 2008 Specialty Drug Trend Report. April 2009. Red Book Update. Vol. 30(1). January 2010.
DMT-Associated CostsDMT-Associated Costs
► Approximately 65% of annual direct per patient Approximately 65% of annual direct per patient healthcare costs in MS are attributable to drug therapyhealthcare costs in MS are attributable to drug therapy
► MS drugs represent 20.2% of specialty drug MS drugs represent 20.2% of specialty drug expenditures within managed care plansexpenditures within managed care plans
► National trend in MS drug expenditures was +18.3% in National trend in MS drug expenditures was +18.3% in 20082008
● 23.5% increase in manufacturer pricing was primary driver 23.5% increase in manufacturer pricing was primary driver of trendof trend
► Comparative AWPs of DMT options:Comparative AWPs of DMT options:AgentAgent DosageDosage AWP/dayAWP/day AWP/yearAWP/year
Interferon beta-1bInterferon beta-1b 0.25 mg SC every other 0.25 mg SC every other dayday $105.41$105.41 $38,475$38,475
Interferon betaInterferon beta-1-1a IMa IM 30 mcg IM once weekly30 mcg IM once weekly $98.66$98.66 $36,010$36,010
Interferon betaInterferon beta-1-1a SCa SC 44 mcg SC 3 times 44 mcg SC 3 times weeklyweekly $106.20$106.20 $38,761$38,761
Glatiramer acetate Glatiramer acetate 20 mg SC daily20 mg SC daily $110.10$110.10 $40,187$40,187

National Clinical Advisory Board of the National MS Society. MS Disease Management Consensus Statement. 2007. http://www.nationalmssociety.org. Accessed February 10, 2010.
MS Consensus GuidelinesMS Consensus Guidelines
► National MS Society Expert Consensus Statement National MS Society Expert Consensus Statement (2007):(2007):
● Initiate therapy as soon as possible following diagnosis of Initiate therapy as soon as possible following diagnosis of active-relapsing disease with an interferon beta agent or active-relapsing disease with an interferon beta agent or glatiramer acetateglatiramer acetate
● Drug therapy should also be considered in patients with Drug therapy should also be considered in patients with first attack at high risk of MSfirst attack at high risk of MS
● Access to medications should not be limited by age, level Access to medications should not be limited by age, level of disability, or frequency of relapsesof disability, or frequency of relapses
● Continue treatment indefinitely unless lack of benefit, Continue treatment indefinitely unless lack of benefit, intolerant adverse effects, or better treatment becomes intolerant adverse effects, or better treatment becomes availableavailable
● Ensure adequate accessibility of all FDA-approved drugs Ensure adequate accessibility of all FDA-approved drugs for MSfor MS
● Change treatments only for medically appropriate reasonsChange treatments only for medically appropriate reasons

No One
Ava
ilable
to G
ive †
*P<.05†P<.01.Treadaway K, et al. J Neurol. 2009;256(4):568-576.
Factors InfluencingFactors InfluencingAdherence with DMT in MSAdherence with DMT in MS
70
60
50
40
30
20
0
10
TotalTotalDos
ing In
conv
enien
t
Pregn
ant o
r Plan
ning
Other
Tired
of S
hots
Not S
ure
of B
enef
its
Didn’t R
efill
Didn’t F
eel L
ike It
Heada
che
Fatigu
e
Wea
knes
s
Flu-Lik
e*
Depre
ssion
Pain @
Inj S
ite
Forgo
t to
Take*
Financ
ial
Skin R
eacti
on
Injec
tion
Anxiet
y**

Promoting Adherence to Promoting Adherence to Therapeutic Regimens in MSTherapeutic Regimens in MS
►Starting TherapyStarting Therapy● EducateEducate● Make a plan with Make a plan with
the patientthe patient● Reconfirm goalsReconfirm goals● Schedule proper Schedule proper
follow-upfollow-up● Treat relapses Treat relapses
appropriatelyappropriately● Treat comorbid Treat comorbid
conditionsconditions● Keep channels of Keep channels of
communication communication openopen
Brandes DW, et al. Curr Med Res Opin. 2009;25(1):77-92. Figure 2.
Establishing a
therapeutic relationship
Educating patient and
family
Managing patient
expectations
Addressing patient
concerns
Managing adverse events
Increased
adherence to
treatment

Treadaway K, et al. J Neurol. 2009;256(4):568-576.
Optimizing Treatment OutcomesOptimizing Treatment Outcomes in MS Patients in MS Patients
► Understanding diseaseUnderstanding disease► Clinical implicationsClinical implications► Rationale for treatmentRationale for treatment► Reviewing treatment Reviewing treatment
optionsoptions► Setting realisticSetting realistic
goals/expectationsgoals/expectations► Potential adverse effectsPotential adverse effects► Ways to minimize and Ways to minimize and
manage adverse effectsmanage adverse effects
► Minimizing fear and Minimizing fear and anxietyanxiety
► Proper injection trainingProper injection training► Recognizing relapsesRecognizing relapses► Tracking and reporting Tracking and reporting
symptoms/relapses/adversymptoms/relapses/adverse effects se effects
► Emphasizing importance Emphasizing importance of adherence to therapyof adherence to therapy
Patient Education Is EssentialPatient Education Is Essential

Rio J, et al. Rio J, et al. Mult Scler.Mult Scler. 2005;11:306-309. Twork et al. 2005;11:306-309. Twork et al. Curr Med Res Opin.Curr Med Res Opin. 2007;23(6):1209-1215. 2007;23(6):1209-1215.O’Rourke KE, et al. O’Rourke KE, et al. Mult Scler.Mult Scler. 2005;11(1):46-50. Ross AP. 2005;11(1):46-50. Ross AP. Neurology.Neurology. 2008;71(Suppl 3):S1-S2. DiMatteo 2008;71(Suppl 3):S1-S2. DiMatteo MR, et al. MR, et al. Arch Intern Med.Arch Intern Med. 2000;160:2101-2107. 2000;160:2101-2107.
Challenges to AdherenceChallenges to Adherence
► Cognition and physical limitations negatively Cognition and physical limitations negatively impact adherenceimpact adherence
► Up to half of patients reportedly discontinue Up to half of patients reportedly discontinue because of an AE or a lack of efficacybecause of an AE or a lack of efficacy
► Association of depression carried a 3-fold risk of Association of depression carried a 3-fold risk of nonadherencenonadherence
► Third-party reimbursement challengesThird-party reimbursement challenges● Formulary statusFormulary status● CopaysCopays
► Adherence tends to decrease over time due to a Adherence tends to decrease over time due to a variety of factors, such as “treatment fatigue,” loss variety of factors, such as “treatment fatigue,” loss of motivation, and complacencyof motivation, and complacency

Recent Analyses of the Economic Recent Analyses of the Economic Impact of MS TreatmentImpact of MS Treatment
► In an analysis of an employer medical, drug and disability In an analysis of an employer medical, drug and disability claims database:claims database:● Baseline MS-related medical costs were higher for treated vs Baseline MS-related medical costs were higher for treated vs
untreated employees ($2520 vs $1012,untreated employees ($2520 vs $1012,PP < 0.0001) < 0.0001)● Risk-adjusted total annual medical costs ($4,393 vs $6,187) Risk-adjusted total annual medical costs ($4,393 vs $6,187)
and indirect costs ($2,252 vs $3,053) were significantly and indirect costs ($2,252 vs $3,053) were significantly lower (lower (PP < 0.0001) for treated vs untreated employees with < 0.0001) for treated vs untreated employees with MSMS
● Study limitation: lack of clinical detail on MS severityStudy limitation: lack of clinical detail on MS severity
► Early use of DMTs in patients with CIS that delayed Early use of DMTs in patients with CIS that delayed conversion to CDMS provided a conversion to CDMS provided a positivepositive incremental cost-incremental cost-effectiveness ratio (ICER) per patient-year compared with effectiveness ratio (ICER) per patient-year compared with no treatment (Euros 2,574.94)no treatment (Euros 2,574.94)
Birnbaum HG, et al. Curr Med Res Opin. 2009;25(4):869-877.Lazzaro C, et al. Neurol Sci. 2009;30:21-31.

*Proportion of individuals unemployed during the study who had been employed at some time during his or *Proportion of individuals unemployed during the study who had been employed at some time during his or her lives.her lives. Dennett SL, et al. Dennett SL, et al. Value HealthValue Health. 2008.11(3):478-486.. 2008.11(3):478-486.
Rates of Unemployment inRates of Unemployment inIndividuals with MSIndividuals with MS
StudyStudy CountryCountryDuration of MS Duration of MS
Since Onset Since Onset (Years)(Years)
UnemploymenUnemployment Ratet Rate
Busche et al., 2003Busche et al., 2003 CanadaCanada 14.8 (median) 14.8 (median) (range 1-47)(range 1-47)
Baseline: 49.9%Baseline: 49.9%
2.5 years later: 59.4%2.5 years later: 59.4%
Jackson and Quaal, 1991Jackson and Quaal, 1991 CanadaCanada > 5 in 80% of patients> 5 in 80% of patients 76%*76%*
Gronning et al., 1990Gronning et al., 1990 NorwayNorway 10 (mean) 10 (mean) (range 1-33 years)(range 1-33 years)
72% of those 72% of those with definite MSwith definite MS
O’Connor et al., 2005O’Connor et al., 2005 U.K.U.K.Employed: 10 (mean)Employed: 10 (mean)
Unemployed: 15 (mean)Unemployed: 15 (mean)64%64%
Beatty et al., 1995Beatty et al., 1995 U.S.U.S. 15.4 (mean)15.4 (mean) 60-66%60-66%
Kornblith et al., 1986Kornblith et al., 1986 U.S.U.S. 13 (mean)13 (mean) 80%*80%*
LaRocca et al., 1982LaRocca et al., 1982 U.S.U.S. 13 (mean)13 (mean) 77%77%

Lage MJ, et al. Work. 2006;27(2):143-151.
Effect of IMT and Other Factors on Effect of IMT and Other Factors on Employment Loss TimeEmployment Loss Time
► Focus: factors that influence time missed from work Focus: factors that influence time missed from work among individuals with MS (N = 284) among individuals with MS (N = 284)
► Records were examined for details of medical Records were examined for details of medical claimsclaims
► Multivariate regressions were performed, Multivariate regressions were performed, controlling for demographic characteristics, type of controlling for demographic characteristics, type of immunomodulatory medication, and overall immunomodulatory medication, and overall severity of illnessseverity of illness
► Looked at total number of days missed from work Looked at total number of days missed from work for any reason and specifically due to absenteeism, for any reason and specifically due to absenteeism, short-term disability, or workers compensation short-term disability, or workers compensation
► Results indicate that lost work time is affected by Results indicate that lost work time is affected by severity of illness and type severity of illness and type of IMTof IMT

Fewer days absent from work from 1999–2002 for individuals with MS treated with GA (n = 28), INF-1a (n = 74), or INF-1b (n = 16) compared to untreated individuals with MS (n = 166) Lage MJ, et al. Work. 2006;27(2):143-151.
Effect of Immunomodulatory Effect of Immunomodulatory Therapy on Employment Loss TimeTherapy on Employment Loss Time
-20-20
-10-10
00
1010
2020
3030
4040
5050
6060
Short-termDisability
WorkersComp
AnyReason
Few
er D
ays
Ab
sen
tF
ewer
Day
s A
bse
nt
(P = .003)
(P = .71)
(P = .09)
(P = .04)
(P = .18)(P = .47)
(P = .03)
(P = .33)
(P = .39)
INFbeta-1a
INFbeta-1b
GA

Specialty Pharmacy OverviewSpecialty Pharmacy Overview
► Key Disease States Managed by a Key Disease States Managed by a Specialty PharmacySpecialty Pharmacy● MS, RA, Hep C, hGH, Oral OncolyticsMS, RA, Hep C, hGH, Oral Oncolytics
► The number of patients utilizing The number of patients utilizing Specialty Pharmacies continues to Specialty Pharmacies continues to increaseincrease● Currently estimated to be 40% - 50% of Currently estimated to be 40% - 50% of
MS patientsMS patients

SP Value PropositionSP Value Proposition
► Compliance & AdherenceCompliance & Adherence● Typically 15% - 20% higher than Typically 15% - 20% higher than
retail*retail*
► Patient EducationPatient Education● Specially trained on rare diseases Specially trained on rare diseases
and therapiesand therapies• Collaborate with manufacturers and MS Collaborate with manufacturers and MS
Specialists to assist with trainingSpecialists to assist with training
► Patient MonitoringPatient Monitoring● EfficacyEfficacy● Side effectsSide effects● Co-Morbid ConditionsCo-Morbid Conditions
*2008 IMS Report*2008 IMS Report

SP Value PropositionSP Value Proposition
► Data Tracking and MonitoringData Tracking and Monitoring● Compliance/AdherenceCompliance/Adherence● EfficacyEfficacy
• BaselineBaseline• RelapsesRelapses• EDSSEDSS
● Side EffectsSide Effects• Flu like symptomsFlu like symptoms• Injection site reactionsInjection site reactions
● Co-Morbidities Co-Morbidities • Asthma, Hypertension, diabetesAsthma, Hypertension, diabetes
● Symptom ManagementSymptom Management• Fatigue,Fatigue,• BladderBladder• DepressionDepression
● Appropriate and timely interventionsAppropriate and timely interventions

TTherapy herapy OPOPtimization in timization in MSMS (TOP MS) (TOP MS)
► An Outcomes Study of disease An Outcomes Study of disease management (DM) for MS based management (DM) for MS based in Specialty Pharmacies who in Specialty Pharmacies who have demonstrated commitment have demonstrated commitment to DM:to DM:
• Therapy Adherence and ComplianceTherapy Adherence and Compliance• Disease CharacteristicsDisease Characteristics• RelapsesRelapses• Disability ProgressionDisability Progression• Quality of LifeQuality of Life• Work / Usual Activity ProductivityWork / Usual Activity Productivity

TTherapy herapy OPOPtimization in timization in MSMS((TOP MS)TOP MS)
► Brief Outline: Brief Outline: ● 3 Specialty Pharmacies3 Specialty Pharmacies● ~3,000 patients followed for 2 ~3,000 patients followed for 2
yearsyears● Patient-specific clinical reports to Patient-specific clinical reports to
physiciansphysicians● De-identified data collected in a De-identified data collected in a
research-quality database will be research-quality database will be available to address outcomes available to address outcomes research questionsresearch questions

Study PopulationStudy Population
► Subjects who are treated with Subjects who are treated with glatiramer acetate or interferon glatiramer acetate or interferon (IFN)-(IFN)-ββ and receive their therapy and receive their therapy from a Specialty Pharmacy:from a Specialty Pharmacy:
• Copaxone®Copaxone®• Avonex®Avonex®• Betaseron®Betaseron®• Rebif®Rebif®• Extavia®Extavia®

Study ObjectiveStudy Objective
► To demonstrate the benefits of To demonstrate the benefits of compliance and adherence to MS compliance and adherence to MS therapy with patient outcomes:therapy with patient outcomes:● RelapsesRelapses● Disability progressionDisability progression● Quality of lifeQuality of life● Work and usual activities Work and usual activities
productivityproductivity

AdvocacyAdvocacy
► Assist patients with resources and supportAssist patients with resources and support► Assist patients with navigation of health Assist patients with navigation of health
care system and insurance coveragecare system and insurance coverage► Speak with third-party payors to advocate Speak with third-party payors to advocate
for coverage for all DMTsfor coverage for all DMTs► Become involved with advocacy Become involved with advocacy
organizations organizations ● IOMSNIOMSN● CMSCCMSC● NMSSNMSS● MSAAMSAA● MSFMSF
• Educational activities for professionals and patients
• Development of written materials
• Working at organizational level for FDA approvals, third-party reimbursement
IOMSN = International Organization of MS Nurses; CMSC = Consortium of MS Centers; NMSS = National IOMSN = International Organization of MS Nurses; CMSC = Consortium of MS Centers; NMSS = National MS Society; MSAA = MS Association of America.MS Society; MSAA = MS Association of America.

ConclusionConclusion
► MS is a chronic, debilitating, and progressive MS is a chronic, debilitating, and progressive diseasedisease
► Economic implications are significant and Economic implications are significant and appear directly correlated with disease appear directly correlated with disease severityseverity
► Although costly, long-term data and expert Although costly, long-term data and expert consensus support the primary role of DMT in consensus support the primary role of DMT in managing disease progressionmanaging disease progression
► Optimal therapeutic benefit with DMT hinges Optimal therapeutic benefit with DMT hinges strongly on multidimensional support from strongly on multidimensional support from the healthcare systemthe healthcare system
► Patient education and careful monitoring are Patient education and careful monitoring are key factors driving success in MS therapykey factors driving success in MS therapy

Challenging Cases Challenging Cases in the in the Management Management ofof Multiple Sclerosis Multiple Sclerosis
Case StudiesCase Studies

► 24-year-old female with diplopia on looking 24-year-old female with diplopia on looking to the right for a day or two – Austin to the right for a day or two – Austin ophthalmologist found nothing unusual ophthalmologist found nothing unusual
► Back in Houston another ophthalmologist Back in Houston another ophthalmologist called it ‘some type of optic nerve called it ‘some type of optic nerve inflammation’ and gave her 5 days of oral inflammation’ and gave her 5 days of oral steroidssteroids
► 2 weeks into symptoms seen by a pro who 2 weeks into symptoms seen by a pro who noted skew deviation, marked asymmetric noted skew deviation, marked asymmetric nystagmus with torsion and jerk greater to nystagmus with torsion and jerk greater to the right, no INO, no APD and normal VERs the right, no INO, no APD and normal VERs to go with complaints of vertical diplopia to go with complaints of vertical diplopia and oscillopsia and oscillopsia
Multiple Sclerosis Case #1Multiple Sclerosis Case #1

UPIN 480406/06/08

UPIN 480406/06/08

► 4 days later continued double vision on 4 days later continued double vision on looking to the rightlooking to the right
► Extensive past history uncovered only one Extensive past history uncovered only one week of nausea and vomiting about 4 week of nausea and vomiting about 4 months ago attributed to food poisoningmonths ago attributed to food poisoning
► Nystagmus to right gaze of greater Nystagmus to right gaze of greater amplitude in adducting eye with incomplete amplitude in adducting eye with incomplete abduction of right eye, remaining exam abduction of right eye, remaining exam normalnormal
► CSF with 10 lymphocytes, IgG index 1.15 CSF with 10 lymphocytes, IgG index 1.15 and 3 OCBsand 3 OCBs
► Intravenous methylprednisolone course Intravenous methylprednisolone course startedstarted
Multiple Sclerosis Case #1Multiple Sclerosis Case #1

UPIN 480407/02/08

UPIN 480407/02/08

► The subject was born and raised outside of the The subject was born and raised outside of the reach of the Scandinavian gene pool - is this reach of the Scandinavian gene pool - is this NMO, and how unusual is this?NMO, and how unusual is this?
► When you have CIS and can’t diagnose more When you have CIS and can’t diagnose more than suspect MS by McDonald’s or Swanton’s, than suspect MS by McDonald’s or Swanton’s, do you just treat, use Frohman?do you just treat, use Frohman?
► When asked about the familial risk of MS in the When asked about the familial risk of MS in the company of the patients twin sister, what is the company of the patients twin sister, what is the best course? best course?
Multiple Sclerosis Case #1Multiple Sclerosis Case #1The IssuesThe Issues

► 30-year-old Caucasian female presented 30-year-old Caucasian female presented initially with right optic neuritis. initially with right optic neuritis.
► Vision improved after high dose intravenous Vision improved after high dose intravenous methylprednisolone treatment methylprednisolone treatment
► T2-weighted MRI brain scan showed 2 areas T2-weighted MRI brain scan showed 2 areas of abnormal signal in the periventricular and of abnormal signal in the periventricular and subcortical white matter.subcortical white matter.
► No disease modifying therapy was started at No disease modifying therapy was started at that time. that time.
Multiple Sclerosis Case #2Multiple Sclerosis Case #2

► 1 year later- numbness and weakness of both legs, 1 year later- numbness and weakness of both legs, urinary hesitancy, and increasing gait difficulties urinary hesitancy, and increasing gait difficulties over several days. over several days.
► MRI cord -increased T2 signal at C8 with a MRI cord -increased T2 signal at C8 with a corresponding area of Gd enhancement on T1. corresponding area of Gd enhancement on T1.
► MRI brain- one new periventricular white matter MRI brain- one new periventricular white matter lesion without enhancement in comparison to last lesion without enhancement in comparison to last year’s. year’s.
► Motor symptoms improved with high dose Motor symptoms improved with high dose corticosteroid therapycorticosteroid therapy
► Residual numbness in the feet and bladder control Residual numbness in the feet and bladder control difficulties. difficulties.
Multiple Sclerosis Case #2Multiple Sclerosis Case #2

► Given diagnosis of MS and therapy with once Given diagnosis of MS and therapy with once weekly IM interferon beta was begun.weekly IM interferon beta was begun.
► 6 months later she complained of markedly 6 months later she complained of markedly increased fatigue and “fuzzy thinking.” increased fatigue and “fuzzy thinking.”
► Brain MRI scan revealed several new T2 lesions Brain MRI scan revealed several new T2 lesions in both cerebral hemispheres and several new in both cerebral hemispheres and several new enhancing lesions around the corpus callosum. enhancing lesions around the corpus callosum.
► Disease modifying therapy was changed to a Disease modifying therapy was changed to a high dose subcutaneous interferon beta. high dose subcutaneous interferon beta.
Multiple Sclerosis Case #2Multiple Sclerosis Case #2

► Over the next year, she had no new Over the next year, she had no new symptoms and there were no new lesions symptoms and there were no new lesions seen on a repeat MRI scan.seen on a repeat MRI scan.
► After several months she complained of After several months she complained of balance difficulties, memory difficulties, and balance difficulties, memory difficulties, and an increase in fatigue.an increase in fatigue.
► MRI scan showed additional Gd+ enhancing MRI scan showed additional Gd+ enhancing lesions. lesions.
► A test for neutralizing antibody against A test for neutralizing antibody against interferon beta (NAb) revealed a titer interferon beta (NAb) revealed a titer greater than 1:100. greater than 1:100.
Multiple Sclerosis Case #2Multiple Sclerosis Case #2

► The same interferon treatment was The same interferon treatment was continued but after several months she continued but after several months she complained of ongoing problems with complained of ongoing problems with memory. memory.
► Several new enhancing lesions were again Several new enhancing lesions were again found on MRI. A repeat NAb titer was found on MRI. A repeat NAb titer was unchanged.unchanged.
Multiple Sclerosis Case #2Multiple Sclerosis Case #2

► Student nurse falls hitting head on Student nurse falls hitting head on concrete when obese patient she is concrete when obese patient she is transporting begins to fall off litter. MRI transporting begins to fall off litter. MRI shows pineal cyst.shows pineal cyst.
► 18 months later, follow-up MRI shows 18 months later, follow-up MRI shows unchanged cyst but single unchanged cyst but single periventricular non-enhancing white periventricular non-enhancing white matter lesion.matter lesion.
► Three yearly follow-ups show no new MRI Three yearly follow-ups show no new MRI lesions, no symptoms and no neurologic lesions, no symptoms and no neurologic abnormalities.abnormalities.
Multiple Sclerosis Case #3Multiple Sclerosis Case #3

► While hiking with physician husband on While hiking with physician husband on hot afternoon, she notes numbness in hot afternoon, she notes numbness in left foot.left foot.
► Spinal cord MRI shows enhancing lesion Spinal cord MRI shows enhancing lesion at T17.at T17.
► Is it MS?Is it MS?
► Treatment recommendations?Treatment recommendations?
Is it Multiple Sclerosis?Is it Multiple Sclerosis?