Embed Size (px)
Citation preview

New Era of COPD TreatmentNew Era of COPD Treatment- Focusing on Treatment-- Focusing on Treatment-
Shih Wei Lee, MDShih Wei Lee, MD
Department of Chest Medicine Department of Chest Medicine
Tao-Yuan General Hospital Department of HealthTao-Yuan General Hospital Department of Health

BackgroundBackground

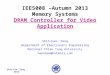
Percent Change in Age-Adjusted Death Rates, U.S., 1965-1998
Percent Change in Age-Adjusted Death Rates, U.S., 1965-1998
00
0.50.5
1.01.0
1.51.5
2.02.0
2.52.5
3.03.0
Proportion of 1965 Rate Proportion of 1965 Rate
1965 - 19981965 - 1998 1965 - 19981965 - 1998 1965 - 19981965 - 1998 1965 - 19981965 - 1998 1965 - 19981965 - 1998
–59%–59% –64%–64% –35%–35% +163%+163% –7%–7%
CoronaryHeart
Disease
CoronaryHeart
Disease
StrokeStroke Other CVDOther CVD COPDCOPD All OtherCauses
All OtherCauses
Source: NHLBI/NIH/DHHSSource: NHLBI/NIH/DHHS
Adapt from 2005 GOLD teaching slide

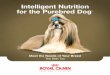
Ischemic heart diseaseCerebrovascular diseaseLower resp infectionDiarrheal diseasePerinatal disordersCOPDTuberculosisMeaslesRoad traffic accidentsLung cancer
Ischemic heart diseaseCerebrovascular diseaseLower resp infectionDiarrheal diseasePerinatal disordersCOPDTuberculosisMeaslesRoad traffic accidentsLung cancer
Stomach CancerHIVSuicide
Stomach CancerHIVSuicide
6th6th
3rd3rd
Murray & Lopez. Lancet 1997
Future Mortality WorldwideFuture Mortality Worldwide1990 2020
Adapt from 2005 GOLD teaching slide

Definition

ERS-ATS COPD Guidelines
Definition of COPD Chronic Obstructive Pulmonary Disease (COPD)
is a preventable and treatable disease state characterised by airflow limitation that is not fully reversible.
The airflow limitation is usually progressive and associated with an abnormal inflammatory response of the lungs to noxious particles or gases, primarily caused by cigarette smoking.

Pathogenesis

Noxious particles
and gases
Lung inflammation
Host factors
COPD pathology
ProteinasesOxidative stress
Anti-proteinasesAnti-oxidants
Repair mechanisms
Adapt from 2005 GOLD teaching slide

Pathology





Inflammation

Inflammatory Mechanisms of COPD
Cigarette smoke
Alveolar macrophage
Neutrophil
PROTEASES
Alveolar wall destruction(Emphysema)
Mucus hypersecretion(Chronic bronchitis)
Neutrophil chemotactic factors
Neutrophil elastaseCathepsins
Matrix metalloproteinases
Cytokines (IL-8)Mediators (LTB4)
?CD8+
lymphocyteMCP-1
PerforinGranzyme B
TNF-

Protease-Antiprotease Imbalance

Pulmonary/bronchial vessel
Neutrophil
Mac-1SLx
AdhesionICAM-1E-selectin
ChemotaxisIL-8, LTB4CXC chemokines
SurvivalGM-CSF
Macrophage
Activation
CXCR1CXCR2 Neutrophil elastase
CathepsinsProteinase 3
ELASTOLYSIS ELASTOLYSIS MUCUS HYPERSECRETIONMUCUS HYPERSECRETION

Mucus secretion
NF-B
IL-8
Neutrophil
recruitment
TNF-
REACTIVE OXYGEN SPECIES IN COPD
Plasma leak BronchoconstrictionIsoprostanes
ANTIOXIDANTSVitamins C and EN-acetyl cysteineGlutathione analoguesNitrones (spin trap)
O2-, H2O2
OH., ONOO-
Anti-proteases
SLPI 1-AT
Proteolysis

Blue Blue bloaterbloater
Pink Pink pufferpuffer


Diagnosis

Normal Alveolar EmptyingNormal Alveolar Emptying

Alveolar Emptying in COPDAlveolar Emptying in COPD
In COPD, airflow is limited because alveoli lose their elasticity, supportive structures are lost, and small airways are narrowed

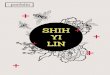
Breathing in COPDBreathing in COPD

Volume- Time-CurveVolume- Time-Curve
Time
Volume
t3 t4t1 t2
V1
: It takes longer to expire the same volume V1
: At the same time (t3) more air is still in the lung, because of flow limitation (due to obstruction and / or loss of elasticity
: more time is needed (t3 to t4) to expire completely
HealthyCOPD

ERS-ATS COPD Guidelines
Diagnosis of COPD (2)Spirometry
Spirometric classification of COPD: Post-bronchodilator FEV1/forced vital capacity <0.7 confirms the
presence of airflow limitation that is not fully reversible.
Severity Postbrochodilator FEV1/FVC
FEV1 % pred
At risk Patients who:
smoke or have exposure to pollutants have cough, sputum or dyspnoeahave family history of respiratory disease
>0.7 80
Mild COPD 0.7 80
Moderate COPD 0.7 50–80
Severe COPD 0.7 30–50
Very severe COPD 0.7 <30

Evaluation

ERS-ATS COPD Guidelines
Definition, evaluation and treatment (3) The Operational Classification of Severity is as follows: ambulatory (Level I), requiring
hospitalisation (Level II) and acute respiratory failure (Level III).
Level I Level II Level III
Clinical historyCo-morbid conditions
History of frequent exacerbations
Severity of COPD
+
+
Mild/moderate
+++
+++
Moderate/severe
+++
+++
Severe
Physical findingsHaemodynamic evaluation
Use accessory respiratory muscles, tachypnoea
Persistent symptoms after initial therapy
Stable
Not present
No
Stable
++
++
Stable/unstable
+++
+++
Diagnostic proceduresOxygen saturation
Arterial blood gases
Chest radiograph
Blood tests
Serum drug concentrations
Sputum gram stain and culture
Electrocardiogram
Yes
No
No
No
If applicable
No
No
Yes
Yes
Yes
Yes
If applicable
Yes
Yes
Yes
Yes
Yes
Yes
If applicable
Yes
Yes
+: unlikely to be present; ++: likely to be present; +++: very likely to be present

ERS-ATS COPD Guidelines
Definition, evaluation and treatment (4) Level I: outpatient treatmentPatient education
Check inhalation technique
Consider use of spacer devices
BronchodilatorsShort-acting β2-agonist and/or ipratropium MDI with spacer or hand-held nebuliser as needed
Consider adding long-acting bronchodilator if patient is not using it
Corticosteroids (the actual dose may vary)Prednisone 30–40 mg per os q day for 10 days
Consider using an inhaled corticosteroid
Antibiotics May be initiated in patients with altered sputum characteristics
Choice should be based on local bacteria resistance patterns
Amoxicillin/ampicillin, cephalosporins
Doxycycline
Macrolides
If the patient has failed prior antibiotic therapy consider:
Amoxicillin/clavulanate
Respiratory fluoroquinolones

ERS-ATS COPD Guidelines
Definition, evaluation and treatment (5) Level II: treatment for hospitalised patient
BronchodilatorsShort acting β2-agonist (albuterol, salbutamol) and/or
Ipratropium MDI with spacer or hand-held nebuliser as needed
Supplemental oxygen (if saturation <90% )
CorticosteroidsIf patient tolerates, prednisone 30–40 mg per os q day for 10 days
If patient can not tolerate oral intake, equivalent dose i.v. for up to 14 days
Consider use inhaled corticosteroids by MDI or hand-held nebuliser
Antibiotics (based on local bacteria resistance patterns) May be initiated in patients that have a change in their sputum characteristics (purulence and/or volume)
Choice should be based on local bacteria resistance patterns
Amoxicillin/clavulanate
Respiratory fluoroquinolones (gatifloxacin, levofloxacin, moxifloxacin)
If Pseudomonas spp. and/or other Enterobactereaces spp. are suspected, consider combination therapy

ERS-ATS COPD Guidelines
Definition, evaluation and treatment (6) Level III: treatment in patients requiring special or intensive care unit
Supplemental oxygen
Ventilatory support
Bronchodilators Short-acting β2-agonist (albuterol, salbutamol) and ipratropium MDI with spacer, two puffs every 2–4 h
If the patient is on the ventilator, consider MDI administration, consider long-acting β-agonist
CorticosteroidsIf patient tolerates oral medications, prednisone 30–40 mg per os q day for 10 days
If patient can not tolerate, give the equivalent dose i.v. for up 14 days
Consider use inhaled corticosteroids by MDI or hand-held nebuliser
Antibiotics (based on local bacteria resistance patterns)Choice should be based on local bacteria resistance patterns
Amoxicillin/clavulanate
Respiratory fluoroquinolones (gatifloxacin, levofloxacin, moxifloxacin)
If Pseudomonas spp. and or other Enterobactereaces spp. are suspected consider combination therapy

Current Treatment

Therapy at Each Stage of COPD
Old 0: At Risk I: Mild II: Moderate
IIA IIB
III: Severe
New 0: At Risk I: Mild II: Moderate III: Severe IV: Very Severe
Characteristics • Chronic symptoms
• Exposure to risk
factors
• Normal spirametry
• FEV1/FVC < 70%
• FEV1 ≥ 80%
• With or without
symptoms
• FEV1/FVC < 70%
• 50% ≤ FEV1 < 80%
• With or without
symptoms
• FEV1/FVC < 70%
• 30% ≤ FEV1 < 50%
• With or without
symptoms
• FEV1/FVC < 70%
• FEV1 < 30% or presence
of chronic respiratory failure
or right heart failure
Avoidance of risk factor(s); influenza vaccinationAvoidance of risk factor(s); influenza vaccination
Add Add short-acting bronchodilator when neededshort-acting bronchodilator when needed
Add Add regular treatment with one or moreregular treatment with one or more
long-acting long-acting bronchodilatorsbronchodilators
Add Add rehabilitationrehabilitation
Add Add inhaled glucocorticosteroidsinhaled glucocorticosteroids
AddAdd
Long-term Long-term oxygen if oxygen if chronic chronic respiratoryrespiratory
failurefailure
ConsiderConsider
Surgical Surgical treatmentstreatments

(GOLD EXECUTIVE SUMMARY2005)

Contraction Relaxation cAMP
AMP
SMOOTH MUSCLE CELL
M1
M2M3
Anticholinergic
-agonisttheophylline
BronchodilatorsBronchodilators

Cell membrane
α s
γβAC
ATP
c-AMP
PKAPKG
GS GS
β 2 Stimulant↓
β 2 Receptor
Ca2+activationK+ channel activation
Na+/K+ ATPaseactivation Hyper-
polarization
Pl decomposition Ca2 +release
inhibition inhibition
Na+/Ca2+ exchange Ca2 +excretion
MLCK inhibition
K+
CHARYBDOTOXINExtracellular
Smooth muscle cell
α s
γβ
AMP
Teophylline
PDESTO
P
K+ Release
STOP
Relaxation ofRelaxation ofmyofibermyofiber
Ca2 + decrease
Ⅱ- 13
PI : phosphatidylinositol AC : adenylate cyclasePKA : protein kinase AMLCK : myosin light chain kinaseGs : Gs protein CHARYBDOTOXIN : Calcium-dependent potassium
channel
Mechanism of relaxation of bronchial smooth muscle
acceleration
2
3
11

Onset And Duration - LIPOPHILICITY
Salbutamol (Albuterol)
hydrophilic short duration rapid onset
Formoterol
Intermediate lipophilicity
long duration
rapid onset
Salmeterol
lipophilic
long duration
slow onset
Anderson GP Life Sci 1993, 52:2145
Aqueous compartment
B2-receptor
Lipophilic bilayer

Pre-ganglionicPre-ganglionicnervenerve
ParasympatheticParasympatheticganglionganglion
Post-ganglionicPost-ganglionicnervenerve
AChACh
Airway smoothAirway smoothmusclemuscle
Nicotinic receptors (+)Nicotinic receptors (+)
MM11 receptors (+) receptors (+)
MM22 receptors (–) receptors (–)
MM33 receptors (+) receptors (+)
BarnesBarnes.. Eur Respir RevEur Respir Rev (1996) (1996)
Tiotropium Provides Specific, Tiotropium Provides Specific, Long-lasting MLong-lasting M33 Receptor Blockade Receptor Blockade

Anticholinergics and Airway Dynamics Anticholinergics and Airway Dynamics in the Normal State in the Normal State

Anticholinergics and Airway Dynamics Anticholinergics and Airway Dynamics in COPDin COPD
In COPD, hypertrophy of the airway wall exacerbates the effects of cholinergic constriction

ERS-ATS COPD Guidelines
Pharmacological Therapy (6)
Medication FEV1Lung volume Dyspnoea HRQoL
Short-acting β-agonist Yes (A) Yes (B) Yes (A) NAIpratropium bromide Yes (A) Yes (B) Yes (A) No (B)Long acting β-agonists Yes (A) Yes (A) Yes (A) Yes (A)Tiotropium Yes (A) Yes (A) Yes (A) Yes (A)Inhaled corticosteroids Yes (A) NA Yes (B) Yes (A)Theophylline Yes (A) Yes (B) Yes (A) Yes (B)
Medication AEExercise endurance
Disease modifier by FEV1 Mortality Side-effects
Short-acting β-agonist NA Yes (B) NA Na SomeIpratropium bromide Yes (B) Yes (B) No NA SomeLong acting β-agonists Yes (A) Yes (B) No NA MinimalTiotropium Yes (A) Yes (B) NA NA MinimalInhaled corticosteroids Yes (A) NA No NA SomeTheophylline NA Yes (B) NA NA Important
Effects on commonly used medications on important clinical outcomes in COPD

Combination Therapy
Chest 1999;115:966–971

Combination Therapy
Chest 1997;112:1514–21

Combination Therapy
James F. Donohue
James F. Donohue

Manage Stable COPD Key PointsManage Stable COPD Key Points
Regular treatment with inhaled glucocorticosteroids is appropriate for symptomatic COPD patients with an FEV1 < 50% predicted (Stage III: Severe COPD and Stage IV: Very Severe COPD) and repeated exacerbations e.g. 3 in the last three years (Evidence A).
Inhaled glucocorticosteroid combined with a long-acting B2-agonist is more effective than the individual components (Evidence A).
Regular treatment with inhaled glucocorticosteroids is appropriate for symptomatic COPD patients with an FEV1 < 50% predicted (Stage III: Severe COPD and Stage IV: Very Severe COPD) and repeated exacerbations e.g. 3 in the last three years (Evidence A).
Inhaled glucocorticosteroid combined with a long-acting B2-agonist is more effective than the individual components (Evidence A).
Adapt from 2005 GOLD teaching slide

ICS and LABAs improve symptoms and lung function via different mechanisms in COPD
Inflammation
Increased neutrophils andCD8+ lymphocytes
Elevated IL–8, TNF
Protease/anti-proteaseimbalance
Structural changes
Alveolar destruction
Collagen deposition
Glandular hypertrophy
Airway fibrosis
Symptoms
FEV1
Exacerbations
Inhaled corticosteroidsreduce
LABAs inhibit
Smooth muscle contraction
Increased cholinergic tone
Loss of elastic recoil
Sensory nerve activation
Airway constriction

Corticosteroid
Corticosteroidreceptors
HSP 90
Long-acting 2-agonists
2- adrenoceptor synthesis
Increased anti-inflammatory effectIncreased anti-inflammatory effect Decreased acquired toleranceDecreased acquired tolerance
Synergistic Interaction of 2-Agonists with Corticosteroid
cyclic AMP
PKA
MAPK

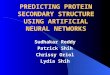
Budesonide/Formoterol Reduces Severe Exacerbations/Patient/Year
Budesonide/Formoterol Reduces Severe Exacerbations/Patient/Year
*†
Red
uct
ion
vs
pla
ceb
o (
%)
*p<0.05 vs placebo†p<0.05 Symbicort vs formoterol
–30
–25
–20
–15
–10
–5
0
Symbicort Budesonide Formoterol
–24%
–15%
–2%
Budesonide/Formoterol Reduces Mild Exacerbations/Patient/Year
Budesonide/Formoterol Reduces Mild Exacerbations/Patient/Year
***p<0.001 vs placebo; p<0.05 Symbicort vs budesonide
–70
–60
–50
–40
–30
–20
–10
0
Symbicort Budesonide Formoterol
–62%
–41%
–55%
***
***
***Red
uct
ion
in m
ild e
xace
rbat
ion
s vs
pla
ceb
o (
%)
(Adapted from Szafranski et al. ERS 2002)(Adapted from Szafranski et al. ERS 2002)
Budesonide/Formoterol Reduces the Use of Oral Corticosteroids in COPD
–35
–30
–25
–20
–15
–10
–5
0
–31%–29%
–3%
**
*p<0.05 vs placebo; p<0.05 Symbicort vs formoterol
Symbicort Budesonide Formoterol
Red
uct
ion
in
ora
l st
ero
id u
se
vs
pla
ceb
o (
%)
Budesonide/Formoterol Reduces the Symptoms of COPD within 1 Week
Budesonide/Formoterol Reduces the Symptoms of COPD within 1 Week
–1.4
–1.2
–1
–0.8
–0.6
–0.4
–0.2
0Symbicort Budesonide Formoterol
p<0.001
p=0.024p=0.004
Mea
n c
han
ge
in t
ota
l sym
pto
m
sco
re v
sp
lace
bo
p<0.001 Symbicort vs budesonide; p<0.001 Symbicort vs formoterol

Budesonide/ Formoterol Reduces 2-agonist Reliever Medication
Budesonide/ Formoterol Reduces 2-agonist Reliever Medication
–1.6
–1.4
–1.2
–1
–0.8
–0.6
–0.4
–0.2
0Symbicort Budesonide Formoterol Placebo
******
p=0.001
Ad
jus
ted
mea
n c
ha
ng
e in
no
. re
liev
er i
nh
ala
tio
ns
/24
h
***p<0.001 vs placebo; p<0.001 Symbicort vs budesonide
Budesonide/ Formoterol Improves Health-related Quality of Life (SGRQ Total Score)
Budesonide/ Formoterol Improves Health-related Quality of Life (SGRQ Total Score)
Adjusted mean change from run-in
–6
–5
–4
–3
–2
–1
0Symbicort Budesonide Formoterol Placebo
*
MCID
MCID = minimum clinically important difference*p<0.05 vs placebo
Budesonide/Formoterol Reduces Shortness of BreathBudesonide/Formoterol Reduces Shortness of Breath
Symbicort Budesonide Formoterol Placebo
–35
–30
–25
–20
–15
–10
–5
0
–32%
–18%
–24%
–10%
Red
uct
ion
in s
ho
rtn
ess
of
bre
ath
se
ver
ity
sc
ore
fro
m r
un
-in
(%)
p<0.001 Symbicort vs placebo and budesonide
Budesonide/Formoterol Reduces Night-time AwakeningsBudesonide/Formoterol Reduces Night-time AwakeningsA
dju
ste
d m
ean
ch
an
ge
(%)
in n
igh
t-ti
me
aw
ake
nin
gs
–0.4
–0.35
–0.3
–0.25
–0.2
–0.15
–0.1
–0.05
0
Symbicort Budesonide Formoterol Placebo
* p<0.05, ** p<0.01, ***p<0.001 vs placebo
p=0.003 Symbicort vs budesonide; p=0.019 Symbicort vs formoterol
***
***
(Adapted from Szafranski et al. ERS 2002)(Adapted from Szafranski et al. ERS 2002)

Combination Therapy
Treat Respir Med. 2004;3:173–181

ERS-ATS COPD Guidelines
Pharmacological therapy (4) Bronchodilators Short-acting bronchodilators can increase exercise tolerance acutely in
COPD.
Anticholinergics given q.i.d. can improve health status over a 3-month period.
Long-acting inhaled β-agonists improve health status, possibly more than regular ipratropium. Additionally, these drugs reduce symptoms, rescue medication use and increase the time between exacerbations.
Combining short-acting agents (salbutamol/ipratropium) produces a greater change in spirometry over 3 months than either agent alone.
Combining long-acting inhaled β-agonists and ipratropium leads to fewer exacerbations than either drug alone.
Combining long-acting β-agonists and theophylline produces a greater spirometric change than either drug alone.
Tiotropium improves health status and reduces exacerbations and hospitalisations compared with both placebo and regular ipratropium.

New Approaches to COPD
P. J. Barnes
EUROPEAN RESPIRATORY REVIEW, 2005;14: 2-11

New Targets for COPD treatment
Alveolar macrophage
Neutrophil
Alveolar wall destruction
(Emphysema)
Mucus hypersecretion
Neutrophil elastaseCathepsinsMatrix metalloproteinases
Cytokines (IL-8)
Mediators (LTB4)
?CD8+
lymphocyte
MCP-1
PROTEASES PROTEASES
Stop smokingbupropion
Mediator antagonistsLTB4 inhibitors
Chemokine inhibitorsAntioxidants
Mucoregulators
Immunosuppressants?
Neutrophil inhibitorsPDE4 inhibitors
p38 MAPK inhibitorsNF-B inhibitors
Protease inhibitorsNE, MMP inhibitors
1-AT, SLPI
Alveolarrepair
P J Barnes

P.J. BARNES AND R.A. STOCKLEY

P.J. BARNES AND R.A. STOCKLEY

Phosphodiesterase-4 inhibtors• PDE type 4 is expressed predominately in inflammatory
cells, such as neutrophils, CD8+ lymphocytes, and macrophages, makes this enzyme an attractive target for the development of new drugs to treat pulmonary inflammation that is characterisitic of COPD.
• Cilomilast, Roflumilast• Postive effect on lung function but also on the frequency
of exacerbations, may also slow disease preogression• Side effect: headache, sleep distubrance, and nausea,
vascular inflammatory( arteritis ) in the messentery and organ organs.
Roland Buhl and stephen G. Farmer 2005 ATS

Antileukotriene drugs
• LTB4: endogeneous chemoattaractants for peripheral blood neutrophils to bronchial tissues
• LTB-109: an oral LTB4 receptor antagonist, clinical trial results have been disappointing.
• BIIL-284:phase I
• Zafirlukask: bronchodilatation
Roland Buhl and stephen G. Farmer 2005 ATS

THANK FOR YOUR ATTENTION

新春愉快