Embed Size (px)
Citation preview

Defining Priorities to Improve End of Life Care in Canada
Daren K. Heyland, MD, MSc 1,2,8
Deborah J Cook, MD, MSc 3
Graeme M.Rocker, DM, MHSc 4 ; Peter M. Dodek, MD, MHSc 5
Demetrios J. Kutsogiannis, MD, MHS 6 ; Yoanna Skrobik, MD 7
Xuran Jiang MD, MSc 8, Andrew G. Day MSc 8
S. Robin Cohen PhD 9
1. Department of Medicine, Kingston General Hospital, Kingston, Ontario.2. Department of Community Health and Epidemiology, Queen’s University,
Kingston, Ontario3. Departments of Medicine, Clinical Epidemiology & Biostatistics, McMaster
University, Hamilton, Ontario 4. Department of Medicine, Queen Elizabeth II Health Sciences Center, Halifax, Nova Scotia5. Department of Medicine and Center for Health Evaluation and Outcome Sciences, St.
Paul’s Hospital and University of British Columbia, Vancouver, British Columbia 6. Division of Critical Care Medicine, University of Alberta, Edmonton, Alberta
7. Critical Care, Hopital Maisonneuve Rosemont, Université de Montréal, Québec8. Clinical Evaluation Research Unit, Kingston General Hospital, Kingston, Ontario9. Departments of Oncology and Medicine, McGill University and Jewish General
Hospital, Montreal, Quebec, Canada, for the Canadian Researchers at the End of Life Network (CARENET)*
Correspondence to:Dr. DK HeylandAngada 4Kingston General HospitalKingston, OntarioK7L 2V7613-549-6666x3339 (Phone)613-548-2428 (FAX)Email: [email protected]
Word Count: 2540
Key words: End of life care, palliative care, satisfaction surveys, health service research,
observational study, quality improvement.
1

Abstract
Background: High quality end of life care should be the right of every Canadian. The
objective of this study was to identify high priority opportunities to improve end of life
care.
Methods: In a multi-center, cross-sectional survey of patients who had advanced, life-
limiting illnesses, and their family caregivers, we administered the Canadian Health Care
Evaluation Project (CANHELP) questionnaire along with an overall global rating
question to measure satisfaction with end of life care. Importance was derived from the
Pearson correlation coefficients between individual questions on the CANHELP
questionnaire and a global rating of satisfaction. To determine high priority issues, we
identified those questions that had high importance and low satisfaction scores.
Results: Of the 471 patients and 255 family members approached, 363 patients and 193
family members participated (response rates of 77% and 76%, respectively). Priority
areas for improvement from the patients’ perspectives related to the feeling of peace,
assessment and treatment of emotional problems, physician availability, and satisfaction
that the physician took a personal interest in them, communicated clearly and
consistently, and listened. Similar priorities were identified from family members’
perspectives; however, additional priorities included timely information about the
patient’s condition and discussions with the doctor regarding final location of care and
use of end of life technology.
2
Interpretation: Our analysis suggests that improved psychological and spiritual support,
better advance care planning, and improved relationships with physicians, including
better communication and decision making, may efficiently improve end of life care in
Canada.
Word count: 243
3
Introduction
Despite the fact that a ‘quality death’ is an espoused right of Canadians,1 this is not
achieved for many dying patients and their families. Recent reviews and observational
studies describe considerable dissatisfaction with end of life care, indicating that there are
still opportunities for improvement.2-5
Improvement initiatives would ideally be informed by the experiences and expectations
of patients and family members. However, efforts to improve end of life care are often
hampered by inadequate definitions of quality and by suboptimal measurement tools.6-8
In a large cross-sectional survey, we recently defined what matters most to seriously ill
patients as they approach the end of life.9 Both patients and family members reported that
it was extremely important that they have trust and confidence in the physicians who are
caring for them or their loved ones.9 Avoidance of unwanted life support, effective
communication, continuity of care, and feelings of life completion were also rated as
highly important.9 Building on these findings, we used these comprehensive ratings of
importance to develop and validate a novel questionnaire to measure satisfaction with end
of life care.10 Using this questionnaire, we have formally evaluated the care received at
the end of life in several Canadian centers.
The objective of this study was to identify opportunities for improvement in care among
patients who had advanced, life-limiting diseases, and their families. We identified these
opportunities by focusing on care issues that were considered important but also had low
4

ratings of satisfaction. By targeting these quality gaps for change initiatives, we can
address the highest priorities in improving end of life care in Canada.
5

Methods
This study was a cross-sectional survey of patients who had advanced, life-limiting
illnesses and their family caregivers. Patients and family caregivers were recruited from
both inpatient and outpatient facilities (and affiliated home-care programs) at the
Kingston General Hospital in Kingston; St. Joseph’s Healthcare, Hamilton; St Paul’s
Hospital, Vancouver; Queen Elizabeth II Health Science Center, Halifax; The New
Brunswick Extra Mural Program; Royal Alexandra Hospital, Edmonton; and Hôpital
Maisonneuve-Rosemont, Montreal.
To be eligible, patients had to understand English or French, be capable of giving
informed consent, and be > 55 years of age with clinical criteria for advanced chronic
obstructive pulmonary disease (COPD), congestive heart failure (CHF), liver disease or
metastatic cancer. In addition, any patient > 80 years of age in hospital who had a
medical diagnosis as the primary cause of admission or any patient > 80 years of age who
was enrolled in a home care program using long term oxygen therapy and who had a
primary diagnosis of COPD, CHF, or metastatic cancer was consider eligible (See
Appendix A for detailed description of inclusion criteria). Using clinical judgment, we
excluded patients who were considered cognitively impaired or otherwise unsuitable for
detailed questionnaire administration because of communication problems, physical or
emotional frailty. We obtained written informed consent from willing patients and then
asked them to identify a suitable family caregiver. If the patient was not competent or
declined involvement, we approached eligible family caregivers independent of the
patient’s involvement (see Appendix A for eligibility criteria). The research assistant then
6
conducted separate face-to-face interviews with the patient and family caregivers and
administered the questionnaires described below.
The Canadian Health Care Evaluation Project (CANHELP) Questionnaire
The details of our initial development of the CANHELP questionnaire have been
published elsewhere.2,9,11-12 In brief, we generated items to be included in this
questionnaire from a review of the published literature, focus groups with experts, and
interviews with patients. We grouped these items into the following6 domains based on
our conceptualization of the major themes that emerged from our data: 1) Characteristics
of the Doctors and Nurses (8 items); 2) Illness Management (7 items); 3) Health Service
Characteristics (4 items); 4) Communication and Decision-making (11 items); 5)
Relationships with Others (4 items); and 6) Spirituality and Meaning (3 items). Prior to
the domain-specific items, the respondents were asked to rate their overall satisfaction
with the care they had received in the past month. We developed one version for the
patient and 2 for the family caregiver (one if the patient was alive, and one if the patient
had died). Response options were: 1=Not at all Satisfied, 2=Not very Satisfied,
3=Somewhat Satisfied, 4=Very Satisfied, and 5=Completely Satisfied. We have
demonstrated that the CANHELP questionnaire correlates as expected with other
established measures at the end of life (construct validity), has good internal consistency
(Cronbach’s alpha >0.70), and can be grouped into valid subscales.10 The finalized
version was used for this study (see www.thecarenet.ca for copy of current
questionnaire).
7
We recorded demographic information at the time of the interview. We assessed patient
functional status using the Palliative Performance Scale;13 co-morbidities were
categorized and calculated according to the Charlson Co-morbidity Index.14
We describe patient and family caregiver characteristics as counts and percentages for
categorical variables and means with standard deviations for continuous variables.
Responses to CANHELP questionnaires were summarized as means with standard
deviations and ranges. To enable comparisons with previous work using this instrument,
we also report the percent of respondents who were ‘completely satisfied.’ To determine
the high priority opportunities for improvement from our satisfaction data, we developed
plots of importance versus performance.15 We defined the relative importance of the
items according to their Pearson correlation coefficient with the global rating of
satisfaction.15 Thus, items uncorrelated with overall satisfaction were considered
unimportant. Scatter plots were used to assess the relationship between this measure of
importance and the mean satisfaction score for each CANHELP question. We used grid
lines to separate the scatter plot into 4 quadrants; the horizontal and vertical lines were
placed at the median of the respective data points to identify 4 separate quadrants.
Questions in the upper left quadrant were important (i.e., they correlated highly with
overall satisfaction) and had the lowest satisfaction scores relative to other questions. We
deemed the care issues identified by these questions to have the highest priority for
improvement.15 All analyses were performed using SAS version 9.1 (SAS Institute,
Cary, NC).
8

Following Queen’s University Research Ethics Board approval of the study, all other
participating site’s Ethics Boards subsequently approved the study.
9
Results
From August 2007 to January 2009, 622 patients at participating sites were identified as
potentially eligible according to the criteria outlined above; 151 were excluded for
communication reasons (e.g., inability to understand English or French; inability to speak
or hear, or impaired mental status); or unsuitability (deemed unable to tolerate an
interview due to lack of physical stamina or their psychological state). Of the 471
remaining eligible patients, 363 consented for an overall response rate of 77.1%. Two
patients withdrew before completing the interview leaving 361 questionnaires evaluable
for analysis. Of the evaluable patients, 175 (48.5%) had an eligible family caregiver
available to interview. Independently, we also approached 80 family caregivers of the
non-participating patients that met the inclusion criteria for a total of 255 family
caregivers. A total of 193 consented for a response rate of 75.7%. Table 1 displays the
demographics of included patients and family caregivers. Due to sporadic missing data,
the number of responses used to calculate the average item scores and correlations with
the global scores is slightly less than 361 patients and 193 family caregivers. The most
frequently missing item was satisfaction with home care services which was missing for
60 (16.6%) patient and 33 (17.1%) caregiver questionnaires. In both questionnaires,
every other item was at least 93.3% complete.
Patients
The correlation coefficient for the score of each individual question with the global
satisfaction rating and the % completely satisfied for each question is shown in Appendix
B. Using the magnitude of these correlation coefficients to determine importance, we
10
identified the 5 most important issues from the patients’ perspectives: 1) being treated by
doctors and nurses in a manner that preserved their sense of dignity (Pearson correlation
coefficient: 0.46); 2) receiving good care when a family member or friend was not able to
be with them (0.42); 3) aspects of their medical care, such as the tests that were done and
the treatments that were given (0.41); 4) the health care workers worked together as a
team to look after them (0.41); and 5) the doctors and nurses looking after them were
compassionate and supportive (0.41).
The mean satisfaction score for the global rating of satisfaction question was 4.3 (SD 0.8,
range 1.0-5.0). Patients were least satisfied with the following issues: 1) doing special
things they wanted to do during the past month (mean satisfaction score 3.08); 2) their
level of confidence in their own ability to manage their illness (3.18); 3) their
understanding of what to expect in the end stage (3.41); 4) their ability to contribute to
others in a meaningful way (3.52); and 5) discussions with their physician regarding final
location of care (3.65 ) and the use of technology at the end of life (3.67) (see Appendix
A).
Figure 1 shows the relationship between the importance scores and the mean satisfaction
scores for each question. The issues localized to the upper left quadrant and deemed the
highest priority relate to the patients’ feelings of peace, the availability of the doctor, the
assessment and treatment of their emotional problems, whether their doctor took a
personal interest in them and listened to them, the consistency of information about their
11

conditions from all doctors and nurses, and whether things were explained in a way they
could understand (see Table 2).
Family Caregiver
Family caregivers’ global rating of satisfaction with how they were treated was 4.2 (SD=
0.8, range 1.0-5.0). Appendix C shows the importance and satisfaction scores for each
question on the family caregiver satisfaction survey. Appendix D shows the performance-
importance plots from the family caregiver perspective. Priority issues from family
caregivers’ perspective are itemized in Table 2.
12

Interpretation
In this study of 361 seriously ill patients and 193 family members from several centers,
we documented that overall satisfaction with end of life care was good (overall score
4.3/5 for patients and 4.1/5 for family members). However, these results should not be
interpreted as saying there are no opportunities for improvement in end of life care for
this population. It has been documented previously that respondents tend to over-report
positive responses.16 For individual patients and their families and for specific aspects of
care, there were many ratings of dissatisfaction and the proportion of respondents that
rated ‘completely satisfied’ was as low as 9% and only as high as 57%. To focus quality
improvement initiatives on issues that matter the most to patients, we determined the
level of importance of each question by assessing the correlation of scores from
individual questions with a global rating of satisfaction,15 thereby reflecting the extent to
which each question is associated with an independent measure of overall satisfaction.
We found that being cared for while preserving dignity, being treated with respect and
compassion, having trust and confidence in the doctor, and being well looked after by the
health care team are all important aspects of good quality end of life care. These findings
are consistent with other populations reporting similar aspects of care as important at the
end of life.9,17-19
Subsequently, we plotted the calculated measures of importance with the directly
measured scores of satisfaction for individual items. For both patients and families, the
highest priority quality improvement issues were improving the emotional support
provided to patients, improving the quality of the relationship between the patient,
13

family, and the doctor, and improving communication and decision making. Deficiencies
in physician relationships and communication and decision-making have been
highlighted previously.2,20-23 In our work, these deficiencies were centered around
physicians’ attentiveness, frequency and consistency of interactions, and planning of the
logistics of end of life care including the limitation of life sustaining therapies. These
gaps did not appear to relate to medical aspects of care; satisfaction with test and
treatments was rated very high by patients.
Whereas high levels of anxiety and depression have been reported previously in cancer
patients,24-25 our finding that there is a large unmet need for emotional support in patients
who have advanced medical diseases and in their families underscores the need to
improve our assessment and treatment of symptoms of depression and anxiety. ‘Being at
peace’ has been identified as a high priority issue for improvement. This finding is
consistent with results from other published studies which state that existential and
spiritual concerns are very prevalent at the end of life.26-27 This issue is also relevant to
family members. Although ‘being at peace’ does not have the same importance to family
caregivers in this survey, there is evidence from a longitudinal study that family members
ratings of satisfaction with issues related to their own spirituality and sense of meaning
significantly deteriorate in the months after the death of a loved one.11 We hypothesize
that a psychological or spiritual supportive intervention may help to improve satisfaction
with end of life care.28
Limitations:
14

The limitations of this study relate to the fact that we did not directly measure
importance. Asking patients directly to rate the level of importance of each question
would have seriously compromised the feasibility of this study by adding to the burden of
data collection. In this analysis, we used median scores for thresholds on the
performance-importance grids. Depending on institutional resources available to
approach opportunities for improvement, the threshold for these lines could be set
elsewhere to identify issues for improvement. Alternatively, institutions could select
among items outside of the upper left quadrant to focus upon. While there is no single
approach to prioritizing these quality gaps, we suggest that such heuristic divisions
provide a useful starting point. Moreover, given the cross sectional nature of this study,
we cannot be certain whether dissatisfaction with care leads to emotional distress or
whether emotional distress leads to dissatisfaction with care. Furthermore, we have used
the CANHELP questionnaire as a ‘screening tool’. Responses to this questionnaire may
illuminate in general terms where the problems lie but in some cases more detailed
assessments will be required to specifically understand the unmet needs. Finally, our
study sample was primarily a Caucasian population; there may be other ethnic or cultural
groups of patients to which our results may not apply. To overcome this deficiency, we
have developed a version of the CANHELP questionnaire to enable individual patients
and family caregivers to rate each aspect of care both in terms of its importance and their
satisfaction so we can derive a priority list of quality improvement targets individualized
to a given patient and/or their family (see www.thecarenet.ca for this individualized tool).
Notwithstanding these limitations, the strengths of this study include the use of a
15
validated questionnaire in patients who had diverse medical conditions in multiple
settings.
Conclusions:
In these patients with advanced, life limiting diseases and their family members, we have
identified, from their perspectives, aspects of care that are a high priority for
improvement and which may have the greatest impact in improving overall end of life
care. Psychological interventions, spiritual support, better advance care planning,
improving the nature of physician, patient, and family relationships and enhancing
specific aspects of communication and decision making could help patients and their
families realize their right to quality care at the end of their lives. Such hypotheses
require empiric testing in future interventional studies.
16

Acknowledgments
We thank all members of CARENET who have contributed to the evolution and development of this work. We would also like to thank the following research assistants who helped in the development of this questionnaire and the execution of this study: Deborah Pichora, Jennifer Korol, Nancy Paul, Joanne Harvey, Sheilagh Mans, Joanne Young, Wendy Conrad, Norine Whalen, Pat Thompson, Jeanette Suurdt, Melissa TeBrake, Neala Hoad, Chantal Tessmer, Janice Palmer, and Annabelle Mathieu. D. Cook holds a Canada Research Chair with the Canadian Institutes of Health Research.
Funding StatementThis study was supported by the Canadian Researchers at the End of Life Network (CARENET). CARENET is supported by a grant from the Canadian Institutes of Health Research and Heart and Stroke Foundation of Canada.
Contributor’s Statement
Heyland, Day, Jiang, and Cohen designed the study protocol with input from other co-investigators. Heyland, Cook, Rocker, Dodek, Kutsogiannis, and Skrobik participated in acquisition, analysis, and interpretation of data and the writing of the manuscript.Jiang, Day, and Cohen were responsible for the analysis and critically reviewed the manuscript. All authors gave final approval of the version to be published
17
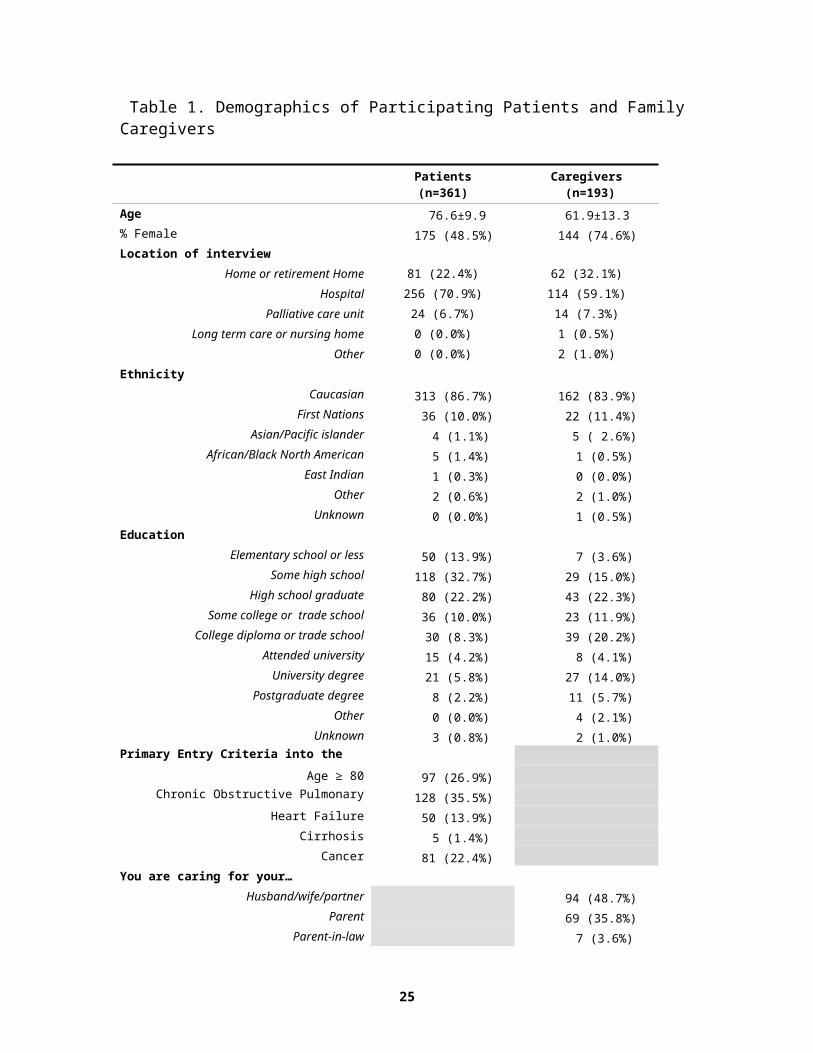
Table 1. Demographics of Participating Patients and Family Caregivers
Patients (n=361)
Caregivers (n=193)
Age 76.6±9.9 61.9±13.3% Female 175 (48.5%) 144 (74.6%)Location of interview
Home or retirement Home 81 (22.4%) 62 (32.1%)
Hospital 256 (70.9%) 114 (59.1%)
Palliative care unit 24 (6.7%) 14 (7.3%)
Long term care or nursing home 0 (0.0%) 1 (0.5%)
Other 0 (0.0%) 2 (1.0%)
Ethnicity
Caucasian 313 (86.7%) 162 (83.9%)First Nations 36 (10.0%) 22 (11.4%)
Asian/Pacific islander 4 (1.1%) 5 ( 2.6%)African/Black North American 5 (1.4%) 1 (0.5%)
East Indian 1 (0.3%) 0 (0.0%)Other 2 (0.6%) 2 (1.0%)
Unknown 0 (0.0%) 1 (0.5%)Education
Elementary school or less 50 (13.9%) 7 (3.6%)Some high school 118 (32.7%) 29 (15.0%)
High school graduate 80 (22.2%) 43 (22.3%)Some college or trade school 36 (10.0%) 23 (11.9%)
College diploma or trade school 30 (8.3%) 39 (20.2%)Attended university 15 (4.2%) 8 (4.1%)
University degree 21 (5.8%) 27 (14.0%)Postgraduate degree 8 (2.2%) 11 (5.7%)
Other 0 (0.0%) 4 (2.1%)Unknown 3 (0.8%) 2 (1.0%)
Primary Entry Criteria into the Study
Age ≥ 80 97 (26.9%)Chronic Obstructive Pulmonary Disease 128 (35.5%)
Heart Failure 50 (13.9%)Cirrhosis 5 (1.4%)
Cancer 81 (22.4%)You are caring for your…
Husband/wife/partner 94 (48.7%)Parent 69 (35.8%)
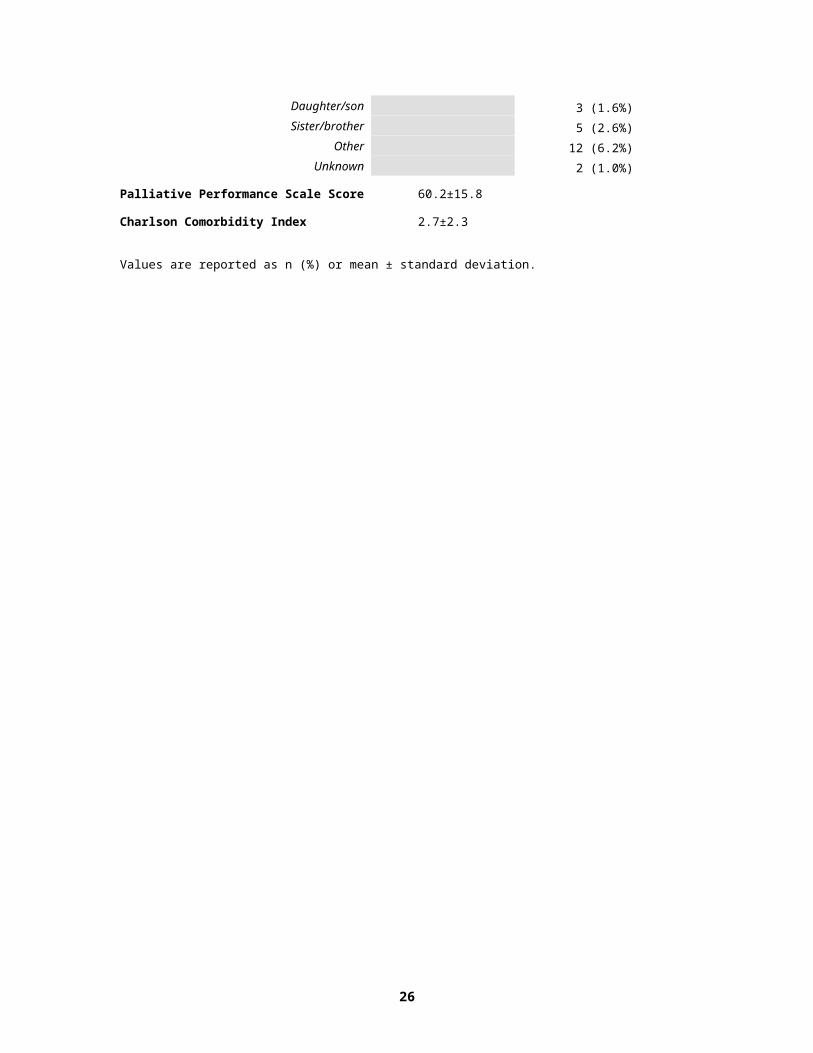
Parent-in-law 7 (3.6%)Daughter/son 3 (1.6%)Sister/brother 5 (2.6%)
18
Other 12 (6.2%)Unknown 2 (1.0%)
Palliative Performance Scale Score 60.2±15.8
Charlson Comorbidity Index 2.7±2.3
Values are reported as n (%) or mean ± standard deviation.
19

Table 2. High Priority Quality Improvement Items
Patients’ Perspective^ Family Caregivers’ Perspective*Spiritual/Emotional needs
38. How satisfied are you that you were at peace during the past month?
12. How satisfied are you that emotional problems you had during the past month (for example: depression, anxiety) were adequately assessed and controlled?
14. How satisfied are you that emotional problems (for example: depression, anxiety) your relative had during the past month were adequately controlled?
Relationship with Doctors3. How satisfied are you that your doctor(s) took a personal interest in you during the past month?4. How satisfied are you that your doctor(s) were available when you needed them (by phone or in person) during the past month?
5. How satisfied are you that the doctor(s) were available when you or your relative needed them (by phone or in person) during the past month?
Communication and Decision Making23. How satisfied are you that the doctor(s) listened to what you had to say during the past month?
26. How satisfied are you that the doctor(s) listened to what you had to say during the past month?
22. How satisfied are you that you received consistent information about your condition from all doctors and nurses looking after you during the past month?
24. How satisfied are you that you received consistent information about your relative’s condition from all the doctors and nurses looking after him or her during the past month?
21. How satisfied are you that doctor(s) explained things relating to your illness in a way you could understand during the past month?
25. How satisfied are you that you received updates about your relative’s condition, treatments, test results, etc. in a timely manner during the past month?27. How satisfied are you with discussions during the past month with the doctor(s) about where your relative would be cared for (in hospital, at home, or elsewhere) if he or she were to get worse?29. How satisfied are you with discussions during the past month with the doctor(s) about the use of life sustaining technologies (for example: CPR or cardiopulmonary resuscitation, breathing machines, dialysis)?
Illness Management
16. How satisfied are you that, during the past month, your relative received good care when you were not able to be with him/ her?
^ number corresponds to question on patient version of questionnaire as illustrated in on line Appendix Table 1.* number corresponds to question on family caregiver version of questionnaire as illustrated in on line Appendix Table 2.
20

Figure 1 – Performance-Importance Grid for Patient CANHELP Questionnaire
3.0 3.5 4.0 4.5 5.0
0.0
0.1
0.2
0.3
0.4
0.5
Satisfaction
Cor
rela
tion
Coe
ffici
ent w
ith G
loba
l Rat
ing
Sat
isfa
ctio
n Q
uest
ion
2
3
4
56
7 8
9
10
11
1213
14
35
29
15
16
17
18
2021
22
23
24
2526
27
28
30
19
31
32
33
34
3637
38
Legend: A plot of the mean patient satisfaction with care for each question on the CANHELP questionnaire and correlation of that question with overall satisfaction from the patient’s point of view. Corresponds to Table 1 in online Appendix. The gridlines are placed at the median value for the question means (4.12) and correlations (0.29).× indicate the actual location of the data and the number closest to the × is the CANHELP question number.

Appendix A:
Detailed Patient Eligibility Criteria
To be eligible for this study, patients had to be able to understand English or French, be
capable of giving informed consent, and meet the following criteria:
A. > 55 years of age and have one or more of the following diseases at an advanced
stage:
i) Moderate to severe chronic obstructive pulmonary disease (COPD) defined by
Canadian Thoracic Society (CTS) criteria. (29) Moderate COPD: shortness of breath
causing the patient to stop walking after 100 meters or a few minutes on level ground
(MRC score of 3-4) and one or more acute exacerbations of COPD requiring hospital
admission within the last year, an ICU admission, a forced expiratory volume in 1 sec
<30% predicted, or a body mass index < 21; Severe COPD: severe shortness of breath
resulting in the patient being too breathless to leave the house, or breathlessness after
dressing/undressing (i.e., Medical Research Council score29 of 5), or the presence of
chronic respiratory failure (PaCO2>45) or clinical signs of right heart failure.
ii) Congestive heart failure (CHF) defined as New York Heart Association class IV
symptoms or left ventricular function < 20%.
iii) Cirrhosis confirmed by imaging studies or documentation of esophageal varices and
at least one of three conditions: a) history of hepatic coma, b) Child’s class C liver
disease, or c) Child’s class B liver disease with gastrointestinal bleeding.
iv) Metastatic Cancer
OR
B. Any patient > 80 years of age in hospital who had a medical diagnosis as the primary
cause of admission;
OR
C. Any patient > 80 years of age who was enrolled in a home care program using long
term oxygen therapy and who had a primary diagnosis of COPD, CHF, or metastatic
cancer.
Family Caregiver Eligibility Criteria
For the purpose of this study, we defined an eligible family caregiver as a family member or close friend of an eligible patient who provided the most care to the patient and was not paid to do so, was greater than 18 years of age, understood English or French, and was competent to give informed consent.

Appendix B. Satisfaction Scores for Patient CANHELP Questionnaire in order of Relative Importance
Questions How satisfied are you ….
Pearson correlation coefficients
(Importance)
Satisfaction (Mean)
%Completely Satisfied
9. that you were treated by the doctors and nurses in a manner that preserved your sense of dignity during the past month? 0.46 4.37 50.28%
14. that during the past month, you received good care when a family member or friend was not able to be with you? 0.42 4.26 46.48%
10. with the tests that were done and the treatments that were given during the past month for your medical problems? 0.41 4.26 43.26%
16. that health care workers worked together as a team to look after you during the past month? 0.41 4.24 43.02%
8. that the doctors and nurses looking after you during the past month were compassionate and supportive? 0.41 4.24 42.34%
7. that the doctors and nurses who looked after you during the past month knew enough about your health problems to give you the best possible care? 0.40 4.22 45.22%
18. with the environment or the surroundings in which you were cared for during the past month? 0.38 4.22 43.14%
11. that physical symptoms you had during the past month (for example: pain, shortness of breath, nausea) were adequately assessed and controlled? 0.38 4.13 40.00%
22. that you received consistent information about your condition from all doctors and nurses looking after you during the past month? 0.37 4.05 37.96%
19. that the care and treatment you received during the past month was consistent with your wishes? 0.36 4.41 57.34%
12. that emotional problems you had during the past month (for example: depression, anxiety) were adequately assessed and controlled? 0.34 3.95 38.58%
4. that your doctor(s) were available when you needed them (by phone or in person) during the past month? 0.34 3.92 36.41%
13. with the help you received with personal care during the past month (for example: bathing, toileting, dressing, eating)? 0.34 4.29 46.07%
6. with the level of trust and confidence you had in the nurses who looked after you during the past month? 0.33 4.44 55.59%
38. that you were at peace during the past month? 0.32 3.77 33.33%5. with the level of trust and confidence you had in the doctor(s) who looked after you during the past month? 0.32 4.24 50.42%
3. that your doctor(s) took a personal interest in you during the past month? 0.30 3.96 36.49%
21. that the doctor(s) explained things relating to your illness in a way you could understand during the past month? 0.29 4.08 42.02%
23. that the doctor(s) listened to what you had to say during the past month? 0.29 3.99 38.66%
20. that the doctor(s) explained things relating to your illness in a straightforward, honest manner during the past month? 0.29 4.13 42.94%
2. that you knew the doctor(s) in charge of your care during the past month? 0.27 3.70 32.78%
24. that you received updates about your condition, treatments, test results, etc. in a timely manner during the past month? 0.26 3.90 33.05%
15. with the home care services you received during the past month? 0.23 4.14 47.51%
28. with your role during the past month in decision making regarding your medical care? 0.22 3.97 37.78%
32. that your relationships with family members and others you care about were strengthened during the past month? 0.22 4.16 44.48%
35. with the level of confidence you felt during the past month in your own ability to manage your illness? 0.21 3.18 14.53%
26. with discussions during the past month with your doctor(s) about the use of life sustaining technologies (for example: CPR or cardiopulmonary resuscitation, breathing machines, dialysis)?
0.21 3.67 34.88%
25. with discussions during the past month with your doctor(s) about where you would be cared for (in hospital, at home, or elsewhere) if you were to get worse?
0.19 3.65 31.75%
37. that you did special things you wanted to do during the past month (for example: resolve conflicts, complete projects, participate in special family events, travel)?
0.19 3.08 18.29%
36. that you were able during the past month to contribute to others in a meaningful way? 0.18 3.52 24.50%
27. that, during the past month, you have come to understand what to expect in the end stage of your illness (for example: in terms of symptoms and comfort measures)?
0.17 3.41 28.65%
17. that you were able to manage the financial costs associated with your illness during the past month? 0.17 4.12 50.56%
33. that during the past month you were not a burden on your family or others you care about? 0.15 3.76 35.69%
30. with discussions during the past month, involving a family member or someone who would make decisions for you, about your wishes for future care in the event you yourself are unable to make those decisions?
0.15 4.26 57.26%
29. with the level of confidence you felt during the past month in the ability of a family member or friend to help you manage your illness? 0.12 3.97 42.12%
34. that you had family or friends to support you when you felt lonely or isolated during the past month? 0.11 4.23 50.85%
31. that you were able during the past month to talk comfortably about your illness, dying, and death with the people you care about? 0.06* 4.12 46.69%
Legend: The Pearson Correlation Coefficient is between individual questions and the global rating of satisfaction. These coefficients are all statistically significant except where denoted with an asterisk (* p>0.05). The higher the coefficient, the more ‘important’ the question is as it has a stronger relationship with overall satisfaction. Questions reported in order of highest to lowest importance. Satisfaction scores can range from 0-5, with higher scores indicating more satisfied where ‘5’ = ‘completely satisfied.’ The highlighted rows are those that are considered high priority quality improvement targets.
Appendix C. Satisfaction Scores From Family Caregivers’ Perspective in Order of Relative Importance to Overall Satisfaction with Care Provided to Family Caregiver
Questions How satisfied are you…
Pearson correlation coefficients
(Importance)
Satisfaction (Mean)
%Completely Satisfied
6. with the level of trust and confidence you had in the doctor(s) who looked after your relative during the past month? 0.58 4.05 38.22%
5. that the doctor(s) were available when you or your relative needed them (by phone or in person) during the past month? 0.55 3.82 31.25%
10. that the doctors and nurses looking after your relative during the past month were compassionate and supportive of you? 0.53 3.95 31.41%
9. that the doctors and nurses looking after your relative during the past month were compassionate and supportive of him or her? 0.51 4.26 42.71%
4. that the doctor(s) took a personal interest in your relative during the past month? 0.50 3.95 33.85%
8. that the doctors and nurses who looked after your relative during the past month knew enough about his or her health problems to give the best possible care?
0.46 4.08 33.33%
15. with the help your relative received with personal care during the past month (for example: bathing, toileting, dressing, eating)? 0.46 3.96 37.70%
24. that you received consistent information about your relative’s condition from all the doctors and nurses looking after him or her during the past month?
0.46 3.85 31.58%
26. that the doctor(s) listened to what you had to say during the past month? 0.46 3.86 30.69%
22. that the doctor(s) explained things relating to your relative’s illness in a straightforward, honest manner during the past month? 0.44 4.03 36.65%
25. that you received updates about your relative’s condition, treatments, test results, etc. in a timely manner during the past month? 0.44 3.66 23.56%
14. that emotional problems (for example: depression, anxiety) your relative had during the past month were adequately controlled? 0.44 3.59 20.86%
16. that, during the past month, your relative received good care when you were not able to be with him/ her? 0.41 3.79 30.89%
11. that your relative was treated by those doctors and nurses during the past month in a manner that preserved his or her sense of dignity? 0.40 4.22 41.97%
27. with discussions during the past month with the doctor(s) about where your relative would be cared for (in hospital, at home, or elsewhere) if he or she were to get worse?
0.40 3.61 30.43%
31. with your role during the past month in decision-making regarding your relative’s medical care? 0.40 3.98 38.50%
13. that physical symptoms (for example: pain, shortness of breath, nausea) your relative had during the past month were adequately controlled? 0.40 4.03 35.23%
18. that health care workers worked together as a team to look after your relative during the past month? 0.38 4.10 33.86%
21. that the care and treatment your relative received during the past month was consistent with his or her wishes? 0.38 4.19 41.80%

29. with discussions during the past month with the doctor(s) about the use of life sustaining technologies (for example: CPR or cardiopulmonary resuscitation, breathing machines, dialysis)?
0.38 3.68 37.22%
23. that the doctor(s) explained things relating to your relative’s illness in a way you could understand during the past month? 0.36 4.05 37.50%
7. with the level of trust and confidence you had in the nurses who looked after your relative during the past month? 0.36 4.23 41.97%
12. with the tests that were done and the treatments that were given during the past month for your relative’s medical problems? 0.33 4.07 34.90%
17. with recent home care services your relative received? 0.30 3.89 39.38%20. with the environment or the surroundings in which your relative was cared for during the past month? 0.29 3.94 26.56%
3. that you knew the doctor(s) in charge of your relative’s care during the past month? 0.29 3.67 27.98%
32. with discussions with your relative during the past month about wishes for future care in the event he or she is unable to make those decisions? 0.28 3.96 42.16%
19. that you were able to manage the financial costs associated with your relative’s illness during the past month? 0.26 4.07 44.21%
38. that you were able during the past month to contribute to others in a meaningful way ? 0.25 3.81 32.45%
30. that, during the past month, you have come to understand what to expect at the end stage of your relative’s illness (for example: in terms of symptoms and comfort measures)?
0.24 3.62 28.11%
36. that during the past month you had enough time and energy to take care of yourself? 0.23 3.29 17.02%
40. that you were at peace during the past month? 0.23 3.33 19.68%34. that your relationship with your relative was strengthened during the past month? 0.23 4.14 47.09%
37. that you had family or friends to support you when you felt lonely or isolated during the past month? 0.21 4.04 43.39%
33. that you were able during the past month to talk comfortably with your relative about his/ her illness, dying, and death? 0.18 3.86 38.10%
39. that you and your relative did special things (for example: resolve conflicts, complete projects, participate in special family events, travel) you wanted to do during the past month?
0.16 3.14 20.11%
35. with the level of confidence you felt during the past month in your relative’s ability to manage his/her own illness? 0.14 2.72 8.90%
28. with the level of confidence you felt during the past month in your ability to help your relative manage his/ her illness? 0.12* 3.67 25.00%
Legend: The Pearson Correlation Coefficient is between individual questions and the global rating of satisfaction. These coefficients are all highly statistically significant except where denoted with an asterisk (* p<0.05). The higher the coefficient, the more ‘important’ the question is as it has a stronger relationship with overall satisfaction. Questions reported in order of highest to lowest importance. Satisfaction scores can range from 0-5, with higher scores indicating more satisfied where ‘5’ = ‘completely satisfied.’ The highlighted rows are those that are considered high priority quality improvement targets.
Appendix D. Performance-Importance Grid for Family CANHELP Questionnaire
2.5 3.0 3.5 4.0 4.5 5.0
0.0
0.1
0.2
0.3
0.4
0.5
0.6
Satisfaction
Cor
rela
tion
Coe
ffici
ent w
ith G
loba
l Rat
ing
Sat
isfa
ctio
n Q
uest
ion
3
4
5
6
7
8
910
11
12
13
1415
16
35
28
17
18
19
20
22
23
242625
27
29
30
31
32
21
33
3436 37
38
39
40
Legend: A plot of the mean satisfaction with care provided to family caregiver for each question on the CANHELP questionnaire and correlation with that question and overall satisfaction from the family caregiver’s point of view. Corresponds to Table 2 in online Appendix. The gridlines are placed at the median value for the question means (3.94) and correlations (0.38).× indicate the actual location of the data and the number closest to the × is the CANHELP question number

References
1. Carstairs S, Beaudoin GA. Quality End of Life Care: The Right of Every Canadian. 2000; Ottawa Ont. Government of Canada
2. Heyland DK, Groll D, Rocker G, Dodek P, Gafni A, Tranmer J, Pichora D, Lazar N, Kutsogiannis J, Shortt S, Lam M, for the Canadian Researchers at the End of Life Network (CARENET). End of life care in acute care hospitals in Canada: A quality finish? J Palliat Care 2005(Autumn);21(3):142-150.
3. Carstairs S. Still Not There. Quality End-of-Life Care: A Progress Report. 2005;Ottawa ON. Government of Canada
4. Workman S and Mann OE. ‘No control whatsoever’: end-of-life care on a medical teaching unit from the perspective of family members. Q J Med 2007: 433-440.
5. Giles S. Palliative stage Parkinson’s disease: patient and family experiences of health-care services. Palliat Med 2009; 23: 120-125.
6. TIME: Toolkit of Instruments to Measure End-of-life care. Satisfaction with Quality of Care. www.cher.brown.edu/pcoc/satisfac.htm. 2002.
7. Lo B. Improving care near the end of life. Why is it so hard? JAMA 1995;274:1634-1636.
8. Mularski R, Dy S, Shugarman L, Wilkinson A, Lynn J, Shekelle P, et al. Systematic Review of Measures of End-of-Life Care and Its Outcomes. Heath Serv Res 2007;42:1848–1870. 9. Heyland DK, Dodek P, Rocker G, et al. for the Canadian Researchers at the End of Life Network (CARENET). What matters most in end-of-life care: Perceptions of seriously ill patients and their family members. Can Med Assoc J 2006(Feb);174(5):627-633.
10. Heyland DK, Cook D, Rocker G, Dodek P, Kutsogiannis DJ, Skrobik Y, Jiang X, Day A, Cohen R. The Development of a Novel Questionnaire to Measure Patient and Family Satisfaction with End of Life Care: The Canadian Health Care Evaluation Project (CANHELP) Questionnaire. Journal of Palliative Care 2010 (in press).
11. Heyland DK, Frank C, Tranmer J, Paul N, Pichora D, Jiang X, Day A. Satisfaction with end of life care: A longitudinal study of patients and their family caregivers in the last months of life. J Palliat Care 2009;25(4):245-256.
12. Heyland DK, Cohen R, Skrobik Y, Harvey J, Pichora D. Content validity and acceptability of “CANHELP” satisfaction instruments for French speaking patients with end-stage medical disease or metastatic cancer. J Palliative Care 2006;22(3):P153.

13. Anderson F, Downing GM, Hill J, Casorso L, Lerch N. Palliative performance scale (PPS): a new tool. J Palliat Care 1996: 12(1): 5-11.
14. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J Chron Dis 1987: 40(5): 373-383.
15. Dodek PM, Heyland DK, Rocker G, Cook DJ. Translating family satisfaction data into quality improvement. Crit Care Med 2004;32(9):1922-1927.
16. Ingram BBL and Chung RS. Client Satisfaction Data and Quality Improvement Planning in Managed Mental Health Care Organizations. Health Care Manage Rev 1997;22:40-52
17. Goodridge D, Bond JB, Cameron C, McKean E. End of life care in a nursing home: a study of family, nurse, and health care aide’s perspectives. Int J of Palliat Nurs 2005;11: 226-32.
18. Vohra JU, Brazil K, Hanna, Abelson J. Family perceptions of end of life care in long-term care facilities. J Palliat Care 2004;20:297-302.
19. Chochinov HM, Krisjanson L, Hack T, Hassard T, McClement S, Harlos M. Dignity in the terminally ill : Revisited. J Palliat Med 2006;9:666-72.
20. Hanson LC, Danis M, Garrett J. What is wrong with end of life care? Opinions of bereaved family members. J Am Geriatr Soc 1997;45:1339-1344.
21. Curtis JR, Patrick DL, Engelberg RA, Norris K, Asp C, Byock I. A measure of the quality of dying and death: Initial validation using after-death interviews with family members. J Pain and Symptom Management 2002;24:17-30.
22. Malacrida R, Bettelini CM, Degrate A, Martinez M, Badia F, Piazza J, et al. Reasons for dissatisfaction: A survey of relatives of intensive care unit patients who died. Crit Care Med 1998;26:1187-1193.
23. Kuhl D. What dying people want: Practical wisdom for the end of life. Toronto: Doubleday Canada. 2002.
24. Breitbart, W., Bruera, E., Chochinov, H. & Lynch, M. (1995). Neuropsychiatric syndromes and psychological symptoms in patients with advanced disease. Journal of Pain and Symptom Management, 19, 131-141.
25. Kissane, D.W., Breitbart, W. & Prigerson, H.G. (2009). Do rates of mental disorders and existential distress among advanced stage cancer patients increase as death approaches? Psycho-Oncology, 18(1), 50-61.

26. Greisinger AJ, Lorimor RJ, Aday LA, Winn RJ, Baile WF. Terminally ill cancer patients: their most important concerns. Cancer Pract 1997;5:147–154.
27. Bolmsjo I. Existential Issues in Palliative Care: Interviews of Patients with Amyotrophic Lateral Sclerosis. Journal of Palliative Medicine 2001:4:499-505.
28. LeMay K, Wilson KG. Treatment of existential distress in life threatening illness: A review of manualized interventions. Clinical Psychology Review 2008: 28:472-493.
29. O'Donnell DE, Aaron S, Bourbeau J, Hernandez P, Marciniuk DD, Balter M, et al. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease - 2007 update. Can Respir J. 2007 Sep;14 Suppl B:5B-32B.









