-
8/7/2019 New E-Service Development in the Home Care Sector:
Beyond Implementing a Radical Technology
1/11
This article appeared in a journal published by Elsevier. The
attached
copy is furnished to the author for internal non-commercial
research
and education use, including for instruction at the authors
institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling
or
licensing copies, or posting to personal, institutional or third
partywebsites are prohibited.
In most cases authors are permitted to post their version of
the
article (e.g. in Word or Tex form) to their personal website
or
institutional repository. Authors requiring further
information
regarding Elseviers archiving and manuscript policies are
encouraged to visit:
http://www.elsevier.com/copyright
http://www.elsevier.com/copyrighthttp://www.elsevier.com/copyright
-
8/7/2019 New E-Service Development in the Home Care Sector:
Beyond Implementing a Radical Technology
2/11
Author's personal copy
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f
o r m a t i c s 7 7 ( 2 0 0 8 ) 679688
j o u r n a l h o m e p a g e : w w w . i n t l . e l s e v i e
r h e a l t h . c o m / j o u r n a l s / i j m i
New e-service development in the homecare sector: Beyond
implementing a radical technology
Anna Essen a,, Moya Conrick b,1
a School of Business, University of Stockholm, Stockholm,
Swedenb School of Nursing, Griffith University, Nathan, Brisbane
4111, Australia
a r t i c l e i n f o
Article history:
Received 4 September 2007
Received in revised form
22 February 2008
Accepted 27 February 2008
Keywords:
Elderly homecare services
Technology
Organizational innovation
Telemedicine
Smart home technology
Aged care
a b s t r a c t
Purpose: This paper explores the constituents of and challenges
related to the innovation of
technology-based services in the long-term homecare sector.
Methods: This research used purposeful extreme case sampling, a
mixed methods approach
to research that included focus groups and interviews, to learn
from the experiences of
an innovative telehomecare project. The paper uses a framework
that integrates service
management; information systems innovation and medical
informatics theory.
Results: Thefindingsindicatethatthe claimed andthe
ratherabstractbenefitsof thetechnol-
ogy espoused by information technology vendors were difficult to
transform into a service
concept. The organization studied is still struggling with
conflicts between technological
possibilities on the one hand, and the prevailing service
delivery systems and user prefer-
ences on theother. Decisionsabout theextent to whichthe service
needs to be reengineered,
what non-technology resources are required, what should be the
role of the consumer in
the new care process and identifying who is actually the primary
beneficiary and user of
the new service remain.
Conclusions:A comprehensive development model and mindfulness is
necessary for radical
service innovation in the long-term homecare sector. Creating
new services that exploit
the capability of radical technical innovations requires
organizational development and the
use of many non-technology innovations and resources. To
understand what combinations
of technological and non-technological resources can provide
sustainable benefit, all key
internal and external stakeholders must be involved from the
beginning of the project.
2008 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Numerous international reports emphasize the need to
develop new models of care service delivery to deal with
the escalating demands and massive increase in costs in the
healthcare sector [1,2]. The potential for new information
and
communications technology (ICT) to underpin these mod-
els has been mooted, especially in the long-term homecare
Corresponding author. Tel.: +46 8 16 11 83; fax: +46 8 674 74
40.E-mail address: [email protected] (A. Essen).
URLs: http://www.annaessen.blogspot.com/ (A. Essen),
http://members.optusnet.com.au/conrick/index.html (M. Conrick).1
Moya Conrick passed away in January 2008. She was a very special
person and an excellent co-author. This paper is dedicated to
her.
setting [35]. While there is a growing body of technology-
oriented literature discussing telehomecare or smart home
technologies for seniors [6], less attention has been paid
to
organizational perspectives in this context. That is,
research
has focused on the technical accuracy of specific telehome-
care applications rather than highlighting more general
issues
related to how organizations can develop effective ways of
using such technologies in their everyday work [3,6].
1386-5056/$ see front matter 2008 Elsevier Ireland Ltd. All
rights reserved.doi:10.1016/j.ijmedinf.2008.02.001
-
8/7/2019 New E-Service Development in the Home Care Sector:
Beyond Implementing a Radical Technology
3/11
Author's personal copy
680 i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i
n f o r m a t i c s 7 7 ( 2 0 0 8 ) 6 7 9 6 8 8
This paper seeks to redress this imbalance particularly in
the telehomecare area, by shifting the focus from technology
to the innovation of new care services. It highlights the
issues
involved in the process of integrating telehomecare technol-
ogy in the daily delivery of long-term elderly care
services.
The paper is organized into five sections. These present:
theresearch background and the frameworks used; data genera-
tion and analysis methods; empirical findings; discussion
and
conclusions.
1.1. Background
This research was undertaken in Sweden where community
care providers are responsible for serving the broad group
of
seniors who need general help with managing their everyday
life at home, as opposed to providing hospital care to
patients
who have medical needs. It was triggered by a group of man-
agers in a community care organization who envisioned that
information technology (IT) could enable them to use theirscarce
resources more effectively.
They decided to invest in an in-home monitoring system
that continuously monitors the activity level of seniors.
This
system is sensor-based and would not require any active
input
from the senior (and computer illiterate) beneficiaries of
care.
The managers identified that this area of information tech-
nology may hold some of the answers to their resourcing
challenges, they had no explicit strategy concerning how to
use it or how to develop new IT-based services on basis of
it.
This paper is based on a case study that focused on how this
new telehomecare technology was introduced in the organi-
zation. It elicits the elements and challenges associated
with
this process in the public elderly care context.
1.2. Frameworks
Research on the use of remote and sensor-based telemoni-
toring to enhance long-term elderly homecare is scarce in
the medical informatics literature [5]. However research
about
implementations of healthcare information systems (HIS)
more generally provides insights that are relevant to this
con-
text. This literature has increasingly broadened its focus
from
the technical to the socio-technical dimensions of
information
systems suggesting that the success of IT implementations
not only depend on the quality of hard- and software used
[79,39]. The literature also argues that organizational fac-tors
are also the key to success [1012]. Several organizational
prerequisites for successful IT implementations are iden-
tified by a number of authors and these include financial
and structural support, mobilizing champions during imple-
mentation, involving, educating and motivating users, and
dealing with confidentiality, standardization and
legal-related
issues [7,10,11,1319]. In general, the importance of embed-
ding thetechnology in practice is underlined andthis
involves
a mutual adjustment of both technology and care practices
[7,13,16,17,20,21]. These are crucial insights that inform
the
current research. However, while claims about the impor-
tance of introducing the technology with consideration to
the
organizational context abound, there are still uncertainties
as
regards how this can be achieved in actual work settings
[10].
This is particularly the case as regards the use of telehealth
in
the care of frail elderly living in their ordinary homes.
Indeed,
there is a lack of studies that outline the issues involvedin
the
organization of telehealth technologies into long-term
elderly
carepractice and the wider public careservicedelivery [10].
We
argue thatthis is a questionof e-service innovation and
believe
that the service management and information systems liter-ature
provide insights helpful in this context. Theories from
this body of literature were drawn on to create a functional
framework for the present study.
At the heart of new e-service development is innovation.
This is broadly defined as an idea, artifact, or behavior that
is
new to the organization adopting it [22,23,38]. Edvardsson
and
Olsson [24] suggested that at general level, service
innovation
includes the development of: (1) the service concept
(consumers
needs and how these are to be satisfied); (2) the service
sys-
tem (static resources required, the organizational, physical
and
technical environment); and (3) the service process (the
chain
of activities that must occur for the service to function).
As
regards to how these dimensions should be innovated studieson
new product/service development proposed a number of
success factors. These include engaging in internal communi-
cation, in particular involving front-line employees [2528]
and
engaging in external communication with consumers, suppli-
ers, competitors and other stakeholders in all stages of the
innovation process. It has been argued that this leads to
more
comprehensive and varied information and thus to a higher
performing development process [2934].
While the service management literature provides insights
about the issues involved in service innovation, it says
little
about the specificity of using a new technology that may
con-
stitute a radical innovation. However,the information
systems
(ISs) literature is helpful in this context. What emerges
fromthis literature resonates with argument in the medical
infor-
matics literature, namely that introducing new ICT systems
in an organization often entails changes in work process and
the organizational structure as well as in the ICT system
itself
[35,36]. Swanson andRamiller [37] identify the issues
involved
in this process. In their model, an organizations interest
in
new technology is often sparked by an organizing vision,
which is describedas the decontextualizedand general advan-
tages of a new technology and often espoused by groups such
as technology vendors, consultants and academics. The orga-
nizing vision typically defines the IT system in broad
strokes,
which helps to legitimize it [36,37]. A mindful organization
is not seduced by the organizing vision but will
objectivelyevaluate a systems suitability for their needs. This is
what
Swanson and Ramiller [37] refer to as comprehension.
Ifadoption
is entertained, a deeper consideration of the system
follows.
Here a context-adjusted supportive rationale is developed by
paying attention to issues specific to the organization. The
implementation phase involves a myriad of considerations,
choices, and actions (p. 557). The mindful enterprise will
make adaptations during implementation in either the sys-
tem or organization to address unanticipated problems or
realize unforeseen potential. A reliance on expertise over
for-
mal authority and a readiness to relax formal structure is
important in this stage. Assimilation commences as the IT
sys-
tem is absorbed into the organizations work practices and
its
usefulness is demonstrated. In time, the innovation becomes
infused and routine [37].
-
8/7/2019 New E-Service Development in the Home Care Sector:
Beyond Implementing a Radical Technology
4/11
Author's personal copy
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f
o r m a t i c s 7 7 ( 2 0 0 8 ) 6 7 9 6 8 8 681
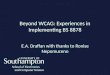
Fig. 1 An ideal framing of the process of innovating
technology-based services.
Combining insights from Swanson and Ramillers [37] ideal
model of IS innovation and Edvardsson and Olssons [24]
model of new service development, the framework in Fig. 1
was created. This depicts an ideal innovation process and
has been inspired by the service management, information
systems innovation and medical informatics literature. This
framework has been used in the generation and analysis of
empirical data in this study.
2. Method
This study forms part of a larger research program on tech-
nology in elderly care. It is based on empirical data
collected
over several years (20032006) during a Smart Home Devel-
opment project in a small municipal care organization in
Sweden. It uses purposeful extreme case sampling; satisfy-
ing the requirements for this method by selecting a case
that
was information rich andspecial in some way [40,41].Acase
study approach allowed the researcher to follow the service
innovation process over time and to use a variety of
informa-
tion sources [42].
Participants in the study included the Home-help man-
agers and Home-helpers involved in the development projectfrom
its inception. The primary researcher (and author) gath-
ered data using e-mail, phone and large numbers of formal
andinformal meetings (31meetings) over a 3-yearperiod. This
was followed by 10 semi-structured, face-to-face interviews
with operational and management personnel in the organiza-
tion who hadbeen directly involved in making theinvestment
decision and/or using the technology. Except for one section
manager, there wasno turnover of personnel during the study
period. The researcher used an interview schedule that con-
tained both open and closed ended questions (see Appendix
A). One hour long non-participant observation of employees
using the new technology was also performed at five occa-
sions.
Data were analyzed, using a combined inductive and
deductive approach [43,44]. The authors departed from the
theoretical framework at an overall level while attempting
to
inductively infer andbe attentive to themes emerging fromthe
empirical material. In all, the analysis process went
through
three iterative rounds of culling the interviews, consulting
the tentative framework, adjusting the analysis and refining
conclusions as required by the research approach [45]. The
findings presented here represent broader sets of empirical
data; the quotes chosen are typical for the interviews and
observation. The names of respondents are excluded for pur-
poses of confidentiality and the study fully complied with
ethical standards for this type of research and was approvedby
the Regional Research Ethics Committee of Stockholm.
It should be noted that in this paper the term The Man-
ager is used for the person making the corporate decisions
and interviewed separately while the term managers refers
to the group of section managers in the organization.
3. Results
The results of this study must be considered in light of the
municipal care organization managers lack of an explicit
strategy concerning how to develop newIT-based services and
their scant knowledgeabout the technologies available. In
thisenvironment, it is not surprising that this study found the
development process used by the organization deviated from
the ideal framework presented in Fig. 1. In
thecurrentclimate
this is probably not a unique circumstance.
3.1. Comprehension and adoption
The managers scanned the market for potential healthcare
technologies and in doing so uncovered a vast number of
radical technologies in the market. They rejected many prod-
ucts because they focused on providing new medical services
to certain groups of chronic patients at home, as a way of
reducing hospital admissions. Few products were promoted
as providing benefits for either the senior consumers mar-
ket or personnel in this non-medical, long-term care
context.
-
8/7/2019 New E-Service Development in the Home Care Sector:
Beyond Implementing a Radical Technology
5/11
Author's personal copy
682 i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i
n f o r m a t i c s 7 7 ( 2 0 0 8 ) 6 7 9 6 8 8
The managers finally selected an activity monitoring system,
which they thought would bring benefits to the broad group
of homebound seniors in general and independent of their
medical diagnosis. Twenty-three units were purchased. These
units replaced the pendant safety alarms that were currently
in use.The system included monitoring units worn on the
wrist,
in similar fashion to traditional alarms. They offered sim-
ilar functionality to traditional alarms with a button that
seniors press in an emergency situation. The new units also
included sensors that continuously monitored non-critical
activity level, which indicated the sleep/wake rhythm of the
seniors. These sensors detect and send automatic alarms to
healthcare personnel if significant changes in activity
level
are detected for example, if a person is inactive due to a
fall.
The systems could provide both non-emergency and emer-
gency information, something that the managers found very
appealing. Because data could be continuously gathered by
remote sensing and subsequently presented in graphical formfor
analysis either in real time or retrospectively, they believed
that the technology represented a radical new way of under-
standing the health-state and needs of their consumers.
3.1.1. Translating the organizing vision into concrete
benefits
Thetechnologywas adopted after thevendor assurance that it
could enhance the organizations capacity to ensure the
safety
of seniors and act as a preventive measure. The Manager
was convinced that seniors would feel safe in their homes,
knowing that they were monitored and that the information
collected by the technology would enable the organization
to know their seniors and their needs better. Initially,
TheManager saw the potential for the information provided by
the system to be used in developing customized care ser-
vice processes. For example, if the client had a disturbed
night Home-helpers could let this senior sleep a bit longer
in the morning and prepare the breakfast one hour later than
usual. . . [The Manager, Group meeting, 2005]. Beyond this,
the
benefit was unclear; The Manager reported that they found it
difficult to predict. . . At this stage, the implicit
understanding
was that the detailed advantage of the monitoring technology
would emerge along with the personnel starting to use it. .
.
[Interview 8, 2006].
3.2. Implementation
The managers were involved in the purchase of the new
technology. However, they werenot engaged in the implemen-
tation phase, which involved many decisions related to the
configuration of the technology as well as decisions related
to
the adjustment of the organization.
3.2.1. Adjusting the technological infrastructure
The system included many features that could be applied and
customized to each individual, or they could be kept latent.
It was possible to configure the technology so that various
alarms were triggered for example, if the senior leaves the
apartment. The decision on what software features to
activate
was delegated to the front-line employees; the home-health
aids and their group leader. Their decision was to use only
the
most basic functions and to send alarms to the home-health
aids on duty in the same manner as the traditional alarm
this
new system was replacing.
Only the home-health aids were given access to the
information showing seniors longitudinal activity patterns
although this non-emergency activity information could bemade
available to others like. The seniors general practi-
tioner and family. As these external parties were not
involved,
their potential needs and roles are not discussed. Ideally,
organizational issues should have been dealt with before the
implementation of the system, as the reconfiguration of the
system is a way of implementing these roles [24]. In this
researchknowledge of allthe internal andexternal actorswho
were to use the system was extraneous and therefore a model
of usage and workflow was not mapped.
3.2.2. Adjusting the organizational infrastructure
The managers were not engaged in developing an organiza-
tional infrastructure supporting the use of the
newmonitoringtechnology. . . .Tasks need to be performed, butwe
neverreally
decided who should do what, and we never really allocated
resources to this. . . [The Manager, Interview 5, 2006].
Hence, the myriad of choices related to how to use the new
technology and who should use it were delegated to opera-
tional personnel. Thispresentedthis group of personnel witha
number of challenges. For one, they did not possess the
power
to provide resources for the new service system: The Group
Leader explained: . . .I cannot employ new personnel. . .I
have
been able to spend time on themonitoringsystem byspending
less time on other tasks. . . [Interview 2, 2006]. It was
decided
informally thatthe Group Leader should install themonitoring
units in the senior households and no maintenance routineswere
developed to cover for when this person was away.
There were four automatic alarms sent by the equipment
during the study period and in all of these cases healthcare
personnel responded in exactly the same way as for the old
system; that is, two Home-helpers immediately drove to the
seniors residence to check on them. In none of these cases,
there was a real emergency. Alarms were rather caused by
various more subtle reasons such as seniors being unusually
weak. The seniors were happy to be paid a visit at these
occa-
sions. There was no routine for examining the longitudinal
non-emergency information gathered by the system. Conse-
quently a Home-helper [Interview 3, 2006] reported, . . .I
look
now and then, when I have a free moment. . .
. The GroupLeader was the most frequent user of the data
devoting a few
minutes to analyze them every third day.
The Group Leader reported findings of abnormal activity
patterns or seniors not wearing their alarm to the Home-
helpers on duty. The system was effective in identifying
these
anomalies but work process remained the same. That was,
during their next scheduled visit the seniors not
consistently
wearing their monitor were reminded to do so. Additional
vis-
its were not activated based on the activity information.
This
was partially due to the Home-helpers being time poor and
unable to providenew or extended serviceswithin theirtight
schedules. These workers lack the authority to change or add
to the services they deliver. Social workers make these
deci-
sions and their budget is provided by government and funds
predefined needs with pre-determined services. Maintaining
-
8/7/2019 New E-Service Development in the Home Care Sector:
Beyond Implementing a Radical Technology
6/11
Author's personal copy
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f
o r m a t i c s 7 7 ( 2 0 0 8 ) 6 7 9 6 8 8 683
a normal activity pattern among seniors is notseen as a part
of this. A home-health aid talked about her limited
possibil-
ities to attend to activity or sleeping disorders illustrated
by
the activity curves:
. . .
There is not much one can do though. I may ask thesenior how he
has been sleeping lately and may ask if he
has sleeping medication etc during my scheduled visit. Of
course, there is much more that one would like to do. For
example activate those seniors who are too often inactive
during the day this would most likely make them sleep
better during night. . .but there is no time for that. . .I
can
onlyprovide services thatare formally granted by the social
workers. . .
[Home-helper, informal meeting, 2005]
In some cases the personnelalso had difficulty interpreting
the problems detected by the system and deciding how to
respond to them.
. . . how long is it normal to have a low activity level?
Some seniors may need a lot of rest while in other cases
low activity level can be a signal that something is wrong
health-wise. . .a sign of depression. . . something that
could
get worse if we do nothing about it. . .but we dont want to
turnthe seniors intohypochondriacs. . . preventive services
are not easy. . .
[Home-helper, Interview 6, 2006].
Home-helpers werehesitant to intervene in the non-urgent
reports. They describe notknowinghow to approachthe client
without sounding as if they were watching them in a nega-
tive big brother sense and without alarming the senior. This
applied to activity information as well as to information
about
those not wearing their alarms.
. . .If an activity curve indicate that something is not OK,
you feel like asking the senior about this. . . But we
cannot
say to a senior that We have seen on the curves that you
are very inactive during the days. This might make the
seniors feel watchedin a negative sense. . .howdoyouaska
senior about her activity level without sounding strange? It
is easy to make seniors worried. . .we found it very
difficult
to define a routine for this. . .
[Group Leader, Informal meeting, 2006]
. . .
I saw that Anton neverwears hisalarmduring thenight.I told one
of the girls to remind him to wear his alarm dur-
ingher regular visit, butshe didnot really know what to say
to him. She didnt want to say that we can see if he wears
it or not. However she managed to tell him in a nice way
and now wesee on the curves that he is always wearing his
alarm. . .
[Group Leader, Personal communication, 2006]
The seniors were informed about the new service via letter
and phone. The personnel had not given much thought to fur-
ther educating the seniors, fearing that this would make the
seniors worried and confused [Group Leader, Project meeting,
2005]. They implicitly assumed that the monitoring technol-
ogy was passive and did not require any input from the user.
As a result, a few of the seniors described being unclear as
to
what to expect from the new service or how they should use
it. Some began to over rely on the technology, believing
that
it could detect any change in their health status. For
example
one Home-helper reported that:
. . .
Jim told me he had felt really bad before my visit. Buthe didnt
call for help, or press the alarm button, as he
thought the technology would notice this. You could see
this on the computer, couldnt you he said. . .but of course
we couldnt. . .
[Interview 1, 2006].
In this case, the Home-helper tried to make clear to the
seniors the limits of the new technologywithout eroding
the seniors faith in the new technology completely. A true
challenge.
3.3. Assimilation
The general claims that inspired the managers adoption of
themonitoring technology were not shared by the operational
employees. They generated their own ideas about the benefits
that could flow from using the technology. Some of these
were
expected while others were unforeseen.
Not surprisingly, the operational employees believed that
the new automatic inactivity emergency alarm function could
increasetheir responsiveness in certain emergency
situations,
particularly if the person was physically unable to manually
call for help. This would mean shorter delays that,
according
to the Group Leader, could produce qualitative and
economicbenefits by reducing the likelihood of permanent
functional
impairments among seniors. . . [Interview 4, 2006].
Less expected was the fact that seniors were more likely
to wear their monitor, because, they realize that staff
could
tell if they were not, unlike with the previous untraceable
alarms. According to the Home-helpers, the seniors them-
selves appreciated this function as they are aware of their
tendency to forget to wear their alarmsand thereducedsafety
this implies in cases of incidents such as fall accidents.
This
function also reassured both staff and relatives and was
seen
as economically important for the service because usually
the relatives apply for nursing home placements. . . [Group
Leader, Meeting, 2006]. Interviewees also reported the abil-ity
for early client interventions and congruent with The
Managers initial visionto provide new customized services
that could lead to an improved general health status of the
seniors. However, not all section managers shared this
vision
considering the provision of such services economically
unvi-
able. One of them remarked: . . .we do not have capacity to
address all seniors sleeping and activity disorders. . . This
is
beyond our commitment. . . we will suffer increased produc-
tion costs. . .without being reimbursed for this. . . [Manager
2,
Interview 10, 2006].
Hence, during the study period Home-helpers responded
immediately to emergency callsbut were hesitantto intervene
in the non-urgent reports. They had ideas about how to act
on
the non-urgency activity data but found it difficult to
realize
such ideas.
-
8/7/2019 New E-Service Development in the Home Care Sector:
Beyond Implementing a Radical Technology
7/11
Author's personal copy
684 i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i
n f o r m a t i c s 7 7 ( 2 0 0 8 ) 6 7 9 6 8 8
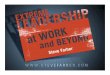
Fig. 2 The major issues in radical ICT services development.
4. Discussion
Thisresearch illustrates thatinnovatingservicesbased on new
radical technology is a complex and multidimensional
under-taking. Not all of the issues that arose were expected
and
participants in this research dealt with them in a variety
of
ways. Some of the issues emerged because of lack of through
decision-making and planning by management and otherper-
sonal. The major issues are presented in Fig. 2 in which the
stages are depicted in the observed rather than an ideal
order.
The project studied began with comprehension and
adoption [37] as the managers took the essential first step
when learning about the new available technologies. The
lack of involvement of the front-line home-help employees
in this phase was unfortunate and ultimately damaging to
the project, as they could have provided crucial insights
into
operational specifics of the organization. The elderly
clientsand their family were similarly excluded from the
decision-
making in the comprehension and adoption phase, contrary to
recommendations in the literature [30,31,47,48]. Instead,
the
managers selected andadopteda new technology on thebasis
of the vendor-claimed benefits. They assumed that benefits
would emerge in use.
The managers did not participate in the implementation
although this phase involves many crucial decisions. Indeed,
although the managers selected an intelligent technology,
which included many automated functions, providing the
monitoring service required the execution of several human
tasks. Someone needed to design the human service elements,
that is, they needed to formulate the complete service pro-cess
with routines for how to use the technology and so forth.
This instead was delegated to the operational personnel, who
developed some new informal routines (or service elements).
This implied incremental rather than radical change in the
existing service processes. Further, these changes were not
transformed into routines and assimilated.
These results need to be understood in light of how theproject
commenced. As the elderly care recipients were not
involved in the first phase, their needs and possible user
roles
were overlooked in the selection of the system. It is impor-
tant to recognize that another technology would perhaps have
been selected had the seniors and their family been involved
in the first place. In general, the needs of the consumer
were
not central and did not guide the project studied. There was
only a diffuse managerial wish to improve the effectiveness
of
care. As a result, there was a lack of direction and the
target
group for whom the service was being developed was unclear.
It is also important to question why considering that the
monitoring technology was installed only modest service
changes were achieved in this study. This answer to this liesin
the failure to reengineer the organization to accommodate
for the possibilities inherent in the newtechnology. In
general,
there were several conflicts between the action made
possible
by the technology on the one hand, and the activity allowed
by prevailing systems on the other. For example, the
technol-
ogy enabled the provision of customized services based on
real time data about the consumer. To realize this
potential,
front-line employee must possess the power to continuously
adjust the services they provide. In the care setting
studied,
this would require giving the Home-helpers the authority to
change theirschedule and the content of the servicesthey
pro-
vide on basis of thelatest consumerdataavailable. This is
far
from todays situation in the Swedish National Health
System,where the Home-helperscannot make anychangesin situ, but
have to defer to the social workers decisions about what
ser-
-
8/7/2019 New E-Service Development in the Home Care Sector:
Beyond Implementing a Radical Technology
8/11
Author's personal copy
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f
o r m a t i c s 7 7 ( 2 0 0 8 ) 6 7 9 6 8 8 685
vices are to be provided to what seniors. These conditions
are
contingent on the prevailing hierarchical system of author-
ity and the financial reimbursement system. There is nothing
a regional care manager can change in this. Hence, issues
related to the national health system impeded the effective
integration of the new technology in existing practice.
Thepresence of structures served as a barrier to radical
service
innovation in this context [10].
Not only the presence but also the absence of systems
impeded a constructive development of new services in the
setting studied. Guidelines and criteria for the use of the
monitoring system were not developed and quality assurance
systems were not in place. Important in this context is
defin-
ingwho should be made accountableif themonitoring system
is deliberately misused, or leads to negative effects in
unpre-
dictable ways.
The findings in this study illustrate that the lack of
infor-
mation provided to consumers about their user role could
threaten their safety. To manage risk effectively,
accountabil-ity for such unintended but negative consequences must
be
established; is it the responsibility of front-line
employees,
the managers or the technology vendor? Further, to ensure
fairness in public service delivery it is important to define
the
criteria that should be used by the social workers when
deter-
mining which seniors are eligible for the new service. Such
criteria were not developed during the study period. This is
related to the fact that theneedto whichthe new monitoring
service actually responds was not clear.
There were further conflicts between the technological
possibilities and the needs and preferences of the senior
con-
sumers. More specifically, the workers struggled with
bridging
the gap between
whatthe technology could monitor andthe seniorsconcern
about privacy,
the possibilities for preventive careand earlystage response
to health changes and the risk of exaggerating the impor-
tance of such changes leading to seniors excessively
worrying about their health and
the actual capability of the technology and seniors inappro-
priate expectations of the technology.
The development process studied began with the man-
agers making a new technical resource available to their
personnel. This approach may have its merits as it
enablesexperiential learning and enhances the chances of the
orga-
nization staying open to the unforeseen potential of the
new resource [22]. Indeed, unexpected possibilities emerged.
However, the managers in this case failed to recognize that
selecting and implementing a radical new technology is not
the same as producing a radically new service innovation.
Hence, the operational employees had to bridge the gap
between the new technology and the new service. This is not
necessarily negative; involving the operational personnel in
the service process innovation is in line with the
literature
[24,3234,5154].
However, contrary to the literature, in this study (and the
Swedish National Health System overall) the operational per-
sonnel were not given the power necessary to enforcechanges.
In general, there were no rewards or other incentives for
oper-
ational employees to innovate new services into their
setting.
Home-helpers were not encouraged to be creative and explore
new models of care delivery partly due to a fear for harm-
ing the consumers and possible legal consequences. In short,
there was no climate for innovation as described in the
litera-
ture [3234]. These factors are very likely to have affected
thedevelopment process performance.
This study lends support to other work that has argued
that in practice telehealthcare systems are highly
problematic
and demand that the organization of care work is radically
re-engineered [10]. Other scholars have also underlined the
need for adjusting technology to existing ways of organizing
care work, andvice versa, andpointed to the practical
difficul-
ties that it poses for care personnel [10,17,21,49,50,55]. In
the
project studied the need to make various design choices were
brought to the fore, to operational personnel as well as
man-
agers(see Fig. 2). Much work remains to effectivelymake
these
decisions. Hence, the development project can be describedas
a learning process andit is difficult to categorize the project
asa success or failure atthisstage. InZoe Stavri and Ash [56]
par-
ticipantsdefine successful IT implementations as those where
the system is accepted and remains operational. According
to this modest definition, the project discussed here was
not
a failure. The organization continues to work with the new
technology and as a result valuable learning for the sector
has resulted. Their perseverance will see this continue in
the
future.
5. Conclusion
This study explores the constituents of and issues involvedin
the development of new technology-based care services in
the long-term elderly care setting. The framework developed
for this project and inspired by insights from the normative
medical informatics, service management and information
systems literature quickly demonstratedthat the project
stud-
ied deviated from the ideal model in several ways. This
had vast implications on what new service processes could
be developed. Although a technology enabling quite radical
changes was used, only incremental changes in care work
were realized.
This paper identifies several reasons for such deviance and
modest result. The presence of national hierarchical deci-
sion systems and rigid financial reimbursement systems
areimportant here. As is the absence of quality assurance and
accountability systems related to theuse of IT in service
deliv-
ery. Most importantly, the paper highlights that there is no
innovation friendly climate in the public long-term elderly
care setting in Sweden. What dominates the care managers
agenda is rather an ambition to survive financially.
The managers appeared to have little knowledge about
change management and further, there was no research and
development department who had the financial resources,
competence and authority to formulate a service concept.
Therefore no one undertookto identify latent consumerneeds
or to develop a technology-based solution that satisfies
these
needs. Indeed, while the community care providers may have
been aware of the problems, they possessed little knowledge
about how technology could be used to solve them.
-
8/7/2019 New E-Service Development in the Home Care Sector:
Beyond Implementing a Radical Technology
9/11
Author's personal copy
686 i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i
n f o r m a t i c s 7 7 ( 2 0 0 8 ) 6 7 9 6 8 8
In these kinds of projects, it might be expected that
development process start with care providers learning from
technology providers and trialing existing technologies.
Yet,
it is important to recognize that this leads to a
technology-
oriented rather than user-needs driven approach. In order
for truly innovative and effective IT-based care services
todevelop, operational employees and clients need a much
more salient role in development projects. Further, opera-
tional employees need to be empowered. This in turn requires
political decisions about changes in the National Health
Ser-
vice delivery structure and new kinds of competences.
5.1. Study limitations and research suggestions
This study illustrates the innovation process observed in
one
case with a particular technology used in the particular
set-
ting and so the findings reported here cannot be
generalized.
Theorganizationstudiedfaced challenges related to thepublic
reimbursement system, and the centralized decision hierar-
chy characterizing the Swedish public care system. Private
firms obviously operate under completely different condi-
tions. The development of preventive care services added to
the challenges in the situation studied here. As did the use
of
a radical technology in the community care setting, which is
far from computerized.
While this study does not offer definitive answers related
to the innovation of technology-based services, it
doesprovide
insights, an in-depth account of the organizations struggles
to
implement a high technology solution into a low technology
setting and this experience may no doubt resonate with expe-
riences in other settings. Most importantly though it
reports
the learning and knowledge gained during this challenging
process. The lessons learned here will be valuable for other
care providers if they are to avoid the pitfalls experienced
by
theactors in this study. It will also improve thechancesfor
the
successful deployment of innovative information technology
into new models of service delivery.
This study may further inspire othersto investigatethe rel-
evance of the model presented as Fig. 2 in contexts other
than
the public care setting studied in this paper. This is needed
in
order to advance and further validate the model to prove its
suitability to underpin the use of technology into the home-
care sector. This is fundamental to successful Smart Home
innovations and deployments wherever they take place. With-
out a workable model it seems that these innovations will
fail.
What emerge from this study are several other questions
that need to be answered by further research.
From the organizational perspective:
How can public healthcare organizations become more
innovation oriented?
What does an innovation-friendly climate imply in the
public care setting?
And concerning the preferences and possible role of con-
sumers:
Is there necessarily a trade-off between the consumersperceived
privacy and safety when developing new care
services on basis of new digital consumer data?
Summary points
What was known before the study?
The interest in Telehomecare and Smart Home
technology is increasing as Governments world-wide plan for the
future healthcare needs of the
elderly.
New telehomecare technology in terms of hardware
and software is continuously emerging and gaining
attention as promising.
Studies have focused on demonstrating the technical
feasibility of specific applications rather than high-
lighting the role of telehomecare in care organizations
that is, the total picture is missing.
The medical informatics literature underlines the
importance of integrating technology into the organi-
zation but offers little guidance as regards how elderly
care providers can exploit technological advance-ments to
provide new care services.
What has the study added to the body of knowledge?
As Telehomecare applications can be used in sev-
eral different ways, understanding the technological
possibilities inherent in a telehomecare application
and installing new hardware and software are only
the first steps in the process of new care service
innovation.
Service innovation involves developing a sustainable
service concept, service process and service system.
Generally, if telehomecare technology complementrather than
supplement existing services, short-term
production costs will rise. Public care providers may
not be reimbursed for such increases in production
cost.
Hierarchical management structure where front-line
employees do not possess the authority to make
changes in the service content impedes the effective
use of real-time patient data generated by many mon-
itoring technologies.
Defining the user-role related to the care consumer
is necessary even in passive technologies, for example
sensor-based monitoring technologies still assumes
certain consumer behavior that needs to be clarified. Personnel
play an important role in using the technol-
ogy in ways that do not intrude on consumers privacy.
How can consumers be involved in the development of
new technology-based services?
How can the role of consumer in service settings, where
passive technologies with completely automated func-
tions are used, be mapped?
Finally, it is crucial that further research examines the
thorny
issues related to the use of technology in long-term elderlycare
in order to understand the promises and perils of these
new technologies.
-
8/7/2019 New E-Service Development in the Home Care Sector:
Beyond Implementing a Radical Technology
10/11
Author's personal copy
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f
o r m a t i c s 7 7 ( 2 0 0 8 ) 6 7 9 6 8 8 687
Acknowledgements
This work was partly supported by a grant from the Swedish
Kinnander foundation. The authors are further grateful for
constructive advice made by the editor and three
anonymousreviewers at the International Journal of Medical
Informatics
Journal.
A.E. initiated and designed the study, formulated the theo-
retical framework and collected the data in Sweden. A.E. and
M.C. were involved in the data analysis phase, as well as in
the
drafting and revision of the paper.
Appendix A. Interview guide
To managers:
How did you decide to invest in this particular technology?Who
did you engage in the decision phase?
Why?
What was problematic in this first stage?
What wasyourintention at this stage?Vision?(whatbenefits
did you foresee at this stage)
How did the project proceed?
Has your vision been realized?
What have you learned?
If it would be up to you to decide, would you recommend a
continued use of the technology?
Why?
How would you explain the results at this stage?
To Home-helpers:
What do you think of the new technology?
How many times per week have you used it, and for how
long?
How have you used it?
Why have you used it in this way?
Has it been difficult?
Did you use all functions/features possible in the applica-
tion?
Why did you not use certain features?
If it would be up to you to decide, would you recommend a
continued use of the technology?Why?
What benefits can the technology produce from your view-
point?
r e f e r e n c e s
[1] Organisation for Economic Co-Operation and
Development,Matching supply with demand for the services of
physiciansand nurses, in: Towards High-performing Health
Systems,OECD Policy Studies, Paris, 2004.
[2] R. Haux, E. Ammenwerth, W. Herzog, P. Knaup, Health care
in the information society. A prognosis for the year 2013,
Int.J. Med. Informat. 66 (2002) 321.[3] G. Demiris, Electronic home
healthcare. Concepts and
challenges, Int. J. Electronic Healthcare 1 (1) (2004) 116.
[4] R. Dixon-Hughes, Business planning and architectures, in:M.
Conrick (Ed.), Health Informatics: TransformingHealthcare with
Technology, Thompson/Social SciencePress, Melbourne, 2006.
[5] M. Hebert, B. Korabek, R. Scott, Moving research
intopractice: a decision framework for integratinghometelehealth
into chronic illness care, Int. J. Med.Informat. 75 (2006)
786794.
[6] S. Koch, Home telehealthcurrent state and future trends,Int.
J. Med. Informat. 75 (8) (2006) 565576.
[7] J. Arts, V. Peel, G. Wright, Organizational issue sin
heathinformatics: a model approach, Int. J. Med. Informat. 52(1998)
235242.
[8] B. Kaplan, N. Shaw. People, organizational and social
issues:evaluation as an Exemplar, in: R. Haux, Kulikowski
(Eds.),Yearbook of Medical Informatics, 2002, pp. 91102.
[9] M.M. Yousof, A. Papazafeiropoulou, R.J. Paul, L.K.
Stergioulas,Investigating evaluation frameworks for health
informationsystems, Int. J. Med. Informat. 77 (6) (2007)
377385.
[10] C. May, R. Harrison, A. MacFarlane, T. Williams, F. Mair,
P.Wallace, Why do telemedicine systems fail to normalize asstable
models of service delivery? J. Telemed. Telecare 9 (1)(2003)
2526.
[11] M. Berg, Patients and professionals in the
informationsociety: what might keep us awake in 2013, Int. J.
Med.Informat. 66 (2002) 3137.
[12] C. May, N.T. Ellis, When protocols fail: technical
evaluation,biomedical knowledge, and the social production of
factsabout a telemedicine clinic, Social Sci. Med. 53
(2001)9891002.
[13] M. Berg, Patient care information systems and
healthcarework: a sociotechnical approach, Int. J. Med. Informat.
55(1999) 87101.
[14] B. Stanberry, Telemedicine: barriers and opportunities in
the21st century, J. Intern. Med. 247 (2000) 615628.
[15] T. Schabetsberger, E. Ammenwerth, S. Andreatta, G. Gratl,
R.Haux, G. Lechleitner, K. Schindelwig, C. Stark, R. Vogl,
I.Wilhelmy, et al., From a paper-based transmission ofdischarge
summaries to electronic communication in healthcare regions, Int.
J. Med. Informat. 75 (2006) 209215.
[16] P. Knaup, R. Haux, A. Haber, A. Lagermann, F.
Leiner,Teaching the fundamentals of information systemsmanagement
in healthcare. Lecture and practical trainingfor students of
Medical Informatics (Heidelberg/Heilbronn),Int. J. Med. Informat.
50 (1998) 195206.
[17] A. Winter, E. Ammenwerth, O.J. Bott, B. Brigl, A. Buchauer,
S.Graber, A. Grant, A. Haber, W. Hasselbring, R. Haux, A.Heinrich,
H. Janssen, I. Kock, O.-S. Penger, H. Prokosch, A.Terstappen, A.
Winter, Strategic information managementplans: the basis for
systematic information management in
hospitals, Int. J. Med. Informat. 64 (2001) 99109.[18] J. Ash,
M. Berg, Report of conference Track 4: socio-technicalissues of
HIS, Int. J. Med. Informat. 69 (2003) 205306.
[19] J.S. Ash, P. Zoe Stavri, R. Kykstra, L. Fournier,
Implementingcomputerized physician order entry: the importance
ofspecial people, Int. J. Med. Informat. 69 (2003) 235250.
[20] N.M. Lorenzi, IMIA Working Group 13: organizational
impactof medical informatics, Int. J. Med. Informat. 56
(1999)58.
[21] C. May, M. Mort, F. Mair, T. Williams, Factors affecting
theadoption of telehealthcare in the United Kingdom: thepolicy
context and the problem of evidence, HealthInformat. J. 7 (2001)
131134.
[22] G. Zaltman, R. Duncan, J. Holbek, Innovations
andOrganizations, Wiley, 1973.
[23] R. Daft, A dual-core model of organizational
innovation,Acad. Manage. J. 21 (2) (1978) 193210.[24] B.
Edvardsson, J. Olsson, Key concepts for new service
development, Service Ind. J. 16 (2) (1996) 140164.
-
8/7/2019 New E-Service Development in the Home Care Sector:
Beyond Implementing a Radical Technology
11/11
Author's personal copy
688 i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i
n f o r m a t i c s 7 7 ( 2 0 0 8 ) 6 7 9 6 8 8
[25] A. Smith, M. Fischbacher, New service development:
astakeholder perspective, Eur. J. Market. 39 (9/10)
(2005)10251048.
[26] A. van Riel, Service innovation management, Manag.
ServiceQual. 15 (6) (2005) 493495.
[27] S. Johnson, L. Menor, A. Roth, R. Chase, A critical
evaluationof the new service development process. New
ServiceDevelopment: Creating Memorable Experiences, Sage,Thousand
Oaks, CA, 2000, pp. 132.
[28] C. Lovelock, Developing and implementing new
services.Developing New Services, American Marketing
Association,Chicago, IL, 1984, pp. 4464.
[29] F. Syson, H. Perks, New service development: a
networkperspective, J. Services Market. 18 (4) (2004) 255266.
[30] E. Von Hippel, Economic of product development by users:the
impact of sticky local information, Manage. Sci. 44 (5)(1998)
629644.
[31] P. Kristensson, A. Gustafsson, T. Archer, Harnessing
thecreative potential among users, J. Product. Innovat. Manage.21
(2004) 414.
[32] R. Cooper, C. Easingwood, S. Edgett, E. Kleinschmidt,
C.Storey, What distinguishes the top performing new productsin
financial services, J. Product. Innovat. Manage. 11 (4)(1994)
281299.
[33] J. de Jong, P. Vermulen, Organizing successful new
servicedevelopment: a literature review, Manage. Decis. 41 (9)
(2003)844858.
[34] D. Kelly, C. Storey, New service development:
initiationstrategies, Int. J. Service Ind. Manage. 11 (1)
(2000)4562.
[35] W.J. Orlikowski, D. Robey, Information technology and
thestructure of organizations, Informat. Syst. Res. 2 (2)
(1991)143169.
[36] E. Swanson, Information systems innovation
amongorganizations, Manage. Sci. 40 (9) (1994) 10691092.
[37] E. Swanson, N. Ramiller, Innovating mindfully
withinformation technology, MIS Quart. 28 (4) (2004) 553583.[38]
E.M. Rogers, Diffusion of Innovations, The Free Press, New
York, 1995.[39] W. Bijker, The social construction of Bakelite:
toward a
theory of invention. The Social Construction ofTechnological
Systems, 1987, pp. 159187.
[40] R. Yin, Case Study Research: Design and Methods,
SagePublications Inc., Thousand Oaks, 2003.
[41] M. Patton, Qualitative Research and Evaluation Methods,
4thed., Sage, London, 2004.
[42] B. Kjellen, S. Soderman. Praktikfallsmetodik.
LiberLaromedel, Stockholm, 9180.
[43] G. Wallen, Vetenskapsteori och
forskningsmetodik,Studentlitteratur, Lund, 1993.
[44] M. Alvesson, K. Skoldberg, Tolkning och
reflektion:vetenskapsfilosofi och kvalitativ metod, 2nd
ed.,Studentlitteratur, Lund, 2006.
[45] B. Glaser, A. Strauss, The Discovery of Grounded
Theory:Strategies for Qualitative Research, Aldine,
Chicago,1967.
[47] Gapp, R Change Management, in: M. Conrick (Ed.),
HealthInformatics: Transforming Healthcare with
Technology,Thompson/Social Science Press, Melbourne, 2006,
pp.154168.
[48] M. Conrick, C. Cameron, Leadership and Management, in:
M.Conrick (Ed.), Health Informatics: Transforming Healthcarewith
Technology, Thompson/Social Science Press,Melbourne, 2006.
[49] C. May, L. Gast, T. Atkinson, N. Ellis, F. Mair, A.
Esmail,Resisting and promoting new technologies in
clinicalpractice: the case of telepsychiatry, Social Sci. Med. 52
(2001)18891901.
[50] B. Kaplan, Addressing organizational issues into
theevaluation of medical systems, JAMIA 4 (2) (1997) 94101.1.
[51] A. Johne, C. Storey, New service development: a review
ofthe literature and annotated bibliography, Eur. J. Market.
32(3/4) (1998) 184251.
[52] L.J. Menor, M.V. Tatikonda, S.E. Sampson, New
servicedevelopment: areas for exploitation and exploration,
J.Operat. Manage. 20 (2) (2002) 135157.
[53] W. Dolfsma, The process of new servicedevelopmentissues of
formalization and appropriability,Int. J. Innovat. Manage. 8 (3)
(2004) 319337.
[54] E. Stevens, S. Dimitriadis, Managing the new
servicedevelopment process: towards a systemic model, Eur.
J.Market. 39 (1/2) (2005) 175198.
[55] E. Ammenwerth, S. Graber, G. Herrmann, T. Burkle, J.
Konig,Evaluation of health information systemsproblems
andchallenges, Int. J. Med. Informat. 71 (2003) 125135.
[56] P. Zoe Stavri, J.S. Ash, Does failure breed success:
narrativeanalysis of stories about computerized provider order
entry,Int. J. Med. Informat. (2003) 1572.